malassezia furfur folliculitis in cancer patients. the need for
TRANSCRIPT

ANNALS O F CLINICAL AND LABORATORY SCIENCE, Vol. 23, No. 5Copyright © 1993, Institute for Clinical Science, Inc.
M alassezia fu rfu r Folliculitis in Cancer PatientsThe Need for Interaction of Microbiologist, Surgical Pathologist, and Clinician in Facilitating Identification by the Clinical Microbiology Laboratory*
RAMON L. SANDIN, M.D., M.S.,f TZANN-TARN FANG, M.D.,* JOHN W. HIEM EN Z, M .D.,t
JOHN N. GREENE, M.D.,§ LINA CARD, M.T. (ASCP),t
ALEXANDRA KALIK, M .D.,t and JENO E. SZAKACS, M .D.t
Departments of Pathology, f Bone Marrow Transplant Service,tand Infectious Diseases,§
H. Lee Moffitt Cancer Center and Research Institute, University of South Florida, Tampa, Florida 33612-9497
ABSTRACTMalassezia fu r fu r (MF) is a lipophilic yeast which can be found as a
m em ber of the indigenous microbiota of human skin. In immunocomprom ised transplant patients, MF can cause a distinctive folliculitis which is a clinical look-alike to Candida folliculitis, the latter of more potentially devastating significance. Recovery of MF in culture is dependent upon the addition to culture m edia of an exogenous source of fatty acids, such as olive oil. The addition of an extra Sabourauds plate with an olive oil overlay to the routine set of media used to inoculate all skin biopsy specimens in order to detect MF is labor-intensive and not cost-effective. Thus, MF may not be isolated in cases of MF folliculitis unless the clinical microbiology laboratory is pu t on alert by the clinical suspicions of the attending physician, or by histopathologic findings suggestive of folliculitis revealed by review of surgical pathology slides. The clinical, pathological, and microbiological findings of two cases of MF folliculitis are presented where an interactive approach featuring communication betw een the microbiologist, the surgical pathologist, and the clinician guided the microbiology laboratory to the isolation and identification of isolates of MF that were clinically- relevant. These cases underscore how a combined approach which features communication betw een the laboratory and the clinical services always provides superio r gu idance in the diagnosis and therapy of in fectious diseases.
* Send reprint requests to: Ramon L. Sandin, M.D., Room 2071 Pathology, H. Lee Moffitt Cancer Center, 12902 Magnolia Drive, Tampa, FL 33612-9497.
3770091-7370/93/0900-0377 $01.20 © Institute for Clinical Science, Inc.
3 7 8 SANDIN, FANG, HIEM ENZ, GREENE, CARD, KALIK, AND SZAKACS
Introduction
Malassezia fu r fu r (MF) is a lipophilic yeast, which is a m em ber of the indigenous m icrobiota of the skin of many warm-blooded hosts.5 Growth of MF on culture m edia is dep en d en t upon the ad d itio n of an exogenous sou rce of medium- to long-chain fatty acids, such as olive oil. Malassezia fu r fu r can cause an erythematous papulopustular folliculitis that may be more common than is rec- o g n i z e d in i m m u n o s u p p r e s s e d patients4,5,7 and which m ust be differentiated from the macronodular lesions of d issem ina ted cand id iasis , as w ell as other conditions.1,5,6, Since distinction
from these other conditions on purely clinical grounds is not always feasible, one a lte rn a te approach to d iagnosis would be to add an extra Sabourauds plate with an olive oil overlay to the routine set of media inoculated with specimens from the skin.
This global approach, however, would be labor-intensive and neither wise nor cost-effective, since the mere recovery of MF from skin biopsies may be hard to interpret in the absence of clinical suspicion, patient history or of histopathologi- cal findings suggestive of a frank follicul it is . S u b s e q u e n tly , an in te ra c t iv e approach which features communication betw een the microbiologist, the surgical
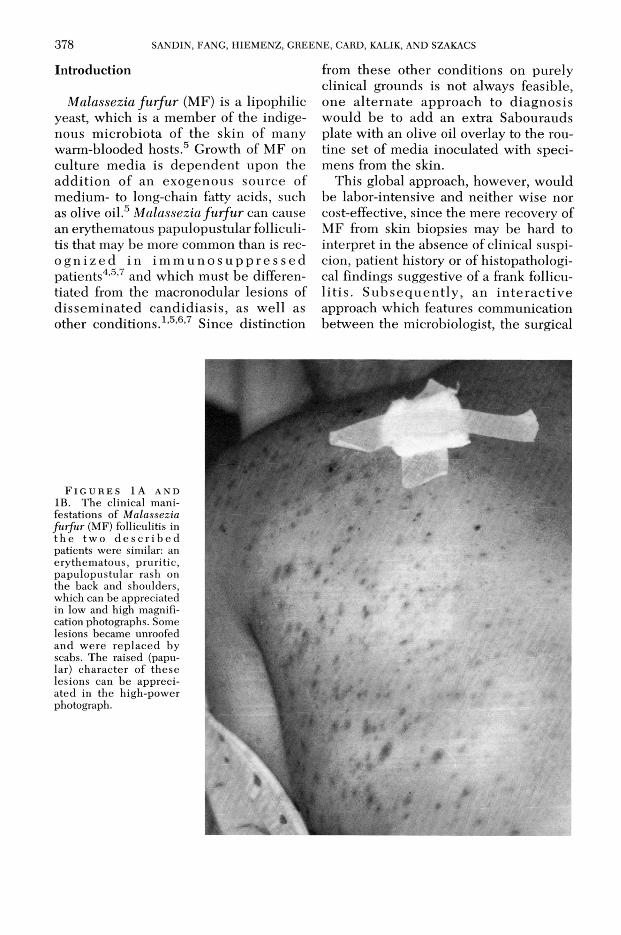
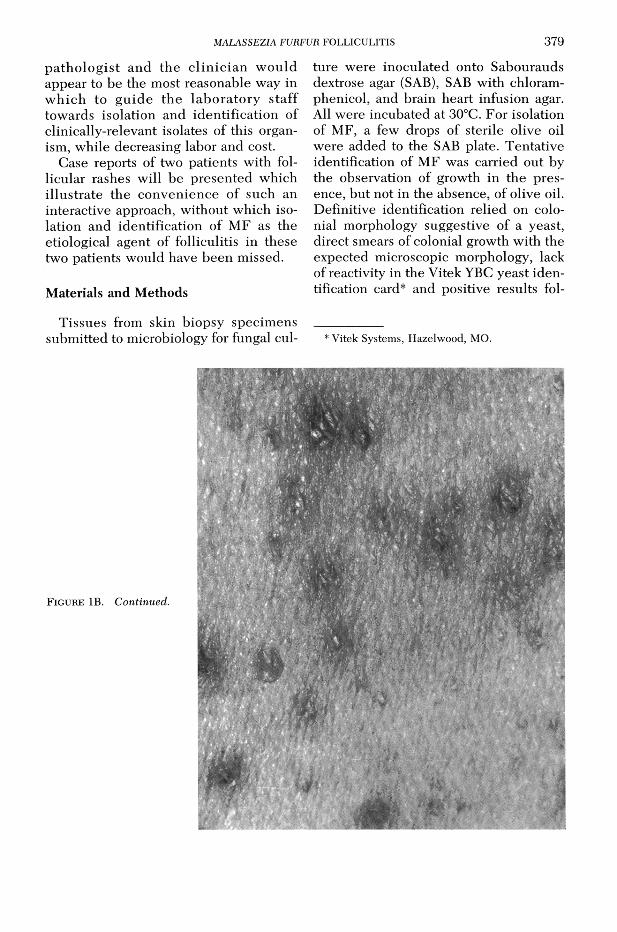
F i g u r e s 1 A a n d IB. The clinical manifestations of Malassezia furfur (M F ) folliculitis in th e tw o d e s c r i b e d patients were similar: an erythem atous, pruritic, papulopustular rash on the back and shoulders, which can be appreciated in low and high magnification photographs. Some lesions became unroofed and w ere rep laced by scabs. The raised (papular) character of these lesions can be appreciated in the high-power photograph.
MALASSEZIA FURFUR FOLLICULITIS 3 7 9
p a th o lo g is t and the c lin ic ian w ould appear to be the most reasonable way in w h ich to g u id e th e lab o ra to ry staff towards isolation and identification of clinically-relevant isolates of this organism, while decreasing labor and cost.
Case reports of two patients with follicular rashes will be presented which illustrate the convenience of such an interactive approach, w ithout which isolation and identification of MF as the etiological agent of folliculitis in these two patients would have been missed.
Materials and Methods
Tissues from skin biopsy specim ens subm itted to microbiology for fungal cul
ture were inoculated onto Sabourauds dextrose agar (SAB), SAB with chloramphenicol, and brain heart infusion agar. All were incubated at 30°C. For isolation of MF, a few drops of sterile olive oil were added to the SAB plate. Tentative identification of MF was carried out by the observation of growth in the presence, but not in the absence, of olive oil. Definitive identification relied on colonial morphology suggestive of a yeast, direct smears of colonial growth with the expected microscopic morphology, lack of reactivity in the Vitek YBC yeast identification card* and positive results fol
* Vitek Systems, Hazelwood, MO.
F i g u r e IB . Continued.

380 SANDIN, FANG, H IEM EN Z, GREENE, CARD, KALIK, AND SZAKACS
lowing the rapid urea test. Skin biopsy specim ens sen t to surgical pathology were formalin-fixed, paraffin-embedded, and stained with hematoxylin and eosin (H & E), gom ori-m ethenam ine silver stain (GMS), and periodic acid-Schiff stain (PAS).
Case Reports
Case #1
A 34-year-old white female with breast cancer metastatic to bone was first diagnosed in January1991. The patient had initial response to cyclophosphamide, adriamycin, and 5-fluorouracil systemic chemotherapy but showed progressive disease by October 1991, as evidenced by increased bone pain, worsening metastatic disease on bone scan, and rising tumor markers (CEA and CA 15-3). The patient was referred to the H. Lee Moffitt Cancer Center at the University of South Florida and relapse therapy was begun with standard dose ifosfamide, carbo- platinum , and etoposide. After docum enting response the patient underwent peripheral stem cell harvest after intravenous cyclophosphamide.
The patient was admitted to the bone marrow transplant unit on April 1, 1992 for high dose chemotherapy and peripheral blood stem cell rescue. On admission, the patient was found to be well developed and in no acute distress. She was afebrile with stable vital signs. No skin rash or lesions were seen. There was no adenopathy. Admission laboratory exam revealed a white blood cell (WBC) count of 3,100 and an actual neutrophil count (ANC) of 2,100. Renal and liver functions were normal. Preadmission scans revealed boney metastatic disease and were otherwise unremarkable.
Therapy was begun with high dose ifosfamide, carboplatinum, and etoposide daily for six days. Treatment was delivered in a single patient hospital room equipped with laminar air flow and HEPA filters. Nystatin was used for oropharyngeal candidiasis prophylaxis, and aerosolized pentamidine for Pneumocystis carinii prophylaxis. No systemic antibacterial or antifungal prophylaxis was utilized. After completion of chemotherapy, two days were allow ed for d rug e lim ination , and cryopre- served stem cells were then thawed and reinfused intravenously.
The patient tolerated chemotherapy relatively well except for nausea controlled with antiemetics and dexamethasone. Peripheral blood counts fell and the patient had her first fever to 38°C the day before transplantation. Cultures were obtained and broad spectrum antibiotic coverage with ceftazidime and vancomycin was begun. The day following transplantation a follicular skin rash over the shoulders, neck and back appeared (figure 1A & IB). Fevers persisted and metronidazole was added for anaerobic coverage with the development of
enteritis and mucositis. Owing to persistent fevers, empiric antifungal coverage with amphotericin B was begun five days post transplant. By this time, the skin rash had begun to resolve. Skin biopsy suggested fungus; however, the rash had significantly improved before cultures of the skin biopsy grew Malassezia furfur. By day 10 post transplant, WBC was 1,200 and the ANC was >500 per mm3. The patient defervesced and was subsequently discharged from hospital 19 days post-transplant with her rash resolved.
Case #2
A 22-year-old white female presented with a history of Burkitt’s lymphoma of the distal ileum diagnosed at laparotomy. After resection of the tumor, the patient was treated with five cycles of cyclophosphamide, adriamycin, vincristine, and prednisone along with prophylactic intrathecal methotrexate. The patient did well off therapy from January to March 1992 when she was noted to have a mandibular and intra-abdominal relapse with retroperitoneal and mesenteric adenopathy. Reinduction was accomplished with high dose cytosine ara- binoside and cisplatinum in April 1992. The patient subsequently was referred to the H. Lee Moffitt Cancer Center and received two cycles of standard dose chem otherapy w ith ifosfam ide, carbop la tinum , and e to p o sid e ach iev in g a com plete remission.
In order to minimize the risk or relapse, the patient was admitted to the bone marrow transplant unit in July 1992 for high dose chemotherapy and autologous bone marrow transplantation. On admission, examination revealed the patient to be a well developed, well nourished young female in no distress. There were no skin rash or lesions. Head and neck exam showed resolution of the mandibular tumor and no other abnormalities. Admission laboratory evaluation revealed WBC 7,200 and ANC 6,300. Chemistry panel was unremarkable with normal renal and liver functions. Preadmission computerized tomography showed resolution of previous adenopathy.
Upon admission, the patient underwent harvest of 922 ml of bone marrow from the posterior iliac crests. The following day she began high dose chemotherapy with ifosfamide, carboplatinum, and etoposide given daily for six days. After two days of rest for drug elimination, cryopreserved bone marrow was thawed and reinfused intravenously. All therapy was delivered in a single bed hospital room equipped with laminar air flow and HEPA filters. Nystatin was used for local oropharyngeal Candida prophylaxis, and aerosolized pentam idine was given for Pneumocystis carinii prophylaxis. No system ic antibacterial or antifungal prophylaxis was utilized.
By completion of chemotherapy, two days before transplantation, WBC had fallen to 2,000 and a follicular rash was noted on the shoulders. The first fever occurred on the day of transplantation and empiric broad spectrum coverage with ceftazidime

MALASSEZIA FURFUR FOLLICULITIS 381
and vancomycin was begun after cultures were obtained. The follicular rash had spread to involve the upper chest but was otherwise asymptomatic. Daily fevers from 38°C to 38.5°C persisted, and metronidazole was added for anaerobic coverage in the setting of worsening mucositis. Skin biopsy was obtained and clotrimazole cream was begun. Owing to persistent fevers in the setting of prolonged neutropenia, empiric antifungal coverage was initiated10 days after transplant with fluconazole. By this time, the follicular rash had already begun to fade before systemic antifungal therapy had been started. Over the next week the rash continued to resolve and bone marrow recovered with an ANC of >500 per mm3 by day 18 after transplantation. All antibiotics were discontinued and the patient was discharged for outpatient followup. The rash had begun to fade once culture results identified Malas- sezia furfur.
Microbiologic and Pathologic Findings
Tissue sent to microbiology from the skin biopsy on patient # 1 failed to show growth after two days of incubation in the absence of olive oil (figure 2A). At that time, review of the H & E slides by the microbiologist, upon requests by the surgical pathology resident, revealed acute fungal folliculitis, with fibrinoid necrosis of one of the walls of the hair follicles, but w ithout inflammatory cells. W ithin the infundibulum of the hair follicle in the necrotic areas, there were m ultiple round yeasts which were highlighted by the PAS (figure 3) and GMS stains. The yeasts w ere sm all w ith un ipo lar and broad-based budding, and a small circ u m fe re n tia l th ic k e n in g at th e b u d attachment. Hyphae and pseudohyphae were absent.
Given such histopathologic findings suggestive of M F, the m icrobiologist requested that the medical technologist add a few drops of sterile olive oil to the plates and spread them over the inoculum. W ithin two days following olive oil addition, the previously negative fungal plates were overrun with small, white, creamy colonies of variable sizes (figure 2B). A w et m ount p repared from the growth on the plate showed small yeasts with unipolar and broad-based budding, and collarettes. The VITEK YBC cards
were set up and were completely unreactive. A rapid urea test was set up and the m ed ium tu rn e d p o s itiv e (re d -p in k ) w ithin a few hours. Besides MF, several species w ithin the genera Cryptococcus, Rhodotorula, and Trichosporon are also urease positive. The latter three genera, however, can be ruled out on the basis of: (1 ) growth in the absence of added oliveoil, (2) their own particular colonial and microscopic morphologic characteristics, and (3) specific patterns of reactivity in the VITEK YBC card.
Specim ens from the skin biopsy on case # 2 w ere inoculated onto fungal media with olive oil from the start, given the clinical suspicion of the astute clinician who alerted the microbiologist prior to the biopsy procedure. W ithin three days, yeast colonies were identified with ch arac te ris tic s id en tic a l to th o se o f p a tie n t # 1 . T he su rg ica l p a th o lo g y specim en from p a tien t # 2 , how ever, failed to reveal the p resence of fungal microorganisms.
Discussion
M a la s s e z ia f u r f u r is a com m o n lipophilic fungal saprophyte of hum an skin that is known to cause the superficial dermatosis tinea (or pityriasis) versicolor, as well as a distinctive folliculitis.5 On occasion, a deep-seated infection may occur particularly in deb ilita ted hosts with central catheters who are receiving intravenous lipid therapy .5 Several studies have established the high incidence of MF skin carriage on normal-appearing skin of the scalp, shoulders and chests of adults.5
The entity of MF folliculitis is probably a more common clinical problem than is currently appreciated and is of particular importance to clinicians because of its potential for confusion with life- th rea ten ing fungal in fec tions .1’5,6,7 It occurs predominately in post-adolescents as opposed to acne vulgaris w hich it
3 8 2 SANDIN, FANG, H IEM EN Z, GREENE, CARD, KALIK, AND SZAKACS
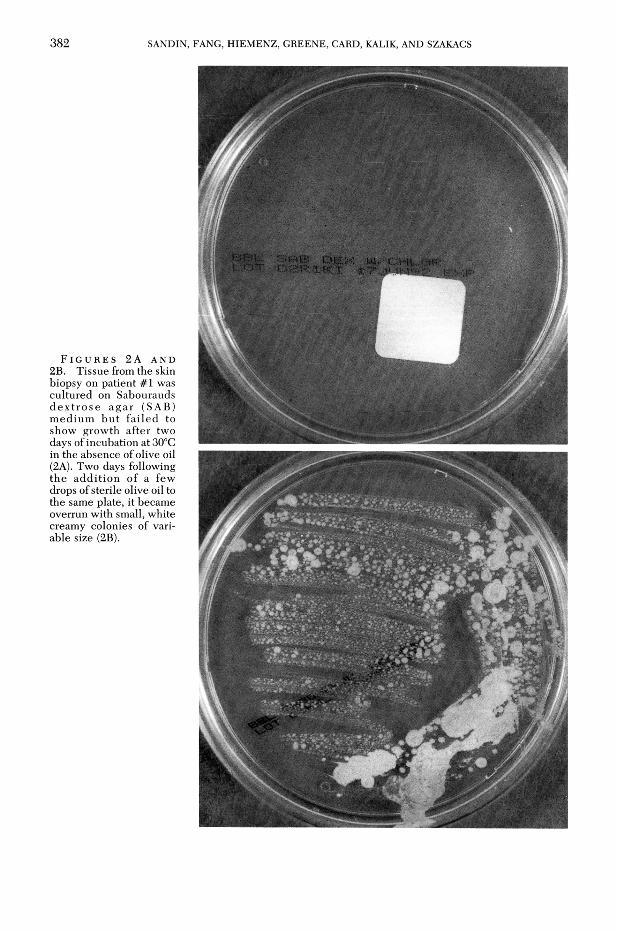
F i g u r e s 2A a n d 2B. Tissue from the skin biopsy on patient # 1 was cultured on Sabourauds d e x tro s e ag a r (SAB) m edium b u t fa iled to show growth after two days of incubation at 30°C in the absence of olive oil (2A). Two days following the add ition of a few drops of sterile olive oil to the same plate, it became overrun with small, white creamy colonies of variable size (2B).

MALASSEZIA FURFUR FOLLICULITIS 3 8 3
F i g u r e 3 . Surgical pathology tissue slides from patient # 1 showed fibrinoid necrosis of the hair follicle walls and the p re s e n c e w ith in th e infundibulum of multiple round yeasts with unipolar broad-based budding. This was highlighted by the periodic acid-Schiff (PAS) and gomori-methe- nam ine s ilv e r (GMS) stains. (PAS stain, lOOOx magnification).
resem bles.5 Many patients with M F folliculitis have underlying debilitative diseases or conditions, such as diabetes mel- l i t u s , c a n c e r , b o n e m a r r o w transplantation , and steroid or broad- spectrum antibiotic administration.1,5
As represented by both cases, lesions o f M F fo llicu litis are usually m ultiple and are distributed over the back, shoulders and/or upper c h e s t .1,5 B iopsy o f affected hair follicles shows a spectrum of pathological findings, from plugging of the hair follicle to frank destruction of the follicular wall with fibrinoid necrosis, as seen in patient # 1 . An infundibular infiltrate consisting of polym orphonuclear and m o n o n u clear leu k o cy tes may or may not be present and was absent in patient # 1 .
W ithin the hair follicle, numerous budding yeasts are usually present without h y p h a l or p se u d o h y p h a l fo rm s, as opposed to C andida which features both filamentous and yeast forms in tissue in cases of deep or disseminated infection (figure 3). An intensely pruritic eosinophilic pustular folliculitis associated with abundant M F yeasts inside hair follicles has also b een associated w ith A ID S p a tie n ts .2 S tu d ies u tiliz in g e le c tr o n microscopy have suggested that follicular occlu sion may be a prim ary ev en t in th e d ev e lo p m en t o f M F fo l lic u li t is , w ith y east overgrow th as a se co n d ary phenom enon.3
The lesions of M F folliculitis are to be contrasted with those of d issem inated can d id iasis , w hich are c lin ic a l look-

384 SANDIN, FANG, H IEM EN Z, GREENE, CARD, KALIK, AND SZAKACS
alikes but are of a much graver significance.1,5,6 The m acronodular lesions of dissem inated candidiasis may be located anywhere on the body but have predilection for the extremities, whereas candidal p a p u lo p u s tu lo s is is m ost com m only found in heroin addicts and most frequently in the bearded area, shoulders, and chest.5 Candida also favors intertrigi- nous moist areas such as the groin, axilla and skin folds, particularly in diabetics and obese patients. Satellite lesions are common as well. Both types of candidal lesions yield the responsible fungus if biopsy m aterial is p laced on standard fungal cu ltu re m edia, w hereas tissue from MF folliculitis requires the lipid supplem entation already alluded to. Surgical pathological examinations in MF folliculitis may disclose the presence of yeasts w ithin the follicular infundibulum and perhaps w ithin the surrounding ep iderm is, b u t w ithout the deep derm al invasion w hich may be observed frequen tly w ith infections by C andida.6 D e s tru c tio n o f th e h a ir fo ll ic le is also possible.
The approach followed in the clinical microbiology laboratory at our institution is a conservative one. It relies on feedback from the surgical pathology resident or attending, and/or clinical attending or fellow, in order to alert the laboratory that a particular specim en from skin is to be tested for the presence of this organism. This is superior to any approach requiring that an additional fungal plate with an olive oil overlay be part of the work-up of all skin biopsy specim ens.
This approach can be adapted by some institutions, and is perhaps already being practiced in many others. It underscores to la b o ra to r ia n s th a t a c o m b in e d approach to patient care, where continual communication exists betw een pathology and the clinical services, provides super io r g u id an ce in th e d iag n o sis and th e ra p y o f in fe c tio u s an d n e o p la s tic diseases.
References
1. B u f i l l , J. A., L u m , L . G., C a y a , J. G., C h i - TAMBAR, C . R ., RlTCH, P . S., ANDERSON, T ., and ASH, R. C.: Pityrosporum folliculitis after bone marrow transplantation. Clinical observations in five patients. Ann. Int. Med. 108:560— 563, 1988.
2. F e r r a n d iz , C ., R ib e r a , M., Ba r r a n c o , J. C ., C l o t e t , B ., and L o r e n z o , J. C .: Eosinophilic pustular folliculitis in patients with acquired immunodeficiency syndrome. Intern. J. Dermatol. 31:193-195, 1992.
3. H il l , M. K., G o o d f ie l d , M. J. D., R o d g e r s ,F. G ., C r o w l e y , J. L., and Sa ih a n , E. M.: Skin surface electron microscopy in Pityrosporum folliculitis. The role of follicular occlusion in disease and the response to oral ketocona- zole. Arch. Dermatol. 226:1071-1074, 1990.
4. J a c in t o -Ja m o r a , S., T a m e s is , J ., and Ka t ig - b a k , M. L.: Pityrosporum folliculitis in the Philippines: Diagnosis, prevalence and management. J. Am. Acad. Dermatol. 24:693-696,1991.
5. Kl o t z , S. A.: Systemic fungal infections: Diagnosis and treatment. II. Malassezia furfur. Infect. Dis. Clin. North Amer. 3:53—64, 1989.
6 . Kl o t z , S. A., D r u t z , D . J., H u p p e r t , M., and JOHNSON, J. E.: Pityrosporum folliculitis. Its potential for confusion with skin lesions of systemic candidiasis. Arch. Intern. Med. 142: 2126-2129, 1982.
7. MARCON, M . J. a n d POW ELL, D. A.: H u m a n in fec tio n s d u e to M a la sse z ia sp p . C lin . M ic ro b io l. R evs. 5:101-119, 1992.