mammary paget disease (mpd) & extramammary paget disease (empd)
TRANSCRIPT

MAMMARY PAGET DISEASE (MPD)



MAMMARY PAGET DISEASE (MPD)/ PD OF THE NIPPLE/ PD OF THE BREAST
MPD is an uncommon skin malignancy
characterized by a chronic eczema-like
lesion of the nipple and adjacent areolar
skin.

MAMMARY PAGET DISEASE (MPD)/ PD OF THE NIPPLE/ PD OF THE BREAST
A progressive, well marginated (well
circumscribed), chronic eczematous change
due to invasion of the epidermis by malignant
Paget cells.
Paget cells originate in either invasive intraduct
carcinoma or ductal carcinoma in-situ (DCIS) of
in the deeper breast tissue.

A 55-year-old woman presented with one year history of unilateral
pruritic eczema-like rash confined to the areolar area of one breast.

MPD
A similar condition that involves the skin of the anogenital
regions of female and male where there are an abundance
of apocrine glands is known as extramammary Paget disease
(EMPD).


INCAIDENCE OF MPD

INCIDENCE OF MPD
Uncommon, 1-4% of female breast carcinoma cases are associated with PD of the nipple, the areola, and the surrounding skin.
Almost exclusively in ♀ involvement of the male breast is rarely reported.
Is most frequent in the 5th and 6th decade mean age at diagnosis of 55 years.
Nearly 100% of mammary PD cases are associated with an underlying carcinoma, either invasive intraduct carcinoma(90%) or ductal carcinoma in-situ (10%).

ETIOLOGY OF MPD

ETIOLOGY OF MPD
Intraepidermal extension of malignant ductal
epithelial cells (Paget cells) through the
lactiferous ducts and ductules into the
epidermis (EPIDERMOTROPISM) infiltrate
and proliferate in the epidermis.

ETIOLOGY OF MPD
PAGET
CELLS
Glandularstemcells
Epi-dermalTokercells

ETIOLOGY OF MPD
PAGET CELLS MAY BE DERIVED FROM:
1. GLANDULAR STEM CELLS:
Paget cell share similar immunohistochemical characteristics with
eccrine and apocrine sweat gland epithelium.
Paget cells are periodic acid-Schiff (PAS) positive and diastase
resistant; and they are Alcian blue positive or…..

ETIOLOGY OF MPD
PAGET CELLS MAY BE DERIVED FROM:
2. EPIDERMAL TOKER CELLS (clear cells of the nipple epithelium):
Due to the similarity of the immunophenotypes.
Toker cells have been found in about 10% of normal nipples and
rarely in supernumerary nipples and apocrine bearing areas.
Like Paget cells of both mammary and extramammary sites, Toker
cells contain prominent clear (vacuolated) cytoplasm, and they are
considered benign counterparts of Paget cells & sometimes
proliferate, resulting in a condition known as clear cell papulosis.


C/P OF MPD



Paget's disease. Images macroscopic woman than 50 years that had
significant areolar eczema in the left region, which had been increasing in
the last six months, accompanied by itching. See as there accompanying
nipple retraction.


A 15yr old girl presented to the clinic with complaints of itching in the
nipple area of left breast for the past 2 years.

Showing an ulcerated erythematous plaque covering whole of the left
breast, the sub mammary area and adjacent part of abdominal wall,
covered with purulent to hemorrhagic crusts

Erythema, erosions and bloody discharge of 20 years old female

C/P OF MPD
SYMPTOMS 1. Nipple rash
2. Redness
3. Itching – Burning - pain
4. Oozing or Bloody Nipple discharge
5. Nipple retraction
6. Scaling- Crusting of skin
7. Swelling
8. Ulceration

C/P OF MPD
PHYSICAL EXAMINATION AT EARLY STAGE: The lesion usually begins at the nipple and gradually spread to the areola.
The early changes may be minimal, with a unilateralsmall, crusted and intermittently moist area on the nipple giving a brownish stain on clothing, or producing itching, pricking or burning sensations. Less often, there is a serous or blood-staineddischarge from the nipple, or a lump may be noticed in the breast.
The surface changes persist and gradually spread to produce an eczematous appearance.

C/P OF MPD
PHYSICAL EXAMINATION AT A LATER STAGE: Skin of the breast is erythematous and moist or crusted sharplymarginated, indurated & thickened plaques and may spare a segment of the areola.
The edge is slightly raised and irregular in outline.
If the crusts are removed, a red, glazed, moist or vegetating surfaceis revealed.
Itching may be a prominent symptom and excoriations may be found in the established lesion.
The nipple itself may be retracted, and a subjacent palpable massor a lump deeper in the breast may be felt. Nipple invagination is sometimes seen.

C/P OF MPD
The regional LN should be examined;
they are rarely enlarged when a mass
cannot be felt, but are enlarged in more
than half the cases with a detectable
tumor.

C/P OF MPD
The changes may occasionally involve not only the skin of
the breast but also spread on to the chest wall.
Poor prognosis is associated with invasive disease and the
presence of a palpable mass.

C/P OF MPD
Pigmented mammary PD and pigmentedextramammary PD are rare clinical entities in both males and females.
These diseases may mimic malignantmelanoma both clinically and histopathologically. They may also mimic melanoma on dermoscopic examination.
In pigmented lesions of PD, numbers of benign melanocytes are present, which may interfere with the correct diagnosis of PD.

DDx OF MPD

DIFFERENCE BETWEEN MPD & ECZEMA OF THE NIPPLE

DDx OF MPD
1) Eczema of the nipple
2) Bowen’s disease (very uncommon on the nipple)
3) Superficial BCC (very uncommon on the nipple)
4) Psoriasis
5) Amyloidosis
6) Erosive adenomatosis of the nipple.
7) Nipple duct adenoma
8) Drug Eruptions
9) Malignant melanoma


INVESTIGATIONS OF MPD

INVESTIGATIONS OF MPD
• Mammography
• MRI
• Ultrasound
I. Imaging: “3”

MPD: an area with microcalcifications in the lower inner left quadrant with
extension towards the nipple which shows retraction and some
calcifications within, there is also minimal extension towards the lower
outer left quadrant.

Paget's disease. Cranio-caudal mammograms of left breast of a patient diagnosed with Paget. Area of 10 cm that affects the external cuadrantswhich identifies multiple pleomorphic microcalcifications, very suspicious of malignancy, which at higher magnification (right) continue the road of
the nipple lactiferous duct (arrow)


MPD in right breast, unifocal, isolated in nipple.

BREAST PAGET DISEASE. 75 years old woman presenting a lesion in the
left nipple since 2 weeks ago. ULTRASOUND left retroareolar area:
where microcalcifications can be identied.

INVESTIGATIONS OF MPD
1. MAMMOGRAPHY:
Radiographic changes seen in MPD include the following: “4”
1. Subareolar microcalcifications (helpful in evaluating and locating
clinically occult, nonpalpable underlying breast carcinoma)
2. Architectural distortion
3. Thickening of the nipple and the areola (reflecting edema)
4. Nipple changes (in a minority of patients)
Negative preoperative mammography findings did not
reliably exclude an underlying carcinoma.

INVESTIGATIONS OF MPD
2. MRI of the involved breast can detect otherwise occult PD in
the setting of negative mammography findings.

INVESTIGATIONS OF MPD
3. ULTRASOUND to establish whether or not there is deeper
pathology in the underlying breast, as this will help determine
the extent of surgery required.

INVESTIGATIONS OF MPD
• Tzanck smear
• Biopsy of the tumor
• Sentinel lymph node biopsy
II. Tissue Analysis: “3”

INVESTIGATIONS OF MPD
TISSUE ANALYSIS: “3”
1. TZANCK SMEAR: The presence of large cells with a high nuclear-to-
cytoplasmic ratio, occasional acinar formation, and intracytoplasmic
vacuoles is diagnostic for malignant Paget cells.
2. BIOPSY OF THE TUMOR: Punch, wedge, or excisional biopsy.
3. SENTINEL LYMPH NODE BIOPSY: is performed in cases with an
invasive component.



Histopathological section showing large atypical round to oval cells
(arrow) infiltrating the lower part of epidermis having a pale cytoplasm
with prominent hyperchromatic nuclei

(A) The epidermis of the nipple infiltrated by large Paget’s cells with pale
abundant cytoplasm
(B) Single groups of Paget’s cells with vesicular nuclei and prominent
nucleoli


HISTOPATHOLOGY OF MPD
THE EPIDERMIS:
Hyperkeratosis or parakeratosis.
Acanthosis, with papillomatosis.
Enlargement of the rete ridges.
Characteristic Paget’s cells singly or in clusters (nests) are dispersed
between the prickle cells. They vary in number, and when profuse
the Malpighian layer may be disrupted and the surface covered by a
crust.
In the later stages, the epidermis may be atrophic or eroded.

HISTOPATHOLOGY OF MPD
Their ultrastructural features of Paget’s cells are those of
glandular epithelial cells it’s cytoplasm is PAS-positive &
packed with numerous rounded, membrane-bound mucin
granules.
Infiltration occurs by variable numbers of signet-ring forms
tumor cells that are present in all layers of the epidermis.
Mitotic figures are occasionally identified.

HISTOPATHOLOGY OF MPD
PAGET CELLS CLASSICALLY HAVE THE FOLLOWING HISTOLOGICAL FEATURES:
1. Large rounded or ovoid atypical cells
2. Abundant pale-staining cytoplasm
3. Mucin-positive
4. Enlarged, scattered mitochondria
5. Large rounded or ovoid vesicular-to-hyperchromatic nuclei with prominent nucleoli.
6. Scanty nuclear chromatin
7. They are devoid of intercellular bridges

HISTOPATHOLOGY OF MPD
In the ulcerated lesions of MPD, the epidermis is totally
replaced by Paget cells.
A large biopsy or excision may demonstrate the presence of
epidermal Paget cells and an underlying infiltrating or
intraductal carcinoma of the breast.
The Paget’s cells may also be seen in appendage ducts.
HISTOPATHOLOGY OF MPD
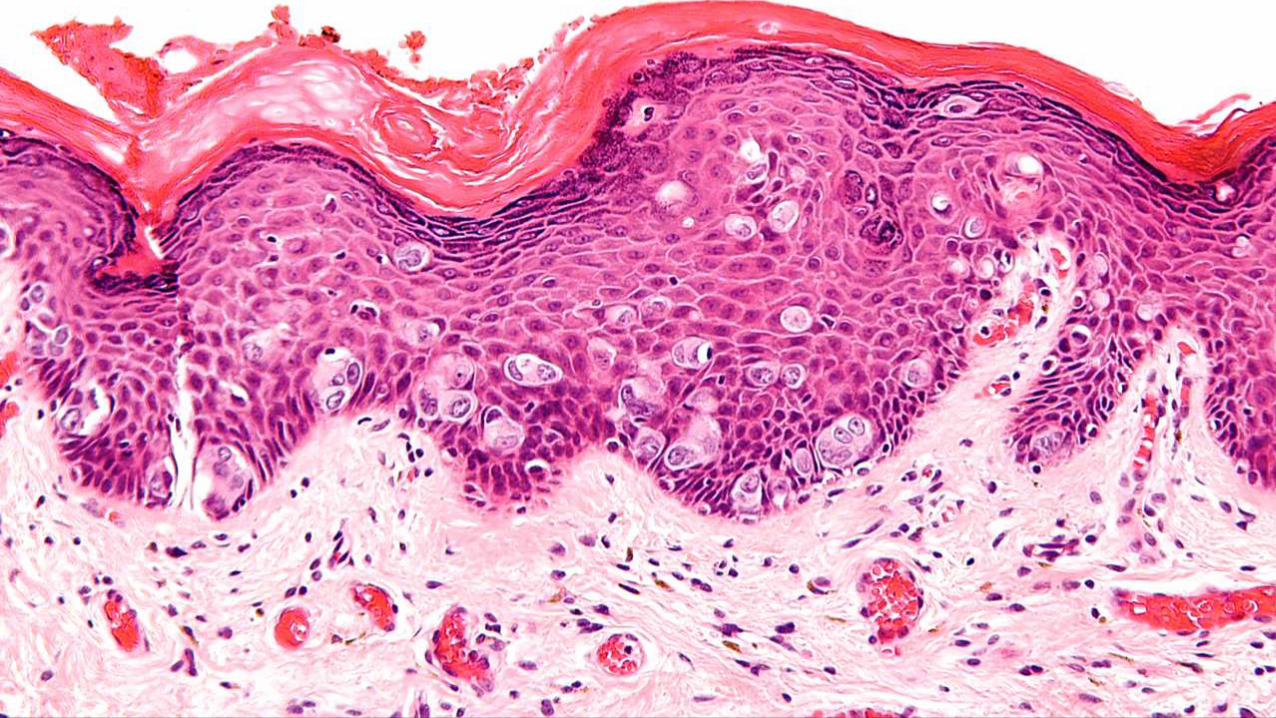
THE DERMIS chronic inflammatory reaction in the upper
dermis contains a dense infiltrate of lymphocytes, histiocytes,
plasma cells, and occasionally eosinophils.
AN UNDERLYING BREAST CARCINOMA may be seen on
large biopsy. The cells may accumulate within and distend
the ducts and spread in both directions. A number of ducts
are usually involved. At a later stage, the carcinoma becomes
invasive and behaves like classic breast carcinoma.

HISTOPATHOLOGY OF MPD
Several histologic variants of PD are as follows: “5”
1. Adenocarcinomalike cell type
2. Spindle cell type
3. Anaplastic cell type
4. Acantholytic cell type
5. Pigmented cell type

The clear appearance of cytoplasm in Paget’s disease is due to their
abundant content of neutral and acidic mucopolysaccharides which can
be demonstrated by PAS stain

The malignant cells are usually immunoreactive for Carcinoembryonic
antigen (CEA)

Immunohistochemistry showing positivity with epithelial membrane
antigen (EMA)

SPECIAL STAINS OF PAGET’S CELLS
1. PAS STAIN:
Paget’s cells shows PAS positive diastase-resistant granules,
indicating the presence of neutral mucopolysaccharides and
supports the glandular origin of the cells.
2. Alcian blue:
Positive.

IMMUNOHISTOCHEMISTRY
POSITIVE MARKERS OF PAGET'S CELLS ARE “5”:
1. CEA (Carcinoembryonic Antigen)
2. EMA (Epithelial Membrane Antigen)
3. CK7 Low molecular weight cytokeratins proposed as a specific and
nearly 100% sensitive marker for MPD.
4. CAM-5.2 (Cellular adhesion molecule) Glandular epithelial cell
markers.
5. erbB-2 (>90%)

IMMUNOHISTOCHEMISTRY
NEGATIVE MARKERS OF PAGET'S CELLS, which serve as
differentiating features from malignant melanoma “5”:
1. Anti-s-100 protein
2. Melan A (MART-1)
3. HMB-45
4. Tyrosinase
5. DOPA


STAGING OF MPD

STAGING OF MPD
Mammary Paget disease has been classified into 4 clinical stages
Stage 0 Lesion confined to the epidermis, without underlying in situ ductal
carcinoma of the breast
Stage 1 Associated with in situ ductal carcinoma just beneath the nipple
Stage 2 Associated with extensive in situ ductal carcinoma
Stage 3 Associated with invasive ductal carcinoma

Rx OF MPD

Rx OF MPD
I. Mastectomy (radical or modified) and LN clearance
II. Photodynamic therapy (PDT)
III. Conservative management

Rx OF MPD
I. Mastectomy (radical or modified) and LN
clearance in cases with palpable mass and
underlying invasive breast carcinoma.

Rx OF MPD
II. Photodynamic therapy (PDT) using aminolevulinic acid (5-
ALA) for low-risk malignant cells

Rx OF MPD
III. Conservative management: In patients with no evidence of
an underlying breast carcinoma. Combination of “3 measures”;
1. Local excision of the nipple,
2. Wedge resection of the underlying breast tissue,
3. Radiation therapy: according to the presence or absence
of an invasive component.


EXTRAMAMMARY PAGET DISEASE

EXTRAMAMMARY PAGET DISEASE
EMPD is an uncommon tumor characterized
by a chronic eczema-like lesion of the skin
around the anogenital regions of males and
females.
In women the most common area involved is
the vulva.
The clinical and the histopathological findings
are very similar to the more common type of
MPD.

Grossly inflamed erythema on the vulva extending to the perineum.
There were whitish cheesy lesions on the wall of the vagina. Superficial
erosions were noted on the left posterior area. Her regional nodes were
not enlarged.



This man presented with a pruritic, erythematous, scaly, eroded dermatitis-like rash involved the perianal area of two months duration.
Three months before rash appearance the patient had suffered constipation and many episodes of rectal bleeding. Sigmoidoscopy
disclosed rectal carcinoma whereas perianal skin biopsy was consistent with extramammary Paget's disease.

Extramammary Paget disease, gross. The patient’s lesion on the glans
penis.

Clinical presentation of the well-demarked pink erythematous patch in
the left axilla

EMPD HAS BEEN CLASSIFIED INTO SEVERAL SUBTYPES:
primary cutaneous extramammary Paget disease arises from apocrine glands within the epidermis (in situ) or underlying skin appendages
primary cutaneous extramammary Paget disease (15-25%) is associated with invasive Paget disease or adenocarcinoma in situ.
extramammary Paget disease originates from underlying anal or rectal adenocarcinoma
extramammary Paget disease originates from bladder adenocarcinoma
Type1a
Type 1b
Type 2
Type 3




Rx OF EMPD
Wide local excision, vulvectomy, or Mohs micrographic
surgery is the standard treatment.
Recurrence is common (30-50%), so patients should be re-
examined every 3 months after surgery for the next 2 years,
after which annual follow-ups are recommended.
Recurrence generally leads to further surgery.

Rx OF EMPD
Non-surgical treatments for recurrent disease may include:
1. Radiotherapy
2. Laser ablation
3. Photodynamic therapy
4. 5-fluorouracil cream
5. Imiquimod cream

REFERENCES
Rook 8th edition.
Bolongia 3rd edition.
Google images.
http://www.dermnetnz.org
www.facebook.com/groups/dermatologycourseonline/
