managing population health - institute for diversity · managing population health ... one solution...
TRANSCRIPT

Managing Population Health: Equity through Person-Centered Care

Linda Alexander, RN, MBA, CCM ● Total Health Care– Chief Clinical Officer ● Plante Moran – Healthcare Consulting ● Detroit Medical Center - Clinical
Operations, Physician Services, and Strategic Post-Acute Integration
● Henry Ford Health System – Nursing, Administration, Quality
● Model 2 Bundling Awardee – DMC 10/9/12

The Era of ACCOUNTABLE CARE---Catalyst for change
Snapshot of Reimbursement in US ● Medicare – 1966 –
Hospital-centric Care ● HMO Act of 1973 –
Managed Care ● Prospective Payment
System (PPS) ● Fee for Service ● PPACA-Healthcare
Reform ● Readmission
Reduction ● Bundled Payment ● ACOs
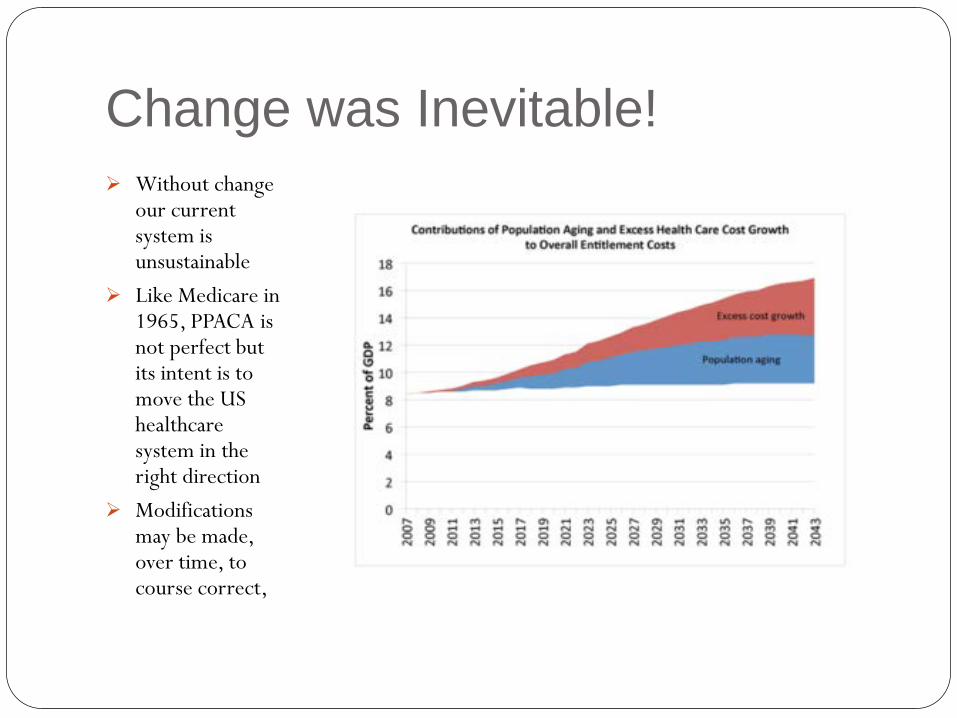
Change was Inevitable! Without change
our current system is unsustainable
Like Medicare in 1965, PPACA is not perfect but its intent is to move the US healthcare system in the right direction
Modifications may be made, over time, to course correct,
Patient Protection and Affordable Care Act
Full title The Patient Protection and Affordable Care Act.
Acronym PPACA
Colloquial name(s) Affordable Care Act, Healthcare Insurance Reform, Obamacare, Healthcare Reform
Enacted by the 111th United States Congress
Effective March 23, 2010 Specific provisions phased in through January 1, 2018
● The law is the principal health care reform legislative action of the 111th United States Congress.
● PPACA reforms certain aspects of the private health insurance industry and public health insurance programs, including increasing insurance coverage of pre-existing conditions, expanding access to insurance to over 30 million Americans that, financially, is achieved through subsidies by the federal government and increased enrollment in federal health care programs (increasing total national medical expenditures in the short term), and additional policy changes to reduce the long-term cost of health care.
Triple Aim Philosophy PPACA was created with a “triple aim” in mind:
1. Improve the health of patient populations
2. Improve patients’ experience of healthcare
3. Reduce per capita costs of healthcare “The components of ” the Triple Aim are not independent of each other. Changes pursuing any one goal can affect the other two sometimes negatively, sometimes positively” Donald Berwick, Triple Aim: Care,, Health and Cost; Health Affairs; 27, no. 3 (2008)

Three Key Components of PPACA
Accountable Care Organizations
Value-Based Reimbursement
Care Integration
Above components are designed to meet the Triple Aim.
Accountable Care Organizations • Primary Care (wellness & prevention) • Physician/hospital alignment • Quality outcomes • Community stakeholder collaboration • Data sharing/integration • Improved care transitions and
efficiency • Capitated payments
Value Based Purchasing
•Readmission reduction strategies •Integrated care delivery systems •Transparency of information – HIEs •Consumer-driven selection – HCAHPS •Cost containment •Linkages between quality and reimbursement
WHO OWNS THE PATIENT???
ACO/Bundled Payment Linkage
● The ACO is viewed by hospitals & physicians as a key strategy to adapting to changes under healthcare reform.
● Many healthcare executives & thought leaders view ACO’s + Value-based payments as a precursor to bundled payments for episodic care.
● Post-acute entities account for 25-30% of healthcare costs and must be prepared to deliver a “value-based” service that aligns with referring source priorities, as part of the episode of care.
ACO + VBP = SBP

Single Bundled Payment Single Bundled Payment is
defined as the reimbursement of health care providers, which may include post-acute, on the basis of expected costs for clinically- defined episodes of care.

MedPAC 2010
Why Post-Acute is Key
PAC Setting % D/C from Hospital to PAC
Setting
% Readmitted after PAC Setting
% D/C to 2nd PAC Setting
SNF 17.3 22.0 29.3
HHC 15.0 18.1 2.3
Acute Rehab 3.2 9.4 56.8
Hospice 2.1 4.5 2.4
LTACH 1.0 10.0 53.4
Psych 0.5 8.7 25.4
Total 40.0 18.0 19.8
ACO Integration for Post- Acute Post-Acute Providers seeking to
participate in the ACO era must integrate ACO programming goals to counteract the legacy of silo-based care present in the PPS Care Continuum. Clinical accuracy, staff control, and care insight required for value concerns are paramount.
The Silo Effect
The Silo effect refers to the lack of communication and support often found in acute care episodes. Provider types focus primarily on their own goals, often ignoring the needs of others.
Post-Acute Benefits to Accountable Care
Pre-PPACA : Focus to reduce LOS Follow hospital plan Payment for readmits Minimal transparency Poor coordination with post-acute
Post-PPACA : Integrate care with
continuing care partners Improve patient experience Decrease post-acute care
costs (SBP) Penalties for readmits Payment for quality
(episode) Increase transparency Selective network partners

Hospital Readmissions
Hospital Readmissions ●Symptom of expensive/uncoordinated system
●Hospitals benefit fiscally from readmits
●2 million-30 day readmits - $17.5 billion
●71% of hospitals penalized 2012 - $280 mil
●Penalties doubled 10/13 increase again 10/14
●Promote safe patient passage from acute care
●Viewed as a new indicator for quality
An acquired, transient period of vulnerability and risk in the critical first 30 days after DC. This period of clinical risk is connected as
much to the stresses of the inpatient admission as it is connected to lingering
effects of the original illness. Patients are not only recovering from their illness, but they are also in a phase of generalized risk for a series
of adverse events. NEJM, 2013
Post – Hospital Syndrome

Equity through Person-Centered Care
Managing the Population vs. Managing an Encounter
Population Health Management Person-centered approach to
care Episodic Care Delivery - looks at
continuum, not merely hospital stay
Holistic assessment and care management
Integrates hospital and community care providers
Evaluates outcomes for chronic disease management
Considers other factors (psychosocial, community) affecting population health
Episodic Care Delivery
The re-engineering of the acute episode derived from acuity-based expectations of patient care requirements, devoid of Provider preference, and driven by the least restrictive/costly care environment.

Critical Success Factors Plethora of theories emerging. Common themes include: Ability to improve patient behavior Establish trust in the community in which you want to
serve Ability to align health continuum partners Ability to leverage risk Access to care-systematic evaluation Talent to execute strategy** **Due to siloed care delivery systems, many healthcare leaders have segmented experience. Each segment of the continuum has unique challenges, payment systems, etc.

What can hospital leaders do today?
Integrated Care Network ICN, IHS, ICS, ACOs, IDN, CCN….. “A network of organizations that provides or arranges to provide a coordinated continuum of services to a defined population and is willing to be held clinically and fiscally accountable for the outcomes and health status of the population served.” Stephen M. Shortell, Ph.D. Dean – School of Public Health University of Cal-Berkley
Benefits of an ICS Additional revenue stream to offset volume reductions Hospitals can acquire new lines of business Risk-sharing to downstream providers can offset cost of
reducing utilization
Opportunity to lean into the curve, yet minimize risk Deliver better care, better outcomes Improve patient satisfaction Flexibility to start at your own pace Establish/expand accountability beyond hospital (take
ownership of patient care continuum)

Getting Started Adoption of Accountable Care Concepts Monitor care for an extended period of time (i.e. 30 days) Clinical care protocols, based on indicators vs. volume It is ok to start small!
Accountability and care coordination with downstream partners
Including quality as a key factor for selection of partners Consider risk-based models to drive change (shared savings) Be sure to include Behavioral Health

Integrating Care……Works! Bundled Payment Pilot Program Acute + Post-Acute for 30 day episode Joint Replacements Reduction of readmissions to 2% Savings of $600k during pre-pilot phase! Coordination with downstream/community partners Culture shift from “encounter” to “episode” Patient/caregiver engagement Physician alignment

Downstream Accountability is Critical Home Care: Start of care within 24 hours or less Shift care focus to self-care determination from dependence Clearly define clinical vulnerabilities and strengthen them Identify system/process for communication and coordination Data integration for sharing of clinical information Outcomes measurement and reporting – transparency Assist with education/development Develop processes for when things go wrong Home to SNF Visiting physician Easy outpatient access
Downstream Accountability, Part 2 SNF/Extended Care: Know the capabilities of your partners (frequency of
physician visits, competency level of staff, etc.) Ensure discharge orders are clear and complete Nurse to nurse report Physician oversight Establish goals of care prior to transfer Process to monitor goal-attainment and when to transition to
home or community LOS is based on clinical indicators not reimbursement
Community Connections Primary care coordination Behavioral health assessment and treatment Psychosocial wraparound services Area Agencies on Aging Community agencies Faith-based organizations
Patient education to support self-determination Support groups Maximize hospital-based case managers (i.e. Navigators)

In closing….. Healthcare Reform, driven by rising costs, seems to be here to
stay Post-acute and community integration is key for hospitals to
manage populations, including behavioral health Integrated Care Networks is one way that hospitals can begin
the shift from volume to value Leveraging risk can create alignment with physicians and
downstream providers
Innovation takes Courage “One isn’t necessarily born with courage, but one is born with potential. Without courage, we cannot practice any other virtue with consistency.” Dr. Maya Angelou, USA Today, 1988

Linda Alexander RN, MBA, CCM [email protected]
313-269-0438
Follow me on Twitter: @JAlex4Health
Thank you!