managing the red eye.ppt
TRANSCRIPT
MANAGING THE RED EYE
American Academy of Ophthalmology
NON-THREATENINGRED EYE DISORDERS
Subconjungtival hemorrhage Hordeolum Chalazion Blepharitis Conjunctivitis Dry eyes Corneal abrasion
VISION THREATENINGRED EYE DISORDERS
Corneal infection Scleritis Hyphema Iritis Acute glaucoma Orbital cellulitis

RED EYE : POSSIBLE CAUSE Trauma Chemicals Infection Allergy Systemic condition
RED EYE : CAUSE AND EFFECT Symptoms
o Itchingo Scratchiness, burning
o Localized lid tenderness
Causeo Allergyo Lid, conjunctival, corneal
disorder, including foreign body, trichiasis, dry eye
o Hordeolum, chalazion
RED EYE : CAUSE AND EFFECT (cont’d) Symptom
o Deep, intense pain
o Photophobia
o Halo vision
Causeo Corneal abrasion,
scleritis, iritis, acute glaucoma, sinusitis, etc
o Corneal abrasion, iritis, acute glaucoma
o Corneal edema (acute glaucoma, contact lens overwear)
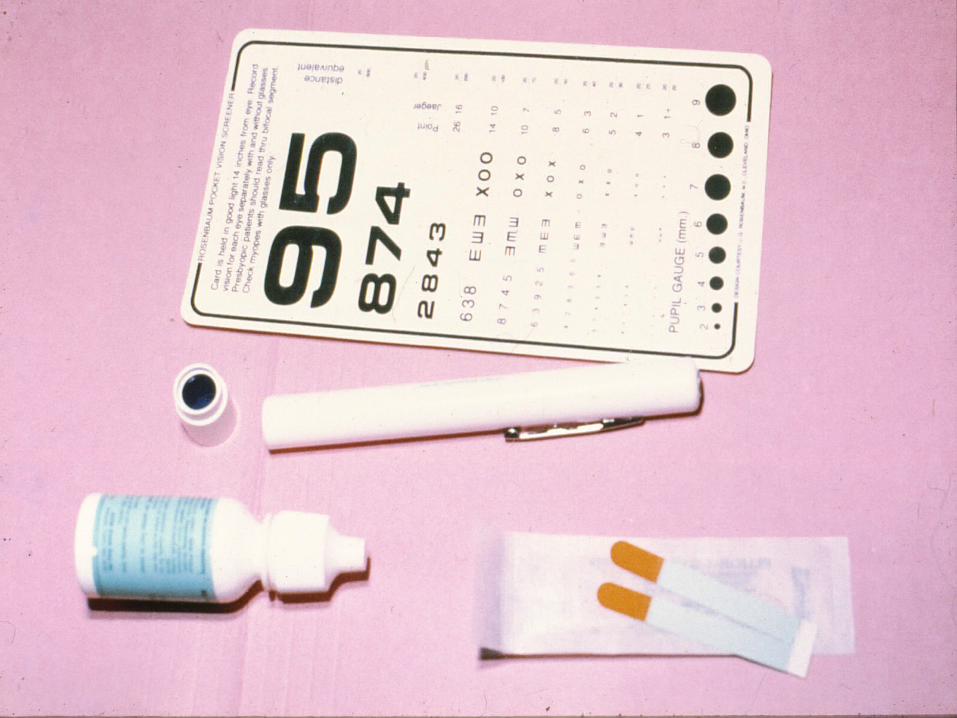

RED EYE EXAM :A SYSTEMIC APPROACH
Face Orbit Extraocular structure Ocular movement Eye

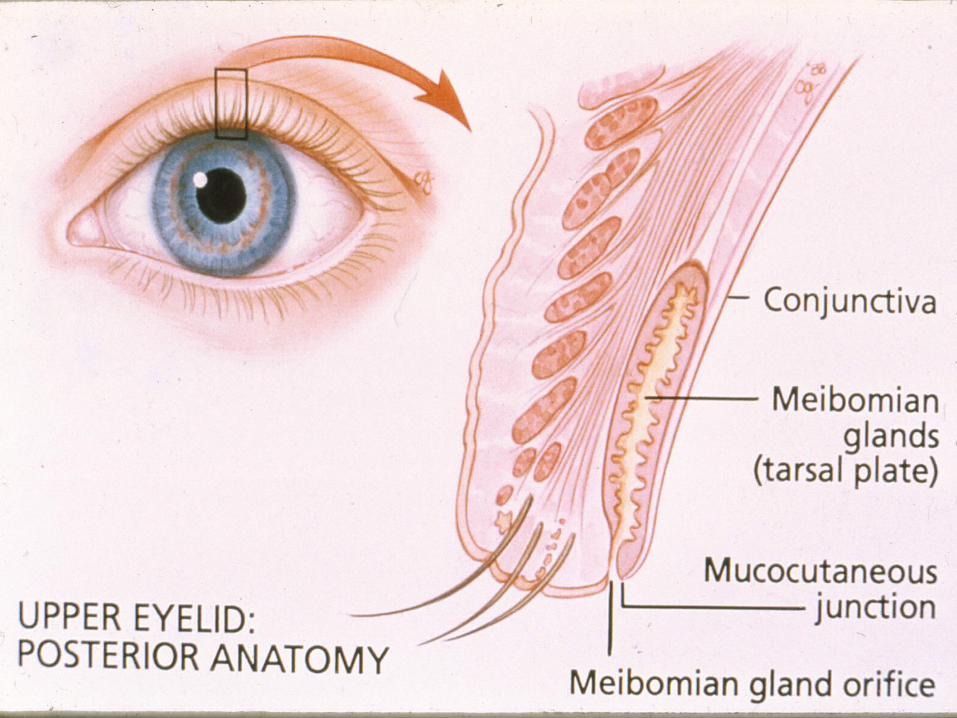
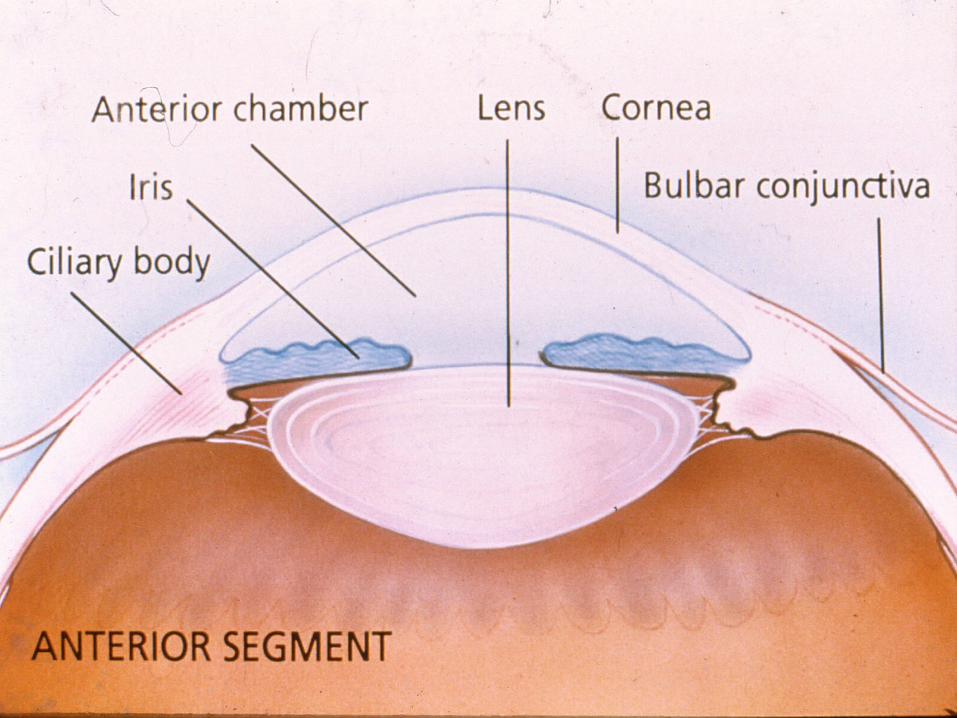
RED EYE DISORDERS :AN ANATOMICAL APPROACH
Lids Orbit Lacrimal system Conjunctiva/sclera Cornea Anterior chamber
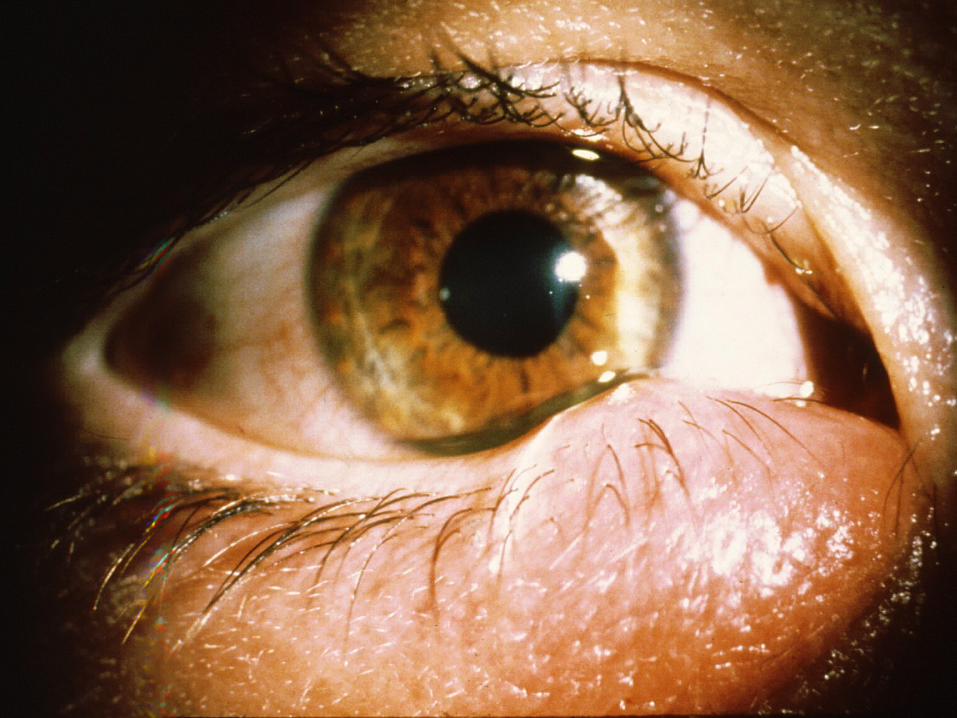

HORDEOLUM / CHALAZION : TREATMENT Goal
To promote drainage
Rx Acute/subacute: warm
compresses tid Chronic: refer to an
ophthalmologist
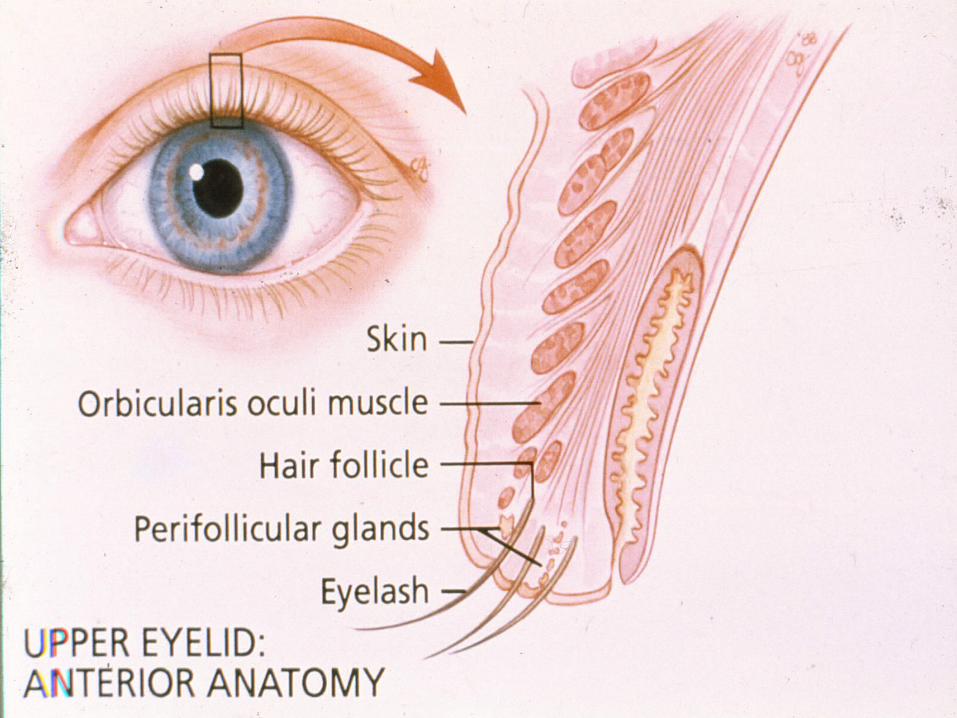
BLEPHARITIS Chronic inflammation of lid margin Types: staphyloccocal, seborrheic, or a
combination Symptoms : foreign body sensation,
burning, mattering
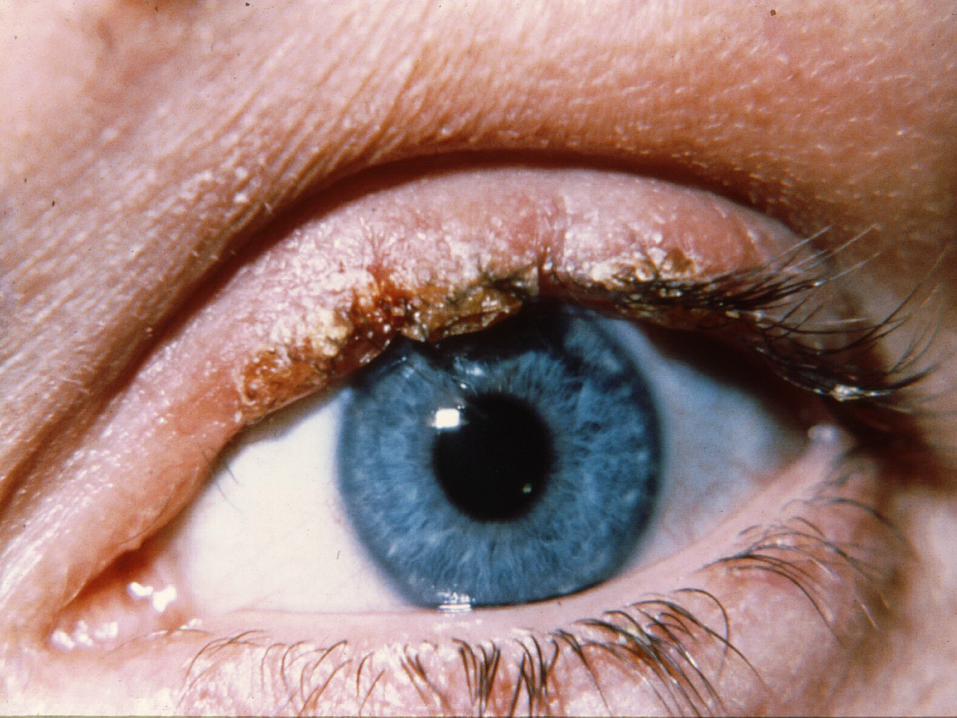
BLEPHARITIS : TREATMENT Lid hygiene: warm compresses, cleansing
with nonirritating shampoo Antibiotic ointment hs x 2-3 weeks



ORBITAL CELLULITIS External signs : redness, swelling Motility : impaired, painful + proptosis + optic nerve: decreased vision, afferent
pupillary defect, disc edema
ORBITAL CELLULITIS :MANAGEMENT
1. Hospitalization
2. Eye consult
3. Blood culture
4. Orbital CT scan
ORBITAL CELLULITIS :TREATMENT
IV antibiotics stat : staphylococcus, streptococcus, H influenza
Surgical debridement if fungus, no improvement, or subperiosteal abscess
Complications: cavernous sinus thrombosis, meningitis
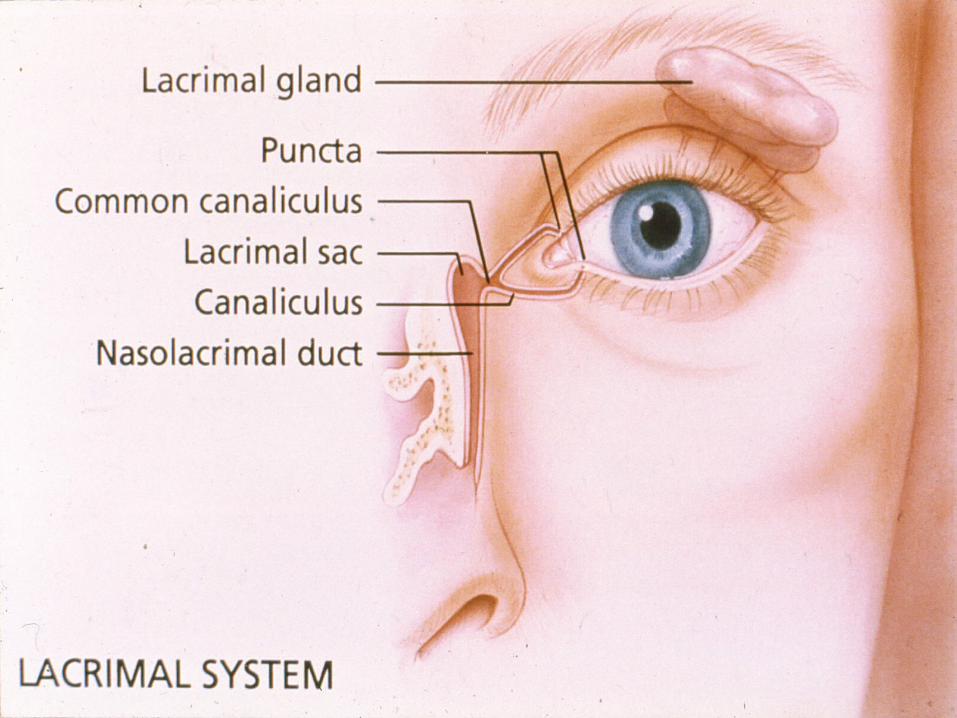

NASOLACRIMAL DUCT OBSTRUCTION : CONGENITAL
Massage tear sac daily Probing, irrigation if chronic Systemic antibiotics if infected
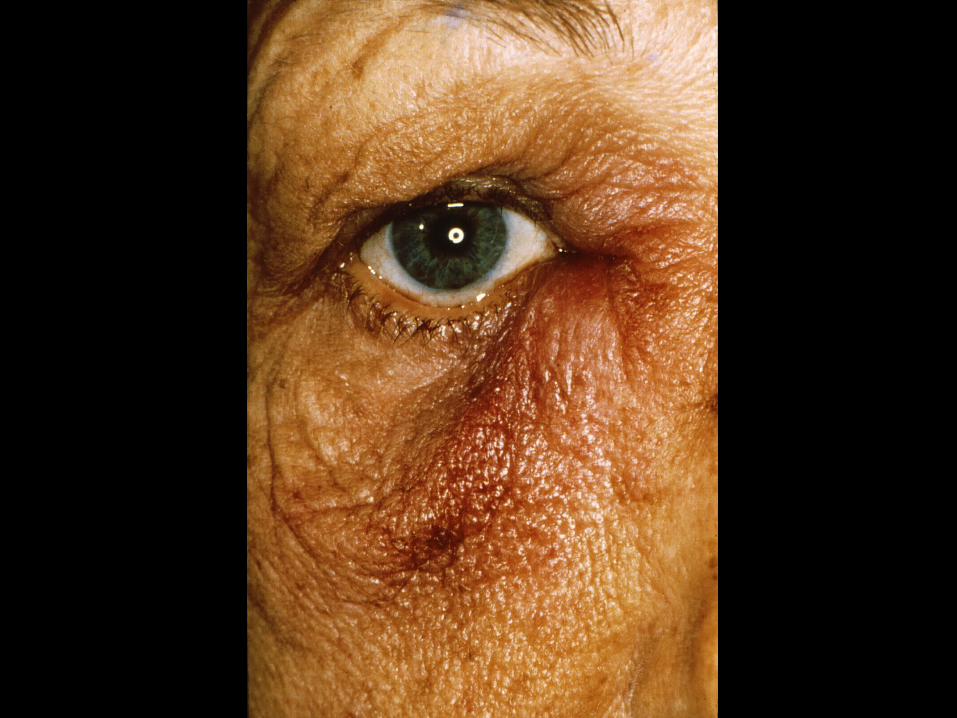
NASOLACRIMAL DUCT OBSTRUCTION : ACQUIRED
Trauma a common cause Systemic antibiotics if infected Surgical procedure
(dacryocystorhinostomy) prn
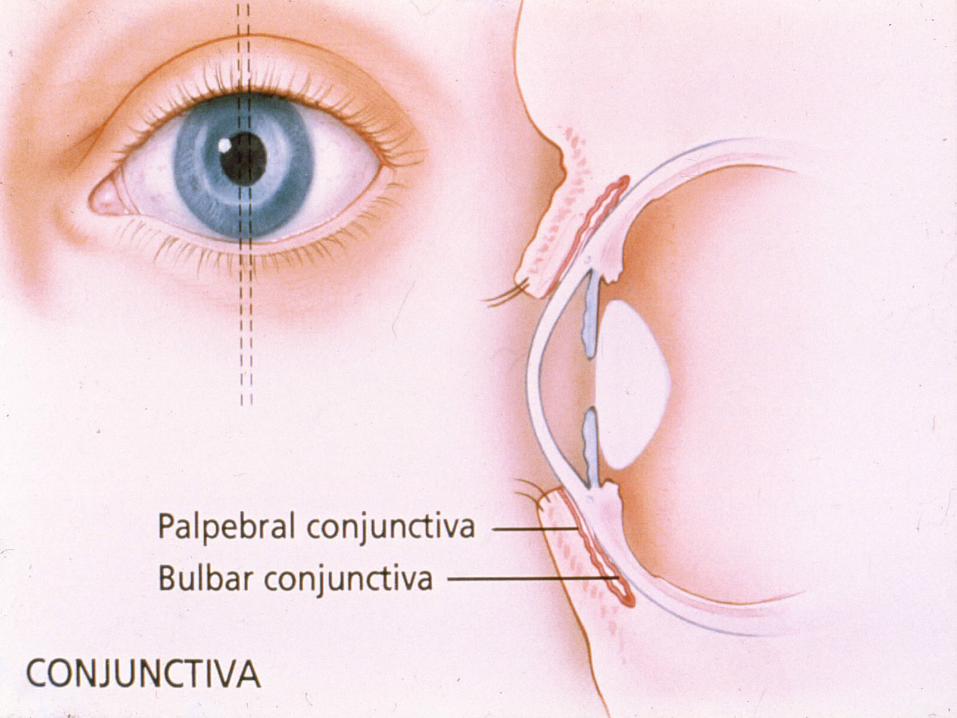

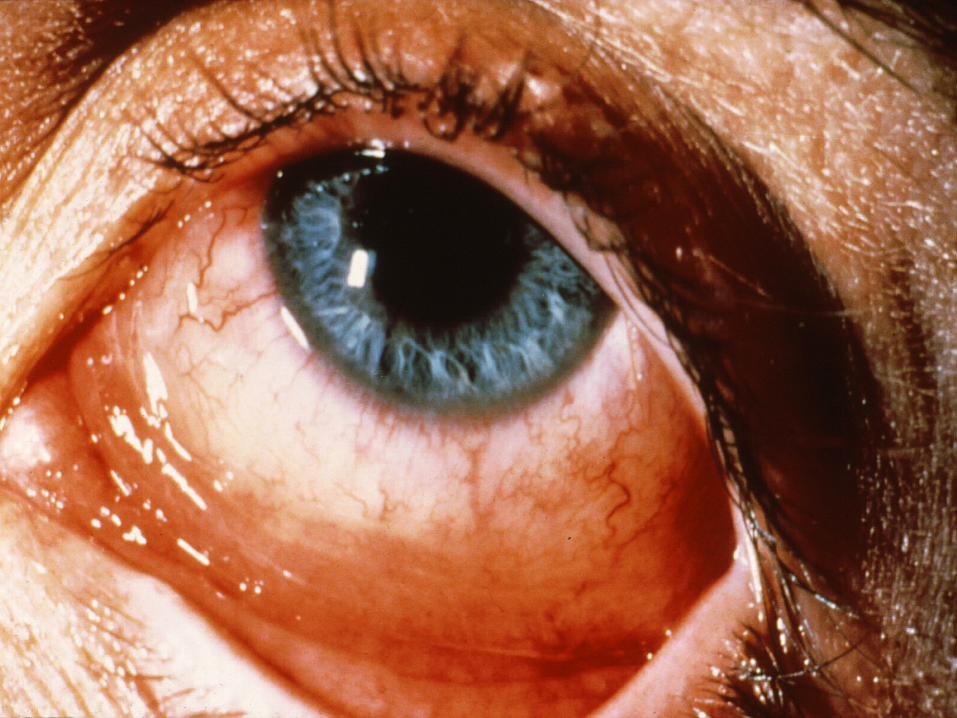
CONJUNCTIVITIS Causes: bacteries, viruses, allergies, tear
deficiencies Pattern: palpebral or diffuse
CONJUNCTIVITIS : DISCHARGE Discharge Purulent Clear Stringy, white mucus Cause Bacteries Viruses* Allergies
* preauricular lymphadenopathy signals viral infection
BACTERIAL CONJUNCTIVITIS :COMMON CAUSES
Staphylococcus Streptococcus Haemophilus
BACTERIAL CONJUNCTIVITIS : TREATMENT
Topical antibiotic qid x 4 days Warm compresses Refer if not markedly improved in 4 days


VIRAL CONJUNCTIVITIS Watery discharge Highly contagious Palpable preauricular lymph node URI, sore throat, fever common
If pain, photophobia, or decreased vision refer
ALLERGIC CONJUNCTIVITIS Associated conditions: hay fever, asthma,
eczema Contact allergy: chemicals, cosmetics Treatment: topical antihistamines, tears to
relieve itching
Refer refractory cases
NEONATAL CONJUNCTIVITIS : CAUSES
Chemical (silver nitrate) Bacteria (N gonorrhea, Staphylococcus,
Streptococcus) Chlamydia Viruses (herpes) Systemic Chlamydial infection

NEONATAL BACTERIAL CONJUNCTIVITIS : G+
Common agents: Staphylococcus aureus, Streptococcus pneumoniae; A, B streptococci
Treatment: erythromycin ointment qid x 4 days
NEONATAL BACTERIAL CONJUNCTIVITIS : G- Common agents: H influenzae, E coli Treatment: Tobramycin ointment q 2-4
hours x 5-10 days Consult ophthalmologist if Pseudomonas
suspected

NEONATAL CHLAMYDIAL CONJUNCTIVITIS : CAUSES
Exposure during vaginal delivery Silver nitrate ineffective against Chlamydia
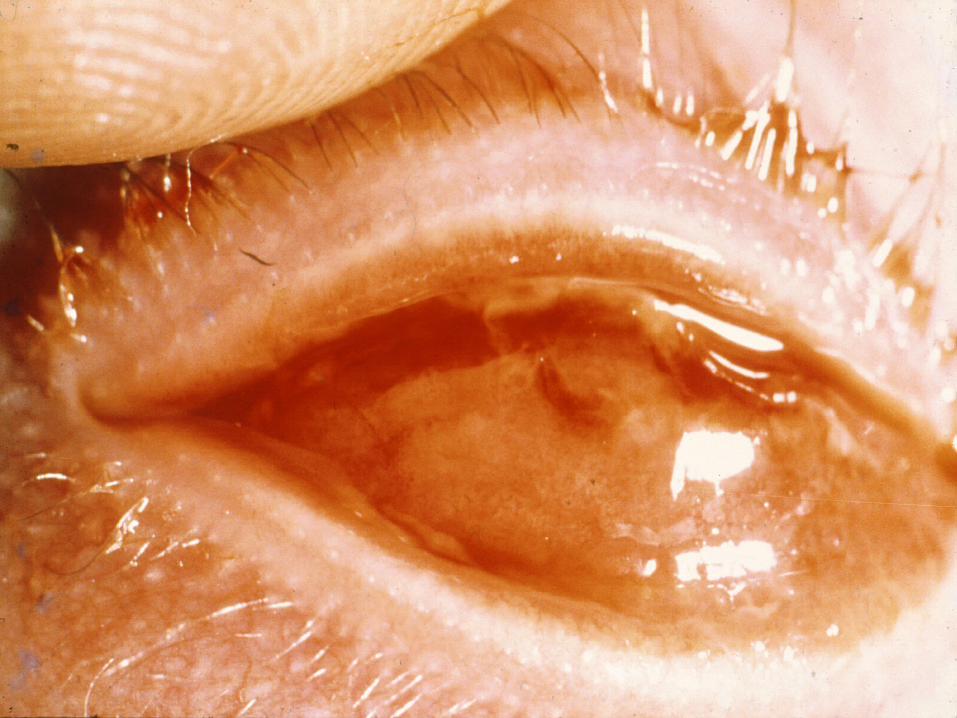
NEONATAL CHLAMYDIAL CONJUNCTIVITIS : TREATMENT
Erythromycin ointment qid x 4 weeks Erythromycin po x 2-3 weeks
(40-50mg/kg/day +4)
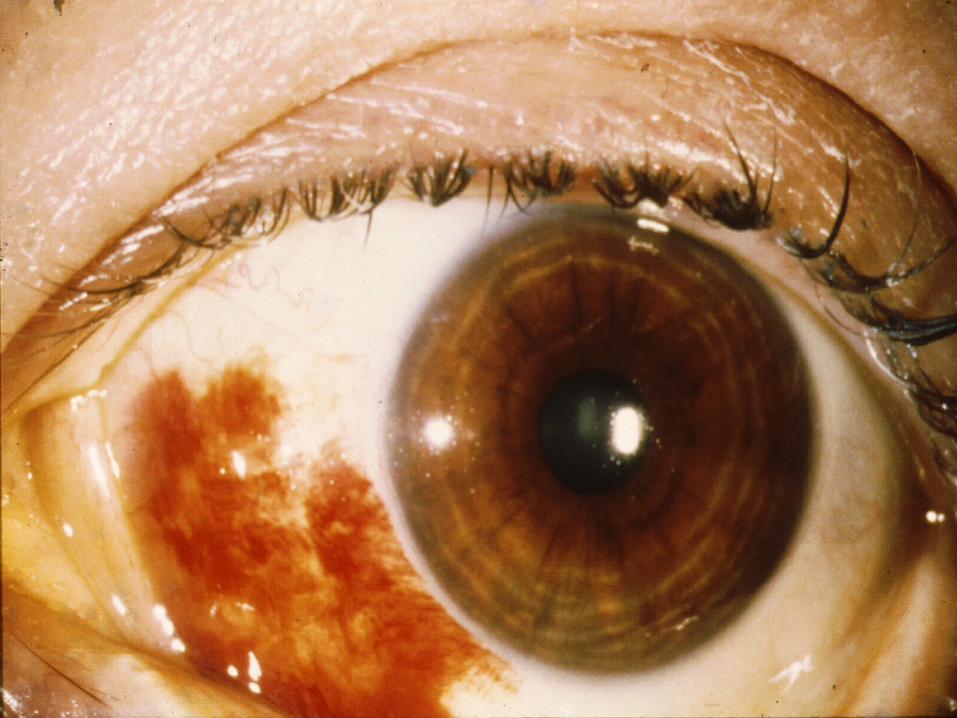
TEARS Process lubricating and bacteriostatic
properties Essential for maintaining a healthy cornea
and conjunctiva Dry eye ( keratoconjunctivitis sicca) is a
tear deficiency state
TEAR DEFICIENCY STATE : SYMPTOMS
Burning Foreign body sensation Reflex tearing
TEAR DEFICIENCY STATE : ASSOCIATED CONDITIONS
Aging Rheumatoid arthritis Steven Johnson syndrome Systemic medications
DRY EYES : TREATMENT Artificial tears Lubricating ointment hs Punctal occlusion

EXPOSURE KERATITIS Due to incomplete lid closure Manage with lubricating solutions/ointments Tape lids shut at night Do not patch Refer severe cases
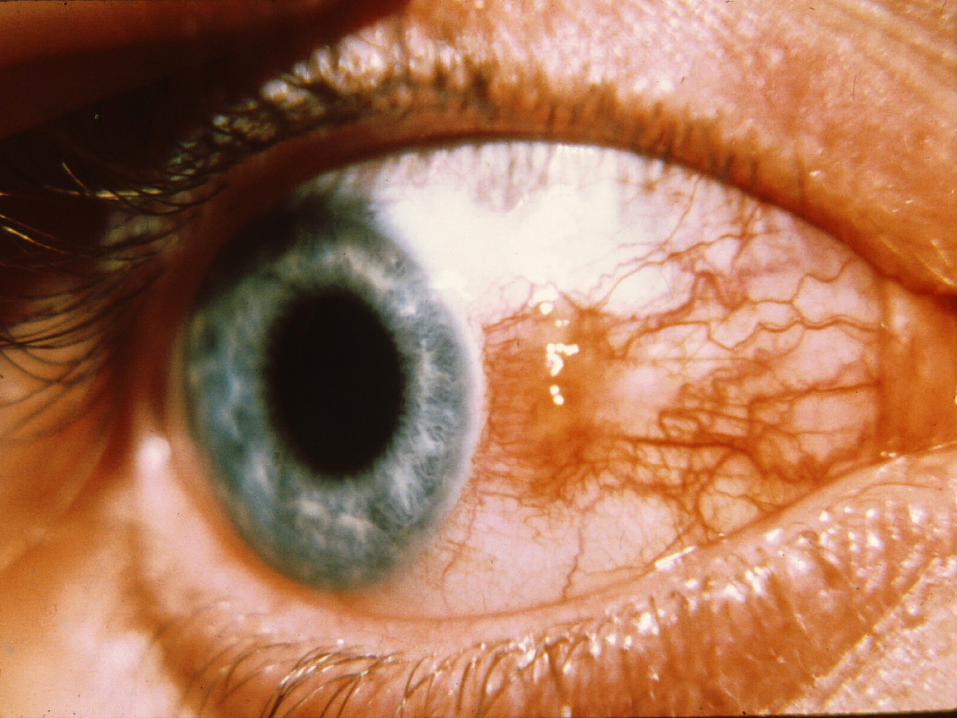

INFLAMMED PINGECUELA AND PTERYGIUM : MANAGEMENT
Artificial tears Topical vasoconstrictors If severe, refer


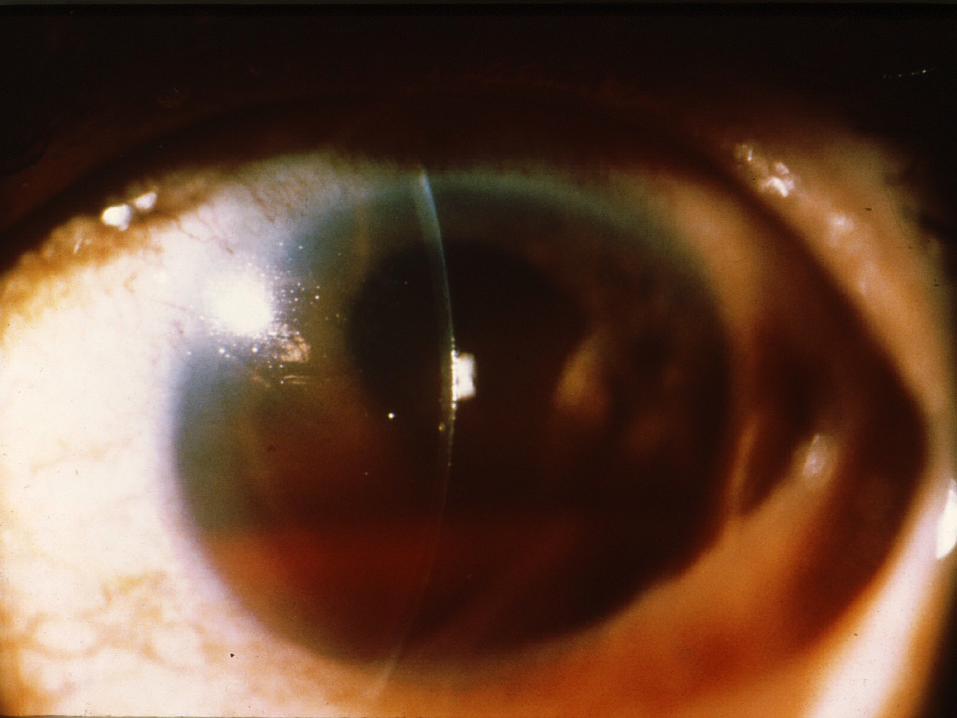
ACUTE CORNEAL DISORDERS : SYMPTOMS
Pain Photophobia Blurred vision
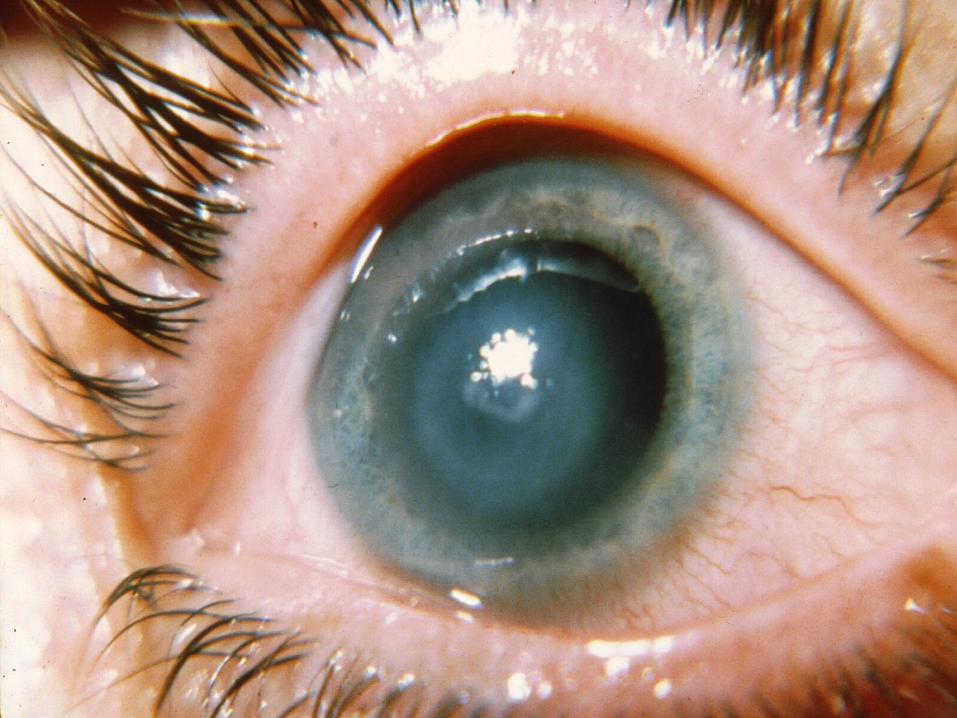

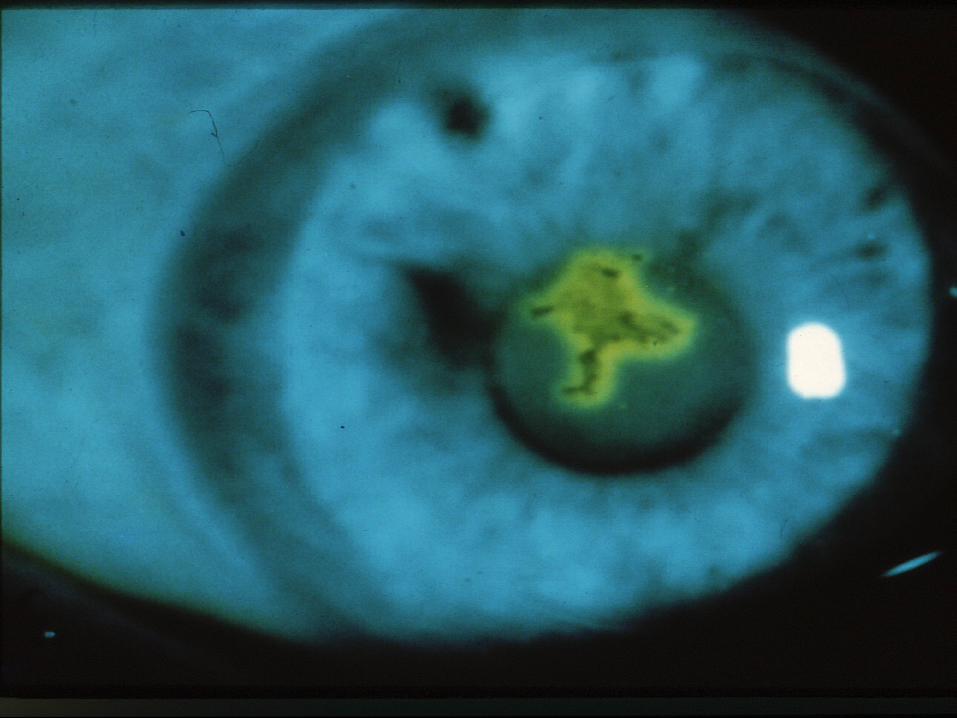
CORNEAL ABRASION Sx/sx: redness, tearing, pain, photophobia,
blurred vision, small pupil Causes: injury, welder’s arc, contact lens
over wear
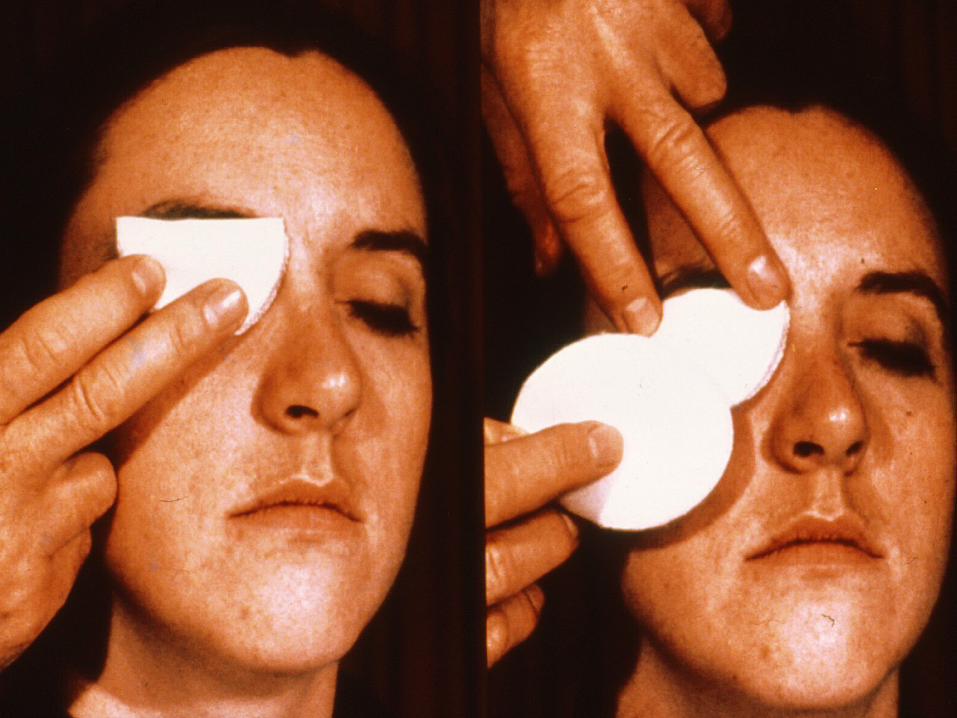
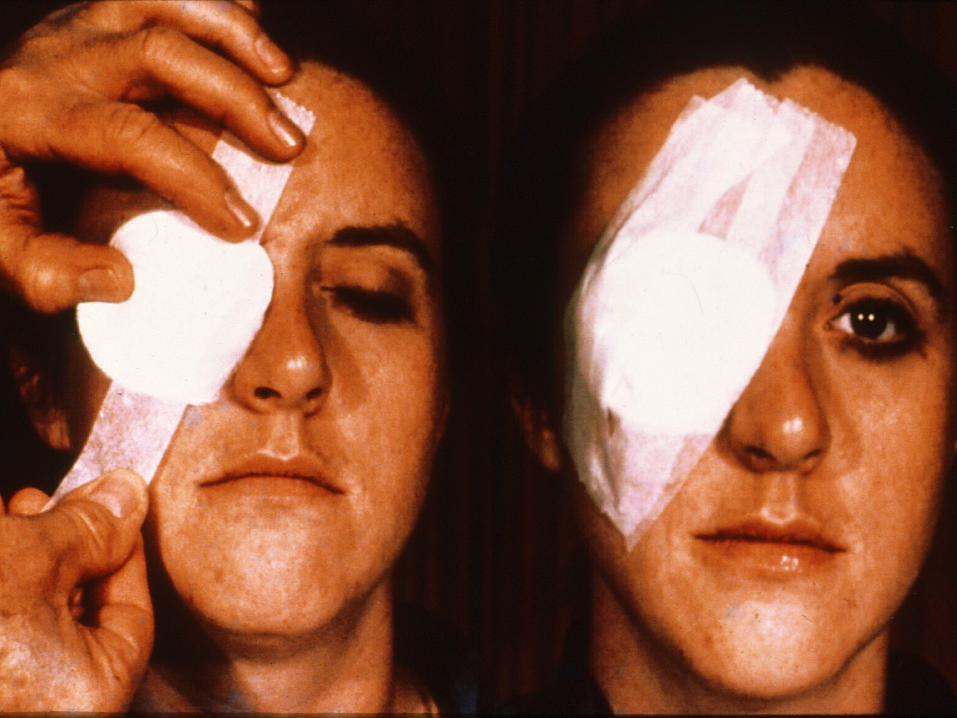
CORNEA ABRASION : TREATMENT Goals
Promote rapid healing Relieve pain Prevent infections
Rx 1 % cyclopentolate or 5 % homatropine Topical antibiotics Pressure patch x 24-48 hours + oral analgesics

Rx topical anesthetics
CHEMICAL INJURY A true ocular emergency Requires immediate irrigation with nearest
source of water Management depends on offending agents
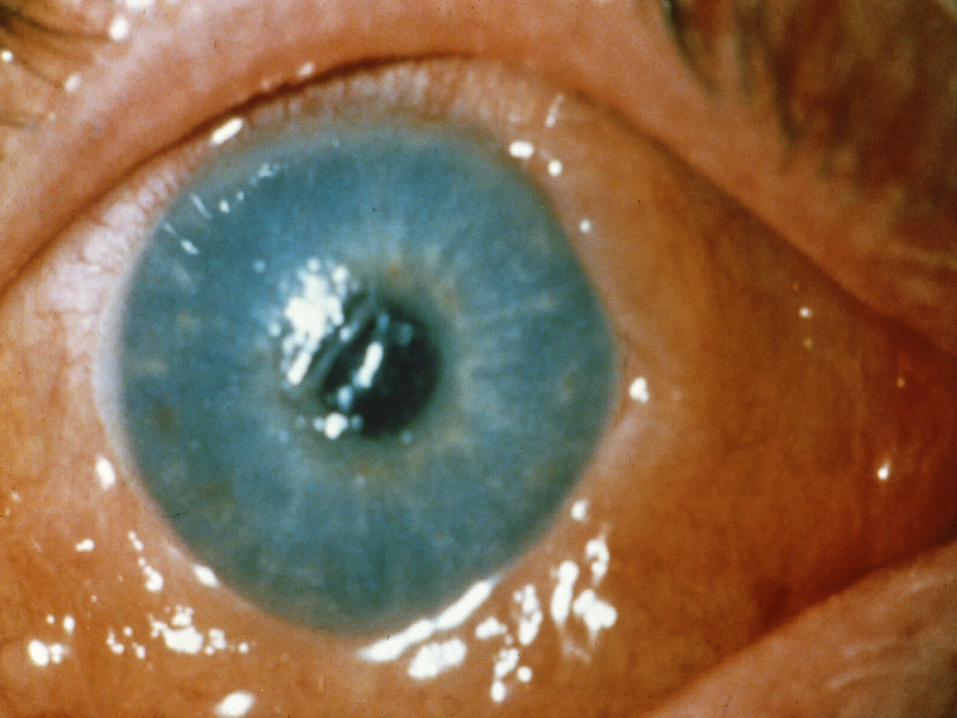
CHEMICAL BURNS : MANAGEMENT
Alkali Immediate irrigation Emergency referral to ophthalmologist
Acid Immediate irrigation Manage as corneal abrasion Referral to ophthalmologist next day
Prolonged contact lens wear
Severe pain and tearing in early AM,
corneal edema
Natural resolution if no corneal abrasion
Reassure/follow up next day
Refer if persist after 24 hours
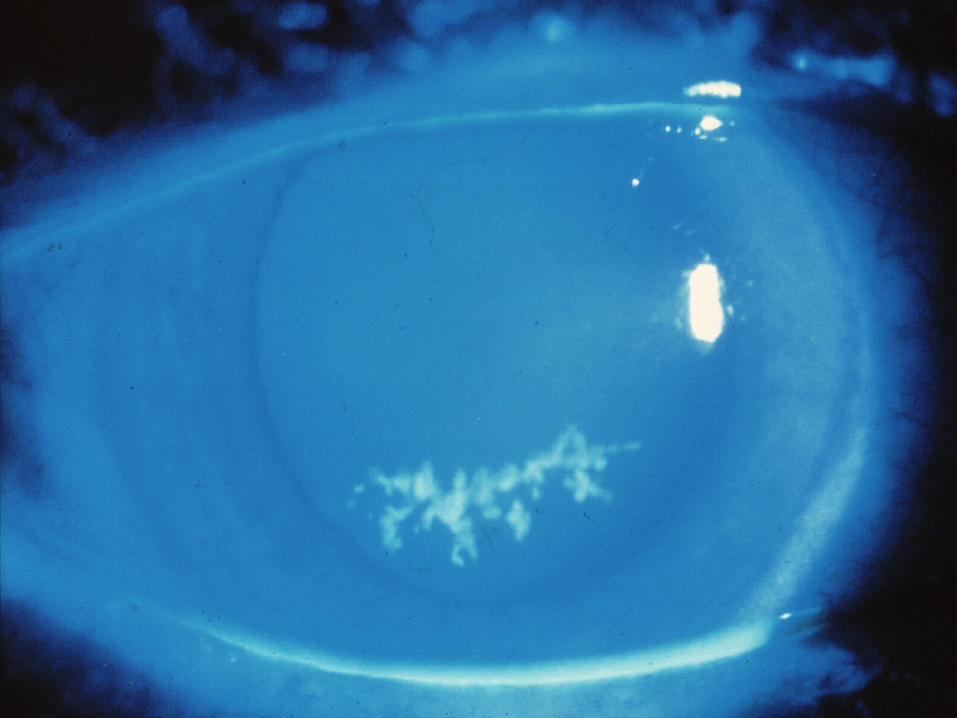
Corneal infections should be recognized and referred


TOPICAL STEROIDS

TOPICAL STEROIDS :SIDE EFFECTS
1. Facilitate corneal penetration of herpes virus
2. Elevate IOP (steroid induced glaucoma)
3. Potentiate fungal corneal ulcers

Hyphema, iritis, and acute glaucoma
should be recognized and referred

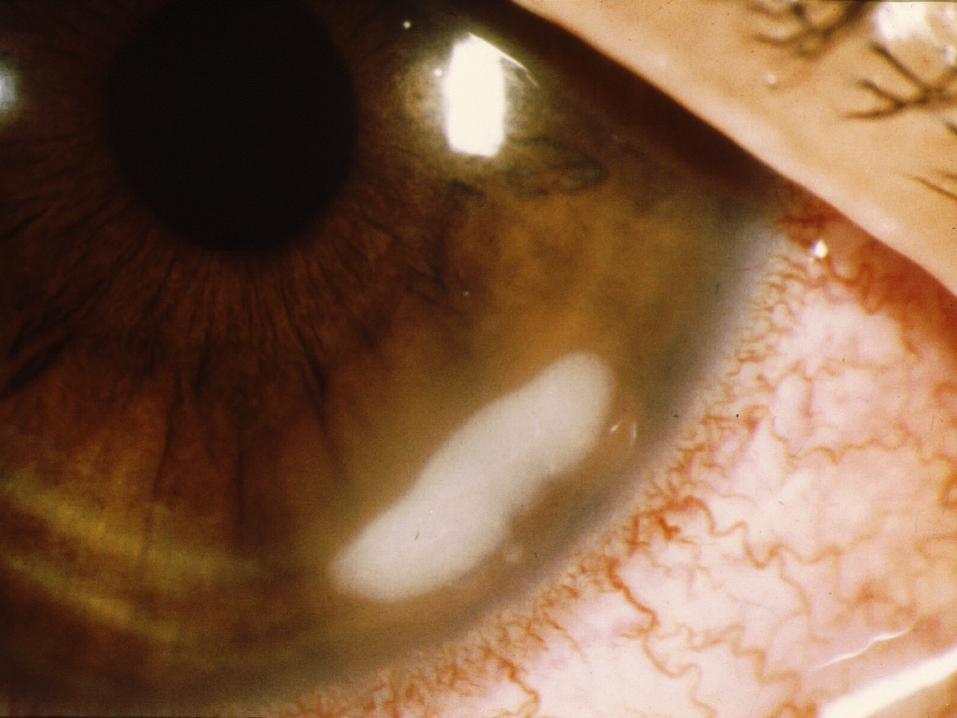
IRITIS Sx/sx
Circumcorneal redness Pain Photophobia Decreased vision Miotic pupil
Recognize and refer
R/o Systemic inflammation Trauma
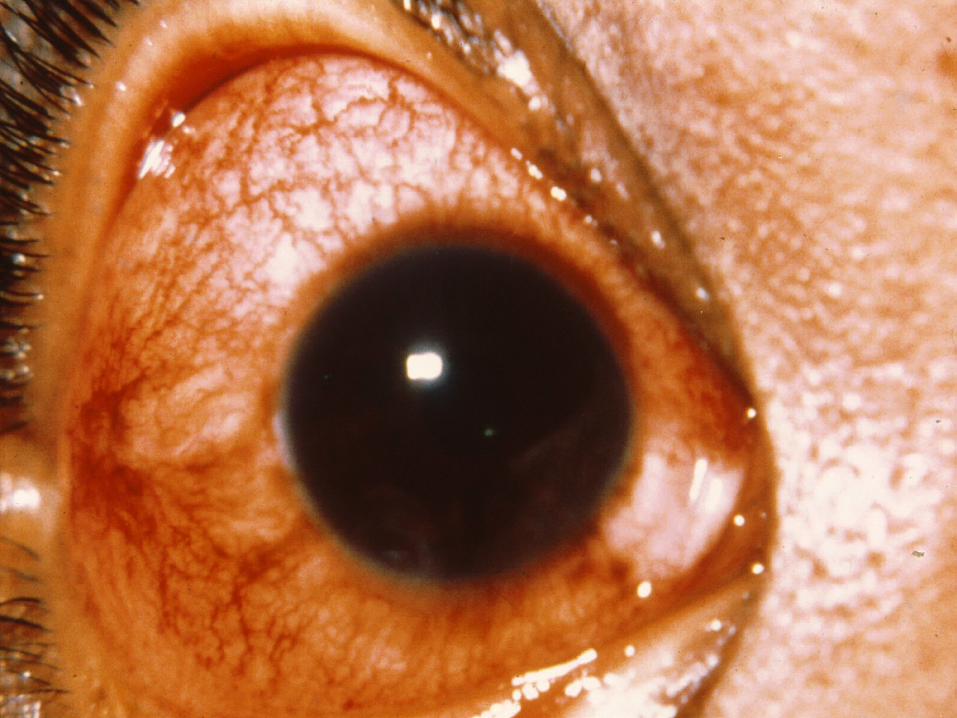
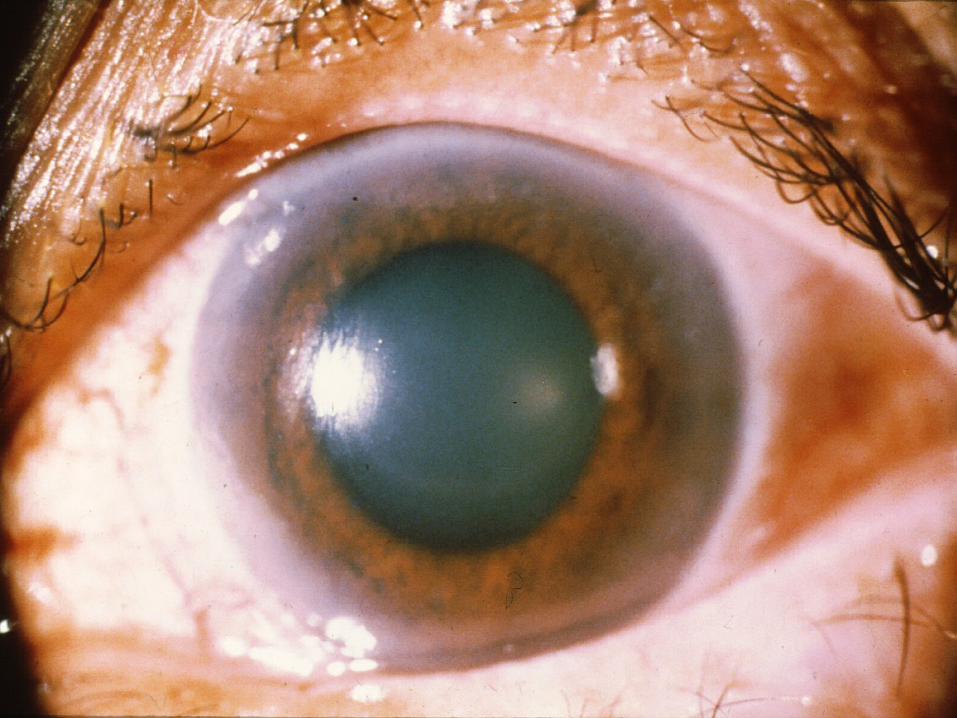
Acute angle closure glaucoma is characterized by a sudden rise in IOP in a susceptible individual with a dilated pupil
ACUTE GLAUCOMA : SYMPTOMS
Severe ocular pain Frontal headache Blurred vision with halos seen around lights Nausea, vomiting
Recognize acute glaucoma, “the great masquerader,” and refer.
ACUTE GLAUCOMA :INITIAL TREATMENT
Pilocarpine 2% gtt q 15 min x 2 Acetazolamide 500 mg po or iv Oral glycerine or isosorbide, 1 cc/kg body
weight IV mannitol 20% 300-500 cc
COMMON RED EYE DISORDERS : TREATMENT INDICATED
Hordeolum Chalazion Blepharitis Conjunctivitis Subconjunctival hemorrhage Dry eyes Corneal abrasions (most)

VISION-THREATENING RED EYE SX/SX : REFERRAL REQUIRED Decreased vision Ocular pain Photophobia Circumcorneal
redness Corneal edema
Corneal ulcers/dendrites
Abnormal pupil Proptosis Elevated IOP
VISION THREATENING RED EYE DISORDERS : URGENT REFERRAL Orbital cellulitis Episcleritis / scleritis Chemical injury Corneal infection Hyphema Iritis Acute glaucoma
CLINICAL EXPERTISE COOPERATION
COMMUNICATION