managment of osa
TRANSCRIPT

MANAGMENT OF OSA
DR MANOHAR, RESIDENT ENTINHS ASVINI

Management under following headings:
• Behavioural measures
• Medical management
- Pharmacologic therapy
- Oral appliances
- Positive airway pressure
• Surgical treatment by site
- Nose
- Oral, oro pharyngeal and Nasopharyngeal procedures
- Hypo pharynx
- Tracheostomy (Bypass procedure)

Approach Considerations
• General and behavioural measures weight loss,
avoidance of alcohol for 4-6 hours prior to bedtime
• Positional therapy: sleeping on one side, head elevated
• 10% reduction in weight leads to a 26% reduction in the
respiratory disturbance index (RDI)

• Benefits of weight reduction in patients with SDB
include the following:
• Decreased RDI
• Lowered blood pressure
• Improved pulmonary function and arterial blood gas
values

• Improved sleep structure and snoring
• Possible reduction of optimum CPAP pressure
required
Benefits of weight reduction contd...
Pharmacologic therapy
• Modafinil 200-400 mg/d
• Binds dopamine transporters and inhibits dopamine
reuptake
• Improve wakefulness in patients with excessive
sleepiness
• Residual daytime sleepiness despite optimal use of CPAP
• Armodafinil
• Mechanical measures:
- Oral appliance (OA) therapy
- Continuous positive airway pressure (CPAP)
- Bilevel positive airway pressure (BiPAP) device

• Indications for OAs:
- Patients with mild-to-moderate OSA who
prefer oral appliances to CPAP devices
- Patients with mild-to-moderate OSA who do
not respond to CPAP therapy

• Patients with mild-to-moderate OSA in whom
treatment attempts with CPAP devices fail
Indications for Oas contd...

• Contraindications for OA:
• Less than 6-10 teeth in each arch
• Patient unable to protrude the mandible forward and
open the jaw widely
• Pre-existing temporo-mandibular joint problems
• Severe bruxism
• Patient with full denture

• Therapeutic nightly stimulation of the hypoglossal
nerve
• Electrical stimulation of genioglossus using
intramuscular or transcutaneous electrodes

CPAP
• CPAP machine
• Three main parts:
- A mask that fits over nose or nose and mouth with
straps
- A tube that connects the mask to the machine's
motor
- A motor that blows air into the tube

Working of CPAP
• Splint the airway open and prevent the collapse of
the upper airway
• Other benefits of CPAP:
• Increased end-expiratory lung volume
• Increase in oxygen stores

• Increased tracheal traction to improve upper airway
patency
• Lower cardiac after- load and consequent increase in
cardiac output
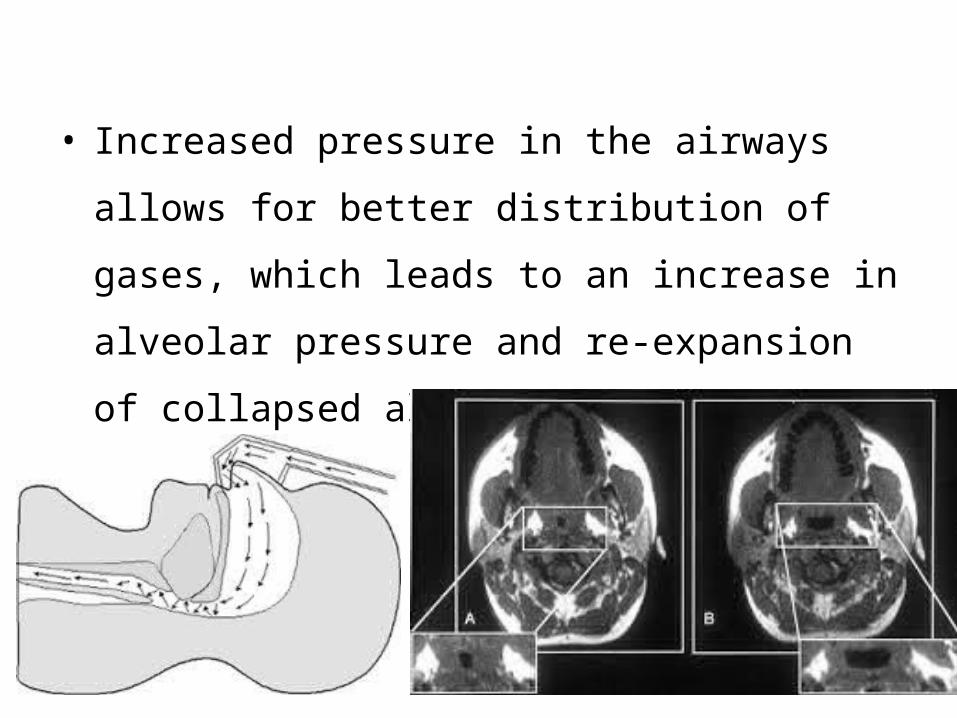
• Increased pressure in the airways allows for better
distribution of gases, which leads to an increase in
alveolar pressure and re-expansion of collapsed
alveoli

• BPAP
- Bilevel positive airway pressure (BPAP) devices
have two alternating levels of pressure
• AutoCPAP machines
- Collect data on compliance, leaks and pressure
profile

• Side effects of CPAP:
• Claustrophobia
• Nasal stuffiness-> poor compliance
• Skin abrasions and leaks
• Ulceration of the bridge of the nose-> ill fitting of
mask
• Air swallowing and pulmonary barotraumas: very rare

Surgical management
INDICATIONS FOR SURGERY
• Patients with severe, antisocial snoring:
- without OSA
- localized obstruction at one level in the upper
airway, usually at palatal level
- multisegmental obstruction with predominant
obstruction at palatal level

• Patients with mild-to-moderate sleep apnoea:
- with severe antisocial snoring;
- failed or inadequate response to CPAP
- localized obstruction at one level in the upper
airway, usually at palatal level

• Patients with moderate-to-severe sleep apnoea:
- with severe antisocial snoring;
- failed or inadequate response to CPAP;
- multisegmental obstruction

Nostrils and Columella

Luminal (Nasal) Valve
• Transverse nasal collapse is seen when the upper and
lower lateral cartilages are deficient in substance
• Lateral nasal walls collapse with inspiration
• Batten grafts can be used to bolster up the width of
the nose and give it more substance and firmness


Hypertrophied Turbinates

Macroglossia (Large Tongue)

Tori of the Maxilla or Mandible
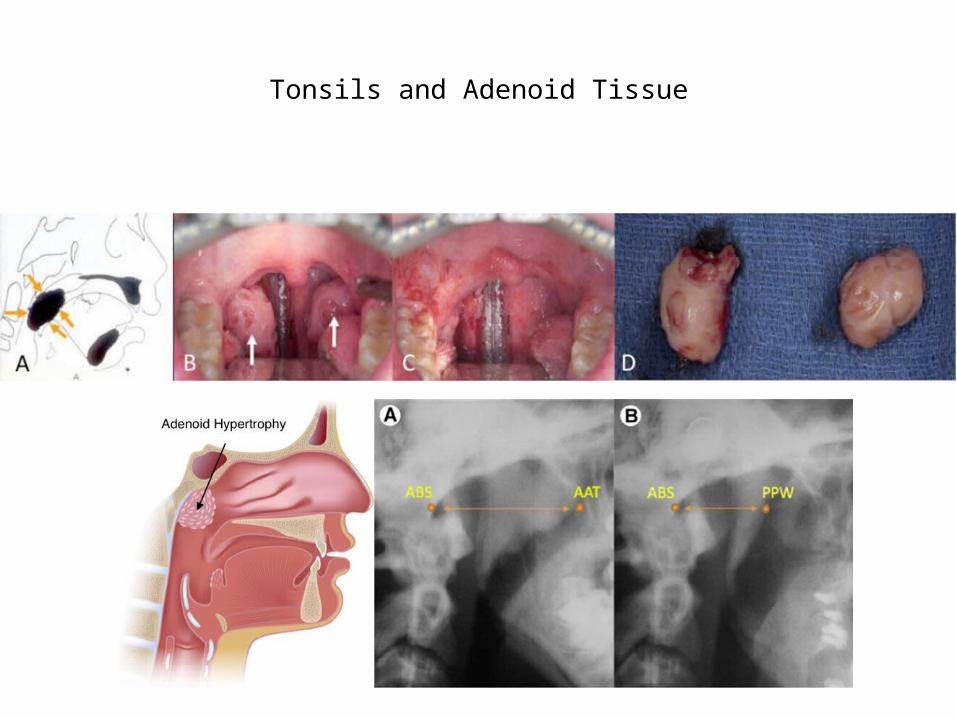
Tonsils and Adenoid Tissue

Uvulopalatopharyngoplasty:
• Ikematsu in the 1950s
• Popularized by Fugita in 1985
• Principle


• Modifications
- Preservation of the uvula
- Eliminating the pharyngoplasty part
• Success: It is effective in 40% of patients
- Recurrence if continue to gain weight
• Complications :
• Severe postoperative pain
• Haemorrhage
• Respiratory events: airway obstruction due to
laryngospasm, postoperative pulmonary
oedema and hypoxia

• Nasal regurgitation due to excessive palatal resection
• Velopharyngeal stenosis
• Dry throat
• Swallowing problems
• Taste disturbances

Radiofrequency tissue volume reduction/
thermal ablation:
• Procedure:
• Thermal injury to specific submucosal sites
in the soft palate resulting in fibrosis of the muscular
layer and volumetric tissue reduction.

• Three types of radiofrequency devices
• Somnus unit
• Celon device: bipolar electrode tip, auto stop
application and reduced procedure time
• Coblator unit: larger electrode tip

Coblation continued..

• Advantages
- OPD procedure
- Local anaesthesia
- Less postoperative pain and other complications
- Single and multilesion groups showed significant
improvement in snoring

• Complications:
• Ulcers of the tongue base or soft palate
• Dysphagia
• Temporary hypoglossal nerve palsy
• Abscess at the base of tongue

• Maxillomandibular procedures:
- Insertion of the genioglossus or geniohyoid muscle
advanced without moving the entire mandible or
teeth- Designed to enlarge and stabilize the retrolingual
airway


• Hyoid myotomy and suspension
- Horizontal anterior cervical neck incision over hyoid
- Released from inferior attachment and advanced
anteriorly and inferiorly over thyroid cartilage

• Maxillomandibular osteotomy and advancement
- Aims to move the maxilla and mandible as far
forward as possible
- Dentofacial deformities
- Consists of Le Fort I osteotomy of the maxilla and
a bilateral sagittal split osteotomy of the mandible
Laser-assisted uvulopalatoplasty:
• Introduced by Kamami in France, in 1993, as OPD
procedure under LA
• Bilateral vertical incisions are made in the soft palate
followed by partial vaporization of the uvula with a
CO2 laser
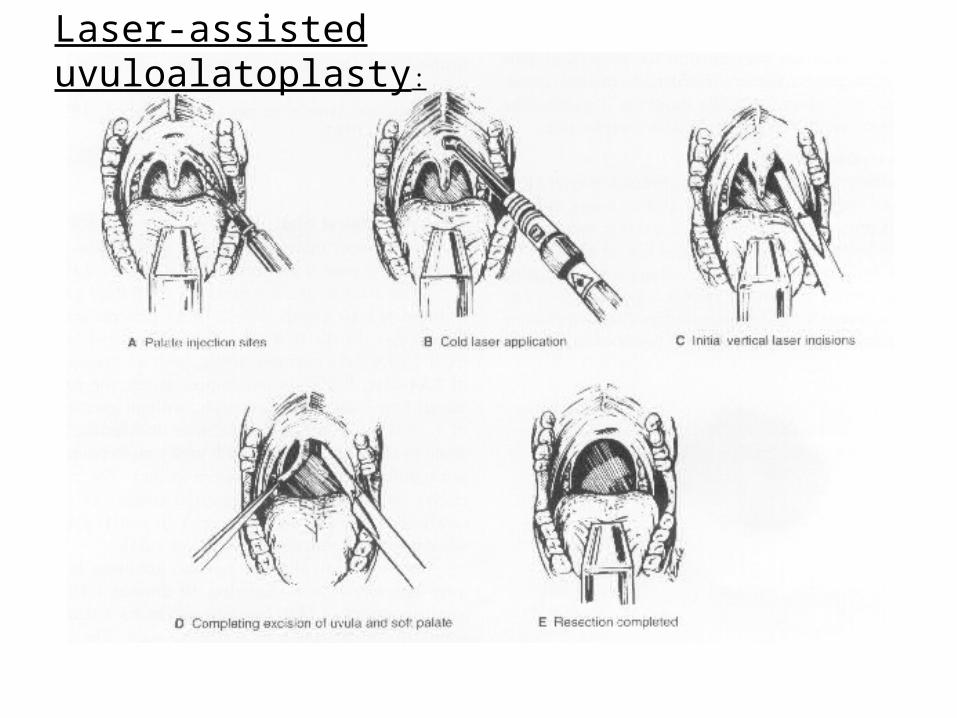
Laser-assisted uvuloalatoplasty:

• Advantages:
- Brief surgical session
- Reduces far less palatal tissue and does not alter the
tonsils or the pharyngeal pillars
- Uses a laser rather than a scalpel
- Requires no wound closure

• Under local anesthesia
• Requires no postoperative hospital stay
Advantages contd...

• Increased tendency of:
- Worsening in nasal breathing in previously simple
snorers

Pillar procedure
• The pillar procedure involves surgically placing small
polyester rods in the soft palate.
• Each implant measures 18 millimeters (mm) in length
— slightly less than an inch — and 1.5 mm in
diameter.

Pillar procedure

Radiofrequency cold ablation

Turbinate reduction
Radiofrequency turbinate ablation


• Tracheostomy:
- Tongue base procedures such as genioglossus
advancement or laser midline glossectomy

Bariatric surgery


References
• Scott-Brown’s 7th edition
• Cummings 5th edition
• OCNA

THANK YOU