machine learning is the next chapter of radiology, …...machine learning is the next chapter of...
TRANSCRIPT

Machine Learning is the Next Chapter of Radiology, Not the Last
RSNA 2018 Abstract Submissions Now Open — See Page 24
April 2018 Volume 28, Issue 4
A L S O I N S I D E :
Mobile Solutions Aid Radiologists Serving Rural U.S.
Link Between Renal Hypoxia and Coronary Disease
Gold Nanoparticles Aid Colorectal Cancer Treatment
RSNA ML Challenge Yields Winning Algorithm
John
s H
opki
ns U
nive
rsity
Sch
ool o
f Med
icin
e

UP FRONT 2 First Impression
2 Numbers in the News
Machine Learning is the Next Chapter of Radiology, Not the Last
RADIOLOGY’S FUTURE
16 R&E Foundation Donors
17 Your Donations in Action
7
Mobile Solutions Aid Radiologists Serving Rural America
14
RSNA ML Challenge Yields Winning Algorithm
12
Gold Nanoparticles Aid Colorectal Cancer Treatment
10
Link Shown Between Renal Hypoxia and Coronary Disease
FEATURES
4
APRIL 2018 • VOLUME 28, ISSUE 4
EDITOR
Gary J. Whitman, MD
R&E FOUNDATION CONTRIBUTING EDITOR
Theresa C. McLoud, MD
EXECUTIVE EDITOR
Shelley L. Taylor
MANAGING EDITOR
Beth Burmahl
STAFF WRITER
Jennifer Allyn
GRAPHIC DESIGNER
Eriona Baholli-Karasek
EDITORIAL ADVISORS
Mark G. Watson Executive Director
Karena Galvin Assistant Executive Director Marketing and International Affairs
Marijo Millette Director: Public Information and Communications
EDITORIAL BOARD
Gary J. Whitman, MD ChairmanVahid Yaghmai, MD Vice ChairmanEzra Bobo, MDStephen D. Brown, MDCarlo Catalano, MDDaniel A. Hamstra, MD, PhDMaureen P. Kohi, MDLaurie A. Loevner, MDTheresa C. McLoud, MDMartin P. Torriani, MDMary C. Mahoney, MDBoard Liaison
2018 RSNA BOARD OF DIRECTORS
James P. Borgstede, MD ChairmanMary C. Mahoney, MD Liaison for Publications and Communications Bruce G. Haffty, MD Liaison for ScienceMatthew A. Mauro, MD Liaison for EducationCurtis P. Langlotz, MD, PhD Liaison for Information Technology and Annual Meeting
Umar Mahmood, MD, PhDLiaison for International AffairsVijay M. Rao, MD PresidentValerie P. Jackson, MD President-Elect
Follow us for exclusive news, annual meeting offers and more!RSNA MISSION
The RSNA promotes excellence in patient care and healthcare delivery through education, research and technologic innovation.
NEWS YOU CAN USE
18 Journal Highlights
20 Radiology in Public Focus
21 Education and Funding Opportunities
23 Member Spotlight
23 Value of Membership
24 Annual Meeting Watch
25 RSNA.org

2 RSNA News | April 2018
FIRST IMPRESSION
Numbers in the News
60Number, in millions, of U.S. residents who live in rural areas, creating challenges for radiologists providing imaging services. Read more on Page 7.
250The number of participants in RSNA's first Machine Learning Challenge, result-ing in a winning alogrithm to predict pediatric bone age from hand x-rays. Read more on Page 14.
3Number of new education grants recently announced by the RSNA Research & Education (R&E) Founda-tion. Get more details on Page 17.
78 Percentage of patients who said they received infor-mation prior to an imaging exam in a recent study in Radiology. Read more on Page 20.
April 2018 • Volume 28, Issue 4 Published monthly by the Radiological Society of North America, Inc. 820 Jorie Blvd., Oak Brook, IL 60523-2251. Printed in the USA.
Postmaster: Send address corrections or changes to: RSNA News, 820 Jorie Blvd., Oak Brook, IL 60523-2251Non-member subscription rate is $20 per year; $10 of active members’ dues is allocated to a subscription of RSNA News.
LETTERS TO THE [email protected] 1-630-571-7837 fax
[email protected] 1-888-600-0064 1-630-590-7770
Contents of RSNA News copyrighted ©2018, RSNA. RSNA is a registered trademark of the Radiological Society of North America, Inc.
REPRINTS AND [email protected] 1-630-571-7829 1-630-590-7724 fax
[email protected] Lisa Lazzaretto Assistant Director: Corporate Relations 1-630-571-7818
Nominate Radiology Articles for the 2018 Margulis Award
The Nominating Committee for the Alexander R. Margulis Award for Scientific Excellence is accepting nominations from
readers for Radiology articles published between July 2017 and June 2018. The main selection criteria are scientific quality and originality. Email your nomination, including the article citation and a brief note highlighting the reasons for the nomination, to [email protected].
RSNA Introduces New Machine Learning Education
RSNA will offer a series of webinars on artificial intelligence to begin in July 2018 and be offered in regular intervals thereafter. Each webinar will be one hour, featuring two 20-minute speakers followed by a 20-minute question-and-answer session. A small registration fee will apply.
RSNA will also offer a new Spotlight Course on machine learning in Fall 2018 at a location to be determined. Watch RSNA.org/News for more information about these courses.
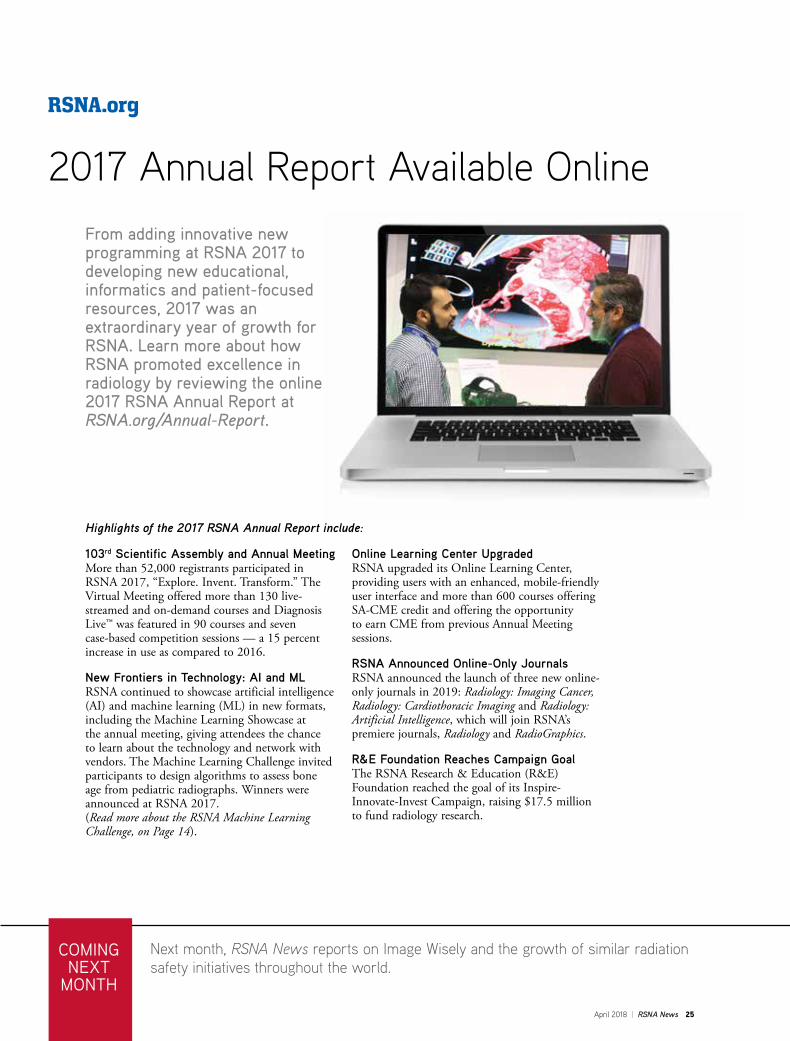
RSNA 2017 Annual Report Available Online
The RSNA 2017 Annual Report highlights the programs and activities that benefited members and the specialty in 2017. Along with annual meeting highlights, content includes the R&E Foundation’s Inspire-Innovate-Invest Campaign, upgrades to the Online Learning Center and the announcement of three new online journals.
Turn to Page 25 to read more highlights and access the entire report at RSNA.org/Annual-Report.
Nomination DeadlineJune 10
At RSNA 2017, Richard L. Ehman, MD, left, presented Walter H. Backes, PhD, with the Alexander R. Margulis Award for Scientific Excellence.

April 2018 | RSNA News 3
SIR Announces 2018 Gold Medal HonoreesGold medals were awarded to John A. Kaufman, MD, Renate L. Soulen, MD, and Karim Valji, MD, at the Society of Interventional Radiology (SIR) annual meeting held recently in Washington, DC.
A past president of SIR, Dr. Kaufman is the chair of the Department of Interventional Radiology, director of the Dotter Interventional Institute and the Frederick S. Keller Professor of Interventional Radiology at the Oregon Health and Science University, Portland. He served as chair of the RSNA Scientific Program Vascular and Interventional Subcommittee and as a plenary and session moderator at
previous RSNA annual meetings.
Dr. Soulen was a section chief at Temple University, Philadelphia, and a professor of radiology at Wayne State University, Detroit, until her retirement in 2005. She served as an RSNA second vice president and chair of the RSNA Scientific Program Cardiovascular Subcommittee as well as an associate editor on the Radiology Editorial Board.
Dr. Valji is a professor of radiology and chief of interventional radiology at the University of Washington, Seattle. He is a former member of the RSNA Scientific Program Vascular and Interventional Subcommittee.
ValjiSoulenKaufman
Register for RSNA Spotlight Course in Argentina The RSNA Spotlight Course will be held in Buenos Aires, Argentina, June 8-9. Presented entirely in Spanish, “Últimas Tendencias en Imágenes Abdominal” will focus on the latest trends in abdominal imaging. The course will include Diagnosis Live™ sessions, giving attendees the opportunity to test their knowledge and engage with renowned global leaders in abdominal imaging.
Space is limited and early registration is encouraged to take advantage of pre-booking rates. For more information and to register, visit RSNA.org/Spotlight.
Gold medals were awarded by the Asian Oceanic Society of Radiology during the recent 17th Asian Oceanian Congress of Radiology.
Rao Receives AOSR Gold MedalRSNA President, Vijay M. Rao, MD, received a gold medal from the Asian Oceanic Society of Radiology (AOSR) during the recent 17th Asian Oceanian Congress of Radiology (AOCR) and the 71st Annual Conference of the Indian Radiology and Imaging Association (IRIA) held in Mumbai, India.
Gold medals were also awarded to Yves M. Menu, MD, and Kazuro Sugimura, MD. Dr. Menu received RSNA honorary membership in 2011. Dr. Sugimura received RSNA honorary membership in 2010.
Dr. Rao also gave a keynote address, “Radiology: Present State and Future State,” during the congress. Dr. Rao has served on the RSNA Research & Education (R&E) Foundation Board of Trustees and currently serves on the RSNA Board of Directors.
The 2018 AOCR also spotlighted the RSNA/AOSR Symposium on multimodality imaging in head and neck cancer featuring speakers from each society discussing the issue.The RSNA-AOSR joint symposium will be repeated at RSNA 2018.
4 RSNA News | April 2018
Machine Learning is the Next Chapter of Radiology, Not the LastBY RICHARD DARGAN
Advancements in artificial intelligence (AI) have raised a new level of possibility for the future of radiology.
News stories herald the impending take-over of the profession by computers armed with machine learning (ML) software possessing the power to recognize patterns of disease that far exceeds that of humans. But leading radiology experts insist that such a takeover is unlikely; in fact, they suggest that ML and its more sophisticated subtype, deep learning (DL), will invigo-rate the profession and make radiologists more vital than ever to patient care.
“One reason radiology has been so suc-cessful is that we are constantly changing,” said Elliot K. Fishman, MD, professor of radiology and oncology at the Johns Hop-kins University School of Medicine in Bal-timore, MD. “If anything, deep learning will guarantee our survival.”
At Johns Hopkins, Dr. Fishman helps spearhead the Felix Project, a multi-year, multi-million-dollar effort to provide earlier detection of pancreatic cancer on imaging by developing computer algo-rithms to read CT scans.
During the first year-and-a-half of the project, named after a potion in the Harry Potter books, multi-disciplinary researchers (radiology, pathology, genetics, computer
vision), including ML expert Alan Yuille, PhD, used more than 1,000 representative normal scans to teach the computer to recognize the pancreas. For the second year, beginning last September, research-ers employed some 180 scans to begin to teach the computer to recognize pancreatic cancer.
Preliminary results of the program, which exploits the fact that computers are better than humans at picking up textural shape changes in organs, have been prom-ising.
“We are getting 60 to 70 percent accu-racy in pancreatic cancer detection on test cases,” Dr. Fishman said. “This is a program that could run on every single abdominal scan in the future and help with the early detection of pancreatic cancer."
Radiologists including Linda Chu, MD, Karen Horton, MD, and Satomi Kawa-moto, MD, were key to the development process, since the gold standard for AI is the radiologist. Each normal case and each case of pancreatic cancer takes approximately four hours to annotate. Without annotated data the task would be impossible.
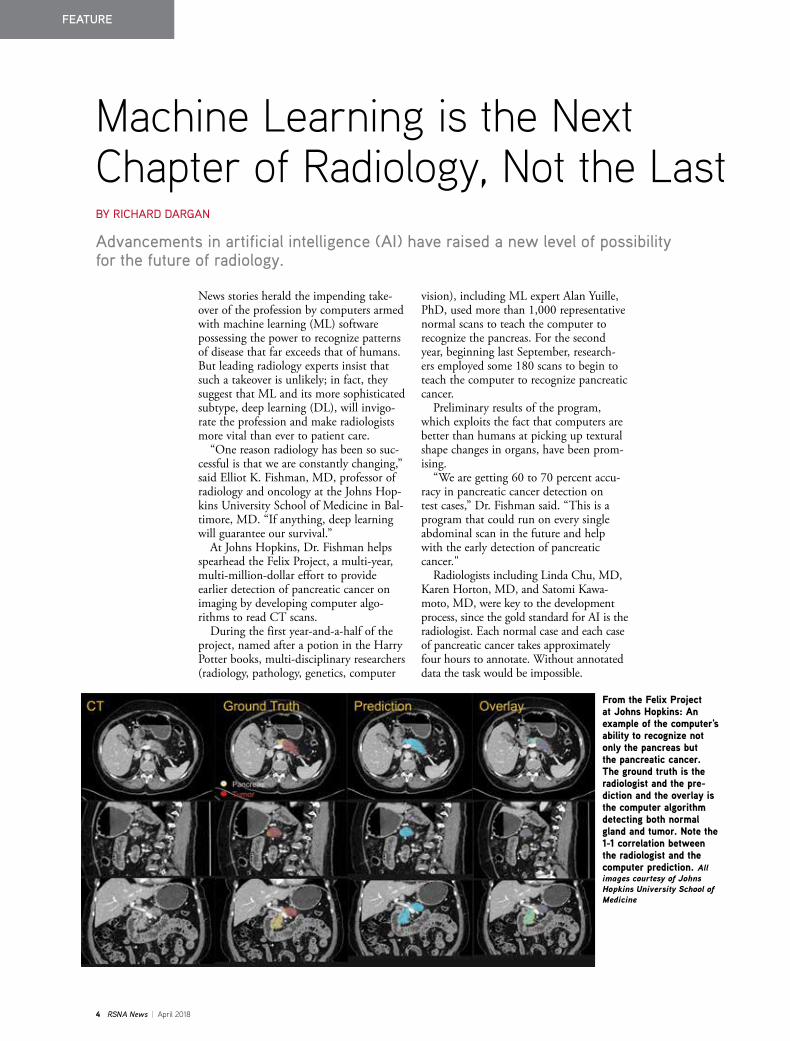
From the Felix Project at Johns Hopkins: An example of the computer's ability to recognize not only the pancreas but the pancreatic cancer. The ground truth is the radiologist and the pre-diction and the overlay is the computer algorithm detecting both normal gland and tumor. Note the 1-1 correlation between the radiologist and the computer prediction. All images courtesy of Johns Hopkins University School of Medicine
FEATURE
April 2018 | RSNA News 5
"Radiologists will play a key role in developing AI and making sure the final products meet our needs and the needs of our patients and referring clinicians," Dr. Fishman said.
AI Revolutionizing Radiology WorkflowRadiology workflow is another active area of AI research. Luciano M. Prevedello, MD, MPH, chief, division of medical imaging informatics and assistant professor of neu-roradiology at the Ohio State University Wexner Medical Center in Columbus, Ohio, served as lead author on a Decem-ber 2017 Radiology study that assessed the performance of an AI tool using a DL algorithm for detecting critical findings on head CT, such as hemorrhage, mass effect, hydrocephalus and stroke. (See Web Extras.)
Using more than 2,500 representative images to train the computer, Dr. Preve-dello and colleagues demonstrated that the tool could one day independently screen non-contrast head CT examinations and notify the interpreting radiologist of critical findings.
“The algorithm analyzes the data set and, if it detects a critical finding, sends it to the top of the list to be read,” said Dr. Preve-dello, who serves as chair of the Machine Learning Subcommittee of the RSNA
Radiology Informatics Committee. “The faster you recognize an important finding, the better it is for the patient.”
ML has some clear-cut advantages over humans. It provides more consistency, Dr. Prevedello said, and is not prone to fatigue, potentially reducing error rates.
“If we consider only things we can see, then radiologists perform at a very high level of accuracy,” he said. “But imaging data contains so much information, and computers can extract features from data in a way that would be very hard for humans to replicate.”
Signs of the feverish activity in the AI-ra-diology arena are everywhere. For example, 2017 saw FDA approval of a self-teaching artificial neural network to help physicians diagnose heart problems and software that provides AI-assisted stroke detection for CT scans and automatically notifies neurovascu-lar specialists by text message. A new smart-phone app uses algorithms based on millions of stored images to calculate the likelihood that a mole is becoming cancerous.
“In the past, this field was evolving at a linear pace, but now we may be getting into an exponential phase of growth,” Dr. Prevedello said. “This now has the attention of people from different backgrounds, and that is one of the many reasons why the evolution is different from before."
“With time, machine learning will become more and more sophisticated. In the future we will look back and say, ‘how were we able to do our job without these tools?'”
LUCIANO PREVEDELLO, MD, MPH
Continued on next page
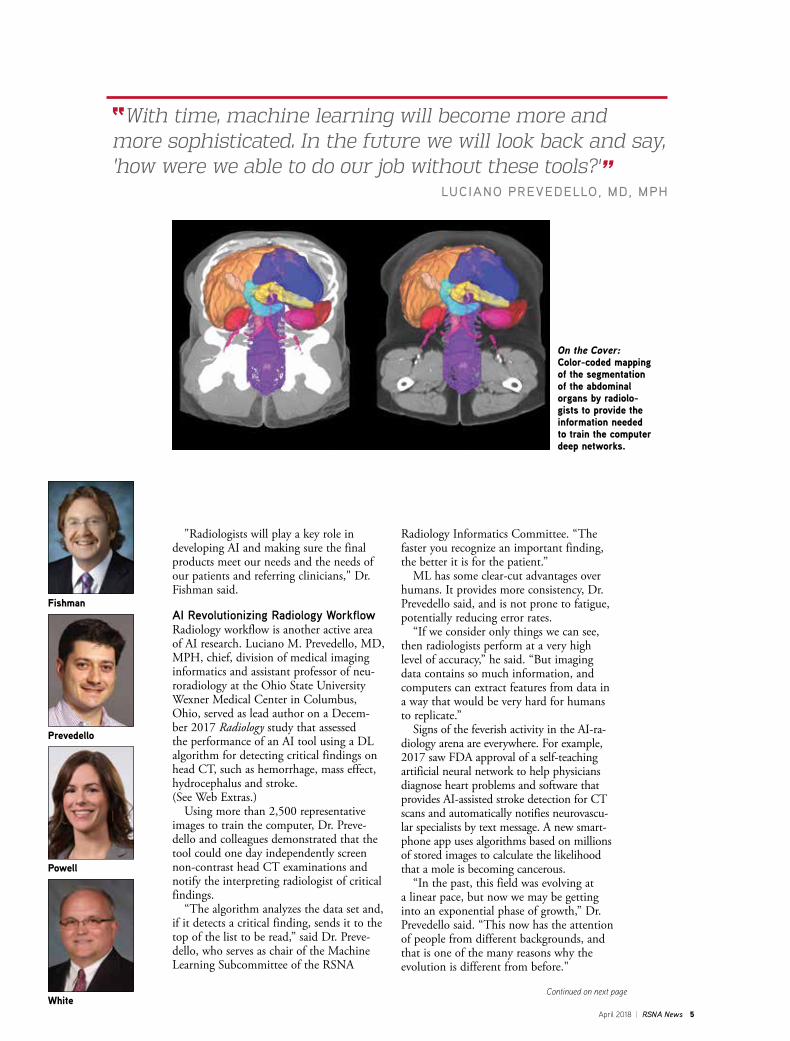
On the Cover: Color-coded mapping of the segmentation of the abdominal organs by radiolo-gists to provide the information needed to train the computer deep networks.
Fishman
Prevedello
Powell
White

6 RSNA News | April 2018
Embracing ML is Key to Radiology’s Future Kimberly Powell, vice president of health-care at NVIDIA, a leading technology company and AI provider, attributes this evolution to the accelerating pace of three developments: more data, better algo-rithms and faster computation.
“We are at a turning point where we can unlock useful applications to help with radiology workflow,” she said. “With the number of imaging exams increasing, radiologists can’t spend as much time on interpretation and AI provides immediate help with that.”
Not everyone is sanguine about these developments, however. There is anecdotal evidence that concern about the future obsolescence of radiology is affecting medical students considering careers in the field.
“The fear is definitely there,” Dr. Pre-vedello said. “My response is that there is no question what we do today is different from what we will do in 10 years, but I say this with a lot of excitement. I feel very strongly that the solution to fear is education, and that we as the radiology community should embrace and under-stand ML as much as we can.”
Richard D. White, MD, chair of the Department of Radiology at the Ohio State University, points out that these pivotal moments are no stranger to radiol-ogy and compares the rise of AI with the arrival of CT in the early 70s and MRI in the early 80s.
“When CT and MRI were introduced, they improved the view of anatomy and insights into tissue properties so much that people said radiologists would no lon-ger be needed," Dr. White said. "But these technologies actually drove the need for
even more imaging and more radiologists with greater knowledge who made bigger contributions. Likewise, this new tech-nology will provide ability to more com-fortably exclude disease and detect even more findings when disease is present. And someone will need to integrate this information for our patients. Our role as clinicians will be expanded and enhanced by this technology.”
While it is difficult to quantify overall trends in radiologists' interest and invest-ment in AI, the 2017 RSNA annual meet-ing offered evidence that more are getting the message.
There was a noticeable rise in atten-dance and interest at AI-related events at RSNA 2017 compared with the previous year. And RSNA’s first-ever Machine Learning Pavilion was packed with attendees at the 2017 meeting.
“There is an understanding in the radiology community that this technol-ogy will benefit everyone in a positive way,” Powell said. "Assisting radiologists with screening, prioritization and using algorithms to see what is difficult to the human eye are all ways AI will empower the profession of radiology."
Powell expects that over the next five years, ML will provide assistance for some of a radiologist’s simpler tasks. Beyond that, she envisions a paradigm shift, where radiologists no longer sit and type at com-puters but speak to instruments instead.
“The time they save will allow them to focus on the imaging that matters for patients,” Powell said.
Integrating ML with EducationEducation and training are critical to moving radiology into the AI age, experts say, and programs are already taking place to help smooth that transition. More than 1,000 radiologists, IT staffers and researchers attended the DL classroom presented by NVIDIA at RSNA 2017. But education must start even earlier, according to Dr. Prevedello.
“We have an obligation to make machine learning part of our medical student and radiology resident education to prepare for the future,” he said. “In the same way we learn about artifacts gen-erated by a defective detector on CT or noise in MRI, we will need to understand why an algorithm may produce unex-pected results."
And what about those radiologists who might not be sold on ML? They could find themselves in a vulnerable position, according to Dr. Fishman.
“If you’re a radiologist and you say, ‘I’m going to close my eyes and hope this [machine learning] will go away,’ you will end up being replaced,” he said. “On the other hand, if you say, ‘I will embrace this technology and use it,’ you will not only stay employed, you will end up improving patient care.”
“With time, machine learning will become more and more sophisticated,” added Dr. Prevedello. “In the future we will look back and say, ‘how were we able to do our job without these tools?’”
Continued from previous page
WEB EXTRAS Access the study, “Automated Critical Test Findings Identification and Online Notification System Using Artificial Intelligence in Imaging” at RSNA.org/Radiology.
In training the computer to detect the pancreas and eventually pancreatic tumors, the Johns Hopkins team also taught the computer an algorithm to rec-ognize all of the key abdominal structures, as shown in this multi-organ segmentation result of the abdomen.

April 2018 | RSNA News 7
Mobile Solutions Aid Radiologists Serving Rural America BY JENNIFER ALLYN
Imagine if an imaging appointment in the nearest big city with an academic medical center required a full day of travel or an expensive boat or plane trip. Now imagine the strain on your monthly budget due to these travel costs plus the medical expenses, especially if you do not have health insurance. For approximately 60 million people who live in rural areas of the U.S., these types of scenarios happen every day.
With barely a tenth of physicians prac-ticing in rural locations, according to the National Organization of State Offices of Rural Health, it can be easy for patients to skip routine imaging screenings, like mammograms, or put off more intensive imaging appointments that require travel to larger facilities.
While physician shortages in rural areas are not specific to radiology, they do bring unique challenges for radiol-ogists who want their patients to have routine screenings and keep important appointments.
Some radiologists are turning to mobile solutions to reach patients in far-flung areas across the U.S.
Lack of Health Insurance a Deterrent for Rural PatientsFor the past 15 years, the University of Virginia, Charlottesville, VA, has oper-ated a mobile mammography unit that brings comprehensive screening services
to women at workplaces and community locations throughout Virginia.
Along with proximity, one of the big-gest challenges facing patients in these rural locations is the lack of health insur-ance, according to Jennifer Harvey, MD, professor of radiology and medical imag-ing and division head, breast imaging, at the University of Virginia.
Dr. Harvey knows how prohibitive the lack of insurance can be when it comes to radiology services, especially mam-mography.
“Many rural residents have jobs that do not offer benefits or find that health insurance is unaffordable,” Dr. Harvey said. “Often, women put their fami-ly’s health needs above their own. As a university, we knew we could travel to these areas and provide women with the screenings that they need.”
Offering screenings free of charge, the mobile mammography unit provides 3-D tomosynthesis mammography and ultrasound, and travels 25 percent of the time to rural locations, usually three to four hours away from the university. The unit typically spends at least 48 hours in one area of the state, traveling between nearby cities. During its stay, 20-25 women are seen each day.
All images are uploaded to the uni-versity where Dr. Harvey and her team review them, sending results and addi-tional information back to the unit. Dr. Harvey and her team are studying the remote use of diagnostic mammography and ultrasound in these rural areas to evaluate whether this improves compli-ance after an abnormal mammogram.
Should a patient require a consultation with a university radiologist, Dr. Harvey said, they can do so during a teleconfer-ence on board the mammography truck.
Harvey
Prabhakar
Continued on next page
FEATURE

8 RSNA News | April 2018
FEATURE
“Much like an in-person meeting when there is something suspicious on an image, the patients can talk with a radiologist to ask questions and get infor-mation to help them make an informed decision,” Dr. Harvey said.
If there is a need for a patient to come into the hospital for additional services, that is discussed at that time as well.
“For many rural patients, taking the time out of their day to even visit the mobile unit is difficult. If there is some-thing abnormal on their scan, it can be challenging for women to travel to a larger medical facility, especially those who cannot afford to take a day off from work or don’t have the gas money to get there and back,” Dr. Harvey said. “We work with the patient’s schedule and even provide gas cards to help get patients to the necessary appointments.”
Because it is challenging for patients in rural locations to travel into the city, the university is currently looking into addi-tional types of medical services — radio-logic and other — that could be provided via the mobile van.
“We have been a steady presence in these communities for so long that we are trying to identify other health resources that are scarce in these rural areas that we might be able to provide,” Dr. Harvey said.
Weather a Factor in Reaching Patients in Difficult LocalesLack of health insurance does not play as big a role for people living on Nantucket, an island 30 miles off the east coast of Massachusetts. It is the potential for bad weather that can wreak havoc on medical care.
“Nantucket can have significant weather issues,” said Anand M. Prabha-kar, MD, assistant professor of radiol-ogy at Massachusetts General Hospital (MGH) in Boston. “Fog and wind are major concerns that have affected the ability of medical personnel to travel to the island and/or remove patients from the island.”
Dr. Prabhakar leads the diagnostic imaging operations at Nantucket Cottage Hospital, a 19-bed hospital on the island.
Once a week, he and a rotating group of MGH radiologists fly on a nine-seat plane over the Atlantic Ocean to the island. No radiologists live on the island, so Dr. Prabhakar travels there to provide fluoroscopy and select minimally invasive interventional procedures.
In addition to his travel to the island, Dr. Prabhakar and his colleagues at
“Many rural residents have jobs that do not offer benefits or find that health insurance is unaffordable. Often, women put their family’s health needs above their own. As a university, we knew we could travel to these areas and provide women with the screenings that they need.”
JENNIFER HARVEY, MD
The mobile mammography unit at the University of Virginia brings free, comprehensive imaging screening services to patients – many who lack health insurance – in rural areas throughout Virginia. Image courtesy of the University of Virginia Radiology and Medical Imaging.
Continued from previous page

April 2018 | RSNA News 9
MGH provide teleradiology reading and interpretation for the Nantucket Cottage Hospital 24 hours a day, seven days a week, when not onsite.
If a patient needs to be transferred off the island to MGH, it is conditional on the weather. At times, the Coast Guard is called in to assist during particularly foul weather. However, most transfers take place without incident.
These transfers are what interested Dr. Prabhakar to field a study, published in the American Journal of Emergency Medicine in 2016, to investigate the role that imaging played in transfers off the island.
He and his co-authors found that less than one in 30 emergency department patients at Nantucket Cottage Hospital required transfer for a higher level of care. Cardiac etiologies were the most
common reason for transfer to MGH. However, imaging only played a role in transfers for noncardiac-related events.
“Most patients were managed with-out needing services available at the higher care facility,” Dr. Prabhakar said. “While cardiac indications were the most common cause for transfer in the study, imaging did not play a major role in these transfers. Potential next steps would be to study whether or not imaging (such as coronary CTA) could reduce potentially unnecessary cardiac transfers.”
“No matter when or how we get to the island, time is well-spent there with the amazing team of physicians at the hospital and the appreciative Nantucket community, who have welcomed the imaging staff from MGH,” Dr. Prabhakar said.
Once a week, a group of radiologists from Massachusetts General Hospital (MGH) fly on a small plane to Nantucket Island to provide imaging services to residents and transport them via helicopter (above) back to MGH if necessary. No radiologists live on the island. Image courtesy of Massachusetts General Hospital.

10 RSNA News | April 2018
FEATURE
BOLD MRI Points to Link between Renal Hypoxia and Coronary Disease BY LYNN ANTONOPOULOS
Researchers may have identified a method for non-invasively measuring the extent of renal hypoxia resulting from myocardial infarction.
In a recent Radiology study, research-ers used blood-oxygen level dependent (BOLD) MRI to measure changes in renal oxygenation in a mouse model, which was demonstrated as a promising step toward better assessing complex dis-ease processes like cardiorenal syndrome (CRS).
Lead author, Di Chang, MD, PhD, corresponding author, Shenghong Ju, MD, PhD, of the Department of Radiol-ogy at Zhongda Hospital, Southeast University (SU) in Nanjing, China, and Dr. Ju's team were conducting a clinical retrospective cohort study to examine the long-term, adverse effects of various con-trast media following coronary angiogra-phy when they discovered an interesting connection.
“Patients who needed to receive percu-taneous coronary intervention (PCI) had
higher serum creatinine values than people who didn’t need the PCI sur-gery,” Dr. Ju said. “This result suggested people with coronary diseases might have an impaired renal function.”
The team used BOLD MRI to explore the potential interaction
between heart and kidney in CRS with a focus on the diagnosis of renal oxygen-ation.
The group randomly subjected 189 male mice to either myocardial infarction (MI) surgery or sham surgery in which they exposed the heart but did not use ligation to mimic a MI.
According to Dr. Chang, maintaining consistency in the size of the MI and improving the survival rate of the mice was a significant challenge. The team practiced the MI surgery for several months and double-confirmed the final MI sizes using enhancement following gadolinium administration and Masson’s trichrome histological staining to align the detailed ligation positions with the targeted infarct sizes.
The mice were then sorted into three
groups according to MI size: large, small and sham. Renal BOLD MRI was per-formed prior to MI and on days one, seven, 14, 28 and 60 after MI. The researchers performed histologic analysis of renal hypoxia-inducible factor-1α (HIF-1α) (a key transcriptional regu-lator of adaptive response to hypoxia) and kidney injury molecule-1 (KIM-1) (a biomarker for renal proximal tubular damage) to evaluate tissue hypoxia and kidney injury in the subgroups for each time point.
Following imaging, the team analyzed the relationships between the BOLD R2* and HIF-1α expression. “We detected the elevation of R2* values in the renal cortex and medulla of the MI groups compared to the sham group from day one to day 60, and it was most pro-nounced on day 60,” Dr. Chang said.
She added, “A greater elevation in R2* was also observed in the large MI group compared to the small MI group from day seven to day 60.”
Further Research Necessary Before Clinical Use In addition to these findings, the team also noted an increase in renal KIM-1 in the MI groups compared with the sham group on day 60. Renal KIM-1 showed
Chang Ju Prasad
“Patients who needed to receive percutaneous coronary intervention (PCI) had higher serum creatinine values than people who didn’t need the PCI surgery. This result suggested people with coronary diseases might have an impaired renal function.”
SHENGHONG JU, MD, PHD

April 2018 | RSNA News 11
a positive correlation with HIF-1α. The researchers concluded that increased renal hypoxia is a potential risk factor for progressive tubulointerstitial injury in mouse kidneys.
Pottumarthi Prasad, PhD, associate director, Department of Radiology at North Shore University Health System, Evanston, IL, coauthored a Science to Practice article in the January 2018 issue of Radiology commenting on the study by Dr. Chang and her col-leagues.
In his review, Dr. Prasad examined whether func-tional MRI can be useful in the evaluation of cardiore-nal syndrome (CRS).
While acknowledging that renal BOLD MRI could have a positive impact on the mechanistic understand-ing of CRS, he noted that additional work is required before the method can be used clinically.
“It is necessary to show a similar trend of increased renal hypoxia in patients with cardiac infarctions or heart failure,” Dr. Prasad wrote. “Such translation is not always easy because the animal models do not replicate all the complexities and co-morbidities seen in real patients.”
Dr. Chang agreed. “Due to the substantial differ-ences between rodents and humans, we would like to perform a clinical study to test whether such func-tional BOLD-MRI methods could be used to detect renal oxygenation alterations in clinical patients with MI.”
Looking ahead, Dr. Chang and her team would also like to use diffusion weighted imaging in a mouse model to examine whether there would be restricted diffusion in the renal tissues after MI.
WEB EXTRAS Access the study, “Noninvasive Identification of Renal Hypoxia in Experimental Myocardial Infarctions of Different Sizes by Using BOLD MR Imaging in a Mouse Model,” at RSNA.org/Radiology.
Access, “Science to Practice: Can Functional MR Imaging Be Useful in the Evaluation of Cardiorenal Syndrome?” at RSNA.org/Radiology.
Renal BOLD measurements. MI-L = large MI, MI-S = small MI. Representative R2* (1/T2*) map of the three groups before (day 0) and 7 and 60 days after MI. Graphs of R2* values in renal cortex in the three groups before (day 0) and 1, 7, 14, 28, and 60 days after MI show that R2* values were significantly higher in large MI group than in sham group from day 1 to day 60 in the renal cortex (P < 0.001). Small MI group also showed a significant increase in R2* compared with sham group from day 1 to day 60 (P < 0.05), but enhancement was less pronounced than that observed in large MI group. Moreover, R2* was significantly higher in large MI group than in small MI group from day 7 to day 60 in the renal cortex (P <0.05). There were six to eight mice per group. There were six to eight mice per group. *** = P < 0.001 for large MI versus sham group; # = P < 0.05, ## = P < 0.01, ### = P < 0.001 for small MI versus sham group; & = P < 0.05, && = P < 0.01, &&& = P < 0.001 for large MI versus small MI group. Data are means ± standard deviations. © RSNA 2018. All rights reserved. Printed with permission.
12 RSNA News | April 2018
FEATURE
Hybrid Magnetic Gold Nanoparticles Effective in Colorectal Cancer TreatmentBY MIKE BASSETT
Colorectal cancer, the fourth most common cancer diagnosed in the U.S. each year, is not only a ubiquitous cancer, it is a deadly one as well. Colorectal is the third most common cancer-related cause of death across the globe, according to the World Health Organization.
Upfront treatment of localized tumors usually involves a combination of surgical resection with or without adjuvant chemo-therapy and/or radiotherapy. However, up to 25 percent of patients with colon can-cer also present with synchronous metasta-ses at diagnosis and a similar percentage of patients will eventually develop colorectal liver metastases.
Only about a quarter of patients with colorectal liver metastases are suitable candidates for surgical resection because of the size, number and location of their metastases.
So for a majority of patients, only non-surgical treatment options — such as chemoembolization, thermal ablation, 90Y radioembolization or external beam radiotherapy — are available. Many of these treatments, including thermal ablation, however, are typically effective only in tumors that are smaller than four or five centimeters in diameter. While in many cases radiotherapy can be utilized in larger tumors, that method has its own limitations in regard to liver and other normal tissue toxicities.
In recent Radiology research, lead author, Sarah B. White, MD, an associate professor of radiology, Medical College of Wisconsin, Milwaukee, and colleagues investigated whether bio-functionalized hybrid magnetic gold nanoparticles could be used to expand the size of ablation zones in order to treat larger colorectal cancer tumors with thermal ablation. These treatment algorithms include a nanomaterial system that permits MRI visualization and quantification and pho-tothermal sensitization.
Dr. White has been particularly inter-ested in developing new drug delivery sys-tems that can be delivered site-selectively, which was the focus of her research project funded by a 2014-2016 Bracco Diagnos-tics Inc./RSNA Research Scholar Grant.
“In addition to or perhaps even instead of giving a patient systemic chemo-therapy, we would use a nanoparticle as the carrier and deliver it directly to the tumor,” Dr. White said, noting that avoiding systemic treatment also will potentially prevent undesired toxicity to other organs.
“In this project we wanted to increase our ablative capability,” Dr. White said, pointing out that ablation can achieve local control for tumors that are three centimeters or less. “Beyond three centi-meters, we are not as good as resection, but by increasing our ablative capability, we may in the future still be able to say that ablation can achieve durable local control."
Increasing the Size of Ablation ZonesNanotechnology has developed over the last 20 years, said study author Dong-Hyun Kim, PhD, assistant professor, Department of Radiology, Feinberg School of Medicine, Northwestern University, Chicago, who operates a nanomedicine laboratory at the univer-sity to study multifunctional therapeutic nano-carriers for cancer treatment.
“Unique features of nanomaterials have been expected to provide new oppor-tunities in early diagnosis, imaging and treatment of cancers. It should be advan-tageous, especially for tumor-localized cancer therapy,” Dr. Kim said.
In their study, Drs. White and Kim pointed out that sensitization with nan-otechnology could potentially increase ablative capabilities without causing further toxicity and/or damage to a liver that may have already been exposed to hepatoxic chemotherapy.
Specifically, the researchers hypothe-sized that the use of anti-MG1 conju-gated hybrid magnetic gold nanoparticles (HNPs) would act as a catalyst during
KimWhite

April 2018 | RSNA News 13
Left: R2 and R2* imaging and quantification. Wistar rats inoculated with CC-531 cells and tumors were allowed to grow for 7–10 days. Image of a rat taken with camera during thermal laser ablation while temperature measurements were being taken. © RSNA 2018. All rights reserved. Printed with permission.
photothermal ablation of colorectal liver metastases and increase the size of ablation zones.
“Conventionally, clinicians use laser to directly ablate the tumors,” Dr. Kim said. “In this case, we use the gold nanopar-ticles to increase the amount of heat generated.”
And since gold converts light energy — particularly laser light energy — into heat, it allows for the capability of a larger ablation zone, wherever the nanoparticles are deposited.
Getting the gold nanoparticles into the tumor was another challenge.
“We made nanoparticles with mono-clonal antibodies that home in and bind to the tumor cell selectively,” Dr. White said. “They are endocytosed into the cell. When we shine the laser on the cell with the nanoparticles inside, the gold heats up and the cell dies.”
Using rat models, Drs. Kim, White and colleagues determined that these anti-MG1 HNPs are noncytotoxic and have a greater than 20 percent intra-tu-moral accumulation compared with HNPs alone (nanoparticles that are not coated with the tumor specific monoclo-nal antibody). They also demonstrated that phototheramal ablation showed more than a two-fold enhancement in tumor response with the administration of anti-MGI HNPs vs. ablation alone.
“By increasing the ablation zone, we are no longer limited by three centime-ters,” Dr. White said. “Maybe we can tar-get a four-centimeter or five-centimeter tumor and get the same results.”
Clinical Applications Possible In a Science to Practice article in the same issue of Radiology, Xiaoming Yang, MD, PhD, Department of Radiology, University of Washington School of Medicine, commented that the concept that targeted HNPs enhance the thera-peutic effect of thermal ablation “presents an exciting strategy for complete removal of [colorectal liver metastases] by inte-grating two rapidly advancing scientific fields — in interventional radiology and nanotechnology.”
According to Dr. Yang, future applica-tion of this technique — if it proves suc-cessful in human subjects — could have further clinical implications.
For example, he suggested that the technique could include the co-loading or coating antitumor therapeutics in these targeted HNPs to promote thera-peutic accumulation at tumor sites.
Dr. White and colleagues are now investigating other types of nanoparticles as well as alternate methods to deliver therapeutics and deposit them into tumors.
“In this study we delivered therapeutics via IV; however, there are problems with that method,” she said. “Administering nanoparticles site-selec-tively is on the horizon, as well as using the technique in other tumor models — not just colorectal liver metastases, but other cancers in the body.”
“When we shine the laser on the cell with the nanoparticles inside, the gold heats up and the cell dies.”
SARAH B. WHITE, MD
WEB EXTRAS Access the Radiology study, “Biofunctionalized Hybrid Magnetic Gold Nanoparticles as Catalysts for Photothermal Ablation of Colorectal Liver Metastases,” at RSNA.org/Radiology.

14 RSNA News | April 2018
FEATURE
RSNA ML Pediatric Bone Challenge Showcases Promising New Tools BY JENNIFER ALLYN
In designing an algorithm to predict skeletal age from pediatric hand x-rays, Mark Cicero, MD, and Alexander Bilbily, MD, demonstrated the potential of machine learning (ML) and artificial intelligence (AI) to aid radiologists in better serving patients.
The algorithm, which won first place in the 2017 RSNA ML Pediatric Bone Challenge, provides radiologists with an automated method for analyzing bone age — a significant improvement on cur-rent methods which can be cumbersome and time-consuming, Dr. Cicero said.
Winning the RSNA competition was just the beginning. Recently, Drs. Cicero and Bilbily, both radiology trainees at the University of Toronto, Ontario, have founded a medical diagnostics AI com-pany, 16 Bit, which has partnered with an AI platform provider to distribute the algorithm to hundreds of U.S. hospitals — free for public research use.
“Artificial intelligence and machine learning will be the foundation of these next generation tools and, ultimately, will allow us to provide faster, better and more reliable care to our patients,” Dr. Bilbily said.
ML Challenge Uses Stanford Data Demonstrating how ML and AI can benefit radiology and improve diagnostic care was the goal of the RSNA ML Pediatric Bone Age Challenge launched by the RSNA Radiology Informatics Committee (RIC) in the fall of 2017.
The online competition drew more than 250 participants, comprised of
radiologists, tech-nology companies, computer scientists, engineers and other medical specialists. Participants worked in 29 teams to submit the outcomes of their algorithms. Teams with the most accu-rate predictions (one winning team and two runners-up) were announced at RSNA 2017 in December.
While there is an overall lack of high quality validated data that is publicly available, the challenge used data sets generously donated by Stanford Chil-dren’s Hospital, CA, and Colorado Chil-dren’s Hospital, Aurora, CO. Stanford researchers published a 2017 Radiology study on deep learning networks to assess pediatric hand images. (See Web Extras.)
“Access to quality image datasets in sufficient quantity to address the problem at hand is often the limiting factor in performing reasonable machine learning with diagnostic imaging,” said Adam Flanders, MD, former RIC chair and professor of radiology at Thomas Jeffer-son University, Philadelphia. “Repurpos-ing large imaging datasets used in other types of image-based research is an attrac-tive ready-made source of data that could be used for machine learning, but in many instances that data is embargoed.”
Participants were given a set of hand radiographs and corresponding skeletal ages to develop and train their prediction models. Then, they were asked to predict the skeletal ages on a test dataset with skeletal ages withheld.
Most, but not all of the best perform-ing submissions utilized deep neural network techniques based on one or multiple convolutional neural networks, said Jayashree Kalpathy-Cramer, PhD, associate professor of radiology, Harvard
Kalpathy-Cramer
Launched in fall of 2017 by the RSNA Radiology Informat-ics Committee, the RSNA ML Pediatric Bone Age Challenge drew more than 250 participants on 29 teams who submit-ted algorithms. The winning team and two runners-up were announced in the Machine Learning Theater at RSNA 2017.

April 2018 | RSNA News 15
“Artificial intelligence and machine learning will be the foundation of these next generation tools and, ultimately, will allow us to provide faster, better and more reliable care to our patients.”
ALEXANDER BILBILY, MD
Left: The winning algorithm was submitted by Marc Cicero, MD, left, and Alexander Bilbily, MD. Top: the RSNA ML Challenge Organizing Committee and the winning teams at RSNA 2017.
Medical School, Boston, who built the platform that hosted the challenge. While similar methodologies may be used to derive the answer, the efficiencies pro-vided through these algorithms make these tools useful for radiologists.
“Challenges can comprehensively assess the performance of algorithms by com-paring them on common, sufficiently large and diverse data sets using realistic tasks and valid evaluation metrics,” said Dr. Kalpathy-Cramer, who also served on the RSNA ML Challenge Organizing Committee. “However, as this technol-ogy evolves and similar algorithms are developed, radiologists will have a choice of algorithms that perform similarly in terms of prediction performance. No one wants to use an algorithm that takes 10 times longer to run.”
A Collaborative Competition“The RSNA ML Challenge provided a format for involving radiology in the transformative AI and ML tools that will impact their practices,” Dr. Bilbily said.
“Increased exposure to artificial intel-ligence and its applications in radiol-ogy gets more people involved, which advances the field faster through research, experimentation, and novel use case development, since we all have challenges in our day-to-day work that can be made more efficient with this technology,” Dr. Cicero said.
Safwan Halabi, MD, clinical assistant professor of radiology and pediatric radiology at Stanford and a member of the RSNA ML Challenge Organizing Committee agrees that the benefits of this type of challenge are far-reaching.
“Instead of standing on the sidelines waiting for what they assume is going to happen — that the technology will take away their jobs — this challenge promoted the idea of radiology being collaborative with this technology,” Dr. Halabi said.
RSNA is planning a 2018 ML chal-lenge and will announce details this summer. The winners will be announced during RSNA 2018.

16 RSNA News | April 2018
RADIOLOGY’S FUTURE
Individual DonorsDonors who give $1,500 or more per year qualify for the RSNA Presidents Circle. Their names are shown in bold face.
$5,000 – $9,999Shirley & Herbert Y. Kressel, MDUmar Mahmood & Karin Sangster
$500 – $1,499Luiz Antonio N. Oliveira, MDKeith A. Phillips, MDHilarion G. Ralaisomay, MDNancy J. Rini, MD & Sean McCourtMarc D. Shapiro, MDRichard D. White, MDDavid M. Yousem, MD
$300 – $499Heba Abdelrahman II, MDSameen Akhtar, MBBChJoseph T. Azok, MDMichael R. Baker, MDSusan & Marc R. Beck, MDMaria R. Beltran, MDIan Boiskin, MDSharon S. Brouha, MD, MPHDouglas C. Brown, MDDarren L. Cain, MDGiovanna Casola, MDSilvia D. Chang, MD & Zuheir Abrahams, MD, PhD
Horacio R. D'Agostino, MD, FACR, FSIRRobert F. Favret Jr., MDHeather C. Finke, MDLori Gottlieb, MD & Elliot K. Fishman, MD
Andrew E. Halpern, MDCameron Hassani, MDSteven W. Hetts, MD & Gloria L. Hwang, MD
Theodore S. Hong, MDKazuya Ichikado, MD, PhDYutaka Imai, MDMaria & Dennis Kay, MDZachary M. Kilpatrick Jr., MDNeha A. Kothari, MD
Klaus Kubin, MDKeiko Kuriyama, MDKevin J. Leonard, MDKenneth K. Lindell, MDJennifer & Eric Meredith, MDSharon & Robert M. Miller, MDMonika Misra, MDPaul Mogannam, MDConstance & James A. Newcomb, MDKenneth C. Ong, MDJosephine Pressacco, MD, PhDMaria T. Ramirez, MDHoward M. Richard III, MDDaniel Riitano Sr., MDRola Saouaf, MDAdnan M. Sheikh, MDRobert I. Silvers, MDRajwinder Singh, MD, MBBSIra S. Smalberg, MDDarrin S. Smith, MDJason W. Stewart, MDTimothy P. Sullivan, MDAmy S. Thurmond, MDYela & Gustav K. von Schulthess, MD, PhDDavid L. Wadley, MDCarolyn L. Wang, MD & George Wang, MDDaniel J. Wunder, MD
$299 or LessDeborah S. Ablin, MD
In memory of William G. Bradley Jr., MD, PhD
Andrea Agostini, MDNicolas R. Ahumada, MDIldefonso G. Almonte, MDDominic Altieri, MDGulcin Altinok, MDMichael D. Ames, MDDana Tell & Nami R. Azar, MDStefan A. Beyer-Enke, MDCarolyn H. & George T. Bolton, DVM, MDPatrick D. Browning, MD, MAKrammie M. Chan, MD
Ling Ling Chan, MBBS, FRCRMaria Castoldi Chiara, MD & Fabio De Stefano
Doris Hausen & Richard S. Clemens, MDThomas P. Cole, MDDerek W. Cool, MD, PhDTiana Crawford, MDJohn J. Culliney, MDRyan K. Cunningham, MDJulianna M. Czum, MDLanita M. Dawson-Jones, MD & Alvin J. Jones
Michael P. Dixon, MDAndrea S. Doria, MDDebra S. Dyer, MD & David RosenbergMargaret & Jimmie L. Eller, MDMonica S. Epelman, MD & Gustavo Epelman
Ricardo Faingold, MDHugo Falcon Jr., MDMary F. & Richard G. Fisher, MDRichard I. Gray, MDMikhail Higgins, MDPeter Hu, MDGregory A. Kaufmann, MDChristine J. Kim, MDSheldon A. Kleiman, MDChristien Kluwe, MD, PhDMyles B. Koby, MD, DDSLisa & Marc D. Kohli, MDYeamie M. Kousari, MD, MACrisostomo V. Lacano, MDEvelina P. Naval & Pedro Danilo J. Lagamayo, MD
Sonia Lee, MDSteven Lev, MDScott Lieberman, MDElizabeth A. Little, MDFlavio C. Lugo, MDDeborah & James A. Lyddon, DOJoy A. Masseaux, MD, MPHBernadette Mayor Chalaron, MDLouis Mazzarelli, MD, MS
Rostislav Medvid, MDFrank R. Mihlon, MD
In memory of William G. Bradley Jr., MD, PhD
Whitney Jo Morgan, MDXuan-Mai T. Nguyen, MDAmber Mercier Nikolaidis & Paul Nikolaidis, MD
Fukiat Ongseng, MDMarco Panfili, MDChang Min Park, MD, PhDJole Antinolfi & Francesco Potito, MDRodolfo Queiroz, MDTrenton D. Roth, MDRocky C. Saenz, DOEvelyn G. Sanchez, MDDeborah & Glenn A. Scheske, MDRebecca L. Seidel, MDSadashiv S. Shenoy, MDMarianne T. Shih, MDFrancisco M. Silva I, MDGary E. Simmons, MDAndres Spirig, MDJennifer M. & Bradley S. Strimling, MDLeena Tekchandani, MDNikhil G. Thaker, BS, MDJason Tholany, MDTimothy S. Tsai, MDBenjamin E. Tubb, MD, PhDRocio J. Urena, MDEster P. Van der Wal, MD & Djavid Hadian, MD
Kimberly & Theodore L. Vander Velde II, MD
Cecilia J. Villasante Luna, MD & Hector J. Caballero Lobera
Stephan Waelti, MDJean C. Wang, MDChao-Jung Wei, MD, PhDLuanne & Alan L. Williams, MDRauf Yagan, MDBrian L. Yemen, MDLeigh A. & Mark S. Yuhasz, MD
Visionaries in PracticeA giving program for private practices and academic departments.
BRONZE LEVEL ($10,000)
Radiology Associates, P.A., Little Rock, AR
The RSNA Research & Education Foundation thanks the following donors for gifts made January 5, 2018 through January 23, 2018.
RESEARCH & EDUCATION FOUNDATION DONORS
Imaging for Life
Visionary DonorsThe following individuals are recognized for cumulative lifetime donations.
BRONZE VISIONARY ($5,000)Umar Mahmood & Karin SangsterMarc D. Shapiro, MD

April 2018 | RSNA News 17
YOUR DONATIONS IN ACTION
R&E Embraces Artificial Intelligence and Machine Learning
At RSNA 2017, two-time Research & Education (R&E) Foundation Grant recipient Stephen Chan, MD, led an insightful conversation among R&E grant recipients who are pursuing various applications of artificial intelligence (AI) and machine learning (ML) in radiology. The grant recipients, Andreas M. Rauschecker, MD, PhD, Brian S. Letzen, MD, Albert Hsiao, MD, PhD, and Manisha Bahl, MD, MPH, discussed why they chose their specific projects and why R&E was the right funding partner for their research.Funded R&E grant projects include: Automated Neuroradiologic Diagnosis
Using Customized Advanced Image Processing Algorithms and Bayesian Networks Development of an Automated Liver
Imaging Reporting and Data System Using Deep Machine Learning Evaluation of Quantitative Cardiac
Function and Volumes With Single Breath-hold Volumetric Cardiac MRI and Deep Learning Segmentation Machine-learning to Predict Risk of
Upgrade and Recurrence of Ductal Carcinoma in Situ
From left: Dr. Chan (standing), Drs. Hsiao, Letzen, Rauschecker and Bahl.
New R&E Education Grant Topics AnnouncedThe RSNA Research & Education (R&E) Foundation Board of Trustees has announced the 2018 topics for new education grants which will be awarded in 2019. Now is the time to start developing topics and gathering your team. The topics are:
Education Innovation Grant Amount: Up to $175,000 per year for three years ($525,000 maximum)Topic: Point-of-care education
Education Development Grant Amount: $30,000 to $100,000 per year for up to three years ($300,000 maximum)Topics:
• Imaging cancer• Patient education• Physician burnout• Women and minorities in
radiology leadership
Derek-Harwood Nash International Education Grant Amount: Up to $75,000 for one year (2-year projects considered in exceptional cases, $150,000 maximum)Topic: International radiology education
The goal of the Foundation’s new education grant program is to enhance education for the benefit of radiology faculty as educators and radiologists and radiology support personnel through creation of educational content, educational products or other innovative means. Additional information will be available soon about the request for application and instructions for the pre-application process.

18 RSNA News | April 2018
NEWS YOU CAN USE
The following are highlights from the current issues of RSNA’s two peer-reviewed journals.
Journal Highlights
Listen to Radiology Editor David A. Bluemke, MD, PhD, discuss this month’s research you need to know. Podcasts summarize the importance and context of selected recent articles. Subscribe today at RSNA.org/Radiology-Podcasts and never miss a single episode.
Thyroid Imaging Reporting and Data System (TI-RADS): A User’s Guide
Radiologists who interpret thyroid ultrasonography
(US) images frequently face the dilemma of how to report nodules, which are extremely common and overwhelmingly benign. The American College of Radiology (ACR) Thyroid Imaging Reporting and Data System (TI-RADS) aims to provide an easy-to-apply method for practitioners to determine manage-ment of thyroid nodules.
In an article published online in Radiology (RSNA.org/Radiology), Franklin N. Tessler, MD, University of Alabama at Birmingham, and colleagues reviewed the ACR TI-RADS and pro-vided guidance on how to implement and apply the system.
Points in five feature categories — composition, echogenicity, shape, margin and echogenic foci — are added together to determine the nodule’s risk level, which ranges from TR1 (benign) to TR5 (highly suspicious). In conjunction with the nodule’s maximum diameters, the TR level determines whether to recommend a fine-needle aspiration (FNA) biopsy, a follow-up US exam or no further action.
Because the threshold size for recommending FNA decreases as the US features become more malignant appearing, adherence to ACR TI-RADS will result in fewer biopsies of benign nodules. Alternately, it will also result in fewer biopsies of malignant nodules and
ACR TI-RADS recommends follow-up for some nodules that do not meet the size criteria for FNA.
“Success demands close cooperation between radiologists and sonographers,
understanding of the nuances and pitfalls of feature assignments, and attention to detail in reporting and making recom-mendations,” the authors write.
Spongiform 0.9-cm nodule in a 59-year-old woman. More than 50% of the nodule is composed of small cystic spaces. The nodule received 0 points for composition because of its spongiform designation and no additional points in other categories (TR1).Radiology 2018;287;1:InPress) © RSNA 2018. All rights reserved. Printed with permission.
This article meets the criteria for AMA PRA Category 1 Credit™. SA-CME is available online only.
March articles are:
"Effects of Career Duration, Concussion History, and Playing Position on White Matter Microstructure and Functional Neural Recruitment in Former College and Professional Football Athletes," Mark D. Clark, BS, and colleagues.
"Effectiveness of a Staged US and Unenhanced MR Imaging Algorithm in the Diagnosis of Pediatric Appendicitis," Elizabeth H. Dibble, MD, and colleagues.
"Flexible Sigmoidoscopy and CT Colonography Screening: Patients’ Experience with and Factors for Undergoing Screening—Insight from the Proteus Colon Trial," Carlo Senore, MD, MSc, and colleagues.

April 2018 | RSNA News 19
“Multiparametric MR Imaging of the Prostate after Treatment of Prostate Cancer,” Pritesh Patel, MD, and colleagues. “Neuromyelitis Optica Spectrum Disorders: Spectrum of MR Imaging Findings and Their Differential Diagnosis,”
Bruna Garbugio Dutra, MD, and colleagues. “MR Imaging of Muscle Trauma: Anatomy, Biomechanics, Pathophysiology, and Imaging Appearance,” Dyan V. Flores, MD,
and colleagues.
Listen to RadioGraphics Editor Jeffrey S. Klein, MD, and authors discuss the following articles from recent issues of RadioGraphics at RSNA.org/RG-Podcasts.
Liver Iron Quantification with MR Imaging: A Primer for RadiologistsMRI is now considered the standard of care for liver iron quantification, includ-ing assessment of distribution, detection, grading and monitoring of treatment response for iron overload. Although iron overload can be seen in many organs, the liver is the main iron storage organ, the first to show iron overload and the only organ to show a linear relation-ship between its iron concentration and total body iron.
In an article in the March-April issue of RadioGraphics (RSNA.org/RadioGraphics), Roxanne Labranche, MD, Centre Hospitalier de l’Université de Montréal, QC, Canada, and colleagues review the
techniques that have been developed for iron quantification and their advantages and limitations.
The liver-to-muscle signal intensity ratio technique is simple and widely
available, but it assumes that the reference tissue is normal and is not accurate for severe
iron overload. Transverse magnetization relaxometry (R2) is prone to respiratory motion artifacts due to a long acquisition time and requires additional cost and delay for off-line analysis. Alternatively, the R2* technique has a faster acquisition time and detects a wide range of liver iron content but requires additional software that is not universally available.
Quantitative susceptibility mapping has the highest sensitivity for detecting iron deposition; however, it is still investiga-tional and the correlation with liver iron content is not yet established.
“Because of the noninvasiveness and the accuracy of these techniques, MR imaging-based liver iron quantification has become part of the standard of care in diagnosis and monitoring of iron overload diseases. In the near future, multipara-metric quantitative protocols will permit simultaneous assessment of liver iron over-load, as well as coexistent fat and fibrosis,” the authors conclude.
Moderate liver iron overload due to hemosiderosis in a 57-year-old man with ß-thalassamia hemoglobin C. Multiecho axial MR images at 1.5 T were obtained according to an earlier Rennes protocol, with echo times of 4.6 msec (T1-weighted) (a), 4.6 msec (proton-density–weighted) (b), 9.2 msec (T2-weighted) (c), 13.8 msec (T2+-weighted) (d), and 18.3 msec (T2++-weighted) (e). Three regions of interest were drawn in the liver (yellow circles) and one in each paraspinal muscle (red circles) for each of the five sequences. Associated splenomegaly is seen. Liver iron content was 160 µmol/g ± 50 (8.9 mg/g dry weight ± 2.8) according to the Rennes protocol. (RadioGraphics 2018:38;2;392-412) © RSNA 2018. All rights reserved. Printed with permission.
This article meets the criteria for AMA PRA Category 1 Credit™. SA-CME is available online only.

20 RSNA News | April 2018
NEWS YOU CAN USE
Radiology in Public Focus
Media Coverage of RSNA
Patients Lack Information about Imaging ExamsPatients and their caregivers desire infor-mation about upcoming imaging exam-inations, but many are not getting it, according to a new study in Radiology.
The researchers found that over one-fifth of patients and caregivers did not receive information prior to their imaging examinations and out of all the people surveyed, half sought information about imaging tests on their own.
“As medicine shifts to an era of patient-centered care, much of the efforts in radiology have focused on commu-nicating the results of imaging tests to patients,” said study lead author Jay K. Pahade, MD, associate professor of radiology, Yale School of Medicine, New Haven, CT. “Less attention has been paid to engaging patients prior to and during the examination.”
Dr. Pahade and colleagues surveyed patients and caregivers at three pediatric
and three adult hospitals across the U.S. about their preferences for receiving imaging test information before an exam-ination and what type of information they found most useful.
Overall, 78 percent of the 1,438 respondents reported receiving information about their examination. Respondents with scheduled MRI or nuclear medicine examinations were more likely to receive information prior to testing (87 percent and 82 percent, respectively), as were patients who had previously experienced more than six radiologic exams (82 percent).
When asked to rate what information they consider to be valuable prior to a radiologic examination, respondents in both types of hospitals placed the highest importance on examination preparation and the lowest importance on whether an alternative radiation-free examination could be used. Parents, who were primarily responding to the pediatric hospital survey, placed an even higher value on any and all pre-examination information.
The single most common source of information about an upcoming radio-logic exam was the ordering provider
(64 percent) and most respondents pre-ferred to receive information from them (72 percent). The radiology department or imaging center was a distant second as a source of information (19 percent) followed by staff members in the depart-ment or imaging center (16 percent).
Half of all the survey respondents (52 percent) reported independently seeking information about radiology examinations themselves, including ask-ing the provider’s office or heading to general websites. Researchers recommend increasing the promotion of available sites such as RadiologyInfo.org, an online resource for medical imaging, jointly sponsored by RSNA and the American College of Radiology.
“A lack of information can negatively affect a patient’s experience and since anxiety is known to be higher among uniformed patients, radiology needs to take more ownership over the entire imaging process,” Dr. Pahade said. “It’s important for radiology to design, improve and implement a more patient-centered model of healthcare delivery that closes the gap for pre-imaging education.”
WEB EXTRAS Access the study, “What Patients Want to Know about Imaging Examinations: A MultiInstitutional U.S. Survey in Adult and Pediatric Teaching Hospitals on Patient Preferences for Receiving Information before Radiologic Examinations,” at RSNA/Radiology.org.
Press releases were sent to the medical news media for the following articles appearing in recent issues of Radiology.
In December, 4,356 RSNA-related news stories were tracked in the media. These stories had an estimated audience reach of 2.4 billion. Coverage included The New York Times, U.S. News & World Report, Yahoo! News, Today.com, MSN.com, The Boston Globe,
WCBS-TV (New York), Doctor Radio, WMAQ-TV (Chicago), WBBM-TV (Chicago), CLTV (Chicago), WBTS-TV (Boston), NECN (Boston), WTXF-TV (Philadelphia), KDKA-TV (Pittsburgh), KPRC-TV (Houston), KING-TV (Seattle), WBAL-TV (Baltimore), The Washington Times, CNN.com, WebMD, Drugs.com, HealthDay, Philly.com and The Arizona Republic.
Media Coverage of RSNA 2017RSNA 2017 annual meeting media coverage tracked through February 14, 2018, has resulted in 30,656 media placements with a potential audience impression of more than 15.2 billion.
Notable placements for RSNA 2017 include: The New York Times, NBC Nightly News, Voice of America, The Washington Post, U.S. News & World Report, Yahoo! News, TIME, The Wall Street Journal, Fox News Channel, CNN, Doctor Radio, The Boston Globe, News-week, Daily Mail (UK), The Telegraph (UK), Today.com, WCBS-TV (New York), KABC-TV (Los Angeles), KTLA-TV (Los Angeles), KTTV-TV (Los Angeles), WMAQ-TV (Chicago), WBBM-TV (Chicago), WTTG-TV (Washington, D.C.), WFXT-TV (Boston), NECN (Boston), KDKA-TV (Pittsburgh), KPRC-TV (Houston), WebMD, HealthDay, Philly.com, The Arizona Republic, Reddit, UPI, Houston Chronicle, Business Insider, Pittsburgh Post-Gazette, Drugs.com, CBSNews.com, BBC.com, Medscape, Forbes and Medical News Today.
April 2018 | RSNA News 21
Education and Funding Opportunities
RSNA/ASNR Comparative Effectiveness Research Training (CERT) Program
Apply now for the RSNA/American Society of Neuroradiology (ASNR) Comparative Effectiveness Research Training (CERT) Program. There is no fee for this course. Apply at RSNA.org/CERT or contact RSNA staff at [email protected] with questions.
Application DeadlineApril 30
RSNA 2018 International Travel Stipend Program
The RSNA International Travel Stipend Program aids eligible members from developing or low-resource nations by partially
defraying travel expenses related to attending the RSNA annual meeting. For more information and to apply, visit RSNA.org/Annual-Meeting-International-Travel-Stipend.
Application DeadlineApril 30
An MRI breast imaging technique that requires no contrast agent, combined with sophisticated data analysis, could reduce the number of unnecessary breast biopsies, according to a new study in Radiology.
Researchers recently studied an alter-native approach to breast MRI with gadolinium-based contrast agents, which is used to screen women at high risk of breast cancer. The alternative eliminates the need for contrast agents in some cases by using diffusion-weighted imag-ing (DWI) measurements derived from MRI. The technique, known as diffusion kurtosis imaging, provides a picture of breast tissue on a microstructural level.
“Diffusion kurtosis imaging has been introduced in DWI to provide import-ant information on tissue structures at a microscopic level,” said study lead author Sebastian Bickelhaupt, MD, from the German Cancer Research Center, Heidelberg, Germany. “Since malignant lesions disrupt the tissue structures at this level, diffusion kurtosis might serve as a relevant marker of changes.”
Dr. Bickelhaupt, co-lead author Paul Jaeger, MSc, and colleagues evaluated a retrospective analysis of data collected from 222 women at two independent study sites. The women had suspicious findings on mammography that were classified under the Breast Imaging Reporting and Data System (BI-RADS) as BI-RADS 4 and 5 breast lesions.
Before biopsy, diffusion-weighted MRI was performed and lesions were segmented. Voxel-based kurtosis fit-ting was performed, with adaptions to
account for fat signal contamination. A radiomics feature model was developed by using a random forest regressor. Con-ventional interpretations of MRI were also assessed for comparison. To prevent new false-negative results and decrease the number of false-positive decisions, the sensitivity of at least 98 percent was retained since that is comparable to core-needle biopsy, which has a sen-sitivity between 87 and more than 97 percent.
In an independent test set of 127 women, the radiomics analysis reduced false-positive findings by 70 percent, while detecting 60 of 61 malignant lesions, or 98 percent in BI-RADS-de-fined 4a and 4b lesions. Those women with BI-RADS-defined 5 lesions had no added diagnosis benefit through the radiomics feature model.
“The model might help to lower the number of BI-RADS 4 lesions suspected of being cancer on the basis of screen-ing mammography while retaining a high sensitivity similar to the sensitivity reported for biopsies themselves,” Jaeger said.
Should the results hold in larger trials, the model has potential advantages in the clinic for women with BI-RADS 4 lesions.
“The new approach is not intended to replace current contrast-enhanced breast MRI protocols in general,” Dr. Bickel-haupt said, “but to expand the spectrum of options available to differentiate between malignant and benign breast lesions.”
MRI Technique Differentiates Benign Breast Lesions from Malignancies
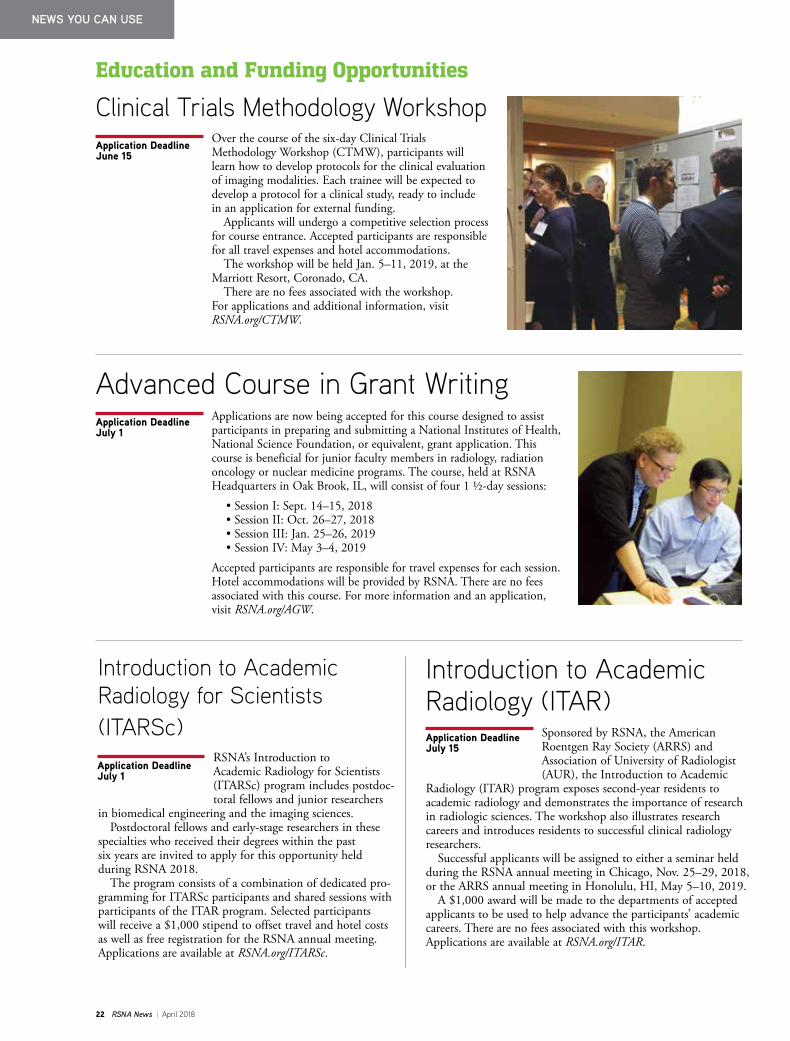
Receiver operating characteristic plot for the radiomics model, apparent kurtosis coefficient (AKC) median and apparent diffusion coeffi-cient (ADC) median. Dots illustrate the resulting thresholds. © RSNA 2018. All rights reserved. Printed with permission.
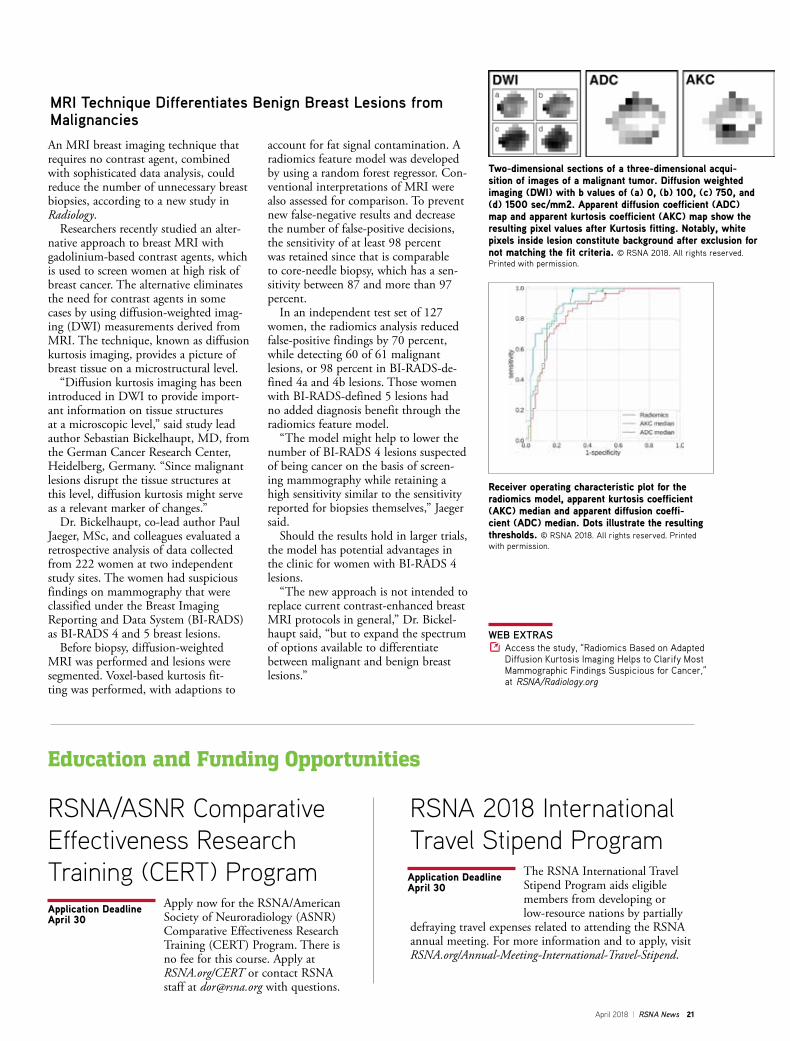
Two-dimensional sections of a three-dimensional acqui-sition of images of a malignant tumor. Diffusion weighted imaging (DWI) with b values of (a) 0, (b) 100, (c) 750, and (d) 1500 sec/mm2. Apparent diffusion coefficient (ADC) map and apparent kurtosis coefficient (AKC) map show the resulting pixel values after Kurtosis fitting. Notably, white pixels inside lesion constitute background after exclusion for not matching the fit criteria. © RSNA 2018. All rights reserved. Printed with permission.
WEB EXTRAS Access the study, “Radiomics Based on Adapted Diffusion Kurtosis Imaging Helps to Clarify Most Mammographic Findings Suspicious for Cancer,” at RSNA/Radiology.org
22 RSNA News | April 2018
NEWS YOU CAN USE
Advanced Course in Grant Writing Applications are now being accepted for this course designed to assist participants in preparing and submitting a National Institutes of Health, National Science Foundation, or equivalent, grant application. This course is beneficial for junior faculty members in radiology, radiation oncology or nuclear medicine programs. The course, held at RSNA Headquarters in Oak Brook, IL, will consist of four 1 1/2-day sessions: • Session I: Sept. 14–15, 2018 • Session II: Oct. 26–27, 2018 • Session III: Jan. 25–26, 2019 • Session IV: May 3–4, 2019 Accepted participants are responsible for travel expenses for each session. Hotel accommodations will be provided by RSNA. There are no fees associated with this course. For more information and an application, visit RSNA.org/AGW.
Introduction to Academic Radiology (ITAR)
Sponsored by RSNA, the American Roentgen Ray Society (ARRS) and Association of University of Radiologist (AUR), the Introduction to Academic
Radiology (ITAR) program exposes second-year residents to academic radiology and demonstrates the importance of research in radiologic sciences. The workshop also illustrates research careers and introduces residents to successful clinical radiology researchers.
Successful applicants will be assigned to either a seminar held during the RSNA annual meeting in Chicago, Nov. 25–29, 2018, or the ARRS annual meeting in Honolulu, HI, May 5–10, 2019.
A $1,000 award will be made to the departments of accepted applicants to be used to help advance the participants’ academic careers. There are no fees associated with this workshop. Applications are available at RSNA.org/ITAR.
Introduction to Academic Radiology for Scientists (ITARSc)
RSNA’s Introduction to Academic Radiology for Scientists (ITARSc) program includes postdoc-toral fellows and junior researchers
in biomedical engineering and the imaging sciences. Postdoctoral fellows and early-stage researchers in these
specialties who received their degrees within the past six years are invited to apply for this opportunity held during RSNA 2018.
The program consists of a combination of dedicated pro-gramming for ITARSc participants and shared sessions with participants of the ITAR program. Selected participants will receive a $1,000 stipend to offset travel and hotel costs as well as free registration for the RSNA annual meeting. Applications are available at RSNA.org/ITARSc.
Application DeadlineJuly 15
Application DeadlineJuly 1
Application DeadlineJuly 1
Clinical Trials Methodology Workshop Over the course of the six-day Clinical Trials Methodology Workshop (CTMW), participants will learn how to develop protocols for the clinical evaluation of imaging modalities. Each trainee will be expected to develop a protocol for a clinical study, ready to include in an application for external funding.
Applicants will undergo a competitive selection process for course entrance. Accepted participants are responsible for all travel expenses and hotel accommodations.
The workshop will be held Jan. 5–11, 2019, at the Marriott Resort, Coronado, CA.
There are no fees associated with the workshop. For applications and additional information, visit RSNA.org/CTMW.
Application DeadlineJune 15
Education and Funding Opportunities

April 2018 | RSNA News 23
Courtney Raybon, MD, is a second-year interventional radiology resident at Vanderbilt University Medical Center in Nashville. She completed her internship in general surgery at the University of California, San Francisco. She serves as the vice chair of the RSNA Resident and Fellow Committee (RFC) and chair of the RFC Program Subcommittee, which plans and oversees the Resident and Fellow Symposium at the RSNA annual meeting. She also serves as the RSNA RFC liaison to the American College of Radiology Resident and Fellow Section executive committee
Member SpotlightCourtney Raybon, MD
What or who sparks your interest in radiology? My passion for the field of radiology, combined with my interest in a procedure-oriented spe-cialty, makes training in interventional radiology the best of both worlds.
What is the biggest reward in your professional life?I have greatly enjoyed my work thus far. I find myself surrounded by talented physicians who are also gifted teachers. I am pleased to have discovered that even a relative beginner like myself is able to help in the diagnosis and treat-ment of a varied and diverse group of diseases.
How does volunteering for RSNA help you in your daily practice?RSNA fosters a community of scholarship through many programs and the RFC is certainly a place to grow and learn. The RFC fosters not only scholarship but also the opportunity to learn from peers, invaluable leadership experience, and countless opportunities for both personal and professional growth.
How do you spend your free time?One of my favorite things is to enjoy the outdoors with my husband and/or friends. We spend time hiking, boating, attending outdoor concerts, visit-ing vineyards, and anything that gets us outdoors together.
Members Receive Free Registration to World’s Premier Radiology MeetingAll RSNA members receive free advance registration for RSNA 2018 — a $950 value. New this year, registration will open for all membership categories on July 18.
Visit Meeting Central (Meeting.RSNA.org) on July 18 to register, access the program and review the exhibitor list. But you don’t have to wait until July to make your hotel reservations, which are open now. RSNA has negotiated special room rates for meeting attendees and even greater savings are available to those who reserve their hotel room before Sept. 12.
Attendees also receive free self-assessment module (SAM) credits and discounted registration for the Virtual Meeting.
Do you know non-member colleagues who would like to attend? Encourage them to join RSNA and attend RSNA 2018 for free.
Apply for or renew your membership at RSNA.org/Membership. Register for RSNA 2018 at RSNA.org/Annual-Meeting.
The Value of Membership

24 RSNA News | April 2018
NEWS YOU CAN USE
Annual Meeting Watch
RSNA 2018 Online Abstract Submission Now Open
NEW: RSNA 2018 Registration Opens July 18 for Everyone
Hotel Rooms for RSNA 2018 Available Now
The online system to submit abstracts for RSNA 2018 is open. The submission deadline is noon Central Time (CT) on Wednesday, April 11, 2018. Abstracts are required for scientific presentations, education exhibits, applied science, quality improvement reports and quantitative imaging reading room showcases.
To submit an abstract online, go to RSNA.org/Abstracts. The easy-to-use online system helps the Scientific Program Committee and Education Exhibits Committee evaluate submissions efficiently. For more information about abstract submissions, contact the RSNA Program Services Department at 1-877-776-2227 within the U.S., or 1-630-590-7774 outside the U.S.
The top neuroradiology scientific paper as selected by the Scientific Program Committee will receive a $3,000 award at RSNA 2018.
Students, clinical trainees and post-doctoral trainees are eligible to receive $500 travel awards for top-rated abstracts accepted for presentation at RSNA 2018. Trainees are also eligible to receive a $1,000 research prize.
Full eligibility requirements for all awards are available with the 2018 Call for Abstracts.
New this year, registration for RSNA 2018 will open on July 18 for all members and non-members. There will no longer be different registration dates based on membership category.
On July 18, Meeting Central (Meeting.RSNA.org) will be available and will include the complete meeting program and exhibitor list, so you can plan your entire meeting experience.
Visit RSNA.org/Annual-Meeting for registration and up-to-date information about RSNA 2018.
If you are planning to attend RSNA 2018, consider reserving your hotel room now. RSNA has negotiated special room rates for meeting attendees and even greater savings are available if you reserve your hotel room before Sept. 12.
Hotel information is available at RSNA.org/hotel-reservations.
November 25-30104th Scientific Assembly & Annual Meeting
April 2018 | RSNA News 25
Next month, RSNA News reports on Image Wisely and the growth of similar radiation safety initiatives throughout the world.
COMING NEXT
MONTH
RSNA.org
2017 Annual Report Available OnlineFrom adding innovative new programming at RSNA 2017 to developing new educational, informatics and patient-focused resources, 2017 was an extraordinary year of growth for RSNA. Learn more about how RSNA promoted excellence in radiology by reviewing the online 2017 RSNA Annual Report at RSNA.org/Annual-Report.
Highlights of the 2017 RSNA Annual Report include:
103rd Scientific Assembly and Annual Meeting More than 52,000 registrants participated in RSNA 2017, “Explore. Invent. Transform.” The Virtual Meeting offered more than 130 live-streamed and on-demand courses and Diagnosis Live™ was featured in 90 courses and seven case-based competition sessions — a 15 percent increase in use as compared to 2016.
New Frontiers in Technology: AI and ML RSNA continued to showcase artificial intelligence (AI) and machine learning (ML) in new formats, including the Machine Learning Showcase at the annual meeting, giving attendees the chance to learn about the technology and network with vendors. The Machine Learning Challenge invited participants to design algorithms to assess bone age from pediatric radiographs. Winners were announced at RSNA 2017. (Read more about the RSNA Machine Learning Challenge, on Page 14).
Online Learning Center UpgradedRSNA upgraded its Online Learning Center, providing users with an enhanced, mobile-friendly user interface and more than 600 courses offering SA-CME credit and offering the opportunity to earn CME from previous Annual Meeting sessions.
RSNA Announced Online-Only JournalsRSNA announced the launch of three new online-only journals in 2019: Radiology: Imaging Cancer, Radiology: Cardiothoracic Imaging and Radiology: Artificial Intelligence, which will join RSNA’s premiere journals, Radiology and RadioGraphics.
R&E Foundation Reaches Campaign Goal The RSNA Research & Education (R&E) Foundation reached the goal of its Inspire-Innovate-Invest Campaign, raising $17.5 million to fund radiology research.

Plan Now. Save BIG!RESERVE YOUR RSNA 2018 HOTEL NOW!New! Begin preparing for RSNA 2018 and reserve your hotel in advance. Get a jump on planning and enjoy the savings when you secure your reservation through RSNA.
Online Reservations Open Plan now to take advantage of the best room selection in downtown Chicago plus RSNA early-discount rates. The earlier you reserve, the more you save! Visit RSNA.org/Hotel-Reservations to secure your discounted RSNA 2018 hotel reservation now!
MTG994.1 Hotel Carrier Sheet for RSNA News Color FIN.indd 1 12/18/17 11:53 AM