management in the pre dialysis patient - 2017 mcgill...
TRANSCRIPT

Management in the Pre Dialysis Patient
Dr. Tiina PodymowAssociate Professor
Division of Nephrology McGill University Health Centre

Disclosures
• None

Objectives1. Understand the importance of proteinuria and use
the kidney failure risk equation to determine the likelihood that a given patient will experience renal failure
2. Recognize and treat hypertension and the complications of renal failure including anemia, bone metabolism disorders, acid base and electrolyte abnormalities
3. Recognize when patients are likely to commence long-term renal replacement therapy

Case• 73M divorce lawyer, referred to nephrology clinic Cr 180 µmol/L
• PMHx• COPD• CABG age 64• AAA rupture/repair age 65• Afib on warfarin
• Medications• Bisoprolol• Atorvastatin• Warfarin• Perindopril
• ROS: no hematuria, some ankle edema, occasional ibuprofen
• Omeprazole• Synthroid• Isosorbide mononitrate• Vitamin D

Questions/Objectives• What is the cause of his chronic kidney disease?
• What is the likely course of his CKD?
• Likelihood of needing dialysis?
• What is the best stabilization/preservation strategy
• What are the “six pillars”?
• When should patients be referred to nephrology?
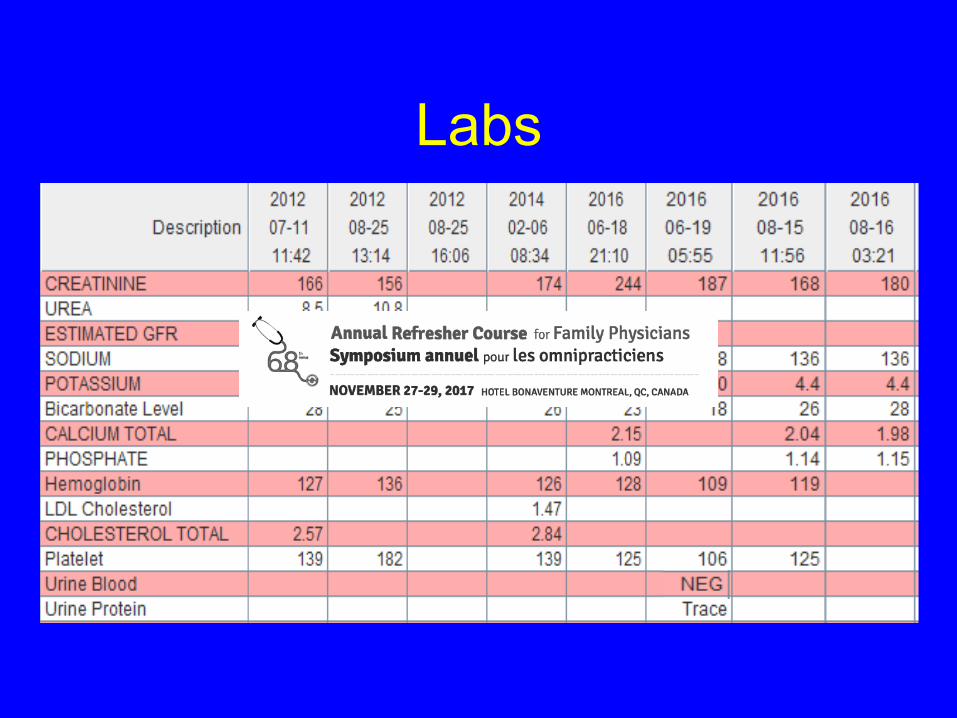
Labs
What is the likely cause of CKD?
• Burned out glomerulonephritis e.g. IgA• Diabetic nephropathy• Glomerulosclerosis• The cause is not especially relevant to
management and prognosis

Urine Protein Interpretation
• Microalbumin: answers the question: is the endothelium healthy?< 1.9 yes it is>1.9 no it might not be
• Urine protein/Cr is a surrogate for 24 hour urine collection and protein quantification
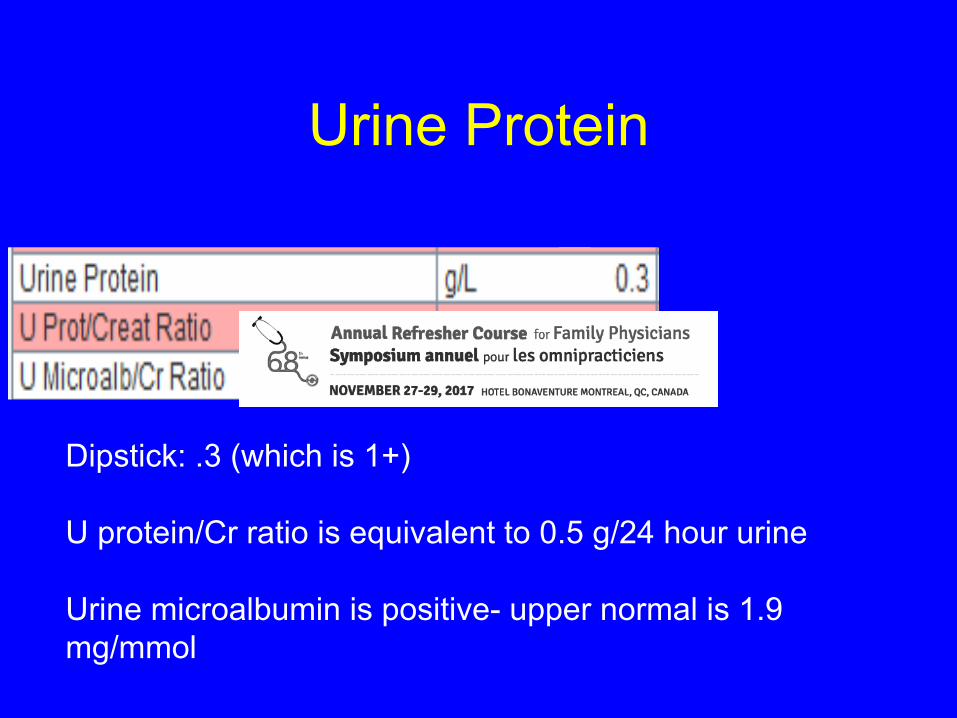
Urine Protein
Dipstick: .3 (which is 1+)
U protein/Cr ratio is equivalent to 0.5 g/24 hour urine
Urine microalbumin is positive- upper normal is 1.9 mg/mmol

Urine Protein Quantification<1 gram tubular or hemodynamic
(glomerulosclerosis- ischemic nephropathy-hypertensive nephropathy)
1-3 g nondiagnostic- could be tubular or glomerular
>3 g/24 h is always glomerular
10

Patient’s diagnosis
• Glomerulosclerosis• U protein ~ 1 g/day• Relatively stable Cr

Hypertensive Glomerulosclerosis
• Bright: “hard pulse means granular kidneys on autopsy”
• Meaning: hypertension clinically predicts glomerulosclerosis on autopsy
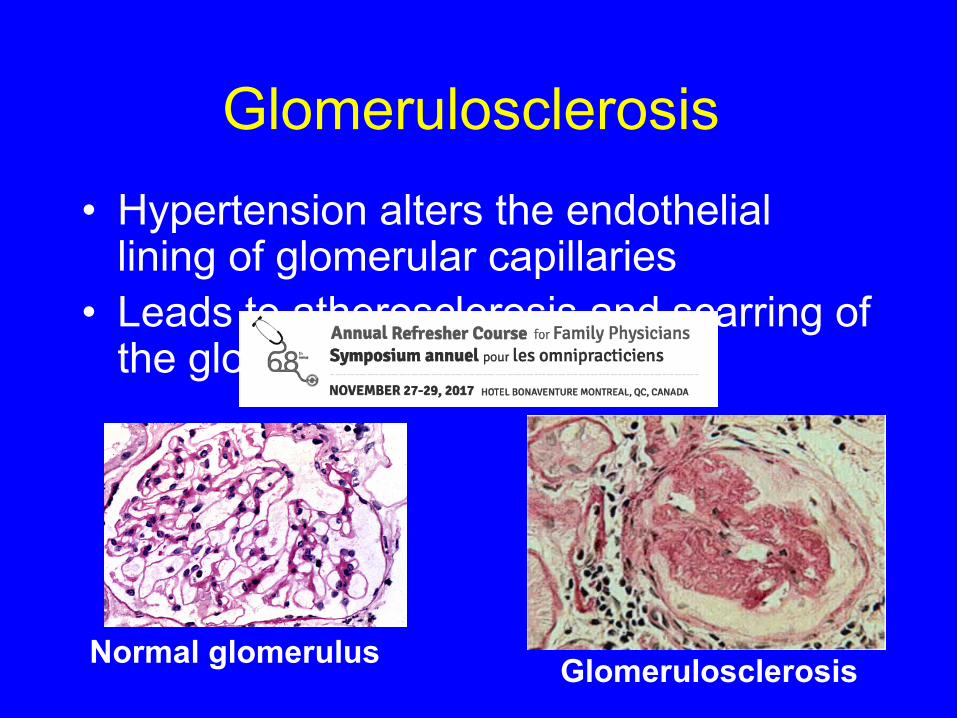
Glomerulosclerosis• Hypertension alters the endothelial
lining of glomerular capillaries• Leads to atherosclerosis and scarring of
the glomerulus
Normal glomerulus Glomerulosclerosis

Question
• If I told you that this patient also had a history of type 2 diabetes x 15 years, could his CKD be attributable to diabetic renal disease?
• Yes• No

Diabetes
Clinically: 1. Microalbuminuria2. Albuminuria3. nephrotic proteinuria4. Cr5. renal failure
Kimmelstiel Wilson lesions
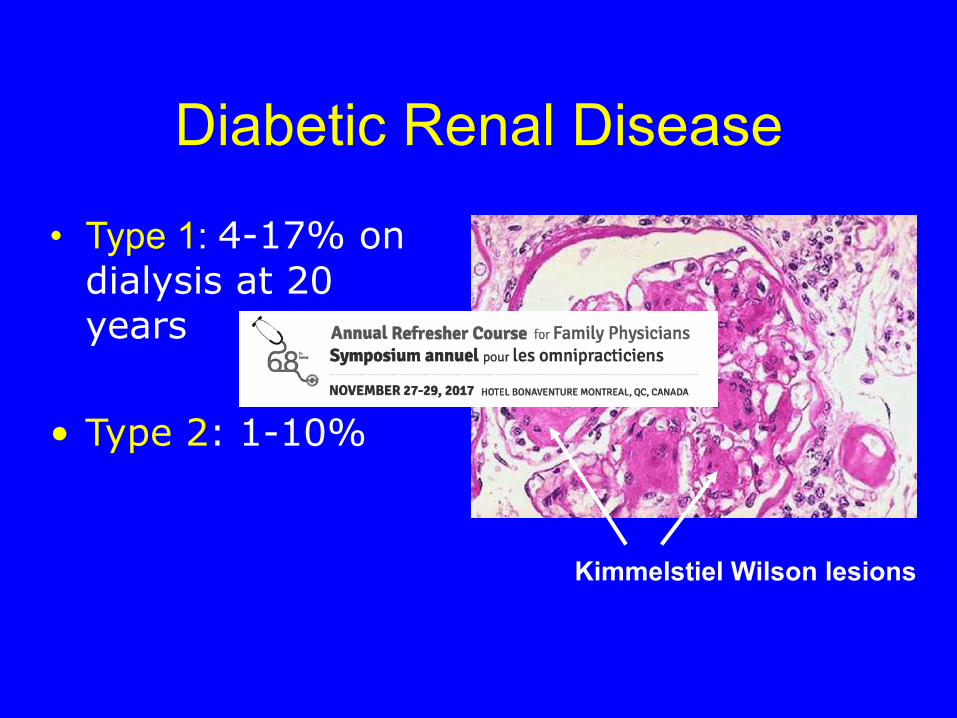
Diabetic Renal Disease
• Type 1: 4-17% on dialysis at 20 years
• Type 2: 1-10%
Kimmelstiel Wilson lesions

41F with Diabetic Nephropathy
Is there any difference in prognosis between:
1. 73M glomerulosclerosis eGFR of 30 ml/min
2. 41F with diabetic nephropathy eGFR 30 ml/min?

73M glomerulosclerosis: what is the likelihood of needing dialysis?• http://mdrd.com/ to calculate GFR• http://kidneyfailurerisk.com/

73M eGFR 31
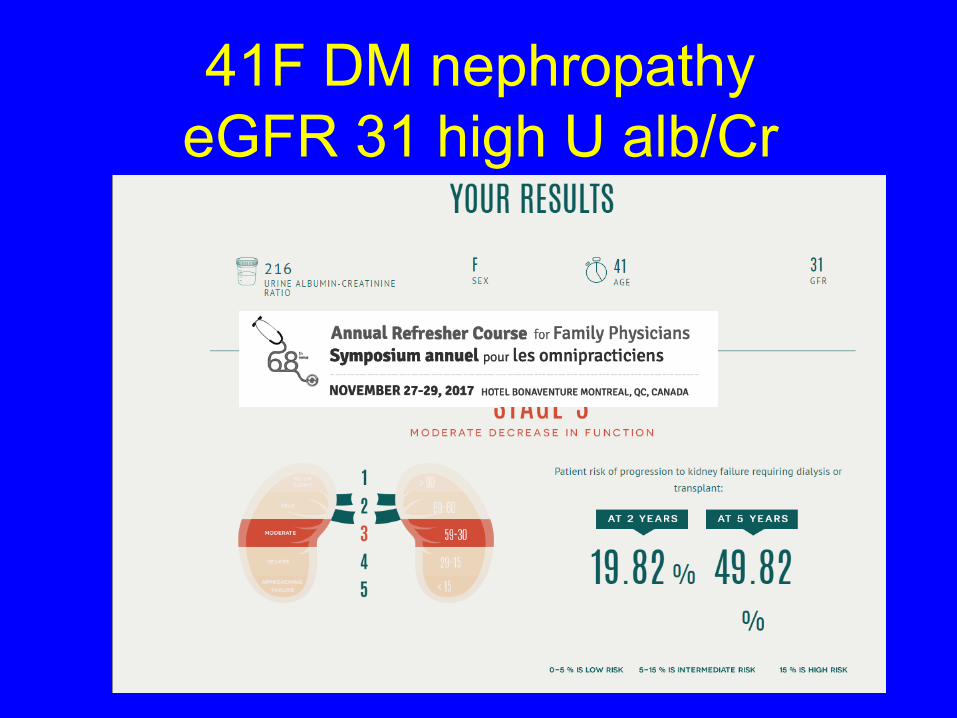
41F DM nephropathy eGFR 31 high U alb/Cr
The difference in these 2 patients: the quantity of protein in the urine.
The amount of albuminuria is a very powerful predictor for deterioration of renal function

Course of CKD due to glomerulosclerosis
• Prognosis is actually quite good
• Patients tend to be very volume sensitive-Cr fluctuates
• No NSAIDS
• Dose meds to GFR 30 ml/min (mdrd.com and Uptodate)
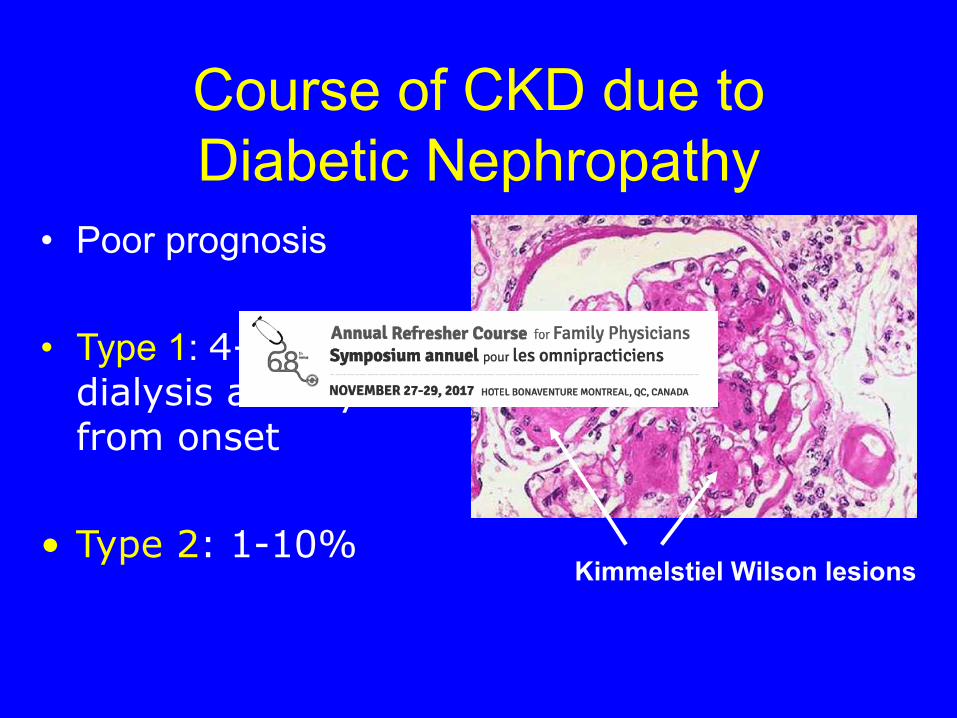
Course of CKD due to Diabetic Nephropathy
• Poor prognosis
• Type 1: 4-17% on dialysis at 20 years from onset
• Type 2: 1-10%Kimmelstiel Wilson lesions
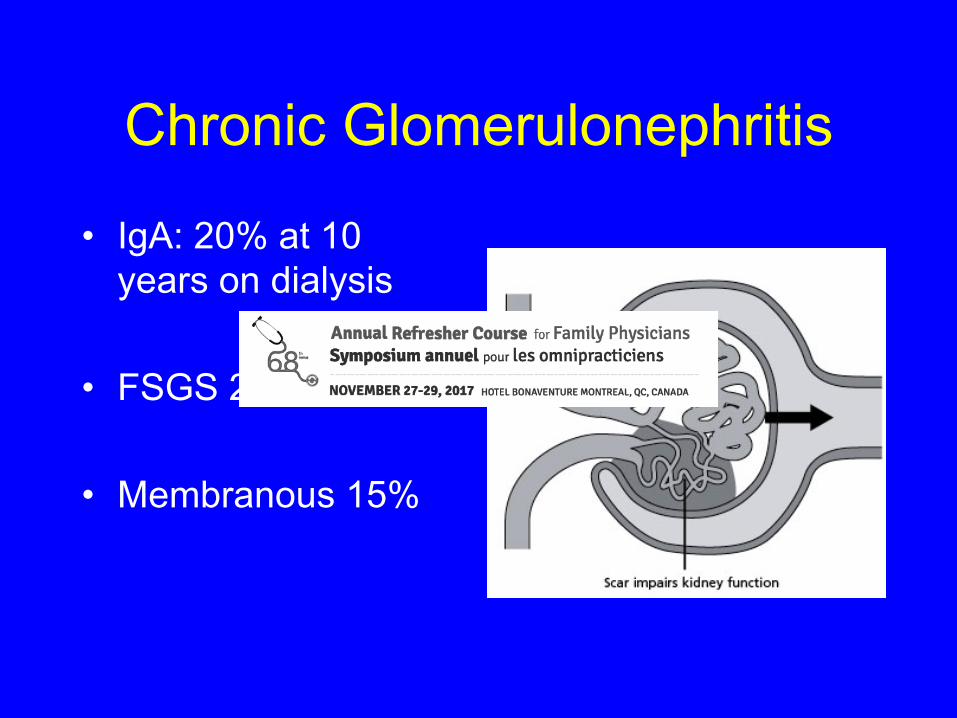
Chronic Glomerulonephritis
• IgA: 20% at 10 years on dialysis
• FSGS 25%
• Membranous 15%
Slowing the Progression of Chronic Kidney Disease

kidney.org and kdigo.org/guidelines
The National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF KDOQI)
Hypertension in CKD• Hypertension is found in 85% with stage 3 CKD
• High systemic BP transmitted to the glomerulus
• Hypertension almost always accelerates the loss of renal function
• BP is the most important thing to control to limit progression of CKD to dialysis
Hypertension and CKD• Most patients with renal failure have
hypertension and need more than 3 meds to control it
• Hydrochlorothiazide no longer works after~ CrCl <20-30 ml/min
• ACEI/ARB- expect a rise in Cr of 15%- this is OK (represents lowered intraglomerular pressure (good), not failing kidney)

Doubling Cr
Jafar, T. H. et. al. Ann Intern Med 2003;139:244-252

• Hypertension and proteinuria conspire to accelerate chronic kidney disease

Proteinuria from Diabetes• Diabetes – type 1 and type 2 are the commonest
causes of chronic renal failure leading to dialysis
• In patients with microalbuminuria treatment of blood pressure to <120/75 mm Hg and use of ACEI or ARBs can reverse proteinuria
• Before these drugs, all patients with proteinuria and CKD ended up on dialysis
• Takes ~ 10 years from onset of DM for microalbuminuria to occur
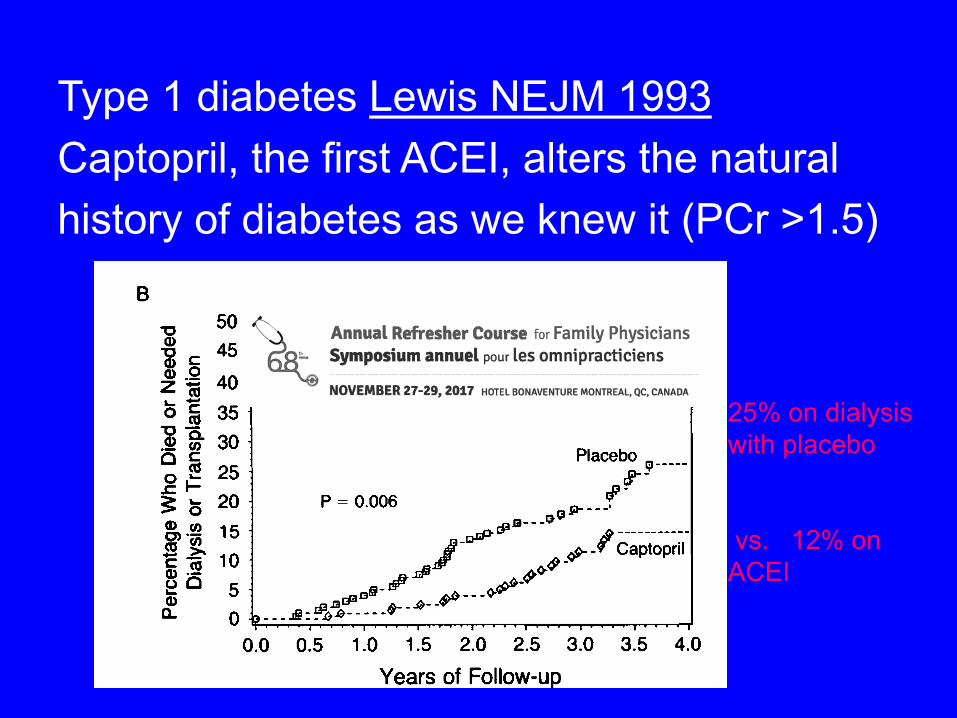
Type 1 diabetes Lewis NEJM 1993Captopril, the first ACEI, alters the naturalhistory of diabetes as we knew it (PCr >1.5)
25% on dialysis with placebo
vs. 12% on ACEI

Blood Pressure Goals• BP goal for uncomplicated hypertension is
<140/90 mm Hg,
• Proteinuria > 1 g/day with CKD, the BP goal is <130/80 mm Hg.
• HOWEVER: No benefit in nondiabetic
• patients with <1 g/day proteinuria-target 140/90
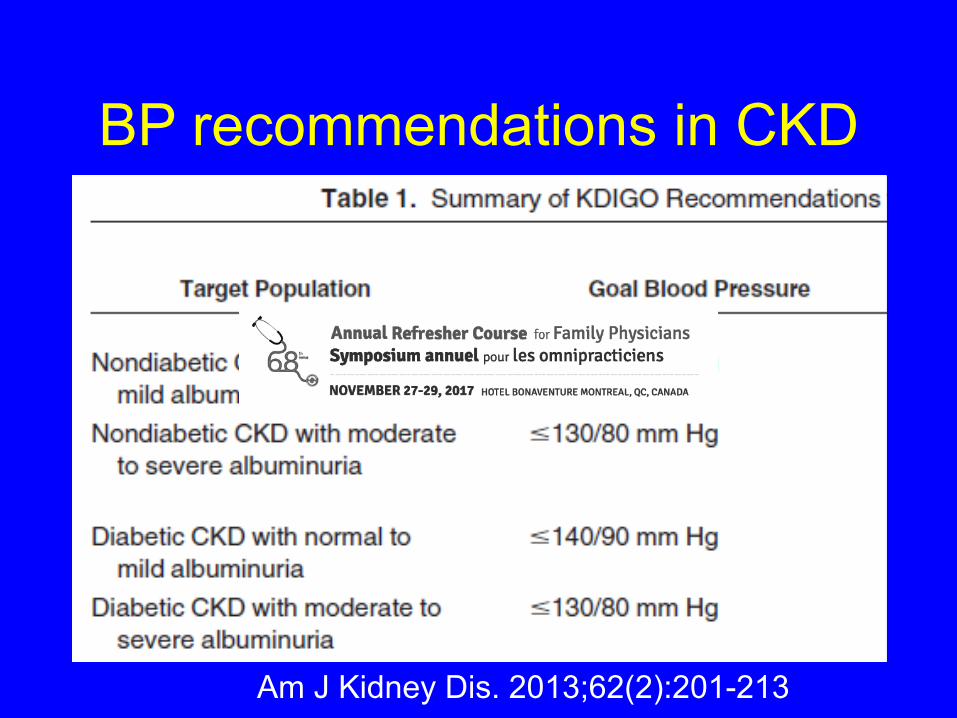
BP recommendations in CKD
Am J Kidney Dis. 2013;62(2):201-213

The 6 Pillars

Chronic Renal Insufficiency1. Anemia2. Bone disease3. Volume overload4. Hypertension5. Increased K6. Acidosis

At what eGFR would you firstexpect anemia, acid base
disturbances, etc.• 50 ml/min• 40 ml/min• 30 ml/min• 20 ml/min• 10 ml/min

1. Anemia in CKD• CrCl below 30 ml/min- usually 15-20 ml/min
• Approach to Hb <95-100
• Target Hb?
1. Check Fe, IBC, % sat and fix iron stores. 2. Then use ESA (erythrocyte stimulating
agents) erythropoetin or darbopoetin
100-120 and not more or less (increased mortality)

40
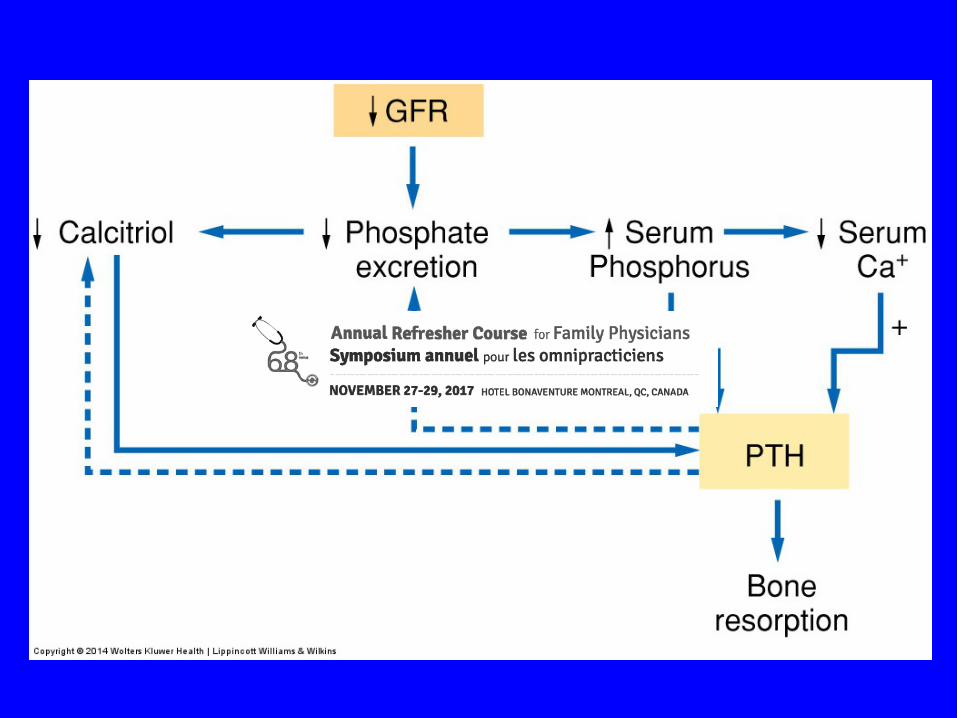
2. Secondary Hyperparathyroidism/ Bone disease
• Comes down to Ca/PO4/ and PTH• PO4 rises in renal failure
• Parathyroid is stimulated to PTH this is secondary hyperparathyroidism
• PO4 uses free Ca and bone for buffer (so Ca can become low)
• Vitamin D is not converted to 1,25 vit D
42
Management• Want normal Ca and PO4• Target PTH 5 x normal (~50 max)
• Low PO4 diet – renal diet
• Binders: CaCO3, Sevelamer, Lanthanum bind PO4 in gut
• Vitamin D = Calcitriol is 1,25 vitamin D and it suppresses PTH BUT it increases PO4 by increasing its gut absorption (so control PO4 first before Rxing)
• Cinacalcet (Sensipar)- a calcimimetic for the calcium sensing receptor in the parathyroid gland- “medical parathyroidectomy” for patients with 3o hyperPTH

43
Ca (2.1-2.6)
PO4(N 0.8–1.6)
PTH pmol/L (target is 35-50)
Rx
Normal 3 35
Normal Normal 70
2.8 2 50
Normal 3 on CaCO3
35
Normal Normal 300 (tertiary hyperPTH)
Start 1,25 vit D (calcitriol)
Low PO4 diet +Start CaCO3
Start sevalemer or lanthanum
Start cinacalcet
Start sevalemer or lanthanum
3. Volume overload• Really becomes a management issue if
LVEF is low
• Fluid restriction
• Furosemide in renal failure doses
• BEWARE of pre renal failure
45
4. Acidosis
• The kidney can’t generate bicarbonate
• Want to give bicarb?
• 500 BID or TID
• Target bicarb >21 mmol/L
• Bicarbonate Supplementation Slows Progression of CKD JASN September 1, 2009 vol. 20 no. 9
5. Increased K• Renal diet
• Avoid K increasing meds- NSAIDS (not to mention that they kill the kidney)
• Kayexelate is a not • a great long term • solution- it
is poorly tolerated

6. Dialysis• Planned start, with a functioning fistula or CAPD
catheter
• GFR 10 ml/min followed monthly in nephrology clinic
• Guided by, but not based on GFR
• Based on how the patient feels
• If the patient starts to have decreased appetite, nausea, feels unwell, trouble concentrating with GFR 15 ml/min or less- start that day or the next

6. Dialysis planning• Need at least 8 weeks for a surgically
created fistula to mature• Save an arm

Peritoneal Dialysis6 weeks for a Tenchoff catheter site to heal
CKD eGFR ≤30 ml/min• Treat or consider
1. Hb and Fe/ESA treatment2. Ca PO4 PTH3. HCO34. K5. Volume status6. Prepare for dialysis- save an arm
• BP to target
• Dose medications to current GFR (Uptodate), and hold the ones that are overtly nephrotoxic like NSAIDS

When to refer to a Nephrologist?
• CKD with kidney failure risk score calculated ≥3% at 5 years
• More than the equivalent of 1 g/day proteinuria or 100 mg/mmol albuminuria and any Cr
• Proteinuria with hematuria
• Pregnancy or contemplating pregnancy with any degree of renal impairment or proteinuria
• Renal disease with uncontrollable blood pressure

AKI on CKD• CKD patients are especially volume sensitive
• NSAIDs, aminoglycoside antibiotics, and radiocontrast media commonly aggravate renal disease
• NSAIDS with ACEI/ARB = AKI
• educate patient to NEVER take Ibuprofen (Advil, Motrin), Aleve, Celebrex etc. (often Rx by surgery)
– Aspirin or Tylenol are fine

Summary• Use U albumin and U protein/Cr ratio to diagnose and risk
stratify
• Use MDRD.com and kidneyfailurerisk.com
• BP is the most important thing for secondary prevention, to limit progression of CRF to dialysis
• use ACEI/ARB for proteinuric patients
• Remember the 6 pillars
• Dose meds to to eGFR
• Nephrologist should co-follow eGFR ≤30 ml/min