march 2011 issue number 118 the skipton fund …ukts.org/pdfs/nwslett/issue118.pdf · southgate...
TRANSCRIPT

A word from our President . . . . . . .2
Latest News . . . . . . . . . . . . . . . . . . . . .3
Medical News . . . . . . . . . . . . . . . . . .7
News from Around the World . . . .13
Office News . . . . . . . . . . . . . . . . . . . .22
co
nten
ts
UNITED KINGDOM THALASSAEMIA SOCIETY
A Charity OrganisationRegistration Number: 275107
19 The BroadwaySouthgate Circus, London N14 6PH
Telephone: 0208 882 0011 • Fax: 0208 882 8618Email: [email protected] • www.ukts.org
The Government has announced that they are increasing the compensation package for individuals who contracted hepatitis C in England from NHS blood and blood products. This compensation is administered by a fund called the Skipton Fund. In addition to increasing the compensation for patients, for the first time it will be possible for dependents
of patients who died before 29 August 2003 to make claims on their behalf. This brings the compensation offered to people infected with hepatitis C by blood transfusions into line with the compensation offered to those infected with HIV by the same route.
Said Health Secretary Andrew Lansley; “I fully recognise that the unintended and tragic consequences of these treatments have seriously impaired the lives of many people, together with those of their families. For too long those people infected with hepatitis C have received different support to those infected with HIV. We now intend to make the financial support for hepatitis C patients fairer and more comparable to the arrangements for those infected with HIV. We have listened carefully to the views of the families and campaigners themselves and I believe that changing the payment structure in England and offering the further assistance we have will improve the lives of these people and their families.”
Any patient who has contracted hepatitis C from infected blood should contact the Skipton Fund by one of the methods below as soon as possible. • onlineat:http://www.skiptonfund.org/Eng/index.html
• byemail:[email protected]• byphone:02078081160.
IMPORTANT NOTE • You can make a claim for increased
compensation even if you have already received an award.
You can read more on the Department of Health website; see below.
http://www.dh.gov.uk/en/Aboutus/Features/DH_123381
IF YOU THINK YOU MAY BE ELIGIBLE CONTACT THE SKIPTON FUND WITHOUT DELAY.
MARCH 2011 ISSUE NUMBER 118
The Skipton Fund Increases Compensation
for Hepatitis C Victims
Health Secretary Andrew Lansley

www.ukts.org2
Dearfriends
Some of you are probably looking at thephoto and thinking, “Where’s Mike?” -I almost feel that way myself! It seemsstrange to be writing my first report asPresident of the UK Thalassaemia Society;and I feel I must start by saying a fewwords about my predecessor. Since I hadthehonourtobeelectedasUKTSPresidentafter the AGM on 7th September 2010, IhavebeenawarethatIhaveaveryhardacttofollow.MikeMichaelhasdoneafantasticjobasUKTSPresidentforthepast10yearsandisnowsteppingdownforawellearnedrest. He has been the public face of theSociety both at home and abroad and hasspoken to countless audiences about thework of the UKTS and every imaginableissue related to thalassaemia care. I knowthat everyone will join me in thanking
Mike for his years of devoted service totheSocietyandinhopingthathewillnowhave more time to spend with his family.Beforehegets too comfortablehowever, IshouldpointoutthatMikeisnotleavingusentirely-hehasagreedtoactasaco-optedCommittee member and will continue asour representative on the Board of theThalassaemia International Federation. Sothankfully we will continue to have thebenefitofhisexperience.
It is a daunting task to step into this rolewhich has been so ably carried out byothers; but I am determined to do myabsolute best to live up to the examplesI have to follow and to the trust that hasbeenplaced inme. I couldnothave takenon this work without knowing I have thehelp and support of my fellow Trustees– the experienced campaigners AndyCharalambous, George Constantinou, NinaDemetriou, Pany Garibaldinos and BharatNathwani;andmyfellow“newbies”ontheteam, Adam Christodoulou and RomaineMaharaj. My thanks to them and also tothe other Committee members who havestepped down, Philip Agathangelou, DrChristos Sotirelis and Menuccia Tassone.Chris remains as a co-opted CommitteememberasdoesMenuccia,despitethefactthatinJanuary2011shedepartedforanewlife inhernativeAustraliaandmarriagetoher fiancé Elton Chisholm. We wish themevery happiness and thank Menuccia for
her invaluable contributions to the workofUKTS.
Last but not least, I mustn’t forget tothank my wife Nishel for supporting andencouraging me in becoming involved intheworkoftheUKTS– in justafewshortmonthsIhavelearnedhowtimeconsumingitis–sothankyouNishelforyourcontinuedpatience.
Finally, I must apologise for the length oftimeithasbeensinceweproducedoutlastnewsletter–thishasbeensolelyduetotheever-increasingamountofworkhandledbytheUKTSoffice.Tomakeupfor it this isa“bumperissue”withmanymorepagesthanususaltomakesureyouareuptodatewiththecurrentnews.
‘Byeuntilthenextissueandbestwishes.
Gabriel TheophanousPresident, UK Thalassaemia Society
(Editor’s note: Gabriel has thalassaemia major. At the risk of embarrassing him we would like to point out that in 2006 he became the first thal in the world to run a Marathon!)
A word from our President
Gabriel Theophanous President
Andy Charalambous Vice-President
George Constantinou Secretary
Romaine Maharaj Assistant Secretary
Bharat Nathwani Treasurer
Nina Demetriou Assistant Treasurer
& TIF Representative
Adam Christodoulou Pany Garibaldinos
Committee
Mike Michael TIF representative
Dr Christos Sotirelis Menuccia Tassone
Co-opted Committee Members
The UKTS ManagementCommittee
Our Mission Statement
■ To be the definitive source of information, education and research for those affected by, or working with thalassaemia.
Thalassaemia Matters ...continuing the fight against thalassaemia 3
latest news
Thalassaemia – Your Life, Your Choice, Your Test
The purpose of this film is to increase awareness of thalassaemia and the importance of pre-natal screening in the community at large. It shows interviews with thalassaemics of varying ages and backgrounds, parents of children with thalassaemia and experienced health professionals.
UKTS thanks the NHS Sickle Cell and Thalassaemia Screening Programme for their contribution to the making of this film.
My ThalThe purpose of this film is to inspire and empower those living with thalassaemia major. It aims to lead them to an understanding that, although they have along term medical condition, it is treatable manageable. Through the medium of interviews with thalassaemics of varying ages and backgrounds, the viewers will see that, notwithstanding the challenges they face, thalassaemics can and do live long, happy and fulfilled lives.
UKTS – Making a DifferenceThis film is a brief introduction to UKTS. It gives
a very brief outline of thalassaemia, the treatment and complications. It explains what the charity does and why its work is so important.
All the interviews in these films are unscripted.
Endorsement from the NHS SC&T Screening ProgrammeThe NHS Sickle Cell and Thalassaemia Screening Programme would like to congratulate the UK Thalassaemia Society on bringing out three new videos to help raise awareness of the challenges of living with thalassaemia, the work of UKTS and the importance of getting testing for this genetic condition. We are delighted to be able to use these in our own outreach work and have already uploaded these to the Programme YouTube channel (www.youtube.com/haemscreening).
Contact the UKTS office today to order your copies!
Introducing Our New DVDs– available now FREE OF CHARGE from the UKTS office and to view on the
UKTS website www .ukts .org!
UNITED KINGDOM THALASSAEMIA SOCIETYA Charity OrganisationRegistration Number: 27510719 The BroadwaySouthgate Circus, London N14 6PHTelephone: 020 8882 0011 • Fax: 020 8882 8618
Email: [email protected] • www.ukts.org
UKTSMaking a Difference
UNITED KINGDOM THALASSAEMIA SOCIETY
A Charity OrganisationRegistration Number: 275107
19 The BroadwaySouthgate Circus, London N14 6PH
Telephone: 020 8882 0011 • Fax: 020 8882 8618Email: [email protected] • www.ukts.org
My Thal
UNITED KINGDOM
THALASSAEMIA SOCIETY
A Charity Organisation
Registration Number: 275107
19 The Broadway
Southgate Circus, London N14 6PH
Telephone: 020 8882 0011 • Fax: 020 8882 8618
Email: [email protected] • www.ukts.org
Thalassaemia
Your Life, Your Choice, Your Test

www.ukts.org4
latest news
N.B. Thalassaemia patients attending the conference who are paid up members of UKTS should contact the UKTS office to find out whether they are eligible for a conference grant of £200.
12th International Conference on
Thalassaemiaand The Haemoglobinopathies14th TIF International Conference For Patients and Parents11-14 MAY 2011WOW Hotels, Topkapi & Kremlin PalaceAntalya – Turkey"HAEMOGLOBIN DISORDERS IN THE NEXT DECADE"THALASSAEMIAS AND SICKLE CELL DISEASE
www.talasemi.org www.thalassaemia.org.cywww.tif2011.org
Organised by
Increase in Prescription ChargesFrom 1st April 2011 the cost of a single prescription item will go up from £7.20 to £7.40. If you have to pay for more than 14 items in 12 months, you may find it cheaper to buy a PPC (prescription prepayment certificate). A PPC for 12 months costs £104.00 and will cover ALL your prescription charges in the 12 month period. Furthermore you can spread the cost of the PPC by paying £10.40 per month for 10 months. You can buy or renew a PPC on-line and set up your direct debit by visiting the NHS Business Services Authority on http://www.nhsbsa.nhs.
uk/1127.aspxThere is also a telephone advice line
and order line you can call 0845 850 0030.
Further information• You must be a resident of England to
purchase a PPC. • You can also pay for a 3-month
PPC which will cost £29.10 from 1.4.2011.
• Those receiving certain benefits (e.g. income support, tax credits) may be exempt from paying prescription charges
• Some pharmacies are registered to sell PPCs. Your local pharmacist will be able to advise you if you need any more information about prescription charges

Thalassaemia Matters ...continuing the fight against thalassaemia 5
latest news
APPG Reception 16th November 2010The All Party Parliamentary Group on Sickle Cell and Thalassaemia held a reception in the Strangers Dining Room, the House of Commons on 16th November 2010. A total of 94 people attended including MPs, peers, parliamentary staff, clinicians and nurse specialists and of course patients and carers. The title of the event was “Sickle Cell Disease and Thalassaemia: What Next?” and the objective was to discuss how, during this time of great change in the NHS, we can ensure that thalassaemia and sickle cell patients are not forgotten. The event was hosted by Diane Abbot MP, Chair of the APPG. Speakers included; Diane Abbot MP, Anne Milton MP (Under-Secretary of State for Health), Anne Welsh, Chair of the Sickle Cell Society and our President, Gabriel Theophanous, introduced our new film “UKTS – Making a Difference” (see page 3).
All those who attended were invited to sign a petition which stated:
“Sickle cell disease and thalassaemia are blood disorders which predominantly affect ethnic minorities. Patients can face a variety of challenges both socially and in their health care, and do not always receive adequate or equal access to services. I, the below signatory, petition the UK Government to ensure that specialised health services for patients with sickle cell disease and thalassemia are funded sufficiently; that managed clinical networks are developed to improve equality of care for the conditions; that the value of specialist nurses for haemoglobinopathies is recognised; and that patients receive the social care and educational and community support they need.”
This petition was handed in to 10 Downing Street on 2nd February 2011 by representatives from UKTS and the Sickle Cell Society, accompanied by David Burrowes MP , who is the constituency MP for our Southgate office (and who tabled the first ever adjournment debate in thalassaemia in the House of Commons on 4th February 2009).
Notes
All Party Parliamentary Group on Sickle Cell and ThalassaemiaThe All-Party Parliamentary Group on Sickle Cell and Thalassaemia is a cross-party group of MPs and Peers who share an interest and concern for these conditions. The Group was first formally established in autumn 2008. The Chair of the APPG is Diane Abbott MP (Lab).
A further 21 MPs and Peers complete the current membership of the APPG. The Sickle Cell Society and the UK Thalassaemia Society help steer the direction of the Group, with the contribution of other stakeholders such as the NHS Sickle Cell
and Thalassaemia Screening Programme and UK Forum on Haemoglobin Disorders.
The APPG’s Mission StatementThe All-Party Parliamentary Group (APPG) on Sickle Cell and Thalassaemia exists to reduce the health inequalities that are faced by sickle cell and thalassaemia patients in the UK, by improving standards of care and by addressing other critical issues, as recommended by the key stakeholders. Members will achieve this aim by engaging with Parliamentary colleagues, the Government, health professionals, and community and patient groups to raise awareness relating to the conditions and the needs of patients.
Reception guests in the Strangers Dining Room, House of Commons.
Diane Abbott MP, Chair of the APPG.
Gabriel and Anne Welsh, Chair of SCS, sign the petition.
UKTS President Gabriel Theophanous introduces our new film.
Handing the petition in at Downing St – L-R Anne Welsh, David Burrowes MP, Gabriel Theophanous, Elaine Miller of UKTS & Philip Nortey of SCS

www.ukts.org6
latest news
This year our annual dinner dance took on an even more festive aspect than usual. As the date fell on 16th December 2010, we decided to make it a Christmas Ball, complete with a red and gold colour scheme and Christmas-themed floral decorations. As on so many previous occasions the event was held at the Regency Banqueting Suite in Bruce Grove, N17; and as usual the staff and management were the epitome of helpfulness and efficiency.
Our special thanks to:David Burrowes MP (member of the APPG on Sickle Cell & Thalassaemia) who took time out of his busy schedule to join us and address our guests.
Maria Couppas, Tas Couppas, Koula Kanias and Mary Zembylas for their help in organising and running the event.
Gina Halwani for preparing the floral decorations, which were kindly sponsored by the Kountourou family, John Triantafillou of Magic Drinks and Andy Petris of Foodco (UK) Ltd.
Koula Horatta of the Wedding Lounge for donating the decoration of the hall.
All who donated prizes for the raffle, auction and £5 in the box.
Mikey Mike, presenter on London Greek Radio, who acted as our MC for the auction and raffle draw.
The winning raffle ticket numbers were:1) 081972) 03543) 098554) 39585) 052316) 053257) 06647
8) 088999) 0627810) 0674711) 0706712) 0775713) 08763
Thankyoutoallwhosupportedusbypurchasingraffletickets.
UK Thalassaemia Society Christmas Ball
UKTS President Gabriel Theophanous and David Burrowes MP
UKTS’ longest serving Trustee George Constantinou with outgoing Trustees Menuccia and Mike
UKTS Presidents past and present – Mike Michael and Gabriel Theophanous
3 of our lady members at the ball L-R Menuccia Tassone, Roanna Maharaj, Maria Couppas

Thalassaemia Matters ...continuing the fight against thalassaemia 7
medical newslatest news
The second national UKTS nurses’ conference took place on 29th September 2010 at King’s Fund, Cavendish Square, London. The conference was attended by 160 nurses from all parts of the UK; who listened to the following presentations:-• Living my life by Mike Michael, UKTS
patient representative• Overview of thalassaemia
treatment by Katherine Stevenson, Haemoglobinopathy nurse specialist, Manchester Royal Infirmary
• A normal life? The importance of chelation therapy by Emma Prescott, Thalassaemia Nurse Specialist, Whittington Hospital, London
• New RCN accredited competences in thalassaemia and sickle cell disease by Sekayi Tangayi, Service Manager and Specialist Nurse, Newham Sickle Cell/Thalassaemia Centre
• Transition from paediatric to adult services by Rebecca Cooke, Transition Nurse Specialist, Birmingham Children’s Hospital
• Improving the quality of life in thalassaemia by Prof Antonio Piga, Professor of Paediatrics, Thalassaemia
Centre, University of Turn, ItalyA question and answer session followed, facilitated by Prof Elizabeth Anionwu CBE FRCN, Emeritus Professor of Nursing, Thames Valley University. Prof Anionwu and Prof Karl Atkin (Professor of Ethnicity and Health, University of York) chaired the morning and afternoon sessions respectively. The conference was accredited with 5 study hours by the Royal College of Nursing Accreditation Unit; and feedback from the nurses who attended was extremely positive.
Our thanks to Prof Elizabeth Anionwu who chaired the conference organising committee; and our sponsors Novartis, Resonance Health, Swedish Orphan Biovitrum and Una Health.
Thalassaemia – Nurses Talking to Nurses 2010
Working Together to Remove Excess IronBy Dr Michael Angastiniotis, Medical Advisor, Thalassaemia International Federation.
This article first appeared in issue 58 of the TIF magazine; and UKTS is grateful to the editors for their kind permission to reproduce it here.
Desferrioxamine and DeferiproneThe effectiveness of combining the two chelation agents, Desferrioxamine (known to most patients by the original commercial name Desferal) with Deferiprone, has been known for some time to be effective in protecting from heart complications and there are several published studies to point this out. It is usually prescribed for patients with accumulation of iron in the heart (measured by T2* >20ms on cardiac magnetic resonance) or liver (when the iron concentration is more than 15mg/g dry
weight measured by liver biopsy or MRI). In Cyprus for example, improved survival
in thalassaemia major was attributed to switching patients to this combination (see the article in Haematologica 2009, 94: 1777-8) and that this approach led to a sevenfold improved survival. Likewise in Greece it was found that the risk for a de novo cardiac event was 23 times less with combination compared to Desferrioxamine used alone and the odds for cardiac death much reduced also (see the article in the Eur J Haematol, 2010, 85:335-44). Good results are also reported in patients with established heart disease in the USA (Blood Cells Mol Dis, 2010, 45:136-9).
There are several other publications demonstrating similar results. Impressive however are the results obtained from a clinical trial conducted in Corinth and Athens, Greece. In this trial the authors, (Farmaki K et al. Brit J Haematol, 2010, 148: 466-75) have looked not only on the effects on heart but also on endocrine
function. They observed 52 thalassaemia patients who were transitioned from desferrioxamine alone to the combination regime because of high iron overload. They were observed for 7 years and apart from reducing ferritin levels, heart and liver iron (measured by MRI), they made the following observations on endocrine functions:• 39 patients had abnormal sugar
metabolism and 44% normalised after the combination treatment.
• 18 had hypothyroidism and 10 (55.5%) were able to stop thyroxin treatment.
• 14 males had hypogonadism and seven of these were able to stop treatment with testosterone
• 19 females had hypogonadism and 6 (31.6%) were able to become pregnant.
All this makes the choice of combination treatment attractive. However it is still used for patients with evidence with heavy iron load because of increased toxicity compared to using one drug alone.

www.ukts.org8
Unomedical Ltd · First Floor, West Wing · Unit 3 Brooklands· Moons Moat Drive · Redditch · Worc's · B98 9DW · UK Tel 01527 583600 · Fax 01527 591198 · www.unomedical.com
Making Desferal Therapy more convenient
Thalassaemia Matters ...continuing the fight against thalassaemia 9
medical news
Prof Sir David Weatherall (Honorary President of UKTS) was a 2010 recipient of the prestigious Lasker-Koshland prize, the top American prize for medical research. As a result he was asked to write a short essay on his life in science; and this fascinating article is the result. The article first appeared in Nature Medicine (Vol 16, no 10, October 2010); and is reproduced here with the kind permission of the Editors.
I owe my long interest in inherited blood diseases and tropical medicine to a series of characteristically bizarre decisions by the British Army. In 1958,2 years after qualifying in medicine from Liverpool University, I was drafted for 2 years of compulsory National Service. Terrified of flying, snakes and bullets, I volunteered to serve in the UK. So it was that a few weeks later, and after a long and eventful voyage on a troop ship that ran aground in the Suez Canal, I found myself in charge of the Children's Ward in the British Military Hospital in Singapore. At that time, the hospital served the soldiers and families of the Commonwealth forces who were engaged in the long war against the Chinese communists in Malaya, as it was
then called. One of my first patients was a Nepalese child whose father was serving in a Gurkha regiment. She had been profoundly anemic from the first year oflife and had been kept alive by monthly blood transfusions. After a long struggle, and with the help of Frank Vella, a biochemist from Singapore University, we found that this child had thalassemia, an inherited blood disease that was thought at the time to be restricted to Mediterranean populations.
I spent the second year of my National
Service working in a military hospital in Taiping, close to the Thai border where the remaining communist terrorists were being rounded up. There I saw a wide spectrum of tropical diseases, and, in my spare
time and with a primitive electrophoresis setup comprising car batteries and filter paper, searched for more individuals with thalassemia.
After my discharge from the army, I went to the US to work at Johns Hopkins University, spending time in the medical genetics, hematology and biophysics departments. By 1960 it was known that human hemoglobin (Hb) consists of four pairs of peptide chains-two α-chains and two ~-chains (a2~2); in fetal life, the main hemoglobin-HbF-has two α-chains and two γ-chains (azyz). It was also known that sickle cell anemia results from an amino acid substitution in the ~-globin chain, and there were also hints that the cause of thalassemia might involve the α- or ~-globin-chain genes. My first work in Baltimore, carried out in Ned Boyer's laboratory, was to trudge around the hospitals collecting cord blood to look for hemoglobin variants that would clarify the genetic regulation of α-globin synthesis in fetal and adult life and that, incidentally, led to the finding of a mild form of thalassemia in many African-American infants. But it was clear that further progress in understanding the cause of thalassemia would require the development of methods for studying hemoglobin synthesis in vitro.
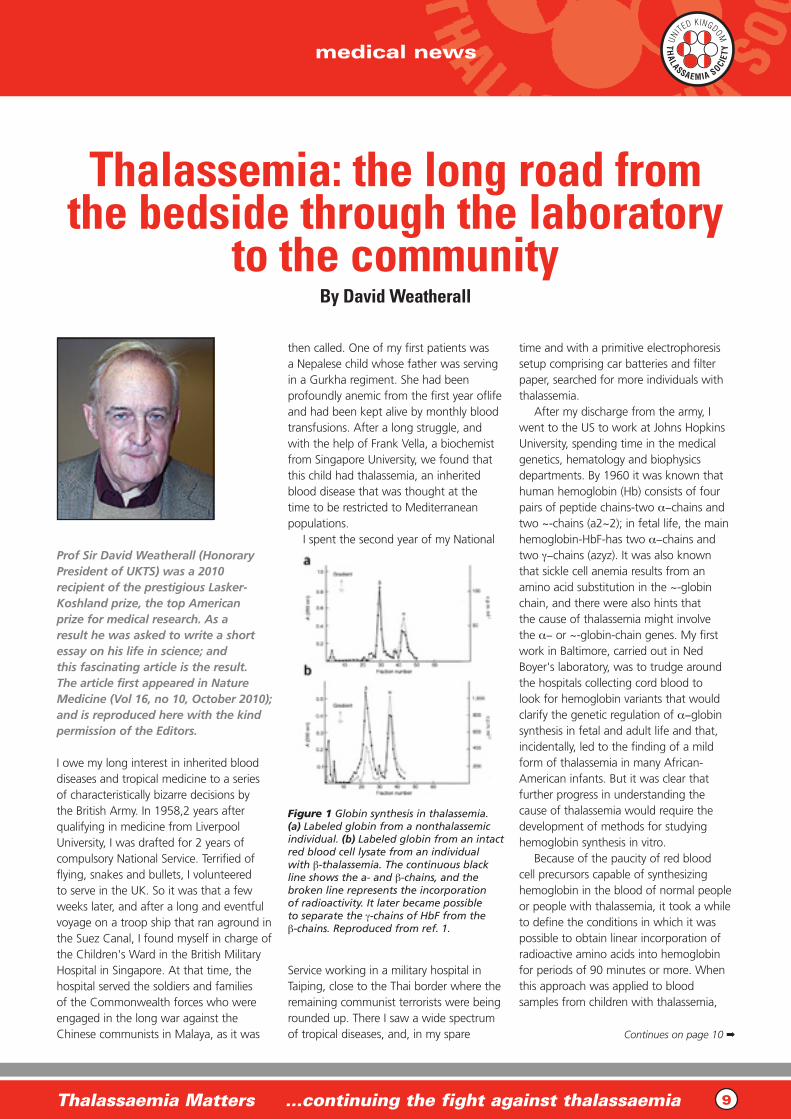
Because of the paucity of red blood cell precursors capable of synthesizing hemoglobin in the blood of normal people or people with thalassemia, it took a while to define the conditions in which it was possible to obtain linear incorporation of radioactive amino acids into hemoglobin for periods of 90 minutes or more. When this approach was applied to blood samples from children with thalassemia,
Continues on page 10 ➡
Figure 1 Globin synthesis in thalassemia. (a) Labeled globin from a nonthalassemic individual. (b) Labeled globin from an intact red blood cell lysate from an individual with β-thalassemia. The continuous black line shows the a- and β-chains, and the broken line represents the incorporation of radioactivity. It later became possible to separate the γ-chains of HbF from the β-chains. Reproduced from ref. 1.
Thalassemia: the long road from the bedside through the laboratory
to the communityBy David Weatherall

www.ukts.org10
medical news
it appeared as though there was unequal labeling of the α- and ~-globin chains. The problem was that there was no method for separating them with anything close to a quantitative yield.
A lucky break was to come, however. Two English protein chemists, John Clegg and Michael Naughton, graduates of Fred Sanger's laboratory in Cambridge, UK, were working in the biophysics department at Johns Hopkins at that time. For reasons that are still obscure to me, they took on the unenviable task of trying to educate me into the basics of protein chemistry. Clegg wondered whether, by adapting methods he had used for separating other protein chains in his doctoral thesis work, we could use a similar approach to separate globin chains. It was remarkably successful, and we were able to examine normal and thalassemic labeled globins and show that the basic defect in thalassemia is unbalanced globin -chain synthesis, with excess α-chains produced in β-thalassemia and excess β-chains in α-thalassemia1 (Fig. 1). This method was subsequently used by many groups to define the different forms of thalassemia and their pathology. And, just a few years later, it was used to diagnose thalassemia during fetal life as an approach to prenatal diagnosis, an advance that led to a marked reduction in the births of babies with severe thalassemia in several countries over the succeeding years.
After returning to England in the mid- 1960s and writing the first edition of The Thalassaemia Syndromes, which has reappeared in several editions over the years2 as a guide to workers in the field, we established a hemoglobin research group, first in Liverpool and later in Oxford. In the early days, and in collaboration with Robert Williamson and John Paul, we were able to show deletions as the cause of severe forms of α-, β- and δβ-thalassemia. Also, after studying a family with an unusual form of α-thalassemia referred to us by Paul Milner from Jamaica, we were able to characterize thalassemia due to mutations in the α-globin chain termination codon3. Later on, these and unrelated mutations were found to be carried by up to 4% of the population of Thailand and to be the cause of α-thalassemia in many other populations.
As direct analysis of DNA became possible, we focused our attention on the remarkable diversity in the structure of the α-globin genes, the numerous mutations that produce the diverse clinical forms of α-thalassemia and the feasibility of early prenatal diagnosis by fetal DNA analysis. We also identified a completely new class of α-thalassemias associated with mental retardation that resulted from subtelomeric deletions affecting the α-globin genes on chromosome 16 or mutations of a gene on the X chromosome. Later on, the first of these two classes led to the recognition of submicroscopic, subtelomeric deletions as a relatively common cause of mental retardation4.
By the late 1970s, we had developed a
team of outstanding scientists supported by the UK Medical Research Council and the Wellcome Trust, including John Clegg, Bill Wood, Douglas Higgs, Swee Lay Thein, Kathryn Robson, John Old, Andrew Wilkie and Richard Gibbons. Later, our interests expanded into the evolutionary biology of the hemoglobin disorders; in particular, to ask why they are so common. In 1949, John B.S. Haldane had suggested that the thalassemias might occur at a high frequency because of heterozygote resistance to severe malaria5. Until the molecular era, this was difficult to prove. However, in a series of studies carried out in the Pacific Islands and in Papua New Guinea, our students Adrian Hill and Jonathan Flint, together with Angela and
Figure 2 Mechanisms for the phenotypic diversity of β-thalassemia. The basic pathology of the disease results from excess α-chains damaging red blood cell precursors and red blood cells. This excess can be modified by different levels of severity of reduction in α-chain production, variable numbers of α-chains resulting from deletion or expansion of the α-globin gene loci, varying ability to produce HbF after birth and, possibly, different rates of removal of α-chains by proteolysis. The many complications of the resulting anemia can also be modified by genetic variability. Coselection indicates that variants of these genes and many others produce different responses to infection among different populations. VDR, vitamin D receptor; ESRl, estrogen receptor-I; COL, collagen; HFE, locus for hereditary hemochromatosis; UGTlAl, UDP glucuronyltransferase involved in bilirubin metabolism; HLA-DR, major histocompatibility complex locus; TNF, tumor necrosis factor; ICAMl, intercellular adhesion molecule-I; DARC, Duffy antigen receptor for chemokines.
Continues from page 9

Thalassaemia Matters ...continuing the fight against thalassaemia 11
medical news
Steve Allen, were able to show without any doubt that the α-thalassemias are highly protective against malaria caused by Plasmodium falciparum6. Some of our other students, notably Tom and Kathryn Williams, who had taken part in this work, continued to work in this field in East
Africa and, aside from replicating these results, described new epistatic interactions between the different hemoglobin variants in Africa with respect to malaria susceptibility.
Throughout these years, we and others continued to explore the reasons
for the remarkable clinical diversity of the thalassemias. In the case of the β-thalassemias, for example, it turned out that the co-inheritance of α-thalassemia has an ameliorating effect on the phenotype by reducing the degree of globin chain imbalance, whereas the inheritance of more α-chain genes than usual has the opposite effect. Similarly, an inherited ability to make more γ-chains of fetal hemoglobin results in a milder phenotype. Many of the complications of the disease are also modified by genetic factors; there are differences in the patterns of adaptation to anemia at different ages, and the environment, notably exposure to malaria7, also modifies the phenotype (Fig. 2). Clearly, this so-called 'simple' monogenic disease is anything but simple, an important message for those who are now doing battle with the complexities of the genetic component of common diseases8.
By the early 1980s, it was clear that the molecular technology that was proving so effective for studying the hemoglobin disorders was going to be applicable to many fields of medical research in the future.
As there were few places where young clinicians could be trained in this technology, or where young scientists could apply it to clinical problems, we decided to establish an Institute of Molecular Medicine in Oxford, where young people of both backgrounds could mingle, obtain training and bring their particular clinical problems into an environment in which molecular technology was available. The Institute opened in 1989 and now houses over 400 scientists.
As early as the 1960s, it was already apparent that the inherited disorders of hemoglobin occur widely throughout the tropical world. In 1967, the World Health Organization (WHO) asked me to go on an extensive tour of Asia to report back on the occurrence of thalassemia and facilities for its diagnosis and care there. On the basis of this experience, we developed partnerships with several countries, partly for training staff in the clinical and diagnostic aspects of thalassemia, but in many cases for long-term associations to develop collaborative research programs. In
Figure 3 Kurunegala, Sri Lanka. (a) The author with a group of staff and thalassemic children in the Children's Ward in the District Hospital at Kurunegala, Sri Lanka. A small alcove behind the children's ward was used to transfuse a population of more than 600 children with thalassemia before the building of the National Thalassaemia Centre. (b) The National Thalassaemia Centre, attached to the pediatric ward, offers transfusion facilities for young children on the ground floor and older children on the middle floor. The top floor provides facilities for genetic counseling, basic hematological studies and small group seminars.
Continues on page 12 ➡

www.ukts.org12
medical news
international health jargon, these 'North-South' partnerships, some of which have been sustained for many years,
have been a cost-effective and productive way of helping countries such as Cyprus, India, Burma (Myanmar), Thailand, Indonesia, South Vietnam, Sri Lanka and Jamaica.
The potential value of sustained partnerships of this type is exemplified by our relationship with Sri Lanka, which has extended over 15 years and during which we have had invaluable support from Nancy Olivieri and her staff in Toronto. As well as developing a long-term research program, it has been possible to carry out a considerable amount of capacity development in Sri Lanka, including building a National Treatment Centre (Fig. 3) and an institute for DNA diagnostics in one of the medical schools. It has also resulted in the establishment of a national thalassemia control program.
Currently, the inherited hemoglobin disorders pose an increasingly serious global health problem. Although their high frequency reflects natural selection against malaria, their incidence is augmented by the large numbers of consanguineous marriages in many of the high-frequency countries. Advances in nutrition and public health, which have reduced childhood mortality in developing countries, have also led to an increased prevalence of the inherited hemoglobin disorders; babies with thalassemia or sickle cell anemia who would otherwise have died early in life are now surviving. So, the annual numbers of births of babies with inherited hemoglobin disorders is in excess of 300,000 (refs. 9,10). Recent estimates suggest that, if the life expectancy of African children with sickle-cell anemia doubles, soon there will be some six million children with this condition in sub-Saharan Africa9.
In 2002, the WHO asked me to write a report on the potential value of genomics for global health in the future!!. In the recommendations I pointed out the proven value of the North-South partnerships and suggested that the next logical development would be SouthSouth partnerships, that is, links between countries that have developed expertise in the management of these genetic diseases and those where no such skills
exist. We are in the process of testing this model in Asia, where we have developed an international network trying to form partnerships with countries such ash Thailand and India, where expertise in the diagnosis and management of these diseases exists, with adjacent countries, including Cambodia and Bangladesh, that do not possess such skills. Although plans for these developments are well advanced, they are extremely difficult to fund. Although both government and charitable funding agencies are willing to accept that there is a substantial research component in such ventures, they are often unwilling to accept the expenses that are also involved in the essential capacitγ-building aspects of these programs. This problem is exacerbated by the fact that the WHO, other nongovernmental organizations and the major international charities have, with a few exceptions, shown no interest in genetic disease, focusing almost entirely on the major communicable diseases.
There is some light on the horizon, however. Our Asian Thalassemia Network is well on the way to being established, and there are recent reports of similar interactions for the management of sickle cell anemia in Africa. If the governments of the developed countries can be persuaded that partnerships of this type are a cost-effective way of helping the developing countries, and that some of their aid should therefore be turned in this direction, there is some hope for the future for the control and management of these increasingly common diseases in the poorer countries of the world.
Taking a broader view, at Oxford we have developed similar long-term partnerships for research and capacity building in other aspects of tropical medicine; our partnership with Thailand recently celebrated its thirtieth year. Besides producing international leaders in tropical medicine research, these connections have led to important developments in the management and control of common diseases such as malaria. Although other universities and related organizations have moved in this direction, there is still enormous scope for closer interactions based on these models between universities in the rich countries and those in the developing world. It is crucial that
governments, national and international funding bodies and all those who are concerned with improving the level of health globally understand this message.
COMPETING FINANCIAL INTERESTS The author declares no competing financial interests. 1. Weatherall, D.J., Clegg, J.B. &
Naughton, M.A. Globin synthesis in thalassaemia: an in vitro study. Nature 208, 1061-1065 (1965)
2. Weatherall, D.J. & Clegg, J.B. The Thalassaemia Syndromes 4th edn. (Blackwell Science, Oxford, 2001).
3. Weatherall, D.J. & Clegg, J.B. The a chain termination mutants and their relationship to thalassaemia. Phil. Trans. R. Soc. Land. B 271, 411-455 (1975).
4. Weatherall, D.J. etal. Hemoglobin H disease and mental retardation. A new syndrome or a remarkable coincidence' N. Engl. J. Med. 305, 607-612 (1981).
5. Haldane, J.B.S. The rate of mutation of human genes. in Proc. Eighth Int. Congress Genetics. 267-273 (Lund, Sweden, 1949).
6. Allen, S.J. et al. α+-thalassemia protects children against disease due to malaria and other infections. Proc. Natl. Acad. Sci. USA 94, 14736-14741 (1997).
7. O’Donnell, A. et al. Interaction of malaria with a common form of severe thalassemia in an Asian population. Proc. Natl. Acad. Sci. USA 106,18716-18721 (2009).
8. Weatherall, D.J. Phenotype-genotype relationships in monogenic disease: lessons from the thalassaemias. Nat. Rev. Genet. 2, 245-255 (2001).
9. Modell, B. & Darlison, M. Global epidemiology of haemoglobin disorders and derived service indicators. Bull. World Health Organ. 86, 480-487 (2008).
10. Weatherall, D.J. The inherited diseases of hemoglobin are an emerging global health burden. Blood 115, 4331-4336 (2010).
11. World Health Organization. Genomics and World Health. <http://whqlibdoc.who.intlhq/2002/a74580. pdf> (WHO, Geneva, 2002).
Continues from page 11

Thalassaemia Matters ...continuing the fight against thalassaemia 13
11th ERTC Workshop on CAVOD11th December 2009, Paris
news from around the world
The UKTS was recently invited to take part in a workshop on European affairs, in a meeting held in Paris.
The meeting was for “Improving Access to Orphan Drugs for all Patients Affected by Rare Diseases in Europe: EU Assessment of Clinical Added-Value of Orphan Drugs (CAVOD) ”.
Through our membership of Eurordis (www.eurordis.org), the pan European association for Rare Diseases, we were involved in using our experiences of the UK for the benefit of all the patients with Rare Diseases in Europe. The meeting was attended by our committee member Chris Sotirelis.
What are rare diseases? Rare diseases, including those of genetic origin, like thalassaemia, cover all life-threatening or chronically debilitating diseases which are of such low prevalence that special combined efforts are needed to address them so as to prevent
significant morbidity or perinatal or early mortality or a considerable reduction in an individual's quality of life or socio-economic potential.
As a guide, low prevalence is taken as prevalence of less than 5 per 10,000 persons in the European Union. But there are a number of diseases within Europe that easily reach a prevalence of 5 per 100,000 persons and higher.
While this number seems small, according to the European Commission, in the EU with 27 Member States:• 75% of rare disease affect children• 30% of rare disease patients die before the
age of 5• 80% of rare diseases have identified
genetic origins. Rare diseases are characterized by a broad diversity of disorders and symptoms that vary not only from disease to disease but also from patient to patient suffering from the same disease. Relatively common symptoms can hide underlying rare diseases, leading to misdiagnosis.
It is estimated that between 5 000 and 8 000 distinct rare diseases exist today, affecting between 6% and 8% of the population in total - in other words, between 27 and 36 million people in the European Union. Thalassaemia is classified as one of these rare diseases, although its prevalence or its frequency in the EU can vary from country to country. Every day in the EU, at least 1,000 patients die of rare diseases.
The main problems faced by the patients with a rare disease, that are also common with thalassaemia include: • Lack of access to correct diagnosis• Delay in diagnosis• Lack of quality information on the disease• Lack of scientific knowledge of the disease• Heavy social consequences for patients• Lack of appropriate quality healthcare• Inequities and difficulties in access to
treatment and care.
Unfortunately the rarity of theses conditions has meant that until recently, drug development is not seen as a priority for the pharmaceutical industry as the numbers of patients are too small to make the expensive research and development process financially viable. To this cost the expense of carrying out clinical trials in the course of achieving the required licensing from the pan European regulatory authority, the European Medicines Agency (EMA) must also be added and its corresponding US counterpart in the USA, the Food and Drug Administration (FDA).Since the late 90s the EU has been increasingly focusing on the issues surrounding rare diseases. It has initially taken action through legislation to accelerate the licensing process and the fast tracking of the drugs that are destined for Orphan
diseases. The creation of the EU Orphan Drugs Regulation 141/2000 has stimulated research and development of orphan medicinal products in the EU. However when a new drug goes thorough this process and is approved i.e. receives its marketing authorisation, (MA), a license for commercial use in the EU, all 27 national pharmacological member state authorities are obliged to ratify it within a short period of time. In reality however according to the EU High Level Pharmaceutical Forum, “effective market access and utilisation vary strongly between and within Member States”.
This meeting was therefore held to better understand the roots of the problem and to find solutions. Because “the know-how to make the value assessment of Orphan Drugs is fragmented over national procedures within the Member States and their regions, there is a disconnection of national and regional processes from the knowledge and experience gathered upfront in the centralised processes does add to this fragmentation”. This situation generates detrimental delays in the national decision-making process aimed at making Orphan Drugs available to patients on national markets.
Faced to this major challenge, interested parties - from the patients and industry arena, as well as EU and national decision-makers - have identified the creation at the European Medicines Authority EMA of a Working Party for the assessment of the clinical added value of Orphan Drugs as being a key instrument
Continues on page 14 ➡

www.ukts.org14
for an increased collaboration between Member States and EU-level authorities. This collaboration is needed to overcome the specific bottleneck created by scarce, uneven and fragmented expertise on Orphan Drugs at national level.
Many of our patients and their doctors in the UK have had personal experience of the problems that arise when new drugs, like new oral iron chelators that have not been accessible to all due to constraints from the regional health authorities and the PCTs who impose a 'postcode lottery' system for funding the drugs.
“Theindustry[andpatients]hastoacceptthatjustbecausenewdrugsarelicenseddoesnotmeanthatthehealthservicewantsorneedstobuythem.”
Professor Michael Rawlins
Chairman of National Institute of
Clinical Excellence (NICE)
In our efforts to alleviate this problem we have been collaborating within a variety of fora like Eurorordis and C.A.V.O.D. and have succeeded in establishing a new methodology of assessment that will included additional criteria to look beyond the safety and efficacy of a new drug but also on its Clinical Added Value.
The main new definitions that will be used are shown below:
Effectiveness: is the extent to which an intervention does more good than harm when provided under the usual circumstances of health care practice.
Efficacy: is the extent to which an intervention does more good than harm under ideal circumstances.
Relative effectiveness: is the extent to which an intervention does more good than harm compared to one or more intervention alternatives.
Relative efficacy: is the extent to which an intervention does more good than harm under ideal circumstances (usual care), compared to one or more alternative interventions.
Significant Benefit: is a clinically relevant advantage or a major contribution to patient care.
Added Therapeutic Value: A new medicinal product can be said to have added therapeutic value if sound clinical data show
that it offers patients better efficacy, and/or better safety and/or simpler administration, than existing alternatives
The CAVOD proposal is a tool to:
• Improve access to orphan medicinal products in a timely manner for all patients whatever their geographical situation in EU.
• Gather the expertise at the European level to share information, experience,
skills, concerns, expectations, between all concerned parties – in particular EMA, HTA bodies, payers - as well as medical experts, patient representatives and sponsors, at the most relevant place to perform these tasks: the European Medicines Agency (EMA).
The UKTS shall continue to monitor these developments on European as well as on a national level in the UK seeking to realise the benefits for UK's thalassaemia patients.
news from around the world
Speech by Chris SotirelisVery grateful for being invited here to have an input to this debate, but I have to confess that I do feel a little bit overwhelmed about the complexity of the task as well as of the absolute necessity of what needs to be achieved.
I see my role here today as a catalyst to further progress in overcoming the barriers, the inertia, the political or institutional games or even the cynicism.
I would like to introduce a term that is widely being used in management and that originated in the computer industry. Fear Uncertainty and Doubt. - F.U.D. It is self explanatory and unfortunately today has a very wide application.
Returning to the quote of Mike Rawlins of NICE in the UK in Kevin’s presentation I would like to give an answer, obvious to any patient, that the main reason we need to have those drugs is that patients with rare conditions will simply keep on dying unless things change. But in order to institutions like NICE are able to respond we need to remove F.U.D.
Until recently there has been a game of cat and mouse between the institutions, Member states and the pharmaceutical industry. But this game costs lives because it puts patients in chronic waiting and does not provide the potential benefits that could be realised.
Until recently it has been a case of “yes.....but...wait and see”, or “maybe…..in the future ….but not yet” etc .
With the CAVOD proposals now it is a case that “…we have a plan and we need to get it implemented with a multilateral consensus.” But how are we going to implement the improvements that are clearly needed, particularly in the vital areas of accessibility, dissemination of scarce knowledge and
reimbursement. Issues of accessibility are quite ranging
and widespread. They really start from the point of the initiation of clinical trials and the eligibility criteria for patient acceptance. Even for those that are initially accepted onto the trials, Marketing Authorisation is not a panacea as there often is a long wait for national registration and budgetary approval by Member States. The added danger in this is when companies use this possibility in a cat and mouse game as a leverage to force the governments’ hand.
More practically, we need to dispel duplication and lack of clarity in the dosages at which optimal efficacy is achieved, at which is the window of effectiveness and at which toxicity occurs. In an ambiguous world we need to clarify how these clinical aspects explored before Marketing Authorisation will remain robust post authorisation during follow up and pharmacovigilance. There is a need to have a mechanism in place so that we totally remove FUD.
As patients willing to try a new drug we are all taking calculated risks with our most precious thing available to us; hope for a better outcome and a better quality of life. We are being responsible and self reliant and are putting our faith as well as our lives in the hands of our doctors, the scientists as well as on those who did the original investigations; a point not always remembered.
But both Member State authorities as well as companies have to be “open”, transparent and proactive in following the “true spirit” of their remit to serve the patient population of Europe. We look in hope for similar fora to achieve the desperately needed progress.

Thalassaemia Matters ...continuing the fight against thalassaemia 15
news from around the world
Brussels, Belgium, 18 November 2010
The UKTS as a member of several European patient institutions has been following development and become involved in a number of pan European initiatives to benefit patients with Rare Diseases like thalassaemia in the UK and in Europe as a whole.
More recently it was represented by our member Dr. Chris Sotirelis in the EPPOSI (European Platform for Patients’ Organisations, Science and Industry) Workshop on Patient Engagement in Health Technology Assessment (HTA).
The role of EPPOSI is an EU multi-stakeholder think tank on health policy, acting as a consensus building forum between patient organisations, science and industry in the process of formulating regulatory and health policy. Its primary mission is to establish a strong European alliance working to promote innovative healthcare best practice and implementation across Europe. (www.epposi.org)
HTAs refer to the investigations and evaluations undertaken by appropriate national HTA agencies of a country, like the National Institute of Clinical Excellence (NICE) of the UK, on behalf of that country’s health care authority or system, in order to examine or appraise it for its clinical effectiveness compared to the other existing or similar medications as well
as to its cost effectiveness, in relation to the benefits it gives the patient in terms of improvement in their quality of life, against the extra cost that the authorities need to pay to make it available to the patients. HTAs take place after a new medical product has been licensed by the European Medicines Authority. HTA is the independent evaluation of the social, economic and ethical benefits (or potential hazards) of treatment methods, drug therapies and health systems and is increasingly playing a central role in how national healthcare priorities are set and service provision is delivered in most EU member states. The objective is to allow faster, evidence-based access to innovative technologies that are clinically sound and cost effective, while helping to eliminate treatments and practices that are shown to deliver limited health benefits or financial value.
As until now in most EU countries these assessments took place either with minimal or no patient involvement, the aim of this workshop, in order to achieve the above objective was for Health Technology Assessment (HTA) agencies to support patients to become full partners in HTA policy and processes if their unique contribution is to be fully utilised to the socio-economic benefit of all in society.
This workshop is very topical for the Thalassaemia in the UK due to the recent decision and invitation received by the UKTS to participate in the consultation
for the forthcoming Health Technology Appraisal that NICE will be undertaking for the 3 iron chelators.
The event, which brought together experts from patients’ associations, national and regional HTA agencies, national health systems, public health and social science academics, clinicians and healthcare practitioners, and the pharmaceutical and biopharma industry, included 4 breakout sessions and it set out to identify the barriers to greater patient engagement in HTA and tried to come up with concrete recommendations to address four key issues:
• When and how should we engage patients in the HTA process?
• What questions can patients ask of the “hard” evidence to be sure that they reflect patients’ concerns?
• How can patient organisations collect evidence that will be useful for HTAs?
• What can HTA Agencies do to improve engagement with patients?
“It’s my view that all agencies should have policies for patient involvement. There is a clear need for more transparency on the work of agencies and clear indications on where patient engagement should take place.” said Finn Børlum Kristensen, (photo above) Chairman of the Executive Committee of the EUnetHTA Joint Action of Member States. This was one of the
Dr Chris Sotirelis
Continues on page 16 ➡

www.ukts.org16
news from around the world
main recommendations of a workshop on Patient Engagement in HTA. Other recommendations included:
1. HTA agency policy for patient engagement: take examples of best practice internationally (e.g. including Canada and Australia) as well as from within Europe to generate minimum standards for involvement that can be adapted and replicated nationally and locally. Take examples from the European regulatory processes where patients and patients organisations are fully involved in the risk/benefit assessment and actively participate in the definition of what constitutes value in diseases management.
2. Education: patients must be educated to better understand the concepts underpinning HTA so they understand how to contribute evidence that provides added value to the process. Similarly, HTA decision-makers and clinicians need to be better educated about patients’ real-life experiences in order to move beyond clinical and cost-effectiveness issues when making decisions to take into account the full range of psychosocial aspects affecting patients’ treatment and care: family and carer support, quality of life and wellbeing, employment etc.
3. Resources: increasing patient engagement will take manpower and resources and should be transparent (educational and financial support to patients’ groups in order for them to participate, extra manpower at HTA agencies to help patients participate).
4. Collaboration: the only way to achieve real patient engagement in HTA is through greater collaboration between patients, HTA agencies, clinicians, academia and industry and to be clear about where and how collaboration can take place.The full recommendations will be
published in December and will form the basis of a new thematic programme to be launched by EPPOSI in 2011 to help facilitate better HTA processes by all partners. We look forward to maintain our involvement in this forum of European healthcare policymaking.
13th Workshop EURORDIS Round Table of Companies13th December 2010
The UKTS has for many years been involved in the pursuit of full and unrestricted access to all the medicinal products required by thalassaemia patients in the
UK. Our policy has been designed and focused on a local-regional level, (Primary Care Trusts) national (NHS, Scottish Medicines Consortium-SMC, NICE) as well as the European level (EMA, DIA, DG SANCO).
In continuation of the UKTS involvement of the European policy making and regulatory institutions and through our membership of EURORDIS, the European Organisation of Rare Diseases, representing all Rare Diseases Patient Organisations, we have been invited to participate in this year’s EURORDIS Round Table of Companies Workshop for "Patients'Access to OMPs, Innovative Pricing Schemes and National Measures in a Global Financial & Economic Crisis Environment". The meeting held in Paris this December was attended by our member Dr. Chris Sotirelis and tried to examine the relationship between pricing and reimbursement that has developed in the EU.
The EURORDIS past surveys on Orphan Drug availability in Europe had pointed out to unacceptable delays and inequalities in rare disease patients’ access to their medicinal products. As also shown by other independent studies, EURORDIS has shown how different factors, like sponsors’ market strategies and local National Competent Authorities (NCA) practices and procedures, result in a disparity of access to OMPs across Europe.
In 2008, among the conclusions and recommendations of the High Level
Pharmaceutical Forum it stated: “Member State authorities, stakeholders and the Commission should strengthen their efforts to ensure access to orphan medicines in all EU Member States. They are therefore called upon to take up the appropriate ideas developed in the Working Group Pricing regarding i) early dialogue on research and development, ii) exchange of knowledge on the scientific assessment of the clinical added value, iii) specific pricing & reimbursement mechanisms and iv) increased awareness on orphan diseases.”
Patients’ associations as well as national Alliances for Rare Diseases, have and need to play a greater role in bring up the awareness and the During this workshop, EURORDIS would like to evaluate how the different stakeholders have implemented the above recommendations and what impact, if any, the financial crisis has had on patients’ access to Orphan Medicinal Products (OMPs), which also include those needed by thalassaemia patients.
However, while these problems were being realised and plans for their correction were underway, the global financial crisis hit the world and today, with this 13th ERTC workshop, EURORDIS would like to evaluate how the different stakeholders have implemented the above recommendations and what impact, if any, the financial crisis has had on patients’ access to OMPs.

Thalassaemia Matters ...continuing the fight against thalassaemia 17
news from around the world
During the workshop and in the morning sessions, three different pharmaceutical companies will be given the opportunity to report on their recent experiences on pricing and reimbursement at national level, highlighting in particular any differences in the national negotiation approaches and attitudes towards new orphan drugs accessing their market. A panel discussion ended the morning session explored what pharmaceutical companies and National Competent Authorities (NCA) are ready to do or accept in order to ensure access to patients in a timely and affordable manner. From these session we learned that the annual treatment cost average for all Orphan Drugs in the market today, across the 8 EU countries is €138,000 and that there are 9 “blockbuster” drugs with a cost greater €200.000 annually.
• In terms of pricing versus prevalence, pricing is NOT based on factors typical of Orphan Diseases, (O.D), but
• Pricing occurs on a case by case basis for each drug.
• On the side of the NCAs however, in view of the high burden of the disease, reimbursement usually happens with limited evidence of the therapeutic value of the drug and this lack of evidence is not reflected in the cost.
• At the moment OD have a minor impact in the overall healthcare budget of a country, but this is forecasted to grow significantly in the coming years causing the NCAs to increase their rate of rejection, even though if we exclude those 9 “blockbuster” drugs the remaining are below € 50,000 per annum and 15 of them are considerably less than € 50,000.
The conclusion one can draw from the
above is that even in the more tolerant countries payers will impose controls for cost effectiveness and stricter evaluations. But under what assumptions? It is most likely that there will be a shift from the “perceived” to “objective value” of a product.
So, we need to build more evidence and to have a more rational drug pricing policy.
Then during the afternoon session, breakout sessions were organised to give the attendees the opportunity to discuss on different related and sensitive issues in parallel working groups such as:
1. Considering the first innovative approaches and concrete experiences, what new pricing scheme could be implemented for orphan drugs in the upcoming years?
2. Which coordinated mechanism of access to orphan drugs is needed at the European level?
3. Some price containment measures are put in place in some Member States: how to handle the specific case of Orphan Drugs?
4. What best practices should be implemented at national level to ensure that stakeholders have a real interaction and participation in the different aspects related to patients’ access to orphan drugs?
The recommendations that emerged included: • Pricing needs to be based on pharma-
economic data to capture the benefit to society, the cost-saving ratio of the benefit instead of just “the cost of the damage caused to budgets”.
• The evaluation needs to encompass other measures apart from cost per QALY such as the Core criteria for used in national commissioning in the UK under the AGNSS process. (see diagram below)
• To overcome local obstacles access, need reassessment of cost to benefit ratios of the real need for common regulation and for an early dialogue.
• A pilot project was proposed for the pricing and reimbursement to be discussed much earlier between
companies and HTA NCAs, for a better understanding of the needs of the stakeholders.
• Increase in participation of disease specific experts, and patient experts in these appraisals, they should receive training for HTAs; broadening the agencies to accept their inputs and perspectives.
In conclusion, we can say that since the adoption of the OMP legislation enacted 10 years ago, a stimulus has been provided for this as is borne out in the statistics of with a doubling of the number of OMPs receiving EU marketing authorisation in the last five years. In 2006, for example, orphan drugs accounted for 23 per cent of all new marketing applications.
There is little doubt that the attractiveness of the orphan disease market has increased in recent years, as manufacturers change their focus from discovery of the next mass market 'blockbuster' to more specialist 'niche busters'. If it is also equally evident that in the UK, patients with rare diseases will continue to be denied access to innovative and effective treatments for rare and neglected diseases, treatment that can make a difference to what are, by definition, life threatening or chronically debilitating illnesses, then there is an imperative for the current methods of evaluating and paying for orphan drugs to be overhauled.
Figure 1: Core criteria for national commissioning: Taken from AGNSS's Decision Making Framework

www.ukts.org18
Nepal Blood Transfusion Clinic is now officially OPEN!!!!
By Wendy Pinker
Our regular readers will no doubt recall earlier articles in TM from Wendy Pinker, the British woman who has single-handedly transformed the lives of the thalassaemia children of Nepal. Without the heroic efforts of this truly inspirational woman, there would have been no money, no clinic and no hope for these children. We at UKTS are honoured to be associated with Wendy and the Nepal Thalassaemia Association; and we are more proud than we can say of her achievements. We are delighted to bring you Wendy’s latest instalment of news from Nepal. It is long but we make no apology for reproducing it in its entirety. It is truly humbling to see how much can be done with so little in the developing world.
At the end of the article are Wendy’s contact details in case anyone wants more information or to make a donation. Our very grateful thanks to those of our members who have supported Wendy and helped her to realise this dream.
N.B. All Wendy’s work for thalassaemia is entirely voluntary. She is not a health professional and has no personal connection with thalassaemia other than her humanitarian feeling for the children.
Dear FriendsI am writing with the most wonderful and exciting news… the long awaited and desperately needed BLOOD TRANSFUSION CLINIC IN KATHMANDU, NEPAL is now OPEN !! Three years ago my dear friend Durga Pathak (Nepal) and I had a dream…it was what seemed like an impossible dream but never the less a dream that we would pursue until it came true.
We wanted to open a blood transfusion clinic for the very sick thalassaemic children of Nepal. As many of you will already know a thalassaemic child has to have a blood transfusion once every two weeks just to survive… Until now it has been a painful and arduous procedure for each and every child and their family. Due to such poor health care facilities in Nepal, blood transfusions are not widely available meaning that most have to travel to Kathmandu (the capital of Nepal) just to receive such a basic treatment. There
are no trains in Nepal and the roads are long, slow and very mountainous… many patients travel over 12hrs by bus every 2 weeks. Others who are more fortunate have been able to afford the costs of relocating nearer to the capital.
On arrival in Kathmandu the patient and parent have to check in to Kanthi Children’s Hospital in Lazimpat. Kanthi Hospital, like most in Nepal is under equipped, under financed and unimaginably dirty. The stench that hits you on entering the hospital is one that will stay with you forever. The child is admitted to the ward and then the parent has to travel across the capital to the Red Cross Blood Bank to collect a packet of blood. In the searing heat of the monsoon period, often the blood is off by the time the parent returns to the hospital and the whole process has to start again. It is a long and heart wrenching procedure. Nobody should have to struggle so much
news from around the world
Members of NTS outside the clinic
One of the children presents Wendy with flowers.

Thalassaemia Matters ...continuing the fight against thalassaemia 19
news from around the world
to help a sick child receive such simple treatment.
After a two-year stay in Nepal I returned to the UK to start my mission. Durga, The Nepal Thalassaemia Society and I had drawn up a financial plan to get our little clinic off the ground. Just £14,000 would be enough to set it up and run it for 2 years offering totally free treatment for every child. It was much to my amazement that many people already knew of my plan and shortly after my arrival 2 incredible ladies contacted me. Sue Woolston and Ann Brodin. They said that they had heard
of my dream and that they were going to help me - I couldn’t believe my ears! There was no turning back now. Without them it may never have got off the ground. Before long garden parties, casino nights and dinner dances were being arranged. Local people came to my home with offerings of personal donations and my very dear friends Alison and Justine Perkins had donations made to my clinic instead of receiving wedding presents! Later that year I was to meet a wonderful lady called Maureen Donnison who went with 12 of her friends to visit my family in Nepal and were so touched by what they saw they decided to help too. After collecting sponsorship for their treks in the Himalayas and arranging a very successful ABBA night back home in the UK they were able to donate just the amount we needed to secure the £14,000 target… mission accomplished! Now all we had to do was start phase 2.
In December 2009 I returned to Nepal to meet with Durga and the Nepal Thalassaemia Society (NTS) members. They had no idea that we now had the funds needed to open the clinic and when I told them they were totally shocked and elated. I will never forget the looks on their faces. The NTS committee is made up totally of members who have thalassaemic children meaning that everybody is working for
the good of their own family. They are an active and enthusiastic team. They now had one of the biggest challenges ahead - to find a suitable building (very close to the Red Cross Blood Bank), furnish and equip it, find a nurse, a doctor and set up the new NTS offices!
After 12 months in the UK while my son had surgery I returned to Nepal at the beginning of February 2011, more than 6 months after the long awaited opening of our life saving Blood Transfusion Clinic. I finally got to see the fruits of all of our work and… it was far and beyond what I ever could have dreamed of.
Early on the morning of 6th February my husband Rishi, son Tall and I got into a taxi and made our way across Kathmandu near to the Red Cross Blood Bank. We didn’t really know where we were going and it was hard to make out where we were with all the dust in the polluted air.The taxi dropped us in the area we were heading to and we walked aimlessly, not really knowing where to look…Then from the corner of my eye I saw it !!!!… In big red letters…
“Nepal Thalassaemia Blood Transfusion Clinic”
Goose bumps shot over my body from head to toe. There it was as real as life… my dream… in a little dusty old side street in the heart of the capital of Nepal… Oh my word… whoever in a million years would have thought this would happen !
I opened the gate to find everybody waiting - society members, parents, nurses and most important of all – the children. It was amazing… a moment in my life I will never ever forget. I was greeted with flowers and dozens of smiles.
We went into the building and had a tour around. First the meeting room, a very simple, clean spacious room with lots of chairs to be used for meetings, resting and private consultations. Then the examination room, again very simple, a room used by the doctor if a child gets sick whilst having a transfusion. Then the office! Well, it was so grand I think the whole country could be run from there! There was even a computer and printer, all lovingly covered with cloths to protect them from the dust. Then the moment of truth - the transfusion room. Wow, what a
The NTS clinic nurse
Paras, Secretary of NTS and the oldest thalassaemic in Nepal at age 23

www.ukts.org20
news from around the world
wonderful surprise it was. It was the most beautiful, brightly coloured, clean, bright, airy, cosy room you could imagine - I was moved to tears instantly.
We all sat (about 40 of us) and talked about how things were going and how life had changed so much since last the time we all met. The parents talked of how their lives have been made so much easier and the children told stories of how they look forward to coming to Kathmandu for their fortnightly transfusions!!!! It was like a fairy tale.
Previously a transfusion would take all day and possibly the next day. Now the patient’s carer just makes one simple phone call to the clinic the day before they are able to come to Kathmandu and Paras (our secretary) calls the blood bank and the blood is prepared for that particular child. The blood is then collected later that day and stored ready for use the next day. The next day the patient arrives and after a few checks the transfusion begins… and thanks to our wonderful nurse there are no tears to seen or cries to be heard and it’s all over in 4 hours. And to top it all, it’s totally free of charge. Cartoons, movies and Nepali music are played all day. It is like a holiday for many of the children who don’t have the privilege of a TV or electricity in their own homes. The children have all become friends and it’s like a big family all with the same illness. The parents sit and talk and compare stories, worries and concerns. Amazingly, two of the older children now walk alone to the clinic so their parents are after many years of being tied now free. It really is a miracle to see.
This little clinic has truly changed the lives of each and every child and parent we support and it’s all down to YOU… each and every one of you who has made even a single pound in donations or has bought my jewellery or helped at one of our many fund raising events - you are the ones who have made this possible. Every single penny has come from the UK and it has come from one of you. It has cost just £13,500 to open and run the clinic for 2 years and… we almost have enough for another year!!!! I can’t thank you enough for all of your support and I dream that we can continue to raise the funds for the years ahead. Every penny you donate goes direct to the clinic fund and not a
single penny goes for administration because I do it all myself. I thank you for your continued support from the bottom of my heart.
My next mission is to try to raise the funds for all the children to have the next stage of their treatment. Chelation treatment is the removal of excess iron caused by having blood transfusions on a regular basis. It is essential for the prolonged life of a thalassaemic. At the moment only 10% of our children are receiving this treatment and all are by donation. It costs just £30 per month or £360 per year. I would like to thank all those who have already sponsored a child for these costs… your love and support has given a new lease of life to an otherwise very sick child. Thank you with all my heart x
If anyone would like to know more about our clinic or make a donation please
call Wendy Pinker on 07836 572 062 or email [email protected]
The oldest thalassaemic in the UK is about 60 years old… the oldest known thalassaemic in Nepal is Paras (shown in the photo above), he is 23. We want to change these statistics and make a more wonderful world for all the thalassaemia children of Nepal.
You can’t change the world… But you can make a difference in your own space x.
Mum and baby resting during transfusion
A busy day at the transfusion clinic

Thalassaemia Matters ...continuing the fight against thalassaemia 21
office news
We provide valuable medicines to rare disease patients
SOIUKP1110 - Date of Preparation: March 2011
SOBI A4 Advert_R+no.ai 1 09/03/2011 15:28

www.ukts.org22
office news
UKTS AGM 2010The 2010 Annual General Meeting of the UK Thalassaemia Society tool place on 7th September at the Society’s premises at 19 The Broadway, Southgate, London. Outgoing President Mike Michael presented his report and was thanked by outgoing Secretary Menuccia Tassone for his 10 years of sterling work as UKTS President. Trustee George Constantinou gave the Treasurer’s report on behalf of Treasurer Bharat Nathwani. Mr Leo Leonidou of UKTS accountants/auditors Lyons Leonidou was also present; and Lyons Leonidou were reappointed for the forthcoming year.
Election of officers: As only 8 people were nominated for the Management Committee they were elected without the need for a vote to be taken. The new Management Committee is as follows (in alphabetical order):-
Andy Charalambous (Vice President)
Andy is a 52 year old beta thalassaemia major patient. He is a founder member of UKTS and has served on the Management Committee for several terms in the past. Andy has always been a regular attendee at both
national and international thalassaemia events and conferences. He has returned to the Committee after a break of over 10 years, having a little more time on his hands now that his children are growing up. Andy is a retail shop manager by profession. He is married with a son and daughter.
Adam ChristodoulouAdam is a 43 year old beta thalassaemia major patient. His experience as a patient is further informed by the fact that his wife’s family is also affected by thalassaemia major. He has been a life member of UKTS since
1991. Adam has been motivated to stand as a Trustee at this AGM by the sad loss in 2009 of his dear friend, our late Trustee Costas Kountourou. Says Adam; “I know that the loss of Costas’ experience and knowledge has been a grievous blow to the Society. I wanted to do my part to step in and help to bridge the gap which has been left by his loss. I look forward to working with the other members of the Management Committee to take the Society forward in the way Costas would have wished.” Adam is a project manager for a mechanical/electrical company by profession; and is married with a son.
George Constantinou (Secretary)George is a beta thalassaemia major patient. He is a founder member of the UKTS, having served on the Management Committee from 1976-1985 and again from 1999 to the present day. George has been a
tireless campaigner on behalf of thalassaemia all his adult life and has conceived and been involved with many UKTS projects including conferences and awareness projects. He was involved in producing the revised version of the UK National Standards for thalassaemia treatment (published October 2008) and with the finance committee of the Society. He has served UKTS in the office of Treasurer in the past. George is a hotel manager by profession and is married and has a daughter.
Katerina (Nina) Demetriou (Assistant Treasurer)
Nina has previously served on the UKTS Management Committee for several terms as the Treasurer. She has also been involved in the sub-committees organising conferences and workshops and is always willing to help
where possible. Nina’s involvement with the UKTS has included the management of the accounts and she is keen to see that funds received through hard work are used efficiently to meet the objectives of the Society. Nina has held the post of Assistant Secretary in 2009/2010. She is a senior finance officer by profession.
Pany GaribaldinosPany is a 53 year old beta thalassaemia major patient. He was a founder member of UKTS in 1976 and served on the Management Committee for many terms in the early years of the Society. He is now keen to
return to add his experience to the Management Committee. As one of the older patients, who has experienced the progression of thalassaemia treatment from the bare minimum of blood transfusions to the sophisticated treatment régimes of the present day, Pany feels that his experiences will enable him to make a valuable contribution to the work of the Society. Pany is married with a son; and he is a driving test examiner by profession.
Romaine Maharaj (Assistant Secretary)
Romaine’s daughter Roanna is a beta thalassaemia major patient. Prior to moving to the United Kingdom in 2004, Romaine served as the President of the Society of Severe and Inherited Blood Disorders, Trinidad and
Tobago, one of the founding members of TIF. She was attached as a Patient Advocate with ApoPharma for a year. She was also the Head of a mortgage division for one of the major banks in the Caribbean, her financial background spanning a period of twenty three years. Currently she is working as an Assistant Attaché at the Trinidad and Tobago High Commission, London.
Bharat Nathwani (Treasurer)Bharat’s daughter Mena is a beta thalassaemia major patient. He is a life member of UKTS. Bharat hopes that his experiences as a parent of a young child with thalassaemia then growing up to adulthood will give
him a valuable insight into the experiences of other parents in the same situation. He is an accountant by profession and is actively involved on the finance committee; having held the post of Treasurer in 2009/2010.
Gabriel Theophanous (President)(In Gabriel’s own words) – I am 33 years old with beta thalassaemia major. I work in accounts and am currently studying towards an ACCA qualification. I would like to be a member of the committee of UKTS because
I admire all the hard work the Society has done in the past and would now like to contribute as much as I can. I also made a promise to my dear friend Costas Kountourou that I would join so I’d like to try and carry on his good work if possible. It would be an honour and a privilege to help those less fortunate than myself. Having become close friends with the current Committee members after attending meetings and conferences, I realise just how much I (as well as all thal patients) have benefited from the hard work the UKTS has done over the past 30 years so this is an opportunity to give something back.
21 voting members attended the AGM.

Thalassaemia Matters ...continuing the fight against thalassaemia 23
office news
This book of personal memories and tributes has been produced by the UK Thalassaemia Society in recognition of the late Costas Kountourou’s lifelong contribution and commitment to the cause of improving the lives of his fellow
thalassaemia patients; both in the UK and worldwide.The UK Thalassaemia Society gratefully acknowledges the assistance of all those who have contributed; with special thanks to Costas’ sister, Gina Halwani, for her devoted work in helping
us produce the book.
For further information or to request a copy please contact the UK Thalassaemia Society office.
Forever in our hearts
Samina’s Skydive for ThalassaemiaOn 17th July 2010 brave Samina Sajad raised over £2,500 by doing a sponsored skydive in aid of the UK Thalassaemia Society. Samina’s nephew, Armaan Jameel, has beta thalassaemia major. At just three years old, Armaan is the youngest life member of UKTS!
Our sincere and grateful thanks to Samina and all the family members, friends and colleagues who sponsored her.
Ronald Lo, the Churchwarden of Christ Church, Southgate, presents a cheque for £2,000 to UKTS Assistant Coordinator Katerina Loizi-Read. This generous donation was raised at the Southgate May Day Fair on 3rd May 2010; which was attended by Katerina. Our grateful thanks to the organisers.
Richard Simon, Products & Marketing Manager of the Bank of Cyprus presents a donation of £3,000 to UKTS President Gabriel Theophanous and Assistant Treasurer Nina Demetriou at the Bank’s Southgate office on 18th January 2011. The bank regularly gives charitable donations rather than sending out Christmas cards. We are extremely grateful to the Bank of Cyprus for their continued support.
Costas Kountourou[1961 - 2009]

www.ukts.org24
office news
Recent Events & Meetings
• 01July2010–NHSSickle/ThalassaemiaScreeningProgrammenewbornoutcomessteeringmeeting,London– Attended by UKTS Coordinator
Elaine Miller
• 06July2010– open evening at UKTS’ office with
presentation on gene therapy by Dr Michael Antoniou
• 07July2010–meetingtoexaminethelatestdevelopmentsintreatmentforHCV,UCLH– Attended by: UKTS Vice-President
Dr Christos Sotirelis, Trustee George Constantinou & Coordinator Elaine Miller
• 13July2010–AwaydaymeetingofUKForumonHaemoglobinDisorders,London– Attended by UKTS Coordinator
Elaine Miller
• 15July2010–MeetingofDHClinicalServicesDevelopmentGroup,London– Attended by UKTS Vice-President
Dr Christos Sotirelis & Coordinator Elaine Miller
• 15July2010–NHSSickle/ThalassaemiaScreeningProgramme
newbornoutcomesclinicalgroup– Attended by UKTS Coordinator
Elaine Miller
• 16July2010–PanLondonHaemoglobinopathyForummeeting,London– Attended by UKTS Coordinator
Elaine Miller
• 27August2010–FuneralofMsSoniaLindsay,CEOofOSCARBirmingham– Attended by UKTS Coordinator
Elaine Miller
• 06September2010–Meetingonmedicaleducation,AllPartyParliamentaryGrouponSickle/Thalassaemia,London– Attended by UKTS Coordinator
Elaine Miller
• 15September2010–NHSSickle/ThalassaemiaScreeningProgrammenewbornoutcomessteeringmeeting,London– Attended by UKTS Coordinator
Elaine Miller
• 16September2010–Serviceusermeetingoncompetencesforhaemoglobinopathynurses,BirminghamSickle/ThalassaemiaCentre– Attended by UKTS Coordinator
Elaine Miller
• 16September2010–NHSSickle/ThalassaemiaScreeningProgrammeLaboratorySubgroupmeeting,London– Attended by UKTS representative
Martin Jarvis, Director, Pathology Laboratory North Middlesex Hospital
• 20September2010–Meetingofblooddonorselectionsteeringgroup,AdvisoryCommitteeintheSafetyofBlood,TissuesandOrgans(SaBTO),DeptofHealth
– Attended by UKTS Coordinator Elaine Miller
• 27September2010–School&PublicHealthNursing4thNationalConference,Birmingham(presentation)– Attended by UKTS Coordinator
Elaine Miller
• 07October2010–SSCATFoundationAwarenessDay,Sheffield(presentation)– Attended by UKTS Coordinator
Elaine Miller
• 07October2010–StThomas’Hospital,Sickle/ThalassaemiaTrainingCourse(presentation)– Attended by UKTS member
Mike Michael
• 08October2010–meetingofprotocoldevelopmentgroupforcarefactorsassociatedwithpositivementalhealthforsickle/thalassaemiapatients,RobertGordonUniversity,Aberdeen– Attended by UKTS Coordinator
Elaine Miller
• 20October2010–PEGASUSevaluationmeeting,London– Attended by UKTS member
Dr Christos Sotirelis
• 04November2010–Awarenesspresentation,SouthgateSchool,London– Attended by UKTS Coordinator
Elaine Miller & member Roanna Maharaj
• 05November2010–meetingonthalassaemiaandsocialintegration,London– Attended by UKTS Secretary George
Constantinou, Asst Secretary Romaine Maharaj, member Dr Christos Sotirelis & Coordinator Elaine Miller

Thalassaemia Matters ...continuing the fight against thalassaemia 25
office news
• 10November2010–SteeringGroupmeeting,NHSSickle/ThalassaemiaScreeningProgramme,London– Attended by UKTS member Dr Christos
Sotirelis & Coordinator Elaine Miller
• 14November2010–meetingofNofEnglandBoneMarrow&ThalassaemiaAssoc,Manchester(presentation)– Attended by UKTS Coordinator
Elaine Miller
• 17November2010–EPPOSIBrussels
• 18-19November2010–ENERCAMadrid
• 18November2010–Academicmeeting,UKForumonHaemoglobinDisorders,London– Attended by UKTS Coordinator
Elaine Miller
• 25November2010–NationalHaemoglobinopathyProjectmeeting– Attended by UKTS member Dr Christos
Sotirelis
• 27-28November2010–ThalassaemiaInternationalFederationBoardmeeting,London– Attended by UKTS TIF representatives
Mike Michael & Nina Demetriou, President Gabriel Theophanous, Secretary George Constantinou, Asst Secretary Romaine Maharaj & member Dr Christos Sotirelis
• 29November2010EPPOSIPrague
• 30November2010–MeetingwithChairofAllPartyParliamentaryGrouponSickle&Thalassaemia,London– Attended by UKTS Coordinator
Elaine Miller
• 01December2010–MeetingofDHClinicalServicesDevelopmentGroup,London– Attended by UKTS member Dr Christos
Sotirelis
• 07December2010–Meetingofblooddonorselectionsteering
group,AdvisoryCommitteeintheSafetyofBlood,TissuesandOrgans(SaBTO),London– Attended by UKTS Coordinator
Elaine Miller
• 13-14December2010EURORDISParis
• 20December2010–Seminar,“CaringforMuslimPatients”,Birmingham– Attended by UKTS Coordinator
Elaine Miller
• 13January2011–meetingwithSecretariatofAllPartyParliamentaryGrouponSickle&Thalassaemia,London– Attended by UKTS Coordinator
Elaine Miller
• 17January2011–GeneticAllianceUKTrusteemeeting,London– Attended by UKTS Coordinator
Elaine Miller
• 18January2011–meetingofworkinggrouponnewcompetencesforhaemoglobinopathynurses,London– Attended by UKTS Asst Coordinator,
Katerina Loizi-Read
• 19January2011–Meetingofblooddonorselectionsteeringgroup,AdvisoryCommitteeintheSafetyofBlood,TissuesandOrgans(SaBTO),London– Attended by UKTS Coordinator
Elaine Miller
• 28January2011–Peerreviewforredcelldisordernetworks(paediatrics)Leeds– Attended by UKTS Coordinator
Elaine Miller
• 29January2011–MeetingwithBradford/Leedsregionpatient&carersgroup,Bradford– Attended by UKTS Vice-President
Andy Charalambous, Secretary George Constantinou, Asst Secretary Romaine Maharaj & Coordinator Elaine Miller
Send Us Your Email Address!!!
Dear Friends
Now we are more than 10 years into the new century and communication is faster and better than ever before. Email is by far the easiest and quickest way to keep in touch. It takes a matter of seconds to send an email to literally hundreds of people; whereas having to write to them all would take days of work! So if you have not already done so, please contact the UKTS office and send us your email address – please send it to [email protected] and include your name and postal address on the email.
Many thanks!
N.B. Many people change their email address and forget to tell us – so if you may have changed your email address since joining UKTS, please let us have your current address!

www.ukts.org26
office news
On the 19th February 2011 we all arrived in Karachi, Pakistan; myself, my husband Amjad and our two children. We were visiting to attend a family wedding. On the 21st we went back to the Edhi Foundation orphanage, from where we found our beloved adopted children Sabrena and Shariq. This was the first time we had all been back. Sabrena, who has thalassaemia major, wanted to go back and see the place she had come from. Her idea was to take wash bags, toothbrushes
and toothpastes back for the children at the Foundation. We managed to collect 552 items. Sabrena and her brother Shariq handed out the wash bags - Sabrena was a little nervous at first but soon got into her stride.
We all enjoyed our experience, my husband and I shed a few tears, but we were so pleased we went. Every time we go home to Pakistan we will go back again and take presents for the children.
By Sobia Afridi
Last year we circulated a patient survey which many of you were kind enough to complete and return. Those who completed the surveys were invited to take part in prize draw for gift vouchers worth £100 from John Lewis. We would like to announce that the lucky winner of the prize draw is Ms Selina Yip from Surrey. Selina, a thalassaemia patient, is under the care of Dr Maria Pelidis at St George’s Hospital, London SW17. We hope she enjoys spending her vouchers!
Going back to the orphanage
Prize Draw Winner
Alastair Kent
Dr Allison Streetly
Alastair Kent, Director of Genetic Alliance UK and Dr Allison Streetly, Programme Director.
NHS Sickle Cell and Thalassaemia Screening Programme were both awarded OBEs in the New Year’s honours list for their valuable contributions in their respective fields. We at UKTS are delighted to see their good work rewarded and we know our readers will join us in congratulating them.
New Year Honours

Thalassaemia Matters ...continuing the fight against thalassaemia 27
UKts Welcomes neW‑MeMBeRs
AnnualMeryam Adem
Azra Bibi Elton Chisholm Eda Mentesh Irsen Oldac
Gagandeep Singh
LifeDr Hafizur Rahman
Our most grateful thanks to all our donors for their generosity.
Dr Aggarwal £20 .00
Mrs Patsy Andrews £10 .00
Prof Elizabeth Anionwu £50 .00
Mr Ash Bhagat £35 .00
Mr G . Cagligione (sponsored run) £100 .00
Mr G . Christodoulou £150 .00
Mr & Mrs Christoforou £30 .00
Mrs B . Dattani £10 .00
Ms M . Gamble £32 .00
Mr S . Gandhi £690 .00
Mr P Garibaldinos £10 .00
G . Gordon £15 .00
S . Hussain £5 .00
Mr & Mrs Ioannou £30 .00
Mr & Mrs Kaimikkami £70 .00
A . Katsouris £50 .00
Mr Chris Kantaris £275 .00
Mr Chris Kantaris (sponsored leg waxing) £1,500 .00
Mr Tanver Khan £10 .00
Mrs T . Kountourou (memorial book for Mr Costas Kountoruou) £519 .95
Mr Kurji £10 .00
Mr & Mrs Louka £150 .00
Ms D . Luka (in memory of Ms Vilas Luka) £175 .00
B . Lysandrou £50 .00
Mr & Mrs Mardia £50 .00
Mr & Mrs Mansi £1,000 .00
Prof B . Modell £20 .00
Mr B . Morrissey £100 .00
Mrs Nicolaou £20 .00
Mrs Amanda Nicola £5 .00
Orion Design & Print £300 .00
Mr & Mrs Patel £50 .00
Mr D . Patel £60 .00
Mr Harpreet Panesar £10 .00
Mrs Papanicola £120 .00
Ms M .S . Pelidis £10 .00
Mr Pike £100 .00
Mr P . Polycarpou £100 .00
Ms D . Ptohopoulos £100 .00
Ms Maria Read £46 .00
Mrs Mary Read £20 .00
Mr Singh £50 .00
Mr Rajpal Singh £100 .00
Mr & Mrs Soni £145 .00
D .W . & V . Stirman £10 .00
Summer Bash Event (Athina Klitou & Tanya Yucel) £1,948 .50
T .A .S .C . £1,000 .00
Nasim Tariq £5 .00
Mr & Mrs Tsikkos £30 .00
Despina Vandi concert brochures £201 .40
Mrs Betty Why £105 .00
Dr Beatrix Wonke £10.00
Mr Yiannis £10 .00
Mr & Mrs Yiannikou (in memory of Stella Yiannikou) £500 .00
In memory of Mrs Fanoulla Christodoulou £3,552.00
In memory of Father Andreas Garibaldinos £2,000.00
DONATIONS
The Editorial Committee reserves the right to alter any articles for publication where necessary and accept and reproduce or copy on good faith.
Neither the Editorial Committee or the Society accept any responsibility for any inaccuracies or omissions.
The views expressed are not necessarily that of the Society.
office news
UKTS in the North of England
We are pleased to announce that as from the 1st May 2011 our Coordinator Elaine Miller will be based in South Yorkshire as our North of England representative. She will be working predominantly in the North of England with patients and families; and will also be extending our awareness work in the community. For those of you who already know Elaine, her contact details will remain the same; email [email protected], telephone 07958 084 892.
UKTS is grateful for the support of the Roald Dahl’s Marvellous Children’s Charity; which is partially funding this project.
Funded by

www.ukts.org
Desi
gned
and
prin
ted
by O
rion
Desi
gn &
Prin
t Ltd
. Tel
: 020
835
1 32
22 E
mai
l: Sa
les@
Orio
n.gb
.com
membership application form
UK Thalassaemia Society, 19 The Broadway, London N14 6PHCharity Reg No. 275107
Your Personal Details
ALL DETAILS AND INFORMATION WILL BE KEPT ON OUR COMPUTERS AND WILL REMAIN IN THE OFFICE AND WILL NOT BE MADE AVAILABLE TO ANYBODY OUTSIDE OF THE UKTS.
If you however do not wish your details kept on our computers please tick this box
OFFICE USE: Date Paid Receipt No. Approval Date
Title (Mr/Mrs/Miss/Ms/Other):
First Name(s):
Surname:
If you are a patient or parent of a patient please complete the section below
Patient’s Name(s):
Hospital where‑treated:
Address:
Date of Birth:
Consultant’s Name:
Consultant’s Telephone:
GP’s Name:
Address:
Telephone:
Transfusion Frequency:
Units received at each transfusion
Blood Type
Type of thalassaemia: (e.g. Major, Intermedia, Haemoglobin H etc)
Sex: Male Female
Address:
Contact Details
Telephone: Home:
Work:
Mobile:
Fax:
Email:
Are you a:
Patient Parent/Relative
Healthcare Professional Association
Other (Please state)
Membership Required (please tick)
ANNUAL (£10.00) LIFE (£100.00) (Please make your cheque payable to U.K.T. Society)
Blood Transfused (please tick)
Whole Washed Frozen Filtered
Chelation (please tick)
Desferal Deferiprone Desferal & Deferiprone
Post Code:
Occupation:
Ethnic Origin:(Optional)