management of chest pain and heart failure. cardiac rehabilitation and secondary prevention wt bong...
TRANSCRIPT

Management of chest pain and heart failure. Cardiac rehabilitation
and secondary prevention
WT BongDept of Family Medicine, HUKM

Case scenario 1
• 60 yo gentleman, a known case of DM for the past 2 years complains of chest pain for the past 2-3 months when he walks more than 10 minutes. The chest pain radiates to left arm, lasts 5 min, relieved by rest. Currently during his visit to the primary care clinic, he has no chest pain. He is a smoker for the past 40 years. He is on metformin 500mh bd only. Clinically, BP 120/60mmHg and cardiovascular examination was unremarkable.

Patient comes in with chest pain..
• ?cardiovascular– Cardiac.
• MV prolapse.pericarditis• ischemic
– Non cardiac. Aortic dissection• ?gastrointestinal. GERD• ?Musculoskeletal.fibromyalgia.• ?pulmonary• ?psychogenic

Patient comes in with chest pain..
• ?cardiovascular– Cardiac.
• MV prolapse.pericarditis• ischemic
– Non cardiac. Aortic dissection• ?gastrointestinal. GERD• ?Musculoskeletal.fibromyalgia.• ?pulmonary• ?psychogenic

We start with stable angina..
• By definition. Clinical syndrome characterised by – discomfort in chest, jaw, shoulder, back or arm– Typically aggravated by exertion or emotional
stress– Reduced by rest or GTN

• Most common cause for stable angina is atherosclerotic coronary artery disease (CAD)
• Other causes could be– Hypertrophic cardiomyopathy– Aortic stenosis– Coronary vasospasm etc

Atherosclerosis process in coronary
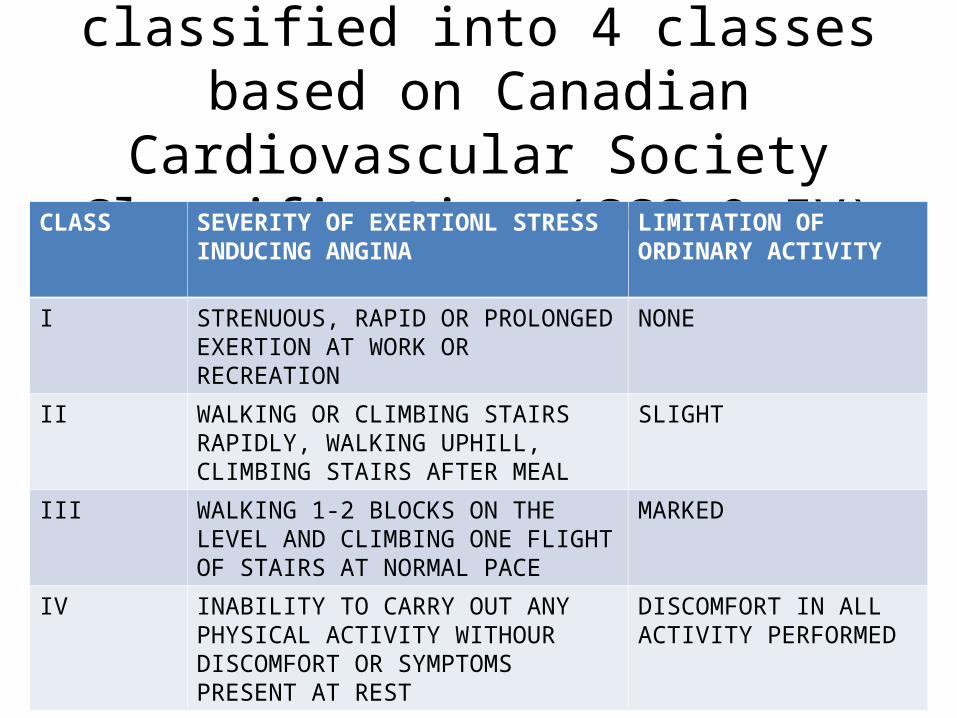
Stable angina is classified into 4 classes based on Canadian Cardiovascular
Society Classification (CCS 0-IV)CLASS SEVERITY OF EXERTIONL STRESS
INDUCING ANGINALIMITATION OF ORDINARY ACTIVITY
I STRENUOUS, RAPID OR PROLONGED EXERTION AT WORK OR RECREATION
NONE
II WALKING OR CLIMBING STAIRS RAPIDLY, WALKING UPHILL, CLIMBING STAIRS AFTER MEAL
SLIGHT
III WALKING 1-2 BLOCKS ON THE LEVEL AND CLIMBING ONE FLIGHT OF STAIRS AT NORMAL PACE
MARKED
IV INABILITY TO CARRY OUT ANY PHYSICAL ACTIVITY WITHOUR DISCOMFORT OR SYMPTOMS PRESENT AT REST
DISCOMFORT IN ALL ACTIVITY PERFORMED

• However, it might become unstable, which is unstable angina, with possible progression to NSTEMI and STEMI too

Diagnosis of stable angina can be established by
• Clinical assessment– Look for complication of CAD.murmur(MR).septal
defect.sign of cardiomegaly.CHF– Other site of atherosclerosis.carotid
bruit.peripheral vascular disease.aortic aneurysm– Risk factor for atherosclerosis.hpt.metabolic syn– Other cause of angina.HOCM.aortic stenosis
• Lab test• Specific cardiac investigation

• Lab test to establish CVS risk factor– FLP. FBS. homocysteine level– Determine prognosis, creatinine– CXR only if suspect CHF if want to see calcification,
cardiomegaly/atrial enlargement, valvular disease, pulmonary congestion (help establish prognosis)
• Specific cardiac investigation

• Specific cardiac investigation, non invasive– ECG. See previous ischemia, LVH, BBB, arrhythmia
or conduction defect– Stress test. More sensitive and specific than
resting ECG– Echo.when there is abnormal auscultation suggest
valvular, if HCM or prev MI changes on ECG, SSx CHF , to study diastolic function

Risk-stratify our patient
• For the purpose of prognosis + treatment (revascularize in high risk patient)

Clinical history – important predictor of adverse outcome in established CAD
DM HPT Metabolic syndrome
Current smoker Increasing age Prior MI
SSx of CHF Recent onset or progressive
angina
Responsiveness of angina to therapy
dyslipidaemia

Risk stratify .. Higher risk if ECG shows
Evidence of prior MI
LBBB Second of third degree
AV block
LVH AF

Other aspects to be considered in risk-stratifying
• Stress test• Ventricular function• COROS LVEF 12- year
survival rate (p<0.0001)
< 35 % 21 %
35-49 % 54 %
> 50 % 73 %

Treatment goal
• Prevent MI & death• Improve SSx of angina & increase QoL
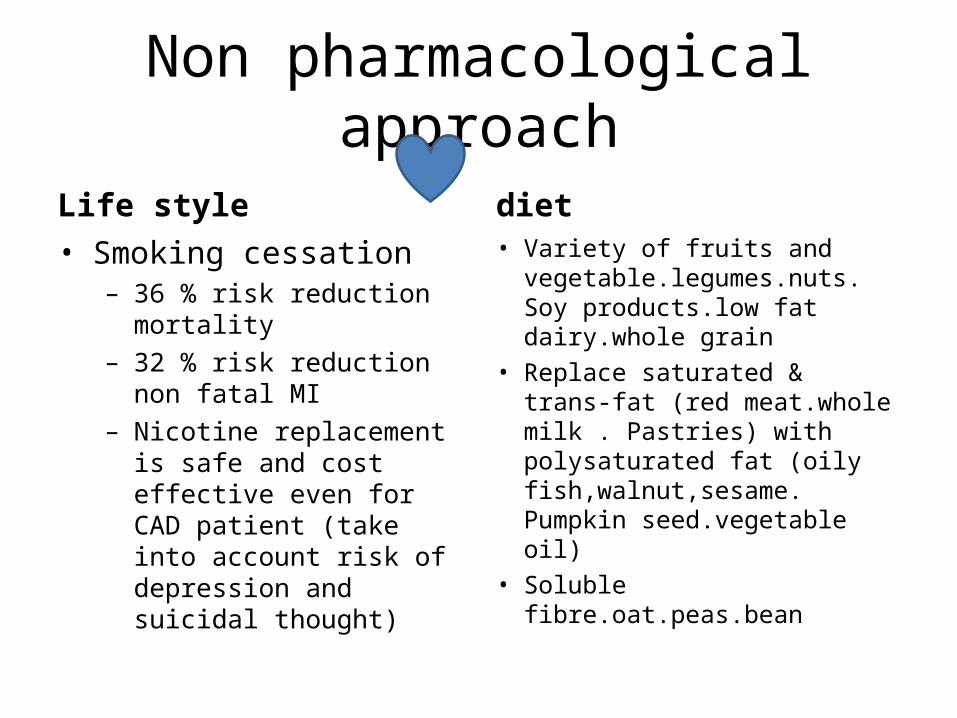
Non pharmacological approach
Life style• Smoking cessation
– 36 % risk reduction mortality– 32 % risk reduction non fatal
MI– Nicotine replacement is safe
and cost effective even for CAD patient (take into account risk of depression and suicidal thought)
diet• Variety of fruits and
vegetable.legumes.nuts. Soy products.low fat dairy.whole grain
• Replace saturated & trans-fat (red meat.whole milk . Pastries) with polysaturated fat (oily fish,walnut,sesame. Pumpkin seed.vegetable oil)
• Soluble fibre.oat.peas.bean

Alcohol restriction. Moderate/beneficial. Insufficient evidence
Physical activity. 30min 3-4x/week
Target BP <130/80
DMGenerally target HbA1c < 6.5 %. Individualize as hypoglycemia worsen angina & increase mortality
Keep waist circumference< 85 cm for men< 80 cm for women
Correct anaemiaCorrect hyperthyroid state
LDL < 1.8 ( primary target) HDL > 1.0 male, 1.2 female( secondary target)
TG < 1.7(secondary target)

education
Can also take GTN as preventive measure if
patient know he is going to have attack while carrying
out some activity
If SSx persist more than 10min at rest or not
improved after 3 tablet of GTN, advice to go to
hospital
Self management
During acute anginal attack-Restrain activity-GTN S/L or spray-Sit . Hypotension. Headache after GTN

Antithrombotic
ASA 75-150mg od. Lower MI, cardiac death or strokeTake into account GI side effect
*double antiplatelet not warranted in angina
Antithrombotic
Clopidogrel 75mg -more effective than ASA in peripheral vascular disease
Ticlopidine – proven efficacy in stroke and post-PCI, no evidence in angina
Lipid lowering
Statin reduce mortality & CV event by 20 – 30 %
Can add ezetimide if target not reached with statin
ACEi
For secondary prevention in post MI + reduced EF < 40 %
Recommended for all patients with CAD esp with concomitant LV dysfunction/DM
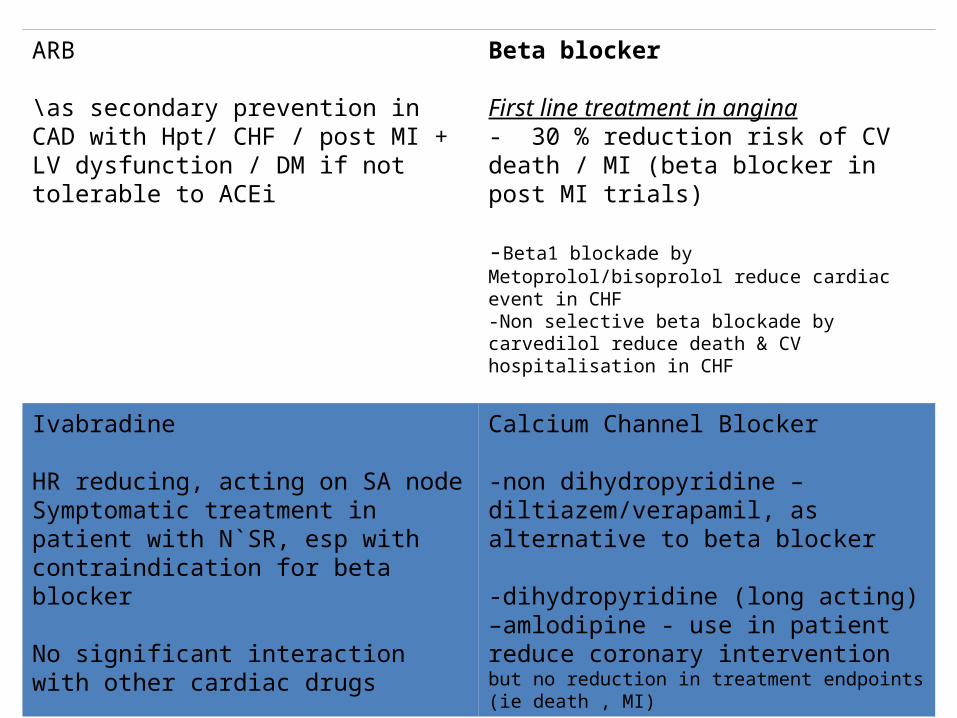
ARB
\as secondary prevention in CAD with Hpt/ CHF / post MI + LV dysfunction / DM if not tolerable to ACEi
Beta blocker
First line treatment in angina- 30 % reduction risk of CV death / MI (beta blocker in post MI trials)
-Beta1 blockade by Metoprolol/bisoprolol reduce cardiac event in CHF-Non selective beta blockade by carvedilol reduce death & CV hospitalisation in CHF
Ivabradine
HR reducing, acting on SA nodeSymptomatic treatment in patient with N`SR, esp with contraindication for beta blocker
No significant interaction with other cardiac drugs
Calcium Channel Blocker
-non dihydropyridine – diltiazem/verapamil, as alternative to beta blocker
-dihydropyridine (long acting) –amlodipine - use in patient reduce coronary intervention but no reduction in treatment endpoints (ie death , MI)

Nitrates
(long acting – isordil,imdur)
Symptomatic improvement of anginaNo prognostic benefit
Trimetazidine
(Vasteral MR)
symptomatic relief of anginaSafe and effective in patient with ED
Dipyridamole
(Persanthine)
not recommended, poor antithrombotic efficacy in angina
Anticoagulant
Not indicated unless has AF

revascularization
• PCI or CABG– In high risk group it is firstline treatment
• Significant LMS ( > 50% stenosis)• Significant proximal mutivessel involvement• Multivessel disease with impaired LV function with
proven viable myocardium– Or if failed medical treatment to control angina
SSx– In asymptomatic patient, consider if there is
extensive inducible ischaemia (stress test)

What if it is aMI ?
Chest pain
ECG ,cardiac biomarker
STEMI
Concomitant initial management
Sublingual GTN, continuous ECG monitoring, oxygen, ASA, clopidogrel, analgesia
Assessment for reperfusion
< 3hrs 3-12hrs > 12 hrs

Onset of symptoms < 3 hrs 3-12 hrs > 12 hrs
Preferred options Primary PCI (preferred in high risk patient or contraindicated for thrombolytic) or fibrinolytic
Primary PCI (if door to balloon time < 90min)
Medical therapy +/- anti thrombotics
Second options fibrinolytics Primary PCI ( if clinically indicated)
Concomitant therapy
Anti thromboticsBeta blockers
ACEi / ARBStatins
NitratesCCB

Secondary prevention
• Basically similar to angina which includeSmoking cessation diet Regular exercise
BP control Glycemic control Antiplatelet agent*consider dual antiplatelet 1mth-1yr depend on stent used
Beta blocker ACEi and ARB Lipid lowering

• Oral Anticoagulant (warfarin)– If AF– LV thrombus for 3-6mths

Secondary prevention
• Hormone replacement therapy is not beneficial for secondary prevention
• Postmenopausal women who were taking HRT at the time of STEMI should discontinue it
• Vitamin E and antioxidants have no clinical benefit
• Garlic, lecithin, vitamin A and C are not beneficial

Heart failure

Heart failure
• Is a complex clinical syndrome results from structural or functional impairment of ventricular filling or ejection of blood
• Cardinal manifestation are dyspnea, fatigue, which may limit effort tolerance, and fluid retention, which may lead to pulmonary or splanchnic congestion or peripheral edema.

Definition of Heart FailureClassification Ejection
FractionDescription
I. Heart Failure with Reduced Ejection Fraction (HFrEF)
≤40% Also referred to as systolic HF. Randomized clinical trials have mainly enrolled patients with HFrEF and it is only in these patients that efficacious therapies have been demonstrated to date.
II. Heart Failure with Preserved Ejection Fraction (HFpEF)
≥50% Also referred to as diastolic HF. Several different criteria have been used to further define HFpEF. The diagnosis of HFpEF is challenging because it is largely one of excluding other potential noncardiac causes of symptoms suggestive of HF. To date, efficacious therapies have not been identified.
a. HFpEF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their characteristics, treatment patterns, and outcomes appear similar to those of patient with HFpEF.
b. HFpEF, Improved >40% It has been recognized that a subset of patients with HFpEF previously had HFrEF. These patients with improvement or recovery in EF may be clinically distinct from those with persistently preserved or reduced EF. Further research is needed to better characterize these patients.

Stages, Phenotypes and Treatment of HF
STAGE AAt high risk for HF but without structural heart
disease or symptoms of HF
STAGE BStructural heart disease
but without signs or symptoms of HF
THERAPYGoals· Control symptoms· Improve HRQOL· Prevent hospitalization· Prevent mortality
Strategies· Identification of comorbidities
Treatment· Diuresis to relieve symptoms
of congestion· Follow guideline driven
indications for comorbidities, e.g., HTN, AF, CAD, DM
· Revascularization or valvular surgery as appropriate
STAGE CStructural heart disease
with prior or current symptoms of HF
THERAPYGoals· Control symptoms· Patient education· Prevent hospitalization· Prevent mortality
Drugs for routine use· Diuretics for fluid retention· ACEI or ARB· Beta blockers· Aldosterone antagonists
Drugs for use in selected patients· Hydralazine/isosorbide dinitrate· ACEI and ARB· Digoxin
In selected patients· CRT· ICD· Revascularization or valvular
surgery as appropriate
STAGE DRefractory HF
THERAPYGoals· Prevent HF symptoms· Prevent further cardiac
remodeling
Drugs· ACEI or ARB as
appropriate · Beta blockers as
appropriate
In selected patients· ICD· Revascularization or
valvular surgery as appropriate
e.g., Patients with:· Known structural heart disease and· HF signs and symptoms
HFpEF HFrEF
THERAPYGoals· Heart healthy lifestyle· Prevent vascular,
coronary disease· Prevent LV structural
abnormalities
Drugs· ACEI or ARB in
appropriate patients for vascular disease or DM
· Statins as appropriate
THERAPYGoals· Control symptoms· Improve HRQOL· Reduce hospital
readmissions· Establish patient’s end-
of-life goals
Options· Advanced care
measures· Heart transplant· Chronic inotropes· Temporary or permanent
MCS· Experimental surgery or
drugs· Palliative care and
hospice· ICD deactivation
Refractory symptoms of HF at rest, despite GDMT
At Risk for Heart Failure Heart Failure
e.g., Patients with:· Marked HF symptoms at
rest · Recurrent hospitalizations
despite GDMT
e.g., Patients with:· Previous MI· LV remodeling including
LVH and low EF· Asymptomatic valvular
disease
e.g., Patients with:· HTN· Atherosclerotic disease· DM· Obesity· Metabolic syndrome orPatients· Using cardiotoxins· With family history of
cardiomyopathy
Development of symptoms of HF
Structural heart disease

Classification of Heart FailureACCF/AHA Stages of HF NYHA Functional Classification
A At high risk for HF but without structural heart disease or symptoms of HF.
None
B Structural heart disease but without signs or symptoms of HF.
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF.
C Structural heart disease with prior or current symptoms of HF.
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF.
II Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF.
III Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF.
IV Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.
D Refractory HF requiring specialized interventions.

Physical examination• BMI and evidence of weight loss• Bp, supine and upright( orthostatic changes – volume depletion)• Pulse – strength and regularity• JVP• Extra heart sound, murmur, apex beat displacement, RV heave• Pulmonary status• Hepatomegaly• Peripheral edema

Lab investigation• Class I• 1.Initial laboratory evaluation of patients presenting with HF should include complete
blood count, urinalysis, serum electrolytes (including calcium and magnesium), blood urea nitrogen, serum creatinine, glucose, fasting lipid profile, liver function tests, and thyroid-stimulating hormone. (Level of Evidence: C)
• 2.Serial monitoring, when indicated, should include serum electrolytes and renal function. (Level of Evidence: C)
• 3.A 12-lead ECG should be performed initially on all patients presenting with HF. (Level of Evidence: C)
• Class Iia• 1.Screening for hemochromatosis or HIV is reasonable in selected patients who present
with HF (Level of Evidence: C)• 2.Diagnostic tests for rheumatologic diseases, amyloidosis, or pheochromocytoma are
reasonable in patients presenting with HF in whom there is a clinical suspicion of these diseases. (Level of Evidence: C)

Recommendations for Biomarkers in HFBiomarker, Application Setting COR LOE
Natriuretic peptides
Diagnosis or exclusion of HFAmbulatory,
AcuteI A
Prognosis of HFAmbulatory,
AcuteI A
Achieve GDMT Ambulatory IIa BGuidance of acutely decompensated HF therapy
Acute IIb C
Biomarkers of myocardial injury
Additive risk stratificationAcute,
Ambulatory I A
Biomarkers of myocardial fibrosis
Additive risk stratification
Ambulatory
IIb B
AcuteIIb A
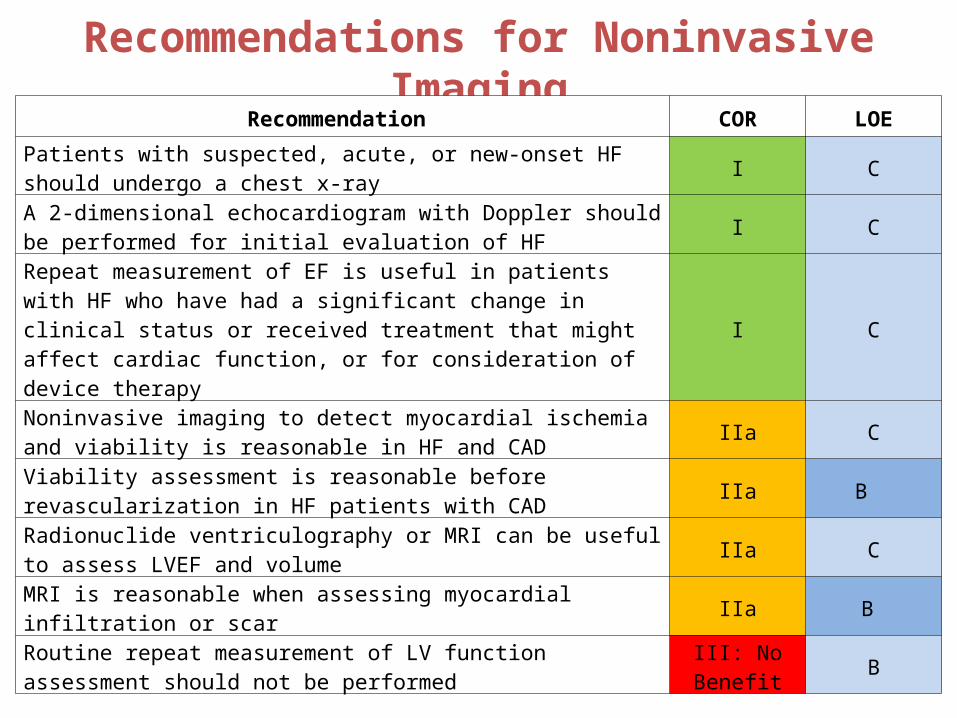
Recommendations for Noninvasive Imaging
Recommendation COR LOE
Patients with suspected, acute, or new-onset HF should undergo a chest x-ray
I C
A 2-dimensional echocardiogram with Doppler should be performed for initial evaluation of HF
I C
Repeat measurement of EF is useful in patients with HF who have had a significant change in clinical status or received treatment that might affect cardiac function, or for consideration of device therapy
I C
Noninvasive imaging to detect myocardial ischemia and viability is reasonable in HF and CAD
IIa C
Viability assessment is reasonable before revascularization in HF patients with CAD
IIa B
Radionuclide ventriculography or MRI can be useful to assess LVEF and volume
IIa C
MRI is reasonable when assessing myocardial infiltration or scar IIa B
Routine repeat measurement of LV function assessment should not be performed
III: No Benefit
B

ACC AHA heart failure 2013
• Treament based on stages of heart failure

ACCF/AHA Stages of HF NYHA Functional ClassificationA At high risk for HF but without structural
heart disease or symptoms of HFnone
B Structural heart disease but without signs or symptoms of HF
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF.
C Structural heart disease with prior or current symptoms of HF
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF.
II Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF.
III Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF.
IV Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.
D Refractory HF requiring specialized interventions
IV Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.

ACC AHA heart failure 2013
• Stage A: Recommendations• Class I• 1.Hypertension and lipid disorders should be controlled in
accordance with contemporary guidelines to lower the risk of HF(Level of Evidence: A)
• 2.Other conditions that may lead to or contribute to HF, such as obesity, diabetes mellitus, tobacco use, and known cardiotoxic agents, should be controlled or avoided. (Level of Evidence: C)

HFSA 2010 Practice Guideline (3.1)
Heart Failure Prevention
A careful and thorough clinical assessment, with appropriate investigation for known or potential risk factors, is recommended in an effort to prevent development of LV remodeling, cardiac dysfunction, and HF. Strength of Evidence = A
Adapted from:

HFSA 2010 Practice Guideline (3.2)
HF Risk Factor Treatment GoalsRisk Factor Goal
Hypertension Generally < 130/80
Diabetes See ADA guidelines1
Hyperlipidemia See NCEP guidelines2
Inactivity 20-30 min. aerobic 3-5 x wk.
Obesity Weight reduction < 30 BMI
Alcohol Men ≤ 2 drinks/day, women ≤ 1
Smoking Cessation
Dietary Sodium Maximum 2-3 g/day 1Diabetes Care 2006; 29: S4-S42
2JAMA 2001; 285:2486-97
Adapted from:

Treating Hypertension to Prevent HF
Aggressive blood pressure control:
Aggressive BP control in patients with prior MI:
Decreasesrisk of new HF
by ~ 80%
Decreasesrisk of new HF
by ~ 50%56% in T2DM
Decreasesrisk of new HF
by ~ 50%56% in T2DM
Lancet 1991;338:1281-5 (STOP-HypertensionJAMA 1997;278:212-6 (SHEP)UKPDS Group. UKPDS 38. BMJ 1998;317:703-713

HFSA 2010 Practice Guideline (3.3-3.4)
Prevention—ACEI and Beta Blockers
ACE inhibitors are recommended for prevention of HF in patients at high risk for this syndrome, including those with:
– Coronary artery disease– Peripheral vascular disease– Stroke– Diabetes and another major risk factor
Strength of Evidence = A
ACE inhibitors and beta blockers are recommended for all patients with prior MI.
Strength of Evidence = A

HFSA 2010 Practice Guideline (4.8, 4.10)
Heart Failure Patient EvaluationRecommended evaluation for patients with a diagnosis of HF:
– Assess clinical severity and functional limitation by history, physical examination, and determination of functional class*
– Assess cardiac structure and function– Determine the etiology of HF– Evaluate for coronary disease and myocardial ischemia– Evaluate the risk of life threatening arrhythmia– Identify any exacerbating factors for HF– Identify co-morbidities which influence therapy– Identify barriers to adherence and compliance Strength of Evidence = C
*Metrics to consider include the 6-minute walk test and NYHA functional class
Adapted from:

Recommendations for Treatment of Stage B HF
Recommendations COR LOE
In patients with a history of MI and reduced EF, ACE inhibitors or ARBs should be used to prevent HF
I A
In patients with MI and reduced EF, evidence-based beta blockers should be used to prevent HF
I B
In patients with MI, statins should be used to prevent HF I A
Blood pressure should be controlled to prevent symptomatic HF I A
ACE inhibitors should be used in all patients with a reduced EF to prevent HF
I A
Beta blockers should be used in all patients with a reduced EF to prevent HF
I C
An ICD is reasonable in patients with asymptomatic ischemic cardiomyopathy who are at least 40 d post-MI, have an LVEF ≤30%, and on GDMT
IIa B
Nondihydropyridine calcium channel blockers may be harmful in patients with low LVEF
III: Harm C

Stage C
Treatment of Stages A to D

Nonpharmacological Interventions
Treatment of Stages A to D

Stage C: Nonpharmacological
InterventionsPatients with HF should receive specific education to facilitate HF self-care.
Exercise training (or regular physical activity) is recommended as safe and effective for patients with HF who are able to participate to improve functional status.
Sodium restriction is reasonable for patients with symptomatic HF to reduce congestive symptoms.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for Stage C
HFrEF
Treatment of Stages A to D

Pharmacologic Treatment for Stage C HFrEF
HFrEF Stage CNYHA Class I – IV
Treatment:
For NYHA class II-IV patients. Provided estimated creatinine
>30 mL/min and K+ <5.0 mEq/dL
For persistently symptomatic African Americans, NYHA class III-IV
Class I, LOE AACEI or ARB AND
Beta Blocker
Class I, LOE CLoop Diuretics
Class I, LOE AHydral-Nitrates
Class I, LOE AAldosterone Antagonist
AddAdd Add
For all volume overload, NYHA class II-IV patients

Pharmacological Treatment for
Stage C HFrEF (cont.)Diuretics are recommended in patients with HFrEF who have evidence of fluid retention, unless contraindicated, to improve symptoms.
ACE inhibitors are recommended in patients with HFrEF and current or prior symptoms, unless contraindicated, to reduce morbidity and mortality.
ARBs are recommended in patients with HFrEF with current or prior symptoms who are ACE inhibitor-intolerant, unless contraindicated, to reduce morbidity and mortality.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Drugs Commonly Used for HFrEF (Stage C HF)
Drug Initial Daily Dose(s) Maximum Doses(s)Mean Doses Achieved in
Clinical TrialsACE InhibitorsCaptopril 6.25 mg 3 times 50 mg 3 times 122.7 mg/d (421)Enalapril 2.5 mg twice 10 to 20 mg twice 16.6 mg/d (412)Fosinopril 5 to 10 mg once 40 mg once ---------Lisinopril 2.5 to 5 mg once 20 to 40 mg once 32.5 to 35.0 mg/d (444)Perindopril 2 mg once 8 to 16 mg once ---------Quinapril 5 mg twice 20 mg twice ---------Ramipril 1.25 to 2.5 mg once 10 mg once ---------Trandolapril 1 mg once 4 mg once ---------ARBsCandesartan 4 to 8 mg once 32 mg once 24 mg/d (419)Losartan 25 to 50 mg once 50 to 150 mg once 129 mg/d (420)Valsartan 20 to 40 mg twice 160 mg twice 254 mg/d (109)Aldosterone AntagonistsSpironolactone 12.5 to 25 mg once 25 mg once or twice 26 mg/d (424)Eplerenone 25 mg once 50 mg once 42.6 mg/d (445)

Drugs Commonly Used for HFrEF (Stage C HF) (cont.)
Drug Initial Daily Dose(s) Maximum Doses(s)Mean Doses Achieved in
Clinical TrialsBeta BlockersBisoprolol 1.25 mg once 10 mg once 8.6 mg/d (118)Carvedilol 3.125 mg twice 50 mg twice 37 mg/d (446)Carvedilol CR 10 mg once 80 mg once ---------Metoprolol succinate extended release (metoprolol CR/XL)
12.5 to 25 mg once 200 mg once 159 mg/d (447)
Hydralazine & Isosorbide Dinitrate
Fixed dose combination (423)
37.5 mg hydralazine/20 mg isosorbide
dinitrate 3 times daily
75 mg hydralazine/40 mg isosorbide
dinitrate 3 times daily
~175 mg hydralazine/90 mg isosorbide dinitrate daily
Hydralazine and isosorbide dinitrate (448)
Hydralazine: 25 to 50 mg, 3 or 4 times daily
and isorsorbide dinitrate:
20 to 30 mg 3 or 4 times daily
Hydralazine: 300 mg daily in divided doses
and isosorbide dinitrate 120 mg daily
in divided doses
---------
Pharmacological Treatment for
Stage C HFrEF (cont.)ARBs are reasonable to reduce morbidity and mortality as alternatives to ACE inhibitors as first-line therapy for patients with HFrEF, especially for patients already taking ARBs for other indications, unless contraindicated.
Addition of an ARB may be considered in persistently symptomatic patients with HFrEF who are already being treated with an ACE inhibitor and a beta blocker in whom an aldosterone antagonist is not indicated or tolerated.
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)Routine combined use of an ACE inhibitor, ARB, and aldosterone antagonist is potentially harmful for patients with HFrEF.
Use of 1 of the 3 beta blockers proven to reduce mortality (i.e., bisoprolol, carvedilol, and sustained-release metoprolol succinate) is recommended for all patients with current or prior symptoms of HFrEF, unless contraindicated, to reduce morbidity and mortality.
I IIa IIb III
I IIa IIb III
Harm

Pharmacological Treatment for
Stage C HFrEF (cont.)Aldosterone receptor antagonists [or mineralocorticoid receptor antagonists (MRA)] are recommended in patients with NYHA class II-IV and who have LVEF of 35% or less, unless contraindicated, to reduce morbidity and mortality. Patients with NYHA class II should have a history of prior cardiovascular hospitalization or elevated plasma natriuretic peptide levels to be considered for aldosterone receptor antagonists.
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)Aldosterone receptor antagonists are recommended to reduce morbidity and mortality following an acute MI in patients who have LVEF of 40% or less who develop symptoms of HF or who have a history of diabetes mellitus, unless contraindicated.
Inappropriate use of aldosterone receptor antagonists is potentially harmful because of life-threatening hyperkalemia or renal insufficiency when serum creatinine greater than 2.5 mg/dL in men or greater than 2.0 mg/dL in women (or estimated glomerular filtration rate <30 mL/min/1.73m2), and/or potassium above 5.0 mEq/L.
I IIa IIb III
I IIa IIb III
Harm

Pharmacological Treatment for
Stage C HFrEF (cont.)The combination of hydralazine and isosorbide dinitrate is recommended to reduce morbidity and mortality for patients self-described as African Americans with NYHA class III–IV HFrEF receiving optimal therapy with ACE inhibitors and beta blockers, unless contraindicated.
A combination of hydralazine and isosorbide dinitrate can be useful to reduce morbidity or mortality in patients with current or prior symptomatic HFrEF who cannot be given an ACE inhibitor or ARB because of drug intolerance, hypotension, or renal insufficiency, unless contraindicated.
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)Digoxin can be beneficial in patients with HFrEF, unless contraindicated, to decrease hospitalizations for HF.
Patients with chronic HF with permanent/persistent/ paroxysmal AF and an additional risk factor for cardioembolic stroke (history of hypertension, diabetes mellitus, previous stroke or transient ischemic attack, or ≥75 years of age) should receive chronic anticoagulant therapy (in the absence of contraindications to anticoagulation).
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFpEF (cont.)Management of AF according to published clinical practice guidelines in patients with HFpEF is reasonable to improve symptomatic HF.
The use of beta-blocking agents, ACE inhibitors, and ARBs in patients with hypertension is reasonable to control blood pressure in patients with HFpEF.
I IIa IIb III
I IIa IIb III

Medical Therapy for Stage C HFrEF: Magnitude of Benefit
Demonstrated in RCTs
GDMTRR Reduction in Mortality
NNT for Mortality Reduction
(Standardized to 36 mo)
RR Reductionin HF
Hospitalizations
ACE inhibitor or ARB
17% 26 31%
Beta blocker 34% 9 41%
Aldosterone antagonist
30% 6 35%
Hydralazine/nitrate 43% 7 33%

Treatment for Stage C HFpEF
Treatment of Stages A to D
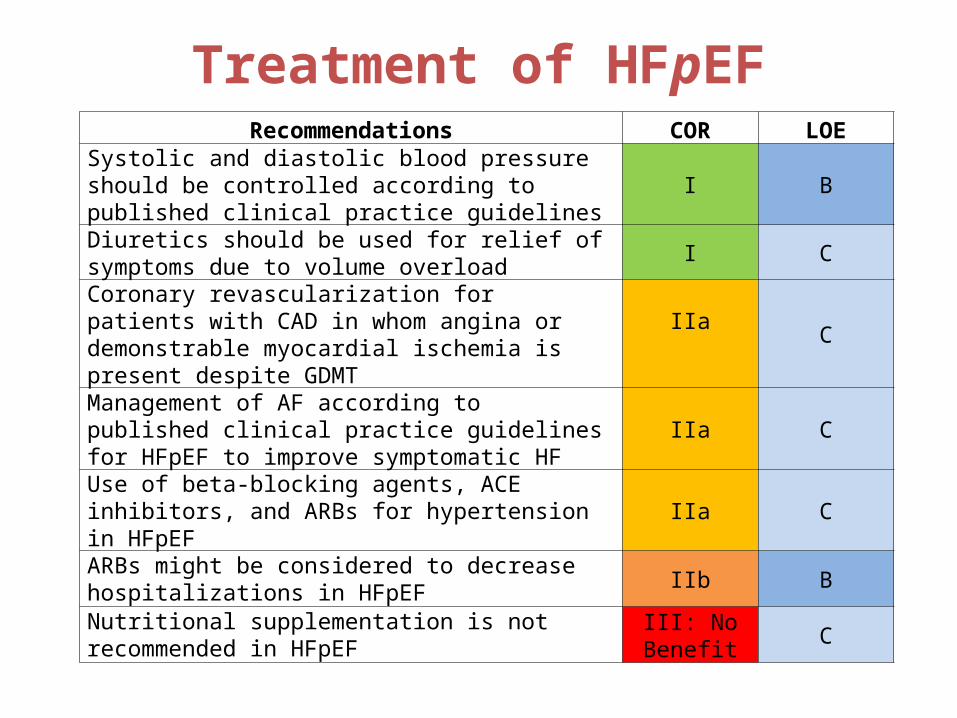
Treatment of HFpEFRecommendations COR LOE
Systolic and diastolic blood pressure should be controlled according to published clinical practice guidelines I B
Diuretics should be used for relief of symptoms due to volume overload
I C
Coronary revascularization for patients with CAD in whom angina or demonstrable myocardial ischemia is present despite GDMT
IIa
C
Management of AF according to published clinical practice guidelines for HFpEF to improve symptomatic HF
IIa C
Use of beta-blocking agents, ACE inhibitors, and ARBs for hypertension in HFpEF IIa C
ARBs might be considered to decrease hospitalizations in HFpEF
IIb B
Nutritional supplementation is not recommended in HFpEF
III: No Benefit
C

Device Treatment for Stage C HFrEF
Treatment of Stages A to D
Device Therapy for Stage C HFrEF
ICD therapy is recommended for primary prevention of SCD to reduce total mortality in selected patients with nonischemic DCM or ischemic heart disease at least 40 days post-MI with LVEF of 35% or less, and NYHA class II or III symptoms on chronic GDMT, who have reasonable expectation of meaningful survival for more than 1 year.
CRT is indicated for patients who have LVEF of 35% or less, sinus rhythm, left bundle-branch block (LBBB) with a QRS duration of 150 ms or greater, and NYHA class II, III, or ambulatory IV symptoms on GDMT.
I IIa IIb III
I IIa IIb III
NYHA Class III/IVI IIa IIb III
NYHA Class II

Stage D
Treatment of Stages A to D

Clinical Events and Findings Useful for Identifying Patients
With Advanced HFRepeated (≥2) hospitalizations or ED visits for HF in the past year
Progressive deterioration in renal function (e.g., rise in BUN and creatinine)
Weight loss without other cause (e.g., cardiac cachexia)
Intolerance to ACE inhibitors due to hypotension and/or worsening renal function
Intolerance to beta blockers due to worsening HF or hypotensionFrequent systolic blood pressure <90 mm Hg
Persistent dyspnea with dressing or bathing requiring rest
Inability to walk 1 block on the level ground due to dyspnea or fatigue
Recent need to escalate diuretics to maintain volume status, often reaching daily furosemide equivalent dose >160 mg/d and/or use of supplemental metolazone therapy
Progressive decline in serum sodium, usually to <133 mEq/L
Frequent ICD shocks
Adapted from Russell et al. Congest Heart Fail. 2008;14:316-21.

Water Restriction
Treatment of Stages A to D
Water Restriction
Fluid restriction (1.5 to 2 L/d) is reasonable in stage D, especially in patients with hyponatremia, to reduce congestive symptoms.
I IIa IIb III

Surgical/Percutaneous/Transcatheter Interventional
Treatment of HFCoronary artery revascularization via CABG or percutaneous intervention is indicated for patients (HFpEF and HFrEF) on GDMT with angina and suitable coronary anatomy, especially for a left main stenosis (>50%) or left main equivalent disease.
CABG to improve survival is reasonable in patients with mild to moderate LV systolic dysfunction (EF 35% to 50%) and significant (≥70% diameter stenosis) multivessel CAD or proximal LAD coronary artery stenosis when viable myocardium is present in the region of intended revascularization.
I IIa IIb III
I IIa IIb III

Heart failure with preserved EF or diastolic heart failure

Heart failure with preserved EF

Case scenario 2• A 55 yo man presents with gradually increasing shortness of breath and
leg swelling that occurred while on a business trip. He has congestive heart failure, which has caused fatigue and shortness of breath if he walks a block or climbs a flight of stairs. BP is 140/ 90; there is no jugular venous distension or gallop, and only minimal pedal edema. AN echo shows left ventricular EF 45 %. Current medication include aspirin and simvastatin. The patient desires to keep medications to a minimum. What additional treatments are indicated at this time?
• A. Spironolactone• B. ACE inhibitor and beta blocker• C. Digoxin• D. Frusemide• E. An implantable defibrillator

Cardiac rehabilitation
• Coordinated interventions designed to optimize a cardiac patient’s physical, psychological, and social functioning, in addition to stabilizing or slowing the progress of underlying atherosclerotic process, thereby reducing morbidity and mortality.
• Answer is B• ACE inhibitor is recommended in both symptomatic n
asymptomatic heart failure• Beta blocker stabilize left ventricular remodeling• Spironolactone recommended for NYHA III-IV with EF <35%
despite on loop diuretic + ACEi + b blocker• Frusemide can improve SSx but patient wants to keep
medication to minimal• Defibrillator not indicated yet

Cardiac rehabilitation
• Include – baseline patient assesssment, – nutritional counselling, – aggressive risk factor management ie
• lipid, hpt, weight, diabetes and smoking, – psychosocial and vocational counseling , and – physical activity counseling and exercise training, in
addition to – appropriate use of cardioprotective drugs that have
evidence-based efficacy for secondary prevention
Who should be included in cardiac rehab ?
• Patient with previous MI• Who had undergone CABG• Those with PCI done• Heart transplant candidate or recipient• Who has stable chronic heart failure,
peripheral arterial disease

Psychosocial intervention (address depression,
anxiety, social isolation. Consider SSRI, cognitive behavioral therapy.
Risk factor modification & interventionAggresive reduction of risk factors via nutritional counselling, weight management, adherence to drug therapy
Exercise training interventionReturn to workCardioprotective mechanism (improve endothelial function)

Thank you for your kind attention