management accounting and supply chain performance of
TRANSCRIPT

UNIVERSITY OF GHANA
(College of Humanities)
Management Accounting and Supply Chain Performance of Healthcare
Institutions in Ghana
Nartey Edward
(10072443)
This thesis is submitted to the University of Ghana, Legon in partial fulfilment of the
requirement for the award of PhD Accounting degree
JUNE, 2018
University of Ghana http://ugspace.ug.edu.gh
i
DECLARATION
I, the undersigned, do hereby declare that this work is the result of my own research and has
not been presented by anyone for any academic award in this university or any other university.
All references used in the work have been fully acknowledged. I bear responsibility for any
shortcomings.
………………………………………… ……….………………….
NARTEY EDWARD DATE
University of Ghana http://ugspace.ug.edu.gh

ii
CERTIFICATION
I, the undersigned, do hereby certify that this thesis was supervised in accordance with the
procedures laid down by the university.
……………………………………………… …….………………
DR. FRANCIS ABOAGYE-OTCHERE DATE
……………………………………………… …….………………
DR. SAMUEL NANA YAW SIMPSON DATE
University of Ghana http://ugspace.ug.edu.gh

iii
DEDICATION
I dedicate this work to my two lovely boys: Nana and June
University of Ghana http://ugspace.ug.edu.gh

iv
ACKNOWLEDGEMENTS
Completing a major research effort would be virtually impossible without getting the energy
and strength given from above. First of all, I thank the almighty God for giving me the strength
to successfully complete this project. This project also couldn’t have seen the light without the
support and assistance from a number of special people. I especially appreciate the assistance
and insight from my supervisors Dr. Francis Aboagye-Otchere and Dr. Samuel Nana Yaw
Simpson who in diverse ways were invaluable in helping me progress through the various
iterations. I was always impressed about how responsive and focused they seem to be when I
need their input. Finally, I would like to express my profound gratitude to Professor Joshua
Abor, Dean of the Business School for his encouragement and support towards the successful
completion of this project.
University of Ghana http://ugspace.ug.edu.gh

v
TABLE OF CONTENTS
DECLARATION.................................................................................................................................... i
CERTIFICATION ................................................................................................................................ ii
DEDICATION...................................................................................................................................... iii
ACKNOWLEDGEMENTS ................................................................................................................ iv
TABLE OF CONTENTS ..................................................................................................................... v
LIST OF TABLES ............................................................................................................................... xi
LIST OF FIGURES ............................................................................................................................ xii
LIST OF ABBREVIATIONS ........................................................................................................... xiii
ABSTRACT ........................................................................................................................................ xiv
CHAPTER ONE ................................................................................................................................... 1
INTRODUCTION ................................................................................................................................. 1
1.1 Brief Overview of the Study ............................................................................................ 1
1.2 Research Background ....................................................................................................... 2
1.3. The Research Problem .................................................................................................... 5
1.4 Study Objectives ............................................................................................................ 10
1.5 General Research Questions........................................................................................... 10
1.6 Significance of the Study ............................................................................................... 11
1.7 Outline of Remainder of Thesis ..................................................................................... 13
1.8 Chapter Summary ........................................................................................................... 13
CHAPTER TWO ................................................................................................................................ 15
CONTEXTUAL BACKGROUND, MANAGEMENT ACCOUNTING SYSTEM DESIGN AND
THE HEALTH SUPPLY CHAIN ..................................................................................................... 15
2.1. Introduction ................................................................................................................... 15
2.2. Recent Studies on MAS Design and Hospital SC Performance ................................... 16
2.3 Ghana’s Health SCM System ......................................................................................... 18
2.4 Managerial and Costing Systems in Ghana’s Healthcare Management ........................ 20
2.5. Reforms in the Health Logistics and Commodity Management System ...................... 21
2.6 The Health Supply Chain ............................................................................................... 27
2.6.1 Elements of the Health Supply Chain ................................................................................... 29
2.6.2 SCM in Healthcare Context .................................................................................................. 30
2.6.3 Minimizing Health Supply Chain Cost ........................................................................ 32
2.7 Nature of MAS Design ................................................................................................... 32
2.8 Functions of the MAS Information in Healthcare Management .................................... 34
2.8.1 Costing Systems Design in Hospitals .................................................................................... 35
University of Ghana http://ugspace.ug.edu.gh
vi
2.8.2 Formal MAS Design in Health SCM Decisions ...................................................................... 36
2.8.3 Inter-Health Organizational Cost Management in Supply Chains ....................................... 37
2.9 Chapter Summary ........................................................................................................... 39
CHAPTER THREE ............................................................................................................................ 41
CONTINGENCY-BASED MANAGEMENT ACCOUNTING STUDIES .................................... 41
3.1 Introduction .................................................................................................................... 41
3.2 Theoretical Background of Contingency Fit .................................................................. 41
3.3 Contingency Fit Models ................................................................................................. 43
3.3.1 Cartesian vs. Configuration .................................................................................................. 43
3.3.2 Congruence vs. Contingency ................................................................................................ 45
3.4 Typology of Contingency Fit Models ............................................................................ 47
3.4.1 Selection Fit Models ............................................................................................................. 48
3.4.2 Matching Fit Models ............................................................................................................ 49
3.4.3 Interaction (Moderation) Fit Models .................................................................................... 52
3.4.4 Mediation Form of Fit .......................................................................................................... 55
3.5 Approaches to Testing Contingency Fit Models ............................................................ 56
3.5.1 Deviation Score and Residual Analysis Techniques .............................................................. 56
3.5.2 Approach to Testing Moderation Fit Models ....................................................................... 60
3.5.3 Approach to Testing Mediation Form of Fit Models ............................................................ 61
3.6 Conceptualization of Contingency Fit and its Attainment ............................................. 62
3.7 Levels of Contingency Fit Analysis ............................................................................... 64
3.8 Early Contingency-Based Management Accounting Studies ........................................ 65
3.9 Selection, Definition and Measurement of MAS Variables ........................................... 66
3.9.1 Arbitrary Selection of Variables ........................................................................................... 66
3.9.2 Empirical Estimation of Contingency Fit Models .................................................................. 70
3.10 Empirical Estimation of Moderation Forms of Fit ....................................................... 71
3.10.1 Hypotheses Formulation and Statistical Analysis .............................................................. 71
3.10.2 Strength of the Relationship .............................................................................................. 78
3.10.3 Lower-Order Effects ........................................................................................................... 79
3.10.4 Interaction and Effect Size ................................................................................................. 82
3.10.5 Multiple and Higher-Order Interaction .............................................................................. 84
3.11 The Use of Higher-Order of Abstraction Models in SEM ........................................... 86
3.12 Chapter Summary ......................................................................................................... 87
CHAPTER FOUR ............................................................................................................................... 89
THEORETICAL MODEL AND HYPOTHESES DEVELOPMENT ........................................... 89
4.1 Introduction .................................................................................................................... 89
University of Ghana http://ugspace.ug.edu.gh

vii
4.2 Theoretical Framework .................................................................................................. 89
4.2.1 Contingency Fit ..................................................................................................................... 90
4.3 Theoretical Foundation of Constructs ............................................................................ 96
4.3.1 Management Accounting Systems (MAS) ............................................................................ 96
4.3.2 Supply Chain Integration (SCI) ............................................................................................ 102
4.3.3 Hospital SC Performance .................................................................................................... 107
4.4 Formulation of Hypotheses .......................................................................................... 109
4.4.1 MAS Information and Hospital Supplier Partnerships ....................................................... 109
4.4.2 MAS Information and Hospital Supply Chain Integration (Internal Integration) ............... 112
4.4.3 MAS Information and Level of Information Exchange ....................................................... 114
4.4.4 MAS Information and Hospital Supply Chain Risk and Uncertainty ................................... 116
4.5. Mediating Role of MAS Information in Supply Chain Performance ......................... 118
4.5.1: MAS and Supplier Relations (External Integration) on Performance ................................ 118
4.5.2. MAS and Supply Chain Integration (Internal Integration) on Performance ...................... 121
4.5.3: MAS and Level of Knowledge Exchange on Performance ................................................. 122
4.5.4. MAS and Supply Chain Risk and Uncertainty on Performance ......................................... 123
4.6 Contingency Effect of the SCM Contextual Dimensions ............................................ 124
4.6.1. Supplier Relations (External Integration) to Performance ................................................ 124
4.6.2. Relationship of Internal Integration to Performance ........................................................ 125
4.6.3. Relationship of Level of Knowledge Exchange to Performance ........................................ 126
4.6.4. Relationship of Supply Chain Risk and Uncertainty to Performance................................. 127
4.7 Chapter Summary ...................................................................................................................... 128
CHAPTER FIVE .............................................................................................................................. 130
METHODOLOGY ........................................................................................................................... 130
5.1 Introduction .................................................................................................................. 130
5.2 The Study’s Philosophical Underpinning .................................................................... 131
5.3. Dimensions of Philosophical Assumptions ................................................................. 132
5.3.1. Ontology ............................................................................................................................ 132
5.3.2. Epistemology ..................................................................................................................... 133
5.3.3. Methodology ..................................................................................................................... 134
5.3.4. Axiology ............................................................................................................................. 134
5.4. Paradigms in Management Research .......................................................................... 135
5.4.1. Positivism .......................................................................................................................... 135
5.4.2. Social Constructivism ........................................................................................................ 136
5.4.3. Pragmatism ....................................................................................................................... 137
5.5. Paradigms in Accounting Research............................................................................. 138
University of Ghana http://ugspace.ug.edu.gh
viii
5.6. The Study’s Philosophical Stance ............................................................................... 139
5.7. Purpose and Design Strategies of the Survey.............................................................. 140
5.8 Survey Strategy ............................................................................................................ 143
5.9. Population, Sample and Sampling Procedure ............................................................. 143
5.9.1. Study Sample ..................................................................................................................... 145
5.9.2. Sampling Procedure .......................................................................................................... 145
5.9.3. Sample Size........................................................................................................................ 146
5.10. Approach to Data Collection ..................................................................................... 147
5.11. Scale Development and Measurements..................................................................... 148
5.12. Constructs and their Sources ..................................................................................... 149
5.13. The Modelling Process .............................................................................................. 151
5.14. Summary of Analysis Procedure ............................................................................... 152
6.15. Chapter Summary ...................................................................................................... 154
CHAPTER SIX ................................................................................................................................. 155
SURVEY ANALYSIS AND RESULTS .......................................................................................... 155
6.1 Introduction .................................................................................................................. 155
6.2 Preliminary Analysis of the Sample Data .................................................................... 156
6.3 Sample Characteristics ................................................................................................. 157
6.4 Assessment of Data for Normality ............................................................................... 159
6.4.1 Assessing Data for Multivariate Outliers ........................................................................... 162
6.4.2 Correlation Analysis ........................................................................................................... 163
6.5 Measures of Reliability and Validity of Scale Items.................................................... 165
6.6 Post Hoc Analysis of Factor Analytic Models ............................................................. 170
6.6.1 Model 2 of the Factor Analytic Models .............................................................................. 172
6.6.2 Model 3 of the Factor Analytic Models .............................................................................. 172
6.7 Structural Model Specification..................................................................................... 175
6.7.1 Specification of the Hypothesized Model ........................................................................... 176
6.7.2 Identification of the Hypothesized Model .......................................................................... 178
6.8 Fitting the Hypothesized Model ................................................................................... 180
6.8.1 Statistical Significance ........................................................................................................ 180
6.8.2 Model Estimation Process .................................................................................................. 180
6.8.3 Structural Model Fitting Process ........................................................................................ 181
6.9 Hypotheses Tests of the Structural Model ................................................................... 181
6.10 Selection Fit Model – Test of H1 (a – d), H2 (a – d), H3 (a – d), and H4 (a – d) ...... 182
6.11 Mediating Effect of MAS Construct – Test of H5 (a) to H5 (d) ................................ 187
University of Ghana http://ugspace.ug.edu.gh

ix
6.11.1. Confounding Variables Effect .......................................................................................... 187
6.11.2 Mediation Effect of the MAS Construct............................................................................ 187
6.13 Moderating Effects of the SCM Constructs – Hypotheses H 6(a) – H 6(d) .............. 193
6.13.2 Inclusion of Lower-Order Effects ...................................................................................... 193
6.13.1 Exclusion of Lower-Order Effects...................................................................................... 198
6.14 Chapter Summary ....................................................................................................... 201
CHAPTER SEVEN ........................................................................................................................... 202
DISCUSSION AND INTERPRETATION OF FINDINGS .......................................................... 202
7.1 Introduction .................................................................................................................. 202
7.2 Recap of Research Objectives, Questions and Hypotheses ......................................... 202
7.2.1. Research Questions ........................................................................................................... 203
7.3 Fit between SCM and MAS Information Characteristics ............................................ 203
7.3.1 Strategic Supplier Partnerships (External Integration) and MAS Information ................... 204
7.3.2 Supply Chain Integration (Internal Integration) and MAS Information ............................. 206
7.3.3 Level of Information Sharing and MAS Information .......................................................... 207
7.3.4 Supply Chain Risk and Uncertainty and MAS Information ................................................. 208
7.4 Interpretation of the MAS Mediation Effect ................................................................ 209
7.4.1 Confounding Variables and Hospital Supply Chain Performance ...................................... 209
7.4.2 Mediating Effect of MAS on Performance ......................................................................... 210
7.4.3 Joint Effect of MAS and SCM on Hospital SC Performance ................................................ 211
7.4.4 Mediating Role of the MAS Information Dimensions......................................................... 212
7.5. Contingency Effect of SCM on Performance ............................................................. 214
7.6 Implications of Findings............................................................................................... 215
7.6.1 Theoretical Implication ...................................................................................................... 216
7.6.2 Practical Implications ......................................................................................................... 216
7.6.3 Policy Implications .............................................................................................................. 218
7.7 Chapter Summary ......................................................................................................... 218
CHAPTER EIGHT ........................................................................................................................... 220
SUMMARY, CONCLUSIONS AND CONTRIBUTIONS ........................................................... 220
8.1 Introduction .................................................................................................................. 220
8.2 Summary of the Study .................................................................................................. 220
8.2.1 The Study’s Main Thrust ..................................................................................................... 220
8.2.2 The Study’s Main Findings.................................................................................................. 227
8.3 Conclusions .................................................................................................................. 230
8.4 Contributions of the Thesis .......................................................................................... 233
8.5. Recommendations ....................................................................................................... 235
University of Ghana http://ugspace.ug.edu.gh

x
8.6 Limitations of the Study ............................................................................................... 236
8.7 Future Research Directions .......................................................................................... 238
8.8 Chapter Summary ......................................................................................................... 239
REFERENCES ................................................................................................................... 240
Appendix A ........................................................................................................................ 262
Questionnaire for Hospital Accountants ............................................................................ 262
University of Ghana http://ugspace.ug.edu.gh

xi
LIST OF TABLES
Table 5.1 Ontology, Epistemology, Methodology, Axiology and Methods Distinguished 135
Table 5.2 Implications of Positivist Philosophical Assumptions 136
Table 5.3 Positivist and Social Constructionist Contrasted 137
Table 5.4 Relationship between Philosophical Assumptions and Paradigms 138
Table 5.5 Distribution of Samples by the Six Regions 147
Table 5.6 Constructs and their Sources of Measured 150
Table 5.7 Summary of Analysis Procedure 153
Table 6.1 Distribution of Hospitals in Terms of Ownerships, Profit Status and Location 158
Table 6.2 Descriptive Statistics for Scale Items 161
Table 6.3 Correlation Analysis, Reliability and Average Variance Extracted of Constructs 164
Table 6.4 Factor Loadings of Scale Items 169
Table 6.5 Post Hoc Analysis for Factor Analytic Models 171
Table 6.6 Structural Path Coefficients and Hypotheses Tests for Fit Relationships 184
Table 6.7 Summary of Goodness-of-Fit Tests for Structural Model 185
Table 6.8 Structural Path Coefficients for Mediation Analysis 189
Table 6.9 Path Coefficients for Moderation Effects – Lower-Order Effects Excluded 196
Table 6.10 Path Coefficients for Moderation Effects – Lower-Order Effects Included 199
University of Ghana http://ugspace.ug.edu.gh

xii
LIST OF FIGURES
Figure 1.1 Research Scope 1
Figure 1.2 Gaps Linking MAS, SCI and SCP 8
Figure 2.1 Ghana’s Health Supply Chain Management System 23
Figure 3.1 (a)-(b) Cartesian and Configuration Models 45
Figure 3.2 (a)-(c) Matching Fit Iso-performance 51
Figure 3.3 Moderation Fit Relationship 53
Figure 3.4 (a-(d) Non-Monotonic (Symmetrical) and Cross Over Interaction 54
Figure 3.5 Euclidian Approach in Determining Matching Form of Fit 59
Figure 3.6 Potential Type II Error Associated with Residual Analysis 60
Figure 3.7 (a) Mediation Form of Fit Models 62
Figure 3.7 (b) Four Step Procedure for Testing Mediation Form of Fit 63
Figure 3.8 (a) Mediation Analysis of Contingency Variables, Budget Participation
and Managerial Performance
76
Figure 3.8 (b) Moderation Analysis of Contingency Variables, Budget Participation
and Managerial Performance
77
Figure 3.9 (a)-(d) Strength Versus Form Interaction 79
Figure 4.1 Theoretical Framework 91
Figure 4.2 Classification of the MAS Dimensions 99
Figure 6.1 (a)-(b) Graphical Output of Factor Analytic Model for SCM Context Factors 166
Figure 6.1 (c) –(d) Graphical Output of Factor Analytical Model for MAS Information
Dimensions
167
Figure 6.1 (c) Graphical Output of Factor Analytic Model for SCP Dimensions 167
Figure 6.2 The Hypothesized Model 177
Figure 6.3 Structural Output for Fit Relationships 186
Figure 6.4 Structural Output of Mediation Analysis 190
Figure 6.5 Structural Output for Mediation Analysis (Second-order) 192
Figure 6.6 Structural Output for Moderation Effects (Lower-order effects
included)
197
Figure 6.7 Structural Output for Moderation Effects (Lower order effects
excluded)
200
University of Ghana http://ugspace.ug.edu.gh
xiii
LIST OF ABBREVIATIONS
CEO Chief Executive Officer
CMS Central Medical Stores
GHS Ghana Health Service
HCSCMP Health Commodity Supply Chain Management Plan
HSC Hospital Supply Chain
MA Management Accounting
MAS-CS Management Accounting System Supply Chain
MAS-SCM Management Accounting System Supply Chain Management
MOH Ministry of Health
NPM New Public Management
RMS Regional Medical Stores
SC Supply Chain
SCI Supply Chain Integration
SCM Supply Chain Management
SCN Supply Chain Network
SDP Service Distribution Points
TCE Transaction Cost Economics
WHO World Health Organization
University of Ghana http://ugspace.ug.edu.gh

xiv
ABSTRACT
This work analyzes the contingency effects of supply chain integration (SCI), information
sharing (or knowledge exchange), supply chain (SC) risk and uncertainty and management
accounting system (MAS) design on hospital SC performance in Ghana. Increasingly seen as
crucial in the management accounting (MA) literature over the past three decades has been the
design and implementation of effective MASs that extend beyond organizational boundaries
for the management and performance of relationships in the inter-firm exchanges domain. Such
studies have become one of the most important and critical areas for the CEOs and executive
leaderships of hospitals in their efforts to improve operational efficiency at minimal costs.
However, while the relationship between several SCM contextual factors and MAS
information, and the impact of SCI on SC performance have been extensively examined,
virtually no study had empirically examined in a single comprehensive study, the SCM-
performance impacts of MAS design. The underdevelopment of such studies is even more
pronounced in service oriented organizations. In addition, the literature on MAS-SCM
relationships had emphasized the design of MAS in the transaction context which in most cases
results in misaligned control. Transactions costs economics (TCE) although provides insights
on the MAS organizations should install to achieve fit, the actual observed patterns of MAS
use and the contextual factors that underpin MAS design in the inter-firm exchanges domain
are not fully explained by the theory. Hence, TCE tends to ignore the dimensions of internal fit
(i.e. internal integration) of the SC. Given this void, a survey of management accountants
drawn from 237 public and private hospitals in Ghana was used to test the contingency effects
of these relationships on hospital supply chain aggregate performance using hierarchical
factorial structures. Whereas the results partially support the presence of the selection and
mediation fit, the moderating form of fit was fully supported by the sample data. Also, internal
University of Ghana http://ugspace.ug.edu.gh

xv
integration was only supported by the moderation fit model. However, level of information (or
knowledge) exchange was not supported by the selection fit model although it was fully
supported by the moderation fit model and partially supported by the mediation model. This
finding suggests that choices of the MAS information characteristics to facilitate SCM
decisions among hospitals in Ghana is either excessive or insufficient. However, the findings
suggest that optimal choices of MAS design in the inter-firm exchanges domain to enhance SC
operational performance can be explained by contingency theory. Consistent with several prior
studies, it can be theorized that SCI as well as level of knowledge exchange and SC risk and
uncertainty have contingency effects in the design of MAS in the inter-organizational domains
in healthcare context. Hence, they could be considered as added external variables in the MAS-
contingency paradigm. The study’s key contribution is the development and testing of a novel
theoretical model of the relationship between the selection, mediation and moderation fit
models that link SCI, level of information sharing, and SC risk and uncertainty and MAS design
on hospital SC performance. It also offers Ghanaian hospital managers the usefulness of the
MAS-contingency framework in enhancing hospital SCM decisions.
University of Ghana http://ugspace.ug.edu.gh

1
CHAPTER ONE
INTRODUCTION
1.1 Brief Overview of the Study
This thesis is concerned with empirical examination of the contingency fit relationships among
four dimensions (broad scope, timeliness, integration and aggregation) of management
accounting system (MAS) information and supply chain integration (SCI), level of knowledge
exchange, and supply chain risk and uncertainty that can leverage hospital supply chain
aggregate performance in Ghana. This represents the intersection of three key areas:
management accounting systems (MAS), supply chain integration (SCI), and hospital supply
chain (SC) performance as shown in Fig 1.1. In this chapter, the background linking the
research problem and layout of the whole thesis’s logical sequence is presented. The chapter
ends with a summary.
Figure 1.1: Study Scope
(Source: Author’s own drawing based on review of literature)
Management Accounting
System (MAS) Design
Hospital Supply Chain Performance
Supply Chain Integration
(SCI)
Fit Relationships in
Healthcare
Institutions
University of Ghana http://ugspace.ug.edu.gh
2
1.2 Research Background
The supply chain (SC) concept which emerged in the 1990s as a strategic management tool,
has become a key driver that enhances overall organizational performance (Maestrini, Luzzini,
Maccarrone & Caniato, 2017; Ataseven & Nail, 2017). This strategic aspect of the SC has been
investigated by several research studies through empirical examination of the associations
between different SCM contextual factors and MAS design on one hand, and both operational
and financial performance on the other (van der Meer-Kooistra & Vosselman, 2000; Dekker,
2004; Flynn, Huo & Zhao, 2010; Wong, Boon-itt & Wong, 2011; Dekker, Groot & Schoute,
2013; Qi, Huo, Wang & Yeung, 2017). However, research that examines the impact of the
MAS information characteristics on either SC operational or financial performance is relatively
underdeveloped and largely remains a void (Burritt & Scaltegger, 2014). While this gap
remains, SCI, and sharing of information (or knowledge exchange) about the risks associated
with inter-firm exchanges have been identified as the most influencing factors that facilitate
the effective design and implementation of MAS information in enhancing hospital SC
performance (Kwon, Kim and Martin, 2016).
In addition, existing works on SCI and performance have predominantly been dominated by
the industrial dynamics and logistics literature as the literature has extensively focused on
product type organizations mostly discrete parts manufacturing and consumer goods (e.g.
Flynn et al, 2010; Wang et al, 2011; Qi et al, 2017). There have been relatively little research
that look at the impact of the MAS information characteristics on SCM decisions in service
oriented organizations, and more specifically, healthcare institutions (Anderson & Dekker,
2015). Consequently, increasingly seen as crucial in the literature over the past two decades
has been the design and implementation of effective MASs that align with contextual factors
within healthcare organizations (Wardhani, Utarini, van Dijk, Post & Groothoff, 2009;
Aidemark & Funck, 2009). This is because the effective formulation, management and efficient
University of Ghana http://ugspace.ug.edu.gh

3
functioning of the SC is highly associated with the fit between MAS information characteristics
and SCM contextual factors (Seal Cullen, Dunlop, Berry & Ahmed, 1999; Reusen &
Stouthuysen, 2017). For example, in healthcare services, information relating to SC costs such
as inventory management, procurement, transportation, warehousing, cost of operating
facilities, link between cost and cost drivers, commodity throughput as well as revealing
information on ineffective and inefficient hospital operations through the consumption of
resources etc., are provided by effective MAS design.
Furthermore, the SC constitutes the most critical element in overall organizational cost control
and has become one of the most important and critical areas for the chief executive officers
(CEOs) and executive leaderships of hospitals (Barlow, 2010c). This is because improvement
upon overall efficiency and cost reduction strategies have been a challenging issue in hospital
management (Pizzini, 2006; Abernethy, Chua, Grafton & Mahama, 2007). Also, the power
structure of healthcare has changed with the evolution of the new public management (NPM),
making MASs more dominant than medical skills in the monitoring and evaluation of clinical
performance (WHO, 2000; Malmmose, 2015). However, for effective monitoring and hence
optimal performance, the MAS design should traditionally be based on the ‘matching’ principle
where the installation of MASs by organizations align with contextual variables (Reusen &
Stouthuysen, 2017). Although these theoretical interrelationships fundamentally underpin the
installation and implementation of MAS for performance, the large volume of MAS-SC studies
had emphasized fit in the transaction context other than fit in the organizational context (van
der Meer-Kooistra & Vosselman, 2000; Dekker, 2004; Dekker et al, 2013). This is because the
theoretical lens of transaction costs economics (TCE) explains how MASs are installed as a
function of the specific transaction context that arises from contracting risks between suppliers
and buyers other than internal dimensions such as internal integration of the SC.
University of Ghana http://ugspace.ug.edu.gh
4
In this regard, TCE tends to ignore the dimensions of internal fit (e.g. internal integration) of
the SC. The internal fit of the supply chain represents the cross-functioning of systems and
collective responsibility across functions from a strategic perspective. Collaborations across
procurement, warehousing and distribution functions take place within internal integration to
meet customer (patient) requirements at a low total cost (Qi et al, 2017). Also, internal
integration efforts facilitate the sharing of real-time information and knowledge across key
functions through the break-down of functional barriers (Wong et al, 2011). These functional
barriers impact significantly on inventory management and warehousing, quality of hospital
processes and clinical costs, operating cost of hospital facilities, commodity throughput, costs
and cost drivers, etc. that have significant effect on SC operational performance (Chen, Preston
& Xia, 2013; Ataseven & Nair, 2017). In addition, the TCE does not seem to fully explain the
actual observed patterns of MAS use and the contextual factors that underpin its design in the
inter-firm exchanges domain, although it provides insights on the MAS organizations should
adopt to achieve fit (Anderson & Dekker, 2015). Furthermore, adoption of the TCE is mainly
based on mitigating the risk associated with the transactions in the inter-firm exchanges domain
(Langfield-Smith, 2008; Dekker et al, 2013). Risks such as heightened vulnerability and the
possibility that partners engaged in the transactions will opportunistically exploit the dependent
relationship are typical examples.
In this regard, the general contention has been that the excessive use of the MAS information
is required for transactions that suggest higher levels of risk attributes in order to foster mutual
collaboration and coordination (Reusen & Stouthuysen, 2017). Whilst there is wide acceptance
of this notion of alignment, the relationship between an organization’s MAS structure and
transactions context will often be in a state of misalignment to adversely affect performance.
Choices that entail either excessive or insufficient use of the MAS relative to the contextual
variable will result in misalignment, and negatively affect performance (Otley, 1980, 2016;
University of Ghana http://ugspace.ug.edu.gh
5
Burkert, Davila, Mehta & Oyon, 2014). Based on these voids, this study tests the contingency
effects of the MAS-SC performance using empirical data from healthcare institutions in Ghana.
In business strategy, the contingency perspective examines a particular set of organizational
and environmental factors at the optimal level (Burkert et al, 2014). However, the benefits of
contingency theory’s application in the inter-firm exchanges domain with respect to MAS
design has received little (or possibly no attention) in the literature (Jamal & Tayles, 2010).
Furthermore, existing works on the contingency paradigm were conducted based on samples
drawn from the developed world such as the US, UK, Canada and Australia (Jamal & Tayles,
2010). Hence arguments regarding the convergence of the contingency theory’s usefulness
remains contested. Similar works in developing economies such as Ghana will allow for the
assessment of the validity of the contingency arguments.
1.3. The Research Problem
The design of MAS information for SCM decisions in the inter-firm exchanges domain has
been considered as mere extensions of the conventional intra-firm cost accounting tools of the
traditional MAS. To this end, no attempt has been made by management accounting researchers
to test the contextual factors that underpin MAS design in the inter-firm exchanges domain as
compared to the intra-organizational domains which have been extensively studied.
Consequently, organizations have relied on the practice of imitating individuals’ MAS
structure when designing and installing MASs in inter-firm exchanges (Reusen & Stouthuysen,
2017). Reusen & Stouthuysen (2017) found this practice to be one of the root causes of
misalignment in the MAS-context relationship in the inter-firm exchanges domain.
It has been argued that ‘‘the planning and controlling processing abilities that are fundamental
to managing costs internally is the same for managing inter-firm relationships hence, can be
University of Ghana http://ugspace.ug.edu.gh

6
applied to SCM activities’’ (Fayard et al, 2012, p.170). In this regard, organizations that have
installed internal cost management systems considered to be at the highest level would be able
to use their expertise and knowledge to model similar costing systems for SCM decisions.
Although it is possible to use the expertise and knowledge of the traditional intra-firm cost
accounting tools to proxy SCM decisions in the inter-firm exchanges domain, the key concept
of fit is missing which ultimately results in misalignment to negatively affect performance.
Studying the impact of the MAS dimensions on SCM characteristics determines the functions
of the MAS in SCM decisions. In other words, the MAS has already been installed and is being
used to make decisions in the SCM context. This aspect of the MA-SC relationship has been
extensively studied from the theoretical lens of transaction cost economics (TCE) which
according to Anderson & Dekker (2015), does not fully explain the actual observed patterns of
the MAS use and the contextual factors that underpin its design in the inter-firm exchanges
domain. On the other hand, studying the effect of the SCM characteristics on MAS design
determines the MAS-context relationship that impact on performance in the inter-firm
exchanges domain. That is, it determines the design and type of MAS that appropriately fits
the SCM characteristics to maximize performance.
This study focuses on hospitals in Ghana because the SCM challenges that confront the health
sector could be as a result of improper design and use of the MAS for SCM decisions resulting
in misalignment between SCM practices and MAS design. (Asamoah, Abor and Opare, 2011;
Manso Annan & Anane, 2013; Denkyira, 2015). This will by extension, translate the body of
literature on MAS-contingency knowledge from the intra-organizational domains (which has
been the predominant MAS design studies in extant literature) to the inter-firm exchanges
domain in supply chains. Management of Ghana’s health commodity and SCM system has in
recent years, been characterized by ineffectiveness and weaknesses as ‘gaps’ (WHO, 2009;
Manso, Annan & Anane, 2013; Denkyira, 2015). To this end, various models (e.g. the five-
University of Ghana http://ugspace.ug.edu.gh

7
year development plan of the Ministry of Health (MOH) spanning the period 2008-2012, and
the MOH’s Health Commodity Supply Chain Master Plan (HCSCMP) of 2012 etc.) have been
tried and tested yet the problem remain unaddressed and have widened rather than curtailed.
For example, a study by Asamoah, Abor and Opare (2011) to examine the healthcare SC for
Artemisinin (ACT) Based Combination Therapies in Ghana revealed weaknesses such as
disruptions and delays in the SCM system due to poor SCI (both internal and external
integration) and weak inventory management systems. They further identified the integration
of the SC and weak information linkages as the main threat to the health SC and this ultimately
results in price increases at the pharmacy level.
The identified weaknesses have significant impact on the design and implementation of MAS
information because MAS serves not only to provide information to oil the wheels of a SC
network but also, integrates functional units and entities which are internal and external to
organizations (Burns, 2002; Thrane & Hald, 2006; Dacosta-Claro, 2002; Scheller & Smeltzer,
2006). It also serves to reduce costs and create value in SCs (Fayard, Lee, Leitch & Kettinger,
2012). However, these relationships have not been examined as part of the numerous models
already tried and tested. Perhaps, the MASs installed and used in hospitals might not be in
alignment (or fit) with hospital SCM activities thereby providing little value for managerial
decisions in the inter-firm exchanges domain. Studies into the contingency models linking
MAS information characteristics and SCM could offer some insights to solving the problem.
Besides, substantial literature document the link between SCI and both SC financial and
operational performance (Flynn et al, 2010; Wong et al, 2011). Another vast stream of literature
examine the relationship between MAS information characteristics and attributes of SCM in
the inter-firm exchanges domain (Copper & Slagmulder, 1999; van der Meer-Kooistra &
Vosselman, 2000; Dekker, 2004, Agndal & Nilsson, 2009; Coad & Cullen, 2006; Fayard et al,
University of Ghana http://ugspace.ug.edu.gh

8
2012; Dekker et al, 2013; Anderson & Dekker, 2015; Reusen & Stouthuysen, 2017). There is
however, virtually no research that simultaneously examines the MAS design, SCI and SC
performance associations in a single comprehensive study. Given the considerable effort
devoted by management accounting researchers in explaining MAS choices in inter-firm
relationships and the fact that SC performance is largely a function of relationship
characteristics, such theoretical interrelationships are important and fill a gap that develops and
tests a novel theoretical model linking both MAS design, SCM, and SC performance in
healthcare context. This is important for the advancement of theory in the inter-firm exchanges
domain. Fig 1.2 illustrates the relationships linking these gaps.
Fig 1.2. Gaps Linking MAS, SCI and SCP
As shown in Fig 1.2, the link between MAS design and SC performance still remains a gap
although they have a strong theoretical background. Besides, the link between SCM and MAS
design is recursive (Ramos, 2004). However, only one-side of this bi-directional relationship
has so far been examined. The impact of SCM on MAS design has virtually received no
University of Ghana http://ugspace.ug.edu.gh

9
empirical investigation. Finally, a study that examines the complete relationship between MAS,
SCM, and SCP hardly exists in the literature. Thus, this study fills a gap by developing a novel
theoretical model that links these three key constructs. Additionally, the link between SCI and
SC performance is associated with levels of effects on various performance dimensions that
differ and vary (Cousins & Menguc, 2006; Devaraj, Krajewski & Wei, 2007; Schoenherr &
Swink, 2012, 2015), rendering the findings of such studies to be inconsistent. More precisely,
the impact of both internal integration and external integration on performance has been
associated with mixed findings. This inconsistencies could be attributed to the measurement of
integration as one construct and also elimination of internal integration in most studies (Flynn
et al, 2010; Ataseven & Nail, 2017).
For example, while Cousins and Menguc (2006) show a positive association between SCI and
suppliers’ communication performance, Devaraj et al (2007) also registered a positive
association between SCI and performance, but found that customer integration and
performance were negatively related. Similarly, Flynn et al (2010) found that supplier
integration and operational performance are not directly related. Schoenherr & Swink (2012)
also found distinct associations between SCI and both financial and operational performance.
Flynn et al (2010) found in both their configuration and contingency approach that SCI was
associated with both operational and business performance and that customer and internal
integration were more strongly associated in enhancing performance than supplier integration.
In general, the literature on the relationship between SCI and performance has very mixed
findings. In order to advance theory development, it is important to ascertain whether
moderating factors underpin certain relationships which is the key concept of contingency
theory and is highly important in situations where the findings about relationships are mixed
(Ataseven & Nail, 2017). Furthermore, much of the literature in this area have been conceptual
in nature coupled with the dominance of inductive methods such as case studies involving two
University of Ghana http://ugspace.ug.edu.gh
10
dyad relationships and occasionally SC triad in the majority of empirical works (e.g. Cooper
& Slagmulder, 2004; Seuring & Muller, 2008; Burritt & Schaltegger, 2014). Although case
studies research can be very helpful for gaining a deeper insights and understanding into factors
that influence the installation of MASs in inter-firm relationships (van der Meer-Kooistra &
Vosselman, 2000), the findings associated with these studies show lack of generalizability and
overall conclusions. This work contributes to filling these gaps.
1.4 Study Objectives
The broad objective of this study is to examine the impact of the relationship between hospital
SCI and four dimensions of MAS design on hospital SC performance. Specifically, the study
seeks to:
1) Examine the association between hospital SCM contextual factors and dimensions of
the MAS information in Ghana.
2) Investigate the mediating effect of the MAS dimensions on SCM contextual factors and
Ghana’s healthcare SC operational performance.
3) Examine the moderating effect of SCM contextual factors on the relationship between
MAS design and Ghana’s healthcare SC operational performance.
1.5 General Research Questions
The following research questions underpin the study:
1) Do the MASs designed and used by healthcare institutions in Ghana align with
internal and external integration, level of information sharing and the risk and
uncertainties of the health supply chain?
University of Ghana http://ugspace.ug.edu.gh
11
2) To what extent do the MASs used in Ghana’s healthcare organizations offer a
mediating role between SCI (internal and external), level of information sharing,
and supply chain risk and uncertainty and hospital SC operational performance?
3) To what extent do SCI (external and internal), level of information sharing, and
supply chain risk and uncertainty have an interaction effect on the association
between MAS information and hospital SC operational performance of healthcare
institutions in Ghana?
1.6 Significance of the Study
The design and use of MAS information in both private and public-sector organizations has
often been encouraged by government policies across the globe (Macinati &Anessi-Pessina,
2014). However, exploitation into its actual usage and benefits in healthcare settings, and
supply chains in particular largely remains a void. Consequently, a study that provides insights
into the performance implications of the causal paths linking SCI and MAS information
characteristics in healthcare context would both extend existing knowledge and provide useful
indications to healthcare managers and policymakers. In addition, modelling and measuring
performance outcomes relating to the MAS-supply chain intersection is needed to permit an
examination of the question of whether an appropriate or inappropriate ‘matching’ between
SCI and MAS information in the hospital SC leads to higher or lower performance. The
findings in this regard, will undoubtedly serve as a reference point (or a guide) for the design
and implementation of MAS information in the SCM context of healthcare institutions. In
particular, it provides empirical evidence that could serve as guiding principles to the health
systems’ pricing decisions, performance assessment, process improvement, and cost reduction
strategies associated with their inter-organizational relations (e.g. suppliers) and the extent of
fit (or alignment) of the managerial and cost information with these decision needs.
University of Ghana http://ugspace.ug.edu.gh

12
This work, apart from the foregoing, also provides information that relates to the current state
of the managerial and cost information systems designed and used by healthcare institutions;
i.e. whether they positively respond to hospital SCM issues and provide management with the
relevant SCM information for effective decisions. In other words, whether the characteristics
of the MASs information and the SCM metrics have any linkage to positively impact on
performance. Given that the accounting systems in these institutions have perhaps reached their
state of obsolescence and hence become dysfunctional due to evolutionary changes in the
processes and procedures of hospital operations that have not been incorporated into their
accounting systems, this work stands in the position to provide information that could lead to
addressing some of these deficiencies and weaknesses. To achieve this, it shows the extent to
which the MAS information designed and used by healthcare institutions fits (or aligns) with
context factors in the inter-organizational domain, and whether per the outcome, these systems
need further improvement or total overhaul.
Indeed, the identified weaknesses and deficiencies in the health SCM system suggests that the
managerial and cost information systems associated with the health logistic and supply chain
have perhaps become obsolete and outdated, and hence, no longer support the strategic
direction of healthcare management although the systems are perfectly adequate for financial
reporting purposes. In this regard, issues on value relevance of the current MAS information
needed for management decision making in terms of the sophistication level of the managerial
and cost information are highly imbedded in this work. For example, issues relating to
advanced accounting techniques such as Activity-Based Costing (ABC) (which is found in
most hospitals’ accounting system) and knowledge of the application of modern costing
concepts become highly relevant.
University of Ghana http://ugspace.ug.edu.gh
13
1.7 Outline of Remainder of Thesis
The remainder of the thesis is organized into seven chapters as follows: Chapters 2 and 3 are
devoted to systematic literature reviews. Chapter two discusses the study’s context, MAS
design and the health supply chain; its distinguishing features from that of the mainstream
discrete parts manufacturing and consumer goods, and the decision-functional role of MAS
information in minimizing hospital supply chain costs. In chapter three, a general discussion
of the study’s theoretical underpinnings is presented together with empirical reviews of the
empirical contingency-based management accounting studies. Chapter four presents the
theoretical framework, and following a refinement of the research questions develops and
formulates the verbal hypotheses. The research methodology is presented in chapter five. It
comprises a detailed discussion of the research design, data collection procedures and
processes, and the approach to statistical tests and analysis. In chapter six, the survey analysis
and results are presented. This is followed by a discussion and interpretation of the findings in
chapter seven. Chapter eight concludes the study with a summary of main findings, key
contributions and future research directions.
1.8 Chapter Summary
In this chapter, the motivation for investigating the contingency fit relationships between MAS
design and SCI, level of information sharing, and SC risk and uncertainty, and their interaction
effect on hospital SC performance in Ghana has been specified. Given that the design and use
of MAS information is known to be commonly associated with organizational contextual
factors that can leverage organizational performance, such studies lack empirical evidence in
the inter-firm exchanges domain in service-oriented organizations. Existing MAS-SC studies
have predominantly not only dominated product type organizations such as discrete parts
manufacturing and consumer goods but also, emphasized the fit in the transaction context to
University of Ghana http://ugspace.ug.edu.gh
14
mainly mitigate the risk between transaction partners. However, an incomplete and potentially
based picture of inter-firm control may be presented when the MAS decisions are explained
using transaction attributes alone as a focus. The actual observed patterns on MAS use, and the
contextual factors that underpin MAS design in the inter-firm exchanges domain are not fully
explained by the TCE. In line with these voids, this study tests the contingency effects of the
MAS-SC performance using empirical data from healthcare institutions in Ghana. Evidence of
the weaknesses and deficiencies that characterize the procurement, warehousing, storage and
distribution arrangements of health commodities which ultimately results in high prices to end
users, have major implications for MAS design in the SCM of Ghana’s healthcare institutions.
Finally, the study outlines the structure and logical sequence of the remainder of the thesis.
University of Ghana http://ugspace.ug.edu.gh

15
CHAPTER TWO
CONTEXTUAL BACKGROUND, MANAGEMENT ACCOUNTING
SYSTEM DESIGN AND THE HEALTH SUPPLY CHAIN
2.1. Introduction
The previous chapter introduced the research problem and the motivation for the study. This
chapter presents a review of the study’s context, the MAS information characteristics and SCM
interactions, and how they combine to impact on the health SC performance. The chapter
begins with a discussion of the importance of hospital SC integration and its effect on
performance. In this case, recent issues on management accounting and SC performance are
discussed. It also gives a description of the study’s context followed by the nature of MAS
design and its possible functions in SCM decisions. The chapter also presents the SCM
challenges that characterize the research sight. It discusses the structure of Ghana’s health SCM
system which basically links three key distributors of health products: the Central Medical
Stores (CMS), the Regional Medical Stores (RMS) and Service Distributed Points (SDP) (or
hospitals). A background of the weaknesses and deficiencies that characterized the current
operations of Ghana’s health logistics and supply management system is also presented.
Furthermore, the current state of the accounting system in the health sector is briefly explained
followed by the numerous reform projects launched by governments since 1998 which were
aimed at transforming the health commodity and supply management system. Finally, a review
of the health SC in terms of levels of complexity and sophistication in comparison to that of
mainstream business organizations is also presented. The chapter ends with a summary.
University of Ghana http://ugspace.ug.edu.gh
16
2.2. Recent Studies on MAS Design and Hospital SC Performance
In this section, a reportage of recent trending issues on the MAS design, SCI and hospital SC
performance both at the local and international levels is presented. According to Ab Talib,
Abdul Hamid and Thoo (2015) the existing body of knowledge on this topic has a number of
trending issues arising from recent studies. These studies investigate the antecedents,
prerequisites, requirements, or critical success factors that affect SCI and hospital SC
performance. Integration of the SC is currently, considered as one of the widely discussed
topics in the SCM research (Polater and Demirdogen, 2018; Abdallah, Abdallah & Saleh,
2017). Polater and Demirdogen (2018) argue that intensive integration between external
partners and internal processes enhances hospital SC operational performance hence, underlies
the basic motivation for healthcare SCM. While hospitals integrate their internal capabilities to
provide a better service for patients, they benefit from their partners’ resources as well. Several
research studies (e.g. Zhao and Huo, 2013; Skandrani et al. ,2011; Kazemzadeh et al. ,2012;
Lee et al., 2011; Rahimnia and Moghadasian, 2010) have argued that an effective integrated
SC is one of the key competitive advantages of leading organizations and is currently one of
the widely discussed topics in the SCM research.
The concept of SCI has therefore become prevalent in both the public and private health sectors
because of the impact it has on enhancing operational efficiencies, customer satisfaction and
quality of care as well as minimizing wastes and medical errors (Schneller .and Smeltzer, 2011;
Polater and Demirdogen, 2018). The supply of medical products has also become critical to all
hospitals so that performance in terms of costs, quality, responsiveness and patient satisfaction
can be enhanced (Asamoah et al, 2011). Consequently, health providers in both the public and
private sectors have paid more attention to healthcare services and their suppliers in order to
achieve higher service quality, lower costs, and enhance operational performance (Hammad,
Jusoh and Ghozali, 2013). In addition, due to the increasing trend in healthcare spending on
University of Ghana http://ugspace.ug.edu.gh

17
supplies, both governments and private health providers are compelled to focus on the
assessment and improvement of hospital operations efficiency especially in relation to
suppliers of medical products and the overall logistics and SC (Watcharasriroj and Tang, 2004).
According to Chakraborty, Bhattacharya and Dobrzykowski (2014) the general perception of
organizations about SCI and SCM in general has budged toward managing relationships rather
than just the purchasing function. These relationships are however, closely related to MAS
information (Dekker, 2013, 2016) which like the objective of SCM, aims at reducing SC cost
and adding value (Burritt & Scaltegger, 2014). Abdallah et al (2017) provide useful insights in
boosting hospital SC performance when they examined the effect of trust (a key construct of
MAS design) with suppliers on hospital-supplier integration and hospital SC performance.
They established that high levels of SCI not only improve hospital SC performance but also
enhance the transformation of trust benefits into SC performance. The paper further documents
that hospital SCI partially mediates the relationship between trust and hospital SC performance.
In another study, Ataseven and Nail (2017) undertook an extensive examination of the
association between SCI and various performance dimensions using a meta-analytical
methodology. They find that supplier integration, internal integration, and customer integration
have a significant impact on both operational (cost, quality, delivery, and flexibility)
performance and financial performance of a firm. They point to the specific relationships
between SCI and performance that need to examined further within contingency framework to
discern the role of moderating factors. Finally, they offered insights on the dimensions of
integration that have the largest breadth and depth of impact on various performance measures
which is relevant for managerial decision-making.
On the local front, Adu-Poku, Asamoah and Abor (2011) examined the logistics SC system of
the Adansi South District Health Directorate from users’ perspective. They document that
University of Ghana http://ugspace.ug.edu.gh

18
adequate information (i.e. management accounting information) needed to support effective
and efficient SCM activities is lacking hence, a poor collation of patients’ needs during
procurement. They also identified problems such as delay in the procurement system in the
district as a result of poor delivery time by suppliers, delay in evaluating bids. Manso, Annan
and Anane (2013) also assessed the logistics management of the Ghana Health Service and
reported several shortcomings associated with the health SC. They found poor procurement
planning and budgeting, poor quantification and forecasting, delay in the procurement process
and order processing, and delay in receiving insurance claims to characterized the health SC.
Asamoah et al (2011) examined the performance of the SCM activities relating the
pharmaceutical SC for artemisinim-based combination therapies (ACT) in Ghana. They
reported that both the public and private SC networks for the ACT depict evidence of long-tern
relationships with external suppliers and factor interdependence. They also reported of the high
prices that characterized the general price level of the although highly subsidised ACT as a
result of disruptions in the health SC. Frequent disruptions in the link between external
suppliers which was found to be the main threat to the health SC, result in price increases of
health commodities at the pharmacy level. As can be seen from these deficiencies, a study to
examine the interaction effect of the MAS design and SCI is crucial because effective MAS
design provides information for the smooth running of the logistics system (Burritt &
Scaltegger, 2014). The next section explains the health SCM system in Ghana.
2.3 Ghana’s Health SCM System
The mission of the Logistics, Clearing and Warehousing Department of GHS reads: Logistics:
‘‘Our mission is to offer, our clients, a competitive advantage through superior transportation
of logistics services. Through timely communications and quality information, we will meet
and exceed our client’s expectations of service. Also, through our commitment to provide
University of Ghana http://ugspace.ug.edu.gh
19
excellent service, Value added service, continued innovation in management, we will
accomplish our mission: 2) Warehousing: To ensure that regular availability and uninterrupted
supply of health commodities are delivered to health institutions at affordable prices. Using
best practices in storage and distribution of quality, we are capable of responding to the total
commodity requirement and as a centre of excellence, and safe efficacious health commodities”
(Ministry of Health (MOH), 2012, p.2).
The SC system of Ghana’s healthcare which manages health commodities through a three-tier
system, is made up of drug manufacturers, suppliers (wholesalers, distributors, and retailers),
the Central Medical Stores (CMS), Regional Medical Stores (RMS), Service Delivery Points
(SDP), and the transportation networks. Through this SC, supplies and drugs as well as
contraceptives are managed and sent to health facilities across the country. The receipt, storage
and distribution of all medical supplies after procurement by the Ministry of Health (MOH) is
the responsibility of the CMS. The CMS in turn, supplies the lower levels of the tier. Depending
on their geographical location, health facilities (SDPs) receive their supplies from the
appropriate RMS. However, the management of vaccines is slightly different from other
medical supplies. These are managed through refrigerated facilities and a network of
warehouses of cold storage across the regions.
The MOH exercises overall oversight control including policy formulation, evaluation and
monitoring of progress in achieving set targets for the whole system. The service delivery and
Teaching Hospitals are largely undertaken by the Ghana Health Service (GHS). Both of these
institutions constitute the bulk of the MOH institutions under the public health system. A four-
tier system made up of regional, district, sub-district and community constitutes the health
system delivery while the management of health services and health supplies as stated upfront
is operated on a three-tier system comprising the CMS, the RMS, and the SDP. The CMS is
responsible for procuring drugs and vaccines that are primarily financed by external financiers.
University of Ghana http://ugspace.ug.edu.gh

20
Occasionally, and this is an exceptional case, the Teaching Hospitals and the Regional
Hospitals procure directly from suppliers but approval must be sought from the MOH. Thus,
whilst the logistics and supply management system is centralized, the healthcare delivery
system is decentralized. Together with suppliers of drugs and other medical supplies at both
local and international levels, pharmaceutical manufacturers, wholesalers, distributors, and
retailers, transportation networks and other distribution networks constitute the SCN in the
health sector.
2.4 Managerial and Costing Systems in Ghana’s Healthcare Management
As a recap of chapter one, the managerial and cost information systems of most healthcare
institutions in Ghana have reached the state of obsolescence and dysfunctional due to
evolutionary changes in the processes and procedures of hospital operations that have not been
incorporated in their accounting systems. The current MASs have little value for management
decisions in the inter-firm exchanges domain as there is limitation in the use and sophistication
of cost and managerial information. Advanced accounting techniques such as Activity-Based
Costing (ABC) are perhaps not applied and modern costing concepts are largely unknown in
most healthcare institutions. Managerial and cost information are mostly associated with
decisions on pricing rather than process improvement, performance assessment, or cost
reduction strategies. The managerial and cost information systems seemed to have become
outdated and no longer support the strategic direction of healthcare institutions though the
systems are perfectly adequate for financial reporting purposes.
There are also illogical relations among operating cost of facilities, value of commodity
throughput and populations served at various levels. Neither commodity throughput nor service
population appear to drive costs as they should be in an efficiently and rationally operating
system (Manso et al, 2013). Non connection between costs and cost drivers – clear indication
University of Ghana http://ugspace.ug.edu.gh

21
of non-linkage between budgeting process and both commodity throughput and service
populations (WHO, 2009; Denkyira, 2015). Currently, there is the unconventional occurrence
of public sector prices for highly subsidised commodities being higher than private sector
prices (Asamoah et al, 2011; Manso et al, 2013). However, Kelle, Woosley and Schneider
(2012) noted that by paying attention to the three dimensions of SCI (supplier, customer and
internal integration) in the inter-organizational linkages and their alignment with accounting
information characteristics, a hospital can improve its performance through the performance of
other organizations in the SC.
In addition, a hospital can improve upon its procurement and logistics activities by aligning its
inventory management system with a just-in-time MAS technique. Another example is where
hospitals provide a perfect fitting information about their inventory needs by helping their
suppliers more efficiently plan their production schedules to meet their needs. In this case
hospitals’ operating costs are minimized because they perform their procurement and logistics
activities in an efficient manner. In addition, they have less of their capital tied up in stock (or
inventory). Furthermore, sharing of knowledge and expertise in the optimum is easier, and
perhaps improve operations and even provide a competitive advantage in a situation where the
MAS information characteristics are well-fitted with SCM context factors. Hence, the perfect
alignment of SCI with the MAS information characteristics is highly critical to SC performance
in the healthcare setting (Aidemark & Funck, 2009). In this regard, improvements in hospital
SC performance have increasingly gained importance as health care institutions strive to
improve upon their operational efficiency as well as minimize costs (Chen et al, 2013).
2.5. Reforms in the Health Logistics and Commodity Management System
A five-year health sector reform under the Health Sector Support Project (HSSP), and
supported by the World Bank, was undertaken by the Ghana government from 1998 to 2002.
University of Ghana http://ugspace.ug.edu.gh

22
From 2002 to 2006, another health sector reforms project under the five-year medium-term
was undertaken. During this period, several reform packages were implemented under several
health reform initiatives. These initiatives were designed to specifically ensure that the reform
packages are successfully implemented.
In 2008, a review to assess the strengths and weaknesses of Ghana’s health commodity supply
and management system was undertaken by the USAID DELIVER PROJECT and
Management Sciences for Health (MSH)/Strengthening Pharmaceutical System (SPS)
(Adegoke, Bruce, Chimnani, Eghan, Tetteh & Veskov, 2008). In collaboration with the
Procurement and Supply Directorate (PSD) and the Foods and Drugs Authority (FDA), the
existence of weaknesses and inefficiencies as ‘gaps’ in the health SCM system was confirmed
(WHO, 2009; MOH, 2012). Prior to this survey, the Ghana Health Service (GHS) had in 2007,
and based on an extensive review, discovered weaknesses in the pharmaceutical SCM system
as well (MOH, 2012).
Based on these voids, the health supply management system was again subjected to multiple
transformations with varying suggested, tested and tried models. For example, the Master Plan
placed much emphasis on the promotion of rational use of drugs, improvement in access to
medicines, increase in quality assurance, and improvement in supply management system. In
spite of these interventions, the identified gaps have remained unaddressed and widened rather
than bridged1. The system as shown in Fig 2.1, is currently characterized by unsound
procedures and inaccessibility of medical products. There is also high and much higher
transportation costs at service delivery points than required for an efficiently and rationally
operating system (Denkyira, 2015).
1 8th Annual General Meeting and Continuous Professional Development Programme on the Health Services Supply Chain Practitioners Association, Ghana (HESSCPAG) Held in Cape Coast on 31st October, 2015
University of Ghana http://ugspace.ug.edu.gh

23
The system also reveals ineffective, sub-optimal and significant non-value-added steps in the
procurement, warehousing and distribution of medical commodities which results in higher
delivery cost for the end user. For example, a significant proportion of a health budget is
represented by storage and distribution costs, and transportation/freight costs can represent
multiples of the value of the drugs distributed to remote areas (WHO, 2009). The general price
level of highly subsidized drugs such as ACT remains relatively high. In addition, procurement
and distribution activities are hampered by unsound procedures, poor information linkages and
weak operation systems to reliable inventory control and demand information (Denkyira,
2015).
Figure 2.1: Ghana’s Health SCM System
(Source: WHO/MOH 2012) Note: CMS = central medical stores, RMS = regional medical
stores; PU = procurement unit; DHMT = district health management team; RHA = regional
health administration; SSDM = CBD = community based
In the wake of these deficiencies, it is believed that healthcare expenditure and associated
problems in the SCM arena which in many countries, account for more than 10% of GDP
(Ferry & Gebreiter, 2016), will increase further due to increasingly expensive medical
University of Ghana http://ugspace.ug.edu.gh

24
technologies, aging population and their mutual interactions. Ferry and Gebreiter (2016) noted
that health reforms are undertaken based on expensive medical technologies, aging populations
and their purported implications for healthcare costs. They argue that issues relating to
healthcare costs are historically contingent rather than inescapable consequences of
demographic and technological change, and that one constitutive and reflective of such
concerns is health service accounting. Clemens, Michelsen, Commers, Garel, Dowdeswell and
Brand (2014) showed that hospital reforms place emphasis on cost containment measures
rather than embarking on structural redesign of the health sector. They emphasized that,
problems associated with effective healthcare management can be resolved through effective
control of health costs and increase efficiency in the health service. Gyimah, Yellu, Andrews-
Annan, Gyansa-Lutterodt and Koduah (2009) undertook an in-depth assessment of the state of
medicine supply management system in Ghana. The research revealed the procurement Law,
ACT 663, as being present and active in guiding the procurement and supplies of medical
products throughout the country; good infrastructure for central level warehousing as the
strengths in the system, and well-defined distribution network. The following were however,
found to be a weakness in the medicines supply management system: limited circulation of
procurement guidelines and the National Essential Medicines list was found to be outdated.
Other findings were; quantification and forecasting of drug supply and related cost information
were found to be weak, and this arises from non-existence of effective coordination that links
the central and the periphery. Rules and guidelines to facilitate the recruitment of personnel,
other engagements and monitoring of drug supply were not in place. Suppliers’ information for
forecasting and quantification decisions which flow to the central procurement unit from the
facility level to was not forthcoming. The engagement of suppliers was not based on any set of
guidelines and rules. Although internal stock control systems have been developed by most
facilities, standardization for effective management is highly crucial. Optional storage and
University of Ghana http://ugspace.ug.edu.gh
25
handling equipment are not allowed by several of the lower level facilities and no standardized
structural plan that ensures adequacy of storage conditions has been developed.
Implementation of the proposed scheduled delivery system has not taken place. Also, the
supervision and monitoring of drug supply management activities which is supposed to take
place on regular basis have not been implemented across levels.
These weaknesses and shortcomings have negatively impacted on the system within the
logistics management system. Some of these include poor cost control in the health system as
well as reduction in healthcare services’ quality offered to the public. Schneller and Smeltzer
(2006) note that, traditionally considered an area of low value in the health care industry is
inventory management and distribution. However, extant literature suggests that potential
revenue can be generated as well as tremendous cost savings with improvement in the
management of inventory and distribution. A hospital can minimize its total expenses through
inventory management and distribution of finished medical materials, by at least two percent.
This does not represent just the amount providers spend on supplies and pharmaceuticals but a
percentage of total expenses.
In addition to a comprehensive transport policy, there was also a decentralized policy
formulated for the regional, district, sub-district and community level of health care.
Transportation plays a significant role in the delivery of health services and is considered an
indispensable resource in the health sector. Procurement, operations, maintenance, disposal and
replacements are also undertaken within a prescribed guidelines and are properly
communicated to the regional and district levels. Although the transport policy at the regional,
district, sub-district and community levels of health care has been formulated and established,
little has been achieved in the transport system. This unfortunate situation is even more
pronounced and more deplorable for health care delivery at the community level.
University of Ghana http://ugspace.ug.edu.gh

26
The major logistical functions in the health SC include forecasting, planning, procurement,
warehousing and the distribution of essential drugs, vaccines and contraceptives. The central
ministry offices across the regions are responsible for the performance and delivery of these
functions. Notoriously, these systems have been inefficient as well as incapable of offering
adequate supplies on a timely basis in many cases. It is therefore important that all the logistical
functions are integrated together by the organizations and other industry players in order to
ensure that healthcare logistics are effectively and efficiently managed. This will ensure regular
availability of health commodities and medicines at all levels all the time. This is largely
achieved by improving management efficiency through effective coordination of the
administration within the sector and the supply systems. However, the system still exhibits lack
of effective coordination.
A study by Bossert, Bowser, Amenyah and Copeland (2004) on the Ghanaian health logistics
systems finds that a bigger space in decision making was associated with better performance
for budgeting, financing and planning; whilst inventory control, procurement, logistics
management information systems, storage, client contact and training, were found to have
performed worse. The author sees some logistics functions within the logistics systems as one
that can be decentralized effectively while for some others, they should remain centralized. In
a similar situation, the report by the USAID/DELIVER project (2011) in Addis Ababa
indicated that information is required for the status of stock levels in order to make vital
decisions about procurement and resupply of drugs. It is also to ensure that hospital logistics
are essentially managed effectively to maintain transparency and accountability within the
health care sector. The report however, showed that the information was improperly organized
or not always easily available and this situation often leads to stock-outs, overstocks, and expiry
of drugs.
University of Ghana http://ugspace.ug.edu.gh

27
2.6 The Health Supply Chain
The hospital SC is unique and have some features not found in those of typical industrial
settings in many respects (Shah, 2004; Chen et al, 2013). First, as noted by Beier (1995),
hospital suppliers are mission critical to sustaining the public health. The needs of patients are
diverse. Hence, adequate, accurate and constant supplies of medical products are required by
clinical operations. Barlow (2010c) has noted that SCI translates its influence and reach to just
about every operational, clinical and performance areas in contemporary hospitals. Second,
hospital supplier selections are underpinned by physician preferences which are medically-
trained oriented, context-specific demands, and experience with specific brands as against
those of discrete parts manufacturing and consumer goods which normally involves the
forecast of production/sales as well as managing costs. As Roark (2005) points out, most often
there is a non-linkage between those who make the purchasing decisions and those who do the
actual buying. However, integration of the supply chain with perfect alignment of MAS
information bridges this gap. Third, as a consequence of the rapid technological and
innovations in medical practices that characterized the diverse types of healthcare supplies,
there is an intensive requirements for healthcare SC management information and effective
sharing of knowledge (Shah, 2004).
A concise definition of the health supply chain is given by the Rockefeller Foundation (2008,
p.1) as:
‘‘the network of entities that distribute products through planning and sourcing as well as
managing the information and finances associated with the distribution from manufacturers
through intermediate warehouses and resellers to dispensing and health service delivery
points.’’
University of Ghana http://ugspace.ug.edu.gh

28
This definition implies that the health supply chain embodies several key players with the
pharmaceutical supply chain being a major component as it captures the chemical plants,
pharmaceutical manufacturers, wholesalers, distributors, and retailers of drugs. Thus, the
health supply chain as defined above is complex, sophisticated and much more expensive to
operate (Shah, 2004). This is perhaps due to the multiplicity of institutional formats
(government, private, non-profit/profit oriented) as well as stakeholders (health administrators,
physicians, professionals, investors, governments, and community), complexities of
technologies being used, distinctive characteristics of health service operations, and dynamic
internal and external environment with diversity in industry and reimbursement policies across
the globe.
While many healthcare organizations recognize the adoption of SCM practices as vital to
overall healthcare management it becomes problematic when the methods, best practices, and
techniques originally designed for the mainstream industrial settings are directly applied (Jan
de Vries & Huijsman, 2011). In particular, the difficulties that confront healthcare institutions
when adopting a SCM philosophy is clearly manifested in the numerous projects they embark
upon. Often, these are targeted at the implementation of planning systems from an integrated
perspective regarding patient flows, and the establishment of partnership relationships among
different healthcare organizations.
Coupled with the foregoing challenges is the fact that for over two decades that SCM has been
around in healthcare institutions, its fundamental key concepts are misunderstood by health
professionals, which makes it more problematic in applying the SCM principles of mainstream
business organizations to healthcare operations. Often, the term ‘supply chain management’ is
used by healthcare professional with no firm idea about its underlying concepts (Schneller &
Smeltzer, 2006). Unfortunately, the health supply chain has, in most parts of the world, been
confined to contract and purchasing management as group purchasing organizations (Kwon,
University of Ghana http://ugspace.ug.edu.gh
29
Hamilton & Hong, 2011). Even with ordinary SCM of mainstream business organizations, it
goes beyond purchasing and contract management. Perhaps, the limited knowledge in the basic
SC concepts and principles have resulted in the narrow definition (e.g. purchasing) by decision
makers in healthcare, and not paying attention to rather the vital parts of the SC unexplored or
totally neglected and hence suboptimal outcomes. The next two sub-sections present the
elements of the health SC and its effective management to minimize costs.
2.6.1 Elements of the Health Supply Chain
Like the mainstream business organizations, elements of the health SC comprises capacity and
production planning, inventory and distribution planning, facility location and design, and
detailed scheduling (Shah, 2004). However, previous studies in the management accounting
field have, to a greater extent, focused on the inventory management component with little
attention given to the other elements (Samuel, Gonapa, Chuadhary & Mishra, 2010). It is
extremely rare to find studies on MAS design for facility location, production planning and
control, or scheduling and distribution even in mainstream business organizations let alone the
health SC.
It also appears that the health SC has been limited solely to the pharmaceutical SC since past
studies focused on the latter in relation to MAS design. Whilst the pharmaceutical SC
constitutes the bulk of the health supply system, it does not provide a complete description of
the players in the healthcare system and hence not fully represented by the health SC. Among
the key players in the healthcare industry include pharmaceutical manufacturers (primary and
secondary), wholesalers/distributors, hospitals/clinics, non-hospital pharmacies, governments,
regulatory bodies, investors, and consumers.
University of Ghana http://ugspace.ug.edu.gh

30
2.6.2 SCM in Healthcare Context
Healthcare SCM encompasses the universally identifiable elements such as facility location
and design, inventory management, capacity and distribution planning, and detailed scheduling
associated with business organizations (Shah, 2004). This is due to the fact that the handling
and treatment of customers (patients) of healthcare organizations is entirely different from
customers of mainstream business organizations. As Kwon, Kim and Martin (2016) contend,
the application of SCM practices in the healthcare sector not only involves the
production/procurement, storage and distribution of physical commodities such as drugs,
pharmaceuticals, medical devices and health aids, but also the flow of patients. The rate at
which patients demand various healthcare services underpins decisions which match demand
and supply throughout the supply chain.
Decisions on patients’ logistics and coordination issues are often related to the complexity and
variability of demand within a hospital. For example, a typical problem that confronts designers
of pharmaceutical SC has been that of striking a balance between future capacity and
anticipated demands (Shah, 2004). What makes it even more complex is the fact that such
decisions are often taken alongside the very significant uncertainty that emanates from
competitor activities and clinical trials.
In addition to the foregoing are other factors accounting for the complexity in healthcare supply
chains. First is the conflict between physicians and health administrators regarding the
procurement of prescription medicines which constitute the bulk of all medical supplies. Whilst
key decisions in this area are taken by physicians, they possess little knowledge and
understanding of SCM systems and practices (Scheller & Smeltzer, 2006). Second, the strong
regulatory and institutional pressures that accompany the operations of the healthcare industry.
As noted by Shah (2004), accurate sales forecasts are difficult to maintain in healthcare industry
not only because of the regulatory regime but also the difficulty in measuring the magnitude of
University of Ghana http://ugspace.ug.edu.gh

31
competitions that emanate from generic drugs. Third, lead times of the developmental cycles
of healthcare products are relatively longer compared to other medical devices.
Situations where the overall supply chain cycle time takes 300 days is not unusual. This is due
to the low manufacturing velocities that characterized the two stages of production and the
possible obstruction to activities by the need for quality assurance at various points. The two
stages as is evident in most pharmaceutical products include primary active ingredient
production referred to as multi-stage chemical processes or bioprocess, and secondary, referred
to as formulation production. According to Shah (2004), SC strategies and capacity planning
in relation to inventory management in the health sector as a whole are significantly affected
by the long lead times that characterize the development of pharmaceutical products. Finally,
unlike other business organizations, the distinctive nature of hospital operations coupled with
the sophisticated mix of patients makes it extremely difficult to predict supply consumption.
As Jan, de Vries and Huijsman (2011) contend, the straight forward application of industrial
oriented SCM practices in a healthcare setting is often impeded by these complexities.
In spite of these complexities, the health SC is recognised as one of the tools that have attracted
the efforts of scholars, researchers, governments, and healthcare providers in managing
healthcare costs while at the same time improving quality (Kwon et al, 2016). For example,
Pricewaterhouse Health Research Institute reported in 2008 that out of the yearly expenditure
of $2.2 trillion on healthcare, $1.2 trillion are incurred as a result of wastes in the supply
management system (Kavilanz, 2009). In Ghana, not only do the cost of distribution and
storage constitute a significant portion of the health budget (MOH, 2012), but also
transportation/freight costs represent multiples of the value of drugs distributed to remote areas
(WHO, 2009). In addition, SC costs represent the single largest health expenditure after
personnel costs (MOH, 2009). These wastes, according to Dooner (2014), are generated from
University of Ghana http://ugspace.ug.edu.gh

32
non-conformance to standardized cost processes which underpin the design and use of MAS
information.
2.6.3 Minimizing Health Supply Chain Cost
Although the phenomenon of SCM has been studied from several different perspectives with
emergence of several aspects such as SC optimization, network coordination, IT-enabled
supply chains, supply chain integration etc., the minimization of costs through a drastic
reduction or complete elimination of wastes as well as improvement in performance through
supply chain coordination constitute the core of SCM relationships (Jan de Vries & Huijsman,
2011). However, the contextual antecedents of SCM affect MAS design which ultimately
impact on supply chain costs. Studies such as Burns (2002) and Dacosta-Claro (2002) suggest
that about 48% of health supply chain costs are reduced through the implementation of
effective SCM practices.
However, a significant scope for improving the overall performance of the supply chain
remains unexplored (Lega, Marsilio & Villa, 2013). It has been argued that effectiveness and
efficiency coexist in supply chains (Kwon et al, 2016). This translates to mean that efficient
management of the health supply chain creates surplus in resources which can be diverted or
reinvested for the benefit of customers (patients) and other stakeholders.
2.7 Nature of MAS Design
Fundamentally, a MAS design can be viewed from two main viewpoints: integrated accounting
systems design where the MAS is integrated into the financial accounting system and the
records of the latter serve as a database for the former, or a separate system for the MAS exists
where besides the financial and tax accounting records, a third set of books is created
(WeiBenberger & Angelkort, 2011). The integrated approach suggests that the management
accounting techniques (e.g. budgeting, product costing and standard costing), reporting and
University of Ghana http://ugspace.ug.edu.gh
33
performance measurement etc., are derived from the database of the financial accounting
records. Such MAS design, which is typical of Anglo-American firms provides information
not only at minimal incremental costs, but also facilitates the reconciliation of the internal and
financial performance measures (weiBenberger & Angelkort, 2011).
A limitation of this approach is that depending on the underlying accounting regulation, the
data on financial accounting may be unsuitable for management control and decision-
influencing purposes (Kaplan, 1984). In the ‘separate’ or ‘dual’ design which has been
traditionally employed in continental Europe particularly in German-speaking countries (Jones
& Luther, 2005), a completely different third set of books is created alongside the financial and
tax accounting records. A third approach to MAS design referred to as hybrid form or partial
integration (Angelkort, Sandt & Weißenberger, 2009) places restriction on the integration of
management accounting and financial information. For example, information relating to top
management or confidential aspects of the databases of the financial records could be restricted.
Past studies on the MAS-contingency framework paid little or possibly no attention to the
design type of the MAS adopted by organizations and the extent to which such designs might
be affected by contextual factors. To a greater extent, the focus has been on the existence of a
particular technique with varying descriptions of the MAS other than the extent and manner of
their use (Otley, 2016). Additions to the MAS variable rather than identifying which design
type is suitable within a particular context has been the norm. For example, following the focus
away from the use of budgets as the MAS variable, subsequent studies have conceptualized
and defined the MAS from diverse perspectives.
In the study of Chenhall and Morris (1986) and that of Bouwens and Abernethy (2000) for
example, the MAS was defined in terms of broad scope, timeliness, aggregation and
integration. In Gerdin (2005a), the MAS was described based on its rudimentary, broad scope
University of Ghana http://ugspace.ug.edu.gh

34
and traditional focus. The study of Gerdin (2005a) was based on the assumption that certain
levels of information provided by the MAS is irrelevant to some context factors hence rarely
leading to such a classification. Others have conceptualized the MAS based on Porter’s (1985)
strategic priorities of low cost strategy and differentiation strategy. However, drawing a
distinction between the MAS and the design type is an important dimension of the MAS-
contingency combination. The reason for the distinction is that the type of design adopted for
the implementation of a particular MAS information requires that the system ‘matches’ with
contextual or situational factors. This requirement of ‘matching’ the MAS with the context
factors is termed contingency-fit (Otley, 1980). As Otley (1980, p.27) states: ‘‘specific aspects
of an accounting system must be identified by a contingency theory and this must be related to
certain defined circumstances as well as demonstrate appropriate matching’’.
2.8 Functions of the MAS Information in Healthcare Management
Although the management accounting function has been conceptualized from several different
angles and assigned different variables to its design and measurement, two main functions
characterize its design: 1) reduces agency costs and 2) facilitates managerial decision-making
process (Davila & Foster, 2005). The former focuses on effective monitoring of performance
in the contracting process between principals and agents while the latter focuses on the update
of managers with both financial and nonfinancial information in their decision-making process.
In the principal-agent setting, managers are contracted to act on behalf and in shareholders’
interest who have contributed economic resources to the affairs of the organization.
Although the healthcare industry ranks among the largest economic sectors in many countries,
and its complexity and richness allows a broad range of economic theories on compensation
contracts, competition, and costs and management behaviors to be studied, the model of
University of Ghana http://ugspace.ug.edu.gh
35
principal-agent relationships of typical mainstream business organizations is not a descriptive
of the typical healthcare setting (Cardinnaels & Soderstrom, 2013). Therefore, the health
system requires a more sophisticated and detailed MAS information as the cost information
generated by hospitals are subsequently used by regulatory bodies for updating or setting prices
associated with public health services (Raulinajtys-Grzybek, 2014). This is because unlike
mainstream business organizations, healthcare providers in most parts of the world operate on
a refund basis (e.g. Ghana’s Health Insurance Scheme) and are legally required to allocate costs
in a predefined manner which MAS information provides (Sutherland, 2015). This legal system
in most cases, follows the step-down cost allocation mode from service departments (such as
administration, laundry, out-patient department, etc.) to internal revenue-generating
departments (such as laboratory, surgery, maternity, etc.) and to patients in some cases.
2.8.1 Costing Systems Design in Hospitals
Inputs such as capital, labour, materials and supplies are normally employed by hospitals to
offer healthcare services consumed by customers (patients) during their episode of care. Since
the services offered (including hours of nursing and X-Ray etc.), are normally associated with
intermediate products, business rules and regulations that govern the generation and
apportionment of costs associated with hospitals’ intermediate products are in most hospital
operations, codified in activity based guidelines (Chapman, Kern, Laguecir, Angele-Halgand,
Angert & Campenale, 2013). The assignment of intermediate product costs to patients’
hospitalization is a result of the output generated by activity-based costing (ABC) systems. As
a consequence, ABC systems have widely been recognized as costing system designs that
provide cost reduction and better cost management information in hospital operations
(Cardinaels, Roodhooft & van Herck, 2004; Sutherland, 2015). ABC systems provide more
detailed costing information relating to hospital activities that yield better cost aggregation for
effective decisions.
University of Ghana http://ugspace.ug.edu.gh

36
Despite this wide recognition and advantages associated with such costing systems as
providing cost-effective solutions to hospital operations, it has generally been documented that
the effective design and efficient implementation of such costing systems is largely influenced
by hospital specific factors (Devine, O’clock & Lyons, 2000; Lawson, 2003; Cardinaels et al,
2004). Issues bothering on fuller support of medical personnel for the use of particular costing
systems, internal financial agreement involving physicians’ type of contract, awareness of
problems with existing costing systems etc., need to be taken into account. In particular, it has
been established that unlike mainstream business organizations, different approaches are
required in cost system design in hospitals, and that the interest of physicians should not be
underestimated in the process of cost systems’ redesign.
2.8.2 Formal MAS Design in Health SCM Decisions
Whilst the accounting literature provides anecdotal evidence of the inappropriateness of
traditional MAS practices to capture and provide SC data for managerial decisions (Otley,
1980; Schulze, Seuring & Ewering, 2012), and the subsequent significant eroding of
confidence in the MAS, little empirical studies that systematically examine the link between
SCM and management accounting performance have been accumulated. The traditional
systems which focused primarily on cost control using tools like variance analysis, marginal
costing, responsibility accounting, standard costing, etc., are task segregation and efficiency
oriented, and well suited for mass producers of standard products with unchanging
characteristics (Chapman et al, 2013). In addition, the implicit task segregation in variance
analysis and responsibility accounting is antithetical to the cross-functional coordination
required in SC networks.
It has been argued that formal MAS design in healthcare organizations has, over the years, been
problematic despite its relevance in addressing concerns from the growing regulatory and
competitive pressures (Aidemark & Funck, 2009; Cardinaels & Soderstrom, 2013). Issues
University of Ghana http://ugspace.ug.edu.gh
37
bothering on goal congruence’s reliance on monetary incentives, the high degree of influence
over operational processes by physicians and nurses, the imposition of a wide range of priorities
by stakeholders who are classified as highly influential, and complex and diverse work methods
and objective functions, and austere budgets that generate unparalleled complexities for
effective design and use of MAS, are just a few of the numerous challenges faced by hospitals
(Abernethy et al, 2007). In addition, it has been reported by many studies in management
accounting (e.g. Abernethy & Stoelwinder, 1995; Jones, 2002; Abernethy et al, 2007) that the
regular conflicts that arise from health administrators’ professional objectives and that of
clinicians2 has been noted to be a hindrance to, and curtailment of effective MAS design.
Notwithstanding, it is strongly believed that effective design and use of MAS information
enhances the identification of value-adding processes and costs across organizational
boundaries hence investments in innovative and sophisticated cost-accounting tools and
systems by healthcare organizations in recent years (Cardinnaels & Soderstrom, 2013). To this
end, past studies in management accounting (e.g. Bai, Coronado & Krishnan, 2010; King &
Clarkson, 2015; Harlez & Malagueno, 2016) have called for research that provides more
insights and understanding of the design and use of MAS in hospitals. By this directive, the
antecedent conditions of effective performance measurement systems in hospitals have also
been emphasized by prior literature (Ballantine, Brignall & Modell, 1998; Cardinaels &
Soderstrom, 2013).
2.8.3 Inter-Health Organizational Cost Management in Supply Chains
The existence of an organization is normally linked to another organization which may be a
supplier of raw materials and/or other services for the running of the former, or a buyer of the
goods and/or services produced. Based on these arrangements, organizations of all kinds are
2 Are in dominance when it comes to core operations of hospitals but the implicit assumption is that they can be controlled through hospital strategies
University of Ghana http://ugspace.ug.edu.gh
38
said to be embedded in supply chains (Dekker, 2016). Like mainstream business organizations
that comprise discrete parts manufacturing and fast-moving consumer goods, healthcare
institutions are embedded in a network of supply chains made up of the focal organization,
suppliers upstream and buyers downstream. For example, none of the constituents of healthcare
delivery, i.e. hospitals/clinics, primary and secondary pharmaceutical manufacturers,
wholesalers, distributors, and retailers of medical suppliers and other health commodities exist
in isolation.
The non-existence of standards for the definition and composition of costs and the
inappropriateness of intra-firm cost accounting tools in the SCM context (Schulze et al, 2012)
have resulted in the development of inter-firm cost accounting tools referred to as inter-
organizational cost management (IOCM). Normally labelled as advanced MAS, IOCM is a
strategic cost management tool used to facilitate the management of costs across organizational
boundaries in supply chains. More specifically, it extends the application of cost management
and control strategies beyond the conventional internal cost management practices to include
cost management among SC partners (Fayard et al, 2012).
The management of costs among these entities from focal organization perspective (e.g. a
hospital) is necessary as far as cost minimization in its operational activities is concerned. As
a consequence, Dekker (2000) pointed out that the design of MAS information in organizations
must be such that they increasingly operate across organizational boundaries.
Although a number of cost management strategies or techniques such as ABC, target costing,
kaizen costing, total cost ownership etc., constitutes IOCM, a common theme that underpins
IOCM is the minimization of costs and other cost control strategies that create value for
organizations in supply chains (Fayard et al, 2012). The ability of firms to identify significant
inter-firm cost saving opportunities is facilitated by IOCM (Schulze et al, 2012). Since this
University of Ghana http://ugspace.ug.edu.gh
39
goal is facilitated by the cooperative and collaborative actions of members in the SC, it
demands organizational resource which takes the form of set of tools.
Advanced MAS (e.g. ABC, value chain analysis, IOCM) not only coordinate supply chain
relationships (Fayard et al, 2012; Anderson & Dekker, 2014) by planning, measuring,
supporting and assessing supply chain activities and performance (Van de Meer-Kooistra &
Vosselman, 2000; Hammad, Jusoh & Oon, 2010), but also provide information to oil the
wheels of supply chain relationships (Burritt & Schalttegger, 2014).
2.9 Chapter Summary
In this chapter, the context of the study has been presented. It outlined the SCM challenges that
characterized Ghana’s healthcare system as well as the weak accounting systems. The chapter
notes that Ghana’s health SC is highly centralised and operates on a three-tier system consisting
of the Central Medical Stores (CMS), Regional Medical Stores (RMS) and Service Delivery
Points (SDP). The supply of medical products begins from the CMS to the RMS, and then to
the SDP in turn. This arrangement is however, characterized by deficiencies and weaknesses
as identified ‘gaps’. Various solution strategies have been pursued by governments yet the
problem continues to persist and have widened than before. Individual studies have also
identified a number of shortcomings and weaknesses in the system. The accounting system has
been also identified as weak and ineffective in controlling the SCM activities of healthcare
institutions. The chapter notes that the accounting system does not support the strategic
direction of healthcare management and needs total revision. It is believed that the institution
of proper MAS which is the focus of this thesis will contribute to solving some of these
problems and challenges.
The chapter also analyzed the characteristics of the health SC and the extent to which the MAS
information relates to its effective and efficient operation. Although the health SC and that of
University of Ghana http://ugspace.ug.edu.gh

40
mainstream business organizations and discrete parts manufacturing concerns have elements
that are similar, the constituents of the health SC encompasses the elements commonly found
in mainstream business organizations. This suggests that the approaches and procedures
employed in MAS design and its implementation in mainstream business organizations are
unlikely to work perfectly in the SCM systems of healthcare institutions. The chapter also
explained the implications of costing system design in hospitals where ABC systems are known
to provide effective cost system design as a consequence of the nature of hospital operations
normally termed as intermediary products. Finally, the chapter highlighted the importance and
relevance of the MAS’s application in the effective management of the health SC.
University of Ghana http://ugspace.ug.edu.gh

41
CHAPTER THREE
CONTINGENCY-BASED MANAGEMENT ACCOUNTING STUDIES
3.1 Introduction
Having discussed the study’s context, MAS design and the health supply chain, a detailed
analysis of the empirical literature on contingency-based management accounting research is
considered in this chapter. As pointed out in the following section, the body of literature on
these studies are mixed, inconsistent and fragmentary in nature. In line with these initial
reviews, the chapter begins with the theoretical underpinnings of contingency fit and the
processes involved in conceptualizing contingency fit and its attainment in management
accounting literature. This is followed by an analysis of the modelling approaches that have
been adopted to examining contingency fit. A discussion of the diversity in the selection,
definition and measurement of contextual and MAS variables is then presented to establish a
proper relationship between extant contingency literature and the current study. Finally, a
review of the linkages among three key areas of contingency hypotheses testing: 1) formulation
of verbal hypotheses relating to specific fit models, 2) the relevant statistical methodology
employed in testing the fit hypotheses, and 3) the interpretation of results is presented. A
summary of the key findings closes the chapter.
3.2 Theoretical Background of Contingency Fit
Central to contingency theory is the concept of fit between structure and context (contingency)
characteristics of organizations although its attainment still remains contested in the
contingency literature (Donaldson, 2001). Fit is the underlying principle of contingency theory
which suggests that fit between variables is important for achieving high performance. This is
so fundamental to the context-structure relationship that failure to attain such a fit results in
University of Ghana http://ugspace.ug.edu.gh

42
outcomes that are inferior. These outcomes are normally a typical of some aspects of
performance (Meilich, 2006; Burkert et al, 2014). In this regard, ‘‘it is generally considered as
the ‘‘heart’’ of contingency theory’’ (Donaldson, 2001, p.181). Hence, finding an appropriate
match between context and structure has been the fundamental notion of contingency-based
MAS design. This matching concept has been appropriately labelled and termed ‘‘contingency-
fit’’ in both the organizational and management accounting literatures alike (Jermias & Gani,
2004).
Investigating the MAS-contingency fit relationships has resulted in several different types of
fit (discussed in the sub-section following), and has led to some confusion and misconceptions
about the fit concept and how it is attained. Drawing on the contingency theory of general
organizational literature, several scholars in the management accounting arena have sought to
investigate the fit relationship between context factors and MAS design. Whilst subsequent
studies expanded the MAS variables in terms of definition and measurement (e.g. Chenhall &
Morris, 1986 conceptualization of broad scope, timeliness, aggregation, integration, etc.), that
of contextual variables (e.g. strategy, size, structure, environmental uncertainty, etc.) remained
fixed and imported from the general organizational literature. However, after decades of
research, there still remains unsettled issues in the management accounting field as the results
accumulated so far have not consistently supported contingency theory’s arguments (Burkert
et al, 2014).
The challenge for management accounting researchers has been how to theoretically derive the
form of fit to be predicted and tested and fail to reject a fit which is true or actually reject one
which is false. This is a key dimension of contingency studies as it provides a basis for the
progression of management accounting knowledge that is theory-consistent. Re-stating Otley
(1980, p. 451) which states that ‘‘specific aspects of an accounting system must be identified
by contingency theory, and this should be associated with certain defined circumstances as well
University of Ghana http://ugspace.ug.edu.gh
43
as demonstrate an appropriate matching,’’ specific aspects point to the specificity of the MAS
variable in relation to theory formulation and usage. Defined circumstances and appropriate
matching differ in the conceptual and empirical differences respectively between a universal
theory and contingency theory of accounting. The identification and testing the true form of
contingency fit warrants an analysis of the types of contingency fit models as discussed in the
subsections that follow.
3.3 Contingency Fit Models
Two main conflicting paradigms: the Cartesian school of thought and the Configuration School
underpin the fit concept. Drawing on these paradigms, researchers from both the general
organizational and management accounting fields conceptualize the relationship between
structure (e.g. MAS variable such as low cost strategy or measurement diversity) and
contingency (e.g. Strategy or perceived environmental uncertainty) from three different levels
of analysis; 1) Cartesian versus Configurational view (Mintzberg, 1983; Miller & Friesen,
1984; Meyer, Tsui & Hinings, 1993; Donaldson, 1996), 2) Congruence versus Contingency
(Drazin & Van de Vein, 1985; Chenhall & Morris, 1986; Gerdin, 2005a, Dunk, 2011), and 3)
Matching versus Multiplicative (Gerdin & Greve, 2008; Burkert et al, 2014). Each of the above
conflicting paradigms is briefly discussed in the next three sub-sections.
3.3.1 Cartesian vs. Configuration
The principal difference between the Cartesian school and that of the Configurational school
lies in their dominant mode of enquiry (Meyers et al, 1993). Advocates of the Cartesian
approach contend that contingency fit between structure and context is a continuum with
varying degrees of fit between the dimensions of structure and pairs of contingency variables
that allow organizations to make small frequent movements from one state of fit to another
University of Ghana http://ugspace.ug.edu.gh

44
(Donaldson, 1996). The dominant mode of enquiry in this paradigm is characterized by what
is described as reductionism. In other words, a limited number of contingency variables are
assumed to offer explanations that are general to the organizational structure (e.g. MAS
design). The extent to which single contextual (contingency) factors influence single structural
attributes and the resulting context-structure combination on performance is the main focus.
Proponents of the configuration paradigm argue that only a few states of fit between structure
and context exist and that a quantum jump of fits from one state of fit to another will have to
be made by organizations. The configuration view opposes partial analysis of context-structure
variables rather, views the context-structure combinations in a holistic manner. This holistic
analysis assumes that the understanding of relationships can only take place based on the
simultaneous analysis of many contextual and structure variables. Whilst the configuration
approach requires researchers to explore only the non-performance effects of the context-
structure relationships, the Cartesian researcher must show that a higher degree of fit is
associated with a higher performance since it assumes varying degrees of fit. Figure. 3.1
illustrates examples of typical associations between structure and context according to the
Cartesian and Configurational approaches as indicated in (Figure 3.1a) and (Figure 3.1b)
respectively.
As Figure 3.1a depicts, both contextual and structural factors are defined as continuous
variables as well as the fit relationships between them giving rise to many points of fit
(Donaldson, 2001). The numerous points of fit result in a continuous solid fit line with high
performance associated with high levels of fit. Figure 3.1b illustrates fit as system states
(configurations) where organizations make quantum jumps to substitute one state for another
when the cost associated with being out of step becomes quite prohibitive. As theory prescribes,
most firms can be assigned to a limited set of configurations which are in existence. A
researcher only identifies the processes and set of organizational structures that are feasible and
University of Ghana http://ugspace.ug.edu.gh

45
effective for different context configurations, and also provides insights into both internal
consistencies and inconsistencies of organizational structure patterns and processes (Drazin &
Van de Ven, 1985, p. 521-522).
Figure 3.1: Cartesian and Configurational Models
Figure 3.1 (a) Figure 3.1 (b)
(Source: Adapted from Gerdin & Greve, 2004)
3.3.2 Congruence vs. Contingency
The congruence and contingency fit models are respectively, antecedents of the
Configurational and Cartesian paradigms. The congruence (also known as selection) model is
a bivariate form of fit model which assumes that organizations that inferiorly combine structure
and contingency variables do not survive and for that matter vanish quickly either by extinction
or by adaptation. In other words, fit is assumed to be the result of a natural selection process
which ensures that only the best performing companies survive and are visible for observation
purposes (Drazin & Van de Vein, 1985). Quick to disappear are unfit combinations of structure
and contingencies. In this model, the fact that unfit combinations of contingency variables and
structure vanish quickly presupposes an unforgiving environment for low performing firms. In
other words, surviving organizations are those whose structural characteristics are congruent
with the organization’s contingencies.
University of Ghana http://ugspace.ug.edu.gh
46
The research task under this model is to examine the nature of context (contingency variable)
and structure (MAS variable) relationships with no examination of their impact on
performance. The MAS variable is assumed to be dependent on contextual variables for its
design and that fit results implicitly from the natural selection forces that link the variables. Fit
is determined by the correlations between contingency and structural variables or regression of
the structural variable on the contingency variables. Testing this link with performance is
therefore regarded as unnecessary.
The underlying assumption of either survival or a complete disappearance is however
unrealistic because in real-world cases, such a harsh environment is not only a non-reflection
of the success of most organizations, but also rarely exists. Organizations fail yet they continue
to survive until things get improved. They do not disappear suddenly or entirely as suggested
by the model. In addition, this model suggests that the outcome variable assumes a categorical
dimension (survive or vanish) yet, this form of fit does not incorporate any variations of
outcome. The implication is that all surviving firms are assumed to be equally fit which is not
the case in real-world situations. Moreover, it has been argued that the non-existence of
performance in this model is a major shortcoming because as stated by Pennings (1992, p. 274)
signalling survival of the fittest as a proxy for performance is too crude (Pennings, 1992,
p.274). Furthermore, the tendency for fit to be undetected is high when the so-called selection
forces are weak. A linear correspondence between the contingency and structural variables is
imposed by this model, which may not exist in a sub-sample leading to erroneous acceptance
of fit.
Following these arguments, contingency models (e.g. matching and moderation forms of fit)
have been developed where fit is conceptualized as a positive impact of context-structure
combinations on performance (Drazin & Van de Vein, 1985). This development stems from
the argument raised by contingency researchers that fit is a continuum and that companies
University of Ghana http://ugspace.ug.edu.gh

47
move between states that are fit and those that are not fit on this continuum (Donaldson, 2001)
so it takes a long time for companies to reach the so-called equilibrium stage specified by the
selection model. Furthermore, since on this continuum, companies of different kinds are
situated at different places, it provides room for the analysis of the performance effects of the
context-structure combinations.
As stated previously, the fit concept is very much central to the contingency model in that
inferior outcomes result in the event of failure to attain such a fit. These inferior outcomes are
typical of some aspects of performance. Unlike the congruence model in which unfit
organizations disappear, both high-performing and low-performing organizations are assumed
to exist in the contingency model. This is due to successful combinations of context and
structure that take place to affect performance. Examining performance variations with respect
to context-structure interactions is the research task. To date, the congruence and contingency
models still remain two irreconcilable ideas about the concept of fit (Burket et al, 2014). The
typologies of contingency fit models used in management accounting studies are now
discussed.
3.4 Typology of Contingency Fit Models
The types of fit models outlined in this study can be found in both the general organizational
literature (e.g. Meilich, 2006; Donaldson, 1996, 2001; Venkatraman, 1989; Drazin & Van de
Vein, 1985; Schoonhoven, 1981; Southwood, 1978) and the management accounting literature
(e.g. Hartmann & Moers, 1999, 2003; Gerdin & Greve, 2004, 2008; Burkert et al, 2014). The
contingency theory of organizational structure is heavily drawn upon by the management
accounting discipline hence, reference to scholars in the general organization field is highly
relevant for a study of this nature. Two main forms of classifications can be identified: those
based on the statistical technique required by the fit type and those based on the fit’s theoretical
University of Ghana http://ugspace.ug.edu.gh

48
underpinning. In the statistical approach, the fit is classified as bivariate, deviation score or
residual analysis, and interaction (Meilich, 2006) whereas those based on theoretical
classification include selection or congruence, matching, moderation, mediation, system, and
multi-fit (Hartmann & Moers, 1999, 2003, Gerdin & Greve, 2004, 2008; Burkert et al, 2014).
The two different forms of classification stem from the fact that a specific relationship between
the structural, contingency and outcome variables is postulated by each form of fit, which is
associated with different theoretical interpretation and requires the application of different
statistical tests. The different typologies of fit and underlying theoretical interpretations and the
required statistical methodology has led to some confusion in the management accounting
literature (Chenhall & Chapman, 2006). In the next four sub-sections that follow, each
contingency fit model together with the theoretical background is discussed while a detailed
discussion of the statistical approaches to testing each model of fit is presented under section
3.5.
3.4.1 Selection Fit Models
As a recap, in this form of analysis, survival constitutes the outcome measure and requires that
surviving organizations exhibit appropriate congruence between contingency and structural
variables. The basic assumption is that structure depends on context with no examination of
whether these context-structure combinations affect performance, hence, a congruence form of
fit (Drazin & Van de Vein, 1985). Proponents of this approach argue that testing the link with
performance is unwarranted because fit is implicitly assumed to emanate from a selection
process that is natural and ensures that only organizations with best performance survive and
at any point in time, can be recognized. Some measure of association (e.g. correlation and
regression) is required to empirically examine the interdependence between context and
structure.
University of Ghana http://ugspace.ug.edu.gh
49
In the management accounting context, the attainment of this type of fit simply means that
organizations have adapted their MAS fully to what their contexts demand or managerial
choices (Hartmann, 2005), and that differences in performance are not expected since
companies have reached equilibrium in their choices of the context-structure combinations.
The research task merely explores the context-structure relationships with no examination of
their effect on performance. Following this approach, many management accounting scholars
have examined the determinants of MAS design from a contextual perspective without
examining how such context-MAS combinations affect performance (e.g. Chenhall & Morris,
1986; Abernethy & Lillis, 2001; Gerdin, 2005a; Ylinen, & Gullkvist, 2012). The statistical
technique used to examine the extent to which MAS variables are related to elements of context
involves tests of associations such as correlation analysis or multivariate analysis such as
multiple regression. As noted earlier, the risk that this approach reaches incorrect conclusions
is very high.
3.4.2 Matching Fit Models
The matching form of fit model examines the impact of the MAS variable and contingency
variable combinations on performance. It is the classical form of fit model with iso-
performance on the fit line (Schoonhoven, 1981; Donaldson, 2001), and assumes an optimality
between the contingency variable and specific dimensions of the MAS. A unique level of an
MAS is assumed to match each level of a contextual (contingency) variable which then
maximizes performance. More specifically, for each level of a contextual variable there is
assumed to be a unique level of a structure (MAS variable) that maximizes performance. Any
deviations (or mismatch) in either directions between the specific level of the contextual
variable and the appropriate MAS variable results in decline in performance.
The key concept underlying the matching fit model is the iso-performance assumption. This
assumption implies that fit is the result of MAS – contingency combinations that are severally
University of Ghana http://ugspace.ug.edu.gh
50
combined (matched), each of which is expected to predict performance at the same level. This
results in the matching fit-line which is conceptualised (under the Cartesian school of thought)
as the line that joins all the points of fit derived from matching the appropriate MAS with the
level of contextual variable. The iso-performance assumption is normally reflected in the fit
line with zero values as illustrated in Fig 3.2. In this Figure, panel ‘A’ depicts a distinct feature
exhibited by the matching form of fit. Considering the fact that the context variable is the locus
of control of an organizational structure and the structural dimension is MAS variable
represented by budgetary participation, there might be a unique level of locus of control and
budgetary participation combinations that maximizes performance.
A curvilinear (i.e. inverted U-shaped) relationship exists between the MAS variable and
performance in the matching fit model. This association implies that only one optimal MAS
variable is attained for a given level of the contingency variable. Any deviation in either
direction (either ‘‘over fit i.e. too many MAS, e.g. too many measurement diversities or under
fit, i.e. too few MAS, e.g. performance indicators that are too few’’ (Meilich, 2006, p.167)) are
equally harmful as they cause the same negative effects on performance. Panel B depicts the
iso-performance on the fit-line with the same level of performance of MAS-contingency
combinations3.
3 This unique level is determined as having an equal score by the scales of measurement used.
University of Ghana http://ugspace.ug.edu.gh
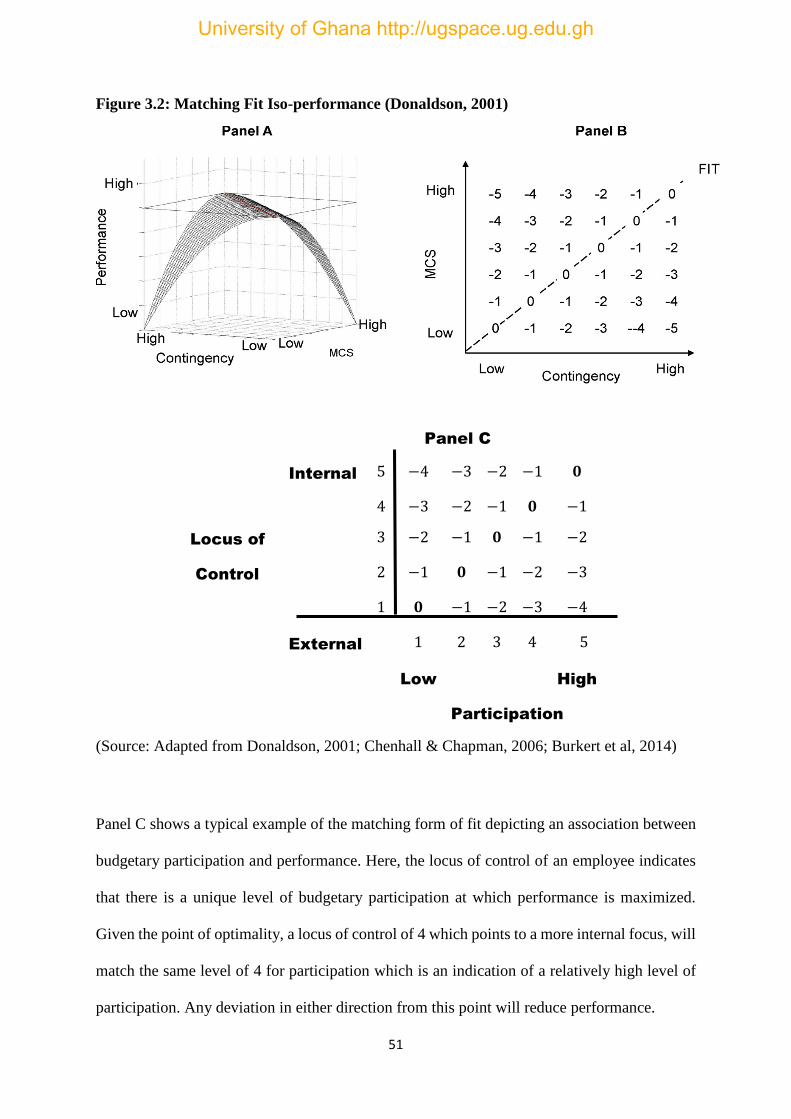
51
Figure 3.2: Matching Fit Iso-performance (Donaldson, 2001)
Panel C
Internal 5 −4 −3 −2 −1 𝟎
4 −3 −2 −1 𝟎 −1
Locus of 3 −2 −1 𝟎 −1 −2
Control 2 −1 𝟎 −1 −2 −3
1 𝟎 −1 −2 −3 −4
External 1 2 3 4 5
Low High
Participation
(Source: Adapted from Donaldson, 2001; Chenhall & Chapman, 2006; Burkert et al, 2014)
Panel C shows a typical example of the matching form of fit depicting an association between
budgetary participation and performance. Here, the locus of control of an employee indicates
that there is a unique level of budgetary participation at which performance is maximized.
Given the point of optimality, a locus of control of 4 which points to a more internal focus, will
match the same level of 4 for participation which is an indication of a relatively high level of
participation. Any deviation in either direction from this point will reduce performance.
University of Ghana http://ugspace.ug.edu.gh
52
The use of the term ‘‘iso-performance’’ was coined by Donaldson (2001). It establishes the
fact that the matching fit that indicates performance is determined by a distance away from the
fit line and not where it is positioned since performance is the same at any point on the fit line.
The matching fit model is however, not tested in this research because this model cannot be
tested via structural equation modelling (Burkert et al, 2014). This is due to its curvilinear (U-
shape) nature of the MAS – contingency combinations. Furthermore, only one MAS variable
and one contingency variable can be tested at any one time on performance.
3.4.3 Interaction (Moderation) Fit Models
Interaction form of fit models investigate the extent to which the MAS-contingency
combinations affect performance. Specifically, these models consider how the MAS variable,
contingencies (or their context) and performance can be brought together. To many accounting
researchers, the absence of performance in the selection fit model is a major shortcoming
because performance is an important variable that cannot be ignored (Chenhall & Chapman,
2006). The argument is that whilst organizations move toward optimal combinations thereby
attaining the equilibrium prescribed by the selection forces, some firms would still be lagging
behind, and in the process of reaching the optimum combination. Others might have changed
their context (e.g. strategy, size, or structure) and may be in the process of adjusting their MAS
to suit or match the new situation. The attainment of an optimal combination of the MAS –
contingency variables is characterized as a dynamic process where organizations move in and
out of equilibrium. In this regard, poor performing organizations with a mismatch of MAS –
contingency combinations are likely to be identified by researchers at any given point in time.
This situation has given rise to the matching fit (discussed in the previous sub-section) and the
moderation fit models.
The moderation fit model assumes that the association between an independent variable and a
criterion variable is a function of a third variable called the moderator. The underlying theory
University of Ghana http://ugspace.ug.edu.gh

53
specifies that the effect an independent variable has on a criterion variable is moderated by a
third variable which is exogenous or uncontrollable. More specifically, the impact of an
independent variable on a criterion variable is contingent upon a third variable (Chenhall &
Chapman, 2006; Luft & Shields, 2003; Venkatraman, 1989, Baron & Kenny, 1986). Unlike
the matching fit model, there is a linearity in the relationship between the MAS variable and
performance, and this gives rise to different levels of variations of the contingency variable.
Conceptually, the relationship between the MAS variable and performance is determined by
the contingency variable as shown in Fig 3.3.
Figure 3.3: Moderation form of Fit Relationship
(Source: Author’s own construction based on Barron & Kenny, 1986)
The contingency variable variations at different levels given by the MAS variable and
performance result in a monotonic or non-monotonic moderation forms of fit. These are further
classified under four sub-form of interaction fit comprising monotonic, non-monotonic
(symmetrical), monotonic and cross over, and ordinal forms of moderation fit. For non-
monotonic fit type, the impact of the MAS variable on performance is positive for the
contingency variable at one level and negative for the contingency variable at another
(Schoonhoven, 1981). In this case the lines cross each other within the range of data as shown
in Fig 3.4. Fig 3.4 (a) depicts a monotonic cross over interaction where a positive relationship
always exists between the MAS variable and performance but the lines do not cross over
MAS Variable
Performance
Contingency
University of Ghana http://ugspace.ug.edu.gh

54
outside the range of data. Fig 3.4 (b) on the other hand, shows a non-monotonic (symmetrical)
interaction as discussed above.
Figure 3.4: Non-Monotonic (Symmetrical) and Cross-Over Interaction
Figure 3.4 (a): Monotonic and Cross Over Interaction Figure 3.4 (b): Symmetrical and
Cross Over Interaction
The other two sub-forms of moderation fit which depict a linear monotonic interaction and
ordinal forms of fit are illustrated in Fig 3.4 (c) and (d) respectively. In Fig 3.4 (c), which shows
a monotonic interaction, a positive association always exists between the MAS variable and
performance but as Donaldson (2001, p. 191) argues, the level of the contingency variable
affects the MAS variable.
Figure 3.4 (c) Figure 3.4 (d)
University of Ghana http://ugspace.ug.edu.gh
55
(Source: Adapted from Burkert et al, 2014)
3.4.4 Mediation Form of Fit
In the mediation fit model, the exogenous variable impacts a criterion variable which then
impacts performance. That is to say that the association between the contingency variable and
performance is affected by the MAS variable which acts as an intervening mechanism between
the exogenous and endogenous variables. Although this form of contingency fit has been tested
in many management accounting studies (Bouwens & Abernethy, 2000; Gerdin, 2005a;
Soobaroyen & Poorundersing, 2008; Hammad et al, 2013), such studies failed to clearly
distinguish a partially-mediated variable from full-mediated variable. The interpretation often
given to mediation forms of fit hypothesis has been that an indirect relationship existing
between the contingent variable and performance or a relationship exists between the
contingency variable and performance acting through the MAS variable. As Burkert et al
(2014) point out, such analysis does not establish true mediation because there were no
theoretical arguments nor empirical tests for true mediation by those studies.
In addition, a confusion arising from both the general organizational literature and management
accounting literature regarding partial mediation and full mediation still remains (Burkert et al,
2014). Prior literature has just by mere inspection, labelled the models in Fig 3.7 (a) and (b) as
full mediation and partial mediation respectively with no consideration given to the theoretical
as well as statistical conditions that need to be satisfied (Hartmann & Moers, 2003, Hartmann,
2005; Burkert et al, 2014). In this regard, prior literature (e.g. Hartmann, 2005; Burkert et al,
2014) have argued that mediation fit models with path analysis do not belong to contingency
theory as the key concept of fit does not exist. This is because explicit tests for true mediation
in such models were not identified. Testing mediation fit models must follow certain theoretical
as well as statistical procedures. These are discussed under section 3.5 following.
University of Ghana http://ugspace.ug.edu.gh

56
3.5 Approaches to Testing Contingency Fit Models
In this section, the statistical methodologies adopted to test contingency fit hypotheses are
discussed. These range from deviation score analysis, residual analysis, moderated regression
analysis, and structural analysis. These are discussed in the next four subsections.
3.5.1 Deviation Score and Residual Analysis Techniques
The Deviation Score Technique (DST) and residual analysis (RA) are the two commonly
approaches used in testing for example, matching fit models (Drazin & Van de Vein, 1985;
Donaldson, 2001; Said, Hassabelnaby & Wier, 2003; Gerdin, 2005a). The former requires the
calculation of a score that deviates from the optimality matching the MAS variable and
contingency variable while the latter tests for the negative effect of misfit on performance given
the level of a contingent value and an optimal value of the MAS variable using the deviations
from a predicted value. A comparison of a predicted optimal level of the MAS variable with
the actual level is normally made by both methods. The DST technique is expressed by the
following equation:
𝑦 = 𝛽0 + 𝛽1𝑋 + 𝛽2𝑍 + 𝛽3|𝑋 − 𝑍| + 𝜀………. (3.1)
where 𝑋 and 𝑍 represent MAS variable and contingency variable respectively. A statistically
significant coefficient of 𝛽3 supports the matching form of fit. Both the DST approach and the
RA technique are discussed next.
3.5.1.1 Deviation Score Approach
Two steps necessitate the deviation score methodology: 1) determining the fit-line theoretically
and 2) estimating the fit-line empirically (Chenhall & Chapman, 2006). As shown in equation
(3.1), the theoretical approach requires the use of a fit term which consists of the variations in
the MAS variable (𝑋) and the contingency variable (𝑍) and regressing the outcome variable
University of Ghana http://ugspace.ug.edu.gh
57
performance (𝑦) on this term (Venkatraman, 1989; Hartmann & Moers, 1999; Gerdin & Greve.
2008). In this form of analysis, fit is attained whenever (𝑋 = 𝑍).
In step two where the fit-line is unknown (Driazin & Van de ven, 1985), but has to be
determined empirically, the space defined by the MAS and contingency variables identifies
each observation in that space. Since the fit line is theoretically unknown, the best performers
in a sub-sample is estimated empirically. The key assumption here is that companies that are
closer to the fit line are regarded as best performers. The structural (MAS) variable is initially
predicted by the contingency variable. The relationship between the predicted value of the
structural variable and the contingency variable becomes a reference point for calculating the
deviation score. From this baseline, the Euclidean distance to the fit line which is expected to
have a negative association between performance is calculated, where given the contingency
variable, performance is optimal.
Specifically, based on the corresponding value of the contingency (i.e. the residual or error
term of the regression), the deviation score is measured as the absolute (or squared) value of
the difference between the actual and predicted structural variable. In this case the MAS
variable is then regressed on the contingency variable. Finally, the fit line is predicted from the
regression coefficients from the subsample of high-performing firms. The implication is that a
linear combination of the deviation score, the structural variable and contingency variable
predicts the outcome variable (performance). The statistical test which is normally applied is a
bivariate correlation between distance and performance.
As noted by Meilich (2006), the deviation score methodology has hardly been incorporated
into empirical studies due to the unreliable and misleading results it produces. It suffers from
low reliability and hence is associated with Type II errors (Donaldson, 2001; Edwards, 2007).
More specifically, the reliability of the MAS variable and contingency variable which
University of Ghana http://ugspace.ug.edu.gh

58
constitute the deviation score exceeds or is higher than the reliability of the deviation score
itself. Low reliability leads to a true matching fit model lacking a statistically significant
support. It also results in Type I error leading to erroneous acceptance of a matching fit model
when a different fit model is rather present. As illustrated in panel A of Fig 3.5 and assuming
that a moderation fit model is present instead of a matching fit model. The first step of the
deviation score is to identify the best performers who are primarily associated with the high
values say 15, 20, 25, etc., in the upper right corner as depicted in panel A. In the second step,
a regression between the contingency variable and the MAS variable for this subsample is
estimated out of best performers where in this case, the fit line is derived. This supports the
matching form of fit as shown in panel B.
In moderation types of fit, an ordinal and a monotonic fit model predicts that an increase in the
MAS (e.g. more performance indicators) has a positive impact on performance. In sharp
contrast to this, the matching form of fit predicts that for a given level of the contingency
variable, performance decreases not only when the MAS is too low, but also when it is too high
which contradicts the key assumption underlying the matching fit model. This suggests that the
matching form of fit has been erroneously supported. In addition, where the fit line is positioned
above most of the observations as depicted in panel C, then it is a very likely for a monotonic
moderation fit model to result. In this regard, a statistically significant matching fit model is
again erroneously supported. These spurious supports which are systematically provided by
the deviation score approach to find a statistically significant matching fit model are associated
with Type I errors. Finally, the difference score methodology impose untested and
oversimplification assumptions: the attainment of fit whenever 𝑋 = 𝑍, and the assumption of
iso-performance.
University of Ghana http://ugspace.ug.edu.gh
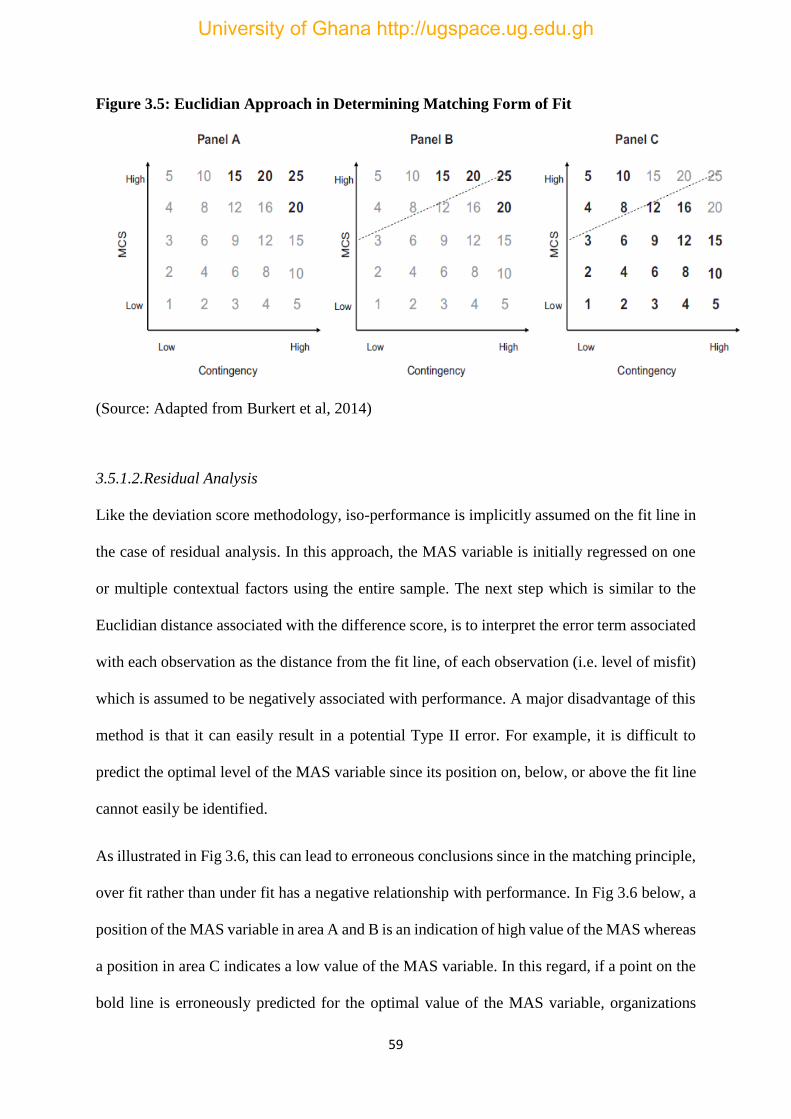
59
Figure 3.5: Euclidian Approach in Determining Matching Form of Fit
(Source: Adapted from Burkert et al, 2014)
3.5.1.2.Residual Analysis
Like the deviation score methodology, iso-performance is implicitly assumed on the fit line in
the case of residual analysis. In this approach, the MAS variable is initially regressed on one
or multiple contextual factors using the entire sample. The next step which is similar to the
Euclidian distance associated with the difference score, is to interpret the error term associated
with each observation as the distance from the fit line, of each observation (i.e. level of misfit)
which is assumed to be negatively associated with performance. A major disadvantage of this
method is that it can easily result in a potential Type II error. For example, it is difficult to
predict the optimal level of the MAS variable since its position on, below, or above the fit line
cannot easily be identified.
As illustrated in Fig 3.6, this can lead to erroneous conclusions since in the matching principle,
over fit rather than under fit has a negative relationship with performance. In Fig 3.6 below, a
position of the MAS variable in area A and B is an indication of high value of the MAS whereas
a position in area C indicates a low value of the MAS variable. In this regard, if a point on the
bold line is erroneously predicted for the optimal value of the MAS variable, organizations
University of Ghana http://ugspace.ug.edu.gh

60
located in area B would over-invest rather than under-invest in the MAS as the incorrect bold
fit line predicts. In this regard, a cancellation of each of the residuals in areas B and C might
result, so that no statistically significant results can be obtained for the ‘‘under-investment’’
hypotheses. In addition, it does not clarify the existence of a true fit line in cases where a
statistically significant finding is not supported. As noted by Burkert et al (2014), unless a
careful analysis is followed, this approach is associated with the risk of erroneously interpreting
a matching fit model when there is existence of another form of fit instead.
Figure 3.6: Potential Type II Error Associated with Residual Analysis
(Source: Adapted from Burkert et al, 2014)
3.5.2 Approach to Testing Moderation Fit Models
In general, contingency researchers have predominantly relied on Moderated Regression
Analysis (MRA) as the main approach to testing moderation forms of fit (Hartmann & Moers,
1999, 2003). MRA is a mere extension of the ordinary least squares (OLS) multiple regression
by the introduction of an interaction term in the multiple regression equation as shown in
equation (3.2) for two independent variables. Since the interaction term in equation (3.2) is
made up of two independent variables, it is a two-way interaction. The moderation fit model is
supported for the statistically significant coefficient, 𝛽3.
𝑦 = 𝛽0 + 𝛽1𝑋 + 𝛽2𝑍 + 𝛽3𝑋𝑍 + 𝜀 …………. (3.2)
University of Ghana http://ugspace.ug.edu.gh
61
This approach which can take various levels of interaction (e.g. two-way interaction, three-way
interaction), has been argued to constitute a weak methodology in detecting the existence of
fit. As can be seen in the next chapter, several underlying assumptions in testing moderation
fit models pose a serious challenge to researchers. These include the inclusion in the model,
lower-order effects, matching verbal hypotheses with statistical model, form and strength of
interaction, and interpretation of results. In this regard, other powerful alternatives such as
structural equation models have been proposed. However, these methodologies have been
marginally employed in contingency fit studies.
3.5.3 Approach to Testing Mediation Form of Fit Models
According to Baron and Kenny (1986), four theoretical and statistical conditions must be met
to establish the existence of true mediation. First, as shown in Fig 3.7 (a) demonstrating that
the mere effect ‘a’ and ‘b’ are both statistically significant and that a statistically significant of
effect size ‘a’ multiplied by effect size ‘b’ establishes full mediation between the exogenous
variable and the endogenous variable is insufficient. Theoretically, the exogenous variable
causes the endogenous variable (Jacobucci, 2008); so the first step which Baron and Kenny
(1986) describe as the ‘classic four-step procedure’, is to empirically show a statistically
significant direct link between the exogenous variable and the final outcome variable as shown
in Fig 3.7 (b). Second, a test between the exogenous variable and the mediating variable
followed by another test between the mediating variable and final endogenous variable is
performed in the third step. In the final test (step 4) a statistically significant effect running
from the exogenous variable to the final endogenous variable needs to reduce for partial
mediations or vanish entirely for full mediation to be established.
University of Ghana http://ugspace.ug.edu.gh

62
Figure 3.7 (a): Mediation Form of Fit Models
effect ‘a’ effect ‘b’
Figure 3.7 (b): Four Step Procedure for Testing Mediation Form of Fit
(Source: Adapted from Baron & Kenny, 1986)
3.6 Conceptualization of Contingency Fit and its Attainment
In this section, a systematic review of the extant empirical literature on contingency-based
MAS design is presented. Arguments in both the contingency-based management accounting
literature and general organizational literature regarding the fit concept and how it is attained
has up to date not been resolved. As Otley (2016, p.45) points out, ‘‘the design of optimal
MASs which results from a mechanistic approach that will develop into a predictive
mechanism misguided’’. Earlier on, Meilich (2006, p.161) has stated ‘‘contingency theory’s
fit concept has been modelled in ways which made its detection to be less conducive’’. These
two statements suggest that the approach to modelling the fit concept in both the management
accounting literature and general organization literature has not followed a precise and
common guidance in advancing theory-consistent knowledge. As Venkatraman (1989) noted,
Contingency
Variable MAS Variable Performance
University of Ghana http://ugspace.ug.edu.gh

63
although different phrases such as ‘contingency upon’, ‘matched with’, ‘fit’, ‘consistent with’,
‘congruence’, and ‘co-alignment’ etc., have been used to explain the fit concept, the provision
of precise guidelines for the translation of the above verbal statements to the required analytical
level is mostly missing. As a consequence, several attacks have been launched on the seemingly
straightforward contingency arguments by scholars such as Schoonhoven (1981) and Drazin &
Van de Ven (1985) as not clear in its predictions and subsequent operationalisations.
In the management accounting field, criticisms are based primarily on the fragmentary and
contradictory nature of contingency-based management accounting studies, which arise from
methodological limitations (see Hartmann & Moers, 1999, 2003; Gerdin & Greve, 2004, 2008;
Burkert et al, 2014; Otley, 2016). Some of these limitations are attributed to insufficient data
and underspecified models and disparate definitions of variables, (Burkert et al, 2014). Aside
the methodological issues and as discussed in the preceding chapter, are confusions
surrounding the fit concept and its conceptualization in management accounting literature.
It has been argued in the management accounting literature that certain contingency hypotheses
that have been discussed and tested (mediation forms of fit) do not belong to contingency
theory as the key concept of fit is missing in these models (Burkert et al, 2014). Hartmann
(2005) argues that mediation forms of fit constitute a violation of contingency theory’s
prediction as they are composed of a mix of matching fit and selection fit which have different
theoretical underpinnings. Gerdin (2005b) had a counter claim about the mediation form of fit
arguing that it is a multi-contingency form of fit. To Burkert et al (2014) any path model with
performance as the criterion variable does not belong to contingency theory.
In line with these arguments, the current study attempts to present a systematic analysis of
empirical contingency work in management accounting. A number of features that
characterized contingency-based empirical research in management accounting was revealed
University of Ghana http://ugspace.ug.edu.gh
64
in a systematic literature review. In the sections that follow, the modelling approaches to
contingency fit hypotheses, selection and measurement of variables, formulation of hypotheses
and subsequent statistical tests applied, are discussed. Also discussed in this sub-section, is an
analysis of the compatibility of verbal hypotheses with their subsequent interpretations in
management accounting literature.
3.7 Levels of Contingency Fit Analysis
Extant empirical literature on contingency-based management accounting research can be
grouped into three main levels of analysis (Otley, 2016). The first level of analysis involves
studies that investigate the relationship between one contingent exogenous variable and one
criterion variable (e.g. Hirst, 1983; Govindarajan, 1984; Brownell & Hirst, 1986; Frucot &
Shearon, 1991; Abernethy & Stoelwinder, 1995; O’Connor, 1995; Bouwens & Abernethy,
2000; Dunk, 2011). The analysis of the joint effect of multiple contingent exogenous variables
on one criterion variable is examined in the second level, where some variables moderate or
mediate (e.g. Merchant, 1981; Kim, 1988). In the third level of analysis, an examination of the
effect of multiple contingent exogenous variables on several criterion variables (e.g. Chenhall
& Morris, 1986; Jermias & Gini, 2004; Gerdin, 2005a; Cadez & Guilding, 2008; Ylinen &
Gullkvist, 2012).
Each level of analysis is based on the selection, matching, interaction (moderation) and
mediation, systems, and multi-fit models. The challenge however, has been how to identify and
test the correct fit model (Burkert et al, 2014). This is particularly associated with the matching
fit models. Although the matching fit model is classic, identifying such studies in management
accounting literature is relatively rare because the iso-performance term has been
misrepresented due perhaps to the two main approaches – residual analysis and deviation score
University of Ghana http://ugspace.ug.edu.gh
65
(discussed in the preceding chapter) that have been used. A classic example is the study by
Brownell (1982) and that of Frucot and Shearon (1991) which used the deviation score
approach. Both studies examined the absolute difference between locus of control (an external
variable) and budgetary participation, and test the relationship between this absolute difference
with performance. In the interest of logical explanation and understanding, a brief background
of the historical antecedents of the contingency-based management accounting literature is
initially presented in the next section. This is followed by a discussion of the selection,
definition and measurement of the MAS variables.
3.8 Early Contingency-Based Management Accounting Studies
Early empirical work in management accounting focused mainly on budgetary participation
for which a match between the MAS variable and context (contingency) variable was
examined. Such studies, to a greater extent, relied on the budgetary design component of the
MAS as the approach to examining the MAS-contingency relationship (see for example,
Argyris, 1952). This period which witnessed the development of contingency theory studies in
management accounting as well as explaining the different aspects of management accounting
practices that were apparent at that time, relied exclusively on the use and deployment of
budgets as the MAS variable.
To that end, emphasis was placed on the extent to which the design of budgets influenced the
behavioral and attitudinal aspects of subordinate managers (see for example, Hopwood, 1972;
Otley, 1978, Merchant, 1981). The concentration on the deployment and use of budgets as the
dominant methodology resulted in the capturing of the MAS variable as ‘Reliance on
Accounting Performance Measures’ (RAPM) but yielded inconsistent results. The mixed
results that characterized these early studies especially those of Hopwood (1972) and Otley
University of Ghana http://ugspace.ug.edu.gh
66
(1978) created the platform for other researchers to advance contingency-based management
accounting studies, which Burkert et al (2014) argue contingency theory’s usage in
management accounting research has attained a dominant position.
3.9 Selection, Definition and Measurement of MAS Variables
Review of past literature indicates that the bulk of empirical work on contingency-based
management accounting research has so far generally been mixed with inconsistent and
fragmentary results. Several factors account for the mixed and conflicting results. First, studies
in this field have generally not been systematic in the selection and measurement of both the
MAS and context variables. Generally, variables (or measures) chosen for analysis in any
particular research do not exactly correspond to those employed in previous works. As Otley
(2016, p.47) points out in his systematic review of contingency theory, ‘‘cumulative results are
rare in this field of research’’. Second, both variable selection and the techniques employed for
analysis in any particular study are arbitrarily determined. Third, past studies have tended to
increase the number of exogenous variables relative to the criterion variable (MAS) rather than
mapping out the boundaries of the field. Fourth, comparability of studies from one period to
another is difficult as most often only a small proportion of the contingency variables used by
organization theorists is employed in any particular study, although these variables have been
used extensively in the management accounting field. Each of these is discussed in the
subsections that follow.
3.9.1 Arbitrary Selection of Variables
Otley (2016) in his review argued that the comparability difficulties arising from empirical
contingency-based management accounting literature is as a result of the limited use, or the use
of a subset of the organizational contingency variables which have been extensively used by
University of Ghana http://ugspace.ug.edu.gh

67
organizational theorists. Indeed, whilst this assertion holds for purposes of cumulative results
and theory consistent management accounting knowledge, it will at the same time be extremely
difficult if not impossible for the analysis of all the contingency variables that have been used
by organizational theorists to be executed in a single comprehensive study. This is due to the
fact that new additions to the independent variables continue to take place in the literature.
Besides, some contingency variables are organizational-specific and may not register their
presence in other organizations. For example, the variable of national culture underpinning an
organization domiciled in an industrialized economy may or may not be relevant in some
organizational types situated in emerging economies. The arguments of Otley (1980) are
genuinely advanced but some appears to be infeasible, at least.
Following the capturing of the ‘‘RAPM’’ which emanated from the budgetary measures era,
both the independent and dependent variables have increased considerably. In broad terms, the
contingent independent variables can be grouped into internal and external (Otley, 2016, p. 48).
Among the major internal independent variables include organizational strategy, structure,
size, compensation systems, information systems, employees’ participation in the control
systems, product life-cycle stage, systems change, market position, and psychological variables
(e.g. tolerance for ambiguity). Major external independent variables include market hostility or
competition, technology, national culture, and environmental uncertainty. The most commonly
used dependent variables (MAS design) include management control systems, performance
measures, effectiveness, budgeting behaviour, job satisfaction, managerial style, and product
innovation.
It can be established from the foregoing that the independent contingency variables have
expanded drastically in relation to the dependent MAS variable, and this development started
right after the contingency theories of management accounting development phase during the
1960s-1970s. Govindarajan (1984) for example, investigated the effects of organizational
University of Ghana http://ugspace.ug.edu.gh

68
effectiveness on the strength of the relationship between organizational uncertainty and
evaluation style. In this study, the MAS variable was defined as the evaluation style of
management in manufacturing concerns. In Chenhall and Morris (1986), the MAS variable was
defined based on the perceived usefulness of four information characteristics which were
considered to be provided by MAS. These information characteristics (broad scope, timeliness,
integration, and aggregation) were regressed on context (contingent) variables composed of
structural decentralization, perceived environmental uncertainty, and organizational
interdependence.
Following from these two studies, Kim (1988) investigated the fit between organizational
context and effective design of MAS in US hospitals. In his study, the MAS variable was
defined as users’ satisfaction with information quality and the extent of system usage and
information value. These variables were regressed on context variables defined by technology
measured by task predictability, and coordination defined as impersonal coordination which
refers to integration of various organizational activities using policies, formalized rules, pre-
established plans, schedules, and procedures, which do not require human input. Using a
multiple contingency approach, Gerdin (2005a) investigated the impact of organizational
contextual factors (composed of organizational structure and departmental interdependencies)
on MAS design in manufacturing departments. He defined the MAS variable as a composite
of rudimentary, broad scope and traditional. Rudimentary MAS information depicts the
aggregation and seldom use of all types of accounting information. Broad scope MAS shows
the extent of detailing and frequent reporting of budgetary and operational information. The
traditional MAS refers to the frequent issuance of detailed budget and product cost reports.
Jermias and Gini (2004) tested contingency hypotheses about the associations between
organizational configurations, MASs, business strategy, and business unit effectiveness. The
MAS variable was defined in this study as low-cost strategy and product differentiation
University of Ghana http://ugspace.ug.edu.gh

69
strategy. These variables were regressed on the context variables represented by competitive
strategy and degree of decentralization. Cadez and Guilding (2008) represented the MAS as
participation in strategic decision process and strategic management accounting use, which
were regressed on the contextual variables represented by prospector/defender, market
orientation and organizational size. In the study of Dunk (2011), the moderating role of budgets
on the relationship between product innovation and firm financial performance was examined.
Ylinen and Gullkvist (2012) in their study, defined the MAS as balanced dimensions and
combined dimensions of accounting information. The context variables were defined as
perceived task uncertainty and tolerance for ambiguity.
Given these few examples above, one can quickly establish that the organizational contextual
variables that underpin the supply chain remained unexplored. As noted by Anderson and
Dekker (2014), all organizations are embedded in supply chains as the existence and
functioning of one particular organization depends on the existence and functioning of another.
In other words, no organization exist and functions in isolation but is embedded in chains of
the activities of other organizations. This makes the efficient and effective management of
supply chains a crucial aspect of contemporary organizational control. The increases in the
organizational contextual variables as outlined above has so far not considered those contextual
variables that fall within the domain of inter-organizational relations in supply chains although
efforts to link MAS design to SCM has been an issue of much concern to management
accounting researchers in recent years (see for example Cooper & Slagmulder, 1998).
To a greater extent, these studies propose the design of MAS techniques (inter-organizational
cost management) for SCM practices by mere extension (or imitation) of the traditional intra
cost management accounting techniques without an examination of the extent to which they
match the contextual antecedents of SCM. The argument put forward by these studies has been
that organizations with much experience and knowledge in intra cost management techniques
University of Ghana http://ugspace.ug.edu.gh
70
would be able to use their knowledge and expertise to develop similar techniques for the
management of supply chains. It can be established from the above literature that the choice of
both the MAS variables and the context (contingency) variables have been arbitrary and
inconsistent. This has perhaps contributed to the different conceptualizations in the
contingency literature in management accounting. The approaches to conceptualizing and
determining what constitutes contingency fit in management accounting literature are
discussed next.
3.9.2 Empirical Estimation of Contingency Fit Models
Extant literature suggests that many different statistical techniques have been used in the
management accounting field to estimate contingency fit. Empirically, estimation techniques
such as the difference in means (or deviation score technique) (Abernethy & Brownell, 1999;
Abernethy & Lillis, 2001; Chenhall & Langfield-Smith, 1998), bivariate correlation
(Khandwalla, 1972; Merchant, 1981, 1984; Haka, 1987; Simons, 1987; Govindarajan, 1988;
Duncan & Moore, 1989), difference in correlation coefficients (strength or form) (Merchant,
1981, 1984; Abernethy & Lillis, 2001; Abernethy & Brownell, 1999), moderated regression
analysis (form-monotonic, form-non-monotonic, strength) (Hirst, 1983; Brownell & Hirst,
1986; Dunk, 2011), and indirect path analysis (Chenhall & Morris, 1986; Chong & Chong,
1997; Bouwens & Abernethy, 2000; Baines & Langfield-Smith, 2003; Gerdin, 2005a) are
statistical models commonly used in estimating contingency fit in management accounting
literature.
The basis for choosing a particular statistical estimation technique for any such epistemic
analysis lies in the fact that each concept of fit is associated with different theoretical meanings,
and requires different statistical tests (Hartmann & Mores, 1999; Gerdin & Greve, 2004).
Although each of the above-mentioned techniques have had one or multiple appearances in the
management accounting literature, the difference in means (deviation score technique),
University of Ghana http://ugspace.ug.edu.gh

71
difference in correlation and MRA have been the dominant statistical approach used in this
field (Hartmann & Moers, 1999, 2003; Dunk, 2003; Gerdin & Greve, 2004, 2008). An analysis
of the strengths and weaknesses of the statistical test conducted in estimating contingency fit
under the interaction models is presented in the sub-sections that follows.
3.10 Empirical Estimation of Moderation Forms of Fit
Management accounting scholars have relied extensively on the use of MRA in testing the
interaction (or moderation) forms of contingency fit (Burkert et al, 2014). However, a review
of empirical studies in this area (e.g. Hartmann & Moers, 1999; 2003, Burkert et al, 2014)
reveals that a weak relationship exists between interaction and (1) the formulation of
hypotheses (Brownell, 1982a, 1982b, 1983), (2) the strength of relationships (e.g. Brownell &
Hirst, 1986), (3) lower order effects (e.g. Merchant, 1990), (4) effect size, (5) multiple and
higher-order interaction (e.g. Mia & Chenhall, 1994), and (6) the issue of monotonicity (e.g.
Frucot & Shearon, 1991). Each of these deficiencies is addressed in the sub-sections that
follow.
3.10.1 Hypotheses Formulation and Statistical Analysis
A fundamental issue in ‘contingency fit’ studies is to ensure that the link between the verbal
statement of hypotheses, the statistical tests applied, and the interpretation of results are
coherent and compatible. From theory, verbal statements of hypotheses are explicitly, logically
and clearly derived, and tested subsequently using an appropriate statistical technique
(Hartmann & Moers, 2003). Failure to ensure this compatibility seriously impedes the
advancement of management accounting studies that is theory-consistent (Burkert et al, 2014).
Apart from the incompatibility of the relationship between the typical format of the underlying
contingency fit hypotheses and the appropriate statistical tests applied in most past
management accounting studies, there are cases of either non-statement of explicit hypotheses
University of Ghana http://ugspace.ug.edu.gh

72
or the statement in a null form of the specified hypotheses. (see for example, Brownell, 1982a,
1982b, 1983; Govindarajan, 1984; Brownell, 1985; Brownell & Hirst, 1986; Chenhall, 1986;
Dunk, 1989; Merchant, 1990; Brownell & Dunk, 1991; Frucot & Shearon, 1991; Harrison,
1993; Mia & Chenhall, 1994; Tsamenyi & Mills, 2002).
Stating a hypothesis in a null form predicts a negative (rather than a positive) relationship
between the variables. In particular, and as stated in the previous chapter, each form of fit is
associated with different theoretical interpretations and different statistical tests and hence, a
null form of a hypothesis is far from adequacy in describing the specific contingency
formulation and the type of statistical test to be performed. In fact, even if the hypotheses
relating to those studies were stated in the positive form, they would still have been inadequate
in describing the specific contingency formulation. Contingency studies require that a proper
match between the underlying contingency fit (e.g. selection, matching, etc.) and the statistical
test applied, be explicitly established. The existence of differences between verbal statements
of hypotheses and statistical tests applied results in erroneous conclusions.
In the study of Frucot and Shearon (1991, p.85) for example, the hypothesis was stated in a
null form as:
‘‘In Mexico, through an interaction effect with budgetary participation, locus of control does
not have a significant effect on performance’’.
They then proceeded to estimate the following statistical model:
𝑌 = 𝛽0 + 𝛽1𝑋1 + 𝛽2𝑋2 + 𝛽3𝑋1 − 𝑋2 + 𝜀 …………… (3.3)
where 𝑋1, 𝑋2 and 𝑌 are locus of control, budgetary participation and performance respectively.
The statement of the verbal hypothesis which refers to interaction form of fit and the statistical
test used are incompatible since equation (3.3) does not measure fit as interaction but rather
measures fit as matching. According to Venkatraman (1989, p. 431), equation (3.3) estimates
a matching rather than an interaction form of fit. Since fit is hypothesized as interaction (form),
University of Ghana http://ugspace.ug.edu.gh

73
there is incompatibility in both the verbal statement of hypothesis and the statistical measure
used; hence, the conclusions drawn and the interpretations thereof remained flawed. The
authors also argued and mentioned the deviation score as a better reflection of the relationship
among the three variables (Frucot & Shearon, 1991, p.90).
Based on this assertion, the hypothesis should have been modified as follows:
There is a unique value of budgetary participation that produces the highest value of
performance for a given value of locus of control in Mexico; deviations from this relationship
in either direction reduce the value of performance (Schoonhoven, 1981; Hartmann & Moers,
1999).
Another incompatibility between the theoretical arguments, verbal hypotheses, and statistical
test used is the work of Tsamenyi and Mills (2002). The authors’ theoretical arguments relate
to ‘‘how perceived environmental uncertainty (environmental level factors) and organizational
culture influence budget participation, and how budget participation in turn influences
managerial performance’’ (Tsamenyi & Mills, 2002, p.17). However, the verbal hypotheses
formulation of this theoretical argument and the statistical analysis (univariate ANOVA) used
were not only incompatible, but also do not fall within contingency theory’s framework and its
key concept of fit.
First, the hypotheses were stated in a null form as follows:
H1: ‘‘There is no difference in budgetary participation when perceived environmental
uncertainty is high or low
H2: There is no difference in budgetary participation when organizational culture has a:
a) high or low power distance b) high or low uncertainty avoidance c) external or
internal focus d) task or social focus e) conformity or individuality focus f) safety
or risk focus, g) adhockery or planning focus’’ (Tsamenyi & Mills, 2002, p. 34)
University of Ghana http://ugspace.ug.edu.gh

74
Formulating verbal statement of hypotheses in a null form in contingency studies seriously
distorts the advancement of management accounting knowledge that is theory-consistent (Luft
& Shields, 2003). Also, the null form possesses limited power in describing the specific
contingency formulation and the associated statistical tests to be employed. In addition, the
hypotheses as specified above do not only mismatch the purpose of investigating the influence
of perceived environmental uncertainty and organizational culture on budgetary participation,
and the corresponding effect of budget participation on managerial performance, but also, do
not capture the key variables that constitute the test. Second, in line with the study’s objectives,
the variable ‘‘budget participation’’ serves both as a mediating variable in which case, a
simultaneous equations analysis involving mediation design would have been the best
statistical alternative to analyze their relationships. The relationship between the four variables
as prescribed by the study objectives, can be illustrated diagrammatically as shown in Fig 3.8
(a) and Fig 3.8 (b).
In Fig 3.8 (a), organizational culture and perceived environmental uncertainty interact to affect
budget participation which then affects managerial performance. This suggests that budget
participation mediates the relationship between the contingency variables and managerial
performance which although according to Hartmann (2005) and Burkert et al (2014), is not
consistent with contingency theory, issues relating to this form of contingency fit hypothesis
still remain unaddressed. If the authors were to test the mediation form of fit, the appropriate
and alternative verbal hypotheses formulation would have been as follows:
‘‘The relationship between organizational culture, perceived environmental uncertainty and
managerial performance is explained by an indirect effect of budget participation whereby both
organizational culture and perceived environmental uncertainty reduce budget participation,
which in turn increases managerial performance’’ (cf. Hartmann & Moers, 1999, 2003)
University of Ghana http://ugspace.ug.edu.gh

75
Also, the variable, ‘budget participation’ was labelled as the contingency variable instead of
the theoretically relevant moderators ‘perceived environmental uncertainty’ and
‘organizational culture’ (see Hartmann & Moers, 1999). The authors even failed to hypothesize
this relationship in the verbal statement when the mediation form of fit was tested. Since
statements of verbal hypotheses are explicitly and logically derived from theory (Hartmann &
Moers, 1999), the hypotheses ought to have captured the theoretical linkages between the
variables.
In Fig 3.8 (b) both perceived environmental uncertainty and organizational culture moderate
the relationship between managerial performance and budget participation. This model is
consistent with contingency theory since the moderators are the theoretically relevant variables
(perceived environmental uncertainty and organizational culture) which suggests that the
relationship between budget participation and managerial performance is contingent upon the
organizational contextual variables of perceived environmental uncertainty and organizational
culture. In conformity with contingency theory, the proper formulation of the verbal hypotheses
(assuming non-monotonic) would be given as:
‘‘For higher values of perceived environmental uncertainty and organizational culture, budget
participation will positively (negatively) affect managerial performance. For lower values of
perceived environmental uncertainty and organizational culture, budget participation will
negatively (positively) affect managerial performance’’ (cf. Hartmann & Moers, 1999, 2003)
University of Ghana http://ugspace.ug.edu.gh
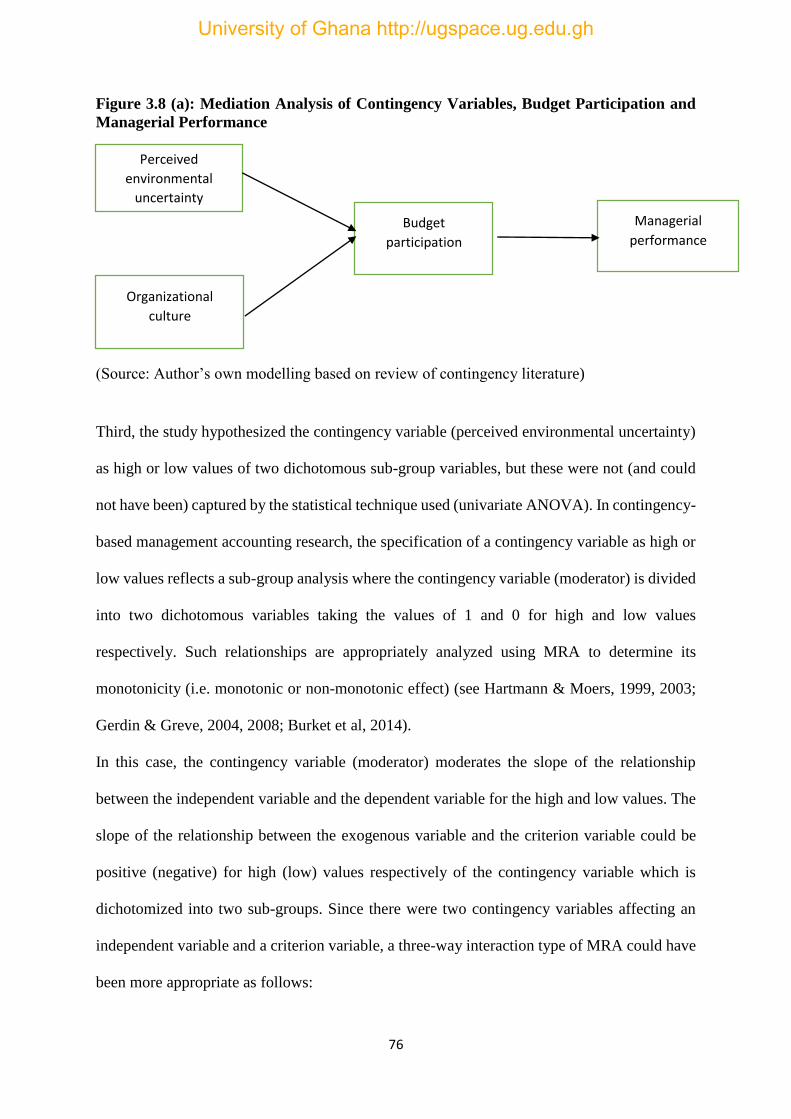
76
Figure 3.8 (a): Mediation Analysis of Contingency Variables, Budget Participation and
Managerial Performance
(Source: Author’s own modelling based on review of contingency literature)
Third, the study hypothesized the contingency variable (perceived environmental uncertainty)
as high or low values of two dichotomous sub-group variables, but these were not (and could
not have been) captured by the statistical technique used (univariate ANOVA). In contingency-
based management accounting research, the specification of a contingency variable as high or
low values reflects a sub-group analysis where the contingency variable (moderator) is divided
into two dichotomous variables taking the values of 1 and 0 for high and low values
respectively. Such relationships are appropriately analyzed using MRA to determine its
monotonicity (i.e. monotonic or non-monotonic effect) (see Hartmann & Moers, 1999, 2003;
Gerdin & Greve, 2004, 2008; Burket et al, 2014).
In this case, the contingency variable (moderator) moderates the slope of the relationship
between the independent variable and the dependent variable for the high and low values. The
slope of the relationship between the exogenous variable and the criterion variable could be
positive (negative) for high (low) values respectively of the contingency variable which is
dichotomized into two sub-groups. Since there were two contingency variables affecting an
independent variable and a criterion variable, a three-way interaction type of MRA could have
been more appropriate as follows:
Perceived
environmental
uncertainty
Organizational
culture
Budget
participation
Managerial
performance
University of Ghana http://ugspace.ug.edu.gh

77
𝑌 = 𝛽0 + 𝛽1𝑃 + 𝛽2𝐶 + 𝛽3𝐵 + 𝛽4𝑃 × 𝐶 + 𝛽5𝑃 × 𝐵 + 𝛽6𝐶 × 𝐵 + 𝛽7𝑃 × 𝐶 × 𝐵 + 𝜀 . (3.4)
Where 𝑌 = managerial performance
𝑃 = perceived environmental uncertainty
𝐶 = organizational culture
𝐵 = budget participation
In this model, the two contingency variables (perceived environmental uncertainty and
organizational culture) interact to affect the relationship between budget participation and
managerial performance. More specifically, the relationship between budget participation and
managerial performance is contingent upon perceived environmental uncertainty and
organizational culture. The relationship between the moderating effect of perceived
environmental uncertainty and organizational culture on the relationship between budget
participation and managerial performance is shown in Fig 3.8 (b).
Figure 3.8 (b): Moderation Analysis of Contingency Variables, Budget Participation and
Managerial Performance
Budget
participation Managerial
performance
Perceived environmental
uncertainty
Organizational
culture
University of Ghana http://ugspace.ug.edu.gh

78
Overall, the formulation of verbal hypotheses, theoretical arguments and statistical analysis
have no match (Hartmann & Moers, 1999).
3.10.2 Strength of the Relationship
Whether an interaction form of fit relates to the ‘strength’ or ‘form’ of a relationship is an issue
that has remained contested among contingency-based management accounting scholars over
the years (Hartmann & Moers, 1999, 2003; Gerdin & Greve, 2004). Govindarajan (1984) tests
a contingency hypothesis involving three variables: organizational effectiveness, evaluation
style, and environmental uncertainty. His hypothesizes that the association between ‘evaluation
style’ and ‘environmental uncertainty’ is affected by ‘organizational effectiveness’, and
therefore formulates the following hypothesis:
‘‘organizational effectiveness affects the strength of the association between evaluation style
environmental uncertainty’’.
Although his verbal hypothesis was compatible with the statistical format used (correlation
analysis) since it contrasts the coefficient of correlations between the two subgroups, the results
which were subsequently interpreted were incompatible with the verbal hypothesis. In his
conclusion, Govindarajan (1984, p. 133) states: ‘‘there is a significant moderating effect of
environmental uncertainty on the association between organizational effectiveness and
evaluation style’’. However, his hypothesis clearly states that organizational effectiveness is
the moderator instead of the theoretically relevant moderator – environmental uncertainty.
As illustrated in Fig 3.9 (a) to (d) the distinguishing features between strength of relationships
and form of relationships can be made. The association between the variables X and Y are
represented by the shaded portions of observable clouds (or scatter diagrams) in each of the
diagrams shown in Fig 3.9. A low correlation is registered by a wide cloud while a high
correlation is represented by a narrow cloud. The first diagram (panel A) shows no correlation
University of Ghana http://ugspace.ug.edu.gh

79
between the variables as represented by the plain area registered by the cloud. The regression
lines for both subgroups are equal. In panel B, there is equal prediction of Y by X in both
subgroups which shows non-existence of strength interaction rather a form of the relationship
between X and Y. The existence of form relationship is evidenced by the different regression
lines for the two subgroups. In sharp contrast to panel B is panel C where the slopes for the
two regression lines are the same but registers difference in strengths where X shows to be a
better predictor of Y in subgroup 1 than in subgroup 2. Panel D shows both strength and form
of relationships as a difference exists between the correlation and slope of the regression lines
for subgroups 1 and 2.
Figure 3.9: Strength vs. Form Interaction
(Source: Quoted from the Literature of Hartman & Moers, 1999, p. 297)
3.10.3 Lower-Order Effects
A statistical format (such as MRA) for testing an interaction form of fit must be such that it
contains the interaction term as well as the main effects (or lower-order effects). This is because
a statistically significant coefficient of the interaction term can be due solely to lower-order
effects and not the interaction term itself (Stone & Hollenbeck, 1984, p. 201). Therefore, in
University of Ghana http://ugspace.ug.edu.gh
80
MRA, lower-order effects are included in order to prevent the existence of an interaction when
in reality such an interaction is due solely to the former. Apart from the misleading conclusions
that can arise if lower-order effects are omitted is the proper interpretation of the coefficients
that relate to the lower order effects. It is argued that the coefficients of lower order effects
show clearly, the main effect of a variable when the value of the other variable is zero, although
a zero value is meaningful only for ratio scale variables (Southwood, 1978, p. 1165).
Furthermore, the lower-order effects and their product (interaction term) are at high potential
of being correlated resulting in multicollinearity (Drazin & Van de vein, 1985).
The review reveals some deficiencies and shortcomings associated with lower-order effects in
terms of inclusion of main variables, proper interpretation of main effects, and the problem
with multicollinearity. In the literature of Hirst (1983) for example, a model to test an
interaction was stated in the form:
𝑌 = 𝛽0 + 𝛽1𝑋1𝑋2 + 𝜀 …………………… (3.5)
This equation does not include an interaction term. As it has been argued, a statistically
significant 𝛽1 could be misleading if the existence of in interaction is supported. This is because
a statistically significant value of 𝛽1 could result from a significant association between 𝑋1 and
𝑌 regardless of 𝑋2 and vice versa. As Cohen and Cohen (1983, p. 305) argue, an interaction
term has the potential of ‘stealing variance’ from its constituent parts because it is the product
of main (or lower-order) effects. In line with this, Stone and Hollenbeck (1984, p. 201) states:
‘‘While the multiplication term ‘‘carries’’ the interaction in a regression equation, the same
multiplication term is not the interaction’’.
According to Southwood (1978, p. 1164), Cohen and Cohen (1983, p. 348) and Stone and
Hollenbeck (1984, p. 201), a partialed out of the lower-order effects should be obtained by
making sure that they are present in the regression equation.
University of Ghana http://ugspace.ug.edu.gh

81
Another deficiency relates to the interpretation of lower-order effects which, as the literature
indicates, are subject to both Type I and Type II errors. Whilst some studies are associated with
invalid lower-order interpretation especially in a two-way interaction and higher-order
interaction, where most are associated with Type I error (Brownell, 1982a, 1983, 1985;
Chenhall, 1986; Brownell & Hirst, 1986; Imoisili, 1989; Mia, 1989), others showed no
interpretation of lower-order effects even though they could have been interpreted (Dunk,
1992, 1993; Brownell & Dunk, 1991; Harrison, 1992, 1993; Mia & Chenhall, 1994; Gul &
Chia, 1994; Lau, Low & Eggleton, 1995), which is associated with a Type II error.
The reason for non-interpretation of lower-order effects are primarily based on Southwood’s
(1978, p.1168) contention that no theoretical meaning is associated with such coefficients.
Southwood’s (1978) argument is based on scale origins of variable measurement in the
behavioral sciences which are based on interval scales rather than ratio scales. Hence, linear
transformations according to Southwood (1978), do change the coefficients of lower-order
effects in MRA equations, and therefore, these coefficients cannot be easily interpreted.
Nevertheless, the zero value of the variables obtained in interval scale has a specific meaning
if the variables are centered on their respective means.
Contingency-based management accounting researchers have erroneously relied on this
assertion and failed to interpret the lower-order effects in MRA. It is argued that the main
effects coefficients obtained when using MRA, are generally different from those that are
obtained from a regression model without an interaction term. Southwood (1978, p. 1168) and
Cohen and Cohen (1983, p. 305-306) further argue and state: ‘‘linear transformations do not
vary the coefficient of the interaction term, not its t-statistic and level of significance’’.
Management accounting researchers have however, relied on the problems associated with
scale origins which are peculiar to interval scales compared to ratio scales. In the study of Mia
and Chenhall (1994) for example, the moderating effect of ‘‘Function’’ on the relationship
University of Ghana http://ugspace.ug.edu.gh

82
between ‘‘the Use of Broad Scope MAS’’ and ‘‘Managerial Performance’’ was investigated.
In their analysis, the MAS variable was estimated as a difference score from the overall mean.
Since the mean is centered, the coefficient of the lower-order effect of Function was
interpretable and could have been interpreted. Referring to Southwood (1978), the authors
state: ‘‘No attempt was made to interpret the coefficients of lower-order effects that related to
the extent of use of broad-scope MAS information or function’’ (Mia & Chenhall, 1994, p. 9).
3.10.4 Interaction and Effect Size
Information about the optimal value of the dependent variable has been confused with that
which relates to changes in the relationship between the variables under consideration.
Champoux and Peters (1987) noted that a statistically significant coefficient of the interaction
term in MRA is only an indication of changes in the relationship between the variables, and
does not provide information about the value (size) of the dependent variable for a given value
of an independent variable. A recognition of the difference between significant interaction and
effect size appears to have been ignored by past studies, leading to wrong interpretation of the
interaction term.
For example, the interpretation of a positive statistically significant coefficient term in an MRA
consisting of two independent variables 𝑋1 and 𝑋2, is not based on the prediction that 𝑌 derives
the highest value for the highest values of 𝑋1 and 𝑋2 , but that 𝑋2 has a more positive effect on
𝑌 for higher values of 𝑋1. The body of literature relating to Brownell (1983), Brownell and
Hirst (1986), Mia (1989), Brownell and Dunk (1991), and Dunk (1989, 1992, 1993) incorrectly
assume that a statistically significant interaction term implies that the dependent variable is
maximized for a given set of certain combination of variables. Dunk (1992) wrongly assumes
that the significant interaction term in the MRA model he used to test his hypothesis contains
information about effect size, and subsequently offers wrong interpretation of the verbal
hypothesis. His hypothesized verbal statement reads:
University of Ghana http://ugspace.ug.edu.gh

83
‘‘production subunit performance is higher for higher (lower) the reliance on budgetary control
and a higher (lower) the level of manufacturing process automation’’ (Dunk, 1992, p. 198)
The use of MRA to test this hypothesis which by implication, a combination of low/low and
high/high of the exogenous variables maximizes the criterion variable as specified in the verbal
hypothesis cannot be interpreted by the interaction term. Another statistically significant
negative coefficient in a three-way interaction MRA model used by Dunk (1993, p. 405-406)
was interpreted to mean that the dependent variable ‘slack’ attains a minimum value when the
independent variables consisting of ‘participation’, ‘information asymmetry’ and ‘budget
emphasis’ are all high. As the main effects (or lower-order effects) are due to the exogenous,
uncontrollable contingency factors, the question of either maximum or minimum 𝑌 value is
somehow not important in contingency models (Hartmann & Moers, 1999).
In addition to the above deficiencies that characterized some empirical contingency literature
on the effect size, confusion still surrounds the use of the Johnson-Neyman (JN) technique in
analyzing effect size in MRA. While Hartmann and Moers (1999) argue that the JN technique
plays no role in hypotheses tests regarding MRA interaction format, as used by Brownell
(1982a) and Lau et al (1995) in performing formal analysis of effect size, Burkert et al (2014),
in their extensive literature review on contingency fit hypotheses, concluded that such a ‘‘lack
of comprehensive explanations of how best to investigate the additional features of an
interaction term which are available now could account for misperception’’ (Burkert et al,
2014, p. 20). On common grounds, the JN is noted for its relevance in determining the ‘region
of significance’ in MRA for the difference between the effects of different values of the
moderator at a given value of the exogenous variable. Its relevance may however, depend on
the way and manner in which it is applied.
University of Ghana http://ugspace.ug.edu.gh

84
3.10.5 Multiple and Higher-Order Interaction
A number of deficiencies such as over-specification of models (Imoisili, 1989), under-specified
theoretical support for interaction terms introduced (Imoisili, 1989; Harrison 1992) and
misapplication of multiple and higher-order interaction models (Harrison, 1992, 1993) etc.,
characterized most studies. Another shortcoming associated with this form of statistical
analysis is the difficulty in interpreting the coefficients of the interaction terms. These
shortcomings seriously affect the validity of the results published by most studies. In the study
of Imoisili (1989) for example, a multiple two-way and higher-order interaction model was
specified as follows:
𝑌 = 𝛽0 + 𝛽1𝑋1 + 𝛽2𝑋2 + 𝛽3𝑋3 + 𝛽4𝑋1𝑋2 + 𝛽5𝑋1𝑋3 + 𝛽6𝑋2𝑋3 + 𝛽7𝑋1𝑋2𝑋3 + 𝜀 …... (3.6)
The two-way interaction term (𝑋2𝑋3) and the three-way interaction term (𝑋1𝑋2𝑋3) as included
in the model were not hypothesized by Imoisili (1989), yet they were retained in the model for
analysis. In this case, the model is said to have contained a redundant two-way interaction and
a redundant three-way interaction which do not form part of the hypotheses, thereby indicating
an incorrect test of the hypotheses. Taking the partial derivative of (3.6) shows that the model
contains an interaction effect (𝑋1𝑋2) not hypothesized. That is
𝜕𝑌
𝜕𝑋1= 𝛽1 + 𝛽4𝑋2 + 𝛽5𝑋3 + 𝛽7𝑋2𝑋3…………………. (3.7)
which means that the association between 𝑋1 and 𝑌 is not only a function of 𝑋2 and 𝑋3 but also
a function of the interaction term (𝑋2𝑋3). The inclusion of the redundant terms was not
specified by theory. As noted by Jacaard et al (1990) any addition of two-way interaction in an
MRA equation should have a theoretical foundation. More specifically, the theory should
dictate that the association between the exogenous variable and an endogenous variable is a
function of two or more independent variables. From these analysis, the results obtained by
Imoisili (1989) do not provide an answer to the verbal hypotheses and hence the conclusions
University of Ghana http://ugspace.ug.edu.gh
85
reached are incorrect. To provide reliable results, the two redundant terms in the equation
should have been excluded.
In another test performed by Harrison (1992) involving a test for the existence of a two-way
interaction between budgetary participation, reliance on job-related tension, accounting
performance measures and nation represented by 𝑋1, 𝑋2, 𝑋3, and 𝑌 respectively, the following
MRA equation was specified:
𝑌 = 𝛽0 + 𝛽1𝑋1 + 𝛽2𝑋2 + 𝛽3𝑋3 + 𝛽4𝑋1𝑋2 + 𝛽5𝑋1𝑋3 + 𝛽6𝑋2𝑋3 + 𝜀……… (3.8)
The aim of the test was to investigate the moderating effect of budgetary participation (𝑋1) on
the association between job-related tension (𝑌) and reliance on accounting performance
measures (𝑋2). As far as this hypothesis is concerned, the multiple interaction equation as
specified in (3.7) is of no relevance as it has no theoretical foundation. Per the verbal
hypothesis, only the first interaction (𝑋1𝑋2) are hypothesized. The other two (𝑋1𝑋3) and
(𝑋2𝑋3) are not. The equations specified in Imoisili (1989) and Harrison (1992) both have high
probability of being over-specified since the extra predictor variables which were included is
unnecessary. A model which is over-specified has the chance of increasing its standard error
of regression coefficients which is highly associated with a Type I error since it influences the
significance of the coefficients. A standard error influenced by over-specification is not
interpretable irrespective of its stability. In addition, a model which is affected by unnecessary
over-specification is hardly interpretable no matter how stable it is (Hartmann & Moers, 1999,
2003). Based on these arguments, a statistically significant coefficient 𝛽4 in Harrison’s (1992)
model could not have been interpreted. In a further analysis, we take the partial derivative of
(3.7) w.r.t. 𝑋2 to give:
𝜕𝑌
𝜕𝑋2= 𝛽2 + 𝛽4𝑋1 + 𝛽5𝑋3………………. (3.9)
which means that the association between 𝑋2 and 𝑌 is a linear function of not 𝑋1 alone, but
also 𝑋3. Consequently, answers to the hypothesis has not been provided in Harrison (1992)
University of Ghana http://ugspace.ug.edu.gh

86
since there is no the statistically significant value of the coefficient 𝛽4 is not in this case, a
measure of the moderating effect of 𝑋1 on the relationship between 𝑋2 and 𝑌 as hypothesized.
3.11 The Use of Higher-Order of Abstraction Models in SEM
Another shortcoming associated with second or third level of contingency fit analysis (Otley,
2016), has been the modelling of multiple independent and dependent variables. These studies
have tended to bundle together, multiple constructs in a single composite score. The outcome
of such modelling is that the explication of the resultant construct generally is incomplete and
the contributions of content domains of the individual construct to the final score by the scale
will be unknown (Gerbing, Hamilton & Freeman, 1994). Alternatively, if all items or manifest
variables are posited as reflective items of a single first-order construct, then it would be
difficult to ascertain the contribution of each domain on the overall construct.
This is of particular importance with multi-dimensional constructs. Several of both the structure
(MAS) and context (contingency) constructs in contingency-based management accounting
studies can be meaningfully conceptualized as higher orders of abstraction. Although
paradigms on the use of structural equation modelling in modelling contingency fit have
appeared in the management accounting field, several SEM techniques still remain unexplored.
Studies that employ advanced SEM techniques such as higher-order modelling, latent growing
models, and multilevel modelling are relatively not in existence. None of the contingency-
based management accounting studies reviewed in this study has produced a manuscript that
employ higher-order (e.g. second-order) modelling.
Indeed, structural equation models are powerful statistical tools that can test all types of
contingency fit models (except matching form of fit) since their correct application drastically
reduces the amounts of Type I and Type II errors (Burkert et al, 2014). Besides, the mere
finding of a statistically significant coefficient of the 𝛽-value for the absolute difference value
University of Ghana http://ugspace.ug.edu.gh
87
and that of an interaction term which are associated with the deviation score and MRA is too
crude a proxy for respectively determining the existence of moderation forms of fit. In SEM,
the test variables in addition to supporting a statistically significant test, must obtain statistical
values (or goodness-of-fit indices) that fall within the specified theoretical range of
acceptability, hence providing concrete evidence of the model adequately fitting the sample
data. In the traditional form of statistical analysis, such goodness-of-fit measures do not exist
which suggests that a statistically significant coefficient of the term representing the
contingency fit does not necessarily imply a fit. Such a statistical analysis has the high risks of
reaching incorrect conclusions.
3.12 Chapter Summary
In this chapter, the two main schools of thought underpinning contingency theory have been
discussed where a clear distinction is drawn between the Cartesian school of thought and the
Configurational school of thought. In addition, the various typologies of contingency fit models
have been presented delineating between the selection, matching, and moderation and
mediation forms of fit. Approaches to conceptualizing as well as testing the types of
contingency fit models have not been left out. Each concept of fit is associated with a different
theoretical interpretation which requires a different statistical analysis. For example, whereas
the selection form of fit requires a correlation analysis that of the matching and moderation
forms of fit require the deviation score technique and moderation regression analysis
respectively. This underscores enormous theoretical implications for management accounting
researchers. A final form of fit, the mediation form of fit, which has attracted several divergent
views as to whether it falls under contingency theory has been discussed. The short comings
and weaknesses associated with tests involving these models, and the theoretical and statistical
University of Ghana http://ugspace.ug.edu.gh
88
conditions (the classic four-step procedure) that need to be satisfied to establish true partial or
full mediations have been fully elaborated.
The empirical review relating to contingency-based studies in management accounting has also
been presented. The review shows that contingency-fit hypotheses testing is underpinned by
three main issues; i.e. a match between the formulation of verbal hypotheses, the statistical
methodology employed, and the interpretation of results. Relating these three dimensions to
existing empirical studies reveals a number of inconsistencies as well as distortions and
fragmentations associated with contingency theory’s requirements. In addition, the review
reveals several complexities and weaknesses associated with the traditional approaches used in
testing contingency fit hypotheses which clearly shows that they are not appropriate statistical
methodology to testing contingency hypotheses especially multiple variables. The higher the
number of the test variables the more complex it becomes. For example, testing a four-way
interaction using MRA would be extremely difficult. This suggests the use of covariance-based
structural equation models which have the advantage of resolving these shortcomings
associated with the traditional approaches.
University of Ghana http://ugspace.ug.edu.gh

89
CHAPTER FOUR
THEORETICAL MODEL AND HYPOTHESES DEVELOPMENT
4.1 Introduction
The preceding chapter reviewed the theoretical and empirical literature on contingency theory’s
application in MAS design, and identified the shortcomings associated with these studies
particularly in relation to testing of contingency hypotheses under the various fit models. The
review identified the common structural characteristics of organizations that have been
incorporated into contingency research during the past three decades. These include strategy,
decentralization, size, organizational culture, formalization, structural differentiation,
technology and perceived environmental uncertainty. This chapter presents a more detailed and
focused description of the variables/constructs that form the conceptual model and the
theoretical linkages or empirical evidence of the extent of their relationships. Building on these
theoretical foundations, the theoretical model that form this research is initially presented. A
detailed discussion of the theoretical background of the individual study variables follows.
Next is the formulation of the testable hypotheses; their formulation which are based on
evidence of theoretical linkages from empirical literature as well as in conformance with the
underlying contingency fit model. The study also controls for hospital specific variables made
up of four variables namely, hospital size, location, ownership and location which have been
shown empirically to influence hospital performance. The chapter concludes with a summary.
4.2 Theoretical Framework
The theoretical model within which this study is conducted is illustrated in Fig 4.1. This model
is developed based on empirical evidence that supply chain integration (SCI) and MAS
information characteristics are important variables that interact to enhance hospital SC
University of Ghana http://ugspace.ug.edu.gh

90
performance. It is also based on empirical evidence that a fit (or alignment) between
organizational contextual variables and MAS information characteristics is important for
achieving high performance.
As shown in Fig 4.1, the SCM variable is represented as a multidimensional construct
comprising four contextual variables. These include SCI (strategic supplier partnerships or
external integration), internal integration, level of information (or knowledge) sharing (or
exchange), and supply chain risk and uncertainty (Li et al, 2006; Chen et al, 2013) and are
hypothesized to influence the design and implementation of MAS information in the health
SCM context. The MAS variable represented by one rectangle is also a multidimensional
construct comprising broad scope, timeliness, integration, and aggregation (Chenhall & Morris,
1986; Bouwens & Abernethy, 2000; Abernethy & Lillis, 2001). Finally, hospital supply chain
performance is although represented in the model by a single rectangle, it is a multidimensional
construct comprised four dimensions namely, cost effectiveness, utilization of hospital asset,
supply chain flexibility and speed, and supply chain quality (Chen et al, 2013; Ataseven &
Nair, 2017).
4.2.1 Contingency Fit
This research is positioned within contingency framework i.e., the three models of contingency
fit relationships: the selection, mediation and moderation fit models. The selection fit model
tests the impact of the four SCM contextual factors on the four dimensions of the MAS design.
In this type of fit, the theory says that effect of the contextual variables is tested not on
performance but the MAS variable (Hartmann & Morris, 1999). The implication is that
companies have fully adapted their MAS to the demands of their context (Hartmann, 2005).
University of Ghana http://ugspace.ug.edu.gh

91
4.1: Theoretical Framework
(Source: Modification from Chen et al, 2013; Hammad et al, 2013; Macinati and Anessi-Pessina, 2014)
Supply Chain Integration
Supplier
relationship
(External
Integration)
Internal Integration
Level of Information
Sharing
Supply chain risk
and Uncertainty
MAS Design
Broad scope
Timeliness
Integration
Aggregation
Hospital Supply Chain
Performance
Supply Chain Cost
Effectiveness
Utilization of
Hospital Assets
Supply Chain
Quality
Supply Chain
Flexibility
Size Location
Profit Status Ownership
H1a,b,c,d H2a,b,c,d H3a,b,c,d H4a,b,c,d
H5 a,b,c,d
H6 a,b,c,d
University of Ghana http://ugspace.ug.edu.gh
92
Because companies are assumed to be in equilibrium, no differences in performance are expected.
Sixteen sub-hypotheses are tested in this model. The other contingency fit is the mediation form
of fit which tests the dimensions of the MAS design on the relationship between SCM contextual
factors and supply chain performance. Here, the MAS serves as an intervening mechanism
between SCM and SC performance. Relating the contingency theory to SCM and MAS design
suggests an alignment of the individual dimensions of SCM with the MAS dimensions in order to
achieve the best performance. Past literature suggests that the dimensions of SCM highly interacts
with other variables to enhance both operational and financial performance (Flynn, Huo and Zhao,
2010). This suggests that the interaction of individual characteristics of SCM to affect performance
is supported by contingency theory (Flynn et al, 2010) hence, organizations make the effort to
integrate SCM characteristics with the dimensions of the MAS to maximize performance. In this
model, four hypotheses are tested. The final model is the moderation fit model which tests
moderation of the SCM contextual factors on the relationship between the dimensions of the MAS
and SC performance. As asserted by Ataseven and Nair (2017), the need for investigating specific
associations between the characteristics of SCM and performance within contingency frameworks
is to discern the role of moderating factors in the dimensions SCM.
4.2.2. Contingency Theory
Contingency theory is a well-recognized and long-standing theoretical framework for explaining
the design and success of organizational structure (Meilich, 2006; Burkert et al, 2014). On general
grounds, contingency-based studies in management accounting aim to find a ‘match’ (or
alignment) between the design and use of MAS information and the context (or environment) in
which it is used for optimal performance.
University of Ghana http://ugspace.ug.edu.gh

93
Contingency theory is known not only to be a major theory and overarching area of management
accounting research, but also a theory that has attained a pivotal stand within the field of general
organizational literature. In management accounting research, it has attained a dominant position
(Hartmann & Moers, 1999; Otley, 2016). As noted by Scott (1998, p.97), ‘‘it is the most
contemporary theoretical approach that has been widely utilized to the study of organizations’’.
The importance of contingency theory is reflected not only in the frequency of its nomination by
scholars of organizational for its relevance (Miner, 1984; Lawrence & Lorsch, 1967), but also the
assertion made by Lawrence (1993, p. 16). He states that ‘‘the strongest research-based body of
knowledge that continues to be relevant to the practical problems of organizational design has been
contingency theory’’. For effective organization and structuring of a firm involved contingencies
that need to be taken into consideration (Miner, 1984). In other words, the effect of organizational
structure on organizational performance depends on contextual aspects that need to be accounted
for.
Contingency theory assumes that no optimal organizational structure exists rather, the design of
an organizational structure is contingent upon both external and internal and (contextual and
environmental) factors such as strategy, size, technology, and perceived environmental uncertainty
(Otley, 1978; 1980; Chenhall, 2003). The contention is that an organization’s structure is not only
contingent upon contextual variables, but that for optimum performance, the different components
of an organization must fit with each other. This notion that performance is the result of the fit
between context and structure is central to contingency theory (Meilich, 2006; Burkert et al, 2014).
Management accounting researchers have drawn on this theory to investigate the ‘match’ between
MAS variables and the context and environment in which they are used. Early studies hypothesized
that a universally appropriate management accounting system which applies equally to all
University of Ghana http://ugspace.ug.edu.gh

94
organizations in all circumstances does not exist rather, appropriate accounting systems depend on
organizational contextual variables (Otley, 2016).
Contingency theories of accounting play a unique role not found in other universal theories and
hence, have been described as the opposites of universal theories of accounting (Hartmann &
Moers, 1999). This unique role lies in the fact that ‘‘they link the impact or the optimality of the
MAS variable to the context or environment in which they are used’’ (Hartmann & Moers, 1999,
p.292). Although contingency theory has a long-standing tradition in both the organizational and
management accounting literatures, the accumulated research evidence has not consistently
supported the arguments put forward by the theory (Otley, 2016). There still remain unsettled
issues regarding the theorizing and testing of contingency hypotheses (Burkert et al, 2014). Weak
relationships between the formulation of verbal hypotheses and statistical analysis, controversy
over the fit concept under the moderation, matching and mediation forms of fit and how it is
attained, statistical methods suitability and their appropriateness in testing contingency hypotheses
etc., are some of the unresolved issues. In spite of these shortcomings, contingency-based
management accounting research contends that the design of MAS is affected by (contingent upon)
the context or situation in which an organization finds itself.
Supply chain studies and management accounting have been undertaken through the theoretical
lenses of mostly transaction cost economics (TCE) and relational theory (Dekker et al, 2013).
These studies however, focus on two dyad supply chain relationships with emphasis on risk
minimization. The TCE argues that partners in inter-firm relations need to safeguard their interest
against the potentially opportunistic behavior of others, which literally is the management of
appropriation concerns (Williamson, 2008). The essence of managing appropriation concerns has
a close relationship with the features of the transactions taking place (i.e. the specific assets that
University of Ghana http://ugspace.ug.edu.gh
95
have been dedicated to the relationship, the rate or frequency at which the transaction occurs, and
the level of uncertainty surrounding the environment), and the features of human beings (i.e.
opportunism and bounded rationality) (Dekker, 2004).
For example, the higher the appropriation concerns in inter-firm exchange, the more partners who
are safeguarded in a transaction need to raise their confidence that the other partner will not engage
in malfeasance, thereby influencing the application of excessive amounts of MASs which
negatively affects performance. From this perspective, and to mitigate underlying transaction risk,
the installation of MAS in the inter-firm exchanges domain has been essentially based on the
‘matching’ principle where the installation of MASs by firms aligns with the transaction context
(Reusen & Stouthuysen, 2017). For example, Reusen & Stouthuysen (2017) found that although
the transaction context is related to the extent of MAS use, significant variations which are
evidenced by performance differences across firms exist. This is because although there is a fit, it
does not reflect the optimum level (Otley, 1980, 2016). This optimality condition is what
contingency theory proclaims as its underlying principle which suggests that fit between
contextual variables and structure is important for achieving high organizational performance
(Chenhall, 2003).
Moreover, choices of MAS design in the inter-firm exchanges domain in SCM decisions have been
based on imitations of individual MAS structure which Reusen & Stouthuysen (2017) find to be
one of the root cause of misalignment in the MAS-context relationship. It has been argued that
‘‘the planning and controlling processing abilities that are fundamental to managing costs
internally is the same for managing inter-firm relationships hence, can be applied to SCM
activities’’ (Fayard et al, 2012, p.170). Hence, organizations with high levels of internal cost
management (ICM) would be able to use their knowledge and experience to model similar costing
University of Ghana http://ugspace.ug.edu.gh
96
systems for SCM decisions. In this regard, MAS information for SCM decisions were considered
as mere extensions of the conventional intra-firm cost accounting tools of the traditional MAS,
and this has come to be known as inter-organizational cost management (IOCM). In the
subsections that follow, the theoretical foundations of each of the four dimensions of the MAS and
SCM contextual factors are discussed.
4.3 Theoretical Foundation of Constructs
Contingency fit is simply a question of alignment between three primary pieces of organizational
puzzle; 1) characteristics (or dimensions) of MAS information, 2) organizational performance, and
3) contingency factors that affect the relationship between MAS design and organizational
performance (Chenhall & Chapman, 2006). Studies in the contingency paradigm attempt to
explain the design and/or use of MAS through arguments and demonstration of the optimality or
fit within the environment context in which the MAS operates (Luft & Shields, 2003; Hartmann,
2005).
4.3.1 Management Accounting Systems (MAS)
Management accounting system has been conceptualized from different perspectives but generally
consist of formalized information systems designed and used by organizations to provide decision-
making information and support for managers (Chenhall & Morris, 1986; Bouwens, & Abernethy,
2000; Gerdin, 2005a). Hoozee and Ngo (2017) note that organizations employ MASs to influence
managerial behaviours such that they are directed towards attaining organizational objectives. This
is because empirical evidence of a positive association among accounting information, improved
decision making, and organizational performance has generally been found among management
accounting scholars (Cooper & Kaplan, 1991).
University of Ghana http://ugspace.ug.edu.gh

97
Jermias and Gani (2004) conceptualized the management accounting function from two broad
perspectives: product differentiation strategy (Type I MAS) and low-cost strategy (Type II MAS)
based on Porter’s (1985) framework for strategic priority. The former enhances the capacity of
companies to differentiate their products as well as meeting the needs of customers by providing
information and measures that relate to key production activities, strategic planning, customer
satisfaction, quality, timely and reliable delivery of goods/services, benchmarking, and employee-
based measures. For companies that adopt low cost strategy, the latter is considered to be more
appropriate as it provides information associated with activity-based costing techniques, variance
analysis, and budgetary performance measures.
In healthcare management, and more specifically the health supply chain, both design types of the
MAS information are relevant in enhancing organizational performance. For example, hospitals
need information and measures that can be used to differentiate medical products at various stock
(or inventory) levels, track operational (or production) costs of facilities, and satisfy customers’
(patients’) needs simultaneously. In particular MASs may reveal sources of inefficiency and
ineffectiveness of hospital operations by providing detailed information about the consumption of
resources by each of the hospital’s operations (Hoozee & Ngo, 2017). A more challenging issue is
where management have to provide quality healthcare services to customers but at relatively low
cost (i.e. adopt a low-cost strategy). Based on these decision-functional roles of the MAS, many
scholars (e.g. Chenhall & Morris, 1986; Bouwens & Abernethy, 2000; Abernethy et al, 2007;
Hammad et al, 2013; Macinati & Asseni-Pessina, 2014) have conceptualized MAS design in terms
of four interrelated dimensions as shown in Fig 4.2: 1) broad scope which refers to external, non-
financial and future-oriented information, 2) timeliness which deals with the frequency and speed
of reporting accounting information, 3) integration which refers to the precise targets set for
University of Ghana http://ugspace.ug.edu.gh
98
activities and the scope of variances calculation, and 4) aggregation which refers to various forms
of aggregation such as time period and functional areas as well as analytical or decision models.
Aggregation also specifies the dimensions of cost disaggregation according to behavior and their
interrelationships within subunits.
These four dimensions have generally been considered as critically intrinsic characteristics of the
MAS designed and used in healthcare setting (Abernethy & Lillis, 2001; Pizzini, 2006; Abernethy
et al, 2007; Hammad et al, 2013; Macinati & Asseni-Pessina, 2014). In addition, these four
attributes of the MAS information are known to be highly significant in assessing managerial
decision-making in hospitals; hence, appropriately describe the MASs designed and used in
healthcare organizations (Pizzini, 2006).
Based on Chenhall and Morris (1986), MAS is conceptualized in this study as formal systems
designed for providing information for managers in healthcare institutions. The prime objective of
this study is to examine the effect of strategic supplier partnerships (external integration), supply
chain integration (internal integration), level of information sharing (or knowledge exchange), and
supply chain risk and uncertainty on the four dimensions of the MAS design in the healthcare inter-
firm exchange domains and the decision facilitating role of the MAS information in enhancing the
performance of the health supply chain. The dimensions of the MAS information are discussed in
the subsections that follow.
University of Ghana http://ugspace.ug.edu.gh

99
Figure 4.2: Classification of the MAS Dimensions
(Source: Adapted from the literature of Chenhall & Morris, 1986; Soobaroyen & Poorundersing,
2008; Hammad et al, 2013; Macinati & Assina-Pessina, 2014).
4.3.1.1 Broad Scope of the MAS Information
Broad scope of MAS information is viewed as a continuum where narrow MAS information is
associated with traditional MAS design which not only focuses on internal information, but also
financial and historical information. Information that is externally focused, non-financial, and
future-oriented pertains to broad-scope information. The extent to which the MAS information is
presented in various forms is represented by broad scope (i.e. both financial and non-financial) as
well as information that predicts future events. Broad scope information is needed in the health
SCM decisions such as operating cost of facilities, value of commodity throughput, procurement,
medical supplies, and inventory management, transportation, etc. The availability of information
that predicts future events depends on the level of detail (Cohen & Kaimenaki, 2011). This
suggests that valuable time that is otherwise spent by managers each time a decision on the
Broad Scope
Timeliness
Levels of
Aggregation
Integrative Nature
MAS Information
Dimensions
External information Non-financial information Future-oriented
Frequency of reporting Speed of reporting
Aggregated by time period Aggregated by functional area Analytical or decision models
Precise targets for activities and interrelationships with subunits Reporting on intra-subunit interactions
University of Ghana http://ugspace.ug.edu.gh

100
formatting of cost data is made is saved. The extent to which decision-making information has the
appropriate level of analysis for purposes and sufficient, and is greater when the level of detail of
the MAS information is higher. It is expected that highly detailed MAS information will provide
managers with a more realistic view and clearer cost objects linked to healthcare SCM. In this
regard, the ways in which these cost objects affect performance is better understood and
contributed. The degree to which costing systems are analyzed for different purposes in the health
SC also depends on the level of detail of the MAS information and the more appropriate and useful
the information.
4.3.1.2 Timeliness of the MAS Information
The time elapsed before information is made available upon request. More specifically, the extent
of fastness or quickness the MAS responses to a requested information. This implies that the
dimension timeliness is associated with frequency as well as speed of reporting information. How
often information is made available to managers is the sub-dimension of frequency whilst the time
lag between the request for information and the time information is made available pertains to
speed of reporting. Also, frequency reflects the extent to which recent actions consequences are
quantified by information. Timeliness of the MAS information is highly essential in the health SC
to reflect a more reliable estimation of costs and up-to-date cost information as well as
identification of cost drivers and tracking of inventory. In this regard, recently made decisions are
safeguarded by a faster feedback system. Potential problems as well as opportunities are identified
in time when users’ available MAS information is frequent and timely. This offers a well-informed
and effective decisions under the attribute of frequency.
University of Ghana http://ugspace.ug.edu.gh
101
4.3.1.3 Integration of the MAS Information
Integration simply refers to the ability of the MAS information to calculate variances that have a
link to the operation of the health supply chain. In this regard, the degree to which budgeted costs
and revenue targets in the area of say procurement and hospital fees collected from patients
respectively are realized is closely monitored. Managers are compelled to evaluate whether their
estimates are close to reality whenever the budgeted is compared to the actual. In this regard,
tangible reasons can be offered for the deviations spotted and easily modify the estimations
accordingly. An extensive variance analysis leads to a modification of the budgets to reflect reality
on frequent basis. Consequently, the MAS offers more accurate, reliable, and ultimately effective
costing decisions. Integration also has to do with information concerning departmental activities
with the organization as well as interdependences constitutes the integration dimension of MAS.
This information relates to inputs, outputs, and the operations of individual departments. In effect,
the coordination of various segments within a sub-unit is facilitated by data that crosses functional
boundaries.
4.3.1.4 Aggregation of the MAS Information
This dimension of the MAS deals with the extent to which the MAS disaggregates cost accounting
to behavior. It reflects the extent to which a summary of information provided by functional units
or managers on time period basis through decision models such as inventory models, cost-volume-
profit analysis, marginal analysis, discounted cash flow analysis etc., constitute aggregated
information. More specifically, the MAS information is categorized into functional area and time
period. It also refers to summation in formats consistent with formal decision-making.
University of Ghana http://ugspace.ug.edu.gh

102
4.3.2 Supply Chain Integration (SCI)
Generally, the supply chain constitutes a series of interrelated and connected activities that involve
planning, controlling and coordinating materials, parts and finished goods from the raw materials
stage to end users (Stevens, 1989). The strategic collaboration of both intra-organizational and
inter-organizational processes constitute SCI (Wong et al, 2011) which is normally collapsed into
supplier, customer (patient) and internal integration (Flynn et al, 2010).
Activities of the supply chain are made up of sourcing and procurement, system management,
inventory management, warehousing, transportation, and customer service (Lambert, Cooper &
Pagh, 1998). SCI involves supplier integration, customer integration and internal integration
(Flynn et al, 2010). According to Flynn et al (2010, p.58)
‘‘it is the degree to which an organization strategically collaborates with its supply chain partners
and collaboratively manages intra-organizational and inter-organizational processes, in order to
achieve effective and efficient flows of products and services, information, money, and decisions,
to provide maximum value to the customer’’.
Integration of these activities affect each other to enhance performance. Based on these elements,
Cooper, Lambert and Pagh (1997) and Lambert et al (1998) describe SCM as the integration of
key business processes which involve end users through suppliers and offer value added products,
services and information to customers and other stakeholders. More precisely SCM constitutes a
key business process integration among a network of inter-dependent suppliers, manufacturers,
distribution centres, and retailers to enhance the flow of goods, services and information from
suppliers to customers at relatively reduced costs.
University of Ghana http://ugspace.ug.edu.gh
103
However, different notions of the SC which demands different forms of accounting information at
different levels of sophistication and complexities exist (Burritt & Schaltegger, 2014) and this
study focuses on that of the health SC which in relation to mainstream discrete parts and consumer
goods, is complex, sophisticated and more expensive to operate (Shah, 2004). Although the SC
has become a key driver that enhances overall organizational performance in contemporary
businesses (Field & Meile, 2008; Maestrini et al, 2017), there is evidence of underdevelopment of
research that relate the specific associations between its contextual factors, MAS design and
organizational performance (Ataseven & Nair, 2017). Like the dimensions of the MAS
information discussed in the preceding subsection, the key SCM dimensions include supplier
integration, customer integration, internal integration, transfer of knowledge (or information
sharing), risk associated with the external environment (or trust), and postponement (Li, Ragu-
Nathan & Rao, 2006; Chen et al, 2013). As stated earlier, various forms of accounting information
are required for their effective management (Ittner, Larcker, Nagar & Rajan, 1999; Dekker, 2004;
Dekker, Sakaguchi & Kawai, 2013).
However, the MAS’s primary objective of minimizing supply chain cost and creating value in
SCM is in perfect alignment with the objective of SCM which aims at creating value to the
customer. Hence, empirical investigation into the relationship between the MAS information
characteristics and SCM contextual antecedents could provide valuable insights, understanding,
and far better theoretically informed evidence and explanations of the management accounting
function in SCM decisions (Dekker, 2016).
In addition, there is diversity of lack of standardization of the nomenclature that characterize the
SCM practices. This has resulted in a confused understanding of the fundamental concepts of the
area (Behesti, Oghazi, Mostaghel & Hultman, 2014). Indeed, intended results that are
University of Ghana http://ugspace.ug.edu.gh

104
unprecedented to other management tools are provided by the supply chain. However, managing
supply chains whether as a strategic, tactical, or operational management tool must be deeply
rooted in four principles; supplier relations, sharing of information (or knowledge exchange), risks
and benefits (Kwon, Hamilton & Hong, 2011). This section explains and discusses the four
dimensions used to operationalize SCM practices in the healthcare context. As Kwon, Kim and
Martin (2016) point out, the non-availability of any one of these dimensions may result in
suboptimal performance.
4.3.2.1 Strategic Supplier Partnerships (SSP) (External Integration)
Strategic supplier partnership refers to a direct, long-term relation that exists between a focal
organization and its suppliers. In the healthcare sector, it represents the long-term relationship
between hospitals and their suppliers such as pharmaceutical manufacturers, wholesalers and
distributors of medical supplies. This relationship is such that it encourages problem-solving
efforts and mutual planning between the parties. The sharing of gains and risks among supply
chain members is the main objective of strategic supplier partnerships. Information sharing, joint
decision-making, and product and process technology transfer constitute the key attributes of
supplier partnerships (Atkinson and Waterhouse, 1996).
In this study, the definition of strategic hospital supplier is based on Vickery, Jayaram, Droge,
Calantone (2003), Barki and Pinsonneault (2005), and Chen et al (2013) as the extent to which the
business processes between a hospital and key supplier such as inter-organizational logistical
activities are strategically coupled and unified as a whole. This definition is chosen because a
major barrier cited as inhibiting the effective implementation of cost effective standardized process
(which is one of the four dimensions of supply chain performance) in the healthcare industry has
University of Ghana http://ugspace.ug.edu.gh
105
been that non-existence of cooperation among healthcare SC partners (Nachtmann & Pohl, 2009).
Either a lack of or absence of collaborative framework between a hospital and its partners.
4.3.2.2 Internal Integration (SCI)
Integration encompasses a broad array of practices emanating from information sharing at the
operational level (e.g. stock levels) to strategic issues (e.g. collaborative efforts towards new
product development) (Behesti et al, 2014; Ataseven & Nair, 2017). A shift from managing
individual functions to integrating activities into key supply chain processes is a major requirement
for successful SCM (Lambert & Cooper, 2000). The supply chain is an integrated process that
encapsulates the transformation of raw materials to final product, and the distribution of final
products to customers (Ataseven & Nair, 2017). In this regard, supply chain integration considers
the formation of networks that encompass the basic elements that form the supply chain: the focal
organization, suppliers upstream and buyers downstream (Zailani & Rajagopal, 2005). This
implies that the integration process is made up of suppliers, producers, distributors, and customers.
4.3.2.3 Level of Information Sharing (or Knowledge Exchange)
Prior studies on SCM suggest that one attribute of SCM that has become a major driver of
competitive advantage that affect performance information sharing has been information sharing.
As an important prerequisite of SCI, hospitals are part of an environment characterized by
networks of inter- and intra-organizational relationships especially in the context of increasingly
globalized and competitive economy. Studies have shown that a prevalent way of effectively
managing SCs which seek improved performance through effective use of resources and
capabilities has been closer information-based linkages. In addition, information sharing is directly
related to the quality of medical products and services, reduce SC costs, improved SC coordination,
University of Ghana http://ugspace.ug.edu.gh

106
and the achievement of competitive advantage. However, little research has been devoted to
information sharing and SC performance in the healthcare context (Chen et al, 2013).
The extent to which critical proprietary information is communicated to an organization’s SC
constitutes the extent or level in which information is shared (Li et al, 2006). Information sharing
can be grouped into four types: intra-organizational information sharing, inter-functional
information sharing, information sharing with suppliers, and information sharing with customers
(patients). The information can take several dimensions including strategic, tactic, market and
customers, logistic activities, inventory levels, product availability, expeditions and production
requirement status etc. (Ou, Liu, Hung & Yen, 2010; Behesti et al, 2014; Ataseven & Nair, 2017).
However, information sharing (or knowledge exchange) has been one of the crucial and
challenging elements in the health SC since the health SC deals with critical services and products
that impact human life (Kwon et al, 2016). Information sharing (or knowledge exchange) fosters
not only innovative capabilities among supply chain partners, but also a spirit of collaboration and
provides supply chain practitioners the opportunity to optimize the entire supply chain (Kwon &
Suh, 2004a). The quality of information is based on its accuracy, adequacy and timeliness.
Improvement in the coordination of supply chains, assurances on the quality, speed and flexibility
of delivery of goods and services, and reduced SC costs are embedded in information sharing
(Barrett & Konsynski, 1982; Sahin & Robinson, 2005; Zhou & Benton, 2007).
Information-based linkages are fundamental to effective SCM practices and performance
enhancements through effective use of resources and capabilities (Lee, So & Tang, 2000; Li &
Lin, 2006). In particular there is growing consensus that information sharing contributes
significantly to: 1) reduced supply chain costs, 2) speeding the material flow process, 3) customer
satisfaction through improvement in the order fulfillment process, 4) improvement in partner
University of Ghana http://ugspace.ug.edu.gh

107
relations, 5) channel coordination enhancements, 6) speeding the delivery of goods and services,
and 7) achieving competitive advantage.
4.3.2.4. Supply Chain Risk and Uncertainty
A significant source of risk exposure and uncertainties characterized the SC as a consequence of
the development of intensified relations with suppliers (external integration) (Dekker et al, 2013).
Thus the SC has become a significant source of risk exposure for many firms. Risks relating to
lack of cooperation between exchange partners, and to performance failures even with full Co-
poration commonly exists in most inter-firm relationships (Langfield-Smith, 2008). In order to
reap collaborative benefits, these risks need to be mitigated. An effective MAS provides timely
information to mitigate these risks. Hence, a high and strong association exists between MAS
information characteristics and SCM.
A key determinant of supply chain risk has been identified by past studies (e.g. Anderson &
Dekker, 2009) to be that relating to outcome of transactions among partners; hence, properly
labelled as transaction risks. This risk underpins two main decisions: buyers’ selection of trusted
suppliers, and collaborative practices used to manage the transactions (Dekker et al, 2013).
Adapting to this assertion, supply chain risk in this study is defined as transaction risks that
essentially relate to the risk that healthcare organizations do not achieve intended or desired
outcomes of supply chain transactions they engage in.
4.3.3 Hospital SC Performance
Judging from a theoretical standpoint, a SCM system is said to have achieved its goal of cost
reduction and value creation when the system guarantees that the correct product is procured at a
reasonable price and delivered at the right location at the right time (Dooner, 2014). In relation to
health service providers, hospital SCM deals with the information, supplies and finances that
University of Ghana http://ugspace.ug.edu.gh

108
characterize the procurement, warehousing and distribution of goods and services from suppliers
to end users with the aim of simultaneously enhancing clinical outcomes and controlling cost at
minimum levels to create value (De Vries & Huijsman, 2011). To achieve this goal, much
emphasis is placed on the integration of processes which in the healthcare setting refers not only
to physical products such as health aids, medical devices and pharmaceuticals, but also patients
related processes. Whichever the case is, the basic rational underpinning health SCM is based on
the proposition that an improved performance of the hospital SC is associated with intensive
integration and coordination of operational processes (De Vries & Huijsman, 2011).
Although different performance indicators have been proposed to capture the multi-dimensionality
measures of supply chain performance, the most frequently quoted model and widely applied has
been that of the supply chain reference model (SCOR) developed by the Supply Chain Council
(Lega, Marsilio & Villa, 2013). The SCOR model which identifies five measurement criteria for
supply chain performance assessment provides a useful framework for supply chain performance
assessment in firms (Chen et al, 2013). These metrics include cost effectiveness, responsiveness,
flexibility and speed, reliability, and efficiency in asset utilization (Zanjirani, Farahani &
Davarzani, 2009).
Various performance measures have been used in SCM studies. These range from financial
performance measures, aggregate performance and operational performance. Although, the current
study examines the relationship between variables of the supply chain and that of accounting
parameters which under normal circumstances, relate to financial performance measures, such
considerations will not address the research objectives. Considering the problem (mainly delays,
inaccessibility of drugs, higher costs, significant non-value adding steps, etc.) that this study seeks
to examine, the use of operational performance measures appropriately suits the research problem.
University of Ghana http://ugspace.ug.edu.gh

109
To operationalize the performance effects of the variables under study, and following Chen et al
(2013) and Ataseven and Nair (2017), various facets including cost effectiveness, speed and
flexibility of delivery, asset utilization and quality of the supply chain are used to measure supply
chain performance.
4.4 Formulation of Hypotheses
A number of areas in which accounting and more precisely management accounting is involved in
the management of supply chains exist in the healthcare context. These include procurement of
drugs and medical equipment, costs involved in hospital operations, inventory management, etc.
In this section, the a priori hypotheses linking the constructs are formulated. The formulation as
presented in the subsections that follow, are based on the theoretical as well as evidence of
empirical linkages between the variables. In addition, each hypothesis is formulated based on the
theoretical requirements underlying the particular contingency model to be tested.
4.4.1 MAS Information and Hospital Supplier Partnerships
One of the most enduring concerns in management accounting literature has been the narrowing
of the interface between MAS information and strategy (Bedford, Malmi & Sandelin, 2016). To
fill out this space, a large body of literature (Abernethy, Bouwens & van Lent, 2004; Auzair &
Langfield-Smith, 2005; Dekker, Groot & Schoute, 2013) adopt the contingency approach to
document systematic relationships strategy and aspects of the MAS information. One of the
features that characterize successful SCM is an earlier involvement of suppliers in buyers’ design
process which is targeted at ensuring a substantial amount of information among the parties to
leverage cost reductions and quality improvement in supply chain output (Baiman & Rajan, 2002).
University of Ghana http://ugspace.ug.edu.gh

110
It has therefore been established (Elmuti, Khoury, Omran & Abou-Zaid, 2013) that the use of SCM
tools reduce operational costs, reduce cycle time and lead to higher performance without
compromising quality. Documented examples of the impact of supply chain partners on an
organization’s overall operations demonstrate significant impact due to partner failure (Sutton,
Smedley & Arnold, 2008).
It has also been argued by management accounting researchers (e.g. Atkinson & Waterhouse,
1996; Gietzmann, 1996, pp. 614-616) that:
‘‘cost management efforts is enhanced by strategic supplier partnerships by accelerating the
product development process, improving product quality, and through supplier-originated ideas
and technologies, increasing process efficiency’’.
In this regard, supplier partners can contribute to a number of mechanisms through which cost
management efforts have been identified in supplier management and management accounting
studies. Among these mechanisms are reduction of costs associated with product development
through initial availability of prototypes, minimizing low quality costs through higher quality
product development. This ensures minimal defects, enhanced consistency between designs and
suppliers’ process capabilities, and improves the efficiency of products and processes by
incorporating supplier-originated ideas and innovations (Agndal & Nilson, 2007).
Studies such as Cooper and Yoshikawa (1994a, p.51) and Gietzmann (1996, pp.616-620) have
established that development of strategic partnerships with suppliers has been the basis for
Japanese manufacturers’ success in cost management efforts. Ittner, Larcker, Nagar and Rajan
(1999) showed that the performance benefits from strategic partnerships practices are contingent
on extensive use of the non-price selection aspects of MAS design, as well as regular meetings and
University of Ghana http://ugspace.ug.edu.gh
111
interactions with suppliers, and supplier certification. On the contrary, they found organizations
that follow arms-length supplier partnerships to make minimal gains as such practices have little
impact on performance. It has also been argued that a close collaboration amongst supply chain
partners tends to reduce transaction costs to the tune of between 35% and 40% of the costs
associated with economic activities (North, 1990; Butler, Hall, Hanna, Mendonca, Auguste, Man-
yika & Sahay, 1997), and up to 50% in IT outsourcing (Rottman & Lacity, 2006). For example,
Chrysler lost USD 24 billion due to lack of collaboration between the company and its suppliers
for over a 12-year period (de Vries & Huijisman, 2011; Henke, Stallkamp & Yeniyurt, 2014).
Maintaining supply chain relationships between SC partners reduces search review costs which
eventually contributes to increased profitability for the entire supply chain partners (Kwon et al,
2016). On the basis of these arguments, the following four hypotheses are formulated:
H1a: A positive association exists between strategic supplier relations (external
integration) and MAS design as operationalized by accounting information scope in
Ghanaian hospitals.
H1b: A positive association exists between strategic supplier relations (external
integration) and MAS design as operationalized by accounting information
timeliness in Ghanaian hospitals.
H1c: A positive association exists between strategic supplier relations (external
integration) and MAS design as operationalized by accounting information
integration in Ghanaian hospitals.
University of Ghana http://ugspace.ug.edu.gh
112
H1d: A positive association exists between strategic supplier relations (external integration)
and MAS design as operationalized by accounting information aggregation in Ghanaian
hospitals.
4.4.2 MAS Information and Hospital Supply Chain Integration (Internal Integration)
A key practice identified to facilitate the management and achievement of superior performance
in SCM has been the integration of supply chains (Wiengarten, Humphreys, Gimenez & Mclvor,
2016). Beheshti et al (2014) found that organizations that operate total supply chain integration
reported the highest level of financial performance. Three perspectives characterize the
development of supply chain integration: strategic, tactical and operational Tseng and Liao (2015).
In their comprehensive review of SCM studies from 1990 to 2011, Shi and Yu (2013) found that
SCI play a critical role in improving firm-level financial performance.
From the perspective that SCM comprises several interrelated facets of integration (Fabbe-Costes
&Jahre, 2008), various facets of the integration dimension in supply chains have been investigated
by scholars. These include external integration with both suppliers and customers and internal
integration with functional units within the organization. These three forms of integration are
defined by Schoenherr and Swink (2012, p. 100) as follows: supplier integration relates to ‘‘the
information sharing and coordination activities involving key or strategic suppliers which provide
the firm with insights related to the processes, capabilities and constraints related to suppliers that
ultimately enable more effective planning, product and process design, forecasting, and transaction
management’’.
University of Ghana http://ugspace.ug.edu.gh
113
Internal integration on the other hand, is the ‘‘cross-functional intra-firm collaborations and
information sharing activities that occur via interconnected synchronized processes and systems’’.
It is clear from this definition that internal integration basically measures an organization’s
logistics, operations, marketing, and sales collaborations for the purposes of realising overall
supply chain objectives. Finally, Schoenherr and Swink (2012, p. 100) define customer integration
as ‘‘the close collaborations and information sharing activities with key customers which furnish
the firm with insights into market expectations and opportunities which ultimately enable more
efficient and effective response to customer needs’’.
Like the mainstream business organizations, all these facets of SCM integration apply to the health
supply chain and accounting information play a significant role in providing the required and
relevant information to achieving these objectives which ultimately enhances performance
(Dekker, 2004; Coad & Cullen, 2006; Fayard et al, 2012). Ataseven and Nair (2017) meta-
analytically examined the association between supply chain integration and its underlying
dimensions and the operational characteristics of cost, flexibility, delivery, and quality of the
supply chain and found a significant impact of the three dimensions of integration: supplier
integration, internal integration, and customer integration on the four performance attributes. It is
therefore expected that the fit between the dimensions of MAS and hospital supply integration will
positively affect performance as operationalized by cost effectiveness, utilization of hospital
assets, speed, flexibility and quality of the supply chain. on the basis of this prediction the
following hypotheses are formulated:
University of Ghana http://ugspace.ug.edu.gh
114
H2a:
H2b:
H2c:
H2d:
There is a positive association between hospital supply chain integration (internal integration)
and MAS design as operationalized by the scope dimension of accounting information in
Ghanaian hospitals.
There is a positive association between hospital supply chain integration (internal integration)
and MAS design as operationalized by the timeliness dimension of accounting information in
Ghanaian hospitals.
There is a positive association between hospital supply chain integration (internal integration)
and MAS design as operationalized by the integration dimension of accounting information in
hospitals in Ghana
There is a positive association between hospital supply chain integration (internal integration)
and MAS design as operationalized by the aggregation dimension of accounting information in
Ghanaian hospitals.
4.4.3 MAS Information and Level of Information Exchange
A key driver in SCM is the flow of information and partners’ ability to analyse information (Coad
& Cullen, 2006; Fayard et al, 2012). Information sharing enhances the channel’s capacity to
developments in the entire market. The receiving and sharing of information by a partner firm
enhances the competitive position of that firm (Chen et al, 2013; Behesti et al, 2014). It is so related
to supply chain integration that the design of the latter is normally not effective in the absence of
the former. The quality of the shared information is highly critical for effective SCM as
organizations feel insecure in giving out more than minimal information (Jamal & Tayles, 2010).
Ataseven and Nair (2017) document that information sharing (or knowledge exchange) involving
process and product designs, coordination, and joint decision making are key elements that are
University of Ghana http://ugspace.ug.edu.gh

115
relied upon by supply chain partners to foster supply chain integration. Information sharing (or
exchange) facilitates the alignment of the interest of all firms within the supply chain which
ultimately enhances overall supply chain performance.
The quality dimensions include scope, accuracy, adequacy and timeliness which underpin the four
MAS information characteristics: broad scope, timeliness, integration, and aggregation of
accounting information (Chenhall & Morris, 1986). MAS design plays a significant role in
enhancing the quality level of information communicated among supply chain partners. The higher
the quality of shared information, the higher the sophistication level of MAS design. Based on
these arguments, the following hypotheses are formulated:
H3a:
H3b:
2H3c:
H3d:
There is a positive association between level of information sharing (or knowledge
exchange) and MAS design as operationalized by the scope dimension of accounting
information in Ghanaian hospitals
There is a positive association between level of information sharing (or knowledge
exchange) and MAS design as operationalized by the timeliness dimension of
accounting information Ghanaian hospitals.
There is a positive association between level of information sharing (or knowledge
exchange) and MAS design as operationalized by the integration dimension of
accounting information in Ghanaian hospitals.
There is a positive association between level of information sharing (or knowledge
exchange) and MAS design as operationalized by the aggregation dimension of
accounting information in Ghanaian hospitals.
University of Ghana http://ugspace.ug.edu.gh

116
4.4.4 MAS Information and Hospital Supply Chain Risk and Uncertainty
To many firms, the supply chain has become a significant source of risk exposure following the
development of intensified relations with suppliers (Dekker et al, 2013). In particular, firms are
exposed to significant risks that need to be mitigated to enhance not only performance of
collaborative relations in supply chains, but also realized the benefits associated with such relations
(Langfield-Smith, 2008). Risks related to both failures associated with performance of full co-
operation and lack of co-operation between exchanges partners have been identified as important
elements of the supply chain.
For inter-firm relations to become successful, adequate risk management is critical (Ding, Dekker
& Groot, 2013). Transaction costs economics (TCE) has been the dominant paradigm in analysing
MAS design in inter-firm relations, including supplier partner selection choices (Anderson &
Dekker, 2009). TCE posits that the choice of controls in inter-firm relations are expected to be
aligned with the underlying exchange hazards in order to minimize transaction costs. Past studies
such as Cooper and Slagmulder (2004) suggest a stronger relational context characterized by trust
between exchange partners is largely supported. This arises from the use of cost management
practices in supply chains.
In testing hypothesis about the relationships between selection of trusted suppliers, transaction
risk, and use of SCM practices in Japanese manufacturing firms, Dekker et al (2013) found that
MAS play a significant role in mitigating the risks associated with intensified collaborations with
supply chain partners. They established that information sharing, operational reviews, contractual
contingency planning, supplier support, performance target setting, , and joint problem solving as
control practices are SCM practices in which MAS can provide information to minimize supply
chain risks. Being the key determinant of risk in supply chain transaction (Anderson & Dekker,
University of Ghana http://ugspace.ug.edu.gh

117
2009), transaction risks are categorized into 1) relational risks, which concerns opportunistic
behaviours of self-interested partners and 2) performance risks, which concern performance
failures even at the instance where partners cooperate fully (Dekker et al, 2013).
The characteristics of transactions considered in empirical studies (e.g. Anderson & Dekker, 2005;
Ellis, Henry & Shockley, 2010) as important and antecedents of governance choices that underpin
transaction risks include size of the transaction, asset specificity, product complexity, uncertainty,
and absence of competition. Uncertainty types that result from environmental changes in market
and technology, unpredictability of technology development, and monitoring problems regarding
suppliers’ behaviours and performance have links with MAS design (Anderson & Dekker, 2005).
Beckmann, Hielscher and Pies (2014) state that supply chain associations are hedged against
complexity and uncertainty and that a decision support for managers in uncertain, globalized,
logistics-oriented and new communication settings must be provided by accounting. Burritt and
Schaltegger (2014), note that the wheels of supply chain relationships are oiled with information
provided by accounting.
Accounting systems require formalized categories for collecting and reporting information as well
as creating a common language with which members of the organization can communicate (Burritt
& Schaltegger, 2014). Financial factors such as revenues, operating costs, hedging against
uncertainties, investment planning and other corporate financial decisions are among the issues
that have strong impact on the configuration of SCNs (Melo, Nickel & Saldanha-da-Gama, 2009).
Based on the foregoing the following hypotheses are formulated:
University of Ghana http://ugspace.ug.edu.gh

118
H4a:
H4b:
H4c
H4d:
A positive association exists between level of supply chain risk and uncertainty and
MAS design as operationalized by the scope dimensions of accounting information
in Ghanaian hospitals.
A positive association exists between level of supply chain risk and uncertainty and
MAS design as operationalized by the timeliness dimensions of accounting
information in Ghanaian hospitals.
A positive association exists between level of supply chain risk and uncertainty and
MAS design as operationalized by the integration dimensions of accounting
information in Ghanaian hospitals.
A positive association exists between level of supply chain risk and uncertainty and
MAS design as operationalized by the aggregation dimensions of accounting
information in Ghanaian hospitals.
4.5. Mediating Role of MAS Information in Supply Chain Performance
Hospital-supplier integration both partially and fully mediate the impact of information sharing on
hospital supply chain performance.
4.5.1: MAS and Supplier Relations (External Integration) on Performance
Although the design and use of MASs have the ultimate goal of improving both financial and
operational supply chain performance, empirical evidence on the positive relationship between
MAS information characteristics and operation performance is relatively scarce (Macinati &
Anessi-Pessina, 2014). This is due mainly to the fact that a greater portion of MAS information
University of Ghana http://ugspace.ug.edu.gh

119
benefits is generally qualitative and intangible in nature. On the other hand, studies such as
Christensen and Demski (2002), Ferreira (2002), and Baines and Langfield-Smith (2003) have
argued that the effect of MAS design on organizational performance depends, to a greater extent,
on the way the MAS information is used by those who receive such information. The wheels of
supply chain relationships are oiled with information provided by the MASs with a stronger focus
on logistics and information flows about corporate performance (Burritt & Schaltegger, 2014).
Accounting offers a significant input to the selection of suppliers through the auditing of supplier
environmental performance, reduction of waste and packaging materials, and health and safety
which enhance operational performance. The monitoring of performance is largely achieved by
means of accounting information with one aspect being supply chain cost. MAS considers the
information involved with external suppliers often working together across multiple supply chains,
are linked together by agreement. Timely cost information is not only a crucial element in the
strategic sourcing decisions but also influences the ongoing management of supplier relations.
In examining the relationship between managers’ beliefs about the relevance and usefulness of
cost data, cost-system functionality, and actual financial performance in US hospitals, Pizzini
(2006) found a positive association between the relevance and usefulness of cost accounting data
as evaluated by managers and the extent of the MAS in providing detailed costing systems, classify
costs according to behaviour, and frequent reporting of cost data. He however, found that out of
the three attributes of the MAS, only the cost detail attribute correlated positively with measures
of financial performance such as cash flow, operating margin, and administrative expenses.
Further, a statistically insignificant relationship between cost-system design and operating expense
per admission was confirmed. The conclusion drawn was that the use of accounting information
has not yet been successfully applied in the management of clinical costs of the sampled hospitals.
University of Ghana http://ugspace.ug.edu.gh
120
The coordination of supply chain relationships and use of management control mechanisms to
support, plan, measure and assess supply chain activities and their results impact significantly on
supply chain performance (Van de Meer-Kooistra & Vosselman, 2000). Also, one of the key issues
in SCM has been supplier selection and more sophistication is the approach being promoted to
address supply chain interrelationships. However, studies into accounting issues that relate to
supplier selection is far limited (Burritt & Scaltegger, 2014). Particularly, in the exchange with
medical suppliers both within and across the country, a simpler costing system in the supplier
collaborative setting examined would be more effective for supply chain performance in relation
to some hospital operations such as minimization of total order cost as well as low inventory cost.
For example, ABC models available for purchasing often regard supplier evaluation and selection,
ordering, transportation, receiving, handling, quality control and storage as a set of standardized
activities carried out in a sequential fashion (Dekker & van Goor, 2000). It has been recognized
that complexity is added by the the global setting, and this affects accounting as supply chain
partners often extend to several logistics service providers, the supplier, the manufacturer, the
retail sector and the final customer. Based on these assertions, the following hypothesis is
formulated:
H5a: The relationship between strategic supplier relations (external integration) and hospital
supply chain performance is explained by an indirect effect of MAS information
whereby strategic supplier relations reduces MAS information which in turn enhances
operational performance of Ghanaian hospitals.
University of Ghana http://ugspace.ug.edu.gh
121
4.5.2. MAS and Supply Chain Integration (Internal Integration) on Performance
Conventional MAS is largely about identifying and recording inter-firm data from which are
derived from external market transactions, intra-firm internal transformations and some events
considered as external. To a large extent, SCM also looks at intra-supply chain processes and
transactions, transformations, and events including non-market interactions (Scaltegger & Burritt,
2014). Whilst a consideration is given to MASs external to the supply chain, inter-supply chain
data from external market transactions, intra-supply chain transactions as well as some external
events of the supply chain are addressed by MAS to enhance performance (Burritt & Scaltegger,
2014). For example, few supply chain settings for accounting arise whenever there is
preponderance for vertical integration. MASs in supply chain integration place much emphasis on
the efficient use of resources and minimization of costs to enhance performance. Inter-firm cost
savings in supply chains is largely promoted by activity-based costings which is the costing system
widely used in hospitals (Schulze, Seuring & Ewering, 2012; Kwon, 2016). As noted by Dekker
and van Goor (2000), to internally integrate supply chain members, a set of MAS standards is
needed. This takes a calculation of the cost of logistics for the supply chain which is based on a
joint definition of activities and their cost drivers. This results in the aggregation of supply chain
activity based costs. In this regard, cost accounting methods such as material flow cost accounting
has been developed for supply chain accounting.
H5b: The relationship between supply chain integration (internal integration) and HSC
performance is explained by an indirect effect of MAS information whereby level of
information exchange reduces MAS information which in turn enhances HSC
performance in Ghana.
University of Ghana http://ugspace.ug.edu.gh

122
4.5.3: MAS and Level of Knowledge Exchange on Performance
Information sharing in SCM has become a major driver that enhances organizational overall
performance (Ataseven & Nail, 2017). Where organizations, particularly healthcare institutions
belong to an environment comprising a network of intra and inter-organizational relationships,
information sharing as an important prerequisite emerges in the integration of supply chains.
However, the effect of information sharing on MAS design and the corresponding impact on
supply chain performance has had very little analysis. It has been argued that improved supply
chain coordination, reduced supply chain costs, quality of products and services, and the
achievement of competitive advantage is directly related to effective information sharing. The
function of MAS is to provide information that assists with the determination and sharing of gains
from supply chains (Burritt & Scaltegger, 2014). The link between information sharing and MAS
information is crucial in SCI as it reinforces connectedness, coordination and collaboration among
supply chain members. Studies have shown that a prevalent way of effectively managing supply
chains is to employ closer information-based linkages. This form of SC management become seeks
improved performance through effective use of resources and capabilities. However, whilst there
have been studies relating information sharing and supply chain performance, there are no studies
that link MAS information characteristics to performance. Very few studies investigate the specific
effect of information sharing (or knowledge exchange) on SC performance. On the basis of this
assertion, the following hypothesis is formulated:
H5c: The relationship between the level of knowledge exchange and HSC is explained by
an indirect effect of MAS information whereby supply chain risk and uncertainty
reduce MAS information which in turn enhances HSC performance in Ghana.
University of Ghana http://ugspace.ug.edu.gh

123
4.5.4. MAS and Supply Chain Risk and Uncertainty on Performance
Supply chain arrangements are normally characterized with risk, complexity and uncertainty
(Beckmann et al, 2014). For example, in testing hypothesis about the relationships between
selection of trusted suppliers, transaction risk, and use of SCM practices in Japanese manufacturing
firms, Dekker et al (2013) found that MAS play a significant role in mitigating the risks associated
with intensified collaborations with supply chain partners. They established that information
sharing, operational reviews, contractual contingency planning, supplier support, performance
target setting, and joint problem solving as control practices, are SCM practices in which MAS
provides information to minimize supply chain risks. In this regard, MASs provide decision
support for managers in the uncertain, new communications settings, logistics-oriented, globalized
settings in supply chain management (Burritt & Scaltegger, 2014). Management accounting
scholars have responded with studies of how firms use MASs to mitigate the risks and uncertainties
associated with inter-firm exchanges (Langfield-Smith, 2008; Anderson & Dekker, 2005). Two
general types of risks are associated with the supply chain: relational risk and performance risk
(Anderson, Christ, Dekker & Sedatole, 2015) and are highly associated with the health supply
chain. Whereas a lack of cooperation between supply chain partners that could result in
opportunistic behaviour and appropriation of firm value by the other partner represents relational
risk, that of performance risk represents the risk of failure despite full cooperation. These risks
normally arise from the complexity and uncertainty that characterize the supply chain as well as
environmental influence. MASs are considered as primary mechanisms for mitigating these risks
through the alignment of partners’ interest and the coordination of their actions across boundaries.
University of Ghana http://ugspace.ug.edu.gh

124
H5d: The relationship between hospital supply chain risk and uncertainty and HSC
performance is explained by an indirect effect of MAS information whereby supply
chain integration reduces MAS information which in turn enhances HSC
performance in Ghana.
4.6 Contingency Effect of the SCM Contextual Dimensions
The interaction of individual characteristics of SCI to affect performance is supported by
contingency theory (Flynn et al, 2010). The environment within which an organization operates
shapes its processes and structures. This implies that in order to maximize performance,
organizations should align their structures and processes to their environment (Donaldson, 2001).
In this regard, organizations make the effort to integrate SCM characteristics with the dimensions
of MAS. To achieve better operational performance, organizations take full advantage of internal
integration. To discern the role of moderating factors in SCI, Ataseven and Nair (2017) point to
the need for investigating specific associations between SCI and performance within contingency
frameworks. This call is based on evidence of underdevelopment of contingency-based studies
that investigate the effect of SCI on organizational performance. They document the moderators
that affect either the strength or form of the relationship between an exogenous variable and a
criterion variable to enhance theory development within the SC are those contextual factors. In
this subsection the theoretical inter-linkages of the moderator between MAS design and hospital
supply chain performance is presented.
4.6.1. Supplier Relations (External Integration) to Performance
Contingency theory suggests that external fit implies that there is consistency between the
strategies an organization adopts in response its organizational structure and its external
University of Ghana http://ugspace.ug.edu.gh

125
environment (Flynn et al, 2010). This means that to form an important element of SCI, supplier
relations are built on hospitals SC internal integration. In this regard, a change in the external
environment should be met by hospitals through the development, selection and implementation
of strategies that will maintain and keep the level of fit. For example, drugs within the Ghanaian
hospitals are either not physically or financially accessible or both. Opportunities for improving
the accuracy of demand information is offered by a close relationship between hospitals and
manufacturers of drugs, which in effect, minimizes the manufacturer’s product design and
production planning time, and allows it to be more responsive to customers (patients) needs. This
also enables manufacturers to detect demand changes more quickly, create greater value, and
reduce costs because supplier integration offers opportunities for the intelligence embedded in
collaborative processes to be leveraged. In an integrated supply chain, an understanding and
anticipation of the manufacturer’s needs in order to better meet its changing requirements is
facilitated through the development of strong strategic partnerships.
H6a: For higher levels of supplier relations, MAS will positively affect hospital supply
chain. For lower levels of supplier relations, MAS information will negatively
affect hospital supply chain performance in Ghana.
4.6.2. Relationship of Internal Integration to Performance
Like the consistency among structural characteristics within an organization which represents
internal fit (Drazin and van de vein, 1985), supply chain integration (internal integration)
recognizes that within a hospital, different functional areas and departments should operate as part
of an integration process. Since within healthcare institutions, functional barriers are broken by
internal integration and fosters cooperation in order to meet customer (patient) satisfaction. Rather
University of Ghana http://ugspace.ug.edu.gh

126
than operating within the functional areas associated with the traditional specialization and
departmentalization, it is expected to have a link to performance. Although hospitals may maintain
a functional organizational structure, patients’ demands normally flow across activities and
functions. Studies (Germain & Iyer, 2006) have shown that the interaction between various forms
of integration (e.g. customer integration and internal integration were linked to logistics and
financial performance. In another study, Droge, Jayaram and Vickery (2004) found that the effect
of strategic supplier relations (external integration) on performance was moderated by internal
integration. Also, Davaraj, Krajewski and Wei (2007) found that the relationship between supplier
integration and performance was moderated by customer integration. No study has however,
interacted either internal integration or external integration with the MAS information
characteristics to affect performance. For the purposes of the link between MAS information and
SCM to advance theory, the following hypothesis is proposed:
H6b: For higher levels of supply chain integration, MAS information will positively
affect HSC performance. For lower levels of supply chain integration, MAS
information will negatively affect HSC performance in Ghana.
4.6.3. Relationship of Level of Knowledge Exchange to Performance
It has been argued that improved supply chain coordination, reduced supply chain costs, quality of
products and services, and the achievement of competitive advantage is directly related to
integration and effective information sharing. The function of the MAS is to provide information
that assists with the determination and sharing of gains from supply chains (Burritt & Scaltegger,
2014). The link between integration, information sharing and MAS information is crucial in SCM
as it reinforces connectedness, coordination and collaboration among supply chain members
University of Ghana http://ugspace.ug.edu.gh

127
(Dekker, 2016). However, whilst there have been studies relating integration, information sharing
and supply chain performance, there are no studies that link MAS information characteristics to
SC performance. In addition, very few studies investigate the specific effect of integration and
information sharing (or knowledge exchange) on SC performance. Furthermore, the effect of both
SC integration and information sharing on MAS design and the corresponding impact on SC
performance has had very little analysis. Chen et al (2013) found that a positive direct relationship
exists between hospital strategic partnership, and information sharing, between information
sharing and hospital-supplier integration, and between hospital-supplier integration and hospital
supply chain performance from a sample of 117 supply chain executives in US hospitals. In
addition, hospital perceived environmental uncertainty was found to moderate the relationship
between strategic supplier partnership and level of information sharing and hospital supply chain
performance. On the basis of this assertion, the hypothesis on both the impact of internal and
external integration, information sharing, and supply chain risk and uncertainty on MAS design is
formulated.
H6c: For higher levels of information exchange, MAS information will positively affect
HSC performance. For lower levels of information exchange, MAS information
will negatively affect HSC performance in Ghana.
4.6.4. Relationship of Supply Chain Risk and Uncertainty to Performance
Literature suggests that SC integration (internal and external integration) has a positive effect on
operational performance outcomes such as cost, speed of delivery, flexibility, and quality (Wong
et al, 2011). Supply chain risk and uncertainty has been identified as a contextual factor which
may affect the effectiveness of a best practice. Whilst some recent studies (Fynes, de Buˇırca &
University of Ghana http://ugspace.ug.edu.gh

128
Marshall, 2004) argue that both internal and external integration and performance are moderated
by supply chain risk and uncertainty. These studies are however problematic because first, they
used different approaches in the conceptualization of supply chain integration, performance and
the contingency constructs which does not permit a meaningful comparison of, or conclusion about
the contingency effects of risk and uncertainty. The following hypothesis is formulated:
H6d: For higher levels of supply chain risks and uncertainties, MAS information will
negatively affect HSC performance. For lower levels of supply chain risk and
uncertainty, MAS information will positively affect HSC performance in Ghana.
4.7 Chapter Summary
In this chapter, the study’s theoretical framework has been presented. It discusses the three main
variables underpinning the study and their sub-constructs. The justification for selecting the
dimensionalities of each of the constructs is given. It shows that each of the four main constructs
is multidimensional which can be explained by several other constructs. The chapter also shows
the theoretical as well as the empirical linkages among the constructs based on which the verbal
hypotheses are formulated.
The hypotheses formulation is based on three models of contingency fit: selection, mediation and
moderation. Hence, three models of contingency fit are to be tested. The chapter shows that
formulation of contingency hypotheses differs from those of universal theories and that the verbal
hypothesis formulated to test a particular form of contingency fit should align with its theoretical
interpretation. The formatted hypotheses also fall in line with the statistical methodology being
employed. For example, the selection form of fit is based on correlation analysis which works very
University of Ghana http://ugspace.ug.edu.gh

129
well with covariance based structures. The same arguments hold for the mediation and moderation
forms of fit. Finally, it outlines the 12 hypotheses to be tested. Each of the three contingency fit
models being theorized has four testable hypotheses. The study’s methodology in terms of the
sample data and the statistical analysis involved are presented next in chapter five.
University of Ghana http://ugspace.ug.edu.gh

130
CHAPTER FIVE
METHODOLOGY
5.1 Introduction
The preceding chapter presented the underlying theoretical framework and the hypotheses that
guide the study. In this chapter, the general approach and methods to the study’s total execution is
presented. The research methodology is a term used to describe the methods, procedures and
assumptions that are applied towards gathering and analysing data in a research work (Creswell,
2014). At the level of documenting a study, the methodology constitutes the specification and
justification of the most suitable methods applied, including an identification of the study’s
philosophical stance, research design, sampling approach and sample size, data collection,
instrumentation, and data analysis method. The overall objective of this study is to investigate the
hospital SC performance effects of the contingency fit between SCI, information sharing, SC risk
and uncertainty and MAS design in healthcare context using empirical data from Ghana.
The chapter has four main sections. In the first section, the philosophical dimension underpinning
the study is briefly presented. In the second section, and following Van de Stede, Young & Chen,
(2005), a discussion of the framework that contains five key elements of a well-designed survey
in management accounting research is presented. These include a description of the (1) design
strategies and purpose of the survey, (2) population and definition of the sampling, (3) research
method issues such as survey questions and others, (4) accuracy of data entry and data collection
techniques, and (5) reporting and disclosure. The modelling approach to empirically analysing and
estimating the sample data is presented in section three. This involves testing and validation of the
measuring instruments/scales for reliability and internal consistency. Finally, a detailed description
University of Ghana http://ugspace.ug.edu.gh

131
of the empirical estimation model and its underlying statistical assumptions is presented. The
chapter ends with a summary.
5.2 The Study’s Philosophical Underpinning
Fundamentally, research in the academic domain is underpinned by some basic philosophical and
meta-theoretical assumptions, and are either explicitly or implicitly defined by the researcher.
Research paradigms underpin the basis of the researcher’s understanding of the research problem
and constitute the foundation for testing criteria as well as answering research questions. Although
paradigms are hidden in most research, their understanding help in the clarity of research designs.
They not only take into account the kind of evidence that is required and how it is to be gathered
and interpreted, but also how the evidence will provide good answers to the basic questions being
investigated. Knowledge of philosophy also assists the researcher in distinguishing the workable
designs from those that are not. Besides, understanding the difference between philosophical
assumptions and theoretical underpinnings is critical to the overall understanding of the
perspective from which the research is designed and conducted.
Philosophical paradigms refer to the basic belief system or world view that guide the study. A
paradigm, according to Kuhn (1962), consists of a cluster of substantive concepts, variables with
attached problems, and corresponding methodological approaches and tools that are integrated in
nature. Originally, Kuhn (1962) used the term to represent a conceptual framework which is shared
by a community of scientists. This provided them with a convenient model that examines and finds
solutions to problems. To this end, he labelled a paradigm as a research culture that possesses
unique values, assumptions and a set of beliefs which are common to a research community
regarding the nature and conduct of research.
University of Ghana http://ugspace.ug.edu.gh
132
Like all other disciplines, research paradigms address the philosophical dimensions of social
sciences within which accounting research is conducted. However, there has been a concern for
increasing narrowness of accounting research in terms of its philosophical assumptions,
methodological approaches, and theoretical underpinnings. For example, Lukka (2010) noted that
the current hegemonising tendencies of mainstream accounting research have led to excessive
homogeneity in accounting research and as reported by Chua (1986) have restricted the range of
problems studied and the methods used. In the notion of paradigms Lukka (2010) states that
fundamentally, different kinds of options for conducting accounting research always exist, at least
in principle, thereby seeking to invigorate accounting researchers’ consciousness of this plethora
of possibilities.
5.3. Dimensions of Philosophical Assumptions
Paradigms are distinguished between the ontology, epistemology, methodology and axiology
dimensions. In this section, each of these individual dimension is discussed. First the philosophy
of reality represented by ontology is discussed. This is followed by epistemology which refers to
the philosophy of knowledge whilst the methodology which dictates the methods used and that of
axiology, which specifies the value of the research follows.
5.3.1. Ontology
When developing their methodologies for conducting research, both social scientists and scientists
generally draw from different ontological and epistemological assumptions. In social research, one
perceives the existence of reality as external, independent of social actors and their interpretations
of it (i.e., objectivist or realist). The other assumption is that reality is dependent on social actors
University of Ghana http://ugspace.ug.edu.gh

133
and that individuals contribute to social phenomenon (i.e., subjectivist or nominalist). Stated
differently, a researcher who views reality as objectively given is labelled positivists and believe
that the reality can be measured by means of the properties which the researcher is independent of
as well as the instruments he/she is using. More specifically a positivist researcher views
knowledge as quantifiable and objective. Scientific methods are adopted by positivist thinkers and
with the help of quantification to enhance precision in the description of parameters and the
relationship among them, systematize the knowledge generation process. On the other hand,
researchers who view reality as consisting of individuals’ subjective experiences of the external
world are labelled interpretive and believe that reality is socially constructed. Based on an in-depth
examination of the phenomenon of interest, they derive their constructs from the field. Four
different ontologies include realism, internal realism, relativism and nominalism.
5.3.2. Epistemology
Epistemology refers to the philosophy of knowledge; that is the belief of knowledge production or
what constitutes acceptable knowledge. It shows that there are different ways into which the nature
of the physical and social worlds are inquired (Easterby-Smith, Thorpe and Jackson, 2012). Having
established the existence of reality, epistemology identifies the processes by which that reality is
known; that is it answers the why of why of how questions. It is the beliefs on the way to generate,
understand and use the knowledge that are deemed to be acceptable and valid. Positivism and
social constructionism represent two contrasting views of how social science research should be
conducted. Epistemology focuses around the respective merits of these two views.
University of Ghana http://ugspace.ug.edu.gh
134
5.3.3. Methodology
Methodology represents a basic belief that affects the ways of investigating reality. In the context
of a particular paradigm, it refers to a model for undertaking a research process. A clear distinction
is always drawn between methodology and methods. Whilst methodology represents a domain or
map or blueprint of the study, method is used to denote the steps to be taken or the techniques to
be employed in gathering and analysing data. Methodologies dictate the methods in that they
comprise the set of beliefs that guide a researcher to select one set of research methods over the
other. Methodologies answer the why of how questions. A research method, on the other hand,
consists of a set of specific procedures, tools and techniques to gather and analyse data and answers
the how questions. A research method falls under theories different from methodologies and
philosophies. A research method refers to the practical application of doing research whereas
methodology represents the ideological and theoretical foundation of the method; hence, the
quantitative-qualitative debate is philosophical not methodological. In this regard, a research
design is required to link an appropriate set of research methods and a methodology in order to
answer research questions and/or test hypotheses that have been verbally formulated to examine a
phenomena.
5.3.4. Axiology
Like methodology, axiology represents the basic beliefs that affect the ways in which realities are
investigated. It is concerned with ethics which encompasses the role of values in research and the
researcher’s stance in connection with the subject being investigated. The essence of ontology,
epistemology, methodology, axiology and methods is summarised in Table 5.1
University of Ghana http://ugspace.ug.edu.gh

135
Table 5.1: Ontology, Epistemology, Methodology, Axiology and Methods Distinguished
Philosophy Meaning
Ontology Philosophical assumptions about the nature of reality
Epistemology A general set of assumptions about ways of inquiring into the nature of the world
Methodology A combination of techniques used to inquire into a specific situation
Methods Individual techniques for data collection and analysis
Axiology The role of values in research and the researcher’s stance
(Source, Captured from Easterby-Smith et al, 2012)
5.4. Paradigms in Management Research
The main paradigms that characterised the philosophical debates in management research include
positivism, post positivism/critical realism, interpretivism or social constructionism and
pragmatism. These are discussed in the ensuing sub-sections.
5.4.1. Positivism
Positivists assume that there is external existence of the social world; hence, objective methods
should be employed to measure its properties rather than being inferred subjectively through
intuition, reflection or sensation. This means that positivists apply the lens of natural science to
social science. Ontologically, social reality is external and objective. Epistemologically, the use of
scientific approach by developing numeric measures to generate acceptable knowledge is
advocated. It is also assumed epistemologically that knowledge is only of significance if it is based
on observations of the external reality. Testing of theories in the form of hypotheses using
statistical tests characterised the research process. In the axiological sense, a separation of the
researcher from the researched is maintained by taking the stance of etic approach or the outsider
perspective. Positivists seek to obtain law-like generalisations by conducting value-free research
University of Ghana http://ugspace.ug.edu.gh

136
to measure social phenomena. Table 5.2 summarises the implications of positivist philosophical
assumptions.
Table 5.2: Implications of Positivist Philosophical Assumptions
Operationalization Concepts need to be defined in ways that enable facts to be measured
quantitatively.
Reductionism Problems as a whole are better understood if they are reduced into the simplest
possible elements.
Generalisation In order to move from the specific to the general it is necessary to select random
samples of sufficient size, from which inferences may be drawn about the wider
population.
Hypothesis/Deduction Science proceeds through a process of hypothesizing fundamentals laws and
then deducing what kinds of observations will demonstrate the truth or falsity
of these hypotheses
Causality The aim of the social science should be to identify causal explanations and
fundamental laws that explain regularities in human social behaviour.
Cross-sectional
Analysis.
Such regularities can most easily be identified by making comparisons of
variations across samples.
Independence The observer must be independent from what is being observed.
Value freedom The choice of what to study, and how to study it, can be determined by objective
criteria rather than by human beliefs and interests.
(Adapted from Easterbay-Smith et al, 2012, P. 23)
5.4.2. Social Constructivism
Referred to as interpretivism, it is a paradigm developed primarily, in reaction to the application
of positivism to the social sciences and stems from the view that reality is not objective and exterior
but is socially constructed and given meaning by people. To this end, interpretivists reject
objectivism and a single truth as proposed in positivism. It focuses on the ways people make sense
of the world especially through sharing their experiences with others via the medium of language.
In this regard, a recognition of individuals with varied backgrounds, experiences and assumptions
is what interpretivists offer. These contribute, through social interaction, to the on-going
construction of reality existing in their broader social context. Interpretivist researchers prefer to
interact and to have dialogue with the studied participants in order to understand the social world
University of Ghana http://ugspace.ug.edu.gh

137
from the subjective meanings people attach to it. Qualitative data which provides rich descriptions
of social constructs and a narrative form of analysis to describe specifics and highly detailed
accounts of a particular social reality being studied is the focus of interpretivists. Table 5.3
summarises the contrasting implications of social constructionism and positivism.
Table 5.3: Positivism and Social Constructionism Contrasted
Positivism Social Constructionism
Explanations Must demonstrate causality. Aim at increasing general understanding
of the situation.
Human Interest Is irrelevant Are the main drivers of science
The observer Must be independent. Is part of what is being observed.
Research Progression Through hypotheses and
deductions
Gathering rich data from which ideas are
induced
Sampling Requirements Large numbers selected
randomly.
Small numbers of cases chosen for
specific reasons.
Unit of Analysis Should be reduced to
simplest terms
May include complexity of whole
situations
Generalization Through Statistical probability Theoretical abstraction
Concepts Need to be defined so that
they can be measured.
Should incorporate stakeholder
perspectives.
5.4.3. Pragmatism
Pragmatists argue that objectivism and subjectivism perspectives as in positivism and social
constructionism respectively are not mutually exclusive and that one should view research
philosophy as a continuum rather than an option that stands in opposite directions. In the
pragmatists view a mixture of ontology, epistemology and axiology is acceptable as an approach
to understanding social phenomena. In this regard, emphasis is on what works best to address the
research problem at hand. Both quantitative and qualitative data are employed by pragmatists as a
way of better understanding social reality. The relationship between ontology, epistemology,
axiology and their respective paradigms are summarised in Table 5.4.
University of Ghana http://ugspace.ug.edu.gh

138
Table 5.4: Relationship between Philosophical Assumptions and Paradigms
Research Paradigm
Fundamental Belief Positivism
(realism)
Post positivism
(critical Realism)
Interpretivism
(constructionism)
Pragmatism
Ontology External External Socially
constructed
External,
Multiple View
Realist Nominalism
Epistemology Objective Objective Subjective Objective
Subjective
Methodology Quantitative Quantitative or Qualitative Quantitative &
Qualitative Qualitative
Axiology Value-free & Value-Laden & Value – Laden & Value-Laden
Etic Etic Emic Etic 7 Emic
(Source: Developed by Author)
5.5. Paradigms in Accounting Research
Paradigms in accounting research are rooted in Burrell and Morgan’s (1979) sociological
framework. Until recently, the widely accepted view of the role of accounting as a research field
has been that of establishing general laws that encapsulates empirical events’ or objects’ behaviour
which is normally concerned with science, and facilitating the connection of the knowledge of
separable known events and to predict reliably, unknown events. This function of accounting was
supposed to have been accomplished within the framework of the natural science model, where
the adoption of careful sampling, accurate measurement, and good design and analysis of theory-
supported hypothesis has been the focus. This single world-view methodology has however, met
objections and criticisms from various schools of thought concerning the restrictive sense in which
accounting research is conducted. For example, Chua (1986) observes that grounding mainstream
University of Ghana http://ugspace.ug.edu.gh

139
accounting in a common set of philosophical assumptions about knowledge, the empirical world
and the relationship between theory and practice has restricted the range of problems studied and
the use of research methods. Debates on the applicable methodologies in the field led to the
emergence of the three main paradigms-functionalist, interpretivists and critical
humanistic/structuralism. While the functionalist paradigm seeks to establish only laws thereby
employing only the methods and procedures that exact science permits, the understanding of some
particular event in society or in nature is endeavoured by the interpretivist sciences.
The functionalist approach is underpinned by the approach and methods used in the natural
sciences. It is pre-occupied with the construction of scientific tests and the analysis of data is
accomplished by means of quantitative methodology. Questionnaires of surveys, standardized
research instruments, and personality tests of all kinds are more pronounced among the tools that
comprise functionalist methodology. They also differ in terms of the mode of inquiry. Functionalist
inquiries from the outside whilst interpretivist inquiries from the inside. Based on these two
frameworks four paradigms in accounting research namely; the functionalist view, the interpretive
view, the radical humanist view and the radical structuralist view can be differentiated.
5.6. The Study’s Philosophical Stance
This study takes the critical realism, quantitative-positivist epistemology perspective in that, it
investigates the impacts of attributes of a phenomenon on another. This is achieved by using
empirical data, and based on a well-grounded theory (contingency theory) in accounting research
to test a priori, hypotheses and knowledge. Specifically, the study employs a hypothetico-
deductive approach to ascertain the relationship between SCM context factors, MAS design, and
University of Ghana http://ugspace.ug.edu.gh

140
supply chain performance in hospitals. The positivist assumption allowed the key factors in the
study to be measured precisely in order to verify or falsify predetermined hypotheses (Easterbay-
Smith et al, 2012). By reducing data to a parsimonious set of variables which are tightly controlled
through statistical analysis, measures or observations for testing a theory is developed (Creswell,
2014).
Following Creswell (2014), this is categorised into research purpose, the nature of reality
(ontology), the nature of knowledge as well as the relationship between the inquirer and the
inquired (epistemology), and the methodological approach. It uses a survey cross-section data
sampled from management accountants/financial controllers and heads of procurement units of
237 hospitals in Ghana to empirically examine the relationship among the constructs.
5.7. Purpose and Design Strategies of the Survey
In this study, the potential hypothesized dimensions of SCI (internal and external), level of
information sharing, and supply chain risk and uncertainty that influence MAS design and its
implementation in hospital SCM decisions to leverage performance is examined. Given that this
study aims at testing the contingency fit relationships in the inter-firm exchanges domain, the
design methodology followed that of a cross-sectional survey research which is employed for
explanations that state the influence of the SCM variables on the MAS variables and their
combined effect on hospital supply chain performance. The use of the cross-sectional survey for
explanations examines the associations between management accounting and other variables
which are guided by theoretical expectations (Pinsonneault & Kraemer, 1993; Sapsford, 1999). In
addition, the study seeks to find answers that relate to the opinions of hospital accountants on the
University of Ghana http://ugspace.ug.edu.gh

141
interaction effects of SCI and MAS design on hospital operational performance. Data for studies
of this nature is not available in secondary form hence, as it has been studied in prior literature
(Chenhall & Morris, 1986; Gerdin, 2005; Soobaroyen and Poorundersing, 2008; Hammad et al,
2013), a cross-sectional survey design was the only appropriate methodology. A cross-sectional
survey design as noted by Creswell (2014) provides a quantitative/calculative or numeric
description of attitudes, trends, or opinions of a population. Generalization or inferences drawn
from the population are normally derived from a study of a sample of the population under
consideration.
In this regard, the study used a cross-sectional design for testing these relationships under three
‘contingency fit’ models: selection, mediation and moderation. The hypotheses were tested under
these three contingency fit models because these models including the matching fit model (which
was not tested because of its underlying theoretical assumption not to be tested under structural
equations model) underpin contingency fit studies in management accounting research. In testing
the existence of contingency theory in the inter-firm exchanges domain, these models
appropriately explain the presence or non-presence of contingency fit relationships. They form the
various contingency fit models that are tested under contingency fit studies. Also, contingency fit
simply means the interaction of the MAS variables with other contextual variables to affect
performance (Chenhall & Chapman, 2006). These relationships were modelled using a
representative measure of activities and attributes for a cross-section of healthcare organizations
in Ghana. To obtain these measures, a quantitative survey methodology that involved Likert scales
for each of the three multidimensional constructs was designed to test the hypotheses specified in
the model. The research design proportionately represented healthcare institutions which consisted
of public and private hospitals. The design stage showed the ‘master plan’ or ‘blueprint’ of the
University of Ghana http://ugspace.ug.edu.gh

142
study which primarily, gave insights on how the study was to be conducted. In effect, all the major
parts of the research (e.g. population and sample, sampling strategy, data and measures, estimation
models and techniques, etc.) were integrated to address each of the research questions and
associated hypothesis. These were clearly spelt out in the study design. The data were generated
using a response scale questionnaire which was self-administered to management accountants and
other accounting personnel/managers of public and private hospitals across six out of the ten
regions. These include the Ashanti, Central, Western, Eastern, Brong-Ahafo and Greater Accra
regions.
The exclusion of the other four regions (Tamale, Upper East, Upper West, and Volta regions) from
the study is based on the fact that the research is based on the Northern, Middle and Southern
Zones where Ashanti and Brong-Ahafo regions represented the Northern Zone, the Eastern and
Central regions represented the Middle Zone and the Western and Greater Accra regions
represented the Southern Zone. The exclusion however, of the other four regions is an important
shortcoming given their economic significance in national development. Consequently, the extent
to which the research was valid to extrapolate the results to all other hospitals across the country
could be subjected to error which could be significant, but the units selected were significant to
mitigate the error significance due to their composition of large proportion of healthcare
institutions. The questionnaire items were based on an adapted version of existing measuring
instruments/scales used in prior studies; hence, consistency and reliability is assured. Using a
covariance-based structural equation modelling (CB-SEM), the hypotheses linking the paths of the
structural model were tested to determine the relationships among the constructs.
University of Ghana http://ugspace.ug.edu.gh
143
5.8 Survey Strategy
Determinism suggests that testing the association between and among variables is key to finding
answers to questions and drawing conclusions on hypotheses through experiments and surveys
(Creswell, 2014). The strategy adopted for this study comprised two main stages: the first stage
involved pertinent measures of SCM contextual factors, drivers and financial operation of SCM,
and the four dimensions of the MAS information and hospital supply chain performance from the
literature and drafted the measuring instrument. The second stage of the survey strategy involved
a preliminary testing of the instrument with 20 hospitals made up of 10 each of public and private
hospitals. This was carried out to enable a thorough revision of the instrument based on the
response from the pilot study. The outcome of the pilot survey showed that the accountants are
familiar and knowledgeable with the questionnaire items except one private hospital who
complained about the understanding of one item under external supplier relationships. This was
subsequently revised before administering to the respondents. Following Li et al (2006), the
method for instrument development was taken through four phases: 1) item generation, 2) pilot
study, 3) large-scale data collection, and 4) reliability and validity assessment of the measuring
scale. In phase four, rigorous statistical analysis was performed to ascertain the reliability and
validity of the constructs. The research framework together with the associated hypotheses was
tested using hierarchical factorial structures.
5.9. Population, Sample and Sampling Procedure
The definition of population and sample is critical in survey research because they constitute the
determinants of the possibility of drawing valid inferences from the sample characteristics (Van
de Stede, Young & Chen, 2005). It is also important because they form a central role in shaping
University of Ghana http://ugspace.ug.edu.gh

144
everyday opinion. The framework for a survey study requires that all relevant respondents are
included in the population and that unknowledgeable, inappropriate, or unconcerned respondents
are excluded (Federal Rules of Evidence, 1971). In addition, it emphasizes the consistency of target
population and survey population (Diamond, 2000). Whilst the target population consists of all
respondents that are under study, survey population refers to the collection of respondents
available to the researcher and which is actually sampled. This consistency is important because
the study is likely to offer results that are biased in situations where subjects not in the target
population are included in the survey population or subjects in the target population are omitted.
Guided by this framework, the study population was defined to include all healthcare institutions
in Ghana. These included hospitals (both public and private), polyclinics, pharmaceutical
manufacturers, wholesalers, and the distribution agencies of medical supplies. However, the focus
was on hospitals since they constitute the largest proportion of healthcare institutions across the
country and also the identified logistic and supply chain problems were found to be more
pronounced in hospitals. Out of this was the sampling frame which comprised the list of all
hospitals in Ghana. This approach differs from most studies in management accounting because
the luxury of obtaining a sample frame is often not a characteristic of survey researchers often (i.e.
a complete list of survey population elements that match the intended target population) and
ensuring that a probability sampling plan is developed. From the sample frame, the sample for the
study was drawn using cluster sampling. This approach was adopted because of the geographical
distribution of the sample units and to ensure that the sample is a representative of the entire
population, and also sample selection (or sampling) directly affects the generalizability of the
survey findings. The list of sampling frame was generated using the databases of the Ministry of
Health and the Ghana Health Service (GHS) respectively.
University of Ghana http://ugspace.ug.edu.gh
145
5.9.1. Study Sample
The sampling frame comprised the list of all healthcare institutions in Ghana. Given that there are
currently 1,409 (public and private) healthcare institutions in Ghana made up of 394 general
hospitals, 32 polyclinics, 982 clinics and 3 psychiatric hospitals (Facts and Figures, GHS, 2015),
the sample size of 274 hospital accountants was initially drawn across these organizations. The
key assumption underlying the method of analysis (covariance structures) is that the sample size
is large; hence, a large sample is required to satisfy the model’s assumptions. Taking into account
non-responses and other factors (e.g. less than 3 years tenure in office) a valid sample size of 237
that meets the model’s assumptions was obtained.
Using the list of healthcare institutions in the GHS database, sample sizes of 131 and 106 were
respectively drawn from the public and private sectors although equal sample sizes were expected
to have been drawn. However, since the study’s focus was not to investigate the differences or
contrasting the MAS-SCM relationships between public and private healthcare institutions, this
had no negative impact on the results. The objective is to provide preliminary empirical evidence
of contingency theory’s application in inter-firm exchanges in the SCM domain. In this regard,
unequal sample sizes will not be an issue of much concern and does not violate the assumptions
of the model being used. Moreover, the GHS (2015) estimates the number of hospital beds to be
11, 689 and 1,145 representing 58.7% and 5.8% for public and private hospitals respectively which
is a clear indication that equal sample sizes may be difficult to obtain..
5.9.2. Sampling Procedure
The sampling procedure followed that of probability sampling. The selection of probability
samples is based on the premise that every element of the survey population (sampling frame) has
University of Ghana http://ugspace.ug.edu.gh

146
a chance of known non-zero of being included in the sample. Also, as noted by Diamond (2000),
the representativeness of the survey results are increased if the scores of probability samples give
high response rates. This permits inferences to be ascertained from the sample to the survey
population within a calculable margin of error. The list of all healthcare institutions (hospitals,
polyclinics, clinics) on regional, district and town basis is available at the GHS database. The
cluster sampling technique was used to draw the required sample for the study by independently
selecting a random sample from the population. The study population was divided into six clusters
comprising the selected six regions (Greater Accra, Eastern, Central, Western, Ashanti, and Brong-
Ahafo) regions followed by a simple random sample drawn from each cluster. The population
dimensions included size, location, ownership, and profit status of each hospital as well as the
profile of respondents. The sampling is clustered on regional basis and does not include details of
districts. The reason is that narrowing the sampling methodology to the 216 districts in Ghana will
be problematic because unlike the regional level where each region has hospitals and clinics, the
same cannot be found at the district level. Some districts do not have hospitals and the available
clinics are for first aid only and are not included in the list in the GHS database.
5.9.3. Sample Size
Literature so far documented has not indicated any standard sample size for a research of this kind.
However, recommendations in most textbooks about sampling offer standard treatment of sample
size by determining the required precision (i.e. confidence interval) which requires an estimate of
both the sample variance and an estimate of the expected response rate. Using the formula of
2)(1 eN
Nn
(Hoyle, 2015), with a 5 percent significance level with maximum permissible error,
e value of 0.05, the final sample units for the study were obtained. (Note: n = sample size; N =
University of Ghana http://ugspace.ug.edu.gh

147
total population of hospitals and e = the level of precision). Out of the 300 questionnaires that were
distributed, 274 responded representing a response rate of 90.13%. However, 37 of the responded
questionnaires (especially those that were sent by post from the regions) were either not completed,
lacked certain information such as number of hospital beds, or the respondent has occupied his/her
position for less than three years and so were excluded from the sample resulting in 237 valid
sample units representing 79% response rate. This approach is consistent with Maiga et al (2013),
Chen et al (2013) and Macinati and Anessi-Pessina (2014). A breakdown of the samples from the
six regions is shown in Table 5.5.
Table 5.5: Distribution of Samples by the Six Regions
Region Population Sample Responses Received
Gt. Accra 367 191 74 Ashanti 235 148 57 Eastern 142 104 40 Central 94 76 32 Western 182 125 37 Brong-Ahafo 132 99 34 Total 743 274
(Source: Sample Survey, 2017)
5.10. Approach to Data Collection
A scale-response questionnaire with a covering letter (see Appendix 1) that explains the
purpose/objectives of the study as well as providing assurance of anonymity of responses, was
distributed personally (with some assistance from some colleagues in the regions) to accountants,
managers, administrators, and departmental heads of hospitals. To address some of the challenges
encountered in the questionnaire administration by commuting on multiple occasions from one
hospital to another to follow-up on the completed questionnaire, a self-addressed envelope was
University of Ghana http://ugspace.ug.edu.gh

148
attached to the questionnaire for especially respondents within the regions, However, for a
responded questionnaire to be included in the sample, the respondent should have held his/her
position for a minimum of three years. This was necessary to reduce errors in the responses. Prior
to the actual data collection, a pilot study involving 20 hospitals (10 public and 10 private) was
conducted within the Greater Accra Metropolis to develop and validate the questionnaire.
5.11. Scale Development and Measurements
Typically, a measurement scale is employed when the constructs involved in a study have no direct
observable measures. In this regard, the unobservable constructs and their dimensions were
measured indirectly through measurement scales of several items (or questions) in which
participants’ responses to the measurement scale questions (or items) determine the measured
value for each construct. The scales (or instruments) used in this study consisted of those developed
and used in prior literature and hence not only ensure consistency but also the reliability and
validity of the measures are guaranteed.
To initiate the scale development process, the guidelines of Jarvis, MacKenzie and Podsakoff
(2003) as well as Bisbe, Batista-Foguet and Chenhall (2007) on reflective and formative constructs
which have been used in many management accounting literatures (e.g. Fayard et al, 2012; Dekker
et al, 2013) was followed. Whether each of the modelled constructs is conceptually reflective or
formative was initially ascertained using the guidelines. For a reflective construct, participants’
responses are assumed to reflect the conditions of the latent construct. In this case changes in the
responses are caused by changes in the constructs. On the other hand, a linear combination of
participants’ responses on a given scale type of modelling reflect formative constructs. Based on
University of Ghana http://ugspace.ug.edu.gh

149
these guidelines, a reflective measurement model in which the manifest item values are considered
to be a function of underlying latent construct value was specified for all the constructs before
administering to respondents.
5.12. Constructs and their Sources
The constructs and their literature sources are shown in Table 5.6. MAS is a multidimensional
construct consisting of four dimensions: scope, timeliness, integration, and aggregation. These
four dimensions were initially conceptualized by Chenhall and Morris (1986) and subsequently
used by Soobaroyen and Poorundersing (2008) to examine the contingency fit relationships. It has
also been used by Hammad et al (2013) and Macinati and Asseni-Pessina (2014) to examine
contingency fit relationships in the Egyptian and the US hospitals respectively. The construct SCI,
level of information sharing and supply chain risk and uncertainty as well as supply chain
performance have been used by Chen et al (2013), Ataseven and Nail (2017), Flynn et al (2010)
and Wong et al (2011).
University of Ghana http://ugspace.ug.edu.gh

150
Table 5.6: Constructs and their Sources of Measures
Construct No.
of
Items
Literature Evidence
Strategic supplier partnership 10 (Li et al, 2006; Chen et al, 2013; Behesti et al, 2014; Ataseven &
Nair, 2017)
Level of information shearing 12 (Mahama, 2006; Dekker et al, 2013; Chen et al, 2013; Behesti et
al, 2014; Ataseven & Nair, 2017).
Supply chain integration 8 (Behesti et al, 2014; Wiengarten, Humphreys, Gimenez &
Mclvor 2016; Ataseven & Nair, 2017)
Supply chain risk and uncertainty 8 Anderson and Dekker (2005), Mahama (2006), Dekker,
Sakaguchi & Kawai (2013), Li, Fan, Lee & Cheng (2015)
Size (Hammad et al, 2013; Macinati and Anessi-Pessina, 2014)
Broad scope of MAS information 5 (Chenhall & Morris,1986; Bouwens, & Abernethy, 2000;
Abernethy & Lillis (1995; Soobaroyen & Poorundersing, 2008;
Hammad et al, 2013; Macinati & Anessi-Pessina, 2014)
Timeliness of MAS information 4 (Chenhall & Morris, 1986; Bouwens & Abernethy (2000),
Abernethy & Lillis, 1995; Hammad et al, 2013; Macinati &
Anessi-Pessina, 2014)
Integration of MAS information 4 (Chenhall &Morris, 1986; Bouwens, & Abernethy, (2000;
Abernethy & Lillis, 1995; Soobaroyen & Poorundersing, 2008;
Hammad et al, 2013; Macinati & Anessi-Pessina, 2014)
Aggregation of MAS information 7 (Chenhall & Morris, 1986; Bouwens, & Abernethy, 2000;
Abernethy &Lillis (1995), Hammad et al (2013; Macinati &
Anessi-Pessina, 2014)
Supply chain cost effectiveness 9 (Li et al, 2006; Ou et al, 2010; Chen et al, 2013; Ataseven & Nair,
2017)
Asset utilization 4 (Ou, et al, 2010; Chen et al, 2013; Behesti et al, 2014; Ataseven
& Nair, 2017)
Supply chain reliability and speed
of delivery
7 (Ou et al, 2010; Chen et al, 2013; Behesti et al, 2014; Ataseven
& Nair, 2017)
Supply chain flexibility 3 (Li et al, 2006; Ou et al, 2010; Chen et al, 2013; Behesti et al,
2014; Ataseven & Nair, 2017)
University of Ghana http://ugspace.ug.edu.gh

151
5.13. The Modelling Process
The modelling process involved a second-order covariance based structural equation modelling
(SEM) because the underlying theory of each of the three constructs suggests that they are
accounted for by sub-multiple lower-order (or first-order) constructs. In this regard, a higher-order
of abstraction was found to be the suitable modelling approach. To this end, the three main
variables: management accounting systems, supply chain management, and hospital supply chain
performance which are second-order level of abstraction were conceptualized as composites of
four dimensions each comprising first-order levels of abstraction. The second-order model was
posited to link the manifest variables to their respective first-order latent variables which were in
turn linked to their second-order variables.
The justification for using structural equations modelling (SEM) and more specifically covariance
based (CB-SEM) is that first, the variables are latent in nature and also has multiple relationships.
That is the analysis requires a single estimate of the variables simultaneously which can be
appropriately been executed using SEM compared to other multivariate models. Second, the study
intends to test or confirm a theory in the inter-firm exchanges domain hence partial least squares
(PLS-SEM) would not be the appropriate tool since it is a non-parametric based SEM compared
to CB-SEM which confirms a theory. Third, the constructs are reflective and CB-SEM analyses
only reflective form of constructs compared to PLS-SEM which analyses both formative and
reflective form of constructs.
The initial part of the modelling process begun with the confirmatory factor analytic structure to
ascertain the reliability and validity of the regression weights; that is the strengths of the regression
paths linking the factors and the indicator variables (factor loadings). Following prior studies (Tan,
2001; Maiga et al, 2013) the two-stage model-building process where testing of the measurement
University of Ghana http://ugspace.ug.edu.gh
152
model precedes that of the structural model was adopted for this study. This is normally done to
avoid possible interactions between the structural and measurement models. In addition, since the
structural portion consists of latent variables and specification of their relations, the extent of their
validity and attainment of psychometric soundness of each construct is critical. The measurement
model specifies how hypothetical constructs are measured in terms of observed variables while the
structural model depicts the hypothesized relationships between latent constructs. From a general
perspective, factor analysis involves the assessment of the covariation among a set of manifest
variables so that information on their underlying latent constructs can be gathered. It explains the
extent to which the manifest variables are linked to their underlying latent constructs. In this
regard, testing for the measurement model prior to evaluating the structural model is an important
preliminary step in analyzing a full SEM.
5.14. Summary of Analysis Procedure
The focal point of analysis of data was hypotheses testing to confirm or reject contingency theory
in the inter-firm exchanges domain. The SEM was therefore employed to test all hypotheses and
simultaneously control for confounding variables. Based on some studies. Table 5.7 shows a
summary of all data analysis steps taken and their respective rationale.
University of Ghana http://ugspace.ug.edu.gh

153
Table 5.7: Summary of Analysis Procedure Analysis
procedure
Stage (of the
analysis) Description Statistical tool Rationale
Data coding Stage 1 All data were assigned a code
Data coding
sheets and SPSS
This step was necessary for avoiding the data of
error items
Data
screening Stage 2
Data was explored to remove
unwanted items and outliers. Descriptive
statistics
This could visualise missing items and potential
unwanted items. Mean scores and standard
deviation give clues about the presence of outliers
The distribution of the data was
examined to establish acceptable
skewness Z-score
This was used because it provides benchmarks for
understanding the distribution of the data
Normality
test Stage 2
Univariate normality of data was
verified and confirmed
Shapiro-Wilk's
test
Shapiro-Wilk's is the most appropriate tool when
the number of data points (n) is not more than
Byrne, 2010)
Multivariate normality of data was
verified and confirmed
Mahalanobis
test
This is a gold standard provided in CFA (Byrne,
2010)
Assumptions
test Stage 2
To ensure that the data came from
a normally distributed population.
Shapiro-Wilk's
test,
Mahalanobis
test Recommended in the literature (Byrne, 2010)
To verify whether error terms of
all predictors are independent of
each other
Durbin-Watson
statistic
Recommended in the literature (Burkert et al,
2014)
To verify homoscedasticity
Variance
Inflation Factor
value
Recommended in the literature (Maiga et al,
2013)
Scale
validation Stage 2
To compute the reliability and
validity statistics of the
measurement scales CFA
This approach is the most robust way to estimate
both the reliability and validity statistics
(Macinati & Asseni-Pessina, 2014)
Hypotheses
testing Stage 3
To test structural CFA model or
the 23 hypotheses of the study,
including the control of
confounding variables and
moderation test CFA
This approach is the most robust way to test
structural hypotheses or models to minimise Type
II error (Maiga et al, 2013)
Source: Researcher’s own construct
University of Ghana http://ugspace.ug.edu.gh
154
6.15. Chapter Summary
In this chapter, the general approach or methodology adopted in testing the contingency fit
hypotheses among the variables has been presented. The statistical tests involved the selection,
mediation and moderation forms of fit. It initially showed the researcher’s philosophical stance
based on which the entire research design was planned. The chapter showed that the research
design is a cross section survey methodology involving management accountants, procurement
officers and hospital managers/administrators in Ghana. The survey strategy, population,
sample size, instruments development and measurement scales, and the method of data
collection have been described.
The chapter also elaborated on the statistical techniques adopted to estimating the variables
involved in the study which was based mainly on the analysis of covariance structures. Under
that section, the modelling process which involved a two-stage second-order covariance-based
structural equations modelling was given a detailed description. Testing of the measurement
CFA model (factor analytic model) and the structural model (path coefficients) have been duly
explained.
University of Ghana http://ugspace.ug.edu.gh

155
CHAPTER SIX
SURVEY ANALYSIS AND RESULTS
6.1 Introduction
The previous chapter outlined the approach to gathering the survey data and how such data
were analyzed to test the research hypotheses and subsequent realization of the study
objectives. In this chapter, the results and findings associated with analysis of the sample data
are presented. It presents the results related to the fit between the test variables, and their joint
impact on performance. It also presents empirical evidence of the management accounting
construct as a mediator between the antecedent conditions of SCM and hospital supply chain
performance. Finally, it presents results of the moderating effect of the contingency variables
(SCM contextual antecedents) on the link between management accounting and hospital supply
chain performance. The analysis is categorized into three sections. The first section details the
preliminary analysis which captures the models underlying assumptions; i.e. reliability and
validity measures (internal consistency, composite reliability, average variance extracted,
(AVE)) of the survey instrument and related items, tests of normality and outliers of the sample
data as well as descriptive measures of the test variables. The second section presents the first
part of the covariance structural equation modelling which involves model specification and
evaluation of the measurement part of the hypothesized model. It also provides evidence on
the extent to which the measurement model adequately fits the sample data. The third section
presents findings related to the modelling and testing of the structural paths linking the latent
variables specified in the model.
University of Ghana http://ugspace.ug.edu.gh
156
6.2 Preliminary Analysis of the Sample Data
Although the three main constructs (supply chain context factors, management accounting
design, and supply chain performance) that form this study were theoretically developed and
based on items proposed and validated in prior studies, an assessment of the sample distribution
to establish that it originated from a normally distributed population is highly important as the
research findings are seriously affected by the credibility (or validity) of the scale items. This
section presents the preliminary findings from tests of normality for the sample data as well as
reliability and validity of the scale items. The section comprises two subsections – the first
subsection presents a summary of hospital characteristics or features represented by size
(measured by the natural log of number of beds), location (urban or rural measures as
dichotomy variable taking the value of 1 if located in an urban center and 0 otherwise),
ownership (public or private measured as a categorical variable taking the value of 1 if
government owned and 0 otherwise) and the qualifications of respondents (must have held
his/her current post for at least 3 years).
The test originally involved 72 items in all for the six factors (or constructs): 9 for strategic
supplier partnership (SSP), 7 for level of information sharing (LIS), 8 for supply chain risk and
uncertainty (SCR), 6 for supply chain integration, 20 for management accounting system
(MAS) made up of 5 accounting information scope (AIS), 4 timeliness (AIT), 4 integration
(AII), 7 aggregation (AIA), and 16 for supply chain performance (SCP) also consisting of 6
supply chain cost effectiveness (SCE), 4 utilization of hospital assets (UHA), 3 supply chain
quality (SCQ), and 3 supply chain flexibility (SCF). However, during the initial analysis, it was
discovered that some items either recorded very low loading (< 0.20) or failed to load and so
were deleted. The resulting data gave 55 items in all: 6 items for SSP, 6 for LIS, 5 for SCR, 6
for SCI, 4 each for AIS, AIA, AIT, and AII, 6 for SCE, 4 for UHA, and 3 each for SCF and
SCQ.
University of Ghana http://ugspace.ug.edu.gh

157
It also evaluates the distribution of the sample data for normality and whether outliers are in
the dataset. More specifically, it assesses the sample data for multivariate normality criterion
and kurtotic conditions which is critical for the analysis of covariance based structures. Given
that structural equation modelling is based on the analysis of covariance structures, tests of
variances and covariance are severely affected by kurtosis compared to skewness (DeCarlo,
1997). As a consequence, the presence of kurtosis, and more importantly multivariate kurtosis
in the dataset is always a concern as it is widely known to be exceptionally detrimental to the
analysis of structural models.
Multivariate kurtosis normally refers to the situation where there are both tails and peaks of the
multivariate distribution of the manifest variables that differ significantly from those of
multivariate normal distribution, and is categorized into multivariate positive kurtosis and
multivariate negative kurtosis. The former exhibits peakeness as well as bold or thick tails in
the distribution while the latter exhibits flat distributions with light tails. In the second
subsection, results of series of tests related to basic fundamental assumptions underlying
multivariate analysis as well as tests for reliability and validity of the measuring instrument are
presented. More precisely Cronbach Alpha (CA) test for reliability, Composite Reliability (CR)
test for internal consistency, Average Variance Extracted (AVE), and Intra-Class Correlations
(ICC) are given.
6.3 Sample Characteristics
Table 6.1 presents the respondents’ characteristics as well as the organizations’ background.
The frequency distribution for the sample hospitals in terms of ownership, profit status, and
location which were categorically measured are presented. The results as reported in Table 6.1
indicate that the sample composition has the larger representation of government hospitals 131
University of Ghana http://ugspace.ug.edu.gh

158
(55.3%) (i.e. are owned by the government) while 106 (44.7%) are represented by
individuals, corporate organizations, religious bodies, and NGOs.
These results suggest that although healthcare delivery is largely controlled by government, an
appreciable number of private entities are involved in this business. Hence their operations can
have significant impact on the health supply chain especially the procurement and distribution
of health products. With regards to the profit status question, only privately-owned hospitals
answered as government hospitals are known to be non-profit oriented. As low as 7.5%
represented by mainly religious bodies are non-profit which further suggests the impact the
private sector healthcare organizations can have on the supply chain. Finally, close to 70% of
the sampled hospitals are located within urban centres. This suggests that costs associated with
transportation and distribution of medical products between suppliers and hospitals (a key
obligation of the MAS function) can be efficiently controlled at lower levels since a large
proportion of pharmaceutical companies (one of the key players in the health supply chain) are
located within urban centers.
Table 6.1: Distribution of Hospitals in Terms of Ownership, Profit Status and Location
(N) Frequency (%)
Ownership 237
Public 131 55.3
Private 106 44.7
Profit Status 106
Profit 98 92.5
Non-profit 8 7.5
Location 237
Urban 165 69.6
Rural 72 30.4
(Source: Author’s computations from Field Survey, 2017)
University of Ghana http://ugspace.ug.edu.gh
159
As these three variables play a significant role in the functioning of healthcare institutions, they
can indirectly influence performance of the hospital SC (Chen et al, 2013) and are thus
controlled for their confounding effects (discussed in subsequent sections). The descriptive
statistics for the scale items is discussed next. However, because hospital size (measured by
the natural log of number of hospital beds) and tenure of respondents (number of years
occupying present position) are continuous variables, they are included in Table 6.2 and are
presented first. The results show that an average number of log 1.70 representing 50 beds are
owned by the sampled hospitals.
Like the other three control variables, hospital size largely influences its supply chain
especially in the area of stock control and inventory management which has serious
implications for management accounting information and hence controlled as well.
Considering the number of years at present position, the results indicate that on average,
respondents have occupied their present positions for 5.7 years. This suggests that the
respondents are not only knowledgeable and experienced in their respective positions, but also
can be provide reliable perceptions based on their access to information. Based on these
findings, the respondents (who were mainly accountants of the sampled hospitals) meet the
requirements to provide the needed information.
6.4 Assessment of Data for Normality
Table 6.2 presents the descriptive statistics concerning means, standard deviations, and kurtosis
of the sample data which are continuous in nature. Raykov and Marcoulides (2000) have noted
that of particularly problematic to the analysis of CB-SEM are data that exhibit multivariate
kurtotic features. In this regard, the results for both univariate kurtosis and their critical ratios
(i.e. z-scores) and multivariate kurtosis assessment of the dataset for all the 55 items are
University of Ghana http://ugspace.ug.edu.gh

160
presented. A review of Table 6.2 indicates that positive values of kurtosis range from 0.046 to
1.090 and negative kurtosis values range from -0.116 to -1.018 which gives an overall average
univariate kurtosis value of 3.466. A normally distributed kurtosis under standardized
conditions has a value of 3 as the kurtosis index (𝛽) where higher values of 𝛽 signifies positive
kurtosis and lower values connotes negative kurtosis.
However, because this value is rescaled to zero in most computer programmes, the index 𝛽
takes the zero value as indicator of normality. Although a positive kurtosis or negative kurtosis
is signaled by the 𝛽 sign, Kline (2005) notes that consensus on the size of the nonzero values
based on which conclusions regarding the presence of extreme kurtosis has still not been
reached. Despite this assertion, West, Finch and Curran (1995) maintain that rescaled 𝛽 values
outside the range 0 ≤ 𝛽 ≤ 7 is an indication of departure from normality. A review of Table
6.2 and following West et al (1995) the items showed no substantial kurtotic values in the
dataset.
In the case of multivariate kurtosis index, the critical ratio value representing Mardia’s (1970)
normalized estimate of multivariate kurtosis was used. In situations where a large sample size
exhibits multivariate normality, a distribution of this index as a unit normal variate takes place
so that significant positive and negative kurtosis are reflected in large positive and negative
values respectively. It has been suggested that data that are non-normally distributed exhibit
normalized estimate of multivariate kurtosis values greater than 5 (Bentler, 2005). In Table 6.2,
the index of multivariate kurtosis and the corresponding critical ratios appear at the bottom of
the z-score and kurtosis columns have values of 4.521 and 3.466 respectively. Following
Bentler (2005) the z-statistic of 4.521 is highly suggestive of normality in the sample. On the
basis of these findings, the next stage of the preliminary analysis which involved checking for
outliers in the dataset are addressed.
University of Ghana http://ugspace.ug.edu.gh
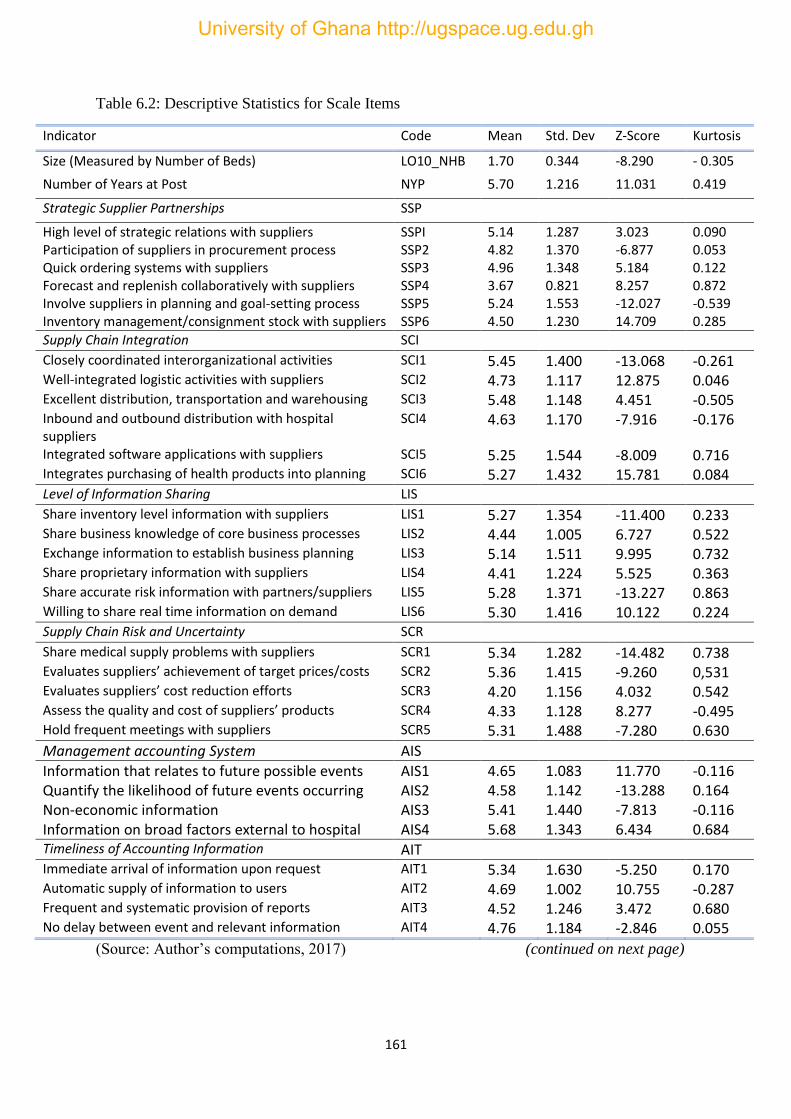
161
Table 6.2: Descriptive Statistics for Scale Items
Indicator Code Mean Std. Dev Z-Score Kurtosis
Size (Measured by Number of Beds) LO10_NHB 1.70 0.344 -8.290 - 0.305
Number of Years at Post NYP 5.70 1.216 11.031 0.419
Strategic Supplier Partnerships SSP
High level of strategic relations with suppliers SSPI 5.14 1.287 3.023 0.090 Participation of suppliers in procurement process SSP2 4.82 1.370 -6.877 0.053 Quick ordering systems with suppliers SSP3 4.96 1.348 5.184 0.122 Forecast and replenish collaboratively with suppliers SSP4 3.67 0.821 8.257 0.872 Involve suppliers in planning and goal-setting process SSP5 5.24 1.553 -12.027 -0.539 Inventory management/consignment stock with suppliers SSP6 4.50 1.230 14.709 0.285
Supply Chain Integration SCI Closely coordinated interorganizational activities SCI1 5.45 1.400 -13.068 -0.261 Well-integrated logistic activities with suppliers SCI2 4.73 1.117 12.875 0.046 Excellent distribution, transportation and warehousing SCI3 5.48 1.148 4.451 -0.505 Inbound and outbound distribution with hospital suppliers
SCI4 4.63 1.170 -7.916 -0.176
Integrated software applications with suppliers SCI5 5.25 1.544 -8.009 0.716 Integrates purchasing of health products into planning SCI6 5.27 1.432 15.781 0.084 Level of Information Sharing LIS Share inventory level information with suppliers LIS1 5.27 1.354 -11.400 0.233 Share business knowledge of core business processes LIS2 4.44 1.005 6.727 0.522 Exchange information to establish business planning LIS3 5.14 1.511 9.995 0.732 Share proprietary information with suppliers LIS4 4.41 1.224 5.525 0.363 Share accurate risk information with partners/suppliers LIS5 5.28 1.371 -13.227 0.863 Willing to share real time information on demand LIS6 5.30 1.416 10.122 0.224 Supply Chain Risk and Uncertainty SCR Share medical supply problems with suppliers SCR1 5.34 1.282 -14.482 0.738 Evaluates suppliers’ achievement of target prices/costs SCR2 5.36 1.415 -9.260 0,531 Evaluates suppliers’ cost reduction efforts SCR3 4.20 1.156 4.032 0.542 Assess the quality and cost of suppliers’ products SCR4 4.33 1.128 8.277 -0.495 Hold frequent meetings with suppliers SCR5 5.31 1.488 -7.280 0.630
Management accounting System AIS
Information that relates to future possible events AIS1 4.65 1.083 11.770 -0.116 Quantify the likelihood of future events occurring AIS2 4.58 1.142 -13.288 0.164 Non-economic information AIS3 5.41 1.440 -7.813 -0.116 Information on broad factors external to hospital AIS4 5.68 1.343 6.434 0.684 Timeliness of Accounting Information AIT Immediate arrival of information upon request AIT1 5.34 1.630 -5.250 0.170 Automatic supply of information to users AIT2 4.69 1.002 10.755 -0.287 Frequent and systematic provision of reports AIT3 4.52 1.246 3.472 0.680 No delay between event and relevant information AIT4 4.76 1.184 -2.846 0.055
(Source: Author’s computations, 2017) (continued on next page)
University of Ghana http://ugspace.ug.edu.gh

162
Table 6.2: Descriptive Statistics for Scale Items - Continued
Indicator Code Mean Std Dev Z-Score Kurtosis
Accounting Information Integration AII
Impact of information on individual decisions AII1 4.66 1.389 6.388 0.135 Influence of individual’s decision on responsibility AII2 4.72 1.182 -11.632 -0.417 Information on precise targets for all activities AII3 4.85 1.100 6.921 0.301 Impact of information on decisions on performance AII4 4.82 1.644 4.581 -1.018
Accounting Information Aggregation AIA
Information on functional areas in your hospital AIA1 5.00 1.451 -7.370 -0.333 Information on the effect of events on time periods AIA2 4.37 1.126 12.027 0.311 Processed information to influence different events AIA3 4.47 1.136 9.027 0,241 Information on summary reports for the hospital AIA4 5,45 1.363 -14.142 0.655
Supply Chain Cost Effectiveness SCE
Cost of order fulfillment reducing over the last 3 yrs SCE1 5.11 1.546 -8.072 0.936 Reduction in order fulfillment cost has improved SCE2 4.38 1.493 -9.981 0.873 Cost of order fulfillment is cost efficient SCE3 4.36 1.616 -10.976 0.474 Purchasing costs have reduced over the past 3 years SCE4 4.82 1.595 15.628 0.433 Operating costs have reduced over the past 3 years SCE5 5.05 1.490 -11.297 -0.845 Inventory costs have reduced over the past 3 years SCE6 4.92 1.261 13.158 -0.377
Utilization of Hospital Assets UHA
Growth rate in internally generated funds over 3 yrs UHA1 5.28 1.499 8.155 0.985 Growth rate in return on assets over last 3 years UHA2 5.22 1.647 -5.216 0.972 Growth rate in return on investments over 3 years UHA3 5.05 1.762 -7.046 0.302 Growth rate profit/accumulated fund over the last 3 years
UHA4 4.35 1.968 5.329 0.241
Supply Chain Flexibility SCF Flexibility of order fulfillment process getting better SCF1 5.30 1.572 -8.072 0.698 Improvement in the order fulfillment process SCF2 5.31 1.558 9.978 -0.507 Improvement in the cycle time of ordering process SCF3 4.30 1.488 13.003 0.748 Supply Chain Quality SCQ
Quality of order fulfillment process getting better SCQ1 5.27 1.517 -9.634 -.0222 Improvement in the order fulfillment process SCQ2 5.41 1.567 4.201 1.090 On-time delivery of medical suppliers from supplier SCQ3 5.33 1,598 -8.123 0.879 Multivariate 4.521 3.466
(Source: Author’s computations, 2017)
6.4.1 Assessing Data for Multivariate Outliers
To detect outliers in the sample, the squared values of the Mahalanobis distance (𝑑2) for each
observation was computed. This statistic measures the distance in standard deviation units
between a set of scores for the sample means for all the variables (centroids) and one
observation. In a particular dataset, outliers exhibit cases of scores that differ substantially from
all the others such that an extreme score in a variable is attributed to univariate outliers while
University of Ghana http://ugspace.ug.edu.gh

163
that of multivariate outliers manifest extreme scores on two or more variables. Using the
Mahalanobis distance approach (Byrne, 2010), a typical outlying case will exhibit a 𝑑2 value
that stands distinctively apart from all the other 𝑑2 values. After reviewing the values produced
by the sample data revealed that serious multivariate outliers that could distort subsequent
analysis is minimal. Also, the 𝑝2 values for all the variables range from 0.000 to 0.001 < 0.05
confirming the absence of outliers in the dataset. Next, is the test for reliability and validity of
scale items.
6.4.2 Correlation Analysis
A review of the standardized estimates for the constructs revealed the highest correlation value
of 0.57 indicating the absence of multicollinearity among the variables. However, their
statistical significance indicates strong relations among the constructs which in contingency
theory applications measures the strength rather than form of relationship among variables. The
presence of multicollinearity signifies that the correlation between two or more variables is so
high that essentially, they are represented by the same underlying construct. In this case, the
presence of a correlation of value close to 1 or more is indicative of inadmissible solution which
is a signal of model misspecification. This situation was however not found in the correlation
matrix produced in Table 6.3.
University of Ghana http://ugspace.ug.edu.gh
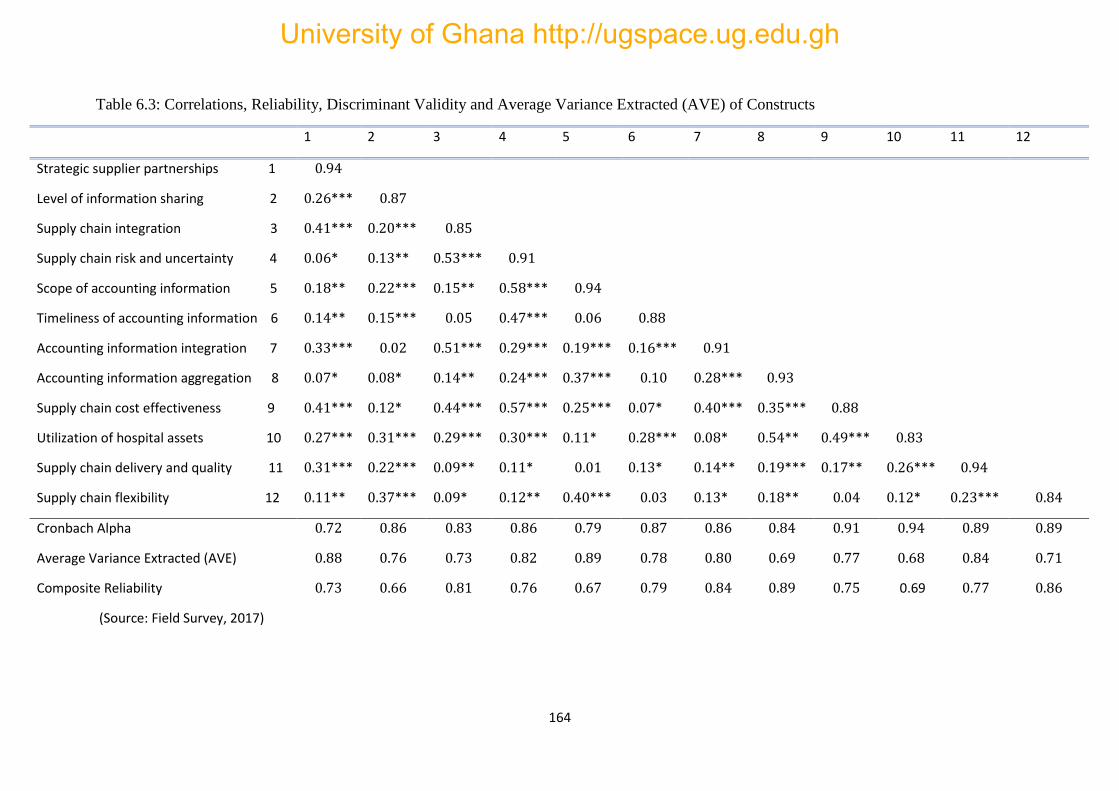
164
Table 6.3: Correlations, Reliability, Discriminant Validity and Average Variance Extracted (AVE) of Constructs
1 2 3 4 5 6 7 8 9 10 11 12
Strategic supplier partnerships 1 0.94
Level of information sharing 2 0.26*** 0.87
Supply chain integration 3 0.41*** 0.20*** 0.85
Supply chain risk and uncertainty 4 0.06* 0.13** 0.53*** 0.91
Scope of accounting information 5 0.18** 0.22*** 0.15** 0.58*** 0.94
Timeliness of accounting information 6 0.14** 0.15*** 0.05 0.47*** 0.06 0.88
Accounting information integration 7 0.33*** 0.02 0.51*** 0.29*** 0.19*** 0.16*** 0.91
Accounting information aggregation 8 0.07* 0.08* 0.14** 0.24*** 0.37*** 0.10 0.28*** 0.93
Supply chain cost effectiveness 9 0.41*** 0.12* 0.44*** 0.57*** 0.25*** 0.07* 0.40*** 0.35*** 0.88
Utilization of hospital assets 10 0.27*** 0.31*** 0.29*** 0.30*** 0.11* 0.28*** 0.08* 0.54** 0.49*** 0.83
Supply chain delivery and quality 11 0.31*** 0.22*** 0.09** 0.11* 0.01 0.13* 0.14** 0.19*** 0.17** 0.26*** 0.94
Supply chain flexibility 12 0.11** 0.37*** 0.09* 0.12** 0.40*** 0.03 0.13* 0.18** 0.04 0.12* 0.23*** 0.84
Cronbach Alpha 0.72 0.86 0.83 0.86 0.79 0.87 0.86 0.84 0.91 0.94 0.89 0.89
Average Variance Extracted (AVE) 0.88 0.76 0.73 0.82 0.89 0.78 0.80 0.69 0.77 0.68 0.84 0.71
Composite Reliability 0.73 0.66 0.81 0.76 0.67 0.79 0.84 0.89 0.75 0.69 0.77 0.86
(Source: Field Survey, 2017)
University of Ghana http://ugspace.ug.edu.gh
165
6.5 Measures of Reliability and Validity of Scale Items
The nomological validity of the research model is established using confirmatory factor
analysis (CFA) to analyze the survey data. In this regard, an assessment of the psychometrical
properties of the scales involved an evaluation of factor loadings, internal consistency, and
discriminant validity. To be consistent with prior studies, the reliability and validity of the
measures which comprised the measurement model (CFA model) were initially evaluated
followed by an evaluation of the structural model to assess strengths of the hypothesized links
among the latent variables.
It should be noted here that each of the three constructs namely, SCM context factors, MAS
design, and hospital supply chain performance are multidimensional in nature. Hence, a
second-order model-fitting approach was used to run the CFA for each of the aforementioned
constructs based on the a priori hypothesis that the other lower-order (first-order) factors
account for the higher-order (second-order) constructs. In other words, the second-order
construct accounts for all the variances and covariance associated with the first-order
constructs. Fig 6.1(a), 6.1(b), 6.1(c) show respectively, the final output of the second-order
factor analytic models for the SCM, MAS, and SCP constructs respectively. Each second-order
factor has four first-order factors.
University of Ghana http://ugspace.ug.edu.gh

166
Fig 6.1(a): Graphical Output of Factor Analytic Model for SCM Context Factors
(Source: Author’s own modelling based on Chen et al, 2013)
Note: SCM = supply chain management context factors; SSP = strategic supplier partnership; SCI = supply chain
integration; LIS = level of information sharing; SCR = supply chain risk and uncertainty
Fig 6.1(b): Graphical Output of Factor Analytic Model for MAS Information Dimensions
(Source: Author’s own modelling based on Chenhall & Morris, 1986)
Note: MAS = management accounting design; AIS = accounting information scope; AIT = accounting
information timeliness; AII= accounting information integration; AIA = accounting information aggregation
University of Ghana http://ugspace.ug.edu.gh

167
Fig 6.1(c): Graphical Output of Factor Analytic Model for SCP Dimensions
(Source: Author’s own modelling based on Chen et al, 2013)
6.1(d) Graphical Output for Combined Factor Analytic Models
University of Ghana http://ugspace.ug.edu.gh

168
The summary statistics for the scale items as presented in Tables 6.4 and 6.5 indicate that the
postulated CFA model was not supported by various fit indices at the initial stages. Evidence
of convergent as well as discriminant validity is provided by these fit indices for the three factor
analytic models along with the t-values in Table 6.4. However, the initial fit statistics of the
measurement model proved to be relatively not well-fitting between the hypothesized CFA
model and the sample data with CFI = 0.805 versus RMSEA = 0.096 for Model 1 of the SCM
construct; CFI = 0.834 versus RMSEA = 0.094 for Model 1 of the MAS construct; and CFI =
0844 versus RMSEA = 0.090, for Model 1 of the SCP construct, which fall outside the
recommended range of acceptability (< 0.05 to 0.08 ) for the RMSEA value in particular. A
review of the Modification Indices (MI) provided by the AMOS Output revealed some
evidence of misfit in all the three factor analytic models. It was discovered that if some
parameters are allowed to be estimated freely, the 𝑋2 values associated with each of the three
models will reduce considerably thereby improving the goodness-of-fit measures.
Subsequently, a post hoc analysis was initiated to improve upon the three models and this
resulted in three modifications and re-specifications of the original models. A re-specification
of Model 1 resulted in Model 2 for each construct. Further modifications resulted in Model 3
after which no further modification was possible. The next two subsections present the post
hoc analysis of the factor analytic models.
University of Ghana http://ugspace.ug.edu.gh

169
Table 6.4: Factor Loadings of Scale Items
Indicator Code Standardized Regression Weights
t-value
Strategic Supplier Partnerships SSP 0.914 12.035
High level of strategic relations with suppliers SSPI 0.725 3.288 Participation of suppliers in procurement process SSP2 0.759 6.808 Quick ordering systems with suppliers SSP3 0.719 6.188 Forecast and replenish collaboratively with suppliers SSP4 0.650 7.512 Involve suppliers in planning and goal-setting process SSP5 0.771 11.761 Inventory management/consignment stock with suppliers SSP6 0.789 Fixed
Supply Chain Integration SCI 0.947 12.760 Closely coordinated inter-organizational activities SCI1 0.761 Fixed Well-integrated logistic activities with suppliers SCI2 0.815 7.882 Excellent distribution, transportation and warehousing SCI3 0.872 10.490 Inbound and outbound distribution with hospital suppliers SCI4 0.881 6.803 Integrated software applications with suppliers SCI5 0.746 11.920 Integrates purchasing of health products into planning SCI6 0.764 12.927
Level of Information Sharing LIS 0.927 11.276 Share inventory level information with suppliers LIS1 0.798 10.031 Share business knowledge of core business processes LIS2 0.648 9.371 Exchange information to establish business planning LIS3 0.749 10.715 Share proprietary information with suppliers LIS4 0.675 9.715 Share accurate risk information with partners/suppliers LIS5 0.726 12.037 Willing to share real time information on demand LIS6 0.709 10.791
Supply Chain Risk and Uncertainty SCR 0.880 13.173 Share medical supply problems with suppliers SCR1 0.841 Fixed Evaluates suppliers’ achievement of target prices/costs SCR2 0.749 13.056 Evaluates suppliers’ cost reduction efforts SCR3 0.794 14.376 Assess the quality and cost of suppliers’ products SCR4 0.711 12.236 Hold frequent meetings with suppliers SCR5 0.9444 10.791 Scope of Accounting Information AIS 0.968 14.286 Information that relates to future possible events AIS1 0.730 8.447 Quantifythe likelihood of future events occurring AIS2 0.767 11.112 Non-economic information AIS3 0.721 12.272 Information on broad factors external to hospital AIS4 0.809 Fixed
Timeliness of Accounting Information AIT 0.919 12.498 Immediate arrival of information upon request AIT1 0.769 12.291 Automatic supply of information to users AIT2 0.740 11.760 Frequent and systematic provision of reports AIT3 0.793 12.663 No delay between event and relevant information AIT4 0.766 Fixed
(Source: Author’s computations, 2017) (continued from next page)
University of Ghana http://ugspace.ug.edu.gh
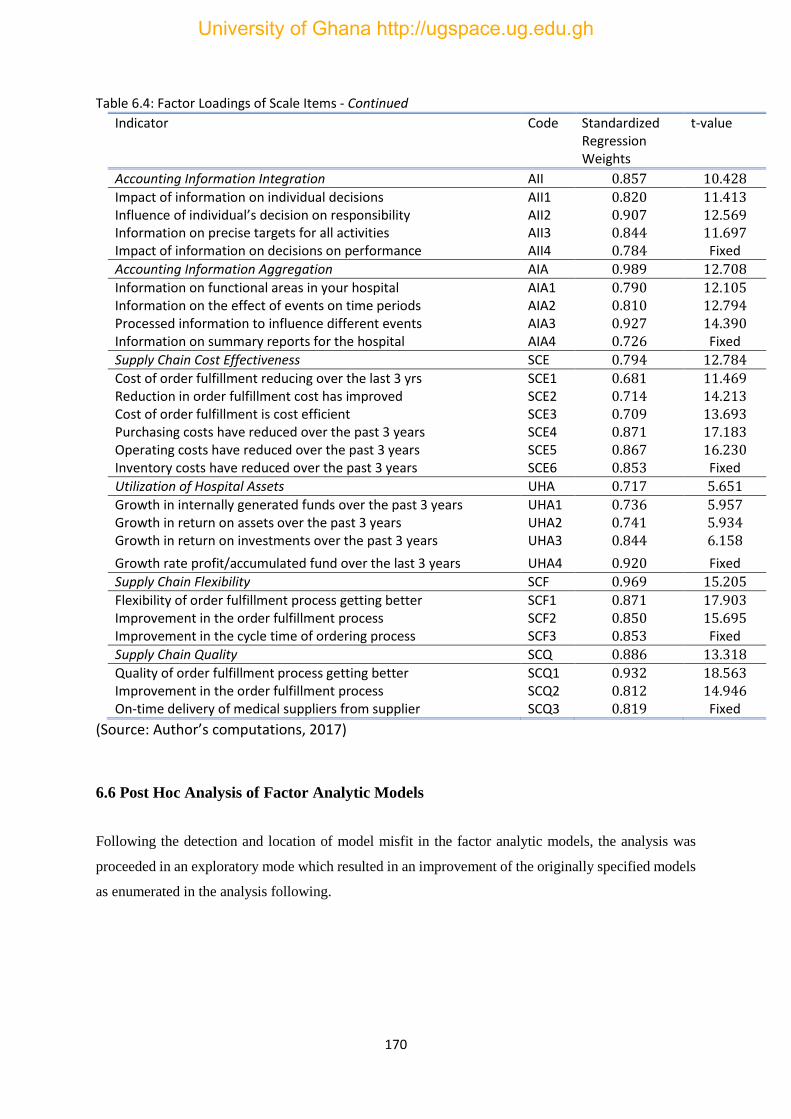
170
Table 6.4: Factor Loadings of Scale Items - Continued
Indicator Code Standardized Regression Weights
t-value
Accounting Information Integration AII 0.857 10.428 Impact of information on individual decisions AII1 0.820 11.413 Influence of individual’s decision on responsibility AII2 0.907 12.569 Information on precise targets for all activities AII3 0.844 11.697 Impact of information on decisions on performance AII4 0.784 Fixed
Accounting Information Aggregation AIA 0.989 12.708 Information on functional areas in your hospital AIA1 0.790 12.105 Information on the effect of events on time periods AIA2 0.810 12.794 Processed information to influence different events AIA3 0.927 14.390 Information on summary reports for the hospital AIA4 0.726 Fixed
Supply Chain Cost Effectiveness SCE 0.794 12.784 Cost of order fulfillment reducing over the last 3 yrs SCE1 0.681 11.469 Reduction in order fulfillment cost has improved SCE2 0.714 14.213 Cost of order fulfillment is cost efficient SCE3 0.709 13.693 Purchasing costs have reduced over the past 3 years SCE4 0.871 17.183 Operating costs have reduced over the past 3 years SCE5 0.867 16.230 Inventory costs have reduced over the past 3 years SCE6 0.853 Fixed
Utilization of Hospital Assets UHA 0.717 5.651 Growth in internally generated funds over the past 3 years UHA1 0.736 5.957 Growth in return on assets over the past 3 years UHA2 0.741 5.934 Growth in return on investments over the past 3 years UHA3 0.844 6.158
Growth rate profit/accumulated fund over the last 3 years UHA4 0.920 Fixed
Supply Chain Flexibility SCF 0.969 15.205 Flexibility of order fulfillment process getting better SCF1 0.871 17.903 Improvement in the order fulfillment process SCF2 0.850 15.695 Improvement in the cycle time of ordering process SCF3 0.853 Fixed
Supply Chain Quality SCQ 0.886 13.318 Quality of order fulfillment process getting better SCQ1 0.932 18.563 Improvement in the order fulfillment process SCQ2 0.812 14.946 On-time delivery of medical suppliers from supplier SCQ3 0.819 Fixed
(Source: Author’s computations, 2017)
6.6 Post Hoc Analysis of Factor Analytic Models
Following the detection and location of model misfit in the factor analytic models, the analysis was
proceeded in an exploratory mode which resulted in an improvement of the originally specified models
as enumerated in the analysis following.
University of Ghana http://ugspace.ug.edu.gh

171
Table 6.5: Post Hoc Analysis for Factor Analytic Models
SCM Construct MAS Construct SCP Construct Combined
Fit
Index
Model 1 Model 2 Model 3 Model 4 Model 1 Model 2 Model 3 Model 1 Model 2 Model 3 Model
𝑋2 491.652 436.791 414.254 233.271 227.653 175.983 135.241 288.564 247.106 223.548 401.232
GFI 0.853 0.807 0.848 0.934 0.807 0.908 0.919 0.901 0.909 0.914 0.911
NFI 0.821 0.829 0.842 0.962 0.813 0.911 0.929 0.910 0.936 0.945 0.901
CFI 0.805 0.872 0.926 0.978 0.834 0.858 0.901 0.844 0.913 0.960 0.966
RMSEA 0.096 0.087 0.071 0,063 0.094 0.089 0.075 0.090 0.076 0.058 0.067
(Source Author’s Computations, 2017)
University of Ghana http://ugspace.ug.edu.gh

172
6.6.1 Model 2 of the Factor Analytic Models
The misfits in Model 1 as indicated in the preceding subsection involved error covariance of
substantially high values following a review of the MIs. In this regard, Model 2 involved the
addition of freely estimated parameters in a systematic manner (i.e. addition to the model, one
parameter at a time) because the MI values have the tendency to vary substantially among
series of parameterization tests. Given this background, Model 2 was built by the initial
addition of the error covariance with the highest MI value associated with each of the factor
analytic model. This parameter represented the error terms for Items 16 and 6, 2 and 3, and 5
and 15 in Model 1 of the SCM, MAS and SCP constructs respectively which from the
parameter change statistic should respectively result in approximately 0.785, 0.618 and 0.887
of parameter estimated value.
The fit indices recorded for Model 2 showed significant improvement upon Model 1 with the
𝑋2 statistic reducing from 491.652 to 436.791, the CFI = 0.872, NFI = 0.829 and RMSEA =
0.087 for the SCM construct. The MAS construct also recorded a decrease in the 𝑋2 value
from 227.653 to 175.983, CFI increased from 0.834 to 0.958 and a reduction in the RMSEA
value from 0.094 to 0.089. Similar results are obtained for the SCP construct where the 𝑋2
statistic decreased from 288.564 to 247.106, CFI increased from 0.844 to 0.953 and the
RMESA reduced from 0.090 to 0.076. Finally, a difference in 𝑋2 values between Model 2 and
Model 1 was an indication of significant improvement in the mode. However, the RMSEA
values still fell outside the acceptable range so a further modification analysis was performed.
6.6.2 Model 3 of the Factor Analytic Models
Although Model 2 showed significant improvement upon Model 1, a review of the MIs
indicated that the error covariance associated with Items 1 and 2 in the SCM factor analytic
University of Ghana http://ugspace.ug.edu.gh

173
model signified strong misspecification parameters to the model. A further examination of
these parameters suggested that an estimated value of approximately . 391 would result if these
parameters were incorporated into the model. Like the error covariance associated with Items
6 and 16, a redundancy due to content overlap was associated with Items 1 and 2. On the basis
of the strength of this MI coupled with the obvious overlap of item content, a further
modification to the model was made by incorporating this error covariance into the model.
Modification and re-specification of Model 2 resulted in Model 3. As shown in Table 6.5, the
output for Model 3 indicated further improvement in the model with the goodness-of-fit
statistics revealing a statistically significant improvement upon Model 2 in terms of model fit
(𝑋(204)2 = 414.254; ∆𝑋1
2 = 22.53). Also, the CFI and RMSEA values improved significantly
from 0.872 to 0.926 and from 0087 to 071 respectively.
Further modifications yielded a CFI value of 0.978 whereas that of the NFI yielded 0.962 and
RMSEA value of 0.063. Also, the GFI recorded 0.934 and the ratio 𝑋2 to degrees of freedom
yielded a ratio of 7.43 and this resulted in Model 4 of the SCM factor analytic model. In spite
of this remarkable improvement in key fit indices, the MIs showed a minimum of two error
covariance with fairly large MIs (i.e. err 1 ↔ 2 and err 2 ↔ 4). However, the substantive
rationale for the addition of the parameters associated with this error covariance to the model
was found not to be strong; hence, were not considered for their inclusion in the model.
With regards to the MAS and SCM factor analytic models, a further review of the MIs showed
cross-loadings with respect to Item 12 on Factor 1 although it was initially postulated as loading
on Factor 3 related to the MAS construct. Yet, the MI indicated that in addition to loading onto
Factor 3, it should load onto Factor 1. Ideally, items on a measuring instrument should clearly
target only one of its underlying constructs (or factors). Given empirical evidence that this same
cross-loading has been documented in prior studies a modification of the model (Model 3) of
the MAS factor analytic model was specified by freely estimating this parameter. A further
University of Ghana http://ugspace.ug.edu.gh

174
statistically significant reduction in the 𝑋2 value of the goodness-of-fit statistic was recorded.
This showed an improvement in Model 3 (𝑋(204)2 = 135.241; ∆𝑋1
2 = 37.742). In addition,
both the CFI and RMSEA values associated with model 3 improved from 0.858 to 0.901 and
from 0.089 to 0.075 respectively. SCP also improved with CFI = 0,960 and RMSEA = 0.058.
A combined model showed a CFI = 0.966 and RMESA = 0.067.
The MIs recorded in the AMOS output however showed no evidence of substantively
reasonable misspecification in Model 3 of both the MAS and SCP factor analytic models. A
review of both unstandardized and standardized factor loadings as well as factor covariance
and error covariance revealed all parameters to be statistically significant with critical ratios
values > 1.96. Given that findings associated with the validity of the three factor analytic
models fell within acceptable range of indices, Model 3 was considered to be the best-fitting
and most parsimonious models to represent the data. As a result of these measurements,
restructuring the revised hypothesized model to be tested replaced the initial hypothesized
model.
Prior literature such as Fornell and Larcker (1981), Maiga et al (2013) and Chen et al (2013)
have indicated that a generally accepted threshold for item loadings and internal consistencies
should not fall below 0.70. Following these guidelines and reviewing all factor loadings and
the significance of their t-values associated with factor to item loadings indicate that they are
above the 0.70 threshold value and beyond 0.80 in most cases. In addition, the critical values
at the 5% level of significance is exceeded by the significance of the t-values associated with
factor loadings. As shown by the factor analysis results in Table 6.4 as well as composite
reliability scores in Table 6.3, the scale used in this study largely meet these thresholds.
Chin (1998) and Hair, Black, Babin and Anderson (2015) have asserted that discriminant
validity is established if first the loadings of items on their respective constructs should be
University of Ghana http://ugspace.ug.edu.gh

175
stronger than any other constructs in the model (or most appropriately zero loadings) and
second, the inter-construct correlations should be lower than the square of the Average
Variance Extracted (AVE). In this regard, and following these guidelines, evidence of
discriminant validity of the constructs in the model was confirmed by a comparison of the
squared correlations of two constructs with their individual AVE. The results as summarized
in Table 6.3 indicate that the AVE of the latent constructs is higher than the squared
correlations. Furthermore, the AVE and composite reliability estimates for each construct fall
beyond acceptable threshold. Based on these overall findings, the analysis proceeded with the
structural model specification and subsequent evaluation to test the hypotheses.
6.7 Structural Model Specification
Having satisfied the underlying assumptions and conditions related to the sample data and the
test items, the analysis proceeded into the real task of fitting the hypothesized model to the
sample data. Hence, the results and findings of the hypotheses tests linking the structural paths
are presented in this final section of the analysis. It has three subsections: the first subsection
specifies the hypothesized model (i.e. model specification). The second subsection identifies
the hypothesized model (i.e. model identification), and the final subsection fits the
hypothesized model to the sample data and presents results of the hypotheses tests. Since the
hypotheses involving the three main constructs – SCM, MAS, and hospital supply chain
performance are categorized into tests of fit, tests of performance, and tests of interactions as
presented under Models 1 to Model 7 in Table 6.7, the final subsection is further divided into
three parts – the first part presents the results on the ‘selection fit’ relationships between SCM
context factors and MAS design whilst the second and final parts present the results on
performance relationships on mediation and interaction effects respectively.
University of Ghana http://ugspace.ug.edu.gh

176
6.7.1 Specification of the Hypothesized Model
The specified hypothesized model that was tested by the sample data is presented in Fig 6.2.
The input model aimed at finding a link between the SCM context factors, MAS design and
hospital supply chain performance. The theoretical foundations and empirical linkages among
the six constructs were presented in chapter five. Three scenarios that relate to model
specification (Joreskog, 1995; Byrne, 2010) include: strictly confirmatory (SC), alternative
models (AM), and model generating (MG). Strictly confirmatory is the scenario where based
on theory or empirical studies, a single model is postulated and appropriate data are collected
to test the fitness of the hypothesized model with the sample data in a single mode.
Here, re-specification of the model does not take place after it has been tested with the sample
data. Hence, further modifications to the model are not made; rather, it is either retained or
rejected based on the results of the test. In the case of the AM scenario, several alternative (or
competing) models which are grounded in theory are proposed by the researcher. The model
that most appropriately represents the sample data is selected following the analysis of a single
set of empirical data to all the models. The MG scenario deals with the situation where the
analysis proceeds in an exploratory (rather than confirmatory) mode following the postulation
and subsequent rejection of a theoretically derived hypothesized model on the basis of its poor
fit to the sample data. Here, the hypothesized model is re-specified and re-estimated after going
through some modification. The primary goal in this scenario is to trace and locate the source
of misfit in the model and produce a model that better describes the sample data.
Given that much resources in both financial and non-financial terms are associated with data
collection, the analysis followed the MG scenario since the research could not have been
abandoned or terminated on the basis of fit inadequacy between the hypothesized model and
the survey data. Joreskog (1995, p. 295) states ‘‘despite the fact that a model is tested in each
University of Ghana http://ugspace.ug.edu.gh
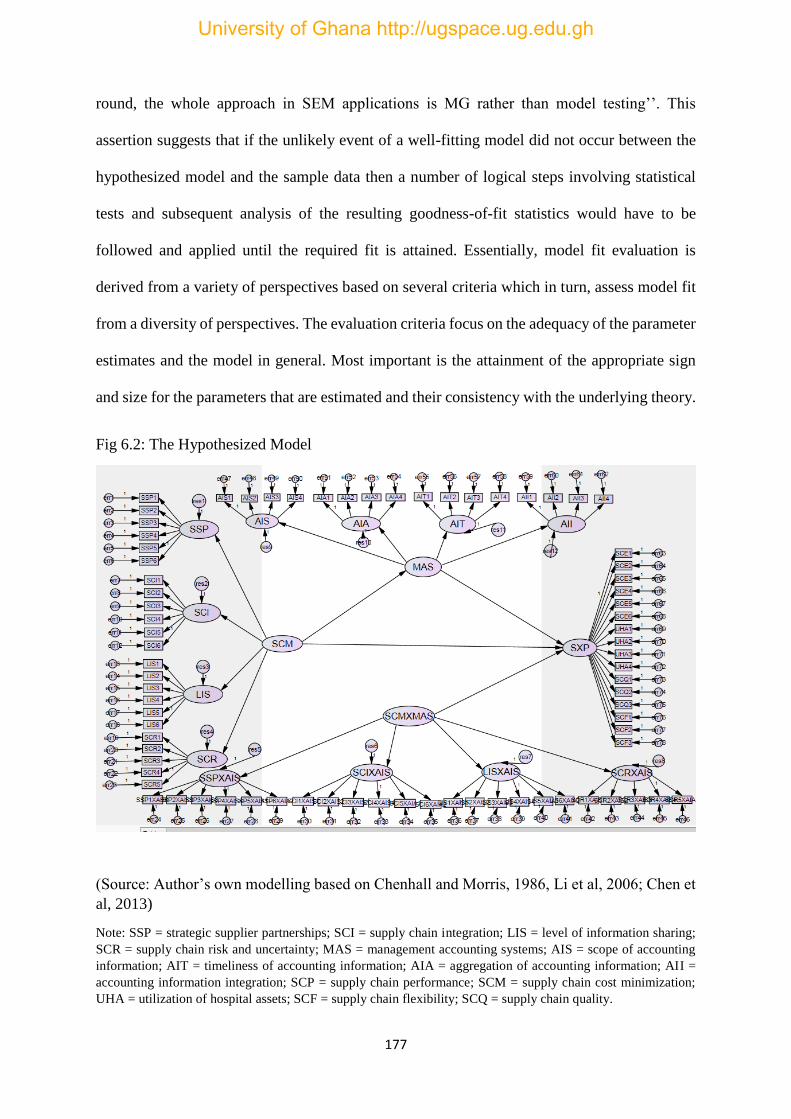
177
round, the whole approach in SEM applications is MG rather than model testing’’. This
assertion suggests that if the unlikely event of a well-fitting model did not occur between the
hypothesized model and the sample data then a number of logical steps involving statistical
tests and subsequent analysis of the resulting goodness-of-fit statistics would have to be
followed and applied until the required fit is attained. Essentially, model fit evaluation is
derived from a variety of perspectives based on several criteria which in turn, assess model fit
from a diversity of perspectives. The evaluation criteria focus on the adequacy of the parameter
estimates and the model in general. Most important is the attainment of the appropriate sign
and size for the parameters that are estimated and their consistency with the underlying theory.
Fig 6.2: The Hypothesized Model
(Source: Author’s own modelling based on Chenhall and Morris, 1986, Li et al, 2006; Chen et
al, 2013)
Note: SSP = strategic supplier partnerships; SCI = supply chain integration; LIS = level of information sharing;
SCR = supply chain risk and uncertainty; MAS = management accounting systems; AIS = scope of accounting
information; AIT = timeliness of accounting information; AIA = aggregation of accounting information; AII =
accounting information integration; SCP = supply chain performance; SCM = supply chain cost minimization;
UHA = utilization of hospital assets; SCF = supply chain flexibility; SCQ = supply chain quality.
University of Ghana http://ugspace.ug.edu.gh

178
6.7.2 Identification of the Hypothesized Model
In order to find a unique solution for values of the structural parameters, the hypothesized
model was subjected to test of identification to establish that a unique set of parameters being
tested in the structural model is consistent with the sample data. This involved a transposition
of the variance – covariance matrix of the manifest variables into the structural parameters of
the hypothesized model. Testing for model identification is a pre-requisite to estimating the
model because in situations where the model cannot be identified, it implies that attainment of
consistent estimates for all parameters is impossible, and that empirical evaluation of the
hypothesized model cannot take place. An unidentifiable model could imply that different
parameter values define the same model where the parameters are subject to arbitrariness.
Three situations arising from model identification can occur: just – identified, over-identified,
and under-identified. To further our understanding of the model identification tests, each of
these is explained briefly in the sub-sections that follow.
6.7.2.1 Just-Identified Model
A just-identified model exhibits a one-to-one mapping (or correspondence) between the dataset
and the structural parameters. In this case, the total number of parameters to be estimated equals
exactly the number of variances and covariance of the manifest variables in the dataset. Studies
in SEM analysis have however shown that in spite of the capability of the just-identified model
in responding to a unique solution for all estimated parameters, it portrays the limitation of
having no degrees of freedom leading to a non-rejection of the model in all cases so it is not
recommended as scientifically appealing.
6.7.2.2 Under-Identified Model
Where the number of variances and covariance in the dataset fall short of the number of
parameters to be estimated, the model is classified as under-identified. In this case, and for the
University of Ghana http://ugspace.ug.edu.gh

179
purposes of attaining a determinate solution of parameter estimation, the information contained
in the model is said to be insufficient and the possibility of resulting in an infinite number of
solutions.
6.7.2.3 Over-Identified Model
In an over-identified model, the number of data points (variances and covariance) exceeds the
number of parameters to be estimated, yielding positive degrees of freedom which allows for
a rejection of the model. Since the aim in SEM analysis is to attain positive degrees of freedom
that can result in the rejection of the model, the over-identification criterion has been proven
to be scientifically usable.
To identify the hypothesized model specified in Fig 7.2 and its underlying assumptions, the 𝑡
-rule principle (Byrne, 2010; Hair et al, 2015) was followed. This is computed as =𝑝(𝑝+1)
2 ,
where 𝑝 represents the number of indicators. After reviewing the specified model, it was
discovered that the number of data points to work with (or the available information with
respect to the dataset) which constitute variances and covariance of the manifest variables (with
𝑝 variables) resulted in 2,628 data points. Given that the number of unknown parameters
(excluding those fixed at 1.00) totaled 160 made up of 63 measurement regression coefficients
(factor loadings), 17 structural regression paths, 3 factor variances, 72 error variances, 12
residual variances and 3 covariances, the model was identified as an over-identified model with
2.458 (2,628 − 170) degrees of freedom. In terms of the second-order model, there are 55
(10(10+1)
2) pieces of information: made up of 10 factor variances, with 24 (12 factor loadings
and 12 residuals) unknown parameters to be estimated resulting in 31(55 − 24) degrees of
freedom. Thus, both the general model and the second-order model were identified as
estimable. After meeting the conditions of identification, the structural parameters were
considered as estimable and a subsequent testable of the model followed.
University of Ghana http://ugspace.ug.edu.gh
180
6.8 Fitting the Hypothesized Model
The final part of the model fitting process involved the structural model which tested and cross-
validated the linkages among the latent constructs. In fitting the structural portion of a full SEM
model which involves linkages among only the latent variables to the sample data, the four
important aspects that characterized model-fitting in full SEM (Byrne, 2010) were followed.
These include: 1) statistical significance, 2) the estimation process, 3) the model-fitting process,
and 4) the goodness-of-fit statistics. Each of these is discussed briefly in the subsections that
follow.
6.8.1 Statistical Significance
Following past studies on full SEM analysis, the test for statistical significance was based
mainly on the analysis of covariance structures which are driven by degrees of freedom (𝑑𝑓)
made up of the number of elements in the sample matrix and the number of parameters being
estimated. This approach is somewhat different from statistical significance testing involving
traditional statistical methods. In this regard, issues such as the use of null hypothesis testing
procedures, the importance of confidence intervals, practical significance etc. are captured in
the fits statistic indices. Although a plethora of criticisms have been generated on the practice
of statistical significance testing over the years, extant literature suggests that these have long
been addressed in SEM applications.
6.8.2 Model Estimation Process
The task in the estimation process (as has been the primary focus of the estimation process in
SEM) was to produce parameter values such that the discrepancy (residual) between the sample
covariance matrix and the population covariance matrix implied by the hypothesized model is
minimal. In full SEM, this task is accomplished by minimizing a discrepancy function behind
the scenes such that the point in the estimation process where the discrepancy between the
University of Ghana http://ugspace.ug.edu.gh
181
sample covariance matrix and restriction covariance matrix implied by the model reflects its
minimal value.
6.8.3 Structural Model Fitting Process
In this part of the analysis, only the causal paths of the model are of interest and hence only the
MIs of the parameters that represent the structural (i.e. causal) paths in the model were detected
for possible misspecifications in the model. The reason is that any misfit to components of the
measurement model in the structural model are normally catered for while that portion of the
model was tested for validity in the factor analytical model. Proceeding from that point, the
extent to which the hypothesized structural model adequately describes (or ‘‘fits’’) the sample
data was assessed in a systematic manner until a well-fitting full structural model was finally
attained.
6.9 Hypotheses Tests of the Structural Model
Since the overall structural model of fits fall within the specified range of acceptability, the
analysis proceeded with testing of the causal relationships between the latent constructs. The
tests involved different modelling techniques for each contingency fit since each is associated
with a different theoretical foundation and interpretation. To evaluate the hypotheses, the
standardized parameter estimates for the model were examined using the significance of
individual path coefficients. The key goodness-of-fit statistics (CFI, GFI, RMSEA) associated
with the structural model are summarized in Table 6.7. A review of these indices showed a
relatively well-fitting model with values 0.979 , 0.906, and 0.062 represented by the CFI, GFI
and the RMSEA respectively for Model 1 and particularly the RMSEA value which fell within
the recommended range of acceptability (< 0.05 𝑡𝑜 0.08).
University of Ghana http://ugspace.ug.edu.gh

182
However, a further review of the MIs of the structural models revealed cross-loadings of an
indicator variable onto a factor other than the one it was originally postulated to measure (MAS
← UHA3) associated with Model 5. In addition, the maximum MI flowing from management
accounting to supply chain performance (SCP ← MAS) was also detected with a value of
116.5 in Model 2. The interpretation is that if that parameter was to be freely estimated in a
subsequent model, a drop of at least this figure will occur in the overall 𝑋2 value. Turning to
the parameter change statistic associated with this parameter revealed a value of 0.572 which
represents the approximate value that would be assumed by the new parameter. specified as a
freely estimated parameter resulting in the final Model 2 with CFI = 0.964 and RMSEA =
0.057. The results of hypotheses tests among the three cases are presented next.
6.10 Selection Fit Model – Test of H1 (a – d), H2 (a – d), H3 (a – d), and H4 (a – d)
The objectives of hypotheses H1 (a – d), H2 (a – d), H3 (a – d) and H4 (a – d) is to test the fit
relationships (selection forces) between the SCM antecedent conditions and the information
characteristics of the MAS. Fig 7.3 shows the graphical view of the results for structural path
coefficients for the fit between the test variables. Each construct is treated as first-order latent
variable.
First, as summarized in Table 6.6, the results show a strong statistically significant positive and
direct association between the strategic supplier relations construct and the four dimensions of
MAS information. Consequently, the hypotheses tests, H1 (a), H1 (b), H1(c), and H1 (d) are
respectively supported at the 0.01, 0.05, and 0.1 significance levels. More precisely, the results
indicate that a strong statistically significant positive and direct relationship exists between
strategic supplier relations and broad scope MAS information (t =5.732, p-value =0.000 <
0.01), MAS information timeliness (t =6.003, p-value =0.07 < 0.1), MAS information
University of Ghana http://ugspace.ug.edu.gh
183
integration (t = 5.273, p-value = 0.03 < 0.05) and MAS information aggregation (t = 7.153,
p-value = 0.02 < 0.05). Supply chain integration recorded statistically significant relationships
for accounting information scope and aggregation (𝑡 = 3.033, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.03 < 0.05) and
(𝑡 = 4.233, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.08 < 0.1) respectively. Hence H2 (a) and H2 (d) are supported.
However, the relationship between supply chain integration and accounting information
timeliness and integration recorded statistically insignificant relationships (𝑡 = 1.758, 𝑝 −
𝑣𝑎𝑙𝑢𝑒 = 0.179 > 0.05) and (𝑡 = 0.519, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.129 > 0.05) respectively. This leads
no support for H2 (b) and H2 (c).
Turning to the relationship between level of information sharing and the four dimensions of
the MAS, none of the hypotheses H3 (a), H3 (b), H3 (c) and H3 (d) recorded a statistically
significant relationship with the MAS information characteristics and hence, were not
supported. In particular, the level of information sharing recorded a statistically insignificant
relationship between accounting information scope (𝑡 = 0.897, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.370 > 0.05),
timeliness (𝑡 = 0.528, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.597 > 0.05), integration (𝑡 = 1.048, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 =
0.295 > 0.05) and aggregation (𝑡 = 1.147, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.251 > 0.05). the relationship
between supply chain integration and accounting information scope, timeliness, integration and
aggregation were all statistically significant (𝑡 = 4.256, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.000 < 0.01), (𝑡 =
6.597, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.04 < 0.05), (𝑡 = 6.291, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.000 < 0.01), and (𝑡 =
5.816, 𝑝 − 𝑣𝑎𝑙𝑢𝑒 = 0.02 < 0.05) respectively. Hence the hypotheses H4 (a), H4 (b), H4 (c)
and H4 (d) are supported.
On the whole, the results provide strong empirical support for the fit existing between strategic
supplier relationship and supply chain risk and uncertainty but partial support supply chain
integration and no support for knowledge exchange in Ghanaian hospitals. In other words, in
designing and implementing MAS information for SCM decisions involving healthcare
University of Ghana http://ugspace.ug.edu.gh
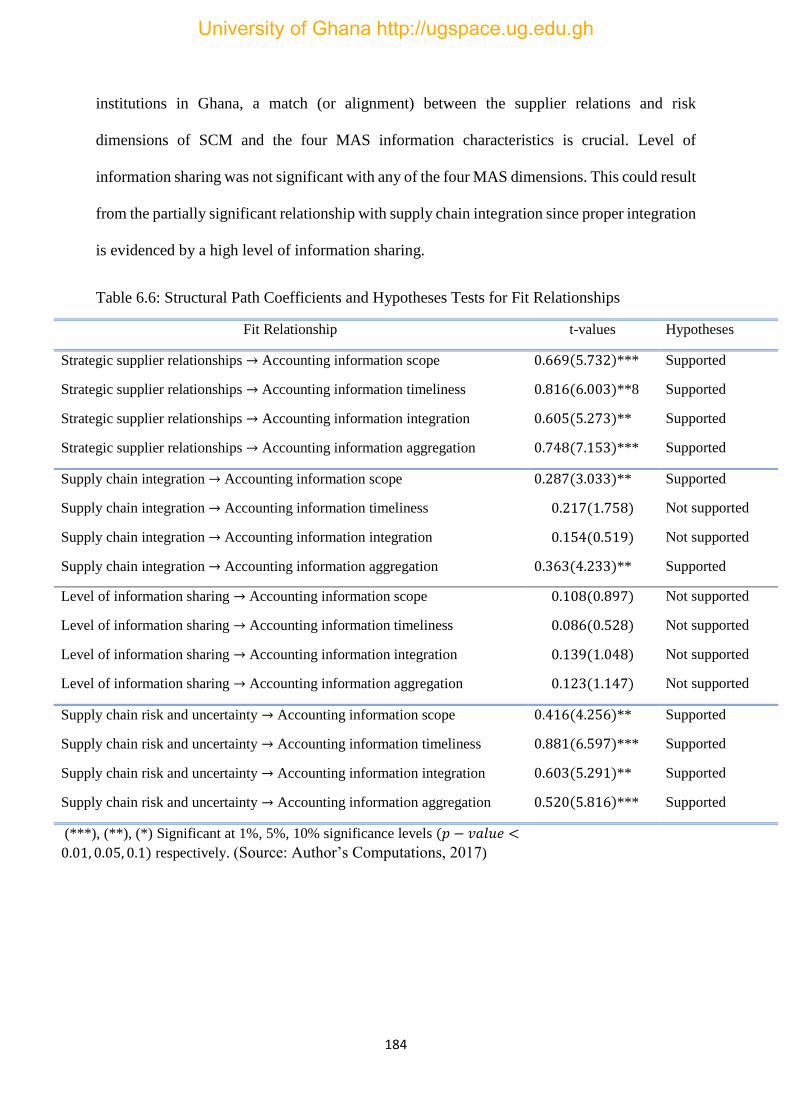
184
institutions in Ghana, a match (or alignment) between the supplier relations and risk
dimensions of SCM and the four MAS information characteristics is crucial. Level of
information sharing was not significant with any of the four MAS dimensions. This could result
from the partially significant relationship with supply chain integration since proper integration
is evidenced by a high level of information sharing.
Table 6.6: Structural Path Coefficients and Hypotheses Tests for Fit Relationships
Fit Relationship t-values Hypotheses
Strategic supplier relationships → Accounting information scope 0.669(5.732)*** Supported
Strategic supplier relationships → Accounting information timeliness 0.816(6.003)**8 Supported
Strategic supplier relationships → Accounting information integration 0.605(5.273)** Supported
Strategic supplier relationships → Accounting information aggregation 0.748(7.153)*** Supported
Supply chain integration → Accounting information scope 0.287(3.033)** Supported
Supply chain integration → Accounting information timeliness 0.217(1.758) Not supported
Supply chain integration → Accounting information integration 0.154(0.519) Not supported
Supply chain integration → Accounting information aggregation 0.363(4.233)** Supported
Level of information sharing → Accounting information scope 0.108(0.897) Not supported
Level of information sharing → Accounting information timeliness 0.086(0.528) Not supported
Level of information sharing → Accounting information integration 0.139(1.048) Not supported
Level of information sharing → Accounting information aggregation 0.123(1.147) Not supported
Supply chain risk and uncertainty → Accounting information scope 0.416(4.256)** Supported
Supply chain risk and uncertainty → Accounting information timeliness 0.881(6.597)*** Supported
Supply chain risk and uncertainty → Accounting information integration 0.603(5.291)** Supported
Supply chain risk and uncertainty → Accounting information aggregation 0.520(5.816)*** Supported
(***), (**), (*) Significant at 1%, 5%, 10% significance levels (𝑝 − 𝑣𝑎𝑙𝑢𝑒 <
0.01, 0.05, 0.1) respectively. (Source: Author’s Computations, 2017)
University of Ghana http://ugspace.ug.edu.gh
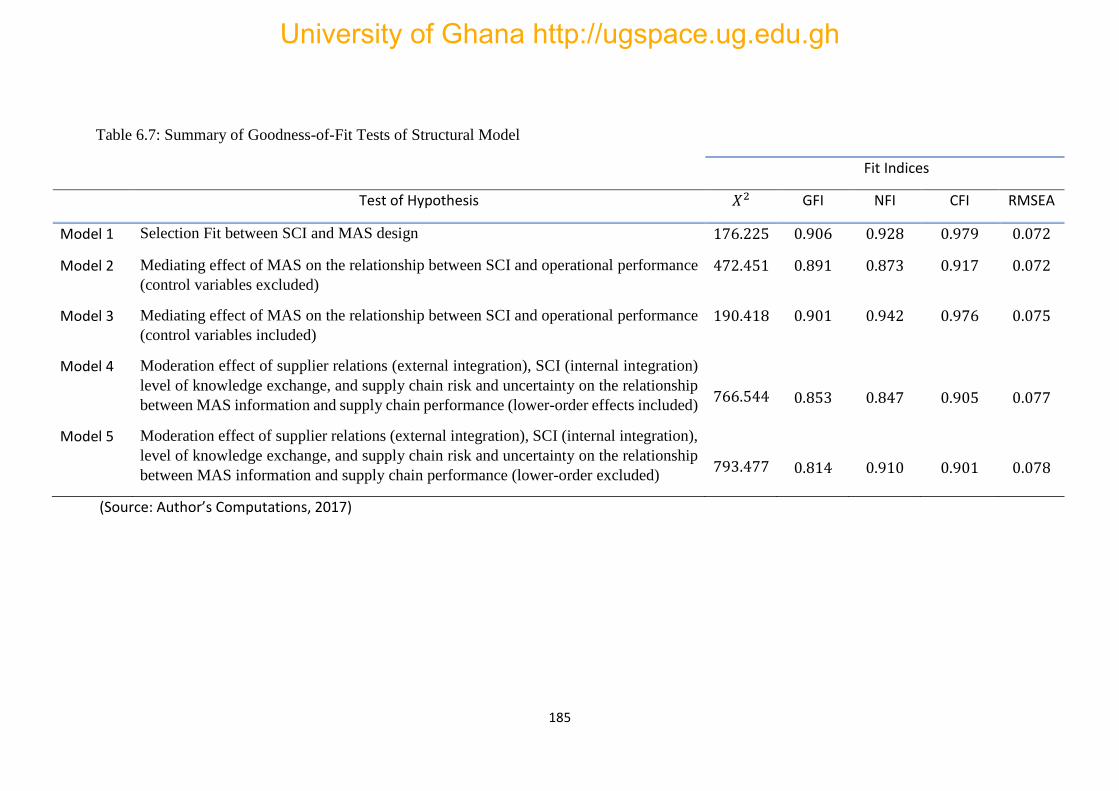
185
Table 6.7: Summary of Goodness-of-Fit Tests of Structural Model
Fit Indices
Test of Hypothesis 𝑋2 GFI NFI CFI RMSEA
Model 1 Selection Fit between SCI and MAS design 176.225 0.906 0.928 0.979 0.072
Model 2 Mediating effect of MAS on the relationship between SCI and operational performance
(control variables excluded)
472.451 0.891 0.873 0.917 0.072
Model 3 Mediating effect of MAS on the relationship between SCI and operational performance
(control variables included)
190.418 0.901 0.942 0.976 0.075
Model 4 Moderation effect of supplier relations (external integration), SCI (internal integration)
level of knowledge exchange, and supply chain risk and uncertainty on the relationship
between MAS information and supply chain performance (lower-order effects included)
766.544
0.853
0.847
0.905
0.077
Model 5 Moderation effect of supplier relations (external integration), SCI (internal integration),
level of knowledge exchange, and supply chain risk and uncertainty on the relationship
between MAS information and supply chain performance (lower-order excluded)
793.477
0.814
0.910
0.901
0.078
(Source: Author’s Computations, 2017)
University of Ghana http://ugspace.ug.edu.gh
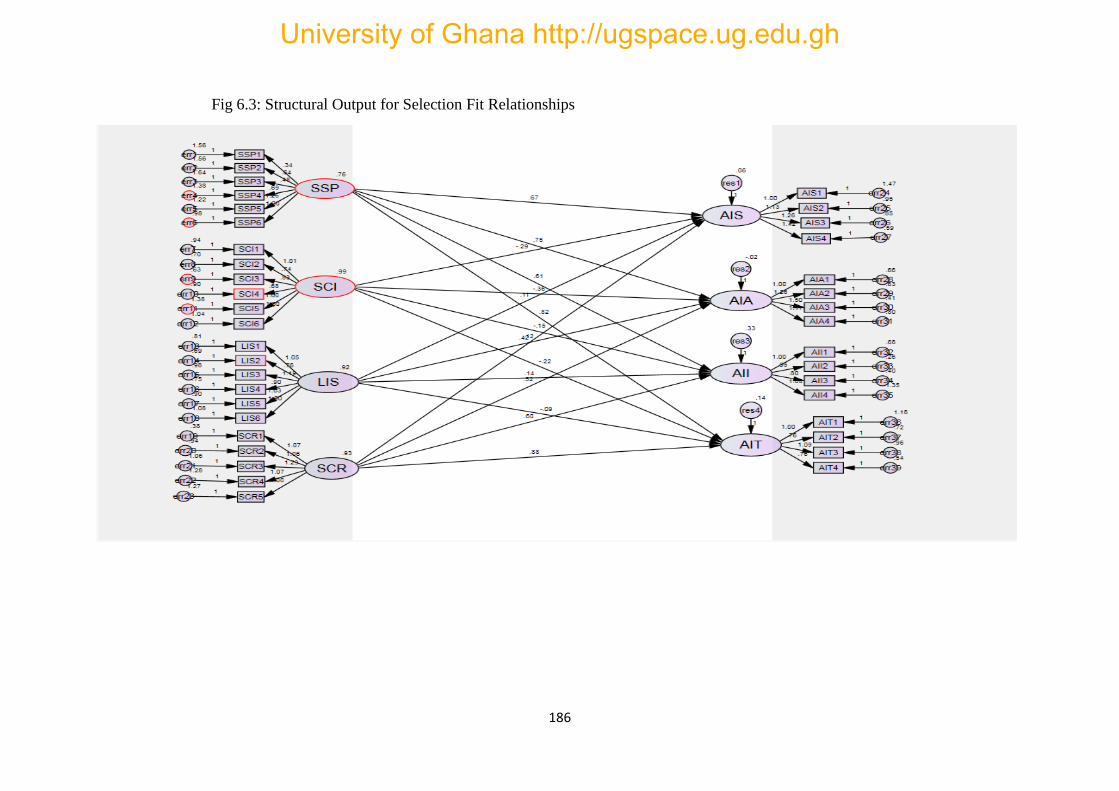
186
Fig 6.3: Structural Output for Selection Fit Relationships
University of Ghana http://ugspace.ug.edu.gh

187
6.11 Mediating Effect of MAS Construct – Test of H5 (a) to H5 (d)
Hypotheses H 5(a), H 5(b), H 5(c), and H 5(d) test the mediating effect of the MAS construct
on the relationship between SCI and hospital supply chain performance. Two models were
tested: first without the confounding variables and second with the confounding variables. The
results are summarized in Table 6.8.
6.11.1. Confounding Variables Effect
Although the threshold for the goodness-of-fit statistics for the mediation effects as evidenced
in Models 2 and 3 in Table 6.5 were met, only the location and profit status were statistically
significant at the 5% significance level. A statistically significant test for ownership and size
was not supported by the sample data in Model 2. In other words, the operational performance
impacts of the four SCM context factors being mediated by the four MAS information
characteristics are affected by hospitals’ location and profit status but not hospital size and
ownership status in the Ghanaian context. The test for hospital size and ownership in Model 2
were statistically insignificant (t =1.163, p-value =0.245 > 0.05) and (t =1.113, p-value =
0.266 > 0.05) respectively. However, profit status and location in Model 1 were statistically
significant (t = 2.824, p-value = 0.034 < 0.05) and (t = 2.078, p-value = 0.022 < 0.05)
respectively for Model 3. The results suggest that location and profit status affect hospital
supply chain performance
6.11.2 Mediation Effect of the MAS Construct
To test for the mediation effect of the MAS construct between SCM and SCP, Baron and
Kenny’s (1986) classic four step procedure was followed. First, a test for the direct effect of
the strategic supplier partnership (external integration), supply chain integration (internal
integration), level of information sharing and supply chain risk and uncertainty on performance
University of Ghana http://ugspace.ug.edu.gh

188
was performed. The results showed that only supply chain integration (i.e. hospital internal
integration) was statistically insignificant (t=1.792, p-value = 0.621 > 0.05); hence, H5 (b) is
not supported. All the three other SCM constructs recorded statistically significant effects on
performance at the 1% and 5% significance levels (t = 2.209, p-value = 0.027 > 0.05); (t =
4.271, p-value = 4.271 < 0.000 < 0.01) and (t = 2.017, p-value = 0.031 < 0.05) for supplier
relations (external integration), level of information sharing and supply chain risk and
uncertainty respectively, supporting H5 (a), H5 (c) and H5 (d). Second, the relationship
between the four SCM test variables and the four dimensions of the MAS information was
tested. Again, only the supply chain integration (hospital internal integration) construct
recorded a statistically insignificant effect (t = 1.149, p-value = 0.142 > 0.05). Supplier
relations (external integration) recorded a statistically significant effect at the 5% significance
level (t = 2.972, p-value = 0.024 < 0.05). A statistically significant effect on the MAS construct
was also recorded for level of information sharing at the 5% significance level (t = 3.734, p-
value = 0.036 < 0.05). Finally, supply chain risk and uncertainty recorded a statistically
significant effect on the MAS construct at the 1% significance level (t = 4.133, p-value = 0.000
> 0.01). Third, the relationship between the four dimensions of the MAS construct and supply
chain performance was tested. Here the MAS construct recorded a high statistically significant
effect on performance (t = 5.269, p-value = 0.000 < 0.01). A final test to confirm for the
existence of mediation was undertaken by testing again the relationship between the SCM
context factors and performance. This time round, only the level of information sharing
construct recorded a statistically significant effect on performance at the 5% level of
significance (t = 2.260, p-value = 0.029 < 0.05).. The remaining three SCM constructs recorded
statistically insignificant effects on performance (t = 1.854, p-value = 0.152 > 0.05), (t = 0.515,
p-value = 0.317 > 0.05) and (t = 0.351, p-value = 0.661) for supplier relations (external
University of Ghana http://ugspace.ug.edu.gh
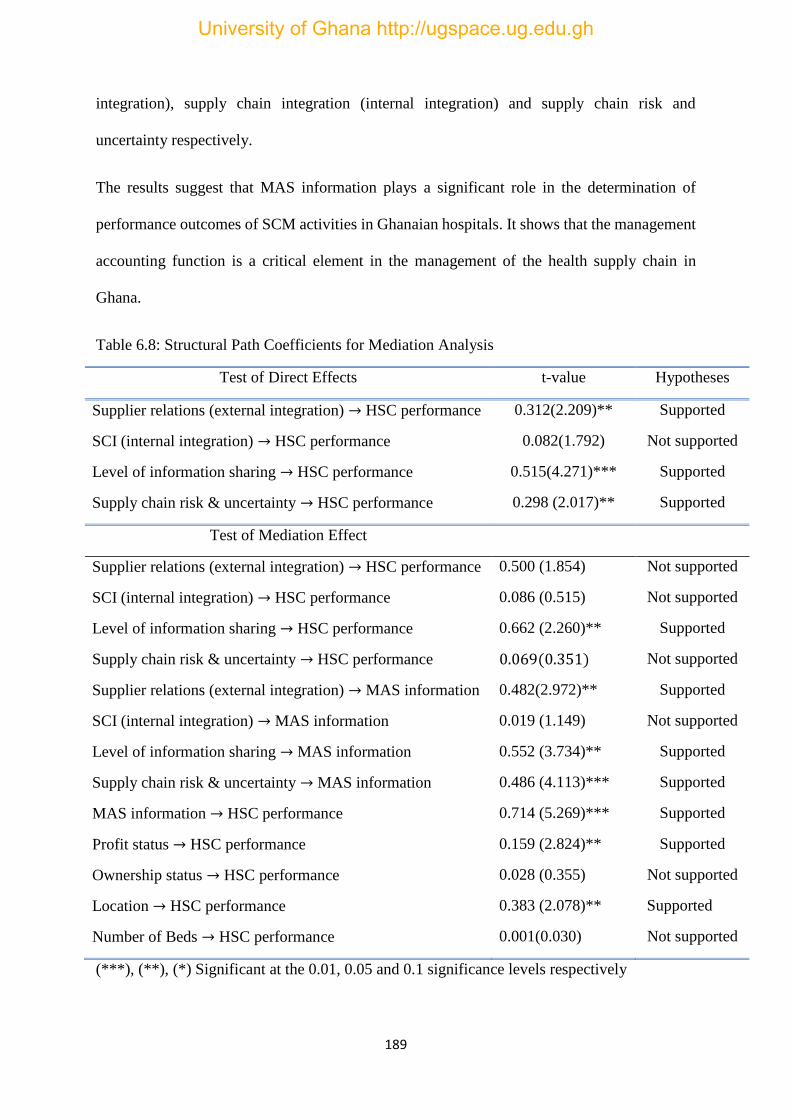
189
integration), supply chain integration (internal integration) and supply chain risk and
uncertainty respectively.
The results suggest that MAS information plays a significant role in the determination of
performance outcomes of SCM activities in Ghanaian hospitals. It shows that the management
accounting function is a critical element in the management of the health supply chain in
Ghana.
Table 6.8: Structural Path Coefficients for Mediation Analysis
Test of Direct Effects t-value Hypotheses
Supplier relations (external integration) → HSC performance 0.312(2.209)** Supported
SCI (internal integration) → HSC performance 0.082(1.792) Not supported
Level of information sharing → HSC performance 0.515(4.271)*** Supported
Supply chain risk & uncertainty → HSC performance 0.298 (2.017)** Supported
Test of Mediation Effect
Supplier relations (external integration) → HSC performance 0.500 (1.854) Not supported
SCI (internal integration) → HSC performance 0.086 (0.515) Not supported
Level of information sharing → HSC performance 0.662 (2.260)** Supported
Supply chain risk & uncertainty → HSC performance 0.069(0.351) Not supported
Supplier relations (external integration) → MAS information 0.482(2.972)** Supported
SCI (internal integration) → MAS information 0.019 (1.149) Not supported
Level of information sharing → MAS information 0.552 (3.734)** Supported
Supply chain risk & uncertainty → MAS information 0.486 (4.113)*** Supported
MAS information → HSC performance 0.714 (5.269)*** Supported
Profit status → HSC performance 0.159 (2.824)** Supported
Ownership status → HSC performance 0.028 (0.355) Not supported
Location → HSC performance 0.383 (2.078)** Supported
Number of Beds → HSC performance 0.001(0.030) Not supported
(***), (**), (*) Significant at the 0.01, 0.05 and 0.1 significance levels respectively
University of Ghana http://ugspace.ug.edu.gh
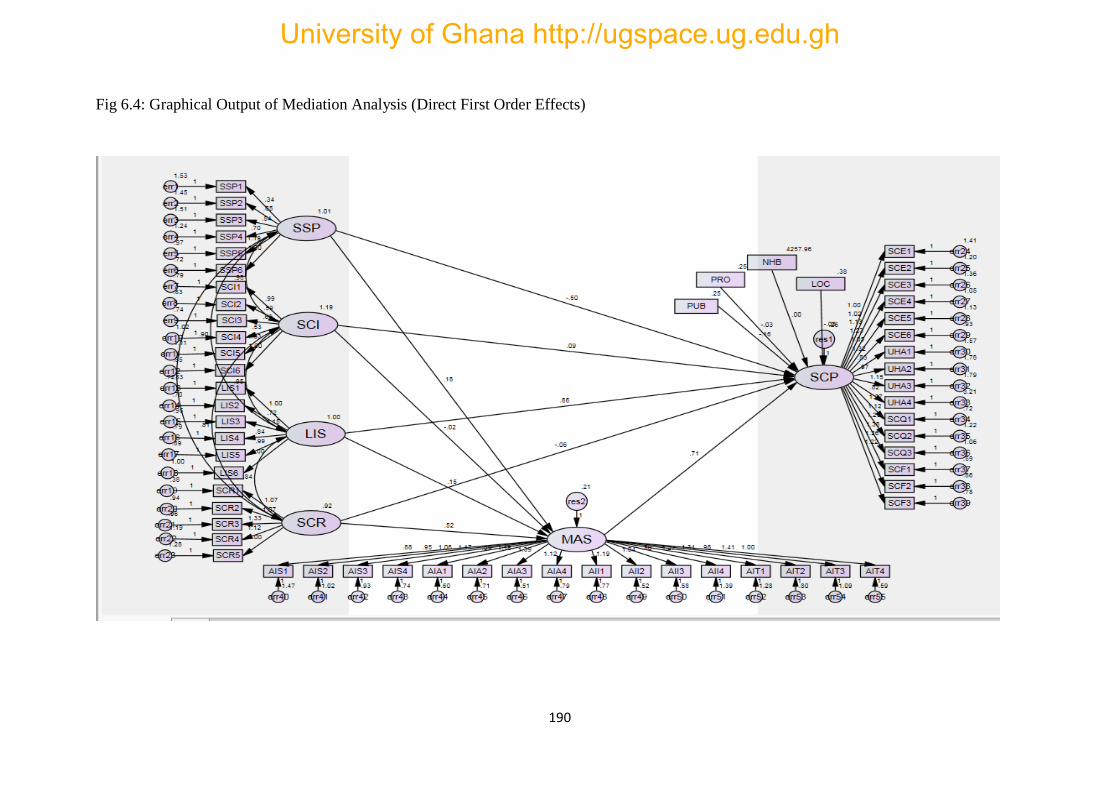
190
Fig 6.4: Graphical Output of Mediation Analysis (Direct First Order Effects)
University of Ghana http://ugspace.ug.edu.gh

191
To check the robustness of the mediation model, a second-order model was tested as shown in
Fig 6.1. The results showed that supplier relations (external integration) fits very well (loading
= 0.91), SCI (internal integration) also loads correctly (loading 0.99), level of knowledge
exchange (loading = 0.98) and supply risk and uncertainty (loading = 0.88) onto the second-
order SCM construct. However, although there was a positive direct relationship between each
of the lower-order (or first-orders) of SCM i.e., strategic supplier relations (external integration,
t = 6.423, p-value = 0.000 < 0.01), supply chain integration (internal integration, t = 4.287, p-
value = 0.014 < 0.05)), level of information sharing (t = 7.192, p = 0.000 < 0.01) and supply
chain risk and uncertainty (t = 5.483, p-value = 0.000 < 0.01), the relationship between SCM
and performance was statistically insignificant (t = 1.273, p-value = 0.336 > 0.05). The results
for the relationship between SCM and MAS information was statistically significant (t = 4.823,
p-value = 0.000 < 0.01) at the 1% level of significance, but the results between the second-
order SCM and performance were statistically insignificant as specified above. This suggests
that the constructs can load excellently unto their second-order SCM constructs but could not
combine to be statistically significant on the relationship between SCM and supply chain
performance. The results in this second-order model hold and suggest that the MAS design
serves as an intervening mechanism between inter-firm management and performance.
University of Ghana http://ugspace.ug.edu.gh

192
Fig 6.5: Graphical Output for Mediation Effects (Second Order)
University of Ghana http://ugspace.ug.edu.gh
193
6.13 Moderating Effects of the SCM Constructs – Hypotheses H 6(a) – H 6(d)
Hypotheses H 6(a), H 6(b), H 6(c), and H 6(d) test the contingent effect of supplier relations
(external integration), SCI (internal integration), level of information sharing, and supply chain
risk and uncertainty on the relationship between MAS information and performance. The
results are summarized in Table 6.9. As contingency theory suggests, the hypothesis in this
study tests the extent to which the design and implementation of MAS information
characteristics in the inter-firm exchanges decisions in supply chains are influenced by SCM
variables in the context of Ghanaian hospitals. As shown in Table 6.5, the fit statistics of Model
4 and Model 5 which analyses the moderating effects with the lower-order effects excluded
and included respectively, falls within the acceptable thresholds. The CFI = 0.905 and RMSEA
= 0.077 for Model 4 and CFI = 0.901 and RMSEA = 0.078 for Model 6. Two main models
were tested for interaction effects: 1) inclusion of lower-order effects, and 2) exclusion of
lower-order effects. The subsections that follow provide evidence of the moderating impact of
the SCM constructs providing contingency relationships between MAS information and
hospital supply chain performance.
6.13.2 Inclusion of Lower-Order Effects
One of the challenging and difficult aspects of SEM analysis is tests involving moderating
impacts in a relationships. Here, the test involves the product of the indicators that measure
each of the constructs to be interacted (Burkert et al, 2014). However, there is always a
redundancy of most of the product terms as the same variables are interacted over and over
again (Burkert et al, 2014). Following this arrangement, the items of each of the constructs to
be interacted were interacted but those that were redundant were eliminated. As the graphical
output shows in Fig 6.2, this test involved a second-order arrangement of the MAS information
University of Ghana http://ugspace.ug.edu.gh

194
characteristics, SCM and the interaction of MAS information characteristics and SCM
constructs on supply chain performance. None of the control variables (i.e. hospital location,
size, ownership status and profit status) was significant. In particular, the results showed (t =
1.542, p-value = 0.123 > 0.05), (t= 0.023, p-value = 0.982 > 0.05), (t = 1.663, p-value = 0.096)
and (t = 0.531, p-value = 0.596 > 0.05) for hospital location, profit status, size and ownership
respectively.
Following prior studies (e.g. Flynn et al, 2010), this test was performed in a hierarchical order;
i.e. substitution of one interaction variable at a time. First, the moderating effect of supplier
relations (external integration) between MAS information and performance was tested. The
results showed the presence of moderating effect of the supplier relations (external integration)
construct between MAS information and performance. A statistically significant positive
relationship (t = 9.030, p-value = 0.000 < 0.01) was recorded at the 1% level of significance.
While the interaction of the supplier relations and MAS information construct recorded a
positive relationship, the lower-order effects (main effect) constructs (i.e. supplier relations and
MAS information) constructs also recorded a positive effect on performance. This shows that
there is an interaction since both are significant. Hence, H6 (a) was supported.
Second, the interaction of SCI (internal integration) and the MAS information construct was
tested. This also recorded a statistically significant positive relationship between MAS
information and supply chain performance with a reduction of the values recorded by the main
effects. Results for the interaction of SCI (internal integration) and MAS information at the 1%
significance level was (t = 17.022, p-value = 0.000 < 0.01). Thus, H6 (b) is supported. A third
test involved the substitution of the interaction between the level of information sharing
construct and the MAS information. Again the results showed a statistically significant positive
relationship (t = 13.505, p-value = 0.000 < 0.01) between the MAS information and supply
chain performance. As the moderating variables increases, the statistically significant effect of
University of Ghana http://ugspace.ug.edu.gh

195
the main effect (lower-order effects) diminishes so there was a further reduction of the main
MAS and SCM variables. Hence, H6 (c) is supported.
Finally, the interaction between supply chain risk and uncertainty and the MAS construct was
included in the model and tested. The results showed a statistically positive relationship (t =
13.440, p-value = 0.000 < 0.01) between the MAS information and supply chain performance,
also at the 1% significance level. Thus, H6 (d) is supported. After substituting the fourth
interacting term, the statistical significance of the main effects got vanished. More precisely,
the relationship between the MAS information and supply chain performance was statistically
insignificant (t = 0.460, p = 0.646 > 0.05). Similar results were recorded for the relationship
between SCM and supply chain performance (t = 1.568, p = 0.117 > 0.05). Thus, the results
provide strong statistical support for the moderating effects of all the four SCM context factors
on hospital supply chain performance
University of Ghana http://ugspace.ug.edu.gh
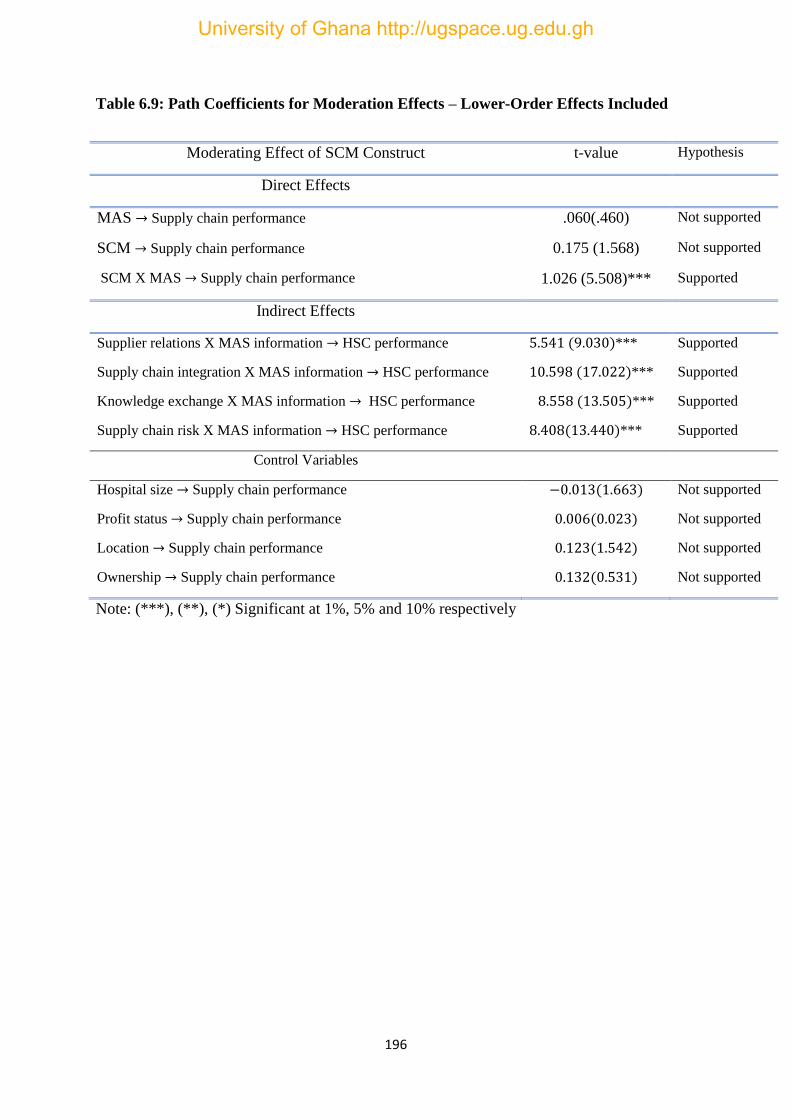
196
Table 6.9: Path Coefficients for Moderation Effects – Lower-Order Effects Included
Moderating Effect of SCM Construct t-value Hypothesis
Direct Effects
MAS → Supply chain performance .060(.460) Not supported
SCM → Supply chain performance 0.175 (1.568) Not supported
SCM X MAS → Supply chain performance 1.026 (5.508)*** Supported
Indirect Effects
Supplier relations X MAS information → HSC performance 5.541 (9.030)*** Supported
Supply chain integration X MAS information → HSC performance 10.598 (17.022)*** Supported
Knowledge exchange X MAS information → HSC performance 8.558 (13.505)*** Supported
Supply chain risk X MAS information → HSC performance 8.408(13.440)*** Supported
Control Variables
Hospital size → Supply chain performance −0.013(1.663) Not supported
Profit status → Supply chain performance 0.006(0.023) Not supported
Location → Supply chain performance 0.123(1.542) Not supported
Ownership → Supply chain performance 0.132(0.531) Not supported
Note: (***), (**), (*) Significant at 1%, 5% and 10% respectively
University of Ghana http://ugspace.ug.edu.gh

197
Fig 6.6: Graphical Output for Moderation Effect – Lower Order Effects Included
University of Ghana http://ugspace.ug.edu.gh

198
6.13.1 Exclusion of Lower-Order Effects
Considering the values of the various measures tested in this study, the results provide strong
support for the presence of moderating contextual variables in the association between hospital
supplier relations (external integration), hospital supply integration (internal integration),
information sharing (or knowledge exchange), hospital supply risk and uncertainty and various
aggregate dimensions of hospital supply chain performance. This suggests that contingency
theory is strongly supported in the inter-organizational relation domains in supply chains. That
is the relationship between MAS information characteristics and hospital supply chain
performance is contingent upon supplier relations (external integration), SCI (internal
integration), level of knowledge exchange, and supply chain risk and uncertainty.
Unlike the results obtained in the preceding section, the control variables for hospital size and
ownership status were not statistically significant. The other two control variables (location
and profit status) were found to be statistically significant at the 5% significance level when
the main effects were excluded from the model (t = 4.132, p = 0.023 < 0.05) and (t = 2.761,
p = 0.042 < 0.05) for profit status and location respectively. As shown in Table 5.9(a), the
hypotheses linking all the path coefficients are statistically significant at the 1%, 5% and 10%
significance levels respectively and hence supported. In particular, the moderating effect of
strategic supplier partnership (external integration) on the relationship between MAS design
and hospital supply chain performance is statistically significant at the 5% significance level (t
= 5.841, p-value = 0.022 < 0.05). This suggests that a high level of supplier relationship tends
to increase hospital supply chain performance and vice versa. Similar results hold for supply
chain integration at the 1% significance level (t = 14.217, p-value = 0.000 < 0.01), level of
information sharing (or knowledge exchange) at the 1% significance level (t = 6.768, p – value
= 0.000 < 0.01), and finally, supply chain risk and uncertainty at the 5% significance level (t =
University of Ghana http://ugspace.ug.edu.gh

199
2.592, p – value = 0.034 < 0.05). The results for the knowledge exchange dimension suggest
that making supply chain information available to supply chain partners enhances supply chain
performance. Similar findings are assigned to supply chain risk and uncertainty. The
implication is that supply chain performance is more enhanced in an unfavourable environment
than in a favourable environment.
Table 6.10 (a): Path Coefficients for Moderation Effects – Lower-Order Effects
Excluded
Moderating Effect of SCM Construct t-value Hypothesis
Strategic supplier partnerships X MAS information → HSC performance 0.567(5.841)** Supported
Hospital supply chain integration X MAS information → HSC performance 0.849 (14.217)*** Supported
Information sharing level X MAS information →HSC performance 0.433(6.768)*** Supported
Supply chain risk and uncertainty X MAS design → HSC performance 0.112(2.592)** Supported
Control Variables
Hospital size → HSC performance −0.113 (0.969) Not supported
Profit status → HSC performance 0.136 (4.132)** Supported
Location → HSC performance 0.142 (2.761)** Supported
Ownership → HSC performance 0.059(1.271) Not supported
(Source: Author’s computations, 2017)
Note (***), (**), (*) Significant at 1%, 5% and 10% respectively
University of Ghana http://ugspace.ug.edu.gh
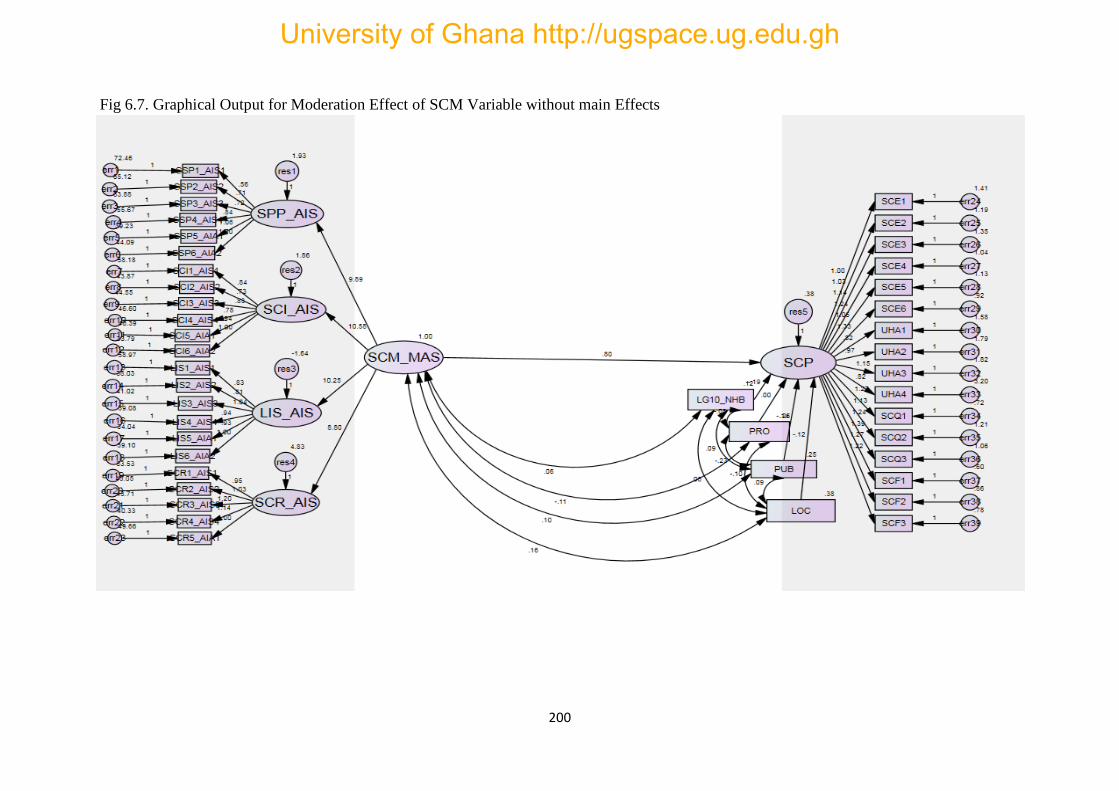
200
Fig 6.7. Graphical Output for Moderation Effect of SCM Variable without main Effects
University of Ghana http://ugspace.ug.edu.gh
201
6.14 Chapter Summary
In this chapter, the results from the survey have been presented. Whilst a detailed discussion
and interpretation of the findings are presented in the next chapter, the overall results suggest
that a direct and positive relationship exists between supply chain context factors and
management accounting system design in the SCM of Ghana’s healthcare context, and that the
management accounting function fully mediates the relationship between supply chain
management and performance. For effective and efficient management of the health supply
chain, a consideration of the fit between the four MAS information characteristics (broad scope,
timeliness, integration, and aggregation) and SCM contextual antecedents namely, strategic
supplier partnerships, supply chain integration, levels of information (or knowledge) sharing,
and the risk and uncertainty dimensions (or environmental uncertainty) are highly critical.
It has also been established from the results that the performance impacts of the management
accounting function in the health supply chain is moderated by the four supply chain
management context factors. In this regard, the performance impacts of the management
accounting function are expected to be high for hospitals that maintain a high level of supplier
relations and knowledge dissemination among members in the supply chain but experience
shortfalls in performance for low levels of supplier relationships and information availability.
With regards to risk and uncertainty in the supply chain, high performance was found to be
associated with unfavourable environments and hence hospitals in unfavourable environments
are likely to have high levels of supply chain integration compared to those in favourable
environments.
University of Ghana http://ugspace.ug.edu.gh

202
CHAPTER SEVEN
DISCUSSION AND INTERPRETATION OF FINDINGS
7.1 Introduction
This study provides preliminary empirical evidence on the contingency fit relationships
between SCI (external and internal integration), level of information sharing, supply chain risk
and uncertainty and four dimensions of MAS information that can leverage various dimensions
of hospital supply chain performance. The study uses empirical data from healthcare
institutions in Ghana. In the preceding chapter, the survey analysis and results relating to the
study variables were presented. In this chapter, the interpretation and discussion of the findings
associated with the survey results are presented. The chapter is made up of three sections. The
first section discusses and interprets the findings associated with the contingency fit
relationships between the constructs. The second section discusses the effect of the MAS
construct as a mediating variable. The final section discusses the interacting effect of the SCM
contextual antecedents and the MAS information characteristics on hospital SC performance.
All discussions and interpretations are expressed within contingency’s theory applications in
organizational design. The chapter ends with a summary.
7.2 Recap of Research Objectives, Questions and Hypotheses
As stated in chapter one, this study design seeks to achieve three main objectives; that is to:
1. Investigate the ‘selection fit’ relationships between SCM contextual antecedents and
MAS information characteristics among hospitals in Ghana.
2. Examine the mediation effect of the MAS construct to leverage hospital supply chain
performance in Ghana.
University of Ghana http://ugspace.ug.edu.gh

203
3. Examine the performance implications of the moderation effect of the SCM contextual
antecedents on the relationship between MAS design and HSC performance.
7.2.1. Research Questions
The three research questions that underpin the study are as follows.
1) Do the MASs designed and used by healthcare institutions in Ghana ‘fit’ (or align with)
the SCM contextual antecedents that characterize Ghana’s health supply chain?
2) To what extent do the MAS information used in Ghana’s healthcare management
systems offer a mediating role between the antecedent conditions and performance
effects of the hospital supply chain?
3) To what extent do the health SCM context factors offer a contingency effect on the
relationship between the MAS and hospital supply chain performance
7.3 Fit between SCM and MAS Information Characteristics
This section discusses and interprets the findings associated with the fit between the contextual
factors of SCM and MAS information characteristics. The study finds a direct and strong
positive association between the supplier integration and each of the four dimensions of the
MAS information. The findings which support hypotheses H1(a), H1(b), H1(c), and H1(d)
suggest that the information characteristics (dimensions) of the MAS (i.e. scope, timeliness,
aggregation, and integration) are useful and highly relevant to supplier relation decisions in
healthcare context. In other words, strategic supplier relations (external integration) strongly
influence the design and implementation of MAS information in hospital SCM decisions. The
findings support that of Ou, Liu, Hung, and Yen (2010) who examined the interactions among
SCM practices and their effect on firm financial performance. Specifically, they reported
findings of the relationship between SCM contextual factors such as external supplier,
University of Ghana http://ugspace.ug.edu.gh

204
customer integration and various dimensions of supply chain performance. They found external
supplier relations to positively impact the internal contextual factors of a firm which in turn
impact positively on firm financial performance. In the following four subsections, a discussion
of the findings related to each of the four SCM dimensions is given.
7.3.1 Strategic Supplier Partnerships (External Integration) and MAS Information
With respect to the fit between strategic supplier partnerships (external integration) and MAS
information, the results show a perfect alignment between the test variables. This suggests that
supplier relations influence MAS design in Ghanaian hospitals. MAS design in healthcare
should consider aligning the characteristics of supplier relationships with the MAS information
characteristics for optimal performance. This is because an effective supply chain strategy
aligns an organization’s performance priorities and objectives and those of its suppliers
(Selviaridis & Spring, 2018). This finding is consistent with that of Harlez and Malagueno
(2016) who documented that the benefits of the alignment between strategic priority choices
of partnerships in managing a hospital’s boundary-spanning activities and the application of
performance management systems (i.e. MAS) in hospitals are positively related. They further
established that a higher emphasis on partnerships or governance strategic priorities leads to
greater positive effect on the interactive use of performance management systems on hospitals.
It is less associated with managers with administrative background than top-level managers
with clinical background.
In another dimension, Guimaaraes and de Carvalho (2013) who examined the notion of
strategic outsourcing in the context of lean thinking inside and beyond healthcare
organizations’ boundaries in extended supply chains found a perfect alignment (or fit) between
SCM notions in healthcare and the application of lean tools. Although not the same SCM
University of Ghana http://ugspace.ug.edu.gh

205
features as in the current study, the finding on supplier strategic relations obtained in the current
study supports and falls in line with that of Guimaaraes and de Carvalho (2013).
The findings also complement the findings of the intra-strategic fit studies conducted by Pizzini
(2006) and Macinati & Anessi-Pessina (2014) in US Private and Italian National hospitals
respectively. Both studies found a direct positive association between strategy and MAS
design. Pizzini (2006) found that cost containment strategies encourage more sophisticated
MAS design while Macinati and Anessi-Pessina (2014) found organizational strategy to
directly influence MAS design. Bouwens and Abernethy (2000), Abernethy and Lillis (2001)
investigated the relationship between strategy and MAS design in hospitals where the MAS
was operationalized by the four dimensions: scope, timeliness, aggregation and integration and
found that the four dimensions of the MAS information are highly suitable for hospital
operations.
Relating the current findings to these prior literatures suggests that the successful design and
implementation of MAS information in hospital SCM systems is affected by the MAS-strategy
fit relationships or the alignment between the MAS information and organizational strategy,
and that organizational strategies (whether internal or external) are critical to the design of
MASs in hospital supply chains. The findings also suggest that the contingency-structure
combinations on strategy can be extended from the intra-organizational domain to the inter-
organizational partnership domain in healthcare setting. It shows that any misfit (or
misalignment) between the MAS information and strategic choices of supply partners within
the SCM context could result in lower outcomes normally some aspects of performance in
terms of inefficient allocation of resources, delay or extended delivery, interruptions or supply
shortages, high costs, etc. For example, the findings are in perfect line with those of Bedford,
Malmi and Sandelin (2016) who found that accounting control (i.e. MAS) and structural control
choices’ effectiveness are determined not only by their fit with strategic context but also by the
University of Ghana http://ugspace.ug.edu.gh

206
extent to which they fit with each other. In general, the findings extend previous works by
providing empirical evidence on the use of MAS information in the hospitals and strategic
choices within the hospital SCM context.
7.3.2 Supply Chain Integration (Internal Integration) and MAS Information
The study finds a statistically significant strong positive support for hospital SCI (internal
integration) with accounting information scope and aggregation but finds no statistical
relationship with timeliness and integration of the accounting information. This finding
suggests that hospital internal integration partially fits the MAS information characteristics. In
particular, there is a misalignment between hospital SCI (internal integration) and MAS design.
There are weak collaborations of procurement, warehousing and distribution of medical
products as well as weak cross-functioning and collective responsibility across functions. This
finding is consistent with the findings of Asamoah et al (2011) who found SCI (internal
integration) as a key challenge within the pharmaceutical supply chain in Ghana. Internal
integration integrates supplier relations, information sharing and risks; hence, an important
dimension of the SCM construct.
This finding is highly inconsistent with existing SCM studies. For example, Ataseven, and Nair
(2017) found in their meta-analytic study, a perfect match between the three dimensions of
integration and various dimensions (cost, speed, flexibility and quality) of supply chain
performance. Although not in line with prior literature, internal integration is critical to the
efficient functioning of the hospital supply chain. Supply chain managers in Ghanaian hospitals
can minimize costs, improve speed of delivery, enhance quality assurance and operate a much
more flexible supply chain for well-integrated SCM components. The findings also did not
support that of Chen et al (2013) who found a positive association between supply chain
integration and various facets of supply chain performance measures. The findings also fall
University of Ghana http://ugspace.ug.edu.gh

207
outside the findings of Behesti et al (2014) who investigated the financial performance impacts
of supply chain integration on Swedish manufacturing firms and found that a strong and
positive relationship exists between supply chain integration and firm financial performance.
They established that any level of supply chain integration in an organization results in
performance enhancements and is highly beneficial to the financial well-being of the firm.
They reported further that the highest level of financial performance was reported by
companies with total supply chain integration. Hospitals in Ghana must consider aligning their
MASs with internal integration for optimal performance.
7.3.3 Level of Information Sharing and MAS Information
Like internal integration, the results for the level of information sharing show no statistically
significant effect on any of the four dimensions (scope, timeliness, integration and aggregation)
of the MAS design. This is true because information sharing is highly associated with internal
integration. The results suggest that hospitals is Ghana might either be using too many MASs
(e.g. too many performance measurement indicators or systems) or too few MASs (e.g. too few
measurement diversity); and it supports contingency theory that either excessive or insufficient
use of the MAS relative to the contextual factor will result in misalignment and negatively
affect performance. That is either the sharing of SC information is excessive or insufficient
among healthcare institutions in Ghana. This result is again inconsistent with prior studies
although decisions on information sharing strongly align with the MAS information
characteristics to positively affect performance. For example, the findings of Mahama (2006)
showed that a direct and positive association between the MAS information represented by
performance measurement systems and information sharing exists in a study that investigated
the relationship between two MAS information and cooperation in strategic supply
relationships. He also found information sharing to be indirectly associated with performance
measurement systems. Information sharing is a critical aspect of hospital SCM because of the
University of Ghana http://ugspace.ug.edu.gh

208
complexity and sophisticated nature of clinical operations. Hospitals have weak information
linkages possibly due to lack of IT integration. However, whilst this finding does not support
most existing literature, it is in perfect alignment with Asamoah, Abor and Opare (2011) who
find weak SCI and information sharing to be the main threat of the pharmaceutical SC although
they measured integration as one construct suggesting that both external and internal
integration are weak in Ghana’s healthcare management. The reason for the findings not
supporting most existing works could possibly be due to the fact that those studies were based
on samples drawn from the developed countries where they have well-structured SCM
environment. Hospitals in Ghana need to put in place mechanisms that will enhance
information sharing to leverage performance.
7.3.4 Supply Chain Risk and Uncertainty and MAS Information
The results show a statistically positive relationship with all the four dimensions (scope,
timeliness, integration and aggregation) of MAS. The risk and uncertainty dimensions of the
supply chain has mostly been examined in management accounting literature in the context of
trust existing between supply chain partners (e.g. Langfield-Smith, 2008; Tsamenyi, Qureshi
& Yazdifar, 2013; Dekker et al, 2013). Hence, the terms risk, trust and environmental
uncertainty are used interchangeably. This makes the findings on the fit between MAS
information and supply chain risk fall in line with a number of management accounting –
supply chain risk studies. Dekker et al (2013) investigated the extent to which firms employ
MAS information to manage risks associated with supply chain partners engaged in intensified
collaborations. More specifically, they examined the extent of the MAS information as well as
multiple interrelated SCM control practices impact (through the selection of supplier partner
in the context of perceived goodwill and competent trust), on inter-firm transactions risk.
University of Ghana http://ugspace.ug.edu.gh
209
The study finds a statistically significant positive association between the very basic
fundamental risks associated with transaction characteristics and collaborated trusted suppliers
and the application of management control systems (MCS) to manage relationships. The
findings also add to the literature of Grotsch, Blome, and Schleper, (2013). They examined the
antecedents that foster proactive supply chain risk management implementation from a
contingency theory perspective and found a positive association between a mechanistic MAS
and proactive supply chain risk management implementation suggesting a alignment between
the MAS information characteristic and the antecedent condition of SCM risk.
7.4 Interpretation of the MAS Mediation Effect
In this section, the mediating effect of the MAS on hospital SC performance is presented. First,
the findings relating to the performance effects of the confounding variables (size, location,
profit status, and ownership) on hospital SC performance are discussed.
7.4.1 Confounding Variables and Hospital Supply Chain Performance
As the results indicated, the geographical location and profit status of the sample hospitals were
found to be statistically significant and hence influence hospital supply chain performance. The
other two variables (ownership and size) were found not to be statistically significant both
under the mediating and non-mediating conditions of the MAS construct. The findings are
consistent with that of Chen et al (2013) who controlled for several confounding variables in
their structural model including hospital size (measured by a variety of proxies: number of
beds, employees, discharges, patients, and patient revenue), purchasing department size,
location (urban/rural), and profit status for a sample of 117 US hospitals.
Only the location and profit status of the 117 hospitals sampled were found to be statistically
significant. The findings also support the findings of Macinati and Anessi-Pessina (2014) who
University of Ghana http://ugspace.ug.edu.gh

210
controlled for the effect of hospital size on hospital financial performance in their model but
found the results to be statistically insignificant. Based on the current findings and those of
prior literature, it can be concluded that location and profit status play critical roles in hospital
supply chain performance. In SCM, the siting or location of a facility is a strategic decision
which impacts significantly on its supply chain activities and hence performance. In hospital
settings, location may positively or negatively affect the flow of customers (patients) to the
hospital as well as distribution of medical products.
One of the key variables of performance measurement is profit hence, organizations with profit
status which comprised the private sector are likely to outperform non-profit organizations
which comprised mainly the public sector. This is because government hospitals are labelled
as non-profit oriented although they generate revenue. This could be one of the reasons for the
high costs associated with the procurement, warehousing, and distribution activities of the
health supply chain resulting in high costs of health products at the pharmacy level for the end
user which is under the oversight responsibility of the MOH. The notion of non-profit status
does not allow for cost-containment strategies to be adopted by the MASs employed in these
organizations compared to private hospitals.
7.4.2 Mediating Effect of MAS on Performance
Although SCI (internal and external integration) was statistically insignificant, the MAS
recorded a partially mediating effect on performance. The findings suggest that the
characteristics of the MAS information is useful for hospital SCM decisions. Consistent with
Abernethy and Lillis (2000), Pizzini (2006), Hammad et al (2013), and Macinati and Anessi-
Pessina (2014) who found a statistically positive association between hospital organizational
context factors and MAS information scope, timeliness, integration and aggregation, the results
suggest that the four characteristics of MAS information are relevant to hospital SCM. Pizzini
University of Ghana http://ugspace.ug.edu.gh

211
(2006) documents a positive association between perceived usefulness of cost data and the
dimensions of MAS information in a survey of 277 US hospitals. These dimensions are
operationalized by the extent to which the system can provide greater cost detail, classification
of costs according to behavior, and the frequency in which cost information are reported. This
operationalization exactly falls in line with Chenhall and Morris’s (1986) conceptualization of
MAS information characteristics of scope, timeliness, aggregation and integration. As in past
studies, the findings contribute to further development of integrative contingency framework
that explains the dimensions of MAS investment in the SCM field.
7.4.3 Joint Effect of MAS and SCM on Hospital SC Performance
The findings related to the joint effects of the MAS information dimensions and the SCI, level
of information sharing, and supply chain risk and uncertainty on hospital SC performance are
now considered. The empirical results highlight the value of the SC context factors and the
dimensions of MAS information as severely underpinning hospital external integration,
internal integration, information sharing and uncertainty to leverage hospital supply chain
performance. The results suggest that the design and use of MAS information is central to
achieving greater hospital SC performance in terms of costs, flexibility and speed, quality and
asset utilization.
The results show some consistencies with contingency theory since the findings indicate that
hospital-supplier partnerships, level of information sharing and risk and uncertainty have direct
and positive influence on MAS design. The findings reveal several sets of interesting mediating
relationships from strategic supplier partnerships, level of information sharing, and supply
chain risk and uncertainty to hospital SC performance through MAS information. In all these
mediating relationships, the study finds MAS design to partially mediate the influence of
hospital SCM on hospital SC performance. These findings are consistent with the findings of
Chen et al (2013) who showed that a direct and positive relationship exists between hospital-
University of Ghana http://ugspace.ug.edu.gh

212
supplier knowledge exchange and the level of hospital-supplier integration from their sample
of 117 US hospitals. In addition, they observed interesting mediating relationships flowing
from knowledge exchange to hospital SC performance through hospital-supplier integration.
In the further analysis, the results indicated positive indirect effects flowing from each of the
supplier relations, internal integration, information sharing and risk and uncertainty through
the second-order SCM construct to hospital SC performance. The study finds the strategic
supplier partnership variable to be statistically significant and positively associated with SC
performance. This finding provides important insights of the supplier partnership as a strategic
factor in enhancing hospital SC performance in terms of reduced cost, flexibility, and quality
of health products. Lee, Lee, and Schniederjans (2011) in their analysis of the impact of SC
innovations on hospital performance among Korean hospitals showed a direct positive
association between supplier partnerships and organizational performance. They show
empirically that supplier cooperation (or strategic supplier partnerships) is an important
element that underpins the innovations related to better value to customers (patients) through
reduced costs and improved product quality and services along the SC. They show further that
a statistically significant relationship exists between hospital supplier cooperation, SC
innovation, and hospital performance in terms of waste reduction, quality, and cost
minimization.
7.4.4 Mediating Role of the MAS Information Dimensions
The study finds the MAS information characteristics to partially mediate the relationship
between supplier relations (external integration), information sharing, risk and uncertainty and
hospital SC performance but an insignificant relationship between internal integration. This
suggests that the results provide some support for an indirect effect of the three SCM constructs
on hospital supply chain performance, acting through the use of optimal amounts of MAS
University of Ghana http://ugspace.ug.edu.gh

213
information for decision making. These findings strongly align with the findings of Hammad
et al (2013) who found the four dimensions (scope, timeliness, integration, and aggregation) of
the MAS information to significantly play an intervening role in the relationship between
decentralization and perceived environmental uncertainty on managerial performance in the
context of Egyptian hospitals.
Their study design which was a contingency-based intervening model showed that the type of
MAS information designed and used by hospitals in Egypt is strongly influenced by the
environment in which they operate. In addition, the findings strongly fall in line with that of
Soobaroyen and Poorundersing (2008) who, by investigating the availability and effectiveness
of MAS information for functional managers in manufacturing firms in Mauritius, found the
available MAS to play a significant intervening role in the relationship between task
uncertainty and decentralization on managerial performance. Like the current study, their study
design was also based on the four dimensions (scope, timeliness, integration, aggregation) of
the MAS developed by Chenhall and Morris (1986) and used a contingency-based intervening
model to examine the intervening role of the MAS information characteristics between task
uncertainty and decentralization on managerial performance.
The findings in a way also complement the findings of Macinati and Anessi-Pessina (2014)
who used covariance based structures to investigate the extent to which contextual variables
influence the design and use of MAS, and the financial performance effects of their
relationships in the Italian National Health Service. They found both MAS design and its usage
to be respectively, directly and indirectly influenced by organizational, contingency, and
behavioral variables. In addition, they found the use of MAS in pursuance of cost containment
strategies in the Italian hospitals to be encouraged by the mediating role of MAS design. They
however, found the existence of a statistically significant weak positive relationship between
MAS use and financial performance.
University of Ghana http://ugspace.ug.edu.gh

214
Linking the current findings to those findings of prior studies suggests that both the design and
use of MASs mediates the performance effects of contextual variables in healthcare setting. It
can be theorized in health inter-organizational relations in supply chains that effective design
and implementation of MASs in healthcare management enhance SCM variables’ impact on
supply chain performance. In this regard, the technical advancement of MAS design as well as
thorough understanding of its usage by users in healthcare inter-organizational management is
critical if the performance effects of the MAS designed and used in such institutions are to be
realized. An appreciation of the qualities and full exploitation of the potentials of the MASs
designed and used in healthcare institutions by managers is critical. Turning to the study by
Gerdin (2005a), the findings confirm that there is an indirect association between inter-
dependence and subunit performance through a greater amount of MAS information use for
decision making using a survey of 132 production managers.
7.5. Contingency Effect of SCM on Performance
Positioning external integration, internal integration, information sharing and risk and
uncertainty as contingency variables, the sample data confirmed the moderating effects on
hospital SC performance, hence supporting contingency theory. The study also offers empirical
evidence for statistically significant positive associations of aggregate performance with each
of the four SCM context factors. The results show the SCM dimensions and the four
dimensions of hospital SC performance having positive associations, hence supporting H6a,
H6b, H6c, and H6d. This result matches that of Ataseven and Nair (2017) who found a
statistically significant positive association between supply chain aggregate integration and
aggregate performance, where aggregate integration relates to the three facets of integration
University of Ghana http://ugspace.ug.edu.gh
215
(supplier integration, internal integration, and customer integration) and aggregate
performance relates to cost, flexibility, speed, and quality of the supply chain.
The findings as obtained in the current study are based on tests conducted in two separate
scenarios. In the first scenario, all main effect variables were included in the model and tested.
The results showed a statistically significant moderating effect for the cross-product term but
showed a statistically insignificant effect of the main effects signifying that the SCM context
factors strongly interact with the dimensions of the MAS information to affect hospital SC
performance. In the second scenario, only the cross-product terms were tested. The results
showed a statistically significant moderation effect on the relationship between SCM context
factors and hospital SC performance. The results support the findings of Grotsch et al (2013)
who found that the relationship between mechanistic MAS information and SC proactiveness
is moderated by SC risk management implementation. Wong et al (2011) also found perceived
environmental uncertainty to moderate the relationship between SCI (external and internal
integration) and performance. The findings support several prior literatures on the moderating
role of SCM on performance hence supporting contingency theory (Flynn et al, 2010; Wong et
al, 2011; Chen et al, 2013; Ataseven & Nail, 2017; Qi et al, 2017).
7.6 Implications of Findings
Beginning with contingency theory’s claim that the product of the relevant contextual
dimensions determines effective managerial performance this study examined MAS
information characteristics in relation to the contingency factors of hospital supply chain
management. The findings suggest several theoretical and practical as well as policy
implications for researchers, practitioners, hospital managers (or administrators) and policy-
makers. This section discusses the implications of the findings and is classified under three
University of Ghana http://ugspace.ug.edu.gh

216
subsections comprising the theoretical, practical and policy implications with respect to
researchers, practitioners (hospital managers/administrators) and policymakers.
7.6.1 Theoretical Implication
Judging from the combined findings from the SCM dimensions on the four dimensions of
performance, it can be theorized that a perfect alignment of the hospital SC with the MAS
information is more likely to provide a broad range of performance benefits for hospitals in
Ghana. That is a high level of SCI (external and internal integration), information sharing, and
high knowledge about risk and uncertainty among healthcare institutions in Ghana is likely to
reduce supply chain cost, improve speed, flexibility, and quality of the supply chain as well as
result in the efficient usage of hospital assets. This theorization holds as these dimensions of
the SC encapsulates all the other SCM contextual dimensions.
Also, compared to the other contextual dimensions, supply chain integration is
multidimensional consisting of supplier integration, customer (patient) integration and internal
integration. Further division of each of the three dimensions of integration shows that
information sharing between suppliers and customers play a significant role in enhancing
supply chain performance. Also, the findings have important implications for management
accounting research. The findings of this study suggest the observance of carefulness and
special attention in the development and testing of contingency hypotheses by researchers.
7.6.2 Practical Implications
Like the case of researchers, the results offer important practical implications for practitioners
who are engage in MAS design in healthcare institutions. From an inter-organizational
perspective, the four dimensions of the MAS information were found to strongly align with (or
fit) the contextual dimensions of hospital SCM. The findings suggest the essence for
practitioners and designers of MAS information in Ghana’s healthcare institutions to focus on
University of Ghana http://ugspace.ug.edu.gh
217
the four attributes of scope, timeliness, integration and aggregation of the MAS information.
Based on the intervening mechanism role exhibited by the dimensions of the MAS information,
the results indicate that effective implementation of SCM decisions requires the use of optimal
amounts of MAS information.
Designers of MAS information in hospitals should ensure that optimal amounts of MAS
information are not only available to SC managers and practitioners, but also accessible to
managers in the SCM department for performance enhancements. The findings highlight the
importance of hospital SC managers maintaining strong ties with key suppliers to ensure
proactive SCM. This is true for relational governance which fosters close information (or
knowledge) exchange as well as building trust. Information sharing has been found to be a key
enabler of proactive SCM. In addition, and from an inter-organizational viewpoint, this study
finds a statistically significant connection between the existence of supply chain risk and
uncertainty and MAS information characteristics.
These results demonstrate that SCM departments in hospitals will be eager to get rid of a
supplier becoming insolvent once a full commitment has been made to that supplier. There is
also the risk of losing specific investments in supplier – relations and the danger of losing
important capabilities and subsequent competitive advantage by switching suppliers. This
reinforces the importance of pursuing proactive supply chain risk management practices by
SCM departments. Careful supplier selection, and risk-reward sharing contracts by hospitals
are some of the proactive measures that can be instituted to mitigate supply chain risks. On the
whole, the findings suggest the need for hospital managers to target appropriate dimension(s)
of hospital SC performance that suits the competitive priority. The results suggest further that
by focusing on the relevant SCM contextual dimensions, the identified dimensions of the
hospital SC performance can be improved via the SCM dimensions with which they are
associated with so that the resources of the organization can be effectively utilized.
University of Ghana http://ugspace.ug.edu.gh

218
7.6.3 Policy Implications
Although the study finds a fit (or match) between the contextual dimensions of SCM and the
four dimensions of the MAS information, these relationships are based on the selection,
moderation and mediation models of fit which in comparison to the other contingency models
of fit (matching fit model), are theoretically incompatible (Luft & Shields, 2003; Chenhall,
2003; Gerdin & Greve, 2004; Hartmann, 2005; Burkert et al, 2014). What this suggests to mean
is that the design and use of MAS information is predicted and explained in response to the
MAS context where causal relations between contextual variables of SCM and MAS
information characteristics are sought.
The implication is that the design and use of particular MAS information characteristics is more
effective if accomplished by the so-called selection forces that characterized the selection fit
concept. In other words, the causality of the SCM context variables – MAS information
characteristic relationship is theoretically argued to root in an optimization process (i.e.
selection forces) that results in MAS – context ‘fit’. Rather than imposing a particular MAS
design and using it in the healthcare sector particularly those in the public sector, policymakers
should allow practitioners in these settings to both theoretically and empirically select their
MAS design or use to ‘fit’ their level of (or congruence with) supply chain complexities and
sophistication. In other words, hospitals should be allowed to adapt their MAS to the full
demands of their contexts.
7.7 Chapter Summary
In this chapter, the discussions and interpretations associated with the survey analysis have
been presented. The discussions show that the sample data supports three models of
contingency fit – the selection, mediation and moderation forms of fit. It highlights the
University of Ghana http://ugspace.ug.edu.gh

219
consistencies and alignments or complementarities of the study’s findings with those of prior
literature, thereby adding to the body of knowledge and understanding of contingency-based
management accounting studies. It also demonstrates the extent to which the contingency
paradigm fits in the external domains of the Ghanaian healthcare industry as a significant
contribution to literature. The chapter also highlighted the theoretical, practical, and policy
implications of the findings as they relate to management accounting researchers, practitioners
and designers of MAS information in healthcare institutions and policy-makers respectively. It
concludes that both researchers and practitioners as well as policymakers have specific roles to
play in testing of contingency hypotheses, designing of MAS information and the selection of
MAS information dimensions respectively in the healthcare context. In the chapter that follows,
a summary of key findings, conclusions and contributions of the thesis are presented.
University of Ghana http://ugspace.ug.edu.gh

220
CHAPTER EIGHT
SUMMARY, CONCLUSIONS AND CONTRIBUTIONS
8.1 Introduction
Following the survey results presented in chapter seven and subsequent discussion and
interpretation of the findings in the preceding chapter, the summary, conclusions and
contributions arising from the findings are presented in this last chapter of the thesis. The
chapter presents the summary of the key findings, conclusions drawn from the findings, and
the contributions arising from the study. Like any empirical work, this research design is not
without limitations. Subsequently, the limitations and weaknesses associated with the study are
presented next whilst avenues for further studies or future research directions draw the curtains
on this chapter.
8.2 Summary of the Study
In this section, the summary of the thesis in terms of the research framework (or main thrust)
and the key findings is presented. It summarizes the thesis in terms of the research problem,
underlying motivation through methodology and key findings.
8.2.1 The Study’s Main Thrust
The SC is being increasingly recognized as a key driver that contributes to overall operational
and organizational performance of both profit and non-profit-oriented organizations (Maestrini
et al, 2017; Jin, Jeong & & Kim, 2017). This wide recognition is based on the significant impact
it has on a company’s financial cycle; hence, interacts with accounting information to leverage
performance. SC performance has become one of the most important and critical areas for the
CEOs and executive leaderships of hospitals (Barlow, 2010c) since improvement upon
University of Ghana http://ugspace.ug.edu.gh

221
efficiency and cost reduction strategies has been a challenging issue in hospital management
(Abernethy & Brownell, 1999; Abernethy & Lillis, 2001; Pizzini, 2006; Abernethy et al, 2007).
Hence, improvements in hospital SC performance has increasingly gained importance as
healthcare organizations strive to improve operational efficiency and to reduce costs (Chen et
al, 2013). In this regard, the design of accounting information systems to enhance SC
performance has become a contemporary issue in management accounting research since the
MAS information not only reduces SC cost, but also creates value to maximize shareholder
wealth and economic sustainability. Several calls have been made by management accounting
scholars to: 1) develop new forms of the MAS information that extends beyond organizational
boundaries in supply chains, 2) depart from a manufacturing corporate focus to the notion of
SC as an entity and, 3) establish relevance within SCM and networking (Burritt & Schaltegger,
2014; Dekker, 2016; Otley, 2016).
Given that there has been large amounts of research on the relationship between MAS
information characteristics and SCM attributes which were predominantly informed by the
TEC, these studies failed to link the MAS information characteristics to SC performance
although the link between SCI and SC performance has been explored extensively in the
literature. There is thus, little systematic evidence on studies that examine the performance
impacts of MAS design on SC performance. This thesis fills this gap using contingency theory
since the TEC emphasizes fit in the transactional context (or external), and neglects the
dimensions of internal fit (e.g. internal integration) of the supply chain which relates to cost of
inventory management and warehousing, product quality and production cost. Contingency-
based research underpins the design and implementation of MAS information effectively in
organizations, and the contingency implications for organizational performance. In addition,
whereas prior works researched the organizational contextual variables that influence the MAS
information characteristics to leverage performance, they focused exclusively on the intra-
University of Ghana http://ugspace.ug.edu.gh

222
organizational domains of the contingency application in MAS design. Consequently, studies
that examine the contingency-MAS application in the inter-firm exchanges domain in the
supply chain remain largely underdeveloped. Also, research on the MAS-SC relationship has
received much attention in mainstream discrete parts manufacturing and consumer goods
entities with little attention given to service-oriented organizations where more sophisticated
MAS information is required for managerial decisions.
The sophisticated level (or nature) of the MAS information has also been noted to be relatively
more associated with (or pronounced) in healthcare institutions due to the complex, multi-
functional, and information-intensive environments that characterize their operations, and the
significant proportion of operation costs that are absorbed by supply and logistic-related
expenditures (Schneller & Smeltzer, 2006). However, whereas cost-containment strategies
even encourage more sophisticated MAS design and use in the healthcare context, there is little
systematic evidence on its use and benefits (Macinati & Anessi-Pessina, 2014). To this end,
prior research in management accounting have called for research that provides more
understanding and insights into MAS design and use in healthcare institutions (Bai et al, 2010;
King & Clarkson, 2015). To contribute to bridging these gaps, this study empirically
investigated the contingency fit relationships between MAS information characteristics and
SCI (external and internal integration), level of information sharing, and supply chain risk and
uncertainty that can leverage various operational dimensions of hospital supply chain
performance in Ghana.
Ghana was selected as the research site because its healthcare SCM system faces challenges of
misfit (or misalignment) hence, experiencing negative performance impacts of its supply chain.
The system has already undergone significant managerial reforms between 2008 and 2012 with
the key objective of improving overall performance of the supply chain in the area of
procurement, warehousing, transportation, inventory management, and distribution of health
University of Ghana http://ugspace.ug.edu.gh
223
products (MOH, 2012). However, the identified gaps as inefficient, ineffective and weaknesses
remain unaddressed and have widened rather than have been bridged. The system currently
reveals ineffective, sub-optimal and significant non-value-added steps in the procurement,
warehousing and distribution of medical products which ultimately results in higher delivery
cost for the end user (Asamoah et al, 2011; Denkyira, 2015). These weaknesses and
inefficiencies have serious implications for the design and use of MAS information. In this
regard, the study provided empirical evidence on the extent to which the design and use of
MAS information relate to hospital SCM contextual conditions and the resulting implications
for hospital managers and health policymakers in Ghana.
Hence the study had three objectives as follows:
1) Provide empirical evidence on the extent to which the design and use of MAS
information ‘fit’ (or aligned) with the boundary-spanning management decisions of
health inter-organizational relations in supply chains to leverage hospital SC
performance in Ghana.
2) Examine the mediation effect of the MAS construct to leverage hospital SC operational
performance in Ghana.
3) Examine the performance implications of the moderation effect of SCI (external and
internal integration), level of information sharing, and supply chain risk and uncertainty
on the relationship between MAS design and hospital SC operational performance.
The study which comprised both theoretical and empirical sections was structured into eight
chapters. Chapter one introduced the study with an outline of the research background and
associated problem identification which has contributed to the study’s underlying motivation.
To this end, the research objectives and questions which were answered through hypotheses
tests were derived. Chapter one also gave a brief definition and discussion of the variables
University of Ghana http://ugspace.ug.edu.gh

224
underpinning the study which comprised the fit relationships between three intersecting
constructs: management accounting systems information, SCM represented by SCI (external
and internal integration), level of information sharing, SC risk and uncertainty, and hospital
supply chain performance. Analysis of the relationship among these variables resulted in the
identification of a number of gaps which motivated this study. Finally, the relevance of the
study and an outline of the logical sequence of the remaining chapters were clearly spelt out.
Chapters two and three were devoted to systematic literature reviews. In chapter two, the
study’s context as well as concept of the health SC in comparison to that of the mainstream
discrete parts manufacturing and consumer goods entities were discussed. Also, the design and
implementation of the MAS information in the SC with a more focus discussion of the
application of the performance implications of the MAS information in hospital supply chain
management was presented.
Chapter three reviewed the theoretical underpinnings of SCM as well as theoretical and
empirical literature on contingency-based management accounting studies. Given that
contingency theory constitutes a major theoretical lens in management accounting research,
and the most widely theoretical approach to the design of MAS information coupled with the
fit concept as its key concept, the study was hooked to this theory as its theoretical lens to
explain the fit relationships between the study variables. However, the review found serious
distortions and non-conformance to the theoretical requirements associated with the various
types of contingency fit models (selection, matching, moderation fit etc.) employed by prior
contingency-based management accounting study designs. In particular, existing studies lack
consistency (or a mismatch) between the formulation of verbal hypotheses, the statistical test
employed and the interpretation of results. Such contingency hypotheses tests seriously
impaired the advancement of theory-consistent management accounting studies.
University of Ghana http://ugspace.ug.edu.gh

225
Chapter four presented the theoretical model and development of the research hypotheses. In
this chapter, a justification for the selection of the study variables and their operationalization
was given. The research model was a modified version of Chen et al (2013) and Macinati and
Anessi-Pessina (2014) which examined the effect of the SCM context factors on hospital
supply chain performance and the MAS information characteristics on hospital supply chain
performance respectively. As a basis to the formulation of the testable hypotheses, the chapter
highlighted the theoretical linkages or showed evidence of empirical linkages between the
study variables. To contribute to the advancement of theory-consistent management accounting
research, it was ensured that the formulated verbal hypotheses align with the contingency fit
models to be tested. Finally, the chapter spelt out the hypotheses that were tested.
Chapter five presented the research methodology. In this chapter, the research design which
was rooted in a quantitative-positivist epistemology was explained. After giving a brief
background of the philosophical assumptions that underpin academic research, the research
design which showed the general approach (or blueprint) to the conduct of the study as well as
the methods and techniques to the collection and analysis of data was captured. The chapter
also highlighted details of the study population, sample composition, and the sampling strategy
adopted. Also, a discussion detailing the data collection instrument and the sources and
development of the adapted scales was presented. The requirements of the construct items or
indicators which comprised the questionnaire that was administered to respondents
(accountants, hospital managers/administrators) was assessed in terms of being reflexive rather
than formative. The chapter gave a further discussion to the techniques of data analysis and the
estimation model which involved mainly covariance-based structural equation modelling.
Included in this discussion was a detailed analysis of the modelling process and the assessment
of model fit between the structural model and the sample data based on goodness-of-fit
statistics.
University of Ghana http://ugspace.ug.edu.gh

226
It was shown that the modelling process which was based on AMOS graphics comprised a
measurement part and a structural part. The measurement part tested the adequacy of reliability
and internal consistency of the observed variables while the structural part tested the
relationship between the constructs.
Chapter six presented the survey analysis and results while chapter eight discussed and
interpreted the findings. In chapter seven, the results of the survey data were presented. First,
the findings relating to the preliminary analysis of the sample data were documented. This
involved tests of normality, outliers, skewness and multivariate kurtosis. Other preliminary
analysis includes tests of reliability, composite reliability, internal consistency, and average
variance extracted (AVE). The chapter also presented as part of the preliminary analysis,
sample means and standard deviations for continuous variables and frequency distribution for
the nominal variables. Second, the results relating to the factor analytic models for all the test
variables and their factor loadings signifying reliability were presented. Included in these
results is the goodness-of-fit indices (or statistic) which assess the adequacy of model fit
between the sample data and the hypothesized model. Finally, the results involving the fit
relationships, performance, mediating and moderating effects of the study variables were
captured.
In chapter seven, a detailed discussion and interpretation of the findings was given. The
discussions were done in the context of the findings relating to existing studies as to whether
the findings support or deviate from those of prior literature. The conclusions, summary of
findings and potential contribution to literature are presented in chapter eight (this chapter). In
this chapter, the key findings of the survey analysis are presented. The survey analysis relates
to the fit relationships, mediating role of the MAS information and the moderating effect of the
SCM context factors on Hospital SC performance.
University of Ghana http://ugspace.ug.edu.gh

227
8.2.2 The Study’s Main Findings
First, the findings revealed the importance and relevance of the contingency fit relationship (or
alignment) between SCI (external and internal integration), level of information sharing, and
supply chain risk and uncertainty of healthcare SCM practices and the four dimensions of the
MAS information in enhancing hospital SC performance. Specifically, decisions on supplier
relations, information sharing (or knowledge exchange), risk and uncertainties associated with
the supply chain, and hospital supply chain integration were found to strongly correlate (or
align with) the four dimensions namely, scope, timeliness, integration and aggregation of the
MAS information.
The findings suggest the strong and positive influence of the four dimensions of SCM practices
on the design, implementation as well as performance implications of MAS information in the
Ghanaian healthcare SCM decisions. As strong positive associations were found to exist
between these SCM context factors and the MAS information dimensions, it supports the
selection, mediation and moderation fit models of contingency theory although SCI and level
of information sharing was not statistically supported in the selection and mediation fit models.
The findings suggest that the scope dimension of the MAS design which relates to external,
non-financial, and future-oriented information strongly support decisions on hospital SC
management practices in Ghana. It further suggests that such information must fit (or align
with) the decision needs of supplier relations, information dissemination and risk-taking in
uncertain environments to integrate the entire health SCN. Such information must also be well-
aggregated in terms of time and frequency of delivery, and interrelationship with subunits and
possess precise targets for activities. Second, the study establishes the fact that hospital
geographical location and profit status do play significant roles in the management of HSCs.
On the other hand, ownership in terms of government-owned or private-owned do not play any
role in enhancing performance of the hospital SC.
University of Ghana http://ugspace.ug.edu.gh

228
Third, the study documents performance impacts of the hospital SC by SCI (external and
internal integration), level of information sharing, and supply chain risk and uncertainty in two
separate scenarios: 1) the presence and 2) absence of the MAS variable as a mediator. In the
former scenario, the significance of SCI was not supported by the sample data. The remaining
three SCM context factors were found to have a positive impact on hospital SC performance
which consists of cost effectiveness, utilization of hospital assets, speed and flexibility of
delivery, and supply chain quality. The non-significant results of the SCI widely support the
findings of Asamoah et al (2012) who found SCI to be weak in Ghana’s pharmaceutical SCM
system. In the latter case, none of the context factors were found to be statistically significant
and hence had no relationship with hospital SC performance. From these results, the study
establishes the fact that the four dimensions of the MAS information serve as strong intervening
mechanisms between the four SCM context factors and hospital SC performance. Stated
differently, the MAS information partially mediates the relationship between the four
dimensions of the supply chain and HSC performance. This finding also supports the mediation
fit model of contingency theory.
Fourth, the study finds the establishment of a MAS-contingency interaction framework within
the inter-organizational domains in supply chains, where the performance effects of the
interaction between SCI, level of information sharing, and SC risk and uncertainty and the
MAS information characteristics on hospital SC is established. These findings strongly support
the moderation fit model of contingency theory in inter-firm exchanges. Given that both the
main effects and the cross-product term in an interaction can result in a statistically significant
coefficient for interaction effect to be supported and interpreted, it has been argued (Hartmann
& Moers, 1999) that all main effects comprising an interaction must be included in the model
when testing for interaction.
University of Ghana http://ugspace.ug.edu.gh
229
This is a necessary condition to satisfy in order to avoid the situation where a statistically
coefficient of interaction is interpreted even though the interaction is due to a significant
relationship between the main effect variables. As noted in chapter three, this argument is
stressed in Stone and Hollenbeck (1984, p. 201) which states that the cross-product term may
not be the interaction even though it carries the interaction term in a regression equation. This
suggests a ‘partialed out’ of the lower-order (or main) effects when an interaction effect is
being tested by including them in the model.
Following these arguments, two models of interaction were tested: one that excludes the lower-
order effects and the other that includes the lower-order effects. In the former, a statistically
significant coefficient was found for all the cross-product terms suggesting that the SCM
context factors interact with the dimensions of the MAS information to affect HSC
performance. In the latter case where all lower-order effects were included in the model, only
the cross-product terms were found to be statistically significant although there was a reduction
in the coefficient values. The main effect variables were however found to be statistically
insignificant, again suggesting that the MAS information characteristics strongly interact with
the SCM contingent variables to affect HSC performance.
Based on these empirical evidence, three key findings were found to be associated with the
moderation tests. First, the study finds that the design and use of the MAS information
operationalized by the four dimensions (scope, timeliness, integration and aggregation) will
have a positive/greater impact on hospital SC performance in hospitals that maintain high levels
of supplier partnerships. The reverse will reduce performance of the hospital SC. Second, the
dimensions of the MAS information designed and used will have a greater positive effect on
hospital SC performance in hospitals that share (or exchange) more information or knowledge.
University of Ghana http://ugspace.ug.edu.gh

230
The reverse will lead to lower performance of the hospital SC. Third, the dimensions of the
MAS information designed and used will have a greater positive effect on hospital SC in
hospitals that experience more risk and an uncertain environment. On the contrary, it will lead
to a greater negative effect on hospital SC performance for hospitals that experience low risk
and a certain environment. The study thus finds a non-monotonic interaction to exist between
the SCM context factors, the dimensions of the MAS information and hospital SC performance.
On the whole, the findings suggest that the selection fit model which falls under the
configuration school of thought, and both the mediation and moderation fit models which fall
under the Cartesian school of thought are strongly supported by the sample data. Hence,
contingency applications of the MAS information characteristics can be extended from the
intra-organizational domains to the inter-organizational domains in supply chains in the
Ghanaian healthcare setting.
8.3 Conclusions
This study investigated the contingency fit relationships between SCI (external and internal
integration), level of knowledge exchange, supply chain risk and uncertainty and four MAS
information dimensions on hospital supply chain performance using empirical data from
healthcare institutions in Ghana. This section presents the conclusions arising from the research
findings and the resulting implications. Based on the findings, the following conclusions can
be drawn.
First, the study provides empirical evidence and documents that the MAS-contingency
combination fits in the inter-organizational relations domain in supply chains and highly
applicable in the external environment of healthcare institutions. The sample data confirms that
SCI made up of strategic supplier relations and internal integration, information sharing (or
University of Ghana http://ugspace.ug.edu.gh
231
knowledge exchange), and supply chain risk and uncertainty should be considered as an added
external variable in the contingency theory paradigm. Perhaps, this conclusion can be extended
to organizations in the mainstream discrete parts manufacturing and consumer goods domains
as well. It concludes that the four antecedent conditions of the supply chain namely, supplier
relations, information sharing (or knowledge exchange), risk and uncertainties, and supply
chain integration are critical for the design and implementation of MAS information in hospital
managerial decisions that extend beyond organizational boundaries.
That is to state that hospitals in Ghana should consider aligning their SCM decisions with the
four dimensions of MAS information (scope, timeliness, integration and aggregation) by
finding answers to the following questions. Does the current MAS information provide timely
and adequate decision-support information for supplier relation decisions (e.g. supplier
selection, switching supplier etc.) or readily make relevant information available to supply
chain members or provide adequate logistic-related information (e.g. tracking of
inventory/stock levels, procurement, warehousing and distribution related information) for
effective SCM decisions? Does the MAS information currently used by our hospital provide
supply chain information that is forward-looking or ahead of time (i.e. future-oriented) or
enable managers to foresee risks measures associated with the supply chain (e.g. supplier
failure, supply shortages, supply chain disruptions, etc.)? Do the MAS information dimensions
aggregate relevant information in terms of time periods to functional units, and provides
information targeted precisely at activities and interrelationships with subunits and external
partners? Does the accounting information provide analytical and decision models or integrated
into the SCM system?
If concrete answers cannot be found for these questions, then it could mean that the MAS
information being used in Ghanaian hospitals have become obsolete and dysfunctional in the
context of SCM and needs to be revised and redesigned. It means that the MAS information is
University of Ghana http://ugspace.ug.edu.gh

232
still based on the intra traditional management accounting system which merely estimate costs
and does not provide information that is non-financial, aggregated and future-oriented in nature
for boundary-spanning managerial decisions. It could suggest that healthcare institutions may
not have incorporated into their MAS information the evolutionary changes in the processes
and procedures of hospital supply chain operations which has rendered the current system to
have little value for managerial decisions in supply chains. As contingency theory suggests,
the design and use of MAS information in organizations should evolve with changing
idiosyncratic circumstances that are both internal and external to the firm. Failure to achieve
this could result in the absence of fit which in turn lowers performance.
Second, the study concludes that the four dimensions of the MAS information could pose as
intervening mechanisms in the effective management of health SC in the Ghanaian context.
This suggests that for enhancements in the hospital SC, the four dimensions of the MAS
information play an indirect role. The most critical element of SCM (i.e. SCI) was found to be
statistically insignificant in both the selection and the moderation model. This suggests that
hospitals in Ghana have weak relationships with their suppliers as well as weak internal
linkages. More precisely, there is weak SCI among hospitals in Ghana. It could mean that either
there is over-fit or under-fit of the use of the MAS information in managing SCM decisions.
The intervening role played by the MAS suggests that hospitals in Ghana will benefit from the
optimal use of the MAS information in enhancing SC performance.
Third, although SCI was statistically insignificant in both the selection and mediation fit
models, it was statistically significant in the moderation fit model. This suggests that SCI
(external and internal integration) combines with the MAS information to derive the best SCM
decisions that will yield high SC performance. The positive effect suggests that a high
performance will be attained for hospitals that have strong SCI (i.e. having strong supplier
relationships and strong internal linkages). The opposite will be an adverse effect on
University of Ghana http://ugspace.ug.edu.gh
233
performance. The same interpretation applies to the level of knowledge exchange and supply
chain risk and uncertainty. Sharing of more information will enhance SCM decisions and have
a positive impact on performance. Furthermore, hospitals that face high levels of supply chain
risk and environmental uncertainties have the tendency to improve on performance than those
in low risk and uncertain environment. The opposite will result in low output.
8.4 Contributions of the Thesis
This thesis which is one of the few studies conducted within the African continent adds to the
management accounting literature by theorizing and testing the existence of fit relationships
between SCI (external and internal integration), level of information sharing, supply chain risk
and uncertainty, MAS design, and supply chain performance in healthcare setting. It provides
useful insights on how hospitals in Ghana should benefit from the MAS-contingency
framework so as to improve hospital SC performance. It shows the joint effect of the
contingency-structure combinations in the supply chain field on MAS design and performance.
First, it fills a gap in both the management accounting and SCM literatures on the link between
MAS information and supply chain performance which has been neglected in MAS-CSM
studies. Theoretically, the relationship between MAS information and SC performance needs
to be advanced since both have similar objective of creating value and reducing SC costs. The
study has thus, provided preliminary empirical evidence on the MAS impacts of SCI, level of
knowledge exchange, and supply chain risk and uncertainty by developing a workable
theoretical framework and hypotheses that links SCM, MAS design, and supply chain
performance in a healthcare setting. Empirical examination of the interaction effects of these
three variables hardly exists in prior management accounting – supply chain literature.
University of Ghana http://ugspace.ug.edu.gh
234
Second, the thesis demonstrates the benefits of conceptualizing the MAS, SCM and SCP
constructs which permits the comprehensive understanding of the details of MAS, SCM and
SCP at the dimension levels. More precisely, the use of multidimensional MAS, SCM and SCP
constructs (Wong et al, 2011) permit the development of a comprehensive model and theory
of the contingency effects of SCI, level of information sharing, and supply chain risk and
uncertainty. This theory is strengthened by the use of a second-order structural equation
modelling which offers a unique contribution as such modelling approaches hardly exists in
the management accounting literature. No study was identified from the extensive reviews, that
has used a second-order SEM in testing contingency hypothesis although there are studies that
have used SEM. Thus, the study presents a paradigm for assessing the multidimensionality
feature of the MAS construct in relation to other organizational constructs.
Third, this study has empirically examined the reverse impacts of the SCM contextual
dimensions on the MAS information characteristics (the selection form of fit) that can leverage
hospital supply chain performance. Compared to existing studies on the MAS-supply chain
interaction, this is an area that lacks empirical investigation in the management accounting
literature. The findings extend contingency theory’s application from the intra-organizational
domain to the inter-organizational domain in supply chains thereby expanding the contingency
variables from existing ones to include SCI (strategic supplier partnerships and internal
integration), level of information sharing (or knowledge exchange), and supply chain risk and
uncertainty. Perhaps, the most significant contribution of this thesis is the development and
testing of a novel theoretical model on the mediating and moderating effects of SCI (external
and internal integration), level of information sharing, and supply chain risk and uncertainty
on MAS design and hospital SC performance relationships. Hospital managers can develop
their MAS based on contingency theory’s lenses given its optimum choices.
University of Ghana http://ugspace.ug.edu.gh
235
Finally, it responds to the several calls for studies that investigate multiple contingency
endogenous variables on multiple endogenous variables for the advancement of theory
consistent with management accounting research.
8.5. Recommendations
Based on the conclusions, the following have been recommended. These recommendations are
in line with the study objectives. First, integration of the health SC is highly crucial to enhance
the operational performance of the SC of healthcare institutions in Ghana. For optimal
performance of the health SC, integration of the required resources in the right place and at the
right time is needed to ensure the availability of supplies to enable healthcare institutions serve
their patients more effectively and efficiently. Second, both public and private healthcare
institutions should give more importance to the SCM principles in relation to MAS design and
apply optimal amounts of the MAS to SCM decisions in order to attain the highest
performance. This should be inculcated into the strategic plans of hospitals. Third, for optimal
performance, hospitals in Ghana should consider aligning (or matching) their SCM activities
with the four dimensions (scope, timeliness, integration and aggregation) of the MAS. This is
because as the results indicated regarding objective one and two, the optimal selection of the
MAS (selection fit model) and mediation effect (mediation fit model) of the MAS dimensions
enhances hospital SC performance since the results suggest that the MAS provides decision
support for effective SCM decisions. That is hospital SCM decisions in terms of operating costs
that are taken outside the MAS dimensions are likely to result in misalignment and negatively
affect performance.
In objective three, the results suggest that a positive (or greater) impact on hospital SC
performance can be attained in hospitals that:
University of Ghana http://ugspace.ug.edu.gh

236
- maintain high levels of supplier partnerships. The reverse would lead to lower
performance
- share (or exchange) optimal MAS information or knowledge relative to their
SCM activities. The excess or insufficient sharing of the MAS information
relative to SCM decisions would lead to lower performance.
- experience high risk and uncertain environment but will lead to negative effects
for hospitals that experience low risk and certain environment.
This suggests that to achieve the benefits in terms of SC optimization, an enterprise-wide-item-
level visibility must be made possible through the SC information structure – which is
underpinned by MAS design and supported by wide area network technologies.
8.6 Limitations of the Study
First, the empirical results are based on sample data relating to only one country (Ghana) given
the number of developing countries hence, possible generalization of the findings to include
the health supply chain in all developing countries is limited. Additionally, it focused only on
healthcare institutions, and more precisely hospitals; hence, its findings may not be applicable
to other organizational contexts. Notwithstanding, the results can be generalized within the
Ghanaian context. Second, not all the contextual variables of the supply chain were examined.
For example, customer relationship, postponement and the separate examination of information
technology (IT) performance impacts on the hospital supply chain are important dimensions of
the SCM practices. Hence, their exclusion from the study could be an important shortcoming
given especially the role of IT in enhancing supply chain integration.
University of Ghana http://ugspace.ug.edu.gh
237
Third, although the use of SEM as a statistical tool for examining fit relationships offers
effective and better insight, meaning and understanding of the fit concept compared to other
statistical methods (e.g. MRA), it cannot be used under the matching form of fit model which
happens to be the most classical form of contingency fit (Burkert et al, 2014). This is due to
the curvilinear dimension (i.e. inverted U-shaped) that underpins the relationship between the
MAS variable and performance. The meaning is that given a certain level of the contingency
variable, only one optimal MAS variable can be attained. On the other hand, linear relationships
are associated with the covariance based SEM methodology and is a key assumption underlying
this approach (Edwards, 2009) as against the curvilinear relationship which is a key feature of
the matching form of fit. Also, the matching form of contingency fit is based on the iso-
performance assumption as its key underlying theoretical concept. Under this concept as
discussed in chapter three, several optimal MAS-contingency combinations are predicted with
the same level of performance produced by each. This form of analysis is not attainable in SEM
as the issue of hetero-performance effect on the fit-line and/or asymmetric effects of misfit on
performance which are highly associated with matching fit models cannot be addressed. The
other forms of fit models (selection, mediation, moderation, etc.) are however effectively and
appropriately tested under SEM than other statistical techniques (Burkert et al, 2014). Another
limitation is the mitigation of the likelihood of common methods bias. This is because the
sections of the questionnaire which was tested on performance were answered solely by
hospital accountants and that they could have answered the questions to their advantage and
this will result in common methods bias. Using the same sample, future studies can test for
common methods bias to see whether there is any significant difference in the responded
sample.
University of Ghana http://ugspace.ug.edu.gh

238
8.7 Future Research Directions
Several avenues for future research can be identified. First, this work only considers the
extension of the MAS-contingency framework from the intra-organizational domain to the
inter-organizational domains relating healthcare institutions, and more precisely hospitals. The
application of the fit concept in the boundary-spanning relationships that can leverage
performance in supply chains involving the discrete parts manufacturing and consumer goods
industry provides avenues for future studies. Second, empirical evidence on the contingency
theory’s application in the SCM field can be extended to include the other dimensions (e.g.
customer relations, postponement, information technology, etc.) of SCM practices which were
not considered in this study. In addition, this study examines supply chain integration as a
composite variable yet, integration is a multidimensional construct consisting of supplier
integration, customer integration, and internal integration. Future studies can examine each of
these dimensions on their own in relation to aggregate performance or each performance
dimension. Third, this work has focused exclusively on the MAS characteristics involving the
four dimensions of scope, timeliness, integration and aggregation in examining its design in
the SCM field. Other numerous dimensions of the MAS design which have been used in prior
studies can be examined in relation to SCM.
For example, the dimensions of the MAS information can be classified under long-term
planning, budgeting, decision support systems, financial and non-financial information, and
others. Fourth, and in addition to the dimensions specified above, the management accounting
techniques (or concepts) (e.g. ABC, value chain analysis, target costing, kaizen costing, open
book accounting, etc.) which have been proposed as SCM tools in inter-organizational relations
are avenues for future research within the contingency framework in relation to organizational
performance.
University of Ghana http://ugspace.ug.edu.gh

239
8.8 Chapter Summary
In this chapter, a summary of the key findings and the conclusions arising from the main
findings have been presented. It also elaborated on the contributions to literature which is
mainly theory-based. The chapter also provided the limitations that are likely to inflict this
study and finally the directions for future research.
University of Ghana http://ugspace.ug.edu.gh
240
REFERENCES
Abdallah, A. B., Abdallah, M. I. and Saleh, F. I. M. (2017). The Effect of Trust on with Suppliers
on Hospital Supply Chain Performance: The Mediating Role of Supplier
Integration. Benchmarking: An International Journal, 24(3), 694-715.
Abernethy, M.A., Brownell, P., (1999). The Role of Budgets in Organizations Facing Strategic
Change: An Exploratory Study. Accounting, Organizations and Society, 24(3),
189–204.
Abernethy, M. A., Bouwens, J., and van Lent, L. (2004). Determinants of Control System
Design in Divisionalized Firms. The Accounting Review, 79(3), 545-570.
Abernethy, M.A., Chua, W.F., Grafton, J. and Mahama, H., (2007). Accounting and Control in
Health care: Behavioural, Organisational, Sociological and Criticalperspectives.
In: Chapman, C.S., Hopwood, A.G., Shields, M.D. (Eds.), Handbookof
Management Accounting Research. Elsevier, Amsterdam, 805–829.
Abernethy M.A and Lillis A. M. (2001). Interdependencies in Organisation Design. A Test in
Hospitals. Journal of Management Accounting Research, 13(1), 107–29.
Abernethy, M.A., and Stoelwinder, J.U., (1995). The Role of Professional Control in the
Management of Complex Organizations. Accounting, Organizations and
Society, 20(1), 1–17.
Ab Talib, M.S., Abdul Hamid, A.B. and Thoo, A.C. (2015). Critical Success Factors of Supply
Chain Management: A Literature Survey and Pareto analysis. EuroMed Journal
of Business, 10(2), 234-263.
Adegoke, C., Bruce, E., Chimnani, B. J., Eghan, K., Tetteh, G. and Veskov, D., (2008), Ghana:
PMI Assessment of the Supply Chain and Pharmaceutical Management for Anti-
malaria and ITNs. Arlington, Via: USAID DELIVER PROJECT, Task Order 3,
and MSH/SPS Programme.
Adu-Poku, S. Asamoah, D. and Abor, P. A. (2011). Users’ Perspective of Medical Logistics
Supply Chain System in Ghana: The Case of Adansi South District Health
Directorate. Journal of Medical Marketing, 11, 176-190.
Aidemark, L.G., Funck, E.K., (2009). Measurement and Healthcare Management. Financial
Accounting Management, 25(2), 253–276.
Agndal, H. and Nilsson, U. (2009). Inter-Organizational Cost Management in the Exchange
Process. Management Accounting Research, 20(2), 85-101.
Anderson, S.W. and Dekker, H.C. (2005). Management Control for Market Transactions: The
Relation between Transaction Characteristics, Incomplete Contract Design, and
Subsequent Performance. Management Science, 51(12), 1734–1752.
Anderson, S. W., & Dekker, H. C. (2009). Strategic Cost Management in Supply Chains, Part
1: Structural Cost Management. Accounting Horizons, 23(2), 201–220.
Anderson, S., and Dekker, H., (2014). From Make-or-Buy to Coordinating Collaboration:
Management Control in Strategic Alliances. In: Otley, D., Soin, K. (Eds.),
University of Ghana http://ugspace.ug.edu.gh
241
Management Control and Uncertainty. Palgrave Macmillan, Basingstoke, UK,
47–68 (Chapter 4).
Anderson, S. W., and Dekker, H. C. (2015). The Role of Management Controls in Transforming
Firm Boundaries and Sustaining Hybrid Organizational Forms. Foundations and
Trends in Accounting, 8(2), 75-141.
Anderson, S. W., Dekker, H. C., & Van den Abbeele, A. (2017). Costly Control: An
Examination of the Trade-Off between Control Investments and Residual Risk
in Inter-firm Transactions. Management Science, 63(7), 2163-2180.
Anderson, S, W. Christ, M. A. Dekker, C. H. and Sedatole, K. L. (2015). Do Extant Management
Control Frameworks Fit the Alliance Setting? A Descriptive Analysis. Industrial
Marketing Management, 46, 36-53.
Angelkort, H., Sandt, J., and WeiBenberger, B. E., (2009). IFRS: Can of Worms or Silver Bullet
for Accounting Systems? CIMA Insight (February) Newsletter/Insights – e-
magazine Insight.
Argyris, C. (1952). The Impact of Budgets on People. Ithaca, New York: The Controllership
Foundation.
Asamoah D, Abor P and Opare M (2011). An Examination of Pharmaceutical Supply Chain for
Artemisinin-Based Combination Therapies in Ghana. Management Research
Review, 34(7), 790-809.
Ataseven, C. and Nair, A. (2017). Assessment of Supply Chain Integration and Performance
relationships: A Meta-Analytic Investigation. International Journal of
Production Economics, 185, 252-265.
Atkinson, A. and Waterhouse, J. (1996). Strategic Performance Measurement: Scope and
Implementation Issues. University of Waterloo working paper.
Auzair, S. M. and Langfield-Smith, K. (2005). The Effect of Service Process Type, Business
Strategy and Life Cycle Stage on Bureaucratic MCS in Service Organisations.
Management Accounting Research, 20(4), 1–17.
Baiman, S. and Rajan, M. V. (2002). Incentive Issues in Interfirm Relationships. Accounting,
Organizations and Society, 27(3), 213-238.
Bai, G., Coronado, F., and Krishnan, R., (2010). The Role of Performance Measure Noise in
Mediating the Relation between Task Complexity and Outsourcing. Journal of
Management Accounting Research 22(1), 75–102.
Baines A, and Langfield-Smith K. (2003), Antecedents to Management Accounting Change: A
Structural Equation Approach. Accounting, Organizations and Society, 28(7-8),
675–98.
Ballantine, J., Brignall, S., and Modell, S., (1998). Performance Measurement and Management
in Public Health Services: A Comparison of U. K. and Swedish Practice.
Management Accounting Research, 9(1), 71–94.
University of Ghana http://ugspace.ug.edu.gh

242
Barki, H., Pinsonneault, A., (2005). A Model of Organizational Integration, Implementation
Effort, and Performance. Organization Science 16(2), 165–179.
Barlow, R.D., (2010c). Navigating the C-Scape in Supply Chain Management. Healthcare
Purchasing News 34, 8–12.
Baron, R. M., Kenny, D. A., (1986). The Moderator-Mediator Variable Distinction in Social
Psychological Research: Conceptual, Strategic and Statistical Considerations.
Journal of Personality and Social Psychology 51(6), 1173–1182.
Barrett S. and Konsynski B. (1982). Inter-Organization Information Sharing Systems. MIS
Quarterly, 6, 93-105.
Beckmann, M., Hielscher, S., & Pies, I. (2014). Commitment Strategies for Sustainability: How
Business Firms Can Transform Trade-offs into Win-Win Outcomes. Business
Strategy and the Environment, 23(1), 18-37.
Bedford, D. S., Malmi, T. and Sandelin, M. (2016). Management Control Effectiveness and
Strategy: An Empirical Analysis of Packages and Systems. Accounting,
Organizations and Society, 51, 12-28.
Beier, F.J., (1995). The Management of the Supply Chain for the Hospital Pharmacies: A Focus
on Inventory Management Practices. Journal of Business Logistics 16(2), 153–
173.
Behesti, H. M., Oghazi, P., Mostaghel, R. and Hultman, M. (2014). Supply Chain Integration
and Firm Performance: An Empirical Study of Swedish Manufacturing Firms.
Competitiveness Review, 24(1), 20-31.
Bentler, P. M. (2005). EQS 6 Structural Equations Program Manual. Encino, CA: Multivariate
Software.
Bisbe, J., Batista-Foguet, J-M. and Chenhall, R. (2007). Defining Management Accounting
Constructs: A Methodological Note on the Risks of Conceptual
Misspecification. Accounting, Organizations and Society, 32(7-8), 789–820.
Bossert T., Bowser D., Amenyah J. and Copeland B., (2004). Ghana: Decentralization and
Health Logistics Systems: Arlington, Va.: John Snow, Inc./DELIVER for
USAID for the U.S. Agency for International Development. Available on:
http://pdf.usaid.gov/pdf_docs/PNADM531.pdf (Accessed 6th
May, 2012).
Bouwens, J. and Abernethy, M. A., (2000). The Consequences of Customization on
Management Accounting System Design. Accounting, Organizations and
Society, 25(3), 221-241.
Braziotis, C., Bourlakis, M., Rogers, H. and Tannock, J. (2013), “Supply Chains and Supply
Networks: Distinctions and Overlaps”, Supply Chain Management: An
International Journal, 18(6), 644-652.
Brownell, P. (1982a). The Role of Accounting Data in Performance Evaluation, Budgetary
Participation and Organizational Effectiveness. Journal of Accounting Research,
20, 12- 27.
University of Ghana http://ugspace.ug.edu.gh
243
Brownell, P. (1982b). A Feld Study Examination of Budgetary Participation and Locus of
Control. The Accounting Review, 57, 766-777.
Brownell, P. (1983). The Motivational Impact of Management- By-Exception in a Budgetary
Context. Journal of Accounting Research, 21, 456-472.
Brownell, P. (1985). Budgetary Systems and the control of functionally Differentiated
Organizational Activities. Journal of Accounting Research, 23, 502-512.
Brownell, P., and Dunk, A. S. (1991). Task Uncertainty and its Interactions with Budgetary
Participation and Budget Emphasis: Some Methodological Issues and Empirical
Investigation. Accounting, Organizations and Society, 16(8) 693-703.
Brownell, P. and Hirst, M. K., (1986). Reliance on Accounting Information, Budgetary
Participation, and Task Uncertainty: Tests of a Three-Way Interaction. Journal
of Accounting Research, 24(2), 241-249.
Burrell G and Morgan G (1979). Sociological Paradigms and Organisational Analysis,
Heinemann, London
Burkert, M., Davila, A., Mehta, K. and Oyon, D. (2014). Relating Alternative Forms of
Contingency Fit to the Appropriate Methods to Test them. Management
Accounting Research. 25(1), 6-29.
Burns, L.R. (2002). The Health Care Value Chain, Jossey-Bass, San Francisco, CA.
Burritt, R. and Scaltegger, S. (2014). Accounting Towards Sustainability in Production and
Supply Chains. The British Accounting Review, 46(4), 327-343.
Butler, P. T.,W. Hall, A.M. Hanna, L.Mendonca, B. Auguste, J.Man- yika, A and Sahay, (1997).
A revolution in interaction. McKinsey Quarterly, 1, 3–14
Byrne, B. M. (2010). Structural Equation Modelling with AMOS: Basic Concepts, Applications
and Programming, 2nd Edition, Routledge, Taylor and Francis Group, 270
Madison Avenue, New York, NY 10016.
Cadez, S. and Guilding, C., (2008). An Exploratory Investigation of an Integrated Contingency
Model of Strategic Management Accounting. Accounting, Organizations and
Society, 33(7-8), 836-863.
Cardinaels, E., Roodhooft, F. and van Herck, G. (2004). Drivers of Cost System Development
in Hospitals: Results of a Survey. Health Policy, 69(2), 239-252.
Cardinaels E. and Soderstrom N., (2013). Accounting Insights from the Healthcare Sector.
European Accounting Review, 22(4), 809-810.
Chapman C.S, Kern A, Laguecir A, Angele-Halgand N, Angert A, and Camp-enale C. (2013).
International Approaches to Clinical Costing, Bristol, UK.
Champoux, J. E., & Peters, W. S. (1987). Form, Effect Size and Power in Moderated Regression
Analysis. Journal of Occupational Psychology, 60(3), 243-255.
University of Ghana http://ugspace.ug.edu.gh

244
Chen, Q. D., Preston, D. S., and Xia, W., (2013). Enhancing Hospital Supply Chain
Performance: A Relational View and Empirical Test. Journal of Operations
Management, 31(6), 391-308.
Chakraborty, S., Bhattacharya, S. and Dobrzykowski, D.D. (2014). Impact of Supply Chain
Collaboration on Value Co-Creation and Firm Performance: A Healthcare
Service Sector Perspective. Procedia Economics and Finance, 11, 676-694.
Chenhall, R. H. (1986). Authoritarianism and Participative Budgeting: A Dyadic Analysis. The
Accounting Review, 61, 263-272.
Chenhall, R. H. (2003). Management Control Systems Design within its Organizational
Context: Findings from Contingency-Based Research and Directions for the
Future. Accounting, Organization and Society, 28(2-3), 127–168.
Chenhall, R.H. and Chapman, C.S. (2006). Theorizing and Testing Fit in Contingency Research
on Management Control Systems. In: Hoque, Z. (Ed.), Methodological Issues in
Accounting Research. Spiramus, London, pp. 35–54.
Chenhall, R. H, and Langfield-Smith, K., (1998) Adoption and Benefits of Management
Accounting Practices: An Australian Study. Management Accounting Research,
9(1), 1–19.
Chenhall, R. and Morris, D. (1986). The Impact of Structure, Environment, and Interdependence
on the Perceived Usefulness of Management Accounting Systems. The
Accounting Review, 61(1), 16-35.
Chin, W. (1998). The Partial Least Squares Approach to Structural Equation Modeling. In G.
A. Marcoulides (Ed.), Modern business research methods, Mahwah. NJ:
Lawrence Erlbaum Associates.
Chong, V.K., Chong, K.M. (1997). Strategic Choices, Environmental Uncertainty and SBU
Performance: A Note on the Intervening Role of Management Accounting
Systems. Accounting and Business Research 27(4), 268–276.
Christensen J, and Demski J., (2002), Accounting Theory: An Information Content Perspective.
New York: McGraw-Hill/Irwin.
Chua W F (1986). Radical Developments in Accounting Thought. The Accounting Review, Vol
LXI, No. 4.
Clemens, T., Michelsen, K., Commers, M., Garel, P., Dowdeswell, B. and Brand, H. (2014).
European Hospital Reforms in Times of Crisis: Aligning Cost Containment
Needs with Plans for Structural Redesign? Health Policy, 117, 6-14.
Coad, A. and Cullen, J. (2006). Inter-organizational Cost Management: Towards an
Evolutionary Perspective. Management Accounting Research, 17(4), 342–369
Cohen, J. and Cohen, P. (1983). Applied Multiple Regression/Correlation Analysis for the
Behavioral Sciences. Hillsdale: Erlbaum.
University of Ghana http://ugspace.ug.edu.gh

245
Cohen, S., and Kaimenaki, E., (2011). Cost Accounting System Structure and Information
Quality Properties: An Empirical Analysis. Journal of Applied Accounting
Research, Vol 12(1), 5-25.
Cooper R, and Kaplan R. S. (1991). The Design of Cost Management Systems: Text, Cases,
and Readings. Englewood Cliffs, N J: Prentice Hall.
Cooper, R., & Kaplan, R. S. (1999). The Design of Cost Management System. Upper Saddle
River, NJ: Prentice Hall.
Cooper, M. C., Lambert, D. M. and Pagh, J. D. (1997). Supply Chain Management: More than
a New Name for Logistics. International Journal of Logistics Management, 8(1),
1-14.
Cooper, R. and Slagmulder, R. (1998). The Scope of Strategic Cost Management. Management
Accounting (USA), 79(7), 18–19.
Cooper, R. and Slagmulder, R. (1999). Supply Chain Development for the Lean Enterprise—
Inter-Organizational Cost Management. Productivity Inc., Portland
Cooper, R. and Slagmulder, R. (2004). Inter-Organizational Cost Management and Relational
Context. Accounting, Organizations and Society 29 (1), 1–16.
Cooper, R. and Yoshikawa, T. (1994a). ‘Inter-Organizational Cost Management Systems: The
Case of the Tokyo–Yokohama–Kamakura Supplier Chain. International Journal
of Production Economics 37(1), 51–62.
Costantino, F., Gravio, G. D., Shaban, A. and Tronci, M. (2015). The Impact of Information
Sharing on Ordering Policies to Improve Supply Chain Performances.
Computers and Industrial Engineering. 82, 127-142.
Counte M. A, and Glandon G. L. (1988). Managerial Innovation in the Hospital: An Analysis
of the Diffusion of Hospital Cost-Accounting Systems. Hospital and Health
Services Administration, 33(3), 71–84.
Cousins, P.D., and Menguc, B., (2006). The Implications of Socialization and Integration in
Supply Chain Management. Journal of Operations Management, 24 (5), 604–
620.
Creswell, J. W. (2014). Research Design: Qualitative, Quantitative and Mixed Methods
Approaches. Fourth Edition, Sage Publications.
Dacosta-Claro, I. (2002), The Performance of Material Management in Health Care
Organizations. International Journal of Health Planning and Management,
17(1), 69-85.
Daft, R. (1983). Organization Theory and Design. New York: West.
D’Avanzo, R., Lewinski, H.V. and Van Wassenhove, L.N.V. (2003). The Link between Supply
Chain and Financial Performance. Supply Chain Management Review, 7(6), 40-
47.
University of Ghana http://ugspace.ug.edu.gh

246
Davila, A. and Foster, G., (2005). Management Accounting Systems Adoption Decisions:
Evidence and Performance Implications from Early-Stage/Start-Up Companies.
The Accounting Review, 80(4), 1039-1068.
DeCarlo, L. T. (1997). On the Meaning and use of Kurtosis. Psychological Methods, 2, 292–
307.
De Harlez, Y. and Malagueno, R. (2016). Examining the Joint Effects of Strategic Priorities,
Use of Management Control Systems, and Personal Background on Hospital
Performance. Management Accounting Research, 30(1), 2-17.
Dekker, H. C., & van Goor, A. R. (2000). Supply Chain Management and Management
Accounting: A Case Study of Activity Based Costing. International Journal of
Logistics: Research and Applications, 3(1) 41-52.
Dekker, H. (2003). Value Chain Analysis in Interfirm Relationships: A Field Study.
Management Accounting Research, 14(1), 1–23.
Dekker, H. C. (2004). Control of Inter-Organizational Relationships, Evidence on
Appropriation Concerns and Coordination Requirements. Accounting
Organizations and Society, 29(1), 27–49.
Dekker, H. C. (2005). Control of Inter-Organizational Relationships, Evidence on
Appropriation Concerns and Coordination Requirements. Accounting
Organizations and Society, 29(1), 27–49.
Dekker, H. C. (2016). On the Boundaries between Intrafirm and Interfirm Management
Accounting Research. Management Accounting Research, 31, 86-99.
Dekker, H. C., Groot, T. L. C. M., and Schoute, M. (2013). A Balancing Act? The Implications
of Mixed Strategies for Performance Measurement System Design. Journal of
Management Accounting Research, 25(1), 71- 98.
Dekker, H. C., Sakaguchi, J. and Kawai, T. (2013), Beyond the Contract: Managing Risks in
Supply Chain Relations. Management Accounting Research, 24(2), 122-139.
Denkyira, A., (2015) 8th Annual General Meeting and Continuous Professional Development
Programme on the Health Services Supply Chain Practitioners Association,
Ghana (HESSCPAG) Held in Cape Coast on 31st October, 2015.
Devaraj, S., Krajewski, L., Wei, J.C., (2007). Impact of e-Business Technologies on Operational
Performance: The Role of Production Information Integration in the Supply
Chain. Journal of Operations Management, 25(6), 1199–1216.
Devine K, O’clock P. and Lyons D. (2000). Healthcare Financial Management in a Changing
Environment. Journal of Business Research, 48(3), 183–191.
De Vries, J. (2011). The Shaping of Inventory Systems in Health Services: A Stakeholder
Analysis International Journal of Production Economics, 133(1), 60-9.
De Vries, J. and Huijisman, R., (2011). Supply Chain Management in Health Services: An
Overview. Supply Chain Management: An International Journal, 16(3), 159–
165.
University of Ghana http://ugspace.ug.edu.gh

247
Diamond, S. S. (2000). Reference Guide on Survey Research. In Reference Manual on Scientific
Evidence (2nd ed., pp. 229–276). Washington, DC: The Federal Judicial Center.
Ding, R., Dekker, H. C. and Groot, T. (2013). Risk, Partner Selection and Contractual Control
in Interfirm Relations. Management Accounting Research, 24, 140-155.
Dogan, I. and Sahin, U., (2003). Supplier Selection using Activity Based Costing and Fuzzy
Present-Worth Techniques. Logistics Information Management, 16(6), 420-426.
Donaldson, L. (1996). For positivist Organization Theory: Proving the Hard Core. London:
Sage.
Donaldson, L., (2001). The Contingency Theory of Organizations. Sage, Thousand Oaks, CA.
Donaldson, L., (2006). The Contingency Theory of Organizational Design: Challenges and
Opportunities. In: Burton, R.M., Eriksen, B., Hakonsson, D.D., Snow, C.C.
(Eds.), Organization Design: The Evolving State-of the- Art. Springer, pp. 19–
40.
Dooner, R., (2014), How Supply Chain Management Can Help to Control Healthcare Cost.
Supply Chain Q. Q. 3, 50–53.
Drazin, R. and Van de Ven, A.H., (1985). Alternative Forms of Fit in Contingency Theory.
Administrative Science Quarterly 30, 514–539.
Droge, C., Jayaram, J., Vickery, S.K., (2004). The Effects of Internal versus External Integration
Practices on Time-Based Performance and Overall Firm Performance. Journal
of Operations Management, 22(6), 557–573.
Dropulic, I., (2013). The Effect of Contingency Factors on Management Control Systems: A
Study of Manufacturing Companies in Croatia. The 6th International Conference,
The Changing Economic Landscape, Issues, Implications and Policy
Implications, Economic Research, 26(1), 369-382.
Duncan, R. B, (1972), Characteristics of Organisational Environments and Perceived
Environmental Uncertainty. Administrative Science Quarterly, 17, 313–27.
Duncan, K., Moore, K. (1989). Residual Analysis: A Better Methodology for Contingency
Studies in Management Accounting. Journal of Management Accounting
Research 1, 89–104.
Dunk, A. S. (1989). Budget Emphasis, Budgetary Participation and Managerial Performance. A
Note. Accounting, Organizations and Society. 14(4), 321-324.
Dunk, A. S. (1992). Reliance on Budgetary Control, Manufacturing Process Automation and
Production Subunit Performance: A Research Note. Accounting, Organizations
and Society, 17(3-4), 195-203.
Dunk, A. S. (1993). The Effect of Budget Emphasis and Information Asymmetry on the Relation
between Budgetary Participation and Slack. The Accounting Review, 68, 400-
410.
University of Ghana http://ugspace.ug.edu.gh
248
Dunk, A. S. (2003). Moderated Regression, Constructs and Measurement in Management
Accounting: A Reflection. Accounting, Organizations and Society, 28(7-8), 793-
802.
Dunk, A. S. (2011). Product Innovation, Budgetary Control, and the Financial Performance of
Firms. The British Accounting Review, 43(2), 102-111.
Easterby-Smith, M, Thorpe, R and Jackson, P (2012). Management Research, 4th Edition,
SAGE London.
Edwards, J. R., (2007). Polynomial Regression and Response Surface Methodology. In: Ostroff,
C., Judge, T.A. (Eds.), Perspectives on Organizational Fit. Taylor & Francis
Group, LLC, New York, NY, pp. 361–372.
Ellis, S.C., Henry, R.M. and Shockley, B. (2010). Buyer Perceptions of Supply Disruption Risk:
A Behavioral View and Empirical Assessment. Journal of Operations
Management 28(1), 34–46.
Elmuti, D., Khoury, R., Omran, O. and Abou-Zaid, A., (2013). Challenges and Opportunities of
Healthcare Supply Chain Management in the United States, Health Marketing
Quarterly, 30(2), 128–143.
Fabbe-Costes, N. and Jahre, M., (2008). Supply Chain Integration and Performance: A Review
of the Evidence. International Journal of Logistics Management, 19(2), 130–
154.
Fayard, D., Lee, L. S., Leitch, R. A., and Kettinger, W. J., (2012). Effect of Internal Cost
Management, Information Systems Integration, and Absorptive Capacity on
Inter-Organizational Cost Management in Supply Chains. Accounting,
Organizations and Society, 37(3), 168-187.
Fayard, D, Lee, L S, Leitch, R A and Kettinger, W J, (2014), “Inter-organizational Cost
Management in Supply Chains: Practices and Payoffs”, Management Accounting
Quarterly, 15(3), 1-9.
Federal Rules of Evidence (1971). New York: Bancroft-Whitney.
Ferreira A., (2002). [Ph.D. thesis] Management Accounting and Control Systems Design and
Use: An Exploratory Study in Portugal. Department of Accounting and Finance,
Lancaster University.
Ferry, L. and Gebreiter, F. (2016). Accounting and the Insoluble Problem of Healthcare Costs.
European Accounting Review, 25(4), 719-733.
Field, J. M. and Meile, L. C., (2008). Supplier Relations and Supply Chain Performance in
Financial Services Processes. International Journal of Operations and
Production Management, 28(2), 185-206.
Fisher, J. G., (1995). Contingency-Based Research on Management Control Systems:
Categorization by Level of Complexity. Journal of Accounting Literature, 14,
24–53.
University of Ghana http://ugspace.ug.edu.gh

249
Flynn, B. B., Huo, B. and Zhao, X. (2010). The Impact of Supply Chain Integration on
Performance: A Contingency and Configuration Approach. Journal of
Operations Management, 28(1), 58-71.
Fornell, C. and Larcker, D. (1981). Evaluating Structural Equation Models with Unobservable
Variables and Measurement Error. Journal of Marketing Research, 18(1), 39–
50.
Frucot, V. and Shearon, W. T. (1991). Budgetary Participation, Locus of Control, and Mexican
Managerial Performance and Job Satisfaction. The Accounting Review, 66, 80-
99.
Fynes, B., de Buˇırca, S., and Marshall, D., (2004). Environmental Uncertainty, Supply Chain
Relationship Quality and Performance. Journal of Purchasing & Supply
Management, 10(4–5), 179–190.
Gerbing, D.W., Hamilton, J.G. and Freeman, E.B., (1994). A Large-Scale Second- Order
Structural Equation Model of the Influence of Management Participation on
Organizational Planning Benefits. Journal of Management. 20(4), 859–885.
Gerdin, J., (2005a). The Impact of Departmental Interdependencies on Management Accounting
System Use on Subunit Performance. European Accounting Review, 14(2), 297-
327.
Gerdin, J., and Greve, J. (2004). Forms of Contingency Fit in Management Accounting
Research – A Critical Review. Accounting, Organizations and Society, 29(3-4),
303–326.
Gerdin, J. and Greve, J. (2008). The Appropriateness of Statistical Methods for Testing
Contingency Hypotheses in Managing Accounting Research. Accounting,
Organizations and Society, 33(7-8), 995-1009.
Germain, R., Iyer, K.N.S., (2006). The Interaction of Internal and Downstream Integration and
its Association with Performance. Journal of Business Logistics, 27(2), 29–53.
Gietzmann, M.B. (1996). Incomplete Contracts and the Make or Buy Decision: Governance
Design and Attainable ¯Flexibility. Accounting, Organizations and Society.
21(6), 611±626.
Gordon L A and Miller D (1976). A Contingency Framework for the Design of Accounting
Information Systems. Accounting, Organizations and Society, 1(1), 59-69.
Gordon, L. A, and Narayanan, V. K. (1984). Management Accounting Systems, Perceived
Environmental Uncertainty and Organisation Structure: An Empirical
Investigation. Accounting, Organizations and Society, 9(1), 33–47.
Govindarajan, V. (1984). Appropriateness of Accounting Data in Performance Evaluation: An
Empirical Investigation of Environmental Uncertainty as an Intervening
Variable. Accounting, Organizations and Society, 9(2), 125-135.
University of Ghana http://ugspace.ug.edu.gh
250
Govindarajan, V. (1988). A contingency Approach to Strategy Implementation at the Business
Level: Integrating Administrative Mechanisms with Strategy. Academy of
Management Journal, 31(4), 828–853.
Grotsch, V. M., Blome, C., and Schleper, M. C., (2013). Antecedents of Proactive Supply Chain
Risk Management – A Contingency Theory Perspective. International Journal
of Production Research, 51(10), 2842.
Guimaaraes, C. M. and de Carvalho, J. C. (2013). Strategic Outsourcing: A Lean Tool for
Healthcare Supply Chain Management. Strategic Outsourcing: An International
Journal, 6(2), 138-166.
Gul, F. A., and Chia, Y. M. (1994). The Effects of Management Accounting Systems, Perceived
Environmental Uncertainty and Decentralization on Managerial Performance: A
Test of Three-Way Interaction. Accounting, Organizations and Society, 19( 4-
5), 413–426.
Gyimah E. P., Yellu D. F., Andrews-Annan E., Gyansa-Lutterodt M. and Koduah A., (2009).
Ghana: Assessment of Medicine Procurement and Supply Management Systems
in the Public Health Sector: Ministry of Health (MoH), Ghana National Drug
Programme (GNDP) Ghana. Available on:
http://apps.who.int/medicinedocs/documents/s18017en/s18017en.pdf
(Accessed, 4th May 2016).
Haavik, S. (2000). Building a demand-driven, Vendor-managed Supply Chain. Healthcare
Financial Management, 54(2), 56-61.
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E. and Tatham, R. L. (2006). Multivariate
Data Analysis, Sixth Edition, Prentice Hall, USA.
Hair, J. F., Black, W, C., Babin, B. J, and Anderson, R. E. (2015). Multivariate Data Analysis,
7th Edition, Pearson.
Haka, S. F. (1987). Capital Budgeting Techniques and Firm Specific Contingencies: A
Correlation Analysis. Accounting, Organizations and Society, 12(1), 31–38.
Hakansson, H., and Johanson, J. (1988). Formal and Informal Cooperation Strategies in
International Industrial Networks. In F. J. Contractor & P. Lorange, Cooperative
strategies in international business. Lexington, MA: Lexington Books.
Hammad S A, Jusoh R and Oon E Y N (2010). Management Accounting Systems for Hospitals:
A Research Framework. Industrial Management and Data Systems, 110(5), 762-
784.
Hammad, S. A., Jusoh, R., and Ghozali, I. (2013). Decentralization, Perceived Environmental
Uncertainty, Managerial Performance and Management Accounting System
Information in Egyptian Hospitals. International Journal of Accounting and
Information Management, 21(4), 314–330.
Handcock, G. R. and Mueller, R. O. (2013). Structural Equation Modelling: A Second Course.
Second Edition, Information Age Publishing Inc, USA.
University of Ghana http://ugspace.ug.edu.gh

251
Harlez, Y. D. and Malagueno, R., (2016). Examining the Joint Effects of Strategic Priorities,
Use of Management Control Systems, and Personal Background on Hospital
Performance. Management Accounting Research, 30, 2-17.
Hartmann, F.G.H., (2005). The Impact of Departmental Interdependencies and Management
Accounting System Use on Subunit Performance: A Comment. European
Accounting Review 14(2), 329–334.
Hartmann, F.G.H., Moers, F. (1999). Testing Contingency Hypotheses in Budgetary Research:
An Evaluation of the Use of Moderated Regression Analysis. Accounting,
Organizations and Society, 24(4), 291–315.
Hartmann, F.G.H., Moers, F., (2003). Testing Contingency Hypotheses in Budgetary Research
Using Moderated Regression Analysis: A Second Look. Accounting,
Organizations and Society, 28(7-8), 803–809.
Harrison, G. L. (1992). The Cross-Cultural Generalizability of the Relation between
Participation, Budget Emphasis and Job-Related Attitudes. Accounting,
Organizations and Society, 17(1), 1-15.
Harrison, G. L. (1993). Reliance on Accounting Performance Measures in Supervisor
Evaluative Style: The Influence of National Culture and Personality. Accounting,
Organizations and Society, 18(4), 319-339.
Henke, J., Stallkamp, T., and Yeniyurt, S., (2014). Lost Supplier Trust and Lost Profit: How
Chrysler Missed Out on $24 Billion in Profit Over the Past 12 Years? Supply
Chain Management Review 18(3), 24–32.
Hill, N. T., (2000) Adoption of Costing Systems in US Hospitals: An Event History Analysis
1980–1990, Journal of Accounting and Public Policy, 19(1), 41–71.
Hirst, M. K. (1981). Accounting Information and the Evaluation of Subordinate Performance:
A Situational Approach. The Accounting Review, 771-784.
Hirst, M. K., (1987). The Effects of Setting Budget Goals and Task Uncertainty on Performance.
The Accounting Review, 62(4), 774-784.
Hirst, M. K., (1983). Reliance on Accounting Performance Measures, Task Uncertainty, and
Dysfunctional Behaviour: Some Extensions. Journal of Accounting Research,
21(2), 596-605.
Hirst, M. K., (1986). Reliance on Accounting Information, Budgetary Participation, and Task
Uncertainty: Tests of a Three-Way Interaction. Journal of Accounting Research,
24( 2), 241-249.
Holweg, M., and Pil, F. K. (2008). Perspectives on the Coordination of Supply Chains. Journal
of Operations Management. 26(3), 389–406.
Hoozee, S. and Ngo, Q. H., (2017). The Impact of Managers’ Participation in Costing System
Design on their Perceived Contributions to Process Improvement. European
Accounting Review, DOI: 10.1080/09638180.2017.1375417.
University of Ghana http://ugspace.ug.edu.gh
252
Hopwood, A.G., (1972). Leadership Climate and the Use of Accounting Data in Performance
Evaluation. Accounting Review, 49(3), 485–495.
Hoyle, R. H. (2015). Handbook of Structural Equation Modelling. Paperback Edition, Guiford
Press, NY, 10012.
Hult, G.T.M., Ketchen, D.J., Cavusgil, T., and Calantone, R.J., (2006). Knowledge as a Strategic
Resource in Supply Chains, Journal of Operations Management, 24(5), 458–
475.
Imoisili, O. A. (1989). The Role of Budget Data in the Evaluation of Managerial Performance.
Accounting, Organizations and Society, 14(4), 325-335.
Ittner, C. D., Larcker, D. F., Nagar, V. and Rajan, M. V. (1999). ‘Supplier Selection, Monitoring
Practices, and Firm Performance. Journal of Accounting and Public Policy,
18(3), 253-281.
Jacobucci, D., (2008). Mediation Analysis. SAGE Publications, Inc, Thousand Oaks, CA.
Jamal, N. M., and Tayles, M., (2010). Management Accounting in a Supply Chain Environment:
Case Study Insights. Asia-Pacific Management Accounting Journal, 5(1), 41-67.
Jan de Vries and Huijsman (2011). Supply Chain Management in Health Services: An
Overview. Supply Chain Management: An International Journal, 16(3), 159-
165.
Jarvis, C. B., MacKenzie, S. B. and Podsakoff, P. M. (2003). A Critical Review of Construct
Indicators and Measurement Model Misspecification in Marketing and
Consumer Research. Journal of Consumer Research, 30(2), 199–218.
Jermias, J. and Gani, L., (2004). Integrating Business Strategy, Organizational Configurations
and Management Accounting Systems with Business Unit Effectiveness: A
Fitness Landscape Approach. Management Accounting Research, 15(2), 179-
200.
Jin, S. H., Jeong, S. J. and Kim, K. S. (2017). A Linkage Model of Supply Chain Operation and
Financial Performance for Economic Sustainability of Firm. Sustainability, 9(1),
139.
Jones, C.S., (2002). The Attitudes of British National Health Service Managers and Clinicians
towards the Introduction of Benchmarking, Financial Accounting and
Management, 18(2), 163–188.
Jones, T.C., Luther, R. (2005). Anticipating the Impact of IFRS on the Management of German
Manufacturing Companies: Some Observations from a British Perspective.
Accounting in Europe 2(1), 165–193.
Joreskog, K. G. (1995). Testing Structural Equation Models. In K. A. Bollen & J. S. Long (Eds.),
Testing structural equation models (pp. 294–316). Newbury Park, CA: Sage.
Kaplan, R.S. (1984). The Evolution of Management Accounting. The Accounting Review 59,
390–418.
University of Ghana http://ugspace.ug.edu.gh

253
Kavilanz, P., (2009). Health Cares' Six Money-Wasting Problems. CNNMoney.com (August
10).
Kazemzadeh, R.B., Sepehri, M.M. and Jahantigh, F.F. (2012). Design and Analysis of a Health
Care Supply Chain Management. Advanced Materials Research, 433, 2128-
2134.
Kelle, P., Woosley, J., and Schneider, H. (2012). Pharmaceutical Supply Chain Specifics and
Inventory Solutions for a Hospital Case. Operations Research for Healthcare,
1(2-3), 54-63.
Khandwalla P. N., (1972), The Effect of Different Types of Competition on the Use of
Accounting Controls, Journal of Accounting Research, 10275–85.
Kim, K. K. (1988). Organizational Coordination and Performance in Hospital Accounting
Information Systems: An Empirical Investigation. Accounting Review, 63, 472–
489.
Kim, S.W. (2009). An Investigation on the Direct and Indirect Effect of Supply Chain
Integration on Firm Performance. International Journal of Production
Economics, 119(2), 328-346.
King, R., and Clarkson, P. M., (2015). Management Control Systems Design, Ownership, and
Performance in Professional Service Organisations. Accounting, Organizations
and Society, 45, 24–39.
Koufteros, X., Babbar, S. and Kaighobadi, M. (2009). A Paradigm for Examining Second-Order
Factor Models Employing Structural Equation Models. International Journal of
Production Economics, 120(2), 633-652.
Kuhn, T (1962), “The Structure of Scientific Revolutions, Chicago University Press, Chicago
Kwon, I.-W., and Suh, T.W., (2004a). Factors Affecting the Level of Trust and Commitment in
Supply Chain Management. Journal of Supply Chain Management, 40(2), 4–14.
Kwon, I.-W., Hong, S.-J., (2011). Health Care Supply Chain Management in the United States:
New Paradigm for Roles of Distributors. International Journal of Health
Management Information, 2(2), 73–82.
Kwon, I.-w., Hamilton, J., and Hong, S.-J., (2011) Trust and Transaction Cost in Supply Chain
Cost Optimization: An Exploratory Study. A Chapter in Inter-Organizational
Information Systems and Business Management: Theories for Researchers by
IGI Global Publisher, pp. 107–119.
Kwon, I. W. G., Kim, S. H., and Martin, D. G., (2016). Healthcare Supply Chain Management:
Strategic Areas for Quality and Financial Improvement. Technological
Forecasting & Social Change, 113, 422-428.
Lambert, D. M., Cooper, M. C. and Pagh, J. D. (1998). Supply Chain Management:
Implementation Issues and Research Opportunities. International Journal of
Logistics Management, 9(2), 1-20.
University of Ghana http://ugspace.ug.edu.gh
254
Lambert, D. M. and Cooper, M. C. (2000). Issues in Supply Chain Management. Industrial
Management and Marketing, 29(1), 65-83.
Langfield-Smith, K. (2008). The Relations between Transactional Characteristics, Trust and
Risk in the Start-Up Phase of a Collaborative Alliance. Management Accounting
Research, 19(4), 344-364.
Langfield-Smith K., (1997), Management Control Systems and Strategy: A Critical Review.
Accounting, Organizations and Society, 22(2), 207–32.
Lau, C. M., Low, L. C., & Eggleton, I. R. C. (1995). The impact of Reliance on Accounting
Performance Measures on Job-Related Tension and Managerial Performance:
Additional Evidence. Accounting, Organizations and Society, 20(5), 359-381.
Lawrence, P. R. (1993). The Contingency Approach to Organizational Design. In R. T.
Golembiewski (Ed.), Handbook of organizational design (pp. 9-18). New York:
Marcel Dekker.
Lawrence, P. R., and Lorsch, J. W. (1967). Organization and Environment: Managing
Differentiation and Integration. Boston: Division of Research, Graduate School
of Business Administration, Harvard University.
Lawson R. (2003). Development of an HMO Cost Management System. Research in
Healthcare Financial Management, 8(1), 31–41.
Lee, S. M., Lee, D. and Schniederjans, M. J. (2011). Supply Chain Innovation and
Organizational Performance in the Healthcare Industry. International Journal of
Operations and Production Management, 31(11), 1193-1214.
Lee H. L, So K. C and Tang C. S. (2000). The Value of Information Sharing in a Two-Level
Supply Chain. Management Science, 46(5), 626–43.
Lee, K. H. and Wu, Y., (2014). Integrating Sustainability Performance Measurement into
Logistics and Supply Networks: A Multi-Methodological Approach. The British
Accounting Review, 46(4), 361-379.
Lega, F., Marsilio, M. and Villa, S. (2013). An Evaluation Framework for Measuring Supply
Chain Performance in the Public Healthcare Sector: the Italian NHS. Production
Planning and Control, 24(10-11), 931-947.
Li, G., Fan, H., Lee, P. K. C., and Cheng, T. C. E., (2015). Joint Supply Chain Risk
Management: An Agency and Collaboration Perspective. International Journal
of Production Economics, 164, 93-94.
Li, S., Ragu-Nathan, B., Ragu-Nathan, T. S. and Rao, S. S., (2006). The Impact of Supply Chain
Management Practices on Competitive Advantage and Organizational
Performance. International Journal of Management Science, 34(2), 107-124.
Li S. and Lin B. (2006). Accessing Information Sharing and Information Quality in Supply
Chain Management. Decision Support Systems, 42(3), 1641-56.
Liker, J. K. and Choi, T.Y. (2004). Building Deep Supplier Relationships. Harvard Business
Review, 82(12), 104-13.
University of Ghana http://ugspace.ug.edu.gh

255
Luft, J. and Shields, M. D., (2003). Mapping Management Accounting: Graphics and Guidelines
for Theory-Consistent Empirical Research. Accounting, Organizations and
Society, 28(2-3), 169-249.
Lukka, K (2010). The Roles and Effects of Paradigms in Accounting Research. Management
Accounting Research, 21(2), 110-115
Macinati M. and Anessi-Pessina E A., (2014). Management Accounting Use and Financial
Performance in Public Healthcare Organizations: Evidence from the Italian
National Health Service. Health Policy, 117(1), 98-111.
Maestrini, V., Luzzini, D., Maccarrone, P. and Caniato, F. (2017). Supply Chain Performance
Measurement Systems: A Systematic Review and Research Agenda.
International Journal of Production Economics, 183, 299-315.
Mahama, H. (2006). Management Control Systems, Cooperation and Performance in Strategic
Supply Relationships: A Survey in the Mines. Management Accounting
Research, 17(3), 315-339.
Mahoney, T. A., Jerdee, T. H., and Carroll, S. J. (1963). Development of Managerial
Performance: A Research Approach. Cincinnati, OH: South-Western.
Maiga, A. S., Nilsson, A. and Jacobs, F. (2013). Extent of Managerial IT Use, Learning
Routines, and Firm Performance: A Structural Equations Modelling of their
Relationship. International Journal of Accounting Information Systems, 14(4),
297-320.
Malmmose, M., (2015). Management Accoounting versus Medical Professional Discourse:
Hegemony in a Public Healthcare Debate – A Case from Denmark. Critical
Perspectives on Accounting, 27, 144-159.
Manso, J. F., Annan, J., and Anane, S. S., (2013). Assessment of Logistic Management in Ghana
Health Service. International Journal of Business and Logistic Research, 3(8),
75-87.
Mardia, K. V. (1970). Measures of Multivariate Skewness and Kurtosis with Applications.
Biometrika, 57(3), 519–530.
Meilick, O. (2006). Bivariate Models of Fit in Contingency Theory: Critique and a Polynomial
Regression Analysis. Organizational Research Methods, 9(2), 161-193.
Melo, M.T., Nickel,S. and Saldanha-da-Gama,F (2009). Facility Location and Supply Chain
Management: A Review. European Journal of Operational Research, 196(2),
401–412.
Merchant K. A., (1981), The Design of the Corporate Budgeting System: Influences on
Managerial Behaviour and Performance, Accounting Review, 56, 813–29.
Merchant, K. A. (1984). Influences on Departmental Budgeting: An Empirical Examination of
a Contingency Model. Accounting, Organizations and Society, 9(3-4), 291-307.
Merchant, K. A. (1990). The Effects of Financial Controls on Data Manipulation and
Management Myopia. Accounting, Organizations and Society, 15(4), 297-313.
University of Ghana http://ugspace.ug.edu.gh

256
Meyer, A. D., Tsui, A. S., and Hinings, C. R. (1993). Configurational Approaches to
Organizational Analysis. Academy of Management Journal, 36(6), 1175–1195.
Mia, L. (1989). The Impact of Participation in Budgeting and Job Difficulty on Managerial
Performance and Work Motivation: A Research Note. Accounting,
Organizations and Society, 14(4), 347-357.
Mia, L., & Chenhall, R. H. (1994). The Usefulness of Management Accounting Systems,
Functional Differentiation and Management Effectiveness. Accounting,
Organizations and Society, 19(1), 1-13.
Miller, D. and Friesen, H. (1984). Organizations: A Quantum View. Englewood Cliffs: Prentice
Hall.
Miner, J. B. (1984). The Validity and Usefulness of Theories in an Emerging Organizational
Science. Academy of Management Review, 9, 296-306.
Ministry of Health (MOH, 2012), Heath Commodity Supply Chain Master Plan, MOH, Accra.
Mintzberg, H. (1983). Structure in Fives: Designing Effective Organizations. Englewood Cliffs:
Prentice-Hall.
Nachtmann, H. and Pohl, E., (2009). The State of Healthcare Logistics; Costs and Quality
Improvement Opportunities. Center for Innovation in Health Logistics,
University of Arkansas, AR.
North, D., (1990). Institutions, Institutional Change and Economic Performance. Cambridge
University Press, Cambridge, U.K
O’Connor, N. G., (1995). The Influence of Organizational Culture on the Usefulness of Budget
Participation by Singaporean-Chinese Managers. Accounting, Organizations
and Society, 20(5), 383-403.
Otley, D. T. (1978). Budget Use and Managerial Performance. Journal of Accounting Research,
16, 122-149.
Otley, D. T. (1980). The Contingency Theory of Management Accounting: Achievement and
Prognosis. Accounting, Organizations and Society, 5(4), 413-428.
Otley, D. (2016). Contingency Theory of Management Accounting and Control: 1980-2014.
Management Accounting Research, 31, 45-62.
Ou, C. S., Liu, F. C., Hung, Y. C. and Yen, D. C. (2010). A Structural Model of Supply Chain
Management on Firm Performance. International Journal of Operations and
Production Management, 30(5), 526-545.
Pennings, J. (1992). Structural Contingency Theory: A Reappraisal. In B. M. Staw, & L. L.
Cummings (Eds.), Research in organizational behavior, vol. 14. Greenwich CT:
JAI Press.
Pinsonneault, A., and Kraemer, K. L. (1993). Survey Research Methodology in Management
Information Systems: An Assessment. Journal of Management Information
Systems, 10(2), 75–85.
University of Ghana http://ugspace.ug.edu.gh
257
Pizzini, M. J., (2006). The Relation between Cost-System Design, Managers’ Evaluations of the
Relevance and Usefulness of Cost Data, and Financial Performance: An
Empirical Study of US Hospitals. Accounting, Organizations and Society, 31(2),
179-210.
Polater, A. and Demirdogen, O. (2018). An Investigation of Healthcare Supply Chain
Management and Patient Responsiveness: An Application on Public Hospitals.
International Journal of Pharmaceutical and Healthcare Marketing, 12(3), 325-
347.
Porter, M. E. (1985). Competitive Advantage: Creating and Sustaining Superior Performance.
New York: Free Press.
Presutti, W.D. and Mawhinney, J.R. (2007). The Supply Chain-Finance Link. Supply Chain
Management Review, 11(6), 32-38.
Qi, Y., Huo, B., Wang, Z., and Yeung, H. Y. J., (2017). The Impact of Operations and Supply
Chain Strategies on Integration and Performance. International Journal of
Production Economics, 186, 162-174.
Rahimnia, F. and Moghadasian, M. (2010). Supply Chain Leagility in Professional Services:
How to Apply Decoupling Point Concept in Healthcare Delivery System. Supply
Chain Management: An International Journal, 15(1), 80-91.
Ramos, M. M. (2004). Interaction between Management Accounting and Supply Chain
Management. Supply Chain Management: An International Journal, 9(2), 134-
138.
Raulinajtys-Grzybek, M. (2014). Cost Accounting Models Used for Price-Setting of Health
Services: An International Review. Health Policy, 118, 341-353.
Raykov, T., & Marcoulides, G. A. (2000). A first course in structural equation modeling.
Mahwah, NJ: Erlbaum.
Reusen, E. and Stouthuysen, K. (2017). Misaligned Control: The Role of Management Control
System Imitation in Supply Chains. Accounting, Organizations and Society, 61,
1-14.
Roark, D.C., (2005). Managing the Healthcare Supply Chain. Nursing Management 36, 36–40.
Rockefeller Foundation (2008). The Private Sector’s Role in Health Supply Chains: Review of
the Role and Potential for Private Sector Engagement in Developing Country
Health Supply Chains. Technical Partner Paper 13, p.1.
Rottman, J.W., and Lacity, M.C., (2006). Proven Practices for Effectively Offshoring IT Work.
MIT Sloan Management Review, Spring, pp. 56–63
Sahin F. and Robinson J.E.P. (2005). Information Sharing and Coordination in Make-to-Order
Supply Chains. Journal of Operations Management, 23: 579-98.
Said, A.A., Hassabelnaby, H.R. and Wier, B., (2003). An Empirical Investigation of the
Performance Consequences of Nonfinancial Measures. Journal of Management
Accounting Research 15, 193–223.
University of Ghana http://ugspace.ug.edu.gh
258
Samuel, C., Gonapa, K., Chuadhary, P. K. and Mishra, A. (2010). Supply Chain Dynamic in
Healthcare Services. International Journal of Health Care Quality Assurance,
23(7), 631-642.
Sapsford, R. (1999). Survey Research. Thousand Oaks, CA: Sage Publications
Schoenherr, T. and Swink, M., (2012). Revisiting the Arcs of Integration: Cross-Validations
and Extensions. Journal of Operations Management, 30(1), 99–115.
Schoenherr, T. and Swink, M., (2015). The Effects of Cross‐Functional Integration on
Profitability, Process Efficiency, and Asset Productivity. Journal of Business and
Logistics, 36(1), 69–87.
Schoonhoven, C. B. (1981). Problems with Contingency Theory: Testing Assumptions Hidden
within the Language of Contingency ̀ Theory'. Administrative Science Quarterly,
26, 349-377.
Schneller, E.S., and Smeltzer, L., (2006), Strategic Management of the Health Care Supply
Chain. Jossy-Bass.
Schulze, M., Seuring, S. and Ewering, C., (2012). Applying Activity-Based Costing in a Supply
Chain Environment. International Journal of Production Economics, 135, 716-
725.
Scott, W. R., (1998). Organizations: Relational, Natural and Open Systems. 4th Edition,
Englewood Cliffs, Nj, Prentice Hall.
Seal,W., Cullen, J., Dunlop, A., Berry, T., and Ahmed, M., (1999). Enacting a European Supply
Chain: A Case Study on the Role of Management Accounting. Management
Accounting Research, 10, 303–322.
Selviaridis, K., and Spring, M. (2018). Supply Chain Alignment as Process: Contracting,
Learning and Pay-for-Performance. International Journal of Operations and
Production Management, 38(3), 732-755.
Seuring, S. and Muller, M., (2008), ‘‘From a Literature Review to a Conceptual Framework for
Sustainable Supply Chain Management,’’ Journal of Cleaner Production, 16,
1699-1710.
Shah, N. (2004). Pharmaceutical Supply Chains: Key Issues and Strategies for Optimization.
Computers & Chemical Engineering, 28(6/7), 929-41.
Shi, M. and Yu, W., (2013). Supply Chain Management and Financial Performance: Literature
Review and Future Directions. International Journal of Productions and
Operations Management, 33(10), 1283-1317.
Simons R. (1987), Accounting Control Systems and Business Strategy: An Empirical Analysis.
Accounting, Organizations and Society, 12(4), 357–74.
Skandrani, H., Triki, A. and Baratli, B. (2011). Trust in Supply Chains, Meanings, Determinants
and Demonstrations: A Qualitative Study in an Emerging Market Context.
Qualitative Market Research: An International Journal,14(4), 391-409.
University of Ghana http://ugspace.ug.edu.gh

259
Soobaroyen, T. and Poorundersing, B. (2008). The Effectiveness of Management Accounting
Systems. Managerial Auditing Journal, 23(2), 187-219.
Southwood, K. E. (1978). Substantive Theory and Statistical Interaction: Five Models.
American Journal of Sociology, 83, 1154-1203.
Stevens, G.C. (1989). Integrating the Supply Chain. International Journal of Physical
Distribution & Logistics Management, 19(8), 3-8.
Stone, E. F. and Hollenbeck, J. R. (1984). Some Issues Associated with the Use of Moderated
Regression. Organizational Behavior and Human Performance, 34, 195-213.
Sutherland, J. M. (2015). Pricing Hospital Care: Global Budgets and Marginal Pricing
Strategies. Health Policy, 119, 1111-1118.
Sutton, S. G., Smedley, G. and Arnold, V. (2008). Accounting for Collaborative Supply Chain
Relationships: Issues and Strategies. The International Journal of Digital
Accounting Research, 4(14), 1-22.
Tan, K. C. (2001). A Framework of Supply Chain Management Literature. European Journal
of Purchasing and Supply Chain Management, 7, 39–48.
Thrane, S. and Hald, K. S. (2006). The Emergence of Boundaries and Accounting in Supply
Fields: The Dynamics of Integration and Fragmentation. Management
Accounting Research, 17, 288-314.
Tsamenyi, M. and Mills, J., (2002). Perceived Environmental Uncertainty, Organizational
Culture, Budget Participation and Managerial Performance in Ghana. Journal of
Transnational Management Development, 8(1-2), 17-51.
Tsamenyi, M., Qureshi, A. Z. and Yazdifar, H. (2013). The Contract, Accounting and Trust: A
Case Study of an International Joint Venture (IJV) in the United Arab Emirates.
Accounting Forum, 37, 182-195.
Tseng, P. H. and Liao, C. H. (2015). Supply Chain Integration, Information Technology, Market
Orientation and Firm Performance in Container Shipping Firms. The
International Journal of Logistics Management, 26(1), 82-106.
Van de Stede, W. A., Young, S. M., and Chen, C. X., (2005). Assessing the Quality of Evidence
in Empirical Management Accounting Research: The Case of Survey Studies.
Accounting, Organizations and Society, 30(7-8), 655-684.
Van der Meer-Kooistra, J. and Vosselman, E. G. J., (2000). Management Control of Interfirm
Transactional Relationships: The Case of Industrial Revolution and
Maintenance. Accounting, Organizations and Society, 25(1), 51-77.
Venkatraman, N. (1989). The Concept of Fit in Strategy Research: Toward Verbal and
Statistical Correspondence. Academy of Management Review, 14, 423-444.
Vickery, S.K., Jayaram, J., Droge, C., Calantone, R., (2003). The Effects of an Integrative
Supply Chain Strategy on Customer Service and Financial Performance: An
Analysis of Direct Versus Indirect Relationships. Journal of Operations
Management 21, 523–539.
University of Ghana http://ugspace.ug.edu.gh

260
Wadongo, B. and Abdel-Kader, M., (2014), ‘‘Contingency Theory, Performance Management
and Organizational Effectiveness in the Third Sector: A Theoretical
Framework,’’ International Journal of Productivity and Performance
Management, 63(6), 680-703.
Wardhani, V., Utarini, A., van Dijk, J.P., Post, D. and Groothoff, J.W., (2009). Determinants of
Quality Management Systems Implementation in Hospitals. Health Policy,
89(3), 239–251.
WeiBenberger, B. E. and Angelkort, H., (2011). Integration of Financial and Management
Accounting Systems: The Mediating Influence of a Consistent Financial
Language on Controllership Effectiveness. Management Accounting Research,
22, 160-180.
West, S. G., Finch, J. F., & Curran, P. J. (1995). Structural Equation Models with Non-normal
Variables: Problems and Remedies. In R. H. Hoyle (Ed.), Structural equation
modeling: Concepts, issues, and applications (pp. 56–75). Thousand Oaks, CA:
Sage.
Wiengarten, F., Humphreys, P., Gimenez, C., and Mclvor, R., (2016). Risk, Risk Management
Practices, and the Success of Supply Chain Integration. International Journal of
Production Economics, 171, 361-370.
Williamson, O.E. (2008). Outsourcing: Transaction Cost Economics and Supply Chain
Management. Journal of Supply Chain Management, 44(2), 5-16.
Wong, C. Y., Boon-Itt, S., and Wong, C. W. Y. (2011). The contingency Effects of
Environmental Uncertainty on the Relationship between Supply Chain
Integration and Operational Performance. Journal of Operations Management,
29, 604-615.
World Health Organization. The World Health Report (2000): Health Systems – Improving
Performance. World Health Organization; 2000.
World Health Organization (WHO, 2009), Assessment of Medicines Procurement and Supply
Management Systems in the Public Health Sector, A Country Report,
Department for International Development (DFID, MOH, WHO.
Ylinen, M., and Gullkvist, B., (2012). The Effects of Tolerance for Ambiguity and Task
Uncertainty on the Balanced and Combined Use of Project Controls. European
Accounting Review, 21(2), 395-415.
Zailani, S. and Rajagopal, P. (2005). Supply Chain Integration and Performance: US versus East
Asian Companies. Supply Chain Management: An International Journal, 10(5),
379-393.
Zanjirani, R., Farahani, N., and Davarzani, H., (2009) Supply Chain and Logistics in National,
International and Government Environment. Heidelberg: Physica-Verlag
Springer.
Zhou H and Benton W. C. (2007). Supply Chain Practice and Information Sharing. Journal of
Operations Managements, 25(1), 348- 65.
University of Ghana http://ugspace.ug.edu.gh

261
Zhao, L., Huo, B., Sun, L. and Zhao, X. (2013). The Impact of Supply Chain Risk on Supply
Chain Integration and Company Performance: A Global Investigation. Supply
Chain Management: An International Journal, 18(2), 115-131.
University of Ghana http://ugspace.ug.edu.gh

262
Appendix A
Questionnaire for Hospital Accountants
Introduction
Dear Respondent,
This PhD research project proposes to investigate the impact of supply chain management
(SCM) contextual factors (or its antecedents) on management accounting system (MAS) design
among Ghana’s healthcare institutions, and the impact of their relationships on performance.
The essence of this research project is to contribute to finding answers to the numerous
challenges that confront the SCM system of the health sector. Issues bothering on procurement
arrangements, inventory management, high variations in the pricing of health products,
inaccessibility of drugs either physically or financially etc., are some of the challenges
mitigating against the efficient operation of the health supply chain. These challenges as noted
in past literature, have major implications for the design and use of MAS. Management
accounting systems play significant role in SCM practices. The findings I believe, will have a
wide range of policy implications for health policy makers and health administrators.
Over 300 government and private hospitals across the country are being sampled and your
hospital has been selected to be part of the sample. I would therefore appreciate it most if you
could take some time off your busy schedule to diligently complete this questionnaire. I trust
that your honest opinion (there is no right or wrong answer) would be provided. Be assured
that this research is solely for academic purposes hence any information given will be treated
as strictly confidential.
Please take note: The information provided will be treated as confidential and the identity
of respondents as it has always been the case, is kept anonymous.
Thank you.
Directions to Respondents
The questionnaire is made up of two sections. Section A requires specific responses whilst
section B is based on ranking.
Section A
Please supply information where applicable
1. Designation/Status of Respondent (e.g. accountant, financial controller, administrator,
etc.)
…………………………………………………………………………………….
2. Years of being at this post (please provide in the box)
3. Hospital type (please tick) public Private
4. If private, is it profit-oriented? Yes No
University of Ghana http://ugspace.ug.edu.gh

263
5. Number of beds in your hospital (please provide)
6. Your hospital is located in (please tick) Urban center Rural area
Section B
This section is made up of 4 parts: A, B, C, and D. Part A concerns SCM context factors, part
B relates to organizational contextual factors and the external environment, part C concerns
management accounting system design in your hospital, and part D relates to supply chain
performance in your hospital.
Please indicate the extent to which your organization (hospital) perform the following supply
chain management (SCM) activities by checking the appropriate box/column where 1 =
strongly disagree/never/not at all 2 = disagree/hardly occur/sometimes; 3 = fairly
disagree/seldom/once a while; 4 = neutral; 5 = fairly agree/often/occasionally; 6 =
agree/regularly/most of the time; 7 = strongly agree/to a greater extent/all the time
Part A – Health Supply Management Context Factors
Strategic supplier partnerships 1 2 3 4 5 6 7
1. Our hospital maintains a high level of strategic relations with key suppliers
2. We encourage a high level of suppliers’ participation in our procurement processes
3. Our hospital establishes quick ordering systems with key vendors/suppliers
4. Our hospital solves logistic problems jointly with key vendors/suppliers
5. We include our key vendors/suppliers in our planning and goal-setting activities
6. Our hospital on frequent basis, arrange for delivery with vendors/suppliers
7. We undertake vendor inventory management or consignment stock with suppliers
8. We plan, forecast and replenish collaboratively with key vendors/suppliers
9. Our hospital dedicates capacity for key vendors/suppliers
University of Ghana http://ugspace.ug.edu.gh

264
Health Supply Chain Integration 1 2 3 4 5 6 7
1. Interorganizational logistics activities between our hospital and major key vendors/suppliers are closely coordinated
2. Our logistics activities are well integrated with the logistics activities of key vendors/suppliers
3. We have seamless integration of logistics activities with key vendors/suppliers
4. Our logistics integration is characterized by excellent distribution, transportation and/or warehousing facilities
5. Our inbound and outbound distribution of hospital supplies with key vendors/suppliers is well integrated
6. Our health organization integrates purchasing of health commodities and other medical equipment into strategic planning.
Level of Information Sharing 1 2 3 4 5 6 7
1. We inform vendors/suppliers in advance of changing needs
2. Our key vendors/suppliers share business knowledge of core business processes with us
3. We and our key vendors/suppliers exchange information that helps establish our business planning
4. Our partners share proprietary information with us
5. We share accurate risk related information with our supply chain members
6. We are willing to share real time information on demands with our suppliers
7. Information is actively shared between functional teams in our hospital
8. Members in the supply chain keep each other informed about events or changes that may affect the other party
9. We share inventory level information with key/strategic suppliers
University of Ghana http://ugspace.ug.edu.gh

265
Health Supply Chain Risk and Uncertainty 1 2 3 4 5 6 7
1. Our hospital establishes target costs/prices for health commodities with suppliers
2. Our hospital evaluates whether suppliers have achieved the target price (cost) for health products.
3. Our hospital evaluates suppliers’ cost reduction efforts for medical supplies.
4. Our hospital assesses the quality and costs of suppliers’ products
5. Our hospital holds frequent meetings with suppliers.
6. Our hospital shares with suppliers’ problems associated with medical supplies
7. Our hospital solves problems associated with medical supplies in conjunction with suppliers,
8. Our hospital compares different suppliers’ products
Part B – Management Accounting System Design
Please indicate the extent to which the following accounting information are generated for
supply chain management decisions.
Scope of Information Provided by Accounting System 1 2 3 4 5 6 7
1. Information that relates to possible future events
2. Quantification of the likelihood of future events occurring
3. Non-economic information
4. Information on broad factors external to your hospital
5. Non-financial information that relates to the efficacy, output rates, employee absenteeism
Timeliness of Accounting Information 1 2 3 4 5 6 7
1. Requested information to arrive immediately upon request
2. Information supplied to users automatically upon its receipt into information systems or as soon as processing is complete
University of Ghana http://ugspace.ug.edu.gh

266
3. Reports are provided frequently on a systematic, regular basis
4. There is no delay between event occurring and relevant information being reported to users
Integration of Accounting Information 1 2 3 4 5 6 7
1. Information on the impact that your decision will have throughout your department,
2. The influence of the individuals’ decision on your area of responsibility
3. Information on precise targets for the activities of all sections within your department
4. Information that relates to the impact that your decisions have on performance of your department
Aggregation of Accounting Information 1 2 3 4 5 6 7
1. Information provided on your different sections or functional areas in your hospital
2. Information on the effect of events on particular time periods
3. Information that has been processed to show the influence of events on different functions
4. Information on the effect of different sections’ activities on summary reports for your department and the hospital as a whole
5. Information in forms that enable you to conduct ‘‘what-if’’ analysis
6. Information in formats suitable for input into decision models
7. Costs separated into fixed and variable components
University of Ghana http://ugspace.ug.edu.gh

267
Part D – Supply Chain Performance
Minimization of Health Supply Chain Costs 1 2 3 4 5 6 7
1. The cost associated with the order fulfillment process in our hospital is getting better (has been reducing) over time
2. We have seen an improvement (reduction) in the cost associated with order fulfillment process over time
3. Based on our knowledge of the order fulfillment process we think it is cost efficient
4. The following costs have been reducing in our hospital over the past three years
a) Purchasing costs
b) Operating costs
c) Inventory costs
d) Warehouse costs
e) Distribution/Transportation costs
Utilization of Hospital Assets 1 2 3 4 5 6 7
1. Our hospital has been experiencing a growth rate in internally generated funds
2. Our hospital has been experiencing a growth rate in return on assets
3. Our hospital has been experiencing a growth rate in return on investments
Supply chain quality and speed of delivery
1. On-time delivery of drugs/medical supplies from our suppliers
2. The length of the order fulfilment process in our hospital is getting shorter with time
University of Ghana http://ugspace.ug.edu.gh

268
3. We have seen an improvement in the cycle time of the order fulfilment process with time
4. Based on our knowledge of the order fulfilment process we think it short and efficient
Health Supply Chain Flexibility 1 2 3 4 5 6 7
1. The flexibility of the order fulfilling process in our hospital is getting better with time
2. We have seen an improvement in the flexibility of the order fulfilment process with time
3. Based on our knowledge of the order fulfilling process, we thing it is flexible
Health Supply Quality 1 2 3 4 5 6 7
1. The quality of the order fulfilment process in our hospital is getting better with time
2. We have seen an improvement in the quality of the order fulfilment process with time
3. Based on our knowledge of the order fulfilment process, we think it is of high quality
University of Ghana http://ugspace.ug.edu.gh