management of postoperative nausea and vomiting in · pdf filemanagement of postoperative...
TRANSCRIPT

Pediatr Drugs 2007; 9 (1): 47-69REVIEW ARTICLE 1174-5878/07/0001-0047/$44.95/0
2007 Adis Data Information BV. All rights reserved.
Management of Postoperative Nausea andVomiting in ChildrenAnthony L. Kovac
Department of Anesthesiology, University of Kansas Medical Center, Kansas City, Kansas, USA
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 481. Incidence, Pathophysiology, and Etiology of Postoperative Nausea and Vomiting (PONV) and Postoperative Vomiting (POV) 49
1.1 Incidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 491.2 Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 501.3 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
1.3.1 Anxiety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 511.3.2 Inhalation Anesthetic Agents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 511.3.3 Other Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
2. Antiemetics for PONV and POV . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 522.1 Ondansetron . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 522.2 Dolasetron . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 532.3 Granisetron . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 532.4 Dexamethasone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 532.5 Droperidol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
3. Non-Pharmacologic Antiemetic Approaches . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 543.1 Isopropyl Alcohol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 543.2 P6 Acupuncture and Acupressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
4. Postoperative Pain, Antiemetic Use, and Patient-Controlled Analgesia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555. Specific Emetogenic Surgical Procedures in Children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
5.1 Strabismus Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555.1.1 Incidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555.1.2 Muscles Repaired and the Oculocardiac Reflex . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555.1.3 Anesthetic Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555.1.4 Antiemetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
5.2 Tonsillectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 585.2.1 Incidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 585.2.2 Anesthetic Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 585.2.3 Antiemetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
5.3 Additional Pediatric Surgeries and Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625.3.1 Tympanoplasty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625.3.2 Ear Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625.3.3 Radiofrequency Catheter Ablation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625.3.4 Burn Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625.3.5 Craniofacial Operations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625.3.6 Neurosurgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625.3.7 Magnetic Resonance Imaging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
6. Development of PONV and POV Management Guidelines and Algorithms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 627. Guidelines for POV Prophylaxis in Children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 638. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65

48 Kovac
Postoperative nausea and vomiting (PONV) continues to be a frequent and important cause of morbidity inAbstractchildren. Postoperative vomiting (POV) is more commonly studied in children than postoperative nauseabecause of a child’s inability to effectively express distress after experiencing nausea. POV is problematic inchildren and is one of the leading postoperative complaints from parents and the leading cause of readmission tothe hospital. POV occurs twice as frequently in children as in adults, increasing until puberty and then decreasingto adult incidence rates. Gender differences are not seen before puberty.
POV remains a main cause of morbidity in children because severe vomiting can be associated withdehydration, postoperative bleeding, pulmonary aspiration, and wound dehiscence. While children have anincreased potential for dehydration and the resulting physiologic impairments, other associated results such as adelay in hospital discharge or an overnight or longer hospital admission also must be considered.
The two most common emetogenic surgical procedures evaluated in children are strabismus repair andadenotonsillectomy. The approach to the management of PONV and POV in children is similar to that in adults.However, as the rate of POV is more frequent in children than in adults, more children are candidates forantiemetic prophylaxis. The management approach is multifactorial and involves proper preoperative prepara-tion, risk stratification, rational selection of antiemetic prophylaxis, choice of anesthesia technique, and a planfor postoperative antiemetic therapy.
It is important to identify children at moderate-to-high risk for POV as prophylactic antiemetic therapy isuseful in these children. Antiemetics of choice for POV in children include dexamethasone, dimenhydrinate,perphenazine, ondansetron, dolasetron, granisetron, and tropisetron. The serotonin (5-hydroxytryptamine;5-HT3) antagonists are the antiemetic drugs of first choice for POV prophylaxis in children because as a groupthey have greater efficacy for preventing vomiting than nausea. The 5-HT3 antagonists can be effectivelycombined with dexamethasone with an increase in efficacy. If possible, regional anesthesia should be consid-ered. For those undergoing general anesthesia, the baseline POV risk should be reduced.
Children at moderate-to-high PONV risk should receive combination therapy with two or three prophylacticantiemetics from different antiemetic drug classes. Reference to and the use of PONV guidelines and manage-ment algorithms help improve cost-effective postoperative care.
It is estimated that following anesthesia and surgery, children More PONV clinical trials have been conducted in adults thanin children. The limitations involved in analyzing and comparinghave more complications in the postoperative anesthesia care unitolder antiemetic studies has resulted in difficulty in applying the(PACU) recovery area than adults.[1] The majority of these eventsresults of randomized clinical trials to actual clinical situations.are age related, occurring mostly in neonates and infants, and mostThe systematic review is an important method that has been usedinvolve the respiratory rather than the cardiovascular system. Asto understand the efficacy of an intervention in actual clinicalchildren become older, postoperative effects include nausea, retch-situations and the likelihood of harm or adverse events. It ising, and vomiting. Nausea is an unpleasant, subjective sensationespecially useful when there is a large amount of data fromthat may or may not be associated with vomiting. Retching is thenumerous clinical trials but still unresolved questions. Concepts
synchronous, rhythmic contraction of the abdominal, diaphrag-such as the number needed to treat (NNT; the inverse of the
matic, and intercostal muscles that occurs with a closed mouth andabsolute risk reduction) and the number needed to harm (NNH; the
glottis. Vomiting is the forceful expulsion of gastric contents frominverse of the absolute risk increase) have been summarized by
the mouth. Postoperative nausea and vomiting (PONV) and post- Tramer[5-7] for PONV and are useful concepts that can be used tooperative vomiting (POV) continue to be important causes of compare antiemetic drug efficacy and adverse events, respective-morbidity in adults and children, respectively.[2,3] They are among ly.the main postoperative complaints from parents, and a leading The improvement resulting from treatment compared with pla-cause of delayed discharge and/or re-admission to the hospital for cebo has been used as a measurement of antiemetic efficacy.the pediatric patient. A review[4] of 10 772 children undergoing Tramer[5] used the example that a 20% improvement in treatmentday surgery found that PONV was the fourth most common reason efficacy above the placebo response indicated that 20% of patientsfor unplanned hospital admission following pain, surgical compli- who received the antiemetic medication would benefit (absolutecations, and surgery late in the day. risk reduction) from the treatment. If a perfect response is defined
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)
Management of Postoperative Nausea and Vomiting in Children 49
as a 100% improvement, then a 20% response yields an NNT of Various investigators[8-19] have evaluated the reasons for POVfive (100% divided by 20%), i.e. five patients would need to and PONV in the pediatric population. Kotiniemi et al.[8] evaluatedreceive the medication for it to have a positive effect in one PONV symptoms in children occurring at home following day-patient. Specifically, for an antiemetic medication, an NNT of five case surgery. PONV occurred in 13% of all children evaluated,indicates that five patients at risk for PONV would need to receive and emetic symptoms were most common following tonsillecto-the medication in order for one patient not to vomit that would my, occurring in 31% of patients. Specific predictors that PONVhave vomited had he or she not received the medication. From would occur at home were: (i) emetic symptoms in the hospital;Tramer’s[7] evaluation, in children, intravenous droperidol 75 µg/ (ii) age >5 years; (iii) pain at home; and (iv) the use of postopera-kg has an NNT of 5 and 4–5 for early (0–6 hours) and late (0–24 tive opioids. However, these authors noted that the intraoperativehours) vomiting, respectively. Intravenous ondansetron 100 µg/kg use of opioids did not affect the incidence of PONV.has an NNT of 4–5 and 2–3 for early (0–6 hours) and late (0–24 Investigators[8-14,16,17] have reported the overall incidence ofhours) vomiting, respectively. Intravenous ondansetron 150 µg/kg POV in children to be between 8.9% and 42% (table I). Surgery-has an NNT of 2–3 for early (0–6 hours) vomiting. Regarding specific POV in children ranges from 9% to 80%. Interestingly,NNH in children, droperidol has an NNH of 91 for extrapyramidalsymptoms. The oculocardiac reflex in children receiving propofolhas an NNH of 4.
This review summarizes the latest data and information regard-ing the management of PONV in the pediatric patient specificallywith respect to strabismus surgery and adenotonsillectomy. Asummary of anesthetic techniques and application of the recentPONV consensus guidelines for pediatric patients is presented.
Study references cited in this article were obtained by anInternet search of Google, OVID, and Netscape databases usingkeywords such as ‘postoperative nausea and vomiting,’ ‘PONV,’‘postoperative vomiting,’ ‘POV,’ ‘pediatrics,’ ‘antiemetics,’‘5-HT3 antagonists,’ ‘ondansetron,’ ‘granisetron,’ ‘dolasetron,’‘dexamethasone,’ ‘droperidol,’ ‘meta-analysis,’ ‘systematic re-view,’ ‘strabismus repair,’ ‘tonsillectomy,’ and ‘adenotonsillecto-my.’
1. Incidence, Pathophysiology, and Etiology ofPostoperative Nausea and Vomiting (PONV) andPostoperative Vomiting (POV)
1.1 Incidence
Despite the introduction of new antiemetic medications, theincidence of POV in children is estimated to be twice the incidencefor both nausea and vomiting after surgery in adults. It is difficultto estimate the true incidence of nausea in children who may not beable to express their degree of discomfort associated with thissubjective feeling. This is the major reason why antiemetic studiesin children have evaluated POV rather than PONV. However,failure to report nausea in these studies does not mean that nauseais not experienced in children. If the true incidence of nausea couldbe measured accurately, the incidence of PONV (see table I)would be even higher in the pediatric age group.[1,8-10]
Table I. Incidence of postoperative nausea and vomiting (PONV) andpostoperative vomiting (POV) in children
Study Year PONV or Incidence (%)POV
Overall
Rowley and Brown[10] 1982 POV 42
Patel and Hannallah[14] 1988 POV 8.9
D’Errico et al.[9] 1989 PONV 19
Schofield and White[16] 1989 POV 14
Karlsson et al.[17] 1990 POV 25
Byers et al.[12] 1995 PONV 18.1
Kotiniemi et al.[8] 1997 PONV 13
Villeret et al.[13] 2002 PONV 9.4
Khalil et al.[11] 2005 PONV 28
Surgery/procedure specific
Strabismus
Abramowitz et al.[21] 1983 POV 80
Kuhn et al.[22] 1999 PONV 37
Tonsillectomy
Ferrari and Donlon[19] 1992 POV 70
Stewart et al.[20] 2002 POV 15.6
Plastic surgery: ears
Ridings et al.[18] 1994 POV 63
Radiofrequency catheter ablation
Erb et al.[23] 2002 PONV 60
Burn reconstruction surgery
McCall et al.[24] 1999 PONV 69
Stubbs et al.[25] 1999 PONV 45 (non-scalp);100 (scalp)
Craniotomy
Furst et al.[26] 1996 POV 66
Magnetic resonance imaging
Murray et al.[15] 1995 POV 9
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

50 Kovac
the study by Stewart et al.[20] in pediatric patients undergoingtonsillectomy revealed a POV incidence of 15.6% despite the factthat these children received intraoperative antiemetics.
A study by D’Errico et al.[9] evaluating the incidence andreasons for prolonged PACU stay and unplanned hospital admis-sion determined that the most common cause of prolonged lengthof PACU stay was due to PONV (19% of children), followed byrespiratory complications (16%). Unplanned hospital admissionsfollowing outpatient surgery were primarily due to respiratory andsurgical reasons (32% and 30%, respectively), and these outcomeshad a significant impact on hospital staffing, institutional costs,family convenience, and patient satisfaction; PONV accounted for8%.
A lower incidence of POV of 22–40% was observed by Rowleyand Brown[10] in children aged <3 years compared with 42–51% inchildren >3 years. This was supported by Khalil et al.[11] whoreported a POV incidence of 27% and 28% in children aged 1–12
Cerebellum
Area postremaand chemoreceptortrigger zone
Nucleus of thesolitary tract
Vomiting centre
Fourth ventricle
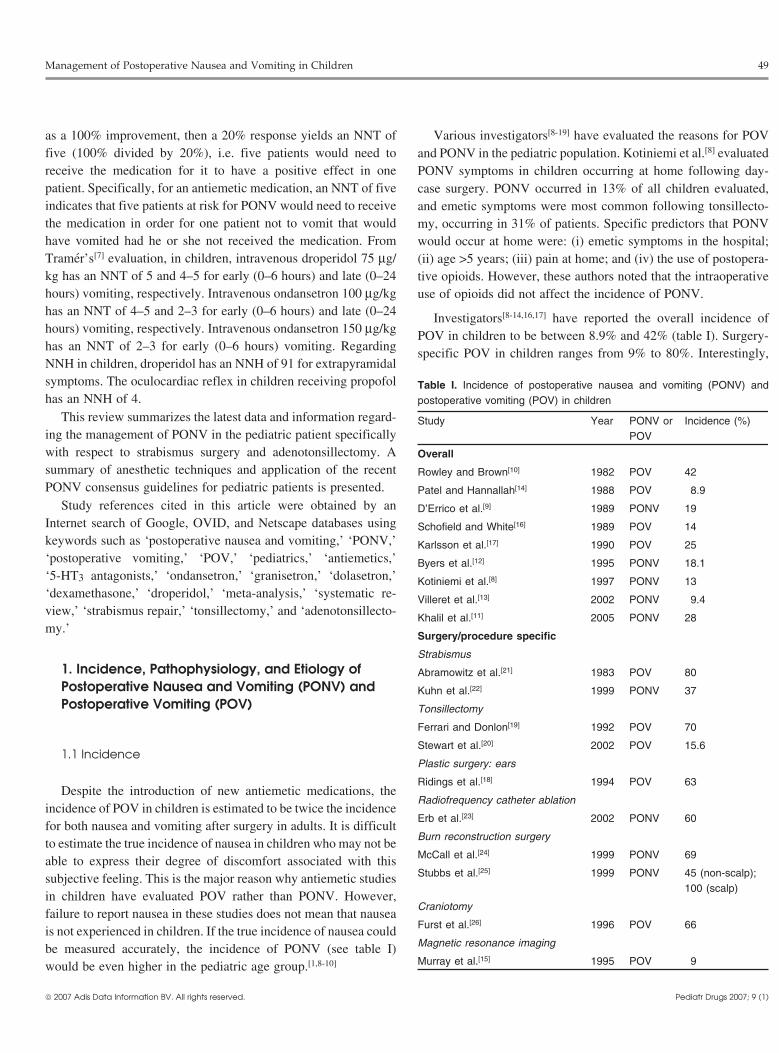
Fig. 1. Anatomic location of the brain postoperative nausea and vomitingreceptor area: vomiting center, nucleus of the solitary tract, area postrema,and chemoreceptor trigger zone (reproduced from Kovac,[29] with permis-sion).months and 13–24 months, respectively. Byers et al.[12] found that
the highest incidence occurred in children undergoing ear, nose,is coordinated by the vomiting center. Stimulation can be initiatedand throat (ENT) procedures and increased with age. Avoidance offrom peripheral areas such as the oropharynx, mediastinum, gas-intraoperative opioids and the use of local anesthesia and/ortrointestinal tract, renal pelvis, peritoneum, or genitalia, and fromNSAIDs for pain control were found to reduce the incidence ofcentral areas such as the cerebral cortex, and labyrinthine, otic, orPONV.vestibular apparatus.[27-29]
Villeret et al.[13] evaluated the incidence of PONV during theIt is hypothesized that PONV after strabismus surgery may befirst 24 hours following elective ambulatory pediatric surgery,
due to an altered visual perception and afferent impulses causingspecifically excluding head and neck procedures. PONV occurredthe oculoemetic reflex, which is analogous to the oculocardiacmost frequently in the hospital during the first 3 hours afterreflex. An increase in the number of ocular muscles that areanesthesia but rarely during the journey home and was associatedrepaired is reported to increase the risk of POV. Afferent stimuliwith: (i) increasing age; (ii) previous history of PONV;are relayed from peripheral to central vomiting centers and the(iii) tracheal intubation; (iv) use of the laryngeal mask airway;area postrema via the glossopharyngeal and vagal nerves, which(v) controlled or manual ventilation; and (vi) opioids. The type ofmay help explain the cause of PONV following adenotonsillecto-surgery, premedication, type of anesthesia induction, regionalmy and hernia repair.[27,28,30-33]anesthesia, use of nitrous oxide, anesthesia duration, length of
PACU stay, and duration of the journey home after discharge were Patients who have a history of motion sickness have a highernot found to be significantly associated with PONV. incidence of PONV, as stimulation of the vestibular apparatus of
the inner ear due to movement of endolymph in the semicircularcanals stimulates otolith cells in the utricle. Transmission of1.2 Pathophysiologyimpulses to the chemoreceptor trigger zone and vomiting centeroccurs, causing the sensation of motion sickness with the occur-Mechanisms of PONV and POV in children are similar to thoserence of nausea and vomiting. Motion sickness or vertigo as ain adults. However, they appear to be more procedure specific inresult of vestibular stimulation also can be a consequence ofchildren as a result of swallowing of blood in adenotonsillectomymiddle ear surgery.[32,33]patients, stimulation of extraocular muscles in strabismus surgery,
and labyrinthine, otic, and vestibular stimulation in ear surgery. Sensory stimuli causing PONV include tactile stimulation ofThe vomiting areas in the CNS include the emetic center, the posterior pharynx (from oral or nasal airway devices, and
nucleus of the solitary tract, area postrema, and chemoreceptor nasogastric or endotracheal tubes), operations on extraocular mus-trigger zone. The chemoreceptor trigger zone is located in the area cles (stimulating the oculocardiac reflex), as well as stretching andpostrema near the emetic center at the bottom of the fourth inflammation or injury to the airway, upper abdomen, gastrointes-ventricle (figure 1). The process of nausea, retching, and vomiting tinal tract, renal pelvis, bladder, or testes.[32-36]
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 51
The close proximity of areas associated with balance, vasomo-tor activity, salivation, respiration, and bulbar control to the vomit-ing center corresponds to the physiologic reactions often seen withPOV and PONV, such as salivation, increased swallowing, sweat-ing, pallor, tachypnea, tachycardia, cardiac dysrhythmias, andmotion sickness.[36,37]
Metabolic, biochemical, and environmental factors that aremediated by the vomiting center and the chemoreceptor triggerzone include uremia, diabetes mellitus (hypo- or hyperglycemia),electrolyte disturbances (sodium, potassium), hormonal imbal-ances (estrogen, progesterone), chemotherapy, and radiation ther-
Table III. Simplified risk score for postoperative vomiting (POV) in chil-dren[44]
No. of risk factorsa POV risk (%)
0 10
1 10
2 30
3 50
4 70
a Risk factors include: strabismus surgery; age ≥3y; surgery >30 min;history of POV or postoperative nausea and vomiting in relatives(mother, father, siblings).
apy.[33,36,37]
These include: (i) strabismus surgery; (ii) duration of anesthesiaThe chemoreceptor trigger zone contains high concentrations>30 minutes; (iii) history of POV or previous history of POV,of enkephalin, opioids, and dopamine (D2) receptors. The areaPONV, or motion sickness in relatives; (iv) age ≥3 years; andpostrema has high concentrations of opioids, D2, serotonin(v) use of postoperative opioids. When 0, 1, 2, 3, or 4 of these risk(5-hydroxytryptamine; 5-HT), and neurokinin-1 (NK-1) receptorsfactors were present, the POV risk was 10%, 10%, 30%, 50%, or(table II). The nucleus of the solitary tract has a predominance of70%, respectively (table III). A variety of authors have alsoenkephalin, histamine, muscarinic, cholinergic, and NK-1 recep-evaluated the effects of other patient- and anesthetic-related fac-tors. These emetic neuroreceptor areas serve as sensors and aretors.[45-59]stimulated by drugs, electrolytes, and metabolic chemicals, caus-
ing impulses to be relayed to the vomiting center, thereby initiat-1.3.1 Anxiety
ing the vomiting reflex. The mechanism of action of the antiemeticThe relationship between anxiety and PONV appears to bemedications commonly used for PONV involves blockade of these
minimal. Wang and Kain[46] determined that preoperatively con-multiple neurochemical receptor sites; this helps explain why atrolling for anxiety had no predictive value for the occurrence ofcombination or multimodal antiemetic approach may be necessaryPONV in children in the PACU or during the first postoperativein some high-risk patients.[20,28,32,37-42]
day.
1.3 Etiology 1.3.2 Inhalation Anesthetic Agents
Numerous studies have evaluated the effect of anesthetic tech-Similar to adults, surgical-, patient-, and anesthesia-relatednique and inhalation agents on PONV.[45-56,59] In an attempt tofactors play an important part in the etiology of PONV and POV inquantify the relative importance of operative anesthetic and pa-children. Lerman[37] noted that while a greater incidence of PONVtient-specific factors for the development of PONV, Apfel et al.[43]
is reported in children compared with adults, this must be inter-conducted a randomized controlled trial of 1180 children and adultpreted with caution; postoperative follow-up data were not collect-patients at high risk for PONV. They concluded that inhalationed prospectively for 24 hours in all patients. However, as previous-anesthetic agents caused early but not delayed PONV, and that thisly determined in adults by Apfel et al.,[43] Eberhart et al.[44]
effect was more significant than the effects of other risk factors.prospectively determined risk factors for POV in pediatric surgery.Their conclusion was that in adult and pediatric patients at highrisk for PONV, it makes better sense to avoid inhalation anesthesiarather than simply adding an antiemetic, which may still be neededto prevent or treat delayed PONV. A similar conclusion wasreached by Elliott et al.[48] who compared inhalation versus intra-venous anesthesia techniques and determined that there was ahigher incidence of pre-discharge PONV and resulting highercosts if sevoflurane was used for anesthesia induction and mainte-nance compared with using propofol.
Goa et al.[49] reviewed the use of sevoflurane in pediatricanesthesia. While sevoflurane provided a more rapid induction andanesthesia emergence than halothane, postoperative pain and
Table II. Mid-brain neurochemical emetogenic receptor locations (repro-duced from Kovac,[29] with permission)
Mid-brain location Receptorsa
Area postrema Opioid, dopamine, serotonin(5-hydroxytryptamine), neurokinin-1
Chemoreceptor trigger Enkephalin, opioid, dopaminezone
Nucleus of solitary tract Enkephalin, histamine, neurokinin-1,muscarinic, cholinergic
a The vomiting center is the coordinator for these receptors to initiatethe vomiting reflex.
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

52 Kovac
PONV were more frequent with sevoflurane. This review brings holding oral fluids was seen in patients who received opioids, inattention to the possible correlation between pain and PONV or the whom POV was reduced from 73% to 36%.[57] Similarly, anothertreatment of pain with opioids and PONV. study[58] determined that not requiring pediatric patients aged 1
month to 18 years to consume clear fluids postoperatively de-Use of regional anesthesia has been suggested to decreasecreased the incidence of POV and time to discharge from thePONV. Oddby et al.[50] evaluated the use of sevoflurane alonePACU.versus spinal anesthesia combined with propofol for sedation in
Murat et al.[61] determined an increased correlation with POV inpediatric ambulatory surgery. While a reduced number of POVthe PACU in children aged ≥8 years who were intubated for ENTepisodes and better immediate postoperative analgesia were foundsurgery.with spinal anesthesia than with propofol sedation, there was no
difference between the two regimens regarding time to discharge2. Antiemetics for PONV and POVor overall patient satisfaction.
Two studies[10,44] determined that length of surgery >30 minuteshas a positive increased correlation with POV in children. 2.1 Ondansetron
The effect of nitrous oxide on PONV in adults and children hasbeen controversial, and most clinical data have come from adult As ondansetron is relatively free of adverse events, numerousstudies. The results of three systematic reviews[51-53] concluded researchers[62-65] have concluded that ondansetron is a safe first-that omitting nitrous oxide from general anesthesia decreases line antiemetic for children. Ondansetron is the only 5-HT3 antag-PONV (NNT = 5). In other words, five high-risk patients would onist with US FDA approval for use in children as young as 1need to undergo a nitrous oxide-free anesthetic for one to not month.[11]
vomit who would have done so if they had received nitrous oxide. Ondansetron has been determined to have good antiemeticNevertheless, the results in children are controversial as two other efficacy for the prevention of POV in children, particularly whenstudies reached different conclusions. Splinter and Komocar[54] combined with dexamethasone. In several large, dose-ranging, andstudied the effects of nitrous oxide on POV in children who placebo-controlled trials,[63-67] intravenous ondansetron 0.05–0.15underwent outpatient dental restorations under halothane anesthe- mg/kg or oral ondansetron 0.1 mg/kg was significantly moresia. Even though the POV rate in the PACU was slightly less for effective than placebo for the prevention of emesis in childrenthe no nitrous oxide versus the nitrous oxide group (15% vs 24%), undergoing highly emetogenic surgery, which included tonsillec-they concluded that nitrous oxide did not significantly affect POV. tomy or strabismus repair. Intravenous ondansetron 0.05 mg/kgSimilarly, another study[55] concluded that nitrous oxide in combi- was determined to be the lowest effective dose.[66] Prophylacticnation with sevoflurane was not associated with an increase in ondansetron 0.1 mg/kg (up to a total dose of 4mg) reduced POV inPOV; the incidence of POV for the nitrous oxide and no nitrous pediatric patients regardless of surgical or anesthesia factors.[67]
oxide groups was similar (14.3% and 15.5%, respectively). The ondansetron-treated children reached the criteria for homeHannallah et al.[56] evaluated speed and quality of recovery, readiness 30 minutes earlier than the placebo-treated patients.
comparing propofol with thiopentone or halothane for induction Rapid intravenous administration of ondansetron 0.15 mg/kg orand maintenance of anesthesia. Children who received propofol metoclopramide 0.25 mg/kg was not associated with changes inhad a faster recovery, were discharged home earlier, and had a vital signs or oxygen saturation.[68]
lower POV incidence. However, it should be stressed that the risk In children undergoing strabismus surgery, a POV prophylacticof propofol-related bradycardia is particularly high in children intravenous study[69] concluded that ondansetron 0.1 mg/kg andundergoing strabismus surgery, due to stimulation of the oculo- droperidol 0.075 mg/kg had similar antiemetic efficacy and werecardiac reflex. The NNH of propofol causing the oculocardic significantly more effective compared with placebo orreflex in children has been estimated to be four despite the prophy- metoclopramide 0.25 mg/kg. A meta-analysis[70] of 54 studieslactic use of anticholinergics.[60] compared the efficacy and safety of ondansetron, droperidol, or
metoclopramide for preventing PONV in adults and POV in1.3.3 Other Factors children. While ondansetron was determined to be more effective
than droperidol, both antiemetics alone were found to be moreWithholding oral fluids postoperatively from children undergo-effective than metoclopramide in preventing POV in children.ing day surgery has significantly reduced the incidence of POV.
This difference was seen whether or not a patient was at high risk Antiemetic studies in children have been limited in studyfor POV (including operations for strabismus, adenoidectomy, design and have had low power, as these studies have beenand/or tonsillectomy). Interestingly, the greatest effect of with- powered to detect differences between an antiemetic drug and
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 53
placebo and not between anesthetic regimens. Prophylactic PONV evaluated the effectiveness of granisetron for the prevention ofantiemetic studies are easier to conduct than treatment studies. POV following pediatric surgery with most clinical studies con-Consequently, as in adults, there have been fewer POV treatment ducted in Japan by Fujii et al.[76-79]
studies in children. A large treatment study[71] evaluated the use of An oral dose of granisetron 40 µg/kg was determined to be theintravenous ondansetron in established POV in 2720 pediatric lowest effective dose for the prevention of POV following ingui-outpatients undergoing general anesthesia with nitrous oxide. A nal hernia and phimosis-circumcision surgery.[76] A dose-rangingsingle intravenous dose of ondansetron 0.1 mg/kg (up to a maxi- study[77] determined that intravenous granisetron 40 µg/kg was themum dose of 4mg) was concluded to be effective and well tolerat- minimally effective dose for POV prevention. After inhalationed (as rescue medication) for prevention of further episodes of anesthesia induction, intravenous granisetron 40 µg/kg was foundPOV and resulted in a shorter time to PACU discharge. to be effective for preventing POV in children with a history of
Ummenhofer et al.[72] conducted a double-blind, prospective motion sickness.[78] Intravenous granisetron 40 µg/kg was also theprophylactic study on the effect of intravenous ondansetron lowest effective dose for preventing POV and retching following0.1 mg/kg or placebo administered before surgical incision, and strabismus repair and tonsillectomy surgery.[79] This conclusionthe effect of rescue antiemetics in patients in whom prophylaxis was also reached by Cieslak et al.[80] who studied pediatric outpa-failed. For rescue medication, patients received either intravenous tients and determined that intravenous granisetron 40 µg/kg wasondansetron 0.1 mg/kg or droperidol 0.02 mg/kg. As ondansetron more effective than intravenous granisetron 10 µg/kg or placebo,was found to be effective for the prevention of PONV for the first but that this dose had a higher acquisition cost.4 hours after general anesthesia with lower sedation scores com- Kranke et al.[81] evaluated the influence of a dominating centerpared with droperidol, this was judged to be advantageous, espe- in a quantitative systematic review of granisetron for preventingcially in ambulatory surgery. Interestingly, the incidence of late- PONV. A total of 27 randomized clinical trials were assessed;onset PONV occurring >4 hours postoperatively was not found to 2938 patients including children and adolescents were included inbe influenced by the preoperative prophylactic administration of a the analysis. In the dominating center, low-dose granisetron wasone-time dose of ondansetron. determined to be ineffective, while high-dose granisetron was
found to be effective. In contrast, the other centers showed both2.2 Dolasetron low- and high-dose granisetron to be effective. These research-
ers[81] concluded that the overall results and dose-response charac-Dolasetron has been recommended for POV prophylaxis in teristics of meta-analyses may be significantly altered by one
children aged 2 years and older. An intravenous equivalence dose- dominating center. A cautious statistical analysis was previouslyranging study[73] determined the lowest effective dose of dolase- conducted by Kranke et al.[82] on the distribution of side effects oftron (45, 75, 350, or 700 µg/kg) that was equivalent to the US comparative groups reported by the dominating center and sug-FDA-approved ondansetron intravenous dose of 100 µg/kg. Intra- gested that the reported data are idealized.venous dolasetron 350 µg/kg was determined to be the lowest
With these data in mind, the safety and efficacy of granisetroneffective dose providing acceptable equivalent efficacy and patient
has not been established in children for the prevention and treat-satisfaction scores to those with the intravenous ondansetron
ment of PONV and does not have US FDA approval for PONV in100 µg/kg dose.
children. The 2003 Consensus Guidelines[83] contained no granise-In a strabismus study, Wagner et al.[74] determined that the tron dosing recommendations for PONV in children.
efficacy of intravenous dolasetron 350 µg/kg in preventing PONVin children was equivalent to that of an intravenous dolasetron
2.4 Dexamethasone12.5mg fixed dose. In a prophylactic intravenous study[75] ofpediatric patients undergoing tonsillectomy who also received
A quantitative, systematic review[84] on the use of dexametha-intravenous dexamethasone 1 mg/kg (up to 25mg), dolasetron 500sone for the prevention of PONV evaluated data from 1946 adultµg/kg (up to 25mg) plus intravenous dexamethasone 1 mg/kg (upand pediatric patients studied in 17 randomized controlled trials into 25mg) was found to be equivalent to a prophylactic ondansetronwhich 16 different dexamethasone dose regimens were used. An 8dose of 150 µg/kg (up to 4mg).or 10mg intravenous dose in adults and a 1 or 1.5 mg/kg intrave-nous dose in children were the most frequently used dex-2.3 Granisetronamethasone doses. Using these doses, the NNT to prevent early
Granisetron has also been recommended for POV prophylaxis (0–6 hours) and late (0–24 hours) POV was seven and four,in children aged 2 years and older. Numerous studies[76-80] have respectively. Late efficacy with dexamethasone was a more pro-
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

54 Kovac
nounced effect in children than in adults. A single prophylactic within 30 minutes of the bolus dose. No associated arrhythmiasdose of dexamethasone was a more effective antiemetic compared were observed. These researchers followed the ECG for a mini-with placebo without any clinically relevant evidence of toxicity mum of 1 hour and were able to evaluate the length of time (15–30or adverse effects in otherwise healthy patients. While the best minutes) in which there was a dose-dependent prolongation of thePONV prophylaxis was achieved with the combination of dex- QT interval. The authors noted that a large prospective study isamethasone and a 5-HT3 receptor antagonist, the authors noted needed to identify the true risk of arrhythmias in the pediatricthat optimal doses of this combination requires further investiga- population.tion. However, other studies[63,64] determined that intravenous The US FDA ‘black box’ recommendation indicated that allondansetron 50 µg/kg when combined with intravenous dex- surgical patients should undergo 12-lead ECG monitoring prior toamethasone 150 µg/kg was significantly more effective at reduc- the administration of droperidol to determine if a prolonged QTcing POV than either medication used alone. interval was present and to continue ECG monitoring for 3 hours
after droperidol administration.[87] Because of these recommenda-tions, this situation places the practising anesthesiologist in a2.5 Droperidoldilemma, as there can be a significant difference between standardclinical practice and the package insert recommendation forHenzi et al.[85] systematically reviewed the efficacy, dose-droperidol.response, and adverse effects of droperidol for the prevention of
An editorial by Berry[89] noted that the Stuth et al.[88] study castPONV in 76 randomized controlled trials involving 5351 patientsdoubt about the recommendations in the ‘black box’ warning forreceiving 24 different antiemetic regimens. The average incidenceECG monitoring. Reasonable practice suggests that proper evalua-of early and late PONV in the control groups was 34% and 51%,tion of patients for potential problems should allow the use of arespectively. Droperidol was determined to be more efficaciousdrug such as droperidol in an appropriate manner while monitor-than placebo in preventing PONV in children with an NNT of fouring for expected potential complications.and five to prevent early and late vomiting, respectively. Two
Further research must be completed to resolve the role of low-children were noted to have had extrapyramidal symptoms, anddose droperidol as an antiemetic. The US FDA is exploringthe NNH in children was determined to be 91. The effect ofoptions to obtain data that satisfy regulatory standards for thedroperidol on nausea was short-lived but was more pronounceddemonstration of safety and efficacy at doses lower than 2mg.than its effect on vomiting, with sedation and drowsiness beingChang and Rappaport[90] urged practitioners to participate in thedose dependent, and a small risk for extrapyramidal symptomspostmarketing safety assessment process by reporting all potentialbeing present.drug-related adverse events. The website www.fda.gov/In 1994 it was reported that droperidol caused a dose-dependentmedwatch[91] contains information on ‘reporting adverse events’.prolongation of the QT interval.[86] While previously there was
warning of potential sudden cardiac death regarding the use of3. Non-Pharmacologic Antiemetic Approachesdroperidol when administered at high doses (>25mg) to psychiat-
ric patients, in December 2001 a ‘black box’ warning[87] of cardiaceffects regarding the use of droperidol for PONV, issued by the US 3.1 Isopropyl AlcoholFDA, was included in the package insert. The revised warning
Isopropyl alcohol is a novel alternative method to alleviatecautioned that even low droperidol doses such as 0.625mg forPONV in children who are scheduled to undergo elective outpa-PONV should be used only when other first-line antiemetic medi-tient surgery under general anesthesia. One study[92] randomizedcations are not effective. Data regarding the NNH of cardiacchildren to inhale an isopropyl alcohol wipe versus saline, repeat-effects with droperidol were not available because of the lowing this for up to three times. After three sequences, 65% in thenumber of adverse events previously reported. The majority of theisopropyl group versus 26% in the saline group had a significantreports of cardiovascular events with droperidol were in adults;reduction of either nausea or vomiting. However, this reductionhowever, cardiovascular effects have also been observed in chil-was transient in children with established PONV; recurrent nauseadren.or vomiting occurred within 20–60 minutes.
Stuth et al.[88] conducted a retrospective analysis of 20 childrenof whom 18 had undergone cardiopulmonary bypass. An intrave-
3.2 P6 Acupuncture and Acupressurenous droperidol 100 µg/kg bolus was given for perioperativesedation. Droperidol caused a significant but transient increase in A meta-analysis[93] was conducted of 19 randomized trials onthe QTc interval; it was still present at 15 minutes but had resolved the efficacy of preventing PONV with acupuncture, acupressure,
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 55
acupoint stimulation, electro-acupuncture, and transcutaneous 5. Specific Emetogenic Surgical Proceduresin Childrenelectrical nerve stimulation in children and adults. The primary
outcomes for the incidence of nausea, vomiting, or both were
evaluated at 0–6 hours (early efficacy) or 0–48 hours (late effica- 5.1 Strabismus Surgerycy) after surgery. While the results of these techniques in adults
5.1.1 Incidencewere found to be statistically significant, no benefit was found inOver the last 20 years the incidence of POV in children havingchildren.
strabismus surgery has ranged from 37% to 80%.[21,22] The effectsIn contrast, Wang and Kain[94] evaluated P6 acupoint injectionsof various anesthetic techniques and antiemetics (see also section
versus droperidol for control of early PONV in children and5.1.3) on POV in children undergoing strabismus surgery are
concluded that the P6 acupoint injections were as effective assummarized in tables IV and V, respectively.[69,100-119]
droperidol in controlling early PONV. Similarly, another study[95]
5.1.2 Muscles Repaired and the Oculocardiac Reflexconcluded that laser P6 stimulation, when administered 15 min-In an evaluation of children who received no prophylacticutes before anesthesia induction for strabismus surgery and 15
antiemetic medication for strabismus surgery, the overall inci-minutes after arriving in the PACU, resulted in a significantlydence of nausea and vomiting was determined as 37% and 32%,
lower incidence of POV. In addition, another study[96] evaluatedrespectively.[115] Splinter et al.[115] determined that while the inci-
the effect of P6 electroacupuncture prophylaxis following pedi-dence of POV was not affected by the use of intravenous midazo-
atric tonsillectomy with or without adenoidectomy and concluded lam, droperidol 50 µg/kg, or duration of anesthesia, the number ofthat perioperative P6 stimulation in awake children significantly repaired eye muscles was a significant predictor of POV, with anreduced nausea, but there was no reduction in emetic episodes or incidence of POV 2.5-fold higher with surgery performed on boththe need for rescue antiemetics. eyes compared with one eye.
The relationship between the oculocardiac reflex and PONVWhile the efficacy of P6 acupuncture for PONV prevention iswas studied in children receiving a prophylactic dose of intrave-believed to be similar to that of commonly used pharmacothera-nous atropine 0.02 mg/kg, alfentanil, and no nitrous oxide. Thepies, its appropriate role in the prevention and treatment of PONVinvestigators concluded that while a thiopental-isoflurane tech-in children requires further study.nique with alfentanil resulted in a moderate risk for POV, addingintravenous ondansetron 4mg significantly decreased this risk.
4. Postoperative Pain, Antiemetic Use, and The NNT in the early postoperative period was six (six childrenPatient-Controlled Analgesia needed to be treated for one to benefit). Propofol and the combina-
tion of intravenous propofol and lidocaine (lignocaine) 2 mg/kgdemonstrated no benefit in decreasing POV but increased the riskSimilar to adults, nausea and vomiting in children related toof the oculocardiac reflex despite a high dose of prophylacticopioids is difficult to treat, and the effectiveness of antiemetics forintravenous atropine 0.02 mg/kg.[117]
opioid-induced nausea and vomiting is controversial.
Children who received intravenous tropisetron 0.1 mg/kg (up to 5.1.3 Anesthetic Techniques
a maximum of 5mg) had a lower incidence and severity of vomit-Diazepam
ing during patient-controlled opioid analgesia, with only one child The combination of diazepam and atropine 0.015 mg/kg hasvomiting more than twice, compared with nine children in the been shown to decrease POV following strabismus surgery.[101]
control group.[97] Prophylactic intravenous dixyrazine was found The overall incidence of POV and the need for rescue antiemeticsto significantly reduce the incidence and severity of PONV in was significantly higher for the first 24 hours after using achildren who used patient-controlled analgesia with morphine sevoflurane-nitrous oxide technique compared with a propofol-
nitrous oxide technique. However, there was a significantly higherafter major surgery.[98] In contrast, another study[99] evaluated theincidence of bradycardia from the oculocardiac reflex, using aeffectiveness of adding antiemetics to the morphine solution inpropofol-nitrous oxide technique.[102]
patient-controlled analgesia syringes used by children after appen-
dectomy, and determined that addition of prophylactic antiemetics Opioids
such as ondansetron or droperidol did not reduce the incidence of Several studies[100,103,104] have evaluated anesthetic techniquesPONV. Thus, this continues to be a controversial topic. combined with opioids for strabismus surgery. Rectal diclofenac
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

56 Kovac
Table IV. Effects of anesthetic techniques on postoperative vomiting (POV) in children
Study Surgery No. of Age Anesthetic technique Conclusions (effect of technique on POV)type pts (y)
Wennstrom and S 50 4–16 Rectal diclofenac vs morphine Diclofenac < morphineReinsfelt[100]
Ozcan et al.[101] S 50 4–15 Diazepam + atropine premedication vs Diazepam + atropine ↓ POV vs placeboplacebo
Gurkan et al.[102] S 40 3–15 Propofol-nitrous oxide vs sevoflurane- Propofol-nitrous oxide < sevoflurane-nitrous oxidenitrous oxide
Standl et al.[103] S 90 3–10 Propofol-sufentanil vs propofol-isoflurane Propofol-sufentanil < propofol-isoflurane
Eltzschig et al.[104] S 81 2–12 Fentanyl vs remifentanil Fentanyl = remifentanil (no change in POV)
Pandit et al.[105] T 60 4–12 Nitrous oxide vs no nitrous oxide Nitrous oxide = no nitrous oxide
Ved et al.[106] T 80 3–10 Halothane + nitrous oxide vs propofol Halothane + nitrous oxide = 3-fold ↑ POV vs propofol
Zestos et al.[107] T 252 2–12 Subhypnotic propofol 0.2 mg/kg dose No effect on POV (subhypnotic dose)
Chhibber et al.[108] T 93 3–16 Atropine-neostigmine vs glycopyrrolate- Atropine-neostigmine < glycopyrrolate-neostigmineneostigmine for muscle relaxant reversal
pts = patients; S = strabismus repair; T = tonsillectomy; < indicates significantly less effect; > indicates significantly greater effect; = indicates similar effect;↑ indicates increase; ↓ indicates decrease.
1 mg/kg was associated with less POV than intravenous morphine ly reduced the incidence of POV following strabismus surgery0.05 mg/kg in children aged 4–16 years.[100] A propofol-sufentanil compared with opioid use.anesthetic technique compared with propofol-isoflurane resulted
Dimenhydrinatein less POV requiring fewer antiemetic rescues during the earlyNumerous studies have evaluated the effectiveness ofpostoperative phase in the PACU, irrespective of the use of nitrous
dimenhydrinate in the management of POV.[109-111,121] Two stud-oxide.[103] One study[104] determined that the number of childrenies[109,110] comparing the efficacy of rectal dimenhydrinate 50mgwho experienced POV did not differ significantly between groupsadministered 30 minutes before the start of strabismus surgery andirrespective of whether or not they received fentanyl. The effectsplacebo reported the incidence of POV to be significantly lowerof ketorolac and fentanyl on POV and analgesic requirementswith dimenhydrinate than placebo (15–30% vs 60–75%). Howev-were evaluated in children who received no antiemetic prophylax-er, the dimenhydrinate-treated patients tended to be more sedatedis.[120] It was concluded by the study investigators that opioids suchand required observation in the PACU for a longer period than theas fentanyl should be avoided as intravenous fentanyl 1 µg/kg hadplacebo group.[109] Another study[111] determined that even thougha greater incidence of POV compared with intravenous ketorolacchildren who received intravenous dimenhydrinate 0.5 mg/kg had0.9 mg/kg.less POV compared with those who received placebo, the time toThis gives further proof of the emetogenic effects of opioidsarousal and hospital discharge did not differ between groups.and how the use of NSAIDs such as ketorolac help decrease
Kranke et al.[121] conducted a meta-analysis of dimenhydrinatePONV.and determined that it was an inexpensive, older antiemetic thatwas effective clinically. However, these researchers also conclud-Clonidine
ed that the dose-response curve, estimation of adverse effects,The effect of oral clonidine on POV following strabismusoptimal time of administration, and benefit of repetitive dosessurgery is controversial. While Handa and Fujii[112] concluded thatremains unclear.oral clonidine 4 mg/kg enhanced the antiemetic effect of propofol,
a study by Gulhas et al.[113] reported that premedication with oralOndansetronclonidine 4 mg/kg 1 hour prior to surgery did not reduce POV.Intravenous ondansetron 75 µg/kg has been determined to be
the optimum, lowest effective dose and to be as effective as5.1.4 Antiemetics150 µg/kg in preventing PONV and improving outcomes for
Dixyrazine strabismus surgery.[119] Antiemetic efficacy was similar with ad-Karlsson et al.[114] concluded that avoidance of opioids and the ministration of intravenous ondansetron 100 µg/kg either before
use of intravenous prophylactic dixyrazine 0.25 mg/kg significant- (at induction) or after surgical manipulation of extraocular mus-
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 57
cles (at the end of surgery).[122] Children given ondansetron had to be more effective than placebo in decreasing the incidence ofless than half the risk of POV compared with those given placebo, post-discharge vomiting.[69] The efficacy and safety of intraopera-with no difference between groups in the incidence of side effects. tive intravenous droperidol followed by an oral dose ofThere was a significant decrease in POV with a corresponding dimenhydrinate at home did not differ from the use of intravenousincrease in dose (0.04, 0.1, or 0.2 mg/kg) of ondansetron.[117] ondansetron administered in the operating room followed by oral
ondansetron at home.[123]While intravenous ondansetron 100 µg/kg and droperidol
75 µg/kg have been determined to be more effective than intrave- Splinter et al.[124] evaluated the effect of intravenous ondanse-nous metoclopramide 250 µg/kg, as compared with placebo, in tron 0.15 mg/kg (up to a maximum of 8mg) versus intravenousdecreasing the incidence of pre-hospital discharge vomiting in propofol 2.5–3.5 mg/kg on POV after strabismus surgery in chil-children undergoing strabismus surgery, no antiemetic was found dren. Inhalation halothane, nitrous oxide, oxygen, or propofol was
Table V. Effects of antiemetics on postoperative vomiting (POV) in children undergoing strabismus surgery
Study No. of Age (y) Antiemetic Conclusionspts
Wennstrom and 50 4–16 Diclofenac 1 mg/kg Diclofenac < morphine sulfateReinsfelt[100] Morphine sulfate 0.05 mg/kg
Welters et al.[109] 30 4–10 Rectal dimenhydrinate 0.50mg Dimenhydrinate > placebo. ↑ sedation with dimenhydrinatePlacebo
Schlager et al.[110] 40 3–12 Dimenhydrinate 50mg Dimenhydrinate < placeboPlacebo
Vener et al.[111] 80 1–12 Dimenhydrinate 0.5 µg/kg Dimenhydrinate > placeboPlacebo
Handa and Fujii[112] 60 2–12 Diazepam 0.45 mg/kg Clonidine > placeboClonidine 4 µg/kg
Gulhas et al.[113] 80 3–12 Clonidine 4 µg/kg Clonidine = placeboPlacebo
Karlsson et al.[114] 58 2–16 Dixyrazine Dixyrazine > placeboPlacebo
Splinter et al.[115] 393 1.5–14 Midazolam 50 µg/kg Midazolam = droperidolDroperidol 50 µg/kg ↑ in the number of eye muscles → ↑ POV
Bowhay et al.[117] 131 2.5–12.5 Ondansetron 0.4 mg/kg Ondansetron 0.4 > ondansetron 0.2 > ondansetron 0.1 >Ondansetron 0.1 mg/kg placeboOndansetron 0.2 mg/kgPlacebo
Scuderi et al.[69] 160 1–12 Predischarge vs postdischarge Predischarge: droperidol = ondansetron > metoclopramide =Placebo placeboMetoclopramide 250 µg/kg Postdischarge: droperidol = ondansetron = metoclopramideOndansetron 100 µg/kg = placeboDroperidol 75 µg/kg
Sadhasivam et al.[118] 180 2–12 Ondansetron 25 µg/kg Ondansetron 75 = ondansetron 100 = ondansetron 150 >Ondansetron 50 µg/kg ondansetron 25 = ondansetron = placeboOndansetron 75 µg/kgOndansetron 100 µg/kgOndansetron 150 µg/kgPlacebo
Shende et al.[119] 240 1–15 Droperidol 15 µg/kg Droperidol + ondansetron > droperidol = ondansetronOndansetron 0.1 mg/kgDroperidol + ondansetron
pts = patients; < indicates significantly less efficacy; > indicates significantly greater efficacy; = indicates similar efficacy; ↑ indicates increase; → indicatesresults in.
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

58 Kovac
Multimodal Antiemetic Anesthetic Techniqueused for anesthesia induction. The incidence of POV in bothSmith and Walton[135] reported the use of a multimodal anesthe-groups was similar pre- and post-hospital discharge. Each episode
sia technique for the prevention of POV following general anes-of in-hospital vomiting prolonged hospital discharge by approxi-thesia in children aged 2 weeks to 18 years undergoing ophthalmo-mately 17 minutes. Prophylactic ondansetron shortened fast-track-logic surgery. General anesthesia was induced with nitrous oxideing time and duration of PACU stay, improving parental satisfac-and halothane in 83% of study patients and intravenous propofol intion and therapeutic outcomes at a lower direct overall treatment17%. Gastric aspiration was performed after endotracheal intuba-cost. Sennaraj et al.[125] noted that the propofol-based techniquetion. Anesthesia was maintained either with halothane or isoflu-had a higher acquisition cost.rane, oxygen, and air. Intravenous morphine, up to a dose of 0.1
Granisetron mg/kg, was administered for pain relief. Combination antiemeticOral granisetron 20 and 40 µg/kg administered prior to anesthe- therapy (intravenous metoclopramide 0.15 mg/kg and intravenous
sia induction was found to be more effective than placebo in ondansetron 0.1 mg/kg) was administered before the end of thereducing the incidence of POV for the first 24 hours after strabis- operation. These researchers concluded that the incidence of POVmus surgery; patients were discharged home earlier, with no was 7.3% with the use of their multimodal protocol. Limited use ofdifference between the granisetron groups.[126] nitrous oxide (for mask induction only), gastric emptying, and
administration of combination antiemetics were believed to beRamosetron
effective methods to reduce POV in a variety of pediatricAntiemetic therapy with intravenous ramosetron 6 µg/kg was ophthalmic procedures.
determined to be comparable to granisetron 40 µg/kg at the end ofstrabismus surgery for the prevention of POV during the early 0-
5.2 Tonsillectomyto 24-hour period, but significantly more effective than granisetronduring the later 24- to 48-hour postoperative period.[127]
5.2.1 IncidenceCombination AntiemeticsAs recently as 2002, Roberts and Jones[136] noted that PONVNumerous combination therapies[63,119,123,128-134] have been
following tonsillectomy continues to be a “big little problem”. Incompared with monotherapy for POV prophylaxis in strabismusan audit of a pediatric day-stay tonsillectomy service, Stewartpatients (table VI).et al.[20] estimated that the overall incidence of POV followingSplinter[128] determined that patients who received intravenoustonsillectomy was 15.6% even in children who received combina-dexamethasone 150 µg/kg alone had more POV compared withtion intraoperative antiemetic therapy consisting of intravenousthe intravenous combination of dexamethasone 150 µg/kg plusdexamethasone 0.4 mg/kg (maximum of 8mg) and ondansetronondansetron 50 µg/kg. Each episode of POV increased the in-0.1–0.2 mg/kg for POV prophylaxis. This was in contrast to thehospital length of stay by 29 minutes. Similarly, another study[129]
findings of Ferrari and Donlon[19] who reported a 70% incidence inalso concluded that the combination of dexamethasone plus low-children undergoing tonsillectomy who received no POV prophy-dose ondansetron was effective in decreasing POV. Shendelaxis. The Stewart et al.[20] study illustrates the fact that POVet al.[119] concluded that intravenous droperidol 15 µg/kg pluscontinues to be a problem despite current antiemetic prophylaxisondansetron 100 µg/kg was more effective in reducing the inci-with combination therapy.dence of POV than either drug given alone.
Nearly all the strabismus combination therapy studies deter-5.2.2 Anesthetic Techniquesmined that antiemetic combinations had a better effect in decreas-
ing the incidence of nausea and vomiting than a single antiemeticInhalation Agents: Nitrous Oxide and Halothanealone. However, this depended on which antiemetics are com-Tables IV and VII, respectively, list anesthetic techniques andbined. When the antiemetic was combined with either droperidol
antiemetics that have been evaluated for their effectiveness inor dexamethasone, the combined effect was better than with eitherdecreasing POV and PONV following tonsillectomy.antiemetic used alone. However, if metoclopramide was one of the
combination antiemetics, the combined effect was not better than As in strabismus surgery (see section 5.1), the use of nitrouswith either agent alone. Children who are at moderate-to-high risk oxide has been controversial. Pandit et al.[105] concluded that,for POV are recommended to receive combination therapy with although a high incidence of POV was noted, there was notwo or three prophylactic antiemetics from different drug clas- difference in either the incidence or severity of POV betweenses.[63,119,123,130-134] children who did or did not receive nitrous oxide.
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 59
Table VI. Combination antiemetic therapy in children undergoing strabismus surgery
Author Antiemetics No. of Study endpoint Results Conclusionspts (% of pts)
Kymer et al.[130] Placebo 34 Emesis 56 Metoclopramide + droperidol = droperidol >Droperidol 0.3 mg/kg PO 41 26 metoclopramide = placebo (metoclopramideDroperidol 0.15 mg/kg PO 42 62 ineffective)Both metoclopramide + droperidol 37 22
Klockgether-Radke Placebo 40 Emesis 98 Ondansetron + droperidol = droperidol =et al.[131] Droperidol 0.075 mg/kg 40 32.5 ondansetron > placebo (all three groups better
Ondansetron 0.1 mg/kg 40 40 than placebo but no one regimen was superior toOndansetron + droperidol (dose 40 45 the other)as above)
Splinter and Ondansetron 0.15 mg/kg 150 Emesis 28 Low-dose ondansetron + dexamethasone > high-Rhine[63] Ondansetron 0.05 mg/kg + 150 9 dose ondansetron
dexamethasone 0.15 mg/kg
Kathirvel et al.[132] Placebo 25 Emesis 72 Ondansetron + metoclopramide = ondansetron >Ondansetron 0.1 mg/kg 25 40 metoclopramide > placeboMetoclopramide 0.25 mg/kg 25 60Ondansetron + metoclopramide 25 44(dose as above)
Fujii et al.[133] Granisetron 0.05 mg/kg 40 No emesis 80 Granisetron + droperidol > granisetron >Droperidol 0.05 mg/kg 40 No rescue 45 droperidolGranisetron + droperidol (dose as 40 medications required 98above)
Shende et al.[119] Placebo 60 Emesis 62.5 Ondansetron + droperidol > ondansetron =Droperidol 0.25 mg/kg 60 32 droperidol > placeboOndansetron 0.1 mg/kg 60 37Droperidol 0.15 mg/kg + 60 13ondansetron 0.1 mg/kg
Splinter[128] Ondansetron 0.05 mg/kg + 111 Emesis 5 Ondansetron + dexamethasone > ondansetrondexamethasone 0.15 mg/kg
Ondansetron 0.05 mg/kg 82 23
Caron et al.[123] Ondansetron 88 Nausea and vomiting 25.3 Ondansetron > droperidol + dimenhydrinate.Droperidol + dimenhydrinate 84 31.6 More emesis during ride home in droperidol
group (12.6% vs 3.6%)
Bhardwaj et al.[134] Placebo 31 Vomiting – early and 64.5 Ondansetron + dexamethasone > ondansetron >Ondansetron 0.15 mg/kg 39 24hr 33.3 placeboOndansetron 0.15 + 30 10 Low power for intergroup difference. Both groupsdexamethasone 0.2 mg/kg better than placebo but no difference between
groups
PO = oral; pts = patients; > indicates significantly greater efficacy; = indicates similar efficacy.
Propofol maintenance. The incidence of POV occurred 3.5 times morefrequently when halothane was used for maintenance of anesthesiaUse of propofol for anesthesia maintenance helps decreasecompared with when propofol was used for maintenance. Howev-PONV. Ved et al.[106] compared the effects of four anestheticer, these authors concluded there was no difference in thetechniques using nitrous oxide with halothane or propofol on POVendpoints of unplanned admissions or discharge times, despite aand recovery after outpatient tonsillectomy and adenoidectomy inreduced rate of POV using propofol rather than halothane pluschildren aged 3–10 years. The anesthetic techniques evaluatednitrous oxide for maintenance. The main factor that delayed hospi-were: (i) halothane for induction and maintenance; (ii) propofoltal discharge beyond 6 hours was POV that occurred within thefor induction and maintenance; (iii) halothane induction and pro-
pofol maintenance; and (iv) propofol induction and halothane first 6 postoperative hours.
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

60 Kovac
Table VII. Effects of antiemetics in children undergoing tonsillectomy on postoperative vomiting and postoperative nausea and vomiting
Author No. of Age (y) Antiemetic Conclusionspts
Rose et al.[137] 136 2–12 Midazolam 0.5 mg/kg PO Ondansetron 0.15 = dexamethasone 0.1 > midazolam >Dexamethasone 0.1 mg/kg ondansetron 0.075 = placeboOndansetron 0.15 mg/kgOndansetron 0.075 mg/kgPlacebo
Splinter and Rhine[138] 240 2–12 Ondansetron 0.15 mg/kg Ondansetron 0.15 > ondansetron 0.05Ondansetron 0.05 mg/kg
Splinter and Rhine[139] 216 2–12 Ondansetron 0.15 mg/kg Ondansetron = perphenazinePerphenazine 0.07 mg/kg
Sukhani et al.[75] 149 2–12 Dexamethasone 1 mg/kg Ondansetron = dolasetron = dexamethasone > placeboOndansetron 0.15 mg/kgDolasetron 0.5 mg/kgPlacebo
Stene et al.[140] 132 2–12 Metoclopramide 0.25 mg/kg IV Ondansetron > metoclopramide = placeboOndansetron 0.15 mg/kgPlacebo
Hamid et al.[141] 74 2–10 Ondansetron 0.1 mg Ondansetron > dimenhydrinate > placeboDimenhydrinate 0.5 mg/kgPlacebo
Fujii et al.[142] 90 4–10 Granisetron 40 µg/kg IV Ramosetron > granisetronRamosetron 6 µg/kg
Jensen et al.[143] 71 2–14 Tropisetron 0.2 mg/kg Tropisetron > placeboPlacebo
Holt et al.[144] 143 2–10 Tropisetron 0.1 mg/kg Tropisetron + dexamethasone > tropisetronTropisetron 0.1 + dexamethasone 0.5mg/kg
IV = intravenous; PO = oral; pts = patients; > indicates significantly greater efficacy; = indicates similar efficacy.
5.2.3 AntiemeticsFor the treatment of POV in the PACU following tonsillecto-my, a subhypnotic intravenous propofol bolus dose of 0.2 mg/kg
Ondansetronwas not effective and caused sedation and pain on injection.[107]
The incidence of POV during the first 24 hours’ post-tonsillec-tomy was significantly reduced by the use of preoperative oralNeuromuscular Blockadeondansetron 0.15 mg/kg compared with oral ondansetron 0.075
Reversal of neuromuscular blockade with intravenous atropinemg/kg or placebo in preadolescent children premedicated with oral
15 µg/kg and neostigmine was associated with a lower incidencemidazolam 0.5 mg/kg and intravenous dexamethasone 0.1 mg/
of POV compared with the combination of glycopyrrolate (gly-kg.[137] Similarly, Splinter and Rhine[138] compared high-dose
copyrronium bromide) 10 µg/kg and neostigmine. However, there(0.15 mg/kg) versus low-dose (0.05 mg/kg) intravenous ondanse-
was no significant difference in the number of patients who tron and concluded that a high dose was more effective than a lowrequired rescue antiemetics or additional analgesics.[108]
dose. While traditional, inexpensive antiemetics such asperphenazine have overall not been well studied in children, a
NSAIDs study by Splinter and Rhine[139] concluded that intravenous ondan-A systematic review[145] of 25 studies involving 1853 patients setron 0.15 mg/kg and intravenous perphenazine 0.07 mg/kg had
was conducted on the use of NSAIDs and the risk of operative-site similar effects on POV after tonsillectomy in day-case surgery.bleeding after tonsillectomy; 970 patients received an NSAID and Sukhani et al.[75] compared the effect of intravenous ondanse-883 received a non-NSAID or placebo. While NSAIDs and tron and dolasetron on POV after ambulatory tonsillectomy inopioids had similar analgesic efficacy, the risk of emesis was dexamethasone pretreated children aged 2–12 years. All childrensignificantly decreased with the use of NSAIDs. received intravenous dexamethasone 1 mg/kg (up to a maximum
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 61
of 25mg) and were randomized to receive before the start of undergoing tonsillectomy. With both drugs administered intrave-surgery intravenous ondansetron 0.15 mg/kg (maximum 4mg), nously during the time of anesthesia induction, these authorsdolasetron 0.5 mg/kg (maximum 25mg), or saline placebo. Both concluded that the combination was significantly more effectiveondansetron and dolasetron were more effective than placebo and than tropisetron alone in reducing PONV. The effectiveness ofhad similar effects on the incidence of POV and the need for dexamethasone used in combination with other antiemetics hasrescue antiemetics. been reviewed by Splinter et al.[63,64] and by Henzi et al.[84]
Steward et al.[147] conducted a systematic review on the effec-Stene et al.[140] evaluated intravenous metoclopramide 0.25 mg/tiveness of corticosteroids as antiemetics for POV following ton-kg, ondansetron 0.15 mg/kg, or placebo administered after ansillectomy. They determined that children who received a singleinhalation induction of halothane, nitrous oxide, and oxygen.intraoperative intravenous dose of dexamethasone 0.15–1 mg/kg,Prophylactic ondansetron was found to be more effective thanwith a maximum dose range of 8–25mg, were two times less likelymetoclopramide or placebo.to have POV in the first 24 hours than children receiving placebo.Hamid et al.[141] concluded that intravenous ondansetronTheir review stated an NNT of four, which indicated that routine0.1 mg/kg was superior to intravenous dimenhydrinate 0.5 mg/kguse of dexamethasone in four children would be expected to resultor placebo. Of special importance was that two children who hadin one less patient experiencing post-tonsillectomy emesis. Addi-received ondansetron vomited large volumes of bloody fluid 9 andtionally, children receiving dexamethasone were found to be more22 hours after surgery without previous signs of occult bleeding.likely to advance to a soft and solid diet on the first post-tonsillec-The authors concluded that, while ondansetron was more effectivetomy day than those who received placebo. No adverse eventsthan dimenhydrinate or placebo, antiemetics may mask the pres-were reported in these trials that could be attributed to the single-ence of bleeding and blood in the stomach by preventing vomiting,dose administration of dexamethasone.and that this should be appreciated when adenotonsillectomy is
Another meta-analysis by Steward et al.[153] concluded that aperformed on an outpatient basis. A similar comment was noted bysingle intravenous dose of dexamethasone was an effective, safe,Courtman et al.[146] who emphasized the importance of earlyand inexpensive treatment for reducing POV following pediatricdiagnosis of bleeding in this patient population who may betonsillectomy. Given the frequency of tonsillectomy procedures,receiving antiemetics such as ondansetron.the relative safety and low cost of dexamethasone, and the reduc-
Ramosetron versus Granisetron tion in postoperative morbidity, the use of a single intravenousFujii et al.[142] compared intravenous granisetron 40 µg/kg dose of dexamethasone during pediatric tonsillectomy was recom-
versus intravenous ramosetron 6 µg/kg for prevention of POV mended. These conclusions were further substantiated in studiesadministered at the end of tonsillectomy surgery. These research- conducted by Aouad et al.,[149] Pappas et al.,[150] and Vosdoganisers concluded that ramosetron was a significantly better antiemetic and Baines.[151]
than granisetron for the long-term prevention of POV. Aouad et al.[149] determined that the effect of a single dose ofintravenous dexamethasone 0.5 mg/kg in children significantlyTropisetrondecreased the incidence of POV during the first 24 hours, short-Jensen et al.[143] evaluated the effectiveness of reducing POV inened the time to first oral intake, and decreased the duration ofchildren undergoing tonsillectomy after administering either pla-intravenous fluid hydration, which in turn improved patient satis-cebo or intravenous tropisetron 0.2 mg/kg (maximum of 5mg) atfaction. Pappas et al.[150] determined that intravenous dex-the time of anesthesia induction with halothane, nitrous oxide, andamethasone 1 mg/kg (maximum dose of 25mg) significantly de-oxygen. Tropisetron had significantly better POV efficacy com-creased the incidence of PONV in the 24 hours’ post-discharge,pared with placebo.improved oral intake, decreased the frequency of parental phone
Dexamethasone calls, and resulted in no returns to the hospital for PONV manage-As corticosteroids have been used for their anti-inflammatory ment or poor oral intake. Vosdoganis and Baines[151] similarly
effect in ENT surgery,[144] numerous studies[52,144,147-152] have eval- determined that dexamethasone substantially reduced POV afteruated the effectiveness of corticosteroids for POV following ton- tonsillectomy.sillectomy. The precise mechanism of action by which corticosteroids such
Holt et al.[144] compared the effectiveness of tropisetron 0.1 mg/ as dexamethasone decrease PONV is not known. Several theo-kg (maximum of 2mg) alone versus the combination of tropisetron ries[152-154] have been proposed and include membrane stabiliza-0.1 mg/kg (maximum of 2mg) plus dexamethasone 0.5 mg/kg tion, anti-inflammatory effect, prostaglandin antagonism, trypto-(maximum of 8mg) for the prevention of PONV in children phan depletion, endorphin release, inhibition of arachidonic acid
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

62 Kovac
5.3.4 Burn Surgeryrelease, and modulation of the by-products of arachidonic acidIn a study on the prevention of PONV in children undergoingmetabolism (i.e. lipoxygenase and a decrease in the amount of
reconstructive burn surgery, the effectiveness of ondansetron 0.1available serotonin). Of importance is the timing of administrationmg/kg and dimenhydrinate 0.5 mg/kg was found to be similar.[24]of corticosteroids as studied by Wang et al.[155] who reported thatA retrospective chart review[25] of 38 pediatric patients aged 5–12to have maximal effect in the PACU (early PONV) and in theyears undergoing a total of 46 burn procedures concluded thatward/at home (late PONV), dexamethasone should be adminis-100% of children with reconstructive surgeries of the scalp exper-tered before anesthesia induction, rather than at the end of surgery.ienced PONV compared with only 45% of children whose sur-Administration of dexamethasone at the end of surgery had nogeries did not involve the scalp. Consequently, an increased timeeffect on PONV at postoperative hours 0–2 in the PACU, but wasto oral intake was also seen in pediatric patients who underwenteffective at hours 2–24 in the ward/at home. However, becauseoperations involving the scalp.pre-induction dexamethasone has reportedly caused perineal dis-
comfort due to the injection solution containing phosphate,[156,157]5.3.5 Craniofacial Operations
administration of dexamethasone either in diluted form or post-Gurler et al.[160] determined that the prophylactic use of intrave-
induction has been recommended.nous ondansetron 0.15 mg/kg versus placebo significantly reducedPOV after craniofacial operations in children.
5.3 Additional Pediatric Surgeries and Procedures
5.3.6 Neurosurgery
Neufeld[161] reviewed the role of ondansetron in the manage-5.3.1 Tympanoplasty
ment of PONV in children following posterior fossa neurosurgicalvan den Berg[158] compared the use of intravenous ondansetronprocedures, noting that the proximity of brain stem emetogenicversus intramuscular prochlorperazine for the prevention ofcenters to the surgical site added to the usual PONV risk factors.PONV after tympanoplasty in pediatric and adult patients, andOndansetron was believed to be more effective than the tradition-reported that the incidence of PONV in the PACU was similarally used antiemetics such as dimenhydrinate and metoclopramidebetween children and adults. While the onset of PONV wasin this patient population.delayed in patients given intramuscular prochlorperazine, vomit-
Furst et al.[26] studied the effect of ondansetron versus placeboing was less severe in patients who received intravenous ondanse-in children undergoing craniotomies for resective procedures. Intron. The author concluded that while prophylactic intramuscularthe first 8 hours postoperatively, the incidence of POV was signifi-prochlorperazine 0.2 mg/kg and intravenous ondansetron 0.06 mg/cantly less with intravenous ondansetron 0.15 mg/kg comparedkg had similar effectiveness in reducing PONV after tympa-with placebo. However, for the 24-hour postoperative time inter-noplasty, intramuscular prochlorperazine 0.01 mg/kg was lessval, the incidence of POV was not significantly different betweeneffective.the ondansetron and placebo groups.
5.3.2 Ear Surgery5.3.7 Magnetic Resonance ImagingWoodward et al.[159] evaluated the effectiveness of a propofolA retrospective review[15] evaluated 234 consecutive cases ofinfusion versus a thiopental/isoflurane anesthesia technique for
POV in children undergoing anesthesia for magnetic resonanceprominent ear correction surgery. In the propofol infusion group,imaging. At an incidence rate of 9%, it was concluded that POVsignificantly fewer children complained of nausea or emesis, andwas an infrequent complication of inhalation anesthesia duringsignificantly more children were considered to be fit for dischargemagnetic resonance imaging.on the day of surgery.
5.3.3 Radiofrequency Catheter Ablation 6. Development of PONV and POV ManagementRadiofrequency catheter ablation is considered to be a high-risk Guidelines and Algorithms
procedure for PONV. Erb et al.[23] reported that in children andadolescents undergoing radiofrequency catheter ablation, the inci- Darkow et al.[162] in 2001 evaluated the impact of antiemeticdence of PONV was high (60%) with an isoflurane-based tech- selection on PONV and patient satisfaction in a prospective obser-nique, whereas the incidence of POV was significantly reduced to vational study. The prophylactic antiemetic that was most oftena very low level (5%) with a propofol-based infusion technique. administered to 292 patients was droperidol (200 patients), fol-While the prophylactic use of ondansetron and droperidol was lowed by metoclopramide (134 patients) or dexamethasone (55ineffective, a propofol-based infusion technique was highly effec- patients). This study was conducted prior to the US FDA ‘blacktive in preventing PONV in these children. box’ warning on droperidol. Nevertheless, these authors deter-
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 63
mined that the choice of antiemetic drug given for PONV prophy- avoiding nitrous oxide, opioids, and neuromuscular antagonists.laxis had little impact on clinical outcome or patient satisfaction. Pain control was believed to be extremely important, and the useThey concluded that traditional antiemetics should form the core of regional blocks was recommended if possible. Double- orof antiemetics selected and used for PONV prophylaxis in an triple-combination prophylactic antiemetic therapy with dex-ambulatory surgery setting. amethasone, a 5-HT3 antagonist, and an antiemetic of a different
class, such as perphenazine or dimenhydrinate, should also beDrake et al.[163] further evaluated the impact of an antiemeticadministered. Non-pharmacologic measures such as acupressureprotocol on PONV in children in an attempt to demonstrate ashould be considered, along with ensuring that the patient avoidsdecreased incidence of PONV with the use of an antiemeticsudden movement, providing a quiet environment, administeringprotocol. PONV was recorded in 272 children aged from 1.5 to 15adequate intravenous fluids, and not forcing oral fluids beforeyears following inpatient surgery under general anesthesia. Studydischarge. All these measures have been found to decrease thegroups were determined based on one group having surgerypossibility of PONV in children. The authors stated that adminis-1 month before the introduction of a formalized antiemetic proto-tration of effective prophylactic antiemetics should be encouraged,col (group 1 = 138 patients) and the other having surgery 2 monthsas emetic symptoms in the hospital were the most significantafter introduction of the protocol (group 2 = 134 patients). Thepredictor of nausea and vomiting at home. Treatment of pain andoverall incidence of postoperative nausea (PON) and POV follow-instructions for antiemetic treatment at home were believed to being introduction of the protocol was 36% and 34%, respectively.important needed improvements in PONV therapy.[166]Moderate-to-severe PON significantly decreased after introduc-
tion of the protocol (18% vs 9%), but the change in moderate-to-severe POV failed to reach statistical significance (19% vs 11%). 7. Guidelines for POV Prophylaxis in ChildrenThe proportion of children who had repeat PON decreased after
Because of the initial suggestions for PONV guidelines (sectionintroduction of the protocol, but the proportion who had repeated6) and the belief that an evidence-based analysis of the PONVepisodes of POV remained unchanged. The authors concluded thatliterature would be beneficial, a panel of pediatric and adultthe introduction of a postoperative antiemetic protocol improved‘PONV experts’ met as an independent panel in February 2002prescribing frequency resulting in a decreased incidence of moder-and November 2005 to summarize the literature and developate-to-severe PON and a reduction in the number of patients withevidence-based guidelines for the management of PONV in adultrepeated PON, but not POV.and pediatric patients. This multispecialty panel consisted of anes-De Negri and Ivani[164] reviewed the management of PONV inthesiologists, a nurse anesthetist, a pharmacist, a nurse, a statisti-children, stating that, while there is little evidence to supportcian, and a surgeon.routine prophylactic administration of antiemetics in children at
According to the revised 2006 Consensus Guidelines for Man-low risk of PONV, populations at higher risk, such as childrenaging PONV,[167-170] an initial approach to the management ofundergoing strabismus surgery or tonsillectomy, could benefitPONV or POV in children is to identify children at high risk.from the use of adequate prophylactic antiemetics.Because of the difficulty in diagnosing nausea in younger children,Initial recommendations for the use of antiemetic guidelines for
chemotherapy-induced nausea and vomiting and PONV have ap-peared in reviews about the American Society of Hospital Pharma-cists Therapeutic Guidelines on the Pharmacologic Managementof Nausea and Vomiting.[165] Advocacy of a particular antiemetictreatment requires knowledge of high-risk groups, accurate assess-ment, timely intervention, and thorough evaluation of pharmaco-logic and non-pharmacologic measures.
Rose and Watcha,[166] in a review of PONV in pediatric pa-tients, stated that based on current knowledge, the anesthetic planfor a child with a previous history of severe PONV and undergoinga procedure known to be associated with a high incidence ofPONV should include premedication with a benzodiazepine orclonidine and preferential use of regional anesthetic techniques. Ifgeneral anesthesia was necessary, anesthesia providers shouldconsider the use of protocols for induction and maintenance,
Table VIII. Recommended antiemetic intravenous doses for chil-dren[167-170]
Drug Dose
Ondansetron[11,171] a 50–100 µg/kg up to 4mg
Dolasetron[73,74] 350 µg/kg up to 12.5mg
Dexamethasone[84,172,173] 150 µg/kg up to 5mg
Droperidol[85] b 50–75 µg/kg up to 1.25mg
Dimenhydrinate[121] 0.5 mg/kg up to 1.2mg
Perphenazine[139,174] 70 µg/kg up to 5mg
Granisetron[80] 40 µg/kg up to 0.6mg
Tropisetron[175] 0.1 mg/kg up to 2mg
a Approved for postoperative vomiting in pediatric patients aged 1month or older.
b US FDA black box warning.
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

64 Kovac
efficacy in the prevention of vomiting rather than nausea, they areconsidered to be the antiemetic drugs of first choice for prophylax-is in children at moderate-to-high risk for POV.[83]
When dexamethasone is used in children at an intravenous doseof 150 µg/kg, the NNT to prevent early and late vomiting isapproximately four. Droperidol has been used for POV prophylax-is, administered in an intravenous dose range of 50–75 µg/kg. TheNNT of droperidol for prevention of early vomiting is approxi-mately five, and for late vomiting is between four and five.However, because of the increased risk of extrapyramidal symp-toms, high levels of sedation found with the use of droperidol, andthe US FDA’s ‘black box’ warning, droperidol was recommendedto be reserved for patients in whom all other therapies have failedand who are being admitted to the hospital.[83] More research needsto be performed to find the best antiemetic for the treatment ofnausea in children to replace the previously used best anti-nauseamedication, droperidol.
An algorithm that can be used for the management of PONV inchildren is shown in figure 2.[83] A new algorithm from theRevised PONV Consensus guidelines is about to be released. As inthe 2003 guidelines, one should evaluate children for their level of
Evaluate risk ofPONV in
surgical patient
Low
No prophylaxisunless there isrisk of medicalsequelae from
vomiting
Moderate
Consider regionalanesthesia
Not indicated
Patients atmoderate risk
Patients athigh risk
Consider antiemeticprophylaxis with
monotherapy (adults)or combination
therapy (childrenand adults)
Initiate combinationtherapy with 2 or 3prophylactic agents
from different classes
If general anesthesia isused, reduce baseline riskfactors and consider using
non-pharmacologic therapies
High
Fig. 2. Algorithm for the management of postoperative nausea and vomit-ing (PONV) [reproduced from Gan et al.,[83] with permission].
PONV risk and reduce baseline PONV risk factors. Patient prefer-ences, cost effectiveness and the level of risk as low, medium orit was noted that studies in children are often limited to POV andhigh should be considered. A portfolio of antiemetics for prophy-not nausea. It is important to identify children at high risk for POVlaxis and treatment as in table VIII is recommended. Droperidolas candidates for prophylactic antiemetic therapy. The risk factorsshould be used in children only if other antiemetic therapy hasfor POV in children are similar to those in adults, but withfailed and the patient is being admitted to the hospital.[167,169]differences such as: (i) vomiting occurs twice as frequently inProphylaxis is believed to be useful only for children at moderate-children as in adults; (ii) differences between boys and girls are notto-high risk for PONV and, if possible, regional anesthesia shouldobserved before puberty (after puberty females have 2- to 3-foldbe considered in these patients. If general anesthesia is planned,the incidence of PONV as males); (iii) as children grow older, the
POV risk increases until puberty, then decreases; and (iv) strabis- one should try to use strategies to reduce the baseline PONV riskmus repair and tonsillectomy are specific surgeries that have a factors (table IX) whenever possible, including the use of non-high POV risk.[83,168] pharmacologic therapies such as acupuncture or acupressure. In
general, combination antiemetic therapy is superior to monother-As the POV rate in children is estimated to be twice as frequentapy for PONV prophylaxis, as antiemetics with differentas in adults, more children than adults are candidates for POV
prophylaxis. Table VIII lists recommended doses of antiemeticsfor children.[167,169] Ondansetron has been studied very extensivelyfor POV prophylaxis in children at an intravenous dose range of50–100 µg/kg up to a maximum of 4mg. Ondansetron 0.1 mg/kghas been shown to be effective in children aged <2 years. Com-pared with placebo, the NNT of ondansetron to prevent early (0–6hours) and late (0–24 hours) vomiting in children is between twoand three. Ondansetron is US FDA approved in children aged 1month and older. The optimal intravenous dose for POV prophy-laxis with dolasetron in children is 350 µg/kg up to a maximum of12.5mg. Because the 5-HT3 antagonists as a group have greater
Table IX. Strategies to reduce baseline postoperative nausea and vomit-ing risk factors (reproduced from Gan et al.,[83] with permission)
Use of regional anesthesia
Use of propofol for induction and maintenance of anesthesia
Use of intraoperative supplemental oxygen
Use of hydration
Avoidance of nitrous oxide
Avoidance of volatile anesthetics
Minimization of intraoperative and postoperative opioids
Minimization of neostigmine
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 65
because of the inability of children to effectively express distressafter surgery, often leading to the ineffective treatment of PONVas well as pain. Strabismus surgery and tonsillectomy are the morefrequent and emetogenic surgeries performed in children. The5-HT3 receptor antagonists, ondansetron, dolasetron, granisetron,and tropisetron, as well as dexamethasone have been effectivetreatments when used alone and as combination and multimodalantiemetic therapy. PONV guidelines and algorithms help clinicalpractitioners evaluate and treat children in a cost-effective manner.
Acknowledgments
In the past Dr Kovac has received grant support from GlaxoWellcome(now GlaxoSmithKline), Roche Pharmaceuticals, Hoechst Marion Roussel(now Sanofi-Aventis), Helsinn, and Merck and has participated in the Speak-ers Bureau for GlaxoSmithKline, Roche Pharmaceuticals, Abbott Laborato-ries, and Baxter Healthcare. Dr Kovac has served as an advisor for Merck,GlaxoSmithKline, Roche Pharmaceuticals, Sanofi-Aventis, Adolor, and Hel-sinn. No sources of funding were used to assist in the preparation of thisarticle.
Table X. Antiemetic treatment for patients with postoperative nausea andvomiting (PONV) who did not receive prophylaxis or in whom prophylaxisfailed – excluding inciting medication or mechanical causes of PONV (re-produced from Gan et al.,[83] with permission)
Initial therapy Treatment
No prophylaxis or dexamethasone Administer small-dose serotonin(5-hydroxytryptamine; 5-HT3)antagonist
5-HT3 antagonista plus second Use drug from different classagentb
Triple therapy with 5-HT3 Do not repeat initial therapyantagonista plus two other agentsb Use drug from different class orwhen PONV occurs <6h after propofol 20mg as needed insurgery postanesthesia care unit (adults)
Triple therapy with 5-HT3 Repeat 5-HT3 antagonista andantagonista plus two other agentsb droperidolc (not dexamethasone orwhen PONV occurs >6h after transdermal scopolamine)surgery Use drug from different class
a Ondansetron, granisetron, dolasetron.
b Dexamethasone, transdermal scopolamine.
c US FDA black box warning.
References1. Westman HR. Postoperative complications and unanticipated hospital admissions.neuroemetogenic receptors and sites of action can be used to
Semin Pediatr Surg 1999; 8 (1): 23-9optimize efficacy. 2. Rose JB, Watcha MF. Postoperative nausea and vomiting. In: Benumof JL,
Saidman LJ, editors. Anesthesia and perioperative complications. 2nd ed. St.Children who are at moderate-to-high risk for PONV shouldLouis (MO): Mosby, 1999: 425-40receive combination therapy with two or three prophylactic drugs
3. Baines D. Postoperative nausea and vomiting in children. Paediatr Anaesth 1996; 6from different drug classes. The 5-HT3 antagonists can be effec- (1): 7-14
4. Awad I, Moore M, Rushe C, et al. Unplanned hospital admission in childrentively combined with dexamethasone to significantly reduce bothundergoing day-case surgery. Eur J Anaesth 2004; 21: 379-83
the frequency and severity of PONV. It has been suggested that in 5. Tramer MR. A rational approach to the control of postoperative nausea andvomiting: evidence from systematic reviews: part I. Efficacy and harm ofchildren, the dexamethasone dose should not exceed 150 µg/kgantiemetic interventions, and methodological issues. Acta Anesthesiol Scand(maximum intravenous dose of 5mg); droperidol should not ex-2001; 45: 5-13
ceed 75 µg/kg (intravenous 1.25mg); dolasetron should not exceed 6. Tramer MR. A rational approach to the control of postoperative nausea andvomiting: evidence from systematic reviews: part II. Recommendations for350 µg/kg (intravenous 12.5mg); and ondansetron should notprevention and treatment, and research agenda. Acta Anesthesiol Scand 2001;
exceed 0.1 mg/kg (intravenous 4mg). Useful combination an- 45: 14-97. Tramer MR, editor. Evidence-based resource in anaesthesia and analgesia.tiemetic therapies in children are: (i) ondansetron 0.05 mg/kg plus
London: BMJ Books, 2000dexamethasone 0.15 mg/kg[63,128]; (ii) ondansetron 0.1 mg/kg plus8. Kotiniemi LH, Ryhanen PT, Valanne J, et al. Postoperative symptoms at home
droperidol 0.15 mg/kg[119]; and (iii) tropisetron 0.1 mg/kg plus following day-case surgery in children: a multicentre survey of 551 children.Anaesthesia 1997; 52 (1): 963-9dexamethasone 0.5 mg/kg.[144] Smaller doses such as intravenous
9. D’Errico C, Voepel-Lewis TD, Siewert M, et al. Prolonged recovery stay andondansetron 50 µg/kg have been found to be effective in combina- unplanned admission of the pediatric surgical outpatient: an observational
study. J Clin Anesth 1998; 10 (6): 482-7tion with other antiemetics in children. Further guidelines for the10. Rowley MP, Brown TC. Postoperative vomiting in children. Anaesth Intensivetreatment of PONV in patients who did not receive prophylaxis or
Care 1982; 10 (4): 309-13in whom prophylaxis failed are shown in table X.[83] Transdermal 11. Khalil SN, Roth AG, Cohen IT, et al. A double-blind comparison of intravenous
ondansetron and placebo for preventing postoperative emesis in 1- to 24-scopalamine is not US FDA approved for use in children.month-old pediatric patients after surgery under general anesthesia. AnesthAnalg 2005; 101: 356-61
12. Byers GF, Doyle E, Best CJ, et al. Postoperative nausea and vomiting in paediatric8. Conclusionssurgical inpatients. Paediatr Anaesth 1995; 5 (4): 253-6
13. Villeret I, Laffon M, Duchalais A, et al. Incidence of postoperative nausea andvomiting in paediatric ambulatory surgery. Paediatr Anaesth 2002; 12 (8): 712-Despite our increased understanding of the etiology of nausea7
and vomiting, POV and PONV continue to be problems in chil- 14. Patel RI, Hannallah RS. Anesthetic complications following pediatric ambulatorydren. POV is more commonly studied in children than PONV surgery: a three-year study. Anesthesiology 1988; 69: 1009-12
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

66 Kovac
15. Murray DJ, Schmid CM, Forbes RB. Anesthesia for magnetic resonance imaging 43. Apfel CC, Laara E, Koivuranta M, et al. A simplified risk score for predictingin children: a low incidence of protracted post-procedure vomiting. J Clin postoperative nausea and vomiting: conclusions from cross-validations be-Anesth 1995; 7 (3): 232-6 tween two centers. Anesthesiology 1999; 91 (3): 693-700
16. Schofield NM, White JB. Interrelations among children, parents, premedication, 44. Eberhart LHJ, Geldner G, Kranke P, et al. The development and validation of a riskand anaesthetists in paediatric day stay surgery. BMJ 1989; 299: 1371-5 score to predict the probability of postoperative vomiting in pediatric patients.
17. Karlsson E, Larsson LE, Nilsson K. Postanesthetic nausea in children. Acta Anesth Analg 2004; 99: 1630-7Anaesthesiol Scand 1990; 34: 515-8 45. Haigh CG, Kaplan LA, Durham JA. Nausea and vomiting after gynecological
18. Ridings P, Gault D, Khan L. Reduction in postoperative vomiting after surgical surgery: a meta-analysis of factors affecting their incidence. Br J Anaesth 1993;correction of prominent ears. Br J Anaesth 1994; 72: 592-3 71: 512-22
19. Ferrari LR, Donlon JV. Metoclopramide reduces the incidence of vomiting after 46. Wang SM, Kain ZN. Preoperative anxiety and postoperative nausea and vomitingtonsillectomy in children. Anesth Analg 1992; 75: 351-4 in children: is there an association? Anesth Analg 2000; 90 (3): 571-5
20. Stewart PC, Baines DB, Dalton C. Paediatric day stay tonsillectomy service: 47. Apfel CC, Kranke P, Katz MH, et al. Volatile anaesthetics may be the main causedevelopment and audit. Anaesth Intensive Care 2002; 30 (5): 641-6 of early but not delayed postoperative vomiting: a randomized controlled trial
21. Abramowitz MD, Oh TH, Epstein BS, et al. The antiemetic effect of droperidol of factorial design. Br J Anaesth 2002; 88 (5): 659-68following outpatient strabismus surgery in children. Anesthesiology 1983; 59: 48. Elliott RA, Payne K, Moore JK, et al. Clinical and economic choices in anaesthesia579-83 for day surgery: a prospective randomised controlled trial. Anaesthesia 2003;
22. Kuhn I, Scheifler G, Wissing H. Incidence of nausea and vomiting in children after 58 (5): 412-21strabismus surgery following desflurane anaesthesia. Paediatr Anaesth 1999; 9
49. Goa KL, Noble S, Spencer CM. Sevoflurane in paediatric anaesthesia: a review.(6): 521-6
Pediatr Drugs 1999; 1 (2): 127-5323. Erb TO, Hall JM, Ing RJ, et al. Postoperative nausea and vomiting in children and
50. Oddby E, Englund S, Lonnqvist PA. Postoperative nausea and vomiting in paedia-adolescents undergoing radiofrequency catheter ablation: a randomized com-
tric ambulatory surgery: sevoflurane versus spinal anaesthesia with propofolparison of propofol- and isoflurane-based anesthetics. Anesth Analg 2002; 95
sedation. Paediatr Anaesth 2001; 11 (3): 337-42(6): 1577-81
51. Tramer M, Moore A, McQuay H. Omitting nitrous oxide in general anesthesia:24. McCall JE, Stubbs K, Saylors S, et al. The search for cost-effective prevention ofmeta-analysis of intraoperative awareness and postoperative emesis in random-postoperative nausea and vomiting in the child undergoing reconstructive burnized controlled trials. Br J Anaesth 1996; 76: 186-93surgery: ondansetron versus dimenhydrinate. J Burn Care Rehabil 1999; 20 (4):
52. Divatia J, Vaidya JS, Badwe RA, et al. Omission of nitrous oxide during anesthesia309-15reduces the incidence of postoperative nausea and vomiting: a meta-analysis.25. Stubbs TK, Saylors S, Jenkins M, et al. Pediatric patients experiencing postopera-Anesthesiology 1996; 85: 1055-62tive nausea and vomiting after burn reconstruction surgery: an analysis. J Burn
53. Hartung J. Twenty-four of twenty-seven studies show a greater incidence of emesisCare Rehabil 1999; 20 (3): 236-8associated with nitrous oxide than with alternative anesthetics. Anesth Analg26. Furst SR, Sullivan LJ, Soriano SG, et al. Effects of ondansetron on emesis in the1996; 83: 114-6first 24 hours after craniotomy in children. Anesth Analg 1996; 83 (2): 325-8
54. Splinter WM, Komocar L. Nitrous oxide does not increase vomiting after dental27. Borison HL, Wang SC. Physiology and pharmacology of vomiting. Pharmacol Revrestorations in children. Anesth Analg 1997; 84 (3): 506-81953; 5: 192-230
55. Bortone L, Picetti E, Mergoni M. Anaesthesia with sevoflurane in children: nitrous28. Wang SC, Borison HL. The vomiting center: a critical experimental analysis. Archoxide does not increase postoperative vomiting. Paedatr Anaesth 2002; 12 (9):Neurol Psychiatry 1950; 63: 928-41775-929. Kovac AL. Prevention and treatment of postoperative nausea and vomiting. Drugs
2000; 59 (2): 213-43 56. Hannallah RS, Britton JT, Schafer PG, et al. Propofol anaesthesia in paediatric30. Brett CM, Zwass MS. Chapter 23: eyes, ears, nose, throat and dental surgery. In: ambulatory patients: a comparison with thiopentone and halothane. Can J
Gregory GA, editor. Pediatric anesthesia. 4th ed. Philadelphia (PA): Churchill Anaesth 1994; 41 (1): 12-8Livingstone, 2002: 691 57. Kearney R, Mack C, Entwistle L. Withholding oral fluids from children undergo-
31. Andrews PLR, Davis CJ, Binham S, et al. The abdominal visceral inervation and ing day surgery reduces vomiting. Paediatr Anaesth 1998; 8 (4): 331-6the emetic reflex: pathways, pharmacology and plasticity. Can J Physiol 58. Schreiner MS. Should children drink before discharge from day surgery? Anesthe-Pharmacol 1990; 668: 325-45 siology 1992; 76 (4): 528-33
32. Borison HL. Area postrema: chemoreceptor circumventricular organ of the medula 59. Sneyd JR, Carr A, Byrom WD, et al. A meta-analysis of nausea and vomitingoblongata. Prog Neurobiol 1989; 32: 351-90 following maintenance of anaesthesia with propofol or inhalational agents. Eur
33. Watcha MF, White PF. Postoperative nausea and vomiting: its etiology, treatment J Anaesthesiol 1998; 15: 433-45and prevention. Anesthesiology 1992; 77: 162-84 60. Tramer MR, Moore RA, McQuay HJ. Propofol and bradycardia: causation, fre-
34. Palazzo MGA, Strunin L. Anaesthesia and emesis: I. Etiology. Can Anaesth Soc J quency and severity. Br J Anaesth 1997; 78: 642-511984; 31: 178-87
61. Murat I, Constant I, Maud’huy H. Perioperative anaesthetic morbidity in children:35. Bellville J. Postanesthetic nausea and vomiting. Anesthesiology 1961; 22 (5): 773-
a database of 24,165 anaesthetics over a 30-month period. Paediatr Anaesth80
2004; 14: 158-6636. Bellville JW, Bross IDJ, Howland WS. Postoperative nausea and vomiting: IV.
62. Culy CR, Bhana N, Plosker GL. Ondansetron: a review of its use as an antiemeticFactors related to postoperative nausea and vomiting. Anesthesiology 1960; 21in children. Pediatr Drugs 2001; 3 (6): 441-79(2): 186-93
63. Splinter WM, Rhine EJ. Low-dose ondansetron with dexamethasone more effec-37. Lerman J. Surgical and patient factors involved in postoperative nausea andtively decreases vomiting after strabismus surgery in children than does high-vomiting. Br J Anaesth 1992; 69 (7 Suppl. 1): 24S-32Sdose ondansetron. Anesthesiology 1998; 88: 72-538. Stefanini E, Clement-Cormier Y. Detection of receptors in the area postrema. Eur J
64. Splinter WM, Rhine EJ, Roberts DJ, et al. Prevention of vomiting after strabismusPharmacol 1981; 74: 258-60surgery in children: dexamethasone alone vs dexamethasone plus low-dose39. Atweh SF, Kuhar MJ. Autoradiographic localization of opiate receptors in the ratondansetron [abstract]. Anesth Analg 1998; 86 Suppl.: S419brain: II. The brain stem. Brain Res 1977; 129: 1-12
65. Furst SR, Rodarte A. Prophylactic antiemetic treatment with ondansetron in40. Palacios JM, Wamsley JK, Kuhar MJ. The distribution of histamine H1-receptorschildren undergoing tonsillectomy. Anesthesiology 1994; 81: 799-803in the rat brain: an autoradiographic study. Neuroscience 1981; 6: 15-7
66. Lawhorn CD, Kymer PJ, Stewart FC, et al. Ondansetron dose response curve in41. Philip BK. Etiologies of postoperative nausea and vomiting. Pharmacy Ther 1997;high-risk pediatric patients. J Clin Anesth 1997; 9 (8): 637-4222 (7 Suppl.): 18S-25S
42. Saito R, Takano Y, Kamiya HO. Roles of substance P and NK (1) receptor in the 67. Patel RI, Davis PJ, Orr RJ, et al. Single-dose ondansetron prevents postoperativebrainstem in the development of emesis. J Pharmacol Sci 2003; 91 (2): 87-94 vomiting in pediatric outpatients. Anesth Analg 1997; 85 (3): 538-45
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 67
68. Rose JB, McCloskey JJ. Rapid intravenous administration of ondansetron or 92. Wang SM, Hofstadter MB, Kain ZN. An alternative method to alleviate postopera-metoclopramide is not associated with cardiovascular compromise in children. tive nausea and vomiting in children. J Clin Anesth 1999; 11 (3): 231-4Paediatr Anaesth 1995; 5 (2): 121-4 93. Lee A, Done ML. The use of nonpharmacologic techniques to prevent postopera-
69. Scuderi PE, Weaver JRG, James RL, et al. A randomized, double-blind, placebo tive nausea and vomiting: a meta-analysis. Anesth Analg 1999; 88 (6): 1362-9controlled comparison of droperidol, ondansetron and metoclopramide for the 94. Wang SM, Kain ZN. P6 acupoint injections are as effective as droperidol inprevention of vomiting following outpatient strabismus surgery in children. controlling early postoperative nausea and vomiting in children. Anesthesiolo-J Clin Anesth 1997; 9: 551-8 gy 2002; 97 (2): 359-66
70. Domino KB, Anderson EA, Polisser NL, et al. Comparative efficacy and safety of 95. Schlager A, Offer T, Baldissera I. Laser stimulation of acupuncture point P6ondansetron, droperidol, and metoclopramide for preventing postoperative reduces postoperative vomiting in children undergoing strabismus surgery. Br Jnausea and vomiting: a meta-analysis. Anesth Analg 1999; 88 (6): 1370-9 Anaesth 1998; 81 (4): 529-32
71. Khalil S, Rodarte A, Weldon BC, et al. Intravenous ondansetron in established 96. Rusy LM, Hoffman GM, Weisman SJ. Electroacupuncture prophylaxis of postop-postoperative emesis in children: S3A-381 Study Group. Anesthesiology 1996; erative nausea and vomiting following pediatric tonsillectomy with or without85 (2): 270-6 adenoidectomy. Anesthesiology 2002; 96 (2): 300-5
72. Ummenhofer W, Frei JG, Urwyler A, et al. Effects of ondansetron in the prevention 97. Allen D, Jorgensen C, Sims C. Effect of tropisetron on vomiting during patient-of postoperative nausea and vomiting in children. Anesthesiology 1994; 81 (4): controlled analgesia in children. Br J Anaesth 1999; 83 (4): 608-10804-10 98. Kokinsky E, Thornberg E, Nilsson K, et al. Postoperative nausea and vomiting in
73. Olutoye O, Jantzen EC, Alexis R, et al. A comparison of the costs and efficacy of children using patient-controlled analgesia: the effect of prophylactic intrave-ondansetron and dolasetron in the prophylaxis of postoperative vomiting in nous dixyrazine. Acta Anaesthesiol Scand 1999; 43 (2): 191-5pediatric patients undergoing ambulatory surgery. Anesth Analg 2003; 97 (2): 99. Munro FJ, Fisher S, Dickson U, et al. The addition of antiemetics to the morphine390-6 solution in patient controlled analgesia syringes used by children after an
74. Wagner D, Pandit U, Voepel-Lewis T, et al. Dolasetron for the prevention of appendectomy does not reduce the incidence of postoperative nausea andpostoperative vomiting in children undergoing strabismus surgery. Paediatr vomiting. Paediatr Anaesth 2002; 12 (7): 600-3Anaesth 2003; 13: 522-6 100. Wennstrom B, Reinsfelt B. Rectally administered diclofenac (Voltaren) reduces
75. Sukhani R, Pappas AL, Lurie J, et al. Ondansetron and dolasetron provide vomiting compared with opioid (morphine) after strabismus surgery in children.equivalent postoperative vomiting control after ambulatory tonsillectomy in Acta Anaesthesiol Scand 2002; 46 (4): 430-4dexamethasone-pretreated children. Anesth Analg 2002; 95 (5): 1230-5 101. Ozcan AA, Gunes Y, Haciyakupoglu G. Using diazepam and atropine before
76. Fujii Y, Tanaka H. Preoperative oral granisetron for the prevention of vomiting strabismus surgery to prevent postoperative nausea and vomiting: a random-following paediatric surgery. Paediatr Anaesth 2002; 12 (3): 267-71 ized, controlled study. J AAPOS 2003; 7 (3): 210-2
77. Fujii Y, Tanaka H. Granisetron reduces post-operative vomiting in children: a 102. Gurkan Y, Kilickan L, Toker K. Propofol-nitrous oxide versus sevoflurane-nitrousdose-ranging study. Eur J Anaesth 1999; 16 (1): 62-5 oxide for strabismus surgery in children. Paediatr Anaesth 1999; 9 (6): 495-9
78. Fujii Y, Saitoh Y, Tanaka H, et al. Prevention of postoperative vomiting with 103. Standl T, Wilhelm S, von Knobelsdorff G, et al. Propofol reduces emesis aftergranisetron in paediatric patients with and without a history of motion sickness. sufentanil supplemented anaesthesia in paediatric squint surgery. Acta Anaes-Paediatr Anaesth 1999; 9 (6): 527-30 thesiol Scand 1996; 40 (6): 729-33
79. Fujii Y, Toyooka H, Tanaka H. Effective dose of granisetron for preventing 104. Eltzschig HK, Schroeder TH, Eissler BJ, et al. The effect of remifentanil orpostoperative emesis in children. Can J Anaesth 1996; 43 (7): 660-4 fentanyl on postoperative vomiting and pain in children undergoing strabismus
80. Cieslak GD, Watcha MF, Phillips MB, et al. The dose-response relation and cost- surgery. Anesth Analg 2002; 94 (5): 1173-7effectiveness of granisetron for the prophylaxis of pediatric postoperative 105. Pandit UA, Malviya S, Lewis IH. Vomiting after outpatient tonsillectomy andemesis. Anesthesiology 1996; 85 (5): 1076-85 adenoidectomy in children: the role of nitrous oxide. Anesth Analg 1995; 80
81. Kranke P, Apfel CC, Eberhart LH, et al. The influence of a dominating center on a (2): 230-3quantitative systemic review of granisetron for preventing postoperative nausea 106. Ved SA, Walden TL, Montana J, et al. Vomiting and recovery after outpatientand vomiting. Acta Anaesthesiol Scand 2001; 45: 659-70 tonsillectomy and adenoidectomy in children: comparison of four anesthetic
82. Kranke P, Apfel CC, Roewer N. Reported data on granisetron and postoperative techniques using nitrous oxide with halothane or propofol. Anesthesiologynausea and vomiting by Fujii, et al. are incredibly nice! Anesth Analg 2000; 90: 1996; 85 (1): 4-101004-7 107. Zestos MM, Carr AS, McAuliffe G, et al. Subhypnotic propofol does not treat
83. Gan TJ, Meyer T, Apfel CC, et al. Consensus guidelines for managing postopera- postoperative vomiting in children after adenotonsillectomy. Can J Anaesthtive nausea and vomiting. Anesth Analg 2003; 97: 62-71 1997; 44 (4): 401-4
84. Henzi I, Walder B, Tramer MR. Dexamethasone for the prevention of postopera- 108. Chhibber AK, Lustik SJ, Thakur R, et al. Effects of anticholinergics on postopera-tive nausea and vomiting: a quantitative systematic review. Anesth Analg 2000; tive vomiting, recovery and hospital stay in children undergoing tonsillectomy90 (1): 186-94 with or without adenoidectomy. Anesthesiology 1999; 90 (3): 697-700
85. Henzi I, Sonderegger J, Tramer MR. Efficacy, dose-response and adverse effects of 109. Welters ID, Menges T, Graf M, et al. Reduction of postoperative nausea anddroperidol for prevention of postoperative nausea and vomiting. Can J Anaesth vomiting by dimenhydrinate suppositories after strabismus surgery in children.2000; 47 (6): 537-51 Anesth Analg 2000; 90 (2): 311-4
86. Lischke V, Behne M, Doelken P, et al. Droperidol causes a dose-dependent 110. Schlager A, Mitterschiffthaler G, Puhringer F. Rectally administeredprolongation of the QT interval. Anesth Analg 1994; 79: 983-6 dimenhydrinate reduces postoperative vomiting in children after strabismus
surgery. Br J Anaesth 2000; 84 (3): 405-687. Gan TJ, White PF, Scuderi PE, et al. FDA ‘black box’ warning regarding use ofdroperidol for postoperative nausea and vomiting: is it justified? [letter]. 111. Vener DF, Carr AS, Sikich N, et al. Dimenhydrinate decreases vomiting afterAnesthesiology 2002; 97: 287 strabismus surgery in children. Anesth Analg 1996; 82 (4): 728-31
88. Stuth E, Stucke A, Cara J, et al. Droperidol for perioperative sedation causes a 112. Handa F, Fujii Y. The efficacy of oral clonidine premedication in the prevention oftransient prolongation of the QTc time in children under volatile anesthesia. postoperative vomiting in children following strabismus surgery. PaediatrPediatr Anesth 2004; 14: 831-7 Anaesth 2001; 11 (1): 71-4
89. Berry F. Droperidol: has it suffered a fatal wound? Pediatr Anesth 2004; 14: 807-9 113. Gulhas N, Turkoz A, Durmus M, et al. Oral clonidine premedication does notreduce postoperative vomiting in children undergoing strabismus surgery. Acta90. Chang N, Rappaport B. FDA alert: update on droperidol and the FDA [newsletter].Anaesthesiol Scand 2003; 47 (1): 90-3Am Soc Anesth Newsletter 2002; 66 (12): 25
91. Food and Drug Administration. MedWatch: the FDA safety and adverse event 114. Karlsson E, Larsson LE, Nilsson K. The effects of prophylactic dixyrazine onreporting program [online]. Available from URL: http://www.fda.gov/ postoperative vomiting after two different anaesthetic methods for squintmedwatch [Accessed 2007 Feb 2] surgery in children. Acta Anaesthesiol Scand 1993; 37 (1): 45-8
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

68 Kovac
115. Splinter W, Noel LP, Roberts D, et al. Antiemetic prophylaxis for strabismus 139. Splinter WM, Rhine EJ. Prophylaxis for vomiting by children after tonsillectomy:surgery. Can J Ophthalmol 1994; 29 (5): 224-6 ondansetron compared with perphenazine. Br J Anaesth 1998; 80 (2): 155-8
116. Tramer MR, Sansonetti A, Fuchs-Buder T, et al. Oculocardiac reflex and postoper- 140. Stene FN, Seay RE, Young LA, et al. Prospective, randomized, double-blind,ative vomiting in paediatric strabismus surgery: a randomised controlled trial placebo-controlled comparison of metoclopramide and ondansetron for preven-comparing four anaesthetic techniques. Acta Anaesthesiol Scand 1998; 42 (1): tion of post tonsillectomy or adenotonsillectomy emesis. J Clin Anesth 1996; 8117-23 (7): 540-4
117. Bowhay AR, May HA, Rudnicka AR, et al. A randomized controlled trial of the 141. Hamid SK, Selby IR, Sikich N, et al. Vomiting after adenotonsillectomy inantiemetic effect of three doses of ondansetron after strabismus surgery in children: a comparison of ondansetron, dimenhydrinate, and placebo. Anesthchildren. Paediatr Anaesth 2001; 11 (2): 215-21 Analg 1998; 86 (3): 496-500
118. Sadhasivam S, Shende D, Madan R. Prophylactic ondansetron in prevention of 142. Fujii Y, Saitoh Y, Kobayashi N. Prevention of vomiting after tonsillectomy inpostoperative nausea and vomiting following pediatric strabismus surgery: a children: granisetron versus ramosetron. Laryngoscope 2001; 111 (2): 255-8dose-response study. Anesthesiology 2000; 92 (4): 1035-42 143. Jensen AB, Chrinsiansen DB, Coulthard K, et al. Tropisetron reduces postoperative
119. Shende D, Bharti N, Kathirvel S, et al. Combination of droperidol and ondansetron vomiting in children undergoing tonsillectomy. Paediatr Anaesth 2000; 10 (1):reduces PONV after pediatric strabismus surgery more than single drug ther- 69-75apy. Acta Anaesthesiol Scand 2001; 45 (6): 756-60 144. Holt R, Rask P, Coulthard KP, et al. Tropisetron plus dexamethasone is more
120. Mendel HG, Guarnieri KM, Sundt LM, et al. The effects of ketorolac and fentanyl effective than tropisetron alone for the prevention of postoperative nausea andon postoperative vomiting and analgesic requirements in children undergoing vomiting in children undergoing tonsillectomy. Paediatr Anaesth 2000; 10 (2):strabismus surgery. Anesth Analg 1995; 80 (6): 1129-33 181-8
145. Moiniche S, Romsing J, Dahl JB, et al. Nonsteroidal antiinflammatory drugs and121. Kranke P, Morin AM, Roewer N, et al. Dimenhydrinate for prophylaxis ofthe risk of operative site bleeding after tonsillectomy: a quantitative systematicpostoperative nausea and vomiting: a meta-analysis of randomized controlledreview. Anesth Analg 2003; 96 (1): 68-77trials. Acta Anaesthesiol Scand 2002; 46 (3): 238-44
146. Courtman SP, Rawlings E, Carr AS. Masked bleeding post tonsillectomy with122. Madan R, Perumal T, Subramaniam K, et al. Effect of timing of ondansetronondansetron [letter]. Paediatr Anaesth 1999; 9 (5): 467administration on incidence of postoperative vomiting in paediatric strabismus
surgery. Anaesth Intensive Care 2000; 28 (1): 27-30 147. Steward DL, Welge JA, Myer CM. Steroids for improving recovery followingtonsillectomy in children. Cochrane Database of Systematic Reviews 2003; (1):123. Caron E, Bussieres JF, Lebel D, et al. Ondansetron for the prevention and treatmentCD003997of nausea and vomiting following pediatric strabismus surgery. Can J
Ophthalmol 2003; 38: 214-22 148. Shott SR. Tonsillectomy and postoperative vomiting: do steroids really work?Arch Otolaryngol Head Neck Surg 2001; 127 (8): 1009-10124. Splinter WM, Rhine EJ, Roberts DJ. Vomiting after strabismus surgery in children:
ondansetron vs propofol. Can J Anaesth 1997; 44 (8): 825-9 149. Aouad MT, Siddik SS, Rizk LB, et al. The effect of dexamethasone on postopera-tive vomiting after tonsillectomy. Anesth Analg 2001; 92 (3): 636-40125. Sennaraj B, Shende D, Sadhasivan S, et al. Management of post-strabismus nausea
and vomiting in children using ondansetron: a value-based comparison of 150. Pappas AL, Sukhani R, Hotaling AJ, et al. The effect of preoperative dex-outcomes. Br J Anaesth 2002; 89 (3): 473-8 amethasone on the immediate and delayed postoperative morbidity in children
undergoing adenotonsillectomy. Anesth Analg 1998; 87 (1): 57-61126. Munro HM, D’Errico CC, Lauder GR, et al. Oral granisetron for strabismussurgery in children. Can J Anaesth 1999; 46 (1): 45-8 151. Vosdoganis F, Baines DB. The effect of single dose intravenous dexamethasone in
tonsillectomy in children. Anaesth Intensive Care 1999; 27 (5): 489-92127. Fujii Y, Tanaka H, Ito M. Ramosetron compared with granisetron for the preven-tion of vomiting following strabismus surgery in children. Br J Ophthal 2001; 152. Andrews PLR, Davis CJ. The mechanism of emesis induced by anticancer thera-85 (6): 670-2 pies. In: Andrews PLR, Sanger GJ, editors. Emesis in anti-cancer therapy:
mechanisms and treatment. London: Chapman & Hall Medical, 1993: 113-61128. Splinter WM. Prevention of vomiting after strabismus surgery in children: dex-amethasone alone versus dexamethasone plus low-dose ondansetron. Paediatr 153. Steward DL, Welge JA, Myer CM. Do steroids reduce morbidity of tonsillectomy:Anaesth 2001; 11 (5): 591-5 meta-analysis of randomized trials. Laryngoscope 2001; 111 (10): 1712-8
129. Subramaniam B, Madan R, Sadhasivam S, et al. Dexamethasone is a cost-effective 154. Woods AJ, Andrews PLR. Cisplatin acutely reduces 5-hydroxytryptamine-inducedalternative to ondansetron in preventing PONV after paediatric strabismus vagal depolarization in the rat: protective action of dexamethasone. Eur Jrepair. Br J Anaesth 2001; 86 (1): 84-9 Pharmacol 1995; 278: 275-8
130. Kymer PJ, Brown Jr RE, Lawhorn CD, et al. The effects of oral droperidol versus 155. Wang JJ, Ho ST, Tzeng JI, et al. The effect of timing of dexamethasone administra-oral metoclopramide versus both oral droperidol and metoclopramide on post- tion on its efficacy as a prophylactic antiemetic for postoperative nausea andoperative vomiting when used as a premedicant for strabismus surgery. J Clin vomiting. Anesth Analg 2000; 91 (1): 136-9Anesth 1995; 7: 35-9 156. Neff SPW, Stapelberg E, Warmington A. Excruciating perineal pain after intrave-
131. Klockgether-Radke A, Neumann S, Neumann P, et al. Ondansetron, droperidol and nous dexamethasone. Anaesth Intensive Care 2002; 30: 370-1their combination for the prevention of post-operative vomiting in children. Eur 157. Perron G, Dolbec P, Germain J, et al. Perineal pruritus after i.v. dexamethasoneJ Anaesthesiol 1997; 14: 362-7 administration. Can J Anaesth 2003; 50: 749-50
132. Kathirvel S, Shende D, Madan R. Comparison of anti-emetic effects of ondanse- 158. van den Berg AA. A comparison of ondansetron and prochlorperazine for thetron, metoclopromide or a combination of both in children undergoing surgery prevention of nausea and vomiting after tympanoplasty. Can J Anaesth 1996;for strabismus. Eur J Anaesthesiol 1999; 16: 761-5 43 (9): 939-45
133. Fujii Y, Saitoh Y, Tanaka H, et al. Combination of granisetron and droperidol for 159. Woodward WM, Barker I, John RE, et al. Propofol infusion vs thiopentone/the prevention of vomiting after paediatric strabismus surgery. Paediatr Anaesth isoflurane anaesthesia for prominent ear correction in children. Paediatr1999; 9: 329-33 Anaesth 1997; 7 (5): 379-83
134. Bhardwaj N, Bala I, Kaur C, et al. Comparison of ondansetron with ondansetron 160. Gurler T, Celik N, Totan S, et al. Prophylactic use of ondansetron for emesis afterplus dexamethasone for antiemetic prophylaxis in children undergoing strabis- craniofacial operations in children. J Craniofac Surg 1999; 10 (1): 45-8mus surgery. J Pediatr Ophthalmol Strabismus 2004; 41: 100-4 161. Neufeld S. Pharmacology review: the role of ondansetron in the management of
135. Smith PV, Walton DS. Prevention of vomiting after general anesthesia for pediatric children’s nausea and vomiting following posterior fossa neurosurgical proce-ophthalmic surgery. AANA J 2001; 69 (1): 39-43 dures. Axone 2002; 23 (4): 24-9
136. Roberts RG, Jones RM. Paediatric tonsillectomy and PONV: big little problem 162. Darkow T, Gora-Harper ML, Goulson DT, et al. Impact of antiemetic selection onremains big! Anaesthesia 2002; 57 (6): 619-20 postoperative nausea and vomiting and patient satisfaction. Pharmacotherapy
137. Rose JB, Brenn BR, Corddry DH, et al. Preoperative oral ondansetron for pediatric 2001; 21 (5): 540-8tonsillectomy. Anesth Analg 1996; 82 (3): 558-62 163. Drake R, Anderson BJ, Persson MA, et al. Impact of an antiemetic protocol on
138. Splinter WM, Rhine EJ. Prophylactic antiemetics in children undergoing tonsillec- postoperative nausea and vomiting in children. Paediatr Anaesth 2001; 11 (1):tomy: high-dose vs low-dose ondansetron. Paediatr Anaesth 1997; 7 (2): 125-9 85-91
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)

Management of Postoperative Nausea and Vomiting in Children 69
164. De Negri PD, Ivani G. Management of postoperative nausea and vomiting in 172. Mathew PJ, Madan R, Subramaniam R, et al. Efficacy of low-dose dexamethasonechildren. Pediatr Drugs 2002; 4 (11): 717-28 for preventing postoperative nausea and vomiting following strabismus repair
165. Anonymous. ASHP therapeutic guidelines on the pharmacologic management of in children. Anaesth Intensive Care 2004; 32: 372-6nausea and vomiting in adult and pediatric patients receiving chemotherapy or
173. Madan R, Bhatia A, Chakithandy S, et al. Prophylactic dexamethasone for postop-radiation therapy or undergoing surgery. Am J Health Syst Pharm 1999; 56 (8):729-64 erative nausea and vomiting in pediatric strabismus surgery: a dose ranging and
166. Rose JB, Watcha MF. Postoperative nausea and vomiting in paediatric patients. Br safety evaluation study. Anesth Analg 2005; 100: 1622-6J Anaesth 1999; 83 (1): 104-17
174. Splinter W, Roberts DJ. Prophylaxis for vomiting by children after tonsillectomy:167. Gan TJ, Meyer T, Apfel CC, et al. Revised consensus guidelines: pediatric POV
dexamethasone versus perphenazine. Anesth Analg 1997; 85: 534-7[poster]. American Society of Anesthesiologists; 2006 Oct 14–18; Chicago (IL)168. Gan TJ, Meyer T, Apfel CC, et al. Revised PONV consensus guidelines [poster]. 175. Kranke P, Eberhart LH, Apfel CC, et al. Tropisetron for prevention of postopera-
American Society of Anesthesiologists; 2006 Oct 14–18; Chicago (IL) tive nausea and vomiting: a quantitative systematic review. Anaesthetist 2002;169. TJ Gan, Meyer TA. Revised consensus guidelines: management of postoperative
51: 805-14vomiting in pediatric patients [abstract no. A-971]. Anesthesiology 2006; 105:A971
170. TJ Gan, Meyer TA. Revised consensus guidelines [abstract no. A-565]. Anesthesi-Correspondence and offprints: Dr Anthony L. Kovac, Department of Anes-ology 2006; 105: A565
171. Tramer MR, Reynolds DJM, Moore RA, et al. Efficacy, dose-response, and safety thesiology, University of Kansas Medical Center, Mail Stop 1034, 3901of ondansetron in prevention of postoperative nausea and vomiting: a qualita-
Rainbow Boulevard, Kansas City, KS 66160, USA.tive systematic review of randomized placebo-controlled trials. Anesthesiology1997; 87: 1277-89 E-mail: [email protected]
2007 Adis Data Information BV. All rights reserved. Pediatr Drugs 2007; 9 (1)
