“manejo(del(riesgo(y(enfermedad(cardiovascular(...
TRANSCRIPT

“Manejo del riesgo y enfermedad cardiovascular en el paciente con esteatohepatitis no alcohólica”
José López MirandaLipid and Atherosclerosis UnitDepartment of MedicineReina Sofia University Hospital University of Cordoba
VALORACIÓN Y MANEJO DEL RIESGO CARDIOVASCULAR
(Lonardo A, et al, Metabolism 2015)
1. ¿Los pacientes con EHNA tienen un mayor riesgo dedesarrollar enfermedad cardiovascular?
2. ¿Cuáles son las principales causas demorbimortalidad cardiovascular en pacientes conEHNA?
3. ¿Cómo podemos reducir el riesgo de padecerenfermedad cardiovascular en pacientes con EHNA?
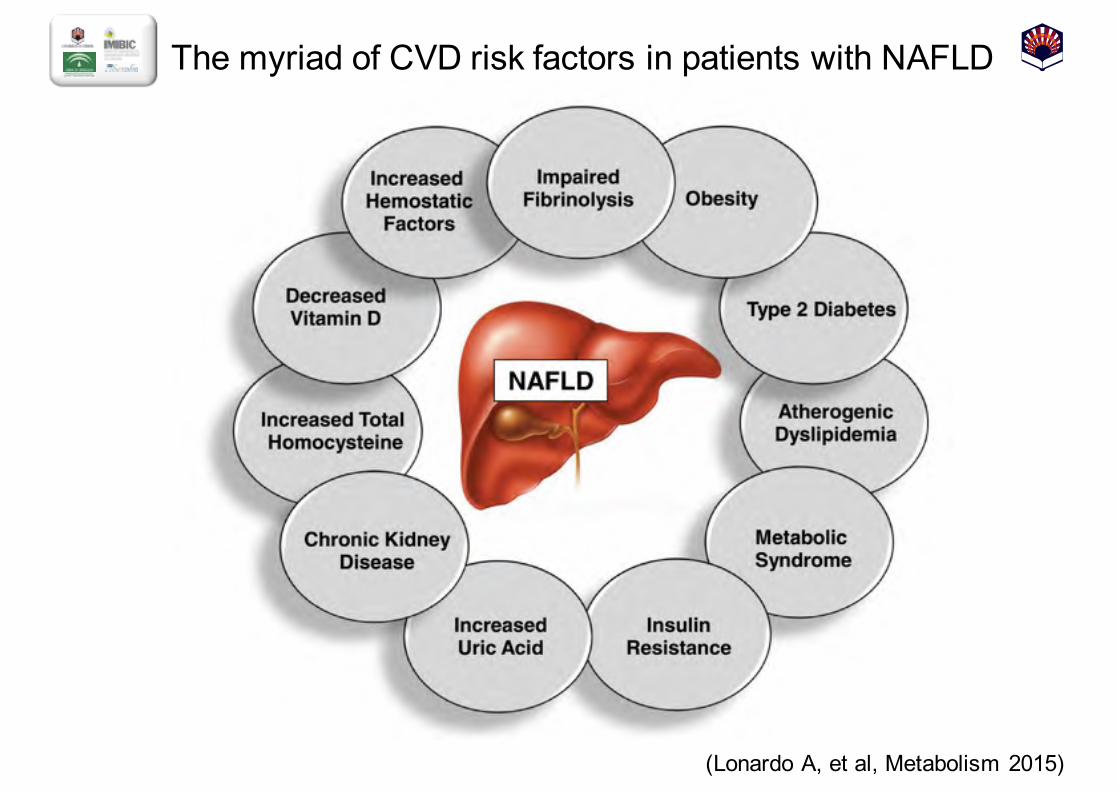
The myriad of CVD risk factors in patients with NAFLD
(Lonardo A, et al, Metabolism 2015)
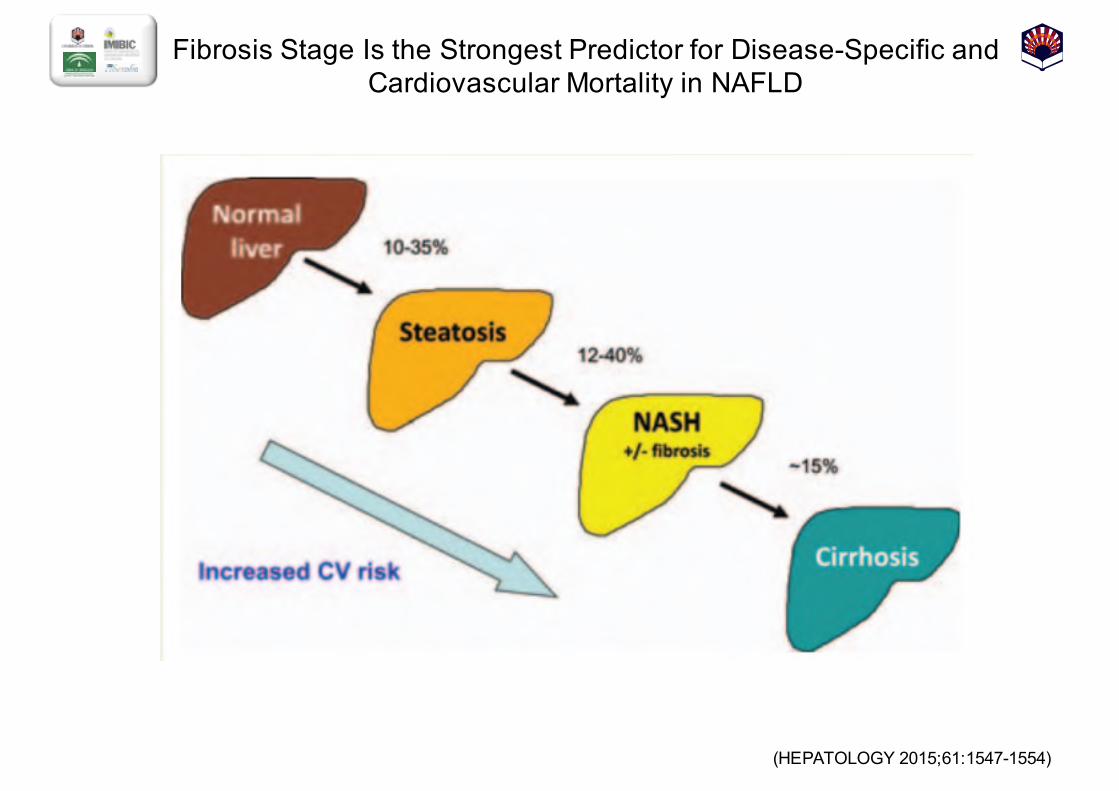
Fibrosis Stage Is the Strongest Predictor for Disease-Specific and Cardiovascular Mortality in NAFLD
(HEPATOLOGY 2015;;61:1547-1554)
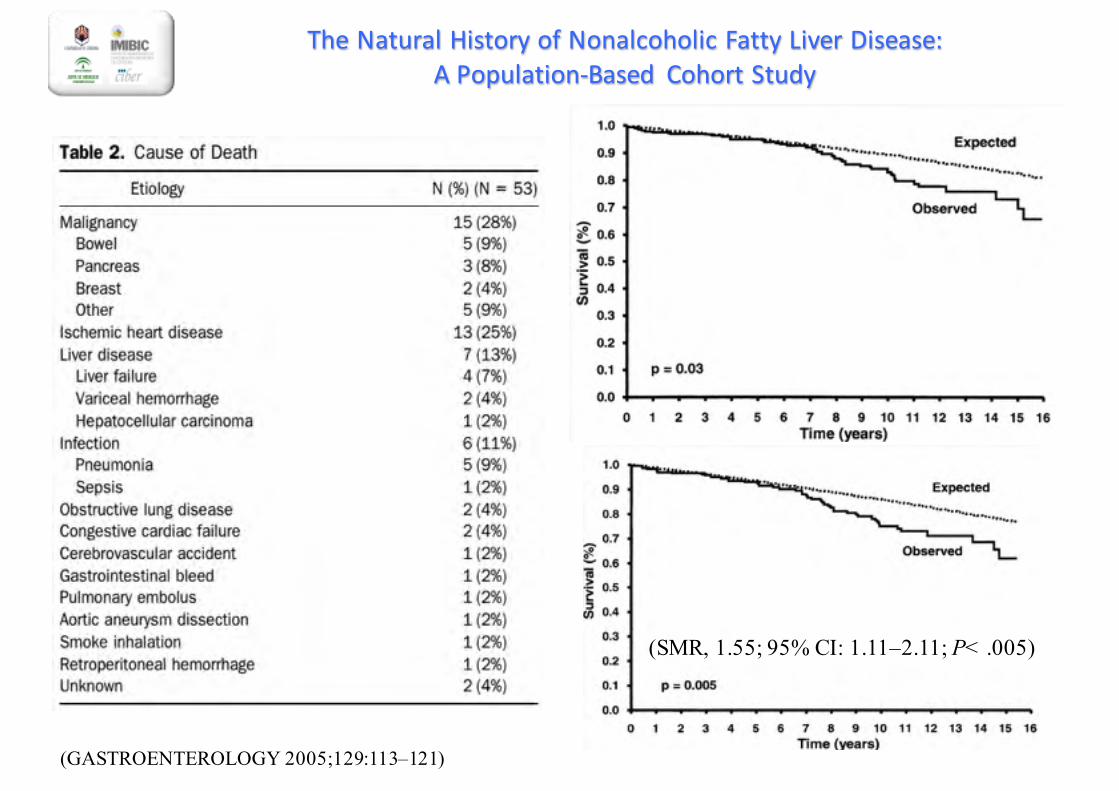
The Natural History of Nonalcoholic Fatty Liver Disease: A Population-‐Based Cohort Study
(GASTROENTEROLOGY 2005;129:113–121)
(SMR, 1.55; 95% CI: 1.11–2.11; P< .005)
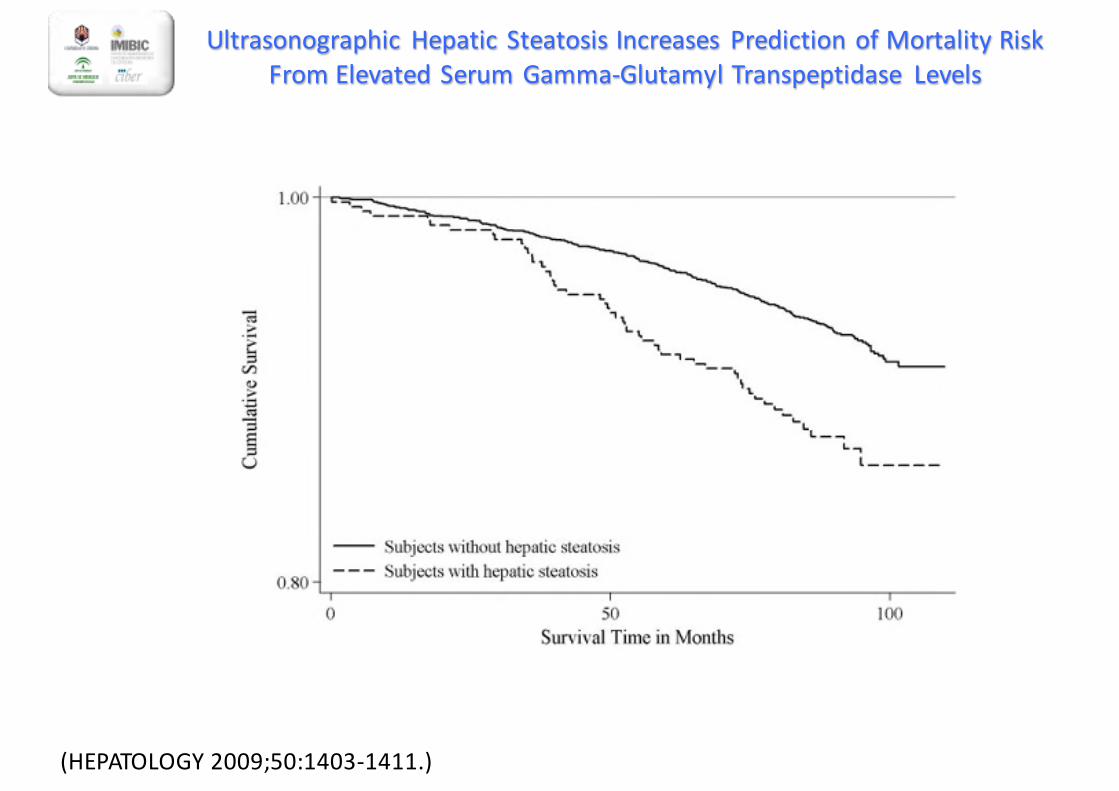
Ultrasonographic Hepatic Steatosis Increases Prediction of Mortality Risk From Elevated Serum Gamma-‐Glutamyl Transpeptidase Levels
(HEPATOLOGY 2009;50:1403-‐1411.)
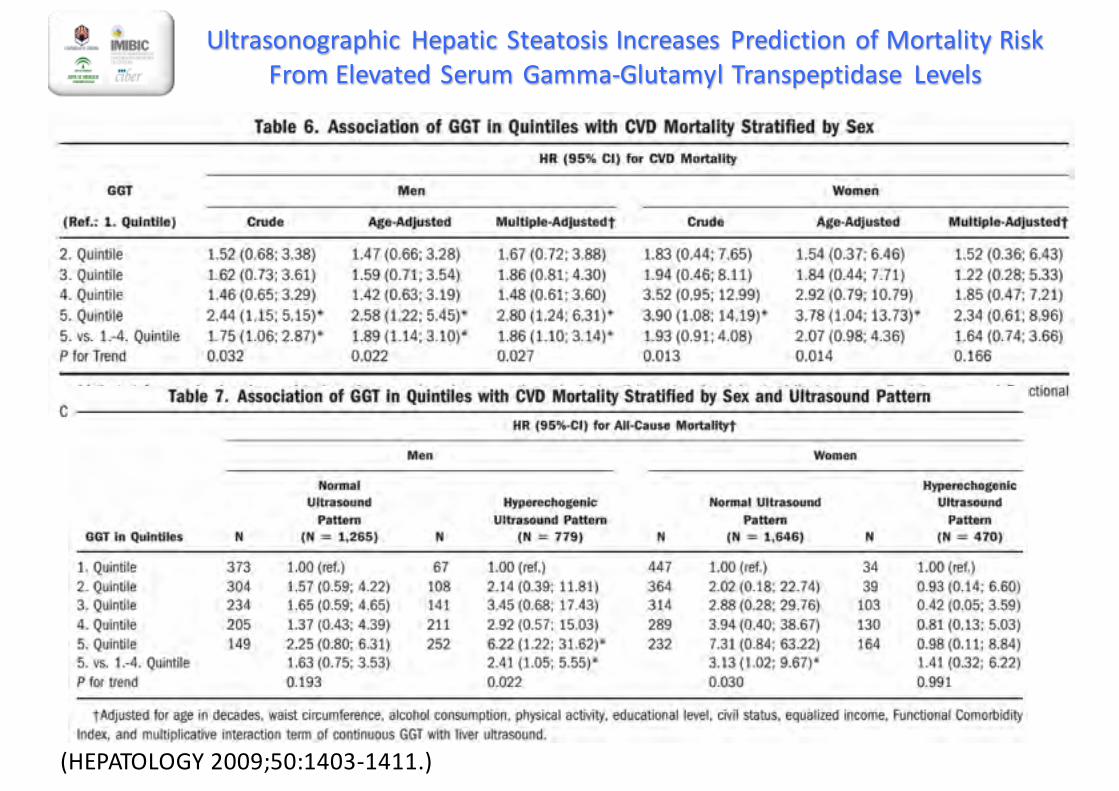
Ultrasonographic Hepatic Steatosis Increases Prediction of Mortality Risk From Elevated Serum Gamma-‐Glutamyl Transpeptidase Levels
(HEPATOLOGY 2009;50:1403-‐1411.)
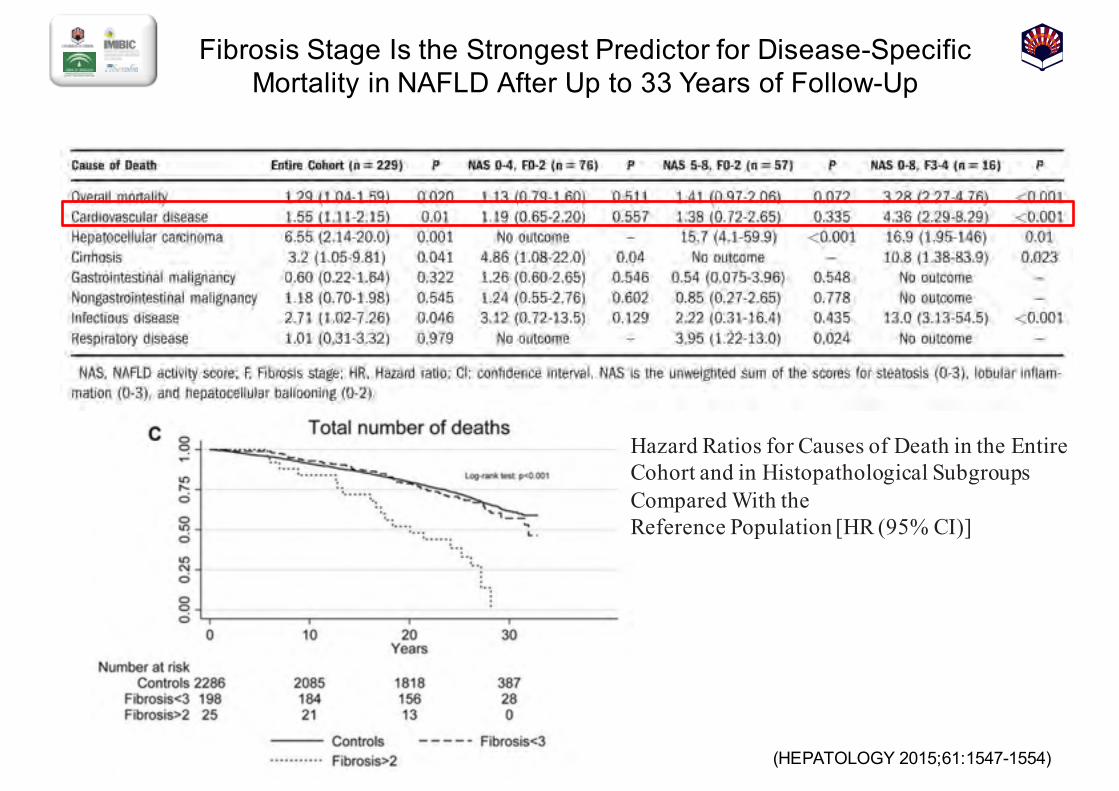
Fibrosis Stage Is the Strongest Predictor for Disease-Specific Mortality in NAFLD After Up to 33 Years of Follow-Up
(HEPATOLOGY 2015;;61:1547-1554)
Hazard Ratios for Causes of Death in the Entire Cohort and in Histopathological Subgroups Compared With theReference Population [HR (95% CI)]
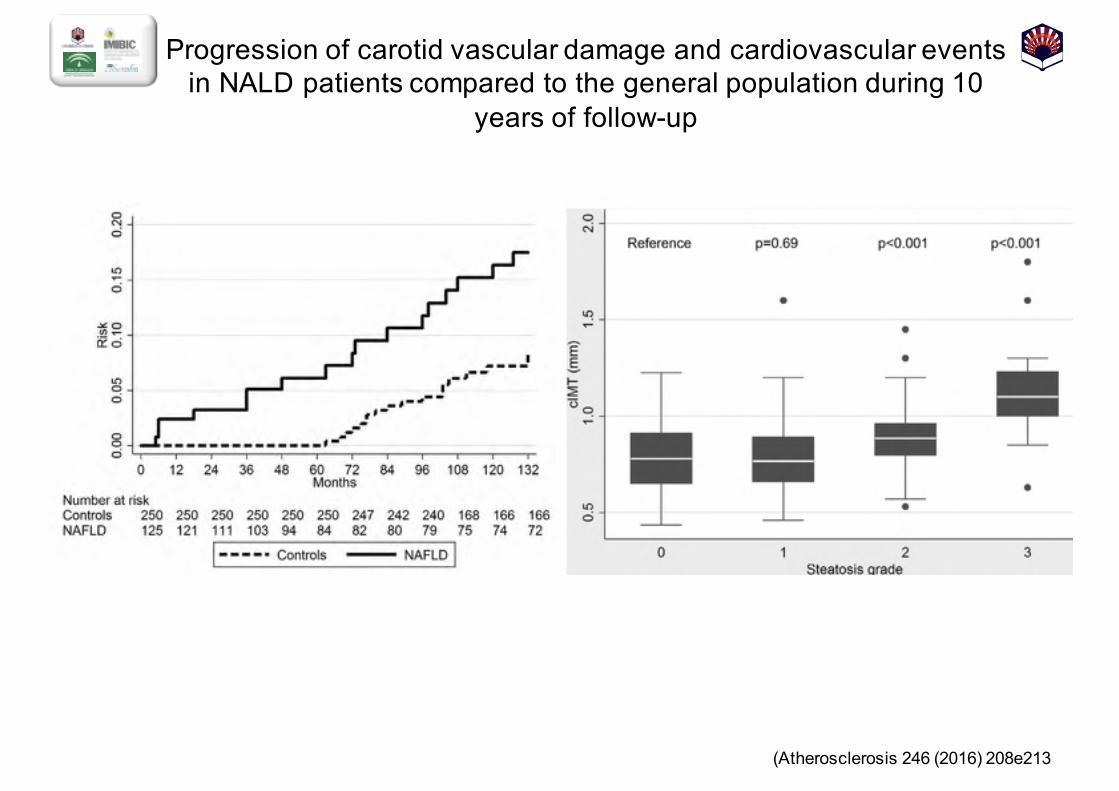
Progression of carotid vascular damage and cardiovascular events in NALD patients compared to the general population during 10
years of follow-up
(Atherosclerosis 246 (2016) 208e213
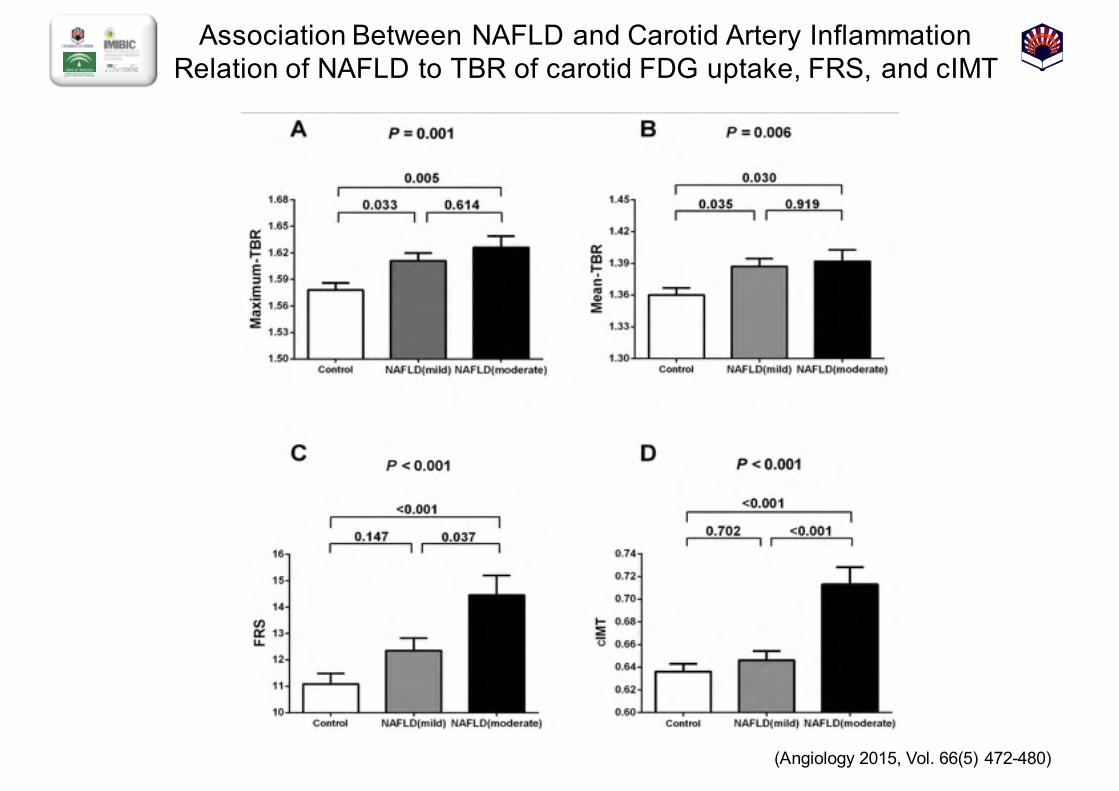
Association Between NAFLD and Carotid Artery Inflammation Relation of NAFLD to TBR of carotid FDG uptake, FRS, and cIMT
(Angiology 2015, Vol. 66(5) 472-480)
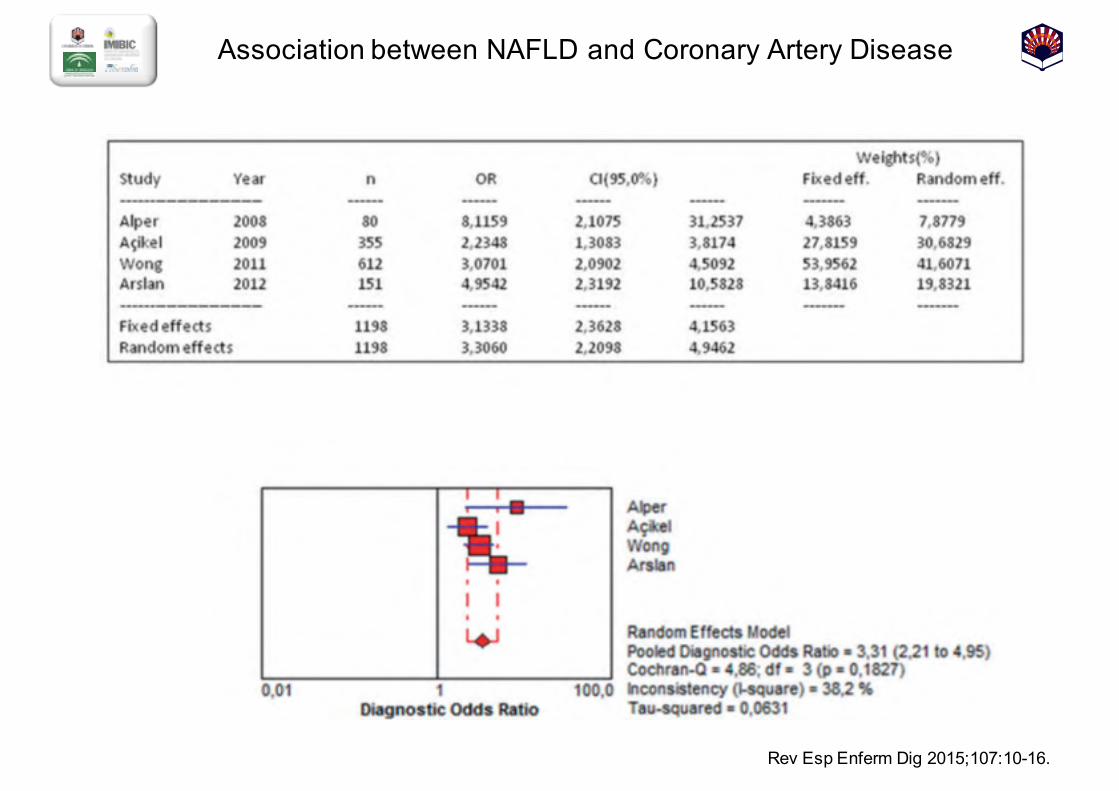
Association between NAFLD and Coronary Artery Disease
Rev Esp Enferm Dig 2015;;107:10-16.
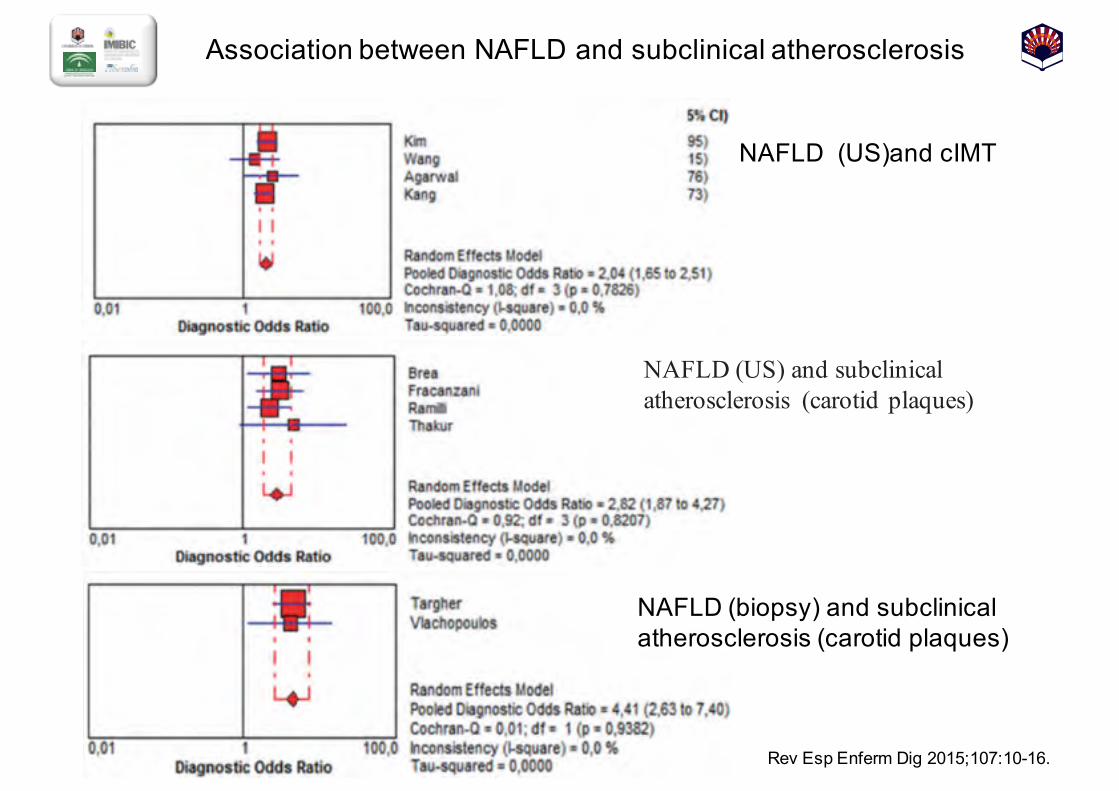
Association between NAFLD and subclinical atherosclerosis
Rev Esp Enferm Dig 2015;;107:10-16.
NAFLD (US)and cIMT
NAFLD (biopsy) and subclinical atherosclerosis (carotid plaques)
NAFLD (US) and subclinical atherosclerosis (carotid plaques)
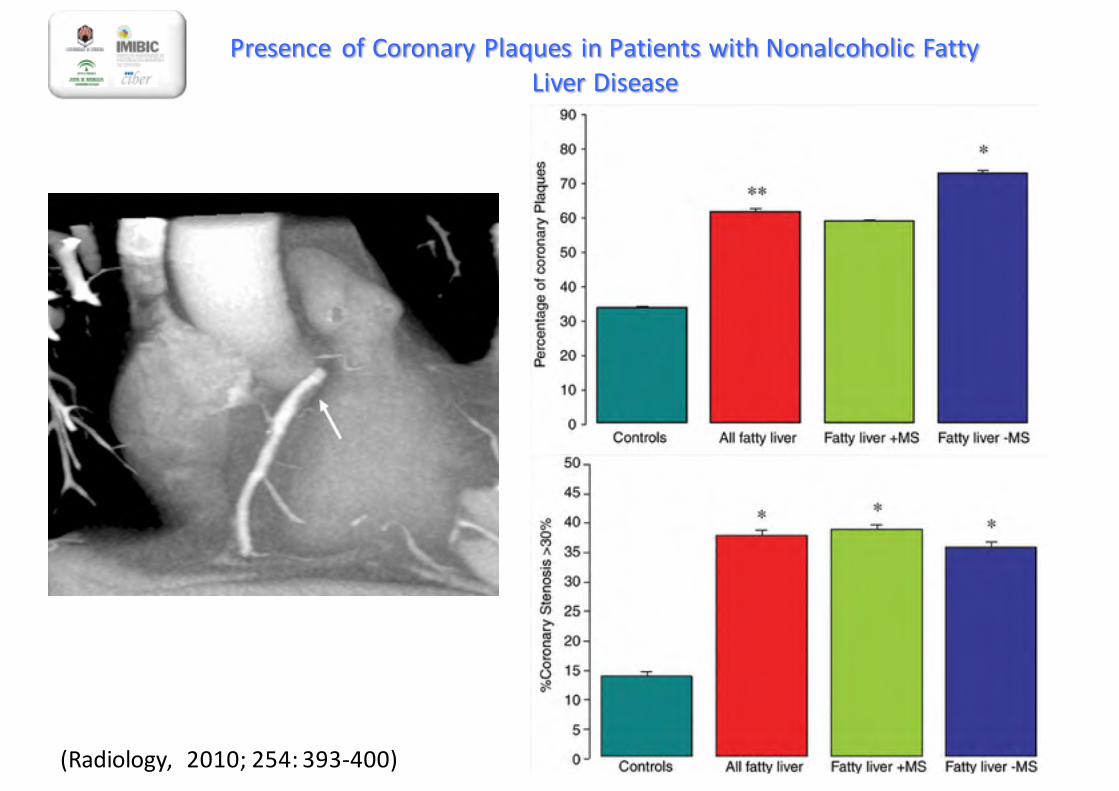
Presence of Coronary Plaques in Patients with Nonalcoholic FattyLiver Disease
(Radiology, 2010; 254: 393-‐400)
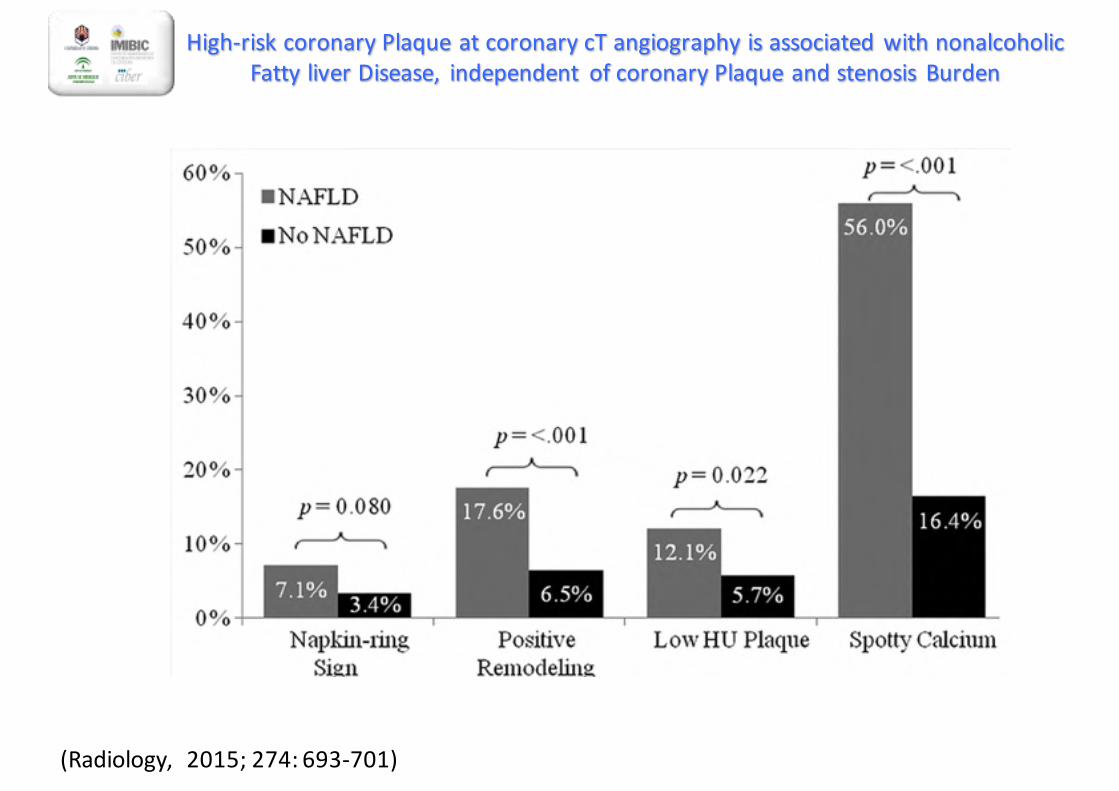
High-‐risk coronary Plaque at coronary cT angiography is associated with nonalcoholic Fatty liver Disease, independent of coronary Plaque and stenosis Burden
(Radiology, 2015; 274: 693-‐701)
VALORACIÓN Y MANEJO DEL RIESGO CARDIOVASCULAR
1. ¿Los pacientes con EHNA tienen un mayor riesgo dedesarrollar enfermedad cardiovascular?
RECOMENDACIÓN:Se debe evaluar el riesgo cardiovascular en todoslos enfermos con EHNA
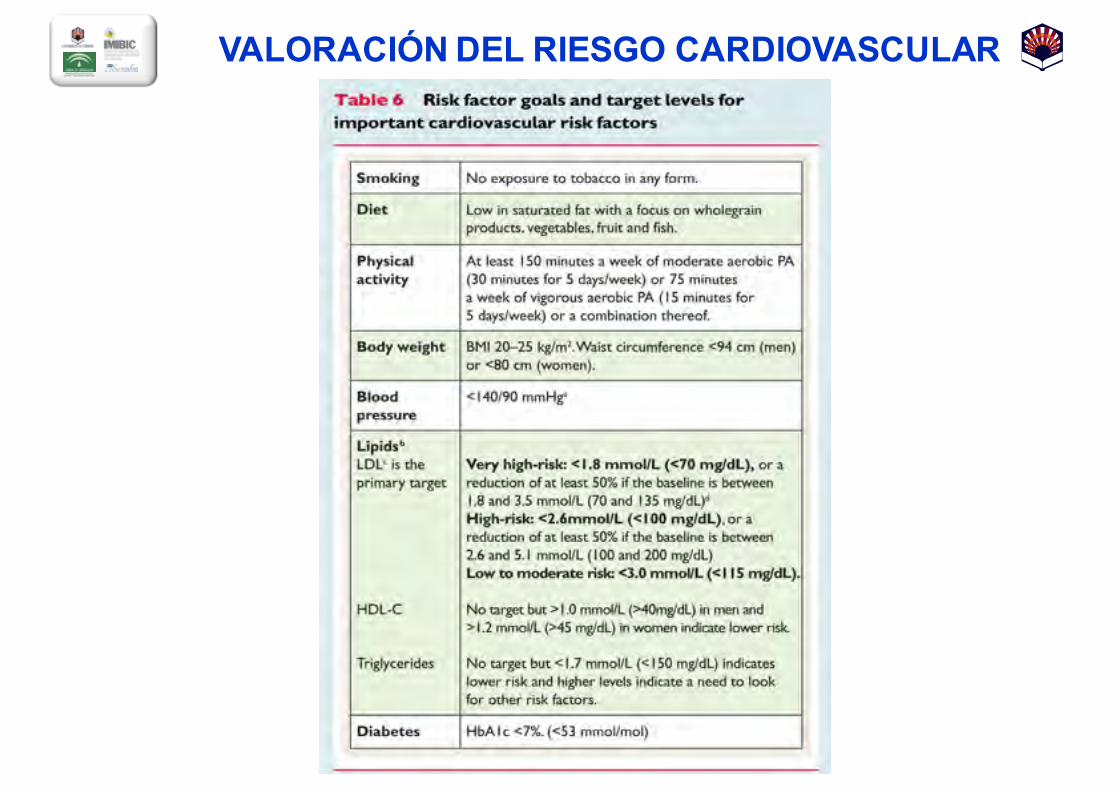
VALORACIÓN DEL RIESGO CARDIOVASCULAR
VALORACIÓN Y MANEJO DEL RIESGO CARDIOVASCULAR
1. ¿Los pacientes con EHNA tienen un mayor riesgo dedesarrollar enfermedad cardiovascular?
2. ¿Cuáles son las principales causas demorbimortalidad cardiovascular en pacientes conEHNA?
3. ¿Cómo podemos reducir el riesgo de padecerenfermedad cardiovascular en pacientes con EHNA?
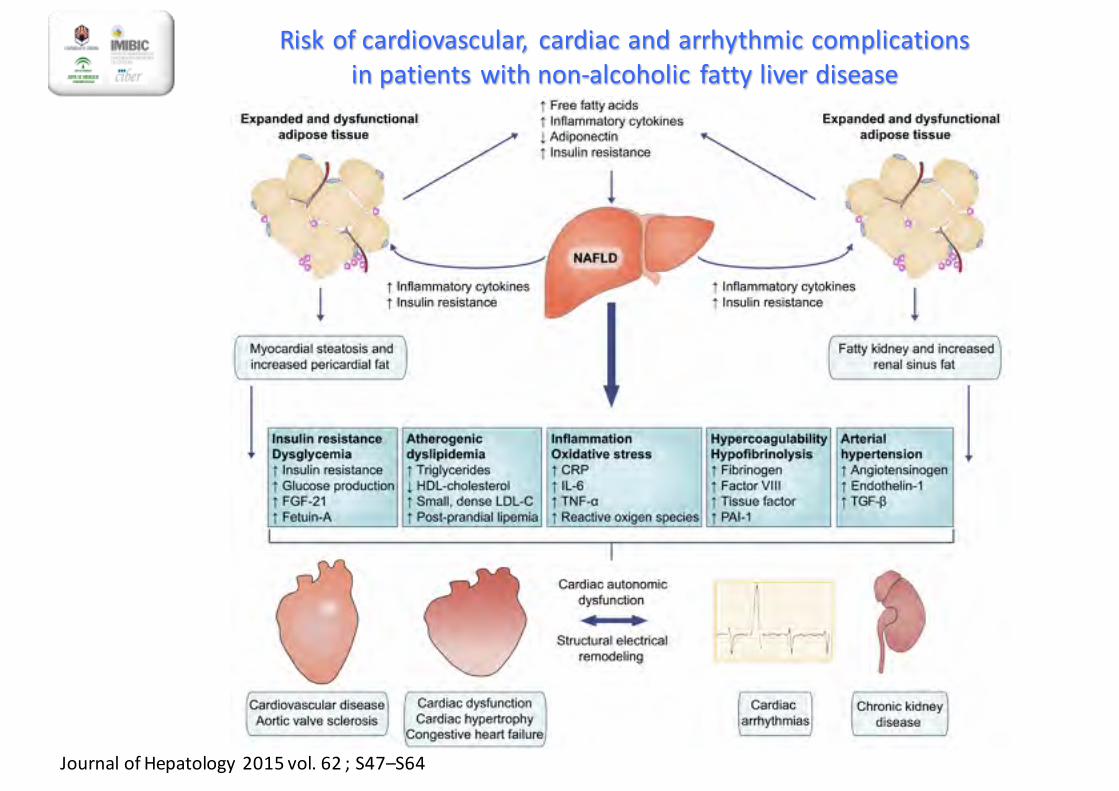
Risk of cardiovascular, cardiac and arrhythmic complicationsin patients with non-‐alcoholic fatty liver disease
Journal of Hepatology 2015 vol. 62 ; S47–S64
VALORACIÓN Y MANEJO DEL RIESGO CARDIOVASCULAR
(Lonardo A, et al, Metabolism 2015)
1. ¿Los pacientes con EHNA tienen un mayor riesgo dedesarrollar enfermedad cardiovascular?
2. ¿Cuáles son las principales causas demorbimortalidad cardiovascular en pacientes conEHNA?
3. ¿Cómo podemos reducir el riesgo de padecerenfermedad cardiovascular en pacientes con EHNA?
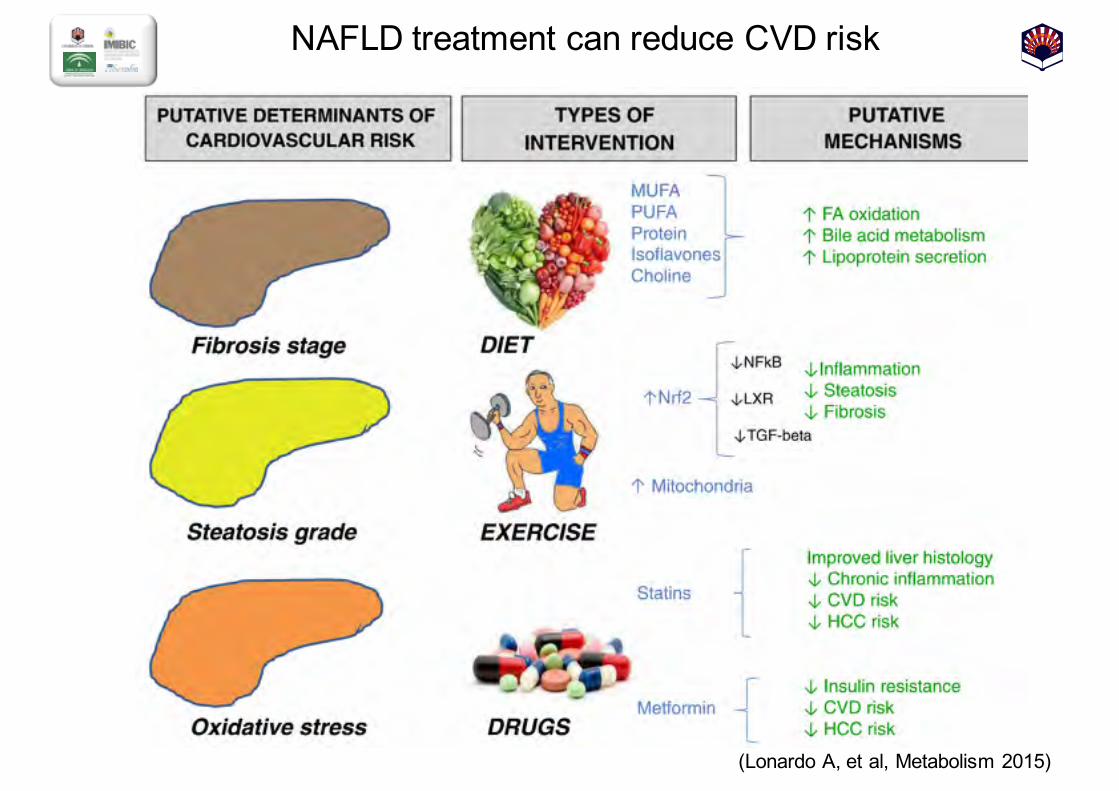
NAFLD treatment can reduce CVD risk
(Lonardo A, et al, Metabolism 2015)
3
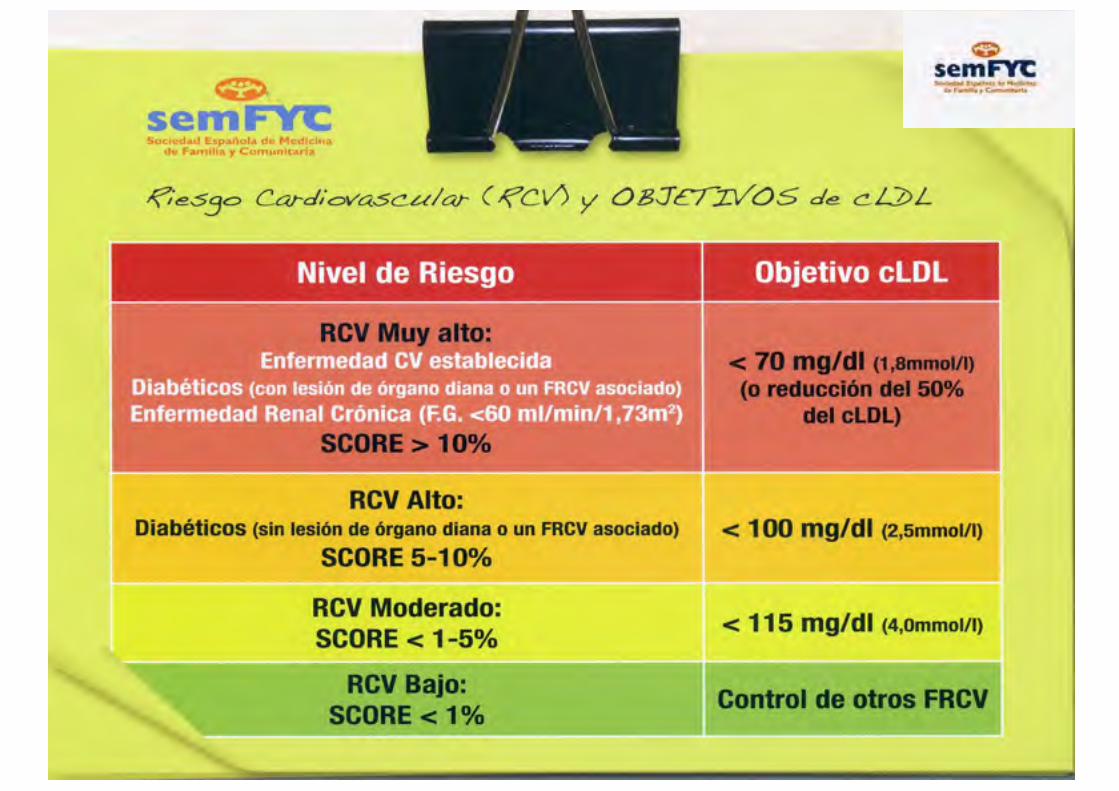
GUÍA semFYC 2012 PARA EL MANEJO PRÁCTICO DE LAS DISLIPEMIAS
3
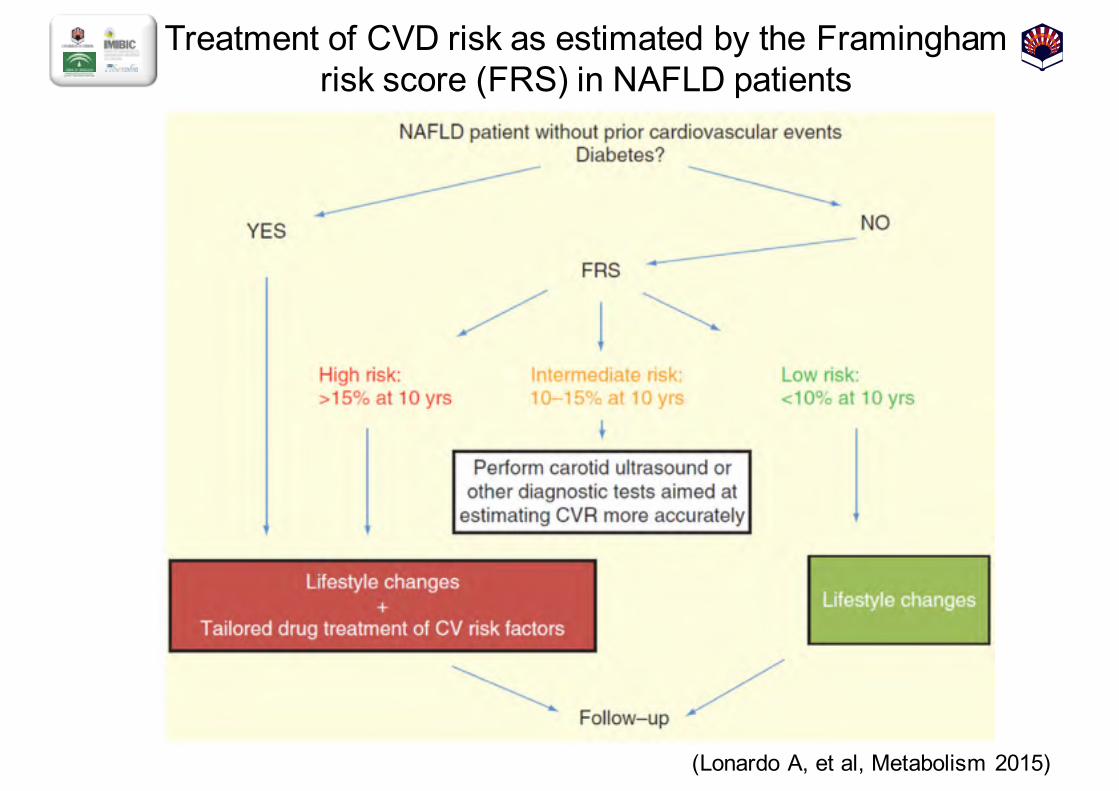
Treatment of CVD risk as estimated by the Framingham risk score (FRS) in NAFLD patients
(Lonardo A, et al, Metabolism 2015)
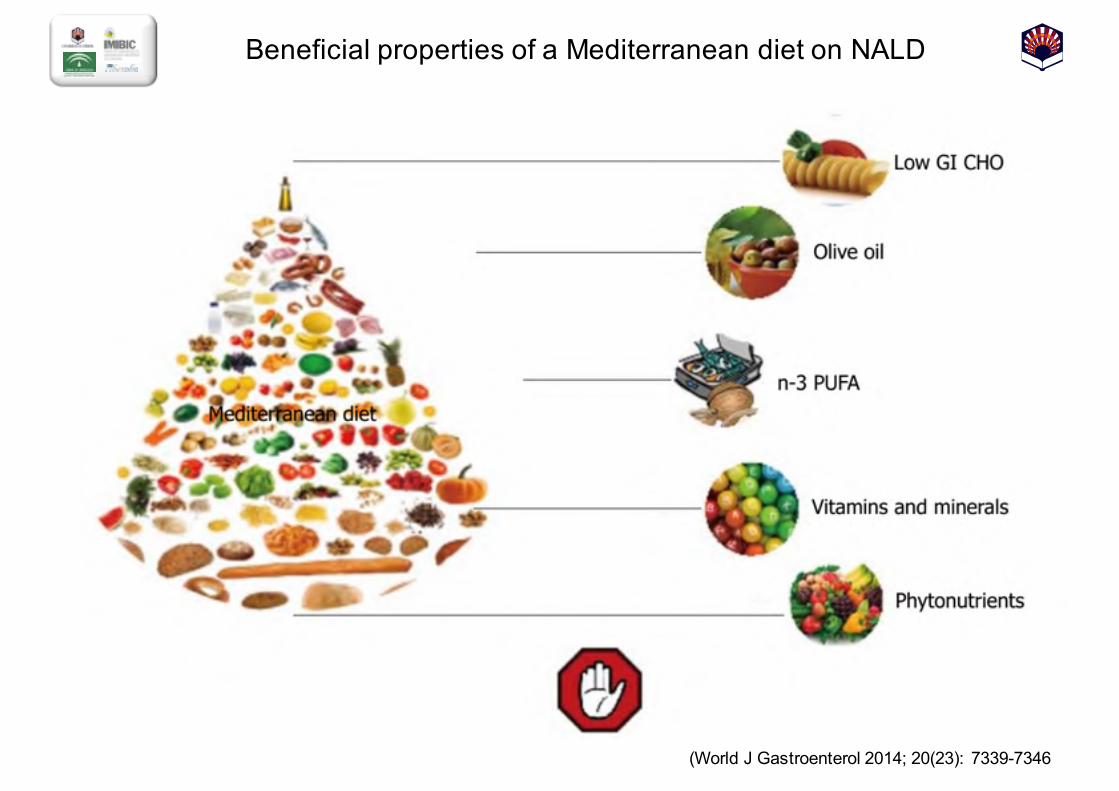
Beneficial properties of a Mediterranean diet on NALD
(World J Gastroenterol 2014;; 20(23): 7339-7346
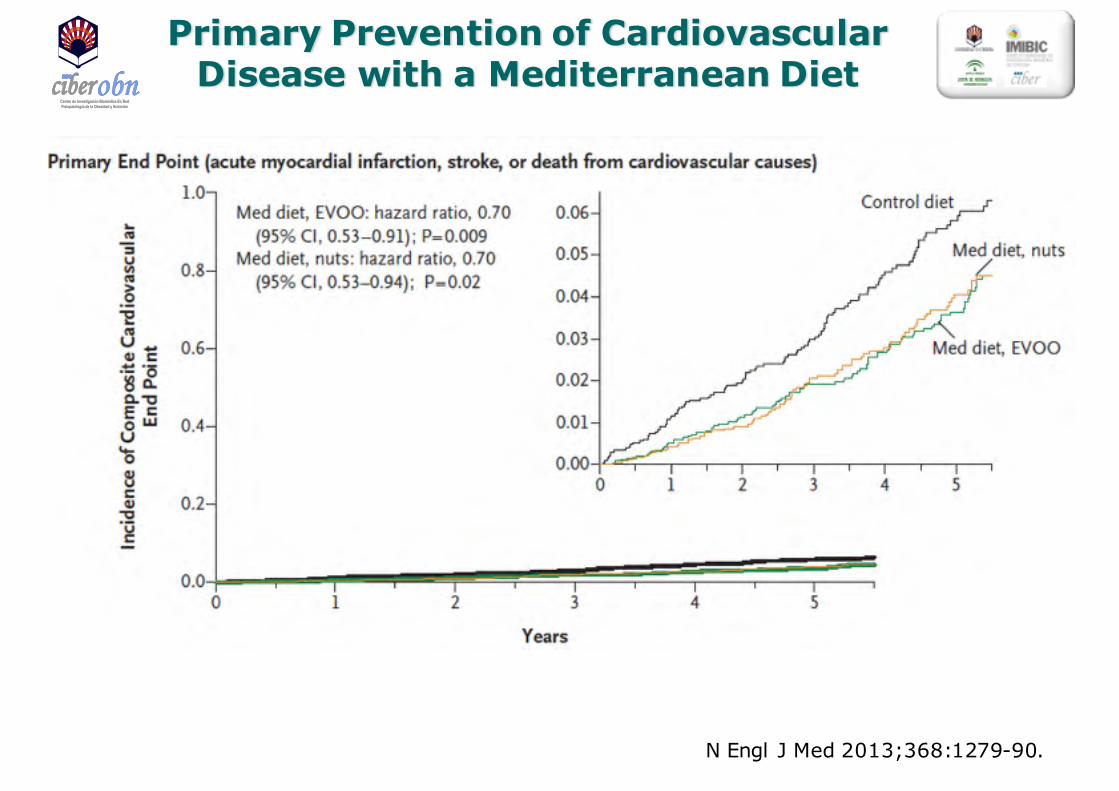
Primary Prevention of Cardiovascular Disease with a Mediterranean Diet
N Engl J Med 2013;368:1279-90.
Centro de Investigación Biomédica En RedFisiopatología de la Obesidad y Nutrición
Centro de Investigación Biomédica En RedFisiopatología de la Obesidad y Nutrición
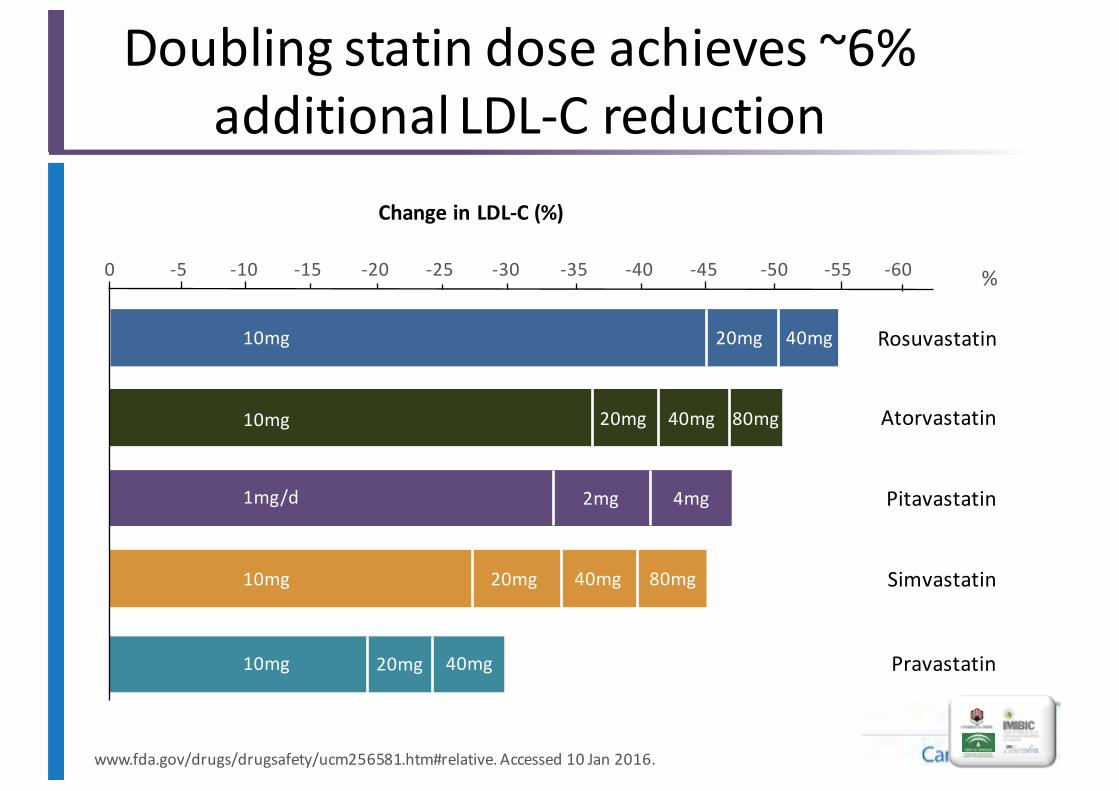
%-‐60-‐55-‐50-‐45-‐40-‐35-‐30-‐25-‐20-‐15-‐10-‐50
Rosuvastatin
10mg
40mg20mg
20mg Atorvastatin80mg40mg
Simvastatin10mg 20mg 40mg 80mg
Pravastatin10mg 20mg 40mg
Pitavastatin1mg/d 2mg 4mg
10mg
Doubling statin dose achieves ~6% additional LDL-‐C reduction
www.fda.gov/drugs/drugsafety/ucm256581.htm#relative. Accessed 10 Jan 2016.
Change in LDL-‐C (%)

CTT Collaborators. Lancet 2005;366:1267–1278.
Relación entre la reducción proporcional de episodios y la disminución media del C-‐LDL al cabo de 1 año
Una reducción del C-LDL de 1 mmol/l (39 mg/dl) se tradujo en...
Re
du
cció
n p
rop
orc
ion
al d
e la
ta
sa d
e e
pis
od
ios
(%±E
E)
Re
du
cció
n p
rop
orc
ion
al d
e la
ta
sa d
e e
pis
od
ios
(%±E
E)
50
40
30
20
10
00,5
(19)1,0
(38)1,5
(58)2,0
(77)-10
Reducción del C-LDL, mmol/l (mg/dl)
50
40
30
20
10
-10
00,5
(19)1,0
(38)1,5
(58)2,0
(77)
Reducción del C-LDL, mmol/l (mg/dl)
Metanálisis prospectivo de los datos de 90.056 pacientes procedentes de 14 ensayos de estatinas
… una reducción de los episodios coronarios principales del 23%
… una reducción de los episodios vasculares principales del 21%
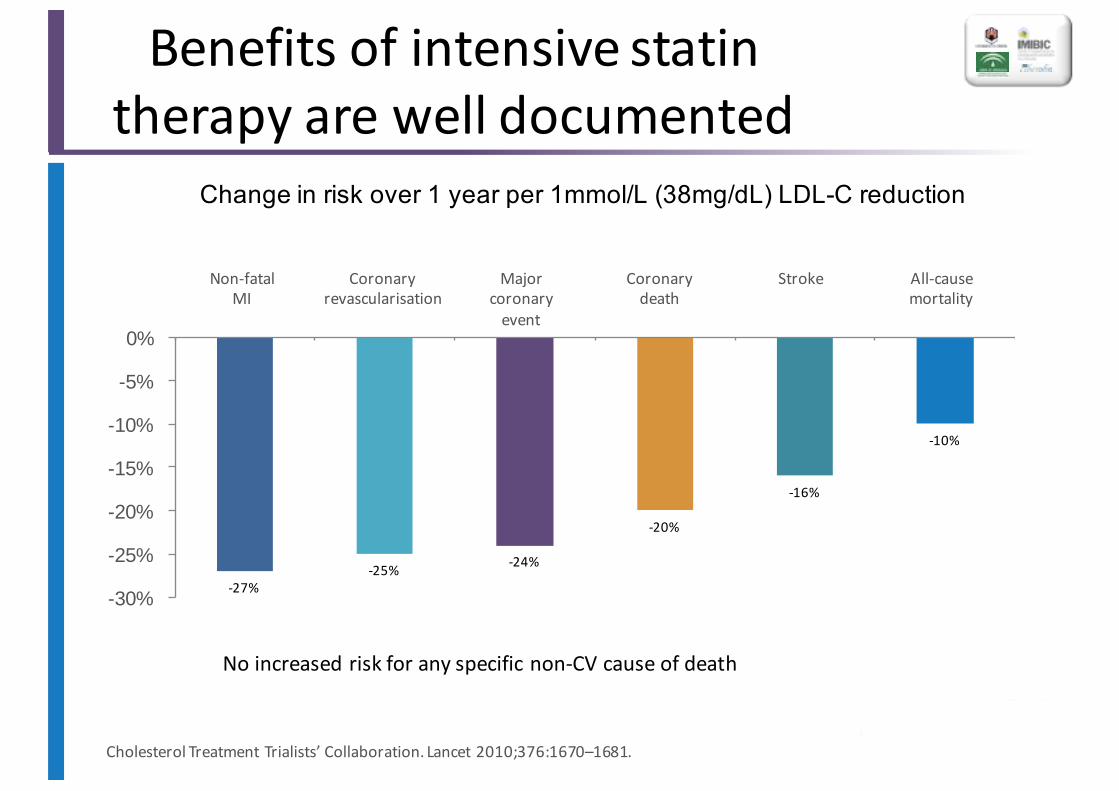
Benefits of intensive statin therapy are well documented
No increased risk for any specific non-‐CV cause of death
Cholesterol Treatment Trialists’ Collaboration. Lancet 2010;376:1670–1681.
-‐27%-‐25% -‐24%
-‐20%
-‐16%
-‐10%
-30%
-25%
-20%
-15%
-10%
-5%
0%
Non-‐fatal MI
Coronaryrevascularisation
Majorcoronaryevent
Coronarydeath
Stroke All-‐causemortality
Change in risk over 1 year per 1mmol/L (38mg/dL) LDL-C reduction
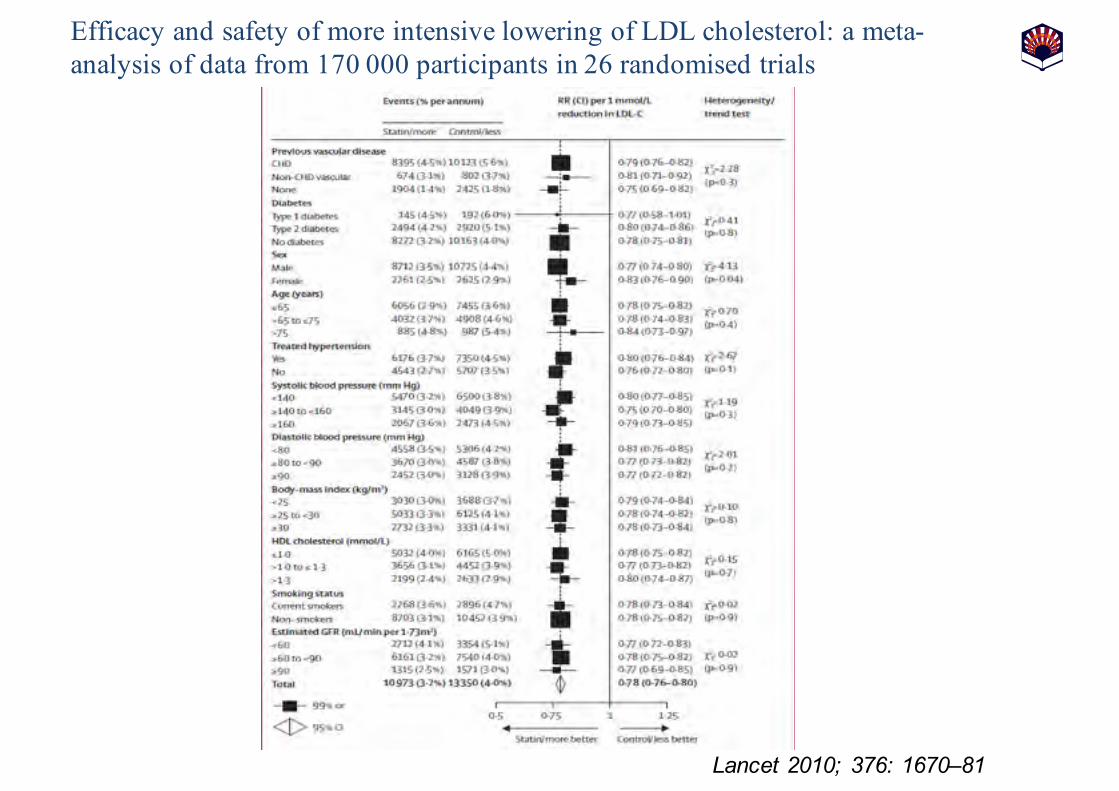
Lancet 2010;; 376: 1670–81
Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials
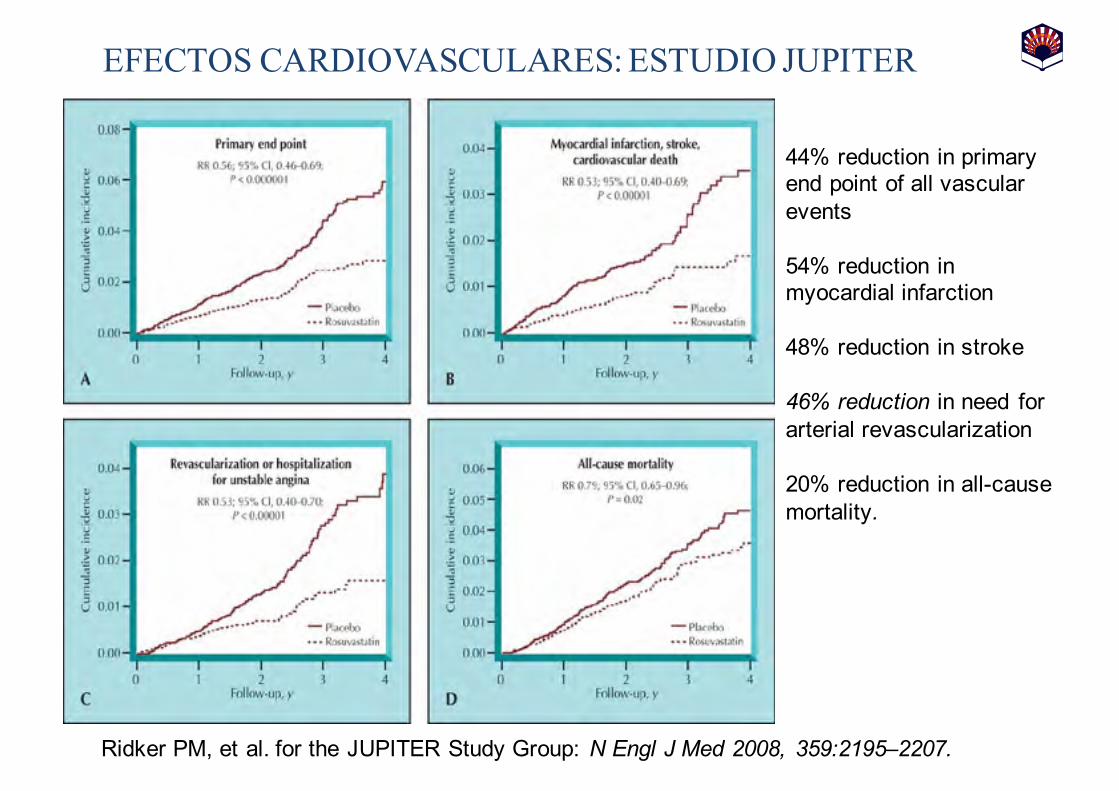
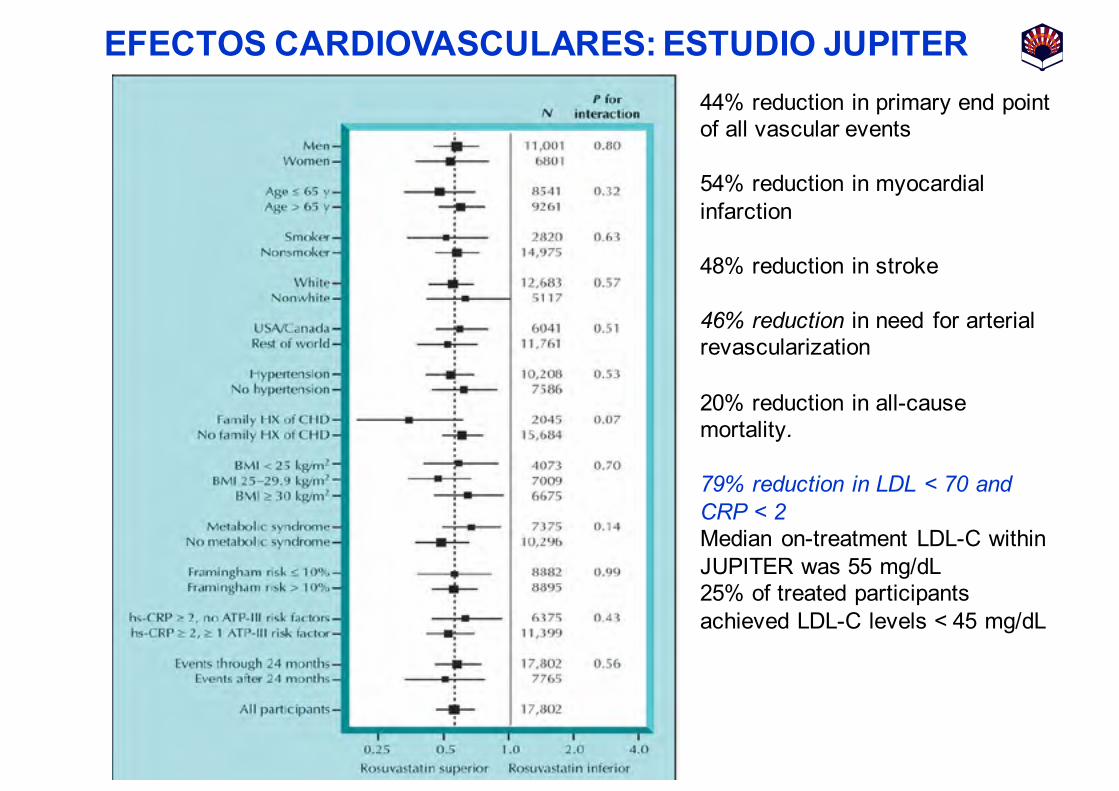
EFECTOS CARDIOVASCULARES: ESTUDIO JUPITER
Ridker PM, et al. for the JUPITER Study Group: N Engl J Med 2008, 359:2195–2207.
44% reduction in primary end point of all vascular events
54% reduction in myocardial infarction
48% reduction in stroke
46% reduction in need for arterial revascularization
20% reduction in all-cause mortality.
EFECTOS CARDIOVASCULARES: ESTUDIO JUPITER44% reduction in primary end point of all vascular events
54% reduction in myocardial infarction
48% reduction in stroke
46% reduction in need for arterial revascularization
20% reduction in all-cause mortality.
79% reduction in LDL < 70 and CRP < 2 Median on-treatment LDL-C within JUPITER was 55 mg/dL25% of treated participantsachieved LDL-C levels < 45 mg/dL
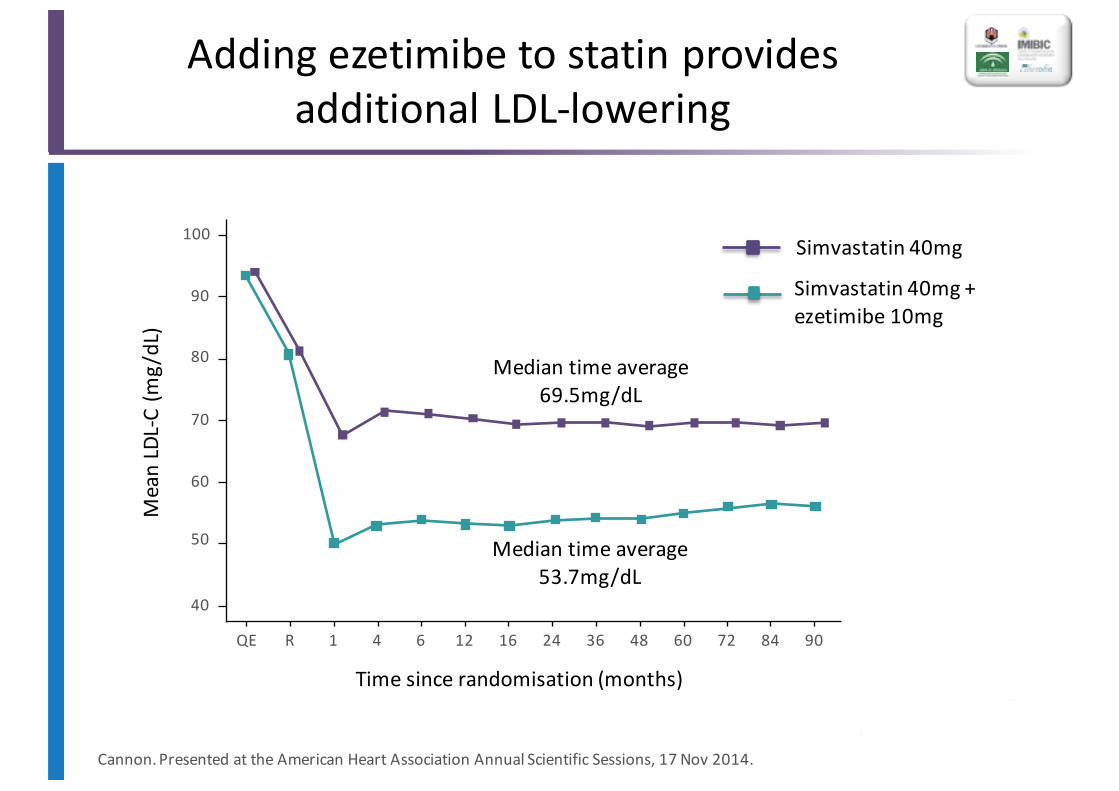
Adding ezetimibe to statin provides additional LDL-‐lowering
Cannon.Presented at the American Heart Association Annual Scientific Sessions, 17 Nov 2014.
100
90
80
70
60
50
40
QE 90R 1 4 847260483624166 12
Mean LDL-‐C (m
g/dL)
Time since randomisation (months)
Median time average53.7mg/dL
Median time average69.5mg/dL
Simvastatin 40mg
Simvastatin 40mg + ezetimibe 10mg
Event rate (%)
Years since randomisation
0
40
30
20
10
0 71 2 3 4 5 6
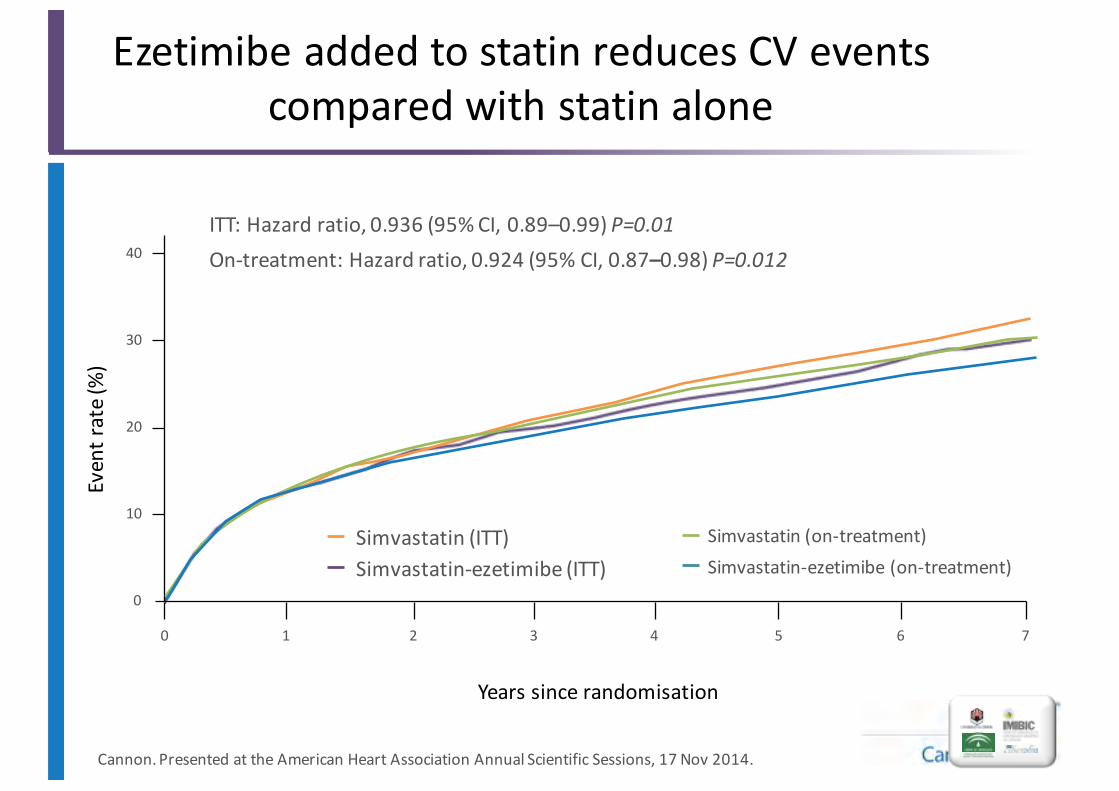
Ezetimibe added to statin reduces CV events compared with statin alone
ITT: Hazard ratio, 0.936 (95%CI, 0.89–0.99) P=0.01
Simvastatin (on-‐treatment)Simvastatin-‐ezetimibe (on-‐treatment)
Simvastatin (ITT)Simvastatin-‐ezetimibe (ITT)
On-‐treatment: Hazard ratio, 0.924 (95% CI, 0.87–0.98) P=0.012
Cannon.Presented at the American Heart Association Annual Scientific Sessions, 17 Nov 2014.
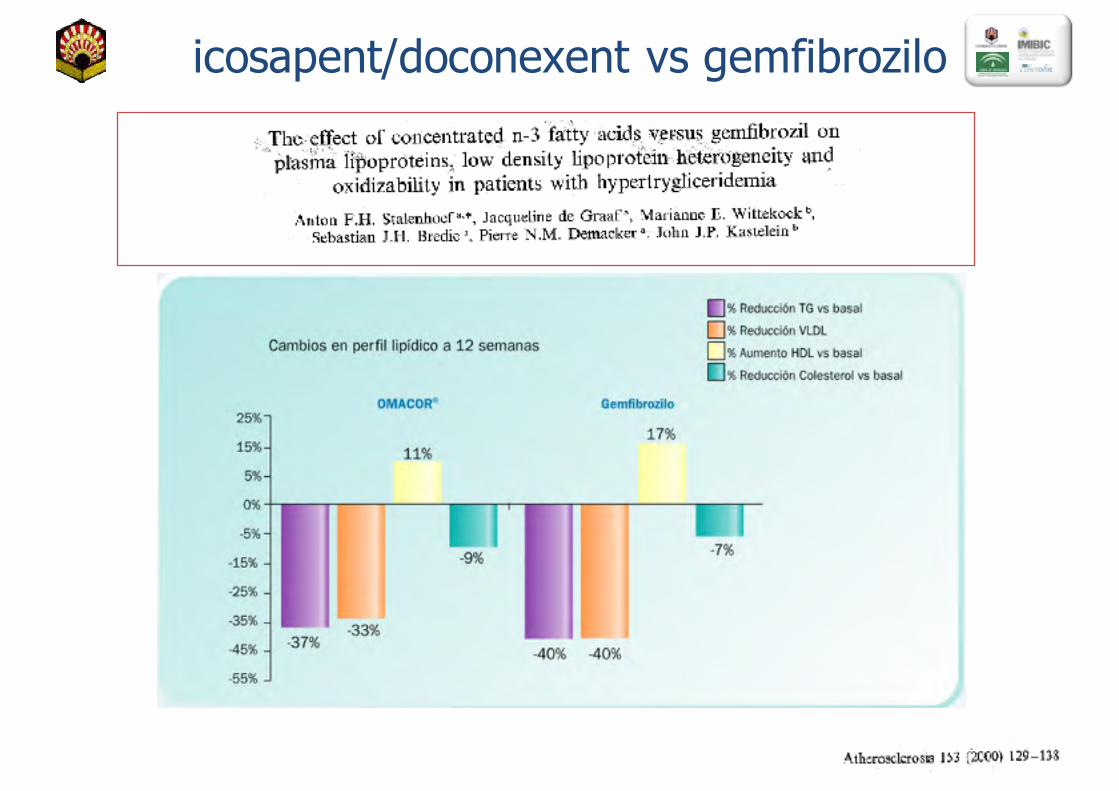
icosapent/doconexent vs gemfibrozilo
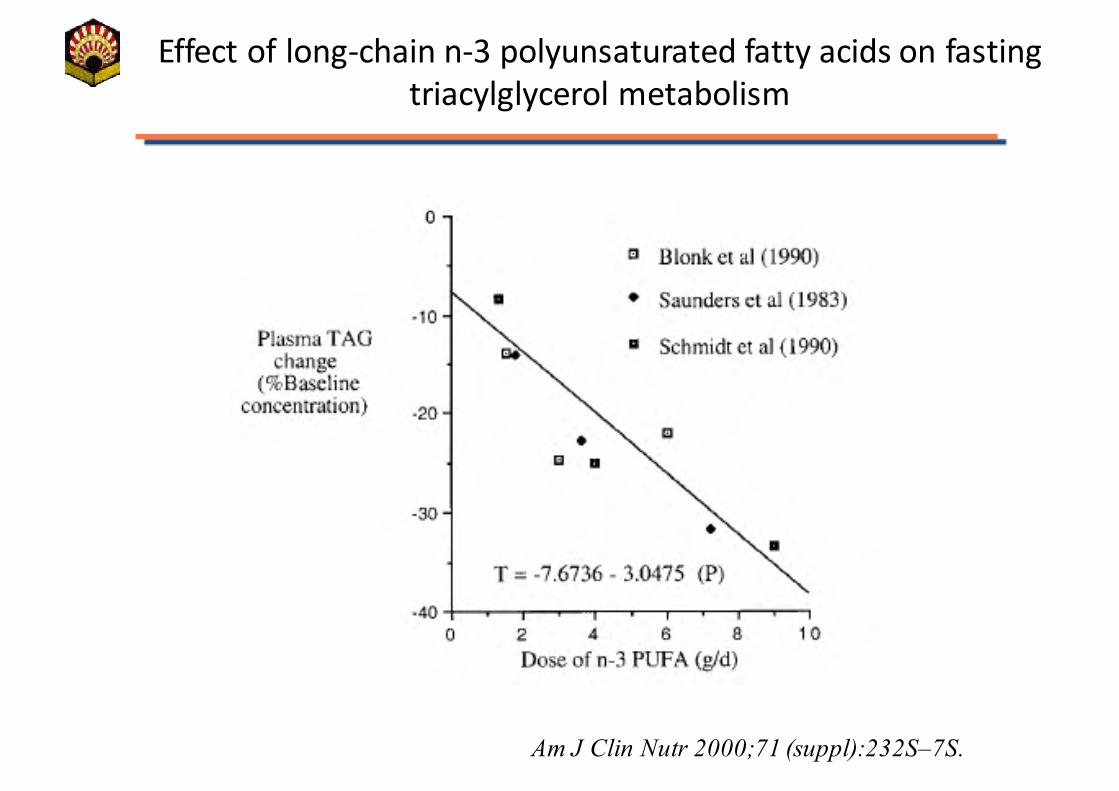
Effect of long-‐chain n-‐3 polyunsaturated fatty acids on fasting triacylglycerol metabolism
Am J Clin Nutr 2000;71 (suppl):232S–7S.
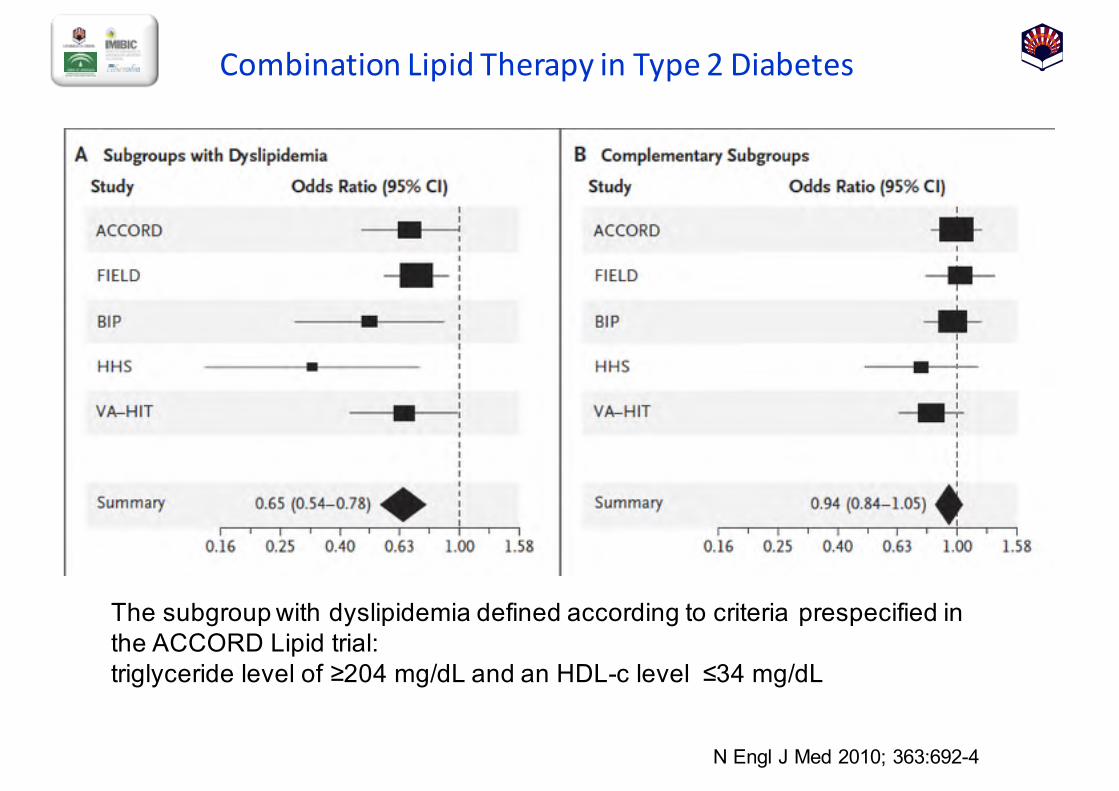
Combination Lipid Therapy in Type 2 Diabetes
N Engl J Med 2010;; 363:692-4
The subgroup with dyslipidemia defined according to criteria prespecified in the ACCORD Lipid trial: triglyceride level of ≥204 mg/dL and an HDL-c level ≤34 mg/dL
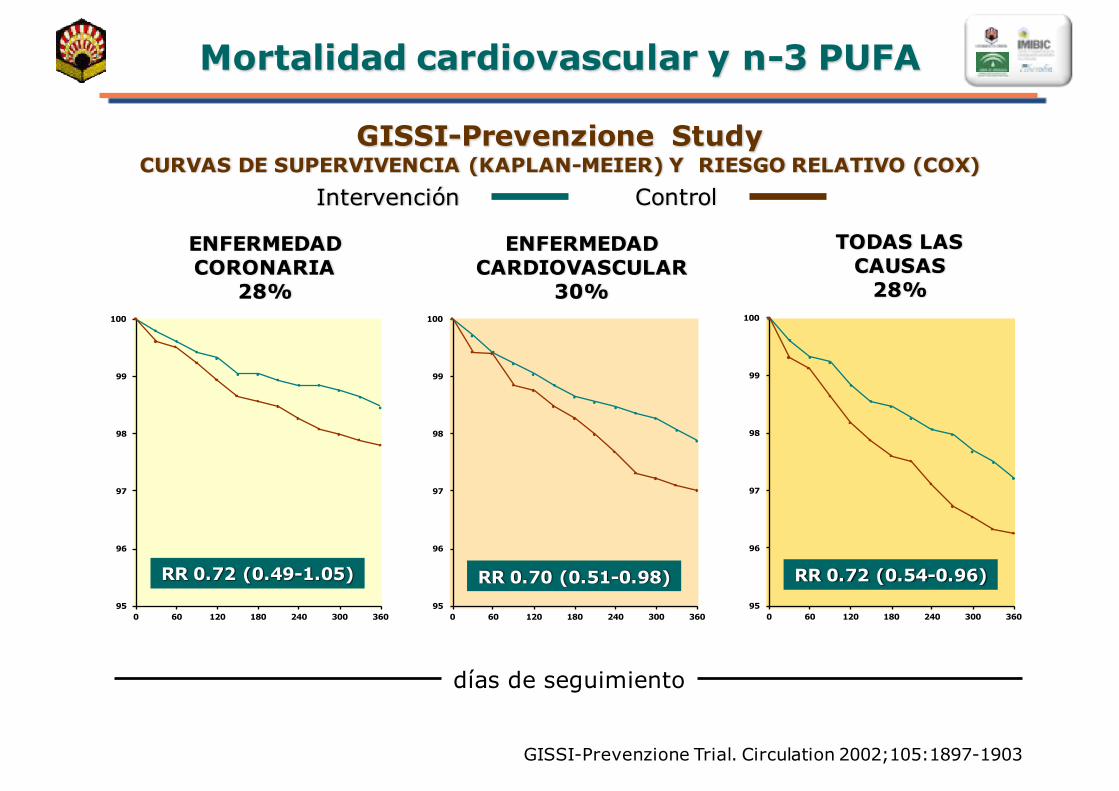
Mortalidad cardiovascular y n-3 PUFA
GISSI-Prevenzione Trial. Circulation 2002;105:1897-1903
días de seguimiento
GISSI-Prevenzione StudyCURVAS DE SUPERVIVENCIA (KAPLAN-MEIER) Y RIESGO RELATIVO (COX)
Intervención Control
95
96
97
98
99
100
0 60 120 180 240 300 360
ENFERMEDAD CORONARIA
28%
RR 0.72 (0.49-1.05)
ENFERMEDAD CARDIOVASCULAR
30%
RR 0.70 (0.51-0.98)95
96
97
98
99
100
0 60 120 180 240 300 360
TODAS LAS CAUSAS
28%
RR 0.72 (0.54-0.96)95
96
97
98
99
100
0 60 120 180 240 300 360
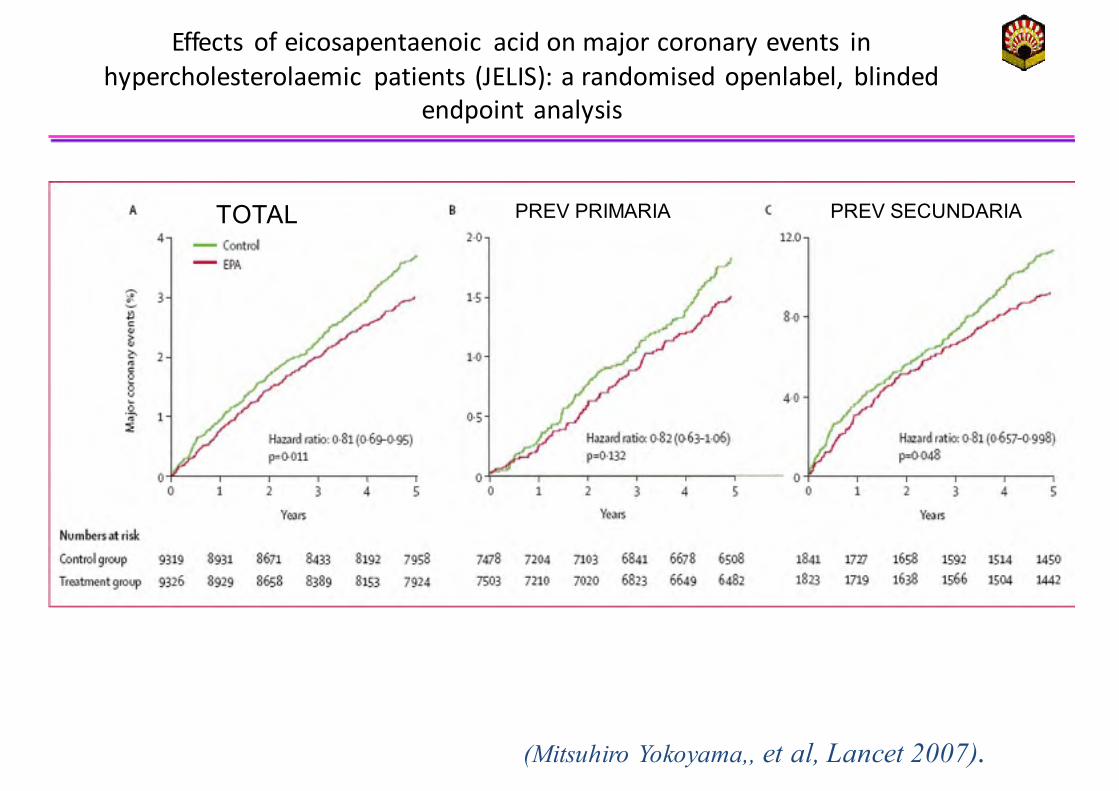
Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised openlabel, blinded
endpoint analysis
(Mitsuhiro Yokoyama,, et al, Lancet 2007).
TOTAL PREV PRIMARIA PREV SECUNDARIA
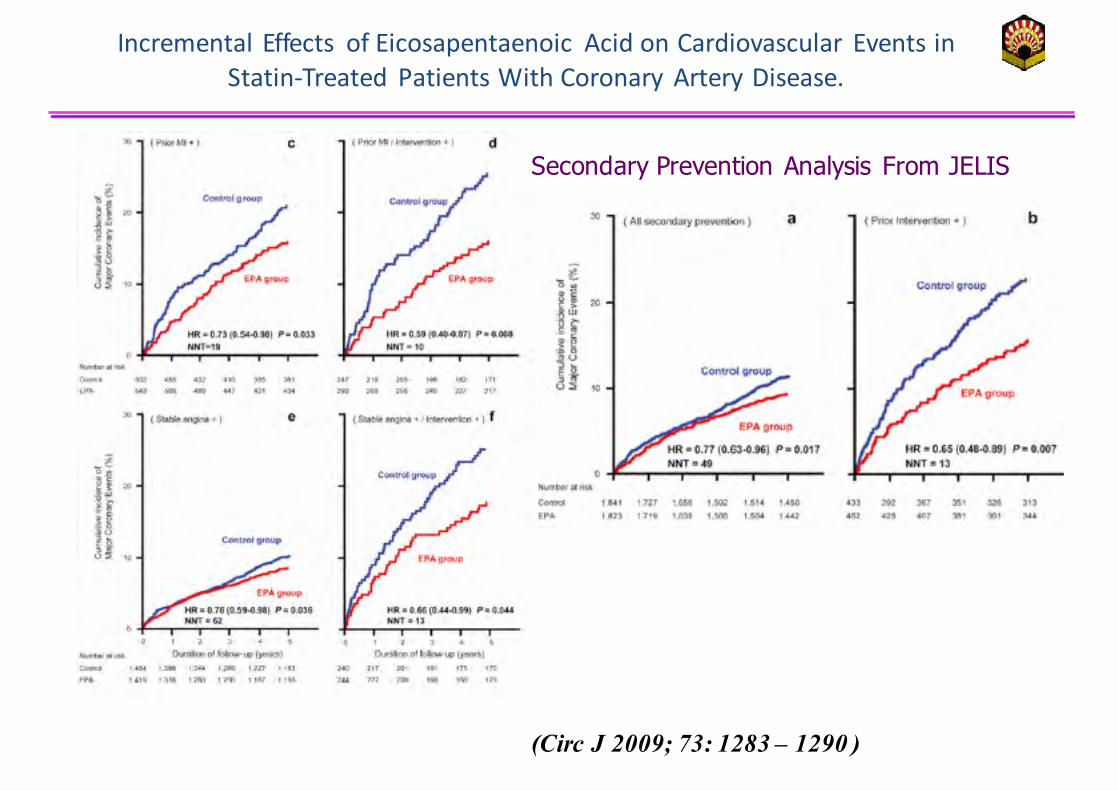
Incremental Effects of Eicosapentaenoic Acid on Cardiovascular Events in Statin-‐Treated Patients With Coronary Artery Disease.
(Circ J 2009; 73: 1283 – 1290 )
Secondary Prevention Analysis From JELIS
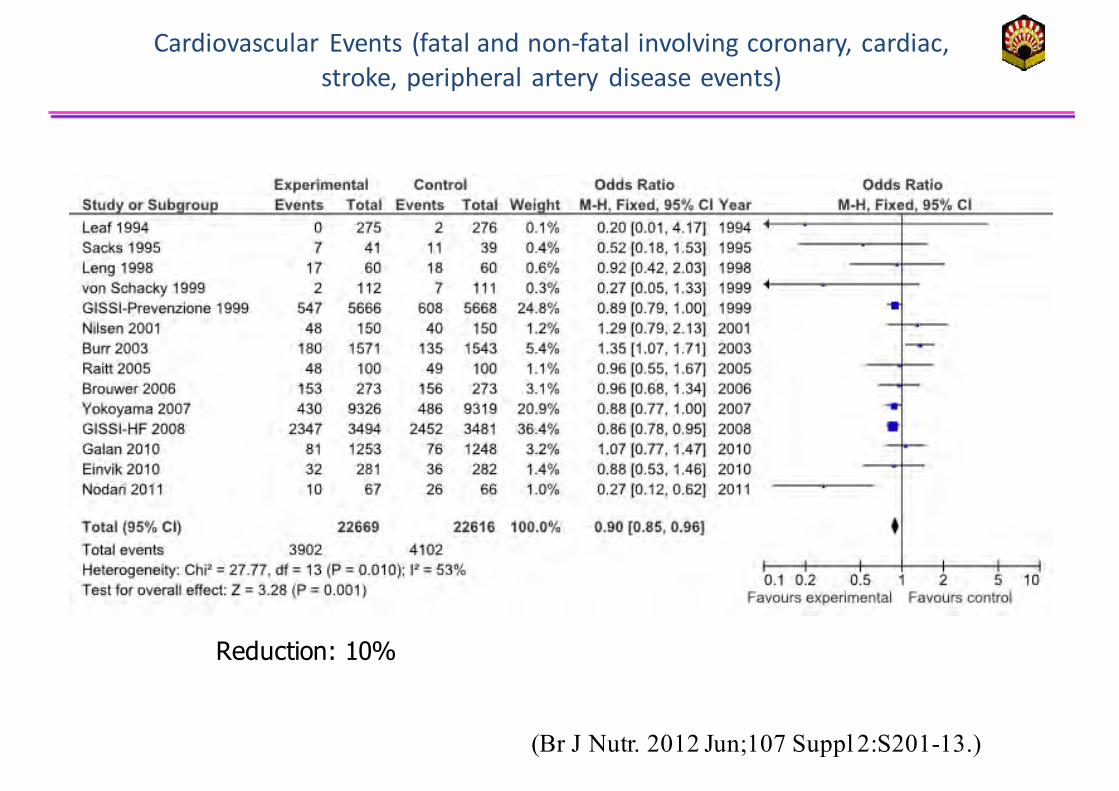
Cardiovascular Events (fatal and non-‐fatal involving coronary, cardiac, stroke, peripheral artery disease events)
(Br J Nutr. 2012 Jun;107 Suppl 2:S201-13.)
Reduction: 10%
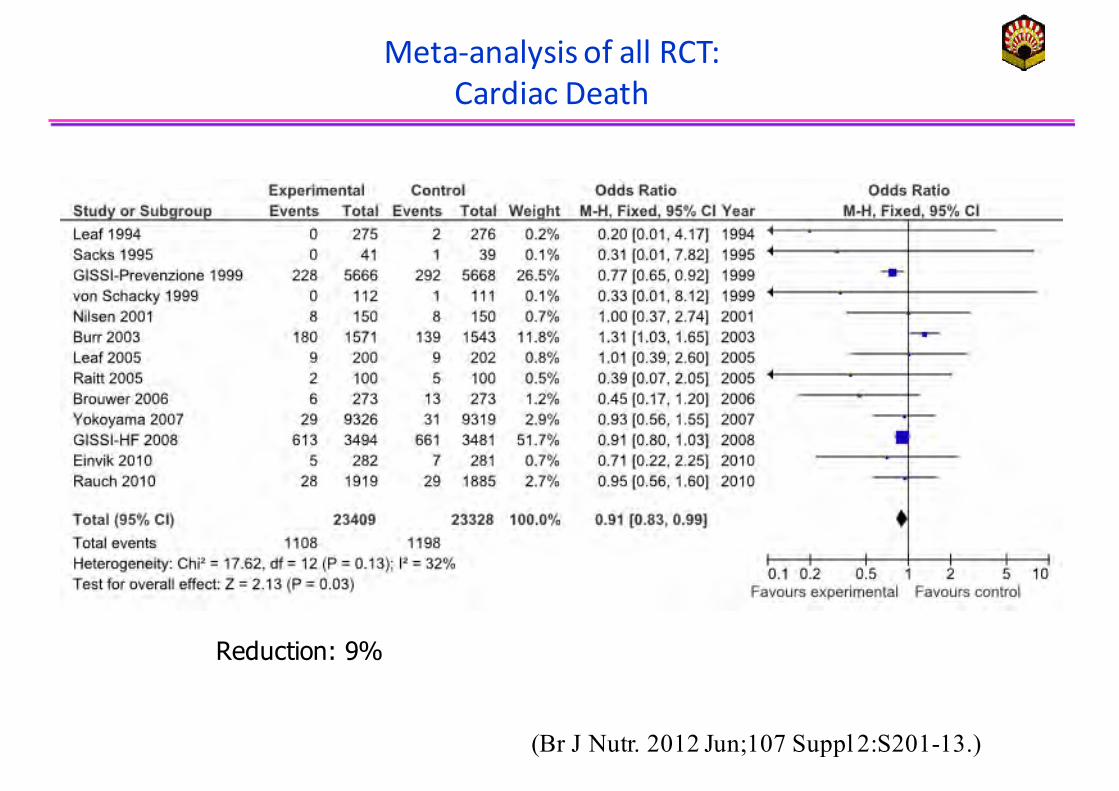
Meta-‐analysis of all RCT:Cardiac Death
Reduction: 9%
(Br J Nutr. 2012 Jun;107 Suppl 2:S201-13.)
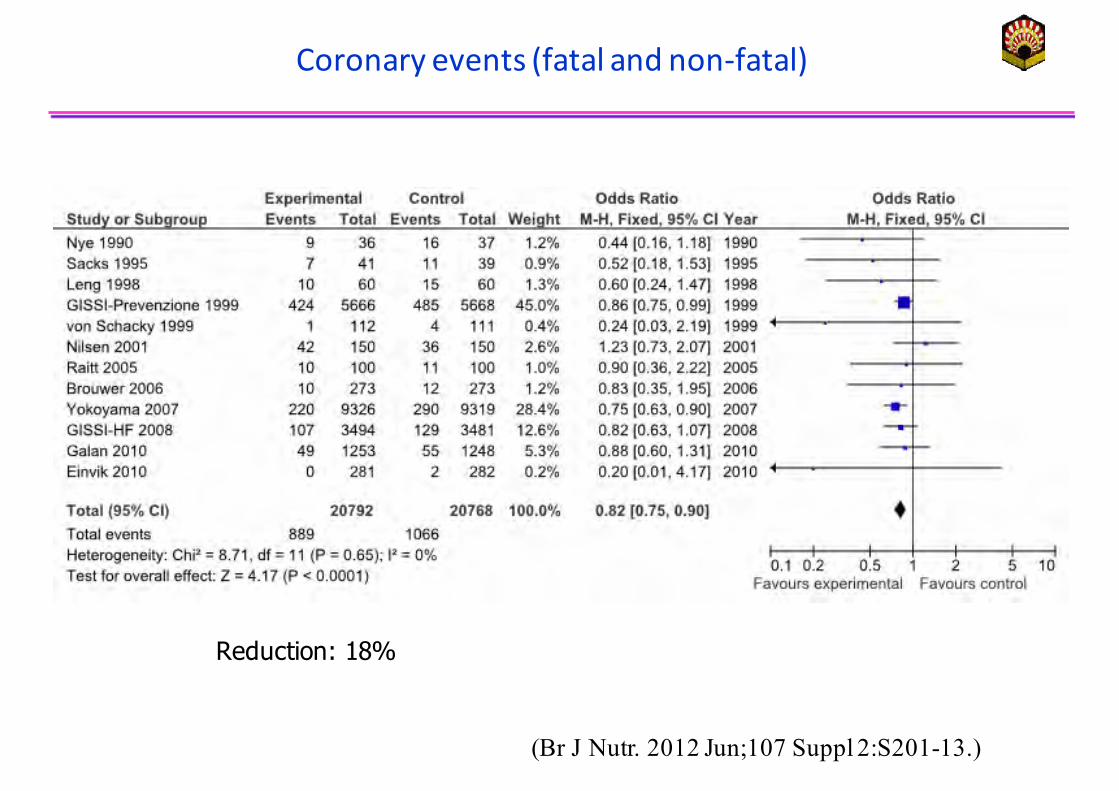
Coronary events (fatal and non-‐fatal)
Reduction: 18%
(Br J Nutr. 2012 Jun;107 Suppl 2:S201-13.)
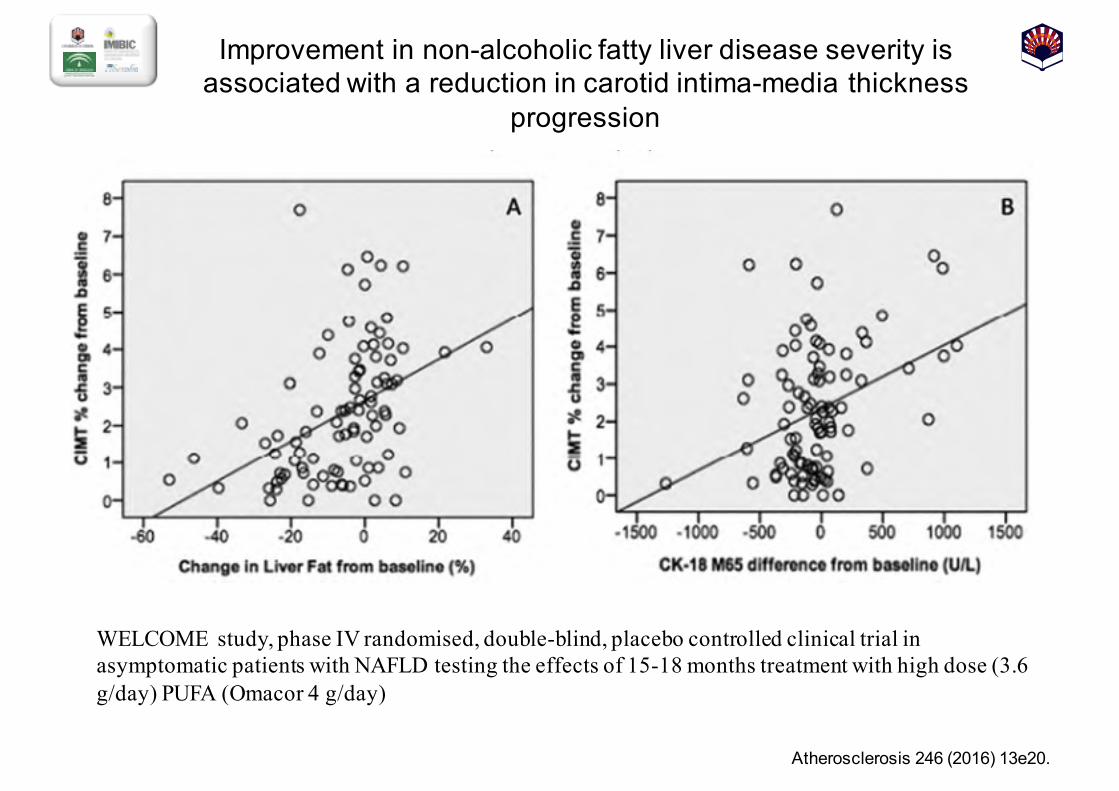
Improvement in non-alcoholic fatty liver disease severity is associated with a reduction in carotid intima-media thickness
progression
Atherosclerosis 246 (2016) 13e20.
WELCOME study, phase IV randomised, double-blind, placebo controlled clinical trial in asymptomatic patients with NAFLD testing the effects of 15-18 months treatment with high dose (3.6 g/day) PUFA (Omacor 4 g/day)
VALORACIÓN Y MANEJO DEL RIESGO CARDIOVASCULAR
1. ¿Cómo podemos reducir el riesgo de padecerenfermedad cardiovascular en pacientes con EHNA?
RECOMENDACIÓN:1. Modificación de la dieta y otros estilos de vida (A;; 1)2. Tratamiento de la hiperlipemia aterógena. • El tratamiento de la hipercolesterolemia aislada debe realizarse con estatinas (A;; 1),
• los pacientes con hipertrigliceridemia y sobre todo en aquellos que presentan bajos niveles de HDL se pueden administrar ácidos grasos omega-3 de larga cadena y fibratos. (B;; 1)
• El manejo y tratamiento de la hiperlipemia en los pacientes con EHNA debe realizarse según los criterios y recomendaciones establecidos para la población general en las guias europeas y americana (B;; 1)
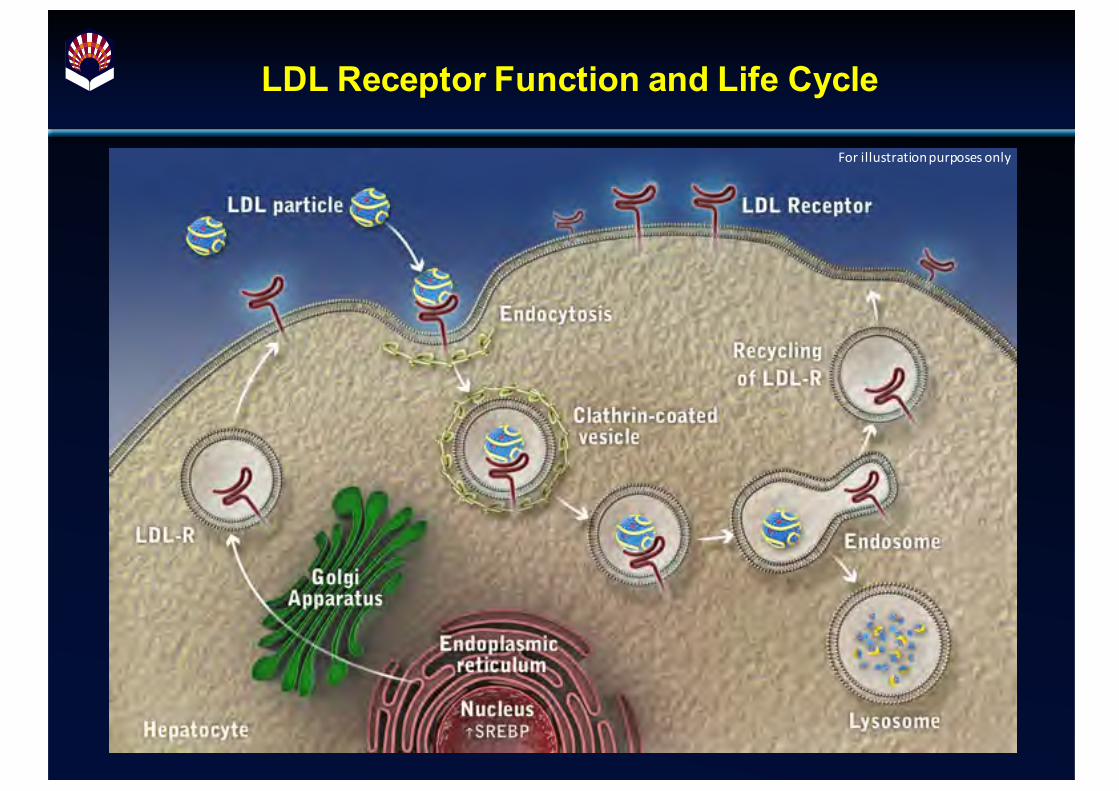
LDL Receptor Function and Life Cycle
For illustration purposes only

The Role of PCSK9 in the Regulation of LDL Receptor Expression
For illustration purposes only
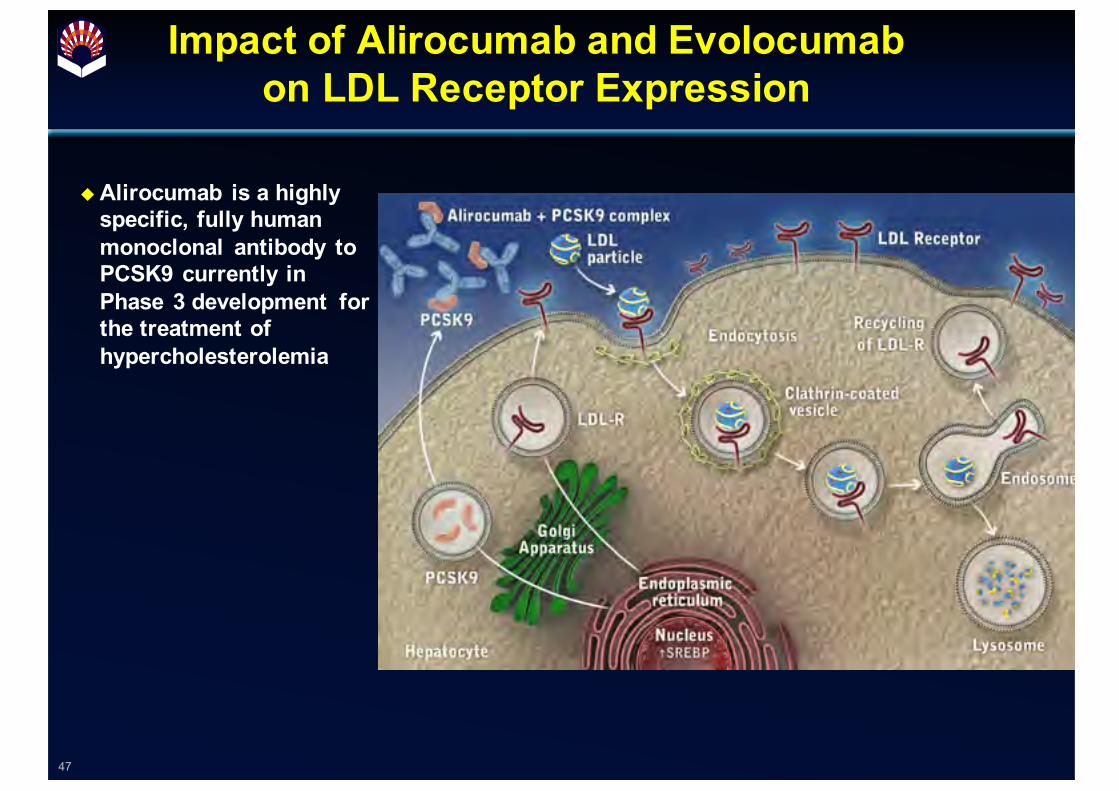
Impact of Alirocumab and Evolocumabon LDL Receptor Expression
47
uAlirocumab is a highly specific, fully human monoclonal antibody to PCSK9 currently in Phase 3 development for the treatment of hypercholesterolemia
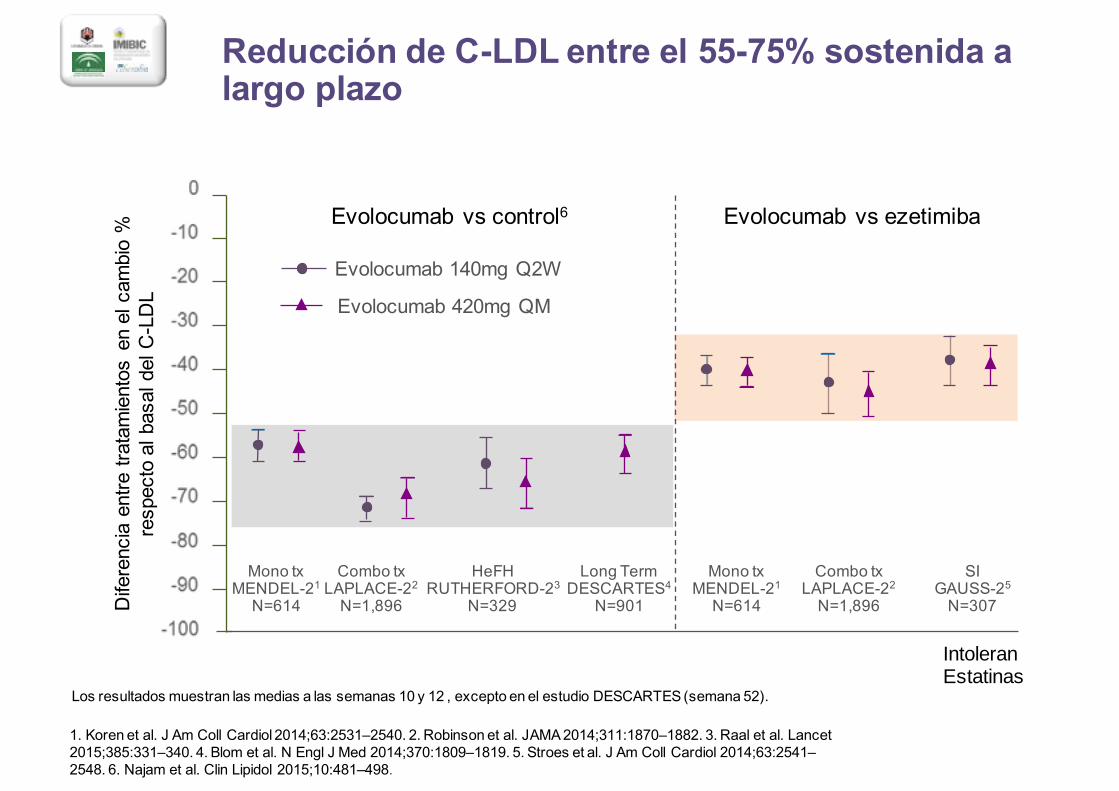
Reducción de C-LDL entre el 55-75% sostenida a largo plazo
1. Koren et al. J Am Coll Cardiol 2014;;63:2531–2540. 2. Robinson et al. JAMA 2014;;311:1870–1882. 3. Raal et al. Lancet 2015;;385:331–340. 4. Blom et al. N Engl J Med 2014;;370:1809–1819. 5. Stroes et al. J Am Coll Cardiol 2014;;63:2541–2548. 6. Najam et al. Clin Lipidol 2015;;10:481–498.
Mono txMENDEL-21N=614
Mono txMENDEL-21N=614
Combo txLAPLACE-22N=1,896
HeFHRUTHERFORD-23
N=329
SIGAUSS-25N=307
Long TermDESCARTES4
N=901
Combo txLAPLACE-22N=1,896
Evolocumab 140mg Q2W
Evolocumab 420mg QM
Diferencia entre tratamientos en el cambio %
respecto al basal del C-LDL
Evolocumab vs control6 Evolocumab vs ezetimiba
Los resultados muestran las medias a las semanas 10 y 12 , excepto en el estudio DESCARTES (semana 52).
IntoleranEstatinas
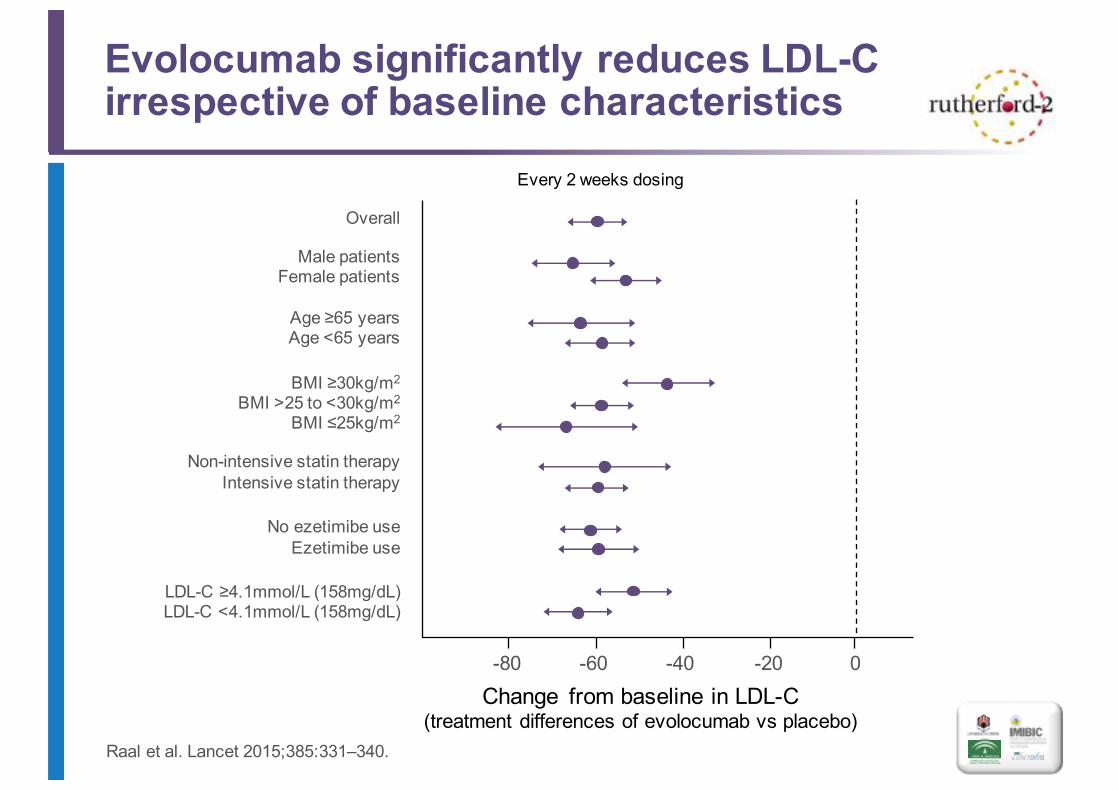
Evolocumab significantly reduces LDL-C irrespective of baseline characteristics
Raal et al. Lancet 2015;;385:331–340.
Every 2 weeks dosing
Overall
Male patientsFemale patients
Age ≥65 yearsAge <65 years
BMI ≥30kg/m2
BMI >25 to <30kg/m2
BMI ≤25kg/m2
Non-intensive statin therapyIntensive statin therapy
No ezetimibe useEzetimibe use
LDL-C ≥4.1mmol/L (158mg/dL)LDL-C <4.1mmol/L (158mg/dL)
-80 -60 -40 -20 0Change from baseline in LDL-C
(treatment differences of evolocumab vs placebo)
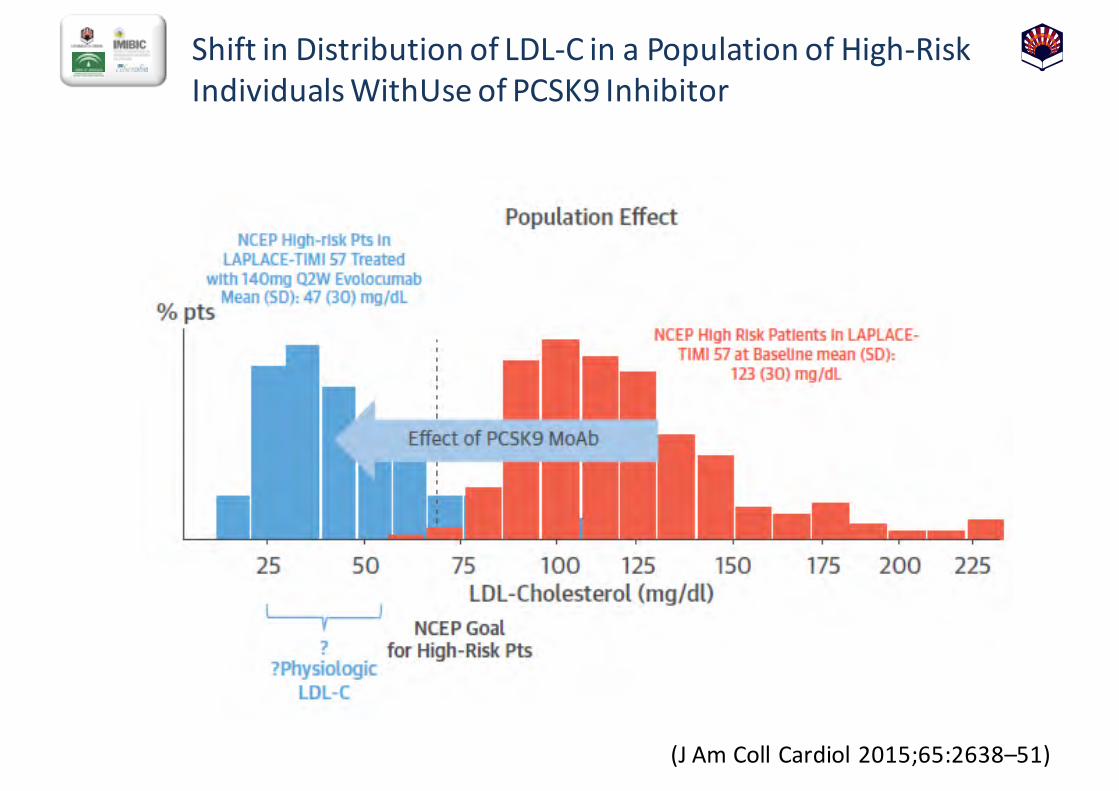
Shift in Distribution of LDL-‐C in a Population of High-‐Risk Individuals WithUse of PCSK9 Inhibitor
(J Am Coll Cardiol 2015;65:2638–51)
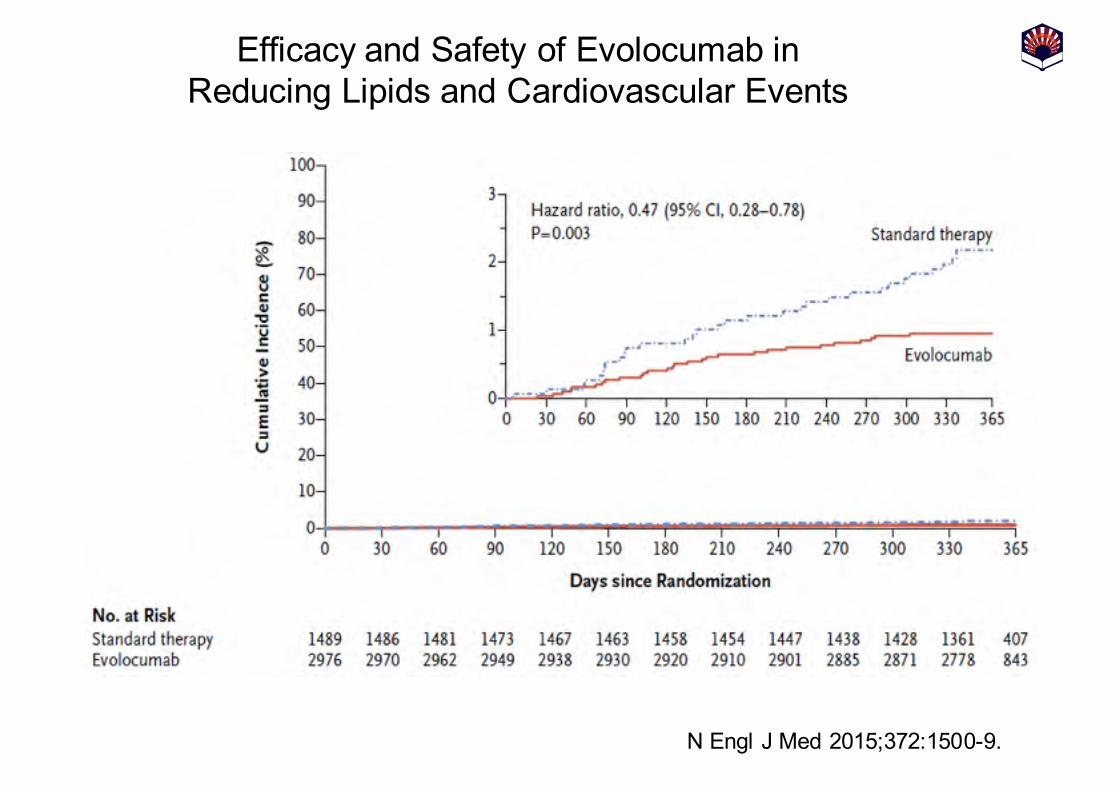
Efficacy and Safety of Evolocumab inReducing Lipids and Cardiovascular Events
N Engl J Med 2015;;372:1500-9.
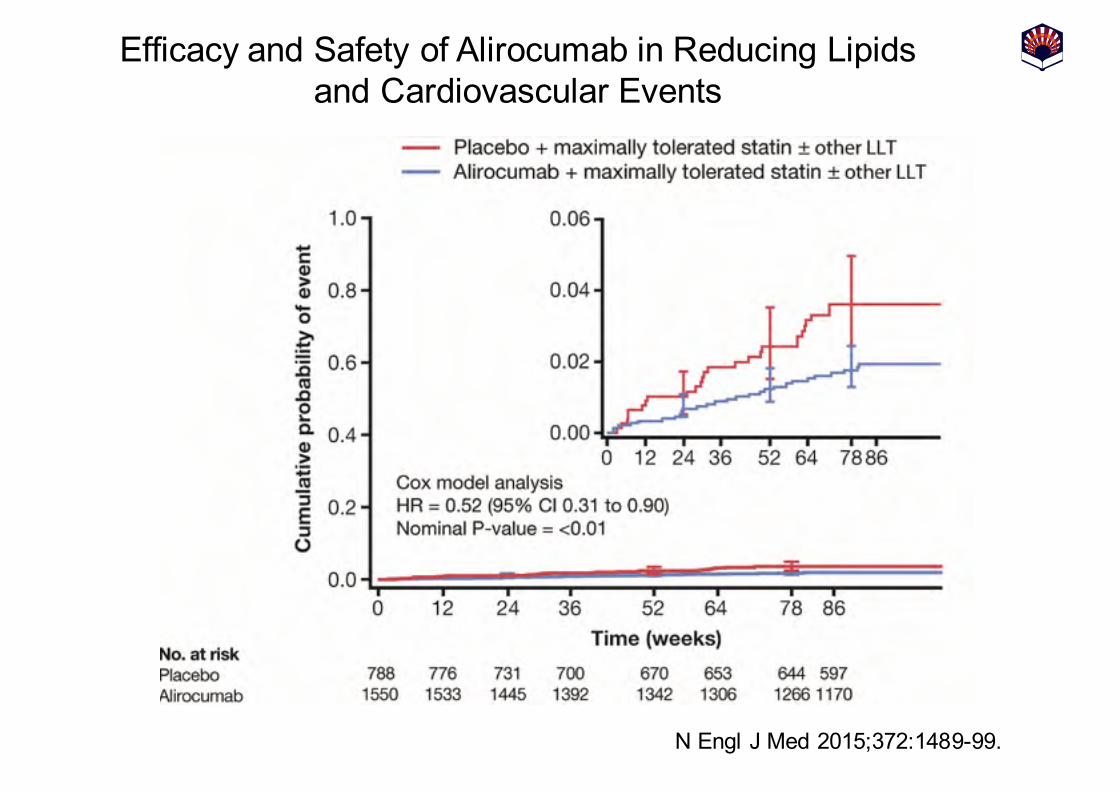
Efficacy and Safety of Alirocumab in Reducing Lipidsand Cardiovascular Events
N Engl J Med 2015;;372:1489-99.
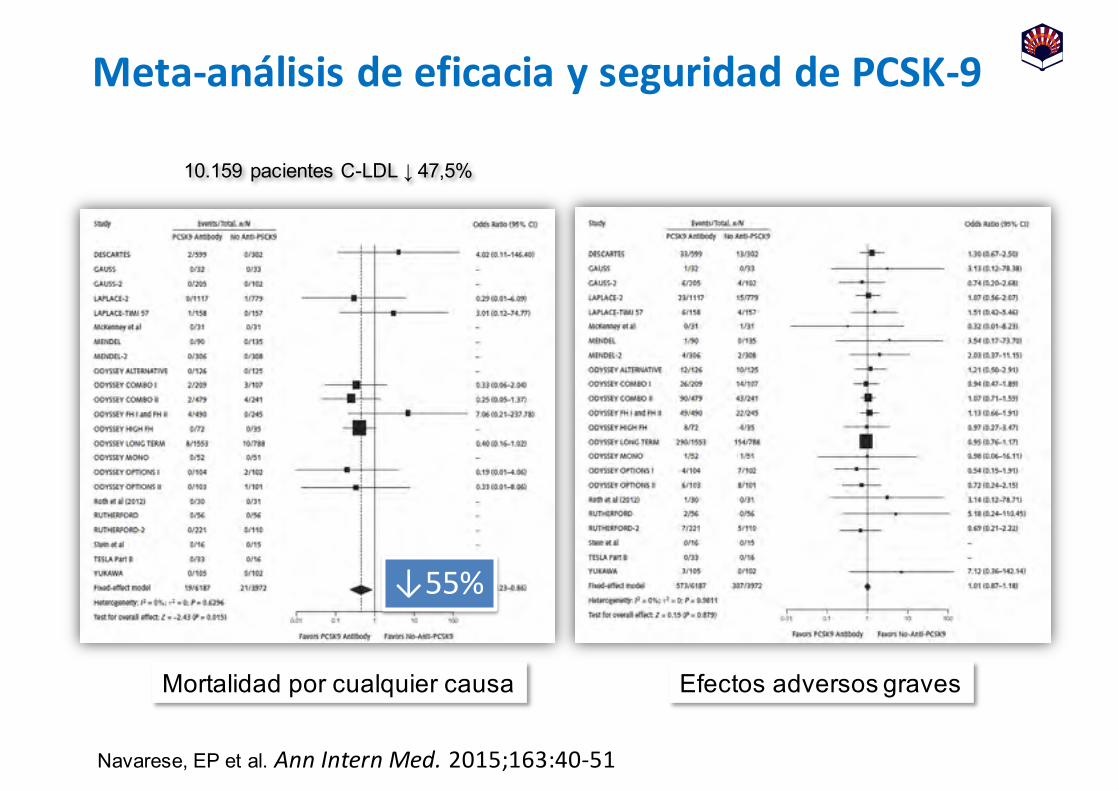
Meta-‐análisis de eficacia y seguridad de PCSK-‐9
Mortalidad por cualquier causa Efectos adversos graves
10.159 pacientes C-LDL ↓ 47,5%
↓55%
Navarese, EP et al. Ann Intern Med. 2015;163:40-‐51

Meta-‐análisis de eficacia y seguridad de PCSK-‐9Mortalidad Cardiovascular
IAMNavarese, EP et al. Ann Intern Med. 2015;163:40-‐51
10.159 pacientes C-LDL ↓ 47,5%
↓51%
↓51%
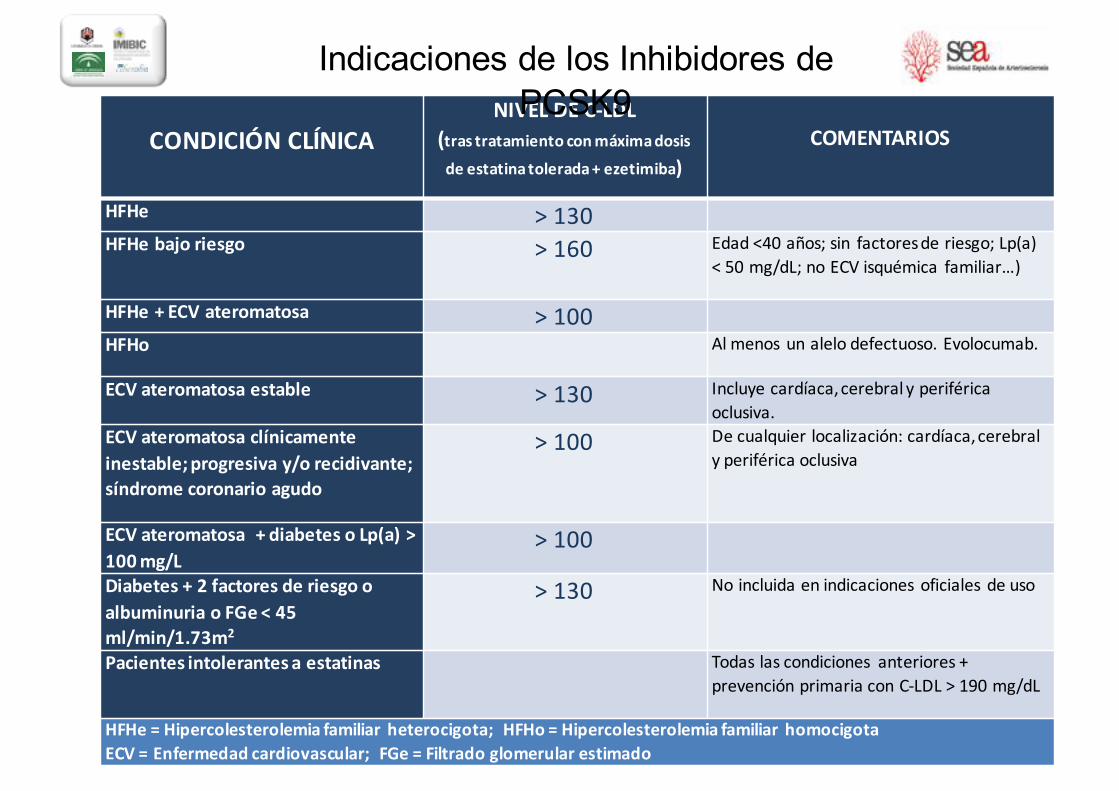
CONDICIÓN CLÍNICANIVEL DE C-‐LDL
(tras tratamiento con máxima dosis
de estatina tolerada + ezetimiba)COMENTARIOS
HFHe > 130HFHe bajo riesgo > 160 Edad <40 años; sin factores de riesgo; Lp(a)
< 50 mg/dL; no ECV isquémica familiar…)
HFHe + ECV ateromatosa > 100HFHo Al menos un alelo defectuoso. Evolocumab.
ECV ateromatosa estable > 130 Incluye cardíaca, cerebral y periférica oclusiva.
ECV ateromatosa clínicamente inestable; progresiva y/o recidivante; síndrome coronario agudo
> 100 De cualquier localización: cardíaca, cerebral y periférica oclusiva
ECV ateromatosa + diabetes o Lp(a) > 100 mg/L
> 100
Diabetes + 2 factores de riesgo o albuminuria o FGe < 45 ml/min/1.73m2
> 130 No incluida en indicaciones oficiales de uso
Pacientes intolerantes a estatinas Todas las condiciones anteriores + prevención primaria con C-‐LDL > 190 mg/dL
HFHe = Hipercolesterolemia familiar heterocigota; HFHo = Hipercolesterolemia familiar homocigotaECV = Enfermedad cardiovascular; FGe = Filtrado glomerular estimado
Indicaciones de los Inhibidores de PCSK9