maintaining agility in an unsteady economy operations improvement strategies saturday, october 11,...
TRANSCRIPT
Maintaining Agility in an Unsteady Economy
Operations Improvement Strategies
Saturday, October 11, 2008
from 2:45 – 4:45 p.m. ET
1
2
Session Agenda: Operations Improvement Strategies
I. Tipping Points for Financial Success
II. Resident Centered Scheduling
III. Questions
3
• Advantage—current Residents are financially set—even in a recession.
Strategy: Increase revenues by selling more services to current Residents.
• Advantage—many AAHSA members have significant opportunities to reduce costs.
Strategy: Review operations and implement improvements enhancing financial performance and creating a competitive advantage.
Advantages and Strategies

4
• Objective—identify revenue/expense improvements that will:
– Strengthen financial performance,– Improve debt service capacity,– Increase days cash on hand, and– Create additional opportunities for communities to act
strategically in order to achieve mission.
Review Operations Annually
5
CCRCs need an 8% to 10% margin from operations in order to act strategically.
Operating Margin
6
• DO NOT focus on past or place blame.
• DO NOT place too much emphasis on the numbers—the INITIATIVES are most important.
• TIME PROCESS—allow adequate time for implementation of findings.
Caution
7
1. Maximizing Occupancy.
2. Premium Pricing.
3. Lean Organizational Structure.
4. Effective Capital Management
5. Optimizing Information Systems
6. Efficient Staffing
Six Tipping Points for Financial Success
8
MAXIMIZING OCCUPANCY
9
• DO two out of three Residents on IL wait lists accept unit when offered?
• ARE units reoccupied within 60-90 days of acceptance?
• ARE admissions to health care processed 24 hours per day, 7 days a week?
Diagnostics
10
• Are more than 40% of new Residents from current resident referrals?
• Are permanent transfers to higher care levels made fairly but expeditiously—temporary stays average 60 days or less?
Diagnostics
11
• Definition—determines maximum revenue at full occupancy (100%) and identifies reasons for the vacancy (unit not ready for occupancy or Resident temporarily in another care level).
• Purpose—focuses management on financial advantage of small increases in occupancy.
Best PracticesLost Revenue Reporting

12
PREMIUM PRICING
13
• Raise monthly service fees consistently and ensure that second-person fees cover costs and set overall fees at or above market rate.
• Continue to keep fees at or above market despite increasing profitability.
• Set fees based on lifetime contractual costs and allow for increased pressure to age-in-place.
Tipping PointPremium Pricing
14
• Service fees = or > than competitors.
• All services not used by most Residents or not desired to be insured as a group against future costs should be extra services at market rate.
• Programs which are the best in your market should be the most expensive.
• Nursing supply charge systems should cover non-billable costs plus at least 40% profit.
Diagnostics
15
• Consider alternate forms of fee increases (e.g., percentage versus per person dollar amount).
• Concentrate on superb resident communications.– Total costs of operations.– Market value of services.– Extra charges.
• Implement an effective POS system.• Consider flexible dining plans that minimize meal
credits.• Implement level of care pricing in Assisted Living.
Best Practices

16
ORGANIZATIONAL STRUCTURE
17
• Create a FLAT Structure—avoid multiple levels (e.g., Vice President + Director + Manager + Supervisor + Assistants).
• Minimize administrative support—set target for support to include only Executive Office, Facilities, Marketing/Development and Health Services.
Tipping PointLean Organizational Structure

18
• Scrutinize for value—evaluate staffing in HR, Security, Information Systems, Compliance, Business Development and IL Social Services.
• Utilize leads instead of supervisors where appropriate.
• Reduce Board size to 8 to 12 challenging, community-minded individuals.
Tipping PointLean Organizational Structure
19
• Centralize Facility Operations to include Maintenance, Grounds, Housekeeping, Laundry, Security and Transportation.
• Schedule Kitchen staff so that cooks open and close.
• Empower Charge Nurses to lead Care Teams to serve specific Residents and consider returning nurse leadership to direct patient care on the floors.
• Limit CEO’s direct reports to 8 or less—empower Senior Management.
Best Practices
20
CAPITAL MANAGEMENT

21
• Consider the possibility of improving programs, quality of service and efficiency of operations before capital spending on facility redesign.
• Boards should hold management accountable for all projects over $1M (e.g., projected rate of return, operating margin).
Tipping PointsEffective Capital Management
22
• Involve operations team in new building design.
• On-time construction with minimal change orders.
• Rapid fill-up at projected rates.
Tipping PointsEffective Capital Management

23
• Target debt service and depreciation at less than 40% of net revenues.
• Ensure that approved projects meet budgeted margins and rate of return.
• Target Days Cash on Hand (DCOH) at 250+.
Diagnostics
24
• Boards should require that management provide annual reporting on projects against projections until stabilized.
• Repositioning should first focus on programming improvements prior to capital expenses (only when unavoidable).
Best PracticesCapital Management
25
OPTIMIZE INFORMATION SYSTEMS

26
• Manage labor costs by providing payroll reports that compare to budget and set productivity targets.
• Provide financial reporting that is concise and action-oriented.
• Provide summary of financial performance using a “dashboard” approach.
• Implement technology that reduces staffing requirements.
Tipping PointsOptimize Information Management
27
• Analyze the number of manual processes.
• Evaluate the integration of time clock/payroll/POS/receivables and clinical/case-mix billing software.
• Evaluate existing security and emergency response systems to determine if technology could improve efficiency.
Diagnostics
28
• Wireless call systems which signal a pager.
• POS system integrated with receivables.
• Electronic medical record combined with service tracking system (i.e. CareTracker or DaRT Chart) , which helps maximize reimbursement under Medicare and case-mix Medicaid.
• Eliminate time-consuming manual processes.
Best PracticesOptimize Information Systems
29
EFFICIENT STAFFING

30
• Efficient use of indirect staff—all employees not performing contractual services (less than $0.30 of payroll dollars & less than 20% of FTEs).
• One supervisor for 15 to 20 FTEs, excluding direct care nurses.
Diagnostics

31
• Eliminate/reduce shift overlaps unless supervisor report is required (15 minutes maximum).
• Use a patterned schedule that provides the appropriate staff at the right time.
• Use performance- not seniority-based compensation structure.
• Utilize technology to reduce staffing requirements.
Tipping PointEfficient Staffing
32
Target salaries and benefits to be around 40-45% of net revenues.
Overall Staffing Targets
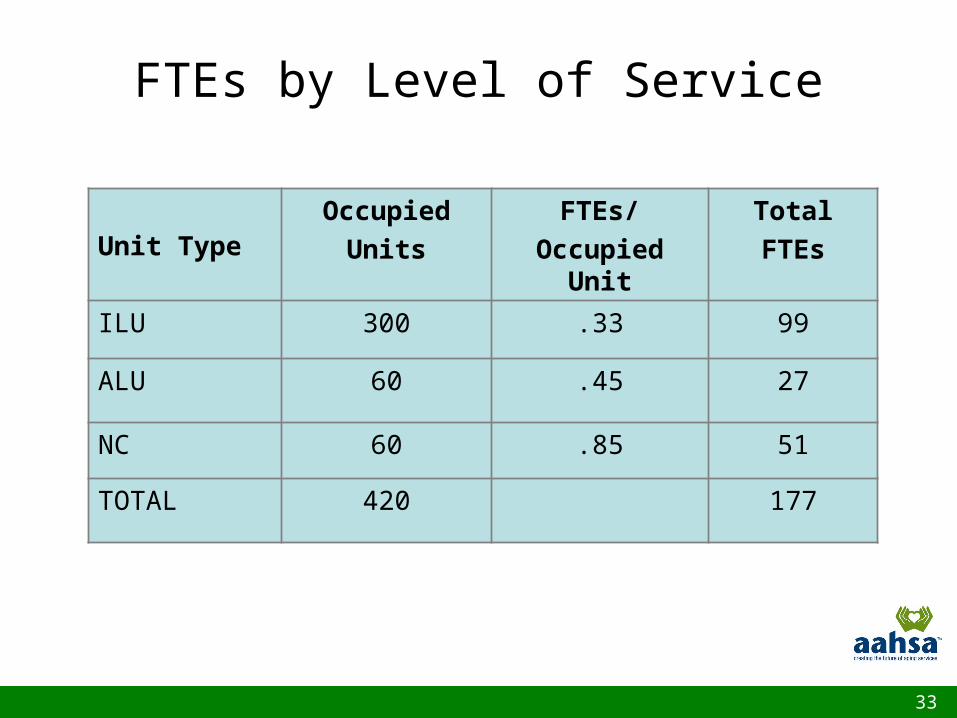
33
Unit TypeOccupied
Units
FTEs/
Occupied Unit
Total
FTEs
ILU 300 .33 99
ALU 60 .45 27
NC 60 .85 51
TOTAL 420 177
FTEs by Level of Service
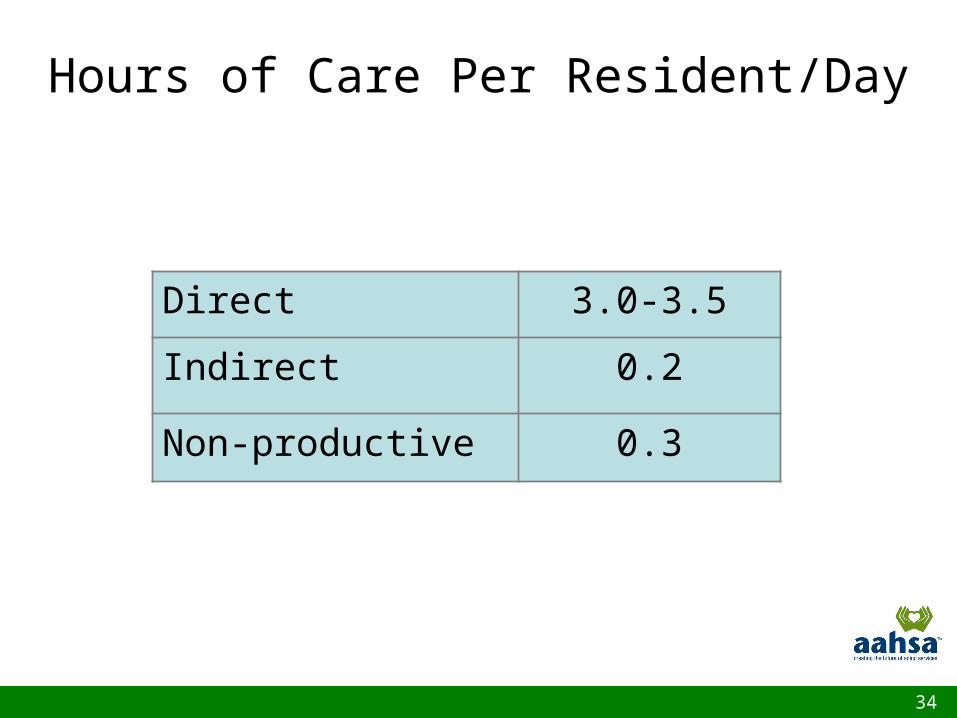
34
Direct 3.0-3.5
Indirect 0.2
Non-productive 0.3
Hours of Care Per Resident/Day
35
• Target 50,000 square feet per maintenance FTE.
• Target square feet per housekeeper.
– ILU = 30,000.
– Assisted living = 20,000.
– Health center = 8,000.
• 60 pounds of laundry cleaned per productive hour.
Facility Operations
36
• Target meals per labor hour.
– Health care = 5.
– Assisted living = 4.
– ILU = 2-3 depending on type of service.
• 40% of labor should be part-time.
Dining Services
37
• Blend security and 24-hour maintenance.
• Create a balance between technical, skilled and general Staff.
• Regularly evaluate contracted versus internalizing services.
Best PracticesMaintenance and Security
38
Create schedules so that:– There is only one housekeeper per apartment.– Housekeepers clean units on same floor or in
the same area (villas/cottages) on the same day.
– Detailed cleanings are incorporated into regularly scheduled cleaning times.
Best PracticesEnvironmental Services
39
• Create drying capacity that is 150% of washing capacity.
• Establish cart exchange system.
• Maintain 5 Turns of linen.
• Close laundry on weekends.
Best PracticesLaundry
40
• Dining staff should clean all dining rooms and kitchens.
• Nourishment costs should be charged to Health Care.
• Implement Liberalized Geriatric Diet Manual.
Best Practices
Dining
41
• Support staff—10-hour shifts, 4 days per week; staggered staffing. BENEFIT: Lower transportation and child
care costs.
Best PracticesAlternative Scheduling
42
• Assisted living and health care—12-hours shifts (7 days in 2 weeks). BENEFITS:
• Minimizes number of shift changes.• Eliminates shift overlap for CNAs.• Staffs the same number of people.• Provides consistency of staff. • Prefers full-time staff.
Best PracticesAlternative Scheduling
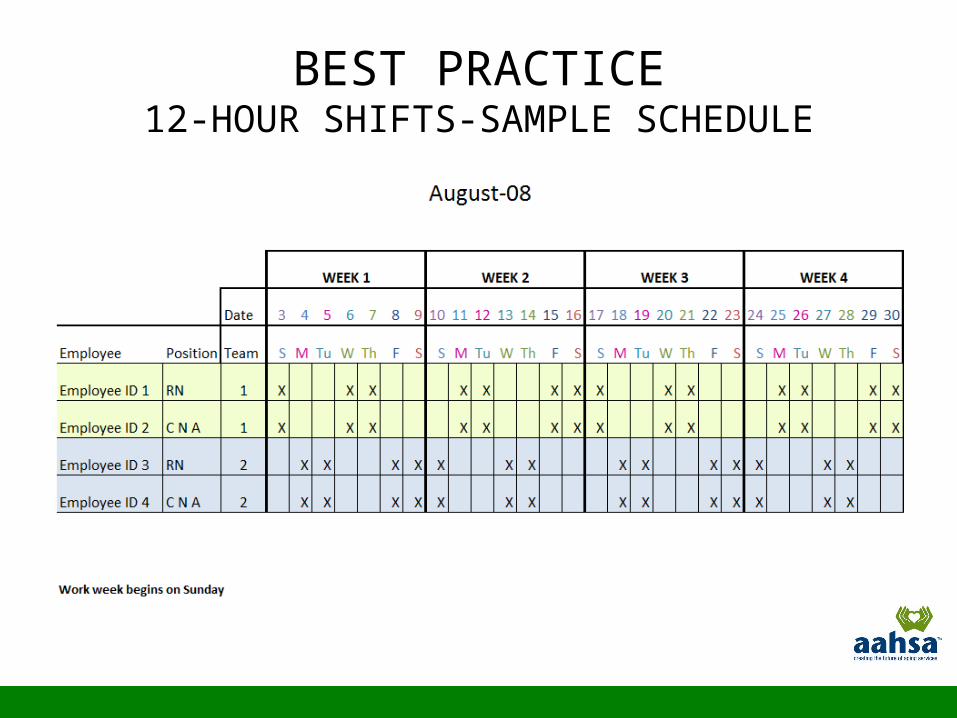
BEST PRACTICE12-HOUR SHIFTS-SAMPLE SCHEDULE
STAFFING
In order to have 3-day weekend on Friday, Saturday, and Sunday, pay period cannot end on Thursday or Sunday
Weekend differential can be eliminated
Shift differential is paid only on night shift (7p to 7a)
STAFFING
• Use day shift staff pattern for Day 12 and night shift staff pattern for Night 12
• Team approach allows reduction of nurse management (e.g., Unit Manager or House Supervisors)
Must be based on over 40 hours not 8 over 80
Overtime versus idle time- One idle hour = wages and benefits—all nonproductive
- Overtime assumes productive work
- Overtime can be more cost-effective
Most nursing home staff day and evening shifts the same—overstaffing between 7p and 11p
OPERATIONSOVERTIME
OPERATIONSFACILITY BENEFITS
• Reporting to the same people at the beginning and end of shifts
• Residents served by the same nursing staff increases consistency of care
• CNAs and nurses are on the same team and have the same days off, which reduces call-offs due to peer pressure
• Improved recruitment • More staff to feed evening meals and
return residents to bed• Less shift-to-shift complaints—problems
are easier to resolve with only two shifts• Less wasted time for reporting with only
two shifts—units are quieter at 3p
OPERATIONSFACILITY BENEFITS
• Scheduling is simple—just fill in names each month and adjust for vacations and/or holidays
• Less complaints– Working long stretches– Too many weekends—12-hour shifts
gives off every other weekend (Fri/Sat/Sun)
OPERATIONSFACILITY BENEFITS
EMPLOYEE BUY-INTIME-OFF
More days off in a two-week pay period (e.g., 7 days versus 4 days)
Never work more than 3 days without 2 days off—3 day stretch is only once every two weeks
Employees have a long weekend (Fri/Sat/Sun) every other week
• Can plan their schedules since the days off are known in advance
• Only need to use 24 hours of PTO to be off for 7 days at a time
• Feels more like working part-time with full-time benefits
EMPLOYEE BUY-ININCREASE CONTROL

EMPLOYEE BUY-INLESS EXPENSE
Transportation Laundry (Uniforms) Child care

EMPLOYEE BUY-INIMPROVED RESIDENT CARE
• Consistent full time staff• Residents receive care from the
same 4 CNAs and 4 nurses• Increases productive hours of care
due to elimination of shift change
IMPLEMENTATION
• Director of Nursing should discuss the benefits with supervisors involved
• DON should meet with the LPN charge nurses to outline benefits and get input for CNA scheduling
• Consider beginning nurse and CNA programs concurrently
• Provide adequate time for management and staff to accept change

IMPLEMENTATION
• Place names on proposed schedule presented at CNA meeting so that days off can be clearly seen
• When creating schedule, 11p to 7a shift should be given priority followed by the 3p to11p shift according to seniority
IMPLEMENTATIONCHALLENGES
• High absenteeism (> than 2% call offs)
• Work force with second jobs
• Work force relying on public transportation
• Child care
• Older staff
• Heavy medication pass at 9p
IMPLEMENTATIONCHALLENGES-POSSIBLE SOLUTIONS
• Interaction with nurses and CNAs who come from facilities where 12-hour shifts have been successfully implemented – As guest speakers– Access in groups for questions on a
more personal level.
58
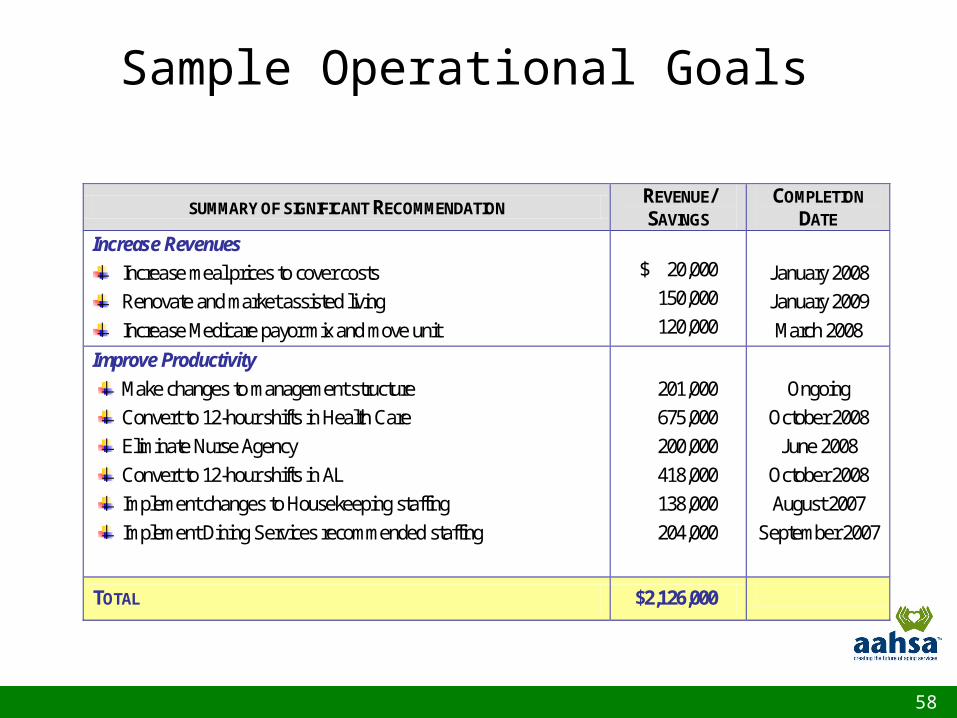
SUMMARY OF SIGNIFICANT RECOMMENDATION REVENUE/ SAVINGS
COMPLETION DATE
Increase Revenues Increase meal prices to cover costs Renovate and market assisted living Increase Medicare payor mix and move unit
$ 20,000 150,000 120,000
January 2008 January 2009 March 2008
Improve Productivity
Make changes to management structure Convert to 12-hour shifts in Health Care Eliminate Nurse Agency Convert to 12-hour shifts in AL Implement changes to Housekeeping staffing Implement Dining Services recommended staffing
201,000 675,000 200,000 418,000 138,000 204,000
Ongoing
October 2008 June 2008
October 2008 August 2007
September 2007
TOTAL $2,126,000
Sample Operational Goals