management of treatment-resistant schizophrenia
TRANSCRIPT

Ismail sadek
Management of Treatment -Resistant Schizophrenia

- 3rd cause of years lived with disability. - Major handicap in social, family and professionnal life.
A chronic and debilitating illness …- Lifetime prevalence of around 1%.- Beginning : 16 - 30 years.- High mortality rates with a loss of 12 to 15 years of life
expectancy
…potentially treatment resistant- Partial response to pharmacological interventions (30 à 60%).- Longer hospitalisations, direct and indirect cost, worsened quality of life.
Introduction
Clinical Point
Before concluding that a patient is treatment-resistant, consider medication adherence and possible substance use
Defining treatment resistance
The label "treatment resistance" is used particularly to refer to patients
whose positive symptoms of schizophrenia (including delusions and
hallucinations) have not responded to treatment.
The focus on positive symptoms has arisen largely because other
domains were either
Not clinically well recognised or understood (eg, cognitive symptoms), or
Considered to be unresponsive to treatment (eg, negative symptoms
such as amotivation, apathy, social withdrawal, blunted affect and
poverty of speech).

Research reports regarding treatment-resistant schizophrenia have relied on operational criteria such as:at least 3 periods of treatment in the preceding 5 years with neuroleptic
agents from at least 2 different chemical classes at dosages equivalent to ≥1000 mg/d of chlorpromazine for 6 weeks, each without significant symptomatic relief, and
no period of good functioning within the preceding 5 years.In that study, patients also underwent a prospective treatment trial with
what we now know are high doses of haloperidol (up to 60 mg/d or higher) and benztropine mesylate (6 mg/d) for a period of 6 weeks to confirm lack of drug responsiveness.

The most clinically relevant definition of treatment
resistance depends on the patient’s individual
circumstances. For some patients, targeting positive
symptoms is a high priority; for others it may be negative
and cognitive symptoms; for others, it may be excitement.
Moreover, families may complain of symptoms or behavior
that are of little or no concern to your patient.
At present, a uniform definition of treatment resistance in
the pharmacotherapy of schizophrenia is not available.
Most treatment guidelines require the failure of at least
two antipsychotic trials with different compounds, including
at least one second-generation antipsychotic, in adequate
dose over a period between 2 and 8 weeks before
treatment resistance can be assumed

It is interesting to note that a neuroimaging study using
[18F]-DOPA positron emission tomography scanning
examined the underlying neurobiological pathophysiology
of resistance to antipsychotic medication by comparing
non-responsive patients with those who had responded
adequately to antipsychotics and healthy volunteers.
Neuroimaging

In this investigation, the dopamine synthesis capacity was lower in participants
with treatment-resistant schizophrenia than in those with sufficient response to
antipsychotic medication.
Moreover, there was no significant difference between participants with
treatment-resistant schizophrenia and healthy volunteers.
These findings suggest that a medication aimed to achieve a blockade of
dopamine receptors may be effective especially in patients who have an elevated
dopamine synthesis capacity but less efficacious in patients with relatively normal
levels of dopamine synthesis capacity and in treatment-resistant patients.
Neuroimaging

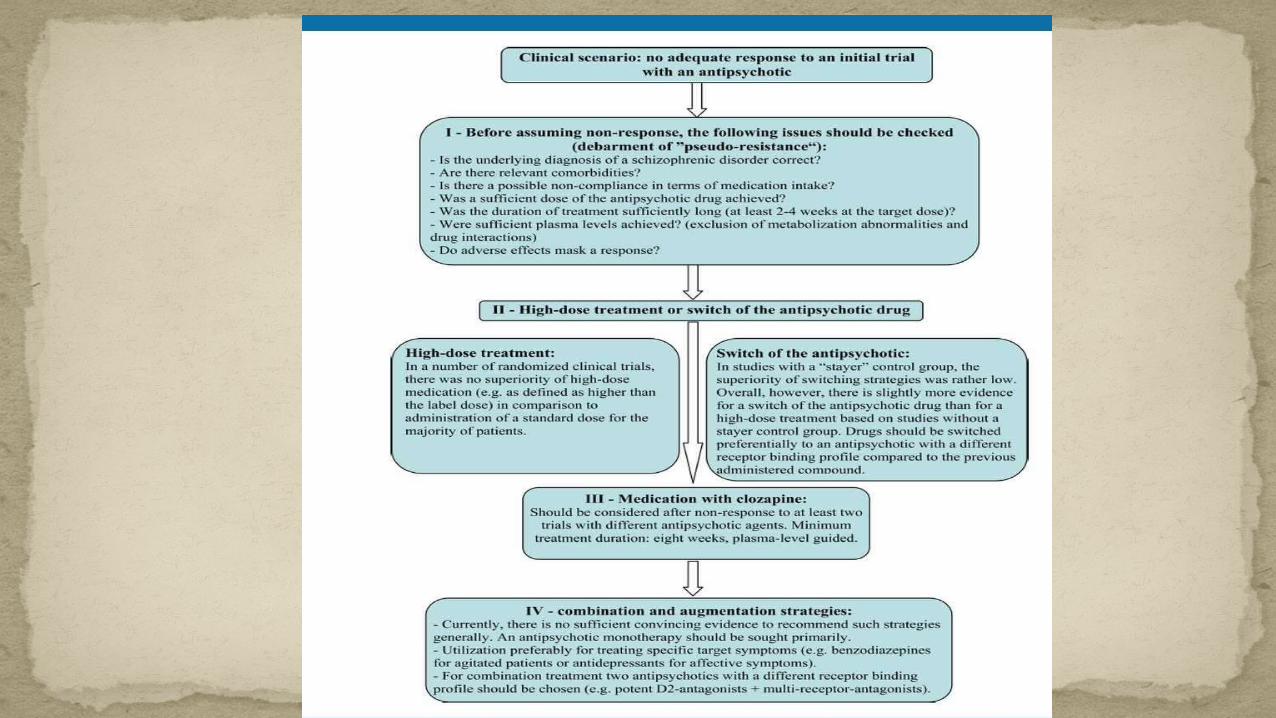
1.Re-evaluation of the diagnosis of a schizophrenic disorder.
Particularly severe personality disorders,
mania or depressive disorders with psychotic features are in
their acute phase sometimes difficult to distinguish from
schizophrenia.
Similarly, brain tumours and encephalopathies can cause
psychotic states.
Furthermore, substance abuse might need to be ruled out.

Non-compliance or non-adherence can be considered as a major reason for non-response to antipsychotic medication. It has been assumed that more than half of the patients do not take the prescribed medication correctly.
To objectify compliance and adherence in terms of medication intake, plasma levels should be considered.
The use of long-acting injectable antipsychotics can sometimes be a possibility to rule out non-adherence
2.Possible non-compliance of the patient regarding medication intake.
Recommended doses, based on an international consensus survey,
Patients with first-episode schizophrenia as well as older patients often require lower doses.
The onset of symptom improvement may vary considerably between individual patients.
International pharmacological guidelines recommend a minimum medication period between 2 and 8 weeks until in case of insufficient response a change of the treatment strategy should be considered.
3.Was the antipsychotic dose sufficient and the treatment duration adequate?

For example, akathisia can be misinterpreted as mental
agitation or parkinsonism may mimic schizophrenic
negative symptoms.
4.Side effects of antipsychotics can mask treatment response.
Currently, there is no convincing evidence for a clear relationship
between drug concentrations in the blood and antipsychotic response,
and an exact dose titration guided by therapeutic drug monitoring (TDM)
may be justified for clozapine, at best.
However, plasma level measurements may be useful in clinical practice
in case of inefficacy of the medication or occurrence of severe adverse
effects even at low doses.
Blood for drug concentration measurement should be withdrawn ideally
before ingestion of the morning dose.
5.Were sufficient plasma levels achieved?

Applying TDM, metabolisation abnormalities as well as insufficient
compliance of the patient can be identified or excluded as reason for
treatment failure.
Polymorphisms in the cytochrome P450 enzyme system, which is
responsible for the metabolisation of most psychotropic drugs, can be also
detected. On the one hand, increased enzyme activity can cause an
accelerated metabolisation of the drugs ('ultrarapid metaboliser', about 1%
of the population), on the other hand, reduced enzyme activity can cause
a slower metabolisation ('poor metaboliser', about 5% of the population).
5.Were sufficient plasma levels achieved?
Clinically relevant in this context is the interaction between
smoking and a medication with drugs that are metabolised
mainly by the cytochrome P450 isoenzyme 1A2 such as the
antipsychotics clozapine and olanzapine. As smoking
induces this isoenzyme, the clearance of these compounds
can be increased significantly. Therefore, a dose escalation
may be necessary to achieve the therapeutic window.
5.Were sufficient plasma levels achieved?

In case of non-response to an initial antipsychotic drug
treatment, two strategies that are often used in clinical
routine care are a dose increase of the current
administered antipsychotic agent (dose escalation, high-
dose treatment) and a switch to another, new
antipsychotic drug
Dose Increase or Switching of the Antipsychotic Drug

A high-dose treatment with an increase of the antipsychotic dose above the officially approved dose range (off-label dose, dose escalation) cannot be recommended as general treatment option for the management of treatment-resistant schizophrenia.
With regard to first-generation antipsychotics many clinical studies and systematic reviews concluded that a daily dose more than 800–1000 mg chlorpromazine equivalents does not improve antipsychotic efficacy but is associated with an increased incidence of especially extrapyramidal adverse effects.
Dose Increase
Use of high dose olanzapine in Treatment Resistant Schizophrenia
High dose olanzapine in TRSSince the late 1990s,
at doses between 25-45 mg/d -> as effective as clozapine (100-600mg/d) (Tollefson
et al., 2001; Bitter et al., 2004; Meltzer et al., 2008)
interesting for cognitive deficit and hallucinations, better social functionning (Qadri et
al., 2006 ; Reich, 2009)
Good tolerance even at very high doses (Batail et al., 2012; Batail et al., 2014)
a worthwhile alternative for clozapine-resistant or intolerant patients (Baldacchino
et al., 1998; Dursun et al., 1999; Martin et al., 1997; Rodriguez-Perez et al., 2002)
24

Question of the psychopharmacological mechanism behind the therapeutic response at such high doses ?
A STUDY ON PHARMACOKINETICS OF HIGH DOSE OLANZAPINE IN PATIENT SUFFERING FROM SCHIZOPHRENIA
Pharmacokinetics ?
Pharmacodynamics ?
Comparison of pharmacokinetics of olanzapine at both conventional and high doses.
?
25
Although a switch of the currently administered
antipsychotic drug is an often employed step in case of
non-response,
the question of the effectiveness of switching from one
antipsychotic drug to a second (each as monotherapy) is
still open.
Switching the Antipsychotic Drug
For switching the antipsychotic drug, it is recommended to taper off the
dose of the first antipsychotic gradually while simultaneously the dose
of the second one is titrated up gradually to its target dose ('crossover
titration'). Alternatively, the dose of the first antipsychotic can be
maintained at the same dose while the dose of the second compound is
increased gradually to a therapeutic level and only then the dose of the
first agent will be decreased ('overlap and taper')
Switching the Antipsychotic Drug

Following pharmacodynamic considerations in case of
switching, it seems preferable to choose a new compound
with a different receptor-binding profile compared to the
first administered agent (eg, a drug with high serotonergic
properties such as quetiapine, if the first compound was
characterised by high affinities to dopamine receptors
such as amisulpride, risperidone or a first generation
antipsychotic agent).

Clozapine, the gold standard
30

Clozapine, the gold standard- Cloza vs First Generation Antipsychotics (FGA):
=> cloza > FGA (relapse rates and repeated hospitalisations) (Meltzer et al., 2008).
- Cloza vs Second Generation Antipsychotics (SGA):
- Cloza > all SGA except olanzapine (OLZ) (Phase II CATIE).
- Cloza > OLZ on suicidal behaviors (Intersept: Meltzer et al., 2003)
- „ pro-cognitive “ effects of OLZ > cloza (anticholinergic properties).
- Tolerance: a limitation of its use (weight, metabolic disturbances,
agranulocytosis, sedation).31

A large number of clinical trials were conducted to elucidate which
antipsychotic is characterised by the highest antipsychotic efficacy.
The second-generation antipsychotics clozapine, amisulpride,
olanzapine and risperidone appear to be slightly more effective in
terms of antipsychotic efficacy than the other antipsychotic drugs.
Pharmacotherapy With Clozapine
However, with the exception of clozapine the differences
in effect sizes are small. In a network meta-analysis
comprising 212 randomised trials and a total of 43,049
patients with schizophrenia, clozapine achieved the
highest effect size in terms of antipsychotic efficacy
followed by amisulpride, olanzapine and risperidone.
Pharmacotherapy With Clozapine
clozapine is currently classified as first-line treatment in treatment-
resistant schizophrenia. This advice is corroborated by an early meta-
analysis that investigated exclusively treatment-resistant participants
and determined that only clozapine was significantly more efficacious
than first-generation antipsychotics.
Similarly, clozapine resulted superior to other second-generation
antipsychotics in a phase II study of the CATIE trial and in the 'Cost
Utility of the Latest Antipsychotic Drugs in Schizophrenia Study
(CUtLASS 2)' when analysing schizophrenic symptom improvement
A first dose of 6.25 mg is given on a Monday morning, and the patient remains at the bed for 3 h.
If there is no significant change in observations, the patient is given the evening dose to take home with them and leaves the department. The patient then self-administers their evening dose at home, just prior to going to bed at night.
On subsequent days, depending on their physical observations and side–effects, patients will wait in the department for 1–2h after taking their morning dose. Patients will attend 5 days a week for the first 2 weeks, after which the frequency of attendance can be gradually reduced if it is well tolerated.
A sample titration chart for the first 2 weeks. For subsequent weeks,
dose increases occur at a rate of 25 mg a day, depending on
tolerability. After 2 weeks of treatment, clozapine plasma
concentrations are checked.
Dosage increases should be titrated against tolerability, clinical
response, and plasma concentration. The average dose in the UK is
around 450 mg/day ; how-ever, interindividual variability is substantial
and the effective dose can range from 150 to 900 mg/ day
Significant effect sizes were also found for the second-generation antipsychotics risperidone, olanzapine and amisulpride.
some treatment guidelines recommend explicitly a treatment preferably with olanzapine or risperidone
The Role of Other Second-generation Antipsychotics in Treatment-resistant Schizophrenia

When Clozapine fails …
• BPRS improvement of < 20% despite a trial with clozapine for ≥ 8 weeks and plasma levels > 350 μ g/L, no stable period of good social and/or occupational functioning for ≥ 5 years,
• Global Assessment of Functioning (GAF) ≤ 40, • BPRS total score ≥ 45, • CGI score ≥ 4, and a score of ≥ 4 on 2 of 4
positive symptom items.
Ultra-resistant schizophrenia

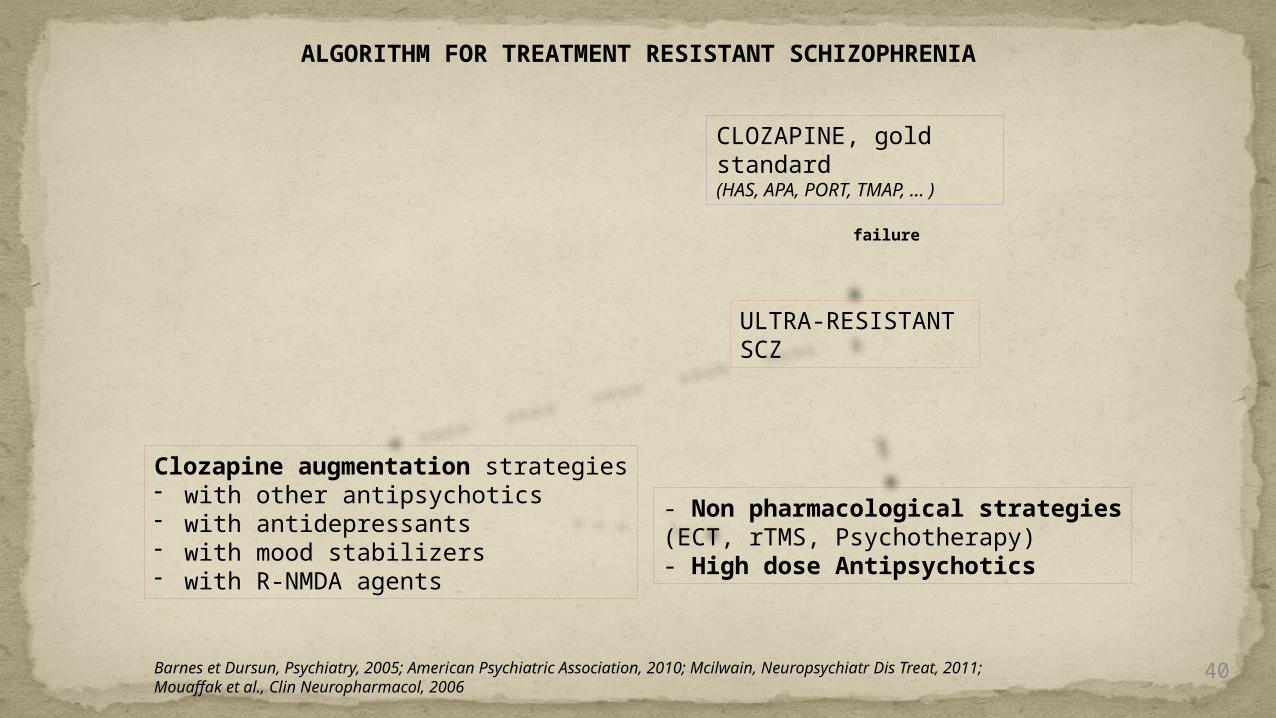
ALGORITHM FOR TREATMENT RESISTANT SCHIZOPHRENIA
CLOZAPINE, gold standard(HAS, APA, PORT, TMAP, … )
ULTRA-RESISTANT SCZ
Clozapine augmentation strategies- with other antipsychotics- with antidepressants- with mood stabilizers- with R-NMDA agents
- Non pharmacological strategies(ECT, rTMS, Psychotherapy)- High dose Antipsychotics
failure
Barnes et Dursun, Psychiatry, 2005; American Psychiatric Association, 2010; Mcilwain, Neuropsychiatr Dis Treat, 2011; Mouaffak et al., Clin Neuropharmacol, 2006
40
Pharmacological combination treatment is defined as the
simultaneous administration of two drugs of the same
group such as two antipsychotics
Combination Strategies

In meta-analysis by Sommer et al, stratified according to the various
compounds combined with clozapine, a significant positive effect was
determined only for sulpiride (based on a single trial) but not for
amisulpride, aripiprazole, risperidone and haloperidol.
Currently, clozapine is the most evaluated antipsychotic drug regarding
combination treatments.

Concerning the partial dopamine agonist aripiprazole,
there is no convincing evidence that a combination
treatment with this compound causes any improvement in
schizophrenic symptoms but it seems that cotreatment
with aripiprazole can reduce antipsychotic-induced
metabolic adverse effects as well as elevated serum
prolactin levels
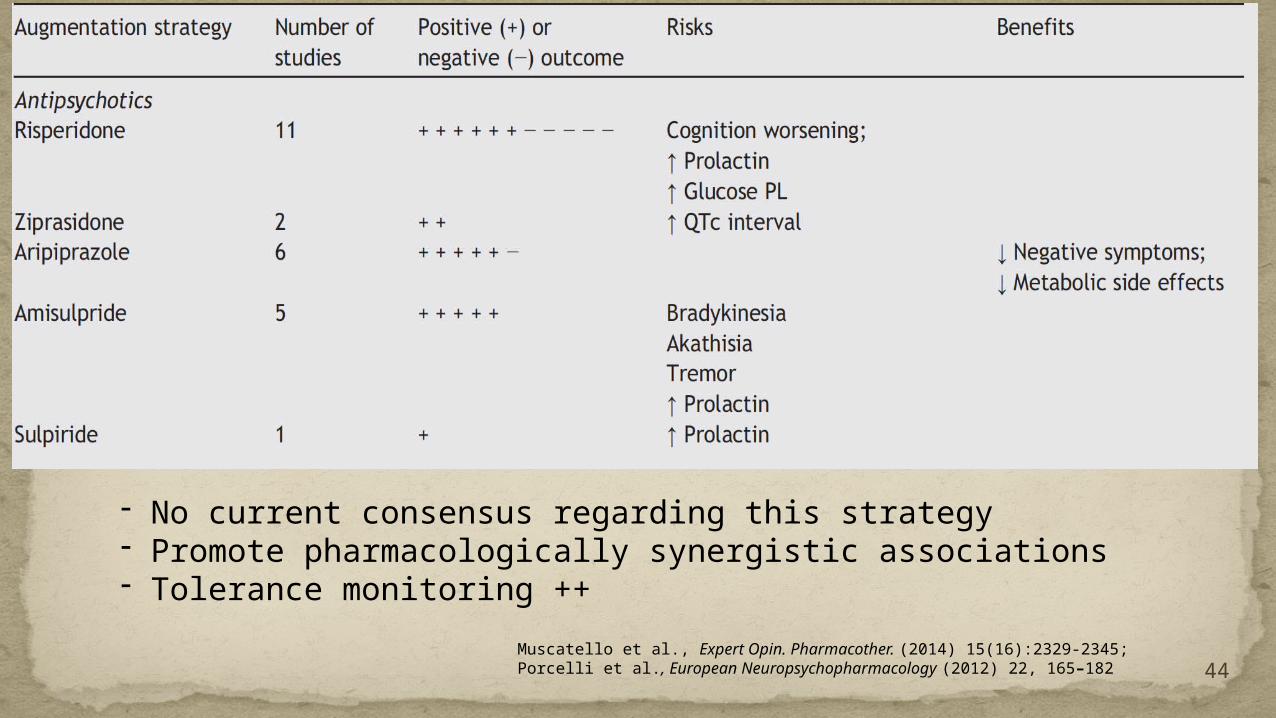
44Muscatello et al., Expert Opin. Pharmacother. (2014) 15(16):2329-2345;Porcelli et al., European Neuropsychopharmacology (2012) 22, 165–182
- No current consensus regarding this strategy- Promote pharmacologically synergistic associations- Tolerance monitoring ++
Augmentation treatment means the concomitant use of two drugs of
different classes, for example the coadministration of an antipsychotic
drug with an antidepressant, mood stabiliser or benzodiazepine.
Evaluated agents are, for example, acetylcholinesterase inhibitors, β-
blockers, carbamazepine, lithium, valproate and memantine.
Augmentation Strategies

Although benzodiazepines may be indicated in short-term treatment of
acutely agitated patients, there is no evidence for the use of
benzodiazepines as long-term adjunctive treatment to improve
psychotic symptoms
Augmentation Strategies

Sommer et al found in their meta-analysis a significant positive effect of
lamotrigine augmentation in clozapine-resistant schizophrenia but this effect
disappeared in a sensitivity analysis after exclusion of an outlier study with high
effect size and small sample size.
Similarly, a significant positive effect of topiramate on schizophrenic positive
symptoms diminished after removal of an outlier study.[36]
Very recent meta-analyses support augmentation with aspirin or other drugs with
effects on the immune system, but these findings are in our opinion not yet ready
for transfer into practice.
Augmentation Strategies
48
Clozapine augmentation strategies

49
Augmentation with mood stabilizers
Muscatello et al., Expert Opin. Pharmacother. (2014) 15(16):2329-2345;Porcelli et al., European Neuropsychopharmacology (2012) 22, 165–182
- Interisting in clozapine treated patients with high epileptic risk,- Schizo-affective disorder,- Favor valproate, take care of lithium (tolerance).
50
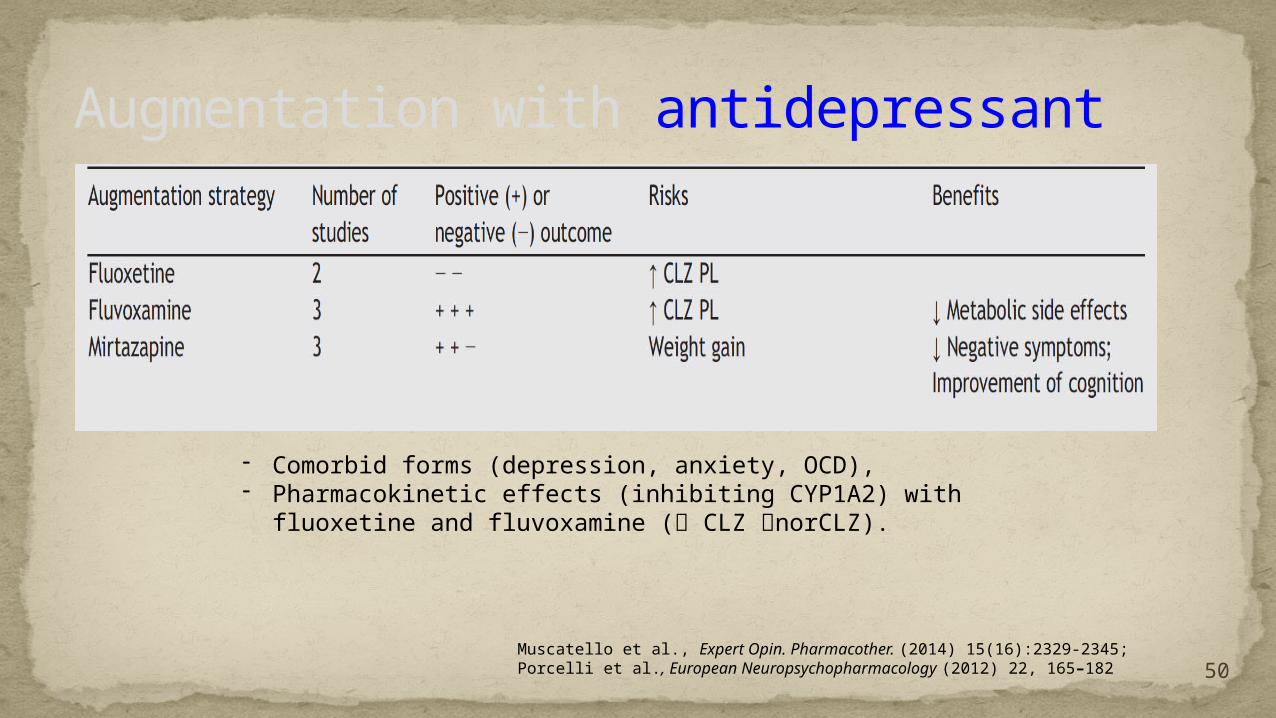
Augmentation with antidepressant
Muscatello et al., Expert Opin. Pharmacother. (2014) 15(16):2329-2345;Porcelli et al., European Neuropsychopharmacology (2012) 22, 165–182
- Comorbid forms (depression, anxiety, OCD),- Pharmacokinetic effects (inhibiting CYP1A2) with fluoxetine and
fluvoxamine ( CLZ norCLZ).

51
Augmentation with other agents
- Agent involved in glutamatergic transmission (glycine, D-serine, D-cycloserine, ampakine CX516, memantine, N-methylglycine), based on R-NMDA hypofunctionning hypothesis.
Muscatello et al., Expert Opin. Pharmacother. (2014) 15(16):2329-2345;Porcelli et al., European Neuropsychopharmacology (2012) 22, 165–182
augmentationglycine and D cycloserine: Much interest has surrounded the use of glycine
and partial agonists acting through the glycine site on NMDA receptors in the treatment of negative symptoms in schizophrenia. High doses of glycine (30-60 mg/day) have shown improvement in negative symptoms when added to antipsychotic medication.
Beta blockers: High dose propranolol up to 1200 mg/ day has been shown to augment antipsychotic efficacy in treatment refractory schizophrenia. It may produce its beneficial effect by its ability to treat akathisia, increasing antipsychotic serum levels, decreasing anxiety symptoms.

Galantamine: Because of the demonstration of a selective alpha nicotinic receptor abnormality in patients with schizophrenia, galantamine was added to the stable regimen of atypical and other antipsychotic medication in a study on a single patient by Rosse et al. Initially in doses of 4 mg bid (1 st week) which was increased up to 12 mg bid.
Galantamine is distinguished from other acetyl cholinesterase inhibitors by its positive allosteric modulatory properties, improving the efficiency of transduction of the acetylcholine signal at nicotinic receptors. This latter property may have contributed to the observed improvement in negative symptoms observed in this study Importantly, positive symptoms were unchanged during the 2-month trial.

The combined use of ECT and clozapine induces seizure
activity, this results in the reduction of psychotic symptoms.
Another possible explanation for the mechanism of
combined therapy with ECT and clozapine is a change in
the blood-brain barrier (BBB) permeability. An increase in
BBB permeability occurs following a seizure caused by
ECT.
Augmentation with ECT
The effectiveness of clozapine is dose–dependent (a higher
dose has a more benefit), but higher doses of clozapine are
associated with various side effects.
Thus, changes in BBB permeability as a result of ECT allow
greater amounts of clozapine to enter the brain without
systemic side effects. In this way, combination therapy with
ECT and clozapine results in a synergistic effect.
Augmentation with ECT

Cognitive-behavioural therapy (CBT) Supportive psychotherapy Psychodynamic psychotherapy Psychoeducation Family intervention Cognitive rehabilitation Social skills training Training in activities of daily living Occupational insertion support Housing resources
Psychosocial interventions
In CBT, the focus on understanding symptoms helps patients accept and continue medications.
Insight is approached systematically, and engagement with the patient is strongly emphasized.
There is often a focus on understanding the first episode when positive symptoms initially appeared, so that the patient has to make sense of these experiences.
To handle delusions, the therapist gathers information on current beliefs and the links between thoughts, feelings, and behavior.
Cognitive-Behavioral Therapy and Treatment-Resistant Schizophrenia

To conclude
Key points:
lack of definition
screening pseudo-resistance (therapeutic drug monitoring, non adherence, …)
pharmacological strategies
Clozapine, remains the gold standard
lack of evidence of pharmacological augmentation strategies
High dose olanzapine, a good alternative and experimental paradigm of TRS
Other alternatives
Non pharmacological therapies (neurostimulation, psychotherapy, …)
Pharmacological therapies modulating glutamatergic transmission

يرحمه الله
شكرا