marianne udd the treatment and risk factors of peptic ... · marianne udd the treatment and ......
TRANSCRIPT

Doctoral dissertation
To be presented by permission of the Faculty of Medicine of the University of Kuopio
for public examination in Auditorium L3, Canthia building, University of Kuopio,
on Friday 9th November 2007, at 12 noon
Department of SurgeryUniversity of Kuopio
MARIANNE UDD
The Treatment and Risk Factors ofPeptic Ulcer Bleeding
JOKAKUOPIO 2007
KUOPION YLIOPISTON JULKAISUJA D. LÄÄKETIEDE 418KUOPIO UNIVERSITY PUBLICATIONS D. MEDICAL SCIENCES 418

Distributor : Kuopio University Library P.O. Box 1627 FI-70211 KUOPIO FINLAND Tel. +358 17 163 430 Fax +358 17 163 410 www.uku.fi/kirjasto/julkaisutoiminta/julkmyyn.html
Series Editors: Professor Esko Alhava, M.D., Ph.D. Institute of Clinical Medicine, Department of Surgery Professor Raimo Sulkava, M.D., Ph.D. School of Public Health and Clinical Nutrition Professor Markku Tammi, M.D., Ph.D. Institute of Biomedicine, Department of Anatomy
Author´s address: Department of Surgery Helsinki University Central Hospital FI-00290 HUS Fax +358 9 471 5646 E-mail : [email protected] i
Supervisors: Docent Risto Julkunen, M.D. Department of Internal Medicine Kuopio University Hospital
Professor Antero Palmu Department of Surgery Central Finland Central Hospital Jyväskylä
Docent Pekka Miettinen, M.D. Department of Surgery Kuopio University Hospital
Reviewers: Docent Anna-Liisa Karvonen, M.D. Department of Internal Medicine Tampere University Hospital
Professor Jyrki Mäkelä Department of Surgery Oulu University Hospital
Opponent: Docent Jari Ovaska, M.D. Department of Surgery Turku University Central Hospital
ISBN 978-951-27-0678-5ISBN 978-951-27-0755-3 (PDF)ISSN 1235-0303
KopijyväKuopio 2007Finland

Udd, Marianne. The Treatment and Risk Factors of Peptic Ulcer Bleeding. Kuopio UniversityPublications D. Medical Sciences 418. 2007. 88 p.ISBN 9789512706785ISBN 9789512707553 (PDF)ISSN 12350303
ABSTRACT The incidence of acute upper gastrointestinal bleeding has been 100/100000 inhabitants inWestern countries. Peptic ulcer bleeding (PUB) was the source of bleeding in 50% of thesecases. The incidence of noncomplicated peptic ulcer has decreased while that of PUB hasincreased. The mortality of bleeding patients has not significantly decreased despite newtherapeutic options. Controversial results in few studies concerning the medical treatment ofPUB after endoscopic treatment complicates sound clinical decision making in patient care.Furthermore, the risk profile of these patients and the impact of treatment on H.pylori have beenstudied seldom, especially in Finnish patients. The significance of gastric acid inhibition following successful endoscopic therapy inpreventing rebleeding and reducing mortality in PUB was studied by testing the equivalence of aregular dose (20 mg once a day for 72 hours, n = 73) and a high dose of omeprazole (80 mgbolus + 8 mg/h for 72 hours, n = 69) in a prospective randomised double blind trial. Both doseswere equally effective based on rebleeding rates, need of emergency surgery and mortality. Thefactors associated with rebleeding were shock on admission and duodenal ulcer (DU). In PUB an intragastric pHlevel > 4 is considered necessary to prevent dissolving of theformed fibrin clot. Therefore, intragastric pH monitoring for 72 hours was performed in 7 ofpatients of the regular and 6 of the high dose group. The regular dose of omeprazole raisedboth mean and median 24hour intragastric pH > 4 in patients with PUB. This reduction in theacidity together with endoscopic therapy is probably sufficient to maintain haemostasis. Thehigh dose kept the pH almost constantly > 6. A casecontrol study of PUB patients (n = 94) and controls (n = 94) of age ( 5 years) and sexmatched nonulcer patients attending elective endoscopy was undertaken to analyse riskfactors for PUB. A questionnaire concerning possible risk factors was completed. H.pylori wasdetermined positive if histology and/or urease test were positive. CagA antibodies of IgG classof H.pylori were determined by an immunoblot method. H.pylori infection, the use of ASA, otherNSAIDs with 1 defined daily doses, smoking 20 cigarettes daily and previous DU wereindependent risk factors for PUB. Two of them were present simultaneously in 2/3 of thepatients. However, the combination of risk factors did not increase the risk. Of H.pylori positivesubjects, 97% of the cases and 96% of the controls had CagA strains. ASA, ibuprofen,ketoprofen and smoking had a dosedependent association with PUB. The effect of a 3day treatment of omeprazole on the colonisation of H.pylori in the stomachwas studied in patients with PUB. H.pylori status was assessed by histology and urease test ofgastric biopsies at preentry and after 3 days of therapy in 51 patients receiving the regular doseand in 50 patients receiving the high dose of omeprazole. A marked disappearance of H.pyloriwas found with both regimens, but with the high dose, tests for the diagnosis of H.pylori becamenegative significantly more often than with the regular dose, 60% vs. 27.5%, p = 0.001 (anytest), 67.6% vs. 31.7%, p = 0.003 (histology) and 82.2% vs. 43.6%, p = 0.001 (urease test).Samples to find H.pylori should be taken before any omeprazole treatment, or the presence ofthe bacteria may be overlooked.
National Library of Medicine Classification: QV 69, QV 95, QW 154, WI 141, WI 350, WI 360, WI370Medical subject headings: AntiInflammatory Agents, NonSteroidal; AntiUlcer Agents; Aspirin;DoubleBlind Method; Duodenal Ulcer; Endoscopy, Digestive System; Helicobacter pylori;Mortality; Omeprazole; Peptic Ulcer Hemorrhage/drug therapy; Peptic UlcerHemorrhage/prevention and control; Prospective Studies; Randomized Controlled Trials; Riskfactors; Smoking; Stomach Ulcer/complications; Warfarin


To Jouko, Maria, Annmari and Max


ACKNOWLEDGEMENTS
The present work was carried out in the Department of Surgery, Central FinlandCentral Hospital, Jyväskylä, and in the Department of Surgery and theGastroenterology Unit of the Department of Internal Medicine, Kuopio UniversityHospital, Kuopio in 19942007. I want to express my respect and appreciation to Professor Esko Alhava, M.D.,Ph.D., Head of the Department of Surgery, for the possibility to carry out this study. Iam indebted to him for his lectures in surgery, because they inspired me to start mysurgical career. I am deeply grateful to my supervisors Professor Antero Palmu, M.D, Ph.D., DocentRisto Julkunen, M.D., Ph.D., and Docent Pekka Miettinen, M.D., Ph.D., for theirpatience and belief in me during these many years. I thank Docent Risto Julkunen, M.D., Ph.D., for his unique and invaluable ideas andprofessional guidance. He revised manuscripts precisely and with excellent English. I am especially grateful to Professor Antero Palmu, M.D., Ph.D., my supervisor, forhis encouragement and support during the scientific work and during early years of mysurgical career in Jyväskylä. Docent Pekka Miettinen, M.D., has been an excellent supervisor and a true friend. Hehas patiently helped me with many problems during this study. His wide clinicalexperience has been of inestimable value. I am deeply indebted to Harri Mustonen, D.Sci., for his indispensable help with thestatistical analyses and other problems with the manuscripts. I want to express my appreciation to all my coauthors Docent Markku Heikkinen,M.D., Ph.D., Esko Janatuinen, M.D., Docent Matti V Kairaluoma, M.D., Ph.D., MarjaLohman M.D., Docent Pentti Pasanen, M.D., Ph.D., and Riitta Tarvainen, M.D., Ph.D.This work was possible, because they took part in the laborious study protocol. JariTöyry M.D., Ph.D., and Professor Esko Vanninen, M.D., Ph.D., did an excellent job withintragastric pH monitoring. I want to acknowledge Docent AnnaLiisa Karvonen, M.D., Ph.D., and ProfessorJyrki Mäkelä, M.D., Ph.D., reviewers of this thesis, for their prompt and professionalwork and valuable comments. I extend my sincere gratitude to all the physicians and nurses who participated inrecruiting patients, performing endoscopies and recording the data in the KuopioUniversity Hospital and the Central Finland Central Hospital. Their contribution wasessential in completing the study. I also wish to thank Docent David Laaksonen, M.D.,Ph.D., MPH, for his excellent work in revising the English text of the thesis. My sincere appreciation goes to Professor Eero Kivilaakso for giving me thepossibility to specialise in surgery in the Department of Gastroenterological andGeneral Surgery, Helsinki University Central Hospital. I am fortunate to have had anopportunity to work in his Department.

I owe my warmest thanks to all my friends and colleagues at the Department ofGastroenterological and General Surgery, Helsinki University Central Hospital, for theirconfidence in me. I am particular grateful to Laura RenkonenSinisalo for friendshipand sincere support. I thank Pauli Puolakkainen for his optimism toward my scientificcareer and offering good facilities for writing the thesis. I offer my warm thanks to my mother Tellervo, my father Oskari, my sister Susanneand my brother Eerik for their love, encouragement and belief in me. I thank my cousinAnne for a lifelong friendship. Finally I want to thank my family Jouko, Maria, Annmari and Max for their love andsupport. I thank Jouko for fulfilling the promise of never having a boring life with him. This study was financially supported by grants from the Finnish GastroenterologicalAssociation, the Finnish Medical Foundation (Duodecim) and the FinnishNorwegianMedical Foundation.
Espoo, October 2007
Marianne Udd

ABBREVIATIONS
ASA acetylsalicylic acidASATP ASA as thrombosis prophylaxisASAP ASA as pain medicineCagA cytotoxin associated gene ADDD defined daily doseDU duodenal ulcerGU gastric ulcerH2 blocker histamine2 receptor antagonistH.pylori Helicobacter pyloriIgG immunoglobulin GIV intravenousNBVV nonbleeding visible vesselNSAID nonsteroidal antiinflammatory drugNANSAID nonASANSAIDOGD oesophagogastroduodenoscopyPPI proton pump inhibitorPUB peptic ulcer bleedingSD standard deviation

DEFINITIONS
Change of H.pylori colonisation byhistology: change to negative colonisation 10: (from grade 1 to grade 0), 20: (from grade
2 to grade 0) and 30: (from grade 3 to grade 0) decrease in density 21: (from grade 2 to grade 1), 31: (from grade
3 to grade 1), 32: (from grade 3 to grade 2) no change in density 11: (remains grade 1), 22: (remains grade 2),
33: (remains grade 3) increase in density 12: (from grade 1 to grade 2), 13: (from grade
1 to grade 3)
Defined daily dose the assumed average maintenance dose perday for a drug used for its main indication inadults
Duodenal ulcer bulbar or duodenal ulcer
Gastric ulcer gastric, prepyloric or pyloric ulcers
High dose of omeprazole infusion 80 mg bolus + 8 mg/ h for 72 hours
Longterm mortality > 30 day mortality
Rebleeding rebleeding found in OGD necessitatingendoscopic therapy and/or surgery; orpersistent bleeding (haematemesis, melena,shock) necessitating repeated endoscopictherapy or emergency operation
Regular dose of omeprazoleinfusion
20 mg once a day for 72 hours
Shortterm mortality 30day mortality

LIST OF ORIGINAL PUBLICATIONS
I. Udd M, Miettinen P, Palmu A, Heikkinen M, Janatuinen E, Pasanen P,Tarvainen R, Kairaluoma MV, Lohman M, Mustonen H, Julkunen R.Regulardose versus highdose omeprazole in peptic ulcer bleeding: Aprospective randomized doubleblind study. Scand J Gastroenterol. 2001;36:13328.
II. Udd M, Töyry J, Miettinen P, Vanninen E, Mustonen H, Julkunen R. Theeffect of regular and high doses of omeprazole on the intragastric acidityin patients with bleeding peptic ulcer treated endoscopically: A clinical trialwith continuous intragastric pH monitoring. Eur J Gastroenterol Hepatol.2005; 17:13516.
III. Udd M, Miettinen P, Palmu A, Heikkinen M, Janatuinen E, Pasanen P,Tarvainen R, Mustonen H, Julkunen R. Analysis of risk factors and theircombinations in acute gastroduodenal ulcer bleeding. A casecontrolstudy. Accepted for publication in Scand J Gastroenterol.
IV. Udd M, Miettinen P, Palmu A, Julkunen R. Effect of shortterm treatmentwith regular or high doses of omeprazole on the detection of Helicobacterpylori in bleeding peptic ulcer patients. Scand J Gastroenterol. 2003; 38:58893.


CONTENTS1. INTRODUCTION .................................................................................................... 152. REVIEW OF LITERATURE .................................................................................... 16
2.1. Definition of peptic ulcer................................................................................ 162.2. Historical aspects of PUB .............................................................................. 162.3. Epidemiology of the PUB............................................................................... 16
2.3.1. Incidence of gastrointestinal bleeding ................................................... 162.3.2. Incidence of peptic ulcer and bleeding .................................................. 172.3.3. Incidence of DU and GU bleeding ........................................................... 172.3.4. Recurrence ............................................................................................... 182.3.5. 30day mortality ....................................................................................... 182.3.6. Longterm mortality ................................................................................. 18
2.4. Risk factors of PUB ........................................................................................ 192.4.1. Previous history of peptic ulcer and bleeding ....................................... 192.4.2. Concomitant diseases and age ............................................................... 192.4.3. H.pylori ..................................................................................................... 192.4.3.1. CagA strains of H.pylori ....................................................................... 202.4.4. NSAIDs including ASA ............................................................................ 212.4.4.1. Recent use of NSAIDs .......................................................................... 212.4.4.2. Different NSAIDs ................................................................................... 212.4.4.3. Dosedependence of NSAIDs ............................................................... 222.4.4.4. Deaths and bleeding associated with NSAIDs .................................... 222.4.5. Anticoagulants ......................................................................................... 222.4.6. Corticosteroids ........................................................................................ 232.4.7. Other drugs .............................................................................................. 232.4.8. Smoking.................................................................................................... 242.4.9. Alcohol consumption .............................................................................. 242.4.10. Combination of risk factors................................................................... 252.4.10.1. H.pylori and NSAIDs ........................................................................... 252.4.10.2. Anticoagulants and NSAIDs ............................................................... 252.4.11. Helicobacter pylorinegative nonNSAID peptic ulcer ......................... 25
2.5. Endoscopic and clinical factors associated with PUB ................................ 262.5.1. Forrest classification ............................................................................... 262.5.2. Endoscopic signs of acute or recent haemorrhage predictingrebleeding .......................................................................................................... 262.5.3. Other endoscopic predictors of rebleeding ........................................... 272.5.4. Clinical risk factors for rebleeding ......................................................... 272.5.5. Timing of rebleeding ................................................................................ 272.5.6. Risk of rebleeding and early discharge .................................................. 28
2.6. Treatment ........................................................................................................ 282.6.1. Endoscopic therapy ................................................................................. 282.6.2. Operative treatment ................................................................................. 292.6.3. Angioembolisation................................................................................... 302.6.4. Drug treatment ......................................................................................... 312.6.4.1. Theory .................................................................................................... 312.6.4.2. H2 receptor antagonists ....................................................................... 312.6.4.3. Proton pump inhibitors......................................................................... 322.6.4.3.1. Proton pump inhibitors without endoscopic therapy ...................... 322.6.4.3.2. Proton pump inhibitors compared with endoscopic therapy ......... 32

2.6.4.3.3. Proton pump inhibitors versus placebo following endoscopictherapy ............................................................................................................... 332.6.4.3.4. Proton pump inhibitors versus H2 blockers following endoscopictherapy ............................................................................................................... 332.6.4.3.5. Proton pump inhibitors and endoscopic therapy ............................ 342.6.4.4. Somatostatin, tranexamic acid and sucralfate.................................... 36
2.7. The effect of drug treatment on intragastric pH ........................................... 362.7.1. Intragastric pH in healthy volunteers ..................................................... 362.7.2. Intragastric pH in peptic ulcer bleeding ................................................. 372.7.3. The effect of H.pylori on intragastric pH ................................................ 382.7.4. CYP2C19 genotype and intragastric pH ................................................. 38
2.8. Omeprazole and H.pylori ............................................................................... 382.8.1. Effect of omeprazole on H.pylori ............................................................ 382.8.2. Detection of H.pylori ................................................................................ 392.8.3. PUB and test reliability for H.pylori ........................................................ 392.8.4. Recurrent bleeding after eradication of H.pylori ................................... 39
2.9. Clinical practice today and future aspects ................................................... 403. AIMS OF THE PRESENT STUDY .......................................................................... 414. PATIENTS.............................................................................................................. 425. METHODS.............................................................................................................. 466. RESULTS............................................................................................................... 507. DISCUSSION ......................................................................................................... 578. SUMMARY ............................................................................................................. 619. CONCLUSIONS ..................................................................................................... 6310. REFERENCES ..................................................................................................... 64ORIGINAL PUBLICATIONS (IIV) .............................................................................. 85

15
1. INTRODUCTION
The incidence of upper gastrointestinal bleeding has been 100/100000 habitants peryear in Western world (Rockall et al. 1995). Of these patients 40 57% have beenreported to have a peptic ulcer (Soplepmann et al. 1997a; van Leerdam et al. 2003). Ithas been estimated that altogether 10 20% of all peptic ulcers bleed. Especially in theelderly, this bleeding event may be the first sign of the ulcer disease (Imhof et al. 1997;Kemppainen et al. 1997). Although the majority of bleeding episodes cease spontaneously, still 20% requireintervention (Choudari et al. 1994; Williams et al. 1993). Before the era of endoscopictherapy, patients with major bleeding events underwent emergency surgery (Wara etal. 1983). Most of the other patients had an early elective operation. Today the diagnosis of PUB is made by endoscopy. Signs of acute or recent bleedingfound on diagnostic endoscopy can predict the risk of rebleeding. Some form ofendoscopic therapy is usually indicated when these high risk signs exist. Afterendoscopic therapy there is still a 20% risk of rebleeding (Thomopoulos et al. 2001;Villanueva et al. 1993). Medical treatment is considered necessary to reduce the risk of rebleeding. PPIsdecrease gastric acid secretion and heal ulcers (Graham et al. 1990). These drugshave also been used in the acute bleeding phase to increase intragastric pH andthereby control bleeding. Although high doses of PPIs have been found superior toplacebo in this respect, the role of regular doses has remained obscure. In casecontrol studies NSAIDs (Imhof et al. 1997; Labenz et al. 1999; Wu et al.1999), smoking (Stack et al. 2002; Tzourmakliotis et al. 2004; Weil et al. 2000) andH.pylori (Labenz et al. 1999; Stack et al. 2002; Wu et al. 1999) have been reported asindividual single risk factors for PUB, but their concurrence in patients has seldom beenstudied. Furthermore, the role of multiple risk factors in the same patient has gainedlittle attention in various investigations. Helicobacter pylori is regarded as one of themost important causes of peptic ulcer. Its early detection is fundamental for thepurpose of eradication to prevent ulcer recurrence. However, there are only scant dataof the early effect of PPI treatment on the detection of H.pylori. The purpose of the present work was to assess the risk profile of PUB patients and tostudy the effect of modern medical treatment after endoscopic therapy on the clinicaloutcome of PUB, on the intragastric acidity and on the detection of H.pylori in PUB in aprospective randomised double blind setting.
16
2. REVIEW OF LITERATURE
2.1. Definition of peptic ulcer
Peptic ulcer is a chronic defect in the gastrointestinal mucosa extending throughmuscularis mucosae (Oi and Sakurai 1959; Oi et al. 1959). The defect persists as afunction of the acid peptic activity in gastric juice. Major bleeding occurs when theulcerative process reaches underlying submucosal vessels.
2.2. Historical aspects of PUB
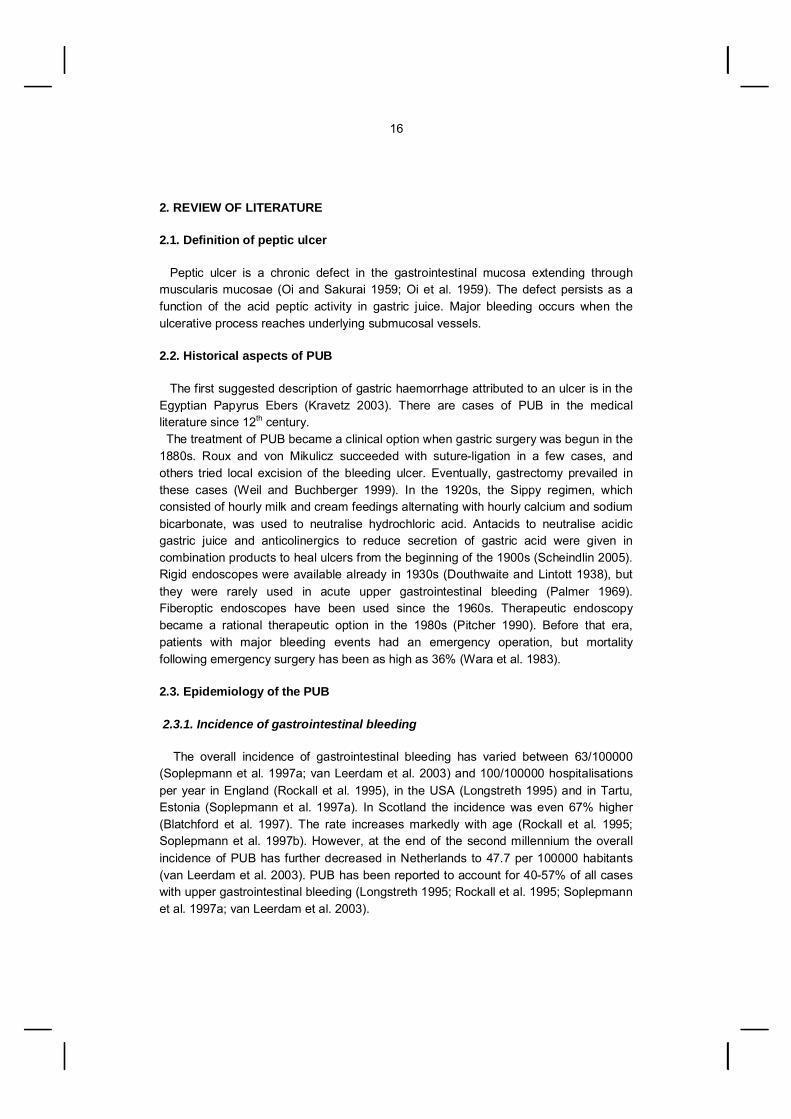
The first suggested description of gastric haemorrhage attributed to an ulcer is in theEgyptian Papyrus Ebers (Kravetz 2003). There are cases of PUB in the medicalliterature since 12th century. The treatment of PUB became a clinical option when gastric surgery was begun in the1880s. Roux and von Mikulicz succeeded with sutureligation in a few cases, andothers tried local excision of the bleeding ulcer. Eventually, gastrectomy prevailed inthese cases (Weil and Buchberger 1999). In the 1920s, the Sippy regimen, whichconsisted of hourly milk and cream feedings alternating with hourly calcium and sodiumbicarbonate, was used to neutralise hydrochloric acid. Antacids to neutralise acidicgastric juice and anticolinergics to reduce secretion of gastric acid were given incombination products to heal ulcers from the beginning of the 1900s (Scheindlin 2005).Rigid endoscopes were available already in 1930s (Douthwaite and Lintott 1938), butthey were rarely used in acute upper gastrointestinal bleeding (Palmer 1969).Fiberoptic endoscopes have been used since the 1960s. Therapeutic endoscopybecame a rational therapeutic option in the 1980s (Pitcher 1990). Before that era,patients with major bleeding events had an emergency operation, but mortalityfollowing emergency surgery has been as high as 36% (Wara et al. 1983).
2.3. Epidemiology of the PUB
2.3.1. Incidence of gastrointestinal bleeding
The overall incidence of gastrointestinal bleeding has varied between 63/100000(Soplepmann et al. 1997a; van Leerdam et al. 2003) and 100/100000 hospitalisationsper year in England (Rockall et al. 1995), in the USA (Longstreth 1995) and in Tartu,Estonia (Soplepmann et al. 1997a). In Scotland the incidence was even 67% higher(Blatchford et al. 1997). The rate increases markedly with age (Rockall et al. 1995;Soplepmann et al. 1997b). However, at the end of the second millennium the overallincidence of PUB has further decreased in Netherlands to 47.7 per 100000 habitants(van Leerdam et al. 2003). PUB has been reported to account for 4057% of all caseswith upper gastrointestinal bleeding (Longstreth 1995; Rockall et al. 1995; Soplepmannet al. 1997a; van Leerdam et al. 2003).

17
2.3.2. Incidence of peptic ulcer and bleeding
The clinical presentation and frequency of peptic ulcer has varied during previousdecades. The incidence of uncomplicated peptic ulcer in terms of hospitalisations hasdecreased, like in the United States between 1970 and 1985 (Kurata and Corboy1988). In the Netherlands the incidence was halved between 1992 and 2003 (Post etal. 2006). In Finland elective operations for peptic ulcer disease decreased by 89%between years 1972 and 1999 (Paimela et al. 2002). In contradiction to the overall decline in the incidence of peptic ulcer complicationslike bleeding have increased in the United States from 1970 1985 (Kurata and Corboy1988), in Denmark from 1981 1993 (Andersen et al. 1998) and in England from 1989 1999 (Higham et al. 2002). Between the years 1974 – 1986 in Massachusetts therewas a decline in elective peptic ulcer operations, but the operations performed due toperforation or bleeding remained constant (Welch et al. 1986). The incidence of emergency operations increased by 44 % (from 5.2 to 7.5 /100000inhabitants) in Finland during the period 1972 1999 (Paimela et al. 2002). The numberof hospitalisations for PUB increased at least twofold between 1979 and 1984 (Tilvis etal. 1987). More recently in Denmark the incidence of uncomplicated and perforated pepticulcers decreased further, in DU from 55 to 37/100000 and in GU from 56 to 40/100000,but that of PUB remained the same, 55/100000 inhabitants (Lassen et al. 2006). On the other hand, the annual incidence of surgery for PUB remained stable during19771988 in Northern Finland (Mäkelä et al. 1992). In Düsseldorf, Germany, theincidence of PUB has been stable between the years 1990 and 2000, at 50 per 100000inhabitants per year (Ohmann et al. 2005).
2.3.3. Incidence of DU and GU bleeding
In the Amsterdam area, the incidence of GU (10/100000 inhabitants per year) andDU bleeding (13/100000 inhabitants per year) has remained the same between years1993/1994 and 2000 (van Leerdam et al. 2003). In Tartu, Estonia, the incidence hasbeen much higher, 57/100000 adults per year (Soplepmann et al. 1997b). It was 82.7/100000 per year for men and 36.1 for women while the male to female ratio for GU was1.6:1 and for DU 4.4:1. In Denmark in 19812003 the hospitalisation rates of PUB in women increased(standardised rate ratio 1.22 for gastric ulcer bleeding and 1.7 for duodenal ulcerbleeding) but that of men remained almost the same (Andersen et al. 1998).

18
2.3.4. Recurrence
After the first episode of PUB, further episodes of bleeding can occur. Recurrencerate of 6% has been found in 3 months followup (Hasselgren et al. 1998), 9% afterfollowup of 36 months (median) (Kubba et al. 1997) and 18% after 8 years (Fischer etal. 1994).
2.3.5. 30day mortality
Despite improvements in therapeutic methods, intensive monitoring and new acidsuppressing medication, the mortality of PUB has remained stable during last decadesin Western countries. The mortality of PUB in general has been 15% in NorthernFinland between 1977 and 1988 (Mäkelä et al. 1992), 8% in 1993 and 1995 (Mäkelä etal. 1996) and 5.5% in Gothenburg in 1989 and 1993 (Hasselgren et al. 1998) whereasthat of complicated peptic ulcer was 11% in Denmark 1993 2000 (Lassen et al. 2006).The combined mortality of peptic ulcer perforation and bleeding increased from 4.2 to7.3/100000 inhabitants per year in Finland 1972 1999 (Paimela et al. 2002). Age and Forrest class (Rockall et al. 1996a; Chow et al. 1998; Hasselgren et al.1998), concomitant diseases, rate of rebleeding (Rockall et al. 1996a) and need foremergency surgery (Chow et al. 1998) have influenced mortality. In another study thenumber of concomitant diseases but not age increased mortality among PUB patients(Mueller et al. 1994). Treating these patients remains a clinical challenge, since many are elderly, withconcurrent illnesses and multiple medications. In these circumstances not only theendoscopic signs of acute or recent bleeding, but also background factors predict theoutcome.
2.3.6. Longterm mortality
After an episode of PUB, the risk of death is estimated to be 2fold compared with thegeneral population. This risk is less than 2fold in the elderly but 7fold in the middleaged, suggesting that PUB could be a marker of a general deterioration in health(Ruigomez et al. 2000). Worsened longterm survival after an episode of PUB has been found in Scottishpopulation (Kubba et al. 1997) and in Gothenburg (Hasselgren et al. 1998). In elderlyPUB patients the 6 year survival estimate was almost 20% worse than expectedaccording to national death rates despite prophylaxis with H2 blockers. Decreasedsurvival was associated with other concomitant diseases (cancer, respiratory,cardiovascular) rather than recurrence of peptic ulcer complications (Hudson et al.1995a).

19
2.4. Risk factors of PUB
2.4.1. Previous history of peptic ulcer and bleeding
Previous peptic ulcer increases the risk of a new episode of ulcer and bleeding. Therisk has been estimated to be 4 to 6 fold (Stack et al. 2002; Weil et al. 2000). Typically26% to 40% of PUB patients have had peptic ulcer or bleeding earlier (Henriksson etal. 1998; Leivonen and Kivilaakso 1991; Savage et al. 1993; Stack et al. 2002). Thisrisk scenario may change in the future, since in years 19992000 PUB patients wereless likely to have a history of ulcer (25% versus 59%) compared with PUB patientstreated 10 years earlier (Ohmann et al. 2005). Previous upper gastrointestinal bleedingalso increases the risk of PUB (Gabriel et al. 1991). However, there are also studiesindicating that previous ulcer treatment has been a protective factor for new bleedingepisode (Imhof et al. 1997).
2.4.2. Concomitant diseases and age
In a metaanalysis (Gabriel et al. 1991) and an overview of epidemiologic studies(HernandezDiaz and Rodriguez 2000), the risk of PUB increases with age. Lungdiseases increased the risk of PUB according to a casecontrol study (Imhof et al.1997).
2.4.3. H.pylori
H.pylori is a spiralshaped gramnegative bacterium colonizing the gastric mucosathat was first discovered by Marshall and Warren (Marshall and Warren 1984). H.pyloricauses chronic gastritis (Goodwin et al. 1986, Sipponen et al. 1994) and increases therisk of peptic ulcer (Voutilainen et al. 2001), especially duodenal ulcer (Graham 1989,Blaser 1998). H.pylori is also considered a risk factor for gastric adenocarcinoma(Parsonnet et al. 1991, Kokkola et al. 2005, Knekt et al. 2006), and it is associated withgastric MALT lymphoma (Wotherspoon et al. 1991). Although half of the population ofthe world is infected with H.pylori, only 20 % of H. pyloripositive subjects developedulcer disease during longterm followup (Forbes et al. 1994). The lifetime risk for ulcerdisease in H. pyloripositive subjects is nonethless 3 times higher than in H. pylorinegative subjects (Nomura et al. 1994). Duodenal gastric metaplasia is associated with high acid output and it is suggested tobe prerequisite for duodenal ulcer, because in the duodenum, H.pylori is found only inareas with gastric metaplasia (Graham 1991). Widespread duodenal gastric metaplasiahas been associated with H.pyloripositive duodenal ulcer disease (Veijola et al. 2006).
Due to a birth cohort effect, the H.pylori seroprevalence has fallen over the lastdecades in developed countries (Banatvala et al. 1993, Sipponen et al. 1994, Kosunen

20
et al 1997). In developing countries, most people are infected with the bacteria(Graham et al. 1991). In PUB the prevalence of H.pylori infection has been lower than in noncomplicatedpeptic ulcer disease (Stack et al. 2002; Wu et al. 1999). This may be due to ongoingPPI medication and inaccurate testing. According to several casecontrol studiesH.pylori has been a risk factor for PUB, with 2 to 3fold risk (Labenz et al. 1999; Stacket al. 2002; Wu et al. 1999). In one casecontrol study H.pylori was inverselyassociated with gastric ulcer bleeding (Pilotto et al. 1997).
2.4.3.1. CagA strains of H.pylori
Virulence factors are related to the ability of a microbe to induce disease. Truevirulence factors should have a disease association, like increased mucosalinflammation. Cytotoxinassociated gene A has been studied vigorously, as a potential virulencefactor. CagA in H.pylori positive subjects has been associated with peptic ulcer diseasein Western Europe (Covacci et al. 1993) and the United States (Cover et al. 1995;Nomura et al. 2002). Cag A has also been associated with PUB (Henriksson et al.1998; Santolaria et al. 1999; Stack et al. 2002; Tzourmakliotis et al. 2004). In a few casecontrol (Hsu et al. 2000; Lanas et al. 2002) and other studies (Grahamet al. 1996a) there was no association between CagA and peptic ulcer disease, and theprevalence of CagA was low in both peptic ulcer, PUB and control patients. On theother hand, in North America (Evans et al. 1998; Go and Graham 1996), Sweden(Hamlet et al. 1999), Estonia (Andreson et al. 2002) and among Asian populations(Park et al. 1998) the prevalence of CagA has been similarly high in patients withpeptic ulcer and controls. Therefore CagA may not serve as an appropriate marker ofmore virulent H.pylori strains. The results from studies comparing the prevalence of antibodies against CagA inpatients with and without peptic ulcer are inconsistent. CagA itself may not beresponsible for the inflammatory process. It is unclear if it has any specific role in pepticulcer disease. Neither CagA nor VacA seropositivities are better predictors of increasedpeptic ulcer risk than antibodies against H. pylori. More than 90% of strains in EastAsia are CagA and VacA positive. These factors may not be sufficient to cause moresevere gastroduodenal disease (Gonzalez et al. 2003). Cytotoxin associated genepathogenicity island PAI, the duodenal ulcerpromoting gene, and the blood groupantigen binding adhesion are possible virulence factors (Lu et al. 2005).

21
2.4.4. NSAIDs including ASA
The ability of ASA to damage gastric mucosa was first described in 1938 (Douthwaiteand Lintott 1938). NSAIDs cause damage in the gastroduodenal mucosa by severalmechanisms. They are topically irritable and suppress mucosal prostaglandin synthesiswhich regulates mucosal defence mechanisms (Wallace 2000). Cyclooxygenase enzyme (COX) is responsible for prostaglandin synthesis byconverting arachidonic acid to prostaglandins and thromboxane. Gastrointestinalprostaglandins protect against injury by stimulating mucosal bicarbonate and mucussecretion and by increasing mucosal blood flow. COX exists in two isoforms, COX1and COX2. The former predominates in the stomach and the whole gastrointestinaltract. With COX2 inhibitor NSAIDs, the incidences of gastroduodenal lesions havebeen lower than with the traditional NSAIDs (Bombardier et al. 2000). However, seriouscardiovascular side effects restrict the use of COX2 inhibitors to rare patients (Grosseret al. 2006; HernandezDiaz et al. 2006). On the other hand, they are not without therisk of upper gastrointestinal complications (Garcia Rodriguez and Barreales Tolosa2007, HelinSalmivaara et al. 1997) especially when used in combination with aspirin(Garcia Rodriguez and Barreales Tolosa 2007). In Finland during year 2000, the total NSAID consumption was 61.2 DDD/1000inhabitants per day. The 1year prevalence of NSAID use was 17.7% in a sample of500 000 persons. Paracetamol is less often used and the consumption of NSAIDs ishigher in Finland than in other Nordic countries (HelinSalmivaara et al. 2003). The use of NSAIDs including ASA (Weil et al. 1995) have been reported to beimportant risk factors for PUB, with a 3 to 8 fold higher risk according to metaanalysesof cohort (Gabriel et al. 1991) and casecontrol studies (Imhof et al. 1997; Labenz et al.1999; Wu et al. 1999). There has been a 4fold risk of PUB with NSAIDs (Cullen et al.1997) and NANSAIDs among the elderly (Griffin et al. 1991).
2.4.4.1. Recent use of NSAIDs
The bleeding event may often occur soon after the initiation of NSAIDs and mostlyduring the first month of the therapy (Somerville et al. 1986). The risk of PUB has beenestimated to be 11fold within the first week of use (Lewis et al. 2002) and 7 to 8 foldwithin the first month in casecontrol studies (Griffin et al. 1991; Lanas et al. 2006) anda metaanalysis (Gabriel et al. 1991).
2.4.4.2. Different NSAIDs
The risk of PUB associated with different traditional NSAID drug regimens varies.According to a metaanalysis and casecontrol studies the risk of upper gastrointestinalbleeding or PUB has been the highest with ketoprofen, from 6 to 30fold (HernandezDiaz and Rodriguez 2000; Lanas et al. 2006; Lewis et al. 2002) and with piroxicam

22
(HernandezDiaz and Rodriguez 2000; Lanas et al. 2006). With ibuprofen anddiclofenac the risk has been the lowest (HernandezDiaz and Rodriguez 2000; Lewis etal. 2002). Ketoprofen 50 mg caused significantly more gastroduodenal injury than ibuprofen400 mg, whereas ketoprofen 12.5 mg was equal to ibuprofen 400 mg (Donnelly et al.2000). The recommended single dose of ketoprofen is 50–100 mg, and that ofibuprofen 200600 mg.
2.4.4.3. Dosedependence of NSAIDs
The risk of PUB is dependent on the dose of NSAIDs according to metaanalyses(Gabriel et al. 1991), casecontrol (Lewis et al. 2002; Stack et al. 2002; Weil et al.1995) and prospective cohort studies (HernandezDiaz and Rodriguez 2000). Similarly,the risk of upper gastrointestinal bleeding and perforation increases with increasing thedose (Gutthann et al. 1997). In the recent study of Stack et al. (2002) half of the casesconsumed some NSAID which may explain the high odds ratios: OR 10.6 for doses 1defined daily doses (DDD) and OR 20.6 for doses 1 DDD. Furthermore, the use ofmultiple NSAIDs has been claimed to increase the risk further compared with singleNSAID use (Gutthann et al. 1997; Weil et al. 1995).
2.4.4.4. Deaths and bleeding associated with NSAIDs
In England, over 40% of the 8528 episodes of ulcer bleeding in patients over 60years and over 40% of the estimated 981 deaths per year are related to NSAID use(Langman 2001). The frequency of episodes of bleeding and deaths would beexpected to be reduced by 70%, if NSAID was converted to the regimen with lowestrisk. If the dose of prophylactic ASA was lowest (75 mg) the frequency of bleedingepisodes and deaths would be expected to reduce by 30%. It has been estimated thaton average 1 in 1200 patients taking NSAIDs for at least 2 months will die fromgastroduodenal complications (Tramer et al. 2000). On the other hand, in womencurrent use of low dose ASA was associated with significantly lower risk of allcausemortality when compared with women who never used ASA regularly (Chan et al.2007a).
2.4.5. Anticoagulants
Warfarin is the most used anticoagulant and acts as a vitamin K antagonist. Warfarinand other anticoagulating drugs delay the coagulation cascade. In placebocontrolledtrials of warfarin there has been no risk of bleeding, but these studies usually excludepatients with history of peptic ulcer (Mant et al. 2003). In a Finnish study 11.3% of PUBpatients but only 1.4% of hospital controls were on anticoagulants (Leivonen andKivilaakso 1991).
23
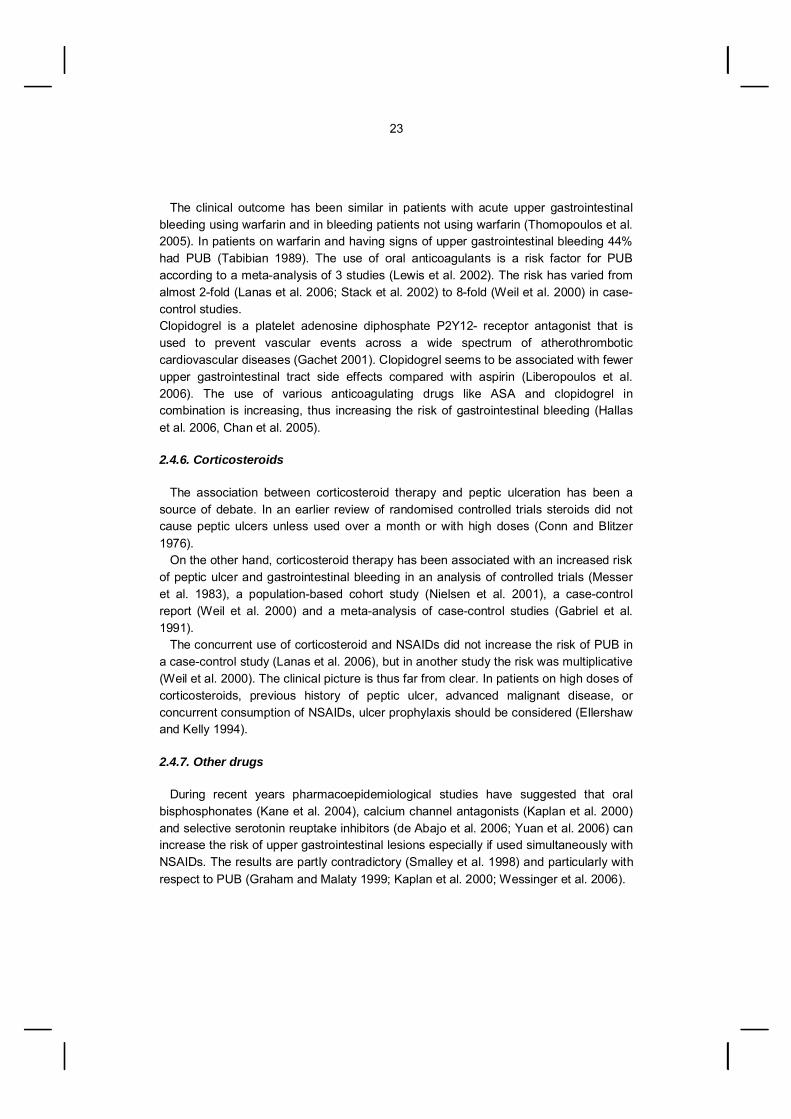
The clinical outcome has been similar in patients with acute upper gastrointestinalbleeding using warfarin and in bleeding patients not using warfarin (Thomopoulos et al.2005). In patients on warfarin and having signs of upper gastrointestinal bleeding 44%had PUB (Tabibian 1989). The use of oral anticoagulants is a risk factor for PUBaccording to a metaanalysis of 3 studies (Lewis et al. 2002). The risk has varied fromalmost 2fold (Lanas et al. 2006; Stack et al. 2002) to 8fold (Weil et al. 2000) in casecontrol studies.Clopidogrel is a platelet adenosine diphosphate P2Y12 receptor antagonist that isused to prevent vascular events across a wide spectrum of atherothromboticcardiovascular diseases (Gachet 2001). Clopidogrel seems to be associated with fewerupper gastrointestinal tract side effects compared with aspirin (Liberopoulos et al.2006). The use of various anticoagulating drugs like ASA and clopidogrel incombination is increasing, thus increasing the risk of gastrointestinal bleeding (Hallaset al. 2006, Chan et al. 2005).
2.4.6. Corticosteroids
The association between corticosteroid therapy and peptic ulceration has been asource of debate. In an earlier review of randomised controlled trials steroids did notcause peptic ulcers unless used over a month or with high doses (Conn and Blitzer1976). On the other hand, corticosteroid therapy has been associated with an increased riskof peptic ulcer and gastrointestinal bleeding in an analysis of controlled trials (Messeret al. 1983), a populationbased cohort study (Nielsen et al. 2001), a casecontrolreport (Weil et al. 2000) and a metaanalysis of casecontrol studies (Gabriel et al.1991). The concurrent use of corticosteroid and NSAIDs did not increase the risk of PUB ina casecontrol study (Lanas et al. 2006), but in another study the risk was multiplicative(Weil et al. 2000). The clinical picture is thus far from clear. In patients on high doses ofcorticosteroids, previous history of peptic ulcer, advanced malignant disease, orconcurrent consumption of NSAIDs, ulcer prophylaxis should be considered (Ellershawand Kelly 1994).
2.4.7. Other drugs
During recent years pharmacoepidemiological studies have suggested that oralbisphosphonates (Kane et al. 2004), calcium channel antagonists (Kaplan et al. 2000)and selective serotonin reuptake inhibitors (de Abajo et al. 2006; Yuan et al. 2006) canincrease the risk of upper gastrointestinal lesions especially if used simultaneously withNSAIDs. The results are partly contradictory (Smalley et al. 1998) and particularly withrespect to PUB (Graham and Malaty 1999; Kaplan et al. 2000; Wessinger et al. 2006).

24
2.4.8. Smoking
Smoking causes ulcers by stimulating basal acid output and increasingduodenogastric reflux. It increases also production of platelet activation factor andendothelin, which are ulcerogens. Smoking decreases prostaglandin generation ingastric mucosa, reduces angiogenesis and blood flow and inhibits mucosal cellproliferation (Ma et al. 1998; Maity et al. 2003). Smoking has been an independent risk factor for peptic ulcer disease in aprospective cohort study in a Danish population (Rosenstock et al. 2003). Furthermore,smoking is a risk factor for PUB in some studies (Aalykke et al. 1999; Henriksson et al.1998; Savage et al. 1993; Stack et al. 2002; Tzourmakliotis et al. 2004; Weil et al.2000) but not all (Gisbert et al. 2001a; Ng et al. 2000; Schubert et al. 1993). However,the risk of PUB has been found not (Aalykke et al. 1999) or only slightly increasedamong NSAID users who smoke compared with nonsmokers (Tzourmakliotis et al.2004; Weil et al. 2000). On the other hand, smoking doubles the risk of PUB in H.pyloripositive patients, and they act synergistically (Stack et al. 2002). There was a dosedependence of smoking in the risk of upper gastrointestinal bleeding according to ametaanalysis (Lewis et al. 2002). In another study, smoking was not a risk factor forPUB, but was for perforated peptic ulcer (Andersen et al. 2000). At present, there areno data concerning risk of PUB and smoking in a Finnish population.
2.4.9. Alcohol consumption
Ethanol causes severe epithelial damage and necrosis of deeper layers of gastricmucosa. Further microvascular damage leads to increased permeability andintramucosal haemorrhage (Tarnawski et al. 1987). Gastric emptying is also disturbedby ethanol (Jian et al. 1986). In Finland alcohol consumption has been significantly more common among PUBpatients than in controls (Leivonen and Kivilaakso 1991). The regular use of alcohol isa risk factor for PUB (Labenz et al.1999), also in patients on lowdose of ASA (Lanas etal. 2002). Alcohol intake has had a dosedependent risk for PUB in New Zealand(Savage et al. 1993) as well as in Denmark (Andersen et al. 2000). However, in several studies alcohol consumption did not differ among cases andcontrols (Schubert et al. 1993; Stack et al. 2002; Tzourmakliotis et al. 2004). Becausemany PUB patients are infected with H.pylori, alcohol and H.pylori may have someinteraction. Helicobacter lipopolysaccharides induce formation of nitric oxide synthase(iNOS), cyclooxygenase (COX2) and heat shock protein 70 (HSP 70) known toincrease resistance to damage caused by ethanol in vivo. Indeed, H.pylori increasesresistance of the gastric mucosa to injury caused by ethanol in vitro (Brzozowski et al.2003).
25
2.4.10. Combination of risk factors
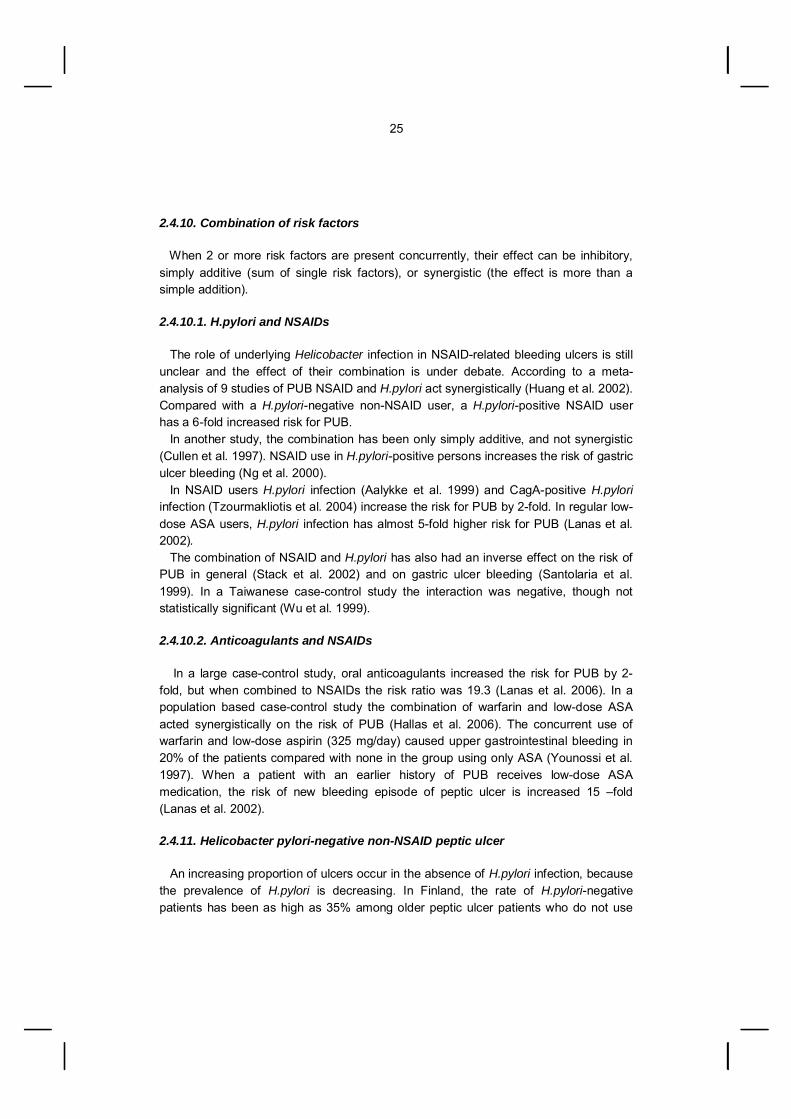
When 2 or more risk factors are present concurrently, their effect can be inhibitory,simply additive (sum of single risk factors), or synergistic (the effect is more than asimple addition).
2.4.10.1. H.pylori and NSAIDs
The role of underlying Helicobacter infection in NSAIDrelated bleeding ulcers is stillunclear and the effect of their combination is under debate. According to a metaanalysis of 9 studies of PUB NSAID and H.pylori act synergistically (Huang et al. 2002).Compared with a H.pylorinegative nonNSAID user, a H.pyloripositive NSAID userhas a 6fold increased risk for PUB. In another study, the combination has been only simply additive, and not synergistic(Cullen et al. 1997). NSAID use in H.pyloripositive persons increases the risk of gastriculcer bleeding (Ng et al. 2000). In NSAID users H.pylori infection (Aalykke et al. 1999) and CagApositive H.pyloriinfection (Tzourmakliotis et al. 2004) increase the risk for PUB by 2fold. In regular lowdose ASA users, H.pylori infection has almost 5fold higher risk for PUB (Lanas et al.2002). The combination of NSAID and H.pylori has also had an inverse effect on the risk ofPUB in general (Stack et al. 2002) and on gastric ulcer bleeding (Santolaria et al.1999). In a Taiwanese casecontrol study the interaction was negative, though notstatistically significant (Wu et al. 1999).
2.4.10.2. Anticoagulants and NSAIDs
In a large casecontrol study, oral anticoagulants increased the risk for PUB by 2fold, but when combined to NSAIDs the risk ratio was 19.3 (Lanas et al. 2006). In apopulation based casecontrol study the combination of warfarin and lowdose ASAacted synergistically on the risk of PUB (Hallas et al. 2006). The concurrent use ofwarfarin and lowdose aspirin (325 mg/day) caused upper gastrointestinal bleeding in20% of the patients compared with none in the group using only ASA (Younossi et al.1997). When a patient with an earlier history of PUB receives lowdose ASAmedication, the risk of new bleeding episode of peptic ulcer is increased 15 –fold(Lanas et al. 2002).
2.4.11. Helicobacter pylorinegative nonNSAID peptic ulcer
An increasing proportion of ulcers occur in the absence of H.pylori infection, becausethe prevalence of H.pylori is decreasing. In Finland, the rate of H.pylorinegativepatients has been as high as 35% among older peptic ulcer patients who do not use

26
NSAIDs (Kemppainen et al. 1997). A prevalence of 20% of nonH.pylori nonNSAIDulcers has been found in Poland in 2000 (Konturek et al. 2003) and in Sweden (Aro etal. 2006). In patients with H.pylorinegative DU some other obvious reason may be present,such as NSAID use, Crohn’s disease, or ZollingerEllison syndrome. H.pylorinegativeDU may also be associated with hypergastrinaemia, increased acid secretion and rapidgastric emptying (McColl et al. 1993). Also increased parietal cell mass, reducedmucosal blood flow, or Cytomegalovirus infection might be explanations for H.pylorinegative ulcers (Peura 2000). H.pylori negative ulcer may also be explained by recentpeptic ulcer medication, antibiotics or inaccurate test.
2.5. Endoscopic and clinical factors associated with PUB
2.5.1. Forrest classification
Signs of haemorrhage seen at endoscopy include localised active bleeding (arterialspurting or oozing) and signs of recent bleeding, like an adherent clot, a nonbleedingvisible vessel (NBVV), or a flat black base. These signs are used in the modifiedForrest classification: Ia = spurting bleeding, Ib = oozing bleeding, IIa = visible vessel,IIb = clot, IIc = black base covering ulcer, III= clean ulcer base (Forrest et al. 1974).The Forrest classification characterises the bleeding point and can predict therebleeding risk in PUB. Major peptic ulcer bleeding is typically from a small (mean external diameter 0.7mm)single submucosal artery just below the ulcer base, which can be seen as a visiblevessel (Swain et al. 1986). It is defined as a protruding red, blue, or white mount, apulsatile pseudoaneurysm or a yellowwhite rod sticking out of the ulcer base (Swain etal. 1986; Wara 1985). Sentinel clot covers a side hole of the bleeding artery runningbeneath ulcer base and the vessel is actually invisible (Johnston 1984). The genericterm protuberance includes both visible vessel and sentinel clot (Consensus statementon therapeutic endoscopy and bleeding ulcers 1990). The prevalence of these signs ofbleeding among PUB patients are: active bleeding 18%, NBVV 17%, adherent clot17%, flat spot 20%, clean base 42% (Laine and Peterson 1994).
2.5.2. Endoscopic signs of acute or recent haemorrhage predicting rebleeding
Endoscopic signs of acute or recent haemorrhage are important predictors ofrebleeding and need of endoscopic therapy or surgery (Branicki et al. 1992; Jaramilloet al. 1994; Mueller et al. 1994). When endoscopy is performed within 24 hours afterthe onset of bleeding, NBVV can be found in 48% of patients, and other signs of acuteor recent haemorrhage in 18% of patients, whereas 34% have no signs (Storey et al.1981).

27
When no endoscopic treatment or surgery is undertaken, the rebleeding riskassociated with each sign are: active arterial bleeding ( Forrest Ia and Ib) 55%, NBVV(Forrest IIa) 43%, adherent clot (Forrest IIb) 22%, flat spot/black base (Forrest IIc) andclean base (Forrest III) 5% (Laine and Peterson 1994). However, there has been aconsiderable interobserver disagreement in the interpretation of the presence ofendoscopic stigmata of recent haemorrhage (Laine et al. 1994). Endoscopic Dopplerultrasound has shown that not all NBVV have submucosal arterial flow (Fullarton andMurray 1990) and that even pigmented spots may have it. Hypovolaemic shockincreases the rebleeding rate of NBVV from 25 to 40%, and that of an adherent clotfrom 17% to 50% (Hsu et al. 1994).
2.5.3. Other endoscopic predictors of rebleeding
The rebleeding risk is associated with ulcers > 1cm in diameter (Branicki et al. 1992),and more so with giant duodenal ulcers ( 2 cm) (Brullet et al. 1996a; Brullet et al.1996b; Collen et al. 1994). An ulcer location high on the lesser curvature (Brullet et al.1996a) or posterior duodenal wall (Brullet et al. 1996b) and possible pulsation are alsorisk factors.
2.5.4. Clinical risk factors for rebleeding
Haematemesis (Jaramillo et al. 1994), a low haemoglobin level (Choudari et al. 1994)and shock on admission are risks for rebleeding (Branicki et al. 1992; Brullet et al.1996b; Choudari et al. 1994; Jaramillo et al. 1994; Mueller et al. 1994). Regardingother clinical risk factors, the situation is not clear. Old age has been a risk factor insome studies (Chow et al. 1998; Inadomi et al. 1995; Jaramillo et al. 1994) while inothers it did not increase the rebleeding risk or mortality (Choudari et al. 1994; Muelleret al. 1994). A similar lack of clarity prevails with alcoholism and concomitant diseases.They have been associated with the risk for rebleeding in one study (Inadomi et al.1995), but in another study concomitant diseases did not increase the risk (Choudari etal. 1994). Even the reports of recent use of NSAID or ASA are inconsistent, becausethey may (Godil et al. 2000) or may not (Choudari et al. 1994; Inadomi et al. 1995) beassociated with rebleeding.
2.5.5. Timing of rebleeding
Rebleeding occurs mostly within 72 hours after the initial incidence (Lin et al. 1996;O'Brien et al. 1986). In cases with NBVV 97% of the occasions took place in 72 hours(Lin et al. 1994). The rest of such episodes in general occur within one week (Hsu etal. 1994; Inadomi et al. 1995; Lin et al. 1994).

28
2.5.6. Risk of rebleeding and early discharge
Different scoring systems to identify those at increased risk of rebleeding may beused in patient management and decision making for discharge. The idea of Rockall’srisk score (age, presence of shock, comorbidity, diagnosis, endoscopic stigmata)(Rockall et al. 1996b) and other scoring systems (Gisbert et al. 2006; Guglielmi et al.2002; Saeed et al. 1995) are to identify those with the risk. Patients at a low risk canaccordingly be safely discharged after endoscopy. These scoring systems have been criticised, because they are not practical and aretoo complex to use in a reallife setting. The Rockall score may predict death, butperforms poorly for endpoints of rebleeding and surgical procedures (Enns et al. 2006). By Saeed et al. (1993) the risk associated with endoscopic signs of bleeding can beeliminated by endotherapy. Therefore clinical factors become primary determinants ofrebleeding. On the other hand, endoscopic factors are more important than clinicalones predicting rebleeding following endoscopic therapy according to Chung et al.(2001). Routine secondlook endoscopies are not recommended (Barkun et al. 2003). In thestudy of Messmann et al. (1998) scheduled secondlook endoscopy did not improveoutcome compared with second endoscopy performed only at recurrent hemorrhage.Though, by Chiu et al. (2003) scheduled repeat endoscopy with appropriate therapy16–24 hours after initial endoscopic haemostasis reduced the number of cases ofrecurrent bleeding.
2.6. Treatment
Patients with signs of upper gastrointestinal bleeding should be carefully monitoredfollowing initial fluid resuscitation even on special observation wards. Plasmaexpanders are needed, if patient remains shocked following initial fluid resuscitation.Blood transfusions are often needed, when patient has ongoing bleeding, or whenhaemoglobin concentration is less than 100g/l (Sanderson et al. 1990; Lin et al. 2002;British Society of Gastroenterology Endoscopy Committee 2002). The schedule of diagnostic endoscopy depends on the bleeding status. If patient hasmajor bleeding, urgent endoscopy is to be performed without delay. Otherwise routineendoscopy is undertaken during routine working hours. The mortality associated withacute gastrointestinal bleeding has diminished to 58% by forming specialisedgastrointestinal units with strict protocols for resuscitation, transfusion and surgery(Sanderson et al. 1990, Barkun et al. 2003).
2.6.1. Endoscopic therapy
Endoscopic therapy in PUB is possible in almost all cases. Permanent haemostasiscan be achieved in 83 % (Choudari et al. 1994). According to Williams et al. (1993),

29
before the era of endoscopic therapy, 1527% of the PUB patients were operated on,with an overall mortality of 22%. During the period of endoscopic therapy, the operationrate has been 6% and the mortality 7%. Endoscopic therapy was presented as a procedure of choice for PUB in 1989 by aConsensus Conference of Therapeutic endoscopy and bleeding ulcers (1989) at theNational Institutes of Health. There has been speculation that when therapeuticendoscopy fails, emergency surgery may be delayed and mortality may increase(Wheatley and Dykes 1990). On the other hand, endoscopic therapy was as effectiveas emergency surgery for PUB in terms of rebleeding, but mortality rates were 0% forendoscopic therapy and 20% for surgery (RalphEdwards and Himal 1992). Adrenaline causes vasoconstriction and has a local tamponade effect. Injection ofsclerosants (like polidocanol and alcohol) results in tissue necrosis, ulceration andthrombosis (Rajgopal et al. 1992). A second method in addition to adrenaline injectionis superior to adrenaline alone according to a metaanalysis of 16 trials (Calvet et al.2004) and Cochrane analysis (Vergara et al. 2007). Several other haemostaticmethods are used during endoscopy, like bipolar coagulation (O'Brien et al. 1986),heater probe thermocoagulation (Lin et al. 1990), fibrin glue (Rutgeerts et al. 1997) orhemoclip (Lin et al. 2002). According to a metaanalysis of 25 randomised controlled trials comparingendoscopic therapy to standard therapy (common antiulcer drugs and emergencysurgery if necessary), endoscopic therapy reduces rebleeding by 68% (Sacks et al.1990). In another metaanalysis of 30 randomised controlled trials, endoscopic therapysignificantly reduced rates of rebleeding (OR 0.57), surgery (OR 0.37) and mortality(OR 0.40) in PUB (Cook et al. 1992). Endoscopic haemostasis is the first line therapyfor PUB.
2.6.2. Operative treatment
Before the era of endoscopic therapy, patients with ongoing bleeding and unstablehaemodynamics were operated on and in the rest the semielective acid controllingsurgery was performed. Due to major improvements in medical and endoscopictreatment, the role of surgery has changed. Emergency surgery in PUB is a lifesavingprocedure in situations where endoscopic treatment fails or cannot be performed. The overall mortality was 12% in 145 PUB patients who had undergone emergencysurgery in Turku, Finland between the years 1973 1985. In this study only a few (2%)patients rebled following gastric resection, whereas 19% of those operated withtransfixation rebled. Furthermore, 44% of the patients who rebled died (Kuttila et al.1991). The mortality of PUB patients with emergency operation was significantly lower(9.8%) than in patients who were operated on after an observation period (16.9%) inHelsinki, Finland in the years 1975 and 1986 (Ovaska et al. 1992). Between 1974 and1986 mortality was 22.1% in Massachusetts when operations were performed for

30
massive peptic ulcer bleeding. Deaths were attributed to sepsis and organ failure, notrebleeding (Welch et al. 1986). Endoscopic treatment has failed in 20 to 25% of the PUB patients with activebleeding or a NBVV (Thomopoulos et al. 2001; Villanueva et al. 1993). Failure isrelated to shock on admission, spurting bleeding at endoscopy, anastomotic ulcer,concomitant diseases, large ulcer size and posterior duodenal ulcer. Therefore,patients with these risk factors should be carefully monitored and considered ascandidates for second look endoscopy or early elective surgery (Thomopoulos et al.2001; Villanueva et al. 1993). Following endoscopic therapy, PUB patients with acute spurting bleeding or NBVVwere randomised to early definitive surgery (n = 23) or repeated endoscopic therapy (n= 32) (Imhof et al 2003). Rebleeding occurred in 1 and 16 patients, respectively.Repeated endoscopic therapy succeeded in 9 of the 16 patients and 7 were furtheroperated on. In the era of endoscopic treatment, primary emergency surgery is considered whenthe ulcer is inaccessible to endoscopic treatment, e.g. in the posterior duodenal wallwith spurting arterial bleeding, when endoscopic therapy is unable to stop the bleeding,or when the patient has lifethreatening bleeding that does not allow endoscopy(Ohmann et al. 2000). Rebleeding after endoscopic therapy can be treated by repeatedendoscopic treatment, and permanent haemostasis is achieved in half of these patients(Villanueva and Balanzo 1997). In the rest, rebleeding is an indication for secondaryemergency surgery (Ohmann et al. 2000). In a randomised study of 120 patients with massive, persistent or recurrent bleedingof DU there was no difference between local (oversewing and vagotomy) and radicalsurgery (gastric resection and ulcer excision) concerning mortality (23 % vs. 22%), butthe rebleeding rates were higher in the local surgery group (17% vs. 3%) (Millat et al.1993). Once the decision to operate has been made, it is important to gain control of thebleeding vessel quickly. For bleeding duodenal ulcers, oversewing and ligation is aprocedure of choice, and for bleeding gastric ulcer excision of the ulcer or ligation ofthe bleeding vessels (Ohmann et al. 2000). In cases of deformed or penetrated ulcer,gastric resections may be an alternative, but in most cases ligation of the bleeding siteand further acidsuppressing medication is effective with a low mortality and lowrecurrence rate (Rogers et al. 1988; Teenan and Murray 1990).
2.6.3. Angioembolisation
New nonsurgical treatment modalities have been used in cases when endoscopictherapy or surgery fails and when the endoscopic access is difficult, like in massiveduodenal ulcer bleeding. In these circumstances arterial embolisation succeeded in allbut 1 of the 13 patients (Toyoda et al. 1995). In another study of bleeding DU

31
permanent haemostasis was achieved in 26 out of 40 patients, but the overall mortalitywas 25% (Holme et al. 2006).
2.6.4. Drug treatment
2.6.4.1. Theory
The gastric proton pump H+K+ATPase situated within the parietal cell is able toproduce large amounts of acidic gastric juice. If a fibrin clot is placed in gastric juicewith a pH < 4, it is dissolved by pepsin in minutes (Berstad et al. 1979). If similarconcentration of hydrochloric acid without pepsin is used, almost nothing happens. At pH 5.4 both platelet aggregation and plasma coagulation are virtually abolished. Invitro, acid and pepsin together inhibit platelet plug formation and fibrin clot generation.They also destroy previously established platelet plugs. Pepsin also digests fibrin clotsat a pH < 4 (Berstad 1982; Green et al. 1978). This is also confirmed by in vitro studieswith thrombelastography (Patchett and O'Donoghue 1995). In vivo more fibrinolyticactivity is found in the gastroduodenal mucosa in biopsies obtained from PUB patientswith signs of acute or recent bleeding than in patients without such signs. Acidsuppression by drugs decreases this activity (Vreeburg et al. 2001). In early stages, the major factors affecting peptic ulcer healing are intragastric acidityand pepsin activity (Tarnawski et al. 1991). Pepsin can be inhibited by acidneutralisation and clots remain stable at a near neutral intragastric pH (Berstad 1982).Therefore, the pharmacologic treatment of PUB is aiming to preserve intragastric pHnear neutral. Keeping the intragastric pH at 6 requires almost complete inhibition ofacid secretion (Green et al. 1978).
2.6.4.2. H2 receptor antagonists
H2 blockers act on histamine receptors outside the parietal cell. These agents reduceacid secretion from parietal cells and therefore help to heal ulcers. According to 2 metaanalyses (Collins and Langman 1985; Levine et al. 2002) theH2 antagonists are only comparable to placebo in acute PUB. Their use should be reevaluated, because they fail to reduce rates of rebleeding, surgery or mortalitysignificantly in patients with bleeding duodenal ulcers. On the other hand, H2 blockersmay prevent recurrent bleeding and the need for surgery in patients with bleedinggastric ulcers, but there was no effect on mortality (Collins and Langman 1985; Levineet al. 2002). In a metaanalysis of 11 studies comparing the use of H2 blockers and PPIs forbleeding peptic ulcer, PPIs have been superior in preventing rebleeding, especially incases with highrisk endoscopic signs of bleeding. However, there was no difference inthe need for surgery or mortality (Gisbert et al. 2001b).

32
The modest acid suppression and rapid development of pharmacological tolerance toH2 antagonists occurring as early as 24 h after the onset of therapy are the mainreasons for the lack of their efficacy.
2.6.4.3. Proton pump inhibitors
PPIs inhibit H+K+ATPase in the parietal cell. The drugs are the most effectivesuppressors of gastric acid secretion. Omeprazole was the first PPI brought to themarket, in Finland in 1991. Omeprazole was soon followed by lansoprazole,rabeprazole and pantoprazole. In recent years esomeprazole has been available andstudies with tenatoprazole have been published recently (Hunt et al. 2005). Oral omeprazole, the most used PPI, is relatively slow to reduce acid secretion. Asan intravenous infusion with an initial bolus dose, however, acid secretion has beenshown to be quickly inhibited and intragastric pH level stays between 4 and 6 in mostcases (Kiilerich et al. 1995).
2.6.4.3.1. Proton pump inhibitors without endoscopic therapy
In PUB patients with endoscopic signs of highrisk bleeding, but without endoscopictherapy oral omeprazole 40 mg twice a day has been superior to placebo, with a lowerrebleeding rate (10.9% vs. 36.4%) and lower rate of surgery (7.3% vs. 23.6%), but nodifference in mortality (Khuroo et al. 1997). Though PPIs without endoscopic therapyreduce rebleeding and need for surgery and repeated endoscopic treatment by a metaanalysis (Leontiadis et al. 2007), therapeutic endoscopy is considered the standard ofthe care of patients with acute PUB.
2.6.4.3.2. Proton pump inhibitors compared with endoscopic therapy
In cases with NBVV omeprazole (80 mg/day) is a valid alternative to endoscopiccombination (adrenaline injection + 0.5% polidocanol) treatment with equal 19%rebleeding rates (Grosso et al. 1995). Similarly, in cases with NBVV or adherent clotsomeprazole 40 mg orally twice a day and endoscopic ethanol injection therapy arecomparable for preventing rebleeding, with rebleeding rates of 22.9% and 20.8%,respectively (Jung et al. 2002). On the other hand, in cases with adherent clots therebleeding rate was significantly lower (0%) after endoscopic treatment with adrenalineinjection and bipolar probe coagulation than after highdose oral PPI therapy (35.3 %),the exact dose of which was not mentioned (Jensen et al. 2002). According to a metaanalysis of 6 studies comparing endoscopic therapy withmedical therapy in PUB with an adherent clot, rebleeding rate was 8.2% vs. 24.7%,indicating that endoscopic therapy is superior to PPI in preventing rebleeding (Kahi etal. 2005). However, there was no difference in mortality, 9.8% vs. 7%.

33
2.6.4.3.3. Proton pump inhibitors versus placebo following endoscopic therapy
Several studies comparing PPI with placebo following endoscopic therapy indicatethat high dose of PPI is superior to placebo in PUB patients with highrisk endoscopicsigns of bleeding in preventing rebleeding (Table 1). In most of the studies acontinuous infusion of a highdose omeprazole (80 mg bolus following infusion of 8mg/h) was compared with placebo for 72 hours (Hasselgren et al. 1997; Lau et al.2000; Schaffalitzky de Muckadell et al. 1997) or a high dose pantoprazole (Zargar et al.2006) was used. Oral omeprazole with doses 40 mg x 2 (Javid et al. 2001) or 20 mg x4 (Kaviani et al. 2003) were also superior to placebo in reducing rebleeding. In these studies, there was no difference in the mortality, or in the need foremergency surgery, exept in the study of Hasselgren et al. (1997), which wasdiscontinued due to a high mortality rate in the omeprazole group (6.9% vs. 0.6% in theplacebo group, p = 0.012). In another study the number of deaths was similar in bothgroups (Schaffalitzky de Muckadell et al. 1997).
2.6.4.3.4. Proton pump inhibitors versus H2 blockers following endoscopictherapy
In 100 PUB patients with active bleeding or NBVV after endoscopic therapy (withheater probe or multipolar electrocoagulation) omeprazole with a 40 mg bolus, followedby 160 mg of continuous infusion daily for 3 days is superior to cimetidine with 300 mgbolus followed by 1200 mg continuous infusion daily for 3 days based on the rate ofrebleeding (4% vs. 24% by day 14 after the enrolment) but there was no difference insurgery rate or deaths (Lin et al. 1998). A lower dose of pantoprazole (40 mg bolus followed by 40 mg every 12 hours for 3days) was compared with ranitidine (bolus of 50 mg followed by 50 mg every 8 hoursfor 3 days) in 102 patients with highrisk bleeding peptic ulcers following endoscopictherapy. The rebleeding rate was significantly lower with pantoprazole (4% vs. 16%),but there was no difference in deaths, 2% in both groups (Hsu et al. 2004).
Altogether 200 PUB patients with active bleeding or NBVV after endoscopic therapywith adrenaline injection received either high or a lowdose omeprazole (40 mg every 6hours, n = 67 or 40 mg every 12 hours, n = 66) as a continuous infusion, or cimetidine(400 mg every 12 hours, n = 67) as a continuous infusion for 3 days. The rebleedingrates and volume of blood transfusion were significantly lower with the highdoseomeprazole than with cimetidine, 9% versus 33%. There was no significant differencein hospital stay, number of operated patients, and deaths. The lower dose ofomeprazole had a rebleeding rate of 21% in contrast to 9% with the higher dose. Thismay have clinical significance, suggesting that a higher dose of PPI should perhaps befavoured in highrisk patients (Lin et al. 2006).

34
2.6.4.3.5. Proton pump inhibitors and endoscopic therapy
In a study of PUB patients with highrisk endoscopic signs of bleeding (activebleeding or NBVV) patients received a highdose intravenous omeprazole (80 mg bolus+ 8 mg/h) and were randomised to have endoscopic therapy or sham therapy (Sung etal. 2003). The importance of endoscopic therapy in preventing rebleeding was affirmed,since none of the patients treated with endoscopic therapy rebled, compared with 9%of the patients treated only with the high dose of omeprazole. PUB patients with concomitant illnesses received 200 or 80 mg/day omeprazole afterendoscopic treatment with adrenaline injection or heater probe, respectively, as acontinuous infusion for 3 days. Increasing the dose of intravenous PPI from 80 mg to200 mg was not adequate to control rebleeding, with rebleeding rates of 15.4% and11.3% by day 3 and 35.4% and 33.3% by day 28, respectively (Cheng et al. 2005). Analbumin level < 3 g/dl was a risk factor for rebleeding suggesting that poor backgrounddisease and poor nutritional status results in poor tissue repair. In these patientsrebleeding occurred during the days 414. End stage liver disease was associated withrebleeding occurring between days 1528. In one study the effect of a high dose of pantoprazole (40 mg intravenous bolusfollowed by 8 mg/h for 3 days) was compared with a regular dose (40 mg intravenousbolus for 3 days) in endoscopically treated patients. There was no difference the inrebleeding rate, 8% versus 12% (Shonekas et al. 1999).

Tabl
e 1.
Ran
dom
ized
tria
ls c
ompa
ring
PPIs
in th
e tre
atm
ent o
f PU
B a
fter e
ndos
copi
c th
erap
y
Stud
yn
Trea
tmen
tR
eble
edin
g%
Surg
ery
%M
orta
lity
%F
Ia%
F Ib
%F
IIa%
F IIb
%Sc
haffa
litzk
y de
Muc
kade
ll e
t al.
1997
*
130/
135
OM
E IV
80m
g+8m
g/h
Plac
ebo
9/19
5 /1
12/
06
2422
48
Has
selg
ren
et a
l.19
97 **
159/
163
OM
E IV
80m
g+8m
g/h
Plac
ebo
3.1/
2.5
4/10
6.9/
0.6
725
1652
Lau
et a
l. 20
0012
0/12
0 O
ME
IV80
mg+
8mg/
hPl
aceb
o7/
233/
84/
1010
431
18
Kavi
ani e
t al.
2003
71/7
8O
ME
PO20
mg/
6hPl
aceb
o17
/33
2/1
0/1
854
380
Javi
d et
al.
2001
82
/84
OM
E PO
40m
g/12
hPl
aceb
o7/
212/
81/
216
2522
37
Scho
neka
s et
al.
1999
82/8
6PA
N IV
40m
g x1
PAN
IV40
mg+
8mg/
h10
/12
/2/
2
* end
osco
pic
ther
apy
in 7
1% a
nd 7
3%**
end
osco
pic
ther
apy
only
in F
Ia b
leed
ing,
OM
E= o
mep
razo
le, P
AN=
pant
opra
zole
, IV
= in
trave
nous
, PO
= pe
rora
l, F=
For
rest
cla
ssifi
catio
n
35

36
2.6.4.4. Somatostatin, tranexamic acid and sucralfate
Somatostatin is presumed to be effective in arresting PUB by inhibiting gastricsecretion and reducing splanchnic blood flow (Bloom et al. 1974). In a metaanalysis ofPUB it has reduced rebleeding (Imperiale and Birgisson 1997). Somatostatinintravenously (250 µg bolus +500 µg/h) had a similar effect as intravenouspantoprazole (80 mg bolus + 8 mg/h) in maintaining a high intragastric pH during 24hours (pH > 4: 83 % vs. 70% of time and pH > 6: 64% vs. 57% of time, respectively)(Avgerinos et al. 2005). Somatostatin is not recommended in the routine managementof patients with acute nonvariceal upper GI bleeding (Barkun et al. 2003). The antifibrinolytic agent tranexamic acid impairs plasminmediated fibrinolysis bygastric juice (Patchett et al. 1989). Administration of tranexamic acid has reduced thetotal amount of blood loss and need for emergency surgery (von Holstein et al. 1987).On the other hand, tranexamic acid partially inhibited gastric juiceinduced clot lysis butdid not have beneficial effect on coagulation in an in vitro study withthrombelastography (Patchett and O'Donoghue 1995). Sucralfate has been used as a protectant of the mucosa, because it forms anulceradherent complex at ulcer site and reduces pepsin activity. Sucralfate inhibitedfibrinolysis, but it had an adverse effect on the dynamics of clot formation. Drugs likeomeprazole that profoundly neutralise gastric acid seem to be more appropriate inupper gastrointestinal bleeding than tranexamic acid or sucralfate (Patchett andO'Donoghue 1995).
2.7. The effect of drug treatment on intragastric pH
2.7.1. Intragastric pH in healthy volunteers
Gastric acid secretion is studied by the measurement of the intragastric pHexpressed in a logarithmic scale. Each increase or decrease of 1 pH unit reflects a 10fold change in acid concentration. There are several studies of intragastric pHmeasurement performed in healthy volunteers to find an ideal acid suppressing drug tobe used in PUB.
During the first 24 hours, ranitidine at doses of 150 mg300 mg/day has beensuperior to intermittent boluses of omeprazole (160 mg/day) in increasing theintragastric pH above 6, 60% vs. 2042% of time, respectively. This is probably causedby considerable interindividual variation in response to omeprazole (Teyssen et al.1995). When intragastric pH measurement is continued beyond 24 hours, H2 blockers fail toincrease the intragastric pH constantly above 4 after the first 24 hours. Thisphenomenon of tolerance has been observed with ranitidine at doses of 300 mg q.d.s

37
(Hurlimann et al 1994), at mean doses of 503 mg and 542 mg (Merki and WilderSmith1994), and with an infusion of 50 mg bolus + 0.25 mg/h (Labenz et al. 1997; Netzer etal. 1999) or injection of 100 mg/6h (Netzer et al. 1999). With omeprazole 40 mg intravenously, the maximal effect on intragastric acidity hasbeen obtained instantly and maintained for 5 days. In contrast, with omeprazole atdoses of 10 mg intravenously and 20 mg orally, the maximal effect on gastric acidity(60% reduction) was obtained only after 5 days. However, the reduction of intragastricacidity in these healthy subjects was less than in duodenal ulcer patients (Cederberg etal. 1993). In a study of Hurlimann et al. (1994), the response of intragastric pH to theadministration of omeprazole 40 mg or ranitidine 300 mg orally was studied in healthyvolunteers. With ranitidine, the maximum acidsuppressing effect was present on day 1(median pH 4.4). Thereafter the effect faded, implying tolerance. With omeprazole, theantisecretory effect (median pH 3.8 on day 1) further increased during the first week. With a continuous omeprazole infusion (80 mg bolus + 8 mg/h) intragastric pH stayed> 4 over 95% of the time during the first day and at 100% on the third day. In contrast,with the injection of omeprazole (80 mg bolus + 40 mg every 6 hours) the result wassignificantly less effective on day 1, but after that pH increased to a similar level withomeprazole infusion (Netzer et al. 1999).
2.7.2. Intragastric pH in peptic ulcer bleeding
There are only a few studies in which intragastric pH measurements have beenperformed in patients with PUB. Omeprazole 120 mg/day has been superior toranitidine 300 mg/day (Lanas et al. 1995), omeprazole infusion superior to cimetidineinfusion (Lin et al. 1998) and omeprazole infusion (80 mg bolus + 8 mg/h) superior toranitidine infusion (50 mg bolus +0.25 mg/kg/h) (Labenz et al. 1997) in increasing thepH above 6. Both 200 mg and 80 mg of omeprazole intravenously increased themedian 24h intragastric pH above 6 (Cheng et al. 2005). With higher doses ofpantoprazole infusion (80 mg bolus + 6 mg/h vs. 8 mg/h) there was better control andlower interindividual variability of the acidity (pH 6 during 48 hours 47% and 64% ofthe time, respectively). In Taiwan, 88 PUB patients who underwent endoscopic therapy were placed onomeprazole (40 mg + 40 mg every 6h) for 3 days. The mean intragastric pH was < 6 in25 patients and < 4 in 4 patients, defined as poor responders to intravenousomeprazole. These patients with pH < 4 had a higher rebleeding rate (Hsieh et al.2004). On the other hand, the rebleeding was not related to the increase of pH, sincepatients with adequate pH control rebled and also deaths occurred (Labenz et al. 1997;van Rensburg et al. 2003). So far, in Finland there is no study reporting the control ofintragastric acidity with the treatment of PUB.

38
2.7.3. The effect of H.pylori on intragastric pH
The increase in pH with omeprazole has been more constant and profound inpatients with DU than in healthy controls (Cederberg et al. 1993). Omeprazole 20 mgincreased the intragastric pH less after the eradication of H.pylori than before the preeradication phase in DU patients (median 24hour pH 5.5 vs. 3.0) (Labenz et al. 1996).Similarly, the median intragastric 24 hour pH decreased from 7.95 in H.pyloripositiveto 3.75 in H.pylorinegative healthy volunteers after 68 weeks of treatment withomeprazole 40 mg daily (Gillen et al. 1999). This difference may be caused by highercontent of buffer substances in the infected stomach or by a higher volume of gastricsecretions. Therefore, the dose of PPI in H.pylorinegative subjects should be reevaluated (Gillen et al. 1999; Labenz et al. 1996).
2.7.4. CYP2C19 genotype and intragastric pH
Omeprazole is completely metabolised by the liver with hydroxylation which iscatalysed by the polymorphic cytochrome P450 isoenzyme CYP2C19. This CYP2C19genotype status can affect the efficacy of the PPI omeprazole (Furuta et al. 1999). Inhomozygous carriers this isoenzyme is absent. Of Caucasians 36 % and of Orientals1830% lack this isoezyme and are called poor metabolisers of omeprazole.Therefore, in Orientals the clearance of omeprazole is on average slower than inCaucasians (Bertilsson 1995; Sagar et al. 1998; Sagar et al. 2000). When combininghomozygous and heterozygous carriers of this mutation, almost 60% of Asianpopulations have a slower metabolism of CYP2C19 substrates than the majority ofCaucasians (Meyer 1996). Genotyping test of CYP2C19 might be valuable indetermining an effective dose of omeprazole in some treatmentresistant, acidrelateddiseases (Ishizaki and Horai 1999).
2.8. Omeprazole and H.pylori
2.8.1. Effect of omeprazole on H.pylori
H.pylori colonises the gastric epithelium and its urease activity is probably essentialfor colonisation. The base produced by the urease may protect the organism fromgastric acid (Eaton et al. 1991). In vitro studies indicate that the survival of H.pylori below pH 4 may be ureasedependent (Bugnoli et al. 1993). Omeprazole inhibits the urease enzyme of H.pylori ina dosedependent manner (Bugnoli et al. 1993). On the other hand, omeprazoledecreases H.pylori survival at low pH also through a mechanism independent of itseffect on urease. The drug also has an antibacterial effect on other bacteria (McGowanet al. 1994).

39
2.8.2. Detection of H.pylori
H.pylori eradication is defined as absence of the bacterium when detection is carriedout at least one month after the cessation of the treatment (Rauws et al. 1988). Inseveral studies omeprazole transiently affects the detection of H.pylori (Stolte andBethke 1990; Yamamoto et al. 1995). After 4 weeks (Fukuda 1996; Logan et al. 1995; Marzio et al. 1995), 2 weeks (Hui etal. 1991) or even after one week of treatment (Verdu et al. 1994) some H.pyloripositivesubjects temporarily turned H.pylori negative. The lack of detection of H.pylori from theantral mucosa after omeprazole treatment was dosedependent and the density ofH.pylori decreased with omeprazole, but not with ranitidine (Hui et al. 1991). After 4 weeks of omeprazole treatment H.pylori colonisation decreased in the antrumand corpus and increased in the fundus (Logan et al. 1995). It was speculated thatH.pylori migrated from the antrum to the corpus (Marzio et al. 1995). Later thisspeculation has been rejected, because in another study the number of H.pyloridecreased both in the antrum and corpus (Graham et al. 1996b). The distribution of H.pylori in gastric mucosa between GU and DU is different, sincethe bacteria is found only in antrum in 7% of GU and 43% of DU cases, but both inantrum and corpus in 82% or 56% of the patients, respectively (Vorobjova et al. 1991).
2.8.3. PUB and test reliability for H.pylori
The prevalence of H.pylori infection in PUB has been lower than in cases ofnoncomplicated peptic ulcer (Lee et al. 2000; Liao et al. 2003). This may be due to thebiopsybased methods (rapid urease test, histology, culture), which have low sensitivity(4570%) but high specificity (9098%) to detect H.pylori in cases of uppergastrointestinal bleeding (Gisbert and Abraira 2006; Grino et al. 2001; Lee et al. 2000;Liao et al. 2003). In contrast, urea breath test has been sensitive (93%) and specific(92%) (Gisbert and Abraira 2006; Liao et al. 2003). Blood in the stomach may interfere the result of rapid urease test (Lee et al. 2000)and also prior PPI medication induces falsenegative results. To increase the accuracy,other additional tests should be used (Grino et al. 2001; Liao et al. 2003). The low rateof H.pylori infection in the acute bleeding phase may also be due to a differentpathogenesis in bleeding peptic ulcers than in uncomplicated ulcers. This is clinicallyimportant because a patient with an overlooked H.pylori infection is more likely toexperience recurrent ulcer and bleeding (Gisbert and Abraira 2006).
2.8.4. Recurrent bleeding after eradication of H.pylori
Eradication of H.pylori infection reduces the rate of ulcer recurrence and rebleedingin complicated ulcer disease (Graham et al. 1993). After the occurrence of PUB,

40
eradication of H.pylori has been superior to maintenance antisecretory treatment inpreventing recurrence of peptic ulcer and rebleeding (Santander et al. 1996).
2.9. Clinical practice today and future aspects
Studies of patients with a history of PUB has revealed that only from 12% (vanLeerdam et al. 2003) to 20% (Hudson et al. 1995b) of the NSAID prescriptions has hadcoprescription of antiulcer drugs. Altogether 50% of the NSAID consuming patients atrisk of ulcers (history of peptic ulcer, > 60 years of age) do not use gastroprotectivetherapy (Lanas and Fernandez 2007). Guidelines of pain management recommend forpatients at risk NSAID with PPI or COX2 inhibitors. Still, in patients with history of PUB,combination of COX2 inhibitor and PPI was more effective than COX inhibitor alone inpreventing a new episode of PUB (Chan et al. 2007b). The routine administration of intravenous PPI to all persons admitted due to uppergastrointestinal bleeding until diagnostic endoscopy is performed and thereafterdiscontinuing the drug in those other than PUB would prevent 40 rebleeding episodes,9 emergency operation and 223 hospital days/1000 patients. This policy is estimated tobe a costeffective treatment strategy in the USA (Gagnon et al. 2003). In Canada, only 13.4% of all patients who had intravenous PPI when admitted tohospital due to suspected upper gastrointestinal bleeding had PUB with high risk signsof bleeding. After diagnostic endoscopy, intravenous PPI was unnecessarily continuedin 57% of the patients with lowrisk or even nonulcer lesions (Enns et al. 2004). In theCanadian practice intravenous PPI infusions before endoscopy compared with afterendoscopy may lower the proportion of actively bleeding peptic ulcer lesions found onendoscopy, but this does not affect the rates of rebleeding, surgery or mortality(Andrews et al. 2005). In Amsterdam, between years 1993/1994 and 2000 the use of H2 blockers hasdecreased from 54% to 6%. High dose intravenous PPI has been administered to 37%of the high risk PUB patients. Despite these new treatment modalities, rate ofrebleeding, emergency surgery and mortality has remained the same (van Leerdam etal. 2003).On the other hand, PPI use and endoscopic haemostasis in patients with highriskstigmata decreased the rebleeding rate in a Canadian registry of nonvariceal uppergastrointestinal bleeding in 1999 and 2002. Generally, rebleeding rate was 14%,surgery rate 7% and mortality 5% (Barkun et al. 2004a). Peptic ulcer is believed to be a disappearing disease, because powerful ulcerhealingdrugs and eradication of H.pylori should abolish the disease. At the same time, there isa clear increase of lifethreatening complications of peptic ulcer disease in olderpeople. This most probably results from comorbidities and increased consumption ofNSAIDs in the elderly. Despite the progress in the treatment of chronic peptic ulcerdisease in the past decades, peptic ulcer bleeding remains a therapeutic challenge.

41
3. AIMS OF THE PRESENT STUDY
The purpose of the current clinical study was to examine controversial aspects ofpeptic ulcer bleeding and its treatment with modern strategies. The following issueswere addressed:
1. Does a highdose of omeprazoleinfusion offer any benefit compared to the regulardose in patients with PUB who have been treated endoscopically?
2. How do different omeprazole doses affect the intragastric acidity in PUB?
3. What are the important risk factors and their possible concurrence in patients withPUB?
4. Do different doses of omeprazole have any impact on the detection of H.pylori ingastric mucosa of patients suffering from PUB?

42
4. PATIENTS
This prospective study was performed between June 1994 and December 1996 inthe Central Hospital of Central Finland, Jyväskylä, Finland and Kuopio UniversityHospital, Kuopio, Finland. The hospitals serve a population of 500 000. During thestudy period 591 patients were admitted with suspected acute upper gastrointestinalbleeding.
Comparison of intravenous omeprazole doses on PUB after endoscopictreatment (Study I)
There were 314 patients with suspected PUB. The characteristics of patients primarilyexcluded, randomised and later excluded are presented in Table 2.
Table 2. Patients excluded and randomised to Study I.
Patients with upper gastrointestinal bleeding n = 591Patients with nonpepticulcer bleeding n = 277Patients with peptic ulcer n = 314 peptic ulcer patients excluded from the randomisation n = 146 Forrest classification III n = 58 H2 blocker or protonpump inhibitor medication on admission n = 32 no definitive diagnosis in first endoscopy n = 15 terminal illness n = 11 refusal to participate n = 9 inability to give informed consent, no cooperation n = 8 immediate failure of endotherapy and operation n = 5 anastomotic ulcer n = 5 no endoscopy n = 3 Peptic ulcer patients randomised n = 168 Randomised but excluded from analysis n = 26 Forrest III n = 13 malignancy n = 4 unwilling to continue n = 2 bleeding and perforation n = 1 study drug unknown n = 6Included in the study n = 142

43
Effect of different doses of omeprazole on intragastric pH in PUB (Study II)
Intragastric pH monitoring was available only in Kuopio University Hospital andduring the working days. Altogether 86 out of 142 acute PUB patients attended thebasic study in Kuopio. Of these patients 17 had diagnostic endoscopy during theweekend. Altogether only 15 of the remaining 69 subjects were willing and gave theiroral consent to participate in the 3day pH monitoring of gastric acidity. Two patientswere later excluded because they removed the nasogastric catheter only two and sixhours after the initiation of the pH monitoring leaving 13 patients for the analysis. Table3 shows that the demographics of the patients with PUB in the basic study (Study I)and those of the patients participating in the intragastric pH monitoring are comparable.
Table 3. Demographics of 129 patients with peptic ulcer bleeding in the basic study andof the 13 patients with intragastric pH monitoring.
Patients of basicstudy*(n = 129)
Patients withintragastric pHmonitoring(n = 13)
p
Male/female 77/ 5259.7%/ 40.3%
8/ 561.5%/ 38.5%
0.89
Age (years) (mean±SD) 64.9 ± 14.5 62.6 ± 15.1 0.5Forrest Ia, Ib 56 (43.4%) 7 (53.8%)Forrest IIa, IIb, IIc 73 (56.6%) 6 (46.2%)
0.56
NSAID 72 (58.5%) 7 (58.3%) 1.0ASA 22 (17.1%) 2 (15.4%) 1.0Oral anticoagulant 13 (10.1%) 1 (7.7%) 1.0Antisecretory drug** 12 (9.3%) 1 (7.7%) 1.0Haemoglobin, mean, on admission (g/l)
91.0 ± 27.4 81.1 ± 25.6 0.2
Size of ulcer (mm)(mean±SD)
13.2 ± 14.3 x12.7 ± 11.9
12.8 ± 8.5 x15.4 ± 12.3
0.90.4
Rebleeding 13 /10.1% 2 /15.4% 0.78Mortality 6 /4.7% 0 0.43
ASATP: acetylsalicylic acid for thrombosis prophylaxisNSAID: non steroidal antiinflammatory drug*basic study = Study I**antisecretory drug used during last month but not on admission.

44
Risk factors and their combinations in PUB (Study III)
Of the 591 patients with upper gastrointestinal bleeding in 277 patients the cause ofbleeding was not peptic ulcer disease. Of the 314 suspected PUB patients in 3 patientsendoscopy was not performed, in 15 patients no definitive diagnosis was found inendoscopy, 4 patient had malignancy and 1 patient had bleeding and perforation. Thecharacteristics of the 291 patients with PUB excluded and finally included in the riskfactor analysis is presented in Table 4.
Table 4. Patients included in the Study III.
Patients with peptic ulcer bleeding n = 291Excluded from the casecontrol study n = 197 Terminal illness n = 11 Refusal to participate or no cooperation n = 17 Previous subtotal gastrectomy n = 4 Ongoing H2 blocker/ PPI medication n = 32 H.pylori eradication previously n = 13 No biopsies in endoscopy n = 35 Forrest III n = 52 Not interviewed n = 33Included in the casecontrol study n = 94
The control group consisted of 94 age (± 5 years) and sexmatched nonulcerpatients attending elective endoscopy during the same year. Because many patientswith pulmonary diseases were sent to exclude reflux esophagitis, there were morepatients with pulmonary disease in the control group, 7 vs. 17, p = 0.047.

45
Effect of different doses of omeprazole on the detection of H.pylori (Study IV)
Of the 168 randomised patients, 114 were H.pylori positive. Thirteen patients wereexcluded from this study because of the lack of control endoscopy or biopsies taken onday 3. There were 101 H.pyloripositive patients left for the analysis.
All patients
Summary of age and sex of the patients participating in studies IIV is presented inTable 5.
Table 5. Age and sex of patients in studies I, II and IV with reference to omeprazoledose and study III with reference to case/control status.
Study IRegular/High
Study IIRegular/High
Study IIICase/Control
Study IVRegular/High
Patients 73/69 7/6 94/94 51/50Age (years,mean) 66/ 63.4 63/60.8 63.7/ 63.8 62.8/62.7Males/Females 44/29 vs.41/28 4/3 vs. 4/2 59/35 vs. 59/35 23/17 vs.29/15
Regular = Regular dose of omeprazole, High = High dose of omeprazole

46
5. METHODS
OGD was to be performed by experienced endoscopists within one to 72 hours ofadmission. No drug treatment for ulcer was given prior to endoscopy. Bleeding wasclassified using a modified Forrest classification (Ia = spurting bleeding, Ib = oozingbleeding, IIa = visible vessel, IIb = clot , IIc = black base, III = clear ulcer base).
Endoscopic therapy
Clots covering ulcers were to be washed gently away. Endoscopic haemostasis usingadrenaline 1/10000 in 0.5 ml doses four to six times around the bleeding site and /orheater probe (Heatprobe unit, model HPY; Olympus Optical Co. Ltd. Japan), orsclerotherapy with ethanolamineoleate was performed. Indications for endoscopictherapy were Forrest classification III ulcers (spurting, oozing, nonbleeding visiblevessel, clot and black base). Patients had been assigned to receive endoscopictherapy, but the endoscopist decided whether the endoscopic treatment wasnecessary. In study I endoscopic therapy was given on demand to 50 (68.5%) patients in theregular omeprazole and to 52 (75.4%) in the high dose omeprazole group. Thirty seven(90.2%) of the regular dose group and 35 (85.4%) of the highdose group patients withhigh risk of rebleeding (Forrest Ia, Ib, and IIa) had endotherapy. Second lookendoscopy on day 3 was performed in 67 (91.8%) and 65 (94.2%) patients,respectively. Ten patients did not undergo control endoscopy after 72 hours. Three ofthem had undergone control endoscopy earlier, 6 underwent operation and 1 wassuffering from continuous ischaemic heart pain.
Proton pump inhibitor treatment
Patients with acute PUB (Forrest III) were randomised to receive a continuousinfusion of highdose omeprazole (Losec® as an 80 mg bolus +8 mg/h for 72 hours, i.e.652 mg/72 hours) or a regular dose of omeprazole (20 mg once a day followed bysaline infusion, i.e. 60 mg of omeprazole/72 hours). The infusion was started during 1hour after the endoscopy at a surgical ward. All investigators were unaware of thepatients’ drug treatment assignment. Patients received only intravenous fluids during the 72 hours and were not allowed toeat or drink, since in case of rebleeding, food in the stomach would have madeperforming of reendoscopy difficult. No other ulcer medication was given. Patients withhaemoglobin concentrations below 100 g/l received blood products until haemoglobinreached 100 g/l. When a patient had clinical signs of continuing bleeding or rebleeding(haematemesis, new signs of melena, shock) endoscopy with the therapeutic optionswere repeated or emergency operation was undertaken.

47
Any signs of continuing bleeding or rebleeding were recorded in the control OGD after72 hours, after which H2receptor antagonist treatment was given for 8 weeks.
Diagnosis of H.pylori infection
H.pylori infection was assessed by histology (2 biopsies from the antrum and 2biopsies from the corpus) and urease test (1 antrum and 1 corpus biopsy; Jatrox ®; H.pTest, CiH.R.Heim Arzneimittel GmbH, Darmstadt). Biopsies were taken before andafter the 3day omeprazole treatment. The diagnosis of H.pylori was made if either ofthe tests was positive. Biopsies were analysed by histology after Giemsa staining tograde H.pylori infection: no bacteria (grade 0), occasional bacteria (grade 1), scatteredbacteria in most fields (grade 2) and numerous bacteria in most fields (grade 3).
Detection of CagA antibodies
Serum CagA antibodies of the IgG class of H.pylori were determined by animmunoblot method (I.D. Blot H.pylori IgG, DPC, Los Angeles, CA, USA).
Intragastric pH monitoring
A flexible glass pH catheter with internal reference (Synectics MedicalInc., Stockholm, Sweden) was introduced through the nostril to reach the stomachwithin 1 hour after the endoscopy. When the pH turned clearly acidic (pH < 3) and thedistance from the tip of the electrode to nostrils was > 55 cm, the electrode wasconsidered to reach the acid secretion environment and it was firmly fixed withadhesive tape to the nose and face. All recordings were performed with Digitrapper MkIII recorders (Synectics Medical Inc.) and analysed with EsopHogram software (version5.60C4, Synectics Medical). The recorder was calibrated according to manufacturer'sinstructions before each recording. Sampling interval was set to 16 s to enable up to 96h recordings. In all patients included the initial intragastric pH was < 3. For the purposes of this study, all time periods with intragastric pH less than 4 andless than 6 were identified and compared with the total measurement time. In addition,by using pHtime curves, the average pHlevel during each 30 min period wasmeasured with 0.2 pH unit accuracy.
Statistics
Comparison of intravenous omeprazole doses on PUB after endoscopic treatment(Study I)
Significance of differences in categorical data was determined using the χ2test orFisher’s exact test. The ttest was used to assess the significance of differencesbetween means of normally distributed continuous variables. The MannWhitneyU

48
test was used when variables were not normally distributed. Results are reported asmeans and standard deviations (SD). A level of p < 0.05 was regarded as statisticallysignificant.
The normal statistical techniques finding differences between treatments is not validwhen the goal is to assess whether the treatments are equally efficacious. Therefore,equivalence testing, which actually reverses the roles of null and alternativehypotheses, was used (Dunnet and Gent 1977; Blackwelder 1998). The study wasdesigned to detect equivalence with equivalence threshold of 0.15 for the difference inproportions presuming 0.1 failure rate, zero hypothesised difference, 0.9 power and0.95 confidence. This would be ensured with 69 patients in each group. In equivalencetesting it is necessary to define tolerance limits and the range of equivalence.Equivalence is thereafter confirmed or rejected by observing if the confidence intervals(CI) of difference of proportions lie totally within the range of equivalence. Thepredefined value for the difference in proportions is +15%, as mentioned above. The goal of this study was to assess whether the regular dose of omeprazole was atleast as effective as high dose of omeprazole in preventing rebleeding in ulcer patients.Therefore onesided equivalence testing was used and only upper tolerance limit fordifference in proportions was defined. For onesided tests at 0.05 level the confidencecoefficient has to be 90% in equivalence testing. Exact confidence limits used inequivalence testing are quite conservative, but they are necessary due to the lowincidence rate. The hypothesis testing for equivalence was performed by testing thenull hypothesis H 0: θ ≥ θ 0 against the alternative hypothesis H 1: θ < θ 0, where θ is thedifference in proportions or odds ratio, and θ 0 is the respective tolerance limit.
Effect of different doses of omeprazole on intragastric pH in PUB (Study II)
For continuous data and median values Wilcoxon’s ranksum was applied. Thelongitudinal data was analysed with linear mixed models using the first orderautoregressive covariance structure and restricted maximum likelihood method forestimation (Singer and Willett 2003). The covariance structure was chosen bycomparing the 2 logarithm of restricted maximum likelihood. Omeprazole dose(high/regular) and measurement time were included in the model. The data arepresented also as mean ± standard deviation (SD). The stratified CochranArmitagetrend test was used to assess significant trends in proportions of time that intragastricpH is below 4.0.
Risk factors and their combinations in PUB (Study III)
Single risk factors and combinations of risk factors were analysed by calculatingsingle odds ratios. Conditional logistic regression analysis was used as a multivariateanalysis to account for simultaneous risk factors in matched data (LogExact, CytelSoftware Corp., Cambridge, MA). Interaction terms of different combinations of risk

49
factors were added one by one into the model to test possible mutual interference ofthe combination of two separate risk factors. Significant interaction term indicates thatsimultaneous risk factors potentiate or attenuate the risk. The CochranArmitage trendtest was used to detect possible trends in proportions of naturally ordered factors. Theeffect of the dose of ASA, ketoprofen, ibuprofen, cigarettes and alcohol on the risk ofbleeding was studied by trend analyses.
Effect of different doses of omeprazole on the detection of H.pylori (Study IV)
Significance of differences in categorical data was determined using the Fisher’sexact test. The Ttest was used when appropriate. Results are reported as means andstandard deviations (SD).
Ethical aspects
Informed consent was obtained from all subjects. The study was approved by theethics committee of each centre and was conducted in accordance with the Declarationof Helsinki.

50
6. RESULTS
Regulardose versus highdose omeprazole after endoscopic treatment in PUB(Study I)
Rebleeding occurred in 6 (8.2%) of the 73 patients receiving the regular dose ofomeprazole and in 8 (11.6%) of the 69 patients receiving the high dose (p = 0.002 forequivalence, equivalence limit 0.15). Three (4.1%) of the former and 5 (7.2%) patientsof the latter group underwent surgery. Four (5.5%) patients in the regular and 2 (2.9%)in the high dose group died in 30 days from the admission. There was no differencebetween the regular and the high dose group in blood transfusions (regular vs. highdose: 5.3 units, SD 7.7 vs. 5.5 units, SD 5.2) or mean hospital stay (5.7 days, SD 2.5,vs. 5.9 days, SD 2.7). In patients with spurting or oozing bleeding or nonbleeding visible vessel ulcers(Forrest Ia, Ib, IIa) the rate of rebleeding was 7.3% in the regular dose group and12.2% in the highdose group (p = 0.7). The rate of rebleeding was 9.7% and 10.3%,respectively in patients with Forrest IIb and IIc ulcers (clot/black base), (p = 0.6). Sincethe rate of rebleeding was similar regardless of the Forrest classification (7.3% vs.9.7% in the low dose and 12.5% and 10.3% in the high dose group), the bleeding datawas combined (Table 6).
Table 6. Rebleeding according to Forrest classification in peptic ulcer bleeding patientsreceiving a regular or a highdose of omeprazole
Forrestclassification
Patients with rebleeding /Regular dose omeprazolen = 73
Patients with rebleeding /High dose omeprazolen = 69
Forrest Ia,Ib, IIa 3/42 5/40 Spurting bleeding (Forrest Ia)
2/11 2/5
Oozing bleeding (Forrest Ib)
0/20 2/27
Nonbleeding visible vessel (Forrest IIa)
1/11 1/8
Forrest IIb, IIc 3/31 3/29 Clot (Forrest IIb)
3/9 2/13
Black base (Forrest IIc)
0/22 1/16
All 6/73 8/69

51
Effect of regular and high doses of omeprazole on the intragastric acidity in PUBtreated endoscopically (Study II)
The mean 24hour intragastric pH (regular versus high dose) on day 1 was 4.9±1.6vs. 6.3±0.5, p = 0.035; on day 2: 4.9±1.8 vs. 6.7±0.3, p = 0.001, and on day 3: 5.7±1.1vs. 6.7±0.5, p = N.S. Medians of intragastric pH were: day 1: 6 vs. 6.5, p = 0.082; day2: 5.8 vs. 6.8, p = 0.001, and day 3:6.2 vs. 6.8, p = 0.17. The mean and median ofintragastric pH in PUB patients during 72 hours is presented in Figures 1 and 2. Bothfigures reveal the efficacy of the high dose of omeprazole in increasing the intragastricpH. There was no statistical difference in the means of the proportion of the time withan intragastric pH < 4 between the regular and the highdose groups on day 1: 29.2%±34.1 versus 5.4% ±5.7, p = N.S; day 2: 24.8% ±41.8 versus 0%; day 3:14.2% ±16.5versus 0%. There was a significant difference in the percentage of time when pH was below 6 onday 1 (46.5%±34 versus 10.5% ±13.8, [p = 0.034]) and day 2 (50.7%±35.5 versus0.3%±0.9, [p = 0.001]), but not on day 3 (30.9% ±27.3 versus 3.2%±6.4 [p = 0.14]).However, there was a significant decrease in the proportion of time the intragastric pHwas below 4.0 over the 3day period in the regular dose group (p=0.029 for a trend).With the regular dose of omeprazole, both mean and median intragastric pH, however,increased > 4.
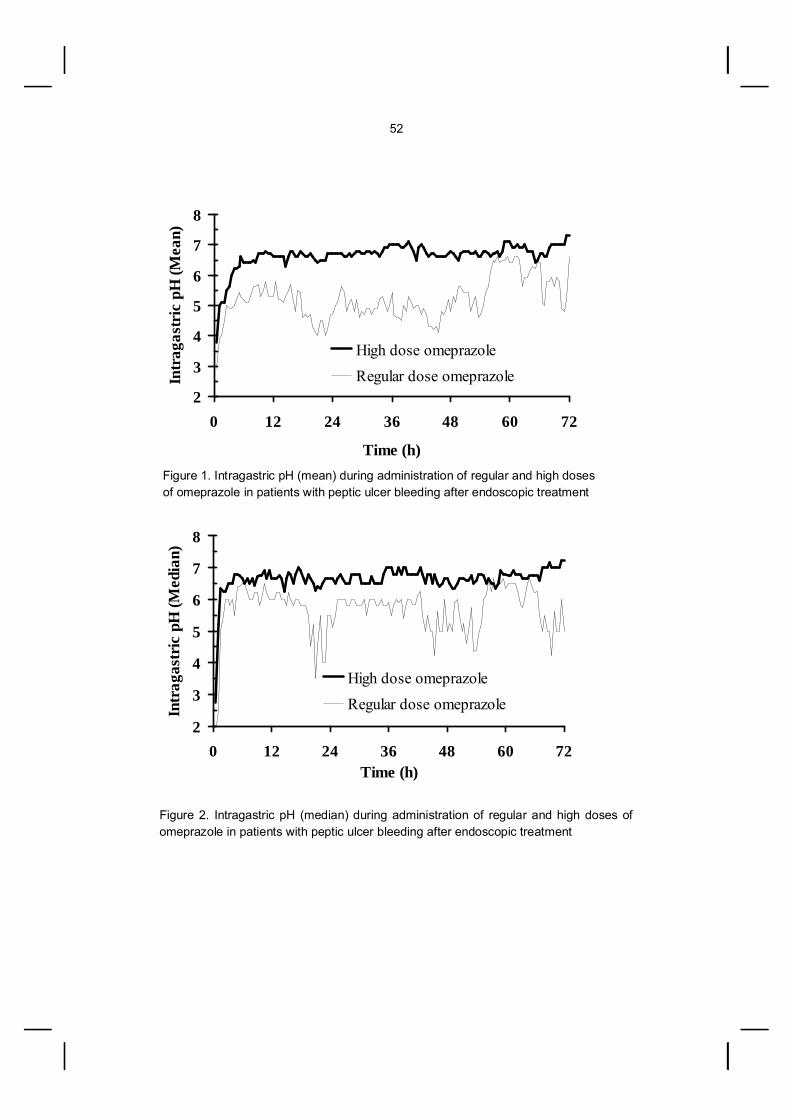
52
Figure 1. Intragastric pH (mean) during administration of regular and high doses of omeprazole in patients with peptic ulcer bleeding after endoscopic treatment
Figure 2. Intragastric pH (median) during administration of regular and high doses ofomeprazole in patients with peptic ulcer bleeding after endoscopic treatment
2
3
4
5
6
7
8
0 12 24 36 48 60 72Time (h)
Intr
agas
tric
pH
(Med
ian)
High dose omeprazoleRegular dose omeprazole
2
3
4
5
6
7
8
0 12 24 36 48 60 72
Time (h)
Intr
agas
tric
pH
(Mea
n)
High dose omeprazoleRegular dose omeprazole

53
Analysis of risk factors and their combinations in PUB (Study III)
H.pylori infection (OR=odds ratio) (OR 8.79, 95%CI:3.6523.3), the use of ASAP(OR 3.45, 95%CI:1.1810.8), ASATP (OR 4.07, 95%CI:1.1216.29), smoking 20cigarettes daily (OR 6.43, 95%CI:1.1944.2), previous DU (OR 8.96, 95%CI:2.0750.43) and NANSAID with 1 defined daily doses (OR 6.56, 95%CI:1.7728.37) wereindependent risk factors for PUB in the logistic regression analysis. ASA, ibuprofen,ketoprofen and smoking had dosedependent associations with PUB as shown bytrend analyses (Table 7). Altogether 75 of the cases and 35 of the controls were defined as H.pylori positive, p<0.001. Of them, 66 (97.1%) and 26 (96.3%) had the CagA strain of H.pylori,respectively. There were only 5 patients who were H.pylori negative and were not usingNSAIDs compared to 25 of the controls, p < 0.001. Seven patients among the caseswere on warfarin therapy, but none among the controls, p < 0.001. The mean numberof independent risk factors (history of DU, H.pylori, ASA, smoking 20 cigarettes, 1DDD of NANSAID) in the group of cases was 1.88 (s 0.89) and in the control group0.73 (s 0.61), p < 0.001. Of the cases 4 did not have any of these risk factorscompared to 33 of the controls, p < 0.001. Furthermore, 3 risk factors were present in24 of the cases but in none of the controls, p < 0.001. One of the following risk factors,namely the use of ASA, 1 DDD of NANSAID and smoking 20 cigarettes waspresent in 63 of the cases and in 31 of the controls, p < 0.001. Two of them werepresent in 16 of the cases but in none of the controls, p < 0.001. Two thirds of the PUBpatients had at least 2 independent risk factors, indicating accumulation of risk factorsin the affected patients.

54
Table 7. Trend analysis of risk factors with a dose effect in PUB.
ASA None <500mg 5001000mg >1000mg p *Case (n) 57 17 13 7Control (n) 74 13 4 0Proportion 0.8 1.3 3.3 0.0001
Ketoprofen None <150 mg >150 mgCase (n) 82 1 12Control (n) 84 5 2Proportion 1.0 0.2 6.0 0.044
Ibuprofen None ≤1200 mg >1200 mgCase (n) 81 7 6Control (n) 86 4 1Proportion 0.9 1.8 6.0 0.043
Smoking None < 20 cigarettes >20 cigarettesCase (n) 59 12 18Control (n) 73 14 4Proportion 0.8 0.9 4.5 0.005
Alcohol None <1 dose 13 dose 3 dosesCase (n) 51 18 10 7Control (n) 58 25 5 4Proportion 0.9 0.7 2.0 1.8 0.205

55
Effect of shortterm treatment with regular or high doses of omeprazole on thedetection of Helicobacter pylori in PUB (Study IV)
After 3day omeprazole treatment the diagnostic tests (urease test, histology) ofH.pylori (any test) were negative in 14 (27.5%) of 51 patients in the regular and in 30(60%) of 50 in the high dose group, p = 0.001. A subanalysis of the patients with positive histology (n = 78) in the first endoscopyand information on the biopsies of the antrum and corpus in both of the endoscopies(preentry and after 3 days) (n = 78) revealed that the negative result of H.pyloricolonisation was found in 13 patients (31.7%) of the regulardose and in 25 (67.6%) ofthe highdose group; p = 0.003. Another similar subanalysis was carried out in patientsassessed by urease test (n = 84). Of the 39 H.pyloripositive patients in the regulardose and of the 45 H.pyloripositive patients in the highdose group, 17 (43.6%) and 37(82.2%), became H.pylori negative, p = 0.001. The change in the distribution of H.pyloriin gastric mucosa after the omeprazole treatment is shown in Table 8. The change incolonisation of the bacterium is presented in Table 9.
Table 8. Distribution of H.pylori in gastric mucosa after 3day omeprazole treatment inpatients with the bacterium both in antrum and corpus (A+C+) assessed by histology.
Before treatment A+C+
Regular doseomeprazole(20 mg/ day)
n = 38
High doseomeprazole(80 mg + 8 mg/h)
n = 34p
After treatment A+C+ 20 8 0.016 A+C 2 1 N.S AC+ 5 2 N.S AC 11 23 0.002
A+C+: antrum positive and corpus positive; A+C : antrum positive and corpusnegative; AC+: antrum negative and corpus positive; AC : antrum negative andcorpus negative for H.pylori

56
Table 9. Change in colonisation of H.pylori (grades 0,1,2,3) in antrum and corpus afterregular and high dose of omeprazole treatment.
Antrum n = 77
Corpus n = 79
Omeprazole OmeprazoleGrade Regular dose
n = 40High dosen = 37
Regular dosen = 41
High dosen = 38
Negative colonisation 16 27* 15 27** 10 6 8 9 10 20 5 13 6 12 30 5 6 0 5
Decrease in density 11 8 9 6 21 7 4 5 6 31 4 4 2 0 32 0 0 2 0
Density remained the same 13 2*** 13 5 11 6 2 9 5 22 6 0 3 0 33 1 0 1 0
Increase in density 1 0 4 0 12 0 0 3 0 13 0 0 1 0
Regular vs. high dose of omeprazole: negative colonisation of H.pylori infection inantrum * p = 0.006, or in corpus ** p = 0.004; density of H.pylori remained the same inantrum *** p = 0.003.

57
7. DISCUSSION
The present study gives information on the treatment of acute PUB, of the pHresponse in gastric juice during regular and highdose omeprazole treatment underthese circumstances and on the detection of H.pylori in the bleeding phase. Also therisk factor profile of PUB patients is presented.
Effect of acid suppression after endoscopic treatment of bleeding peptic ulcer onrebleeding rate and mortality (Study I)
A regular dose of omeprazole was compared with a high dose in a prospectiverandomised double blind setting. The high dose of omeprazole was compared with aregular dose rather than placebo, because it was considered unethical to leave patientswith acute peptic ulcer and bleeding complication without definitive treatment after thediagnostic endoscopy for 3 days. There is only 1 study with a similar setting, publishedin an abstract form (Shonekas et al. 1999). In our study, the rebleeding rate was low,and the inclusion of Forrest IIb and c patients has been criticised (Lin et al. 2006).However, in subgroup analyses the rebleeding rate in Forrest IIb and c patients wasnot significantly different from Forrest Ia, Ib and IIa cases, indicating that after the initialhaemostasis by endoscopy some other patientrelated factors may cause rebleedingand mortality. We had similar criteria as in the study of Hasselgren et al. (1997), in which Forrest IIbwas defined as a clot/black base, indicating that they also included patients withForrest IIc, i.e., with a black base. In the study of Lau et al. (2000) 51% of the patientshad spurting or oozing bleeding (Forrest I). Of our patients 45%, of the patients in thestudy of Hasselgren et al. (1997) 30% and of the patients in the study of Schaffalitzkyde Muckadell et al. (1997) 32% had such bleeding. There was a protocol violation inthe present study, because endoscopic therapy was given as needed to 50 (68.5%)patients in the regular and to 52 (75.4%) in the high dose group, but not to all patients.On the other hand, 37 (90.2%) of the regular dose group and 35 (85.4%) of the highdose group patients with the highest risk of rebleeding (Forrest Ia, Ib, and IIa) receivedendotherapy, a rate similar in another North European multicenter study (Schaffalitzkyde Muckadell et al. 1997). In metaanalyses a high dose of continuous infusion of omeprazole is effective, andalso other routes and doses of PPIs have reduced rebleeding rate, but none have hada significant effect on mortality (Leontiadis et al. 2005). By metaanalysis of Khuroo etal. (2005), ulcer deaths showed a significant reduction, while nonulcer deaths showedsignificant increase. In clinical trials a high dose of intravenous PPIs have beensuperior to placebo. Routine use of highdose intravenous PPIs prior to diagnosticendoscopy is recommended (Barkun et al. 2004b) and is a clinical practise in severalunits around the world. PPIs initiated prior to endoscopy for upper gastrointestinal

58
bleeding significantly reduced the proportion of patients with stigmata of recenthaemorrhage, but PPIs prior to endoscopy did not improve mortality, rebleeding or theneed for surgery (Dorward et al. 2006). Prospective studies using doses other thanhigh doses are needed, especially in connection with endoscopic therapy, because it isunclear what the lowest effective dose would be.
Effect of regular and high doses of omeprazole on the intragastric acidity in PUB(Study II)
The pHanalysis was available only on working days and in the Kuopio UniversityHospital participating in the study. There were only 15 patients willing to attend the pHmonitoring. In addition 2 of them discontinued the procedure by their own initiative. The regular dose of omeprazole (20 mg intravenously/day) is sufficient in decreasingthe intragastric acidity and raising the pH above 4 in patients with PUB. This should,theoretically hinder the dissolving of the fibrin clot (Berstad 1982; Green et al. 1978)produced primarily by endoscopic treatment and consequently prevent rebleeding.There was a pH difference during the first and second days between regular and highdose omeprazole dosage groups, but difference was diminished during the third day,indicating the efficacy of the regular dose of omeprazole in the long term. Furthermore,the fluctuation of the intragastric pH in the regular dose omeprazole group causes therise of intragastric pH temporarily above 6 for a considerably long time period, whichmight have a promoting effect on platelet aggregation and blood coagulation. On theother hand, the high dose of omeprazole maintains the intragastric pH above 6 for themost of the time. This does not seem necessary if a pH >4 is adequate to preventrebleeding. Intragastric pH above 4 seems to be sufficient to maintain haemostasis providing thatulcer bleeding is primarily ceased by endoscopic techniques. The clinical role of acidsuppression is thus probably more dependent upon the prevention of fibrin clotdissolution than on its effects on platelet aggregation and blood coagulation.
Risk factors and their combinations for acute PUB (Study III)
In general, studies of PUB risk factors have been focused on a single risk factor, oron the combination of H.pylori and NSAIDs. Only Stack et al. (2002) have analysed therole of occurrence of several possible risk factors (CagA/ H.pylori, the use of NSAID orASA, smoking) in patients with PUB. The role of alcohol and warfarin is also oftenneglected. According to the present results the highest risk was with previous duodenalulcer and H.pylori infection. In this study the high rate of H.pylori infection among PUBpatients can be partly due to the low rate of PPI treatment prior to diagnosticendoscopy. In earlier studies (Labenz et al. 1999; Santolaria et al. 1999) not excludingpatients with ongoing PPI treatment may have resulted in underestimation of the risk of

59
H.pylori. Consequently, H.pylori had a higher OR (8fold risk of PUB) in the presentstudy than in studies published earlier. Almost all of the cases and controls infected with H.pylori had CagA status in thisstudy. Therefore CagA did not increase the risk of bleeding. A similar frequency ofCagApositive H.pylori infection between peptic ulcer patients and nonulcer dyspepsiacontrols has also been found elsewhere (Evans et al. 1998; Go and Graham 1996;Hamlet et al. 1999; Park et al. 1998). These studies are in accordance with the presentresults suggesting that CagA is not a marker of a more virulent H.pylori strain withrespect to PUB. Although the overall use of NANSAID among the cases was not significantly differentfrom that among the controls, the onset of using NSAID was significantly more oftenacute and when used, NSAIDs were taken daily and with doses of 1 DDD by the PUBpatients. The findings are similar to earlier reports (Lanas et al. 2006; Weil et al. 1995). The control patients in the present study used more NSAIDs than control patients inother case control studies. The estimated risk for PUB of using NSAIDs is affected bythe relative consumption of the drugs among the cases and the controls. This probablyexplains why the risk of bleeding was lower than in earlier studies. Concurrent use ofNANSAIDs and ASA or 2 NSAIDs, recent beginning to use the NSAIDs, dailyconsumption and doses of 1 DDD of NANSAIDs were associated with an increasedrisk of PUB. ASA for prophylaxis of thrombosis and at analgetic doses were also riskfactors. Altogether 7.2% of the cases but none of the controls in the present study usedwarfarin. Therefore, numerical calculations of risk are not possible. In an earlier reportwarfarin doubled the risk for PUB (Lanas et al. 2006). The majority of PUB patients in this study were affected by at least one of the mainrisk factors, the use of NSAIDs or H.pylori infection, but the combination of risk factorsdid not potentiate the risk of bleeding. The combination seemed to increase the risk ofPUB in some studies (Aalykke et al. 1999; Labenz et al. 1999). A significant doseresponse for the risk of PUB with smoking and the use of ASA, ibuprofen andketoprofen was also found in that study. When we conducted the study 19941996 the selective inhibitors of cyclooxygenase2 (COX2) were not generally available. Their promise to displace traditional NSAIDsincluding acetylsalicylic acid (ASA) as antiinflammatory and pain medication with lessupper gastrointestinal complications has failed. The risk of serious cardiovascular sideeffects by COX2 inhibitors (HernandezDiaz et al. 2006; Grosser et al. 2006) hasrestricted their use to rare patients. Additionally, their gastrointestinal safety did notdiffer from traditional NSAIDs in reallife setting in general population (HelinSalmivaaraet al. 2007). Therefore the present study still represents the most usual clinicalbackground of patients with PUB.

60
Effect of regular and high doses of omeprazole on detection of H.pylori in PUB(Study IV)
PUB patients randomised to receive either the regular or the high dose ofomeprazole who were H.pylori positive by histology and/or the urease test wereanalysed. The finding that H.pylori is less often found in the gastric mucosa after a 3day administration of the high dose of omeprazole than after the regular dose indicateslack of detection or suppression of the bacteria. With either of the dose regimens theability to diagnose H.pylori infection by histology or the urease test decreased ascompared with pretreatment biopsies. If samples to find H.pylori are not taken before the treatment, the presence of thebacteria may be overlooked and left untreated. Later on in these patients a possiblerecurrence of ulcer is a true risk. It is therefore recommended that endoscopy withadequate biopsies for the diagnosis of H.pylori infection is performed before PPItreatment in cases with acute PUB. It is advisable primarily to use other acidsuppressing or neutralising agents other than PPI if diagnostic endoscopy ispostponed. If PPIs are given prior to diagnostic endoscopy, H.pylori should be testedafter cessation of the PPI treatment (Guell et al. 2006).

61
8. SUMMARY
A series of studies concerning modern drug treatment of PUB after endoscopictherapy and risk factors of PUB were undertaken. Because profound acid inhibitionfollowing endoscopic therapy may prevent rebleeding and reduce ulcer related deathsin PUB, the equivalence of a regular dose (20 mg once a day for 72 hours, n = 73) anda high dose of omeprazole (80 mg bolus + 8 mg/ h for 72 hours, n = 69) was tested in aprospective randomised double blind setting in patients with acute or recent bleeding ofwhom 102 (71.8%) had endoscopic treatment at preentry. The main results for regular vs. high dose omeprazole: rebleeding 6 (8.2%) vs. 8(11.6%), p = 0.002 for equivalence; emergency surgery: 3 (4.1%) vs. 5 (7.2%) and 30day mortality: 4 (5.5%) vs. 2 (2.9%). The regular dose of omeprazole seems to beequal to the high dose in preventing rebleeding, provided that endotherapy is given. In PUB, an intragastric pHlevel > 4 is considered necessary to prevent dissolving ofthe formed fibrin clot. PUB patients received either the regular dose or the high dose ofomeprazole for 72 hours. Monitoring of intragastric pH was performed for 3 days in 13of these randomised patients, 7 of them from the regular and 6 from the highdosegroup. The mean 24hour intragastric pH (regular vs. high dose) on day 1 was 4.9 ± 1.6 vs.6.3 ± 0.5, p = 0.035; on day 2 4.9 ± 1.8 vs. 6.7 ± 0.3, p = 0.001 and on day 3 5.7 ± 1.1vs. 6.7 ± 0.5, p = N.S. The medians of intragastric pH were: day 1 6 vs. 6.5, p = 0.082;day 2 5.8 vs. 6.8, p = 0.001 and day 3 6.2 vs. 6.8, p = 0.17. The proportion of the timethat the pH was 4 on day 1 was 29.2% ± 34.1 versus 5.4% ± 5.7, p = N.S. The regulardose of omeprazole raises the mean and median 24hour intragastric pH > 4 inpatients with PUB. This reduction in the acidity together with endoscopic therapy isprobably sufficient to maintain haemostasis. The high dose of omeprazole keeps thepH almost constantly > 6. NSAIDs including ASA (ASATP as thrombosis prophylaxis, ASAP as painmedication) and NANSAIDs, H.pylori infection, CagA strains of the bacteria andsmoking are reported risk factors for PUB, but their combined and dose effects arecontroversial. Therefore, a casecontrol study of PUB patients (n = 94) and controls (n= 94) of age and sex matched nonulcer patients attending elective endoscopy wasundertaken. A questionnaire on possible risk factors (previous GU or DU, use of anyNSAIDs, warfarin, alcohol and smoking) was completed. H.pylori was classified aspositive if histology or the urease test was positive. CagA antibodies of IgG class weredetermined by an immunoblot method.
H.pylori infection, the use of ASAP, ASATP, NANSAID with 1 defined daily dose,smoking 20 cigarettes daily and previous DU were independent risk factors for PUB.Previous DU, H.pylori, the use of any ASA and smoking explained the majority of thePUB episodes. At least 2 risk factors were present in 2/3 of the PUB patients. CagAwas present in 97% of the H.pyloripositive cases and in 96% of the respective

62
controls, and it was not associated with PUB. ASA, ibuprofen, ketoprofen and smokinghad a dosedependent association with PUB. It is unknown if a shortterm regular or high dose of omeprazole has an influence oncolonisation of H.pylori in the stomach. In PUB the effect of 3day treatment of twodifferent doses of omeprazole on colonisation of H.pylori in the stomach was studied. PUB patients received either the regular or the high dose of omeprazole for 72 hours.There were 101 H.pyloripositive patients, of whom 51 received the regular and 50 thehigh dose of omeprazole. H.pylori status was assessed by histology and urease test ofgastric biopsies at preentry and after the 3day treatment. With the high dose ofomeprazole, tests for the diagnosis of H.pylori became negative significantly moreoften than with the regular dose, 60% vs. 27.5%, p = 0.001 (any test), 67.6% vs.31.7%, p = 0.003 (histology) and 82.2% vs. 43.6%, p = 0.001 (urease test). Theconversion of the tests to H.pylori negative after the 3day treatment of omeprazolewas dose dependent.

63
9. CONCLUSIONS
1. The regular dose of omeprazole is as good at preventing rebleeding in PUB as thehigh dose following endoscopic treatment of bleeding and signs of recent bleeding inthe ulcer (Forrest III).
2. The regular dose of omeprazole raises the mean and median 24hour intragastric pH> 4 in patients with PUB. An intragastric pH above 4 seems to be sufficient to maintainhaemostasis following endoscopic therapy. The clinical role of acid suppression maybe more dependent upon the prevention of fibrin clot dissolution than on its effects onplatelet aggregation and blood coagulation. Therefore, maintenance of intragastric pHabove 6 is not necessary.
3. Previous duodenal ulcer, H.pylori infection and the consumption of any dose of ASAare independent risk factors for PUB. The role of CagA strains of H.pylori is probablyunimportant. Smoking and the use of ASA, ibuprofen and ketoprofen have significantdosedependent association with PUB. A PUB patient typically presents with at leastone of these risk factors: history of duodenal ulcer, H.pylori infection, the use of ASA,NANSAID dose 1 DDD and smoking 20 cigarettes. Two thirds of the PUB patientshave at least 2 of these risk factors. However, the combination of the risk factors didnot seem to potentiate the overall risk.
4. H.pylori is less often found in the gastric mucosa after a high dose of omeprazole for3 days than after a regular dose for the same period of time. Using either of the doseregimens for only 3 days decreases the ability to diagnose H.pylori infection whencompared to biopsies taken prior to omeprazole. The role of H.pylori may thus beoverlooked and necessary eradication not performed. This may result in ulcerrecurrence later.

64
10. REFERENCES
Aalykke C, Lauritsen JM, Hallas J, Reinholdt S, Krogfelt K, Lauritsen K. Helicobacterpylori and risk of ulcer bleeding among users of nonsteroidal antiinflammatory drugs: Acasecontrol study. Gastroenterology 1999; 6:13051309.
Andersen IB, Bonnevie O, Jorgensen T, Sorensen TI. Time trends for peptic ulcerdisease in Denmark, 19811993. Analysis of hospitalization register and mortality data.Scand J Gastroenterol 1998; 3:260266.
Andersen IB, Jorgensen T, Bonnevie O, Gronbaek M, Sorensen TI. Smoking andalcohol intake as risk factors for bleeding and perforated peptic ulcers: A populationbased cohort study. Epidemiology 2000; 4:434439.
Andreson H, Loivukene K, Sillakivi T, Maaroos HI, Ustav M, Peetsalu A, Mikelsaar M.Association of cagA and vacA genotypes of Helicobacter pylori with gastric diseases inEstonia. J Clin Microbiol 2002; 1:298300.
Andrews CN, Levy A, Fishman M, Hahn M, Atkinson K, Kwan P, Enns R. Intravenousproton pump inhibitors before endoscopy in bleeding peptic ulcer with highriskstigmata: A multicentre comparative study. Can J Gastroenterol 2005; 11:667671.
Aro P, Storskubb T, Ronkainen J, BollingSternevald E, Engstrand L, Vieth M et al.Peptic ulcer disease in a general adult population: The Kalixandra study: a randompopulationbased study. Am J Epidemiol 2006; 163:10251034.
Avgerinos A, Sgouros S, Viazis N, Vlachogiannakos J, Papaxoinis K, Bergele C,Sklavos P, Raptis SA. Somatostatin inhibits gastric acid secretion more effectively thanpantoprazole in patients with peptic ulcer bleeding: A prospective, randomized,placebocontrolled trial. Scand J Gastroenterol 2005; 5:515522.
Banatvala N, Mayo K, Megraud F, Jennings R, Deeks JJ, Feldman RA. The cohorteffect and Helicobacter pylori. J Infect Dis 1993; 1:219221.
Barkun A, Bardou M, Marshall JK, Nonvariceal Upper GI Bleeding ConferenceConcensus Group. Concensus recommendations for managing patients withnonvariceal upper gastrointestinal bleeding. Ann Intern Med 2003;139:843857.
Barkun A, Sabbah S, Enns R, Armstrong D, Gregor J, Fedorak RN, Rahme E, TouboutiY, Martel M, Chiba N et al. The Canadian registry on nonvariceal upper gastrointestinalbleeding and endoscopy (RUGBE): Endoscopic hemostasis and proton pump inhibitionare associated with improved outcomes in a reallife setting. Am J Gastroenterol2004a; 7:12381246.
Barkun A, Fallone CA, Chiba N, Fishman M, Flook N, Martin J, Rostom A, Taylor A,Nonvariceal Upper GI Bleeding Consensus Conference Group. A Canadian clinicalpractice algorithm for the management of patients with nonvariceal uppergastrointestinal bleeding. Can J Gastroenterol 2004b; 10:605609.
Berstad A, Holm HA, Kittang E. Experience with antipeptic agents. Scand JGastroenterol Suppl. 1979; 14 Suppl55:121123.

65
Berstad A. Management of acute upper gastrointestinal bleeding. Scand JGastroenterol Suppl. 1982; 14 Suppl75:103108.
Bertilsson L. Geographical/interracial differences in polymorphic drug oxidation.Current state of knowledge of cytochromes P450 (CYP) 2D6 and 2C19. ClinPharmacokinet 1995; 3:192209.
Blackwelder WC. In: Armitage P, Colton T, editors. Encyclopedia of biostatistics. NewYork: John Wiley& Sons Inc.; 1998.
Blatchford O, Davidson LA, Murray WR, Blatchford M, Pell J. Acute uppergastrointestinal haemorrhage in West of Scotland: Case ascertainment study. BMJ1997; 7107:510514.
Blaser M. Helicobacters are indigenous to the human stomach: duodenal ulceration isdue to changes in gastric microecology in the modern era. Gut 1998; 43:721727.
Bloom SR, Mortimer CH, Thorner MO, Besser GM, Hall R, GomezPan A, Roy VM,Russell RC, Coy DH, Kastin AJ et al. Inhibition of gastrin and gastricacid secretion bygrowthhormone releaseinhibiting hormone. Lancet 1974; 7889:11061109.
Bombardier C, Laine L, Reicin A, Shapiro D, BurgosVargas R, Davis B, Day R, FerrazMB, Hawkey CJ, Hochberg MC et al. Comparison of upper gastrointestinal toxicity ofrofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR study group. NEngl J Med 2000; 21:15201528.
Branicki FJ, Coleman SY, Lam TC, Schroeder D, Tuen HH, Cheung WL, Pritchett CJ,Lau PW, Lam SK, Hui WM. Hypotension and endoscopic stigmata of recenthaemorrhage in bleeding peptic ulcer: Risk models for rebleeding and mortality. JGastroenterol Hepatol 1992; 2:184190.
British Society of Gastroenterology Endoscopy, Committee. Nonvariceal uppergastrointestinal haemorrhage: Guidelines. Gut 2002; Suppl 4:16.
Brullet E, Campo R, Calvet X, Coroleu D, Rivero E, Simo Deu J. Factors related to thefailure of endoscopic injection therapy for bleeding gastric ulcer. Gut 1996a; 2:155158.
Brullet E, Calvet X, Campo R, Rue M, Catot L, Donoso L. Factors predicting failure ofendoscopic injection therapy in bleeding duodenal ulcer. Gastrointest Endosc 1996b;2:111116.
Brzozowski T, Konturek PC, Moran AP, Kwiecien S, Pajdo R, Konturek SJ, DrozdowiczD, Ptak A, Pawlik W, Hahn EG. Enhanced resistance of gastric mucosa to damagingagents in the rat stomach adapted to Helicobacter pylori lipopolysaccharide. Digestion2003; 4:195208.
Bugnoli M, Bayeli P, Rappuoli R, Pennatini C, Figura N, Crabtree JE. Inhibition ofHelicobacter pylori urease by omeprazole. Eur J Gastroenterol Hepatol 1993; 5:683685.

66
Calvet X, Vergara M, Brullet E, Gisbert JP, Campo R. Addition of a second endoscopictreatment following epinephrine injection improves outcome in highrisk bleedingulcers. Gastroenterology 2004; 2:441450.
Cederberg C, Rohss K, Lundborg P, Olbe L. Effect of once daily intravenous and oralomeprazole on 24hour intragastric acidity in healthy subjects. Scand J Gastroenterol1993; 2:179184.
Chan FK, Ching JY, Hung LC, Wong VW, Leung VK, Kung NN et al. Clopidogrelversus aspirin adn esomeprazole to prevent recurrent ulcer bleeding. N Engl J Med2005; 352:238244.
Chan FK, Wong VW, Suen BY, Wu JC, Ching JY, Hung LC, Hui AJ, Leung VK, LeeVW, Lai LH et al. Combination of a cyclooxygenase2 inhibitor and a protonpumpinhibitor for prevention of recurrent ulcer bleeding in patients at very high risk: Adoubleblind, randomised trial. Lancet 2007b; 9573:16211626.
Chan TA, Manson JA, Feskanich D, Stampfer MJ, Colditz GA, Charles S. Fuchs CS.Longterm Aspirin Use and Mortality in Women. Arch Intern Med 2007a; 167:562572.
Cheng HC, Kao AW, Chuang CH, Sheu BS. The efficacy of high and lowdoseintravenous omeprazole in preventing rebleeding for patients with bleeding pepticulcers and comorbid illnesses. Dig Dis Sci 2005; 7:11941201.
Chiu PW, Lam CY, Lee SW, Kwong KH, Lam SH, Lee DT, Kwok SP. Effect ofscheduled second therapeutic endoscopy on peptic ulcer rebleeding: a prospectiverandomised trial. Gut 2003; 52:14037.
Choudari CP, Rajgopal C, Elton RA, Palmer KR. Failures of endoscopic therapy forbleeding peptic ulcer: An analysis of risk factors. Am J Gastroenterol 1994; 11:19681972.
Chow LW, Gertsch P, Poon RT, Branicki FJ. Risk factors for rebleeding and death frompeptic ulcer in the very elderly. Br J Surg 1998; 1:121124.
Chung IK, Kim EJ, Lee MS, Kim HS, Park SH, Lee MH et al. Endoscopic factorspredisposing to rebleeding following endoscopic hemostasis in bleeding peptic ulcers.Endoscopy 2001; 33:96975.
Collen MJ, Santoro MJ, Chen YK. Giant duodenal ulcer. Evaluation of basal acidoutput, nonsteroidal antiinflammatory drug use, and ulcer complications. Dig Dis Sci1994; 5:11131116.
Collins R and Langman M. Treatment with histamine H2 antagonists in acute uppergastrointestinal hemorrhage. Implications of randomized trials. N Engl J Med 1985;11:660666.
Conn HO and Blitzer BL. Nonassociation of adrenocorticosteroid therapy and pepticulcer. N Engl J Med 1976; 9:473479.

67
Consensus conference: Therapeutic endoscopy and bleeding ulcers. JAMA 1989;10:13691372.
Consensus statement on therapeutic endoscopy and bleeding ulcers. Consensusdevelopment panel. Gastrointest Endosc 1990; 5 Suppl:S625.
Cook DJ, Guyatt GH, Salena BJ, Laine LA. Endoscopic therapy for acute nonvaricealupper gastrointestinal hemorrhage: A metaanalysis. Gastroenterology 1992; 1:139148.
Covacci A, Censini S, Bugnoli M, Petracca R, Burroni D, Macchia G, Massone A,Papini E, Xiang Z, Figura N. Molecular characterization of the 128kDaimmunodominant antigen of Helicobacter pylori associated with cytotoxicity andduodenal ulcer. Proc Natl Acad Sci USA 1993; 12:57915795.
Cover TL, Glupczynski Y, Lage AP, Burette A, Tummuru MK, PerezPerez GI, BlaserMJ. Serologic detection of infection with cagA+ Helicobacter pylori strains. J ClinMicrobiol 1995; 6:14961500.
Cullen DJ, Hawkey GM, Greenwood DC, Humphreys H, Shepherd V, Logan RF,Hawkey CJ. Peptic ulcer bleeding in the elderly: Relative roles of Helicobacter pyloriand nonsteroidal antiinflammatory drugs. Gut 1997; 4:459462.
de Abajo FJ, Montero D, Rodriguez LA, Madurga M. Antidepressants and risk of uppergastrointestinal bleeding. Basic Clin Pharmacol Toxicol 2006; 3:304310.
Donnelly MT, Richardson P, Hawkey CJ, Courtauld E, Stack WA. Dosedependenteffects of ketoprofen on the human gastric mucosa in comparison with ibuprofen.Aliment Pharmacol Ther 2000; 5:543549.
Dorward S, Sreedharan A, Leontiadis GI, Howden CW, Moayyedi P, Forman D. Protonpump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinalbleeding. Cochrane Database Syst Rev 2006; 4:CD005415 UI: 17054257.
Douthwaite AH, Lintott GA. Gastroscopic observation of the effect of aspirin and certainother substances on the stomach. Lancet 1938; 1:12221225.
Dunnet CW, Gent M. Significance testing to establish equivalence between treatmentswiht special reference to data in the form of 2x2 tables. Biometrics 1977; 33:593602.
Eaton KA, Brooks CL, Morgan DR, Krakowka S. Essential role of urease inpathogenesis of gastritis induced by Helicobacter pylori in gnotobiotic piglets. InfectImmun 1991; 7:24702475.
Ellershaw JE and Kelly MJ. Corticosteroids and peptic ulceration. Palliat Med 1994;4:313319.
Enns R, Andrews CN, Fishman M, Hahn M, Atkinson K, Kwan P, Levy A. Description ofprescribing practices in patients with upper gastrointestinal bleeding receivingintravenous proton pump inhibitors: A multicentre evaluation. Can J Gastroenterol2004; 9:567571.

68
Enns RA, Gagnon YM, Barkun AN, Armstrong D, Gregor JC, Fedorak RN, RUGBEInvestigators G. Validation of the Rockall scoring system for outcomes from nonvariceal upper gastrointestinal bleeding in a Canadian setting. World J Gastroenterol2006; 48:77797785.
Evans DG, Queiroz DM, Mendes EN, Evans DJ,Jr. Helicobacter pylori cagA status ands and m alleles of vacA in isolates from individuals with a variety of H. pyloriassociatedgastric diseases. J Clin Microbiol 1998; 11:34353437.
Fischer I, Madsen MR, Thomsen H, Host V, Wara P. Peptic ulcer hemorrhage: Factorspredisposing to recurrence. Scand J Gastroenterol 1994; 5:414418.
Forbes GM, Glaser ME, Cullen DJ, Warren JR, Christiansen KJ, Marshall BJ, CollinsBJ. Duodenal ulcer treated with Helicobacter pylori eradication: Sevenyear followup.Lancet 1994; 8892:258260.
Forrest JA, Finlayson ND, Shearman DJ. Endoscopy in gastrointestinal bleeding.Lancet 1974; 7877:394397.
Fukuda Y. Suppression of Helicobacter pylori colonization with omeprazole. Scand JGastroenterol Suppl. 1996; 31Suppl214:5455.
Fullarton GM and Murray WR. Prediction of rebleeding in peptic ulcers by visualstigmata and endoscopic doppler ultrasound criteria. Endoscopy 1990; 2:6871.
Furuta T, Ohashi K, Kosuge K, Zhao XJ, Takashima M, Kimura M, Nishimoto M, HanaiH, Kaneko E, Ishizaki T. CYP2C19 genotype status and effect of omeprazole onintragastric pH in humans. Clin Pharmacol Ther 1999; 5:552561.
Gabriel SE, Jaakkimainen L, Bombardier C. Risk for serious gastrointestinalcomplications related to use of nonsteroidal antiinflammatory drugs. A metaanalysis.Ann Intern Med 1991; 10:787796.
Gachet C. ADP receptors of platelets and their inhibition. Thromb Haemost 2001;1:222232.
Gagnon YM, Levy AR, Eloubeidi MA, Arguedas MR, Rioux KP, Enns RA. Costimplications of administering intravenous proton pump inhibitors to all patientspresenting to the emergency department with peptic ulcer bleeding. Value Health 2003;4:457465.
Garcia Rodriguez LA and Barreales Tolosa L. Risk of upper gastrointestinalcomplications among users of traditional NSAIDs and COXIBs in the generalpopulation. Gastroenterology 2007; 2:498506.
Gillen D, Wirz AA, Neithercut WD, Ardill JE, McColl KE. Helicobacter pylori infectionpotentiates the inhibition of gastric acid secretion by omeprazole. Gut 1999; 4:468475.
Gisbert JP, Gonzalez L, de Pedro A, Valbuena M, Prieto B, Llorca I, Briz R, KhorramiS, GarciaGravalos R, Pajares JM. Helicobacter pylori and bleeding duodenal ulcer:
69
Prevalence of the infection and role of nonsteroidal antiinflammatory drugs. Scand JGastroenterol 2001a; 7:717724.
Gisbert JP, Gonzalez L, Calvet X, Roque M, Gabriel R, Pajares JM. Proton pumpinhibitors versus H2antagonists: A metaanalysis of their efficacy in treating bleedingpeptic ulcer. Aliment Pharmacol Ther 2001b; 7:917926.
Gisbert JP, Legido J, Castel I, Trapero M, Cantero J, Mate J, Pajares JM. Riskassessment and outpatient management in bleeding peptic ulcer. J Clin Gastroenterol2006; 2:129134.
Gisbert JP and Abraira V. Accuracy of Helicobacter pylori diagnostic tests in patientswith bleeding peptic ulcer: A systematic review and metaanalysis. Am J Gastroenterol2006; 4:848863.
Go MF and Graham DY. Presence of the cagA gene in the majority of Helicobacterpylori strains is independent of whether the individual has duodenal ulcer orasymptomatic gastritis. Helicobacter 1996; 2:107111.
Godil A, DeGuzman L, Schilling RC,3rd, Khan SA, Chen YK. Recent nonsteroidal antiinflammatory drug use increases the risk of early recurrence of bleeding in patientspresenting with bleeding ulcer. Gastrointest Endosc 2000; 2:146151.
Gonzalez CA, Pena S, Capella G. Clinical usefulness of virulence factors ofHelicobacter pylori as predictors of the outcomes of infection. What is the evidence?Scand J Gastroenterol 2003; 9:905915.
Goodwin CS, Armstrong JA, Marshall BJ. Campylobacter pyloridis, gastritis, and pepticulceration. J Clin Pathol 1986; 4:353365.
Graham DY. Campylobacter pylori and peptic ulcer disease. Gastroenterology 1989; 2Suppl:615625.
Graham DY, McCullough A, Sklar M, Sontag SJ, Roufail WM, Stone RC, Bishop RH,Gitlin N, Cagliola AJ, Berman RS. Omeprazole versus placebo in duodenal ulcerhealing. The United States experience. Dig Dis Sci 1990; 1:6672.
Graham DY. Helicobacter pylori: Its epidemiology and its role in duodenal ulcerdisease. J Gastroenterol Hepatol. 1991; 2:105113.
Graham DY, Adam E, Reddy GT, Agarwal JP, Agarwal R, Evans DJ,Jr, Malaty HM,Evans DG. Seroepidemiology of Helicobacter pylori infection in India. Comparison ofdeveloping and developed countries. Dig Dis Sci 1991; 8:10841088.
Graham DY, Hepps KS, Ramirez FC, Lew GM, Saeed ZA. Treatment of Helicobacterpylori reduces the rate of rebleeding in peptic ulcer disease. Scand J Gastroenterol1993; 11:939942.
Graham DY, Genta RM, Graham DP, Crabtree JE. Serum CagA antibodies inasymptomatic subjects and patients with peptic ulcer: Lack of correlation of IgG

70
antibody in patients with peptic ulcer or asymptomatic Helicobacter pylori gastritis. JClin Pathol 1996a; 10:829832
Graham DY, Genta R, Evans DG, Reddy R, Clarridge JE, Olson CA, Edmonds AL,Siepman N. Helicobacter pylori does not migrate from the antrum to the corpus inresponse to omeprazole. Am J Gastroenterol 1996b; 10:21202124.
Graham DY and Malaty HM. Alendronate gastric ulcers. Aliment Pharmacol Ther 1999;4:515519.
Green FW,Jr, Kaplan MM, Curtis LE, Levine PH. Effect of acid and pepsin on bloodcoagulation and platelet aggregation. A possible contributor prolonged gastroduodenalmucosal hemorrhage. Gastroenterology 1978; 1:3843.
Griffin MR, Piper JM, Daugherty JR, Snowden M, Ray WA. Nonsteroidal antiinflammatory drug use and increased risk for peptic ulcer disease in elderly persons.Ann Intern Med 1991; 4:257263.
Grino P, Pascual S, Such J, Casellas JA, Niveiro M, Andreu M, Saez J, Grino E,Palazon JM, Carnicer F, and others. Comparison of diagnostic methods forHelicobacter pylori infection in patients with upper gastrointestinal bleeding. Scand JGastroenterol 2001; 12:12541258.
Grosser T, Fries S, FitzGerald GA. Biological basis for the cardiovascularconsequences of COX2 inhibition: Therapeutic challenges and opportunities. J ClinInvest 2006; 1:415.
Grosso C, Rossi A, Gambitta P, Bini M, Zanasi G, Pirone Z, Arcidiacono R. Nonbleeding visible vessel treatment: Perendoscopic injection therapy versus omeprazoleinfusion. Scand J Gastroenterol 1995; 9:872875.
Guell M, Artigau E, Esteve V, SanchezDelgado J, Junquera F, Calvet X. Usefulness ofa delayed test for the diagnosis of Helicobacter pylori infection in bleeding peptic ulcer.Alim Pharm Ther 2006; 23:5359.
Guglielmi A, Ruzzenente A, Sandri M, Kind R, Lombardo F, Rodella L, Catalano F, deManzoni G, Cordiano C. Risk assessment and prediction of rebleeding in bleedinggastroduodenal ulcer. Endoscopy 2002; 10:778786.
Gutthann SP, Garcia Rodriguez LA, Raiford DS. Individual nonsteroidal antiinflammatory drugs and other risk factors for upper gastrointestinal bleeding andperforation. Epidemiology 1997; 1:1824.
Hallas J, Dall M, Andries A, Andersen BS, Aalykke C, Hansen JM, Andersen M,Lassen AT. Use of single and combined antithrombotic therapy and risk of seriousupper gastrointestinal bleeding: Population based casecontrol study. BMJ 2006;333:72630.
Hamlet A, Thoreson AC, Nilsson O, Svennerholm AM, Olbe L. Duodenal Helicobacterpylori infection differs in cagA genotype between asymptomatic subjects and patientswith duodenal ulcers. Gastroenterology 1999; 2:259268.

71
Hasselgren G, Lind T, Lundell L, Aadland E, Efskind P, Falk A, Hyltander A, SöderlundC, Eriksson S, Fernström P. Continuous intravenous infusion of omeprazole in elderlypatients with peptic ulcer bleeding. Results of a placebocontrolled multicenter study.Scand J Gastroenterol 1997; 4:328333.
Hasselgren G, Blomqvist A, Eriksson S, Henningsson A, Lundell L. Short and long termcourse of elderly patients with peptic ulcer bleedinganalysis of factors influencing fataloutcome. Eur J Surg 1998; 9:685691.
HelinSalmivaara A, Klaukka T, Huupponen R. Heavy users of nonsteroidal antiinflammatory drugs: A nationwide prescription database study in Finland. Eur J ClinPharmacol 2003; 56:477482.
HelinSalmivaara A, Saarelainen S, Grönroos JM, Vesalainen R, Klaukka T,Huupponen R. Risk of upper gastrointestinal events with the use of various NSAIDs: Acasecontrol study in a general population. Scand J Gastroenterol 2007; 42:92332.
Henriksson AE, Edman AC, Nilsson I, Bergqvist D, Wadstrom T. Helicobacter pyloriand the relation to other risk factors in patients with acute bleeding peptic ulcer. ScandJ Gastroenterol 1998; 10:10301033.
HernandezDiaz S and Rodriguez LA. Association between nonsteroidal antiinflammatory drugs and upper gastrointestinal tract bleeding/perforation: An overviewof epidemiologic studies published in the 1990s. Arch Intern Med 2000; 14:20932099.
HernandezDiaz S, VarasLorenzo C, Garcia Rodriguez LA. Nonsteroidal antiinflammatory drugs and the risk of acute myocardial infarction. Basic Clin PharmacolToxicol 2006; 3:266274.
Higham J, Kang JY, Majeed A. Recent trends in admissions and mortality due to pepticulcer in England: Increasing frequency of haemorrhage among older subjects. Gut2002; 4:460464.
Holme JB, Nielsen DT, FunchJensen P, Mortensen FV. Transcatheter arterialembolization in patients with bleeding duodenal ulcer: An alternative to surgery. ActaRadiol 2006; 3:244247.
Hsieh YH, Lin HJ, Tseng GY, Perng CL, Wang K, Lo WC, Chang FY, Lee SD. Poorresponders to intravenous omeprazole in patients with peptic ulcer bleeding.Hepatogastroenterology 2004; 55:316319.
Hsu PI, Lin XZ, Chan SH, Lin CY, Chang TT, Shin JS, Hsu LY, Yang CC, Chen KW.Bleeding peptic ulcer risk factors for rebleeding and sequential changes in endoscopicfindings. Gut 1994; 6:746749.
Hsu PI, Lai KH, Tseng HH, Lin CK, Lo GH, Cheng JS, Chan HH, Chen GC, Jou HS,Peng NJ et al. Risk factors for presentation with bleeding in patients with Helicobacterpylorirelated peptic ulcer diseases. J Clin Gastroenterol 2000; 4:386391.
Hsu PI, Lo GH, Lo CC, Lin CK, Chan HH, Wu CJ, Shie CB, Tsai PM, Wu DC, WangWM et al. Intravenous pantoprazole versus ranitidine for prevention of rebleeding after

72
endoscopic hemostasis of bleeding peptic ulcers. World J Gastroenterol 2004;24:36663669.
Huang JQ, Sridhar S, Hunt RH. Role of Helicobacter pylori infection and nonsteroidalantiinflammatory drugs in pepticulcer disease: A metaanalysis. Lancet 2002;9300:1422.
Hudson N, Faulkner G, Smith SJ, Langman MJ, Hawkey CJ, Logan RF. Late mortalityin elderly patients surviving acute peptic ulcer bleeding. Gut 1995a; 2:177181.
Hudson N, Faulkner G, Smith SJ, Logan RF, Hawkey CJ. Morbidity and treatment inelderly patients surviving hospital admission with bleeding peptic ulcer. Gut 1995b;2:182186.
Hui WM, Lam SK, Ho J, Lai CL, Lok AS, Ng MM, Lau WY, Branicki FJ. Effect ofomeprazole on duodenal ulcerassociated antral gastritis and Helicobacter pylori. DigDis Sci 1991; 5:577582.
Hunt RH, Armstrong D, James C, Chowdhury SK, Yuan Y, Fiorentini P, Taccoen A,Cohen P. Effect on intragastric pH of a PPI with a prolonged plasma halflife:Comparison between tenatoprazole and esomeprazole on the duration of acidsuppression in healthy male volunteers. Am J Gastroenterol 2005; 9:19491956.
Hurlimann S, Abbuhl B, Inauen W, Halter F. Comparison of acid inhibition by either oralhighdose ranitidine or omeprazole. Aliment Pharmacol Ther 1994; 2:193201.
Imhof M, Ohmann C, Hartwig A, Thon KP, Hengels KJ, Roher HD. Which peptic ulcersbleed? results of a casecontrol study. DUSUK study group. Scand J Gastroenterol1997; 2:131138.
Imhof M, Ohmann C, Roher HD, Glutig H, DUESUC study group. Endoscopic versusoperative treatment in highrisk ulcer bleeding patients results of a randomised study.Langenbecks Arch Surg 2003; 910:327336.
Imperiale TF and Birgisson S. Somatostatin or octreotide compared with H2antagonists and placebo in the management of acute nonvariceal uppergastrointestinal hemorrhage: A metaanalysis. Ann Intern Med 1997; 12:10621071.
Inadomi J, Koch J, Cello JP. Longterm followup of endoscopic treatment for bleedinggastric and duodenal ulcers. Am J Gastroenterol 1995; 7:10651068.
Ishizaki T and Horai Y. Review article: Cytochrome P450 and the metabolism of protonpump inhibitorsemphasis on rabeprazole. Aliment Pharmacol Ther 1999; Suppl 3:2736.
Jaramillo JL, Galvez C, Carmona C, Montero JL, Mino G. Prediction of furtherhemorrhage in bleeding peptic ulcer. Am J Gastroenterol 1994; 12:21352138.
Javid G, Masoodi I, Zargar SA, Khan BA, Yatoo GN, Shah AH, Gulzar GM, Sodhi JS.Omeprazole as adjuvant therapy to endoscopic combination injection sclerotherapy fortreating bleeding peptic ulcer. Am J Med 2001; 4:280284.

73
Jensen DM, Kovacs TO, Jutabha R, Machicado GA, Gralnek IM, Savides TJ, Smith J,Jensen ME, Alofaituli G, Gornbein J. Randomized trial of medical or endoscopictherapy to prevent recurrent ulcer hemorrhage in patients with adherent clots.Gastroenterology 2002; 2:407413.
Jian R, Cortot A, Ducrot F, Jobin G, Chayvialle JA, Modigliani R. Effect of ethanolingestion on postprandial gastric emptying and secretion, biliopancreatic secretions,and duodenal absorption in man. Dig Dis Sci 1986; 6:604614.
Johnston JH. The sentinel clot and invisible vessel: Pathologic anatomy of bleedingpeptic ulcer. Gastrointest Endosc 1984; 5:313315.
Jung HK, Son HY, Jung SA, Yi SY, Yoo K, Kim DY, Moon IH, Lee HC. Comparison oforal omeprazole and endoscopic ethanol injection therapy for prevention of recurrentbleeding from peptic ulcers with nonbleeding visible vessels or fresh adherent clots.Am J Gastroenterol 2002; 7:17361740.
Kahi CJ, Jensen DM, Sung JJ, Bleau BL, Jung HK, Eckert G, Imperiale TF. Endoscopictherapy versus medical therapy for bleeding peptic ulcer with adherent clot: A metaanalysis. Gastroenterology 2005; 3:855862.
Kane S, Borisov NN, Brixner D. Pharmacoeconomic evaluation of gastrointestinal tractevents during treatment with risedronate or alendronate: A retrospective cohort study.Am J Managed Care 2004; 10:S216226.
Kaplan RC, Heckbert SR, Koepsell TD, Rosendaal FR, Psaty BM. Use of calciumchannel blockers and risk of hospitalized gastrointestinal tract bleeding. Arch InternMed 2000; 12:18491855.
Kaviani MJ, Hashemi MR, Kazemifar AR, Roozitalab S, Mostaghni AA, Merat S,AlizadehNaini M, Yarmohammadi H. Effect of oral omeprazole in reducing rebleedingin bleeding peptic ulcers: A prospective, doubleblind, randomized, clinical trial. AlimentPharmacol Ther 2003; 2:211216.
Kemppainen H, Räihä I, Sourander L. Clinical presentation of peptic ulcer in theelderly. Gerontology 1997; 5:283288.
Khuroo MS, Yattoo GN, Javid G, Khan BA, Shah AA, Gulzar GM, Sodi JS. Acomparison of omeprazole and placebo for bleeding peptic ulcer. N Engl J Med 1997;15:10541058.
Khuroo MS, Khuroo MS, Farahat KL, Kagevi IE. Treatment with proton pump inhibitorsin acute nonvariceal upper gastrointestinal bleeding: A metaanalysis. J GastroenterolHepatol 2005; 1:1125.
Kiilerich S, Rannem T, Elsborg L. Effect of intravenous infusion of omeprazole andranitidine on twentyfourhour intragastric pH in patients with a history of duodenalulcer. Digestion 1995; 1:2530.

74
Knekt P, Teppo L, Aromaa A, Rissanen H, Kosunen TU. Helicobacter pylori IgA andIgG antibodies, serum pepsinogen I and the risk of gastric cancer: Changes in the riskwith extended followup period. Int J Cancer 2006; 119:702705.
Kokkola A, Louhimo J, Puolakkainen P, Alfthan H, Haglund C, Rautelin H. Helicobacterpylori infection and low serum pepsinogen I level as risk factors for gastric carcinoma.World J Gastroenterol 2005; 7:10321036.
Konturek SJ, Bielaski W, Plonka M, Pawlik T, Pepera J, Konturek PC, Czarnecki J,Penar A, Jedrychowski W. Helicobacter pylori, nonsteroidal antiinflammatory drugsand smoking in risk pattern of gastroduodenal ulcers. Scand J Gastroenterol 2003;9:923930.
Kosunen TU, Aromaa A, Knekt P, Salomaa A, Rautelin H, Lohi P, Heinonen P.Helicobacter antibodies in 1973 and 1994 in the adult population of Vammala, Finland.Epidemiol Infect 1997; 119:2934.
Kravetz RE. Antacid powders. Am J Gastroenterol 2003; 4:924925.
Kubba AK, Choudari C, Rajgopal C, Ghosh S, Palmer KR. Reduced longterm survivalfollowing major peptic ulcer haemorrhage. Br J Surg 1997; 2:265268.
Kurata JH and Corboy ED. Current peptic ulcer time trends. An epidemiological profile.J Clin Gastroenterol 1988; 3:259268.
Kuttila K, Havia T, Pekkala E, AliMelkkilä T. Surgery of acute peptic ulcerhaemorrhage. Ann Chir Gynaecol 1991; 1:2629.
Labenz J, Tillenburg B, Peitz U, Idstrom JP, Verdu EF, Stolte M, Borsch G, Blum AL.Helicobacter pylori augments the pHincreasing effect of omeprazole in patients withduodenal ulcer. Gastroenterology 1996; 3:725732.
Labenz J, Peitz U, Leusing C, Tillenburg B, Blum AL, Borsch G. Efficacy of primedinfusions with high dose ranitidine and omeprazole to maintain high intragastric pH inpatients with peptic ulcer bleeding: A prospective randomised controlled study. Gut1997; 1:3641.
Labenz J, Peitz U, Kohl H, Kaiser J, Malfertheiner P, Hackelsberger A, Borsch G.Helicobacter pylori increases the risk of peptic ulcer bleeding: A casecontrol study. ItalJ Gastroenterol 1999; 2:110115.
Laine L and Peterson WL. Bleeding peptic ulcer. N Engl J Med 1994; 11:717727.
Laine L, Freeman M, Cohen H. Lack of uniformity in evaluation of endoscopicprognostic features of bleeding ulcers. Gastrointest Endosc 1994; 4:411417.
Lanas A, Artal A, Blas JM, Arroyo MT, LopezZaborras J, Sainz R. Effect of parenteralomeprazole and ranitidine on gastric pH and the outcome of bleeding peptic ulcer. JClin Gastroenterol 1995; 2:103106.

75
Lanas A, Fuentes J, Benito R, Serrano P, Bajador E, Sainz R. Helicobacter pyloriincreases the risk of upper gastrointestinal bleeding in patients taking lowdose aspirin.Aliment Pharmacol Ther 2002; 4:779786.
Lanas A, GarciaRodriguez LA, Arroyo MT, Gomollon F, Feu F, Gonzalez Perez A,Zapata E, Bastida G, Rodrigo L, Santolaria S et al. Risk of upper gastrointestinal ulcerbleeding associated with selective COX2 inhibitors, traditional nonaspirin NSAIDs,aspirin, and combinations. Gut 2006; 55:17318.
Lanas A and Ferrandez A. Inappropriate prevention of NSAIDinduced gastrointestinalevents among longterm users in the elderly. Drugs Aging 2007; 2:121131
Langman MJ. Ulcer complications associated with antiinflammatory drug use. What isthe extent of the disease burden? Pharmacoepidemiol Drug Saf 2001; 1:1319.
Lassen A, Hallas J, Schaffalitzky de Muckadell OB. Complicated and uncomplicatedpeptic ulcers in a Danish county 19932002: A populationbased cohort study. Am JGastroenterol 2006; 5:945953.
Lau JY, Sung JJ, Lee KK, Yung MY, Wong SK, Wu JC, Chan FK, Ng EK, You JH, LeeCW, and others. Effect of intravenous omeprazole on recurrent bleeding afterendoscopic treatment of bleeding peptic ulcers. N Engl J Med 2000; 5:310316.
Lee JM, Breslin NP, Fallon C, O'Morain CA. Rapid urease tests lack sensitivity inHelicobacter pylori diagnosis when peptic ulcer disease presents with bleeding. Am JGastroenterol 2000; 5:11661170.
Leivonen M and Kivilaakso E. Peptic ulcer bleeding today: Risk factors andcharacteristics of the disease. Scand J Gastroenterol 1991; 10:10131019.
Leontiadis GI, Sharma VK, Howden CW. Systematic review and metaanalysis ofproton pump inhibitor therapy in peptic ulcer bleeding. BMJ 2005; 330:568586.
Leontiadis GI, Sharma VK, Howden CW. Proton pump inhibitor therapy for peptic ulcerbleeding: Cochrane collaboration metaanalysis of randomized controlled trials. MayoClin Proc 2007; 3:286296.
Levine JE, Leontiadis GI, Sharma VK, Howden CW. Metaanalysis: The efficacy ofintravenous H2receptor antagonists in bleeding peptic ulcer. Aliment Pharmacol Ther2002; 6:11371142.
Lewis SC, Langman MJ, Laporte JR, Matthews JN, Rawlins MD, Wiholm BE. Doseresponse relationships between individual nonaspirin nonsteroidal antiinflammatorydrugs (NANSAIDs) and serious upper gastrointestinal bleeding: A metaanalysis basedon individual patient data. Br J Clin Pharmacol 2002; 3:320326.
Liao CC, Lee CL, Lai YC, Huang SH, Lee SC, Wu CH, Tu TC, Chen TK, Bai CH.Accuracy of three diagnostic tests used alone and in combination for detectingHelicobacter pylori infection in patients with bleeding gastric ulcers. Chin Med J 2003;12:18211826.

76
Liberopoulos EN, Tselepis MS, Archimandritis AD, Kiskinis D, Cokkinos D, MikhailidisDP. Upper gastrointestinal haemorrhage complicating antiplatelet treatment with aspirinand/or clopidogrel: Where are we now? Platelet 2006; 17:16.
Lin HJ, Lee FY, Kang WM, Tsai YT, Lee SD, Lee CH. Heat probe thermocoagulationand pure alcohol injection in massive peptic ulcer haemorrhage: A prospective,randomised controlled trial. Gut 1990; 7:753757.
Lin HJ, Perng CL, Lee FY, Lee CH, Lee SD. Clinical courses and predictors forrebleeding in patients with peptic ulcers and nonbleeding visible vessels: Aprospective study. Gut 1994; 10:13891393.
Lin HJ, Wang K, Perng CL, Lee FY, Lee CH, Lee SD. Natural history of bleeding pepticulcers with a tightly adherent blood clot: A prospective observation. GastrointestEndosc 1996; 5:470473.
Lin HJ, Lo WC, Lee FY, Perng CL, Tseng GY. A prospective randomized comparativetrial showing that omeprazole prevents rebleeding in patients with bleeding peptic ulcerafter successful endoscopic therapy. Arch Intern Med 1998; 1:5458.
Lin HJ, Hsieh YH, Tseng GY, Perng CL, Chang FY, Lee SD. A prospective,randomized trial of endoscopic hemoclip versus heater probe thermocoagulation forpeptic ulcer bleeding. Am J Gastroenterol 2002; 9:22502254.
Lin HJ, Lo WC, Cheng YC, Perng CL. Role of intravenous omeprazole in patients withhighrisk peptic ulcer bleeding after successful endoscopic epinephrine injection: Aprospective randomized comparative trial. Am J Gastroenterol 2006; 3:500505.
Logan RP, Walker MM, Misiewicz JJ, Gummett PA, Karim QN, Baron JH. Changes inthe intragastric distribution of Helicobacter pylori during treatment with omeprazole. Gut1995; 1:1216.
Longstreth GF. Epidemiology of hospitalization for acute upper gastrointestinalhemorrhage: A populationbased study. Am J Gastroenterol 1995; 2:206210.
Lu H, Yamaoka Y, Graham DY. Helicobacter pylori virulence factors: Facts andfantasies. Curr Opin Gastroenterol 2005; 6:653659.
Ma L, Chow JY, Cho CH. Effects of cigarette smoking on gastric ulcer formation andhealing: Possible mechanisms of action. J Clin Gastroenterol 1998; Suppl 1:S806.
Maity P, Biswas K, Roy S, Banerjee RK, Bandyopadhyay U. Smoking and thepathogenesis of gastroduodenal ulcer recent mechanistic update. Mol Cell Biochem2003; 12:329338.
Mant JW, Richards SH, Hobbs FD, Fitzmaurice D, Lip GY, Murray E, Banting M,Fletcher K, Rahman J, Allan T, and others. Protocol for Birmingham atrial fibrillationtreatment of the aged study (BAFTA): A randomised controlled trial of warfarin versusaspirin for stroke prevention in the management of atrial fibrillation in an elderly primarycare population. BMC Cardiovasc Disord 2003; 3:9. http://www.biomedcentral.com/14712261/3/9

77
Marshall BJ and Warren JR. Unidentified curved bacilli in the stomach of patients withgastritis and peptic ulceration. Lancet 1984; 8390:13111315.
Marzio L, Biasco G, Cifani F, DeFanis C, Falcucci M, Ferrini G, Grossi L, Iannetti G,Larcinese G, Lattanzio R. Short and longterm omeprazole for the treatment andprevention of duodenal ulcer, and effect on Helicobacter pylori. Am J Gastroenterol1995; 12:21722176.
McColl KE, elNujumi AM, Chittajallu RS, Dahill SW, Dorrian CA, elOmar E, Penman I,Fitzsimons EJ, Drain J, Graham H. A study of the pathogenesis of Helicobacter pylorinegative chronic duodenal ulceration. Gut 1993; 6:762768.
McGowan CC, Cover TL, Blaser MJ. The proton pump inhibitor omeprazole inhibitsacid survival of Helicobacter pylori by a ureaseindependent mechanism. Republishedfrom Gastroenterology. 1994;107:73843; PMID: 8076759. Gastroenterology 1994;5:15731578.
Merki HS and WilderSmith CH. Do continuous infusions of omeprazole and ranitidineretain their effect with prolonged dosing? Gastroenterology 1994; 1:6064.
Messer J, Reitman D, Sacks HS, Smith H,Jr, Chalmers TC. Association ofadrenocorticosteroid therapy and pepticulcer disease. N Engl J Med 1983; 1:2124.
Messmann H, Schaller P, Andus T, Lock G, Vogt W, Gross V et al. Effect ofprogrammed endoscopic followup examinations on the rebleeding rate of gastric orduodenal peptic ulcers treated by injection therapy: a prospective, randomizedcontrolled trial. Endoscopy 1998; 30:5839.
Meyer UA. Metabolic interactions of the protonpump inhibitors lansoprazole,omeprazole and pantoprazole with other drugs. Eur J Gastroenterol Hepatol 1996;Suppl1:S215.
Millat B, Hay JM, Valleur P, Fingerhut A, Fagniez PL. Emergency surgical treatment forbleeding duodenal ulcer: Oversewing plus vagotomy versus gastric resection, acontrolled randomized trial. French associations for surgical research. World J Surg1993; 5:568573.
Mueller X, Rothenbuehler JM, Amery A, Harder F. Factors predisposing to furtherhemorrhage and mortality after peptic ulcer bleeding. J Am Coll Surg 1994; 4:457461.
Mäkelä J, Laitinen S, Kairaluoma MI. Complications of peptic ulcer disease before andafter the introduction of H2receptor antagonists. Hepatogastroenterology 1992; 2:144148.
Mäkelä JT, Kiviniemi H, Laitinen ST. Randomized trial of endoscopic injection sclerosiswith ethanolamine oleate and ethanol for bleeding peptic ulcer. Scand J Gastroenterol1996; 31:10591062.
Netzer P, Gaia C, Sandoz M, Huluk T, Gut A, Halter F, Husler J, Inauen W. Effect ofrepeated injection and continuous infusion of omeprazole and ranitidine on intragastricpH over 72 hours. Am J Gastroenterol 1999; 2:351357.

78
Ng TM, Fock KM, Khor JL, Teo EK, Sim CS, Tan AL, Machin D. Nonsteroidal antiinflammatory drugs, Helicobacter pylori and bleeding gastric ulcer. Aliment PharmacolTher 2000; 2:203209.
Nielsen GL, Sorensen HT, Mellemkjoer L, Blot WJ, McLaughlin JK, TageJensen U,Olsen JH. Risk of hospitalization resulting from upper gastrointestinal bleeding amongpatients taking corticosteroids: A registerbased cohort study. Am J Med 2001; 7:541545.
Nomura A, Stemmermann GN, Chyou PH, PerezPerez GI, Blaser MJ. Helicobacterpylori infection and the risk for duodenal and gastric ulceration. Ann Intern Med 1994;12:977981.
Nomura AM, PerezPerez GI, Lee J, Stemmermann G, Blaser MJ. Relation betweenHelicobacter pylori cagA status and risk of peptic ulcer disease. Am J Epidemiol 2002;11:10541059.
O'Brien JD, Day SJ, Burnham WR. Controlled trial of small bipolar probe in bleedingpeptic ulcers. Lancet 1986; 8479:464467.
Ohmann C, Imhof M, Röher HD. Trends in peptic ulcer bleeding and surgical treatment.World J Surg 2000; 3:284293.
Ohmann C, Imhof M, Ruppert C, Janzik U, Vogt C, Frieling T, Becker K, Neumann F,Faust S, Heiler K et al. Timetrends in the epidemiology of peptic ulcer bleeding. ScandJ Gastroenterol 2005; 8:914920.
Oi M and Sakurai Y. The location of duodenal ulcer. Gastroenterology 1959; 1:6064.
Oi M, Oshida K, Sugimura S. The location of gastric ulcer. Gastroenterology 1959;1:4556.
Ovaska JT, Haapiainen RK, Voutilainen PE, Linnankivi AP. Acute surgical treatment ofbleeding peptic ulcer. A retrospective analysis of 193 patients. Ann Chir Gynaecol1992; 1:3336.
Paimela H, Paimela L, MyllykangasLuosujärvi R, Kivilaakso E. Current features ofpeptic ulcer disease in Finland: Incidence of surgery, hospital admissions and mortalityfor the disease during the past twentyfive years. Scand J Gastroenterol 2002; 4:399403.
Palmer ED. The vigorous diagnostic approach to uppergastrointestinal tracthemorrhage. A 23year prospective study of 1,4000 patients. JAMA 1969; 8:14771480.
Park SM, Park J, Kim JG, Cho HD, Cho JH, Lee DH, Cha YJ. Infection withHelicobacter pylori expressing the cagA gene is not associated with an increased riskof developing peptic ulcer diseases in Korean patients. Scand J Gastroenterol 1998;9:923927.

79
Parsonnet J, Friedman GD, Vandersteen DP, Chang Y, Vogelman JH, Orentreich N,Sibley RK. Helicobacter pylori infection and the risk of gastric carcinoma. N Engl J Med1991; 16:11271131.
Patchett SE, Enright H, Afdhal N, O'Connell W, O'Donoghue DP. Clot lysis by gastricjuice: An in vitro study. Gut 1989; 12:17041707.
Patchett SE and O'Donoghue DP. Pharmacological manipulation of gastric juice:Thrombelastographic assessment and implications for treatment of gastrointestinalhaemorrhage. Gut 1995; 3:358362.
Peura DA. The problem of Helicobacter pylorinegative idiopathic ulcer disease.Baillieres Best Pract Res Clin Gastroenterol. 2000; 1:109117.
Pilotto A, Leandro G, Di Mario F, Franceschi M, Bozzola L, Valerio G. Role ofHelicobacter pylori infection on upper gastrointestinal bleeding in the elderly: A casecontrol study. Dig Dis Sci 1997; 3:586591.
Pitcher JL. Therapeutic endoscopy and bleeding ulcers: Historical overview.Gastrointest Endosc 1990; 5 Suppl:S27.
Post PN, Kuipers EJ, Meijer GA. Declining incidence of peptic ulcer but not of itscomplications: A nationwide study in the Netherlands. Aliment Pharmacol Ther 2006;11:15871593.
Rajgopal C, Lessels A, Palmer KR. Mechanism of action of injection therapy forbleeding peptic ulcer. Br J Surg 1992; 8:782784.
RalphEdwards A and Himal HS. Bleeding gastric and duodenal ulcers: Endoscopictherapy versus surgery. Can J Surg 1992; 2:177181.
Rauws EA, Langenberg W, Houthoff HJ, Zanen HC, Tytgat GN. Campylobacterpyloridisassociated chronic active antral gastritis. A prospective study of its prevalenceand the effects of antibacterial and antiulcer treatment. Gastroenterology 1988; 1:3340.
Rockall TA, Logan RF, Devlin HB, Northfield TC. Incidence of and mortality from acuteupper gastrointestinal haemorrhage in the United Kingdom. Steering committee andmembers of the national audit of acute upper gastrointestinal haemorrhage. BMJ 1995;6999:222226.
Rockall TA, Logan RF, Devlin HB, Northfield TC. Risk assessment after acute uppergastrointestinal haemorrhage. Gut 1996a; 3:316321.
Rockall TA, Logan RF, Devlin HB, Northfield TC. Selection of patients for earlydischarge or outpatient care after acute upper gastrointestinal haemorrhage. Nationalaudit of acute upper gastrointestinal haemorrhage. Lancet 1996b; 9009:11381140.
Rogers PN, Murray WR, Shaw R, Brar S. Surgical management of bleeding gastriculceration. Br J Surg 1988; 1:1617.

80
Rosenstock S, Jorgensen T, Bonnevie O, Andersen L. Risk factors for peptic ulcerdisease: A population based prospective cohort study comprising 2416 Danish adults.Gut 2003; 2:186193.
Ruigomez A, Garcia Rodriguez LA, Hasselgren G, Johansson S, Wallander MA.Overall mortality among patients surviving an episode of peptic ulcer bleeding. JEpidemiol Community Health 2000; 2:130133.
Rutgeerts P, Rauws E, Wara P, Swain P, Hoos A, Solleder E, Halttunen J, Dobrilla G,Richter G, Prassler R. Randomised trial of single and repeated fibrin glue comparedwith injection of polidocanol in treatment of bleeding peptic ulcer. Lancet 1997;9079:692696.
Sacks HS, Chalmers TC, Blum AL, Berrier J, Pagano D. Endoscopic hemostasis. Aneffective therapy for bleeding peptic ulcers. JAMA 1990; 4:494499.
Saeed ZA, Winchester CB, Michaletz PA, Woods KL, Graham DY. A scoring system topredict rebleeding after endoscopic therapy of nonvariceal upper gastrointestinalhemorrhage, with a comparison of heat probe and ethanol injection. Am JGastroenterol 1993; 11:18421849.
Saeed ZA, Ramirez FC, Hepps KS, Cole RA, Graham DY. Prospective validation of theBaylor bleeding score for predicting the likelihood of rebleeding after endoscopichemostasis of peptic ulcers. Gastrointest Endosc 1995; 6:561565.
Sagar M, Seensalu R, Tybring G, Dahl ML, Bertilsson L. CYP2C19 genotype andphenotype determined with omeprazole in patients with acidrelated disorders with andwithout Helicobacter pylori infection. Scand J Gastroenterol 1998; 10:10341038.
Sagar M, Tybring G, Dahl ML, Bertilsson L, Seensalu R. Effects of omeprazole onintragastric pH and plasma gastrin are dependent on the CYP2C19 polymorphism.Gastroenterology 2000; 3:670676.
Sanderson JD, Taylor RF, Pugh S, Vicary FR. Specialized gastrointestinal units for themanagement of upper gastrointestinal haemorrhage. Postgrad Med J 1990; 778:654656.
Santander C, Gravalos RG, GomezCedenilla A, Cantero J, Pajares JM. Antimicrobialtherapy for Helicobacter pylori infection versus longterm maintenance antisecretiontreatment in the prevention of recurrent hemorrhage from peptic ulcer: Prospectivenonrandomized trial on 125 patients. Am J Gastroenterol 1996; 8:15491552.
Santolaria S, Lanas A, Benito R, PerezAisa M, Montoro M, Sainz R. Helicobacterpylori infection is a protective factor for bleeding gastric ulcers but not for bleedingduodenal ulcers in NSAID users. Aliment Pharmacol Ther 1999; 11:15111518.
Savage RL, Moller PW, Ballantyne CL, Wells JE. Variation in the risk of peptic ulcercomplications with nonsteroidal antiinflammatory drug therapy. Arthritis Rheum. 1993;1:8490.
81
Schaffalitzky de Muckadell OB, Havelund T, Harling H, Boesby S, Snel P, VreeburgEM, Eriksson S, Fernström P, Hasselgren G. Effect of omeprazole on the outcome ofendoscopically treated bleeding peptic ulcers. Randomized doubleblind placebocontrolled multicentre study. Scand J Gastroenterol 1997; 4:320327.
Scheindlin S. A century of ulcer medicines. Mol Interv 2005; 4:201206.
Schubert TT, Bologna SD, Nensey Y, Schubert AB, Mascha EJ, Ma CK. Ulcer riskfactors: Interactions between Helicobacter pylori infection, nonsteroidal use, and age.Am J Med 1993; 4:413418.
Shonekas H, Ahrens H, Pannewick U. Comparison of two doses of intravenouspantoprazole in peptic ulcer bleeding. Gastroenterol 1999; 116:A305.
Singer JD, Willett JB. Applied longitudinal dataanalysis modelling change and eventoccurrence. New York: Oxford University Press 2003.
Sipponen P, Helske T, Järvinen P, Hyvärinen H, Seppälä K, Siurala M. Fall in theprevalence of chronic gastritis over 15 years: analysis of outpatient series in Finlandfrom 1977, 1985, and 1992. Gut 1994; 35:116771.
Smalley WE, Ray WA, Daugherty JR, Griffin MR. No association between calciumchannel blocker use and confirmed bleeding peptic ulcer disease. Am J Epidemiol1998; 4:350354.
Somerville K, Faulkner G, Langman M. Nonsteroidal antiinflammatory drugs andbleeding peptic ulcer. Lancet 1986; 8479:462464.
Soplepmann J, Udd M, Peetsalu A, Palmu A. Acute upper gastrointestinalhaemorrhage in Central Finland province, Finland, and in Tartu county, Estonia. AnnChir Gynaecol 1997a; 3:222228.
Soplepmann J, Peetsalu A, Peetsalu M, Tein A, Juhola M. Peptic ulcer haemorrhage inTartu county, Estonia: Epidemiology and mortality risk factors. Scand J Gastroenterol1997b; 12:11951200.
Stack WA, Atherton JC, Hawkey GM, Logan RF, Hawkey CJ. Interactions betweenHelicobacter pylori and other risk factors for peptic ulcer bleeding. Aliment PharmacolTher 2002; 3:497506.
Stolte M and Bethke B. Elimination of Helicobacter pylori under treatment withomeprazole. Z Gastroenterol 1990; 6:271274.
Storey DW, Bown SG, Swain CP, Salmon PR, Kirkham JS, Northfield TC. Endoscopicprediction of recurrent bleeding in peptic ulcers. N Engl J Med 1981; 16:915916.
Sung JJ, Chan FK, Lau JY, Yung MY, Leung WK, Wu JC, Ng EK, Chung SC. Theeffect of endoscopic therapy in patients receiving omeprazole for bleeding ulcers withnonbleeding visible vessels or adherent clots: A randomized comparison. Ann InternMed 2003; 4:237243.

82
Swain CP, Storey DW, Bown SG, Heath J, Mills TN, Salmon PR, Northfield TC,Kirkham JS, O'Sullivan JP. Nature of the bleeding vessel in recurrently bleeding gastriculcers. Gastroenterology 1986; 3:595608.
Tabibian N. Acute gastrointestinal bleeding in anticoagulated patients: A prospectiveevaluation. Am J Gastroenterol 1989; 1:1012.
Tarnawski A, Hollander D, Stachura J, Klimczyk B, Mach T, Bogdal J. Alcohol injury tothe normal human gastric mucosa: Endoscopic, histologic and functional assessment.Clin Invest Med 1987; 3:259263.
Tarnawski A, Stachura J, Krause WJ, Douglass TG, Gergely H. Quality of gastric ulcerhealing: A new, emerging concept. J Clin Gastroenterol 1991; Suppl 1:S427.
Teenan RP and Murray WR. Late outcome of undersewing alone for gastric ulcerhaemorrhage. Br J Surg 1990; 7:811812.
Teyssen S, Chari ST, Scheid J, Singer MV. Effect of repeated boluses of intravenousomeprazole and primed infusions of ranitidine on 24hour intragastric pH in healthyhuman subjects. Dig Dis Sci 1995; 2:247255.
Thomopoulos KC, Mitropoulos JA, Katsakoulis EC, Vagianos CE, Mimidis KP,Hatziargiriou MN, Nikolopoulou VN. Factors associated with failure of endoscopicinjection haemostasis in bleeding peptic ulcers. Scand J Gastroenterol 2001; 6:664668.
Thomopoulos KC, Mimidis KP, Theocharis GJ, Gatopoulou AG, Kartalis GN,Nikolopoulou VN. Acute upper gastrointestinal bleeding in patients on longterm oralanticoagulation therapy: Endoscopic findings, clinical management and outcome.World J Gastroenterol 2005; 9:13651368.
Tilvis RS, Vuoristo M, Varis K. Changed profile of peptic ulcer disease in hospitalpatients during 19691984 in Finland. Scand J Gastroenterol 1987; 10:12381244.
Toyoda H, Nakano S, Takeda I, Kumada T, Sugiyama K, Osada T, Kiriyama S, SugaT. Transcatheter arterial embolization for massive bleeding from duodenal ulcers notcontrolled by endoscopic hemostasis. Endoscopy 1995; 4:304307.
Tramer MR, Moore RA, Reynolds DJ, McQuay HJ. Quantitative estimation of rareadverse events which follow a biological progression: A new model applied to chronicNSAID use. Pain 2000; 12:169182.
Tzourmakliotis D, Economou M, Manolakopoulos S, Bethanis S, Bergele C,Lakoumentas J, Sclavos P, Milionis H, Margeli A, Vogiatzakis E et al. Clinicalsignificance of cytotoxinassociated gene A status of Helicobacter pylori among nonsteroidal antiinflammatory drug users with peptic ulcer bleeding: A multicenter casecontrol study. Scand J Gastroenterol 2004; 12:11801185.
van Leerdam ME, Vreeburg EM, Rauws EA, Geraedts AA, Tijssen JG, Reitsma JB,Tytgat GN. Acute upper GI bleeding: Did anything change? Time trend analysis of

83
incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. AmJ Gastroenterol 2003; 98:14941499.
van Rensburg CJ, Hartmann M, Thorpe A, Venter L, Theron I, Luhmann R, Wurst W.Intragastric pH during continuous infusion with pantoprazole in patients with bleedingpeptic ulcer. Am J Gastroenterol 2003; 12:26352641.
Veijola L, Sankila A, Rautelin H, Kosunen TU, Sipponen P, Hyvärinen H, Tilvis R,Sarna S, Arkkila PE, Seppälä K. Clinical significance of widespread gastric metaplasiain the duodenal bulb. J Clin Gastroenterol 2006; 6:510514.
Verdu EF, Fraser R, Armstrong D, Blum AL. Effects of omeprazole and lansoprazoleon 24hour intragastric pH in Helicobacter pyloripositive volunteers. Scand JGastroenterol 1994; 12:10651069.
Vergara M, Calvet X, Gisbert JP. Epinephrine injection versus epinephrine injectionand a second endoscopic method in high risk bleeding ulcers. Cochrane DatabaseSyst Rev 2997; 2: 005584.
Villanueva C, Balanzo J, Espinos JC, Domenech JM, Sainz S, Call J, Vilardell F.Prediction of therapeutic failure in patients with bleeding peptic ulcer treated withendoscopic injection. Dig Dis Sci 1993; 11:20622070.
Villanueva C and Balanzo J. A practical guide to the management of bleeding ulcers.Drugs 1997; 3:389403.
von Holstein CC, Eriksson SB, Kallen R. Tranexamic acid as an aid to reducing bloodtransfusion requirements in gastric and duodenal bleeding. Br Med J 1987; 6563:710.
Vorobjova T, Maaroos HI, Uibo R, Wadström T, Wood WG, Sipponen P. Helicobacterpylori: Histological and serological study on gastric and duodenal ulcer patients inEstonia. Scand J Gastroenterol Suppl. 1991; 26Suppl186:8489.
Voutilainen M, Mäntynen T, Färkkilä M, Juhola M, Sipponen P. Impact of nonsteroidalantiinflammatory drug and aspirin use on the prevalence of dyspepsia anduncomplicated peptic ulcer disease. Scand J Gastroenterol 2001; 36:81721.
Vreeburg EM, Levi M, Rauws EA, Deventer SJ, Snel P, Bartelsman JW, Ten Cate JW,Tytgat GN. Enhanced mucosal fibrinolytic activity in gastroduodenal ulcer haemorrhageand the beneficial effect of acid suppression. Aliment Pharmacol Ther 2001; 5:639646.
Wallace JL. How do NSAIDs cause ulcer disease? Baillieres Best Pract Res ClinGastroenterol 2000; 1:147159.
Wara P, Berg V, Amdrup E. Factors influencing mortality in patients with bleeding ulcer.Review of 7 years' experience preceding therapeutic endoscopy. Acta Chir Scand.1983; 8:775785.
Wara P. Endoscopic prediction of major rebleeding a prospective study of stigmata ofhemorrhage in bleeding ulcer. Gastroenterology 1985; 5:12091214.

84
Weil J, ColinJones D, Langman M, Lawson D, Logan R, Murphy M, Rawlins M,Vessey M, Wainwright P. Prophylactic aspirin and risk of peptic ulcer bleeding. BMJ1995; 6983:827830.
Weil J, Langman MJ, Wainwright P, Lawson DH, Rawlins M, Logan RF, Brown TP,Vessey MP, Murphy M, ColinJones DG. Peptic ulcer bleeding: Accessory risk factorsand interactions with nonsteroidal antiinflammatory drugs. Gut 2000; 1:2731.
Weil PH and Buchberger R. From Billroth to PCV: A century of gastric surgery. World JSurg 1999; 7:736742.
Welch CE, Rodkey GV, von Ryll Gryska P. A thousand operations for ulcer disease.Ann Surg 1986; 4:454467.
Wessinger S, Kaplan M, Choi L, Williams M, Lau C, Sharp L, Crowell MD,Keshavarzian A, Jones MP. Increased use of selective serotonin reuptake inhibitors inpatients admitted with gastrointestinal haemorrhage: A multicentre retrospectiveanalysis. Aliment Pharmacol Ther 2006; 7:937944.
Wheatley KE and Dykes PW. Upper gastrointestinal bleeding when to operate.Postgrad Med J 1990; 781:926931.
Williams RA, Vartany A, Davis IP, Wilson SE. Impact of endoscopic therapy onoutcome of operation for bleeding peptic ulcers. Am J Surg 1993; 6:712714.
Wotherspoon AC, OrtizHidalgo C, Falzon MR, Isaacson PG. Helicobacter pyloriassociated gastritis and primary Bcell gastric lymphoma. Lancet 1991; 8776:11751176.
Wu CY, Poon SK, Chen GH, Chang CS, Yeh HZ. Interaction between Helicobacterpylori and nonsteroidal antiinflammatory drugs in peptic ulcer bleeding. Scand JGastroenterol 1999; 3:234237.
Yamamoto I, Fukuda Y, Okui M, Tamura K, Shimoyama T. Proton pump inhibitors forHelicobacter pylori eradication in patients with peptic ulcer. J Clin Gastroenterol 1995;Suppl 1:S3842.
Younossi ZM, Strum WB, Schatz RA, Teirstein PS, Cloutier DA, Spinks TJ. Effect ofcombined anticoagulation and lowdose aspirin treatment on upper gastrointestinalbleeding. Dig Dis Sci 1997; 1:7982.
Yuan Y, Tsoi K, Hunt RH. Selective serotonin reuptake inhibitors and risk of upper GIbleeding: Confusion or confounding? Am J Med 2006; 9:719727.
Zargar SA, Javid G, Khan BA, Yattoo GN, Shah AH, Gulzar GM, Sodhi JS, Mujeeb SA,Khan MA, Shah NA, and others. Pantoprazole infusion as adjuvant therapy toendoscopic treatment in patients with peptic ulcer bleeding: Prospective randomizedcontrolled trial. J Gastroenterol Hepatol 2006; 4:716721.

85
ORIGINAL PUBLICATIONS (IIV)
Udd M, Miettinen P, Palmu A, Heikkinen M, Janatuinen E, Pasanen P,Tarvainen R, Kairaluoma MV, Lohman M, Mustonen H, Julkunen R.Regulardose versus highdose omeprazole in peptic ulcer bleeding: Aprospective randomized doubleblind study. Scand J Gastroenterol. 2001;36:13328.
Udd M, Töyry J, Miettinen P, Vanninen E, Mustonen H, Julkunen R. Theeffect of regular and high doses of omeprazole on the intragastric acidity inpatients with bleeding peptic ulcer treated endoscopically: A clinical trial withcontinuous intragastric pH monitoring. Eur J Gastroenterol Hepatol. 2005;17:13516.
Udd M, Miettinen P, Palmu A, Heikkinen M, Janatuinen E, Pasanen P,Tarvainen R, Mustonen H, Julkunen R. Analysis of risk factors and theircombinations in acute gastroduodenal ulcer bleeding. A casecontrol study.Accepted for publication in Scand J Gastroenterol.
Udd M, Miettinen P, Palmu A, Julkunen R. Effect of shortterm treatmentwith regular or high doses of omeprazole on the detection of Helicobacterpylori in bleeding peptic ulcer patients. Scand J Gastroenterol. 2003; 38:58893.

Kuopio University Publications D. Medical Sciences D 400. Vasara, Anna. Autologous chondrocyte transplantation: Properties of the repair tissue in humans and in animal models. 2007. 92 p. Acad. Diss. D 401. Andrulionyte, Laura. Transcription factors as candidate genes for type 2 diabetes: studies on peroxisome proliferator-activated receptors, hepatic nuclear factor 4α and PPARγ coactivator Iα. 2007. 112 p. Acad. Diss. D 402. Raatikainen, Kaisa. Health behavioural and social risks in obstetrics: effect on pregnancy outcome. 2007. 100 p. Acad. Diss. D 403. Kinnunen, Tuure. The role of T cell recognition in the immune response against lipocalin allergens: prospects for immunotherapy. 2007. 76 p. Acad. Diss. D 404. Gratz, Silvia. Aflatoxin binding by probiotics : experimental studies on intestinal aflatoxin transport, metabolism and toxicity. 2007. 85 p. Acad. Diss. D 405. Ming, Zhiyong. Upper limb musculoskeletal disorders with special reference to sympathetic nerve functions and tactile sensation. 2007. 91 p. Acad. Diss. D 406. Timonen, Leena. Group-based exercise training in mobility impaired older women. 2007. 91 p. Acad. Diss. D 407. Mättö, Mikko. B cell receptor signaling in human B cells. 2007. 74 p. Acad. Diss. D 408. Polychronaki, Nektaria. Biomarkers of aflatoxin exposure and a dietary intervention: studies in infants and children from Egypt and Guinea and young adults from China. 2007. 114 p. Acad. Diss. D 409. Mursu, Jaakko. The role of polyphenols in cardiovascular diseases. 2007. 88 p. Acad. Diss. D 410. Wlodkowic, Donald. Selective targeting of apoptotic pathways in follicular lymphoma cells. 2007. 97 p. Acad. Diss. D 411. Skommer, Joanna. Novel approaches to induce apoptosis in human follicular lymphoma cell lines - precinical assessment. 2007. 80 p. Acad. Diss. D 412. Kemppinen, Kaarina. Early maternal sensitivity: continuity and related risk factors. 2007. 80 p. Acad. Diss. D 413. Sahlman, Janne. Chondrodysplasias Caused by Defects in the Col2a1 Gene. 2007. 86 p. Acad. Diss. D 414. Pitkänen, Leena. Retinal pigment epithelium as a barrier in drug permeation and as a target of non-viral gene delivery. 2007. 75 p. Acad. Diss. D 415. Suhonen, Kirsi. Prognostic Role of Cell Adhesion Factors and Angiogenesis in Epithelial Ovarian Cancer. 2007. 123 p. Acad. Diss.