management of tibial plateau fractures - boolean education
TRANSCRIPT
MANAGEMENT
OF
TIBIAL PLATEAU
FRACTURES
RAJESH J. SAWARBANDHE
MANAGEMENT OF
TIBIAL PLATEAU FRACTURES
A
THESIS
FOR
M.Ch. ( ORTHOPAEDICS)
By
RAJESH J. SAWARBANDHE
UNIVERSITY OF SEYCHELLES
&
AMERICAN INSTITUTE OF MEDICINE ( USAIM)
2012
ACKNOWLEDGEMENT
I owe a great debt of gratiute to Dr. Anil Golhar,
M.S. (Ortho) , Hon. Professor & Head of the Department of
Orthopaedics, NKP Salve Medical College, Nagpur for his
valuable guidance & supervision in completing this work. It was
because of his suggestions & constant encouragement that I am
able to overcome my own shortcomings.
I am also thankful to Dr. Sushil Mankar, M.S. (
Ortho), Hon. Professor of Orthopaedics for his timely criticism
& overlasting help during the project.
I am also thankful to Dr. Ravi Bhajani, M.S. (
Ortho), Practicing in Nagpur for his guidance.
Rajesh J. Sawarbandhe
CONTENTS
S. No. Chapter Page No.
1. INTRODUCTION . . 1
2. HISTORICAL REVIEW . . 3
3. ANATOMY . . 6
4. REVIEW OF LITERATURE . . 13
5. MATERIAL AND METHODS . . 35
6. OBSERVATIONS . . 39
7. DISCUSSION . . 46
8. SUMMARY AND CONCLUSIONS . . 54
BIBLIOGRAPHY I to VII
INTRODUCTION
INTRODUCTION
The luxuries of our life in the present time is at the cost of rapidly
increasing industrialization, urbanization and mechanisation – so also the
traumatic cases are on increase. crowed cities, irregular traffic
arrangement, fast moving vehicles are the most important contributory
factors causing bony injuries, particularly polytrauma, comminuted
fractures and also the soft tissue injury. Tibial plateau fracture is one of
them.
Tibial plateau fractures have been studied and reported extensively
and exhaustively but still controversy exists over its management,
whether surgical or conservative. Excellent results have been published
in both groups. On one hand, we have got a group of surgeons who says
that most of the tibial plateau fractures [eighty-five percent] can be
managed by conservative treatment and on the other hand, other group
says conservative treatment means therapeutic nihilism and except for
undisplaced fracture every tibial plateau fracture should be operated upon
to achieve anatomical reduction and rigid internal fixation. Even
undisplaced tibial plateau fractures should be operated, so that early
mobilization of knee it is possible.
Before deciding the line of treatment one must bear in mind the
following facts :
1. Extent of damage in tibial plateau fracture is often greater than
what is seen on x-ray.
2. Malunion is exteremely common where as non-union is
unknown.
3. Painful knee and stiffness are the most serious and common
complications of the tibial plateau fracture.
In this small study, it is intended to outline the various principles of
management of tibial plateau fracture especially rigid fixation and to put
forward fresh clinical material to evaluate the results of surgical and
conservative methods.
HISTORICAL REVIEW
HISTORICAL REVIEW
Fractures of tibial condyles were brought into promience in 1929
by the papers of cotton F.J. Berg R. in Boston, and cubbins W.R., Seiffert
G. and coneley A.H., from chicago – mone calling them as fender
fracture and other as bumper fracture because they were often caused by
“automobile in contact with the jay walking citizens.”
Server J.W. had already reported three cases of fracture tibial
plateau in 1916 and discussed them again in 1922. During this time, most
of the fractures were treated by immobilization.
In 1940 Barr J.S. described the operative treatment of tibial plateau
fracture where depressed plateau is elevated by spike and supported by
cancellous bone grafts. This started a new era of operative intervention in
tibial plateau fractures, where anatomical reduction was thought to be
mandatory, so also support by variety of implants- [Foged J. 1943, palmer
I. 1951, jakobsen A. 1953, slee G. 1955, Turner V.C. 1959, Duparc J. and
ficate P. 1960, Courvoisier E. 1965, Fryjordet A. Jr. 1967].
During the same time, studies were carried out by many surgeons
by conservative approach and early mobilization of knee. In 1956, G.
Apley published the series of patients treated by skeletal traction and
early mobilization with excellent results. by this time, so many methods
of closed reduction and traction were published with excellent results.
[Inclan A. 1937, Dobelle M. 1941, Motz A.R., Householder R and
Depree J.K. 1943, Bagdley C.E. and o’connor S.J. 1952, Fyshe T.G.
1952, Lindholm R.V. 1954, Ilfeld F.W. and Hohl M. 1960 ].
In the meantime, different experimental studies were carried out.
Haldeman K.O. 1939, proved that hyaline cartilage is replaced by
fibrocartilage. Hohl M. 1956 proved that prolonged immobilization
leads to formation of intra-articular adhesions. Martin A.F. 1960 carried
out experimental study on dissected knee joints of cadevera and put
forward the machanism of injury. A.G. Apley, 1956, Hohl M. 1956,
Rasmussen P.S. 1973 put for ward the systeme of grading the results.
Moor T.M. and harvey J.P. [1974] deacribing the tibial plateau
view for measuring the exact depression of plateau. Fagerburg S. 1958,
Schioler G. [1971] and Elstrom j, panko vich Am, Sassoon H. of al
[1976] lauded the use of tomogram for the measurement of depression
and type of fracture. Many varieties of implants have been developed
and used to fix the plateau fracture.
Later AO [ASIF] described that the surgical treatment is mandatory
for tibial plateau fractures. Aim is to achieve anatomical reduction, rigid
internal fixation and early mobilization. They developed their own
contoured Buttress plates and DCP plates. AO PRINCIPLES for the
management of tibial plateau fracture have wide acceptance now a days.
Till the date, controversy still exists between the choice of the
treatment – conservative or surgical. But definitely trend is towards
operative treatment.
ANATOMY
ANATOMY
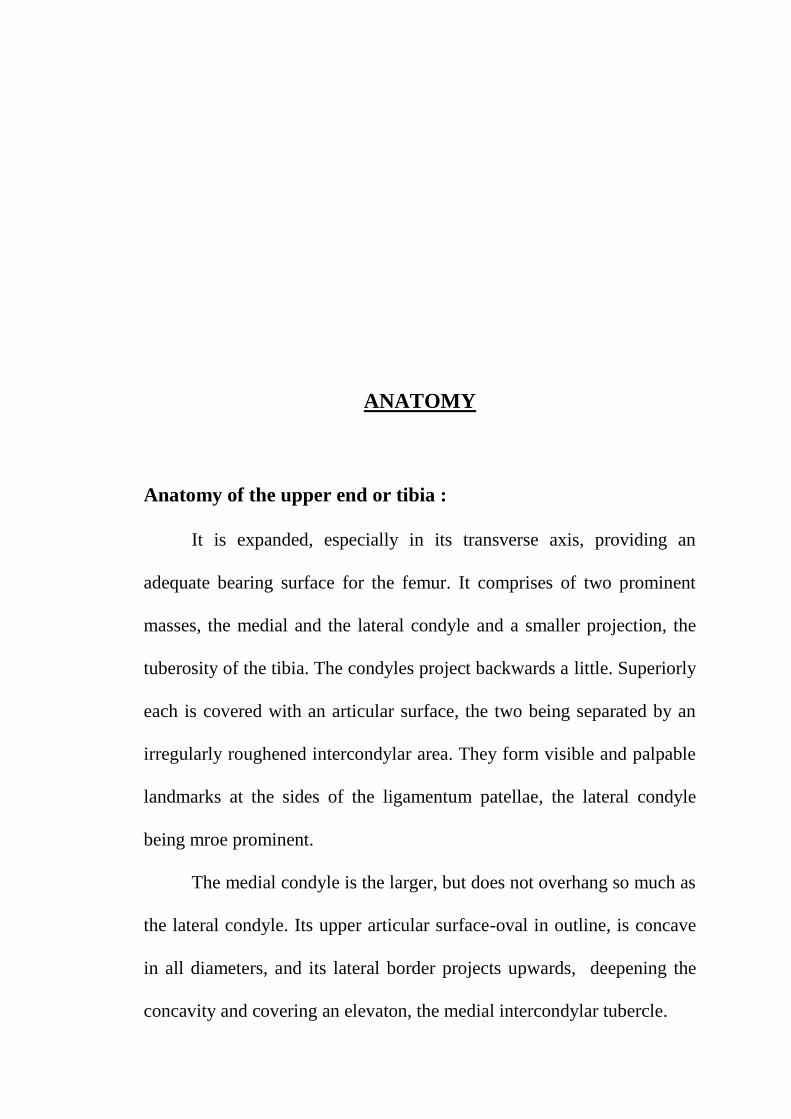
Anatomy of the upper end or tibia :
It is expanded, especially in its transverse axis, providing an
adequate bearing surface for the femur. It comprises of two prominent
masses, the medial and the lateral condyle and a smaller projection, the
tuberosity of the tibia. The condyles project backwards a little. Superiorly
each is covered with an articular surface, the two being separated by an
irregularly roughened intercondylar area. They form visible and palpable
landmarks at the sides of the ligamentum patellae, the lateral condyle
being mroe prominent.
The medial condyle is the larger, but does not overhang so much as
the lateral condyle. Its upper articular surface-oval in outline, is concave
in all diameters, and its lateral border projects upwards, deepening the
concavity and covering an elevaton, the medial intercondylar tubercle.
The posterior surface of the condyle is marked immediately below the
articular margin by a rough strip asperated from the medial surface of the
shaft by an inconspicuous ridge.
The lateral condyle overhange the shaft, especially at its
posterolateral part, which bears on its inferior surface a small circular
facet for articulation with an upper end of the fibula. The upper surface is
covered with an articular surface for the lateral condyle of the femur,
nearly circular in outline, it is slightly hollowed in its central part, and its
medial border extends upwards to the lateral intecondylar tubercle. The
anterior surfaces of the two condyles become continuous in front with the
tuberosity of the tibia.
The intercondylar area :
This area is a roughened area on the superior surface which
intervenes between the articular surfaces of the two condyles. It is
narrowest at its middle, where it is elevated into the intercondylar
eminence. The lateral and medial parts of the eminence project alightly
upwards, and constitute the lateral and medial intercondylar tubercles.
Both behind and in front of the eminence the intercondylar area becomes
wider, as the curved margine of the articular surfaces recede from each
other.
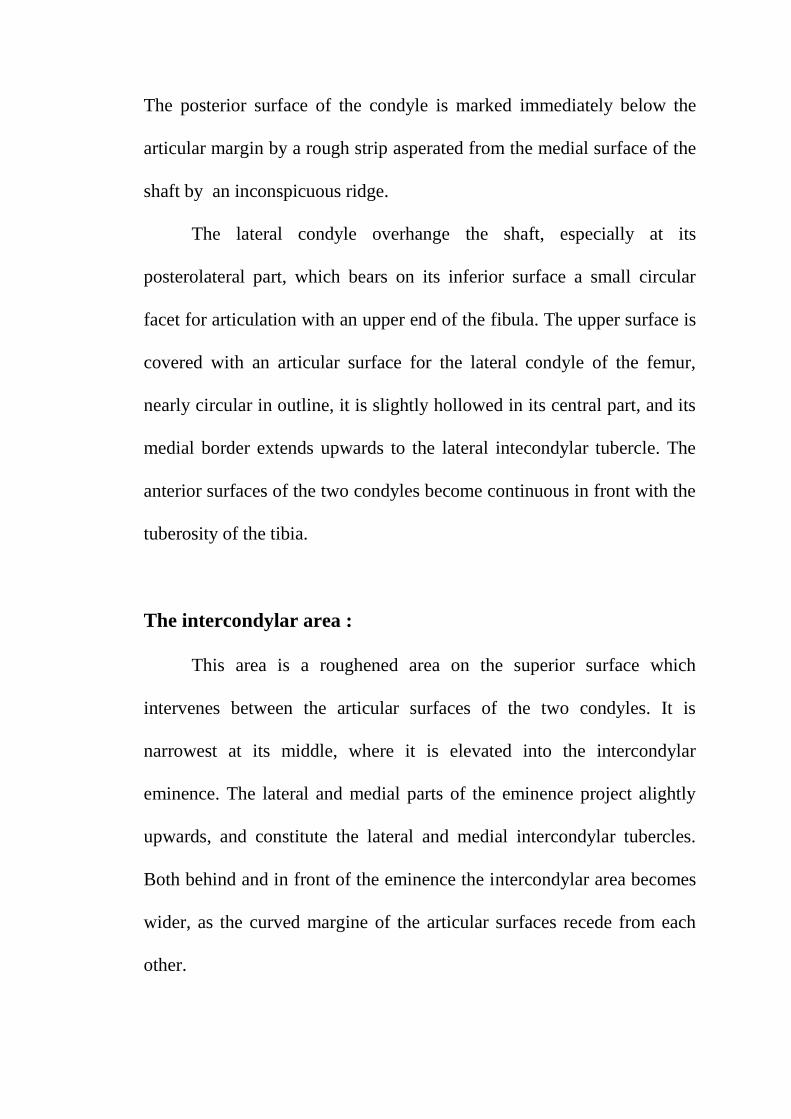
Knee Joint :
This joint occurs between the large, rounded condyles of the femur
and the much flattened condyles of the tibia. It is a midified syunovial
hinge type of joint. The knee joint is held together by a capsule that is
strengthened by the patellar ligament, and tibial and fibular collateral
ligaments; several intracapsular ligaments also aid in maintaining the
joint.
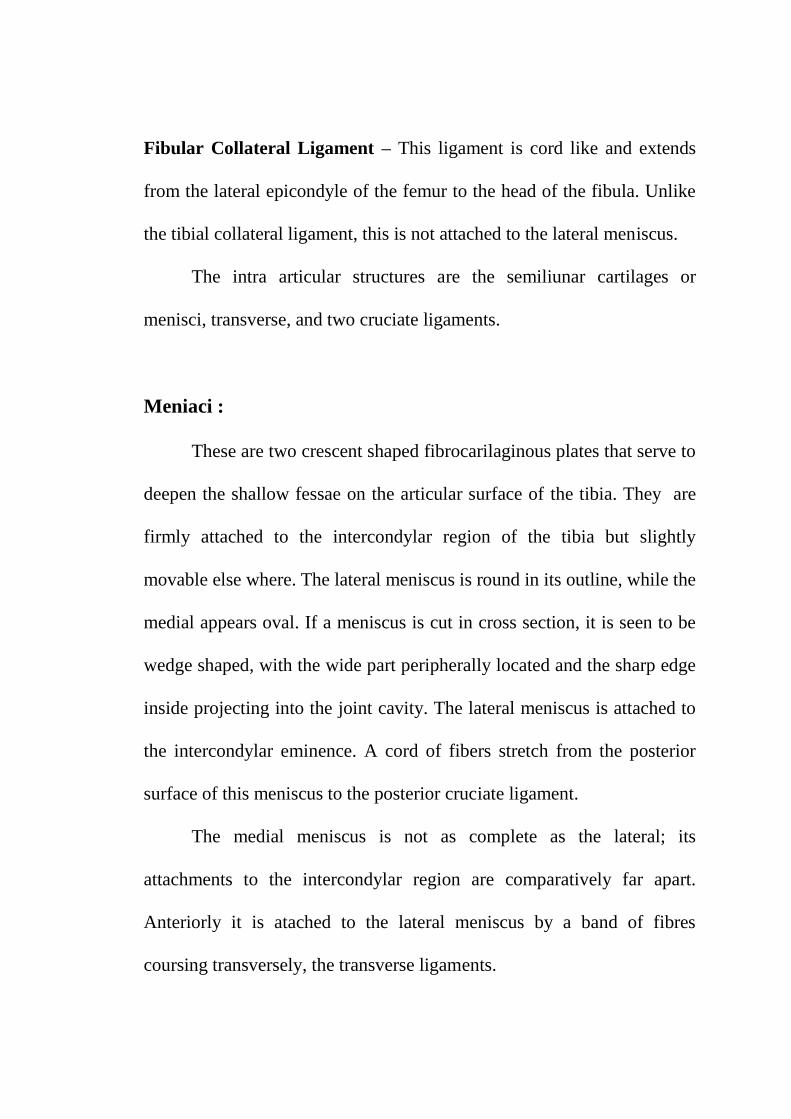
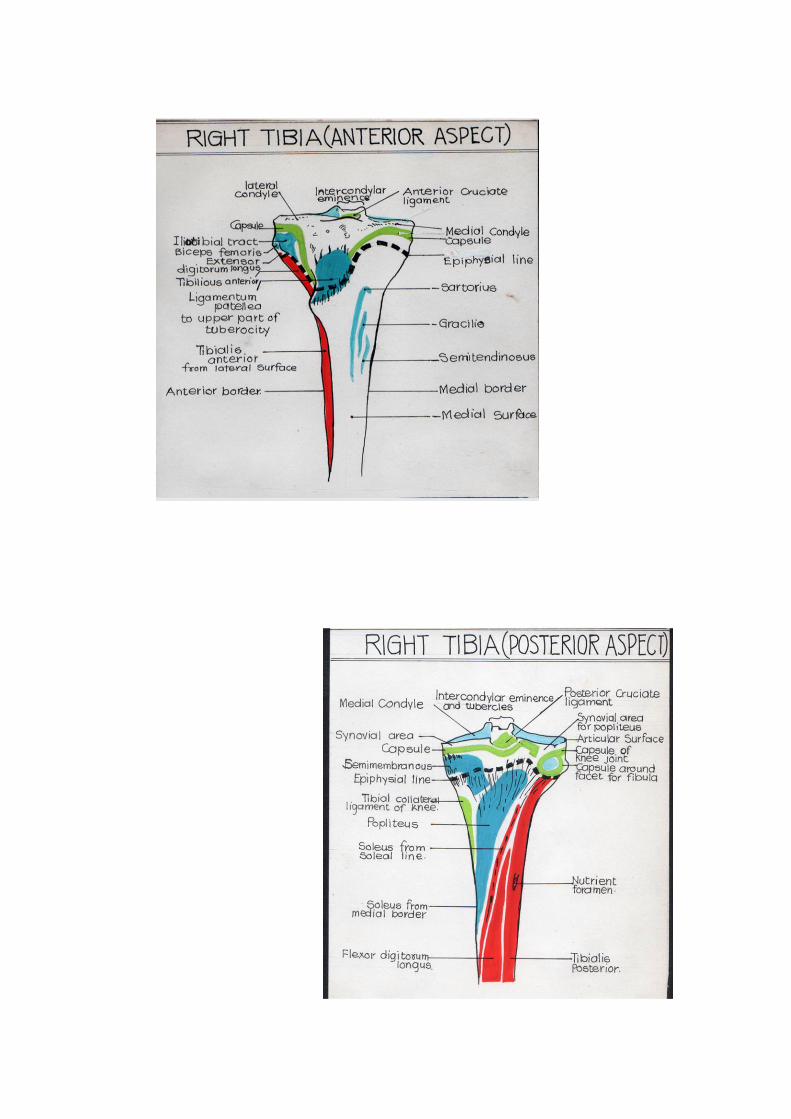
Capsule – The capsule completely surrounds the knee joint. Its
attachments to the femur area as follows. Anteriorly, the capsule is
attached to the arterior surface of the femur. Laterally, the capsule is
attached to the lines between the epicondyles and the condyles.
Posteriorly the superior edges of the rounded condyles serve as the line of
capsular attachment. The capsular attachments of the upper end of tibia is
shown in the diagram.
Patellar Ligament – The quadriceps tendon, the patella, and the patellar
ligament form the anterior wall of the knee joint. Lateral expansions from
the quadriceps tendon (retinaculi) blend with the capsular ligament.
Tibial Collateral Ligament – This thin band of ½ “ in width extends
from the medial epicondyule of the femur to the side of the tibia. It is
attached to the medial meniscus.
Fibular Collateral Ligament – This ligament is cord like and extends
from the lateral epicondyle of the femur to the head of the fibula. Unlike
the tibial collateral ligament, this is not attached to the lateral meniscus.
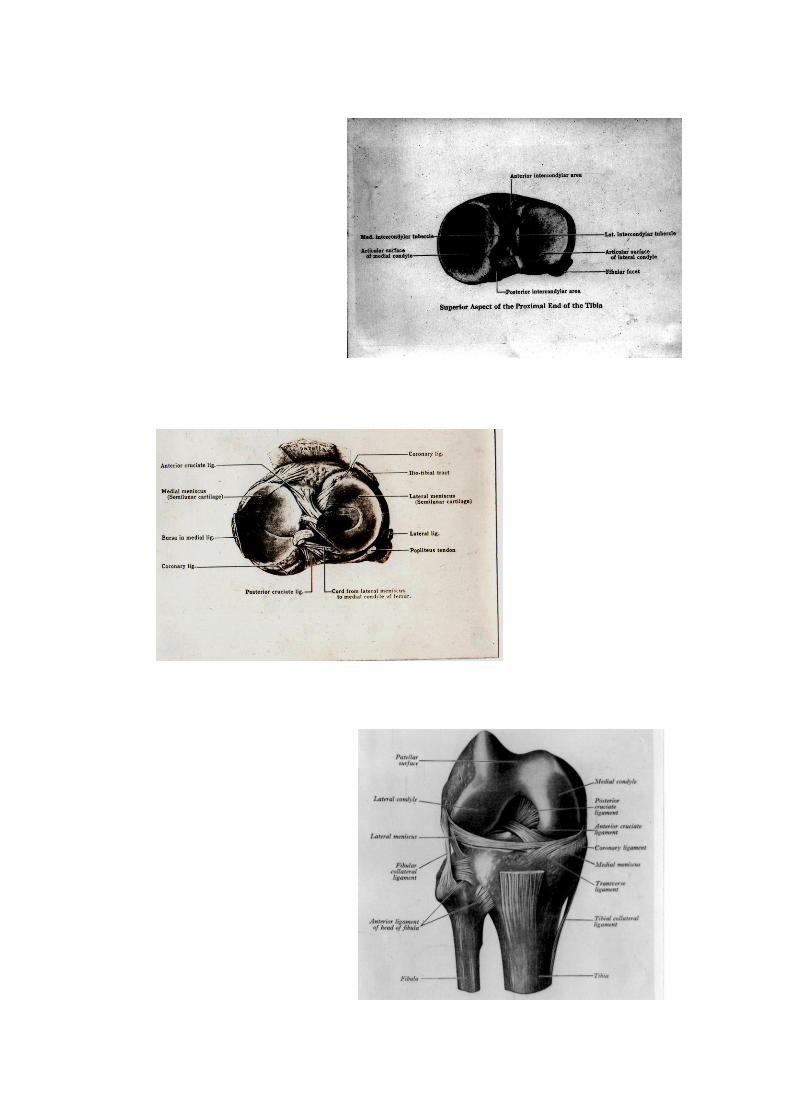
The intra articular structures are the semiliunar cartilages or
menisci, transverse, and two cruciate ligaments.
Meniaci :
These are two crescent shaped fibrocarilaginous plates that serve to
deepen the shallow fessae on the articular surface of the tibia. They are
firmly attached to the intercondylar region of the tibia but slightly
movable else where. The lateral meniscus is round in its outline, while the
medial appears oval. If a meniscus is cut in cross section, it is seen to be
wedge shaped, with the wide part peripherally located and the sharp edge
inside projecting into the joint cavity. The lateral meniscus is attached to
the intercondylar eminence. A cord of fibers stretch from the posterior
surface of this meniscus to the posterior cruciate ligament.
The medial meniscus is not as complete as the lateral; its
attachments to the intercondylar region are comparatively far apart.
Anteriorly it is atached to the lateral meniscus by a band of fibres
coursing transversely, the transverse ligaments.
Cruciate Ligaments :
These important ligaments are actually hold the femur and tibia
together and the name is derived from the fact that they across one
another. The anterior cruciate ligament arises from the anterior
intercondylar region of the tibia, and courses posteriorly and laterally to
attach to the posterior end of the lateral condyle of the femur on its
medial surface. This ligament become tense in extension of the joint,
prevents overextension, and is thought to induced the medial rotation
needed to lock the knee joint. The posterior cruciate ligament arises from
the psoterior part of the intercondylar region of the tibia, courses
superiorly in an anterior and medial direction to reach the medial condyle
and is atached to its lateral surface. This ligament becomes tense in
flexion of the joint and prevent overflexion, and may be involved in
locking the joint.
The knee joint is strengthened by various muscles that surround it.
They are the quadriceps femoris anteriorly; the biceps femoris laterally,
the sartorius, semitendinosus, and gracilis muscles medially and the
popliteus, gastrocnemius, semimembranosus, and plataris muscles
posteriorly.
The geometrical features of the knee joint cannot be appreciated
from standard anteroposterior and lateral x-ray and has been well studied
from specimens of amputed limb. The combined transverse diameters of
articular surface of femoral condyles is less anterior than posteriorly,
where condyles spread on each side of the intercondyular notch.
Therefore, in flexed position of knee, the posterior flared position of
femoral condyle is directed above tibial plateau and when knee is
extended, the narrower wedge shaped anterior surface of the femoral
condyle is opposed to the upper end of tibia. Viewed from the front , the
flexed knee resembles a flanged wheel rolling on the track. In extension,
femoral condyle comes like a bumper against the anterior margin of both
the menisci and the tibial condyles beneath.
The screwhome phenomena where by femur is internally rotated on
the tibia takes place in the last few degrees of extension. Because of this
internal rotation of femur and the juxtaposition of the narrowed anterior
part of the lateral femoral condyle to lateral tibial condyle when the knee
is extended , a substantial portion of the upper articular surface of the
lateral tibial plateau is left uncovered.
A routine x-ray shows (lateral view) a difference in the contours of
the femoral condyles, one is round from anterior to posterior while other
is flattened in its anterior quadrant. Examination of amputated specimens
reveal that the medial femoral condyle is uniformly semicircular in
contour. The upper surface of the lateral tibial plateau is uniformly
convex upward when seen from lateral aspect. The convexity is not
distinct on lateral x-ray. The tibial plateau is usually considered concave
on the AP x-ray. In reality it is saddle shaped facet, convex in sagital
plane and concave in coronal plane.
Normally the axial weight bearing thrust on the knee passess
thorugh the medial compartment of knee joint. This is reflected by the
trabecular pattern of the cancellous bone in the tibial condyle. In a
coronal section through the upper end of tibia, vertical trabeculations can
be seen extending from the medial cortex of the metaphysis upward to the
medial plateau. Beneath the articular surface here, there are intersecting
transverse trabeculae. The longitudinal trabeculae which extend from the
lateral cortex of the tibial metaphysis upward towards lateral tibial
plateau are less dense. The transverse trabeculae immediately beneath the
articular surface of the lateral tibial plateau are similarly thin. This subtle
but distinct difference is commonly visible on routine AP x-ray of upper
end of tibia and is an indication of the reactive vulnerability of lateral
tibial plateau to injury.
REVIEW OF LITERATURE
REVIEW OF LITERATURE
A] Mechanism of Injury :
Cotton F.J. and Berg R. (1929) considered it to be caused by the
fender of the automobile striking the extended leg of the “Jay Walking
citizens”. This was supported by Klin R. (1934).
According to Graham Apley (1956), when a straight Knee is
subjected to an abduction or valgus strain, the medial ligament may tear
or lateral tibial plateau may fracture. This view was also suggested by
Cubbins W.R., Conley A.H. and Callahan J. (1934). Later on Wilson W.J.
and Jacob J.E. (1952), Goylling U. and Lindholm R. (1953) suggested
that when the abduction force is combined with compression force,
fracture of tibial plateau may occur and this is the common mechanism.
Experimental study of Kennedy J.C. (1968) shows that forced abduction
and compression are necessary for the production of condyle fracture.
Forced abduction may cause external margin of the lateral femoral
condyle to press against the lateral tibial plateau. The levarge of the
femur acts on the plateau against the tensile strength of medial collateral
ligament and anterior cruciate ligament. Should the load on lever exceed
the tensile strength of tissue, the lesion may be a fracture or a ligament
injury or both. Forced vertical compression as in a fall from height
produce characteristic fracture configuration, usually T or T type. Pure
valgus or varus force tend to cause ligament tearing injuries rather than
fracture but when body weight is on the knee (axial compression) various
types of fracture configuration can occur. Twisting type of force can also
cause variety of fractures (Hymbert R. 1939).
According to Hohl M. and Robert Larson (1975) location and to
some extent the amount of depression in a fracture depends upon the
flexion angle of the knee at the moment of injury. With the knee in full
extension, the compression force is exerted anteriorly on the tibial
condyle. However, with knee in flexion, there is no such restrain on the
extent of compression, the medial or posterior part is usually involved.
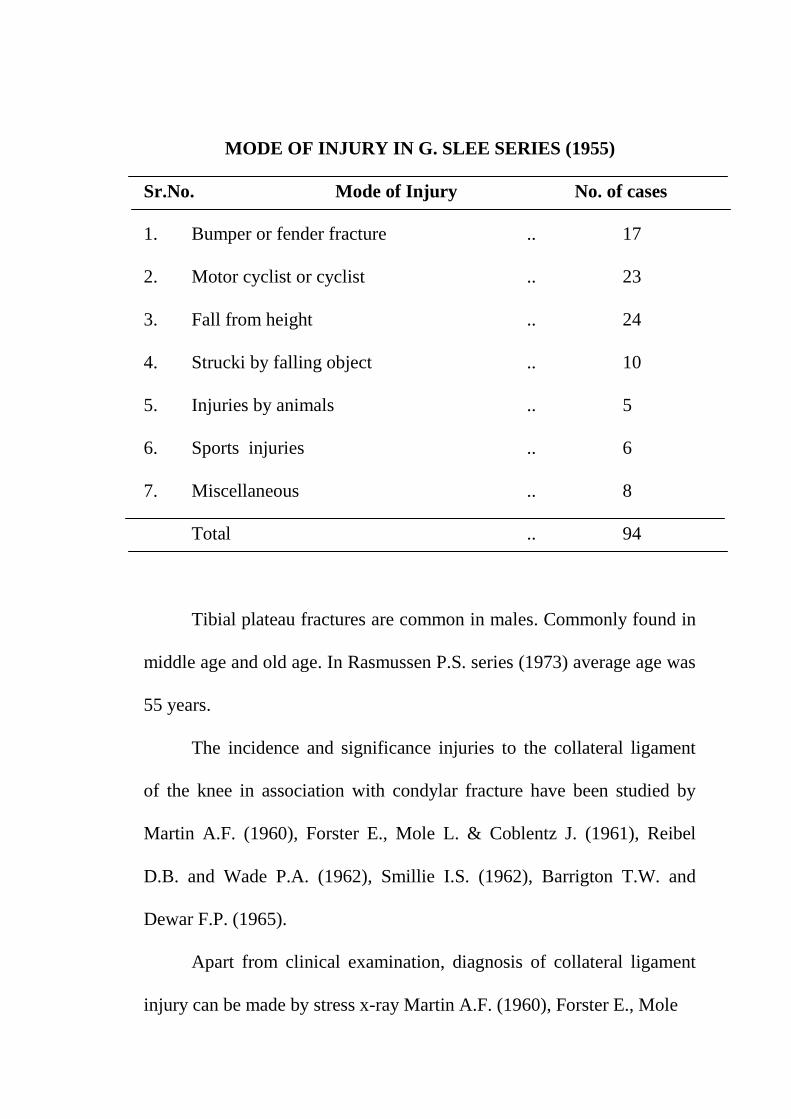
MODE OF INJURY IN G. SLEE SERIES (1955)
Sr.No. Mode of Injury No. of cases
1. Bumper or fender fracture .. 17
2. Motor cyclist or cyclist .. 23
3. Fall from height .. 24
4. Strucki by falling object .. 10
5. Injuries by animals .. 5
6. Sports injuries .. 6
7. Miscellaneous .. 8
Total .. 94
Tibial plateau fractures are common in males. Commonly found in
middle age and old age. In Rasmussen P.S. series (1973) average age was
55 years.
The incidence and significance injuries to the collateral ligament
of the knee in association with condylar fracture have been studied by
Martin A.F. (1960), Forster E., Mole L. & Coblentz J. (1961), Reibel
D.B. and Wade P.A. (1962), Smillie I.S. (1962), Barrigton T.W. and
Dewar F.P. (1965).
Apart from clinical examination, diagnosis of collateral ligament
injury can be made by stress x-ray Martin A.F. (1960), Forster E., Mole
L. and Coblentz J. (1961) and Hohl M. (1967), Diagnosis can also be
made by examining the patient under anaesthesia. Recently arthroscopy is
also used for diagnosis of ligamental injuries in tibial plateau fracture
(Reiner M.J. 1982.)
J.C. Kennedy and W.H. Bailey (1968) in their experimental study
found only two specimens of ligamental injury. Graham Apley (1978)
said – bone gives way before excessive stress is placed upon the
ligament, that is why ligamental injury is less common than what is often
supposed. Angular, torsional and shearing forces which produce
disruption of the tibial condyle may avulse corresponding meniscus from
peripheral attachment or may tear its substance. (Bradford C.H., Kilfoyle
R.M> and Kellener J.J. (1950), Hohl M. and Luck J.V. (1956) and Wolf
M.D. & While E.H. (1963)].
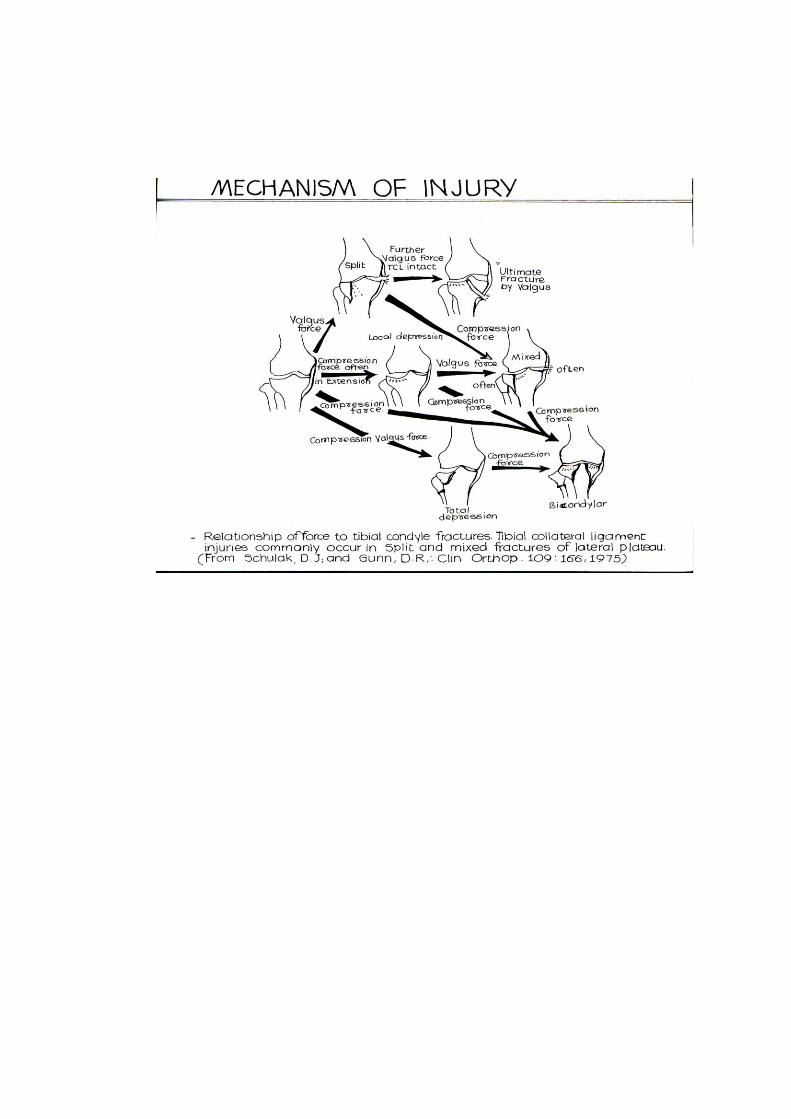
The mechanism of ligamental injury in tibial plateau fracture is
already discussed in previous section and also shown in opposite
diagram. Early diagnosis and treatment of ligamental as well as meniscal
injury should be carried out so as to prevent instability
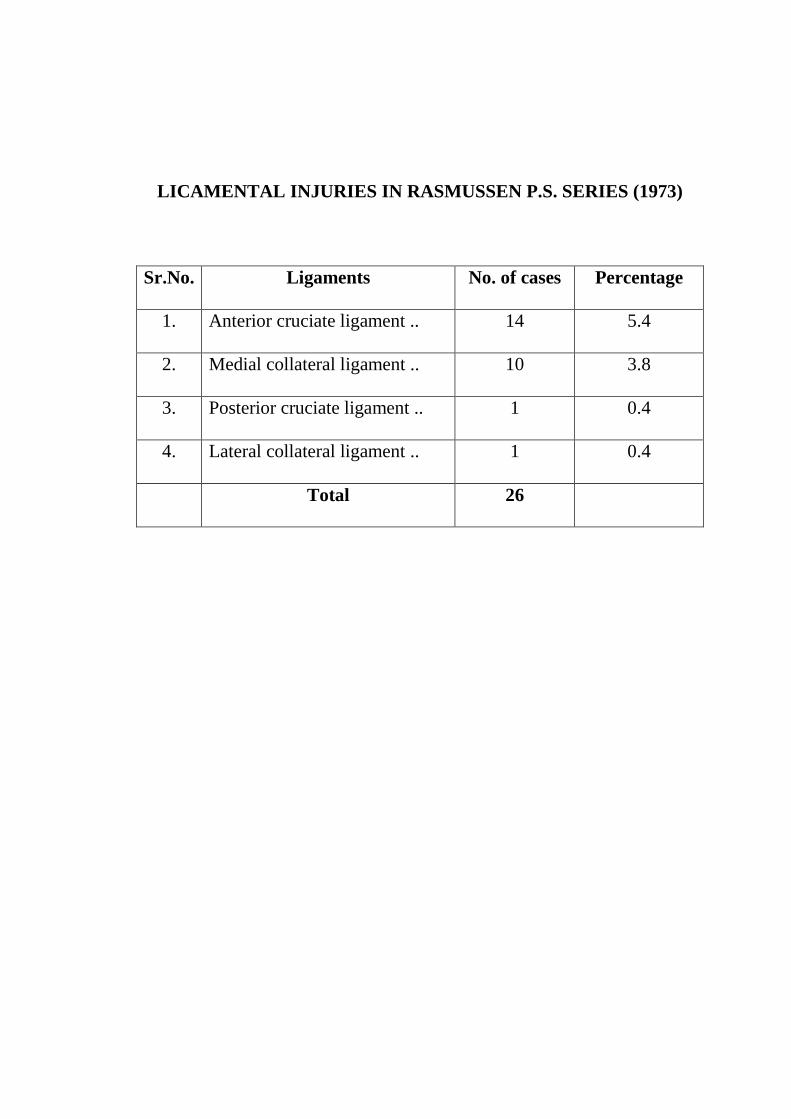
LICAMENTAL INJURIES IN RASMUSSEN P.S. SERIES (1973)
Sr.No. Ligaments No. of cases Percentage
1. Anterior cruciate ligament .. 14 5.4
2. Medial collateral ligament .. 10 3.8
3. Posterior cruciate ligament .. 1 0.4
4. Lateral collateral ligament .. 1 0.4
Total 26
B] CLASSIFICATION OF FRACTURES :
Many classifications have been put forward from time to time. Aim
of classification should be its practical utility for carrying out treatment
and prognosis.
a) Knight’s classification (1945) :
Type – I Lateral Condyle
a) Depression of the entries condyle is often associated with
a fracture of the neck of fibula. Complete tearing of the
collateral and cruciate ligament or avulsions of the tibial
attachment of the lateral condyle may also occur.
b) Lateral displacement of the rim of the tibial plateau with
depression and comminution of the central part of
condyle. This may be associated with ligamental injury.
Type – II Medial condyle
Depression of medial condyle is usually without
displacement of peripheral rim.
Type-III Inverted `T’ fracture of both condyles
a) Communited crushing fracture of entire plateau.
b) More severe fracture of one condyle than the other.
b) Watson – Jone’s classification (1955)
Type – I Depressed fracture
Without comminution
Without injury to articular surface
With displacement of fragment.
Type-II Comminuted fracture with separation of the margical
fragment. Often, there is severe injury to the articular
surface with displacement of fracture. It may be
associated with ligamental injury.
Gerald C. Slee’s Classification (1955)
Type – I Split fracture
There is a common type of fracture. The lateral edge of the lateral
femoral condyle is driven down into the articular surface of the
lateral tibial condyle causing a wedge shaped fragment of varying
size to become split off and is displaced outward. There is seldom
downward displacement of lateral fragment. Fracture is associated
with sprain of the medial ligament of varying severity. Similarly
the fracture of medial condyle with sprain of lateral ligament may
occur.
Type-II Compression fracture
Displacement caused by this injury ranges from depression of
anterior, posterior, lateral or medial part of the plateau with
comminution of the area to depression of whole condyle. Fracture
line from the non articular region of the tibial spine to the base of
the condyle and may be associated with the fracture of neck of
fibula. It is usually associated with collateral and anterior cruciate
ligament injury.
Type-III T or Y Shaped fracture
a) Both the condyles are fractured and displacement
outward and downward as one fragment. Their
particular surface appear to be undamaged.
b) Both the condyles fracture and displaced outward and
shows the features of compression.
d) Graham Apley’s classification (1956)
Type – I Linear fracture – vertical/ oblique
split or comminution – 1
Type – II Displaced fracture
- Slight displacement With or without
- Severe displacement Comminution
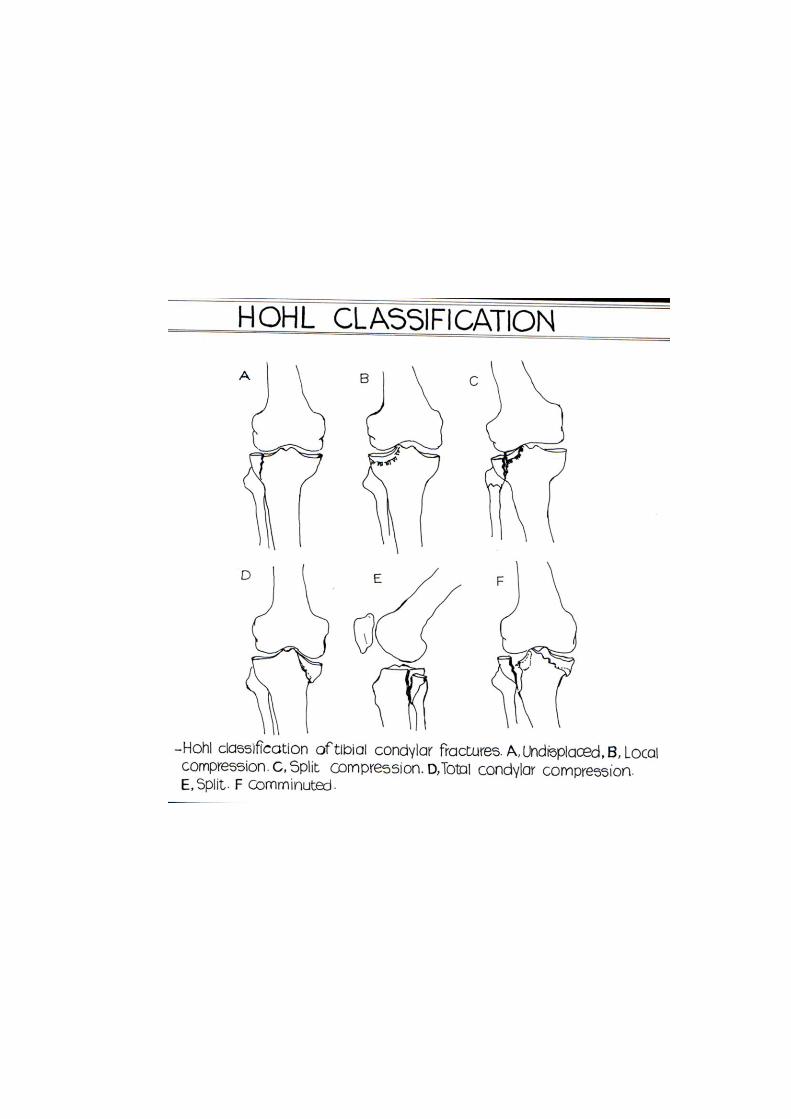
e) Hohl’s classification (1967)
This classification is excellent and provide a guide to optimum
treatment. Each type has got characteristic roetengenographic
features, problems, management and prognosis.
Type-I - Undisplaced fracture .. 24%
Type – II - Displaced fracture .. 76%
1. Local depession – Central depression .. 26%
– Split depression .. 26%
2. Total depression .. 11%
3. Split fracture .. 3%
4. Comminuted upper end of tibia .. 10%
f) John Robert’s classification (1968)
Type – I Non displaced fractures. A linear fracture may involve
the medial or lateral or both condyles. There is little or no
displacement. Fracture may be comminuted but still placed in this
group as the general contour of the surface of the tibial plateau is
undisturbed.. Fibula is usually intant.
Type – II Local depression type – For anatomical reasons this
fracture can occur only in lateral tibial plateau. There is a
circumscribed area of subchondral comminution or depression. The
mosaic like area of involvement lies in the anterior or central
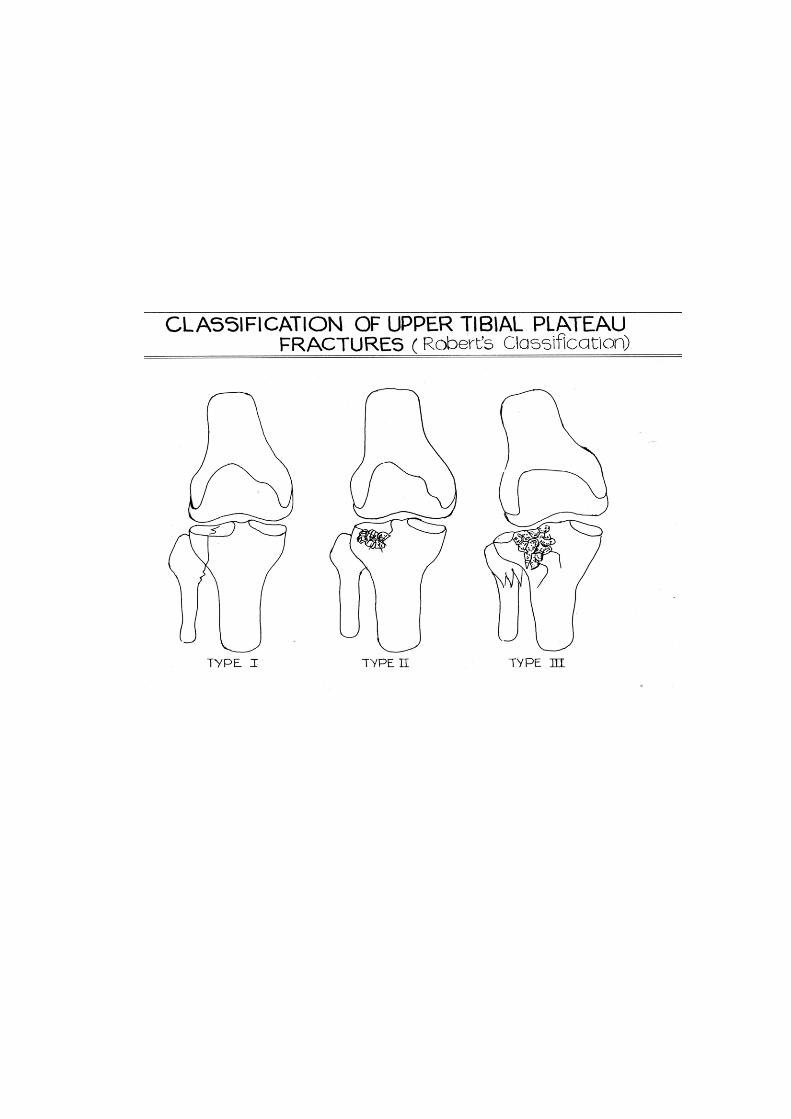
portion of the lateral plateau. The peripheral rim and posterior
portion are intact. Proximal end of fibula is intact. Less commonly,
the depression fragment remains at or near the normal joint level.
Less commonly the depressed portion is confined to the posterior
quadrant of the plateau when knee was fixed at the time of injury
but fracture still classified as Type-II, if the stability of the joint is
maintained by intact or lateral fragment.
Type – III Significant displacement of peripheral fragment and
gross disruption of the articular surfaces are present. The knee joint
is rendered unstable because the peripheral portion is displaced
either literally or distally from its normal relation, to the
corresponding femoral condyle. Associated fracture of the
proximal part part of the fibula is commonly present.
g) John Kennedy & Bailey W.H. (1968) classification
Type – I - Abduction fracture
- Central
- Rim
- Complete Condylar
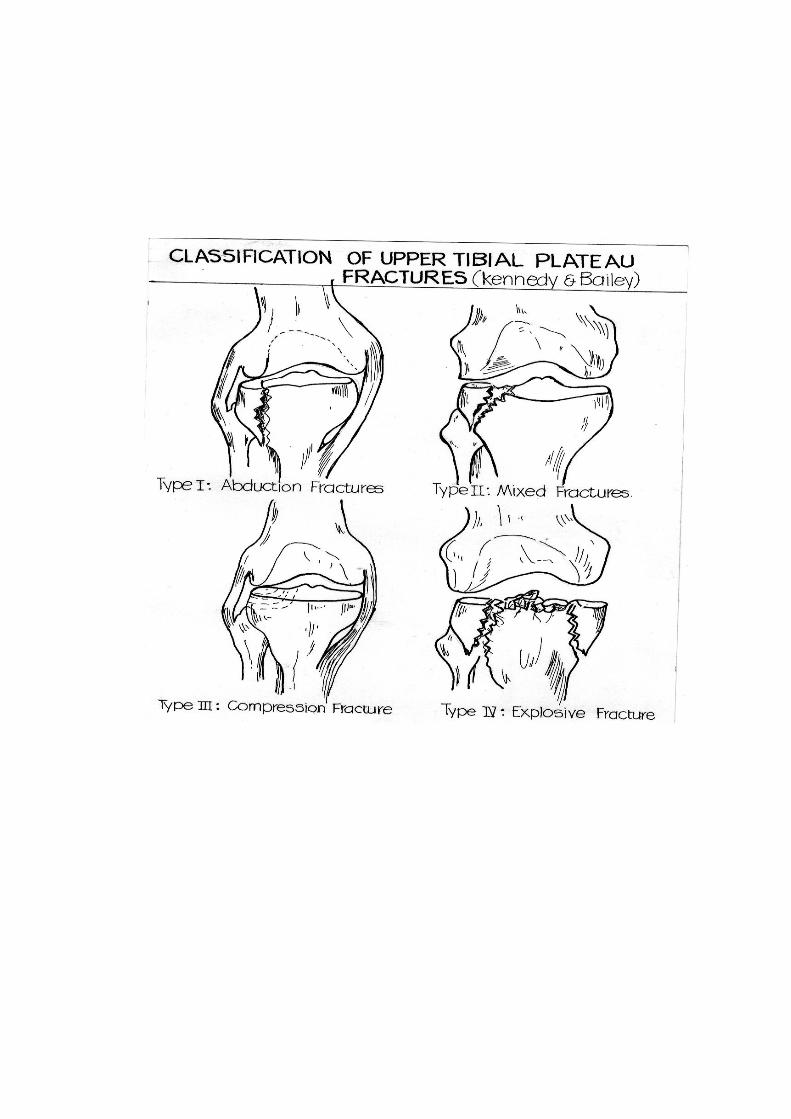
Type – II - Compression fracture : Central
Lateral
Anterior
Posterior
Type-III - Abduction and compression,
Type – IV - Explosive (T or Y type )
h) AO classification (Muller, M.E. , Allgower M. and
Willenegger H., (1970)]
Type – I - Pure wedge fracture : These are relatively rare and
occur most commonly laterally or posteriorly. If they occur
medially, then they give rise to a corresponding varus
deformity. The fracture plane is either in the frontal or sagittal
plane.
Type - II - Pure depression fracture : The result of valgus
overload. The lateral tibial plateau is pushed in by the lateral
femoral condyle. The plateau itself is not widened.
Type - III - Combination of types I and II with joint
depression and fracture of the lateral cortex. on the AP
projection, the plateau always appears widened. In the lateral
projection the anterior or posterior part of the articular surface is
either intact or depressed.
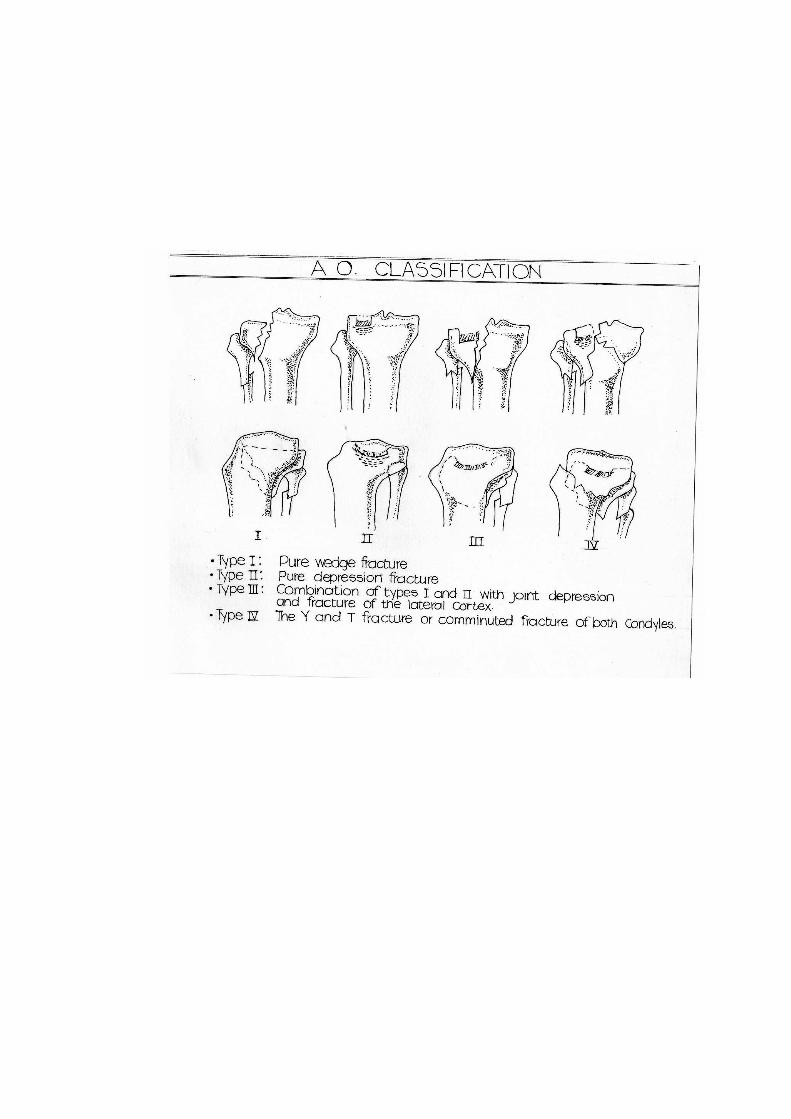
Type - IV – The Y and T fractures or comminuted fractures of
botrh condyles at times associated with fractures of the
intercondylar eminence. The lateral plateau is usually the more
severely damaged.
As far as anatomical distribution of tibial plateau fracture is
concerned lateral condyl is most commonly affected followed by
bicondylar fracture and lastly medial condyle.
Following table shows distribution of freactures in Rasmussen P.S.
Series (1973).
Condyle No. of cases Percentage
Lateral .. 183 70%
Medial .. 29 12%
Bicondylar .. 48 18%
Total .. 260 100%
Investigations :
Roetengenography is the most important investigation for
diagnosis of tibial plateau fracture. Antero posterior, lateral and oblique
views are sufficient to locate the site and type of fracture.
Stress x – rays give adequate clue of ligamental injury. Increase in
joint space more than one mm., when compared to the normal knee is
suggestive of ligamental injury. (Forster E., Mole L. and Coblentz J.
(1961), Hohl M. (1967)] Moor T.M. and Harvey J.P. Jr. (1974) the
method of taking tibial plateau view where AP view is taken with the
central ray directed at an angle of 105o to tibial crest. It permits accurate
measurement of tibial plateau depression.
Fagerburg S. (1958), Schioler G. (1971), Elstrom J. Pancovich Am,
Sasoon H. et. al . (1976) lauded the use of tomogram and showed that
displacement is often grossly underestimated on standard x-ray views and
that depression upon 7.5 mm. may pass unnoticed. Most striking failure
in examining plain x-ray is inability to distinguish clearly between the
mixed fractures. The value of tomogram in classifying fractures of tibial
plateau and in assessing the extent of fracture displacement and
depression is evident, from the following table.
Type of fractures
I II III IV Total
Plain x- ray 1 5 11 4 21
Tomogram 8 3 4 6 21
Verification at surgery 7 2 2 2 13
Recently arthroscopy has been used to examine the ligamental
injuries in tibial plateau fracture. [Reiner M.J. (1982).
TREATMENT :
Historically, the treatment part of tibial plateau fracture can be
divided into 3 phases. In the early days, immobilization was though to the
mandatory along with reduction of fracture. (Severe J.W. 1916, Cotton J.
and Berg R. 1929, Klin R. 1934, Perking G. 1940, Dobelle M. 1941,
Maisel B. and Cornell N.W. 1948, Dikson J. 1937, Fyshe T.G. 1952].
The second phase was of early active knee mobilization. [Badgley
C.E. and O’connor S.J. 1952, Fairbank T.J. 1955, Apley A.G. 1956, Hohl
M. and Luck J.V. 1956, Borrows H. 1956, Ilfeld F.W. and Hohl M. 1960,
Barrigton T.W. and Dewar F.P. 1965).
The last phase which has a wide acceptance nowadays is the
surgical treatment i.e. open reduction, internal fixation and early
mobilization [Foged J. 1943, Palmar I. 1951, Wilson W.J. and Jacob J.E.
1952, Jakobsen A. 1953, Slee G. 1955, Lee H. 1957, Dupare J. and Ficate
P. 1960, Rombold Charles 1960-, Courvoisier E. 1965, Fryjordet A. Jr.
1967, Muller M.E., Allgower M. and Willenegger H. 1970, Kennedy
W.R. 1978, Clyton Perry, Lawerence G. Evans, Semrile et.al. 1984].
Still the treatment of tibial plateau fracture is controversial.
Surgeon must choose that method or combination of methods best suited
to the clinical situation basing the choice on the reasonable demands of
the patient as well as medical condition, age, physical capability, on his
own professional experience and facilities available to him [Heppenstal
R.B. (1979).
The treatment of all types of intra-articular fractures aim at
restoration of normal joint function and preservation of late post-
traumatic osteoparthritis. Permanent or progressive disability in the knee
is caused by instability, angular deformity, restricted movement and pain.
(Hohl M. and Luck J.V. 1956).
The extent of damage in the tibial plateau fracture is often greater
than indicated by roetengenography, yet paradoxically patient frequently
does well than one prognosticate (Rombold Charles 1960).
Haldman K.O. (1939) studied the healing of intra-articular cartilage
and concluded that normal hyaline cartilage is replaced by fibrocartilage.
Healing of osteocarticular fracture was studied by Hohl M. and Luck J.V.
in 1956 on rhesus monkey and concluded that immobilization in
osteoarticular fracture for a long time will result in formation of
intraarticular adhesions and stiff knee.
In the initial days, immobilization was thought to be mandatory
during this time preferred regime was reduction with immobilization in
plaster. The force of manipulation can be augmented by using traction
table and compression claimp. (Watson J. 1955).
Inclan A. (1937) introduced a different method of treatment called
traction, compression and reduction.’ Hereunder anaesthesia heavy
skeletal traction is applied and compression is given at fracture site by
Esmarch bandage. If reduction is not achieved padded mallet is used to
press the displacedd fragment. Fyshe T.G. (1952) treated the patients with
immobilization in stader splint. Metz A.R., Householder R. and Depree
J.F. (1943) used larged pressure tonge maintain the reduction of fragment
with good results.
A.G. Apley 1956 published the results of conservative treatment
i.e. by putting a steinman pin two inch below the fracture, attempt to
reduce the fracture by traction and compression at fracture site. From next
day active knee bending exercises are given. Traction is continued for six
weeks. Excellent results were obtained. According to Hohl M. and Luck
J.V. (1967) tibial plateau fracture having depression less than five mm.
can be manged well by conservative treatment i.e. skeletal traction and
early knee bending exercises. Rusmusson (1973) used to treat most of the
patients conservatively except those having lateral instability (varus or
valgus more than 10o in extended position) y closed reduction and skeletal
traction or only skeletal traction. Recently Dennis Drennam and F.
Locher (1979) published the series of tibial platea fracture where patients
were treated by reduction followed by moulded hip spica with good
results. Eighty five percent of patients had good results.
RESULT OF FEW SERIES OF CONSERVATION TREATMENT
Sr.
No.
Author No. of
Cases
Excellent Good Fair Poor
1. Parey O. (1952) 22 11 - 8 3
2. Goylling and
Lindholm (1953)
47 6 25 13 3
3. Jakobsen A. (1953) 65 35 16 4 10
4. A.G.Apley (1956) 41 22 11 7 1
5. Perkin G. (1940) Excellent results were obtained.
6. Fairbank
T.G.(1955)
Excellent results were obtained.
While controversy over management of tibial plateau fracture
continues, excellent results of surgical treatment were shown by Palmer I.
1939 and 1951, Slee G. 1955, Duparc J. and Ficate P. 1960, Rombold
Charles 1960, Reibel D.B. and wade P.A. 1962, Courvoisier E. 1965,
Fryjordet Arne Jr. 1967, Gottofries A., Hagert G. and Sorensen S.E.
1971.
Palmer I (1952) said if there is any displacement or depression,
surgery should be performed and conservative treatment is the therapeutic
nihilism. Courvoisier E. (1965) stated that if there is any depression or
displacement, open reduction should be carried out. Hohl M. (1967) and
Rombold C. (1940) suggested open reduction and internal fixation when
depression is more than five mm. or when the lateral displacement is
more than one cm. Rasmussen (1973) did open reduction for valgus or
varus instability of 10o or more in extended position.
Moor T.M. and Harvey J.P. Jr. (1974) used the tibial palteau view
to measure the exact degree of depression before planning any surgery.
According to Elstrom J., Pankovich AM, Sasson H. et. al. (1976) before
planing any surgery tomography should be done to know the exact
depression, separation of fragment and type of fracture.
According to A.O. ASIF principles except for undisplaced
fractures, every plateau fracture should be operated to achieve anatomical
reduction and internal fixation.
Barr JS (1940) suggested the method of elevation of depressed
plateau, bone grafting and internal fixation. Autogenous bone grafts can
be augmented with bank bone. Methylmethocrylate has also been used
for fixation of fragment. (Kenney W.R. 1978).
Recently Clyton perry and Lawerence G. Evans and samrile
(1984) described a new approach where anterior horn of lateral meniscus
is incised and detached so that the split fragment can be opened like book.
Incision of the anterior horn minimizes the need to free the lateral
meniscus from its attachment.
Variety of implants have been used for internal fixation like Dowel
bone grafts, K wires (Turner V.C. 1959), wire loops (Rasmussen P.S.
1973), Gottfries A. Hagert CG and Sorensen S.E. 1971) Bolts and
washers (Barr J.S. and McAusland W.R. Jr. (1958), Hohl M. and Luck
J.V. 1956) Knowel pins (Robert J.M. 1968) Buttress plates T or L type
(Hohl M. 1967), Muller M.E., Allgower M. Wilengger H. 1970),
Cancellous screws : Charnely’s clamp (Black Burn J.W. 1977)].
Nowdays internal fixation with butress plate and cancellous screws
has been widely accepted.
Principle of Buttress plate : (Muller M.E., Allgower M. Wilenegger H.
1970) – a plate may be used to buttress or to support a thin cortical wall
and maintains its length. A buttress plate functions in a manner opposite
to tension band plate in that it is always under compression. Buttress
plates are used where cortices are thin, medullary bone is cancellous and
often compressed. They prevent the recurrence of slowly progressive
deformity with settling or bone absorption. Once the plate has been
applied, the fixation should be supported by packing cancellous bone
grafts into the defect to prevent the loss of height. A plate used as a
buttress is never under tension. Regular round hole ASIA – A.O. plate,
D.C.P. or contoured T or L plate can be used as a buttress plate.
Wilson and Jacob JS (1952) independently described an original
method of treating severely depressed comminuted fracture of lateral
tibial plateau where patella is removed and is used to replace the articular
surface of condyle. Lee H. (1957) used pear shaped graft from anterior
superior iliac spine to fill, the defect of articular surface of lateral
condyle.
Percutaneous bolting of minimally displaced fracture was
described by D’ Aubigne, R and Mazar F. (1960). Miller T.S. (1965)
published the report on closed reduction and traction followed by
percutaneous introduction of wire or pins under roentgenographic control.
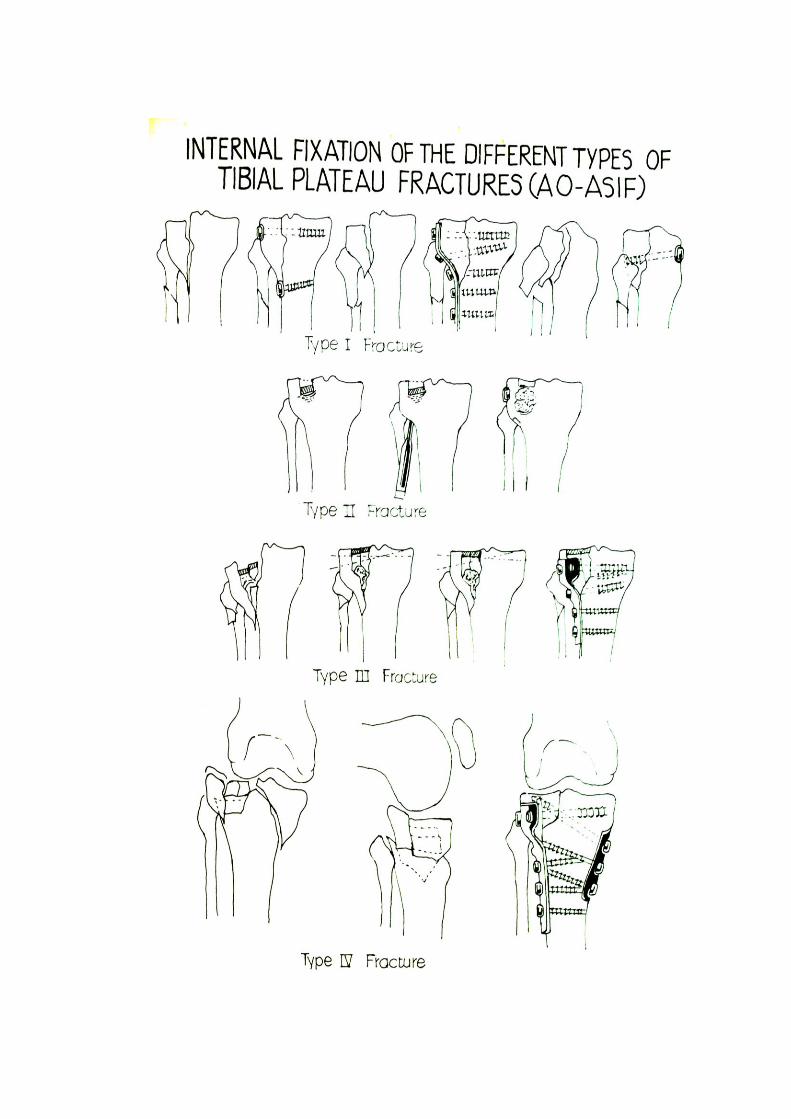
Internal fixation recommended by A.O. ASIF is shown in diagram.
Ligamental repair – It has been a common practice over the years to
repair the bone damage and to expect theligamental injury to heal with
immobilization. Analyusis of results have shown that this does not occur
always. (Bick E.M. 1941, Knight R.A. 1945, Maisel B. and Cornell N.W.
1948, Bradford C.H., Kilfoyle, R.M. Kellecher J.J. 1950, Badgley C.E.
and O’Connor S.J. 1952, Hohl M., Luck J.V. 1956, O’Donoghue D.H.
1962, Solomen K.A. 1963). Maximum integrity of both soft tissue and
bone structure about knee joint will result in best possible function.
However, only few ligament in presence of condylar fracture have been
reported [Eliason E.L. and Eberling W.W. 1933, Naviaser J.S. and
Eisenberg S.H. 1956, Rombold Charles, 1960].
According to Muller, M.E., Allgower M. and Willenegger H.,
twenty percent of compression fracture of the lateral plateau are
associated with injuries of the medial collateraal ligament, which is either
avulsed out of bone or torn through its substance together with a tear of
the posterior capsule. Therefore, once the lateral plateau is reconstructed,
it is necessary to test the stability of the medial collateral ligament and
capsule by applying a valgus force with the knee first in full extension
and then in 30o of flexion. One must also test for meniscal injuries and for
injuries to the cruciate liagments.
When meniscus is torn, removal is indicated but when peripheral
attachment is torn, it can be sutured in place with little risk of subsequent
derangement (Hohl M. and Luck J.V., 1956).
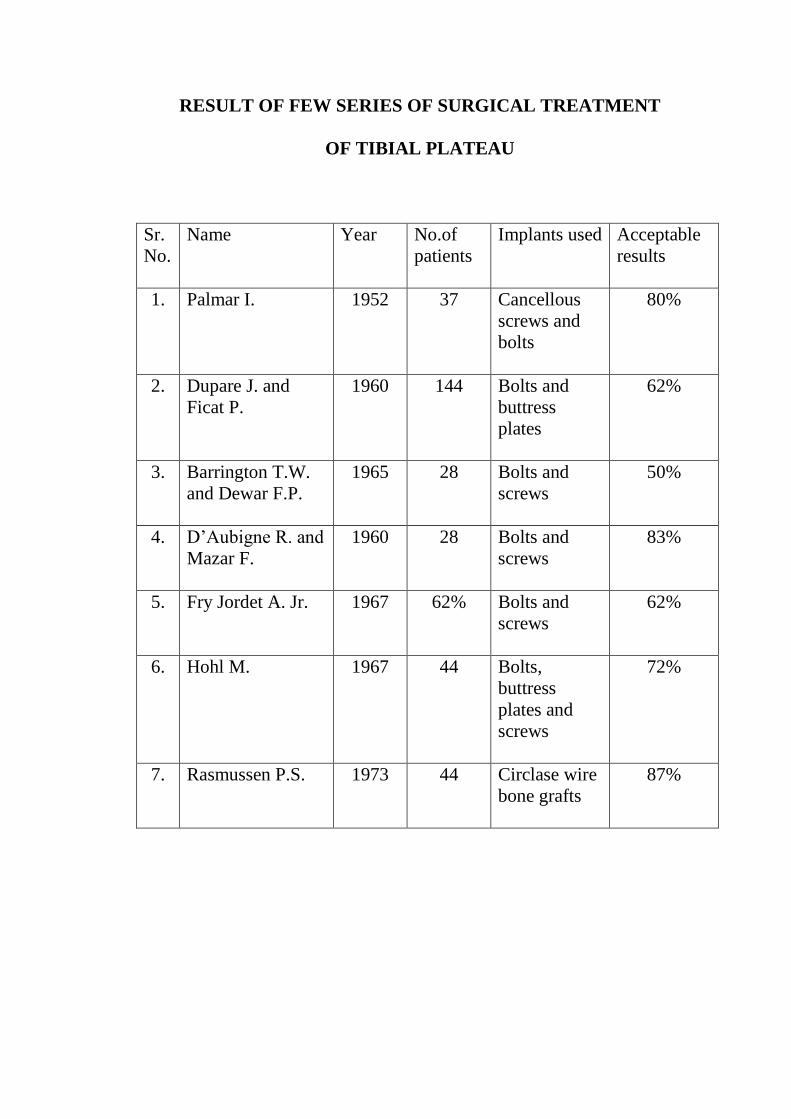
RESULT OF FEW SERIES OF SURGICAL TREATMENT
OF TIBIAL PLATEAU
Sr.
No.
Name Year No.of
patients
Implants used Acceptable
results
1. Palmar I. 1952 37 Cancellous
screws and
bolts
80%
2. Dupare J. and
Ficat P.
1960 144 Bolts and
buttress
plates
62%
3. Barrington T.W.
and Dewar F.P.
1965 28 Bolts and
screws
50%
4. D’Aubigne R. and
Mazar F.
1960 28 Bolts and
screws
83%
5. Fry Jordet A. Jr. 1967 62% Bolts and
screws
62%
6. Hohl M. 1967 44 Bolts,
buttress
plates and
screws
72%
7. Rasmussen P.S. 1973 44 Circlase wire
bone grafts
87%
MATERIAL AND METHODS
MATERIAL AND METHODS
First 30 cases of tibial plateau fractures admitted in Indira Gandhi
Medical College and Mayo Hospital were studied from the date 1.3.1984
to 31.5.1985. All the cases were diagnosed, treated and followed
according to prescribed proforma.
Once the patient was admitted, x-rays were taken (AP and lateral),
posterior cast was given for support and analgesics and anti-inflammatory
drugs were given. All the associated injuries were treated accordingly.
Type of fracture was decided according to AO classification. Line of
treatment was decided according to the type of fracture, degree of
displacement and depression, and general condition of the patient. Out of
30 patients 15 were treated surgically and 15 were by conservative
method.
All displaced, depressed fractures were operated upon to achieve
anatomical reduction, rigid internal fixation and early mobilization.
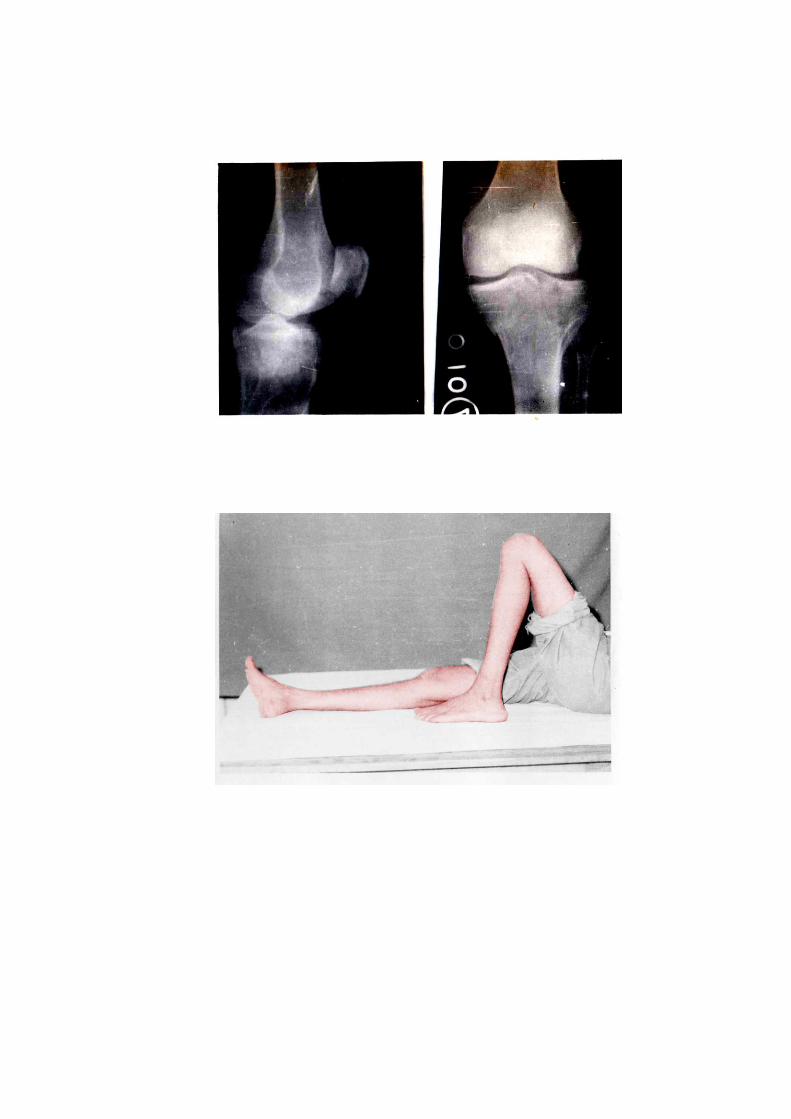
Out of 15 patients treated conservatively i.e. by skeletal traction
and early mobilization, six were advised primarily conservative treatment
because of linear and undisplaced fracture, and nine were either those
who refused surgery or medically unfit patients.
Whenever conservative treatment was decided, patient was taken to
operation theatre. Under all stertile precautions, Steinman pin was
passedthrough the lower one-third of tibia. Haemarthrosis, if present was
aspirated and Jones bandage was given. No attempt was made to reduce
the fracture. The patient was shifted to the ward, where affected limb was
kept on Bohler’s splint and traction of 2 ½ kg. was applied. Quadricepa
exercises were begun from the next day. Guarded knee bending exercises
were started from 7th
day. Average duration of skeletal traction was 4-6
weeks. Before discharge range of movement, angular deformity were
measured and check x-ray was also done. Patient was discharged with the
instruction of knee bending exercise, quadriceps exercisee and non
weight bearing. Patient was followed every month, at each visit check x-
ray was done, range of movement angular deformity, were measured.
Patients’ complaints were noted and data was filled in the proforma.
Partial weight bearing was started between 10-12 weeks while complete
weight bearing was started approximately between 12-16 weeks.
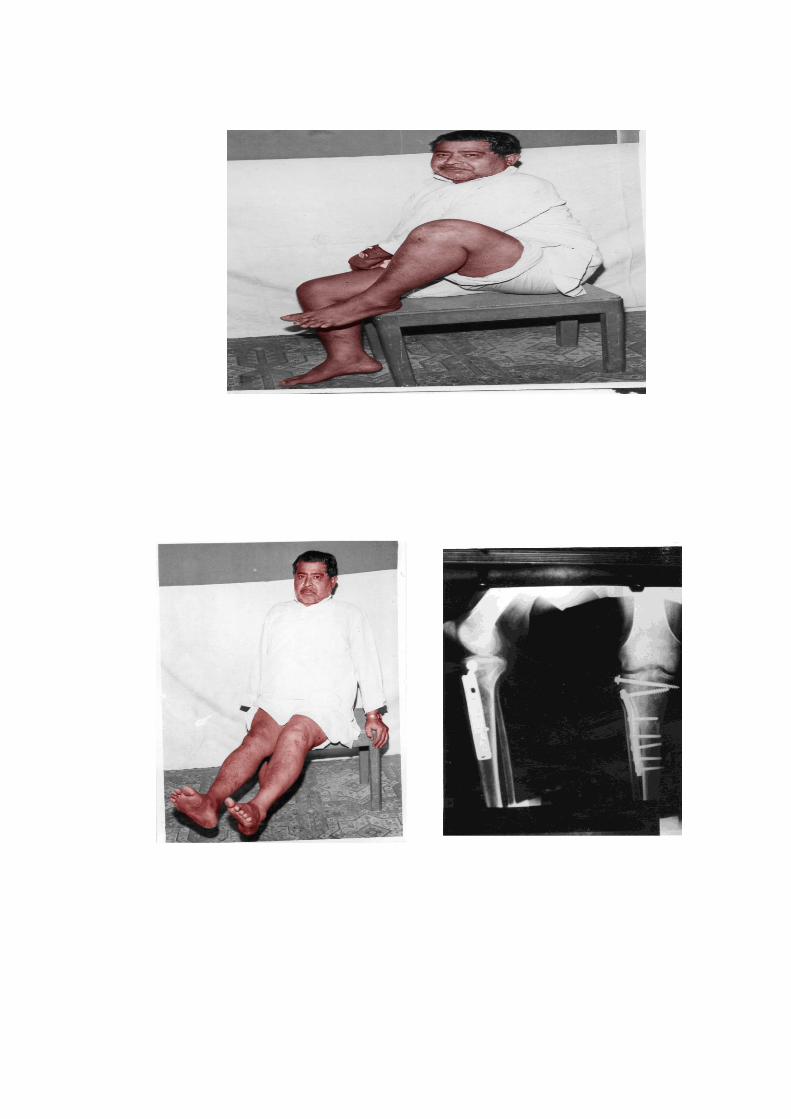
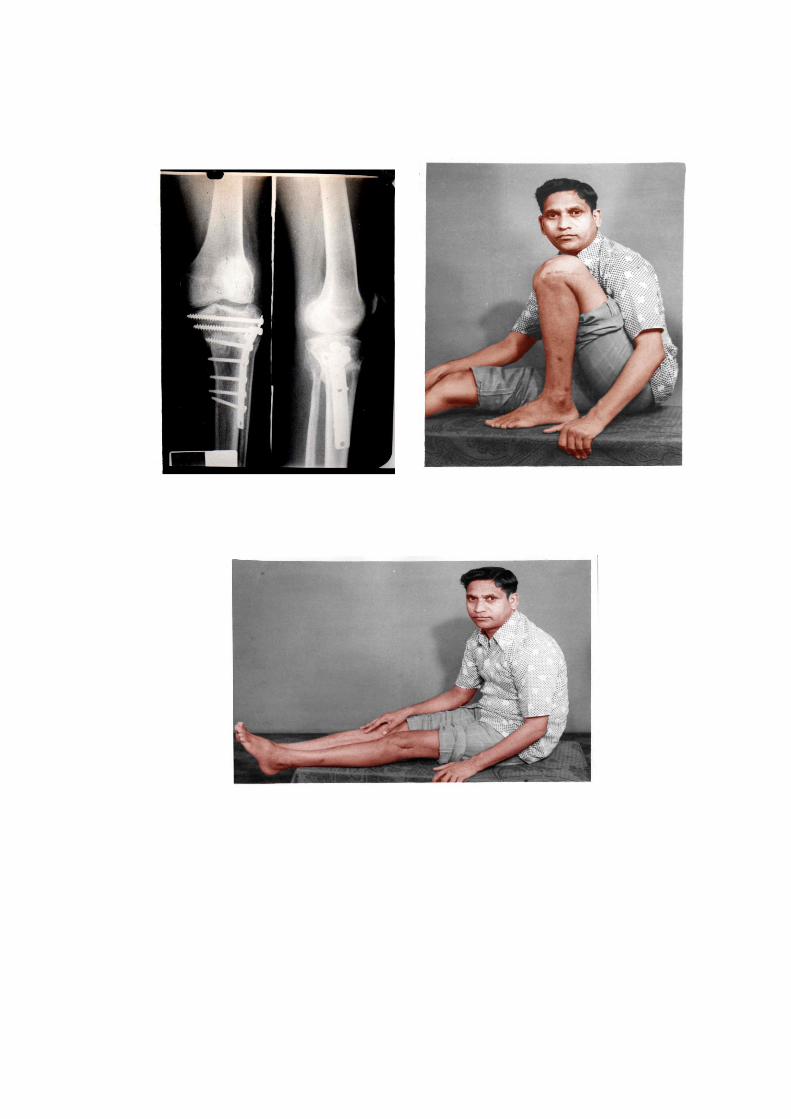
Whenever surgery was decided, patient was thoroughly
investigated, affected knee and iliac crest was prepared. All patients were
operated under spinal anaesthesia and tourniquent. In all patients,
parapatellar approach (medial or lateral) was preferred. Once fracture site
was exposed, depression and displacement was noted by elevating the
meniscus.
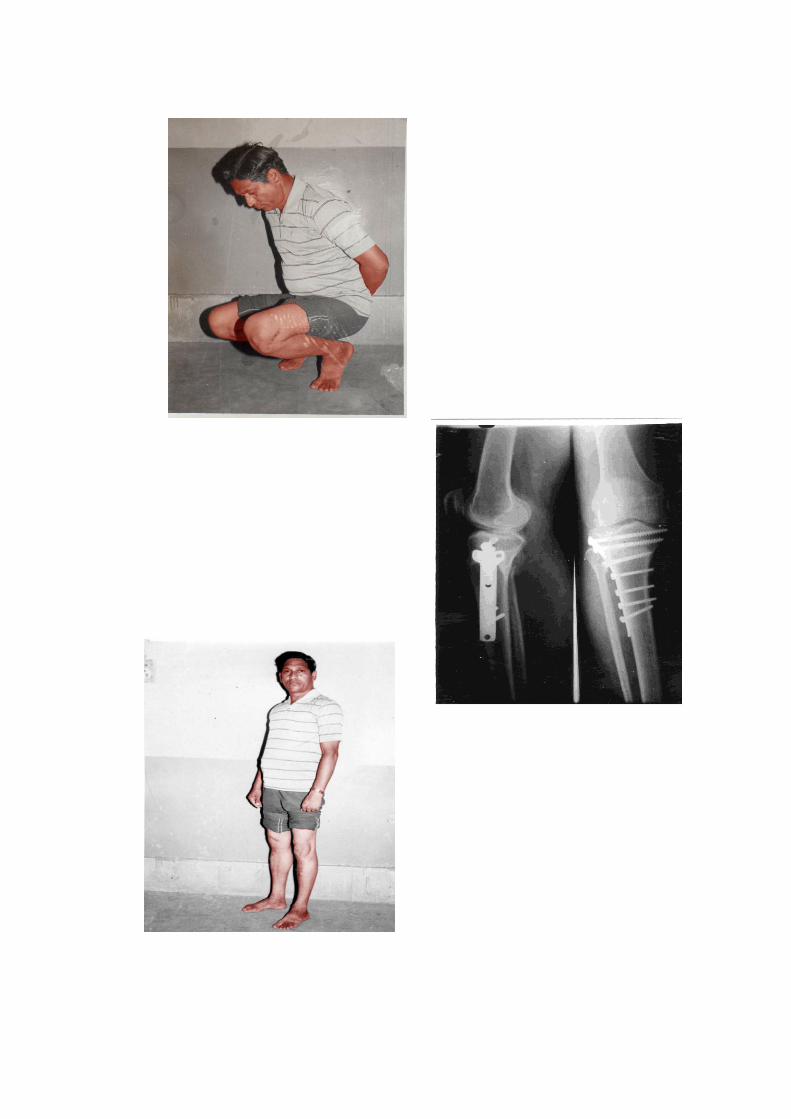
In type-I fracture when wedge was small, it was fixed by
cancellous screws while when wedge was large, buttress plate was used.
In type-II fracture, elevation of depression was carried out by
introducing a spike through the window in the cortex. Subarticular space
was filled by cancellous bone grafts. Elevated articular surface was
supported by placing single or double cancellous screws.
In type-III, reduction, elevation, bone grafting followed by fixation
by cancellous screws and buttress plate was done.
In type-IV fracture, reduction, elevation, bone grafting and
followed by fixation by double T plates and cancellous screws was
carried out.
Check x-rays were taken in the operation table before closing the
wound. Post-operative treatments consists of antibiotics, analgesics,
quadriceps exercises.
Gentle knee bending exercise was started after 72 hours while
vigorous knee bending exercise and crutch walking with non weight
bearing was allowed after removal of stitches. Patient was discharged
with the instruction of knee bending exercise, quadriceps exercise and
non weight bearing. Range of movement was noted. Patient was followed
every fifteen days. Every month angular deformity, loss of extension,
pain, and range of knee movement was measured so also check x-ray was
done. All the data obtained were filled in the proforma. Non weight
bearing continued for approximately 10-12 weeks, complete weight
bearing was started aftter 12 weeks.
OBSERVATIONS
OBSERVATIONS
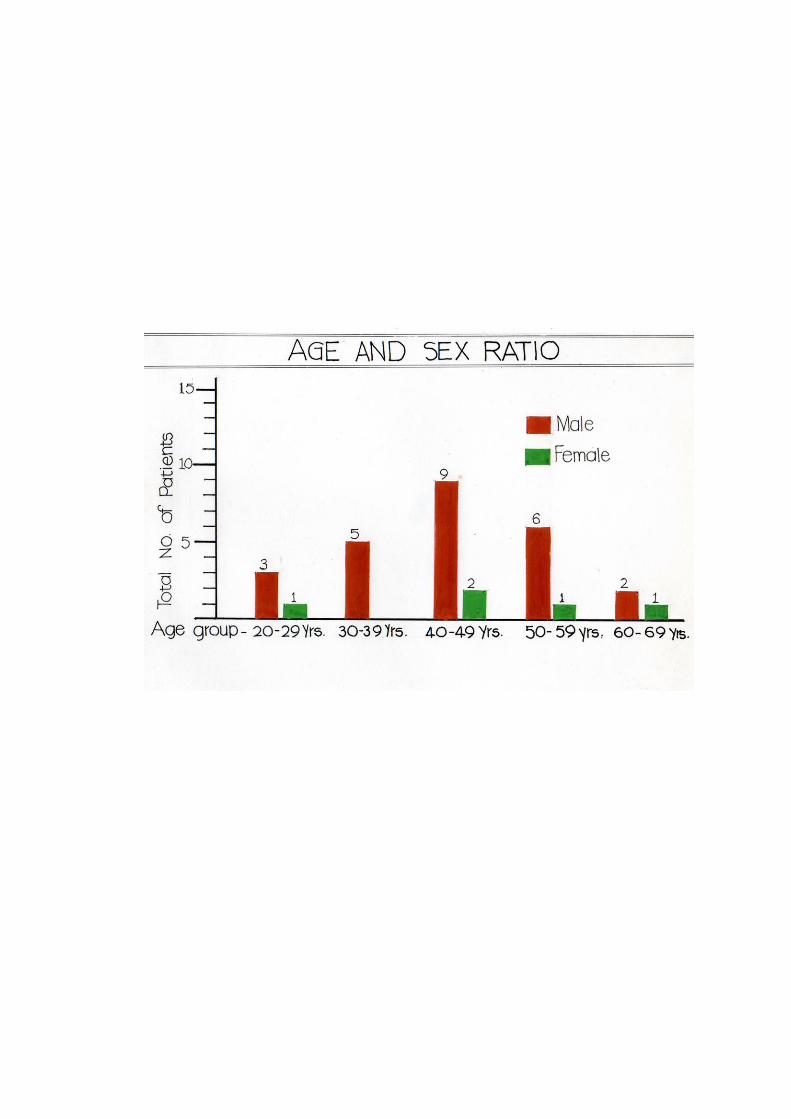
Total 30 patients were studied in this series. Observations made are
given below :
A] Age and Sex Distribution ;
In this study most of the patients belong to the middle age. Mean
age was aproximately 45 years. As far as the sex ratio is concerned, out of
30, 25 were males and only 5 were females. Male to female ratio was 5:1.
Graph of opposite page gives the details of age and sex distribution.
B] Mode of Injury :
In this study, vehicle accidents and fall from height were the
common modes of injury. Minor fall or slip was also an important mode
of injury particularly in the old age.
Following table shows mode of injury in our study.
Sr.
No.
Mode of trauma No. of cases Percentage
1. Minor fall 11 36.66%
2. Fall from height 7 23.33%
3. Struck by vehicle 6 20.00%
4. Fall from vehicle 4 13.33%
5. Unknown 2 6.60%
C] Anatomical Distribution :
As far as the involvement of knee joint is concerned, table shows
that it is approximtely equal in both the knees.
Sr.
No.
Side No. of patients
1. Right knee 16
2. Left knee 14
Distribution of fracture among the medial condyle, lateral condyle
or bicondylar fracture is shown in the following table.
Sr.
No.
Condyle/ Condyles No. of cases Percentage
1. Lateral Condyle 25 83.33%
2. Medial Condyle 1 3.33%
3. Bicondylar 4 13.33%
Total 30 100.00%
D] Associated Injuries :
Although majority of fractures of tibial plateau in the series were
caused by vehicle accident and fall from height, only few patients had
other significant associated injury.
Sr.
No.
Associated Injury No. of cases
1. Head injury 1
2. Fracture spine
compression type – L1
1
3. Fracture calcaneum – Rt 1
4. Fracture nasal bone 1
5. Fracture right radius, ulna and fracture shaft of
humerus right
1
6. Visceral injury 0
7. Contusions 8
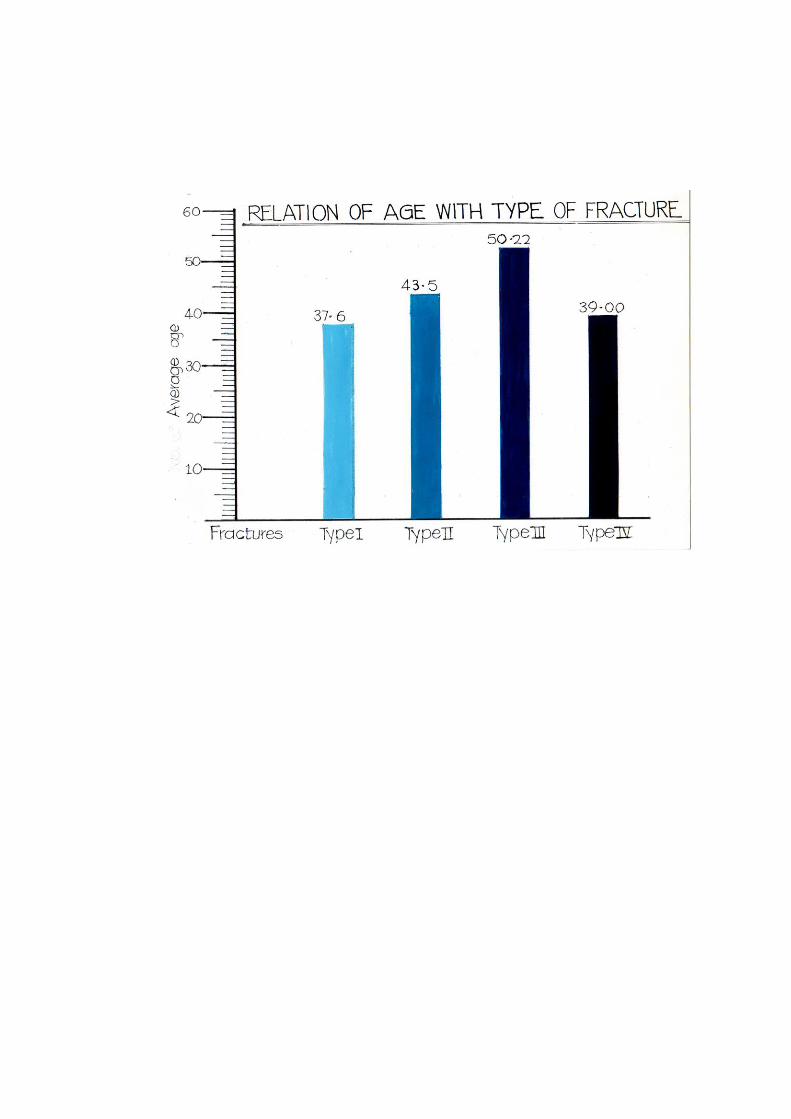
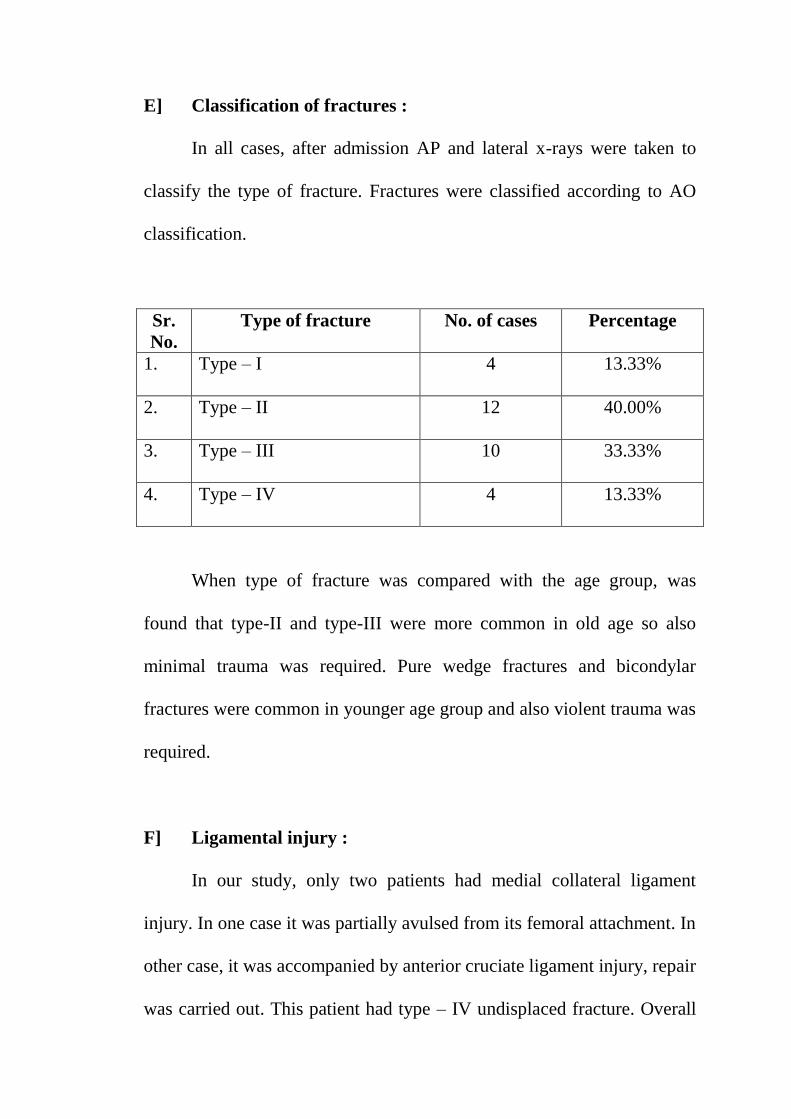
E] Classification of fractures :
In all cases, after admission AP and lateral x-rays were taken to
classify the type of fracture. Fractures were classified according to AO
classification.
Sr.
No.
Type of fracture No. of cases Percentage
1. Type – I 4 13.33%
2. Type – II 12 40.00%
3. Type – III 10 33.33%
4. Type – IV 4 13.33%
When type of fracture was compared with the age group, was
found that type-II and type-III were more common in old age so also
minimal trauma was required. Pure wedge fractures and bicondylar
fractures were common in younger age group and also violent trauma was
required.
F] Ligamental injury :
In our study, only two patients had medial collateral ligament
injury. In one case it was partially avulsed from its femoral attachment. In
other case, it was accompanied by anterior cruciate ligament injury, repair
was carried out. This patient had type – IV undisplaced fracture. Overall
incidence of ligamental injury was ten percent. One patient who was
operated for type – II fracture had detached lateral meniscus which was
removed at surgery.
Sr.
No.
Ligament No. of cases
1. Medial collateral ligament 2
2. Anerior cruciate ligament 1
3. Posterior cruciate ligament 0
4. Lateral collateral ligament 0
5. Meniscal injury – lateral 1
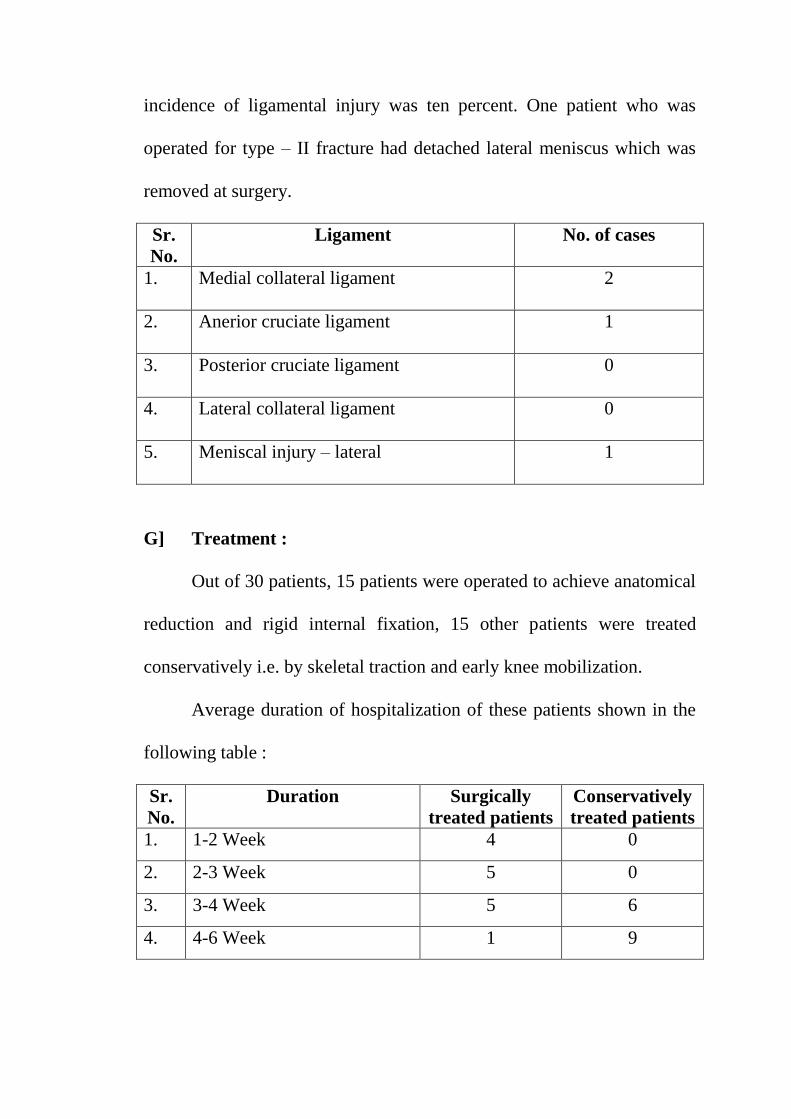
G] Treatment :
Out of 30 patients, 15 patients were operated to achieve anatomical
reduction and rigid internal fixation, 15 other patients were treated
conservatively i.e. by skeletal traction and early knee mobilization.
Average duration of hospitalization of these patients shown in the
following table :
Sr.
No.
Duration Surgically
treated patients
Conservatively
treated patients
1. 1-2 Week 4 0
2. 2-3 Week 5 0
3. 3-4 Week 5 6
4. 4-6 Week 1 9
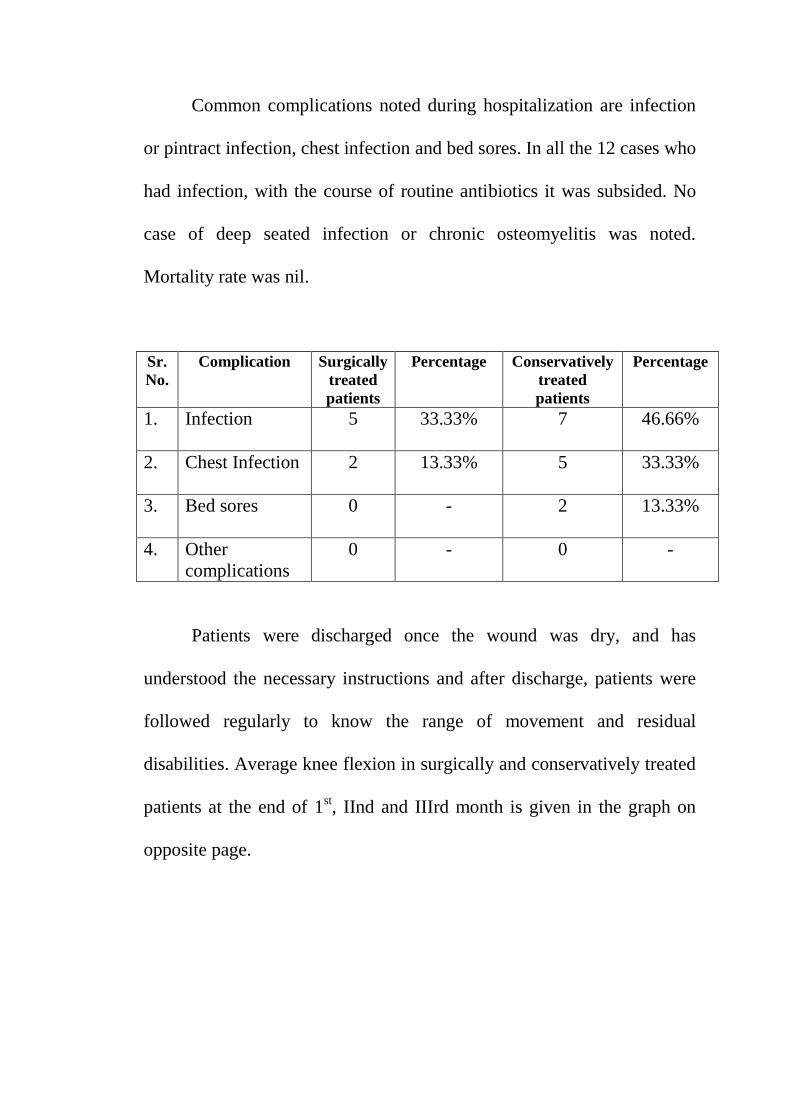
Common complications noted during hospitalization are infection
or pintract infection, chest infection and bed sores. In all the 12 cases who
had infection, with the course of routine antibiotics it was subsided. No
case of deep seated infection or chronic osteomyelitis was noted.
Mortality rate was nil.
Sr.
No.
Complication Surgically
treated
patients
Percentage Conservatively
treated
patients
Percentage
1. Infection 5 33.33% 7 46.66%
2. Chest Infection 2 13.33% 5 33.33%
3. Bed sores 0 - 2 13.33%
4. Other
complications
0 - 0 -
Patients were discharged once the wound was dry, and has
understood the necessary instructions and after discharge, patients were
followed regularly to know the range of movement and residual
disabilities. Average knee flexion in surgically and conservatively treated
patients at the end of 1st, IInd and IIIrd month is given in the graph on
opposite page.
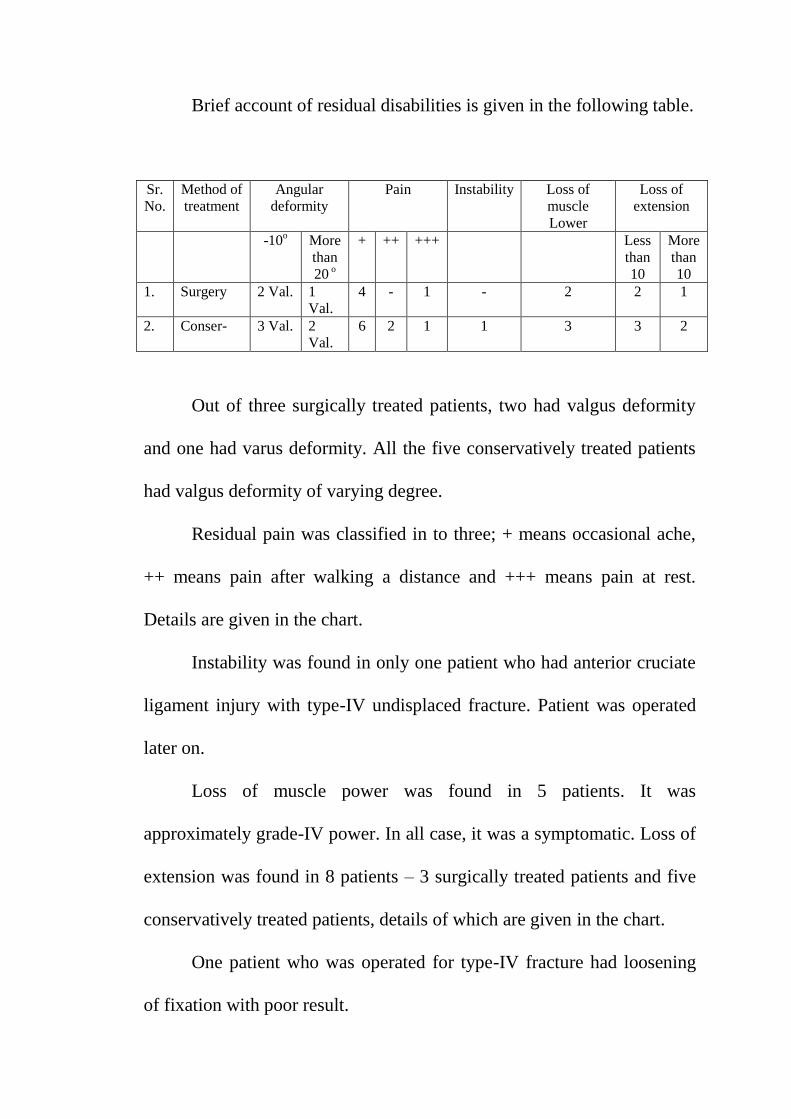
Brief account of residual disabilities is given in the following table.
Sr.
No.
Method of
treatment
Angular
deformity
Pain Instability Loss of
muscle
Lower
Loss of
extension
-10o More
than
20 o
+ ++ +++ Less
than
10
More
than
10
1. Surgery 2 Val. 1
Val.
4 - 1 - 2 2 1
2. Conser- 3 Val. 2
Val.
6 2 1 1 3 3 2
Out of three surgically treated patients, two had valgus deformity
and one had varus deformity. All the five conservatively treated patients
had valgus deformity of varying degree.
Residual pain was classified in to three; + means occasional ache,
++ means pain after walking a distance and +++ means pain at rest.
Details are given in the chart.
Instability was found in only one patient who had anterior cruciate
ligament injury with type-IV undisplaced fracture. Patient was operated
later on.
Loss of muscle power was found in 5 patients. It was
approximately grade-IV power. In all case, it was a symptomatic. Loss of
extension was found in 8 patients – 3 surgically treated patients and five
conservatively treated patients, details of which are given in the chart.
One patient who was operated for type-IV fracture had loosening
of fixation with poor result.
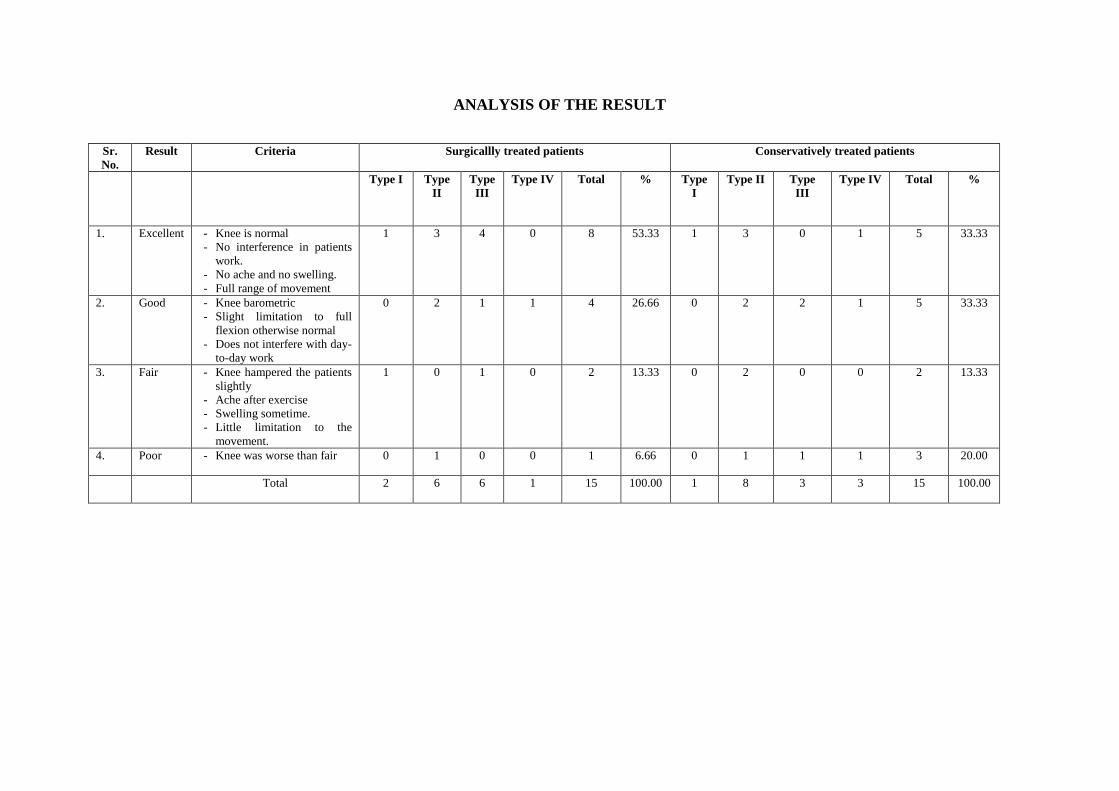
ANALYSIS OF THE RESULT
Sr.
No.
Result Criteria Surgicallly treated patients Conservatively treated patients
Type I Type
II
Type
III
Type IV Total % Type
I
Type II Type
III
Type IV Total %
1. Excellent - Knee is normal
- No interference in patients
work.
- No ache and no swelling.
- Full range of movement
1 3 4 0 8 53.33 1 3 0 1 5 33.33
2. Good - Knee barometric
- Slight limitation to full
flexion otherwise normal
- Does not interfere with day-
to-day work
0 2 1 1 4 26.66 0 2 2 1 5 33.33
3. Fair - Knee hampered the patients
slightly
- Ache after exercise
- Swelling sometime.
- Little limitation to the
movement.
1 0 1 0 2 13.33 0 2 0 0 2 13.33
4. Poor - Knee was worse than fair 0 1 0 0 1 6.66 0 1 1 1 3 20.00
Total 2 6 6 1 15 100.00 1 8 3 3 15 100.00


DISCUSSION
DISCUSSION
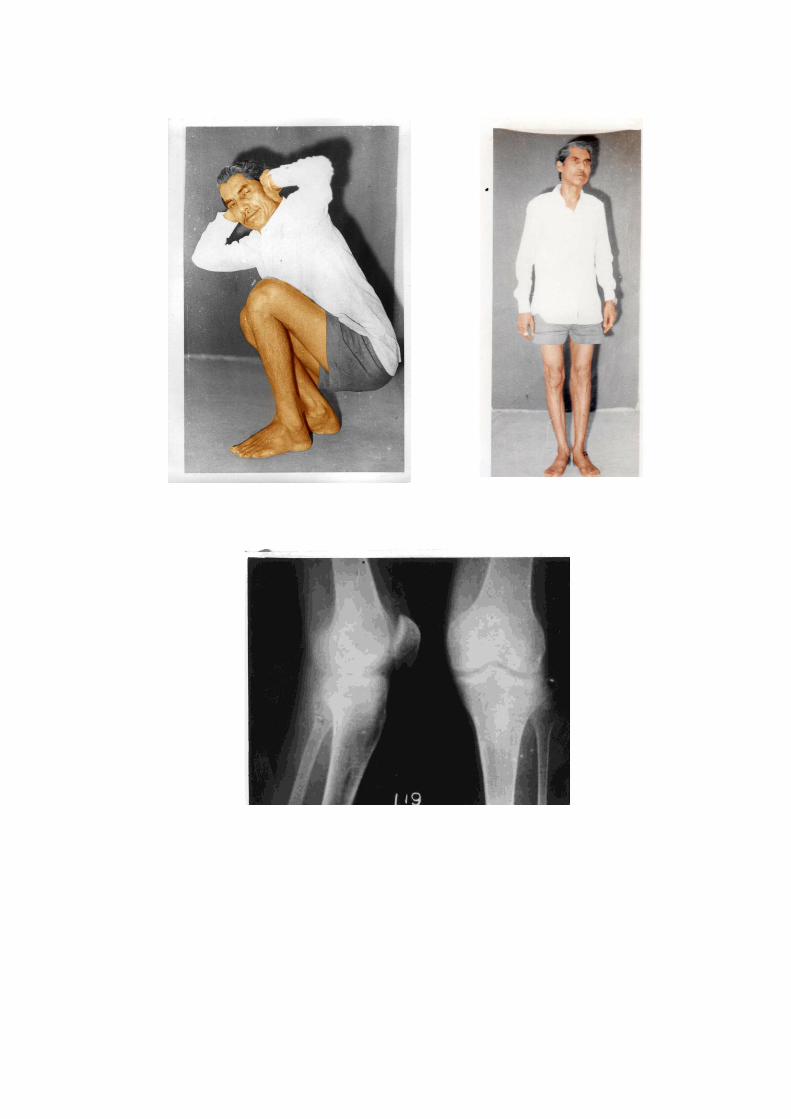
Osteoarticular fractures particularly tibial plateau fractures still
possess the problem of stiff knee and early osteoarthritis. It’s
management still remains controversial, whether surgical or conservative.
Both the schools have divergent thoughts and have published excellent
results. Keeping in mind the controversity of management this study of
30 cases was carried out. Out of 30, 15 patients were treated surgically
and 15 conservatively. All the patients were admitted, treated and
followed regularly.
Common modes of injury in this study were minor fall (36.6%),
vehicle accidents (33.3%) and fall from height (23.33%). This fracture
usually occurs in middle and old age probably due to reduced strength of
subarticular calcellous bone. In Rasmussen P.S. (1973) series average age
was 55 years. In our study, average age was 45 years. Male of female
ratio was 5:1 which corresponds to most of the series.
Antero-posterior, lateral and oblique x-rays are sufficient to
diagnose the extent of depression, displacement and type of fracture.
Tibial plateau view suggested by Moor T.M., Harvey J.P. (1974) is useful
to evaluate the extent of depression. Stress x-rays (Forster E., Mole L.,
Coblentz J. 1961, Martin A.F. 1960) are useful in diagnosis of ligamental
injury.
In our study we preferred AO Classification because it is simple,
uncomplicated and no special x-rays are required. Its practical utility to
carry out treatment and prognosis has got an upper hand. Although
Hohl’s classification is detailed and excellent, it is complicated.
From the observation tables, it is clear that type II and III i.e.
depression type of fractures are more common followed by type IV and I.
In Hohl M. and Luck J.V. (1956) series depressed type of fractures were
63.3%. In our study, it was 72.6%. According to Muller M.E., Allgower
M. and Willengger H. type I is uncommon, but in our study it was
13.33%. Type IV fracture is usually found in pure compression type of
injuries. Type II and III are commonly found in old persons while type I
and IV are commonly found in young patients – this is shown in the
graph.
Frequency of involvement of right and left knee is same. In our
study it was 16:14. Lateral condyle is most commonly affected followed
by medical condyle and finally bicondylar. (Hohl M. 1967). But in our
study following lateral condyle (83.33%) next in frequency was
bicondylar fracture (13.33%) and finally medial condyle (3.33%).
Diagnosis of ligamental injuries should be made at the earliest to
prevent residual disabilities. In Rasmussen P.S. series (1973) overall
incidence of ligamental injury was 2.5%. According to Schulak D.J. and
Gunn D.R. (1975) wedge and bicondylar fractures are commonly
associated with ligamental injury. According to Muller M.E. , Algower
and Willengger depressed type of fractures are very commonly associated
with ligamental injury (20%). In our study incidence of ligamental injury
is 10% (2 Medial Collateral ligaments and 1 anterior cruciate ligament).
In our study 15 patients were treated surgically. Indication of
surgery was either depression or displacement Aim of Surgery was to
achieve anatomical reduction, rigid internal fixation and early
mobilization. Indication of surgery varies in different series.
We have followed AO Technique which is given in diagram. DCP
plates, Buttress plates and cancellous screws were used. For type II, III
and IV bone grafts were used. Surgery requires skill, proper technique
and instrumentation. Check x-rays were done before closing the wound,
stability of the joint was tested. Associated ligamental injury should be
repaired at the time of Surgery. Knee bending was started after 72 hours,
while mobilization with crutches was allowed after removal of stitches.
Average duration of hospitalization was 21 days. It is because of high rate
of post-operative wound infection (33.3%).
As far as conservative treatment is concerned, we employed
Apley’s method of skeletal traction and early mobilization. No attempt
was made to reduce the fracture. Average duration of hospitablization
ranges from 4 to 6 weeks. Two patients had bed sores, while incidence of
chest infection is higher in conservatively treated patients. Incidence of
pin tract infection was 46.66 (7 patients).
Awareness of the factors producing permanent disability after tibial
condylar fractures permits critical appraisal of current methods of
treatment. These factors are limited motion, instability, angular
deformitym, lack of full extension, pain and post-traumatic arthritis and
muscle weakness.
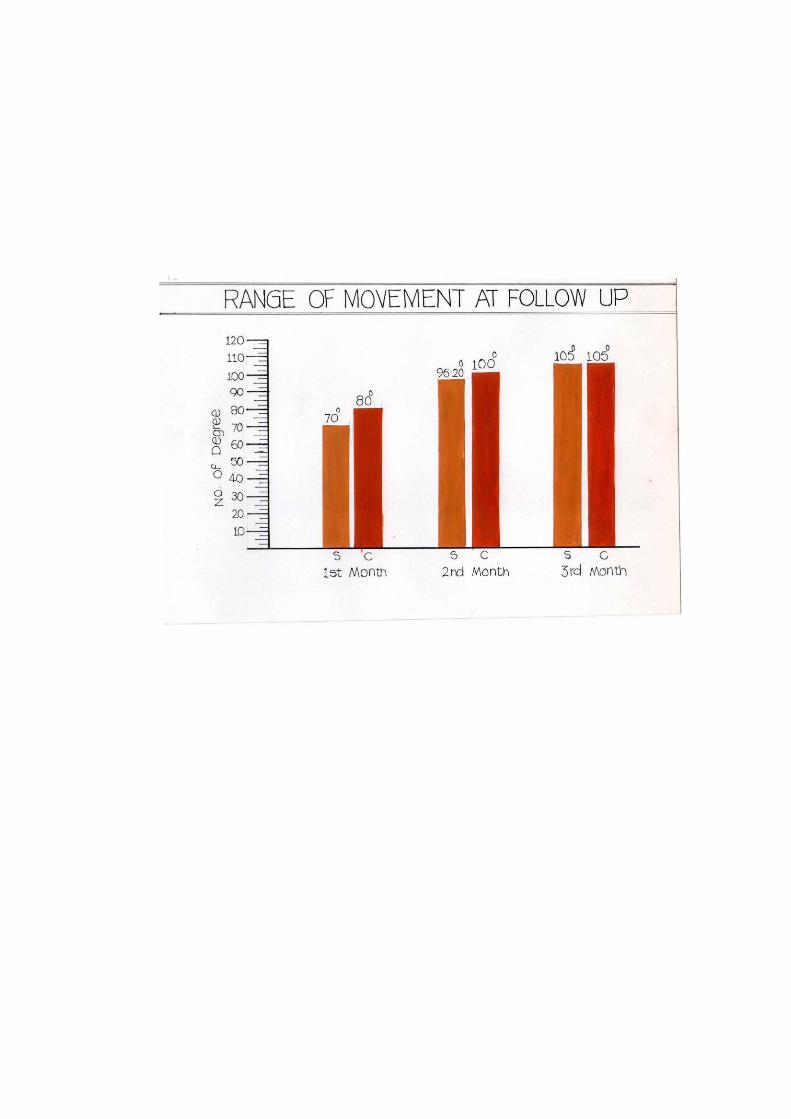
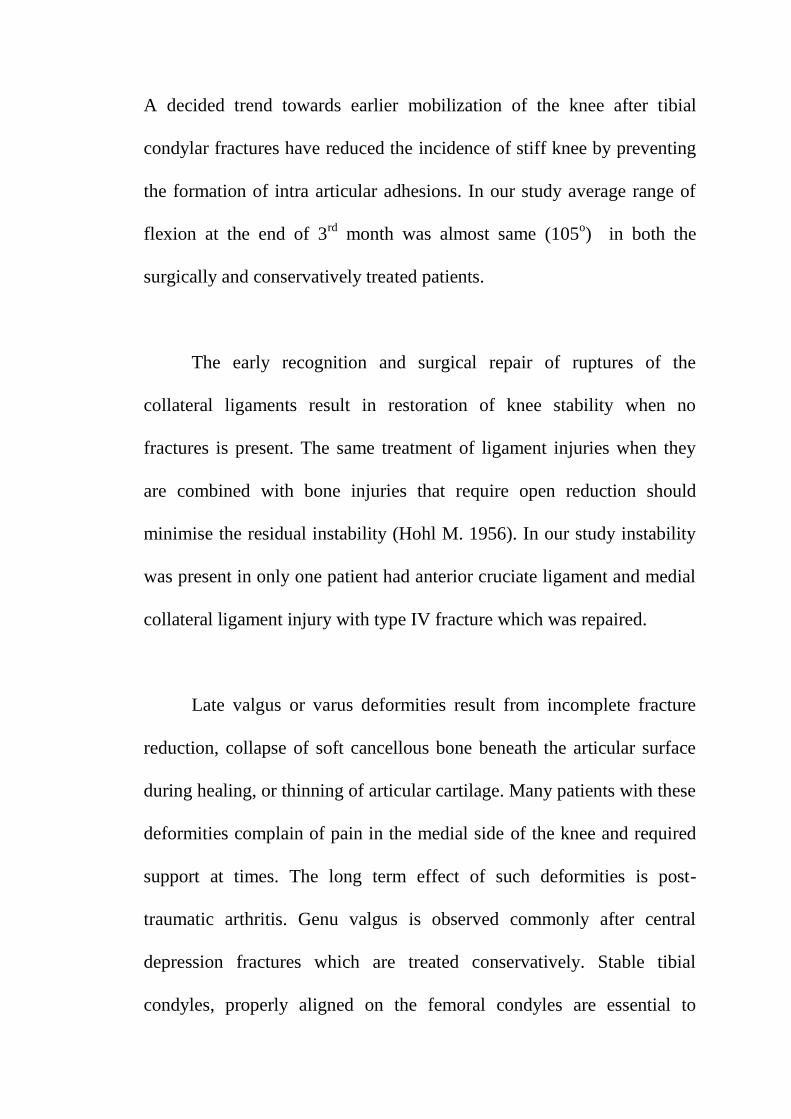
A decided trend towards earlier mobilization of the knee after tibial
condylar fractures have reduced the incidence of stiff knee by preventing
the formation of intra articular adhesions. In our study average range of
flexion at the end of 3rd
month was almost same (105o) in both the
surgically and conservatively treated patients.
The early recognition and surgical repair of ruptures of the
collateral ligaments result in restoration of knee stability when no
fractures is present. The same treatment of ligament injuries when they
are combined with bone injuries that require open reduction should
minimise the residual instability (Hohl M. 1956). In our study instability
was present in only one patient had anterior cruciate ligament and medial
collateral ligament injury with type IV fracture which was repaired.
Late valgus or varus deformities result from incomplete fracture
reduction, collapse of soft cancellous bone beneath the articular surface
during healing, or thinning of articular cartilage. Many patients with these
deformities complain of pain in the medial side of the knee and required
support at times. The long term effect of such deformities is post-
traumatic arthritis. Genu valgus is observed commonly after central
depression fractures which are treated conservatively. Stable tibial
condyles, properly aligned on the femoral condyles are essential to
prevent angular deformity of the knees. In our study angular deformity
was present in 3 surgically treated patients (2 valgus and 1 vargus) and
five (5) conservatively treated patients (valgus).
Lessening the duration of rigid immobilization and insisting upon
early movement, always starting and ending movement with the knee in
full extension prevent limited extension. This principle applies to traction
treatment. 3 operated and 5 conservatively treated patients had loss of
extension of variable degrees.
Disabling pain years after a tibial condylar fracture is uncommon,
although discomfort is noted frequently. Often the discomfort is on the
medial side over the collateral ligament and is the result of chronic strain.
Less often the pain is localized in the previously injured compartment of
the knee and is caused by the traumatic arthritis that results from irregular
surfaces, angular deformity , or degeneration of the articular surface.
Prevention of late valgus or varus deformity seems essential to minimize
the later development of knee pain from strain or traumatic arthritis. In
our study, occasional acheme which is insignificant and was more
common in conservatively treated patient. Pain at rest was present in one
surgically treated patient and three conservatively treated patients.
Muscle Weakness was present in five patients (16.6%). It was
almost grade IV. But in all cases, it was asymptomic.
On an average incidence of residual disabilities was more in
conservatively treated than surgically.
Partial weight bearing was started between 12 to 16 weeks. This
corresponds to most of the series.
Results of treatment depends upon final outcome of the patients.
Hohl M. and Luck J.V., 1956, Rasmussen P.S. (1971) put forward
excellent methods of grading the anatomical and functional results. But
both the systems are complicated. In 1956 G. Apley put forward the
simple method of grading the results, which is utilized in our study.
In surgically treated patient, acceptable results were obtained in
80% of patient (excellent 53.33% and good 26.66%) which corresponds
to series of Palmer I. (1959), Rasmussen P.S. (1973). Poor result was
obtained in one patient who had tyupe IV fracture with varus deformity of
20o
, loss of extension of 10o
, pain at rest and loosening of fixation.
About 93.33% patients were satisfied with the final result, and resumed
their duties. Only drawback of our treatment was high rate of infection
(33.33%) and long duration of hospitalization (25 days).
Those who were treated conservatively excellent results were
obtained in 33.33% (5 patients), good in 33.33% (5 patients) fair in 2
patients (13.33%) and poor in 3 patients (20%). Overall results
corresponds to series of Jakobsen A. (1953), Parey O. (1952) and A.G.
Apley (1956). Drawbacks of conservative treatment were pintract
infection (46.66%) chest infection (33.33%) bed sores in 2 patients
(13.33%) and high rate of residual disabilities.
SUMMARY AND CONCLUSION
SUMMARY & CONCLUSIONS
30 cases of tibial plateau fracture were treated and studied in Indira
Gandhi Medical College and Mayo Hospital. Fractures were classified
according to AO classification. 15 patients treated surgically i.e.
anatomical reduction, rigid internal fixation and early mobilization. 15
patients were treated conserevatively i.e. skeletal traction and early
mobilization. All the patients were following regularly.
Following conclusions were drawn :
1. Tibial plateau fractures are common in middle and old age (average
age is 45 years). More common in Males (Male to female ratio is
4:1) because of more outdoor activities.
2. Vehicle accidents, fall from height and minor fall are the common
modes of injury.
3. Type II and III (Depression type) fractures are more common than
type I and IV.
4. Incidence of ligamental injury is 10%.
5. Duration of hospitalization is more in conservatively treated
patients.
6. Incidence of post-operative infection is 33.33% while pin tract
infection is conservatively treated patients was 46.66%.
7. Chest infection and bed sores are common problems of
conservative treatment since the patients are bed ridden.
8. Overall incidence of residual disabilities is high in conservatively
treated patients.
9. Acceptable results were obtained in 80% of surgically treated
patients, and 66.66% of conservatively treated patients. Poor
results are frequently seen in conservatively treated patients.
10. Overall surgical treatment is useful in ostechondral fractures of
tibial plateau particularly depressedand displaced. It is associated
with very few complications provided it is carried out properly.
11. Conservative treatment is useful in undisplaced and minimally
displaced fractures but incidence of residual disabilities is high.
BIBLIOGRAPHY
BIBLIOGRAPHY
1. Apley, A.G. : Fractures of the lateral tibial condyle treated by
skeletal traction and early mobilization. J.Bone Joint Surg.
38B:699-708, Aug. 1956.
2. Apley A.G. : Fractures of the tibial plateau : The orthopaedic
clinics of North America, Vol. 10, No. 1 – 61-74 , 1978.
3. Badgley, C.E., and O’Connor, S.J. : Conservative treatment of
fractures of the tibial plateau. Arch. Surg.. 64:506-515, 1952.
4. Barr, J.S. : The treatment of fracture of the external tibial
condyle (bumper fracture), J.A.M.A. , 115:1683-1687, 1940.
5. Barr, J.S., and MacAusland. W.R., Jr. : Injuries involving the
knee joint. In Cave, E.F. [ed.] : Fractures and other injuries.
Chicago, Year Book Publishers, 1958.
6. Barrington, T.W., and Dewar, F.P. : Tibial plateau fractures,
Can. J. Surg.,8 : 146-152, 1965.
7. Bick, E.M. : Fractures of the tibial condyles. J. Bone Joint
Surg., 23:102-108, Jan. 1941.
8. Black Burn J.E. : Maintenance of tibial plateau fractures by
Charnley’s Compression device. Clinical Orthopaedics 123:
112- 113, March-April 1977.
9. Bradford, C.H., Kilfoyle, R.M., Kelleherk, J.J., And Magill,
H.K. : Fractures of the lethal tibial condyle, J.Bone Joint Surg.,
32A:39-47, 1950.
10. Burrows, H. : Fractures of the Lateral Condyle of the Tibia. J.
Bone Joint Surg., 388: 612-613, 1956.
11. Clyton Perry, Lawerence G. Evans., Samrile et. Al – A new
surgical approach to fractures of lateral tibial plateau. J. Bone
Surg.l 66A : 1236-1241, 1984.
12. Cotton, F.G., and Berg. H. : Fender fracture of the tibia at the
knee, New Eng. J. Med., 201:989-995, 1929.
13. Cotton F.J. : Fender fractures, Surg, Gynecol, Obstet., 62-442-
444-1936.
14. Couvoisier, E. : Les Fractures intra-articulaires de l’ extremite
superieure du tibia. Helv. Chir. Acta, 32:257-263, 1965.
15. Cubbins, W.R., Conley, A.H., and Seiffert, G.S.: Fractures of
the lateral tuberosity of the tibia with displacements of the
lateral meniscus between the fragments, Surg. Gynecol, Obstet.,
48:106-108, 1929.
16. Cubbins, W.R. Conley, A.H. Callahan, J.J. and Scuderi, C.S. :
Fractures of the lateral condyle of the tibia – classification,
pathology, and treatment, Surg. Gynecol. Obstet., 59: 461-468,
1934.
17. D’Aubigne, R., and Mazar, F. : Formes anatomiques and
traitement deks fractures de 1’ extremite superieure du tibia.
Rev. Chir. Orthop., 46: 289-318, 1960.
18. Dickson, J. : Fractures of the knee involving the tibia. Amer. J.
Surg., 38:700-705, 1937.
19. Dobelle, M. : A new method closed reduction of fractures of the
lateral condyle of the tibia. Amer. J. Surg., 53:460-462, 1941.
20. Drennam D.B. and Fedrik Locher : Fractures of tibial plateau,
Treatment with closed reduction & spica cast., J. Bone Joint
Surgery 61A: 991-995, 1979.
21. DuParc, J., and Fiscat, P. : Fractures articulaires de 1’ extremite
superieure du tibia. Rev. Chir. Orthop., 46:399-486, 1960.
22. Eliason, E.L., and Eberling, W.W. : Non-operative treatment of
fractures of the tibia and femur involving the knee joint. Surg.
Gynecol. Obstet ., 57:658-667, 1933.
23. Elstrom J., Pankovich Am, Sassoon H. and Rodriguer J. : The
use of tomography in the assessment of fractures of tibial
plateau. J. Bone Joint Surgery 58A: 551-555, 1976.
24. Fageburg, S. : Tomographic analysis of depressed fractures
within the knee joint, and of injuries to the cruciate ligaments.
Acta Orthop. Scand., 27:219-2227, 1958.
25. Fairbank, T.J. : Condylar fractures of the knee joint. Proc. Roy.
Soc. Med., 48:95 -96, 1955.
26. Foged, J.: Operative treatment of fracture of a tibial condyle.
Ugeskr. Laeger, 105:451, 1943.
27. Forster, E., Mole, L., and Coblentz, J. : Etude des lesions
ligamentomes dans les fractures du plateau tibial Ned. T.
Geneesk, 105:2173-2181, 1961.
28. Fryjordet, A., Jr. : Operative treatment of tibial condylar
fractures. Acta Chir. Scand., 133:17-21, 1967.
29. Fyshe, T.G. : Fractures of the condyles of the tibia immobilized
by the Stander splint. Can. Med. Ass. J., 67:103-107, 1952.
30. Gottfries, A., Hagert, C.G. , and Sorensen, S.E. : T-and Y-
fractures of the tibial condyles. A follow- up study of cases
treated with closed reduction and surgical fixation with a wire
loop. Injury, 3:56-63, 1971.
31. Goyling, U., and Lingdholm, R.: Fractures of the tibial condyle.
Ann. Chir. Gynaecol. Fenn., 42:229-235, 1953.
32. Haldeman, K.O. : The healing of joint fractures. A clinical and
experimental study. J. Bone Joint Surg., 20:912-922. 1939.
33. Heppanstall R.B. : Fracture, healing and treatment. W.B.
Saunders and Co. 735-745, 1979.
34. Hohl, M., and Luck, J.V. : Fractures of the tibial condyles. A
clinical and experimental study. J. Bone Joint Surg., 38A :
1001-1018, 1956.
35. Hohl, M. : Tibial condylar fractures. J. Bone Joint Surg., 49A :
1455-1467, 1967.
36. Hohl M. and Robert Larson : Fractures and dislocations of the
knee- Fractures Vol. 2 by Rockwood & Green : J.B. Lippincott
and Co. 1158-1178, 1975.
37. Hymbert, R. : Contribution a 1’etude du traitement des fractures
du plateau tibial par 1’ extersion au fil de Kirschner. Rev. Med.
Suisse Romande, 59:641-646, 1939.
38. Iifeld, F.W., and Hohl, M. : Closed reduction treatment of tibial
condylar fractures (abstr.) J. Bone Joint Surg., 42A:534-535,
1960.
39. Inclan, A. : El tratamiento quirurgico de las fractures graves de
las tuberosidades de la tibia. Cir. Ortop. Traumatol, Habana, 5 :
32, 1937.
40. Jacobs , J : Patellar graft for severaly depressed comminuted
fractures of the lateral tibial condyle. J. bone Joint Surg. ,
47A:842-847, 1965.
41. Jakobsen, A. : Operative treatment of the lateral tibial condyle
fractures. Acta Orthop. Scand., 23:34-50, 1953.
42. Kennedy, J.C., and Bailey, W.H. : Experimental tibila-plateau
fractures. J. Bone Joint Surg., 50A:1522-1534, 1968.
43. Kennedy W.R. : Fractures of tibial condyles – a preliminary
report on supplementary fixation with methylmethocrylate.
Clin. Orthop. 134 :153-157, July-Aug. 1978.
44. Klin R. : Usual etiology of fender fractures : New England J.
Medi. 210:480-481 , 1934.
45. Knight, R.A. : Treatment of fractures of the tibial condyles,
Southern Med. J., 38 : 246-255, 1945.
46. Lee, H. : Osteoplastic reconstruction in severe fractures of the
tibial condyles. Amer. J. Surg., 94:940-944, 1957.
47. Lindholm, R.V. : Treatment of fractures of the tibial condyles
by active movement theraphy. Acta Orthop. Scand., 23:320-
323, 1954.
48. Maisel, B., and Cornell, N.W. : Conservative treatment of
fractures of the tibial condyles. Surgeryu, 23:591-598, 1948.
49. Martin, A.F. : The pathomechanics of the knee joint. I. The
medial collateral ligament and lateral tibial plateau fractures. J.
Bone Joint Surg., 42A:13-22, 1960.
50. Metz, A.R., Householder, R., and Depree, J.F. : Impaction of
fractgures by large pressure tongs, Amer. J. Surg., 59:447-449,
1943.
51. Miler T.S. Du traitment des fractures des condyles du femur et
du fibia par embrochange Lyon Chir. 61: 89-92 , 1965.
52. Moore, T.M. and Harvey, J.P. , Jr. : Roentgenographic
measurement of tibial plateau depression due to fracture. J.
Bone Joint Surg 56A:155-160, 1974.
53. Muller, M.E., Allgower, M., and Willenegger, H. : Manual of
Internal Fixation, New York, Springer- Verlag, 1970.
54. Meviser, J.S., and Eisenberg, S.H. : Diagnostic and therapeutic
obstacles encountered in tibial plateau fractures. Bull. Hosp.
Joint Dis., 17: 48-57, 1956.
55. O’Donoghue, D.H. : Treatment of Injuries to Athletes.
Philadelphia, W.B. Saunders, 1962.
56. Palmer, I. : Compression fractures of the lateral tibial condyle
and their treatment. J. Bone Joint Surgery., 21: 674-680, 1939.
57. Palmer, I. : Fractures of the upper end of the tibia. J. bone Joint
Surg., 33B: 160-166, 1951.
58. Perey, O. : Depression fractures of the lateral condyle. Acta
Chir. Scand., 103:154-157, 1952.
59. Perkin G. : Fractures : London Humphery Melford Oxfor
University Press, 1940.
60. Porter, B. : Crush fractures of the lateral tibial table. J. Bone
Joint Surg., 52B : 676-k1687, 1970.
61. Rasmussen, P.S. : Tibial condylar fractures. J. Bone Joint Surg.,
55A:1331-1350, 1973.
62. Reibel , D.B. and Wade, P.A. : Fractures of the tibial plateau. J.
Trauma, 2: 237-352, 1962.
63. Reiner M.J. : The arthroscope in tibial plateau fracture – its use
in evaluation of soft tissue injury and bony injury.. JAOA –
100(6) – 704-707, 1982.
64. Roberts, J.M. : Fractures of the condyles of the tibia. J. Bone
Joint Surg., 50A: 1505-1521, 1968.
65. Rombold, CS : Depressed fractures of the tibial plateau. J. Bone
J Joint Surg., 42A 783-797, 1960.
66. Schioler, G. : Tibial condylar fractures with a particular view to
the value of tomography. Acta Orthop. Scand., 42:462, 1971.
67. Schulak, D.J. , and Gunne, D.R. : Fractures of the tibial condyles
: a review of the literature Clin. Orthop. 109 : 166, 1975.
68. Sever, J.W. : Fracture of tuberosities of the tibia. A report of
three cases. Amer. J. Orthop. Surg. , 14:299-302, 1916.
69. Sever, J.W. : Fractures of the tibial spine combined with
fractures of the tuberosities of the tibia. Surg. Gynecol Obstet.,
35:558-564, 1922.
70. Slee, G.C. : Fractures of the tibial condyles. J. Bone Joint
Surgy., 37B: 427-437, 1955.
71. Smillie, I.S. : Injuries of the Knee Joint. ed. 3 Baltimore,
Williams and Wilkins, 1962.
72. Solonen, K.A. : Fractures of the tibial condyles. Acta Orthop.
Scand., 63:[Suppl.] : 1-32, 1963.
73. Turner, V.C. : Fractures of the tibial plateaus, J.A.M.A., 169:
923-926, 1959.
74. Watson-Jones, R. : Fractures and Joint Injuries. ed. 4. Baltimore
Williams & Wilkins, 1955.
75. Wilson, W.J. , and Jacobs, J.E. : Patellar graft for severly
depressed comminuted fractures of the lateral tibial condyle. J.
Bone Joint Surg. 34A : 436-442, 1942.
76. Wolf, M.D., and White, E.H. : Depressed fractures of the tibial
plateau. Surg. Gynecol. Obstet., 1165:457-462, 1963.
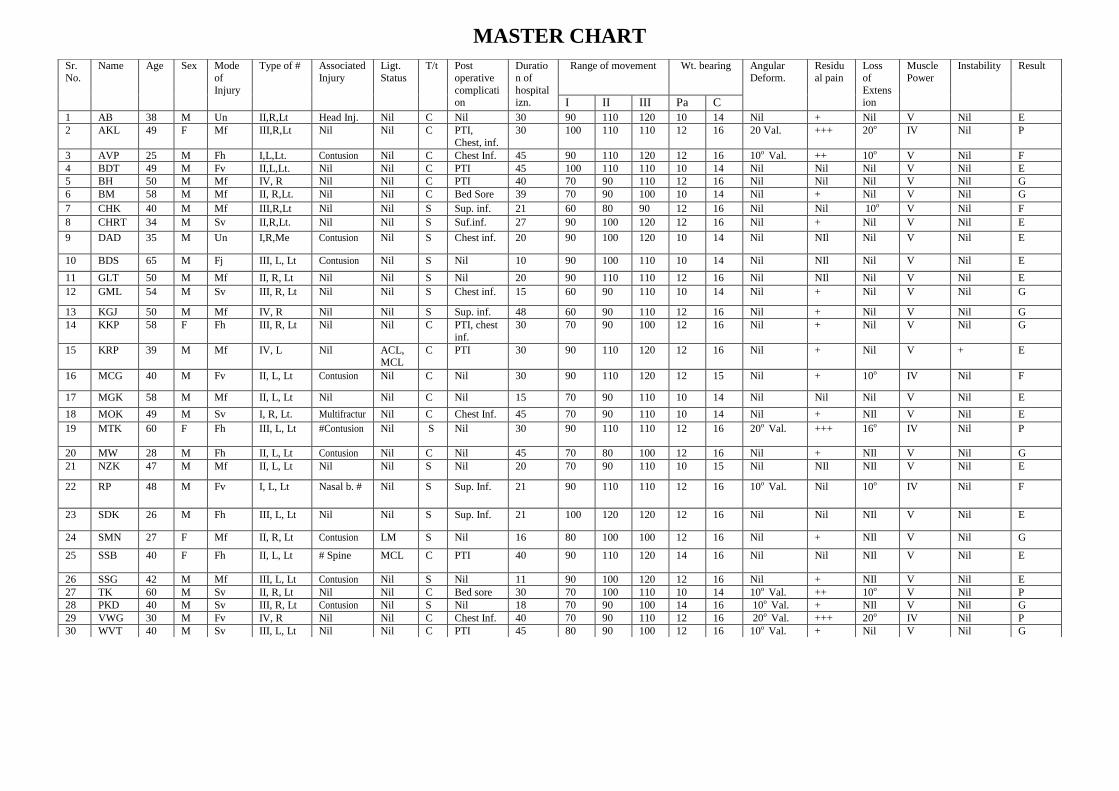
MASTER CHART
Sr.
No.
Name Age Sex Mode
of
Injury
Type of # Associated
Injury
Ligt.
Status
T/t Post
operative
complication
Duratio
n of
hospitalizn.
Range of movement Wt. bearing Angular
Deform.
Residu
al pain
Loss
of
Extension
Muscle
Power
Instability Result
I II III Pa C
1 AB 38 M Un II,R,Lt Head Inj. Nil C Nil 30 90 110 120 10 14 Nil + Nil V Nil E
2 AKL 49 F Mf III,R,Lt Nil Nil C PTI,
Chest, inf.
30 100 110 110 12 16 20 Val. +++ 20o IV Nil P
3 AVP 25 M Fh I,L,Lt. Contusion Nil C Chest Inf. 45 90 110 120 12 16 10o Val. ++ 10o V Nil F
4 BDT 49 M Fv II,L,Lt. Nil Nil C PTI 45 100 110 110 10 14 Nil Nil Nil V Nil E
5 BH 50 M Mf IV, R Nil Nil C PTI 40 70 90 110 12 16 Nil Nil Nil V Nil G
6 BM 58 M Mf II, R,Lt. Nil Nil C Bed Sore 39 70 90 100 10 14 Nil + Nil V Nil G
7 CHK 40 M Mf III,R,Lt Nil Nil S Sup. inf. 21 60 80 90 12 16 Nil Nil 10o V Nil F
8 CHRT 34 M Sv II,R,Lt. Nil Nil S Suf.inf. 27 90 100 120 12 16 Nil + Nil V Nil E
9 DAD 35 M Un I,R,Me Contusion Nil S Chest inf. 20 90 100 120 10 14 Nil NIl Nil V Nil E
10 BDS 65 M Fj III, L, Lt Contusion Nil S Nil 10 90 100 110 10 14 Nil NIl Nil V Nil E
11 GLT 50 M Mf II, R, Lt Nil Nil S Nil 20 90 110 110 12 16 Nil NIl Nil V Nil E
12 GML 54 M Sv III, R, Lt Nil Nil S Chest inf. 15 60 90 110 10 14 Nil + Nil V Nil G
13 KGJ 50 M Mf IV, R Nil Nil S Sup. inf. 48 60 90 110 12 16 Nil + Nil V Nil G
14 KKP 58 F Fh III, R, Lt Nil Nil C PTI, chest
inf.
30 70 90 100 12 16 Nil + Nil V Nil G
15 KRP 39 M Mf IV, L Nil ACL, MCL
C PTI 30 90 110 120 12 16 Nil + Nil V + E
16 MCG 40 M Fv II, L, Lt Contusion Nil C Nil 30 90 110 120 12 15 Nil + 10o IV Nil F
17 MGK 58 M Mf II, L, Lt Nil Nil C Nil 15 70 90 110 10 14 Nil Nil Nil V Nil E
18 MOK 49 M Sv I, R, Lt. Multifractur Nil C Chest Inf. 45 70 90 110 10 14 Nil + NIl V Nil E
19 MTK 60 F Fh III, L, Lt #Contusion Nil S Nil 30 90 110 110 12 16 20o Val. +++ 16o IV Nil P
20 MW 28 M Fh II, L, Lt Contusion Nil C Nil 45 70 80 100 12 16 Nil + NIl V Nil G
21 NZK 47 M Mf II, L, Lt Nil Nil S Nil 20 70 90 110 10 15 Nil NIl NIl V Nil E
22 RP 48 M Fv I, L, Lt Nasal b. # Nil S Sup. Inf. 21 90 110 110 12 16 10o Val. Nil 10o IV Nil F
23 SDK 26 M Fh III, L, Lt Nil Nil S Sup. Inf. 21 100 120 120 12 16 Nil Nil NIl V Nil E
24 SMN 27 F Mf II, R, Lt Contusion LM S Nil 16 80 100 100 12 16 Nil + NIl V Nil G
25 SSB 40 F Fh II, L, Lt # Spine MCL C PTI 40 90 110 120 14 16 Nil Nil NIl V Nil E
26 SSG 42 M Mf III, L, Lt Contusion Nil S Nil 11 90 100 120 12 16 Nil + NIl V Nil E
27 TK 60 M Sv II, R, Lt Nil Nil C Bed sore 30 70 100 110 10 14 10o Val. ++ 10o V Nil P
28 PKD 40 M Sv III, R, Lt Contusion Nil S Nil 18 70 90 100 14 16 10o Val. + NIl V Nil G
29 VWG 30 M Fv IV, R Nil Nil C Chest Inf. 40 70 90 110 12 16 20o Val. +++ 20o IV Nil P
30 WVT 40 M Sv III, L, Lt Nil Nil C PTI 45 80 90 100 12 16 10o Val. + Nil V Nil G

ABBREVIATIONS
1. Acl : Anterior Cruciate ligament
2. C : Complete
3. E : Excellent
4. F : Fair
5. Fh : Fall from height
6. Fv : Fall from vehicle
7. G : Good
8. Inf : Infection
9. Lm : Lateral meniscus
10. Lt : Lateral
11. Mcl : Medial collateral ligament
12. Me : Medial
13, Mf : Minor fall
14. P : Poor
15. Pa : Partial
16. Sv : Struck by vehicle
17. Un : Unknown
18. Val : Valgus
19. Var : Varus
