madagascar: sustainable health system development project (world bank - 2007)
TRANSCRIPT

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 1/103
Document o f
The World Bank
FOR OFFICIALUSE ONLY
Report No: 38898 - MG
PROJECT APPRAISAL DOCUMENT
ON A
PROPOSED CREDIT
IN THE AMOUNT OF SDR 6.7 MILLION(US$lO MILLIO N EQUIVALENT)
TO THE
REPUBLIC OF MADAGASCAR
FOR A
MADAGASCAR SUSTAINABLE HEALTH SYSTEM DEVELOPMENT PROJECT
April 20,2007
Human Development I11Country Department 8Africa Region
This document has a restricted distribution and may be used by recipients only in theperformance o f their off icialduties. I t s contents may not otherwise be disclosed without WorldBank authorization.

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 2/103
CURRENCY EQUIVALENTS(Exchange Rate Effective March3 1,2007)
Currency Unit = AriaryAriary2050 = USDl
USD1.51326 = SDRl
A F D
AfDBA I D S
FISCAL YEARJanuary 1 - December31
Agence Franqaise de Dkveloppement MDG Mille nni um Development Goals(French Development Agency)African DevelopmentBank M IS Management Information SystemAcquired Immuno Deficiency Syndrome M O H Ministry o f Health,Family Planning and Social
H IPCHIVIBRDI C BIDAI M C I
Zusammenarbit GmbHHeav ily Indebted Poor Countries STI Sexually Transmitted InfectionsHuman ImmunodeficiencyVirus SSD Healt h DistrictsInt. Bank for Reconst. & Dev. sss Central He alth Statistics ServiceInternational Competitive Bidding UN United NationsInternational Development Association UN AI DS United Nations Programme on HIV /AI DSIntegrated Management o fChildhood UN DP United Nations Development Programme
I IllnessesI Insti tut Nationalde la Statistique (NationalN S TAT I U N FPA I United NationsFund or Population Activities
JICAM&EM A P
- .Statistical Institute)Japanese International Cooperation Agency UN ICE F Uni ted Nations Children’s FundMonitorin g and Evaluation US AI D U S Agency for International DevelopmentMadagascar Act ion Plan W HO Wo rld Healt h Organization
Acting Vice President: Hartwig SchaferCountry Director: Ritva ReinikkaCountry Manager Robert Blake
Sector Manager: Laura FrigentiTask Team Leader: Mukesh Chawla
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 3/103
FOR OFFICIAL USE ONLYMADAGASCAR
Sustainable Health System Development Project
TABLE OF CONTENTS
Page
STRATEGIC CONTEXT AND RATIONA LE .................................................................. 1
A .B
C .
I1
A.B
C .D
E
I11
A .B
C .D
E
F .
I V
A .B
C .D
EF .G
Coun try and sector issues .................................................................................................... 1Rationale for B an k involve men t.......................................................................................... 3
Higher l evelobjectives to w hic hthe project contributes.................................................... 4
PROJECT DESCRIPTION ............................................................................................. 5
Lending nstrument.............................................................................................................. 5
Project development objectiveand key indicators.............................................................. 5
Proje ct components.............................................................................................................. 5
Lessons learned and reflectedin the project design ............................................................ 8
Alternatives considered and reasons for rejectio n............................................................... 9
IMPLEMENTATION ..................................................................................................... 10
Partnership arrangements, coo rdina tion and impl em ent atio n support mechanisms.......... 0
Institutionaland implem entat ion arrangements................................................................ 10
Monitoring and evaluation o foutcomes/results ................................................................ 11
Sustainability..................................................................................................................... 12
Criticalrisks and possible contro versia l aspects............................................................... 12
Lo ad cre dit co nditions and covenants............................................................................... 13
APPRAISAL SU MMARY .............................................................................................. 13
Eco nom ic and financial analyses....................................................................................... 13
Technical ........................................................................................................................... 15
Fiduciary............................................................................................................................ 16
Social ................................................................................................................................. 18
Environment...................................................................................................................... 19Safeguard polici es.,............................................................................................................ 19
Poli cy E xceptions an d Readiness...................................................................................... 20
Annex 1: Country and Sector o r Program Background .......................................................... 21
has a restr icted distr ibution and ma ybe used by recipients on ly in the performance o ftheir o f f ic ia lduties I t s contents m ay n ot be otherwise disclosed without W or ld B an k authorization.

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 4/103
Annex 2: Major Related Projects Financed by the Bank and/or other Agencies .................. 5
Annex 3: Results Framework and Monitoring ......................................................................... 38
Annex 4: Detailed Project Description ...................................................................................... 48
Annex 5: Project Costs ................................................................................................................ 54
Annex 6: Implementation Arrangements .................................................................................. 55
Annex 7: Financial Management and Disbursement Arrangements ..................................... 57
Annex 8: Procurement Arrangements ....................................................................................... 68
Annex 9: Economic and Financial Analysis .............................................................................. 75
Annex 10: Safeguard Policy Issues ............................................................................................. 85
Annex 11: Project Preparation and Supervision ...................................................................... 87
Annex 12: Documents in the Project Fi le.................................................................................. 88
Annex 13: Statement o f Loans and Credits ............................................................................... 90
Annex 14: Country at a Glance .................................................................................................. 92
Annex 15: Map IBRD 33439....................................................................................................... 95
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 5/103
MADAGASCAR
MADAGASCAR SUSTAINABLE HEALTH SYSTEM DEVELOPMENT PROJECT
PROJECT APPRAISAL DOCUMENT
AFRICA REGION
AFTH3
Date: April 20,2007Country Director: Ritva S . ReinikkaSector ManagerDirector: Laura Frigenti
Team Leader: Mukesh ChawlaSectors: Health(100%)Themes: Child health (P);Othercommunicable diseases (P);Health systemperformance (P);Population and reproductivehealth (P);Nutrition and food security (S)
Environmental screening category: PartialAssessmentProject ID: P103606
Lending Instrument: Specific Investment L o a n
[ ] Loan [X I Credit [ ] Grant [ ] Guarantee [ ] Other:
For Loans/Credits/Others:Total Operation Cost (US$m.): 15.00Total Bank financing (US$m.): 10.00Proposed terms: The proposed credit would be on standard ID A terms, with a maturity o f40-vears. including a grace period o f e n vears.u u 1 .’
Financing Plan (US$m)Source Local Foreign TotalBORROWERRECIPIENT 5.00 0.00 5.00InternationalDevelopment Association 10.00 0.00 10.00(IDA)Financing Gap -10.00 10.00 0.00Total: 5.00 10.00 15.00
Amount o f financing to be provided bySource I Amount (US$m)
I
Borrower:MINISTRY OF HEALTH AND FAMILY PLANNINGMadagascar
Responsible Agency:

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 6/103
-Y4nnualSumulative
[XIYes [ ] N ooes the projec t meet the Regional criteriafor readiness for implementation?
Ref: PAD D. 7Project development objectiveRe$ PAD B.2, Technical Annex 3The project development objective (PDO) o fhe proposed Madagascar Hea lth SWA P i s tocontribute t o the strengthening o fhe health system, includingfinancing, delivery andmanagement, in order to improvethe access and uti l izat ion o fhealth services, especially in ruraland remote areas, and scale-up the production anddelivery o fhealth programswith an emphasiso n endemic infectious diseases, reproductive health (including fam ily plan ning sexuallytransmitted diseases, and H IV IA ID S) and nutrition.
0 0 0 0 0 0 0 0 00.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Project description[one-sentence summary o each component] Ref: PAD B.3.a, TechnicalAnnex 4
W hi ch safeguard policie s aretriggered, i f any? Ref: PAD D.6, Technical Annex 10
Significant, non-standard conditions,if any, for:Re$ PAD C. 7Bo ard presentation:5/22/2007
Lo ad cre dit effectiveness:
6/29/2007
Covenants applicable to projec t implementation :

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 7/103
I. STRATEGIC CONTEXT AND RATIONALE
A. C o u n t r y and sector issues
1. Madagascar has witnessed a remarkable dow ntur n since beco ming independentin 1961,with real per capita GDP decliningby over 25 percent during the last four decades to US$ 290 in2005. Caused in part by inward looking,highly protectionist policies and poor governance,Madagascar’s disappointing economic outcome has resultedin a deterioration o f physical andhuma n capital. T w o libera lization episodesin the late 1980s and 1990s led to growthbut provedshort-lived. The reforms o f he late 1990s, aided by pre fere ntia l trade access, resulted in export-oriented, private-sectorled growth, averaging ove r fou r percentduring 1997-2001. This progresswas interruptedby a politi cal crisis overthe contested 2002 elections, resulting in an economiccrisis, with GDP decliningby 13 percent in that one year alone. However, the polit ical crisisdidbring to po wer a democratic forcewith a refo rm agenda and renew ed hope fo ra more prosperousfuture.
2. Go od progress has been achieved since the polit ical and economic crisis o f2002. Prudentmacroeconomic management created an environment conducive t o economicrebound, reapingthe fruits o fprevio us liber aliz atio n reforms. De spite exogenous shocks such as cyclones andhigho i l prices, the macro-economic situation stabilized andthe economy grew at about 10 percent in2003 and has since continued to grow at a respectable 5 percentper year. Growth has comelargely through improved performancein agriculture, especiallyhigher rice production, highertourism receipts, and continued pub licinvestments. Despite increases in wo rld petroleum prices,a tight monetary po lic y has resultedin a decline in annual infla tion f rom 27 percentin end-2004to 10 percent in mid-2006. Similarly,th e measures adopted to ensure exchange rate stab ility andcompetitiveness and to secure an adequate l e v e l o f international reserves were broadlysuccessfbl, leading to greater stability o f the market-determined exchange ratein 2005. TheGovernment has also taken steps to confront corruptionand to improve the quali ty o f publ icsector governance. In an effort to improve public resource managementand strengthen publicservice delivery, the Government i s preparing a legal framew ork f or decentralization t o thel e v e lo fcommunes.
3. High gro wth has also resulted in improvements in basic social indicators, albeit from al o w base. Mo re children arein scho ol today, and netprimary enro lmen t rates exceed 90 percent.Immunization rates have improved andthe number o f births assisted by skilled medicalpersonnel has increased. I nfan t and ch il d morta lity rates have declined sig nifican tly over the lastdecade and chronic malnutrition has decreased. Similarly, progress hasbeen made o n reducingpoverty, wh ich declined to 69 percent fro mi t s peak l evel o f 80 percent at the time o f he 2002crisis. With the implementation o fthe rural roads program, reliable access to transport forth e
rural population has increased from45 percent in 2003 to 57 percent in 2005. Access to safedrinking water in rur al areas also im pro vedduring this period.
4. These positive developments are encouraging,but there is s t i l l a long way to go givenwhere Madagascar i s today relative to the rest o f the world. The macroeconomic situationremains fragile, especially as revenue mobilization remains weak. Poverty rates ares t i l l veryhigh wh ile social indicators are low, and Madagascari s not li ke ly to reach the poverty alleviationand health-related Millennium Development Goals (MDGs). The country also continues to face
1

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 8/103
fiscal problems, with significant revenue shortfalls in customs and tax collections leading to adecl ine in ta x revenues. Althoughthe economy has been on a rebound in the last tw o years, thecapacity o fthe Government to raise revenue remains severely constrained. Moreover, externalaid has been dwindling in recent years. As a result, overall government expenditurei s falling inreal t e rms and public spending on social programs i s declining bothin real terms and as apercentage o f he government budget.
5. Health i s a key goal o f Madagascar's second-generation p ove rty red ucti on strategy, theMadagascar A cti on P lan(MAP), 2007-201 1. T he MAP - which sets very ambitious targets inthe areas o f maternal and ch ild mortality,fertility rate, malaria, tuberculosis, sexually transmitteddiseases and HIV/AIDS control, and reductiono f malnutri t ionin childrenunder the age o f five -i s multi-sectoralin nature and recognizes the importance o fsystem and institutionstrengthening.Fol lowingthe MAP, the health sector strategy formulatedby the Ministry o f Health, FamilyPlanning and Social Protection (henceforth: M O H )in the Plan de De'veloppement du SecteurSante', or the PDSS, identifiesa number o fkey bottlenecks to increased access and use o f hea lthservices and improvements in health indicators in Madagascar. Four critical areas o fweakness
are highlighted: (i) oorly equipped health centers and low levelso capacity to produce anddeliver health services, especially in r ur a l and remote areas(managerial capacity atthe l e v e lo fcommunes i s weak); (ii) neven staffing o health facilities, especially in r ur al a nd remote areas(a large number o f health centers, partic ularlyin rural and remote areas, do not have adequatenumbers o f qualified staff);(iii) ow levels of health financing and inefficiencies in resourceallocation (Madagascar spent around US$6 per capita o n health care in 2005, significantly lowerthan the average for sub-Saharan Africa, exclud ing Sou th Africa, o f US$15.4 pe r capita); and(iv) inadequate demand for health services and low levelso uti l izat ion(only 10 percent o f thepopu lation reports an illness annually, and o f this, on ly 40 percent seekscare from qualifiedme dica l personnel). The MAP provides the appropriate entry poin t fo r a n integrated sector-wideapproach in the design o f he Sustainable HealthSystem Developme nt P roject (SHSDP).
6. The Wo rld Bank has been supporting the health sector through a number o f heal th-specific and multi-sectoral projectsin the past decade, several o f whic h are ongoing. Theseinclude the Second Health Sector Support Project (CRESAN 2), which was approved inNovember 1999 in the amount o f US$40 mill ion,with the objective o f contributing toth eimprovement o f the population's hea lth status thro ugh mo re accessible andbetter quality o fhealth services, especially primary health care services in rura l areas. CR ES AN 2, wh ichreceived a supplemental credit o f US$18 m ill io nin M a y 2005, supports priority health programs(with an emphasis on endemic infectious diseases, reproductive health and nutrition) andcontributes to the strengthening o f sector management a nd ad ministrative capacitywithin M O H ,especially at provincialand district levels. CRESAN2 i s expected to close in December 31,2007. Other projects inclu dethe MultisectoralSTI/HIV/AIDS Project (US$20 million, closing
date: December 2007), Second Multise ctoral STI /HIV /AID S Project (US$30 million , closingdate: December 2009), Co mmu nity Developme ntFund (US$l78 million, closing date:June2008), and Second Commun ity Nut rit io n Project (US$47.6 million, closing date: December2008).
7. The proposed Madagascar SHSDP represents the next stage with respect to the Wo r l dBa nk and other development partners' support for the he alth sector.There i s general consensus
2

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 9/103
among development partners that a sector investment and maintenance loan for financingthesupport to the health sector i s preferred to general budget support as the primary vehicle forfinancing. Therei s widespread recognition thatthe challenges in health are too specific and th esector i s too fragmented to fully benefit from pure budget support, and that a transition phase o fsector specific support i s needed. The World Bank’s Independent Evaluation Group (which
completed a country assistance evalua tionin July 2006 o fIDA’S nvolvement in Madagascar fo r1995-2005) also recommends limitingthe role o f budget support until there i s a sustainedimprovementin collectingand managing pub lic resources.
8. The approach that has been used in the design o f this sector investment credit i s one thatencompasses the entire health sector and supports the health reform and scaling-up program o fthe Government o f Madagascar. Man y development partners, in clud ingUnited NationsChildren’s Fund (UNICEF), United Nations Fund for Population Activities (UNFPA), WorldHealth Organization(WHO), United Nations D evelopment Programme (UNDP),United StatesAgency for International Development(US AID), Japanese International Cooperation Agency(JICA), European U ni on(EU), African Development Bank (AfDB), Agence Franqaise de
De‘ve‘loppement (AFD) as well as th e French Cooperation, are currently workingin Madagascarthrough parallel financing to addressthe dysfunctions and bottlenecks within the health caresystem. The Madagascar SHSDP wo uld add valueby facilitating greater coordination amongdevelopmentpartners and ensuring that the ongoing interventions and support do not overlap,butrather are synergistically related to one another and consistent with the Government o fMadagascar’s vision for developmentresults to be achieved in the sector. This intervention i sthus part o f a more complex, multisectoral agendain Madagascar, and one o f t s m ain functionsi s to coordinate efforts o f various stakeholdersin order to achieve greater cohesion. Moreexplicitly, giventhe on-going activitiesand the small amount o fthe proposed financing (U S$ l 0million), this project aims at building capacity within M O H and coordinating on-goinginterventions in Madagascar and l inking these closely to results. Based on a sector-wideapproach, Madagascar SHSDP embodiesa process that has Government leadership as i t s startingpointand progresses towards increased harmonization o f mplementation mechanismsand us e o fcountry systems. What distinguishesthis projec t fro m others beforei s the sustained, country-ledpartnership among development partners and key stakeholders in support o f country-ownedsector policies and strategies.
B. Rationale for Ba nk involvement
9. The proposed operation i s included in the Country Assistance Strategy (CAS) forMadagascar covering the period o f 2007-11. Key CAS goals supported by the project include“improving services to people” (Pillar I1 o f the CAS) and “achieving better outcomes ineducation and health.” In health, the focus in the CAS i s on helping the Government make
further progress on reducing child and maternal mo rtality b y offerin g access to reproductiveservices, reducing child malnutrition, improvingthe availability o fclean water and sanitationservices, and keeping HIV/AIDS and sexually transmitted disease rates under control. Theapproach o f the proposed Madagascar SHSDP - alignment with the government program asoutlined in the MA P, harmonization and coordinationwith other donors, and integrated sector-wide approach to health - s consistent with the CAS principlesand approach.
3

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 10/103
10. The rationale for the Bank’s continued involvement in th e health sector i s strong.Consolidationand scaling-up o f support for basic servicesin health is essential for Madagascarto achieve progress towards meeting the MDGs. The current financial support providedbyC R E S A N 2 will be exhausted by September 2007. The proposed Madagascar SHSDP willsustain and gradually enhance IDA financing as well as leverage other donor financing forthehealth sector in Madagascar within an agreed medium-term fiscal framework.The Bank i s in aunique position tohelp Madagascar po sitio ni t s e l fto p ro fit f ro m scaling-up opportunities astheyarise and play a catalytic role in leveraging addit ional resources, including those from otherdevelopmental partners. In l i ne with ID A-1 4 goals on leveraging andpartnerships, the IDAcommitment to th e health sector will be critical in leveraging a large amount o f developmentassistance from other donors. The Bank i s a nodal agency in a consortium that i s being puttogether to support the health sector via the sector-wide approach. The consortium includes theAfDB, AFD, the EU, the French Cooperation, JICA, UNICEF, U NFP A, U SA ID , WH O, andtheWo rld Bank.
11. Madagascar SHSDP supports clear opportunities to boost progress o n pro-poorand
potentiallyhigh impact activities, inclu din gthe immuniza t ion o fchildren, controlo f malaria, andpopulation and familyplanning. Finally,the Bank and otherpartners ar e well positioned to wo rkwith the Government o n challenges o fthe health sector at the po li cylevel . The involvement o fthe Bank i s important to bring Government, civil society,and development partners togetheraround a common vision o feffective service deliveryand improved accountability.
C. Hig her level objectives to whi ch the p roject contributes
12. Madagascar SHSDP supports the development o fthe health sector in Madagascar, with astrong focus on strengthening al l aspects o f health systems, in clu din g production, financing,delivery, stewardship and governance. The achievement o f he goals o fhe sector wide programwill, inter alia, include reductionin maternal, ch il d andinfant mortality, fertility rate, chronicmalnutri t ionin children under the age o f hree, HIV prevalence, and prevalence o fsyphilis inpregnant women. The successful adoption o f SHSDP i s expected to yield a number o f o therdevelopment benefits as well, including strongercountry ownership and leadership, and greaterfocus on results. In addition, the Sector-Wide Approach o f Madagascar SHSDPwill encourageand foster coordinated and open policy dialogue, guide alloca tion o f resources based onpriorities, and facilitate scaling-up o fbenefits to entire sector. I t will also enhance sector-wideaccountabilitywith com mon fidu ciary standards, andstrengthen the country’s capacity, systemsand institutions.
13. The project’s fiduciary dimensions and focus onstrengthening public budgeting,financial management and procurem ent alsofit with broader efforts in this directio n supported
by other Bank projects, especially the fourth Poverty Reduction Support Credit (PRSC).Channeling funds o fparticipatingdevelopment partners throug h a com mon an dwidely acceptedprogram o f eformwill help strengthen oversight o fsectoral progra ms and will have externalitiesbeyond the health sector. Ac tivitie sunder Madagascar SHSDP also emphasize transparency andpredictabilityin budgeting and sectoral planning and are thus in keeping with higher-levelobjectives in governance and public sector, and public expenditure management reform.Aspects
4

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 11/103
o f he project and PDSS also respond to CA S objectives o n stemmin g the declinein ke y servicesand addressing governance constraints t o grow th and p ove rty reduction.
11. PROJECT DESCRIPTION
A. Lending instrument
14. The proposed proje ct will be financed through a sector investment credit o f an amountequivalent to US$1 0 million,implemented over a 30 -month perio d from July 2007 to December2009. The ini t ial IDA financing will be pooled with contributions from theAFD (tentativelyUS$15 mi l l i o nbeginning January 2008), and supported through parallel financingby otherdevelopment partners, includingAfDB (US$lO mill ion), JIC A (US$2 mill ion), UN IC EF (US$14million), UNFPA (US$2 million),USAID (US$15 mill ion), and WHO (US$lO mill ion).TheEuropean Union will continue to provide direct budget support to the Government o fMadagascar, wh ich i ndir ectl y supportsthe hea lth sector. This project isthe f i r s tphase o f a longert e r m program which, overtime, wo ul d a im at results-based financing.At the end o f he two-and-a-half years o f mplementation, additional financing wou ldbe sought to continue support t oth emedium-term objectives o f heMAP and PDSS through 2011.
B. Project development objective and key indicators
15. The project development ob jective o f Madagascar S HSD P is to contribute t oth estrengthening o f he health system and enhance the institutiona l capacity o fM O H o im pr ov etheaccess and utiliza tion o fhea lth services, especially in rura land remo te areas.
16. A series o f ndicators will be used to monitor project, programand sector performanceunder SHSDP. Since the engagement o f he World Ba nk and use o fIDA resources will leveragewider support for the MAP and provide the necessary technical expertise and support forrealization o f MAP’S objectives, Bank’s performance will be measured by i t s abil i ty toharmonize resources and efforts o f a ll development partners, facilitate th e measurement o fresults, strengthen capacity for measuring results; and improve management capacity withinM O H . A broader panel consists o f indicators trackingand measuring resources, processes,outputs and outcomes will be used to m onitor the objectives o fMAP and interventionsunderPDSS. For each series o f indicators, the M O H will record the baseline value, confirm thefrequency o f monitoring andthe institutions responsible for doingso, and se t targets forachievement by 2011. These are summarized in detail in Annex 3.
C. Project components
17. T w o fundamental guiding principles formthe basis o f the proposed health project inMadagascar. First, strengthening o fthe health system (including the private sector)i s central toensuring the production, financing anddelivery o f specific interventions such as thoseneeded t oreduce infant, child and maternal mortality, improve maternal health, dramatically reducemalaria, sexually transmitted infections, andHIV/AIDS, and improve the nutritio n status o fchildrenin Madagascar. Th e hea lth system encompasses a l l activities, organizations, governancearrangements, and resources (public and private) dedicated prim ari ly t o im provin g, m aintaining,
5

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 12/103
or restoring the health o f ndividuals and populations,and to prevent households from fallingin to pover ty o r becomingfurther impove rished as a resul t o f llness. Second, he alth outcomes aremulti-sectoralin nature, and are strong ly influen cedby income, education, access to clean waterand sanitation, access to clean ind oo r environments, goo d countr y governance, and soundmacroeconomic polic y. I mp rov ing health outcomes, therefore, requiresan effective multi-sectoral approach to health performanceand outcomes.
Table 1: Rc
Provision ofquality healthservices, esp. inremote areas
Eradication o fmajor diseases
Implementationof a familyplanningstrategy
Reduction inInfant andChild Mortality
Reduction inMaternalMortality
Promotion o fHygienicPractices
ationship between MAPStrengthening Deliver y
- Strengthen health centers to deliverbasic package of services- Ensure adequate supply of drugsand equipment at al lhealth centers- Provide Mobile Health Centers forremote areas- Strengthen capacity andcompetencies at decentralized evels
- Strengthen capacity andcompetencies at decentralized levelsto manage and coordinate campaignsfor vaccination etc. and maximizecoverage- Strengthen capacity andcompetencies at decentralized levelsto manage and coordinate effectivecontrol o fmalaria, includingspraying, bed-nets, etc.- Ensure adequate supply ofequipment and testing facilities at a l lhealth centers for STIs- Strengthen capacity andcompetencies at decentralized levelsto manage and coordinate campaignsfo r family planning- Ensure application o f agreedquality standards and protocols at al lhealth centers- Ensure adequate supply o f servicesand drugs for infant and child healthat al lhealth centers- Strengthen capacity andcompetencies at decentralized levelsto organize and manage communityagents and health workers onuniform procedures for treatingchildren under 5 .- Ensure adequate supply o f drugsand equipment for management ofpregnancies and deliveries at al lhealth centers- Strengthen capacity andcompetencies at decentralized levelsto manage community agents forimplementation of the roadmap forreduction of maternal mortality.- Strengthen capacity andcompetencies at decentralized levelsto organize and manage communityagents for promotion of hygienicpractices
bjectives and Me asu iManagement o f HumanResources- Contract and redeploy nursesand midwives to al l level 1 and2 health centers- Improve working conditionsof health personnel, especiallyin rural areas- Train nurses and midwives todeliver basic health services- Empower decentralizedlevels by transferring thenecessary competencies andresources to better staff andmanage health centers- Improve training o f healthagents to prevent, diagnoseand adequately treattuberculosis- Strengthen capacity o fprivate services providers todiagnose and treat STIs.
- Improve training of healthagents in family planning
- Improve raining of healthagents on uniform proceduresfor dealing with diseases i nchildren under 5- Train staff n health centersand first level hospitals ntreating children and new-bornbabies
- Train a ll staff n healthcenters and first level hospitalsin pregnancy and deliverymanagement
s to Strengthen H eInnovations n HealthFinancing- Develop nnovativeprovider paymentmechanisms to contractand redeploy nurses andmidwives to a ll level 1 and2 health centers- Develop nnovativefinancing methods, such associal insurance or socialsecurity, to increase the useo fhealth services by thepoor
-Develop nnovativefinancing strategies toensure sustainability andavailability of FamilyPlanning programs andtraining of health agents infamily planning
!th SystemStimulation demandand Utilization- OrganizenationaVdistrictcampaigns to increaseawareness so as tomaximize utilizationand effectiveness
- OrganizenationaUdistrictcampaigns to increaseawareness so as tomaximize utilizationand effectiveness
- Organize campaignsto promote familyplanning and use oflong-lastingcontraceptive methods
- Organize campaignsto raise awareness fo rimproved managementof children diseases
- Organize campaignsto mobilizecommunities forincreased uti lization o fmaternal and neo-natalservices
- Organize campaignsto promote widespreadutilization of hygienicpractices, including theWASH strategy
6
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 13/103
18. The design o f SHSDP has been developedby M O Hand the development partners o n th ebasis o f a ma tr ix o fkey health programsand interventions, in whi ch the rowsl i s t the interventionareas o f the MAP and the columns l i s t the key elements o f system capacity that need to bestrengthened. The project seeks t o shift away f ro m specific vertical interventions andstrengtheninstitutio nal arrangements o fthe hea lth sector, so as to increase the efficien cy o f donor support(includingIDA resources) t o the Government’s health pol ic y and programs. Table1 shows therelationship between MAP objectives and measures supported by SHSDP to strengthen keysystemic elements. M O H hasfull ownership o f hismatrix and o f all the tasks listedin each o fthe cells, while the essential role o f the Ban k is seen to be that o f providin g assistance andsupport through this project to stitch together the different elements o f he systemic and relatedinterventions. The Bank’s role i s thus t o guide the matrix and help the Government o fMadagascar develop and use tools to track and monitor resource flow s in tothe sector and todevelop and use tools that will help sectoral leadership track changes in health systemperformance and h ealth outcomes.
19. Activities and interventions directed toward con trol o fHIV-AIDS and malaria, currently
financed almost entirelyby l ine in tervent ions o f M O Hand some development partners, are notincluded as part o f SHSDP att h i s stage, but will be gradually integrated in subsequent stages.
20. Madagascar SHSDP thus supports the four critical components as suggestedby the fourcolumns in Table 1 wh ich seek to im prove he alth financing, delive ry and management through aprogrammatic approach encompassing strengthening delivery o f resources, developing andmanaging human resources, improving health financingand management, and stimulatingdemand and utilization o f health services.The fifth component o f SHSDP i s institutionalstrengthening, which will support the capacity and abil ity o f M O H o track progress and makenecessary adjustments in the course o f implementation,and support the strengthening o f thecapacity o f M O H in various domains, including planning and programming, financialmanagement and procurement. Indica tive allocationsby component and by activitywi ll be madefor the project period; however, the actual allocationswill be adjusted based on the bi-annualjoi nt reviewsby Government and i t s development partners in he he alth sector and based o n theGovernment’s A nnu al W or k Program, asprepared by M O H .The detailed project descriptionbycomponent i s in Annex 4.
21. Component 1: Strengthening Delivery of Health Services (US$5.3 million): Thiscomponent seeks to strengthen healt h service delive ryand quality o f services at the prim ary andfirst referral levelsin districts throug h capacitybuilding o f districts tobetter organize, manageand deliver hea lth goods an d services, and provision o f goods and services tostrengthen healthcenters, includingdrugs, medic al supplies an dequipment.
22. Component 2: Development and Management of Human Resources in the HealthSector (US$U.9 million): The objective o f t h i s component i s to improve human resourcemanagement in the health sector with particular emphasis on rural areas. To this end, thiscomponent will finance development o f innovative mechanisms t o prov ide incentives to ru ralbased personnel and promote enhanced performance o f such personnel, and trainin g o fal l healthpersonnel o n basic he alth service delivery, such as diagnosis and treatment o f nfe ctio us diseases,pregnancy and delivery management, and health care-for childre nand new -bo rn babies.
7

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 14/103
23. Component 3: Innovations in Health Financing Management (US$O. 6 million): Thiscomponent seeks to support creative resource mobilizat ion and strengthen health resourceallocation, through the developmento f a variety o f mechanisms designed to m obilize additionalhea lth resources throu gh programs su ch as social insurance, and thro ug h imp ro ved managemento fexisting private and publicfunds fo r the health system.
24. Component 4: Improving Demand and Utilization of Health Sewices (US$l.O5million): This component will endeavor to stimulate demand fo r quality health services throughcommunity education and awareness campaigns, and developing mechanisms for conditionalcash transfers.
25. Component 5: Institutional Strengthening (US$2.15 million): This component willsupport a number o f system development a nd institu tional strengthening activities, such asprocurement and finan cial managementand program oversight. In addition, the component willfinance a number o f monito ringand evaluation (M&E) activities, including development o f an
M&E plan, support to the National Health InformationSystem and strengthening o fGovernment’s ana lytical capacity forbetter use and management o fdata.
26. Activities undertaken underthese components are expected to result in significantimprovemen ts across a range o fdemand-side, supply-side and institutio nal aspects o f he healthsystem, especially in the production anddelivery o fquality services in ru ra l and remote areas, inboth publicand private sectors. Visi bleresults are expected in he deployment, effectiveness andmorale o fhea lth teams at service delivery points, in particular in remote areas, accompanied byless obviousbut important changes in the nature o f support p rovided tothem by district, re giona land central l eve l managers. Teams at the regional and district levels and at health care servicedelivery points will wo rk together to plan,implement and monitortheir programs in compliancewith national priorities and strategies, and will be encouraged to systematically use qualityassurance methods to solve problems, work collaborativelywith local authorities, NGOs andother partners, and dra w upo n resources fro m outside o fthe health budget to address healthproblems in their communities.
D. Lessons learn ed and reflected in the pr oject design
27. The design o f Madagascar SHSDP draws upon a number o f lessons learned fr ominternational experience and fr om implementation o f a series o f health projectsin Madagascar.The follo wing arethe most impo rtant lessons:
28. Need for clear development goals acceptable to all stakeholders. Also linkedto this i s theneed to agree on a coherent results cha in and choose appropriate per forma nce indicatorsthat arein l i ne with the development objectives. These shouldthen be used for systematic monitoringand regular discussion o f mplem enta tion performancewith the Government.
29. Importance of a comprehensive and harmon ized approach to the health sector. There i sfull agreement among the Government and the development partners on the need for a
8

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 15/103
comprehensive approach to decrease the burden o n the health system at a ll levels o fthe healthpyramid. The elaboration o f a c ommo n strategyin t he fo rm o fthe PDSS was the f i r s t step inmo vin g towards a comprehensive and harmonized approach.This planning exercise has helpedboth the Government andthe donors to w or kin close pa rtnership and share information,so as todevelop an integrated and common strategy. By improving coordination and harmonization
among donors, Madagascar SHSDP i s expected to improve allocative efficiencyby diminishingtransaction costs for the Government. Moreover, budget execution in the health sector i s veryl o w in large part because M O H has problems in managing the available financial resourcesbecause o f the difficulty o f coordinatingand monitoring donors’ projects, limited financialabsorption capacity, and heavy and comp lex procedures that vary fro m one donor t o another.Madagascar SHSDP should help alleviate these difficulties .
30. Technical assistance and capacity building in planning and management is critical tosuccess on the ground. Implementation experience fro m C RE SA N2 demonstrates the need fo rsubstantial technical assistance to MOH, particularlyin th e areas o f planning, budgetmanagement and tracking. Since the 1990s, several donors have been strengthening the
capacities at the health districtlevel . The
planning, programming and mon itorin g functions o fregional and district health management teams have been strengthened through CR ES AN 2,wh ich has supported 40 percent o f recurrent costs at the district level . The performance o f hedistrict management teams has improved as a result o f echnical support ands taff recruitment.All but a f e w o f he districts are n ow able to formulatetheir three-year plans and develop annualwork programs using clear norms and criteria. Healthsystem management at the district l e v e l i sthus improving, althoughbudget management capacity remains a major challenge. Experienceshows that bottom-up planning accompanied by capacity strengthening activities and flexiblefinancial resources to implement the activities arekey elements for achieving results o n theground. For example, budget execution i s much higher in CRESAN-supported districts thaninothers. Further, while the internal state budget has l i t t l e flexibility across categories o fexpenditures, the more flexible CR ES AN allocation to districts has allowedthem to carry outinnovative outreach activities to increase utiliza tiono f preventive hea lth care services.
31. Analysis and use of data for decision-making. Madagascar has already se t up a systemo f routine data collection forthe health sector, and a large number o f studies an d surveys havebeen undertaken. Unfortunately, mu ch o fthis info rma tion and data remainsunused, and there i sa pressing need to d evelop ana lytical capacitywithin this system t o ensure better us e o f availabledata. Further, the creation o f an integrated and comprehensive he alth sector mon itorin g an devaluation system will be essential for pr oject managementand will facilitate periodic evaluationo fprogress an d decision-making.
E. Alternatives considered and reasons fo r re jection
32. Support to the health sector throu ghbudget support under the Poverty Reduc tion SupportCredits was rejected because o f the relative fra gilityo f the macro environment which wouldexpose the sector to economy-wide shocks outside the control o fthe Government. Althoughinrecent years the Governme nt has imp rove d management o f these external shocks (such ascyclones, o i l pric e increase etc.), pr io rit y sectors cannot yet be insu lated as necessary fr o m such
9
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 16/103
negative events. The perceived fragil i ty o fpublic financial management, procurement systemsand ministry efficiency in service delivery cautions against the use o f budget support for aministry which provides vital services to the population. Based on this assessment, i t wasdeemed critical t o earmarkfunds fo r the health sector under Madagascar SHSDP. The use o f anAdaptable Progr am Lo an was also considered given the phased programmatic approach.
However, the development partners group did no t want to condit ion subsequent phases o finvestment. Thus a sector investment loa nwas considered to be the best optionunder the currentcircumstances.
111. IMPLEMENTATION
A. Partnership arrangements, coordination and implementation support mechanisms
33. M O Hwill establish and agree o n an Annual Wo rk Programin cooperationwith financingand implementing partners, consistent with the policy framework outlinedin th e PDSS and anestimated resource envelope fo rth e follo wing year.The Annual W ork Programwill also foreseeappropriate technical assistance, training and institutionstrengthening measures to support thefull integrat ion o fplanning and managerial functions i nto theexisting core government agencies.A Memorandum o fUnderstanding signed by the Government and i t s development partnerspo oli ng their resourceswill outline organizational, institutio nal and co ordina tion arrangementsfor implementation and the roles and responsibilities o f each partner. Co operationwithdevelopment partners and supervision will be coordinated by means o f bi-annual He althSummits between the Government andimplementing agencies.
B. Institutional and implementation arrangements
34. M O Hwill be responsible for the overall oversight o fhe nation al health program aswell
as o f Madagascar SHSDP. The Ministry’s Management Team will function as the steeringcommittee fo r oversight o f implementation o f projectact ivi t ies and monitoring o f progress toachieving development objectives.The existing project coordinationunit (PCU) for CRE SA N2will be uti l ized for the day-to-day coordin ation o f projec t activities.This PCU has alreadydemonstrated i t s capacity both to manage IDA’S financial management and procurementprocedures and to innovate effectivelyat a l l levels o f the healt h care system to improve theaccessibilityand quali ty o fhea lth services.
35 . In close collaborationwith the Directorate o f Financial Affairs andthe Directorate o fPlanning within M O H , the P C U will be responsible fo r annual program planning an dbudgeting.MO H, throughi t s Secretary General, will: (i) nsure consistency o fprogram activitieswith the
Government’s po li cy an d strategy;(ii) pprove the annual works pro gram andbudget; and (iii)follow-u p o n project performanceand implementation progress. Specifically,the P C U will beresponsible for program management including:(i) oordination o f program implementation;(ii) onsolidation o f district-level w ork programs andbudgets; (iii) aintenance o f records andseparate accounts for all transactions related to the PCU; (iv) preparation, consolidation andproduction o fthe progra m finan cial statements, quarterly financia l management reports(FMRs)and other financial informationrequired by the Government; (v) management o f the pooledaccount; and (vi) monitoring and evaluation o fhe various activities supported under the project.
10

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 17/103
The P C U i s currently headed by a Coordinator nominatedby MO H, and exist ings taff includespecialists in accounting, procurementand monitoring and evaluation.
36. The implementation o f program activitieswill be entrusted to : (i) echnical departmentso f M O H ; and (ii) perating units at the regional/district levels,which will receive timely
payments from the P C U based u pon submission o f satisfactory quarterlybudgeted wo rk plans.The operating u n i t s at the regional/district levelswill manage disbursements fr om the ir o w n bankaccounts. Under the supervision o f the financ ial officer(s),they will maintain records andaccounts fo r a ll transactions, and prepare financial report and other basic in form atio n o n proje ctmanage ment/monitoring asrequired by the PCU.
37. The P C U will continue reporting directly to the Secretary-General andwill carry outadministrative tasks, inclu din g keep ing accounts, organ izing an d overseeing procurement,andoverseeing activit ies carried outby other M O Hdirectorates, districts or undertakenwith externalassistance. An in-depth capacity assessment o f the P C U and M O H under takenduring appraisalconfirms that the P C U s adequately staffe d and that appropriate resources havebeen earmarked
to meet project imp lemen tation needs.
38. Bi-annual health summits will be led by M O Hwith the participation o f a ll stakeholdersand development partners as we ll as representatives f ro m c iv il society, private sector and otherrelevant ministries. Progress o n the national programwill be reviewedduring these summits andwill provide input into the Annual Work Program forthe Ministry. These Summits will alsoall ow evaluation o f progressin achieving the development objectives and towards the MDGs.These discussions will also b e used to fine-tune the project and the program to changes thatmight occur in the sector and t o coordinate, at technica llevel, with al l partners.
C. Mo n i to r in g and evaluation o f outcomeshesults
39. The five-year PDSS lays down aResults Framework to be used as the foundation forseveral critical program maticevents and processes, including strategic planning, communication,monitoring and evaluation, and learning. The Results Framework focuses on monitoringresources, processes and outpu ts directly related to actions and activitiesimplemented by M O H .In order t o assess the relevance, performance a nd success o f ongo ing and completed prog ramsand projects, three broad sets o f indicators will be used: (i) ne se t to measure and trackavailabilityand use o f esources; (ii) ne se t t o assess the effectiveness o f system processes, and(iii) ne se t to measure the outputs resulting from these processes. Finally, a se t o f outcomeindicatorswill be used for b road sector m onit oringand attentionby high-level pol icy makersanddevelopment partners. In addition, the interventions supportedby the World Bank andIDA willbe monitored through a parallelbut relat ed system that will track the specific inputs and results
that will be facilitated, enabled or procured throug h Ban k andIDA involvement.
40. The institutional arrangements for monitoring and evaluationunder the ResultsFramework will invo lve a progressive absorption o fthe functions o f the P C U into the coredepartments o f the Ministry. In the meantime, the PCU will be responsible for organizingthecollection, analysis, presentation an d dissem inatio n o fthe four sets o f indicators, with thetechnical support o f development partners. D ata collect ionwill mainly take place usingthe
11

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 18/103
existing report ing mechanisms. O vert ime, a Center f or H ealth Po licy and Developmentwill beestablished within the Ministry, wh ich w ould overseethe mo n i to rin g o fprogress o n the ResultsFramework. Other functions o fhis body w ou ld include data analysis fo r dec ision making, heal thpo licy analysis, and health po licyand management training.
Risk rating w/mitigation
S
D. Sustainability
Risk M itigation measures
A specific project component focuses on identifying innovativesolutions o attract qualified health personnel to rural areas.
41. Although the Government will continue to rely o n extern al assistance f or health sectorfinancing in the foreseeable future, the Government will need to take steps to improve thefinancing o f recurrent expenditures within the national budget. The Sector-Wide Approachadopted for this project, based on the n ational health polic y and an integrate d annual budget,i s
expected to reduce the fragmentat ion o f inancing provided tothe sector, imp rove tech nical andallocat ive efficiency o f public expenditures, and contribute tothe sustainabil i ty o f nvestments.Moreover, the al ignment o f the national heal th budget and h um an resource strategy with th eagreed prio rities w ou ld further enhance sustainability, especially since a ll development partnerswould have a de facto vested interest in building the institution al capacity o fthe M i n i s t r y t o
make allocationand disbursement decisions, implement strategies, an d evaluate im pac t.
M
M
M
S
M
S
M
E. Critical risks an d possible contro versial aspects
The project s part of a long term multi-donor effort and aimsduring the first two years at strengthening the health systems.A specific component deals with stimulating health servicepreventive behavior as well support to the poorestT h e Bank health team wil l work closely with the macro team toensure budget tracking by Finance and protect certain priorityprograms. Government’s commitment o MA P goals at the highestlevel helps maintain focus on priorities.The program ncludes support to increase the quality and quantityof services supplied. Demand stimulation activities may be linkedto capacity increases.Experience with FANOME / solidarity funds suggests that somepeople may be lef tout o f community-based targeting. The projectincludes development and piloting o f alternative argetingmechanisms.Integration of he CRESAN 2 accounting staff into the PCUstructure. Elaboration and implementation of an accountingmanual o fprocedures and organization o f raining for staff.Review of he CRESAN 2 computerized accounting system inorder to satisfy reporting requirements. Recruitment of aninternational auditing firm acceptable to I DA to carry out annualaudits of the project financial statements.
Table 2: Risks and Risk Mitipation MeasuresRisks
F ro m Outputs to Objectives:Health personnel do not want to moveto rural areas.Project time i s too short and resourceslimited to have a measurable mpactHealth service strengthening does notresult in utilization o f health servicesMinistry moves away from agreedactivities and redirects own budgetresources away from agreed priorities
From Components to Outputs:Demand for basic health services i s
stimulated but supply cannot respondConditional cash transfers do notreach the intended target population
Risk o f delays in he production offinancial reports, and audit may not beconducted in compliance withinternational auditing standards.
Overall Risk Rating I
12

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 19/103
F. Loadcredit conditions and covenants
42. Con dition s and covenantspertaining o the credit include the followin g:
(a) Board Conditions: (i) pening o f pooled account in a local commercial bank under
cond itions acceptable to donors.
(6) Conditions o Effectiveness: (i) stablishment o f an internal audit departmentwithin M O H ;and (ii) dopt ion o fproject implementation manualand the proje ct accounting manual.
(c) Financial Covenants:(i) he P C U shall ma intain records and accountsin accordance withsound acc ount ing practices; (ii) ina ncia l statements sha llbe audited bi-annuallyby independentauditors acceptable to IDA; (iii) ndependent auditors will be appointed within four months afterthe effectiveness date; and (iv) P C Uwill produce quarterly FMRs.
IV. APPRAISAL SUMMARYA. Economic and financial analyses
43. The underlying rationale for Madagascar SHSDP - he need for the Government toimpro ve budget sustainabilityby incrementally increasing pub lic fin ancing f o r the health sector,mitigating allocative and technical inefficiencies, imp rovin g targeting o f esources fo r vulnerablegroups and high prior ity health programs, and fo r reducing fragmentationin donor support an dstrengthening inkages with M A Pand PDSS - s a val id one.
44. With less than US$300 per capita and about 7 0 percent o f ts populationliving in poverty,Madagascar i s one o f he poorest countries in the world. After beco ming independentin 1961 the
country witnessed a lo ng period o f economic declinedue to p oor governance and protectionistand inward lo okin g policies. T wo liberalization episodesin the late 1980s and 1990s imp rove deconomic performance. After the second episode, the country experienced a period o f growthpowered by the dynamisms o f the industries that benefited from preferential trade access.Between 1997 and 2001, GDP grew at about 4 percent per year, while infla tion waskept undercontrol. However, the political crisisin 2002 halted this trend as GDP dropped by about 13percent. After 2002 the new Government’s sound macroeconomic management was able toconsolidate the gains o f previous liberalizationsand, despite large external shocks, growthresumed and has contin ued at about 5 percentper year. Despite al lthis progress many challengesremain given the country’s l o w socioeconomic indicators and the government’s diffi culti esinmo bi liz in g interna l resources. Fiscal resources havenever been above 11 percent o fGDP and the
countrydepends more and more onhighly unpredictable fo reig nfunds.
45. Madagascar spends very l i t t l eo n health, a situation thatwill worsen once don or financedprojects close. Ac cord ing t o the Natio nal He alth Accounts 2003, Madagascarspent about US$12per capita o n health that year, corresponding t o about 3.5 percent o fGDP. At the cd-rent l evel o fexpenditures, the country will no t be able to achieve the health-related MDGs. M O H , with thesupport o f UNICEF, calculated that an additional US$5.40per capita wou ld be needed in thenext three years t o achieve a 41 percent reduction in ch ild mort ality and a 35 percent reductionin
13
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 20/103
neonatal and maternal mortality needed to sustain progress in achieving these MDGs. Thisfinanc ing gap cannotbe lessened in the short run with intern al resources given the Government’smacroeconomic constraints.
46. The Government i s unlikely to sustain even these l o w levels o f expenditures on health,
mu ch ess achieve the expenditure levels o fhe Medium Term Expenditure Framew ork(MTEF),withou t additional financial aid fro mthe donor community. The CRE SA N2 project, which hassupported financially the health sector since1999, is scheduled t o close in December 2007. Thispro ject alone increasedthe funding o f he ministry by U S $ 4 0 mil lio n. Fo r instance,in 2004 thisproject financed close to 31 percent o f all M O H expenditures classified asinvestments. Thisfigure rose to 65 percent in 2005. Other projects that have also supported the sector are alsoapproaching their closing dates, including th e Multisecto ral STI/HIV/AIDS Project(US$20mill ion), whichwill close in December 2007, and the Community DevelopmentFund (US$ 176million), whic hwill close in December 2008.
47. Madagascar SHSDP a ims at filling this gap whi le at the same time lessening some o f he
public expenditure management bottlenecks confrontingthe Government, including vola tility o fdonor funds and large transaction costs created by projects with different management andreportin g mechanisms. In addition, the proposed projec t will contribute t olessening some o f hedistortions created by the fragmented foreign aid, especially as all donors agree not only tosupport a health strategy with a corresponding MTEF, and to progressively harmonize theirprocedures to follow a unique monitoring and evaluation system. This coordination andharmo nizatio n between donorswill lessen the volat i l i ty o f donor supportand will decrease thetransaction costs o f the ministry as i t would no tneed t o fo l lowdifferent procedures to managedifferent projects.
48. Government interventionin some o f the activities financedby Madagascar SHSDP i sjustified as they are aimed at reducing market failures due t o the presence o f externalities orpublic goods. Infectious diseases, particularly malaria,are th e major causes o f mortalityandmorbidity in Madagascar, especially among childrenunder five. SHSDP will finance manyactivitiesaimed at preven tion and treatment o fm a ny o f hese diseases, such as imm un iza tio n fo rchildhood illnesses, testing and treatment o f sexually transmitted diseases, etc. In addition,SHSDP will finance activities aimed at reducingthe inequalities in access and utiliza tion o fheal th services. Some o f these activities will also improve efficiency in the use o f publ icresources.
49. There are large income inequalitiesin the utilization o f health servicesin Madagascar,due partly to lower physical access to health servicesin rural isolated areas, and partly tofina ncia l and cu ltur al barriers to access services.The recurrent budget o f he ministry o fhealth i s
unequally distributed across regions, and in general, richer regions receive higher amounts o frecurrent budget per capita than poorer regions. This partly reflects an unequal distribution o fqualified medical personnel, which benefits richer urban areas, and partly thehigherconcentration o f health facilitiesin better-off regions. SHSDPwill seek to lessen this unequaldistribution o f resourcesby financ ing the development o f mechanisms t o pro vide servicesinunderserved areas. Th e proj ect will also finance the re -deployment o f medical personnel to theseunderserved areas.
14

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 21/103
50. An estimated 39 percent o f all resources managed by M O H were spent o n ambulatoryservices provided by basic health centers (centres de sante' de base - CSBs) and hospitals, 17percent on p reventive and pu blic health services,and 7 percent o n inpatient care. In general, thedistribution o f public resourcesin the health sector gives priority to the most costeffectiveinterventions to ensure health improvements as the largest percentage was used for bothpreventive and public health services and ambulatory care. However, there i s room forimprovement, as a fifth o f all resources go to the central administration o fthe ministry and asmany resources, about 0.5 percent o f he ent i re budget o f 2006, went t o the construction o f amedical complex in Antananarivo. SHSDP will further improve the allocative efficiency o fpublic expenditure as i t will finance preventive care, public health activities, andf i r s t referralhospitals fo r activities related to maternal health. M o re specifically,the focus o fSHSDP i s in hemost cost-effective interventions to pre vent and treat theillnesses that represent th e major burdeno f disease in Madagascar by focusing on health interventions that canbe provided by th ehouseholds and communities themselves and for those that canbe provided at primary healthcare facilities. Thisi s reflected in the project's emphasis on consumer awareness campaigns,strengthening o f community participation o n health care,and on improving the qual i ty o fthe
services provided at health centers. By improving coordination and harmonization amongdonors, Madagascar SHSDP will also improve allocative efficiencyby diminishing transactioncosts and thus diminishing administrat ive costs o f M O Hwhen handling different donorsupported projects.
51. The benefits o f the proposed project can also be determined in t e rms o f systems andprocess related benefits, e.g., better planning, financing, organizationand management o f thehealth sector and other key actors, and household-oriented benefits, as exemplifiedby betteraccess and util izati on o f health servicesand improve d health status, especially o f vulnerablegroups living in rura l areas, wom en an d children.
B. Technical
52. The project will rely o n simple, cost-effective andwidely available techniques t o addresspriority health issues. In some problem areas, new strategies will be studied and tested. Theproject components have been prepared o n th e basis o f nternationalas we ll as regional normsand practices, and will be implemented in accordance with acceptable standards. Decisions onciv i l works andequipment necessary to expand and upgrade the health deliv ery systemwill bemade based on an approved H ealth Infrastructure Development Plan(Carte Sanitaire), and o nstandardized architectural plansand l i s t o f equipments, discussed and agreed with Governmentand donors. Investments and recurrent costs estimates for the project have been based onestimates o f prevailing marketunit costs, with appropriate allowance for inflation.A reasonablel eve l o fphysic al contingencies hasbeen ncluded in the cost estimates.
53. The Strengthening o f decentralized h ealth services, na tionwide,will require significantinvestments to strengthen management and plannin g capacities at provi ncia l and districtlevels.Accordingly, the project will support capacity building activities at all levels. Capacities toproperly maintainbuildings and equipment will also be strengthened at provincialand districtlevels and a greater involveme nt o fhe private sector will be sought. Lastly, the projectwill alsostrengthen the capacity o f selective tech nical programs dea lingwith sector pr ior ity problems
15

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 22/103
such as infectious diseases, nutrition, family planning, and emerging diseases, such asHIV/AIDS.
C. Fiduciary
54. Procurement. The third Country Procurement Assessment Review (CPAR) fo rMadagascar was conducted in November 2002, and as a result o f reforms undertaken, the newprocurement code was adopted on July 2004, with simplification o f procedures and compliancewith international standards. To ensure that the new regulations are adequately applied, providesuff icient oversight and control, and improve efficiency through proper delegation o fresponsibilities, new procurement institutions have been established, and the legal texts, such asdecrees fo r implementation and standard bidding documents, were issued. During the preparationo f he proposed project, the World Bank team agreed with the Borrower that IDA Guidelines andStandard Bidding Documents (SBDs) would be widely used. To mitigate risks o f delays for theproposed project, proper prerequisites for the use o fBank SBDs, including evaluation reports fo rNational Competitive Bidding (NCB) procedures were agreed upon with Government during
negotiations. The existing Project Implemental Manual (PIM) will be updated to reflect thearrangements fo r the proposed project.
55. A Procurement Capacity Assessment o f MOH, including training needs andarrangements, was conducted as part o f the project preparation. M O H has proposed that theexisting procurement unit o f he CRESAN 2 will continue to functionas the procurement unit forthe new project and in accordance with the provisions o f the Procurement Code. This unit i sadequately staffed with two procurement officers and an assistant. O n the basis o f theassessment, i t was agreed that the PCU will maintain these staff members and will keeptransactions separate based on source o f financing. Nevertheless, the PIM wi ll need to be revisedto address the needs for the new project. This update will need to be completed by effectiveness.Moreover, the organization o f the procurement filing needs to be reviewed and procurementtraining undertaken fo r PCU staff on the new features o f the Bank’s procedures in accordancewith 2004 Guidelines. As part o f supervision missions and in addition to regular postprocurement reviews, independent procurement and technical audits wi ll be carried out asneeded.
56. Financial management. The conclusion o f the financial management assessment i s thatthe existing PCU for CRESAN 2 and the related operating u n i t s o f the MOH satisfy the Bank’sminimum financial management requirements specified in OP/BP 10.02. However, someimprovements will be needed to further strengthen the financialmanagement system and alloweff icientuse o f report-based disbursement.
57 . To efficiently address the challenges o f the proposed project, a financial managementplan has been developed and agreed upon with MOH to ensure an environment which mitigatesfiduciary risk. This plan includes measures to be taken prior to effectiveness and actions to beimplemented in the medium-term. As a result, transitional financialmanagement arrangementswill need to be established while the sectorhational fiduciary systems are being strengthened.Measures to be taken are the following:
16

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 23/103
Avai labil ity o f a qualified technical assistant acquaintedwith both national f inancialmanagement system and Ban k financ ial management procedures t o strengthenth e financialmanagement capacity o fthe M O Hand specially the Direction Administrative et Financierand supervise the fina ncia l management aspects o fal l programs to beimplemented by M O H ;Extension o f he contracts o f he 17 financ ial management officers recruite dunder C R E S A N2 to : (i) rovid e the regional operatingunits with necessary capacities t o qu ick ly disburse an daccount for projectfunds; (ii) nsure, at the regional and districtlevels, the use o f funds fo rthe purposes intended; and (iii) ssure timely preparation o f periodic financial reportsrequired for proper monitoring o f act ivi ties implementedby regional operatingunits, withrespect to fina nci al and ph ysica l aspects;Elaboration o fa chart o f accounts to satisfythe requirements o f he borrower, IDA and otherdevelopment partners in inancial/accounting/technical informa tion related tothe program;Update and implementation o f the Program Acc ounting Man ual t o ensure consistentapplication o f policies and operating instructions, proper recordkeeping and adequatesafeguarding o fassets. This manual spells out procedures to be ap plied not o nly atthe centralbut also at the regiona l evels;
Customizingand upgradingthe computerized accountingsystem acquired within the contexto f C R E SA N2 in order to: (i) eet user needs; (ii) atisfy the Government, IDA and otherdonor financialhechnical info rma tion requirements; and(iii) nsure timely product ion o fannual finan cial statements and quarte rlyFMRs fo r m onitoring program activities;Creation o f an internal audit departmentwithin M O H to enhance internal controls andaddress areas o f concern identified during program implementation.This department will bestaffed with an adequate number o f auditors, andwill collaborate closelywith the GeneralInspectorate fo r Finance oncei t s fully functional;A Pooled Account will be opened in a commercial bank (BFV: Bank for TradeDevelopment) in the name o f M O H o receive credit/grant proceeds fro mIDA and AFD aswell as other donors who may wish t o p o o lfunds; andThree regional accounts will be opened in a commercial bank to deposit funds f rom thePooled Dep osit accountin order to ensure prompt payment o fcontractors/suppliers operatingin the regions.
58. To mitigate risks raised by the limited capacity o f the Audito r General(Chambre desComptes) the partners and Government agreed that, as an interim measure, an internationalprivate auditingfirm acceptable to donors will carry out the audi t o f he program accounts jo in tl ywith the Auditor General. This auditwill be performed bi-annua lly and conductedin accordancewith International Standards o fAuditing. The auditors will be recruitedwithin three months afterthe effectiveness date. The audit reportwill be submitted to IDA no later than six months afterthe end o f each period. N o significant problems have been encounteredso fa r in terms o f auditcovenants: al l audit reports related to B ank-financed p rojectsin Madagascar have been received
in due time.
59 . T o build and strengthen the financ ial management capacity o fM O H staff at al l levels, acapacity building program i s being developed in the medium-term through the ongoing publicfinancial management reforms supportedby IDA (Governance and Institutional DevelopmentProject) and other development partners. Institutional strengthening activities are alsobeingundertaken under Component 5 o f this project. A techn ical assistant will be also recruitedwithin
17

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 24/103
three months after credit effectiveness to strengthen M O Hin project financial management andsupervise the fina ncia l management aspectso f a ll programs to be implemented by th e Ministry.
D. Social
60. A poverty and social impact analysis carried outin 2005 highlighted the absence o fcitizen involvementin monitoring service qualityin healt h as well as a lack o f empowerment o floca l health committees, wh ichrepresent a key focus o f community level involvementin th ehealth system. More over, Madagascar’s phys ica l characteristics o fhav ing numerous remote anddi ffi cu lt to access areas makesi t difficult torely only o n op-down supervision to monitor quali tyand performance o f the 2,240 CSBs. The poverty and social impact analysis found that poorquality o f serviceswas one o f he tw o key factors limiting use o f public health centers, the otherconstraint being financial.
61. In this context, the quality o f health services couldbe improvedi f here was support forengaging local communitiesin the monitoring o f health quali ty,and i f the accountability and
transparency o f he relationship betweenthe service providers andusers was strengthened at thelocal level. Social accountability mechanisms need to be established in order to providecommunitymembers with simple but effective reportingmechanisms as well as sensitize them toservice norm s and rights and responsibilities o fvario us actors in provision o fhealth care.
62. Experience with the application o f social accountability mechanismsin other countrieshighlights their effectiveness in redu cing absenteeism, i mp rov ing treatment o f clients,andincreasing utilization o fhea lth services. Su ch mechanisms ma y also prov ide greater transparencyand demand for timely allocations from th e communes to pay for medicine dispensers andguards. Empo wering the health committees to apply pressure onthe mayors’ office to allocatethese funds for trainingthem and providing themwith transport allowances to participateinhea lth management committees alsohelp. These represent relatively smallinvestments, since thepotential payoffcan be large, especially given the critical role playedby th e dispenser inprovidingdrugs, an essential element in access and quality o fhealt h care.
63. An ongoing pilo ti s testing and adapting a co mm unit y score card to the heal th sector, a ndi s expected to provid e valuable lessons o n h o w such mechanisms co uldbe adapted and moresystematically integrated intothe health sector mo nitoring .A draft imp lementation manual hasbeen developed, and could be used for eventually scalingup these mechanisms. These pil ots arebeing tested both in areas in wh ich top-down performance and qualityenhancement programsare in place as well as in areas wit ho ut these programs.
64. During the pi lo t stage, the Co mm un ity Scorecard mechanism was selected becausei t was
a more accessible mechanism for a wider variety o f actors, anddid not require sophisticatedstatistical or analyticalskills. The proposed social accountability mechanisms wo ul d directlyt i einto the multiple activities o fthe project, in clud ing development and management o f hum anresources in the health sector, imp rov ing demand and utiliza tion o f health services, andmon itorin g and evaluation.
18
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 25/103
E. Envi ronment
65.purposes, given the risks associated with the handling and disposal o fme dical wastes.
The proposed project has been classified as Category B for environmental screening
F. Safeg uard policies
66. The o nly safeguard triggeredi s the environmenta l assessment, because a Med ic al WasteManagement Plan (MW MP )i s required. The Project does no t trigger any o fthe Banks socialsafeguard’s policies, since land will not be acquired and civil works will be limited torehabilitation o f existing infrastructures. Altho ug hthe project may finance malaria campaignactivities as a lender o f last resort if the Presidential M alaria Initiativ ei s not able to sufficientlyfinance the malaria program, Madagascar has rat ifiedthe Stockholm conventionin 2005, and theGovernment does no t plan to use any DDT in spraying duringthe Bank Project implementationperiod.
67. A M W M P was developed forthe Multi-Sectoral H IV /A ID S Prevention Project (MSPP),and i s under implementation. Sincethat date, M O H has installed 200 sm all-scaleburners to burnmedicalwastes in al l 200 healthcenters rehabilitatedunder CRESA N 2.The construction o ffullincinerators at district level i s underway, and some are already functional. The M W M P alsospecifies medical waste disposal and management actions that are to be carried out in thedifferent, ypes o fhealth facilities.
68. The National Policy on Medical Waste Management was adoptedin September 2005.This policy primarilyrelates to solid waste with a summary description o nthe liquid waste, andcontains the followingelements: (i) lobal and specific objectives as regards management o fmedical waste; (ii) he legal framework and law; (iii) aste characteristics with the prescribedelimination modes; (iv) norms,safety standards and measures to be adopted as well as criticalequipment; and (v) a description o fthe monitoringsystem and an action pla n with impact andresults indicators for a periodo f four years. The Government recent ly modified the plan andpolicy to include more details on the management o f liquid waste from health facilities. Therevised pla n was approved and disclosed on March 23, 2007 in the Infoshop and disclosed in-country overthe period M arch 20-26,2007.
69. M O H has demonstrated clear ownership o fthe problems related to management o fmedical waste, as well as the ability to plan forand prepare these activities. I t has been anintegral player in the development o f this policy as well as information, education andcomm unication activities and training conducted at various levels.
19

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 26/103
Table 3: Safeguard PoliciesSafegua rd Policies Trigger ed by the Project Yes N oEnvironmentalAssessment (O PB P 4.0 1) [XI [INatural Habitats (O P B P 4.04) [I [X IPest Managem ent (OP 4.09) [I [X IPhysical Cu ltural Resources (O PB P 4.1 1) [I [X IInvoluntaryResettlement (OPBP 4.12) [I [X IIndigenous Peoples (O P BP 4.10) [I [X IForests (O PB P 4.36) [ I [X ISafety o fDams (OP BP 4.37) [ I [X IProjects in Disputed Areas (O PB P 7.60)* [I [X IProjects on International Waterways (OP BP 7.50) [ I [XI
G. Policy Exceptions a nd Readiness
70.
policies.
Policy Exception. The proposed project does not require any exceptions from Bank
71. Readiness. The main design parameters and operating systems fo r the project wereestablished under CRESAN 1and 2. The project i s deemed ready for implementation,subject tofulfillment o f the conditions fo r effectiveness.
* By supportin g the propose dproject, the Bank doesnot intend to prejudice thefinal determinationo the parties' claims on thedisputed areas
20

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 27/103
Annex 1: Countr y and Sector o r P rogr am Background
Madagasc ar Sustainable He alt h System Development Project
I. MACROECONOMIC EVELOPMENTS
72. Madagascar has witnessed a remarkable dow ntur n since beco ming independentin 1961,with rea l per capita GDP decliningby over 25 percent during the last fou r decades to U S$2 90 in2005. Caused in part by inward looking, highly protectionist policiesand poor governance,Madagascar’s disappointing economic outcome has resultedin a deterioration o f physicalandhum an capital. T w o libera lization episodesin the late 1980s and 1990s led to growthbut provedshort lived. The reforms o f he late 1990s, aided by preferentialtrade access, resulted in export-oriented, private-sector led growth, averaging over 4 percentduring 1997-2001. This progresswas interrupted by a political crisis over the contested 2002 elections that resultedin aneconomic crisis, with GDP decliningby 13 percent in hat one year alone. However, the po liti calcrisis did bring to po wer a democratic forcewith a reform agenda and renewed hope for a moreprosperous future.
73. Indeed, goo d progress has been achieved since the polit ical and economic crisis o f2002.Prudent macroeconomic management followingth e crisis created an environment conducive t oeconomic rebound, reaping the f ru i t s o f previous liberalization reforms. Despite exogenousshocks such as cyclones and high o il prices, the macro-economic situation stabilizedand theeconomy grew at about 10 percent in 2003 and has since continued to grow at respectable 5percent. Growth has come largely through improved performance in agriculture, especiallyhigher rice production, higher tourism receipts, and continued public investments. Despiteincreases in wo rl d petroleum prices, atight monetary pol icy has resultedin a decline in annualinflation from 27 percentin end-2004 to 10 percent in mid-2006. Similarly, the measuresadopted to ensure exchange rate st abi lity a nd competitiveness, and to secure an adequatel evel o f
international reserves were broad ly successful leading to greater stab ility o f the market-determined exchange rate in 2005. The governmen t has also taken steps to confro nt corru ptionand to improvethe quali ty o fpublic sector governance. In an effort to improve pub lic resourcemanagement and strengthen the system o f delivery o f pub lic services, the government i spreparing a legal framework for decentralization to thel e v e lo fcommunes.
74. High grow th has also resulted in improvements in basic social indicators, albeit fromal o w base. Mo re children arein school today, and net pr im ar y enrolment rates exceed 90 percent.Immunization rates have improvedand the number o f births assisted by skilled medicalpersonnel has increased. Infant and ch ild mortality rateshave declined significantly overthe lastdecade and chronic mal nut ritio n has decreased. Similarly, progress has been made o n reducin gpoverty, wh ich declined to 70 percent fro mi t s peak level o f 80 percent at the t ime o f he 2002crisis. With the implementation o f he roads programin rur al areas, rur al popu latio nwith reliableaccess to transport increased from 45 percent in 2003 to 57 percent in 2005. Access to safedrinking water in ural areas also i mpr ove dduring this period.
75. These positive developments are encouraging, but there i s s t i l l a long way to go givenwhere Madagascar i s today relative to the rest o fthe world. The macroeconomic situationremains fragile, especially as revenue mo bi liza tio n remains weak. Pove rty rates are st il lvery
21

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 28/103
high while social indicators are very low, and Madagascar is not likely to reachthe povertyalleviationand health-related MDGs. The country also continues to face f i sca l problems, withsignificantrevenue shortfallsin customs and tax collections leadin gto a decline in tax revenues.Although th e economy has been o n a rebound in the last tw o years, the capacity o ftheGovernment to raise revenue remains severely constrained. Moreover, external aid hasbeendwindling in recent years. As a result, o vera ll governmentexpenditure i s fa l l ingin real t e rms andpublic spending on social programs is declining bothin real terms and as a percent o f theGovernment budget.
11. H E A LT H ECTOR
Hea lth Status and Outcomes
76. The last decade witnessed marked health improveme ntsin Madagascar, especiallyamong children. According tothe Demographic and Health Survey (DHS), infant and ch il dmortality f e l l by 43 percent and 41 percent, respectively, between 1997 and 2004. Although
some issues have been raised regarding the reliability o fhese marked drops in mortality, otherdeterminants o f chil d survival- such as morbidity and coverage o f important healthinterventions - have also improved. For instance, the prevalence o f diarrhea in childrendecreased about 63 percent and the proport ion o f anemic childrenf e l l about 3 1 percent between1997 and 2004. At the same time, vaccination, vitaminA supplementation, and exclusivebreastfeeding increased.
Table I : Neonatal, Infant, Child, and Ma tern al Mor tality, Madag ascar, 1997-2004
1997 40.4 96.3 159.2 488200312004 31.6 57.8 93.9 469Source: DHS 1997, 2003/2004.Note: maternal mortality is expressedper 100,000 l ive births among children bornin the four
years before the survey.
Neonatal Infant Under-5 Maternal
77. Mate rnal mor talit y has remained stable at about 470per 100,000 livebirths since 1997,jeopardizingthe like lih oo d that Madagascarwill reach this MDG by 2015. While antenatal carehas increased to 80 percent and the presence o f skilled staff at birth has increased f rom 47percent to 54 percent, the full benefit o f skilled attendance at birth ca n only be realized i f thereferral system, comprising a l l o fthe essential elements o f access to the whole spectrum o fobstetric care including emergency services, i s fully functional. Some progress has beenachieved in recent years in addressing this challenge through such means as establishment o fbetter communication networksbetween primary and first l eve l referral facilitiesusing solarbased radios, strengthening o f b lo od banks at district level, provision o f ambulances andobstetric care equipment and the rehabilitation andre-equipping o f some district and referralfacilities. Moreover, deathsdue to abortion contribute significantly tothe maternal mortality rate(40 percent in rura l areas, and approximately 52 percentin Antananarivo alone), suggesting thatimproved access to family planning advice and services would considerably improve maternalhealth in the medium-term. Overall, significantly moreintensified efforts are needed for moresystematic improvementsin referral services and emergency obstetric care, particularlyin ruralareas.
22

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 29/103
78. Com mun icable diseases, espe cially malaria, diarrhea, and respi ratory track infections,often in association with malnutrition, arethe ma in causes o f mortal i ty andmorbidity in thecountry, mainly among childrenunder five. The M O H statistical yearbook 2004 shows that 24percent o foutpatient consultations aredue to respiratory track infections, fol low edby 18 percentdue to fever (suspected malaria), a nd 8 percen t due to diarrheal illnesses. A mo ng childrenunder
five, respiratory track infections, suspected malaria,and diarrheas represented 33 percent, 22percent, and 14 percent o fprimary health care consultations in 2004. Mo st vaccine preventablediseases seem to be under control in Madagascar - ndicative o fhigh vaccina tion coverage- andin 2004 less than 1 percent o f al l children’s consultations atthe prim ary he alth care leve l weredue to measles.
79. Although the prevalence o f H IV /A ID Sin the country remains low, i t has rapidlyincreased amon g high risk groups. With a prevalence o fabout 1 percent amon g pregnant wome n(overall, there were an estimated 180,000 persons were living with HIV in 2005) HIV/AIDS inthe country s t i l l does not represent the heavy burden i t does in other Sub-Saharan Africancountries. While knowledge o fHIV/AIDS satisfactorily progressed between 1997 and 2003/04
fr om 6 9 percent to 79 percent for women, and to 88 percent for men, be havior change has laggedbehind among high-risk groups in ho t spot areas as well as among the general population. Sincethe establishment o f the Comite‘ Nationalde Lutte contve le SIDA (CNLS) to implementtheHIV/AIDS program, a sector-wide approachhas been put in place with the ma inpartners (WorldBank, GlobalFund, AfDB, USAID, GTZ, UNICEF, UNAIDS, etc.) to implement numerousactiviti es (information, education, mass med ia comm unica tion, cinemo bilesin villages,distributiono f STI treatment kits, etc.). The C NL S i s rightly reorienting i t s strategy to: (i)concentrate activities o n beha vioral changeand in the most high risk zones; (ii) trengthen massand peer comm unication on STI, HIV testing, and reduction o f stigma; (iii) evelop routinetesting, an d volunt ary counseling; and(iv) strengthen public private partnerships as a way toaddress the weakness o f pub lic health services.
80. Bilha rziosis , lym pha tic filariases, tuberculosis, lepro syand ma lari a also represent a largehealth burden to the population. Bilharziosis affects about two and a halfmillion people inMadagascar, mostly in the western an d centralparts o f he country. Lymphatic filariases affectsal l areas o f the country but especially the poo r ru ral coastal areas. In some o f these areas, th eprevalence i s thought to be higher than 50 percent. T uberculosis alsorepresents an importanthealth burden in the country with an estimated 20,000 cases per year with a detection rate o fonly62 percent. Fina lly,despite marked reductions in the incidence o f eprosy, Madagascar remainsone o f he few countriesin the w or ld that has not eradicated this disease.By end 2005 i t had thehighest registered prevalence in the wo rl d (2.5 per 10,000). While Madagascar has made someheadway o n the con trol o f malaria, tuberculosisand leprosy, these efforts have lost some gro undmain ly due to delays in access to resources, and the deterioration o fthe existing surveillance
system. Madagascar has secured sizable resources for the contro l o f malaria, tuberculosis a ndHI V/ AI DS treatment mainly throughthe GlobalFund grant facility. Recently however, delaysinimple menta tion have occurreddue len gth y processes in defining appropriate strategies (e.g., f o rmalaria) or delays in access to available funds. Nevertheless, social marke ting o fhighlysubsidized permanently impregnate dbed nets have increased moth er and chil d preventionin hecoastal regions. D iagnosis and treatment o f tuberculosis imp rove dwith the expansion o f thedire ctly observed therapysystem and increased drug availability nationwide.
23

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 30/103
i n t ~ ~ e ~ ~ ~ o ~ so improve child sttwivtrl hasstfeeding. t h e use o f oral
have markedly i i ic rp ~ ~ ~ ~ ~ c ~ ~rctd
cnts in childsurvival.
83. Thcre are large s ~ ~ c i o - e ~ o i ~ ~ ~ ~ i i ~i f f e r e n ~ e sn rho coverago o f ~ a ~ yf the high impactheafth i I ~ ~ e ~ ~ e ~ ~ i o ~ s ~s ~ ~ c i a ~ ~ ~hose needed to imp ro v e ch i ldsurvival. For ~ ~ s ~ a ~ ~ e *he percentof childretiM y ~ ~ r ~ ~ ~ i ~ ~ ds 2.5 times her among the richrst 20 perccrit of the p ~ p ~ l ~ ~than among the poorest 20 percent. In the case o f v i t a m i n A ~ ~ p p l e r n e ~ t ~ ~ ~ ~ ~ ,he socio-
economic ~ i ~ ~ e r e n c ~ ~re mu ch lower but s t i l lpersist. These d i f ~ e r ~ ~ ~ e ~lso reflect Fhe failure orth e health system to react1 the l?#ortlst s ~ ~ ~ c ~ i ~ sf" he p ~ ~ u l ~ ~ ~ ~ ~ .
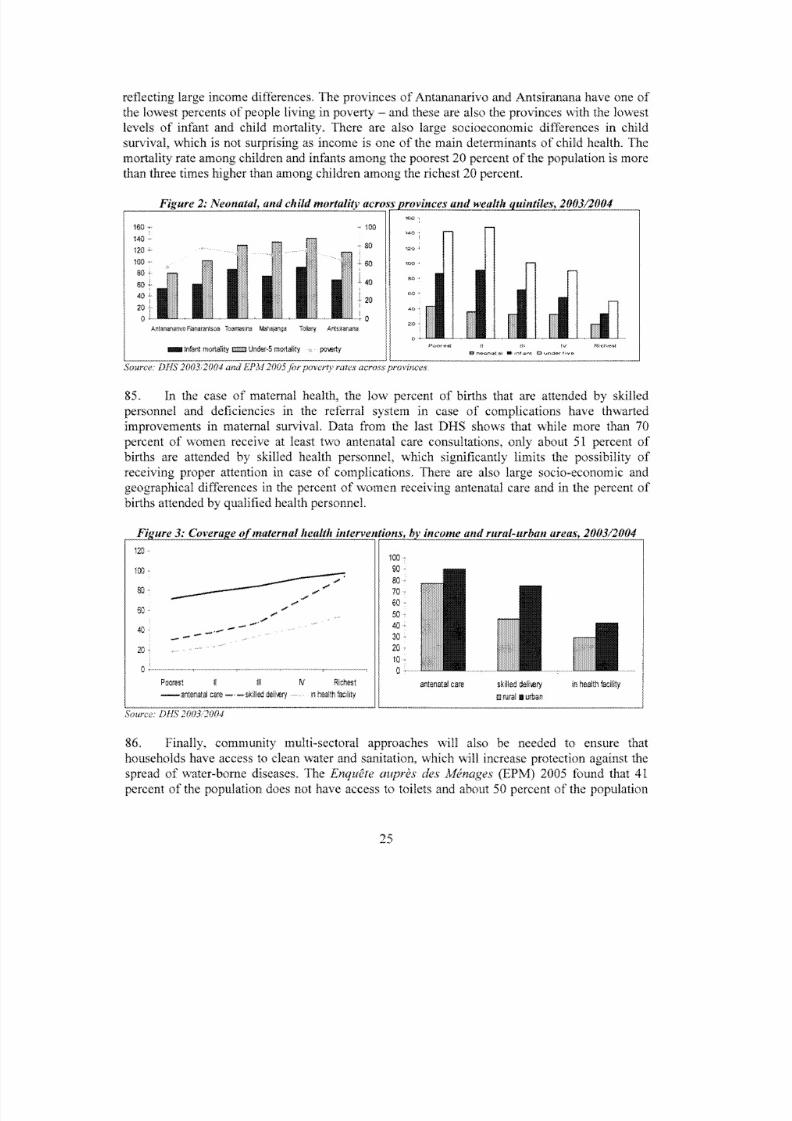
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 31/103
25

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 32/103
does no t have access to a safe source o f drinking water. Imp rovin gthis situationdoes not dependonly on MOH ,but these interventions will have a high impact on health.
Organization o f the H ea lth System
87. The health delive rysystem in the country follows a four-level pyramidalsystem. Thebasic he alth centers (centre de sante' de base - CSB I nd CSB 11) are the f i r s t poin t o fcontact inthe system. In 2004, there were 1,106 CSB I nd 1,842 CSB I1 spread across the entire countryand catering to approximately 10,000 people each. In addition, there are 85 district-levelhospitals in district headquarters (centre hospitalier de district - C H D I) ased in districtheadquarters but offering similar services to those offered in a CSB 11. The second step in th epyramid i s made up o f 55 C H D I1 hospitals (2004), also based in district headquarters butoffering emergency surgery and comprehensive obstetrical care. At the third l ev e l there are 4regional hospitals (centre hospitalier regional- CHR) in the whole country, offering secondreferral services. At the fourth level, there are six university hospitals (centre hospitalieruniversitaire - CHU) offeringcomprehensive nation al refe rral services.
88. The public sector - and especially the primary health care facilities (CSB I nd 11) -
offers the bulk o f health care services in the country, especially in rural areas. In urb an areas,more than 30 percent o f f i r s t contacts with the health system o ccur in a public primary healthcare facility, whilein rura l areas more than 70 percent o fa l l f i r s t contacts occur at a publicfacili ty. O nhe other hand, the privat e sector accounts for about30 percent o fa l l f i r s t contacts inurba n areas and about 14 percent in rural areas. Overall, morethan 40 percent o f consultationstake place at private provide rs amongthe richest 20 percent o f he population.The privat e sector,ma inl y concentratedin urba n areas, also represents an important share o fservice delivery. Abo utone out o f everyfive primary health care faci l i tyand two ou t o fevery five referra l hospitals areprivately owned. The majori ty o fthese facil i t ies are concentrated in Antananarivo and othermajor cities.The priva te sector has an even larger presence in the retail sale o fpharmaceuticals.There are 203 pharmacies, located mai nl yin Antananarivo, and 1,625 drug retai lers distributedthroughout the country.
Table 3: Consultation at public and private facilities, by income quintiles (EPM 2005)CH* CSB1 CSB 2 Private Clinic Private doctor Other Total
UrbanMo st poor 20.1 18.6 38.8 3.1 3.2 16.2 100
2emeQu intile 14.9 11.3 31.6 5.9 24.3 11.3 1003emeQu intile 20.4 14.7 25.4 16.3 13.2 8.8 100
4emeQuintile 11.2 10.5 29.4 8.1 31.9 7 100Mo st rich 23.3 4.9 20.6 7.5 32.7 7 100
Tot al 19.0 9.5 26.2 8.3 26.0 8.6 100Rural
Mo st poor 5.1 25.5 58.0 0.9 6.2 4.1 1002emeQuin tile 4.9 19.0 53.9 2.1 7.0 13 1003emeQu intile 3.5 12.9 56.9 3.0 12.6 11.3 1004emeQuin tile 1.2 11.6 66.9 2.1 11.4 6.9 100
Mo st rich 5.7 10.0 50.8 3.6 20.4 7.4 100
Total 4.0 15.1 57.3 2.5 12.2 8.6 100
26

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 33/103
Financing o f the H eal th Sector
89. Foreign aid reprcscnts the largest source o f finance for the ~ e a ~ ~ hystem, fol lowed bypublic and private funds. Thc 2001 NIL4 e x e r c i s e e s~ i ~ a t e dhat donor funds represented 37percent o fa l l filnances ~ ~ o ~ ~ n ~o the hestth sector. ~ u ~ l i cunds represent about 32 percen~ frhetotal, and include resources that the ~~~~~~s~~o f Economy, Finance, and Budget allocates forhealth related ~ x p e n ~ ~ t u r e ~ ,ther public lunds such as direct loans to the treasury~and p ~ ~ l ~ cemployee funds. 'I'he m i j o r i t yo f itte public resources come from ~ e ~ ~ e r a laxation a l ~ ~ ~ ~ u ~share comes from loans from external agencies. ~ ~ i c ~ u d ~ n ~he Wo rld Rank. Finally,th e privatesector r e p r e s e ~ ~ s1 percent o f rh e rota1~ i n ~ ~ t c ~ i ~ ~y source. ~ ~ ~ u ~ e ~ o ~ ~ s~ i e ~ ~ s ~ ~ ~ ~ e ~rc the mainsourcc o f private an^^^^^ r e ~ r e ~ e ~ t t i n ~0 percent o f a l l r e s ~ u r c e s l o ~ i ~ ~o th e sector. Thema.jority o f h o ~ ~ e l t ~ ~ ~~ p e ~ ~ ~ t ~ ~ r es ~ ~ ~ ~ - ~ ~ f ~ p ~ ~ ~ ~ t~ ~ ~ n d ~ ~ u r ~n both p ~ i ~ ~ ~ cd privatef a c ~ ~ i t ~ e ss ~ r e - p a ~ ~ e ~ r~ e c ~ i a n ~ s m snly ci)ver a small ~ r o p o ~ i o ~ if the fonnaf sector workers.~ ~ ~ ~ ~ ~ ~ n i ~e alth ~ n ~ u r a ~ t c c :chemes arc: only j u s t s t a r ~ ~ l n ~n he coulntry, and cover a very smallpercent o f he p o p u ~ a ~ ~ o n .
~ ~ a ~ t ~ector ~ h a ~ ~ e n ~ ~ ~nd Issues
n. These are discussed in
27

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 34/103
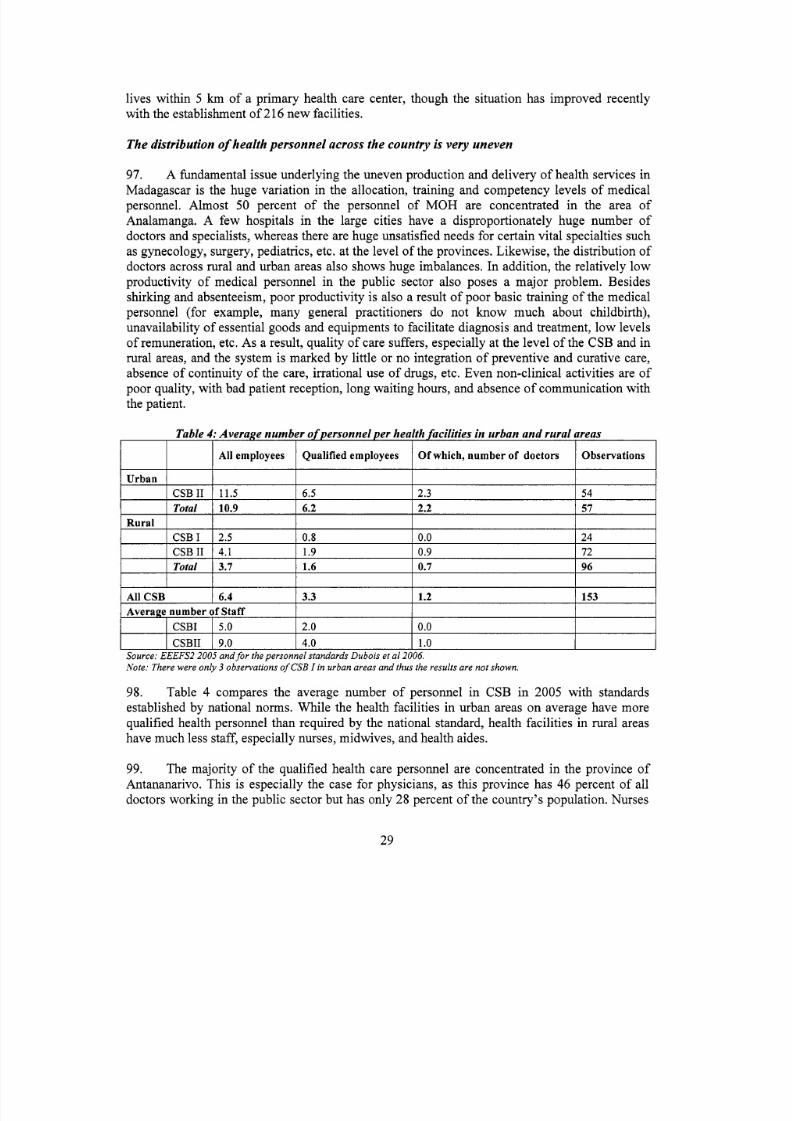
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 35/103

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 36/103
muc h better dist
r the 2001 crisis, thc Gavlevel and started to d i s r r ~ b u ~ e ~ ~ a r ~ ~ ~ ~ u t i c a ~ sree o f charge. During this time, a heatth facilitysufz.ey recorded w~ d~ sp re adnig stock-outs in the CSBs. Only I 5 percent nf the public prima ryh e ~ ~ t hare centers did not suffer shortage in the s ~ ~ p p l yf a group o f csscntiaf drugs.About 30percent of f ~ c ~ l ~ ~ i ~ sad s ~ ~ o ~ a ~ e sf c h l o r ~ ~ ~ ~ ~ n e ,o ~ r i ~ i o ~ ~ z o l ~ ,i ~ b e n d ~ ~ ~ ~ ~ ,nd a ~ c ~ ~ ? h ~ ~about 36 percent had shortages o f ~ a r a c e t a ~ o ~ :nd more than hal fwere out o f a c ~ ~ ~ l s a ~ i c ~acid. The m e m ~ ~ i ~ a ~ i o nf the s ~ o ~ ~ - ~ ? u taried from 70 days for a ~ c t ~ l s a l ~ c ~ l ~ cci d to 32 daysfor ~ i i e ~ e n d a ~ o l e .fter the ~ ~ - i n ~ r ~ ~ d u ~ ~ i o nf fees and the ~ A ~ ~ ~ ~'und, the s ~ t ~ a t ~ o nhas ~ ~ i p r o ~ ~ e ~l t ~ ~ ~ u g ~rug s h o ~ a ~ e sre s t i l l a ~ r ~ ~ ~ l e ~ ~ ~ ,ver 20 percent o f health facilities,c ~ ~ c c ~ a ~ l ~n rural areas. have ~ ~ o r ~ a ~ e ~f"nrst r e ~ ~ ~ d ~ ~ t ~ ~ ~ nalts, serum glucose, folic acid. and~ i d o c ~ ~ ~ ~ c .or some of ttcse drugs the ~ i ~ ~ d ~ a ~~ r ~ ~ t ~ ~ ~ nf ~ ~ o ~ ~ - ~ ~ u ~as three months.
30

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 37/103
Table 5: Percent of CSB with drug shortages, by type of drugs and rural-urban areas, 2005
IRural
1Urban
1Total
1Average number of daysSB only Median number o f days
Number o Observations. I 96 I 57 I 153 ISource: EEEFS I I2005
102. There are other indications o f o w quali ty o fservices at public facilities.In 2003, only59percent o f pub lic basic healt h centers had accessto clean water, 53 percent ha d electri city,andon ly 16 percent h ad transportation.Further, only 21 percent o f public faci l i ties collected al l theinforma tion requiredby the I M C Ipro toc ol (age, weig ht, hea lth card, temperature,and breathingfrequency). Similarly, in only 8 public faci li t ies out o f58 children were examined for thestandard four signs o f h ea lt h risk (vomit, convulsions, anemia, and capacity todrink).Additionally, on ly 61 percent o f anemia or severe malnutrition cases were correctly identifiedinpublic facilities.The situation has changed onl y ma rgin allyin 2005, and 61 percent o fCSB n o w
have access to a water source and 54 percent to electricity. However,in 2005 more than 90percent o f acilities collected inform atio n o n age, weight, he alth care and temperature o fchildren.
103. The health system performs poorly atthe hospital l evel also, limiting referral to urbanareas and only when i t i s no t further com poun dedby financial barriers. Th e qu ality o f servicedelivery in hospitals i s affected by the lack o f proper me dical specialists, equipment,maintenance, proper drugs and consumables. However, the creation o f the health regions hassignificantly mod ified the set-up o f district health facilitiesand reference hospitals. With supportfrom development partners, hospitall e v e l services are being reviewed and should lead to areorganization o fhe referralsystem and a transformation o f he role and mandates o fdistrict andregional hospitals for more effectiveand efficien t servicedelivery. The program o f crea tion o fessential services particularly in surgery and emergency medicine and the re-equipment andrehabili tation o fhealth facilities i s progressing well and will continue.
31

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 38/103
Wa te r (pump and tap)r S R
Electricity Means o f transport Fosse A ordures Obs..
Source: EEEFS II, 2005.
PublicRrivate
PublicPrivate - non religious
Private - religious
Budget execution i s weak
61.4 53.6 51.0 55.6 15371.9 96.9 45.3 56.3 64
89.7 94.8 43.1 34.5 58
104. Management o f the health system at the local level i s improving, althoughbudgetmanagement capacity remains a major challenge. The planning, programming and monitoring
functions o f regional and district health management teams havebeen strengthened. All regionsand d istricts have adjusted their budgeting process to the new budget/program format, a nd somehave begun to introduce performance-based planning using management tools and technicalsupport fr om various partners.The performance o fthe dis tric t management teams has started toimprove as a result o f echnical support and staff recruitment.All but a few o f he districts aren ow able to formulate their three year plans and develop annual work programs along clearnorms and criteria. However, implementation o f those annual plansi s s t i l l weak due to poorimplementation capacity, insufficient resource flows to the regions and districts and l o w capacityfor procurement o fthe large quantities o f comm odities and equipment needed toexpand healthservices. Furthermore support from regional and communal administrative authoritiesi s s t i l lweak. This situation i s in part due to substantial limitations at centrallevel, where budgetmanagement functions remain weak and require increased efforts to strengthen theadministrative and managerial capacityo f the health system. The e xe cu tio n o f M O Hbudget in2005 and 2006 was low, and there i s need for contin uing efforts at developin g capacity at central,regional and district levels and at devoting increased attention for more systemic support andmonitoring o fbudget distributionand implementation.
32

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 39/103
Heal th Sector R eform Program
105. M O H s continuing toimplement initiatives to improve accessand ut i liza tion o f hea l thservices and imp rov e hea lth outcomes.A new sector p ol ic y was adoptedin June 2005, in whichemphasis was p laced o n the need to re-orient health resource allocations to underserved areas
and improve publicexpenditure management. P revention and treatment o f malariaand otherma jo r commu nicab le diseases were also am ong thekey priorities. Moreover, the p ol icy sought toachieve closer integ ration and coordin ation o f healt h sector intervention swith other activitiesthat im pact h eal th status such as water and sanitation, nutrition, transport, andru ral development,and aimed to expand the coverage o f risk-coping strategies such as mu tual health insuranceschemes and soli dar ity mechanisms.
106. T o estimate the sector's inves tmen tneeds over the next ten years, a process o f analyticwork was initiated using the Marginal Budgeting for Bottlenecks programming tool. Theanalysis has highlighted the importance o f adequate investment in the development o fhumanresources as well as infrastructure, especially referral facilities. The analysisi s based on a
dynamic path characterized by various growth scenarios including linear increasesin servicedelivery and/or frontloading for infrastructure andequipment supply. Estimates f rom themode ling exercise indicate that significant resources wou ldbe necessary to enable Madagascarto meet the health-related MDGs by the target date o f2015. The planned expansion o f essentialhealth services, i nclu ding enhanced clinica l refe rral capabilities fo r neo-natal and obstetric care,would require additional resources over the short-to-medium term tose t the country on adynamic path toward realizingthe health-related MDGs. The first base scenario calls for anincrease o f U S 3 . 8 0 per capita and aims at progressing steadily towardsthe chil d m ortali ty,malnutrition, malaria andHIV MDG targets through increased use o f w el lknown high impacthealth interventions such as imm unization,family planning, use o f impregnatedbed-nets andsocial market ing o f health and sanitation products inclu din g oral re-h ydratio n therapy.The otherscenarios call for a tripling to quadrupling o fspending on health to support a significantexpansion o f clinical services whic hwill be necessary to make progress on the maternalmortal i tyMDGs.
107. Madagascar's effo rts t o pro vide services tothe poor focus on increasing theavailabilityo f qual ityservices and ensuring the financial accessibility o fhese services. He alt h is a key goalo f Madagascar's pove rty red uction strategy, and health poli cy issues feature p rom inen tlyin thecountry development plans, including the Madagascar Ac ti on Pla n (MAP), 2007-2011. TheNational Health Sector Strategy and Development Plan(Plan de De'veloppement du SecteurSante', or PDSS), coveringthe period 2007-2011 eeks to l i s t and define the various interventionsnecessary fo r the realizat ion o f heMAP objectives in a logica l framework o f priorities, activitiesand results.
108. The primary focus o f the reforms in the he alth sector i s to strengthen the health systemand increase i t s capacity to provide the necessary production, financing, delivery andmanagement support for delivery o f services necessary to meet the eventual o bjectives o freducing child and maternal mortality, controlling illnessesdue to malaria, sexuallytransmitteddiseases, and HIV-AIDS. Accordingly, ongoing efforts arebeing targeted to strengthen deliveryo f hea lth services, develop and manage human resources in the health sector, introduceinnovations in health financing, inclu ding resource mob iliza tion an d resource allocation, and
33

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 40/103

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 41/103
Annex 2: Major Related Projects Financed by the Bank and/or other Agencies
Madagascar Sustainable Health System Development Project
World Bank Proiects
109. Second Health Sector Support Project (US$40 million credit; US$22 millionsupplemental credit). The project was approved in November 1999, and a supplemental credit(US$18 Million) preparedin 2005. The development objective o f he projecti s to contribute tothe improvement o fhe health status o f he p opulatio n through more accessible andbetter quali tyhea lth services. Th e proje ct has three sp ecific objectives:(i) mprove qual ity o fhealth and accesst o primary health care services with a focus o n rur al areas; (ii) upport prior ity health programswith emphasis on endemic infectious diseases, reproductive health(including family planning,sexually transmitted diseases and HIV/AIDS) and nutrition; and (iii) trengthen sectormanagement and administrative capacitywithin M O Hand at provincial a nd districtlevels. Theproject i s rated satisfactory o n bo thIP and DO ratings.
110. Multisectoral STI/HIV/AIDS Project - MSPP I US$20 million credit). This projectwas approved in November 2001. Its development objectivei s to support the Government o fMadagascar’s efforts to promote a multi-secto ral response tothe H I V / A I D Scris is and containthe spread o f HIV/AID S oni t s territory. T o doso, the project builds capacity a nd scales up thenational response to HIV/AIDSand STIs, a key risk factor and contributor to the spread o fHIV/AIDS. The project has financed, inter alia, sector strategies and p il o t projects, inc lud ingcomm unica tion campaigns, the implementat ion o fthe local response, and M&E activities. I t i srated satisfactory o n bot hIP and DO ratings.
111. Second Multisectoral STI/HIV/AIDS Project - MSPP II(US$30 million credit). Theproject was approved in July 2005, and made effective in M ay 2006. The closing date i s
Decembe r 31,2009. The development objectives o fMSPP I1 are the same as those o f he MSPP,i.e., to support the Government o fMadagascar’s efforts to promo te a multi-secto ral response tothe HIV/AIDS crisis and to co ntain the spread o fHIV/AIDS o n t s territory. T o doso, the proje ctwill intensify and will build capacity to carry out th e national response to HIV/AIDS andsexually transmitted infections (STIs), a key risk factor for and contributor to the spread o fHIV/AIDS. In addition, MSPPI1 will seek to improve the quali ty o fi f e o f persons living withHIV/AIDS hrough increased access to quality med ical care a nd to n on-medical support services.Given the current epidemiological situation, the projectwill put an even stronger focus than theorig inal project o n at-risk groupsin high prevalence areas, while moderately expandingservicesto other affected groups (e.g., orphans and other vulnerable children).The project consists o f hefollowing components and sub-components: (i) armonization, dono r coordination, a ndstrategies; (ii) upport f or hea lth sector response; (iii) TI/HIV/AIDS preve ntion an d care; (iv)monitoring and evaluation; and(v) project management and capacity building. The project i srated satisfactory o n bot hIP and DO ratings.
112. Community Development Fund (US$178 million). The project was approved in April2001 and made effective in October 2001. The closing date i s June 30, 2008. The project hasbenefited fro m tw o supplemental credits. Th e objectives o fhe project ar e to improve the use o fand satisfaction with project-supported socia l and economic services amongstparticipating rura l
35

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 42/103
and urban communities. The project has six components: (i) ransfers o f funds to communityassociations; (ii) apacity building activities; (iii) ransfers o f funds to communes; (iv) projectadministrationand supervision; (v) social safety net activities; and (vi) cyclone emergency anddisaster r e l i e factivities. Th e proje ct is rated satisfactory.
113. Second Community Nutrition Project (US$47.6 million). The projec t was approved inM a y 1998, and received two supplemental creditso f US$10 mi l l io n eachin December 2003 a ndNove mber 2006. The closing date i s December 2008. The development objectives o fhe Projectare to improve the nutritiona l status o f childrenunder the age o f hree, pregnant and lactatingwomen, and school-aged children . Th e Project also aims to ensure long -term sustainability o fnutrition outcomesby improving the quali ty and quanti ty o f food intakeby children at home.The Project i s implemented by SEECALINE, an executing agency operating since 1993 whi chhas demonstrated capacity in effectively supporting poor communities andin monitoringnutritio nal status throug h contracting loca l NG Os whose capacity hasbeen built by the project.
114. Governance and Institutional Development Project (US$30 million). The
Governance and Institutio nal Development (PG DI) proje ct was approvedin November 2003 andbecame effective in Ma rch 2004. The clos ing date is June 30, 2009. An addit ional f inancing o fUS$5 m i l l i o ni s under preparation. The development objective o fthe project i s to assist theGovernment o f Madagascar in implementingthe Poverty Reduction Strategy Paper (PRSP), byrationalizing and modernizing budget, and publicexpenditure management; improvingaccountability and transparency o f Government operations; and,by strengthening the capacity o fpub lic institutions,in light o f comp lex change processes. The tw o m ai n components addressthefol lowing:i) mp rov ing transparency, and economic governancewill require a comprehensivere form o f the public finance system; and ii) nstitutional developmentand capacity buildingactivitiesin selected government institu tions .
36

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 43/103
Proiects of O th er Develop ment Agencies
Project name
0 Budget Support (PAW)
0 SANTEII
Donors Sector Issue ImplementationStatus
General budget Ongoing
Provision o f Ongoingsupport
essential drugs,health acilities
EuropeanUnion
0 SANTE I11 HIV/AIDS andtransmissible diseases
0 Mother and child health0 Family planning and
reproductive health0 Nutrition0 STI/HIV/AIDS0 Malar iagrant round 3 and 4
(CRESAN and PSI)0 HN/A IDS round 4
(SE/CNLS)0 Tuberculosis round 4
(SE/CNLS)0 Mother and child health
Child health
AfricanDevelopmentBank(AfDB)
HIV/AIDSandtuberculosis
0 Hospital
0
rehabilitation
USAID
0 HIV/AIDS0 Reproductive health0 Malaria0 Insti tutionalcapacity
building0 Immunization0 HIV/AIDS
0 Reproductive health0 FSP
0 Immunization0 District,regional support0 HIV/AIDS
GLOBALFUND
Technical Ongoingassistance
0 Technical Ongoing
OngoingTechnical Ongoing
assistance
assistance,training,HIV/AIDS,hospitalsrehabilitation,district support
OngoingMahajunga Ongoing
0 TechnicalSUPPOrt,public-privatepartnership
JICA
UNICEF
WHO
UNDP
UNFPAFrenchCooperation
GAVIGTZ
Ongoing
Ongoing
Ongoing
Ongoing
37
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 44/103
Annex 3: Result s Frame wor k and Mon i to r ing
Madagascar Sustainable He alth System Development Project
115. The National HealthSector Strategy and Development Plan (Plan DCveloppement duSecteur SantC, or PDSS) lists and defines th e various interventions necessary forth e realization o fthe MAP objectives in a logical f iamework o fpriorities, activitiesand results. The five-year PDSSlays dow n a Results Framework wh ich captures thekey elements o f the resul ts chain and l i n k sinputs, resources, outputs and outcomes. Developed through extensive consultationwithdevelopment partners and others stakeholders, the Results Framework provides program-levelbases fo r managers to gauge progress towa rd the achievement o f results and t o adjust relevantprograms and activities accordingly.In addition, i t provides an important opportunity for M O Hto workwith i t s development partners an d stakeholders t obuild consensus and own ership a roundshared objectives and approaches to meeting those objectives. M O Hsees th e Results Frameworkas a “living” management tool, t obe used as the foundation fo r critical programmatic events andprocesses, including strategic planning(by outlining program objectivesand contributions o f
operations and their outputs to achieving these objectives), comm unicat ion(by setting outpriorities, clarifying expectationsand accountabilities, and identifying common areas andsynergies across operations), mo nit or ing an d evalu ation(by measuring progress and makingadjustments as needed) and learning (by determining what works andwhat does not andcomp aring across sim ilar operations).
116. The fundamental premise o fthe Results Framework i s that health status and outcomesdepend o n a host o f factors that inclu de pub lic h ealth interventions, economic environment,social environment, sociop olitical environment, and life-cycle-relatedissues. I t recognizes thatactivities and actions within the health system, while necessary, would be insufficient bythemselves t o bring about the desired improvements in health, includingmeeting the health-
related MDGs, since measures to achieve these improvements w ou ld require interventions acrossma ny other sectors, such as water an d sanitation, infrastructure, educ ation and environment,wh ich also have a direct or indirect effect on health andwell-being. Reco gnizing that measuringand tracking the myriad interventions across allthese sectors would be a huge and di ff i cu l texercise for any one implementing agency, the Results Framework focuses on monitoringresources, processes and outputs dire ctly re lated to actions a nd activiti esimplemented by M O H ,and tracking a set o f broad indicators o f health outcomeand status that would subsume theeffects o f nterventions o f other sectors andministries. The dashboard o f outcome indicators-effective ly the end-result o fal l interventionsby a ll sectors as well as households and individualsthemselves that have some bearing on health and well-being - will be used for broad sectormonito ring and attentionby high-level policymakers and development partners. Tab le 1 presentsthe full M A P P D S SResults Framework.
38

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 45/103
cm
3
0
.-
6
0
wa
m
B
111
311-::3
s
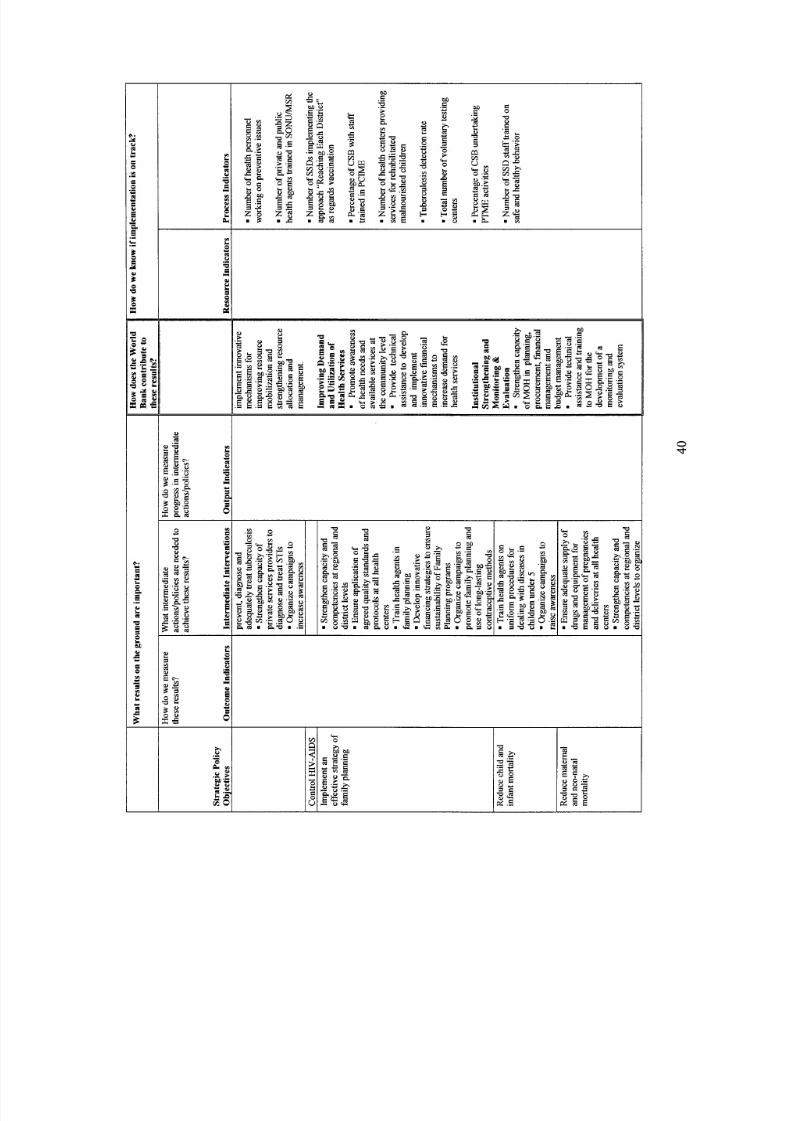
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 46/103
0d
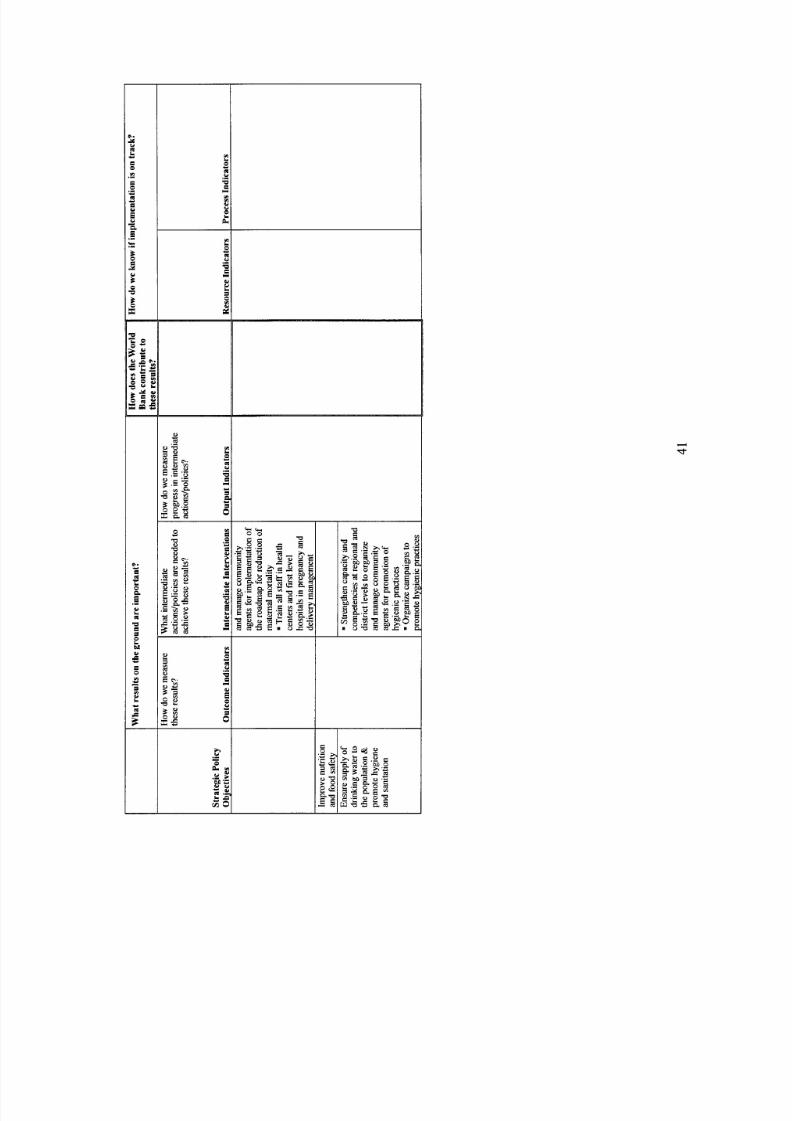
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 47/103
3
d

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 48/103
117. The engagement o f the Wo rld Bank anduse o f IDA resources will be used to leveragewider support for the MAP and to provide the necessary technical expertise and support forrealizat ion o fMAP’S objectives. Besides pro vid ing finan cial resources to upgradehealth centersat district and regional levels, the Bank will contribute significantly toward institutionalstrengthening and capacity building, bo th for measurement o f esul ts as well as for strengthening
management in the health system. Indeed, building capacity to define, measure, and useinformation on health outcomesand health system performance would be a practicalandvaluable o utcome t o achieve, especiallygiven the limited amount o f DA financing o fhe project(total o fU S $ l O million). Moreover, such capacitybuilding would be very beneficial to th eGovernment o f Madagascar and the development partners in terms o f measuring progress andidentifying areas o f need based o n data. Ulti ma tely , stronger capacityin measuringresults wo u l dprovide the country with the abil i ty toevaluate performance and use performance data for well-informed policy making. Table2 presents a se t o f quantitative and qualitative indicatorswill beused to track the results o f Bank interventions. The output indicators are a subset o f theindicators developedby M O H o tra ckprogress in he PDSS.
ExternalEvaluationExternalEvaluationM O H
Table 2: Bank’s Results Indicators
Annu al ’Full harmonization
Annual Full harmonization
End o f Project Center developed
Process Indica torsNumber of jo in t work plans prepared
M O H
Number of oin t annual review withdevelopment partners undertakenCenter for Health Po licy and Planningi sdeveloped in M O HNation al Health Information Systemi sdeveloped and function ingin M O HData on illness, utilization and treatmentarecollected regularly at district lev el andreported to a central coordina ting agencyUtiliza tion and treatment datai s used toinform policy makingin the health sector
Regional and district levelsare more able tomanage health centers and coordinateprov ision o f health servicesIncreased resources transferred to regions anddistricts and used to impro ve healthcenterperformanceInnova tive provider payment mechanisms tocontract and redeploy nurses and midwiv esinremote areas developed
End o f Project
Harmonization andCoordinationHarmonization andCoordinationCapacity building onmeasurement o f esultsCapacity building onmeasurement o f esultsAb ility to measureresults
Management capacitybuilding
Management capacitybuilding
Management capacitybuilding
Improvementsin HealthFinancing
I IxternalEvaluation
42

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 49/103
Innovative financing methods developed toincrease the use of health services by the poor,through such mechanisms as equity funds andsocial insuranceNumber o f national/district campaignsorganized to increase awareness so as tomaximize utilization and effectivenessNumber o f community health provisionscorecards prepared, discussed anddisseminated
Stimulation of Demand
Social Accountability
Improvements n Health MO H End o fProjectFinancing I / I
MOH Annual
MOH Annual
Parameter m easuredby this indicator
Contribution of he stateto th e health sectorAbility o f MOH omanage their allocations
Total spending on health
118. Tables 3 to 5 present selected indicators from the general Results Framework fo r thePDSS that will be monitored by the Bank during the implementation o f Madagascar SHSDP totrack and evaluate progress under the PDSS.
Source o f info and Frequency o f Baseline
National Budget; AnnualLaw o f Finances 2005National Budget; Quarterly 65% inLaw o f Finances; 2005MO HNational Health Annual $11.9 inAccounts 2003
data measurement8.74% in
Indicators
fo r health
~~
Number o f regions that havecomputerized management of HumanResourcesPercentage of CSBs upgraded o be incompliance with national normsNumber o fCHRRs upgraded to be incompliance with national normsNumber o fCHDs upgraded to be incompliance with national normsNumber o f health personnel trained onpreventive issuesNumber o Comm unity agents on
Number o f private and public healthsector agents trained in emergencyobstetric careNumber of health districtsinstitutionalizing routine EPINumber of malnutrition treatmenthealth centers upgraded to be incompliance with national norms
I (public A d private) per capita
Management o f HumanResources
Infrastructure Standards
Equipment Standards
Essential surgery services
Management of qualityassurance
maternal care and neonatals
SONUet MSR comptencies
Supply o fvaccinationservicesNutrit ion services
Table 4: PD SS Process Indicators
11.67%
100%
316.00
Indicators Parameter measured bythis indicator 1
ource o f theinformationand data
MO H
MO H
MO H
MO H
MO H
MO H
MO H
MO H
MO H
MOH/ONN
Irequency of Baseline 2011measurement I 1 I
I I
Annual 130% in1 80%2006
Annual 16 22
11,238
I
43

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 50/103
Table 4: PD SS Process Indicators, cont 'd
Indicators
Popula tion Coverage
Number o f CSBs that have at leastone qualified physician availableand workin gfull timeAvailability of racer drugs atthelevel of CSBsProportionill seeking outpatientcare at CSBsAverage occupancy rate o fhospital bedsPercentage of children bornin
health facilitiesProportion o f pregnant womensleeping under ITNProportion women usingcontraceptivesFu ll vaccine coverage for ch ildrenunder 1 yearTuberc ulosis cure ratePercentage o f CSB wit h ava ilablewater supply
119.that will also be monitoredby th e Bank during the implementa t ion o fMadagascar SHSDP.
Table 6 presents selected indicators from the general Results Framework forthe M A P
120. There are ma ny issues with the existing institutionalarrangements o fcollection, reportingand use o f data . The Hea lth Information Systemin Madagascar collects data on 74 indicatorsrelated to service pro visi on (outpatient care, fa mi ly plan ning program, m atern al health, ch il dhealth, STU AID S, co mm un icab le diseases (in clu din g tuberculosis, malaria, bilharziose, etc.),dentistry, evo lution o f pathologies, logistic management data fo r fa mil y planning, nutr itiona lsurveillance o f children (g rowth monitoring), surveillance o f pregnant wom en (antenatal care,delivery), and cost recovery from drug sales. The smallest data collection unit i s the CSB, and
44

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 51/103

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 52/103
121. T o ensure effective planning, monitoringand evaluation o f ts various programs, M O Hhas decided to establish regionall e v e lunits responsible for planning, monitoringand evaluation.The 22 regional health offices have o nlyrecently been established and have a key role to playsupporting program implementation vi a the 111SSDs, and the approximately 2500 CSBs andloca l hospitals. Terms o f eference for these units and fori t s key staff were approvedin February
2007. These uni ts , which report to the regional health directors, represent the central l evelDirectionde Suivi-Evaluation and Audit.As such, the principal function o f hesenew u n i t s willbe to ensure that reliable and time ly data concerning healt h indicatorsi s provided to the regionalhealth directorsand to the central leve lSSS so that this data can be used for planning, monitoringand ove rall management purposes.
122. Currently, although an extensive and often overlapping data collection systemexistswithin the Madagascar health sector, the system exhibits serious problems concerning dataquality and timeliness andi t s poten tial as a management to ol i s not being realized. Given thissituation, the World Bank will support M O H to strengthen these regional level unitsso theybecome operational within a reasonable time peri od (6-12 months). Fo llo wi ng that fora period
o f 12-24 months, the Bank will support M O H o provide targeted support toth e district healthservices and front-line community levelhealth service providers within their jurisdictions toensure that improvements are made in the collection, transmission, analysis anduse o f h ea lt hsector data so that verifiable progress i s made towards achieving national development andhealth sector objectives. In a l l these efforts, th e emphasis will be o n ensuring the accuracy(quality) andt imel iness o f data. I t wil l also require ensuring that al l those w ho require this datawill have easy and reliab le access t o it . A Center for H ealth Policy and Developmenti s proposedto be established under MOH, which would take data fromS S S and carry out the necessaryanalysis to i nfo rm pol icy formulation and decisionmaking.
123. An impor tant aspect o f he support to be provided tothe regional u n i t s will be ensuring aclear and effective definition o f heir roles and responsibilitiesvis a vis SSS and SSD. Significantprogress has been made under CR ES AN2 in developing the district level capacity to analyzedata coming fro mthe CSBs an d hospitals in order to identify progr am goals that were no tbeingmet in order to ensure that these facilities and -their staff receive the attention and supportrequired to improvetheir performance and results. I t i s expected that a si mila r management forresults approach can be instilled in the new region al health offices and at the centrallevel . Forthis reason, i t will be important to ensure an appropriate articulation and complementarity o froles and responsibilities betweenth e different administrativelevels.
124. Related to improvin gthe efficiency o fthe Madagascar health information system int e rms o f the quality and t imeliness o f data, while ensuring this data i s more widely used formanagement purposes, there i s also the need t o simplify and rationalize the different data
collectionrequirements. Currently, for example, s taff wo rkin gin a CSB is required each monthto complete at least ten different data collection forms.This arises in part because the various“vertical” programs such as vaccinations, fa m il y planning, malaria, and nut ritio n, do no t receivethe data they require f rom SSS for repor ting purposes due tothe delays experienced in preparingthe consolidated national data.As a result they seek this data directly at the district level . Thisduplication o f data collection and reportingi s excessive and means a significant po rtion o f CSBstaff time i s devoted t o filling forms rather than to treating patients or w orkin g in prevention
46

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 53/103
programs. M O H hasestablished a working group(comite' ad hoc) to look intothis and prepare aharmonized data collectionsystem. A f inal element that merits support concerns huma n resourcemanagement. Currently there is no data base or computerized system to monitor and helpmanage MOH's approximately15,000 staff. Althougha Department o f Human Resources wascreated three years ago, i t i s s t i l l being organized and i s not yet able to play i t s role effectively.As a result, there are serious problems in all areas including assignments, promotions andrationale allocation o fstaff.
47
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 54/103
Annex 4: Detailed Pro ject Description
Madagas car Sustainable Hea lth System Development Pro ject
Component 1: Strengthening Delivery o f Health Services (IDA financing: US$5.3 millionequivalent)
125. The ob ject ive o fthis component i s t o strengthen th e delivery o f heal th services at thepr imary andf i rs t referral levels in districts and to significantly improv e the availabil i ty o fquali tyhealth services, especially in remote areas. Fo llow ing the country’s ongoing efforts todecentralize resources, functions and responsibilities to districtlevels, this component willsupport the strengthening o f he capacity o fthe districts to better organize, manage and deliverhealth goods and services to all, especially those living in rural and remote areas, but withcontinuing technical support and stewardship from the center. Community actionin themanagement an d financ ing o f peripheral health servicesi s seen as the most cri t ical element forimp rovin g service quali ty andensuring long-te rm sustainability.This will provide the basis onw h i c h prime mother and ch ild health care interventions, such as imm unizat ion, pre vention and
co n tro l o fcom mo n diseases and pre- an d post-n atal care, will be made accessible to the major i tyo f he populat ion, and on wh ich HIV/A IDS-re lated actionswill be accelerated.
126. The fol lo wing act ivit ies are includedunder this component:a) Support in improving functionality o existing primary and fi rst referral health centers at the
district and community level, to del iver the basic package o f services, inclu ding thep ro v is io n o fthe necessary drugs, equipments and testing facilities, especially f or infan tand c hi ld health, materna l health, and prio rity infectiou s diseases,and p ro v is io n o f b asicwater a nd sanitation facilities at hea lth centers that d o no t haveexisting water supply on -site. The projectwill:. Rehabilitate, equip and upgrade prim ary and f i r s t referra l health care facilitiesso at to
bring them up to compliance with national norms. The rehabil i tat ionwill includep ro v is io n o fbasic water and sanitation facilities.Prov ide a package o f drugs and consumables to selected prim ary a ndfirst referralhealth care facilities, with priority accorded to health facilities that are properlystaffed a nd record high utiliza tion rates.Contribute to the fight against pr iori ty infectiou s diseases, inclu dingbut not restr ictedto : (i) n-house insec ticide campaigns to prevent ma laria outbreaks (financier o f astresort i f support through other initiatives such as GlobalFund and the PresidentialMa laria Ini t iat ive is not available ontime); (ii) mm uniz atio n against rabies; (iii) estpre ven tion and surveillance activities; an d(iv) f i lariosis el imination.Support im provemen t o f mother and ch ild heal th and increasefamily planningthrough prov is ion o f safedelivery kits for normal and complicatedbirths, maternalkits, an d purchase o fcontraceptives.. Support implementat ion o f innovative strategies t omeet the health needs o fpopulations in em ote areas.
.
.
.
b) Provision o technical assistance to MOH in order to identify gaps in the del ivery o fhealth services and suggest actionable recommendations to strengthen supply. Inparticular, the projectwill:
48

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 55/103

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 56/103
b) Provision of training and coaching to health personnel to strengthen capacity to strengthencompetencies at regional and district levels in order to assume a leadership role inmobilizinghealth providers as well as organizin g and coord inating co mm unit y agents toimplement the roadmap for reduction o f maternal mortality, promotehygienic behavior,and promote the integrated use o f amil y pla nning services. Th e projectwill:
. Support training o f al l health personnel, inclu din g doctors (public and private),nurses, midwives and other health agents, in the pro vis ion o f services necessary toprovide quality services, including capacityto diagnose and treat infectiousdiseases,children and new-bo rn babies, and management o fpregnancies an d deliveries.Support the development o f new training strategies, both for basic and continuingeducation such as the creation o f new a nd or shorter curriculddiploma,implementationo f pi lo t experienceswith private paramed ical schools t o increasethenumber o f paramedics available throughout the country,strengthening o f basictraining in coherence with the burde n o f diseases and public health objectives, andcreative wa ys to gain access to medic al trainin g and expertise.
Component 3: Innovations in Health Financing Management (IDA financing: US$0.6million equivalent)
131. Accord ing to NHA 2003, total health expenditure in Madagascar is estimated to beapproximatelyUS$l1.9 per person, equivalent to about 3.5 percent o f GDP. Ext ern al assistancerepresents over 37 percent o f otal spendingin he hea lth sector. P ubli cfunds constitute the nextlargest source (32 percent), followedby out-of-pocket payments (31 percent). Currently donorsupport i s provide d main ly throu gh projects, th ough the sector has also benefited fr om generalbudget support that the Government has received fro m PR SC financedby the Wo r l d Bank andthe European Uni on. Com mu nity insurance systems areat an early stage o f development, andonl y cover avery sma ll percentage o f he population.
132. The pub lic sector i s the principal financing agent, managing 55 percent o f totalfunds,with the bulk o f he operationalbudget o f he Ministry devoted t o salaries. Budget execution hasbeen weak, averaging abou t 77 percent annually, and hasbeen below the average o f the otherMinis t r iesduring most o f he last decade.
133. In terms o f distrib ution , there are large inequa lities across regions,with richer regionsreceiving relatively more resources. This regressive distribu tion o f resources constitutes anobstacle to ensuring access and utiliz atio n o fqualityhealth care by all, a key goal o f he Nat ionalHealth Policy and the MAP. Moreover, insufficient resources fl o w to the CSBs, pa rtiallyexplainingthe low quality o f he servicesrendered at this level. There are no clear criteria fordistribu tion o f health resources across regions thattake int o account the size o f the population
and their needs, the l eve l o fpoverty in the region, andthe number o f acil it ies.
134. Resource mobilization and allocation remain the cornerstones o f the health sectorstrategy in Madagascar, as the country strives to increase the resources allocated to the healthsector. Inno vative ways o f mobilizi ng resources, inclu ding social and co mmun ity healthinsurance, are being considered under the strategy. In addition, public-private partnerships arealso under being exploredas potential means o fgenerating new resources.
50
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 57/103
135. The follo wing activities are includedunder this component:Provision o technical assistance and support for the development and selectiveimplementation o innovative mechanisms for improving resource mobilization andstrengthening resource allocation across sectors in order to meet the priori ty objectives o fthe government. The projectwill finance te chnica l assistance to develop the fol lowing tools:
. nnovative resource mobilization mechanisms, including equityfunds, socialinsurance, community insurance, etc.. Mechanisms for better management o f available pub lic and privatefunds, includingpoo ling o f budgetary and non-budgetary sources o f financing, pri ori ty spendingandpro visio n fo r catastrophic care.The project will finan ce tech nical assistance (togetherwith the Bank’s Governance and Instit utiona l Deve lopm ent Project)so as to increasethe budget execution rate, and foster accountability and efficiencyin financialresource allocations and a reserve fund fo r catastrophicand epidemic care.Innovative provider payment mechanisms, including contracting, especially fo rnurses and midwives for deployment in rur al and remote areas. Some o f thesemechanisms will be tested through implementation .
.Component 4: Improving Demand and Ut i l iza t ion o f He alt h Services (IDA financing:US$1.05 m illion equivalent)
136. Utiliz ation o f health servicesin Madagascar is very low. Onl y 10 percent o fthepopu lation reports anillness, and o f hose, only 40 percent seek care. There are huge variationsin service use across regions, with significantly lower rates o futi l izat ionin the remoter areas o fthe country. Utiliza tion o fhea lth services i s especially l o w amongthe poor, implying nequity inut i liza tion o fcare. This l o w evel o futili zatio n also resultsin an unde rutilized health system an did le resources.
137. The follo wing activities are includedunder this component:a) Promotion o awareness of health needs and a vaila ble services at the community levelin
order to support increased utiliz atio n rate o fhea lth services. The projectwill:. Support strengthening o f comm unity education to increase awareness o fhealth needsand available services so as to increase utilizationand effectiveness through bothmass me dia campaigns and community-based a ctivities .Support the organization o fnational/regional/district campaigns to prom ote improv edand integrated management o fchildren illnesses, family planning,use o f ong- te rmcontraceptives, increased utiliz atio n o f maternaland neonatal services, hygienicpractices, etc. The projectwill support selective innov ative p il ot experiences aime d atincreasingthe utilization rate o fhe alth services.
.
b) Provision o technical assistance for the development and selective implementation oinnovative fzn anc ial mechanismsto increase demand fo r hea lth services. The proje ctwill:. Support development o f asystem o f conditional cash transfersin order to provide
financial incentives toseek care, especially fo r the po or and vulnerable sections o fsociety. A pi lo twill be launched to increase co mplia ncewith tuberculosis treatment.
51

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 58/103
Component 5: Institutional Strengthening (IDA financing: USfi2.15 million equivalent)
138. A critical objective o fthis component i s to provide support t o the strengthening o fcountry systems in the health sector and specificallywithin th e Ministry o f Health, includingprocurement capacity, financial management systems, budget execution, program oversight and
planning and use o f data for decision making (evidence basedplanning). Moreover, closepartnerships need to be developed between the Ministry o f Heal th and other relevantministries,in particular Water and Education. Finally,the oversight and mo nitoring o f private sectorpartners in the health sector i s fundamental to havin g a comprehensive picture o f the healthsystem in Madagascar.
139. Another objective o fthis component i s to support the establishment o f an effec tiveMonitoring and Evaluation(M&E) system. M&E systems provide information on inputs,structures, outputs and outcomes, and are central to im pro vin g management o fresults andstrengthening performance. The goal o f the proposed M&E plan i s to link the systemstrengthening activities supportedby the project to the MAP objectives and create an integrated
and coherent fr amew ork t o mo nito r a nd evaluate progress across mu ltip le dimensions.This wil lprovide the necessary in form atio nto decision-makers to assess achievement o fproject objectivesand make the necessary adjustments fr om time t o t ime in response to evo lving con ditions eitherwithin or external tothe project.
140. International experience o fM&E systems points to the importance o f engaging al lstakeholders in the M&E development process. The project’s M&E plan will present a specialchallenge and opportunity to assist in the coordination and implementat ion o f mult isectoralactivitie s aswell as monitoring the impact o fhea lth ac tivities across sectors.
141. The follo wing activities are includedunder this component:a) Strengthening of the capacity of MOH in plan ning and programming, procurement,
financial management and budget management, and strengthening supervisorycapacity o f districts, and support t othe preparation and implementation o f Annu alW or k Plans. The projectwill:. Provide support to th e decentralization process at th e regional and district health
operational distric tl eve l through strengthening o f supervisory capacityled by thedistrict level to ensure smooth and regular functioning o fhealth facilities,including CSBs and f i r s t referral he alth facilities, especially for emergencysurgeries, and support the move towards more integration o fhealt h activities.. Provide support to the bottom-up planning through subsidizing theimplementat ion o fthe district annual work plan (continuation o f CRE SAN 2support t o avo id disruption o f financialflows at the peripheral level). The
Government commits however to start increasingi t s allocation to the peripherallevel, and to improve i t s in te rna l procedures to be able to manage the districtfinanc ial allocationswith the same flexibility asthe IDA projects by the e nd o fend o f the project.. Provide support for the establishment o f a Center fo r Hea lth Polic y andDevelopment in order to strengthen the capacity o f the Ministry in the areas o fplanning, data analysis, p oli cy fo rmu latio n and program oversight.
52
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 59/103
b) Provision o technical assistance and training to MOH for the development andoperationalization of a monitoring and evaluation system and strengthening capacityto collectand analyze health informa tionand data. The projectwill:
Provide support to the development and operationalizationo f an M&E system,
including at the regional and district levels,including capacity building andtechnical assistance for implementing entities in M&E through education andtrainin g at central, region al and district levels.Provide support to the development o f a Na tional H ealth Inform ation System(NHIS) to im prove routine data collection.Provide support to strengthening o f analytical capacity to facilitate analysis o fnational, regiona land community-level data collected through a varietyo f sourcesat different time intervals andusing multiple data collectio n methodologies.Contribute t othe f inancing o f heDHS.Undertake annual financial auditsand one technical audit during the projectimplementation period.
Support operating costs o f he PCU.
53

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 60/103
Annex 5: Project Costs
Madagascar Sustainable Health System Development Project
Local Foreign TotalUS$ million US$ million US$ million
roject Cost By Component and/or Activity
Component 1 Strengthening De liveryo fHealth 4.3 1 o 5.3ServicesComponent 2: Development and Managemento fHuman ResourcesComponent3: Innovations in He alth FinancingManagementComponent 4: Im pro ving Demand andUtilizationo fHealthServicesComponent5: Institutional Strengthening
Tota l Baseline CostPhysical ContingenciesPrice Con tingencies
Total Project CostsInterest during constructionFront-endFee
0.6 0.3 0.9
0.3 0.3 0.6
0.55 0.5 1.05
1.55 0.6 2.15
7.3 2.7 10.0
7.3 2.7 10.0
Total Financing Required
54

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 61/103
Annex 6: Implementation Arrangements
Madagascar Sustainable Health System Development Project
I. INSTITUTIONAL ARRANGEMENTS
142. The implementat ion o f the National Health Programi s overseen by M O H th ro ug hi t srelevant directorates a nd services. De cision s are madeby a management tea m comprised o f alldiv isio n chiefs and representativesfrom health districts. This team will be responsible f or clos elymon itorin g projec t activities (including the fo llo w- up o f performance indicators, sector issuesand hea lth status/epidemic trends), don or coordination, and for making concreterecommendations o fways to improve overall project implementation.
143. Responsibility for Madagascar SHSDP coordinationwill rest with the ProjectCoordinationUnit (PCU), made up essentially o f staff from the projectunit o f the current IDAfinanced health project.This Unit has also been selected by the Global Fund to manage theMalaria 4th and 5th round funds. I t has performed i t s duties satisfactorily and acquiredexperience in managing IDA-funded activities, coordinating donors,NGOs, var ious M O Hservices and district health authorities. Other donors haveexpressed interest in using t h is PC Ufor the execution o f heir activities, andthe P C U will be staffed accordingly.
144. Given the project's wide array o f act ivi t ies in differen t sectors, the Proje ct Coord inationUnit will collaborate with the fol lowingMOH Directorates: (a) Hea lth Dis tric t Deve lopme nt(Direction de developpement des districts sanitaires); (b) Infectious diseases directorate(Direction de la lutte contreles maladies transmissibles); (c) Preventive medicine (whichincludes Nu tri tio n and Fa mily planning services);(d) Planning and research, (e) Health careestablishments (Direction des etablissementsde soins), and (f) Pharmacy and laboratory fortheproject component o n institu tional strengthening.
145. The head o f he P C U will repo rt to the Secretary Generaland th e Minister o f Health, andwill participate in the M O Hmanagement team together with the other centra l directors, an d thesenior staff o f he hea lth districts. The project staffwill have an internal controller t o oversee a lladm inistra tive and finan cial transactions; ahighly qualified accountant with at least oneassistant; tw o procurement specialists; a procu reme nt assistant; a n architect/engineerin charge ofthe ci vi l works; and at least oneassistant. Implementat ion o f project act ivi t ieswill be theresponsibili ty o fthe above-listed M O H Directorates whowill collaborate with the decentralizedhea lth districts. The project implementation manualwill be revised to further define the roles andresponsibilities o f al l concernedpartners.
11. PARTNERSHIP ARRANGEMENTS
146. A large number o f donors are active in the health sector in Madagascar. Donorcollaboration o n thedesign and implementation o f he health strategyin Madagascar has beenexcellent, andthe scope o f partnerships i s expected to increase even more under the sector wideapproach - both because o f the more forma l approach to donor coordinationunder SHSD P aswe ll as because the health sector strategy as outlined in the PDSS i s comprehensive and includesal l areas o f the health system, in ter alia including populationand fa mi ly planning, disease
55

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 62/103
control, management o fpreventive and acute health care services, strengthening o f the healthsystem, and promotion o fhygiene. Three formalmechanisms o f coordinationwill be used
(1) Health Summits
147. M O Hwill organize two summits a year, one in Mar ch and one in September, and willinvite officials fromMinis t r i eso f Finance, Water and Sanitation, Education, etc., developmentpartners, civil society organizations activein the he alth sector, and other stakeholders. The f i r s tHealth Summit would review the previous year’s performance and resul t in a set o f conclusionsand recommendations fo r M O H hat are endorsedby the Summit’s participants and will fo rm thebasis o f the Ministry’s actions during th e rest o f he year, in clud ing adjustmentsin the Annua lWork Program for the remaining part o f the year. The second Health Summit wo uld reviewprogress over the last six months and providethe basis fo r adjustments an d course correction fo rthe next year. Participants wo uld re viewth e Annual Work Prog ram for consistency with M A Pand PDSS and with findings o f the annual sector review carried out in the f i r s t Summit. Thiswould resul t in a final Annual Work Program for the coming year that is agreedwith
participating development partners, incorporatestheir respective contributions, reflects theircollective recommendationson priority areas for action, and formsthe basis for the fo l lowingSummit’s monitoring o f performance.This collective approach to sector monitoring andcoordinationi s expected to improve efficiency, accountability and prioritization o fdonor supportto the hea lth sector. T he first such Summit will take place in September 2007.
(2) Memoranda o f Understanding
148. A Memorandum o f Support will be signed by agencies pooling their funds forMadagascar SHSDP, in this case the Wo r l d B a n k and AFD. This Memorandum will specifyissues o f special relevance to the pooled funds: namely, institutionalarrangements, fiduciaryarrangements, assessment and monitoring provisions, disbursement arrangements, information-sharing and con flict resolut ion expectations,and arrangements fo r addin g n e w partners duringimplementation. A broader Memoran dum o f Support will be signed by the President o fMadagascar, Ministers o fHea lth and Finance, a ndrepresentatives from a l l development partners,includingthe Wo rld Bank, UN ICEF,UNFPA, WHO, USAID, AfDB, EU, JICA, etc.
(3) Joint Supervision Arrangements
149. Participating development partners will arrange regular jo in t supervision missions andwork closely together o n team composition, plann ingand implementationwith counterparts tominimize administrative efforts fo rthe government. This will include coordination o fthe pol i cydialogue in l i n e with specific areas o f expertise o f individual agencies to al lo w for efficient
allocation o f resources and us e o f government capacities. Regular supervision missions areenvisaged twice every year, and in addition to the fiduciary requirements o f part ic ipa t ingdevelopment agencies, will support the bi-annual Health Summits in their review o f theimplementation o fthe PDSS and SHSDP. T o the extent possible, development partnerswill alsocoordinate the us e o f pa ra ll elfunds available fo r imple menta tion support measures and shareevaluationresults and backgr ound repor ts as applicable.
56

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 63/103
Annex 7: Financial Management and Disbursement Arrangements
Madagascar Sustainable Health System Development Project
Introduction
150. Madagascar SHSDP represents the next stage in support to the hea lth sectorby the B a n kand other development partners. The ma in objective is to contribute tothe strengthening o f hehealth system, inclu ding financing, delive ryand management, so as to imp rove th e access andutiliz atio n o f health services, especiallyin rura l and remote areas, a nd scale-up the p rod uctio nand delivery o f hea lth programswith an emphasis o n endemic infectio us diseases, reproductivehealth and nutrition. To support this strategy, IDA financing i s l i ke ly to be pooled withcontributions fro mAFD and supported through parallel financingby other development partners.To strengthen donor collaboration and ensure harmonization o f borrower and donor fiduciarysystem, a Memorandum o fUnderstandingwill be signed by the governmentand the cooperatingpartners poo lin gtheir funds for this project.
151. The Madagascar SHSDP has five components to be implemented by M O H a n d r el at edoperating uni t s located at the regional and district levels. A prelimin ary financial managementassessment carrie d o ut at the concept stage determined that the program will be implementedin ahigh-risk environment. This i s derived from the fact that Government’s financia l managementsystems are generally weak and capacity i s low. The Ministry o f H e al th i s no exception. Inaddition, financial management capacity at the regionaland district levels is weak. T o addressthis high fiduciaryrisk and efficientlymeet the challenges o f Madagascar SHSDP, transitio nalinstitutional arrangement was agreed with M O H specifying that the f inancial managementaspects o f this program will be entrusted t o the financial management unit o f the ProjectCoordinationUnit (PCU) o fthe ongoing Second Health Sector Support Project (CR ES AN2)which has extensive experience in managing Bank Funds. This unit will keep the existing
experienced and qualified fiduciary staff from C RE SA N 2, includingthree accountants, and willbe in charge o f overal l coordination o fthe prog ram as well as the fiduciary aspects, includingbudgeting, accounting, f ina nci al reporting, disbursement operations and procurement.The unit i sexpected to be supplemented with the redeployment o f a M O H accountant. Theunit wil l besupervised by the Administrative and Financial Director, w hoin turned will be supported by atechnical assistant for the durati on o f he project.
152. The financial management arrangements o f M O H (through CR ES AN2) and relatedoperating u n i t s were assessed during th e pre-appraisal mission.The objective o fthis assessmentwas to determine whether these implementing entities have capacity to handle pooled donorfunds and have also in place acceptable financial management arrangements, whichwill ensure:i) he funds are used only forthe intended purposes in an efficient and economical way;ii) hepreparation o faccurate, relia ble and timely periodic financial reports that w ou ld allo w the Bank,other donors and the Government to plan and implementthe program, monitor compliancewithagreed procedures, and assess progress towards its objectives; and iii) he entities’ assets andrecords are safeguarded. Given the decentralized nature o f the program andthe number o foperating u n i t s involved, the coordination and repo rting mechanisms betweenthese entities andthe PC U has been also loo ked at to ensure that the arrangements in place will allow for smoothimplementation o fprogram’s activities aswell as to ensure that c red it proceeds areused only fo r
57

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 64/103
the purposes for which the credit was granted, with due regard to economy, efficiency,and thesustainable achievement o f he program’s development objectives. The assessment also includesa determination o fhe prog ram’s readiness for report-based disbursement.
IDAAFDTotal
153. The financial management assessment was carried out jointly with the AFD in
accordance with the World Bank Financial Management Practices Manualissued by th eFinancial Management B oard o n November 3,2005. With regard to operatingu n i t s responsiblefo r the implementat ion o fproje ct activities atthe region al and district levels,the assessment wasundertaken for a representative sample, by using a set o f financ ial criteria, asthese entitiesgenerally use the same system and procedures, and have the same l e v e l o f capacity. Theconclusions o f this assessment were discussed with M O H representatives, i.e. the Director o fFinance within M O Hand the national Coordinator o f he ongoing CR ES AN2.
$ US$10 million$ US$18 million$ U S 2 8 million
Summary Project Description
154. The primary focus o fMadagascar SHSDP i s t o strengthen the health system and increase
i t s capacity to provid ethe necessary prod uction , financing, delivery and management support fo rdelivery o f services necessary to meet the eventual objectives o f reducing chi ld and maternalmortality, controllingillnesses due to malaria, sexually transmitted diseases, andHIV-AIDS.Activities undertaken are expected toresult in significant improvemen ts across a range o fdemand-side, supply-side and institutio nal aspects o f the health system, especially in theproduction and delivery o f quality servicesin rur al and remote areas, in bot h public and privatesectors.
155. The likely contribution o f each donori s as fol lo ws (subject to change):
Country issues
156. The Wo rldBank’s CFANCPAR, comple tedin 2003, and some diagnostic work s carriedout over the last three years by the Ban k and other donors, identified a range o f weaknesses andissues hampering th e performance o f Madagascar’sbudget and expenditure management system.T o address these issues, the Government developed in 2004, 2005 and 2006, in conjunctionwitha l lkey development partners, a pri ori ty action pla n fo r publ ic finance re form.
157. Wh ile overall implementation progress o fthe reform programi s encouraging, significanteffort s are needed in the following areas:i) mprovement o f hebudget execution rate in pr io r i tysectors; ii) trengthening o fthe capacity o fthe l i ne ministries in public financial management,especially in the implementation o fthe new program budget structure; iii) trengthening o f cashmanagement; iv) production o fthe treasury accounts within the legal timeframe; v) increase inthe number o f skilled and experienced auditors at the “Chambre des comptes” commensuratewith the com plex ity and increasednumber o f missions to be undertaken; and vi) reinforcement
58

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 65/103
o f contro l over State-owned companies an d nation al pub lic institutions.To mitigate r i sks inpublic expenditure management, the World Bank, throughthe Governance and InstitutionalDevelopm ent Program, and anumber o fdonors continue to support Government’s pub lic financereform s reflectedin ts annual priority actionplan.
158. Regarding the accounting profession, some positiv e developments h ave been noted ove rthe last three years. However, a number o f oca l accountingf i r m s continue to operate be lo w theinternational standards. T o i mpr ove the capacityand the competitiveness o f ocal auditingf irms,the following measures have been taken while audit ing Bank /IDA financed projects:i)mandatory partnerships o f local auditors with international accounting f irms; ii) ffectivepart icipation o fthe international accountingfirm in audit fieldwork;and iii) ubmission o f auditreport joint l ysigned by the local and international auditf irms. An accounting and auditingReview on Standards and Codes w ou ld be certainlyhelpful to identify clearly bot hissues andactions t o be taken to strengthen the capa city o fhe accounting professionin Madagascar.
159. The use o f country systems s t i l l remains risky for Madagascar due to some fiduciary
weaknesses that require much more time to solve. As a result and after exchanges o fviews withthe borrower (Ministry o f F inance and M O H ) i t was agreed, in the context o f SHSDP t ousepartially the country system and to establish transitional financial managementsystemarrangements while the sectorhational fiduciarysystems are being strengthened.
Strengths, Weaknesses and Action Plan
160.0
0
The project financ ial management isstrengthened by the fo ll ow in g salient features:The orga nizat iona l structurewithin M O H K R E S A N2 defines the l ines o f esponsibili t iesandauthority thatexist and seems appropriate for planning, directin g and control ling operations.C R E SAN2 has strong experience in managing W orld Bankfunds. The accountinghudgetingsystem i s adequate as well as the intern al con trol system.I t has also a quali fied a nd trainedaccounting staff very knowledg eablewith Bank procedures.Existence o fan internal auditorwithin C R E S A N2 that couldbe integrated into the InternalAudit Department tobe created within M O H .
0
16 1.follow ing table which also providesre levan t measures to address them:
The ma in deficiencies notedin the finan cial management system are summarized in th e
Significant weaknesses
The Directorate of FinancialAffairs (within MOH) which i ssupposed to supervise the PCUaccounting staff i s not familiarwith the Bank procedures infinancial management anddisbursement.
Actions
Ensure CRESAN 2 accounting staff retainedin the PCU structure.
Strengthening the financialmanagementcapacity of the M OH by hiring, under termsand conditions acceptable to IDA, aTechnical Assistant acquainted with bothnational financial management system andBank FM procedures.
Datedue by06101 07
No t laterthan three
months aftereffectiveness
Responsible
MOWDFB
59

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 66/103
Significant weaknesses
Lack o fqualified s taff attheregional and district levels
Absence o fa Chart o f accountsreflecting program componentsand activities outline din heProject Concept NoteIProjectAppraisal Document.
Absence o f an appropriateaccounting manual o f
procedures describingtheaccounting system, the projectChart o f accounts, po licies andprocedures o be applied, andmodels o f financial statementsand FMR s.
Absence o f an internal auditfunction
Incapacity o fhe computerizedsystem in place (used b y theCRESAN2) to satisfy entirelythe needs o f MadagascarSHSDP and the requirements o fthe Government,IDA, and otherdevelopment partners infinanciallaccounting /technicalinformation.
Actions
Extension o fthe contract o fthe seventeen(17) financial management officers recruitedunder CRES AN2 to : i) rovidethe regionaloperatingunits w ith necessary capacities toquick ly disburse and account for funds o fSHSDP; ii) nsure, at the regional anddistrict levels,the use o f unds forthepurposes ntended; and iii) ssure timelypreparation o f periodic financial reportsrequired fo r proper monitoring o f activitiesimplementedby regional operatingunits,wi th respect to financial and physicalaspects.
Before credit effectiveness, a traini ng sessionw il l be organized to familiarize accountingstaff o f MOH , PCU and all f inancialmanagement officers wit hthe Bankprocedures in financial management anddisbursements.Elaboration o f a chart o f accountsinsufficient details (by categories, projectcomponents/activities/objects,budgetarynomenclature, geographic codes) to satisfyreporting requirements. The Chart o faccounts and related accounting proceduresw il l be formalizedin the updated accountingmanual.
Update and implementation o f an accountingmanual o fprocedures acceptable to donors to
provide clear guidance to project s taffworkin g both atthe central, regional anddistricts levels
Organization o fusers training toensureproper ap plication o f procedures, properrecord kee ping and adequate safeguarding o fassets.Creation o f an internal audit departmentwi thi n M O H o enhance internal controls andaddress areas o f concern identified duringprogram implementation.Customizing and upgradingthecomputerized accoun ting system acqu ired byCRESAN2 in order to: i) meet the usersneeds; ii) atisfy the government,ID A andother don ors requirementsinfinancialltechnical information; andiii)ensure timely production o f annual financialstatements and quarte rly Financ ialMon itoring Reports (FMRs) for mon itoringprogram activities.
Datedue by06/01/07
06/30/07
0513 1/07
BeforeEffectiveness
06115/07
Beforeeffectiveness
06115/07
Responsible
MOH/DFB
Consultant‘IDA
Consultant
Consultant
Consultant
M O H
Consultant
60

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 67/103
Absence o f acceptablearrangements in auditing.
Organization o fusers training bytheconsultant to ensure efficien tus e o f a l lmodules offered b ythe software.Recruitment o f an international privateauditing firm acceptable o ID A to carry outthe audit o fMadagascar SHSDP accountsjoint ly wi ththe Aud itor General.This auditw il l be performed bi-annually and conductedin accordance wit h Internation al Standards o fAuditing.
due bv06/30/07
Threemonths aftereffectiveness
Consultant
MOH, IDA
Institutional and Implementation arrangements
Project oversight
162. Pol icy guidance and overall project oversightwill be the responsibility o fhe Minis t e r o f
Health who will execute i t s mandate by liaising with the Pool’s Donors. The PCU, in closecollaborationwith Directorate o fFinancial Affa irs(DAF) an d the Directorate o fPlanning (DEP),will be in charge o f the annual program planning and budgeting. M O H through i ts GeneralSecretary will: i) ssure consistency o f program activitieswith the Government’s policyandstrategy; ii) pprove the annual works programs and budgets; and iii) ollow-up on projectperformance and impl em ent atio n progress.
Project coordination and implementation
163. The C R E SAN 2 P C U will be responsible for program management including: i)coordination o f the implementat ion o fthe program; ii) onsolidation o f the district work
programs and budgets; iii) maintenance o f records an d separate accounts fo r al l transactionsrelated to the PCU; iv) preparation, consolidation and produ ction o f the program financialstatements, quarterly FMRs and other financial information requiredby the government; v)management o f the pool account; and vi) monitoring and evaluation o fthe various activitiessupported under the project. The P C U s currently headedby a Coordinator namedby M O Handincludes specialists in accounting, procurement and mon itori ng and evaluation.
164. The implementat ion o fprogra m activitieswill be entrusted to: i) echnical departments o fM O H ; and ii) perating units at the regional/district levels, whichwill receive timely paymentsfr om the PCU-based up on submission o f satisfactory quarterly bud geted wo rk plans. T heoperating uni t s at the regional/district levelswill manage disbursements fr om their o w n bankaccounts. Under the supervision o f the finan cial officer(s),they will maintain records andaccounts for all transactions related to them, and prepare financial report and other basicinforma tion o n project management/monitoring asrequired by the PCU.
Budgeting
165. The expected program period for Madagascar SHSDPi s tw o years and six months. Aprogram implementation plan anddisbursement schedule has been drawn up and i s includedin
61

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 68/103
the Project Appraisal Document.I t s f rom thisdisbursement schedule (as may be subsequentlyrevised) that annual budgets will be drawn.
166. Th e annual budget will be prepared in l i ne with the Government's policyand strategy.The DAF, DEP and the Program Coordinatorwill be responsible fo r coo rdinatin g the preparation
o f an annual budget for the program.Budgeting arrangements for the projectwill be described indetails in the project accounting manual o fprocedures. T he ann ual estimates will reflect financialrequirements o f the program and should be finalizedthree months before the beginning o f hefiscal year, and submitted to the Ministry o f Finance fo r discussion and decision-makinginconformity with the defined calendar. The budget format will be based o n the programcomponents/activities/categories/geographiccodes. I t will show: i) xpenditure estimates perquarter and a total expenditure for the wholeyear; and ii) unds expected from IDA, AFD andother donors (i f any). The upgraded accounting software tobe implemented will be able to cateradequately for the budgeting arrangements, comparing planned and actual costs and reportingvariances. Pr ior to implemen tation o fthe project , M O H staffwill attend a specific training toensure efficient use o fhe new system and prope r preparationo f FMRs.
Accounting
167. Madagascar SHS DP will use an accounting system in compliance with generallyaccepted accounting standards and the Plan Comptable des Ope'rations Publiques and donorrequirements. This system will operate o n a double ent ry accrual principle s andwill us e standardbook accounts (journals, ledgers and trial balances) to enter and summarize transactions.Revenue will be recorded when cash i s received, while expenses and related liabilitieswill berecorded when incurred, especially upon receipt o fgoods, works and services.
168. The regional operating units will maintain a simple cash book showing clearly cashreceived, payments made for each component/activities for which they have implementationresponsibility, and cash balances. They also will prepare on a quarterly basis, in collaborationwith the financ ial officers, a moresimplified orm o f eport ing on sourcesand uses o f funds, andsend i t to PC U or consolidationwith their acti vity reports.
169. To strengthen the project financial managementsystem, i t was agreed that a consultantwill be recruited to update the accounting manual o f procedures (for M OH /P C U and relatedoperating un i t s ) describing the outl ine o fhe accounting system(s), the accounting policies to befollowed, the Chart o f accounts, th e formats o f books and records, the financial reporting, andrelevant informa tion to facilitate recordkeeping and maintenance o f proper con trol over assets.The consultant will also provide adequate training to staff toensure better understanding andproper application o f a ll procedures describedin this manual. The accounting manual o f
procedures shou ld be finalized andsubmitted to IDA pri or to credit effectiveness.
170. While all the donors involvedin Madagascar SHSDP appreciate the need to usegovernment systems, the IFMIS system implemented within the Ministry o f Finance does n otserve the needs o f SHSDP without manyurgent corrections in the short term. As this i s notpracticable, an interim measure has been therefore taken while the government system i s beingimproved. To ensure timely production o f financial information required for managing and
62
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 69/103
monitoring program activities,the P C U will use an integrated computerized system acquiredwithin the context o f the CRE SAN 2, whic hin particular facilitates: annual progra mming o factivities and project resources, record-keeping (general accounting and costaccounting),financial and budgetary management, fixed assets management, procurement management,preparationo f C R E S A N2 financia l statements and quarterlyFMRs as required by IDA.
171. However, this software needs to be customized an d upgraded to: i) ee t the users needs;ii) satisfy the Government, IDA and other donors requirements in financial/technicalinformation; and iii) nsure timely productio n o f SHSDP program financial statementsandquarterly FMRs as required by donors fo r mon itoring program activities. T o avo id double datacapture, this system should also allow fo r extracting efficiently a ll required information f ro mthedatabase ORACLE presently in place and used by M O H for recording commitments,“liqui datio ns” and settlement orders.The consultant in charge o f his update will pro vide userstraining t o ensure efficient use o fa l lmodules offeredby the software. The t e rms o f eference forthis consultant have been reviewed by the Bank Financial Management Specialist. Since theupdate o f the software i s underway and expected to be finalized prior to June 15, 2007,the
inc lusion o fhis measure as effectiveness conditionwill no t be necessary.Internal Control and Internal Auditing
172. The C R E SAN2 P C U s being transformed into the P C U for the Madagascar SHSDP.I twill be staffed with: i) qualified Financial Management Specialist acquaintedwith bothnational financial managementsystem and Bank financial management procedures, responsiblefor overa ll supervision o f inance, accounting,budgeting and reporting; andii) wo qualified andexperienced accountants f ro m C R ES AN 2. T o ensure effectivetransfer o f ski l ls and al low theP C U to respond to a possible increase o f he volume o f financial management tasks once otherdonors provide financing, an accounting assistantwill be selected am ong the M O H s ta ff basedon qualification and experience. To strengthenthe financia l management capacity o fthe DAFand to help i t to adequately supervise the PCU, a technical assistant acquainted with Bankprocedures will be recruited not later than tw o m onth s after credit effectiveness.
173. T he M O H P C Uand related operating u n i t s will have an administrative and accountingprocedures manu al describing cle arly the lines o f responsibilities and authority thatexist withappropriate segregation o f duties. I t will also p rovide sufficient informationto facilitate record-keeping and the maintenance o fproper con trol over assets.
174. To ensure efficient use o f credit funds fo r the purposes intended and consistentapplicat ion o fprocedures o n procurement, financial management, disbursement, a n inte rna l audi tDepartment will be created within M O H p rio r t ocredit effectiveness. This Department will
collaborate closelywith the General Inspectorate fo r Finan cewhen this later is fully functional,and will report directly to the Minister o f Finance andthe Minister o f Heal th .All issuesidentified during internal audit should be addressed quickly to improve the programperformance.
63

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 70/103
Financial Reporting
175. T o monitorthe implementat ion o f SHSDP, P C Uwill produce the fol l owi ng reportsthatshould be prepared n compliancewith international accounting standards:0 Annualfinancial statements comprising: i) ummary o f Sources and Uses o f Funds (by
components/project activitieshre dit category and showing a ll sources o ffunds); ii) rojectBalance Sheet; iii) he Accounting Policies Adoptedand Explanatory Notes; iv) aManagement Assertion.Quarter& FMRs: F M R s include financia l reports, physica l progress reportsand procurementreports to facilitate proje ct monitoring .FMRs should be submitted t o IDA within 45 days o fthe end o f the reporting period (quarter). Mode ls o f quarterlyFMRs and annual financialstatements will be presented in he project accounting manual o fprocedures.
Auditing
176. The financial statements o f SHSDP (includingthe P H R D grant) will be audited by an
international private auditin gfirm acceptable to donor, in collaborationwith the Auditor General.This audit will be performed bi-annually and conducted in accordance with InternationalStandards o f Auditing. The auditors should be recruited within three months after theeffectiveness date. The audit reportwill be submitted t o IDA not later than six months after theend o feach period. The auditors will be required to: i) xpress an opinion on the project f inancialstatements; ii) arry out a comprehensive review o f he internal control procedures and provide amanagement report outlining any recommendations fortheir improvement. The t e rms o freference o f the audit will be reviewed by the financial management specialisto f the Bank/IDAto ensure the adequacy o f the audit scope, drawing special attention to particularrisk areasidentified during proje ct preparation.
64
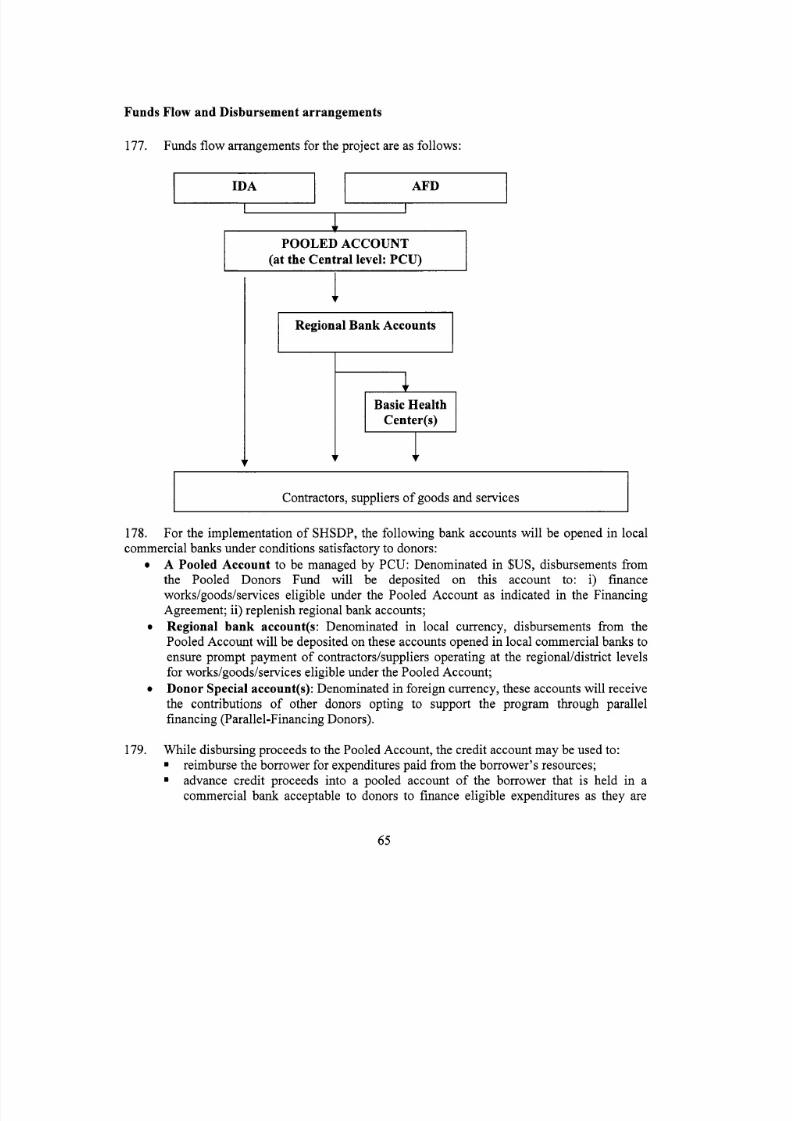
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 71/103
Funds Flow and Disbursement arrangements
177. Funds flo w arrangements forthe project are as follows:
POOLED ACCOUNT
Basic Health
Contractors, suppliers o f goods and services
178.commercialbanks under conditions satisfactory to donors:
0
For the implementation o f SHSDP,the followingbank accounts will be opened in local
A Pooled Account to be managed by PCU : Denominatedin $US, disbursements fromthe Pooled Donors Fund will be deposited on this account to: i) financeworks/goods/services eligibleunder the Pooled Account as indicated in the FinancingAgreement; ii) eplenish regional bank accounts;Regional bank account(s: Denominated in local currency, disbursements f iom thePooled Accountwill be deposited on these accounts opened in oca l commercial banks toensure prom pt payment o f contractordsuppliers operating atthe regional/district levelsfor works/goods/services eligibleunder the Pooled Account;Donor Special account(s):
Denominated in oreign currency,these
accountswill receive
the contributions o f other donors opting to supportthe program through parallelfinancing (Parallel-Financing Donors).
0
0
179. W hi le disbursing proceeds tothe Pooled Account, the credit account ma y be used to:. reimburse the borrower fo r expenditures paid f romthe borrower’s resources;. advance credit proceeds into a pooled account o f the borrower that i s held in acommercial bank acceptable to donors to finance eligible expendituresas they are
65

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 72/103
incurred and for which supporting documents will be provided at a later date (seebelow: Disbursement from the Pooled Account).make a direct payment to a third party;enter into special commitments in writing to pay amounts to a third party in respect ofexpenditures to be financed out o f the credit proceeds, upon the borrower’s request
and under terms and conditions agreed th e Bank and the borrower.
..180. There will be a minimum value for applications fo r direct payment, and specialcommitment that may have to be made for transaction-based disbursements. The minimumvalue will be documented in the disbursement let ter related to SHSDP. The accounting manualof procedures describes in details the application steps and requirements fo r requesting areimbursement, a direct payment fo r third party, and applying fo r a special commitment.
Disbursement from the Pooled Account
181. Flows o f funds from the Pooled Account will be governed by a Memorandum of
Understanding hat will be signed by a l l donor partners and the government. IDA and AFD willdeposit in the Pooled account their contribution as per agreed Annual Work Program, in anagreed proportion and periodicity (on a six months basis) as defined in the Memorandum.Disbursements to the Pooled account will be done based on quarterly FMRs. Under thisdisbursement method, a forecast o fprogram expenditures will be agreed between the MOHPCUand donors, covering a period o f six months. The borrower may request an advance for anamount not exceeding this cash forecast. Supporting documentation or these disbursements wi llsubmitted with the subsequent FMR and reviewed by donors to confirm eligible expendituresduring th e period covered by the FMR. The project will finance Goods (equipment, safe deliverykits, drugs and medical supplies and maternal kits -- estimated total value US$4.9 million) andConsulting Services fo r technical assistance, training and strengthening supervisory andimplementation capacity at district and regional levels (estimated value US$4.25 million). Inaddition, the project wil l finance project operating costs, financial audits and local costs of theDemographic Health Survey (estimated value U S $ 0.85 million). The cash request at thereporting date will be the amount required for the forecast period as shown in the approvedFMRs less the balance in the Pooled Account at the end o f the quarter. Subsequentdisbursements from Pooled Account w ill therefore be made in respect o f this cash request.Detailed disbursement procedures will be described in the project accounting manual ofprocedures.
Disbursement from regional bank accounts
182. The amount to be advanced to each regional operating unit will be determined on th e
basis o f a quarterly work program for an amount not exceeding a fixed ceiling indicated in theoperations manual. Subsequent payments will be based on the satisfaction o f certain criteria: atechnical (physical progress) and financial performance assessment carried out by M O H P C Uand submission o facceptable documentation for previous releases.
183. Each regional operating unit will submit quarterly the following documents: i) progressreport showing physical achievements, a summary o f the use o f funds by activity, and a copy of
66

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 73/103
the bank statement. All documents supporting expenditures will be retained by the operatingunits and made available for review by the PCU staff, the internal auditor, Badddonorssupervision mission andthe independent auditors as necessary.
Supervision Plan
184. Taking into accountthe l e ve l o frisk associated with the financ ial management aspects o fthis program, the financial management specialist will pay more frequent visits to theMOH/ C R E SAN2 to ensure timely implementation o f al l actions expected tobe in place prior t ocredit effectiveness. When project expendituresbegin, a supervision miss ionwill be conducted atleast twice a year based on the risk assessment o f the project. The mission’s objectives wil linclude that o fensuring that strong financial management systems are maintainedfor the projectthroughout i t s l i f e .A reviewwill be carried out reg ularly t o ensure that expenditures incurre dbythe project remain eligible fo rSHSDP funding. The Imple menta tion Status Reportwill include afinanc ial management rating for the component. The finan cial management specialistwil l alsoreview quarterly FMRs, the audit reports and fol low-up o n t imely implementation o frecommendations from auditors.
67
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 74/103
Annex 8: Procurement Arrangements
Madagascar Sustainable Health System Development Project
A. GENERAL
185. Procurement for the proposed projec t wo ul dbe carried out in accordance with the Wo r l dBank's "Guidelines: Procurementunder IBRD Loans and IDA Credits" dated M a y 2004; and"Guidelines: Selection and Employmen t o f Consultantsby Wo rld Ba nk Borrowers'' dated Ma y2004, and the provisions stipulated in the Legal Agreement. The various itemsunder differentexpenditure categories are described in general below. For each contract to be financed by th eCredit, the different procurement methods o r consultant selection methods,estimated costs, priorreview requirements, and time frame are agreed between the Borrower and the Bank in theProcurement Plan. The Procurement Plan will be updated at least annually or as required t ore f lec tth e actual proje ctimplementation needs and improvements in nstitutio nal capacity.
186. Advertisement: A General Procurement No tice will be published in UN DevelopmentBusiness and Development Gateway Market (dgMarket) and will show all InternationalCompetitive Bidding (ICB) for goods and wor ks and major con sulting servicerequirements.Specific Procurement Noticeswill be issued in Developme nt Business and dgM arketand at leastone newspaper with nationwide circulation for I C B contracts and before preparation o fshortlistswith respect to consulting contracts above US$200,000,in accordance with the Guidelines.
187. Procurement o f Works: Works procured underthis project wou ld include: provision o fbasic water and sanitation facilities at health centers, services to strengthen health centers.Theprocurement will be done using the Bank's Standard Bidding Documents (SBD) f o r a l l I C B a ndNationalSBD agreed with or satisfactory to the B ank. T othe extent practicable, contractshall begrouped into bid packages estimated to cost th e equivalent o f US$500,000 or more and wou ldbe
procured throug h I C B procedures. F or contract estimated to costless than US$500,000equivalent per contract, ci vi l wo rk procurement ma ybe carried out through NationalCompetitive Bidding (NCB) and contracts for sma ll works, estimated to costless thanUS$50,000, may be procured through quotations procedures. The bidding documents shallinclude a detailed description o f the works, inclu ding basic specifications, therequiredcomp letion date, basic form s o f agreement acceptable toIDA and relevant drawings whereapplicable. Specific procedures detailscan be found in the Project ImplementationManual(PIM).
188. Procurement o f Goods: Goods procured under this project would include, officefurniture and equipment, vehicles, comp uter hardwareand software, office equipment,mobilehea lth centers, an d goods to strengthen heal th center to de live r basic package o fservicesincludingthe provision o f necessarydrugs, equipment and testing facilities. The procurementwill be done using the Bank's SBD for a l l IC B and Nat ionalSBD agreed with or satisfactory tothe Bank. To the extent practicable, contracts shall be grouped intobid packages estimated tocost the equivalent o fUS$250,000 or more and wou ld be procured through I C B procedures. Fo rcontract estimated t o cost less than US$250,000 equivalentper contract, procurement o f goodsmay be carried out through N C B procedures and purchase o f smallfurniture estimated to costless than US$30,000 will be conducted throu ghprudent shopping procedures.
68

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 75/103
189. Direct Contracting for works and goods may be used in exceptional cases, such as forthe extension o f an existing contract, standardization, proprietary items, spare parts for existingequipment, and urgent repairs and emergency situations, accordingto paragraphs 3.6 an d 3.7 o fthe Guidelines. The items to be procured through Dire ct Contracting wo ul d be agreed onin the
procurement plans.
190. Procurement o f non-consulting services: Procurement from United Nat ion s agenciesfor supplies carried out under their ow n procedures may includ eUNDP, UNICEF, WHO and/orthe International Agency Procurement Services Organization. The standard for m o f contractwith UN agencies will be used for such procurement. The items to be procured from UNagencies would be agreed on in the procurement plan i f and when t o be used. In addition,SALAMA services ma y be used as a procurement agent to purchase drugs and me dica l suppliesin accordance with Art ic le 3 .10 o f heGuidelines.
191. Selection o f Consultants: The project will finance the contracting o f consultancy
services f or techn ical assistance, finan cial a nd technica l audits, and capacitybuilding. Firms wi llbe recruited on the basis o f the Quality and Cost Based Selection (QCBS)method, using th eBank’s Standard Request fo r Proposals. Selectio n based o n consultant’s qua lificatio ns (CQ) canbe used fo r the recruitment o f raining institutions and for assignmentsthat meet criteria set outin Para. 3.7 o f he Consultant Guidelines. Sing le source selec tion canbe used to contract f i r m s o rindividuals for assignment thatmeet criteria set out in Para. 3.9 to 3.13 o f the ConsultantGuidelines and for contract which amount do not exceedUS$lOO,OOO. Specialized advisoryservices would be procured throu gh Indiv idu al Consultants S election (ICs), based onthequalifications o f ndiv idua l consultants f orthe assignment in accordance with the provisions o fparagraphs 5.1 thro ug h 5.3 o fhe Consultant Guidelines.
192. Operating Costs financed throughthe project w ou ld be procured usingthe implementingagency’s adm inistra tive procedures, wh ic hwere review ed and foun d acceptable tothe Bank. Theprocurement procedures and SBDs t o be used for each procuremen t method, as well as modelcontracts f or w ork s an d goods procured, are presentedin the P I M .
193. Review by the Bank o f Procurement Decisions: The thresholds for prior reviewbyBank are specified in the procurement plans. Table 1 shows (a) th e proposed thresholds for thedifferent procurement methods, a nd (b) the proposed initially-a greed thresholds fo rprior reviewby the Bank. The Bank will preview procurement arrangements proposed by th e Borrower forthe items specified in the procurement plans for their conformitywith the Finan cing Agreementand the applicable Guidelines. Any procurement item not specified for priorreview may besubjected t o a post-review o fhe procurement process.
69
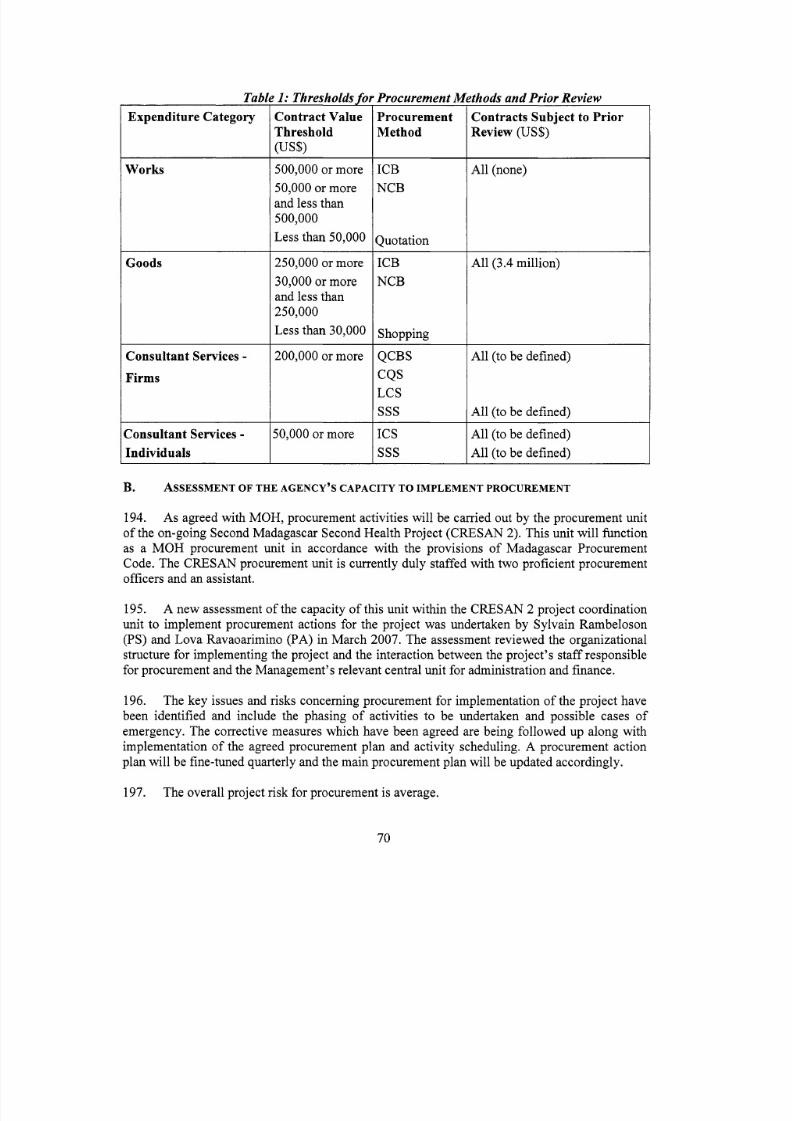
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 76/103
Table 1: Thresholds for Procurement MExpenditure Category
Works
Goods
Consultant Services -Firms
Consultant Services -Individuals
Contract ValueThreshold(US$)
500,000 or more50,000 or moreand less than500,000Less than 50,000
250,000 or more
30,000 or moreand less than250,000Less than 30,000
200,000 or more
50,000 or more
ProcurementMethod
I C BN C B
Quotation
I C BN C B
Shopping
QCBS
CQ SLC SsssI C ssss
rthods and Prior Review
Contracts Subject to PriorReview (US$)
All (none)
All (3.4 million)
A ll (to be defined)
All (to be defined)
All (to be defined)All (to be defined)
B. ASSESSMENT F THE AGENCY’S CAPACITY TO IMPLEM ENT PROCUREMENT
194. As agreed with MO H, procurement activitieswill be carried out by th e procurement unito f the on-going Second Madagascar SecondHealth Project (CRES AN2). This unit will functionas a M O H procurementunit in accordance with the provisions o f Madagascar ProcurementCode. The CRE SAN procurementunit i s currently duly staffedwith two proficient procurementofficers and an assistant.
195. A new assessment o f the capacity o fthis unit within the CR ES AN 2 project coordinationunit to implement procurement actions for the project was undertaken by Sy lvain Rambeloson(PS) and Lov a Ravaoarimino (PA)in Mar ch 2007. The assessment review ed the organizationalstructure for implementing the project and the interactionbetween the project’s s taff responsiblefor procurementand the Management’s relevant centralunit for administration and finance.
196. The key issues and risks concerning procurement fo r implementation o fthe project havebeen identified and include the phasing o f activities to be undertaken and possible cases o femergency. The corrective measures which have been agreed are being fo llow edup along withimplementation o fthe agreed procurement pla n and activity scheduling.A procurement actionplan wil l be fine-tuned quarterly and the ma in procurement plan wi llbe updated accordingly.
197. The overall projectrisk for procurementi s average.
70
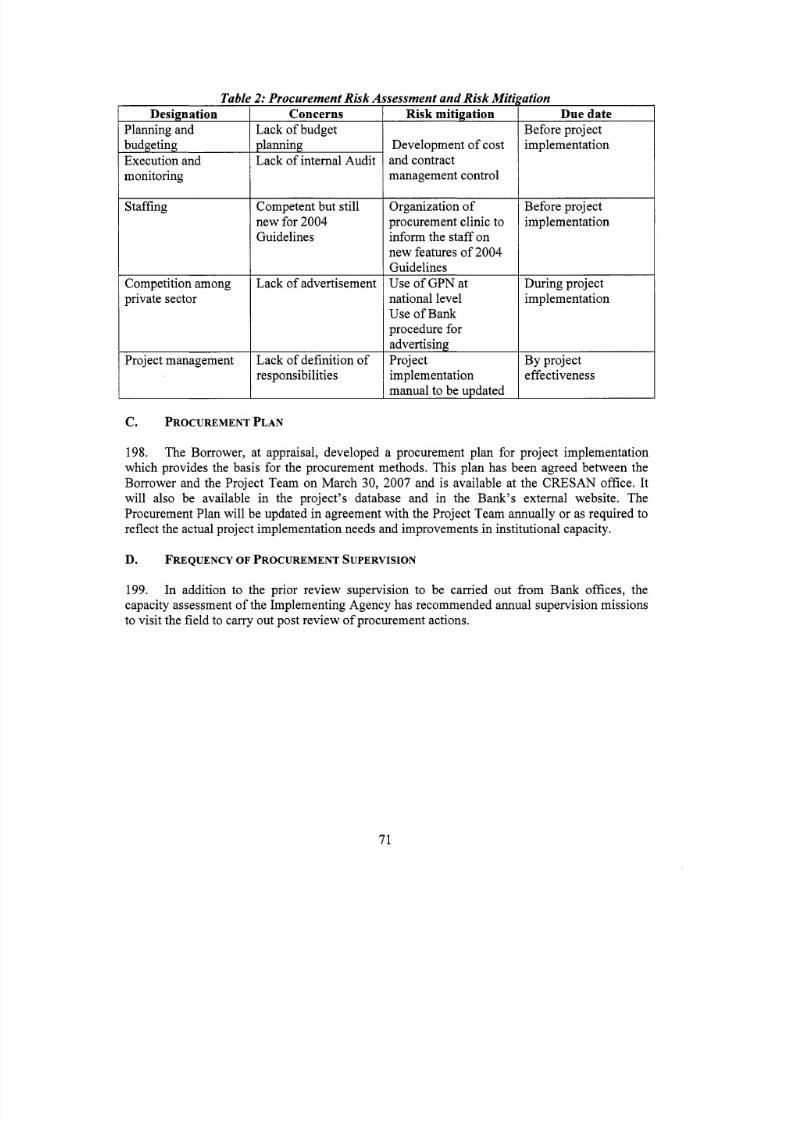
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 77/103
TabkDesignation
PlanningandbudgetingExecution andmonitoring
Risk mitigation
Development o fcostand contractmanagement contro l
Organization o fprocurement clinic toin formthe staff o nnew features o f2004
Staffing
Due dateBefore projectimplementation
Before projectimplementation
Competition amongpriva te sector
GuidelinesUse o f G P N at
Proje ct management
During project
2: Procurement Risk AConcerns
L a c k o fbudgetplanningLack o f nternalAudit
nationall eve lUse o fBankprocedure fo r
advertisingProjectimplementationmanual to be ur>dated
Competent but st i l lnew for 2004Guidelines
implementation
By projecteffectiveness
L a c k o fadvertisement
Lack o f de f ini ti ono fresponsibilities
C. PROCUREMENT LAN
198. The Borrower, at appraisal, developed a procurementplan for project implementationwhich provides the basis forthe procurement methods. This pl an has been agreed between theBorrower andthe Project Team on M arc h30, 2007 and i s available at the CR ES AN off ice .I twill also be available in the project’s database and in the Bank’s external website. TheProcurement Pla nwill be updated in agreement with the Project Team annually o r asrequired oreflect the actual project implem entat ionneeds and improvementsin nstitutio nal capacity.
D. FREQUENCY OF PROCUR EMEN T SUPERVISION
199. In addition to the prior review supervision t o be carried out from Bank offices,thecapacity assessment o f he Implementing Agen cy has recommended annual supervision missionsto visit the fie ld to carry out post review o fprocuremen t actions.
7 1
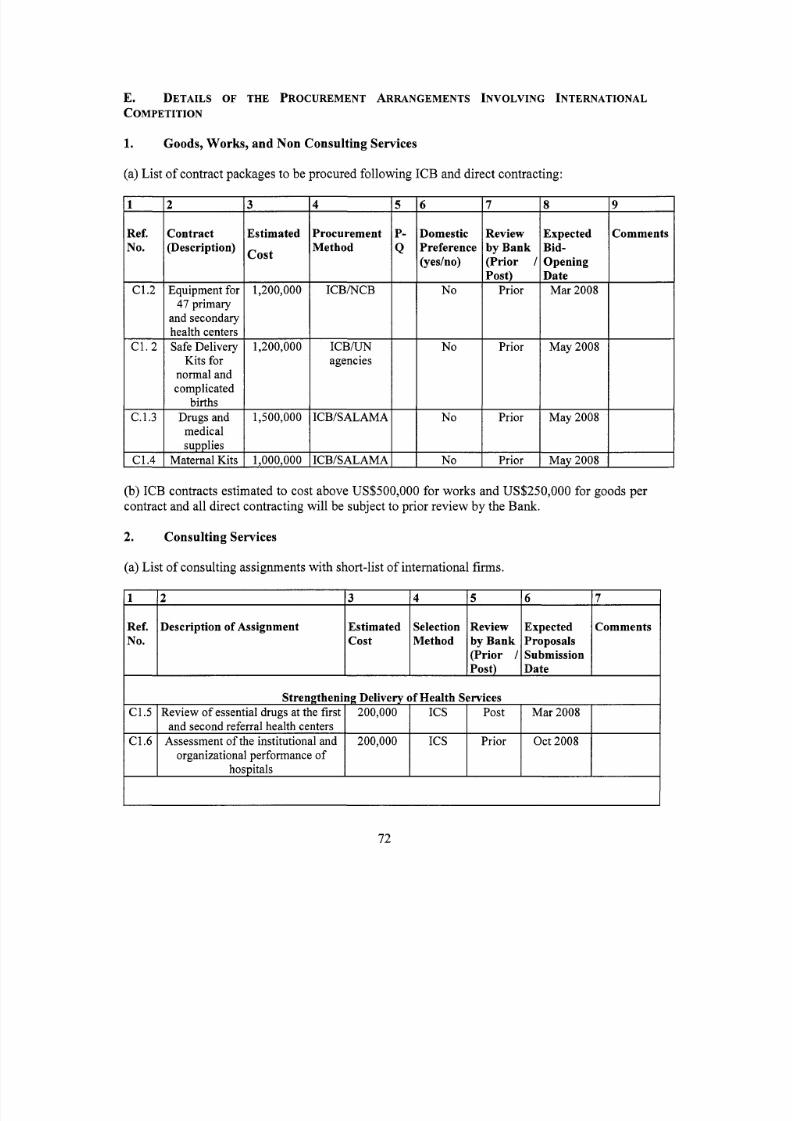
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 78/103
E. DETAILS OF THE PROCUREMENT ARRANGEMENTS NVOLVING INTERNATIONAL
COMPETITION
1 2
Ref. Description o f AssignmentNo.
1.
(a) L i s to f contract packages to be procured following I C B and direct contracting:
Goods, Works, and Non Consulting Services
3 4 5 6 7
Estimated Selection Review Expected Commentscost Method by Bank Proposals
(Prior / SubmissionPost) Date
Ref.YO .
C1.5 Review o f essential drugs atthe f i rs tand second referral h ealth centers
C1.6 Assessment o fthe institutional andorganizational performance o f
hospitals
Contract(Description)
200,000 ICs Post M ar2008
200,000 IC s Pr ior Oct2008
47 primary
Kits fo rnormal andcomplicated
birthsC.1.3 Drugs and
medical
3
Estimated
cos t
1,200,000
1,200,000
1,500,000
1,000,000
4
ProcurementMethod
ICB/NCB
ICBAJNagencies
ICB/SALAMA
I C B B A L A M A
(yesho)
I No
7 18 19I I
Review Expected Commentsby Bank Bid-(Prior / Opening
Prior May2008
Irior I May2008 I
__c;_c_r ior M a 2008
(b) IC Bcontracts estimated to cost above US$500,000 for works andUS$250,000 fo r goods percontract and a ll direct co ntractingwill be subject to prior rev iewby the Bank.
2. Consulting Services
(a) L i s to f consu lting assignments with short-list o f nternationalf i rms.
72

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 79/103
C2.1 Development o f protocols forimprovingthe workin g conditions o f
medica l personnelin rur al areasC2.2 Deve lopment and managemento f
career plans and effective hum anresources management tools
new tra ining strategiesC2.3 Development and implementation o f-
3.1
75,000 IC s Prior Jan 2008 M ulti pleContracts
75,000 QC BS Post Jan 2008 Multiple
Contracts
750,000 CBS Prior N o v 2007 Multiplecontracts
C3.2-3.3
Development of nnovative resourcemo biliza tion mechanisms
200,000
Development o f ools to improvemanagement o f available public and
private funds
innovative provider paymentmechanisms and contracts,
Development and testing o f
200,000
200,000
icin Mana ement
contracts
QCBS Prior Ma y 2008 Multip leCQS contractsI C s
QCBS Prior Ma y 2008 Multiple
Contracts
C4.1 Incentives for promo ting safe
C4.2 Strengthening comm unity awarenessdelivery in hea lth centers
through social mob ilizationn 6communes
C4.3 Implementation o f(( Communemendrika )) approach in 6
500,000
150,000
150,000
CQS/I C sCQS
QCBS
Prior Jan 2008 Mu ltip lecontracts
Prior M ar 2008 Multiplecontracts
Post May2008 Multiplecontracts
73
C4.4
C4.5
C5.1
C5.2
C5.3
communesOrganizationo f ntegrated E C 150,000 QCBS Post M ay 2008 Multiple
campaigns at al l levels contractsPil ot initiative t o increase rateo f 100,000 CQS Prior April 2008tuberculosiscure
Institutional StrengtheningStrengthening supervisory and 1,000,000 I C s Prio r Dec 2007 Multiple
implem entation capacity at district contractsand regiona l levels
Strengthen nationalM&E system 100,000 QCBS/ Prior Feb 2008 Multiple(MAP,PDSS, PGE) I C s contracts
Support to the Natio nal Health 100,000 CQS/ I Prior Mar2008 Multiple
C5.4
C5.5
Info rma tion System(NHIS) ICs ContractsEstablishment o f a Center for He alth 100,000 CQS/ Prio r April 2008 Multiple
Policy and Development IC s ContractsSupport to the DHS for operating 400,000 Jan 2008
C5.6
C6.6
costsFinancial and TechnicalAudits 100,000 QCBS/ Prio r Jan 2009 Tw o
ICs ContractsProject Opera ting Costs 350,000

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 80/103
(b) Consultancy services estimated to cost above US$lOO,OOO per contract and single sourceselection o f consultants( f i rms) and o f ndividual consultants assignments estimated to cost aboveUS$50,000 will be subject to pri orreview by the Bank.
(c) Short l i s t s composed entirely o f national consultants: Short listso f consultants for servicesestimated to cost less than US $l OO, OOO equivalent per contract m ay be composedentirely o fnational consultants in accordance with the provisions o f paragraph 2.7 o f the ConsultantGuidelines.
74
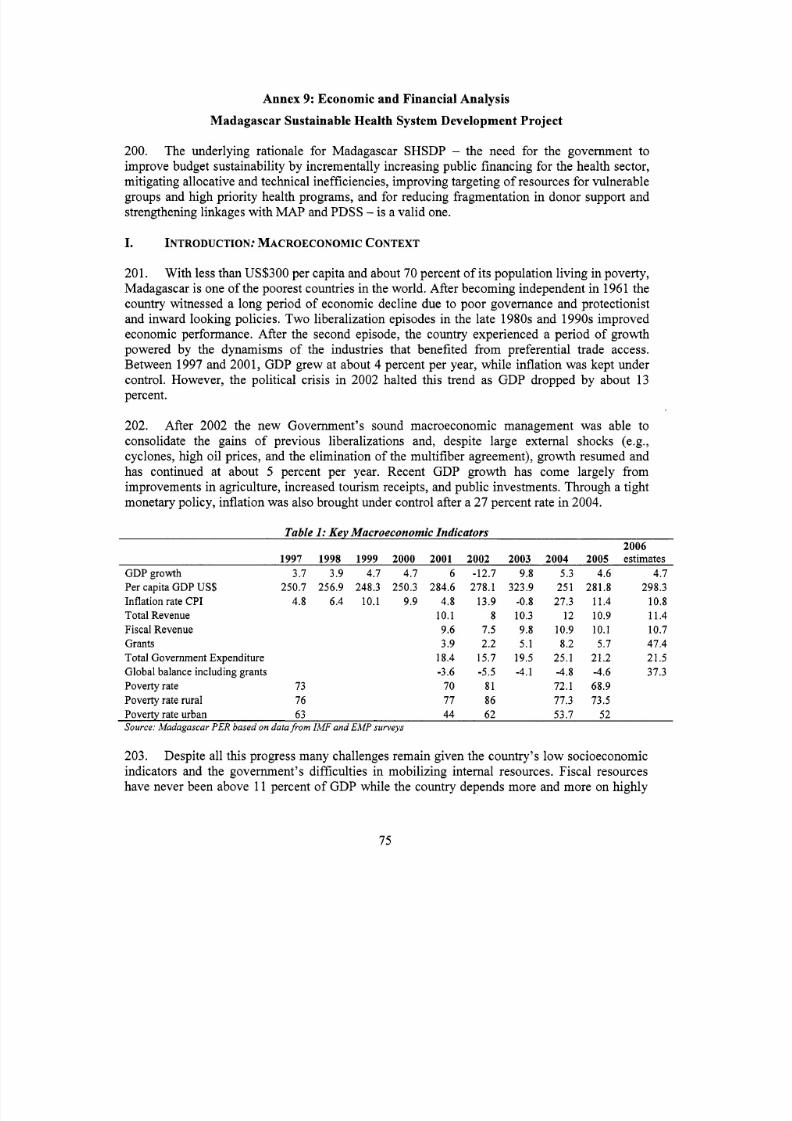
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 81/103
Annex 9 : Economic and Financial Analysis
Madagascar Sustainable Health System Development Project
200. The underlying rationale for Madagascar SHSDP- the need for the government to
improve budget sustainabilityby incrementally increasing public financing fo r the health sector,mitigating allocativeand technical inefficiencies, impro ving targeting o f esources fo r vulnerablegroups and high prior ity health programs, and for reducing fragmentationin donor support andstrengthening linkageswith M A Pand PDSS - s a valid one.
I. INT RODUCT ION: ACROECONOMIC ONTEXT
201. Withless than U S 3 0 0 per capita and about 70 percent o f ts populationliving in poverty,Madagascar i s one o f he poorest countries in he world. After becoming independent in 1961 thecountry witnessed a lon g period o f economic declinedue to poor governance and protectionistand inwa rd lookin g policies. T w o liberalization episodesin the late 1980s and 1990s improvedeconomic performance. After the second episode, the country experienced a period o f grow thpowered by the dynamisms o f the industries that benefited from preferential trade access.Betw een 1997 and 2001, GDP grew at about 4 percent per year, wh ile in flatio n waskept undercontrol. However, the political crisisin 2002 halted this trend as GDP dropped by about 13percent.
202. After 2002 the new Government’s sound macroeconomic management was able toconsolidate the gains o f previous liberalizations and, despite large extern al shocks(e.g.,cyclones, high o i l prices, and the eliminationo f he multifiber agreement), growth resumed andhas continued at about 5 percent per year. Recent GDP growth has come largely f romimprovementsin agriculture, increased tour ism receipts,and pub lic investments. Th rough atightmonetary policy, inf lat ion was also broughtunder con trol after a 27 percent ratein 2004.
Table 1: Key Macroeconomic Ind icators2006
1997 1998 1999 2000 2001 2002 2003 2004 2005 estimatesGD P gro wth 3.7 3.9 4.7 4.7 6 -12.7 9.8 5.3 4.6 4.7Per capita GDP US$ 250.7 256.9 248.3 250.3 284.6 278.1 323.9 251 281.8 298.3In fla tio n rate CP I 4.8 6.4 10.1 9.9 4.8 13.9 -0.8 27.3 11.4 10.8To tal Revenue 10.1 8 10.3 12 10.9 11.4Fiscal Revenue 9.6 7.5 9.8 10.9 10.1 10.7Grants 3.9 2.2 5.1 8.2 5.7 47.4Tota l Governm ent Expe nditure 18.4 15.7 19.5 25.1 21.2 21.5
Pove rty rate 73 70 81 72.1 68.9
Pove rty rate urban 63 44 62 53.7 52Source: Madagascar PER based on data ro m IMF and EMP surveys
Globa l balance including grants -3.6 -5.5 -4.1 -4.8 -4.6 37.3
Poverty rate rura l 76 77 86 77.3 73.5
203. Despite al lthis progress many challenges remaingiven the country’s l o w socioeconomicindicators and the government’s difficultie sin mo bil izin g in ternal resources. Fisc al resourceshave never been above 11 percent o f GDP whil e the country depends mo re and more onhighly
75

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 82/103
unpredictable fo reig nfunds. Nevertheless, the country has benefitedfrom the HI PC initiat ive;in2006 alone the country received US$2.3 billionin debt reduction, close to 43 percent o ft s GDP.
Ethiopia
Kenya
Malawi
11. ECONOMIC ANALYSIS I: TRENDS N HEALTH INANCING AND IMPLICATIONS FOR
BUDGET USTAINABILITY'
5.7 4.3 55.1 44.94.9 19.2 56.0 44.09.8 Not available 58.9 41.1
204. The country spends very l i t t l eo n health, a situation thatwill worsen once donor financedprojects close. This financing gap cannot be lessened in the short run with interna l resourcesgiven the Government's macroeconomic constraints. Madagascar SHSDP aims atfilling this gapwhile at the same time lessening some o f he public expenditure management bottleneckstheGovernment confronts: vola tility o f donorfunds and la rge transaction costs created by projectswith different management and report ing mechanisms.
Uganda
Zambia
205. Accordingto th e Nation al Health Accounts(NHA) 2003, Madagascar spent about US$12per capita on he alth that year, corresponding to about 3.5percent o f G DP. As seen in Table 2,these numbers are below the median in the region and mu ch belowthe US$30 to US$40 per
person per year recommended by the W H O to finance a package o f essential services(Commission for Hea lth and Macroeconomics, W HO , 2002).At the current l e ve l o fexpenditures, the country will not be able to achieve the health related MDGs. M O H , with thesupport o f UNICEF, calculated that an additionalUS$ 5.40 per capita woul d be needed in th enext three years to achieve a 41 percent reductio nin chi ld morta l i tyand a 35 percent reductioninneonatal and maternal morta lityneeded to sustain progress in achieving these MDGs.
7.4 Not available 72.1 27.95.8 17.4 47.1 52.9
Table 2: Comparison in h ealth expenditure indicators between Madagasc ar
(Mozambique I 5. 8 I 8.9 I 71 O I 29.0 IIRwanda I 4.1 I 12.7 I 50.6 I 48.8 IITanzania I 4.9 I Not available I 45.2 I 54.8 I
I 12.9 I 57.1 I 42.9 Iub-Saharan African 6.0countries median
Source: MOH. 2005. Madagascar National Health Accounts2003
206. Ext ern al assistance i s the mai n source o f financingin the sector, representing about 37percent o f total spending on health (NHA, 2003). This large percentage o f total expenditurefinanced by fo rei gn ai d represents a challengefor M OH , wh ich manages most o f hese resources.
' This section borrows heavily from the Madagascar PER Health Chapter.The expenditure o f he rest o f he world (5 percent) was added to that o f he public sector (55 percent).
76

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 83/103
207. The high volat i l i ty and unpredictabil ity o fhese funds and the complexityo f managingprojects with different procurement and monitorin g mechanisms make budget planning andexecution in the ministry difficult.
Tota l budget allocation (realin billion Ariary)
Source: Madagascar PER Heal th Chapter based on data ro m the Ministry of Economics, Finance, and Budget
208. Public funds represent the next largest source (32 percent), followedby private, mainlyout-of-pocket expenditure (3 1 percent). Even thou gh fore ign aid represents the pri ncip al sourceo f inancingin the sector, the pub lic sector is the m ai n financ ing agent, manag ing55 percent o fthe funds. M O H managesthe large majori ty o f hesefunds, more than 80 percent o f al l pub licexpenditure o n healthin the last decade. Pub lic expenditure o n health, m ore specific ally M O Hexpenditure, has rema ined stable in the last years at about 6 to 7 percent o f otal Gove rnmentexpenditure. However, the budget allocation to the Ministry has actually decreased slightly aspercentage o f he total Governmentbudget fro m almost 8 percentin 2000 to about 6 percent in2006 (see Table 3).
Thisdecrease moves the country farther away fromthe Ab uj a consensus o f
alloca ting 15 percent o f ota l Government expenditure tothe hea lth sector.
209. N o t only havebudget allocations t o the sector decreased as percentage o f ot al budget,the execution rate o fhe budget has remained low . Betwe en 1997 and 2005the execution rate o fM O H has averaged 77 percent only, well bel ow levels in other ministries. Factors that explainthe limited absorptive capacity include: (i) ate nomination o f key functionariesin theexpenditure chain; (ii) imited management capacity and lack o f clear def ini t ion o fresponsibilities among the budget administrators; (iii) omplex and numerous budget andprocu reme nt procedures; and (iv) difficultiesin he coordination o fdonors.
210. The per capita rea l expenditure f ro mMOH in dollar t e rms has remained belo w US $4 inthe last decade, showing .a marked decrease after 2003. In 2005 the country was spending onlyabout US$ 2 per capita o n health care, p artlydue t o a marked devaluation o fthe loca l currency.The total healthbudget fo r M O H n 2006 fel l short o fhe projections made in the Medium TermExpenditure Framework (MTEF) o f the sector (2005). The MTEF document contains fourscenarios o f possible health expenditures fr om 2006 to 2014. Table 4 shows tw o o f thosescenarios. The first i s the most conservative one, in that i t assumes that the country will notachieve the Abu ja consensus o f having a health budget equal to 15 percent o f the total
77

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 84/103
Government budget by the year 2014. The other three scenarios make this assumption but th eincrease in expenditure across the years fol low sdifferent paths. Th e second scenario, also show nin Table 4, assumes a linea r increase in he health budgets.
Health budget (in billions o fAriary) 141.96 86.93 164.61Health budget per capita/MGA 5779 7955 9094
Health expenditure per capita/MGA 8554 5082Health expenditure per capita/US$ 4.57 2.53
Budget per capita/ US$ 3.09 3.97 4.17
211. As can be seen in Table 4, even in the most conservative scenario the projected budget
fo r 2006 i s mu ch larger than the actual budget; the difference i s about MGA 28 bi l l ion .In th esecond scenario the difference i s MGA 80 bi l l ion .Due t o the lo w execu tion rateo f he ministry,the differencewith actual expenditure i s mu ch arger.
245.35 315.19 385.0313518 16944 20 196
7.5 1 9.41 11.22
Table 4: Comp arison between actual he alth budget and prcActual2004 2005 2006
Scenario 1Health budget as % o f otal 7.60 5.80 5.90Government budget
Health budget (in billions o f Ariary) 141.96 86.93 164.61Healthbudget per capita/MGA 5779 7955 9094Budget per capita/ US$ 3.09 3.97 4.17Health expenditure per capita/MGA 8554 5082Health expenditure per capita/US$ 4.57 2.53Scenario 2Health budget as % o f total 7.60 5.80 5.90Government budget
ections of th e MTEFMTEF Projections2006 2007 2008
~~ ~~ ~
6.59 6.97 7.35
192.39 235.75 279.1110 600 12 673 14 640
5.89 7.04 8.13
7.50 8.33 9.16
212. The Government i s unlikely to sustain even these l o w levels o f expenditures o n health,m u c h less achieve the expenditure levels o fMTEF, without addit ional f inancial aid from thedonor community. The C R E S A N 2 project wh ich has f inancial ly supportedthe health sectorsince 1999 i s expected to close in December 2007. This project alone increased the funding o fthe ministry by US$40 m illion . F or instance,in 2004 this projec t financed close to31 percent o fa ll M O Hexpenditures classified as investments. This figure rose to 65 percent in 2005. Otherprojects that have also supported the sector are also approaching their clos ing dates, in clu din gthe M ult isectoralSTI/HIV/AIDS Project (US$20 mil l ion) , whichwill also close in December
2007, and the Comm uni ty DevelopmentFund (US$ 176m),w h i c h will be closing o n December2008.
213. Madagascar SHSD P intends t o fill the finan cial gap for the sector,while at the same timelessen some o f he distortions created by the fragmented foreign aid. Cu rrently fore ign support tothe sector i s ma inly orga nized throu gh projects, althoughthe government has also benefited f r o mgeneral budget support from the W o rld Ban k an d th eEU. As mentione d above, the volat i li ty o fdonor funds as well as the complex and different management and monitoring procedures for
78

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 85/103
each proje ct has created large transaction costs fo r the ministry. As seen in Table 5, investmentexpenditure in th e sector has experienced large variations, partlydue to th e vola t i li ty o f donorfunds wh ich financed most o f his expenditureand to a l o w execution rate o f his expenditure.Asin all programmatic approaches, all donors agree not only to support a health strategywith acorresponding MTEF but also to progressively harmonizetheir procedures to followa uniquemonitoring and evaluationsystem. This coordination and harmonization between donors willlessen the volat i l i ty o f donor support andwill decrease the transaction costs o f he ministry as i twou ld no t need to fo llo w different procedures to managedifferent projects.
Table 5: Growth rate of investment expenditure o M OH1998 1999 2000 2001 2002 2003 2004 2005
Yearly change in investment expenditure 65 -3 26 8 -79 396 164 -82Source: Wo rld Bank.PER Health Chapter
111. ECONOMIC ANALYSIS 11: ADDRESSING EFFICIENCY AND EQUITY I N THE HEALT H
SECTOR-JUSTIFICATION F GOVERNMENT NTERVENTION AND EFFICIENCY BENEFITS FROMM A D A G A S C A R HSDP
214. Governmen t interve ntionin some o f the activities financedby Madagascar SHSDP i sjustifiedas they are aimed at reducing market failuresdue t o the presence o f externalities orpub lic goods. In addition, SHSDPwill also finance activities aime d at reducingthe inequalitiesin access and utiliz atio n o f heal th services. Fina lly, some o fhese activitieswill also improveefficiencyin the use o fpublic resources.
Externalities
215. One o f he comm on ustifications for government interventionin markets i s the presence
o f externalities, where ec ono mic agents can impose a cost orbenefit to others without payi ng orcharging for it . Withou t government intervention too mu ch o fthe negative effect o r tool i t t l eo fthe benefit wo u l dbe produced.
216. Infe ctio us diseases, par ticu larl y malaria, arethe maj or causes o f mortal i ty and morbidityin Madagascar, especially among childrenunder five. When preventing or treating an infectiousdisease individua ls do n ot necessarily take in to account the effect o fheir action (or lack thereof)on others. Without government interventionthe l e v e l o f preventive and curative effortswill belower than optimal. Madagascar SHSDP aims precisely at financing many activities aimed atprevention and treatment o f many o f these diseases such as: immun ization for childhoo dillnesses, testing and treatment o f sexually transmitted diseases, etc (see Tables 9-13 below).
Public Goods
217. In addition some o f the interventionsused t o prevent infectious diseases can becharacterized as pu bli c goods. No bo dy canbe excluded from benefit ing fro m a public good and aperson benefiting f rom i t does not decrease the potentialbenefit to others. These characteristicsrender almost impossible the private provisio n o f hese goods.One example o f public goods isvector control, such as indoorand outdoor spraying to co ntrol malaria; another example i sthe
79

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 86/103
collect ion and dissemination o fpubl ic in format ion fo rthe co n t ro l o fdiseases an d the supportivelaboratories to m on itor safedrugs, food, a nd water. S HS DP will finance such activities. In fact,th e entire component 5 o f he p roposed pro ject- wh ich aims at the development o fa mon itoringand evaluation plan, development o fa Nat ional Heal th In format ionSystem, and strengthening o fthe analyt ical capacity o fthe Government fo r mo nitorin g and evaluat ion- ca n be justified bythese same considerations.
120 -
100 -
80 -
60 -
40 -
20 -
0 7
218. Similarly, some information campaigns for activities without an associated marketableproduct will make private provisionvery difficul t ,justifying government intervention. Am on gthe activities financed by Madagascar SHSDP that fi t into that category are campaigns tosensitize fam ilies o n behavior change, and campaigns t o pro mo te and widespreadthe W A S Hstrategy.
10 0 1
, , , , ,0
Equity
219. There are large income inequalities in the uti l izat ion o f heal th servicesin Madagascar,
due part ly to lower physical access to health services in rural isolated areas, and par t ly tofinancia l and cultural barriers t o access services. Governm ent pr ovis ion o f services ca n alsobejustified on the bas is o f equity considerations, and many activities that will be financed byMadagascar SHSD P meet this criterion.
220. In general, a case can be made for the p ro v is io n o fhea lth services that the poo r consumemore than the non-poor, where the income elas t ic i ty o f consumpt ioni s low. People living inrura l isolated areas are m ore likely t o be poor than people living in urba n areas. The p overty ratein urba n areas i s about 52 percent while in rur al areas i s about 74 percent. Therefore, servicestargeted to the latter are mo re likely t o be used by the poor, which i s the case fo r mo bile c linicsfor isolated areas and areas with lo w density o f population, f inancedby SHSDP. In addition,preventive an d treatment services f or infect ious diseases can also benefit the poor more than ther ic h as they are more likely to suffer fromthese diseases. For instance, even though in generalpeople in he upper end o f the income d istr ibutiontend to report more i l lness cases than the non-poor, the last EPM household survey showed that the poor were more likely to rep ort malariaand diarrhea than the non-poor (Table 7). The prov ision o f services to t reat andprevent thesediseases will therefore bene fitthe poor more than the non-poor.
80

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 87/103
Table 7: Type of illness reported in the last tw o weeks across income quin tilesI l lness Poorest I1 I11 Iv Richest Total
Diarrhealdiseases 12,s 14,2 13,l 12 ,l 10,6 12,4Source: EM P 2005
Fever or suspicion o f malaria 46,9 42,9 48,9 41,9 39,9 43,9
22 1. A simila r case can be made fo r the financ ing o f basic health services, especiallyin ruralareas, as these services tend t o be used more by the poor than by the r ic h who visit privateservices or higher l eve l public facilities (Table 8). Madagascar SHSDP will finance therehab ilitation and equipment o f basic h ealth services in all the country, the contracting andredeployment o f nurses and midwives to basic h ealth centers, and efforts to improve maternaland ch ild health. These latter efforts wil l be main ly done through community m obilization toensure that the po or and vulnerable benefit fro mthem.
222.by pub lic service facilities does no t ris k the displacement o f he private sectorin hese areas.
As the private sector i s almost n ot present in rur al areas, im pro vin gthe services prov ide d
Table 8: Place of consultation across income quintiles and u rban a nd ru ra l areasC H * C S B1 CSB 2 Private clinic Private doctor Other Tota l
UrbanPoorest 20.1 18.6 38.8 3.1 3.2 16.2 100.0
I1 14.9 11.3 31.6 5.9 24.3 12.1 100.0
I11 20.4 14.7 25.4 16.3 13.2 10.0 100.0I V 11.2 10.5 29.4 8.1 31.9 8.9 100.0
Rich est 23.3 4.9 20.6 7.5 32.7 11.0 100.0
To tal 19.0 9.5 26.2 8.3 2 6.0 11.0 100.0
Rura lPoorest 5.1 25.5 58.0 0.9 6.2 4. 1 100.0
I1 4.9 19.0 53.9 2.1 7.0 13.0 100.0I11 3.5 12.9 56.9 3 .O 12.6 11.3 100.0
IV 1.2 11.6 66.9 2.1 11.4 6.9 100.0Rich est 5.7 10.0 50.8 3.6 20.4 9.4 100.0
Total 4.0 15.1 57.3 2.5 12.2 9.1 100.0Source: EM P 2005
223. Madagascar SHSDP will also finance activities aimed at identifying andimplementinginnov ative fina ncing strategies to p rovi de consistent quality services a nd to increasethe use o fthese services by the poor, through mechanisms such as mutual insurance or social security.Currently, most private expenditure o n healthi s out-of-pocket expenditure, w h ic h i s extremelyregressive and exposes families to the risk o f impover ishment in case o f illness. O n averagehouseholds spend about 1 percent o f their total expenditure on health. However, not a llhouseholds report expenditures on health in a given year, but for those that do this expenditurecan represent a larger burden. Fo r instance, the average cost o f an outpatient cons ultation (asreported in EPM 2005) was about MGA 6,000 or about 2 percent o f the yearly per capitaexpenditure in the country.
81

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 88/103
82
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 89/103
improvemen ts as the largest percentage was used for bo th preventive and pub lic health servicesand ambulatory care. Howeve r, therei s ro om for improvement, asa fifth o f a l l resources went t othe central administration o fthe ministry and as many resources, a bout 0.5 percent o f he entirebudget o f 2006, went to the construction o fa medical complex in Antananarivo. MadagascarSHSDP project will further improve the allocative eff ic iency o f publicexpenditure as i t will
finance preventive care, public health activities, and- n the case o f hospital care - will onlyfinance f i rs t referral hospitals for activities related to maternal health. More specifically, thefocus o fMadagascar S HSDP i s on the most cost-effective interventions toprevent and treat theillnesses that represent the major burden o f disease in Madagascar by emphasizing healthinterventions that canbe provided by the households and comm unitie s themselves and fo r thosethat can be pro vide d at prim ary he alth care facilities.This is reflected in the project’s emphasison in formation campaigns, strengthening o f commun ity participation o n health care, and o nimpro ving the q uality o f the services pro videdby basic health centers. By improvingcoordination an d harmon ization among donors, MadagascarSHSDP will also improve allocativeeff ic iencyby diminishing transaction costs and thus diminishing administrative costs that M O Hhas when handlingdifferent dono r supported projects.
Iv . ECONOMIC NALYSIS 111: SYSTEMS AND PROCESS-RELATED BENEFITS
227. The benefits o f Madagascar SHSDP can be determined in terms of: (i) ystems- andprocess-related benefits, e.g., better planning, financing, organization and management o fthehea lth sector an d other key actors; and (ii) ousehold-oriented benefits, as exemplifiedby betteraccess and utilization o f health services and imp roved health status, especially o f vulnerablegroups living in rur al areas, wom en and children.
228.improve both hequality o f services and access to the po or:
Hea lth care delivery reforms under PDSS and the activities supportedby SHSDP a im to
Access to good qua lityprim ary care services.A key element o f he PDSS i s strengthening o faccess to basic health services in rural and remote areas, which are services usedpredominantlyby poor, rural populations. Impr oved quality o f care at the prim ary care le ve land improved access will have positive impacts on poverty reduction.The increasedut i liza tion o fquali tyhealth services at the primary acre leveli s expected t o reduce the needfor hospitalization, protect poor householdsagainst financial shocks. The benefits o fincreased primary care funding will go disproportionately tothe poorer households whocurrentlyreceive no or poor quality o fservices.Expansion of coverage for p riori ty program s.Improvements in mother a nd c hil d health,prevention o fthe spread o f HIV/AIDS addressing communicable diseases, etc. have beenidentified as priority areas for coverage expansionunder PDSS. All four are critical healthissues for the poor, and tothis extent the expansion o f services will directlybenefit the poor
by red ucin g barriers t o access to careImprovement in implementation and monitoring capacity.Even if Madagascar SHSDP andthe government health strategy are technically sound and cost effective, the expectedresul tswill not be attained i f the government does not have the capacity to implementthem. MOHhas not been able to execute i t s entire budget in recent years and has had difficultiesinensuring an equal or at least a progressive di strib utio n o f financial an d huma n resourcesacross the country, and therefore no tbeen able t o reach vulnerable and isolated pockets o fhe
83

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 90/103

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 91/103
Annex 10: Safegua rd Po licy Issues
Madag ascar Sustainable He alt h System Developm ent Project
230. The objective o f MadagascarSHSDP i s to strengthen the he alth system and increase it scapacity to providethe necessary production, financing, del ivery and management support f ordelivery o f key services, and as such, will mostly involve activities such as: policyandinstitutio nal reforms; financ ing reforms;strengthening hum an and institution al capacity; supportto p rio rity health programs to con trol m ajo r diseases or t o address health issues;and communityinvolvement in local health service management and support to community-based healthactivities. C iv il works involve dwill be mostly rehabil i tat ion o f exist ing health facil i t ies and theproject will not support acquisi t ion o f and forthe construction o f health facil i ties. N o negativeenvironmental imp acti s envisaged in he proposed program. Thu s the proje ct i s rated as categoryB and only triggers OP 4.01 with regards to arrangements fo r h andling a nd disposal o f medicalwaste. Althoughthe project may finance malaria campaign activities as a lender o f ast resorti fthe Presidential Malaria Initiativei s not able to sufficiently finance the malaria program,Madagascar ra tifiedthe Stockholm conventionin 2005, a nd the Gove rnment does no t pla n touseany DDT in spraying during the Ba nk Project implemen tation period.
231. The handling, collection, disposal and management o f health care waste and otherinfecte d materialsi s the most significant environmenta l issue associatedwith the national healthprogram. The inappropriate h and ling o f nfecte d materials constitutes arisk not only forthe staffin hospitals and in municipalities who are involved in health care waste handling andtransportation, but also for familie s and street children wh o scavenge o ndump sites, most whichare inadequate. To mitigate this risk, a Medica l Waste Management Pl an(MWMP) should beavailable and be a ppropriately costedwith clear ins titutiona l arrangements fo r i ts execution.
232. A MWMPwas developed fo r the Multi-Sectoral H IV /A ID S Prevention Project(MSPP),and i s under implementation. Prior to appraisal o fthe MSPP 11 i t was disclosed in-country andin the Infoshop. The existing MWMP includes prop er disposal o f hazardous bio -med ical wasteand a bio-safety training program fo rthe staff o f all hospital, health centers andcommunity-based programs, including traditional midwifesand practitioners, who maybe involved inHIV/AIDS testing and treatment.
233. Moreover, the Nationa l Policy on Me dica l Waste Management was adoptedin September2005 by an interdepartmental decree N o 2006-680 o f September 12, 2006.This pol icy pr imari lyrelates t o solidwaste with a summary description o n theliquid waste, and contains the fo l lowingelements: (i) lobal and specific objectives as regards management o f m edical waste; (ii) helegal frameworkand law; (iii) aste characteristics with the prescribed elimination modes;(iv)norms, safety standards and measures to be adopted as well as critical equipment; and(v) adescription o fthe monito ring system and an action planwith impa ct and results indicators fo r aperiod o f our years.
234. The Government recent ly modified the plan and policy to include more details o nthemanagement o f iquid waste fr om h ealth facilities.The revised pl an was approved and disclosedon March 23,2007 in the Infoshop and disclosed in-country ove rthe peri od Mar ch 20-26, 2007.
85

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 92/103
Two agencies are responsible, respectively, for: (i) mplementation o f the plan; and (ii)supervision o fhe implementat ion o fhe plan at the provincial anddistrict levels.
235. ImpZementing the plan. M O H has been responsible fo r implementation o fthe MWMP,and has demonstrated capacity to properly implement the plan.Since May 2004, MOH has
installed200 small-scale burners t o burn medical wastes in al l health centers rehabilitatedunderthe C R E SAN I1 Project. Supervision missionsdetermined that burners are being used at theC H D o f Ankazobe, Antanifotsy and Faratsiho.The Plan also includes specific medical wastedisposal and management actions, to be carried out in Madagascar’s different types o f h ea lt hfacilities.M O Hhas demonstrated the abil i ty to pla n for and preparethese activities.
236. Supervising implementation of theplan. The Office forthe Environment o fhe Ministryo f he Environment hasbeen responsible for supervising its impleme ntation atthe provincialanddistrict level. I t has performed this role satisfactorily. Thus the Bor row er has demonstrated thecapacity to properly developand implement a MWMP, which i s the on ly safeguard-related studyrequired for this project.M O Hhas demonstrated clear ownership o f the problems related to
management o f medical waste.I t has been an integral playerin the development o f his pol icy aswell as I E C and trainin g activities conducted at various levels.
86

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 93/103
Annex 11: Project Preparatio n an d Supervision
Madaga scar Sustainable He alt h System Development Project
Planned ActualPCN review 2/12/2007 2/12/2007Initial PID to PIC 211 212007 2/12/2007Initial I S D S to PIC 211 212007 2/15/2007Appraisal 3/22/2007 3/27/2007Negotiations 4/10/2007 4/3/2007BoardKVP approval 5/22/2007Planned date o feffectiveness 8/29/2007Planned date o fmid-term review 913012008Planned closing date 12/31/2009
Key institutions responsible for preparation o fhe project:--
in Government : Ministry o fHeal thand Fam ily Planning, CR ES ANDonor partners included: Africa n Development Bank,AFD , EU, French Cooperation,
JICA, UNIC EF, UNFPA,USAID, W H O
Bank staffand consultants who worked onthe project included:
Name Title UnitMukesh Chawla Lead Economist AFTH3Maryanne SharpMontserrat Meiro-LorenzoAnne-Claire HayeMaria Eugenia Bonilla-ChacinStefan0 PaternostroGervais RakotoarimananaSylvain Rambeloson
Gilles VeuillotWolfgang ChadabT. Jeffrey RaminNorosoa AndrianaivoHerinjara Maria RanohatraPablo GottretPeyvand KhaleghianJulie McLaughlinOscar Picazo
Sr. Operations OfficerSr. Public Health SpecialistConsultantSr. EconomistLead EconomistSr. Financial Management SpecialistSr. Procurement Specialist
Sr. CounselSr. Finance OfficerSr. Operations OfficerProgram AssistantProgram AssistantLead Economist Health & Peer ReviewerSr. Health Specialist & Peer ReviewerLead Health Specialist & Peer ReviewerSr. Economist & Peer Reviewer
AFTH3AFTH3AFTH3AFTH3AFTH3AFTFMAFTPC
LEGAFLOAG2AFTQKAFTH3AFTH3HDNHEECSHDAFTHlAFTHl
Bank funds expended to date on project preparation:1. Ba nk resources: $60, 002. Trust funds: --3. Total: $60,000
Estimated Approv al and Supervision costs:1. Remaining costs to approval: $ 10,0002. Estimated annual supervision cost: $100,000
87
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 94/103
Annex 12: Documents in the Project File
Madagasca r Sustainable He alth System Development Projec t
The fo llow ing documents are availablein the project f i le:
A. Project Documents
Project ConceptNote January 2007Manuel de ProcCdures, CRESAN 2
Appraisal Mis sionAide Memoire,April 2007QualityEnhancement Review Report, M ar ch 2007Identification Missio nAide Mem oire, January 2007
B. He alth Sector Documents
Ministere de l a SantC et du Planning Familia l. 2005.(( Comptes Na tionauxde l a SantC 2003 D.
Madagascar.
Ministere de l a SantC et du Planning Fam ilial . 2005. CadredCpenses a moyen erme du secteursantC 2006-2008. Projetde note technique de prCsentationD. Madagascar.
Institut Nationalde la Statistique (INS TA T)et ORC Macro. 2005.EnquQte DCmographiquee t deSantC de Madagascar 2003-2004. Calberton, M aryland,USA : INSTAT e t ORC Macro.
Institut Nationalde la Statistique (INSTAT) et ORC M acro. 2005.EnquQte DCmographiquee t deSantC de Madagascar, editions o f 1993 and 1997. Calberton, Maryland,USA : INSTAT et ORC
Macro.
Institut Nationalde la Statistique, D irec tiondes Statistiques des Menages. RCpublique deMadagascar. Enquete PCriodique aupresdes mCnages, Rapport Principal. Ed itionsde 2002,2003,2004,2005,2006.
Elaborationdu plan de dCveloppementdes ressources humaines pour l e secteur de la santC aMadagascar, rapport prdliminaire. Ca rl-A rdy Dubo is, Suzanne Boiv in,Lucien Albert. Unit6 desantC internationale, U niversitede MontrCal.M a i2006.
Pub lic Expendituresreview, health sector chapter. The W or ld Bank, February 2007
Poverty and Social Impac t Analysis; He alth careand the Poor. Republic o f Madagascar. TheWor ldBank. June, 2006.
Rapport fonds d’equite au CH D I1 de Marovoay. GTZ. Avril2004.
Feuille de route sur l e s fonds d’CquitC hospitaliers, Madagascar. Ma thie u Noirho mm e.Institut deMCdecine Tropicale, Anvers. 2005.
88

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 95/103
Health Sector Note, Madagascar. The W or ld Bank. M a y 2005.
Annuaire des statistiques de santC, INS TA T, 2003-2004-2005-2006
Carte sanitaire de Madagascar, MinsanPF. 2000.
EnquCte eff icienceet CquitC des Formations Sanitaires, EEFS 1 (2003)
EnquCte efficience et CquitC des FS 2005, EEFS 2, (draft 2006)
MIC S 2000
PC IME communautairea Madagascar (document de bonne pratique, UNIC EF , 2005
Rapport de l’expertise de la fonctionnalitddes CHD, CRES ANMinsanPF , anvier 2004
Rapports techniques des phases 1 et 2 d’appui ii a m i se en oeuvre des plans de diveloppementdes distric ts sanitaires. 2004.
Services d’Cducationet de santC ii Madagascar : ’utilisatione t les ddtenninants de l a Demande,P.Glick, J. Razafindravona,juin 2000
The potential o f comm unity based insurance towards healthfinance in Madagascar, article, B.Minten, M. Over, M. Razakamanantsoa, M a y 2006.
Etude sur l e secteur pharmaceutique, Tahina Andrianjafy, 2004
C. Policy Documents
Politique Nationalede SantC Cjuin 2005)Feuille de route p our l a reductionde la MortalitCMaterne l lea Madagascar, 2005-2015Madagascar, chaine du froid 2004-2013Plan de viabilitC financi2redu programme elargide vaccinationPlan StratCgique National IS TN IH IS ID A, revision 2007-2011Politique Nationale contre la BilharziosePolitique Nationale contrel e Paludisme (2005)Politique Nationalede contractua lisation dans l e secteur de la SantC ii Madagascar (2004)Politique n ationalede gestion des dCchets mCdicaux(SAGS 2005)Politique Nationalede SantC de 1’Enfant (2005)
Politique Nationale Nu triti on (2004)Proposition Mala ria aux rounds 1-2-3-4-5-6du Fonds Mo ndia lPropos ition Tuberculose aux rounds 1-2-3-4-5-6du Fonds Mondia lPropositionVIH aux rounds 1-2-3-4-5-6du Fonds Mo ndia l
89

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 96/103
Annex 13: Statement o f Loans and Credits
Madagascar Sustainable Health System Development Project
Original Amountin US$ Millions
Difference betweenexpected and actualdisbursements
ProjectID FY Purpose BRD ID A SF GEF Cancel. Undisb. Orig. Frm. Rev’d
PO95240
PO74086
PO90615
PO83351
PO74235
PO74236
PO74448
PO82806
PO76245
PO73689
PO72160
PO72987
PO55166
PO51922
PO51741
PO52186
PO01568
2007
2007
2006
2006
2004
2004
2004
2004
2003
2003
2002
2002
2001
2001
2000
1999
1998
MG Pwr/WtrSect. Recovery and Restruct.
MG-Irrigation& Watershed Project (FY07 )
MG-MultiSec STI/HIV/AIDS 2 (FY06)
Integ G rowth Poles
MG-Env Prgm3 (FY04)
MG-GEF Env Prgm3 (FY04)
MG-Gov& Inst Dev TA L (FY04)
MG-Transp In frastr Invest Prj (FY04)
MG-M ineral Res GovSIL (FY03)
MG-R ural TranspAPL 2 (FY03)
MG -Priv Sec Dev 2 (FY02)
MG-MultiSec STI/HIV/AIDS Prev APL(FY02)
MG-Com Dev FundSIL (FYO1)
MG-R ural Dev SuptSIL (FYOl)
MG-HealthSec Prgm Supt 2 (FYOO)
MG-Microfinance (FY99)
MG-Comm unity Nutrition 2 (FY98)
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
10.00
30.00
30.00
129.80
0.00
0.00
30.00
150.00
32.00
80.00
23.80
20.00
110.00
89.05
40.00
16.40
27.60
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
9.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
0.00 0.00
10.06
30.39
28.21
105.17
23.46
5.27
11.36
85.25
9.06
34.61
7.40
2.95
26.99
21.57
3.98
1.02
11.20
0.00 0.00
0.54 0.00
8.42 0.00
5.25 0.00
6.22 0.00
4.67 0.00
1.96 0.00
55.09 33.80
-4.67 0.00
3.78 -6.31
3.13 -1.46
0.07 0.00
-59.28 -4.28
3.82 -1.42
-15.02 1.77
0.33 0.53
-9.68 0.00
Total: 0.00 818.65 0.00 9.00 0.00 417.95 4.63 22.63
90

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 97/103
M A D A G A S C A RSTATEMENT OF IFC’s
Held and Disbursed PortfolioIn Mill ionso fU S Dollars
Committed Disbursed
IF C
FY Approval Company Loan Equity Quasi
1997 AEF GH M 0.46 0.00 0.00
1995 AEF Kari bote l 0.19 0.00 0.00
BFV-SocGen 6.37 0.00 0.00
1991 BNI 0.00 2.09 0.00
2005 B N I 6.37 0.00 0.00
2000 BOA-M 0.00 0.82 0.72
2004 BP Madagascar 0.00 3.51 0.00
CREDIT LYON NAIS 1 6.37 0.00 0.00
Partic.
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
I FC
Loan Equity Quasi
0.46 0.00 0.00
0.19 0.00 0.00
0.00 0.00 0.00
0.00 2.09 0.00
0.00 0.00 0.00
0.00 0.82 0.72
0.00 0.00 0.00
0.00 0.00 0.00
Partic.
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
Tota l portfolio: 19.76 6.42 0.72 0.00 0.65 2.91 0.72 0.00
Approvals Pending Commitment
FY Approval Company Loan Equity Quasi Partic.
2001 Besalampy 0.02 0.00 0.00 0.00
2006 IDA -IFC PCG 0.01 0.00 0.00 0.00
Total pending commitment: 0.03 0.00 0.00 0.00
91
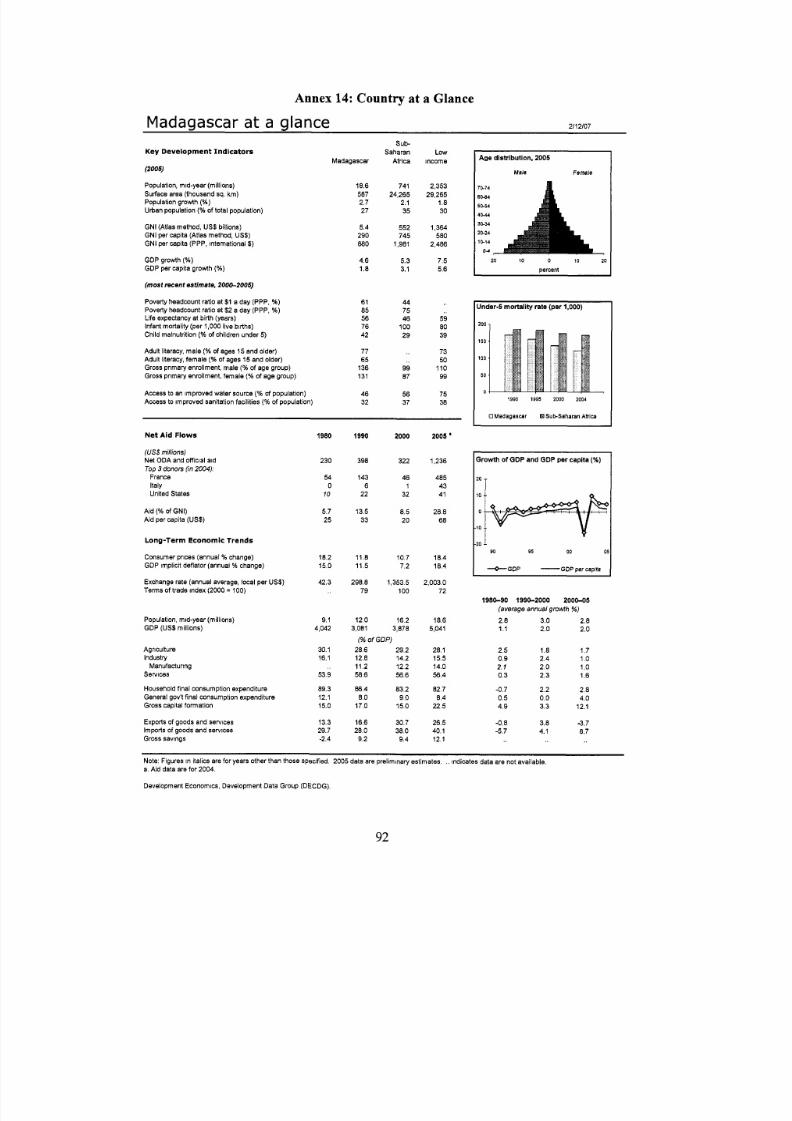
8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 98/103
Annex 14: Country at a Glance
Madagascar a t a glance 2/12/07
K e y D e v e l o p m e n t I n d i c a t o r s
(2005)Population, m d-year (millions)Surface area (thousand sq. km )Population growth(%)Urban population(W of total population)
GNI (Atlas method, US$ billions)GNI per capita (Atlas method, US$)GNI per capita (PPP, international$)
GDP growth(% )GDP per capita growth( 5 6 )
(most rec ent estimate, 200&2005)
Poverty headwunt ratio at$1 a day (PPP, %)Poverty headcount ratio at$2 a day (PPP, %)Life expectancy at birth (years)Infant mortality (per1,000 ive births)Child malnutrition(% of children under5)
Adult literacy, male(56 of ages 15 and older)Adult literacy, female(% of ages 15 and older)Gross pnmaryenrollment, male(% of age group)Gross primary enrollment, female(5 6 of age group)
Access to an improve d water source(% of population)Access to improved sanitation facilities(% of population)
Madagascar
18.85872.727
5.4290880
4.61.8
6185567642
7765
136131
4632
sub-Saharan
Africa
74124,265
2.135
552745
1,981
5.33.1
447546
10029
9987
5637
LOWincome
2,35329,265
1.830
1,364580
2,486
7.55.6
598039
7350
11099
7538
N e t A i d Flows
(US$ millions)Net ODA and o fficial aidTop 3 donors (in 2004):
FranceItalyUnited States
Aid (% of GNI)
Aid per capita (US$)
L o n g - Te r m E c o n o m l c Tr e n d s
Consumer prices (annual% change)GDP implicit deflator (annualO change)
Exchange rate (annual average, local per US$ )Terms of trade index(2000 = 100)
Population, mid-year (millions)GDP (US$ millions)
AgricultureIndustry
services
Household inal consumption expenditureGeneral gov't final consu mption expenditureGross capital formation
Exports of goods and sewicesImports of goods and servicesGross savings
Manufacturing
1980
230
540
10
5.7
25
18.215.0
42.3
9.14,042
30.116.1
53.9
89.312.115.0
13.329.7-2.4
1990
398
1436
22
13.5
33
11.811.5
298.879
12.03,081
2000
322
481
32
8.5
20
10.77.2
1,353.5100
16.23,878
(% of GDP)28.6 29.212.8 14.211.2 12.258.6 56.6
86.4 83.28.0 9.0
17.0 15.0
16.6 30.728.0 38.0
9.2 9.4
2005 '
1,236
4854341
28.8
68
18.418.4
2,003.072
18.65,041
28.115.514.056.4
82.78.4
22.5
26.540.112.1
Age dis t ribut ion,2005
Male Female
70-74
60-84
50-54
4 0 4 4
30-34
20-24
10-14
0-4
20 10 0 10 20
percent
Und er4 mortal i ty rate (per1,000)
200 1
150
100
50
01990 1995 2000 2004
UMadagascar HSubSaharanAhica
Zrowthof GD P an d GDP per capita (%)
m T
90 95 00 O!
--O-GDP-
DP per capita
1980-90 1990-2000 2000-05(average annual growth %)
2.8 3.0 2.81.1 2.0 2.0
2.5 1.8 1.70.9 2.4 1 o2.1 2.0 1 o0.3 2.3 1.6
-0.7 2.2 2.80.5 0.0 4.04.9 3.3 12.1
-0.8 3.8 3 . 7-5.7 4.1 8.7
Note: Figures in italics are for years other than those Specified.2005 data are preliminary estimates. ,, indicates data ere not available.a. Aid data ere for2004.
Development Economics, Development Data Group (DECDG).
92

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 99/103
P Madagascar
Balance of Payments and Trade
(US$millions)
Total merchandise exports (fob)Total merchandise mports (cif)Net trade in goods and services
Workers' remittances andcompensation of employees (receipts)
Current account balanceas a % of GDP
Reserves, including gold
Central Government Flnance
(% of GDP)Revenue
Expense
Cash surplus/deficit
Highest marginal tax rate(36)
Tax revenue
IndividualCorporate
External Debt and Resource Flows
(US$ millions)Total debt outstanding and disbursedTotal debt serviceHlPC and M DRl debt relief (expected; flow)
Total debt (% of GDP)Total debt service(% of exports)
Foreign direct investment (net inflows)Portfolio equity (net inflows)
2000
8291,097-283
11
-218-5.6
288
11.711.315.9
-3.5
3535
4,691117
1,900
121.09.7
700
2005
8371,6526 8 8
16
-524-10.4
498
10.910.121.3
-8.9
3030
3,46578
68.75.7
86
Composi t ionof total external debt, 2005
pnvde Shon-term, 75
US$ millions
Private Sector Development 2000 2006
Time requ ired to start a business (days) - 21
Time requ ired to register property (days) - 134Cost to start a business (% of GNi per capita) - 35.0
Ranked as a major constraint to business(% of managers surveyed who agreed)
Cost of financing .. 66.9Macroeconomic nstability .. 64.4
Stock market capitalization(5 6 of GDP)Bank branches (per 100,000 people) .. 0.7
IGovernance indicators ,ZOO0an d 2005
Voice and accountability
Politicalstability
Regulatory quality
Ruleof law
Controlof corruption r2005 Country's percentile rank(0-100)0 2 0 0 0 kghw vduet mphl h U c r ntmngr
Technology and Infrastructure
Paved roads (% of total)Fixed line and mobile phone
High technology exportssubscribers (per 1,000 people)
(% of manufactured exports)
Environment
Agncultural land(U of land area)Forest area (% of land area, 2000 and 2005)Nationally protected areas(% of land area)
Freshwater resources per capita (cu. meters)Freshwater withdrawal(% of internal resources)
C 0 2 emissions per capita (mt)
GDP per unit of energy use(2000 PPP $ per kg of oil equivalent)
Energy use per capita (kg of oil equivalent)
2000 2004
11.6
7 19
1.0 0.8
47 4722.4 22.1
.. 4.3
,, 18,606.. 4.4
0.14 0.13
(US$miliions)
IBRDTotal debt outstanding and disbursed 0 -Principal repayments 0 -Interest payments 0 -Disbursements 0 -
IDATotal debt outstanding and disbursed 1.378 2,298Disbursements 94 221Total debt service 27 29
IFC (fiscai year)Total disbursed and O utstanding portfolio 8 6
of which IFC own account 8 6Disbursements for IFC own account I 0
Portfolio sales, prepayments andrepayments for IFC own account 2 1
1 1MlGA
Gross exposure0 0
Note: Figures n italics are for years other than those specified.2005 data are preliminary estimates.. indicates data are not available. -indicates observation is not applicable.
Development Economics, Development Data Group (DECDG).
2/12/07
93

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 100/103

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 101/103
Annex 15: M a p IBRD 33439
Madag ascar Sustainable He alt h System Development Proje ct
95

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 102/103

8/4/2019 Madagascar: Sustainable Health System Development Project (World Bank - 2007)
http://slidepdf.com/reader/full/madagascar-sustainable-health-system-development-project-world-bank-2007 103/103
A n k
a r a t a
Massif ass i fT saratananaa r a t a n a n a
C l i f f
o f
A n g a v o
C l i
f f o f
B o n g
o l a v a
Maromokotro aromokotro(2,876 m)2,876 m)
T siafajovonaiafajovona(2,642 m)2,642 m)
M a n a m b a h o
M a h a v a v y
B e t s i b o k
a
M a h
a j a m b a a
B e m a r i v o
S o f i a
Lake akeAlaotralaotra
M a n g o r o
M a n i a
T s i r i b i h i n a
F I A N A R A N T S O AI A N A R A N T S O A
M A H A J A N G AA H A J A N G A
A N T N TANANARIVO N A N A R I V O T O A M
A S I N
A
ANTSIRANANANTSIRANANA
Manjaanja
Mandabeandabe
Berorohaeroroha
Ambohimahasoambohimahasoa
Moramangaoramanga
Antanifotsyntanifotsy
Ambositrambostra
Ambatofinan-mbatofinan-drahanarahana
Antsirabentsrabe
Miandrivazoiandrivazo
Malaimbandyalaimbandy
Vohidialahidiala
Andilamenandilamena
Andriamenandriamena
Maevatananaaevatanana
Kandrehoandreho
Ankazobenkazobe
Soavinandrianaoavinandriana
Ambaravaranalambaravaranala
Ambilobembilobe
Andapandapa
MandritsaraandritsaraMampikonyampikony
Befandrianaefandriana
Bealananaealanana
Fianarantsoaanarantsoa
ANTNTANANARIVONANARIVO
F I A N A R A N T S O A
M A H A J A N G A
AN TAN AN ARIVO T O A M
AS
INA
ANTSIRANANA
Vatomandry
Mahanoro
Varika
MananjaryManja
Mandabe
MorombeBeroroha
Ambohimahasoa
Antalaha
Maroantsetra
Mananara
Fenoarivo-Atsinanana
Moramanga
Antanifotsy
Ambositra
Ambatofinan-drahana
Antsirabe
Miandrivazo
Malaimbandy
Belo Tsiribihi na
Morondava
Vohidiala
Andilamena Soanierana-Ivongo
Andriamena
Maevatanana
Soalala
Besalampy
Maintirano
Antsalova
Kandreho
Ankazobe
Soavinandriana
Ambaravaranala
Sambava
VohimarinaAmbilobe
Andapa
MandritsaraMampikony
Befandriana
BealananaAntsohihy
Ambanja
Toamasina
Antsiranana
Mahajanga
Fianarantsoa
ANTANANARIVO
Mayotte (France)
M a n a m b a h o
M a h a v a v y
B e t s i b o k
a
M a h
a j a m b a
B e m a r i v o
S o f i a
Lake Alaotra
M a n g o r o
M a n i a
T s i r i b i h i n a
I N D I A N
O C E A N
Mo z a m
b i q ue
Ch a n n e l
An
k a r a t a
Massif Tsarat ana na
C l
iff
o f
A n g a v o
C l i
ff o f
B o n g
o l a v a
Maromokotro (2,876 m)
Tsiafaj ovona(2,642 m)
45 ° E 50 ° E
20°
S
15 ° S
20°
S
15 ° S
M ADAGASCAR
0 40 80 120 160 200 Kilometers
IBRD 33439