lyn's drug study
TRANSCRIPT
8/9/2019 Lyn's Drug Study
http://slidepdf.com/reader/full/lyns-drug-study 1/2
DD RR UU GG SS TT UU DD Y Y
PPREPAREDREPARED BY BY :: NNALMALYNALMALYN S. SS. SHALIMHALIM, BSN III – NCM 101, B, G, BSN III – NCM 101, B, GROUPROUP # 8# 8
Drug(Generic Name,Dosage, Route,
Frequency &Indication)
BrandName
PharmacologicAction of the
Drug
Adverse/SideEffects of Drug
Contrain-dications
NursingResponsibiities/Preca
ons
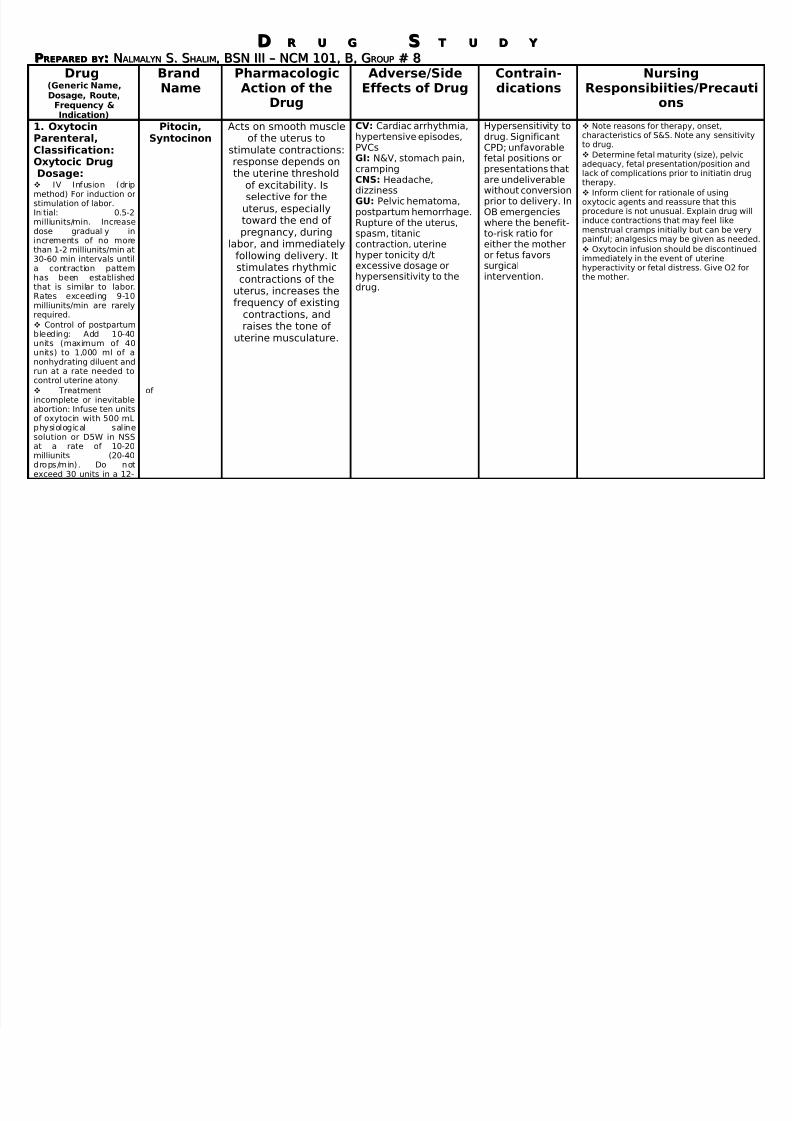
1. Oxytocin
Parenteral,Classification:Oxytocic DrugDosage: IV Infusion (dripmethod) For induction orstimulation of labor.Initial: 0.5-2milliunits/min. Increasedose gradually inincrements of no morethan 1-2 milliunits/min at30-60 min intervals untila contraction pattern
has been establishedthat is similar to labor.Rates exceeding 9-10milliunits/min are rarelyrequired.
Control of postpartumbleeding: Add 10-40units (maximum of 40units) to 1,000 ml of anonhydrating diluent andrun at a rate needed tocontrol uterine atony.
Treatment of incomplete or inevitableabortion: Infuse ten unitsof oxytocin with 500 mLphysiological salinesolution or D5W in NSSat a rate of 10-20milliunits (20-40drops/min). Do notexceed 30 units in a 12-
Pitocin,
Syntocinon
Acts on smooth muscle
of the uterus tostimulate contractions:response depends onthe uterine threshold
of excitability. Isselective for the
uterus, especiallytoward the end of pregnancy, during
labor, and immediatelyfollowing delivery. Itstimulates rhythmic
contractions of theuterus, increases thefrequency of existing
contractions, andraises the tone of
uterine musculature.
CV: Cardiac arrhythmia,
hypertensive episodes,PVCsGI: N&V, stomach pain,crampingCNS: Headache,dizzinessGU: Pelvic hematoma,postpartum hemorrhage.Rupture of the uterus,spasm, titaniccontraction, uterinehyper tonicity d/texcessive dosage or
hypersensitivity to thedrug.
Hypersensitivity to
drug. SignificantCPD; unfavorablefetal positions orpresentations thatare undeliverablewithout conversionprior to delivery. InOB emergencieswhere the benefit-to-risk ratio foreither the motheror fetus favorssurgical
intervention.
Note reasons for therapy, onset,
characteristics of S&S. Note any sensto drug.
Determine fetal maturity (size), pelvadequacy, fetal presentation/position lack of complications prior to initiatin therapy.
Inform client for rationale of usingoxytocic agents and reassure that thisprocedure is not unusual. Explain druginduce contractions that may feel likemenstrual cramps initially but can be painful; analgesics may be given as n
Oxytocin infusion should be discontimmediately in the event of uterinehyperactivity or fetal distress. Give O2
the mother.

8/9/2019 Lyn's Drug Study
http://slidepdf.com/reader/full/lyns-drug-study 2/2
hr period due to risk of water intoxication.
2.MagnesiumSulfateClassification:Anticonvulsant,Laxative and
SalineDosage: Seizures associatedwith eclampsia: 10-14g.
To initiate therapy, 4gMagSul in water forinjection or 4-5g in 250ml of D5W or 0.9% NaClmay be given IV.
IV Infusion:Hypomagnesemia,severe: Adults: 5g(40mEq/L of D5Winjection of NaClinjection by slow infusion
over period of 3 hrs. Usecaution to preventexceeding renalexcretory capacity.
3.
Epsom Salts It is an essential
element for musclecontraction, certain
enzyme systems, andnerve transmission.Extracellular fluid
levels: 1.5-2.5 mEq/L.Mg depresses the CNS
and controlsconvulsions by
blocking release of acetylcholine at themyoneural junction,
MagnesiumIntoxication: Cardiac & CNSdepression preceding
respiratory paralysis,circulatory collapse,depressed reflexes,flaccid paralysis,flushing, hypotension,sweating.CNS: DepressionCV: Flushing,hypotension, circulatorycollapse, depression of the myocardium.
In the presence of heart block ormyocardialdamage. Intoxemia or
pregnancy duringthe 2 hr prior todelivery.
Reserve IV use in eclampsia forimmediate control of life-threateningconvulsions. Give slowly to avoid prodhypermagnesemia.
With premature labor, continually asfetal heart rate, intensity and timing o
contractions. Before administering IV check for thconditions:- absent patellar reflexes- respirations below 16/min- urine output <100 ml in past 4 hr- early signs of hypermagnesemia:
flushing, sweating, hypotensionmhypothermia.
- Past history of heart block ormyocardial damage; prolonged Pwidened QRS intervals in ECG she