mabee-capa cxr workshop - amazon...
TRANSCRIPT

10/16/2012
1
Basic Radiology:Chest X-Ray Fundamentals
John Mabee, PhD, PA-CAssistant Professor Clinical Family Medicine
Keck School of Medicine of USCDivision of Physician Assistant Studies
Primary Care Physician Assistant ProgramOctober 4, 2012
BASI
CS
http://www.med-ed.virginia.edu
Underpenetrated
Exposure
BASI
CS
Overpenetrated
http://www.med-ed.virginia.edu
Exposure
BASI
CS http://www.med-ed.virginia.edu
Rotation
http://www.med-ed.virginia.edu

10/16/2012
2
BASI
CS
T-spine disc spaces barely visible thru heartBronchovascular structures seen thru heart
Diaphragm: 8th-10th posterior or 5th-6th anterior rib
12
345
6
7
8
9
10
11
1
2
3
4
5
6
http://www.med-ed.virginia.edu
PAView
Sternum should be seen edge onSpine darkens as you move caudally
Posteriorly, you should see 2 sets of ribs
BASI
CS
http://www.med-ed.virginia.edu
LateralView
BASI
CS
KeyLandmarks
Horizontal fissureparallels 4th rib
Oblique fissuresparallel 5 - 6th ribs
4
5
6
BASI
CS

10/16/2012
3
BASI
CS
R RibsL Ribs
BASICS
• One approach to reading a CXR: - A: Airways- B: Bones- C: Cardiomediastinal silhouette- D: Diaphragm- E: Everything else (plus lungs!)
Selected CXR Findings & Case Demonstrations
Normal• A: Airways• B: Bones• C: Cardio-
mediastinalsilhouette
• D: Diaphragm• E: Everything
else (+lungs)

10/16/2012
4
Emphysema
• Bilateral diffuse hyperinflation, flattening of diaphragms, bullae
• Narrowing of the cardiac silhouette
EmphysemaDilated Airways
Emphysematous subpleural
spaces(“Blebs”)
• A 66-year old man is seen in the office for progressive shortness of breath for the past 2 months. He smokes 2 packs of cigarettes per day for the past 40 years. Physical examination shows pursed lip breathing, and mild curvature of the thoracic spine. Heart sounds are distant, but without murmur or gallop. Lung sounds are normal. Chest x-ray study is shown.
Case 1 Case 1En.wikipedia.orgwili/File:Emphysema2008.jpg

10/16/2012
5
Case 1En.wikipedia.orgwili/File:Emphysema2008.jpg
- Hyperinflation- Hyperlucency- Flattening of
the diaphragm- Narrowing of
the cardiacsilhouette
• Dx: Emphysema
Cardiome
galy
En.wikipedia.orgwiki/File:Cardiomegally.png
Normal: ≯ 50% of thoracic diameter
Pulmonary Edema• “Bat wing" pattern & air bronchograms
www.med-ed.virginia.edu
Pulmonary Edema• Cephalization of pulmonary vessels, Kerley B
(septal) lines, peribronchial cuffing
www.med-ed.virginia.edu www.med-ed.virginia.edu

10/16/2012
6
LVH & Pulmonary Edema
Alveolar Edema
Library.med.utah.edu/WebPath/webpath.html
Library.med.utah.edu/WebPath/webpath.html
• A 58-year old man is seen in the emergency department because of increasing dyspnea and orthopnea for the past 2 days. Vital signs: pulse 98, BP 132/84, respirations 22. Physical examination shows bilateral scattered rales, intermittent wheezes, and an S3. Chest x-ray study is shown.
Case 2
Case
2
- Cardiomegaly- Prominent
bilateralpulmonaryvasculature
- Cephalizationof vessels
- Kerley B lines
• Dx: Heart failure; pulmonary edema
Case 2

10/16/2012
7
• Airspaces filled with pus (pneumonia)or other fluid (inflammation, CA, blood)
• “Infiltrate”
• Usually no loss of lung volume
www.med-ed.virginia.edu
Consolidation
• Loss of the silhouette or lung/soft tissue interface caused by a mass or fluid in the normally air filled lung
Silhouette Sign
RML
Bronchopneumonia vs.Lobar Pneumonia
Bronchopneumonia Lobar Pneumonia
Inflammatory “infiltrate” (pus)
in alveoli ➙consolidation of
airspaces
Bronchopneumonia Lobar Pneumonia
Pneumonia: Gross Pathology
Library.med.utah.edu/WebPath/webpath.htmlLibrary.med.utah.edu/WebPath/webpath.html
10/16/2012
8
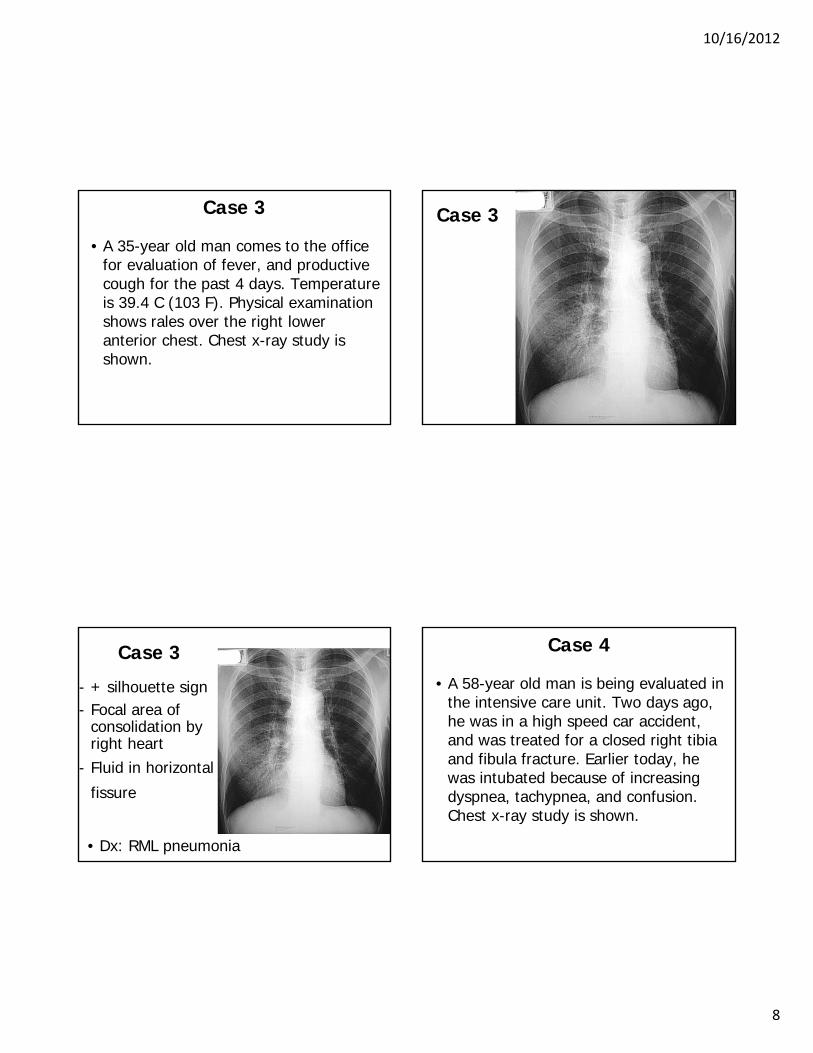
• A 35-year old man comes to the office for evaluation of fever, and productive cough for the past 4 days. Temperature is 39.4 C (103 F). Physical examination shows rales over the right lower anterior chest. Chest x-ray study is shown.
Case 3 Case 3
- + silhouette sign- Focal area of
consolidation byright heart
- Fluid in horizontal
fissure
• Dx: RML pneumonia
Case 3• A 58-year old man is being evaluated in
the intensive care unit. Two days ago, he was in a high speed car accident, and was treated for a closed right tibia and fibula fracture. Earlier today, he was intubated because of increasing dyspnea, tachypnea, and confusion. Chest x-ray study is shown.
Case 4

10/16/2012
9
Case 4- Diffuse
bilateralinfiltrates
- Appropriatepositioning ofET tube
• Dx: ARDS
Case 4
Mediastinum
Mediastinum: ≯ 8 cm
AorticKnob
PulmonaryArtery
Aorto-PulmonaryWindow
Mediastinal Mass
• Note aorto-pulmonary window

10/16/2012
10
Aortic Dissection
Library.med.utah.edu/WebPath/webpath.html
• A 68-year old man is seen in the emergency department because of sharp tearing chest pain radiating to the upper back that began 1 hour ago. He is lightheaded, and has nausea. Vital signs: pulse 80, BP 200/110, respirations 18. Physical examination shows grade II/VI diastolic murmur over the aortic area, and diminished pulses in both lower extremities. Chest x-ray study is shown.
Case 5
Case 5
- Mediastinalwidening
- Trachealshift
• Dx: Aortic dissection
Case 5
10/16/2012
11
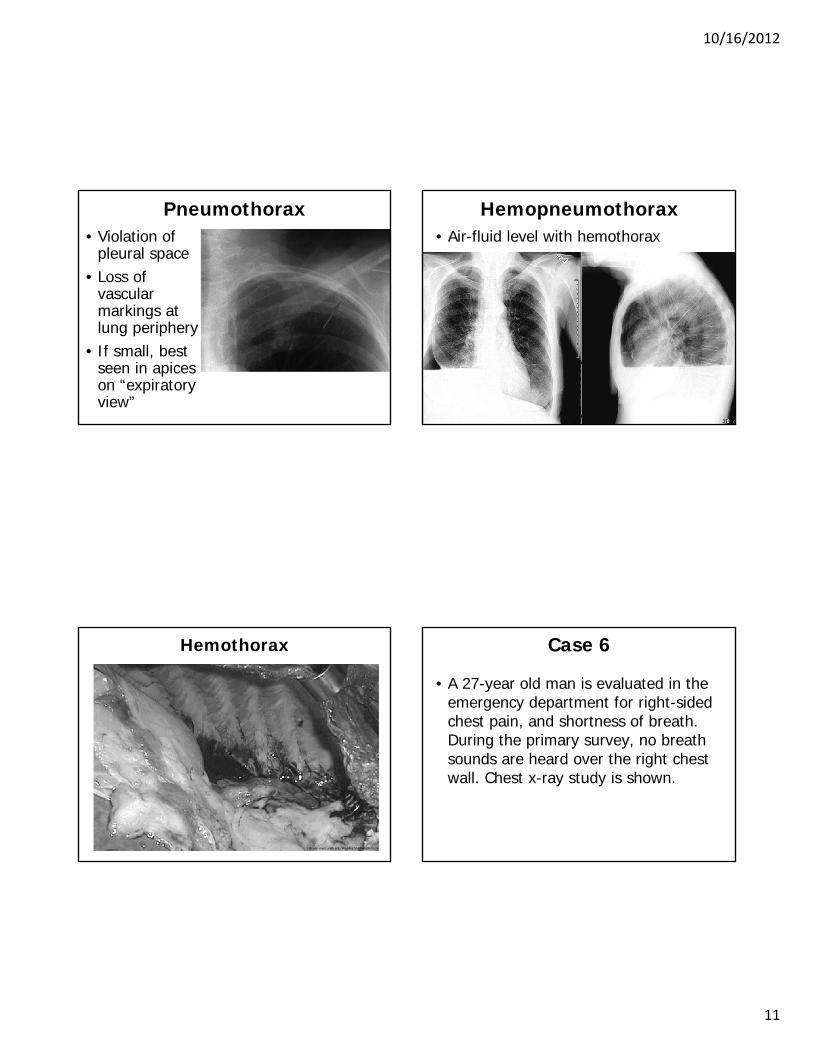
Pneumothorax• Violation of
pleural space• Loss of
vascular markings at lung periphery
• If small, best seen in apices on “expiratory view”
Hemopneumothorax• Air-fluid level with hemothorax
Hemothorax
Library.med.utah.edu/WebPath/webpath.html
• A 27-year old man is evaluated in the emergency department for right-sided chest pain, and shortness of breath. During the primary survey, no breath sounds are heard over the right chest wall. Chest x-ray study is shown.
Case 6

10/16/2012
12
Case
6
- Hyperlucentright hemithorax
- No lungmarkings
- Ipsilateral lungedge parallel tochest wall
• Dx: Pneumothorax
Case 6
Pleural Effusion• Fluid collection
in pleural space blunting of costophrenic
• Minimum vol:- 250 mL onPA view
- 75 mL on lateral view www.yale.edu/imaging
Pleural Effusion• Lateral decubitus view fluid “layering”
10/16/2012
13
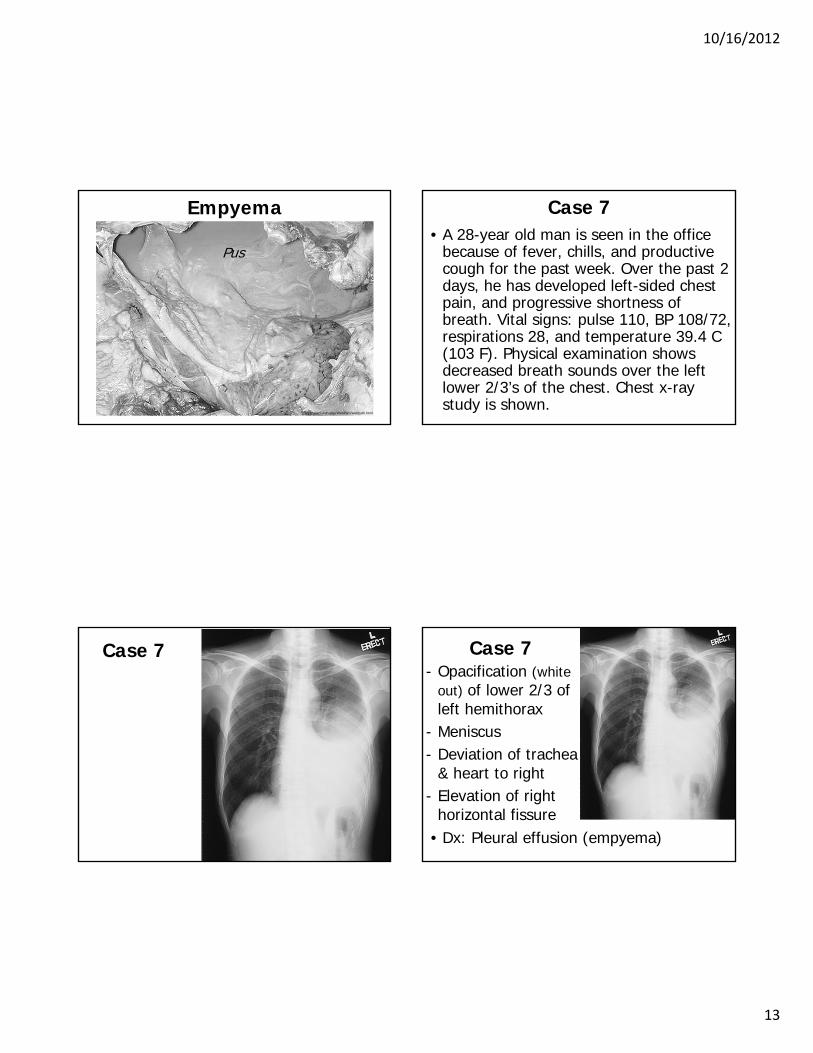
Empyema
Pus
Library.med.utah.edu/WebPath/webpath.html
• A 28-year old man is seen in the office because of fever, chills, and productive cough for the past week. Over the past 2 days, he has developed left-sided chest pain, and progressive shortness of breath. Vital signs: pulse 110, BP 108/72, respirations 28, and temperature 39.4 C (103 F). Physical examination shows decreased breath sounds over the left lower 2/3’s of the chest. Chest x-ray study is shown.
Case 7
Case 7- Opacification (white
out) of lower 2/3 ofleft hemithorax
- Meniscus- Deviation of trachea
& heart to right- Elevation of right
horizontal fissure• Dx: Pleural effusion (empyema)
Case 7

10/16/2012
14
Atelectasis• Collapse or incomplete expansion of
lung or lung segment • Characteristics:
- opacity of airless lobe (+ volume loss)- displacement of fissures, hilar &
cardiomediastinal structures towardside of collapse
- elevation of ipsilateral hemidiaphragm- lucency of aerated lung- silhouette sign
Atelecta
sis
RULRadiopaedia.org
RML
Atelectasis
En.wikipedia.org
Atelecta
sis
RLL

10/16/2012
15
Atelecta
sis
Radiopaedia.org
LUL
Atelecta
sis
LLL