maintenance of chest wall stability - thorax · chest wall, usually the sternum, for correction of...
TRANSCRIPT
Thorax (1964), 19, 397.
Maintenance of chest wall stabilityB. T. LE ROUX
From the Department of Thoracic Surgery, The Royal Infirmary, Edinburgh
The surgeon is faced with the need to assist inthe maintenance of stability of the chest wallin two sets of circumstances: (1) when stabilityhas been disrupted by accidental trauma withresultant 'flail' or 'stove-in' chest; (2) whenstability has been jeopardized by surgical inter-vzntion, likely again in two circumstances:(a) with intentional mobilization of part of thechest wall, usually the sternum, for correction ofcongenital deformities, of which pectus excavatumis the most common, and (b) with resection ofpart of the chest wall in the management ofprimary or metastatic rib tumours, or pulmonarytumours which have invaded the chest wall.The purpose of this paper is to list some of the
methods described in the literature for the main-tenance of chest wall stability (and from theirnumber none can be uniformly satisfactory) andto review the methods used, in the circumstancesoutlined above, in the Regional Thoracic Unit inEdinburgh.
FLAIL CHEST
The reasons for and the urgency of stabilizing aflail chest are now well recognized (Barrett, 1960).Fixation of the mobile segment in an orthopaedicsense is difficult and probably unnecessary, andthe object of treatment is the prevention of para-doxical movement of the chest wall with respira-tion. The time-honoured method, of Hippocraticantiquity, is by external support, with strappingapplied directly or over pads, or with sandbags orbags containing lead shot. External support issometimes a satisfactory manceuvre both as a'first-aid' gesture and, with devoted maintenanceof a clear airway, as definitive management(Sandor, 1963). All methods of external supporthave, however, this in common-they hide fromthe observer visual evidence of paradoxicalmovement of the mobile segment whether or notthey prevent it, and the surgical trainee, stilloften responsible for the early management ofpatients with flail chest, may, by not seeing para-doxical movement, be persuaded that stability ofthe chest wall has been achieved. The patient'srespiratory efforts may well be less strenuous,
because movement of the chest wall has beeninhibited by the strapping; and when to thisdeceptive calm is added the effect of morphia usedto diminish pain, the stage is set for the disasterswhich are consequent upon hypoxia and the reten-tion of carbon dioxide. There is certainly a groupof patients in whom the extent of trauma to thethoracic cage justifies their inclusion in the groupof stove-in chest injuries and in whom the applica-tion of strapping, with or without tracheostomy(Carter and Giuseffi, 1951), has been successful;but where disruption of the respiratory mechanicsis more than trivial other steps are usually neces-sary to maintaini satisfactorily stability of thechest wall.The alternative forms of management fall into
three groups: (1) Fixation, which may be called'closed', since fracture sites are not exposed, andwhich depends on the use of various types ofhooks and slings, towel clips or transfixing pins,more commonly suggested as satisfactory wherethe mobile segment includes the sternum, whichis slung by these supports to a plaster or otherform of cuirass or to a specially designedframe (Heroy and Eggleston, 1951 ; Hudson,McElvenny, and Head, 1954; Proctor and Lon-don, 1955; and Sillar, 1962); (2) fixation of thefractured ribs at open operation by wiring,stapling, or intramedullary nailing (Blades andKent, 1940; Coleman and Coleman, 1950;Crutcher and Nolen, 1956); and (3) indirectsplinting of the chest wall by intermittent positivepressure artificial respiration through a cuffedtracheostomy tube in a patient pharmacologicallyrendered apnioeic (Avery, Morch, and Benson,1956; Griffiths, 1960).The methods of closed fixation are criticized on
the grounds that they fail adequately to controlparadox and easily cut out, and this criticismis substantiated by the experience in Edinburghwith some of these methods in the early part ofthe last decade. Internal fixation of fractured ribends by wiring has been reported to fail to achieveits object (Windsor and Dwyer, 1961) and has alsobeen seen to fail in Edinburgh (Griffiths, 1960).It is the patient whose mobile chest most needsfixation who is usually least able to tolerate an
397
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from
B. T. le Roux
extensive procedure, the aim of which is internalfixation of a large number of fractures, many ofthem through cartilage, and many of thosethrough rib difficult to identify on chest radio-graphs obscured by surgical emphysema andmottled, traumatized lung.
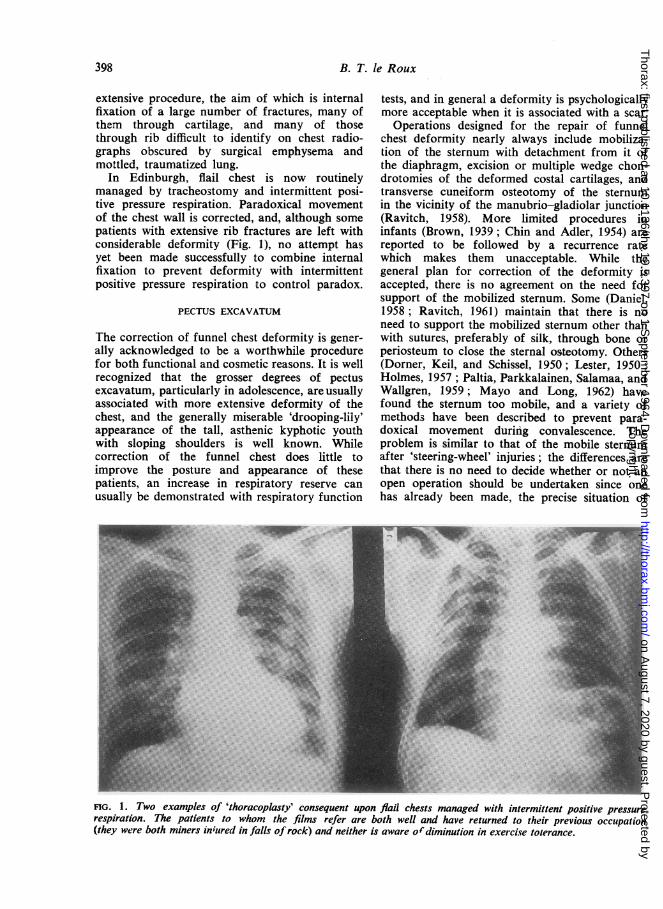
In Edinburgh, flail chest is now routinelymanaged by tracheostomy and intermittent posi-tive pressure respiration. Paradoxical movementof the chest wall is corrected, and, although somepatients with extensive rib fractures are left withconsiderable deformity (Fig. 1), no attempt hasyet been made successfully to combine internalfixation to prevent deformity with intermittentpositive pressure respiration to control paradox.
PECTUS EXCAVATUM
The correction of funnel chest deformity is gener-ally acknowledged to be a worthwhile procedurefor both functional and cosmetic reasons. It is wellrecognized that the grosser degrees of pectusexcavatum, particularly in adolescence, areusuallyassociated with more extensive deformity of thechest, and the generally miserable 'drooping-lily'appearance of the tall, asthenic kyphotic youthwith sloping shoulders is well known. Whilecorrection of the funnel chest does little toimprove the posture and appearance of thesepatients, an increase in respiratory reserve canusually be demonstrated with respiratory function
tests, and in general a deformity is psychologicallymore acceptable when it is associated with a scar.
Operations designed for the repair of funnelchest deformity nearly always include mobiliza-tion of the sternum with detachment from it ofthe diaphragm, excision or multiple wedge chon-drotomies of the deformed costal cartilages, andtransverse cuneiform osteotomy of the sternumin the vicinity of the manubrio-gladiolar junction(Ravitch, 1958). More limited procedures ininfants (Brown, 1939; Chin and Adler, 1954) arereported to be followed by a recurrence ratewhich makes them unacceptable. While thegeneral plan for correction of the deformity isaccepted, there is no agreement on the need forsupport of the mobilized sternum. Some (Daniel,1958; Ravitch, 1961) maintain that there is noneed to support the mobilized sternum other thanwith sutures, preferably of silk, through bone orperiosteum to close the sternal osteotomy. Others(Dorner, Keil, and Schissel, 1950; Lester, 1950;Holmes, 1957; Paltia, Parkkalainen, Salamaa, andWallgren, 1959; Mayo and Long, 1962) havefound the sternum too mobile, and a variety ofmethods have been described to prevent para-doxical movement during convalescence. Theproblem is similar to that of the mobile sternumafter 'steering-wheel' injuries; the differences arethat there is no need to decide whether or not anopen operation should be undertaken since onehas already been made, the precise situation of
FIG. 1. Two examples of 'thoracoplasty' consequent upon flail chests managed with intermittent positive pressurerespiration. The patients to whom the films refer are both well and have returned to their previous occupation(they were both miners inured in falls of rock) and neither is aware ofdiminution in exercise tolerance.
398
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from
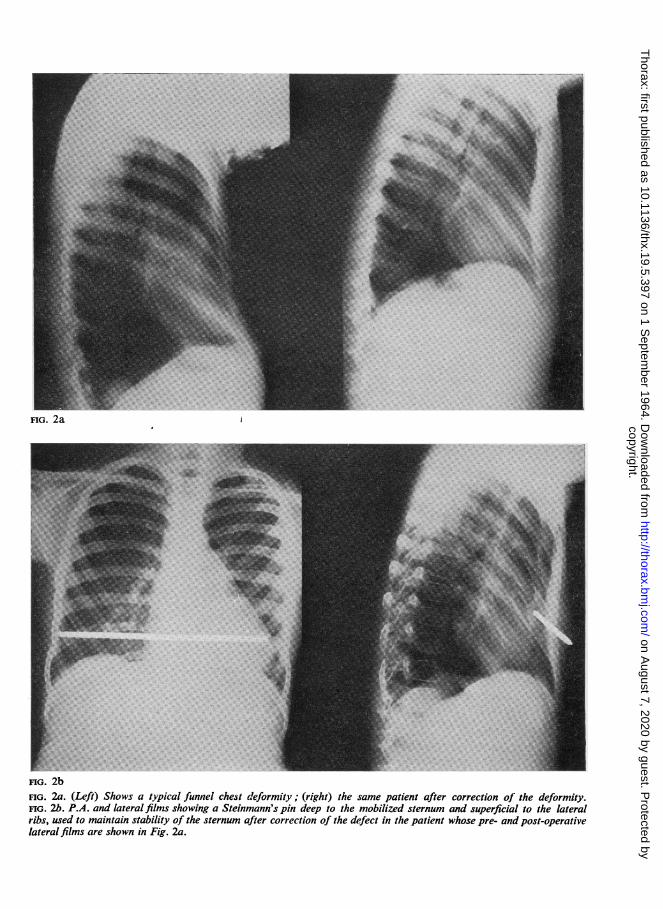
FIG. 2a
FIG. 2bFIG. 2a. (Left) Shows a typical funnel chest deformity; (right) the same patient after correction of the deformity.FIG. 2b. P.A. and lateral films showing a Steinmann's pin deep to the mobilized sternum and superficial to the lateralribs, used to maintain stability of the sternum after correction of the defect in the patient whose pre- and post-operativelateral films are shown in Fig. 2a.
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from
B. T. le Roux
sternal and costal fractures is known, and thepatient has not been jeopardized by gross traumaand a period of uncontrolled paradoxical respira-tion.Homologous rib struts passed horizontally be-
hind the sternum have been used, -the ends of therib resting laterally on the bony chest wall at themargins of the defect (Dorner et al., 1950). Ribshave the advantage of easy availability, and twodisadvantages: (1) the length of rib used inevitablycurves and lies conveniently only with its con-cavity directed anteriorly, so that the deformitytends to be under-corrected and the lateral endsof the rib project forward; (2) the thoracoplasticeffect of resection of a single rib is appreciable,and, while of value in thoracotomy for limitedpulmonary resection (le Roux, 1961), is undesir-able in a patient whose respiratory reserve isalready diminished by chest deformity.
Steinmann's pins have been used to maintainstability of the sternum. Holmes (1957) skeweredthe sternum in its length, across the osteotomy,to fix the gladeolus to the manubrium at anappropriate angle, the pin emerging through theskin of the anterior abdominal wall, and tractionbeing maintained on the projecting end. In hiscases the pin was removed after two or threeweeks. Griffin and Minnis (1957) and Mayo andLong (1962) reported series in which the mobil-ized sternum was transfixed from side to sidebetween the anterior and posterior cortical tablesat the level of the fourth or fifth cartilage. Eithera Steinmann's pin or a Kirschner wire was used,and the support became cutaneous just below thenipples where the points were protected with corksand a collodion dressing was used to cover the sitesof pin-puncture; the pin was removed after threeweeks. A Kirschner wire is a dangerously slendersternal support.
Paltia et al. (1959) advocated the use of stainlesssteel struts to support the sternum, and variationson this technique have been described by Adkinsand Blades (1961) and by Jensen, Schmidt, andGaramella (1962). The last-mentioned authorsdesigned a set of malleable stainless steel alloystruts which they have called 'stribs' and whichthey advise should be left in situ for the betterpart of a year in children and permanently inadults.
In Edinburgh, the patients with funnel chestsin whom corrective procedures were undertakenin the early part of the last decade were nearlyall children; in these patients the sternum wasnot supported, correction was satisfactory in allexcept one, in whom a second operation becamenecessary, and in most of them paradoxical move-
ment of the mobilized sternum proved anembarrassment in the early post-operative period.During this period 11 patients were treated. Fivepatients were subsequently managed by mobiliza-tion of the sternum and its support with an homo-logous rib strut; in these, the disadvantages ofthis procedure enumerated above were recognized.A Steinmann's pin has been used in six successivepatients in thb simplest possible way, by laying thepin across the gap created by the excision ofdeformed cartilage deep to the sternum and super-ficial to the ribs laterally. The ends of the pinhave been left buried under the skin where one orother is easily found by palpation six to eightweeks later, and the pin is withdrawn through asmall incision. The sternum has been secure fromthe moment of recovery from anaesthesia in allthese patients; convalescence has been uneventfuland the chest wall solid after removal of the pin.The pre- and post-operative films of one of thesepatients are shown (Fig. 2 a and b).
TUMOURS OF THE CHEST WALL
Primary rib tumours are not common; metastaticrib tumours are often multiple and do not there-fore present a surgical problem; bronchial carci-noma which invades the chest wall is relativelyinfrequently amenable to resection. In Edin-burgh, during a 10-year period when 3,00)patients with bronchial carcinoma were seen, partof the chest wall was resected in 40 patients. Ofthese resections, 18 were undertaken forriblesionsthought pre-operatively to be primary ribtumours; of the 18, four were shown to beplasmacytomata, and in these patients generalizedmanifestations of their disease later became ob-vious; two were metastases from unsuspectedprimary renal tumours in patients with normalpyelograms; the remaining 12 were primary ribtumours. In two other patients resection of a ribmetastasis from renal carcinoma was undertakenin the belief that the rib lesion represented theonly metastasis, and in both survival for morethan two years has justified the procedure. In fivepatients, inflammatory rib lesions were resected,and in 15 patients pulmonary carcinomata, whichhad invaded the chest wall lateral to the posteriorrib angle, were managed by lobectomy or pneu-monectomy and resection of that part of the chestwall invaded by the tumour.There is no clearly defined circumstance in
which it is necessary to repair with autogenousor prosthetic material a defect in the chest wallas opposed simply to covering the defect with theoverlying soft tissues or the scapula. Wide exci-
403
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from
Maintenance of chest wall stability
sion of rib tumours is a prerequisite of adequatesurgical management, and it is usually necessaryto resect at least 6-7 in. (15-18 cm.) of three ribsand the soft tissues of the two intercostal spacesbetween the ribs. When the defect left after theresection of such an area of chest wall is coveredby scapula, it is probably not necessary to supportthe chest other than by formal closure of thethoracotomy. A defect of similar size elsewhere,and especially anteriorly, should bz repaired bothto prevent paradoxical movement with respirationand for cosmetic reasons.A wide range of autogenous material has been
used to support the chest wall after the ablationof tumours-periosteal flaps, musculoperiosteal-osseous flaps, free rib grafts, tibial grafts, fascialata, rectus sheath, breast flaps, sliding flaps oflatissimus dorsi and pectoralis major, and fullthickness skin grafts. None except bone is suffi-ciently rigid, and it is now rare to read of the useof autogenous material in the repair of defects inthe thoracic wall. In recent years prostheticmaterials have been used with increasing fre-quency, and it is possible to suggest the pre-requisites of the ideal prosthetic material for thispurpose. The material should be and remain suffi-
ciently rigid to abolish paradox. It should be inert,tolerated, and incorporated by the host, able to bemanipulated and shaped to fit a defect the extentof which cannot be determined before operation,and it should be radio-translucent so as not toobscure the lung fields on post-operative chestradiographs.Metals-tantalum and stainless steel as plates
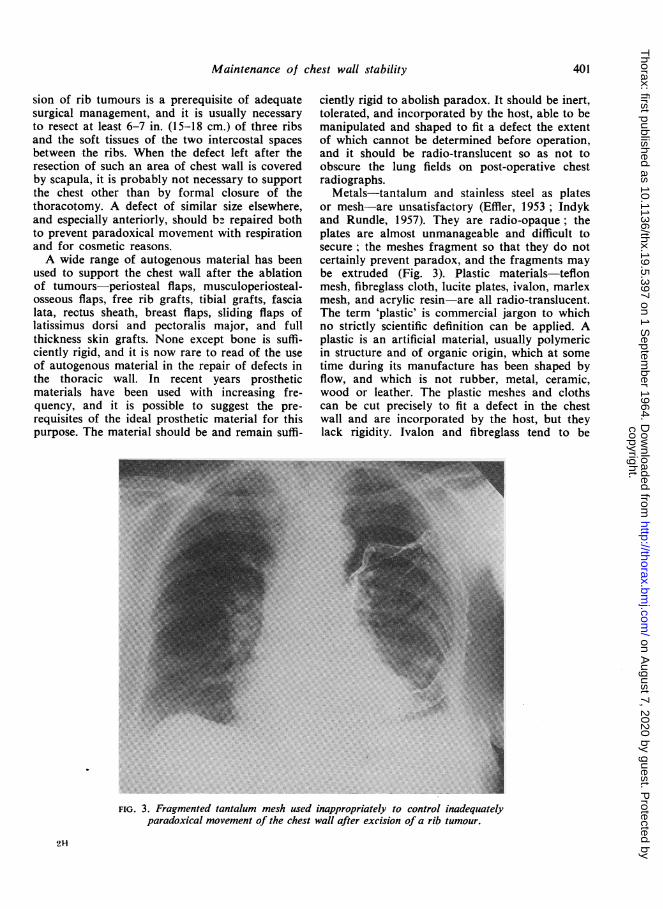
or mesh-are unsatisfactory (Effler, 1953 ; Indykand Rundle, 1957). They are radio-opaque; theplates are almost unmanageable and difficult tosecure; the meshes fragment so that they do notcertainly prevent paradox, and the fragments maybe extruded (Fig. 3). Plastic materials-teflonmesh, fibreglass cloth, lucite plates, ivalon, marlexmesh, and acrylic resin are all radio-translucent.The term 'plastic' is commercial jargon to whichno strictly scientific definition can be applied. Aplastic is an artificial material, usually polymericin structure and of organic origin, which at sometime during its manufacture has been shaped byflow, and which is not rubber, metal, ceramic,wood or leather. The plastic meshes and clothscan be cut precisely to fit a defect in the chestwall and are incorporated by the host, but theylack rigidity. Ivalon and fibreglass tend to be
FIG. 3. Fragmented tantalum mesh used inappropriately to control inadequiatelyparadoxical movement of the chest wall after excision of a rib tumour.
21-
401
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from
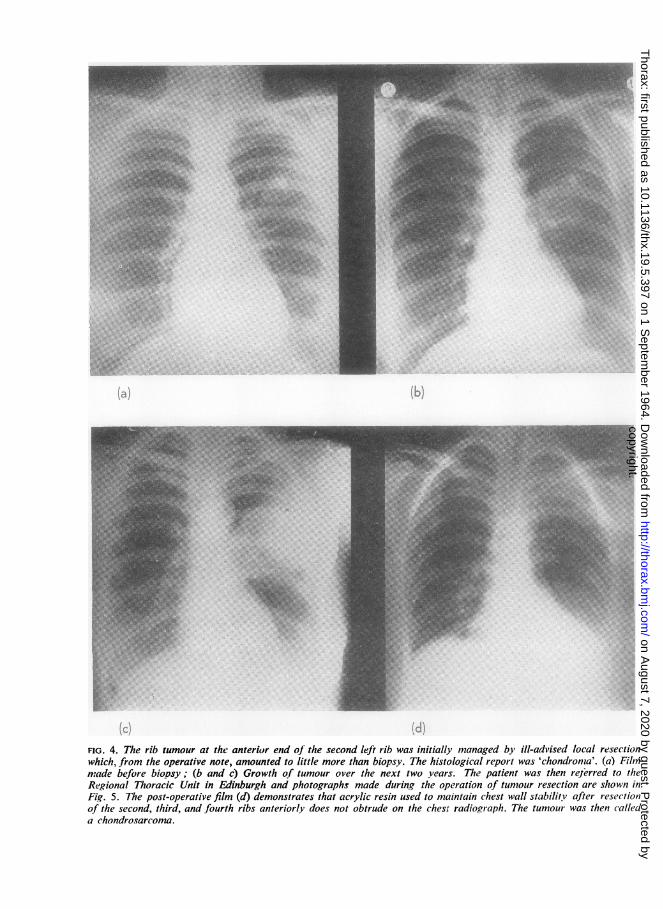
FiG. 4. The rib tumour at the anterior end of the second left rib was initially managed by ill-advised local resectionwhich, from the operative note, amounted to little more than biopsy. The histological report was 'chondroma'. (a) Filmmade before biopsy; (b and c) Growth of tumour over the next two years. The patient was then rejerred to theRegional Thoracic Unit in Edinburgh and photographs made during the operation of tumour resection are shown inFig. 5. The post-operative film (d) demonstrates that acrylic resin used to maintain chest wall stabilitv after r-esectionof the second, third, and fourth ribs anteriorly does not obtrude on the chesr radiograph. The tumour was then calleda chondrosarcoma.
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from
Maintenance of chest wall stability
-
..0~~~~~.
.Rol.:.'.
(b)
(d)
AI
((f)(e)
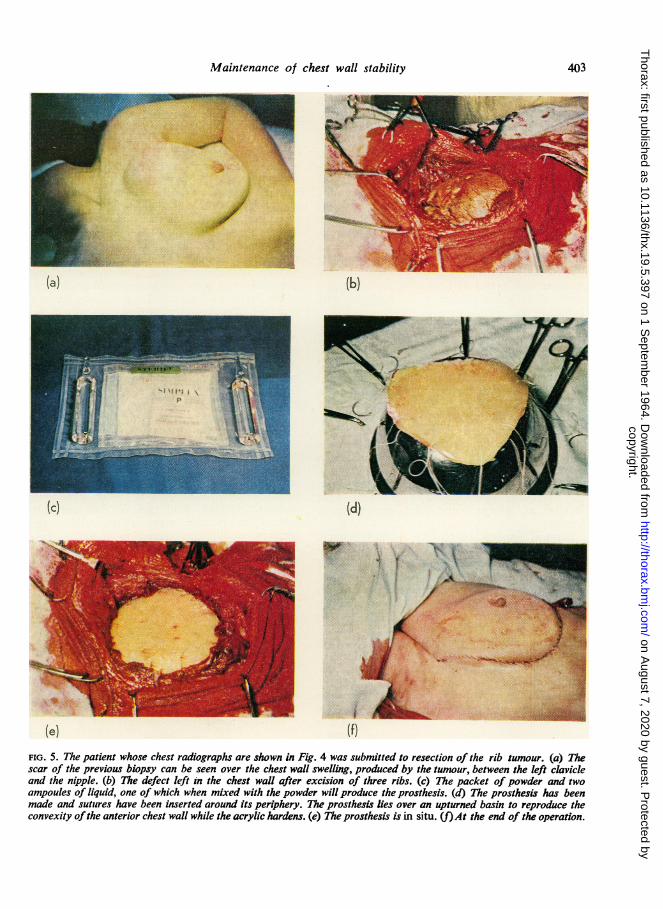
FIG. 5. The patient whose chest radiographs are shown in Fig. 4 was submitted to resection of the rib tumour. (a) Thescar of the previous biopsy can be seen over the chest wall swelling, produced by the tumour, between the left clavicleand the nipple. (b) The defect left in the chest wall after excision of three ribs. (c) The packet of powder and twoampoules of liquid, one of which when mixed with the powder will produce the prosthesis. (d) The prosthesis has beenmade and sutures have been inserted around its periphery. The prosthesis lies over an upturned basin to reproduce theconvexity ofthe anterior chest wall while the acrylic hardens. (e) The prosthesis is in situ. (f)At the end of the operation.
(a)
(c)
403
I
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from
B. T. le Roux
rejected, especially in the presence of infection(Usher and Wallace, 1958). Lucite is not con-veniently manipulated at operation. Marlex mesh(Graham, Usher, Perry, and Barkley, 1960) isregarded with enthusiasm in the American litera-ture, and it fulfils many of the criteria of a satis-factory chest wall prosthesis. It does not imme-diately control all paradox, but control of paradoxis said to be adequate, and the mesh form of thematerial allows of incorporation in the host.Marlex is a polyethylene with a high tensilestrength easily made into a monofilament fromwhich mesh can be made. It is said to excite lessforeign body reaction than, for example, dacron,orlon, or nylon, and it is not rejected in the pre-sence of infection (Usher, Fries, Ochsner, andTuttle, 1959).
In Edinburgh, acrylic resin has been used satis-factorily to restore the rigidity of the chest wallafter resection of rib tumours. The material(Surgical Simplex PI) was originally borrowedfrom the neurosurgical unit where it had beenused for cranioplasty. The use of acrylic for thispurpose is well documented (Robinson and Mac-alister, 1954; Rietz, 1958). An acrylic is a syn-thetic plastic resin derived from acrylic acid. Thetwo important polymers that are included in thegroup of acrylic resins are polymethyl acrylate, atough rubbery material used, for example, as asafety-glass interlay, and polymethyl methacry-late, a hard clear thermoplastic resin mostfamiliar as 'perspex' and used extensively indentistry.
Surgical Simplex is a powder to which a liquidis added to form a putty-like paste which, withina few minutes, changes, with the production ofconsiderable heat, to an inert solid state. Whenin paste form the plastic can be moulded to anyshape, cut, and transfixed with sutures, and onhardening it retains its shape faithfully. Theliquid is a powerful lipoid solvent which is steril-ized during manufacture by being passed througha bacterial filter; it is supplied in ampoules. Thepowder is supplied in plastic packets and is steril-ized by gamma irradiation.The powder, contained in an inner sterile plastic
packet, is removed under surgical conditions froman outer packet, a corner of the inner packet issnipped off, and the liquid contents of an ampouleare poured into the packet. Within a few minutesof mixing, a paste is formed of a sufficiently tackyconsistency to allow a thin (41 in.) sheet of thematerial to be moulded by hand within the plasticpacket. This sheet can be cut, together with itsI Obtainable from North Hill Plastics, Limited, London
containing packet, to the shape required to fillthe defect in the chest wall, and a series of silksutures can be placed around the periphery ofthe prosthesis. After some six to eight minutes theprosthesis quite suddenly becomes hot, and when,a few minutes later, it has cooled it is very hard,and it retains its shape. It is still sandwichedbetween layers of plastic, the remains of thepacket in which it was contained. These are peeledoff in such a way as not to remove the sutures,and the prosthesis is then secured in position.A defect in the chest wall has been repaired
with acrylic resin on 14 occasions. In these 14patients convalescence has been uneventful, thechest wall has been completely rigid at the siteof the defect, and paradoxical respiration has notoccurred. The first few patients, in whom theacrylic prosthesis has now been in situ for sixyears, remain well. The pre- and post-operativechest radiographs and intra-operative photographof a patient with a chondrosarcoma of the chestwall, in whom the tumour was resected and thedefect closed with acrylic resin, are shown inFigs. 4 and 5.
SUMMARY
The maintenance of chest wall stability after acci-dental and surgical disruption of part of the chestwall is discussed, and the techniques used in Edin-burgh for the management of the unstable chestwall are outlined. Flail chest is managed withintermittent positive pressure respiration ; thesternum, mobile after correction of funnel chestdeformity, is supported with a Steinmann's pin;a defect left after resection of part of the chestwall is closed with acrylic resin.
REFERENCES
Adkins, P. C. and Blades, B. (1961). A stainless steel strut for correc-tion of pectus excavatum. Surg. Gynec. Obstet., 113, 111.Avery, E. E., Morch, E. T., and Benson, D. W. (1956). Criticallycrushed chests. J. thorac. Sung., 32, 291.Barrett, N. R. (1960). The treatment of stove-in chest. Lancet, 1,
293.Blades, B. and Kent, E. M. (1940). Individual ligation technique forlower lobe lobectomy. J. thorac. Surg., 10, 84.Brown, A. L. (1939). Pectus excavatum (Funnel chest). Ibid., 9, 164.Carter, B. N., and Giuseffi, J. (1951). Tracheotcmy: A useful
procedure in thoracic surgery, with particular reference to itsemployment in crushing injuries of the thorax. Ibid., 21, 495.
Chin, E. F. and Adler, R. H. (1954). The surgical treatment of pectusexcavatum (funnel chest). Brit. med. J., 1, 1064.
Coleman, F. P. and Coleman, C. L. (1950). Fracture of ribs-Alogical treatment. Surg. Gynee. Obstet., 90, 129.
Crutcher, R. R. and Nolen, T. M. (1956). Multiple rib fracture withinstability of chest wall. J. thorac. Surg., 32, 15.Daniel, R. A. (1958). The surgical treatment of pectus excavatum.
Ibid., 35, 719.Dorner, R. A., Keil, P. G., and Schissel, D. J. (1950). Pectus
excavatum. Ibid., 20, 444.Effiler, D. B. (1953). Prevention of chest wall defects: Use oftantalum
and steel mesh. Ibid., 26, 419.Graham, J., Usher, F. C., Perry, J. L., and Barkley, H. T. (1960).
Marlex mesh as a prosthesis in the repair of thoracic wall defects.Ann. Surg., 151, 469.
404
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from

Maintenance of chest wall stability
Griffin, E. H., and Minnis, J. F. (1957). Pectus excavatum: A surveyand a suggestion for maintenance of correction. J. thorac. Surg.,33, 625.
Griffiths, H. W. C. (1960). Crush injuries of the chest. J. roy. Coll.Surg. Edinb., 6, 12.
Heroy, W. W., and Eggleston, F. C. (1951). A method of skeletaltraction applied through the sternum in ' steering wheel' injuriesof the chest. Ann. Surg., 133, 135.
Holmes, C. L. (1957). Pectus excavatum. Surgical technique: A newform of external traction to the elevated sternum. J. thorac.Surg., 33, 321.
Hudson, T. R., McElvenny, R. T. and Head, J. R. (1954). Chest wallstabilization by soft tissue traction. J. Amer. med. Ass., 156, 768.
Indyk, J. S. and Rundle, F. F. (1957). Closure of a chest wall defectwith tantalum mesh gauze. Med. J. Aust., 2, 465.
Jensen, N. K., Schmidt, W. R., and Garamella, T. J. (1962). Funnelchest A new corrective procedure. J. thorac. Surg., 43, 731.
le Roux, B. T. (1961). Techniques ofThoracotomy. E. & S. Livingstone,Edinburgh and London.
Lester, C. W. (1950). Funnel chest Its cause, effects and treatment.J. Pediat., 37, 224.
Mayo, P. and Long, G. A. (1962). Surgical repair of pectus excavatumby pin immobilisation. J. thorac. Surg., 44, 53.
Paltia, V., Parkkalainen, K. V., Salamaa, M., and Wallgren, G. R.(1959). Operative technique in funnel chest. Acta chir. scand.,116, 90.
Proctor, H. and London, P. S., (1955). The stove-in chest with para-doxical respiration. Brit. J. Surg., 42, 622.
Ravitch, M. M. (1958). Operation for correction of pectus excavatum.Surg. Gynec. Obstet., 106, 619.(1961). Operative treatment ofcongenital deformities ofthe chest.Amer. J. Surg., 101, 588.
Rietz, K.-A. (1958). The one-stage method of cranioplasty withacrylic plastic. J. Neurosurg., 15, 176.
Robinson, R. G., and Macalister, A. D. (1954). Acrylic cranioplasty.A simple one-stage method using a cold curing material. Brit. J.Surg., 42, 312.
Sandor, F. F. (1963). Treatment of stove-in chest with "paradoxicalrespiration" in peripheral hospitals. Thorax, 18, 116.
Sillar, W. (1962). The crushed chest. J. roy. Coll. Surg. Edinb., 7, 101.Usher, F. C. and Wallace, S. A. (1958). Tissue reaction to plastics.
Arch. Surg., 76, 997.- Fries, J. G., Ochsner, J. L., and Tuttle, L. L. D. (1959). Marlex
mesh, a new plastic mesh for replacing tissue defects. Ibid., 78,138.
Windsor, H. M. and Dwyer, B. (1961). The crushed chest. Thorax, 16, 3.
405
copyright. on A
ugust 7, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.5.397 on 1 Septem
ber 1964. Dow
nloaded from