management of mastalgia, hormonal, and benign breast
TRANSCRIPT

ramsayhealth.com
Mr Neil Johns
Consultant Oncoplastic and Reconstructive Breast Surgeon
East and North Hertfordshire NHS Trust
Pinehill Hospital Hitchin
Management of Mastalgia, Hormonal,
and Benign Breast Changes in Primary
Care

Disclaimer
• I run the rapid diagnostic clinic at Pinehill with Miss HarleenDeol
2

Breast Pain
• Approximately 70% of women experience breast pain• Most common breast symptom
• Frequently results in primary care visits
• Breast Pain usually resolves spontaneously without any treatment
• Rarely, some types of breast pain may indicate an underlying problem with the breast
• 11% -21% get severe breast pain
• 36% consult a doctor
• Most common age 30-50
3

Breast pain -2 main types
1. True Mastalgia - Pain that arises in the breast tissue
2. Musculoskeletal chest wall pain - Referred pain felt in the breast
Nerve supply of breast : anterolateral and anteromedial branches of the T3-T5 intercostal nerve. Branch of T4 penetrates the deep surface of the breast and runs up to the nipple.
Referred pain through the intercostal brachial nerve to inner aspect of arm.

Clinical Evaluation of Breast Pain
• Clinical exam should involve palpation of both breasts and axillae, as well as the chest wall
• Important to assess the nature of breast pain:• Unilateral or Bilateral
• Focal or diffuse
• Cyclical or constant
• Superficial or deep?
• Associated with any additional symptoms – palpable lump, skin changes, nipple discharge
5

Breast pain – Chest wall pain
• Primary care studies : most common mastalgia is referred chest wall pain
• Breast clinics: chest wall pain now more common than true breast pain
• Even classic cyclical breast pain often associated with chest wall tenderness as site of origin of the pain

Chest wall pain -history
• Unilateral
• “Burning, shooting, deep, shooting up to the nipple, up to axilla and across to the upper arm, deep itching. Feels like a pulled muscle.”
• Brought on by activity-recent increase in exercise or starting at a gym, gardening, heavy lifting, decorating, strain to the arm , repetitive sustained work at a computer. (RSI of the upper limb)
• Lateral or medial in the breast
• Reproduced by pressure on a specific area of the chest wall.
• factors pointing to musculoskeletal pain rather than breast pain
• Pre-existing spondylosis
• Pre-existing osteoarthritis
• Postmenopausal
• No hormonal medication

True mastalgia - history
• Pain arising in the breast tissue
• Associated with cyclical nodularity often in the UOQ
• Often hormonal-week prior to menstruation, relieved by onset of period
• Associated with exogenous hormones –HRT

Medication that does not cause True Mastalgia
• Combined contraceptive
• No link (placebo = coc) but patches can cause more discomfort. Cochrane review. Bancroft and Rennie 1993
• Progestogen contraception
• No evidence of link but can get breast discomfort following mirena coil insertion in the first 3/12
• Some evidence to suggest benefit from parenteral progestogen (Mirena, implant, depo provera)
• ? Abolition of the menstrual cycle/ low luteal phase progesterone

Medication that may cause True Mastalgia
• HRT
• Antidepressants, antipsychotics, anxiolytic-sertraline, venlafaxine, haloperidol
• Cardiac drugs –spirinolactone, methyldopa, minoxidil
• Antimicrobials-ketoconazole, metronidazole

True Mastalgia-Theories of pathophysiology
• Too much oestrogen
• No evidence this is the case
• Too little progesterone
• Single study has shown a reduced serum progesterone in the luteal phase in women with mastalgia
• Too much prolactin
• Breast biopsy prolactin levels no difference between those with pain and those with out
• Studies have shown women with mastalgia produce more prolactin for longer in response to stimulation suggesting a prolactin pathway problem at the hypothalamus
• Increased receptor sensitivity/abnormal fatty acids
• Increased ratio of saturated fatty acids to essential fatty acids, the cell membrane is more ridged ,easier for ligands to bind ,making the oestrogen receptor more available thus making the breast cells more sensitive to the effects of oestrogen

True Mastalgia-prognosis
• CYCLICAL
• 20-30% resolution in 3/12
• Relapse and remit
• 60% recurrent symptoms within 2 years
• NON-CYCLICAL
• 50% spontaneous resolution

Breast pain –clinical examination
• Clinical examination helps determine the origin of the pain
• Full breast exam
• Palpation of the chest wall, muscles and ribs. –roll patient on side left and right to allow breast to fall away from ribs. Lift breast to examine inferiorly.
• Note any localised tenderness
• Ask is the pain similar to the pain they are experiencing.
• Confirmation by the patient is effective in reassurance

Types of Breast Pain
• Non – clinically significant
• Cyclical breast pain
• Diffuse breast pain
• Pain referred to the breast
• Clinically significant
• Focal pain, especially that which is associated with another symptom, such as a palpable lump or nipple discharge
14
Not known to correlate with the presence of breast cancer
Infrequent, but existent, association with breast cancer

Cyclical Breast Pain
• Most common, accounting for around 2/3 of cases of breast pain
• Typically bilateral and symmetrical• Lateral breast most common location
• May radiate to the axilla
• Can be stabbing, burning or shooting pains
• May be associated with breast heaviness
15

Cyclical breast pain
• Due to hormonal changes during the menstrual cycle
• Most common during periods of hormonal imbalance
• Puberty, peri-menopause, first trimester of pregnancy, following childbirth
• Not related to ‘abnormal’ hormone levels, but rather an increase sensitivity of the breast to hormonal changes
16
Cyclical breast pain
• Treatment involves reassurance
• Encourage use of properly fitting bra
• Encourage physical activity
• Consider reduction in caffeine intake
• Evening Primrose Oil capsules or massages
• If pain is severe and refractory, some endocrine treatments may be considered, but can be associated with side effects, and therefore should only be used in severe cases
17

Non-cyclical breast pain: Without clinical symptoms
• Accounts for around 1/3 of breast pain• More common above 40 years old
• Typically unilateral, can vary in the location
• May relate to trauma to the breast, or can be related to referred pain, such as that from the chest wall
18

Non-Cyclical breast pain: Without clinical symptoms
• Specific causes may include:
• Chest wall shingles
• Costochondritis
• Pain related to breast implants or large, pendulous breasts
• Medication use
• Referred pain: heart conditions, oesphageal spasm, pneumonia or pleural irritation
19

Non-cyclical breast pain: without clinical symptoms
• Incidence of breast cancer in patients with breast pain only is 0 – 3%
• Arslan et al. J Breast Health, 2016
• Barton et al. Ann Intern Med, 1999
• Chetlen et al. Acad radiol, 2017
• Several studies have found no association between cancer and focal breast pain
• Leddy et al. Breast J, 2013.
• Leung et al. J Ultrasound Med, 2002
• In fact, some studies suggest the rate of malignancy is the same among women with a normal physical exam who have no breast pain, and those who have focal breast pain alone
• Duijm et al. BJM, 1998.
20

Clinically significant focal breast pain
• Well localized
• Persistent, not intermittent or cyclical
21

What about imaging
Symptomatic Breast Imaging
Conventional routine techniques for breast imaging are x-ray mammography and ultrasound.
Ultrasound and x-ray guided biopsy procedures and MRI are also employed in the investigation of symptomatic breast disease.
Imaging Over 40 years:
Mammography. Two views, mediolateral oblique and cranial caudal projection.
Ultrasound adds additional information if focal problem.
Imaging not necessary for those with pain unless over 40 when mammograms are recommended if not performed in the last 2 years.
Under 40 years
May not require imaging as part of diagnostic assessment.
Ultrasound is technique of first choice in women with focal breast problem.
Mammography — Where malignancy is suspected. Two views as > 40 years of age breast.
22

Imaging performance in breast pain evaluation
• Mammography and ultrasound are useful in excluding cancer in women with breast pain
• 99.8% Negative Predictive Value (NPV) of mammography, with or without Ultrasound, in women with isolated breast pain
• Noroozian et al. Breast Cancer Res Treat 2015; 149417-424
• 100% NPV of mammography and ultrasound in women with isolated breast pain
• Tumyan et al. Breast J 2005; 11:333-337
• However, often times patients with isolated breast pain who undergo imaging evaluation subsequently undergo biopsy with benign results
23

Breast pain with clinical symptoms
• Common clinical symptoms associated with breast pain may include:
• Palpable lump
• Nipple discharge
• Skin thickening
• Fever
• Breast inflammation
24

Breast Lumps

Age Normal process Aberration
< 25 Breast development
Lobular
Stromal
Fibroadenoma
Juvenile hypertrophy
25-40 Cyclical activity Cyclical mastalgia
Cyclical nodularity
(diffuse/ focal)
35-55 Involution
Lobular
Stromal
Ductal
Cysts
Sclerosing lesions
Duct ectasia
Aberrations of Normal Development
and Involution (ANDI)

Abnormalities of Breast Development:
The Fibroadenoma

Fibroadenoma: Aetiology
• 12 % of all palpable symptomatic lesions
• Commonest breast lump in women 15 -25
• 15% of discrete lesions in women age 30 - 40
• median age of diagnosis 30yrs
• Commoner in left breast

Fibroadenoma: Management
• If assessment is benign discharge with breast awareness advice
• Change in size, atypical clinical / radiological / cytological assessment or > 4cm – Excise
• Most stay the same size, some get smaller and disappear over time
• A small number get bigger

Breast Pain with Palpable lump: Common benign causes
• Fibrocystic changes
• Common 20-40
• Thickening of breast tissue (+/- Fibrosis)
• Development of cysts
• Results in swollen, painful, lumpy breasts
30

Abnormalities of involution: Fibrocystic
change
• Commonest symptomatic presentation to GP/ BU
• 70% of breast lumps in <40
• Histological Basis
• Increased glandular elements
• Multiple small cysts
• Apocrine change

Focal nodularity / Fibrocystic
change: management
• Clinical examination
• Mammography if >35
• USS on occasions; is there a discrete lesion?
• FNAC/ core biopsy if discrete
• Open biopsy if any clinical doubt
• Normally discharged at ‘one-stop facility

Breast Pain with Palpable lump: Common benign causes
Aberrations of involution: Breast cysts
33

Breast cysts: Classification
• Simple
Solitary
Multiple
• Galactocele
• Intracystic carcinoma
• Rarities
7% of all women at some time during their lives

Breast cysts: aetiology and
pathology
• Aberration of normal involution
• Vary in size
• Blue domed appearance
• First presentation age 35-55
• No discernible hormonal abnormality

Breast cysts: Clinical features
• Smooth, discrete fluctuant mobile
• Often painful
• 50% single cyst
• 33% 3-5 cysts
• 17% > 5 cysts
• Recurrence in 40% (interval reduces with age)

Breast cysts: management
• At presentation:
Triple assessment
Aspiration
No residual mass
clear aspirate
Discharge / Review
3 months
Bloody
aspirate
residual mass
Core biopsy
Further
cyst
No further
cyst
Discharge

Breast cysts: Diagnostic pitfalls
Bloody aspirate
Residual mass
Intracystic carcinoma
until proved otherwise

39

Risk Factors for breast cancer
Salzman 202140

Breast pain and breast cancer
• Breast pain is a rare symptom of breast cancer.
• 10 year survey in Edinburgh
• 8504 patients presenting with breast pain as their major symptom 220 (2.7% ) were subsequently diagnosed with breast cancer .
• 4740 patients during this period had breast cancer thus 4.6% of women with breast cancer had pain as an important presenting symptom
• BMJ 2013; 347 doi: http://dx.doi.org/10.1136/bmj.f3288 (Published 13 December 2013) Cite this as: BMJ 2013;347:bmj.f3288
• Undetected cancer found in 2-7% patients with pain as the only complaint (PREECE P et al. BMJ 1982; 284: 1299 -300]

Breast Pain and Lifetime risk of Breast cancer
• Fonseca et al. Breast Cancer Research and treatment, 2019
• 971 exams in 953 patients with breast pain only
• 8 cancers detected in total
• 4/8 cancers corresponded to the area of pain
• 2/8 cancers did not correspond to the area of pain
• 2/8 cancers the correlation with the location of pain was unclear
• Overall cancer detection rate (CDR): 0.8%
• CDR in average risk patients: 0.6%
• CDR in higher than average risk patients: 1.5%
• The authors conclude that diagnostic evaluation of breast pain may lead to unnecessary workup and biopsies, which leads to overutilization of healthcare recourses and can provoke anxiety among patients
• Routine screening mammogram should be encouraged, and patients with higher than average lifetime risk may benefit from additional tests such as annual screening MRI
42





Breast Pain –true mastalgia and chest wall-management-
first line
• Reassurance
• 85% that is all that is required
• Identify and avoid precipitating activity for chest wall pain, gentle exercises, Computer workstation ergonomics.
• Well Fitting Bra
• Complete relief in 25% and partial in 50% Wilson and Sellwood1976
• Topical NSAIs
• 1 RCT more effective than placebo both types of pain
• Colaket al 2003
• Simple oral Analgesia

True Mastalgia-Dietary factors
1. Low Fat High carbohydrate diet
• Little evidence . 1 small RTC showed significantly less tenderness than general diet : 6/9 v 9/9 but hard to maintain such a diet.Boydet al 1988
2. Caffeine
• No evidence restriction is beneficial although some studies did show some benefit others did not.
• Studies with diet or caffeine restrictions showed poor compliance

True Mastalgia-Treatment-second line
• Pain severe enough to effect QOL
• Pain that does not respond to first line treatment
• To keep pain chart for 2 months to evaluate severity and timing of pain and to gauge response to treatment.

True mastalgia-Second line drugs
• Danazol 100mg bd(Antigonadatrophin)
• Weight gain, deepening of voice , menorrhagia, hirsutism, teratogenic .Use in the luteal phase has fewer side effects
• £16 /day
• Tamoxifen 10mg daily (SERM)
• PV bleeding, discharge, DVT, hot flushes, most effective with least side effects of all the drugs . Can use in the leutealphase of cycle only. New in pipeline tamoxifen gel ( fewer systemic s/e)
• £ 1.77/day
• Goserelin 3.6mg monthly +/-HRT( LHRH analogue)
• Vaginal dryness, hot flushes ,acne, depression.

Tamoxifen 10 mg v Danazol 200mg
1. Both Superior to placebo
• Tamoxifen 20mg relief maintained in 72 % at 1 year
• Tamoxifen fewer adverse effects than danazol
• Tamoxifen 53% v danazol37% pain free at 1 year
• 85% cyclical mastalgiapain -free with tamoxifen given in luteal phase of cycle
2. 10mg v 20 mg tamoxifen :
• Pain at 1 year 25% v 30%
• Side effects : 21% v 35%
3. Tamoxifen the most effective of all modalities with least side effects
Breast pain –musculoskeletal management
• NSAIs oral or topical
• Chest wall pain localised to 1 spot, very troublesome, interferes with daily. Rarely required
• Prednisolone 40mg in depot + long acting local anaesthetic can produce long lasting pain relief.
• 50% benefit single injection
• Repeat 4-6 weeks later increases response to 2/3rds.

Breast pain – post surgery
• Pain 1 year post surgery survey 282 women
• Mastectomy + reconstruction-49%
• Mastectomy only –31%
• Breast reduction –22%
• Cosmetic Breast Augmentation –38%
• Pain Vol66.issues 2-3 Aug 1996.195-205 Wallace et al 1996
• No role for primary surgery for any type of breast pain
• Lipofilling? Watch this space
53
Chronic pain post breast surgery
• Similar symptoms to chest wall pain
• Up to 50%
• Exclude local recurrence/bony metastasis
• Pain management treatments
• amitriptyline., gabapentin, pregabalin
• TENs
• Referral to pain clinic
54

Breast Infection / Inflammation
• Lactating vs non lactating
• Different organisms
• Is there an abscess present?
• Ultrasound
• Other causes
• Periareolar infection - Periductal mastitis
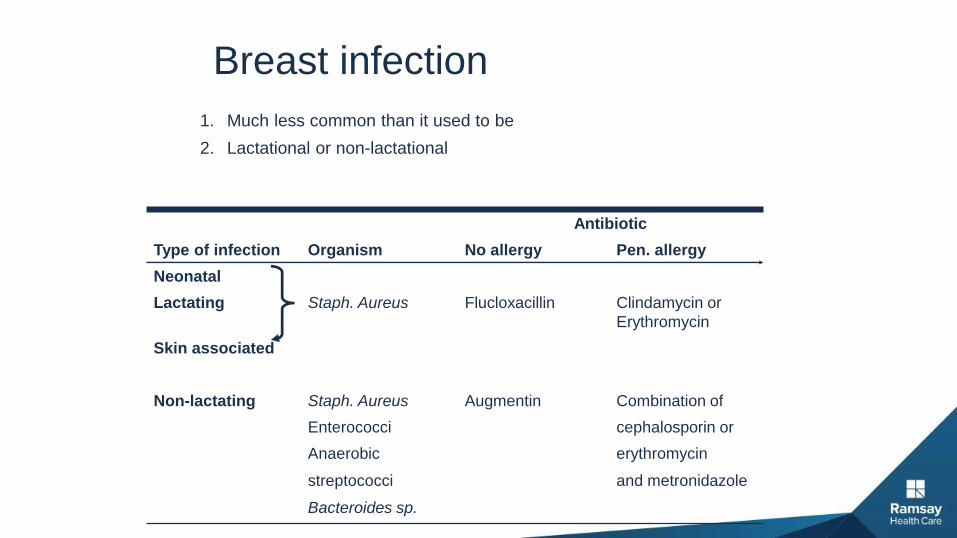
1. Much less common than it used to be
2. Lactational or non-lactational
Breast infection
Antibiotic
Type of infection Organism No allergy Pen. allergy
Neonatal
Lactating Staph. Aureus Flucloxacillin Clindamycin or
Erythromycin
Skin associated
Non-lactating Staph. Aureus Augmentin Combination of
Enterococci cephalosporin or
Anaerobic erythromycin
streptococci and metronidazole
Bacteroides sp.

Lactational Breast Abscess
• Cracks/breaks in nipple
• 0.4-33% breastfeeding women
• Commonly skin flora
• Risk factors -mother >30, over 41 weeks gestation, first month after beginning feeding
• Gradually progressive symptoms
• Assessment –clinical (necrosis, mass, infection)
• ultrasound

Skin
Normal
Aspirate – USS guidedIrrigate with local
anaesthetic - oral antibiotics
Reaspirate every2-3 days tillno more pus
USS shows pus is present
Treatment of Breast Abscesses

USS shows pus is present
Skin
Normal Thinned or necrotic
Aspirate – USS guidedIrrigate with local
anaesthetic - oral Mini I + Dantibiotics
Reaspirate every Irrigate with2-3 days till saline everyno more pus 2-3 days
Treatment of Breast Abscesses

Breast Infection / Inflammation
• Lactating vs non lactating
• Different organisms
• Is there an abscess present?
• Ultrasound
• Other causes
• Periareolar infection - Periductal mastitis

ramsayhealth.com
Periductal Mastitis

Periductal mastitis
• Mean age 32 yrs
• Active inflammation around non-dilated ducts
• Plasma cell rich
• Not duct ectasia
• Smoking virtually ubiquitous
• May present with inflammation or abscess
• Antibiotics +/- standard treatment for abscess
• Often recurrent

Duct ectasia
• Part of ANDI
• Women >50
• Nipple discharge, retraction, doughy palpable mass
• Discharge cheesy/ white
• Slit-like nipple retraction
• Management conservative or surgical
• Surgical = total duct excision

PDM and DE: Key Points
• Separate conditions
• Affect different age groups
• Different aetiologies
DE: ageing - aberration of normal process
PDM: smoking and bacteria - disease
• Management totally different

Mammary duct fistula
• Major complication of periductal mastitis
• Median age 35
• > 90% smokers
• Usually preceding episodes of abscess
• Usually single involved duct
• May have several openings