managing wounds in diabetes - professional eventspresence of callus signs of infection. neuropathy...
TRANSCRIPT

Assessment and Management of Wounds In Diabetes
Maria Mousley
Northamptonshire NHS Foundation
Trust
Background� At least 61000 people with diabetes in
England have a foot ulcer at any given time
� There are around 6000 lower extremity
amputations a year in people with diabetes
� Diabetic foot ulcers are the most common
cause of non-traumatic limb amputation
� The risk of a lower extremity amputation in a
person with diabetes is 23 x that of a person
without diabetes

Background� Diabetes is one of the
biggest health challenges
facing the UK today
� Diabetic foot problems
have a significant financial
impact on the NHS and a
significant impact on
patients’ quality of life.

CostsCostsCostsCostsCostsCostsCostsCosts……………………
Average annual cost of one foot ulcer treatment?£3,600(York Health Economics Consortium, The diabetic
Foot. Vol 1; No 3, 109-115, 1998)
Average cost of one lower limb amputation?£16,300 - £32,600(IDF, 2005)
Estimated Health Care budget in the UK
Up to £502m per year(DoH 2002)
The Indirect CostsThe Indirect CostsThe Indirect CostsThe Indirect CostsThe Indirect CostsThe Indirect CostsThe Indirect CostsThe Indirect Costs……………………
Restricted
mobility
Restricted
mobility
EmbarrassmentEmbarrassment
Loss of
earnings
Loss of
earnings
DepressionDepression
Social
isolation
Social
isolation
PainPain
Human
Costs
Human
Costs
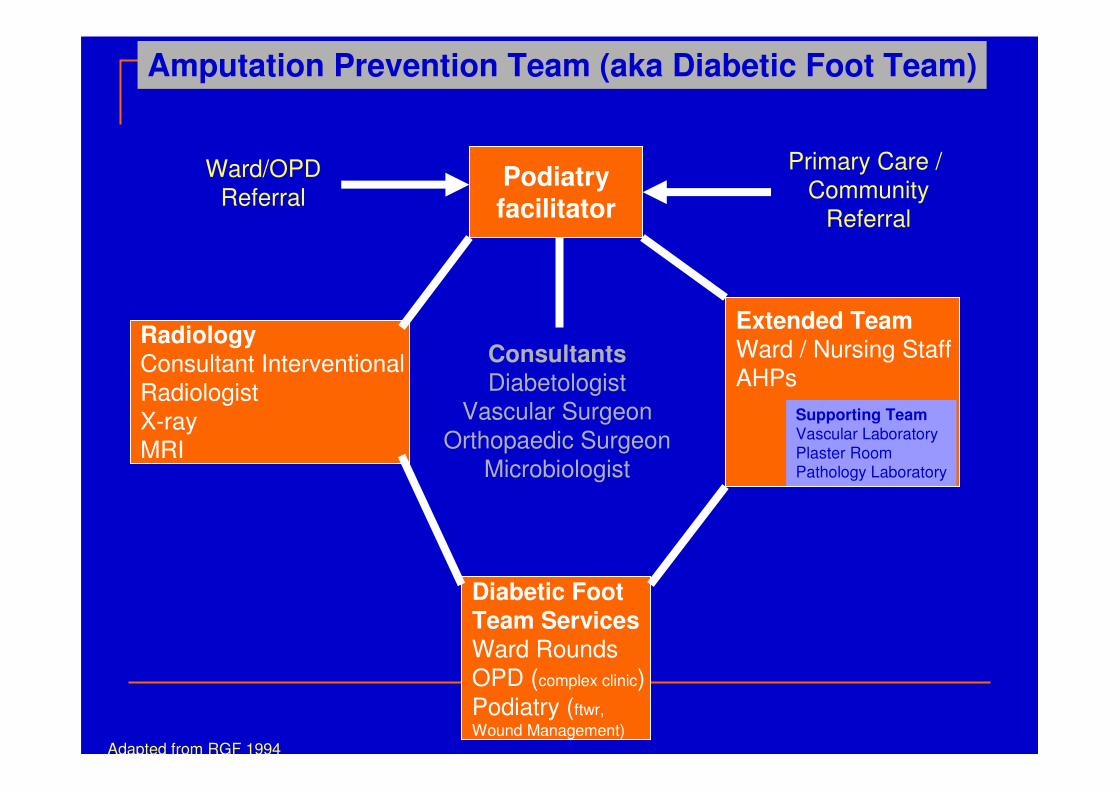
Podiatryfacilitator
Radiology
Consultant Interventional
Radiologist
X-ray
MRI
Extended TeamWard / Nursing Staff
AHPs
Diabetic Foot
Team ServicesWard Rounds
OPD (complex clinic)
Podiatry (ftwr,
Wound Management)
Consultants
Diabetologist
Vascular Surgeon
Orthopaedic Surgeon
Microbiologist
Ward/OPD
Referral
Primary Care /
Community
Referral
Amputation Prevention Team (aka Diabetic Foot Team)
Supporting TeamVascular Laboratory
Plaster RoomPathology Laboratory
Adapted from RGF 1994

Podiatryfacilitator
MDfT Services
Ward Rounds
OPD (complex clinic)
Specialist Podiatry (footwear,
Wound Management)
Ward/OPD
Referral
Primary Care /
Community
Referral
Amputation Prevention Team (aka Diabetic Foot Team)
Diabetic Foot ScreeningDiabetic Foot Protection Programmes

Refer?..................as?

Stage 1 - hard skin builds up (fire)

Pressure may not be noticeable at first
This may not be painful! (undetected)

Stage 2 - Tissue damage begins
beneath the surface (starts to spread)

Stage 3 - Skin breaks open and an ulcer
is revealed. This is prone to infection.
(spot the signs)

Extravasation – a precursor of ulceration
Prevention of Foot Attack

The faster you act the more of a foot you save


Escalating needs; deteriorating condition

Deterioration� Wound getting worse
� Increase in size
� Increase in depth
� Development of complications

NEUROPATHIC VS ISCHAEMIC ULCERS� Symptoms
� Circulation
� Site
� Presence of callus
� Signs of infection

Neuropathy Nerve damage in diabetes leads to altered pain sensation
Big toe
Ball of foot
Heel area
Tip of toes


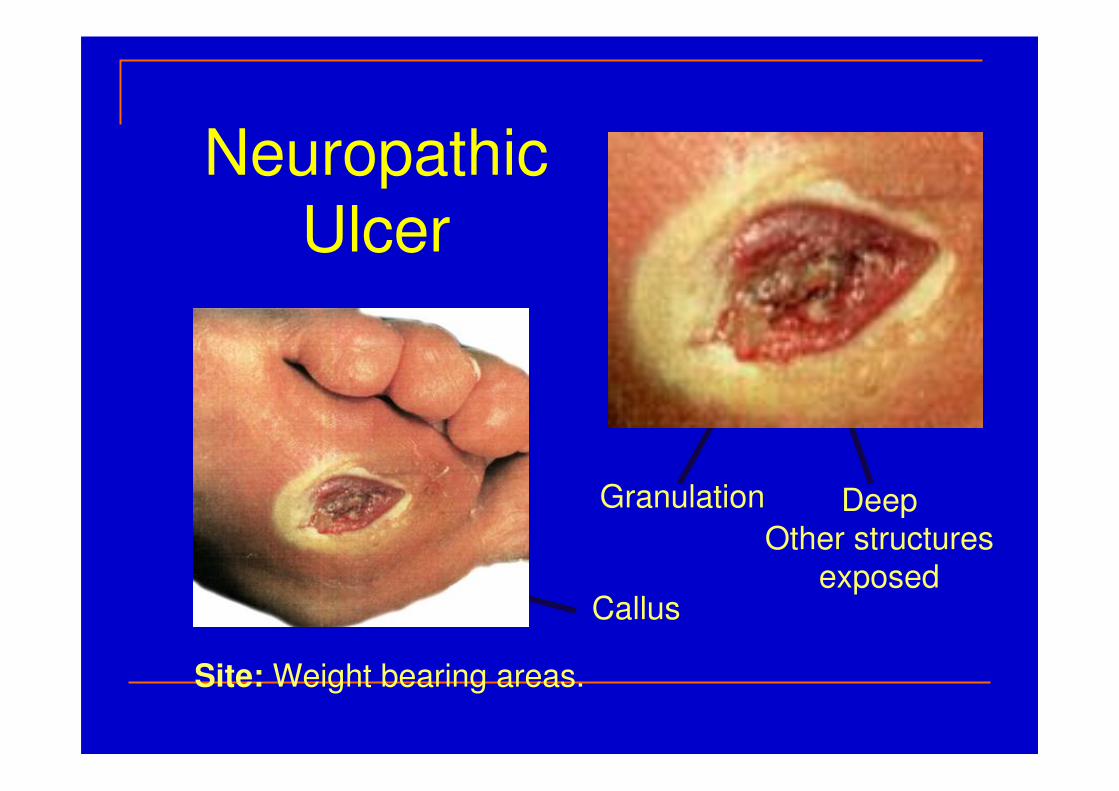
Neuropathic
Ulcer
Site: Weight bearing areas.
DeepOther structures
exposedCallus
Granulation

Clinical Examination
Insensate foot:repeated minor trauma causes ulceration

The importance of neuropathy� Ulcers will not heal unless offloaded
� Ulceration leads to infection, often
exacerbated by poor diabetes control
� Untreated or inadequately treated infection
leads to osteomyelitis
� Neuropathic ulcers may be small and
apparently insignificant – ALWAYS look
under the dressing
� NB – ‘infection ? cause’

Pressure offloading Total contact casting is the gold standard……… AND REST!!!!!!!!

Peripheral Arterial Disease� Palpate foot pulses:-
Dorsalis Pedis
Posterior Tibial
� Doppler—sounds� Monophasic?
� Ankle-Brachial Index
(ABPI) <0.8

Ischaemic
Ulcer
Necrotic centre
Surrounding
Erythema
Site: borders of the feet.
Painful
Cool FootPulseless

Neuroischaemic ulcers -Refer

Refer

Refer

Summary of Neuropathic foot ulcersNICE Clinical Guideline CG10 Type 2 Diabetes - Foot care 2004CREST guidelines 1998 www.gain-ni.org/Guidelines/wound-management-diabetic-foot.pdf
� Neuropathic foot
� Warm
� Numb
� Dry
� Usually painless
� Palpable pulses
� Neuropathic foot ulcers
� Commonly resulting from callus
� On weight-bearing areas
� Punched out appearance

Summary of Neuroischaemic foot ulcersNICE Clinical Guideline CG10 Type 2 Diabetes - Foot care 2004CREST guidelines 1998 www.gain-ni.org/Guidelines/wound-management-diabetic-foot.pdf
• Neuro-ischaemic foot ulcers
– Commonly result from tight shoe
– On non-weight-bearing areas of foot, toe tips & beneath toenails
� Neuro-ischaemic foot
� Cool/cold to touch
� Absent/diminished pulses
� Pain at rest

Tissue
Necrosis
InfectionNeuropathy Ischaemia
The Deadly Triad
(Edmonds 1984))

‘Line of least resistance’

Spreading infection
Mr G W 52 years� April 10 – picked hard skin off foot at base of
R hallux
� Not diabetic but family history of diabetes in
two relatives – one an amputee
� Foot became infected – generally unwell
� Saw private podiatrist and advised to go to
GP
� Prescribed flucloxacillin over the phone

� 2 days later – reviewed by podiatrist
� not happy and referred to A&E
� seen by orthopaedic SHO and advised to
continue antibiotics and return in 2 days
� 2 days later (1 week after first became
unwell) saw GP
� blood glucose 16.8
� pyrexial
� cellulitis
� Admitted under orthopaedic surgeons for iv antibiotics

� IV flucloxacillin and benzylpenicillin
(hospital guidelines advise co-amoxiclav for
diabetic foot infections)
� cultures subsequently grew haemolytic strep,
staph aureus and anaerobes
� 2 days after admission, debrided by
orthopaedic surgeon
� Further debridement 1 week later
� Referred to vascular surgeon and podiatrist


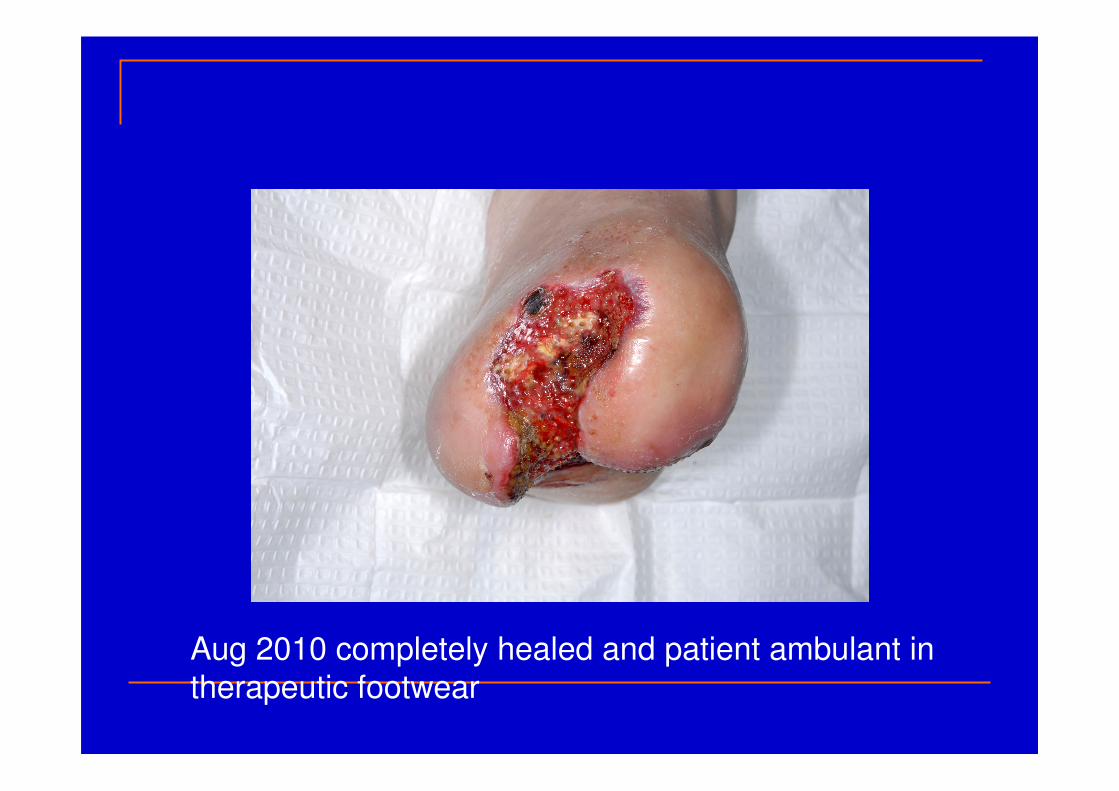
Aug 2010 completely healed and patient ambulant in
therapeutic footwear

Missed Opportunities� Primary care
� Lack of specialist knowledge and referral routes
� failure to assess patient
� delayed diagnosis of diabetes
� Secondary care
� failure to recognise need for intravenous antibiotics when seen in A&E
� inadequate antibiotic cover
� inadequate debridement
� failure to involve the specialist diabetic foot
team

Neuropathic ulcer – presentation with cellulitis and …………

Neuropathic ulcer - tracking


� If the following are present, obtain urgent
advice from an appropriate specialist:
� redness or warmth are present
� systemic sepsis
� deep seated infection
� limb ischaemia
Initial examination and assessment

‘‘‘‘Kissing UlcersKissing UlcersKissing UlcersKissing Ulcers’’’’
(Ref. Jeffcoate & Macfarlane 1995)
Kissing Ulcers


Tip, Top Toe!
(Ref. Irion 2002)
Increased presure

Avoidable pressure ulcers are a key indicator of the quality of care. Preventing them will improve all care for at risk patients (harm free care)


Debridement



Neuropathic Ulcer
•No pain•Warm Foot•Pulses present
Profuse slough
Conversion to Infection

ManagementManagementManagementManagementManagementManagementManagementManagement……………………

Managing infection in the diabetic foot Clinical Knowledge Summaries Type 2 Diabetes 2008
� Infection presents a threat to (life and) limb and should be treated promptly and aggressively
� Foot care infections in patients with diabetes are classified as non-limb threatening (urgent referral to a multidisciplinary diabetes foot care team within 24
hours) or limb-threatening (usually require hospital admission)
� Infected diabetic feet should only be treated by clinicians who have sufficient experience and facilities available
� A non-limb threatening infection can quickly become limb threatening
Managing infection in the diabetic foot Clinical Knowledge Summaries Type 2 Diabetes 2008
Non - limb threatening Infection - refer within 24 hours
� Includes those with infection of a superficial ulcer, no
bone or joint involvement, no signs or symptoms of systemic toxicity, no significant ischaemia
� If referral within 24 hours is not possible, start empiric
antibiotic treatment in interim.
� If deeper infection, seek urgent advice
� Review after 7 days
� Swabs should be taken before starting antibiotics
Managing infection in the diabetic foot Clinical Knowledge Summaries Type 2 Diabetes 2008
Limb threatening infection - consider hospital admission
� Includes those with spreading cellulitis, systemic signs of infection, lack of response to oral antibiotics, malodorous
wounds, soft tissue necrosis or suspected bone
involvement

Continuum of microbial load
http://www.education.woundcarestrategies.com/coloplast/resources/Clinical%20Wound
%20Assessment-Pocket%20Guide.pdf
Increasing bioburden

Conversion to Infection and necrosis

Why Why Why Why Why Why Why Why ‘‘‘‘‘‘‘‘high riskhigh riskhigh riskhigh riskhigh riskhigh riskhigh riskhigh risk’’’’’’’’ woundswoundswoundswoundswoundswoundswoundswounds……………………????????Vascular disease
Nerve damage
Hyperglycaemia
Underlying susceptibility to infection

Classic Signs of Infection
Rubor et tumor cum calore et
doloreredness swelling heat
pain
(Celsus c. 3-64AD)

Diagnose Infection Based on any 2 features Diagnose Infection Based on any 2 features Diagnose Infection Based on any 2 features Diagnose Infection Based on any 2 features ((((BerendtBerendtBerendtBerendt & & & & LipskyLipskyLipskyLipsky 2003)2003)2003)2003)
Minor increase in
volume
Increased, +/-
viscosity
Exudate levels
Increased painLittle or nonePain
Little changeLocalised –generalised
Swelling
Little change -dusky red
Erythematouseg.pillar box red
Colour
Little change -
cooler
Comparative
increase
Temperature
IschaemicNeuropathicFeature
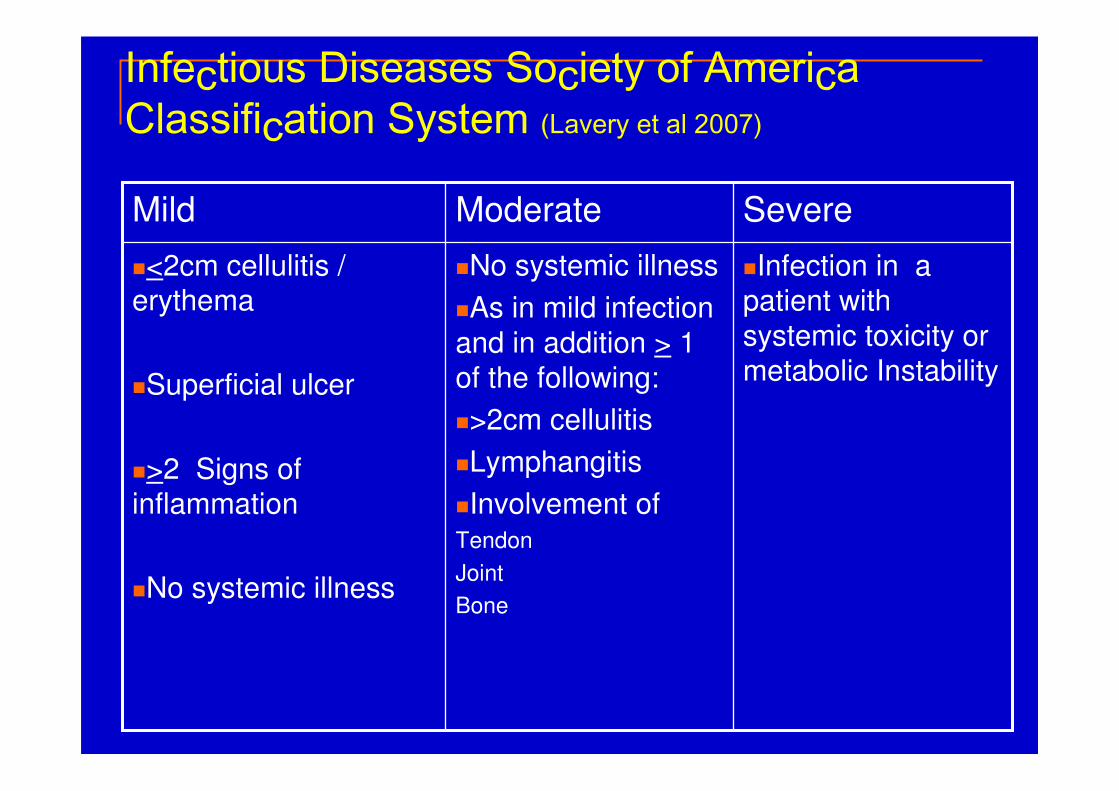
�Infection in a patient with
systemic toxicity or metabolic Instability
�No systemic illness
�As in mild infection
and in addition > 1 of the following:
�>2cm cellulitis
�Lymphangitis
�Involvement of Tendon
Joint
Bone
�<2cm cellulitis / erythema
�Superficial ulcer
�>2 Signs of inflammation
�No systemic illness
SevereModerateMild
Infectious Diseases Society of America Classification System (Lavery et al 2007)

REMEMBERREMEMBERREMEMBERREMEMBER…………....
Risk of treating infection too late, with it’s associated morbidity & mortality…, while giving antibiotics freely carries a risk of inducing antibiotic resistance….use of clinical skills & judgement is vital!

What antibiotic do I use?
Broad Spectrum
Eg. Co-amoxiclav
Culture and sensitivity
Culture directed
narrower spectrum

Antibiotics in Diabetic foot Disease
� IDSA http://www.idsociety.org
� Scottish Diabetes Group Consensus (Leese et
al The Diabetic Foot Journal vol 12 2 2009)
� Clinical Knowledge Summaries (CKS)� http://www.cks.nhs.uk/diabetes_type_2/management/detailed_answers/foot_problem
s

Treatment of infection
Osteomyelitis

� When choosing wound dressings take into account:
– clinical assessment of the wound
– patient preference
– clinical circumstances eggranulating, sloughy, necrotic
– which wound dressing has the lowest acquisition cost.
Management of diabetic foot ulcers

Guidelines on wound and wound-bed management (2011)IWGDF Game et al 2012 Diab Metab Res Rev;28:232-233
‘In the absence of strong clinical or cost effective evidence, health care professionals should use wound dressings that best match clinical experience, patient preference, the site of the wound and the cost of the dressings.’
‘Wounds should be closely monitored and dressings changed regularly.’
(NICE, 2004 )

Health Technology Assessment

WHAT MAKES AN IDEAL DRESSING for WHAT MAKES AN IDEAL DRESSING for WHAT MAKES AN IDEAL DRESSING for WHAT MAKES AN IDEAL DRESSING for WHAT MAKES AN IDEAL DRESSING for WHAT MAKES AN IDEAL DRESSING for WHAT MAKES AN IDEAL DRESSING for WHAT MAKES AN IDEAL DRESSING for ‘‘‘‘‘‘‘‘High High High High High High High High RiskRiskRiskRiskRiskRiskRiskRisk’’’’’’’’ WoundsWoundsWoundsWoundsWoundsWoundsWoundsWounds…………………….?.?.?.?.?.?.?.?
• Designed to minimise cross-contamination
• Maintains a moist environment for optimal wound healing
(Sibbald et al, 2004)
• Absorption and retention at varying exudate levels (Chen
et al, 2003)
• Minimises risk of damage to peri-wound skin (Jones et al,
2004)
• Conformable to the wound (Armstrong S.H. 2004)
• Versatile, for use on a wide range of wounds
• Comfortable for patient (Mortimer D)
• Control odour
• Easy to use
• Cost-effective

WWWWWWWWoundoundoundoundoundoundoundound bedbedbedbedbedbedbedbed colour...colour...colour...colour...colour...colour...colour...colour...
� Black (necrotic)
� Yellow / grey (sloughy)
� Red (granulating)
� Pink (epithelising)

ThinkThinkThinkThinkThinkThinkThinkThink……………………........Consideration should be given to the fact that these properties
may be altered when dressing the feet (Morgan
D, Formulary of Wpund Management
Products, 7th Ed: 26, 29-30, 1997) as
dressings are not designed to take the
high & repetitive forces exerted on the sole of the foot! (Baker N,
Journal of Wound Care 6 (1): 1997)
High & repetitive forces
Body weight
pressure
Footwear accommodation
Movement
Friction
INFECTION MASKED…!

Vascular controlVascular control……..

Mechanical controlMechanical controlMechanical controlMechanical controlMechanical controlMechanical controlMechanical controlMechanical control……………………........Rest
Avoidance of
pressure

GlycaemicGlycaemicGlycaemicGlycaemicGlycaemicGlycaemicGlycaemicGlycaemic controlcontrolcontrolcontrolcontrolcontrolcontrolcontrol……………………........
Consider any systemic, metabolic or
nutritional disturbances that may impair
the response to infection and retard
healing of wounds.

Educational controlEducational controlEducational controlEducational controlEducational controlEducational controlEducational controlEducational control……………………........
Patient education / empowerment is critical if successful management is to be achieved.
(Day J, Diabetes Metab Res Rev; 16 (Suppl 1): S70-74, 2000)

Key points for education (NICE 2004)
� Self-care and self-monitoring
� Knowledge of when & where to seek advice
� Awareness of possible consequences of
neglecting the feet
� Management of symptoms (pain, odour)

SummarySummarySummarySummarySummarySummarySummarySummary1. Vascular disease
2. Nerve damage
3. Hyperglycaemia (infection)
4. Pt education

Questions?

Find out more�Visit www.nice.org.uk/guidance/
� www.woundsinternational.com
ReferencesReferencesReferencesReferencesBanga JD. (1994), Lower extremity arterial disease in diabetes mellitus Diabetes Reviews International 3;4:6-11 Dejgaard A. (1998), Pathophysiology and treatment of diabetic neuropathy Diabetic Medicine 15:97-112 Edmonds ME. (1984), The Diabetic Foot Practical Diabetes 1;1:36 Young MJ et al. (1993), A Multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population Diabetologia36:150-154