management of women with clomiphene citrate resistant polycystic ovary syndrome dr seyed mehdi...
TRANSCRIPT


Management of Women with Clomiphene Citrate
Resistant Polycystic Ovary Syndrome
DR Seyed Mehdi Ahmadi
OB & Gynecologist
Isfahan Fertility & Infertility Center

Indications
I. Ovulation induction: in the following cases: a) C.C resistant PCO: Defined as failure to ovulate on a dose of 100 mg, for 5 days
(recently in 3 cycles, in contrast to 6 cycles in the past ) orfailure to ovulate on incremental doses of CC(50-150mg).
b) C.C failure PCO: Defined when pregnancy does not occur despite of regular
ovulation on C.C for 6-9 cycles.c) C.C pregnancy failure: Defined as failure to maintain pregnancy conceived with C.C.


IncreasedSerine
phosphorylation
Decreased glucose
transport
Hyperinsulinemia
P450c 17 &17,20 lyase
activity
Adrenals : Increased DHEAS
Ovaries : Increased
Androstenedione&testosterone

Various treatment modalities
Tre Pharmacological
CC
Gonadotropin Hyperinsulinemia?
hMG Insulin sensitizer
uFSH GnRH-analogs
HP-FSH
rec-FSH

A. Medical Treatment
Infertility is treated by increasing the rate of ovulation, in part by reducing insulin drive through exercise and weight loss .
Ovarian stimulation is used for those patients who do not ovulate, despite loosing weight by different drugs and different protocols.
Medical Treatment (cont.)
Treat Hyperprolactinaemia with Bromocriptine.
Glucocorticoids for adrenal hyperplasia .
( 0.25mg Dexamethasone at night )
COC pills or POP for dysfunctional uterine bleeding and to reduce the risk of endometrial carcinoma .

B. Surgical treatment modalities
Surgical Treatment
Cauterization Wedge resection
( laser, electric )

Methods of Ovarian Surgery For Ovulation Induction In PCOS
Laparoscopic Techniques of Ovarian Surgery (LOS) Laparoscopic Ovarian Drilling (LOD) :
Diathermy / LASER.
Transvaginal Techniques of Ovarian Surgery (TVOS) 1) Transvaginal mini-laparoscopy (Fertiloscopy)
2) Transvaginal ultrasound (TVS)-guided ovarian drilling.
LASER versus electrocautery for LOS:
Electrocautery IS superior why?
1) Less coast &easy application.
2) Achieve higher ovulation and pregnancy rate.
3) Less surface injury than CO2 LASER → Surface adhesion.
4) Effect of diathermy may last longer than the effect of LASER .

1) lifestyle modifications :
Weight loss Caffeine intake Alcohol consumption Smoking Dietary modification Exercise Psychosocial stressors

Role of weight loss in PCOS treatment:
Reduce insulin resistance by about 50%
Restore ovulation
Regulate menstrual cycles
Reduce pregnancy complications
Improve fertility
Improve health during pregnancy
Improve the health of a child during pregnancy
Improve emotional health (self-esteem, anxiety, depression)
Reduce risk factors for diabetes and heart disease

PROTOCOLS OF MANAGEMENT IN ADOLESCENTS
Counselling for weight reduction and life style modification.
Carbohydrate and fat restricted diet. Diet restriction and exercise is the sheet
anchor of treatment for overweight. Low glycemic index diet upto 85% will
improve menstrual cycle regularity and ovulation in about six months

Even 7% weight reduction may lead to spontaneous resumption of menses.
Moderate physical activity, 30-60 minutes per day should be goal of all patient with adolescent PCOS.M.O.A:-
lowers circulating free androgen and insulin levels. Increases SHBG, thereby decreases level of free
testosterone.
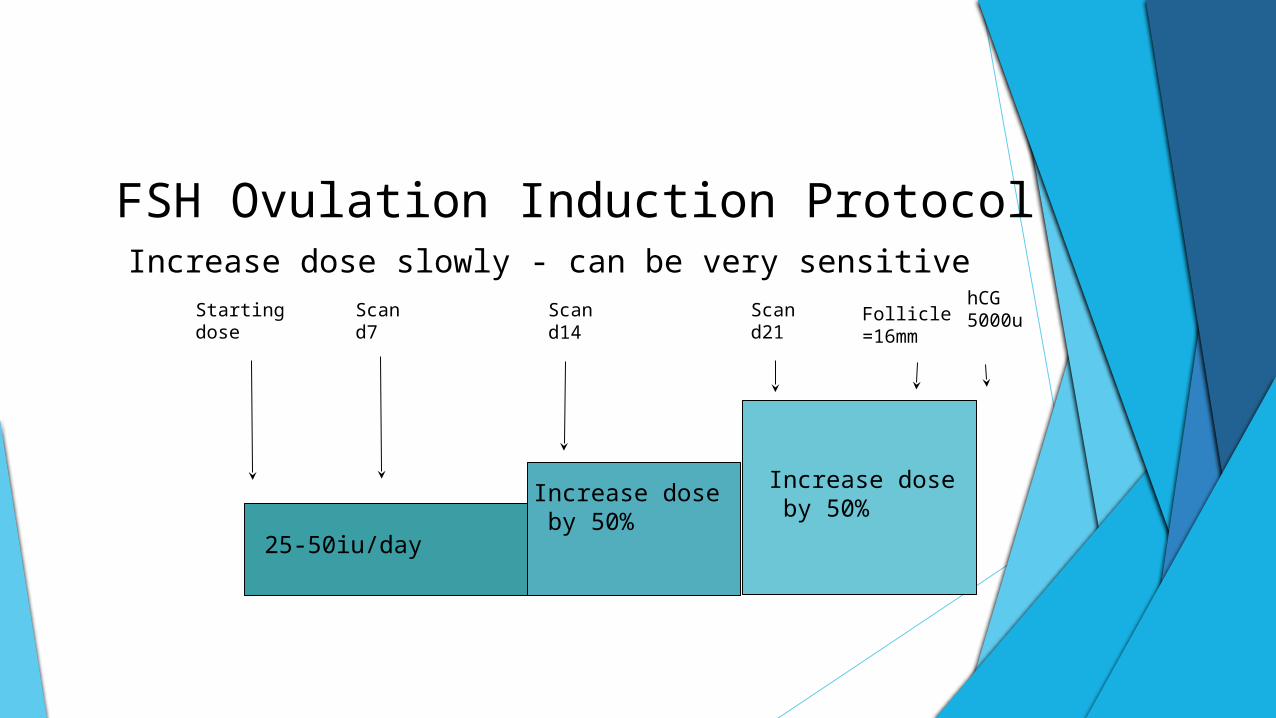
FSH Ovulation Induction ProtocolIncrease dose slowly - can be very sensitive
25-50iu/day
Increase dose by 50%
Increase dose by 50%
Startingdose
Scan d14
Scan d7
Scand21
hCG 5000uFollicle
=16mm


2) Gonadotrophins :
Ovulation induction with gonadotrophins has been used as a second line treatment for CC-resistant PCOS women.
Disadvantage : expensive/ requires extensive monitoring /risk for OHSS & multiple pregnancy .
The high sensitivity of the PCOS to gonadotrophic stimulation is: they contain twice the number of FSH -sensitive antral follicles than the normal ovary.
A lowdose,step-up gonadotrophin therapy should be preferred.
Recommended approach is :
begin with a low dose of gonadotrophin, (typically 37.5– 75 IU/day)
increasing after 7 days or more if no follicle >10 mm has yet emerged, in small increments, at intervals, until evidence of progressive follicular development is observed.
The maximum required daily dose of FSH/hMG seldom exceeds 225 IU/day.
There is no evidence of a difference between recombinant FSH (rFSH) and uFSH for ovulation induction in CC- resistant PCOS women.

3) Laparoscopic Ovarian Drilling
WHO BENEFITS FROMMechanism LEOS
• ?Removalresistant, CC androgen-producing tissueProblems Slim, Anovulatory ,
• Hazards of laparoscopic surgery & GA (although rare) raised S.LH
• TemporaryEfficacy
• <50% clomiphene-resistant women conceive (ovulation rate 80%+)
• Hormone profile returns to normal
• ?Fewer miscarriages compared to gonadotrophin injection treatment
3) Laparoscopic Ovarian Drilling (LOD):
Being as effective as gonadotrophin treatment and is not associated with an increased risk of multiple pregnancy or OHSS.
When applied properly, does not seem to compromise the ovarian reserve in PCOS women.
n economic evaluation has shown that the cost of a live birth after LOD is approximately one-third lower than the equivalent cost of gonadotrophin treatment.
Four punctures per ovary using a power setting of 30 W applied for 5s per puncture.

Unilateral LOD being equally efficacious as bilateral drilling in inducing ovulation and achieving pregnancy in CC resistant PCOS patients and may be regarded as a suitable option with the potential advantage of decreasing the chances of adhesion formation.
Mechanism : LOD drains the ovarian follicles containing
a high concentration of androgens and inhibin reduction of blood androgens and blood inhibin resulting in an increase of FSH and recovery of the ovulation function .

poor responders to LOD :
- Women with marked obesity (BMI >35 kg/m2)- Marked hyperandrogenism (serum testosterone
concentration >4.5 nmol/l- free androgen index (FAI) >15- long duration of infertility (>3 years)
Predictor of higher probability of pregnancy : LH levels >10 IU/l in LOD responders

Technique of Laparoscopic Ovarian Drilling

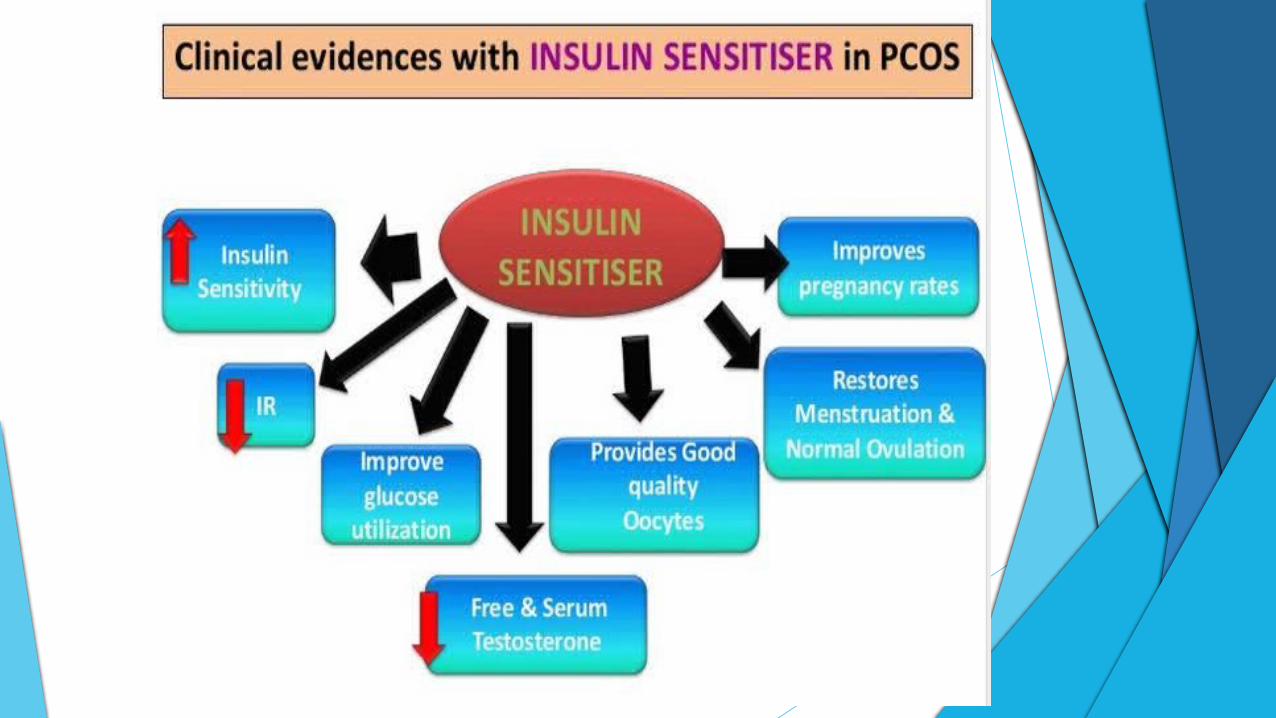
4) Insulin-sensitizing drugs :

IMPROVEMENT OF HYPERINSULINEMIA BY INSULIN
SENSITIZERS Directly sensitizing insulin receptors. Preventing neoglucogenesis. Reducing absorption of glucose from
intestine. Increasing hepatic synthesis of SHBG level
thereby reducing the level of bioactive free testosterone
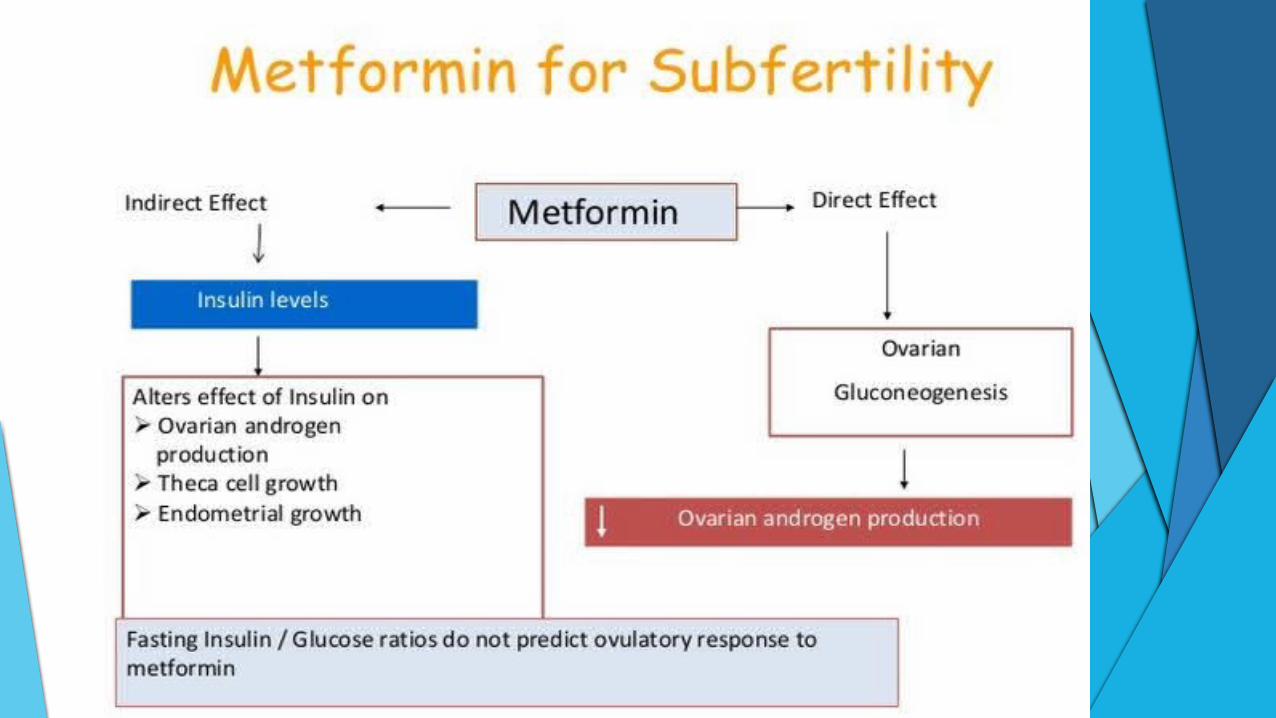
Metformin
Decreases basal hepatic glucose output in patients and lowers fasting plasma glucose concentration.
It increases the uptake and oxidation of glucose by adipose tissue as well as lipogenesis.
S/E- diarrhoea, nausea, vomiting ,specially initially. To avoid them metformin should be taken with meals and the dose increased gradually. Or SR release formulations are used once a day 1000 mg SR or 500mg SR twice a day
OTHER DRUGS WHICH CAN BE USED
• Rosiglitazone ,
• Pioglitazone,
• D chiro inositol,
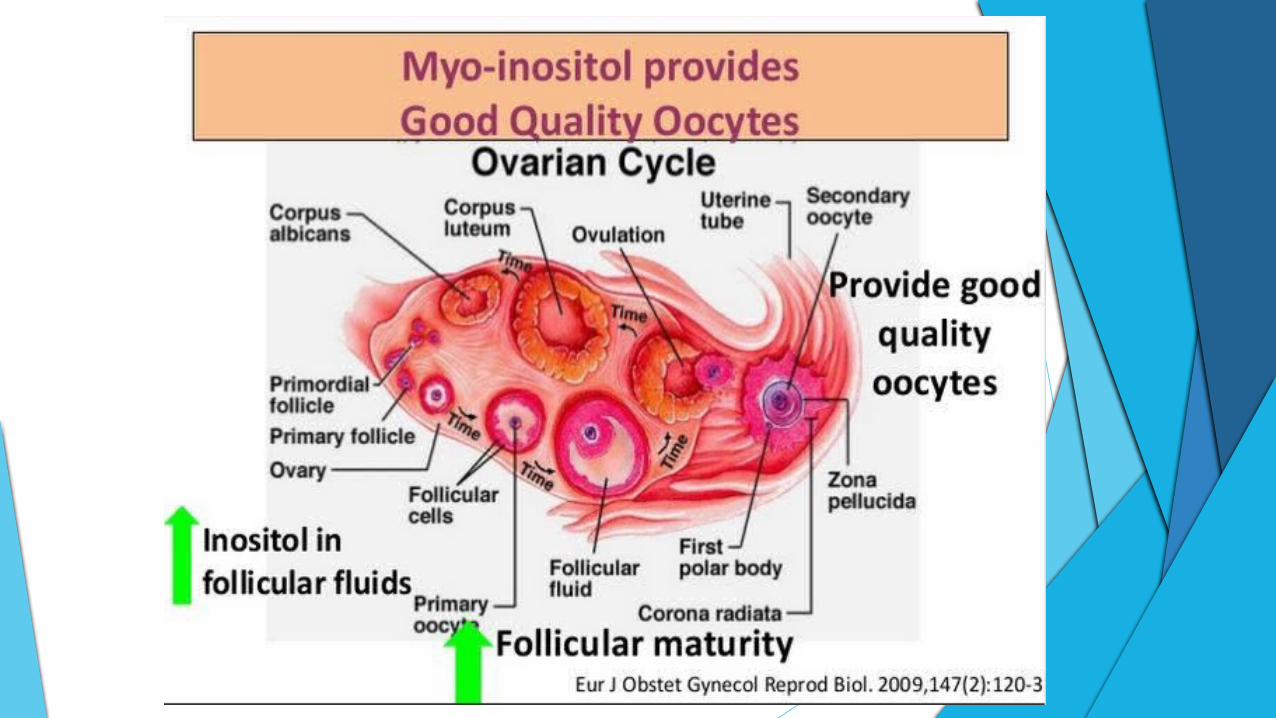
• Myoinositol
• N acetyl cysteine.
• Micronutrients

OTHER DRUGS WHICH CAN BE USED IN ADDITION TO O.C.P
In cases of failure or where there is clinical or biochemical evidence of gross hyperandrogenicity or hyperinsulinemia, addition of metformin is recommended.
Spironolactone- it has antiandrogenic effects in doses 100-200 mg daily.
Finasteride - a competitive inhibitor of Type-2 5a reductase to treat hirsutism. Dose 1-5 mg/day.





5) Third-generation aromatase inhibitors :
Anastrozole, Letrozole, Exemestane


DURING PREGNANCY
RECURRENT MISCARRIAGES 50% GESTATIONAL DIABETES PREGNANCY INDUCED HYPERTENSION INTRAUTERINE GROWTH RETARDATION

6) Oral contraceptives :
Oral contraceptive administration
reduce serum LH, estradiol and androgen levels
improving the ovarian microenvironment
Inhance ovarian response to CC

7) N-acetyl-cysteine :
N-acetyl cysteine (NAC) is the acetylated variant of the amino acid L-cysteine.
It is an excellent source of sulfhydryl groups and is converted in vivo into metabolites that stimulate glutathione production, promote detoxification, and act directly as free-radical scavengers.
combination of CC and NAC increases ovulation and pregnancy rates in CC-resistant PCOS patients who also suffer from infertility.
NAC has antiapoptotic effects on the ovary and apoptosis is definitely responsible for the process of follicular atresia.
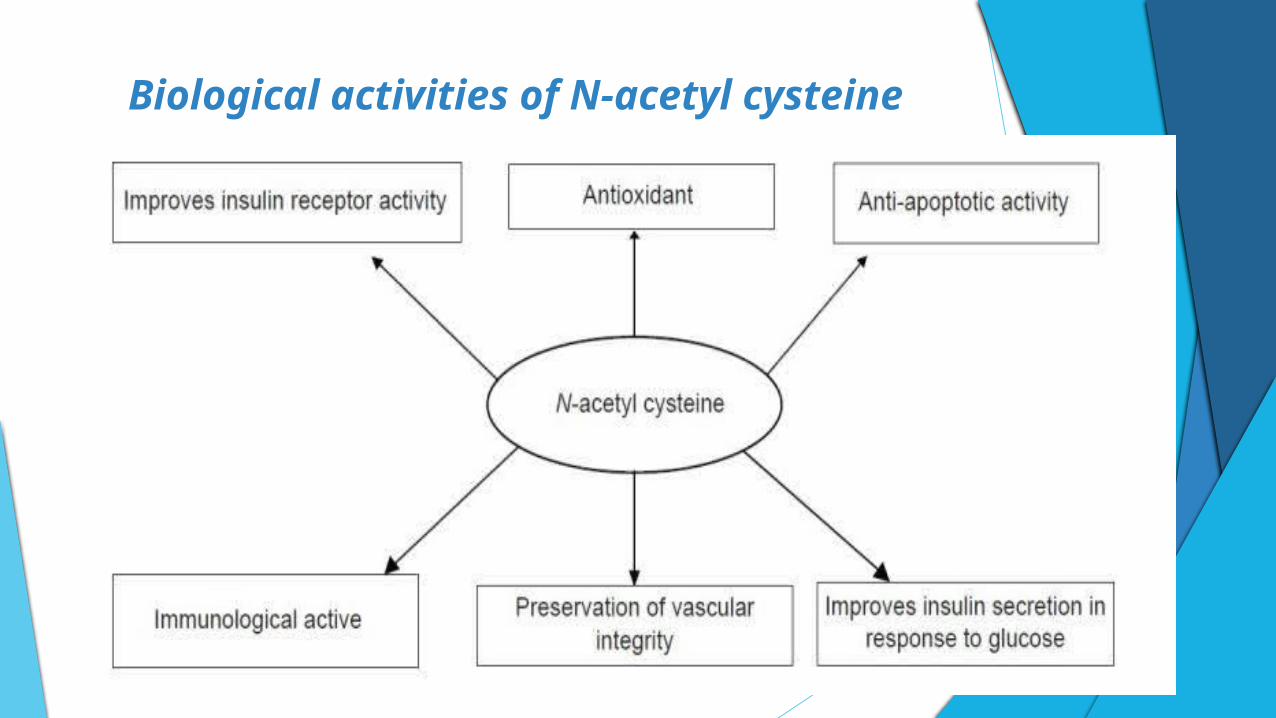
Biological activities of N-acetyl cysteine

8) Dexamethasone therapy :
Dexamethasone (after 2 weeks of treatment )
Reduced DHEAS
Reduced Testostrone
Reduced LH levels and the LH/FSH ratio
Inhance ovarian invironment

9) Bromocriptine :
Bromocriptine administration provided no benefit in CC-resistant PCOS patients with normal prolactin levels.
Bromocriptine administration improve ovarian response in hyperprolactinemic patients.
Dopaminergic components have control of LH release in PCOS patients

10) IVF/ET or IVM :
If all else fails for the infertile PCOS patient then in-vitro fertilization is a last resort providing excellent results.

33-50% OF PATIENTS REFERRED FOR IVF HAVE PCOS


MANAGEMENT
life style and exercises diet insulin sensitisers ocp’s progesterone for bleed statins/diabetes /antihypertensives if needed omega 3 and micronutrients(inositol or myoinositol or
n-actyl cysteine or alternative medicines

Algorithm for ovulation induction treatment in anovulatory infertile women with CC-resistant
PCOS