magnetic resonance imaging findings associated with...
TRANSCRIPT
1005
Magnetic Resonance Imaging FindingsAssociated With Cardiac Arrest
Risto 0. Roine, MD; Raili Raininko, MD; Timo Erkinjuntti, MD;Ari Ylikoski, MD; Markku Kaste, MD
Background and Purpose: The frequency and prognostic significance of neuroradiological findings aftercardiac arrest are unknown. Using healthy volunteers as control subjects, we studied the magneticresonance imaging (MRI) findings associated with cardiac arrest, adjusted for confounding factors.Methods: The presence of cerebral infarcts, leukoaraiosis, atrophy, and edema on ultra-low-field MRI
was assessed in 88 community volunteers and 52 cardiac arrest survivors enrolled in a placebo-controlled,randomized, double-blind trial of nimodipine in out-of-hospital ventricular fibrillation.
Results: Cardiac arrest was an independent risk factor for the presence of infarcts in a logisticregression model adjusted for age, sex, and history of myocardial infarction, stroke, coronary heartdisease, cardiac failure, and hypertension (odds ratio, 3.6; 95% confidence interval, 1.3 to 9.9; P=.01).Leukoaraiosis was associated with increasing age but not with cardiac arrest. Adjusted for age, the delayof advanced life support had an inverse correlation with the degree of atrophy in placebo-treated patients(r= -.62, P<.0001) but not in patients treated with nimodipine (r= -.10, P=.43). Lack of age-relatedatrophy, possibly implicating the presence of brain edema, predicted poor outcome after cardiac arrest(odds ratio, 4.6; 95% confidence interval, 1.4 to 15.8; P=.01).
Conclusions: Cardiac arrest was associated with deep cerebral infarcts but not with leukoaraiosis. MRIfindings did not predict the functional outcome at 1 year. Nimodipine treatment had no significant effecton the MRI findings, but delayed resuscitation was associated with probable brain edema only inplacebo-treated patients. (Stroke 1993;24:1005-1014)KEY WoRDs * cerebral infarction * heart arrest * magnetic resonance imaging * nimodipine
C ardiac arrest (CA) followed by resuscitation is acombination of complete and incompleteglobal ischemia. As spontaneous circulation
has been restored, multifocal hypoperfusion syndromemay result, depending on the severity and duration ofischemia as well as other hemodynamic factors.1-5 It isnot known whether multifocal hypoperfusion can leadto completed infarction. Only a few neuroimaging stud-ies have addressed either functional or structural as-pects of human CA, and no controlled magnetic reso-nance imaging (MRI) studies have been published.3-8
Cerebral hypoperfusion of cardiac origin, especiallyin association with hypotension caused by cardiac fail-ure or by arrhythmias, has been suggested as one of theunderlying mechanisms of leukoaraiosis.9-1" Therefore,both watershed infarcts and leukoaraiosis might beexpected to result from CA and resuscitation. To deter-mine whether the victims of CA would have morecerebral infarcts, leukoaraiosis, or other pathologicalfindings on MRI than would control subjects, we carriedout a comparative study on survivors of out-of-hospitalventricular fibrillation and a group of healthy commu-
Received December 17, 1992; final revision received February 8,1993; accepted February 25, 1993.From the Departments of Neurology (R.O.R., T.E., A.Y., M.K.)
and Radiology (R.R.), University of Helsinki, Finland.Correspondence and reprint requests to Department of Neurol-
ogy, University of Helsinki, SF-00290 Helsinki, Finland (DrRoine).
nity volunteers matched by age and sex. Our second aimwas to assess the prognostic significance of the MRIfindings after CA and to assess the effects of nimodipineon MRI in a placebo-controlled clinical trial, the resultsof which have been previously published.12 Since theresults of a subgroup analysis performed post hoc hadsuggested that the possible effect of nimodipine mightbe related to the delay of resuscitation, we also wantedto examine the relation between MRI findings, delay ofadvanced life support, and nimodipine treatment.
Subjects and MethodsSubjectsThe present study included fifty-nine survivors out of
155 CA patients enrolled in a placebo-controlled, ran-domized clinical trial studying the effect of nimodipineon the outcome of patients resuscitated from out-of-hospital ventricular fibrillation by a physician-mannedadvanced life support unit. The complete study designhas been reported earlier.'2 Between January 1, 1986,and June 30, 1988, there were 677 out-of-hospitalresuscitation attempts, and 210 patients had ventricularfibrillation as the presenting rhythm. Of these 210patients, the spontaneous circulation could be restoredand the entry criteria met for 155 (74%) of the patients,who were randomly assigned to receive either nimod-ipine or placebo in a randomized, double-blind fashion.The dosage was 10 ,ug/kg body weight as an intravenous
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1006 Stroke Vol 24, No 7 July 1993
injection immediately after restoration of spontaneouscirculation, followed by an infusion of 0.5 ,g/kg perminute for 24 hours. The study treatment was alwaysstarted at the site of the resuscitation outside thehospital. The delays of basic life support and advancedlife support (defined as the time from the estimated CAtime to the start of resuscitation by the ambulancepersonnel or by the physician-manned unit, respec-tively) and additional features of CA and resuscitationas well as medical history were obtained for all CApatients (Table 2). Blood pressure was carefully con-trolled during the treatment. Systolic blood pressurebelow 80 mm Hg any time during the first day afterresuscitation was considered to indicate hypotension.The Mini-Mental State Examination (MMSE) was per-formed at 1 week and 1 year for all surviving patients.13The results of the detailed neuropsychological examina-tion and MMSE have been previously reported.14Of the 155 enrolled patients, MRI could be per-
formed in 59 of 107 patients (55%) that survived for atleast 2 weeks. Of the 59 scans, 52 could be completedand were legible for the analysis. Seven patients weretoo restless or their medical condition was too unstableto allow completed imaging. Of the 52 patients whounderwent MRI, 28 were treated with nimodipine and24 received placebo. The most common reasons for lackof MRI scan were unstable medical condition anddifficulties in providing adequate intensive care duringimaging; the presence of an implanted cardiac pace-maker, which is an absolute contraindication for MRI;and the refusal of the patient to enter the MRI scanner.The 1-year outcome of CA patients was assessed by
careful neurological examination, MMSE score anddetailed neuropsychological examination, and by ques-tioning close relatives. The Glasgow Outcome Score ofthe patients was dichotomized into good (good recoveryor moderate disability) or poor (severe disability, veg-etative state, or death) outcome.15
Eighty-eight control subjects were selected from arandom cohort of normal aged community volunteersincluded in the Helsinki Aging Study to create a controlgroup of equal age and sex. A detailed neurologicalexamination, including MMSE, was performed in thecontrol subjects before MRI. The histories of hyperten-sion, coronary heart disease, previous myocardial in-farction, cardiac failure, diabetes, and previous resusci-tation were obtained for CA patients and controlsubjects using all available medical records. An oralinformed consent was obtained from all control sub-jects, and a deferred oral consent was obtained fromresuscitated patients or their relatives.16 The study wasapproved by the Ethical Committee of the UniversityCentral Hospital of Helsinki and the University ofHelsinki.
Magnetic Resonance ImagingThe magnetic resonance imaging was performed with
an ultra-low-field magnetic resonance imager (Acut-scan. Instrumentarium Corporation, Helsinki, Finland)operating at 0.02 T. Axial T2-weighted spin-echo im-ages (repetition time/echo time, 2000/150 or 2300/120,with three averages) were obtained in each examina-tion. Additional pulse sequences and sagittal or coronalslices were used in selected cases. The slice thickness
was 10 mm, and there were no gaps between the slices.The field of view was 30 cm and the matrix size 128 x256pixels. Contrast enhancement was not used.The MRI scans were performed an average of 12±8
(mean±SD; range, 1 to 47) days after CA. At the timeof imaging, twelve patients were still comatose; all buteight patients ultimately regained consciousness. Coma-tose patients as well as those with respiratory problemswere ventilated by hand during the imaging process.The MRI scans were reviewed by a neuroradiologist
(R.R.) blinded to the clinical data. Leukoaraiosis wasdefined as diffuse or patchy areas of increased signalintensity in T2-weighted images. Leukoaraiosis wasseparately evaluated in frontal, parietal, and occipitallobes, including both periventricular and deep whitematter as well as subcortical areas. The changes werevisually graded as mild (if less than one quarter of thewhite matter was affected), moderate (if one quarter toone half was affected), and severe (if more than one halfof the white matter had increased signal intensity inT2-weighted images). Infarcts were recorded by num-ber, size, and arterial territory and were classified asdeep or cortical. Infarcts located in border zone areas ofarterial territories, either in cortical or deep regions,were considered watershed infarcts. Wedge-shaped pe-ripheral lesions and well-defined, small, round or ovalhyperintensities in the basal ganglia, thalami, or deepwhite matter were considered infarcts. Because thedifferentiation of infarcts from other lesions was basedmainly on the form of the lesions, the differentiationbetween infarcts and leukoaraiosis was arbitrary insome cases; therefore, the presence or absence of anywhite matter hyperintensities was also assessed.
Cortical, central, and posterior fossa atrophy wereeach rated as absent, mild, moderate, or severe, consid-ering both sides of the brain simultaneously. Except forthe most severe cases, generalized brain edema isdifficult to diagnose by radiological means, but dimin-ished size of subarachnoidal spaces and cerebral ventri-cles may signal its presence. Thus, cerebral atrophy onMRI indicates lack of concurrent edema, whereas thefinding of missing cortical, central, and posterior fossaatrophy may represent generalized brain edema. Here-after, the term "probable edema" is therefore used todescribe the patients in whom generally reduced cere-brospinal fluid spaces are demonstrated by MRI.The MRI scans of CA patients and control subjects
were compared to clarify the frequency of pathologicalfindings after CA and to identify the findings associatedwith CA. The impact of important prognostic factors ofout-of-hospital cardiac arrest (namely, the delay ofadvanced life support and hypotension) was assessed inCA patients.17 The MRI findings were correlated with1-year functional outcome of resuscitation to identifythe findings with prognostic value. Finally, the results ofMRI in CA patients treated with nimodipine or placebowere compared.
Statistical MethodsThe homogeneity of CA and control patient groups
regarding demographic data, and the homogeneity ofnimodipine- or placebo-treated patient groups for themain characteristics of CA and resuscitation, outcome,and demographic data were tested using Fisher's Exact
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Roine et al MRI After Cardiac Arrest 1007
TABLE 1. Demographic Features of Cardiac Arrest Patients and Control Subjects
Cardiac arrest Control subjectsVariable (n=52) (n=88) P
Age (years; mean+SD) 65+11 65±7 .92Range (36-85) (55-76)
MMSE score (mean±SD) 21±12 28±2 <.0001Range (0-30) (21-30)
Males 36 (69) 48 (55) .12
Hypertension 13 (25) 24 (27) .93Coronary disease 27 (52) 18 (21) .0003
Myocardial infarction 18 (35) 5 (6) <.0001Cardiac failure 25 (48) 4 (5) <.0001Resuscitation 5 (10) 0 (0) .013
Diabetes 3 (6) 5 (6) 1.00
Stroke 5 (10) 2 (3) .13
n, Number of patients or control subjects; MMSE, Mini-Mental State Examination (scale 0 to 30).Values in parentheses are percent. Probability values indicate the significance level of Student's t test
for age and of Fisher's Exact Test for all other variables.
Test or Student's t test. The frequencies of individualMRI findings in each group are given as percentageswith probability values of Fisher's Exact Test. Oddsratios (ORs) with 95% confidence intervals (CIs) werecalculated for CA and other risk factors for the MRIfindings, first in univariate models and subsequently inmultivariate models. The effect of confounding factorsunevenly distributed in CA and control groups wascontrolled by logistic regression analysis, which wasused to identify parameters associated with the pres-ence of different MRI findings, adjusted for all otherrisk factors in the model. Nonparametric correlationswere calculated using Spearman's correlation coeffi-cient, Kendall's rank correlation coefficient, or Ken-dall's partial rank correlation coefficient. The differenceof two nonparametric correlation coefficients was testedusing Fisher's z transformation.18 The two-sided a<.05was considered statistically significant in all compari-sons. The statistical analyses were performed usingBMDP statistical software19 and a personal computer.
ResultsThe 52 CA patients did not differ from the 88 normal
control subjects with respect to age and sex; however, ahistory of coronary heart disease, myocardial infarction,cardiac failure, or resuscitation was much more com-mon than in the control group (Table 1).
Forty-four of 52 patients (85%) recovered conscious-ness (Table 2). Thirty-three patients (63%) survived forat least 1 year. Twenty-three patients (44%) reachedthe best Glasgow Outcome category, five (10%) hadmoderate disability, and five (10%) were severely dis-abled. Nineteen (37%) patients died during the 1-yearfollow-up, eleven (58%) due to anoxic encephalopathy.Thus, 24 patients (46%) had a poor outcome (defined asdeath by 1 year or severe disability) compared with 28patients (54%) with good outcome (defined as good ormoderate recovery). The outcome of the 52 studiedpatients was somewhat better than that of all the 155enrolled patients, of whom 100 (65%) recovered con-sciousness (P=.008), 59 (38%) survived for at least 1year (P=.003), and 50 (32%) had a good outcome
(P=.01). Of the 96 patients who died during follow-up,death was related to anoxic encephalopathy in 50 cases(52%). The demographic data and the characteristics ofcardiac arrest were similar in patients studied by MRIand in all 155 patients.12 The patients studied by MRIthus represented fairly well the victims of out-of-hospi-tal ventricular fibrillation enrolled in the randomizedtrial.The CA patient groups receiving either nimodipine or
placebo did not differ in gender or history of mainvascular disorders, but the patients treated with nimod-ipine were slightly younger (P=.06, Table 2). The delaysof basic and advanced life support, the duration ofcoma, and the rate of recovery of consciousness wereequal in both treatment groups.
Cerebral InfarctsCerebral infarcts demonstrated by MRI were more
common after CA than in normal control subjects(Table 3 and Fig 1), but the difference was significantonly for deep infarcts (P=.0007). The number of in-farcts was increased as well (P=.0001), and 8 of 52patients (15%) had multiple infarcts compared with 3 of88 controls (3%) (P=.03).CA was a univariate risk factor for the presence of
cerebral infarcts (OR, 4.6; 95% CI, 2.0 to 10.3; P=.0003)and for the presence of any white matter hyperintensities(OR, 2.4; 95% CI, 1.2 to 4.8; P=.02) but not for leuko-araiosis (OR, 1.2; 95% CI, 0.5 to 2.5) or atrophy (OR, 1.2;95% CI, 0.6 to 2.3).
In multivariate logistic regression analysis, CA was anindependent risk factor (OR, 3.6; 95% CI, 1.3 to 9.9;P=.01) for the presence of infarcts, adjusted for theeffects of age, sex, and previous myocardial infarction,stroke, coronary heart disease, cardiac failure, andhypertension. Age was another independent risk factor(OR, 1.08; 95% CI, 1.02 to 1.13; P=.006), whereashypertension (OR, 1.0; 95% CI, 0.4 to 2.7; P=.95) andhistory of stroke (OR, 3.1; 95% CI, 0.5 to 17.2; P=.21)were not. CA was an especially important risk factor fordeep infarcts (OR, 16.7; 95% CI, 2.6 to 108; P=.0001)when controlled for the factors above. CA was also an
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from
1008 Stroke Vol 24, No 7 July 1993
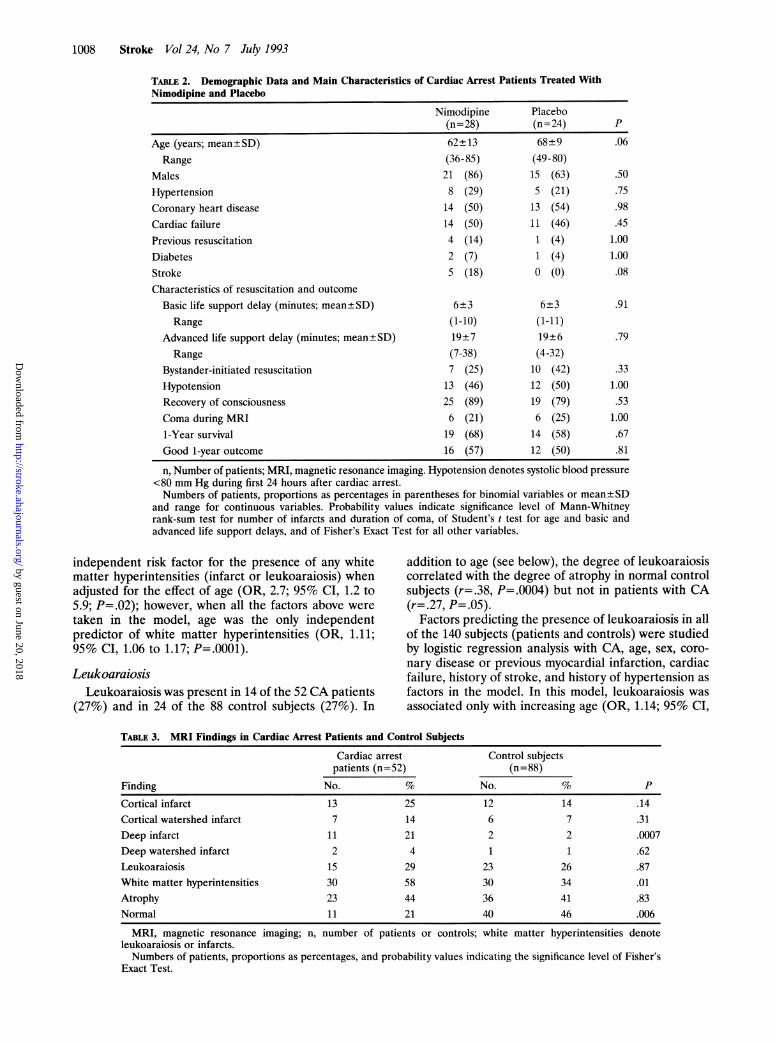
TABLE 2. Demographic Data and Main Characteristics of Cardiac Arrest Patients Treated WithNimodipine and Placebo
Nimodipine Placebo(n=28) (n=24) P
Age (years; mean+SD) 62+13 68+9 .06Range (36-85) (49-80)
Males 21 (86) 15 (63) .50Hypertension 8 (29) 5 (21) .75Coronary heart disease 14 (50) 13 (54) .98
Cardiac failure 14 (50) 11 (46) .45Previous resuscitation 4 (14) 1 (4) 1.00
Diabetes 2 (7) 1 (4) 1.00Stroke 5 (18) 0 (0) .08
Characteristics of resuscitation and outcome
Basic life support delay (minutes; mean±SD) 6+3 6±3 .91
Range (1-10) (1-11)Advanced life support delay (minutes; mean±SD) 19±7 19±6 .79
Range (7-38) (4-32)Bystander-initiated resuscitation 7 (25) 10 (42) .33Hypotension 13 (46) 12 (50) 1.00
Recovery of consciousness 25 (89) 19 (79) .53Coma during MRI 6 (21) 6 (25) 1.00
1-Year survival 19 (68) 14 (58) .67
Good 1-year outcome 16 (57) 12 (50) .81
n, Number of patients; MRI, magnetic resonance imaging. Hypotension denotes systolic blood pressure<80 mm Hg during first 24 hours after cardiac arrest.Numbers of patients, proportions as percentages in parentheses for binomial variables or mean±SD
and range for continuous variables. Probability values indicate significance level of Mann-Whitneyrank-sum test for number of infarcts and duration of coma, of Student's t test for age and basic andadvanced life support delays, and of Fisher's Exact Test for all other variables.
independent risk factor for the presence of any whitematter hyperintensities (infarct or leukoaraiosis) whenadjusted for the effect of age (OR, 2.7; 95% CI, 1.2 to5.9; P=.02); however, when all the factors above were
taken in the model, age was the only independentpredictor of white matter hyperintensities (OR, 1.11;95% CI, 1.06 to 1.17; P=.0001).
LeukoaraiosisLeukoaraiosis was present in 14 of the 52 CA patients
(27%) and in 24 of the 88 control subjects (27%). In
addition to age (see below), the degree of leukoaraiosiscorrelated with the degree of atrophy in normal controlsubjects (r=.38, P=.0004) but not in patients with CA(r=.27, P=.05).
Factors predicting the presence of leukoaraiosis in allof the 140 subjects (patients and controls) were studiedby logistic regression analysis with CA, age, sex, coro-
nary disease or previous myocardial infarction, cardiacfailure, history of stroke, and history of hypertension as
factors in the model. In this model, leukoaraiosis was
associated only with increasing age (OR, 1.14; 95% CI,
TABLE 3. MRI Findings in Cardiac Arrest Patients and Control Subjects
Cardiac arrest Control subjectspatients (n=52) (n=88)
Finding No. % No. % P
Cortical infarct 13 25 12 14 .14Cortical watershed infarct 7 14 6 7 .31Deep infarct 11 21 2 2 .0007Deep watershed infarct 2 4 1 1 .62Leukoaraiosis 15 29 23 26 .87White matter hyperintensities 30 58 30 34 .01Atrophy 23 44 36 41 .83Normal 11 21 40 46 .006
MRI, magnetic resonance imaging; n, number of patients or controls; white matter hyperintensities denoteleukoaraiosis or infarcts.Numbers of patients, proportions as percentages, and probability values indicating the significance level of Fisher's
Exact Test.
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Roine et al MRI After Cardiac Arrest 1009
Cerebral infarcts on MRI
- _ 4
0- -e
A/
/
\4 /
0C
0
:5
p
- -l
45 50 55 60 65 70 75 80 85
Age, yearsFIG 1. Proportion (percentage) of patients with cerebralinfarcts demonstrated by magnetic resonance imaging (MRI)in different age groups by 5-year intervals in 88 normalcontrol subjects and 52 cardiac arrest patients.
100 -
90 -
80 -
70 -
60 -
50 -
40 -
30 -
20 -
10 -
0 -
Leuko-araiosis on MRI
Arrest a ----.
Control G---
0_-Sew
---l
45 50 55 60 65 70 75 80 85
Age, yearsFIG 2. Proportion (percentage) ofpatients with leukoaraio-sis demonstrated by magnetic resonance imaging (MRI) indifferent age groups by 5-year intervals in 88 normal controlsubjects and 52 cardiac arrest patients.
1.07 to 1.21; P=.0001), whereas hypertension (OR, 1.4;95% CI, 0.5 to 3.8; P=.51) and history of stroke (OR,2.1; 95% CI, 0.3 to 14.4; P=.48) were not significant riskfactors for leukoaraiosis.White matter hyperintensities were more common in
the CA group of patients than in healthy control sub-jects (P=.01, Table 3). The frequency of white matterhyperintensities increased in parallel with increasingage in both the CA patients (r=.96, P=.0005) andcontrol subjects (r=.94, P=.01).
Effects ofAgeIncreasing age correlated with the frequency of in-
farcts in the CA group of patients (r=.86, P=.01; Fig 1).Infarcts were rare in the control group, and only thefrequency of deep infarcts had a significant correlationwith age (r=.89, P=.04). A normal MRI was seen in 46%of control subjects but in only 21% of CA patients(P=.006). In subjects younger than 65 years, MRI wasnormal in 48% compared with 23% in those 65 or older(P=.004). The frequency of atrophy increased with ad-vancing age in CA patients (r=.77, P=.04) and normalcontrol subjects (r=.75, P=.14). In healthy control sub-jects, age correlated with the frequency (r=.96, P=.01)and degree of central atrophy (r=.33, P=.0004), but thiswas not the case in CA patients (r=.68, P=.09 and r=.22,P=.11, respectively). Nevertheless, the frequency of at-rophy was the same in both groups (Table 3).
In CA patients, age correlated with the frequency(r=.91, P=.004) and degree of leukoaraiosis, especiallyin the frontal (r=.50, P=.0004) and temporoparietalareas (r=.34, P=.01). In control subjects, age had a
similar correlation with the frequency (r=.89, P=.05)and degree of leukoaraiosis, especially in the temporo-parietal areas (r=.39, P=.0002). The frequency of leu-koaraiosis in different age groups in the control and CApatients is depicted in Fig 2. In CA patients, leukoarai-osis tended to occur earlier than in controls, althoughthe difference was not significant.
Delay ofAdvanced Life Support and Cerebral EdemaThe 19 patients with the longest (more than 10
minutes) delays of advanced life support did not havemore infarcts, leukoaraiosis, or any other abnormalitieson MRI than the 33 patients with shorter (10 minutes or
less) delays of advanced life support (Table 4). Thedelay of advanced life support did not correlate with thedegree of leukoaraiosis or the number of infarcts either,but it had an inverse correlation with the degree ofcerebral atrophy (r= -.42, P=.003).
Probable cerebral edema was observed in 13 of the 33patients (39%) with short delays compared with 16 ofthe 19 patients (84%) with long delays of advanced lifesupport (P=.0004). Probable edema was somewhatmore common in patients who underwent MRI duringthe first 3 days (5 of 6 patients [83%]), compared withpatients imaged later (24 of 46 patients [52%], P=.32),but it was even observed in 7 of 15 patients (47%) whounderwent MRI later than 2 weeks after cardiac arrest.In two patients, a diffuse and generalized hyperintensityof the cerebral white matter was observed as a distinc-tive sign of severe edema and fatal hypoxic-ischemicencephalopathy after CA.
In a logistic regression model controlling for theeffects of age, sex, delay of MRI scan in days, treatmentby nimodipine or placebo, coronary disease or previousmyocardial infarction, and history of stroke, cardiacfailure, hypertension, and hypotension, the delay ofadvanced life support was the only independent riskfactor of probable edema (OR, 1.28; 95% CI, 1.1 to 1.6;P=.01). In other words, the risk of probable edema onMRI increased by 28 percentage units per each minutebefore the start of advanced life support.
HypotensionHypotension is commonly associated with cardiac
arrest and resuscitation, and it has been proposed as
one of the risk factors for both cerebral infarcts andleukoaraiosis. Therefore, we wanted to determine
100 -
Arrest *-.Control ---
0)
0
90 -
80 -
70 -
60 -
50 -
40 -
30 -
20 -
10 -
0 -
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1010 Stroke Vol 24, No 7 July 1993
TABLE 4. MRI Findings in Cardiac Arrest Patients With Long (>10 minutes) and Short (.10 minutes) AdvancedLife Support Delays
Long delay Short delay(n= 19) (n=33) P
Days since cardiac arrest (mean±SD) 12+9 11 +6 .62Range (2-47) (1-25)
Age (years; mean±SD) 65±11 64 .90Range (36-80) (41-85)
Cortical infarct 4 (21) 9 (27) .88Cortical watershed infarct 2 (11) 5 (15) .99Deep infarct 5 (26) 6 (18) .72
Deep watershed infarct 1 (5) 1 (3) 1.00Leukoaraiosis 6 (32) 9 (27) .98White matter hyperintensities 11 (58) 17 (52) .88Atrophy 3 (16) 20 (61) .0004Normal 6 (32) 5 (15) .30
MRI, magnetic resonance imaging; n, number of patients; white matter hyperintensities denote leukoaraiosis orinfarcts.Numbers of patients, proportions as percentages in parentheses for binomial variables. Probability values indicate
significance level of Student's t test for age and for delay of MRI scan and of Fisher's Exact Test for all other variables.
whether the presence of hypotension (defined as systolicblood pressure below 80 mm Hg any time during thefirst day) would be associated with any pathologicalfindings on MRI. Hypotension was observed in 25 of 52CA patients (48%). There was no difference in thefrequency of hypotension in nimodipine- (13 of 28[46%]) and placebo- (12 of 24 [50%]) treated patients.The frequencies of cortical (28% vs 22%) and deep(20% vs 22%) infarcts, also in watershed areas, leuko-araiosis (28% vs 30%), any white matter hyperintensi-ties (52% vs 56%), atrophy (44% vs 44%), and thenumber of all infarcts (0.6 vs 0.6) were equal in hypoten-sive and normotensive patients. Hypotension was notassociated with an increased risk of cerebral infarcts(OR, 1.02; 95% CI, 0.3 to 3.1; P=.97) or LA (OR, 1.08;95% CI, 0.3 to 3.7; P=.90) in univariate models or in alogistic regression model controlling for the effects ofage, sex, coronary disease or previous myocardial infarc-tion, history of stroke, and history of hypertension(cerebral infarct: OR, 0.99; 95% CI, 0.3 to 3.8; P=.99;leukoaraiosis: OR, 1.04; 95% CI, 0.16 to 6.9; P=.97).
Hypotension following CA was not a risk factor for anyof the abnormalities observed on MRI.
NimodipinePatients treated with nimodipine or placebo had
similar demographic data, characteristics of CA andresuscitation, and similar 1-year outcome (Table 2).There was also no significant difference in any of theMRI findings between the treatment groups. The fre-quency of deep infarcts was 29% (7 of 24) in theplacebo-treated group and 14% (4 of 28) in the nimod-ipine-treated group (P=.33, Table 5). The frequency ofleukoaraiosis and atrophy were similar in each group.However, 8 of the 12 nimodipine-treated patients (67%)with atrophy had a good outcome compared with 8 of 16patients (50%) without atrophy. In the placebo group, 9of 11 patients (82%) with atrophy had a good outcomein contrast to the 3 of 13 (23%) without atrophy(P=.01). The presence of atrophy was associated withreduced risk of poor outcome in placebo-treated pa-
tients (OR, 0.24; 95% CI, 0.07 to 0.86; P=.01) but not in
TABLE 5. MRI Findings in Cardiac Arrest Patients Treated With Nimodipine and Placebo
Nimodipine Placebo(n=28) (n=24) P
Days since cardiac arrest (mean±SD) 13±9 10±5 .29Range (1-47) (2-20)
Cortical infarct 7 (25) 6 (25) 1.00Cortical watershed infarct 3 (11) 4 (17) .82Deep infarct 4 (14) 7 (29) .33Deep watershed infarct 0 (0) 2 (8) .42Leukoaraiosis 9 (32) 6 (25) .80White matter hyperintensities 15 (54) 15 (63) .71Atrophy 12 (43) 11 (46) 1.00Normal 6 (21) 5 (21) 1.00
MRI, magnetic resonance imaging; n, number of patients; white matter hyperintensities denote leukoaraiosis orinfarcts.Numbers of patients, proportions as percentages in parentheses for binomial variables. Probability values indicate
significance level of Student's t test for delay of MRI scan and of Fisher's Exact Test for all other variables.
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Roine et al MRI After Cardiac Arrest 1011
TABLE 6. MRI Findings in Cardiac Arrest Patients With Good and Poor 1-Year Outcomes
Good outcome Poor outcomeFinding (n=28) (n=24) PDays since cardiac arrest (mean+SD) 12+6 11+9 .36Range (1-25) (2-47)
Age (years; mean±SD) 64±12 65±11 .68Range (36-83) (45-85)
Cortical infarct 6 (21) 7 (29) .75Cortical watershed infarct 2 (7) 5 (21) .30Deep infarct 4 (14) 7 (29) .33Deep watershed infarct 0 (0) 2 (8) .42Leukoaraiosis 8 (29) 7 (29) 1.00White matter hyperintensities 14 (50) 16 (67) .35Atrophy 17 (61) 6 (25) .02Normal 6 (21) 5 (21) 1.00
MRI, magnetic resonance imaging; n, number of patients; good outcome denotes good recovery or moderatedisability; poor outcome, severe disability or death according to the Glasgow Outcome Score; white matterhyperintensities are leukoaraiosis or infarcts.Numbers of patients, proportions as percentages in parentheses for binomial variables. Probability values indicate
significance level of Student's t test for age and for delay of MRI scan and of Fisher's Exact Test for all other variables.
nimodipine-treated patients (OR, 0.67; 95% CI, 0.26 to1.70; P=.62). Nimodipine-treated patients with proba-ble edema also had good outcome (8 of 16 patients[50%]) more often than placebo-treated patients withthis finding (3 of 13 patients [23%]), but the differencedid not reach statistical significance (P=.27).
In the placebo group, increasing delays of advancedlife support were associated with an increased risk ofedema shown on MRI. The risk more than doubledeach minute before the start of advanced life support(OR, 2.07; 95% CI, 1.1 to 3.8; P=.01). This was notobserved in the nimodipine group (OR, 1.07; 95% CI,0.9 to 1.3; P=.56).Adjusted for age, the delay of advanced life support
correlated inversely with the degree of atrophy inplacebo-treated patients (r= -.62, P<.0001) but not inpatients treated with nimodipine (r= -.10, P=.43; Fish-er's z value for the difference, 2.06; P=.04). Thus,increasing delays of advanced life support were associ-ated with increasing edema in placebo-treated but notin nimodipine-treated patients.
Functional OutcomeThe 28 patients with good 1-year outcome (good
recovery or moderate disability according to the Glas-gow Outcome Scale) had fewer MRI-confirmed infarctsthan those with poor outcome (severe disability ordeath by 1 year), but none of the differences reachedsignificance (Table 6). Atrophy was much more com-mon in patients with good outcome (17 of 28 [61%])than in those with poor outcome (6 of 24 [25%], P=.02),most of whom had probable brain edema. The degree ofatrophy also correlated with the Glasgow OutcomeScore (r=.34, P=.01), whereas the degree of leukoarai-osis (r= -.09, P=.54) and the number of infarcts(r= -.17, P=.23) did not correlate with outcome. Noneof the MRI findings correlated with the MMSE score inany of the subgroups.The results of the logistic regression analysis revealed
that the presence of atrophy (or lack of edema) was the
only significant factor predicting good outcome at 1 year(OR, 4.6; 95% CI, 1.4 to 15.8; P=.01) in a multivariatelogistic regression model adjusting for the effects of age,sex, delay of MRI scan in days, treatment by nimodipineor placebo, coronary heart disease or previous myocar-dial infarction, previous stroke, cardiac failure, andhypertension. Probable edema shown on MRI had asensitivity of 75% and a specificity of 61% in predictingpoor outcome.
DiscussionIn the present study, CA and age were independent
risk factors for cerebral infarcts, especially deep ones,demonstrated by MRI. Ciortical infarcts were observedin 25% of the patients and deep infarcts in 21%.Cerebral infarcts, verified by autopsy, have previouslybeen reported in only 5% of 135 CA survivors.20,21 If theassociation of CA and cerebral infarcts is explained byhemodynamic factors, an increased number of infarctswould be expected on watershed areas, which we didnot observe. However, multiple infarcts were morecommon after CA.The frequency and degree of leukoaraiosis were
closely associated with increasing age, but not with CAor with any of the cardiovascular disorders in univariateor multivariate analysis. This is in contrast to some ofthe previous reports.22-25 However, Schmidt and co-workers26 recently analyzed the occurrence of whitematter hyperintensities in stroke patients and normalvolunteers. In multivariate analysis, white matter hyper-intensities were independently associated with age anddiabetes mellitus only. CA is a combination of completeand incomplete global ischemias often associated withhypotension during reperfusion. Unexpectedly, hypo-tension associated with CA was not a risk factor for anyof the abnormalities observed on MRI, including leu-koaraiosis, although global ischemia is believed to un-couple cerebral autoregulation, making the brain morevulnerable to fluctuations in blood pressure.7,21 Leuko-araiosis and watershed infarcts do not seem to be
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1012 Stroke Vol 24, No 7 July 1993
associated with short-lived hemodynamic disturbancessuch as CA followed by hypotension.
Early computed tomographic (CT) findings (within 5days of global cerebral ischemia) have previously beenstudied by Kjos and coworkers in 10 patients.6 The mostcommon finding was diffuse cerebral edema, observedin all but 1 patient, accompanied by loss of normalgray-white matter differentiation in 6 patients. Thediffuse mass effect with obliteration of the sulci with noareas of decreased density was hypothesized to reflectearly cytotoxic edema.6 MRI and CT are known to havelimited capacity to detect generalized brain edemaexcept in the most severe cases, with markedly obliter-ated cerebrospinal fluid spaces and abnormal signalintensity in the brain parenchyma. We observed anincreased signal intensity in the cerebral white matter inthe T2-weighted images of 2 patients, both of whomdied without recovery of consciousness. The generallydiminished subarachnoid spaces and cerebral and cer-ebellar ventricles suggest the presence of brain edema.In CA patients, atrophy had no correlation with age asit did in control patients. Since the lack of atrophy wasthe only significant predictor of poor outcome in bothunivariate (Table 6) and multivariate analyses, thefinding was most likely associated with cerebral edema.In addition, atrophy was usually absent in patients withdelayed resuscitation but present in most patients withearly resuscitation; again, this was the only differencebetween these two groups of patients demonstrated byMRI. Probable edema shown on MRI was associatedwith a fivefold risk of poor 1-year outcome. It had a highsensitivity (75%) in identifying the patients with poor1-year outcome, but the specificity of the finding wasinsufficient for clinical purposes.The risk of probable edema on MRI increased by
approximately 30 percentage units per each minutebefore the start of advanced life support. The delay ofadvanced life support, known to be an important pre-dictor of survival in out-of-hospital CA,17 had an inde-pendent association with probable edema on MRI,which suggests that every minute of delay significantlyincreases the edema caused by global cerebral ischemia.However, increasing delays of resuscitation were notsignificantly associated with cerebral infarcts orleukoaraiosis.
Brain edema is related to increased intracranial pres-sure, which is believed to be rare after CA. Monitoringof intracranial pressure has not been routine in thepostresuscitative intensive care of adult patients.27-29However, the mean intracranial pressure measured byextradural electrodes was recently reported to exceed 25mm Hg during the second postarrest day in 22 of 84 CApatients (26%) and to be associated with poor out-come.30 At present, there is no evidence that anytreatment of increased intracranial pressure would alterthe outcome of hypoxic-ischemic encephalopathy.Nimodipine has not been proved to be beneficial after
human CA, although it has reduced delayed ischemicdeficits and the number of cerebral infarcts shown byCT after subarachnoid hemorrhage.12,3132 In the pres-ent study, the frequency of abnormal MRI findings didnot differ between the nimodipine- and placebo-treated
fewer infarcts in deep and watershed areas, but thedifference was not significant (Table 5).
Adjusted for age, the delay of advanced life supportcorrelated with probable edema in placebo-treated butnot in nimodipine-treated patients (P=.04). This findingmay suggest that nimodipine limited brain edema andimproved the tolerance for global ischemia associatedwith delayed resuscitation. It may also offer one expla-nation for the post hoc subgroup result obtained in theplacebo-controlled, double-blind, randomized trial of155 patients with out-of-hospital ventricular fibrillation,which suggested a beneficial effect of nimodipine forpatients with delayed advanced life support.12 Thepresent results agree with those of Gueugniaud et al,33who reported that both the mean and maximum intra-cranial pressures after CA were significantly lower in 19nimodipine-treated patients than in 20 control subjects.According to experimental evidence, nimodipine mayprevent the development of cerebral edema and theincrease of intracranial pressure associated with focal orglobal ischemia.34-38 Increased regional cerebral bloodflow (CBF) in the ischemic core of hemispheric infarctshas been demonstrated by positron emission tomogra-phy in humans.39 According to Forsman and cowork-ers,40 nimodipine nearly doubled the postischemic CBFin humans, probably due to uncoupling of cerebralautoregulation. Nimodipine-treated patients, however,did not experience better recovery; but the patients withthe highest CBF values had the worst outcome. In-creased CBF is not a favorable prognostic sign; it may beassociated with irreversible brain damage and deathafter human CA.7 Although nimodipine could make thebrain more vulnerable to hypotension by its demon-strated ability to inhibit normal regulation of CBF, wefound no evidence of such an effect.36,41,42One of the limitations of the present study is the
relatively low resolution of the 0.02-T ultra-low-fieldMRI scanner used. The smallest lesions (laminar necro-sis in particular) are likely to remain unobserved.Low-field MRI is not the method of choice for detectinggeneralized edema, either. Using the same ultra-low-field MRI scanner, white matter hyperintensities haverecently been shown to be associated with advanced ageand increased blood pressure.4344 Infarcts may not besuccessfully differentiated from leukoaraiosis usingMRI; especially, the differentiation between recent andold lesions is impossible. However, CA and other car-diovascular disorders correlated well with the presenceand number of cerebral infarcts, particularly deep in-farcts; CA, however, did not correlate with the presenceof leukoaraiosis, which suggests that the lesions weredifferentiated from each other. Furthermore, the corre-lation of leukoaraiosis and infarcts with age in CApatients and the correlation of atrophy with age andleukoaraiosis in control subjects are in accordance withresults published earlier.45 In the present study, theMRI findings correlated with the MMSE score neitherin CA patients nor in normal controls, which is inagreement with previous studies.44Another limitation of the study was that in some
patients MRI was performed too late for practicalprognostic purposes and in others it could not beperformed at all for reasons related to outcome, such as
patients. Nimodipine-treated patients tended to have poor medical condition or early death. This biased the
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Roine et al MRI After Cardiac Arrest 1013
population studied slightly toward better outcome andmay have diminished the accuracy of MRI in outcomeprediction.Compared with other published methods predicting
poor outcome after CA, MRI seemed to be comparableto single-photon emission computed tomography using99mTc-hexamethylpropyleneamine oxime (HMPAO-SPECT) but less accurate than neuron-specific enolasemeasured from the cerebrospinal fluid.5,46 To avoid anoverly pessimistic prognostication, tests used in criticalcare are generally required to have high specificity forpoor outcome, which is more important than highsensitivity. The only distinctive MRI finding indicativeof inevitable death may be the presence of severeedema, which we observed in two patients.
In conclusion, the present study demonstrated thatCA was associated with deep cerebral infarcts on MRIbut not with cortical watershed infarcts or leukoaraiosis,even in the presence of postarrest hypotension. Increas-ing delays of resuscitation were associated with proba-ble brain edema, which seemed to be suppressed bynimodipine treatment. The use of nimodipine in resus-citation is not justified, however, since it has not alteredthe outcome of CA.12,14 MRI can reveal the presence ofcerebral infarcts and probable brain edema associatedwith CA, but it seems to have only limited prognosticvalue and may not be the diagnostic method of choice inthe management of patients with hypoxic-ischemic en-cephalopathy after CA.
AcknowledgmentsThis work was supported by grants from the Finnish Heart
Association, the Paulo Foundation, the Finnish Medical Soci-ety Duodecim, the Finnish Neurology Foundation, the Acad-emy of Finland, and the Paavo Nurmi Foundation, all locatedin Helsinki, Finland; and from Bayer AG, Wuppertal,Germany.We thank Seppo Sarna, PhD, associate professor, Depart-
ment of Biometry, University of Helsinki, for statistical reviewof the manuscript. We also thank the personnel of the MobileIntensive Care Unit of Helsinki, the Emergency Department,the Intensive Care Unit, the Department of Radiology, andthe Neurological Outpatient Clinic of the Helsinki UniversityCentral Hospital.
References1. Wolfson SK, Safar P, Reich H, Clark JM, Gur D, Stezoski W, Cook
EE, Krupper MA. Dynamic heterogeneity of cerebral hypoperfu-sion after prolonged cardiac arrest in dogs, measured by the stablexenon-CT technique: a preliminary study. Resuscitation. 1992;23:1-20.
2. White BC, Winegar CP, Henderson 0. Prolonged hypoperfusion inthe cerebral cortex following cardiac arrest and resuscitation indogs. Ann Emerg Med. 1983;12:414-417.
3. DeVolder AG, Goffinet AM, Bol A, Michel C, de Barsy T, LaterreC. Brain glucose metabolism in postanoxic syndrome: positronemission tomographic study. Arch Neurol. 1990;47:197-204.
4. De Reuck J, Van Aken J, Decoo D, Strijckman K, Lemahieu I.Cerebral blood flow and oxygen metabolism in leuko-araiosis: a
positron emission tomography study. Cerebrovasc Dis. 1991;1:25-30.5. Roine RO, Launes J, Nikkinen P, Lindroth L, Kaste M. RegionalCBF after human cardiac arrest: HM-PAO SPECT study. ArchNeurol. 1991;48:625-629.
6. Kjos BO, Brandt-Zawadzki M, Young RG. Early CT findings ofglobal central nervous system hypoperfusion. Am J Neuroradiol.1983;4:1043-1048.
7. Cohan SL, Mun SK, Petite J, Correia J, Taveira Da Silva A,Waldhorn RE. Cerebral blood flow in humans following resusci-tation from cardiac arrest. Stroke. 1989;20:761-765.
8. Martin GB, Paradis NA, Helpern JA, Nowak RM, Welch KM.Nuclear magnetic resonance spectroscopy study of human brainafter cardiac resuscitation. Stroke. 1991;22:462- 468.
9. Torvik A. The pathogenesis of watershed infarcts in the brain.Stroke. 1984;15:221-223.
10. De Reuck J, Crevits L, DeCoster W, Sieben G, VanderEecken H.Pathogenesis of Binswanger chronic progressive subcortical enceph-alopathy. Neurology (Cleveland). 1980;30:920-928.
11. Sulkava R, Erkinjuntti T. Vascular dementia due to cardiacarrhythmias and systemic hypotension. Acta Neurol Scand. 1987;76:123-128.
12. Roine RO, Kaste M, Kinnunen A, Nikki P, Sarna S, Kajaste S.Nimodipine after resuscitation from out-of-hospital ventricularfibrillation: a placebo-controlled, double-blind, randomized trial.JAMA. 1990;264:3171-3177.
13. Folstein MF, Folstein SE, McHugh PR. "Mini-Mental State": a
practical method for grading the cognitive state of patients for theclinician. J Psychiatr Res. 1975;712:189-198.
14. Roine RO, Kajaste S, Kaste M. Neuropsychological sequelae ofcardiac arrest. JAMA. 1993;269:237-242.
15. Jennett B, Bond M. Assessment of outcome after severe braindamage: a practical scale. Lancet. 1975;1:480-484.
16. Abramson NS, Meisel A, Safar P. Deferred consent: A new
approach for resuscitation research on comatose patients. JAMA.1986;255:2466-2471.
17. Weaver WD, Cobb LA, Hallstrom AP, Fahrenbruch C, CopassMK, Ray R. Factors influencing survival after out-of-hospital car-
diac arrest. JAm Coll Cardiol. 1986;7:752-757.18. Woolson RF. Statistical Methodsfor theAnalysis ofBiomedical Data.
New York, NY: John Wiley & Sons; 1987.19. Dixon WJ, Brown MB, Engelman L, Hill MA, Jennrich RI. BMDP
Statistical Software Manual. Vols 1 and 2. Berkeley, Calif: Univer-sity of California Press; 1990:1,2.
20. Torvik A, Skullerud K. How often are brain infarcts caused byhypotensive episodes? Stroke. 1976;7:255-257.
21. Strandgaard S, Paulson OB. Cerebral autoregulation. Stroke. 1984;15:413-416.
22. Awad IA, Spetzler RF, Hodak JA. Incidental subcortical lesionsidentified on magnetic resonance imaging in elderly: I. Correlationwith age and cerebrovascular risk factors. Stroke. 1986;17:1084-1089.
23. Inzitari D, Diaz F, Fox A, Hachinski VC, Steingart A, Lau C,Donald A, Wade J, Mulic H, Merskey H. Vascular risk factors andleuko-araiosis. Arch Neurol. 1987;44:42-47.
24. Sullivan P, Pary R, Telang F, Rifai AH, Zubenko GS. Risk factorsfor white matter changes detected by magnetic resonance imagingin the elderly. Stroke. 1990;21:1424-1428.
25. Kobari M, Meyer JS, Ichijo M. Leuko-araiosis, cerebral atrophy, andcerebral perfusion in normal aging. Arch Neurol. 1990;47:161-165.
26. Schmidt R, Fazekas F, Kleinert G, Offenbacher H, Gindl K, PayerF, Freidl W, Niederkorn K, Lechner H. Magnetic resonance imag-ing signal hyperintensities in the deep and subcortical white mat-ter: a comparative study between stroke patients and normal vol-unteers. Arch Neurol. 1992;49:825-827.
27. Sakabe T, Tateishi A, Miyauchi Y, Maekawa T, Matsumoto M,Tsutsui T, Takeshita H. Intracranial pressure following cardiopul-monary resuscitation. Intensive Care Med. 1987;13:256-259.
28. Schmidt A, Binner L, Mayer U, Stauch M. The role of intracranialpressure (ICP) monitoring after cardiopulmonary resuscitation(CPR). Crit Care Med. 1988;16:389. Abstract.
29. Roine RO. Out-of-hospital cerebral resuscitation. In: Vincent J-L,ed. Update in Intensive Care and Emergency Medicine. Berlin, FRG:Springer Verlag; 1990:621-631.
30. Gueugniaud PY, Garcia Darennes F, Gaussorgues P, Bancalari G,Petit P, Robert D. Prognostic significance of early intracranial andcerebral perfusion pressures in post-cardiac arrest anoxic coma.
Intensive Care Med. 1991;17:392-398.31. Pickard JD, Murray GD, Illingworth R, Shaw MD, Teasdale GM,
Foy PM, Humphrey PR, Lang DA, Nelson R, Richards P, Sinar J,Bailey S, Skene A. Effect of oral nimodipine on cerebral infarctionand outcome after subarachnoid hemorrhage: British AneurysmNimodipine Trial. Br Med J. 1989;298:636-642.
32. Ohman J, Heiskanen 0. Effect of nimodipine on the outcome ofpatients after aneurysmal subarachnoid hemorrhage and surgery.J Neurosurg. 1988;69:683-686.
33. Gueugniaud PY, Gaussorgues P, Garcia Darennes F, Bancalari G,Roux H, Robert D, Petit P. Early effects of nimodipine on intra-cranial and cerebral perfusion pressures in cerebral anoxia afterout-of-hospital cardiac arrest. Resuscitation. 1990;20:203-212.
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1014 Stroke Vol 24, No 7 July 1993
34. Hadley MN, Spetzler RF, Fifield MS, Bichard WD, Hodak JA. Theeffect of nimodipine on intracranial pressure: volume-pressurestudies in a primate model. J Neurosurg. 1987;66:387-393.
35. Jacewicz M, Brint S, Tanabe J, Wang XJ, Pulsinelli WA. Nimod-ipine pretreatment improves cerebral blood flow and reduces brainedema in conscious rats subjected to focal cerebral ischemia.J Cereb Blood Flow Metab. 1990;10:903-913.
36. Gaab MR, Hollerhage HG, Walter GF, Hocheder M, Haubitz I.Brain edema, autoregulation, and calcium antagonism: an experi-mental study with nimodipine. Adv Neurol. 1990;52:391-400.
37. Bielenberg GW, Burniol M, Rosen R, Klaus W. Effects of nimod-ipine on infarct size and cerebral acidosis after middle cerebralartery occlusion in the rat. Stroke. 1990;21(suppl 4):IV-90-IV-92.
38. Hara H, Nagasawa H, Kogure K. Nimodipine attenuates bothischaemia-induced brain oedema and mortality in a rat novel tran-sient middle cerebral artery occlusion model. Acta Neurochir Suppl(Wien). 1990;51:251-253.
39. Hakim AM, Evans AC, Berger L, Kuwabara H, Worsley K, Mar-chal G, Biel C, Pokrupa R, Diksic M, Meyer E. The effect ofnimodipine on the evolution of human cerebral infarction studiedby PET. J Cereb Blood Flow Metab. 1989;9:523-534.
40. Forsman M, Aarseth HP, Nordby HK, Skulgerg A, Steen PA.Effects of nimodipine on cerebral blood flow and cerebrospinal
fluid pressure after cardiac arrest: correlation with neurologic out-come. Anesth Analg. 1989;68:436-443.
41. Haws CW, Heistad DD. Cardiovascular effects of nimodipine: I.Effects on distribution of blood flow, II: Inhibition of cerebralvasoconstrictor responses. J Cereb Blood Flow Metab. 1983;3(suppl 1):524-525.
42. Hollerhage H-G, Gaab MR, Zumkeller M, Walter GF. The influ-ence of nimodipine on cerebral blood flow: autoregulation andblood-brain barrier. J Neurosurg. 1988;69:919-922.
43. Wahlund L-O, Agartz I, Almqvist 0, Basun HM, Forssell L, SaafJ, Wetterberg L. The brain in healthy aged individuals: MR imag-ing. Radiology. 1990;174:675-679.
44. Almkvist 0, Wahlund LO, Andersson-Lundman G, Basun H,Backman L. White-matter hyperintensity and neuropsychologi-cal functions in dementia and healthy aging. Arch Neurol. 1992;49:626-632.
45. Mirsen TR, Lee DH, Wong CJ, Diaz JF, Fox AJ, Hachinski VC,Merskey H. Clinical correlates of white matter changes on MRIscans of the brain. Arch Neurol. 1991;48:1015-1021.
46. Roine RO, Somer H, Kaste M, Viinikka L, Karonen S-L. Neu-rological outcome after out-of-hospital cardiac arrest: predic-tion by cerebrospinal fluid enzyme analysis. Arch Neurol. 1989;46:753-756.
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from
R O Roine, R Raininko, T Erkinjuntti, A Ylikoski and M KasteMagnetic resonance imaging findings associated with cardiac arrest.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1993 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.24.7.1005
1993;24:1005-1014Stroke.
http://stroke.ahajournals.org/content/24/7/1005World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from