making the most of payment reform
DESCRIPTION
WELCOME April 18,2014 This webinar will begin promptly at 1pm EDT. Making the most of payment reform. presenters. Host: Sabrina Edgington , MSSW, Program and Policy Specialist, National Health Care for the Homeless Council - PowerPoint PPT PresentationTRANSCRIPT

This activity is made possible by grant number U30CS09746 from the Health Resources and Services Administration, Bureau of Primary Health
Care. Its contents are solely the responsibility of the presenters and do not necessarily represent the official views of HRSA.
MAKING THE MOST OF PAYMENT REFORM
WELCOMEApril 18,2014
This webinar will begin promptly at 1pm EDT

PRESENTERS
• Host: Sabrina Edgington, MSSW, Program and Policy Specialist, National Health Care for the Homeless Council
• Melissa Hansen, MPH, Program Principal, National Conference of State Legislatures
• DaShawn Groves, MPH, Assistant Director, State Affairs, National Association of Community Health Centers
• Monica Bharel, MD, Chief Medical Officer, Boston Health Care for the Homeless Program

OVERVIEW
The role of the state in payment reform
State efforts and health center engagement
The Boston HCH Program experience

HEALTH CENTERS AND PAYMENT REFORM
• In expansion states, health centers are expected to absorb many newly eligible beneficiaries.
• Many high cost health system users with complex health needs will now have coverage.

BALTIMORE HEALTH CARE FOR THE HOMELESS PROGRAM

TRIPLE AIM
Improved health (outcomes)
Improved quality (patient satisfaction)
Reduced cost

MANY PAYMENT MODELS BEING TESTED
• Global Payment• ACO Shared Savings
Program• Medical Home• Bundled Payment• Hospital-Physician
Gainsharing• Payment for Coordination
• Hospital Pay-for Performance
• Payment Adjustment for Readmissions
• Payment Adjustment for Hospital-Acquired Conditions
• Physician Pay-for-Performance
• Payment for Shared Decision making
Source: Schneider, E., Hussey, P., and Schnyer, C. (2011). Payment Reform: Analysis of Models and Performance Measurement Implications. http://www.rand.org/pubs/technical_reports/TR841.html
Making the Most of Payment ReformPayment Reform and State Legislatures
Introduction: Payment Reform & State Legislatures
• History of reforms– Private market reforms – Medicare activities– State activities
• Payment reform efforts have accelerated in last few years for multiple reasons

• Improving Medicaid value is at the top of some legislative agendas (over 520 Medicaid related bills filed)
• Driven by a number of factors:• Continual pressure on state budgets;• Health reform: challenges and opportunities;
• Reforms aimed at better care, better outcomes, lower cost – provides potential for bipartisan efforts (payment reform)
10
Medicaid Policies & Payment Reforms, State Legislatures

11
Legislative Role in Payment Reform Efforts
• Purchaser of health care– Medicaid, state employers, other programs
• Purse strings and policymaking – Infrastructure (e.g. HIT)– Regulatory levers (state agencies)
• Convening key stakeholders• Focus on Medicaid reform
Factors to Consider Budgetary pressures ACA: challenges and opportunities Federally support for payment reform

Pressure on State Budgets
Revenues are expected to meet estimates, but growth is expected to taper off.
Spending is generally on target.
Year end-balances generally have improved.
Despite stabilizing fiscal conditions, uncertainties persist.

Top Fiscal Issues for 2014 Legislative Sessions
Medicaid/ Health Care State Employee Salaries and BenefitsTaxes and Revenues
Education Infrastructure Corrections/ Public Safety
29 13 13
6912
Source: NCSL survey of state legislative fiscal offices, fall 2013.
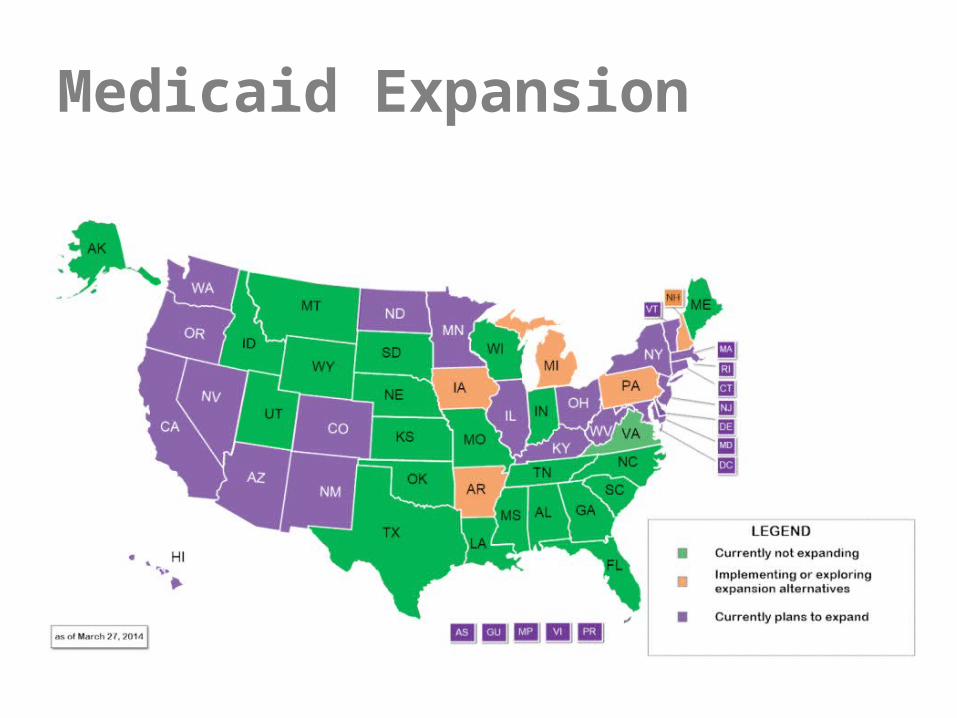
Medicaid Expansion

State Structures for Health Insurance Marketplaces/Exchanges
NCSL Data: April 1, 2014

The “New Coverage Gap”

• Medicaid (examples) – Health Homes for Enrollees with Chronic Conditions– State Innovation Models Initiative
• Medicare (examples)– Medicare Shared Savings Program– Medicare Value-based Purchasing Program
• Federal Employees Health Benefit Program (examples)– Office of Personnel Management Support for Patient-Center Medical
Homes
18
Payment Reform: Federally Supported Opportunities

•Risk based managed care•Non-risk care management•ACOs (CCOs, RCCOs, ACEs)•Health homes• Integrated primary care and behavioral health
19
Triple Aim – Better Care, Better Outcomes, Lower Cost – Medicaid Payment and Delivery System Reforms
Sources: • Kaiser Commission on Medicaid and the Uninsured, Medicaid in a Historic Time of Transformation: Results
from a 50-State Medicaid Budget Survey for State Fiscal Years 2013 and 2014, October 2013, available at http://kff.org/medicaid/
• Joan Henneberry joined Health Management Associates 2013

State-Based Medical Home Initiatives
WA
OR
TX
CO
NC
LA
PA
NY
IA
VA
NE
OK
AL
MD
MT
ID
KS
MN
NHME
AZ
VT
MOCA
WY
NM
IL
WI
MI
WV
SC
GA
FL
UTNV
ND
SD
AR
INOH
KY
TN
MS
DE
RI
NJ CT
MA
HI
Medical home activity (45 states and Washington, D.C.)
Making medical home payments (29 states)
Payments based on provider qualification standards (27 states)
AK
As of August 2013
Source: NASHP

State Innovation Models InitiativeTypes of Awards

Workforce Demands of New Payment and Delivery Models Models
New or Expanded Roles for:– Nurses– Behavioral Health Specialists– Community Health Workers– Social Workers– Peer Specialists– Pharmacists– Health Coaches

Mandated Coverage for Telehealth Services

Becoming a Key Stakeholder• Track payment reform efforts in your state (or local area).• Establish and maintain a relationship with legislator(s)
representing your area(s).• Get involved in collaborative efforts.• Self assessment of capacity (infrastructure, HIT,
workforce).• Be clear, concise in communications.

• Privacy issues• Fraud and abuse• Market concerns (anti-trust)• Network adequacy and patient satisfaction • Do new payment methods improve value?
Legislative Concerns With Payment Reform Activities, Some Examples

Contact:Melissa Hansen
For More Information
http://www.ncsl.org/documents/health/PaymentRTK13.pdf

Making the Most of Payment Reform
DaShawn Groves, MPH
Assistant Director, State Affairs
National Association of Community Health Centers

Overview
• State Developments on Payment Reform Impacting Health Centers
–Missouri (Health Homes)
–Minnesota (ACOs)
–Oregon (APM Development)
• Successfully Engaging in Payment Reform
–Considerations for PCAs
–Key Capabilities for Health Centers
–Key Steps
• Resources

Missouri
• First Section 2703 Health Homes for Chronically Ill State Plan Amendment (SPA) targeting safety-net providers
• 18 Health Centers• Eligible chronic conditions include:
– Asthma
– Diabetes
– Heart disease
– BMI >25
– Development Disabilities
• State pays $58.47 PMPM• Performance measures outlined in SPA • Developing shared savings methodology

Missouri: Lessons Learned–Be involved from early stages
–Set clear, simple goals
–View 2703 as a “safe” opportunity to leverage
federal funds and take a step towards capitation

Minnesota (FUHN ACO)• Part of a three-year Medicaid payment reform
demonstration• Ten urban health centers located in Minneapolis
and St. Paul• Paid on PPS basis• Total Costs of Care targets include:
– Inpatient– Outpatient– Professional– Ancillary – Some mental health and chemical health services
• Savings– 1st 2% will be retained by state– 98% will be split equally between the state and FUHN

Minnesota (FUHN ACO)• Keys to Success
–Appropriate program governance
–Access to population health management technology
–Inclusion of performance management coaches
–Enhancing care coordination

Oregon
• Health centers asked PCA for methodology to better align to PCMH model
• Delinks payment from a face-to-face visit
• Convert PPS into a capitated bundled payment
–Includes:
• Physical health services
• Mental health services after one year
• Eventually Dental services
• Able to receive incentive payments
• Three-year commitment from both parties

Oregon: Lesson Learned
• Hard to keep all the balls in the air–APM implementation and refinement
–Bridging towards value-based pay
–Practice transformation• Data collection• Patient engagement• Population management• Access• Team-based care
• Clinics face many demands

Successfully Engaging in Payment Reform Considerations for PCAs

Considerations for PCAs
• Keep a Pulse on the Broader Payment Reform Environment
• Build Support for Delivery System Transformation as a Primary Goal of Payment Reform
• Secure Input in Payment Reform Design
• Encourage Innovation among Leading Health Centers
• Facilitate Development of Health Center Capacity for Participation.

Key Capabilities for Health Centers

Analytic Capabilities
1. Document the Value of Enabling Services• coding in billing systems• enabling services in EHR/PM templates
2. Assess Impact of Social Determinants• Define and capture social determinants
Analytic Capabilities (continued)
3. Use Data for Design, Monitoring, and
Evaluation• Develop data partnerships/ strategies to
secure data– inpatient– specialty care– long-term care – ancillary data
• Use data robustly: prospectively as well as retrospectively

Operational Capacities
• Leadership and Appetite for Innovation
• Sophisticated use of Health Information Technology
• Partnership Capabilities

Key Steps for PCAs and Health Centers
Key Steps• Robust understanding of payment reform efforts in the
state and local environment
• Ensure a clear, shared vision of organization’s role in achieving the Triple Aim.
• Critically assess current operations and capabilities.
• Work collaboratively with other health centers, stakeholders, and partners to accelerate transformation.
Publications:
• Health Center and Payment Reform: A Primer
• Health center Payment Reform: State Initiatives to Meet the Triple Aim, State Policy Report #47
www.nachc.com/state-policy.cfm
Contact Info:DaShawn Groves. MPH
202-331-4606
Resources

MONICA BHAREL, MD, MPHBOSTON HEALTH CARE FOR THE
HOMELESS PROGRAM
Payment Reform: Experiences from the Field

A Framework for Preparing for Health Care Reform at your Program
Clearly defining the issueHaving data and knowing the factsUsing the data to be involved early in processUnderstanding that change is hardWorking collaborativelyBe willing to be in it for the long run

A Framework for Preparing for Health Care Reform at your Program
Clearly defining the issueHaving data and knowing the factsUsing the data to be involved early in processUnderstanding that change is hardWorking collaborativelyBe willing to be in it for the long run

Current situation Future possibility
Volume incentives
Fragmented payment
Accountable Care
Vuln
erab
le
popu
lation
s
Accountability for defined population
Pay for value
Comprehensive and transparent care
Fragmented delivery
Inconsistent quality

A Framework for Preparing for Health Care Reform at your Program
Clearly defining the issueHaving data and knowing the factsUsing the dataUnderstanding that change is hardWorking collaborativelyBe willing to be in it for the long run

U.S. Health Care Expenditures are Rising
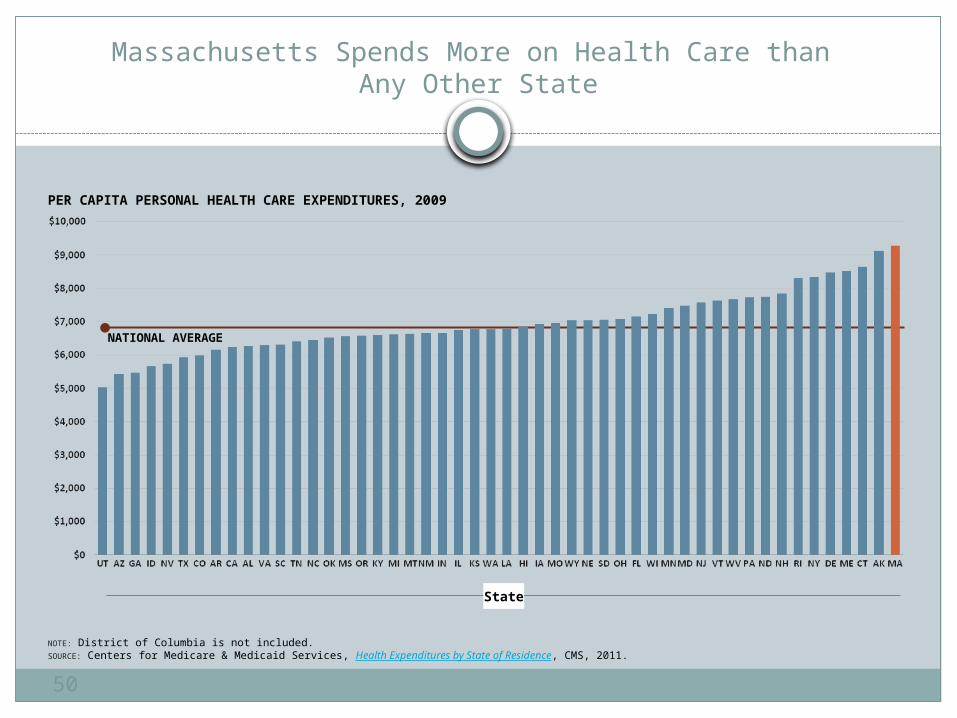
Massachusetts Spends More on Health Care than Any Other State
50
PER CAPITA PERSONAL HEALTH CARE EXPENDITURES, 2009
NOTE: District of Columbia is not included.SOURCE: Centers for Medicare & Medicaid Services, Health Expenditures by State of Residence, CMS, 2011.
State
NATIONAL AVERAGE

The Increasing Costs of Health Care Squeeze Out Other Public Spending Priorities
51
MASSACHUSETTS STATE BUDGET, FY2001 VS. FY2011
SOURCE: Massachusetts Budget and Policy Center Budget Browser.
STATE SPENDING (BILLIONS OF DOLLARS) FY2011FY2001
+$5.1 B(+59%)
-38% -33%
-15%
-23%
-13%
-50%
-11%
-$4.0 B(-20%)
Health Care Coverage(State Employees/GIC;
Medicaid/Health Reform)
PublicHealth
MentalHealth
Education Infrastructure/Housing
HumanServices
LocalAid
PublicSafety

How does this compare to homeless individuals in Massachusetts?
Lack of data tracking homeless individuals Starting point becomes obtaining data
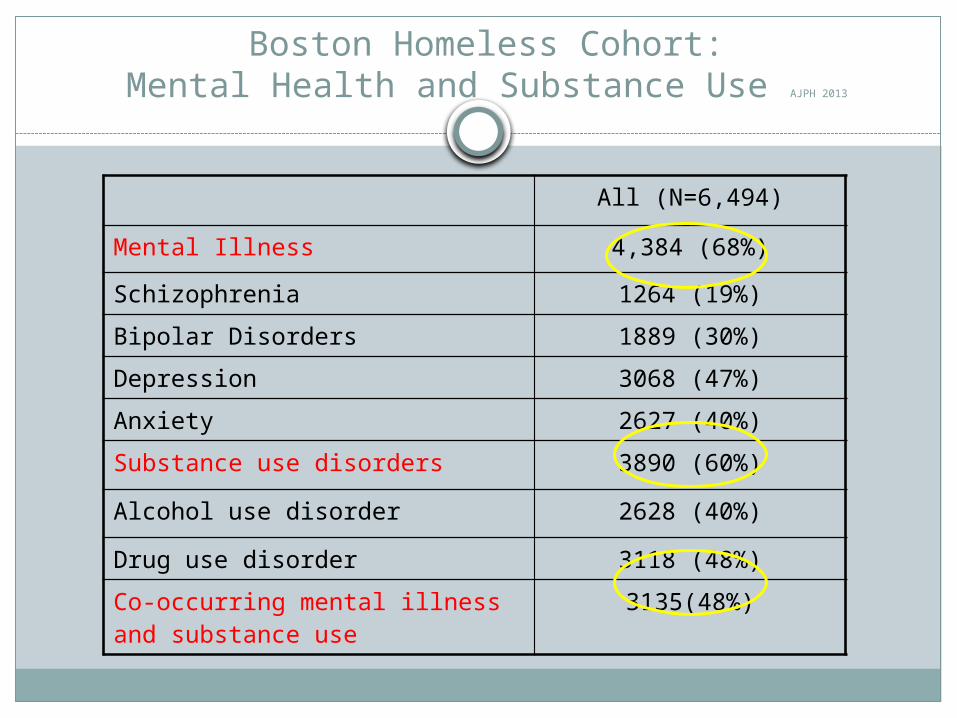
Boston Homeless Cohort:Mental Health and Substance Use AJPH 2013
All (N=6,494)
Mental Illness 4,384 (68%)
Schizophrenia 1264 (19%)
Bipolar Disorders 1889 (30%)
Depression 3068 (47%)
Anxiety 2627 (40%)
Substance use disorders 3890 (60%)
Alcohol use disorder 2628 (40%)
Drug use disorder 3118 (48%)
Co-occurring mental illness and substance use
3135(48%)

Boston Homeless Cohort:Selected Chronic Physical Conditions AJPH 2013
18
10
37
26
4
6
23
0 10 20 30 40Diabetes
Ischemic HD
HTNAsthma/COPD
Cirrhosis
HIV
Hep C
Ch
ron
ic C
on
dit
ion
Percentage
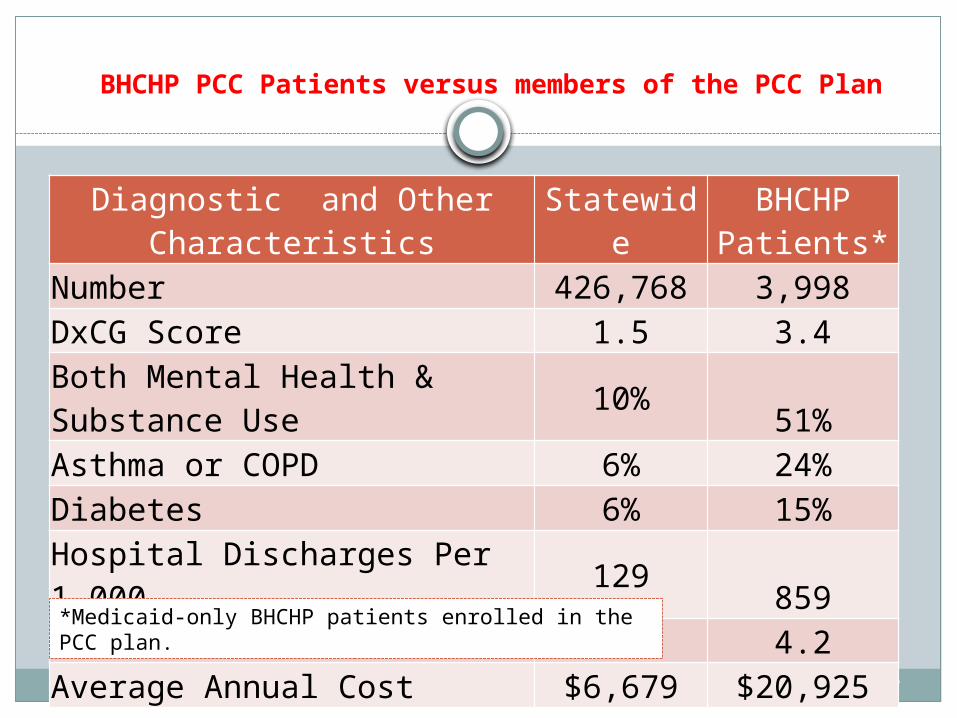
BHCHP PCC Patients versus members of the PCC Plan
Bharel et al, AJPH 2013
Diagnostic and Other Characteristics StatewideBHCHP
Patients*Number 426,768 3,998DxCG Score 1.5 3.4Both Mental Health & Substance Use 10% 51%Asthma or COPD 6% 24%Diabetes 6% 15%Hospital Discharges Per 1,000 129 859ED Visits Per Person 1.1 4.2Average Annual Cost $6,679 $20,925
*Medicaid-only BHCHP patients enrolled in the PCC plan.

Total Annual Expenditures by Expenditure Group for BHCHP Users with Medicaid in 2010
Users (N=6,493) Expenditures ($149 million)0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
25.0%
1.4%
25.0%
6.5%
25.0%
18.6%
15.0%
25.5%
10.0%
48.0%
Total Annual Expenditures by Expenditure Group for BHCHP Users with Medicaid, CY 2010
90 – 100% (650 users)
75 – 90% (974 users)
50 – 75% (1,623 users)
25 – 50% (1,623 users)
Lowest 25% (1,623 users)

Health Care Utilization and Housing
Studies in New York, Seattle and Chicago have found that housing homeless individuals can decrease use of services including: Emergency department Hospital inpatient Detoxification services
Am J Public Health. Apr 2004, JAMA. Apr 1 2009, JAMA. May 6 2009.

A Framework for Preparing for Health Care Reform at your Program
Clearly defining the issueHaving data and knowing the factsUsing the data to be involved early in
processUnderstanding that change is hardWorking collaborativelyBe willing to be in it for the long run

Long History of Reform in Massachusetts
1997
• Medicaid 1115 waiver to expand Medicaid, including MCO development
2006
• Comprehensive Health Reform: shared individual and state government, responsibility for access
2007
• Despite a recession, Massachusetts succeeds at having the lowest rate of uninsured in the nation
2012
• Chapter 221 passed with focus now on cost containment while providing high quality care
2013
• One Care Program begins to coordinate care for dual eligible patients (both Medicaid and Medicare)
2014
• Primary Care Payment Reform beings to coordinate behavioral health and primary care services in a global payment to primary care practices
One Care: Medicaid Plus Medicare
• October 2013• MA launched program to integrate care and align
financing for dual eligible patients• Interdisciplinary Care Teams develop patient care
plans and covered services include primary care, BH, specialty care, dental, vision ,medications and long term care.
• March 2014• 9,722 members have enrolled• Payments remain fee-for-service with a supplemental
payment for care coordination and management

Primary Care Payment Reform Initiative (PCPRI)
• Chapter 221 requires transition of Medicaid patients from fee-for-service to alternate payment methods with 80% transformation by July 2015
• PCPR is an alternative payment program where primary care providers are held accountable for cost and quality of care using a BH integration model and patient centered medical home.
• Payments are risk adjusted per member per month global payments
• Goal of delivery system to increase care coordination and care management, improve access to primary care, integrate BH and practice population management

Collaborator Issue
Local community organizations
Academic medical centers
MedicaidExecutive Office of
Health and Human Services
Elected Officials
Special populationAttribution of care
issueMedical respite
needsBH integration
needs
Using the data to advocate
A Framework for Preparing for Health Care Reform at your Program
Clearly defining the issueHaving data and knowing the factsUsing the data to be involved early in processUnderstanding that change is hardWorking collaborativelyBe willing to be in it for the long run

Opportunities Flexibility in clinical
design Flexibility in outreach
model Behavioral health and
primary care integration
Coordination across the health care system
Challenges Change is hard Uncharted territory Attribution of patients Risk adjustment is not
adequate Taking on risk at
provider level Want clinical staff to
remain blind to insurance type
Payment Reform and Health Care for Homeless Individuals

A Framework for Preparing for Health Care Reform at your Program
Clearly defining the issueHaving data and knowing the factsUsing the data to be involved early in processUnderstanding that change is hardWorking collaborativelyBe willing to be in it for the long run

Collaborations: who else is a stakeholder?
Neighborhood hospitals and academic medical centers
State MedicaidState Legislators/local politicians Consumer advocacy groupsOther organizations caring for special
populationsNational advocacy groupsShelter alliancesAnd more….

A Framework for Preparing for Health Care Reform at your Program
Clearly defining the issueHaving data and knowing the factsUsing the data to be involved early in processUnderstanding that change is hardWorking collaborativelyBe willing to be in it for the long run

Mission Statement:
Photos courtesy of J O’Connell
Provide and assure access to quality health care for all homeless individuals and families in the greater Boston area.

QUESTIONS AND ANSWERS
For more informationwww.nhchc.orgwww.nachc.orgwww.ncsl.org

THANK YOU FOR YOUR PARTICIPATION
Upon exiting you will be prompted to complete a short online survey. Please take a minute to complete the survey to evaluate
this webinar production.