marketa marvanova, pharmd, phd, bcgp, bcpp, fascp
TRANSCRIPT

2/25/21
1
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
Supported in part by an educational grant from the ASCP Foundation. March 9-11, 2021
Psychiatric Disorders in the Older Adult
Marketa Marvanova, PharmD, PhD, BCGP, BCPP, FASCPDean and Professor
University of Montana, College of Health/Skaggs School of Pharmacy
1
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Meet The SpeakerDr. Marvanova serves as Professor and Dean of theSkaggs School of Pharmacy and Acting Dean of theCollege of Health of the University of Montana. She is aBoard Certified Psychiatric Pharmacist and GeriatricPharmacist and Fellow of the American Society ofConsultant Pharmacists. She has completed M.S.(Pharm), Pharm.D. and Ph.D. (PathologicalNeurobiochemistry) degrees from the Charles University(Czech Republic) as well as a Ph.D. (Neuropharmacology)from the University of Eastern Finland. She alsocompleted a medical research fellowship inneuropharmacology at Vanderbilt University School ofMedicine and a Parkinson’s disease traineeship atNorthwestern University. Her clinical expertise isneuropsychiatry and geriatrics and she has practiced in avariety of inpatient and outpatient clinical settings.
Insert photo of speaker
2

2/25/21
2
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Disclosure
• Dr. Marvanova serves as a clinical pharmacy specialist consultant in neurology and psychiatry for Lexicomp, Wolters Kluwer.
• Dr. Marvanova will discuss off-label use of select medications
3
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Learning Objectives
1. Determine therapeutic options for depression, anxiety, sleep disturbances and substance abuse in the older adult.
2. Interpret psychiatric clinical findings and incorporate functional status into therapeutic decision-making.
3. Resolve and/or prevent psychiatric medication-related problems.4. Apply psychiatric therapy recommendations and person-specific
goals to senior patient cases.
4

2/25/21
3
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
Supported in part by an educational grant from the ASCP Foundation. March 9-11, 2021
Depression
5
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Major Depression Disorder (MDD) in Older Adults• Depression is a true and treatable medical condition, not a normal
part of aging• Commonly misdiagnosed or undertreated in older adults• Less likely remission and high relapse rate• More common in older adults
• Co-occurrence with medical illnesses and disabilities
• Prevalence: • 1-5% in community dwelling older adults• 11.5-15% in those who require home healthcare or are hospitalized
• Suicide rates in older adults are the highest of any age group Centers for Disease Control and Prevention, “Depression is Not a Normal Part of Growing Older,” Division of Population Health, updates January 31, 2017. Available at https://www.cdc.gov/aging/mentalhealth/depression.htm. Accessed on January 22, 2020.Kok RB, Reynolds CF. JAMA 2017; 317(20):2114-22.
6

2/25/21
4
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
MDD is a Chronic Disorder
70%90%
0%
50%
100%
After 1 Episode After 2 Episodes After 3 Episodes
Prob
abili
ty o
f Rec
urre
nt E
piso
des
J Clin Psychiatry 1991; 52:(suppl 5):28-34.
50%
Recurrent episodesSingle episode
7
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
• ≥ 5 of the following most days for at least 2 weeks and one of them needs to be depressed mood or anhedonia
S: changes in Sleep
I: decreased Interest (anhedonia)*
G: excessive Guilt
E: decreased Energy
C: decreased ConcentrationA: Appetite change
P: Psychomotor change
S: Suicidal thoughts & behavior
MDD Diagnostic Criteria (DSM-5)
• Not due to effects of substances or general medical conditionsAmerican Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
8
2/25/21
5
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Secondary Depression (Induced)Drug-induced Depression• Corticosteroids (>80 mg/day prednisone equivalents)
• Efavirenz (2.74 mcg/L during long-term treatment)
• Progesterone
• Isotretinoin
• Interferon-a and Interferon-b
• Levetiracetam
• Natalizumab
Medical Causes of Depression• Hypothyroidism
• Folate deficiency
Ganzini, L., et al. Drugs & Aging 1993; 3:147–58.Botts S, Ryan M. Drug-induced Diseases: Prevention, Detection, and Management, 2010. Available at https://www.ashp.org/-/media/assets/pharmacy-practice/resource-centers/medications-suicidality/drug-induced-diseases.ashx. Accessed on January 25, 2020.
9
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
MDD Clinical Presentation in Older AdultsGeriatric Specific Symptoms of Depression:
• “Depression without sadness “o May not report depression or sadness
• Often have somatic complaints: fatigue or pain• Memory complaints• Insomnia• Reduction in appetite/weight loss• Social withdrawal
Kaplan M, Huguet N, McFarland B, et al. Psychology of Men & Masculinity 2012; 13: 65-74.Kok RB, Reynolds CF. JAMA 2017; 317(20):2114-22.
10

2/25/21
6
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Depression with Melancholic Features
• More common in older age than younger depressed population• Severe form of depression characterized by anhedonia plus
additional 3 features:o Increased morning severityo Early morning awakening (at least 2 hours before usual awakening
time)o Marked psychomotor retardation (slowing) and/or agitationo Significant anorexia or weight losso Excessive or inappropriate guilt
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013Gili M. PLoS One 2012; 7(10): e48200.
11
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Depression Evaluation/Diagnosis• Medical and family history
• Important to rule out bipolar depression• Social history (substance use)• Labs: CBC, CMP, TSH, folate level, & urine drug screen • Medication review• Physical & mental state examination (MSE)
o Depression rating scales (self- or clinician-administered)
a) Presenceb) Severityc) Response to therapy
12

2/25/21
7
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Depression Rating Scale Administrator/Rater #Q T (min)
Hamilton Rating Scale for Depression (HAM-D)Clinical trials and practice: response, severity
Response ≥ 50% score reductionRemission score ≤ 7
Clinician/Trained rater 17 20-30
Beck Depression Inventory (BDI)Response ≥ 50% score reductionRemission score ≤ 10
Self-rated 21 5-10
Quick Inventory of Depressive Symptomatology (QIDS-SR) or (QIDS-C)Clinical trials and practice: response, severity
Response ≥ 50% score reductionRemission score ≤ 5
Self-ratedClinician rated
16 5-10
Patient Health Questionnaire (PHQ)-9Diagnostic and rating scale in clinical practice or trials
Response ≥ 50% score reductionRemission score ≤ 5
Self-rated 9 5
Geriatric Depression Scale (GDS)-15Clinical practice screening tool and monitor depression
Response ≥ 50% score reductionRemission score ≤ 5
Self-rated 15 5
13
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
The Patient Healthcare Questionnaire (PHQ-9)
Scoring:0-4: No depression5-9: Mild depression10-14: Moderate depression15-19: Moderately severe depression≥20: Severe depression
91-94% Specificity
Maurer D, Raymond T, Davis B. Am Fam Physician 2018; 98(8):508-15. http://www.integration.samhsa.gov/images/res/PHQ%20-%20Questions.pdf. Accessed on February 7, 2021.2020.
14

2/25/21
8
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
The Patient Healthcare Questionnaire (PHQ-2)
Scoring:≥ 3 suggestive of depression
78-92% SpecificityKroenke, K., Spitzer, R.L., Williams, J.B. Medical Care 2003; 41:1284–92.https://aidsetc.org/sites/default/files/resources_files/PHQ-2_English.pdf. Accessed on February 7, 2021.
15
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
The Geriatric DepressionScale (GDS-15)
Does not assess suicidality
Scoring:0-4: No depression5-10: Mild depression> 10: Severe depression
92% sensitivity 89% specificity
Yesavage, et al. J Psychiatr Res 1983; 17:37-49https://dementiapathways.ie/_filecache/0c8/57e/37-gds.pdf. Accessed on February 7, 2021.
16

2/25/21
9
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Depression Assessment in Dementia• The Cornell Scale for Depression in Dementia
(CSDD) • 19-items • ~20 min• Administered in a semi-structured interview
format to residents (also direct observation) and to caregivers independently.
• Information is obtained from interview of a caregiver as well as from direct observation and interview of the patient
• The final ratings represent the rater's clinical impression
• Scores of ≥12 indicate probable depression
Alexopoulos GA, et al. Biol Psych 1988; 23:271-84.
https://cgatoolkit.ca/Uploads/ContentDocuments/cornell_scale_depression.pdf. Accessed on February 7, 2021
17
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Classes of Antidepressants
Depression: Decreased level of 5-HT, NE & DA in the brain
Therapeutic Class/CategorySSRIs (selective serotonin reuptake inhibitors)
SNRIs (serotonin-norepinephrine reuptake inhibitors)
SSRI + partial 5-HT1A agonist (vilazodone)
SSRI + 5-HT1A agonist, 5-HT1B partial agonist, 5-HT3, 5-HT1D and 5-HT7 antagonist (vortioxetine)
NDRI (norepinephrine-dopamine reuptake inhibitors)
TCAs (tricyclic antidepressants)
MAOIs (monoamine-oxidase inhibitors)
Serotonin modulator (mirtazapine)
5-HT2A receptor antagonists & reuptake inhibitors (trazodone; nefazodone)
5-HT=serotonin; NE=norepinephrine; DA=dopamine
18

2/25/21
10
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Potential Neurotransmitter-Specific Adverse Effects
• Noradrenergic (NE)- Dry mouth- Increased BP- Increased HR- Hyperhidrosis- Urinary hesitation- Insomnia
• Dopaminergic (DA)- Psychomotor activation- Nervousness
• Serotonergic (5-HT)- GI upset- Sexual dysfunction- Irritability and jitteriness- Insomnia- Headache - Suppression of dopamine
release (possibility of Extrapyramidal symptoms
19
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
MDD
SSRI SNRI MIRT BUP
MIRT = mirtazapine; BUP=bupropion; VTX = vortioxetine
CitalopramEscitalopramFluoxetineSertraline Paroxetine
VenlafaxineDesvenlafaxineDuloxetineLevomilnacipranMilnacipran (just for fibromyalgia)
1. Adequate trial: 6-12 weeks2. Adequate Dose
3. Assessment using standardized tools (PHQ-9; QIDS; GDS-15)
VTX
Marvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.Canadian Network for Mood and Anxiety Treatments (CANMAT). Can J Psychiatry 2016; 61(9):504-603.American Psychiatric Association (APA). Practice guideline for the treatment of patients with major depressive disorder, 3rd ed. Arlington, Virginia: American Psychiatric Association, 2010.Veterans Health Administration and Department of Defense. VA/DoD practice guideline for the management of major depressive d, version 3.0. Washington, D.C.: Veterans Health Administration and the Department of Defense, 2016.
• Psychotherapy (CBT) could be used as monotherapy in mild-moderate
• St. John’s wort could be considered as therapy in mild depression if a patient prefers natural therapy (however watch for interactions as it is CYP3A4 inducer)
20

2/25/21
11
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Patient-Centered Approach to Selection of Antidepressant
Patient Factors
• Depression clinical features
• Comorbid conditions
• Patient preference
• Response & adverse effects during previous use
Medication Factors
• Efficacy to treat other conditions outside of MDD
• Pharmacokinetics
• Pharmacodynamics
• Tolerability/Safety/Interactions
• Simplicity of use
• Cost/formularyMarvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.Canadian Network for Mood and Anxiety Treatments (CANMAT). Can J Psychiatry 2016; 61(9):504-603.
21
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Selective Serotonin Reuptake Inhibitor (SSRIs)Adverse Effects: appetite change, gastrointestinal (N/V/D), sexual side effects, falls, hyponatremia, risk of GI bleeds, serotonin syndrome (SS), tremor, and headache
Citalopram* Max dose of 20 mg in older adults due to QTc prolongation risk
Escitalopram Risk of QTc prolongation
Fluoxetine Long half-life (~72 hours), active metabolite does notrequire taper; Less weight gain; ↑drug interactions (CYP2D6 inhibitor)
Paroxetine Anticholinergic properties; ↑drug interactions (CYP2D6 inhibitor); short half-life, higher risk of discontinuation/withdrawal symptoms(Headache, insomnia, nightmares, irritability, anxiety, paresthesia and shock-like sensation)
Sertraline Highest for diarrhea side effect (14% vs ~7%)
Marvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.Sanchez C, et al. Int Clin Psychopharmacol 2014; 29:185-96.Prescribing information. Available at http://www.fda.gov/Drugs/DrugSafety/ucm297391.htmLexicomp Online Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2019
Monitor: ECG; K+; Mg2+
*Interaction with CYP2C19 inhibitors (cimetidine, omeprazole)Beers Criteria: caution w h/o falls or fractures and SIADH: TCAs, SSRIs, SNRIs
22
2/25/21
12
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
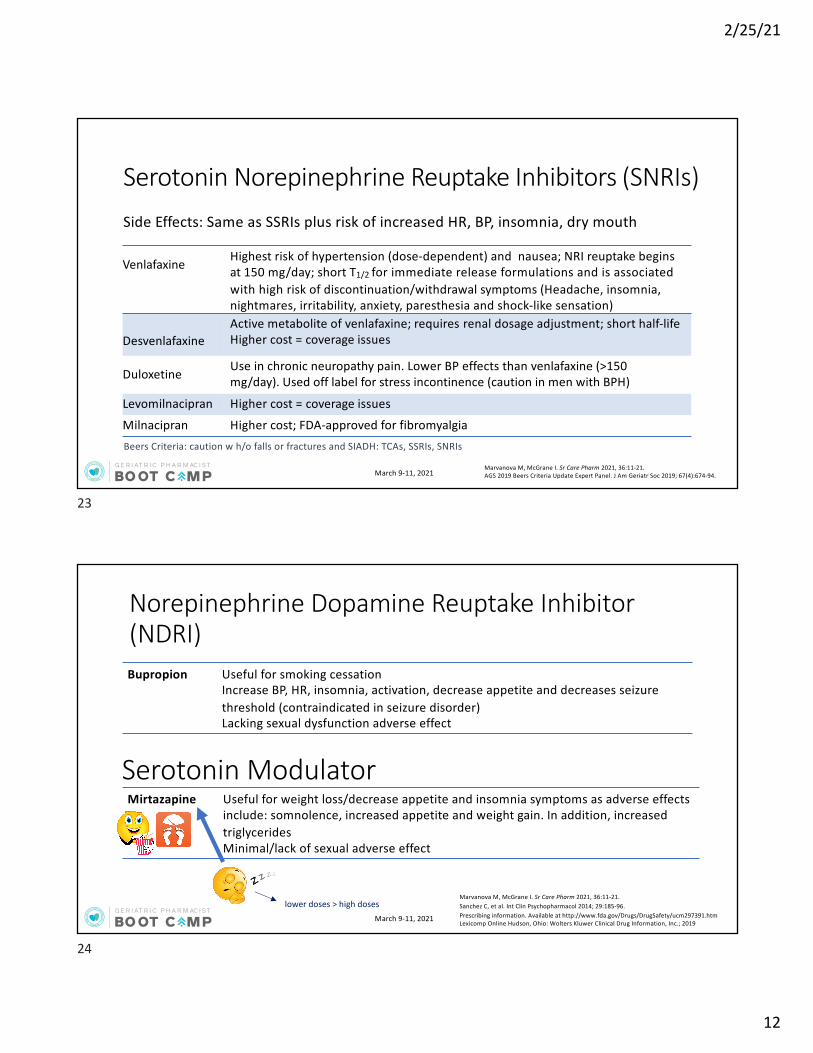
Venlafaxine Highest risk of hypertension (dose-dependent) and nausea; NRI reuptake begins at 150 mg/day; short T1/2 for immediate release formulations and is associated with high risk of discontinuation/withdrawal symptoms (Headache, insomnia, nightmares, irritability, anxiety, paresthesia and shock-like sensation)
DesvenlafaxineActive metabolite of venlafaxine; requires renal dosage adjustment; short half-lifeHigher cost = coverage issues
Duloxetine Use in chronic neuropathy pain. Lower BP effects than venlafaxine (>150 mg/day). Used off label for stress incontinence (caution in men with BPH)
Levomilnacipran Higher cost = coverage issues
Milnacipran Higher cost; FDA-approved for fibromyalgia
Serotonin Norepinephrine Reuptake Inhibitors (SNRIs)Side Effects: Same as SSRIs plus risk of increased HR, BP, insomnia, dry mouth
Marvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.AGS 2019 Beers Criteria Update Expert Panel. J Am Geriatr Soc 2019; 67(4):674-94.
Beers Criteria: caution w h/o falls or fractures and SIADH: TCAs, SSRIs, SNRIs
23
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Norepinephrine Dopamine Reuptake Inhibitor (NDRI)Bupropion Useful for smoking cessation
Increase BP, HR, insomnia, activation, decrease appetite and decreases seizure threshold (contraindicated in seizure disorder)Lacking sexual dysfunction adverse effect
Mirtazapine Useful for weight loss/decrease appetite and insomnia symptoms as adverse effects include: somnolence, increased appetite and weight gain. In addition, increased triglyceridesMinimal/lack of sexual adverse effect
Serotonin Modulator
lower doses > high dosesMarvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.Sanchez C, et al. Int Clin Psychopharmacol 2014; 29:185-96.Prescribing information. Available at http://www.fda.gov/Drugs/DrugSafety/ucm297391.htmLexicomp Online Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2019
24

2/25/21
13
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Tricyclic Antidepressants (TCAs)*• Blocking serotonin reuptake, norepinephrine reuptake, and histamine 1, muscarinic and alpha
receptors
• Adverse Effects: anticholinergic effects, tachycardia, orthostatic hypotension, weight gain, sedation, hyponatremia due SIADH, risk of bleeding, serotonin syndrome, risk of seizures, QTc prolongation
SecondaryNortriptyline
Best tolerated TCA in older adults, often used for sleep disturbances, can check serum levels metabolite ofamitriptyline
Desipramine Metabolite of imipramine
Tertiary
Amitriptyline Most anticholinergic TCA
Imipramine Often used for nocturnal enuresis
DoxepinLow doses used for insomnia, avoid doses >6 mg in older adults due to anticholinergic properties (Beers)
* Beers Criteria: Avoid in older adults with syncope, history of falls or fractures, SIADH; highly anticholinergic.
Marvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.AGS 2019 Beers Criteria Update Expert Panel. J Am Geriatr Soc 2019; 67(4):674-94.
25
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Other Antidepressants
5HT2A, Alpha1, HA
antagonist + serotonin reuptake inhibitor
Trazodone50-100 mg/dose is used for insomniaAdverse effects of orthostatic hypotension and priapism
SSRI, 5HT1apartial agonist Vilazodone Higher cost, same adverse effects as SSRIs
SSRI, 5HT1aagonist, 5HT3
antagonist Vortioxetine Higher cost; “studied” in older adults (age range 55-88; average 62 years), similar AEs as SSRI (primarily headache, dizziness and constipation)
Marvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.Stahl; SM. The Prescriber’s Guide, 4th ed. Cambridge University Press, 2011.Nomikos GG et al. CNS Spect 2017; 22:348-62.
26
2/25/21
14
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
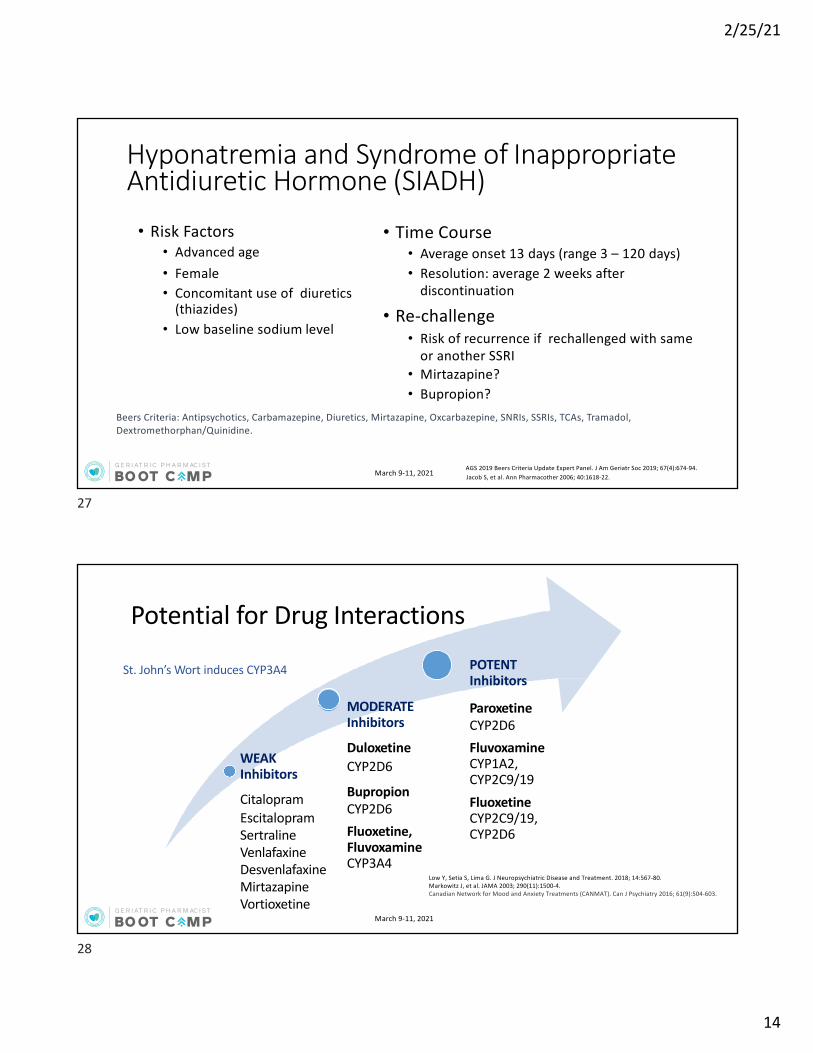
• Risk Factors• Advanced age• Female• Concomitant use of diuretics
(thiazides)• Low baseline sodium level
• Time Course• Average onset 13 days (range 3 – 120 days)• Resolution: average 2 weeks after
discontinuation
• Re-challenge• Risk of recurrence if rechallenged with same
or another SSRI• Mirtazapine?• Bupropion?
Hyponatremia and Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
Beers Criteria: Antipsychotics, Carbamazepine, Diuretics, Mirtazapine, Oxcarbazepine, SNRIs, SSRIs, TCAs, Tramadol, Dextromethorphan/Quinidine.
AGS 2019 Beers Criteria Update Expert Panel. J Am Geriatr Soc 2019; 67(4):674-94.Jacob S, et al. Ann Pharmacother 2006; 40:1618-22.
27
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Potential for Drug Interactions
WEAKInhibitors
Citalopram Escitalopram Sertraline VenlafaxineDesvenlafaxineMirtazapineVortioxetine
MODERATEInhibitors
DuloxetineCYP2D6
BupropionCYP2D6Fluoxetine, Fluvoxamine CYP3A4
POTENTInhibitors
ParoxetineCYP2D6Fluvoxamine CYP1A2, CYP2C9/19Fluoxetine CYP2C9/19, CYP2D6
St. John’s Wort induces CYP3A4
Low Y, Setia S, Lima G. J Neuropsychiatric Disease and Treatment. 2018; 14:567-80.Markowitz J, et al. JAMA 2003; 290(11):1500-4.Canadian Network for Mood and Anxiety Treatments (CANMAT). Can J Psychiatry 2016; 61(9):504-603.
28

2/25/21
15
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Antidepressant Interaction with Warfarin
• INCREASED RISK OF BLEEDINGo TCAs, SSRI, SNRI increase risk of bleeding (pharmacodynamic effect)o CYP2C9 inhibitors increase S-warfarin
Warfarin Active Metabolites CYP1A2
R-warfarin
CYP2C9
Major S-warfarin
CYP Inhibitors Fluvoxamine Fluoxetine
Fluvoxamine
Andrade C, et al. J Clin Psychiatry 2010; 71(12):1565-75.
S-warfarin – active form
29
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Comorbid Depression and PainAnalgesic ProdrugNeed CYP2D6 for Activation
Active Metabolite/Potency of Active Metabolite vs Prodrug
Codeine Morphine (300x more potent)
Tramadol O-desmethyltramadol/M1 metabolite (200x more potent)
Hydrocodone Hydromorphone (20x more potent)
DDI (failure to achieve analgesia/decreased analgesia) with SSRI and SNRI with strong CYP2D6 antagonistic properties
• Fluoxetine• Paroxetine• Duloxetine• Bupropion Yiannakopoulou E. Int J Genomics 2015:368979. Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4446490/. Accessed on January 24, 2021.
30

2/25/21
16
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Comorbid Depression in Dementia
PHARMACOKINETIC
Galantamine, Donepezil
Tolerability
CYP2D6 inhibitorsDuloxetineParoxetineBupropionParoxetine
PHARMACOKINETIC
Galantamine, Donepezil
Efficacy
CYP3A4 inducersSt. John’s wart
• Prevalence 32%
• Pharmacokinetic interactions• Pharmacodynamic interactions
o TCAs and paroxetine: anticholinergic effect
Pasqualetti G, et al. Clin Interv Aging 2015; 10:1457-66.
31
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Question 1: Clinical Vignette72-year-old presents with symptoms of depression including depressed mood, anhedonia, excessive guilt, insomnia, and lack of concentration for the past 6 weeks.PMH: low back pain due to inoperable spine compression (currently well controlled on tramadol after several medication trials), and hyperlipidemiaMedications: tramadol 100 mg twice daily, atorvastatin 40 mg dailyVS: 130/85 mm Hg; HR 78 bpm, RR 14 rpm, BMI 28 kg/m2
Labs: CBC: WNL; CMP: WNL; CrCl=85 mL/minPE: pulmonary and cardiovascular exam: unremarkable; PHQ-9 score 13 with no suicidal thoughts or plan
32

2/25/21
17
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Which of the following antidepressant might be a best option at this time?A. ParoxetineB. BupropionC. EscitalopramD. Amitriptyline
Self-Assessment Questions #1:
33
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Electroconvulsive Therapy (ECT)• Place in therapy: second-line for MDD, first-line for catatonia,
psychosis or acute suicidal thoughts/behaviors
• Onset: after 6 treatments (~2-3 weeks)
• Treatment:1) Acute: 2-3 times/week for 3-4 weeks (controlled clinical setting)
2) Maintenance: monthly or as needed • Comments:
o Most effective treatment for MDDo General anesthesia, muscle relaxants o Use of antidepressant post ECT reduces risk for relapse
• AEs: amnesia, headache, myalgiaMarvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.Canadian Network for Mood and Anxiety Treatments (CANMAT). Can J Psychiatry 216; 61(9):504-603.American Psychiatric Association (APA). Practice guideline for the treatment of patients with major depressive disorder, 3rd ed. Arlington, Virginia: American Psychiatric Association, 2010.
34

2/25/21
18
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
If At First You Don’t Succeed in Older AdultsNOResponse
Try another first-line antidepressant (in the same or different class)
PARTIALResponse
Switch to different first-line antidepressant (monotherapy is preferred in older adults but it depends on clinical situation and the response rate)Combination therapy: add bupropion or mirtazapine (Do not combine SSRIs and SNRIs) Augmentation strategies: most evidence with lithium and aripiprazole. Other options: liothyronine (T3), buspirone, or quetiapine, and brexpiprazolePotential role of stimulants in older adults (citalopram + methylphenidate)
Treatment-RESISTANCE(failed ≥ 2 district trials)
Electroconvulsive therapy or EsketamineRefer to a geriatric psychiatrist
Marvanova M, McGrane I. Sr Care Pharm 2021, 36:11-21.; Canadian Network for Mood and Anxiety Treatments (CANMAT). Can J Psychiatry 216; 61(9):504-603.; American Psychiatric Association (APA). Practice guideline for the treatment of patients with major depressive disorder, 3rd ed. Arlington, Virginia: American Psychiatric Association, 2010.; VA/DoD practice guideline for the management of major depressive d, version 3.0. Washington, D.C.: Veterans Health Administration and the Department of Defense, 2016.; Casey D. Primary Care: Clinics in Office Practice 2017; 44(3):499-510.
35
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
Supported in part by an educational grant from the ASCP Foundation. March 9-11, 2021
Anxiety
36

2/25/21
19
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Anxiety in the Older Adult• Higher rates of anxiety in older adults with medical illness, homebound and
nursing home residents.• Common problem (25% of new-onset generalized-anxiety disorder)• Often unrecognized because may present as somatic complaints
o GI distress, pain, chest pain
• Depression, anxiety and/or insomnia often co-exist
Cassidy KL, et al. Geriatrics and Aging 2008; 11:150-6. Caleo J, Stanley M. Anxiety Disorders in Later Life. Psychiatric Times. 2008. Available at http://www.psychiatrictimes.com/anxiety/anxiety-disorders-later-life. Accessed on January 25, 2021.
37
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Significant anxiety symptoms & impaired functioning
Panic Disorder(3.1%)
Specific Phobia(~10.1%)
Social Anxiety Disorder (~8.0%)
Generalized Anxiety Disorder(2.9%)
Persistent, uncontrolled worry about several areas
Intermittent panic/anxiety attacks & avoidance
Some Uncued /spontaneous
Discrete objects /situations
Fear of social scrutiny
IRRATIONAL fear/anxiety
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
38
2/25/21
20
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Diagnosis of Generalized Anxiety Disorder (GAD)• Unrealistic or excessive anxiety or worry for at least 6 months + ≥ 3 of
the following symptoms(1) Restlessness or feeling on edge(2) Easily fatigued(3) Difficulty concentrating(4) Irritability(5) Muscle tension(6) Sleep disturbance
• Clinically significant distress or impairment in social, occupational, or other important areas of functioning
• Not a result of substance abuse or medical condition or medication
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
39
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Drug- and Condition Induced Anxiety Symptoms
• CNS Depressant withdrawalo Benzodiazepines, ethanol
• CNS Stimulantso Illegal: cocaine; PCPo RX: albuterol, amphetaminesoNon RX: caffeine, nicotine, pseudoephedrine
• Miscellaneouso Corticosteroidso Antidepressants when initiatedo Levothyroxine
• Rule out medical condition as a cause:o TSH; CBC; CMP; ECG (chest pain/palpitations); Urine/serum toxicology
screen
40

2/25/21
21
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Screening Tools• Generalized Anxiety Disorder 7-item scale (GAD-7)
o Self-rated and brief (5 min)o Utility: Screens for GAD and severity assessmento Scores: mild (5-9); moderate (10-14); severe (≥15)o If positive (≥10 score) further evaluation is recommended
• Generalized Anxiety Disorder 2-item scale (GAD-2)o First 2 questions of GAD-7. If score 3-6 probable GAD and further screening
• Hamilton Anxiety Rating Scale (HAM-A)o Clinician (trained rater) rated (10-15 min)o 14 item scale screens symptoms of anxiety as well as somatic symptoms (sensory, GI, CV)o Assessment of severity and response to treatment (remission is ≥70% symptom improvement
or score <7; improved is 50% better improvement)o Scores
• ≤ 17 mild• 18-24 mild-moderate• 25-30 moderate-severe
HAM-A Scale https://dcf.psychiatry.ufl.edu/files/2011/05/HAMILTON-ANXIETY.pdf. Accessed on February 7, 2021.Spitzer RL Arch Intern Med 2006. Available at http://austintmsclinic.com/blog/wp-content/uploads/2015/09/Scoring-the-GAD-7-Dr-Vache.pdf GAD=7 Scale. https://www.crossroadscounselingcenters.com/pdf/Generalized%20Anxiety%20Disorder.pdf. Accessed on February 7, 2021.
41
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Geriatric Anxiety Inventory (GAI)• Reliable, valid and easy-to-use instrument for anxiety that is specifically
targeted at older adults• Administered either as a self-report or health professional-administered
measure• 20 “Agree/Disagree” items• Topics covered include feelings of fearfulness, worry, physical symptoms
of anxiety, and concerns about the impacts of worry and anxietyoMinimizes the emphasis of somatic symptoms which can be confounded with
physical health problems in older adults
• Assessment of anxiety symptoms in general
GAI. Available at https://www.apa.org/pi/about/publications/caregivers/practice-settings/assessment/tools/geriatric-anxiety. Accessed on January 25, 2021Pachana, N, et al. International Psychogeriatrics 2007; 19:103-14.
42
2/25/21
22
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
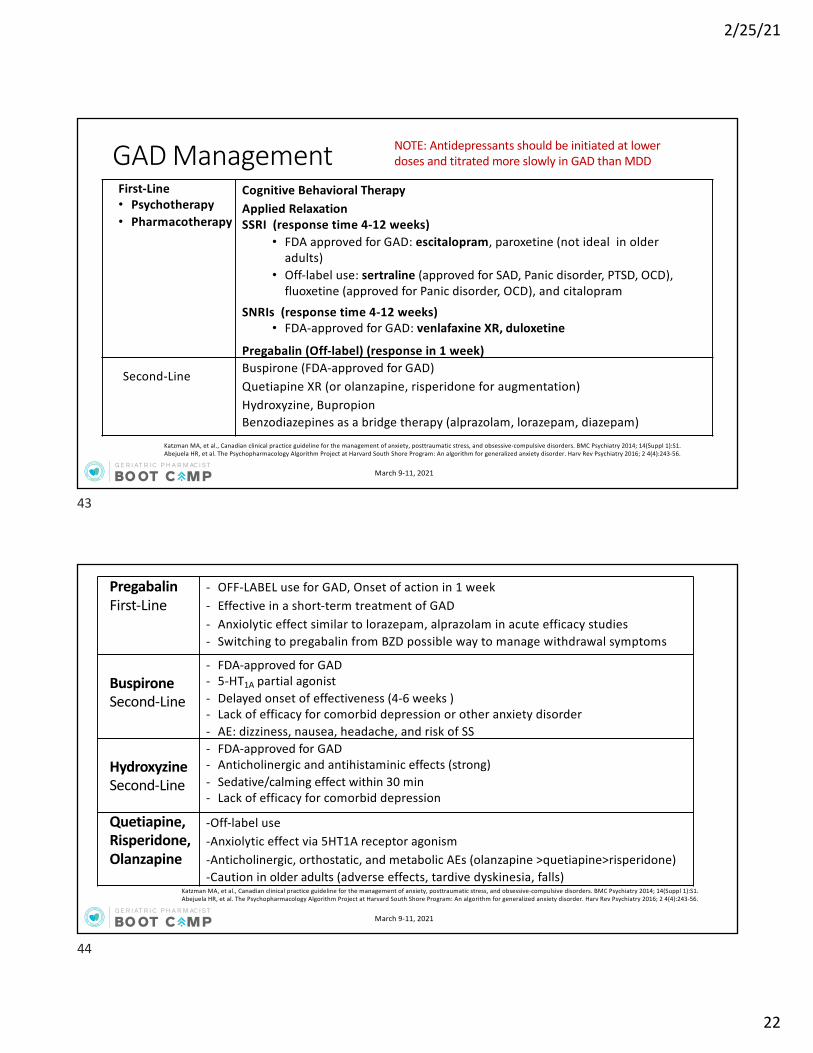
GAD Management
Katzman MA, et al., Canadian clinical practice guideline for the management of anxiety, posttraumatic stress, and obsessive-compulsive disorders. BMC Psychiatry 2014; 14(Suppl 1):S1.Abejuela HR, et al. The Psychopharmacology Algorithm Project at Harvard South Shore Program: An algorithm for generalized anxiety disorder. Harv Rev Psychiatry 2016; 2 4(4):243-56.
First-Line• Psychotherapy• Pharmacotherapy
Cognitive Behavioral TherapyApplied RelaxationSSRI (response time 4-12 weeks)
• FDA approved for GAD: escitalopram, paroxetine (not ideal in older adults)
• Off-label use: sertraline (approved for SAD, Panic disorder, PTSD, OCD), fluoxetine (approved for Panic disorder, OCD), and citalopram
SNRIs (response time 4-12 weeks)• FDA-approved for GAD: venlafaxine XR, duloxetine
Pregabalin (Off-label) (response in 1 week)
Second-Line Buspirone (FDA-approved for GAD)Quetiapine XR (or olanzapine, risperidone for augmentation)Hydroxyzine, BupropionBenzodiazepines as a bridge therapy (alprazolam, lorazepam, diazepam)
NOTE: Antidepressants should be initiated at lower doses and titrated more slowly in GAD than MDD
43
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
PregabalinFirst-Line
- OFF-LABEL use for GAD, Onset of action in 1 week- Effective in a short-term treatment of GAD- Anxiolytic effect similar to lorazepam, alprazolam in acute efficacy studies- Switching to pregabalin from BZD possible way to manage withdrawal symptoms
BuspironeSecond-Line
- FDA-approved for GAD- 5-HT1A partial agonist- Delayed onset of effectiveness (4-6 weeks )- Lack of efficacy for comorbid depression or other anxiety disorder- AE: dizziness, nausea, headache, and risk of SS
HydroxyzineSecond-Line
- FDA-approved for GAD- Anticholinergic and antihistaminic effects (strong)- Sedative/calming effect within 30 min- Lack of efficacy for comorbid depression
Quetiapine, Risperidone, Olanzapine
-Off-label use -Anxiolytic effect via 5HT1A receptor agonism-Anticholinergic, orthostatic, and metabolic AEs (olanzapine >quetiapine>risperidone)-Caution in older adults (adverse effects, tardive dyskinesia, falls)
Katzman MA, et al., Canadian clinical practice guideline for the management of anxiety, posttraumatic stress, and obsessive-compulsive disorders. BMC Psychiatry 2014; 14(Suppl 1):S1.Abejuela HR, et al. The Psychopharmacology Algorithm Project at Harvard South Shore Program: An algorithm for generalized anxiety disorder. Harv Rev Psychiatry 2016; 2 4(4):243-56.
44

2/25/21
23
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Lorazepam (L) In general, LOT - Preferred in older adultsModerate to fast onset, short duration, only Phase II metabolism and no activemetaboliteTemazepam only FDA-approved for insomnia but not anxietyOxazepam has risk of rebound anxiety due to short half-life
Oxazepam (O)
Temazepam (T)
Alprazolam -Alprazolam and clonazepam are FDA-approved for panic disorder-Alprazolam and diazepam are FDA-approved for anxiety disorders and short-term reliefof anxiety.-Rebound anxiety with alprazolam due to short half-life; CYP450 metabolism but noactive metabolite-If a longer acting benzodiazepine is to be considered, clonazepam undergoes Phase I metabolism (oxidation & nitro-reduction) with no active metabolite
Clonazepam
Benzodiazepines (BZD)Adverse Effects: Drowsiness, fatigue, confusion, addiction, decreased breathing, falls. Beers Criteria: not recommended but may be appropriate for seizure disorders, REM sleep disorder, benzo/alcohol withdrawal, and severe GAD as a bridge therapy.
www.accessdata.fda.govAGS 2019 Beers Criteria Update Expert Panel. J Am Geriatr Soc 2019; 67(4):674-94.Lexicomp Online Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2019
45
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Benzodiazepine Considerations• Usually used only for management of acute anxiety
o Rapid relief of anxiety symptomsoOnly use of 2-3 weeks max until SSRI/SNRI in effect
• Not effective for depression and depression can worsen if used long-term
• Risk for psychological and physiological dependenceoWithdrawal symptoms in ~44% of patients on BZD as short as 4-6 weeks
o 25% reduction in dose per week until 50% of dose reached, then reduce dose by 1/8 every 4-7 days
o Rebound anxiety can be part of the withdrawal symptoms
• Avoid in:• Delirium; Dementia; History of Falls; Myasthenia gravis; PTSD; Severe respiratory obstructive disease
AGS 2019 Beers Criteria Update Expert Panel. J Am Geriatr Soc. 2019; 67(4):674-94.
46

2/25/21
24
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Which of the following is true regarding SSRIs used in the treatment of generalized anxiety disorder versus their use in major depression?
A. SSRIs should be initiated at lower doses and titrated more slowlyB. SSRIs are less effective as monotherapyC. SSRIs are more likely to cause suicidal ideationD. SSRIs are used for a shorter duration
Self-Assessment Questions #2:
47
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Panic Disorder• Recurrent, spontaneous panic attacks• At least one of the attacks has been followed by 1 month of one
(or more) of the following:1. Persistent concern about having additional attacks2. Worry about the implications of the attack or its
consequences 3. Significant change in behavior related to the attacks
• Not due to the direct physiological effects of a substance or a general medical condition
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
48
2/25/21
25
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
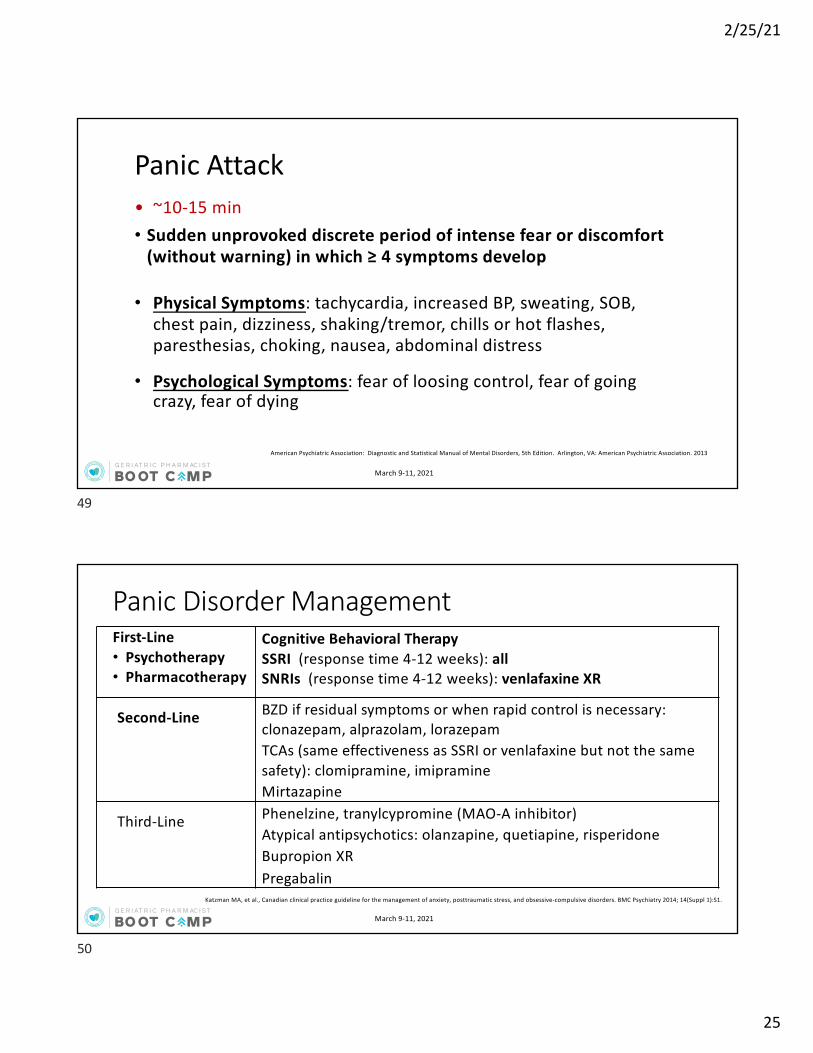
Panic Attack• ~10-15 min• Sudden unprovoked discrete period of intense fear or discomfort
(without warning) in which ≥ 4 symptoms develop
• Physical Symptoms: tachycardia, increased BP, sweating, SOB, chest pain, dizziness, shaking/tremor, chills or hot flashes, paresthesias, choking, nausea, abdominal distress
• Psychological Symptoms: fear of loosing control, fear of going crazy, fear of dying
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
49
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Panic Disorder Management
Katzman MA, et al., Canadian clinical practice guideline for the management of anxiety, posttraumatic stress, and obsessive-compulsive disorders. BMC Psychiatry 2014; 14(Suppl 1):S1.
First-Line• Psychotherapy• Pharmacotherapy
Cognitive Behavioral TherapySSRI (response time 4-12 weeks): allSNRIs (response time 4-12 weeks): venlafaxine XR
Second-Line BZD if residual symptoms or when rapid control is necessary: clonazepam, alprazolam, lorazepamTCAs (same effectiveness as SSRI or venlafaxine but not the same safety): clomipramine, imipramineMirtazapine
Third-Line Phenelzine, tranylcypromine (MAO-A inhibitor)Atypical antipsychotics: olanzapine, quetiapine, risperidoneBupropion XRPregabalin
50
2/25/21
26
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
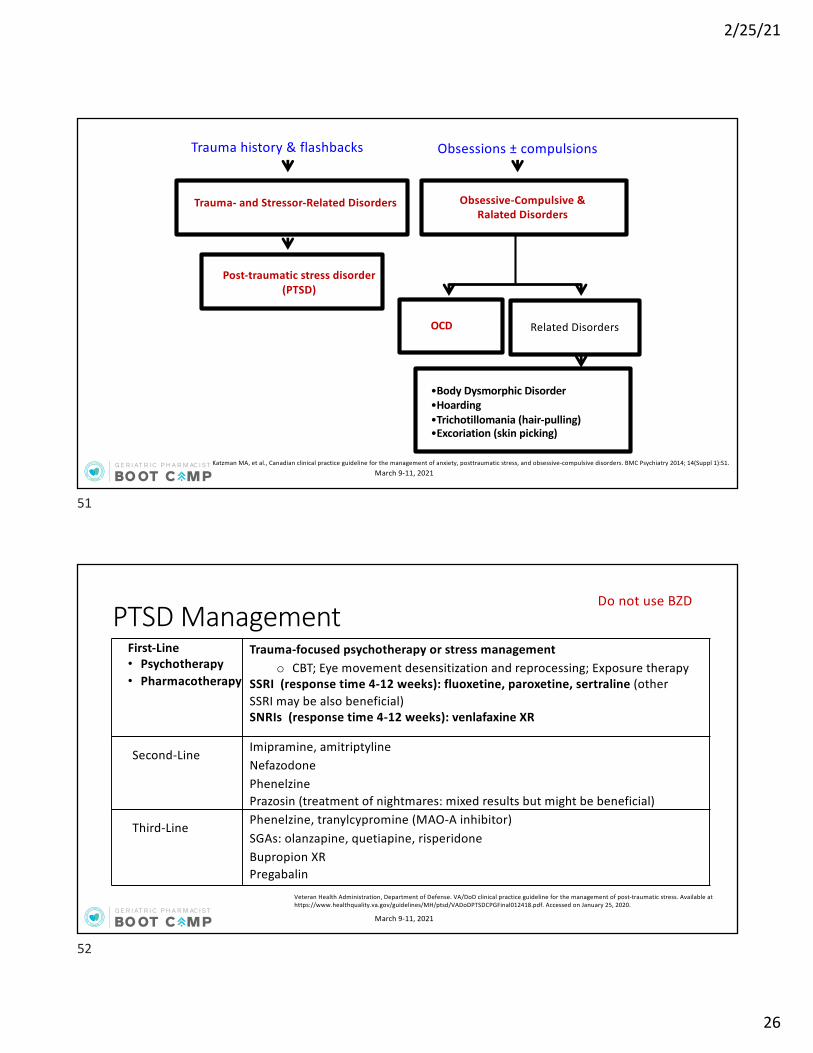
•Body Dysmorphic Disorder•Hoarding•Trichotillomania (hair-pulling)•Excoriation (skin picking)
Trauma- and Stressor-Related Disorders Obsessive-Compulsive & Ralated Disorders
Trauma history & flashbacks Obsessions ± compulsions
OCD Related Disorders
Post-traumatic stress disorder (PTSD)
Katzman MA, et al., Canadian clinical practice guideline for the management of anxiety, posttraumatic stress, and obsessive-compulsive disorders. BMC Psychiatry 2014; 14(Suppl 1):S1.
51
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
PTSD Management
Veteran Health Administration, Department of Defense. VA/DoD clinical practice guideline for the management of post-traumatic stress. Available at https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal012418.pdf. Accessed on January 25, 2020.
First-Line• Psychotherapy• Pharmacotherapy
Trauma-focused psychotherapy or stress managemento CBT; Eye movement desensitization and reprocessing; Exposure therapy
SSRI (response time 4-12 weeks): fluoxetine, paroxetine, sertraline (other SSRI may be also beneficial)SNRIs (response time 4-12 weeks): venlafaxine XR
Second-Line Imipramine, amitriptylineNefazodonePhenelzinePrazosin (treatment of nightmares: mixed results but might be beneficial)
Third-Line Phenelzine, tranylcypromine (MAO-A inhibitor)SGAs: olanzapine, quetiapine, risperidoneBupropion XRPregabalin
Do not use BZD
52
2/25/21
27
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
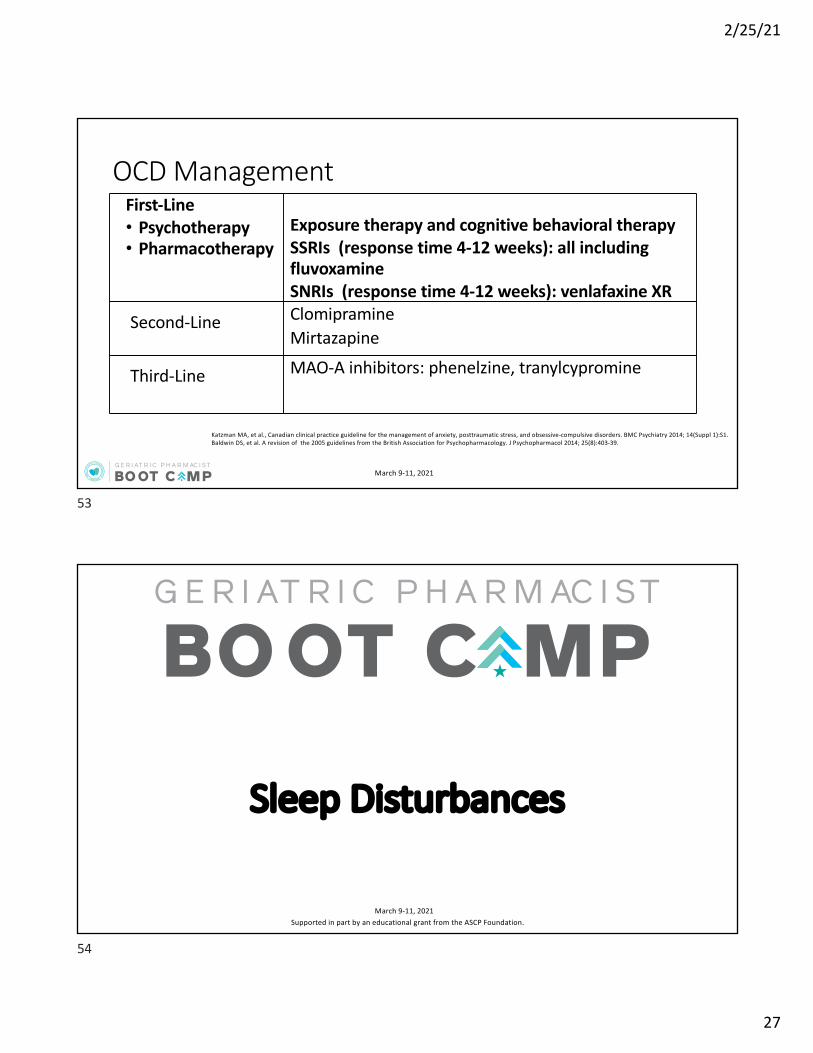
OCD ManagementFirst-Line• Psychotherapy• Pharmacotherapy
Exposure therapy and cognitive behavioral therapySSRIs (response time 4-12 weeks): all including fluvoxamineSNRIs (response time 4-12 weeks): venlafaxine XR
Second-Line ClomipramineMirtazapine
Third-Line MAO-A inhibitors: phenelzine, tranylcypromine
Katzman MA, et al., Canadian clinical practice guideline for the management of anxiety, posttraumatic stress, and obsessive-compulsive disorders. BMC Psychiatry 2014; 14(Suppl 1):S1.Baldwin DS, et al. A revision of the 2005 guidelines from the British Association for Psychopharmacology. J Psychopharmacol 2014; 25(8):403-39.
53
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
Supported in part by an educational grant from the ASCP Foundation. March 9-11, 2021
Sleep Disturbances
54
2/25/21
28
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
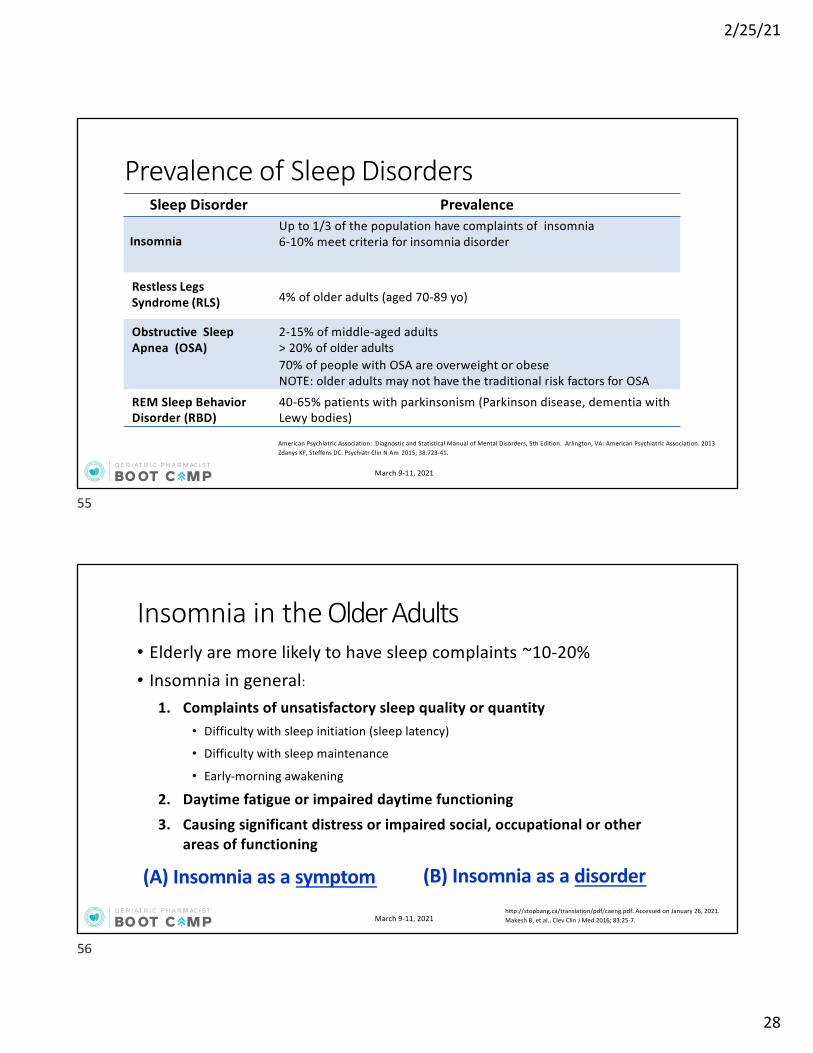
Prevalence of Sleep DisordersSleep Disorder Prevalence
InsomniaUp to 1/3 of the population have complaints of insomnia6-10% meet criteria for insomnia disorder
Restless LegsSyndrome (RLS) 4% of older adults (aged 70-89 yo)
Obstructive SleepApnea (OSA)
2-15% of middle-aged adults> 20% of older adults70% of people with OSA are overweight or obeseNOTE: older adults may not have the traditional risk factors for OSA
REM Sleep Behavior Disorder (RBD)
40-65% patients with parkinsonism (Parkinson disease, dementia with Lewy bodies)
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013Zdanys KF, Steffens DC. Psychiatr Clin N Am 2015; 38:723-41.
55
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Insomnia in the Older Adults• Elderly are more likely to have sleep complaints ~10-20%• Insomnia in general:
1. Complaints of unsatisfactory sleep quality or quantity• Difficulty with sleep initiation (sleep latency)
• Difficulty with sleep maintenance
• Early-morning awakening
2. Daytime fatigue or impaired daytime functioning
3. Causing significant distress or impaired social, occupational or other areas of functioning
(A) Insomnia as a symptom (B) Insomnia as a disorderhttp://stopbang.ca/translation/pdf/caeng.pdf. Accessed on January 26, 2021. Makesh B, et al., Clev Clin J Med 2016; 83:25-7.
56

2/25/21
29
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Insomnia as a SYMPTOMConditions/Illnesses
• Pain and breathing difficulty• impaired mobility• Depression• Hypomania/mania• Restless leg syndrome• Increased urination urges
Medication/Substance-Induced• Stimulating medications
• Decongestantso Pseudoephedrineo Epinephrine
• Stimulantso Caffeineo Nicotineo Amphetamineso Cocaine
• Stimulating Antidepressants and AEDs
• Alcohol• Diuretics
Dopp JM, et al. Pharmacotherapy: A Pathophysiologic Approach, 2014.
57
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Insomnia DISORDER1. Unsatisfactory sleep quantity or quality + presence of ≥ 1 of the
following:1. Difficulty with sleep latency2. Difficulty with sleep maintenance 3. Early-morning awakening
2. Significant distress or impairment in social, occupational or other areas of functioning
3. Sleep difficulty happens with ample sleep opportunity4. Sleep complaints for ≥3 night/week and has been present for at
least 3 months5. Not associated with substance use, psychiatric disorders, or
other medical disorderAmerican Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
58

2/25/21
30
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Insomnia TreatmentsLevel of Intervention ACP (2016)1 AASM (2017)2
First-Line Cognitive Behavioral Therapy including stimulus behavioral therapy
Cognitive Behavioral Therapy
Second-LineWeigh risk vs benefit of medication
General population potential benefit• Non-benzodiazepine receptor
agonist (NBRA)• Suvorexant• Doxepin
Older adults• NBRA (eszopiclone, zolpidem)• Ramelteon• Doxepin
- Sleep onset and maintenance: eszopiclone, temazepam, zolpidem
- Sleep onset: ramelteon, triazolam, zaleplon
- Sleep maintenance: doxepin, suvorexant
1 American College of Physicians: Qaseem A, et al. Ann Intern Med 2016; 165:125-33.2 American Academy of Sleep Medicine: Sateia MJ, et al. J Clin Sleep Med 2017; 13:307-49.
Not recommended1: diphenhydramine; L-tryptophan; melatonin, valerian, trazodoneAgent selection should be based on patient’s factors and T1/2 of the medication and sleep need to decrease risk of AEs such as next-day somnolence (potential risk of all hypnotics) and cognitive impairment.
59
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Beers Updates: InsomniaDrug/Drug Class 2015; 2019 Updates
Benzodiazepines (BZD) AVOID
NBRA or “Z” hypnotics AVOID; risk similar to BZDs
Diphenhydramine AVOID
TCAs AVOID all tertiary amines except doxepin doses ≤ 6 mg (OK)
Beers changes over time – Previously lower doses of short acting BZDs temazepam ≤15 mg; triazolam ≤ 0.25 mg consider OK over long-acting BZDsPreviously “z” hypnotics stated to avoid chronic use ≥ 90 days
AGS 2019 Beers Criteria Update Expert Panel. J Am Geriatr Soc 2019; 67(4):674-94.AGS 2015 Beers Criteria Update Expert Panel . Am Geriatr Soc 2015; 63(11):2227-46.
60
2/25/21
31
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
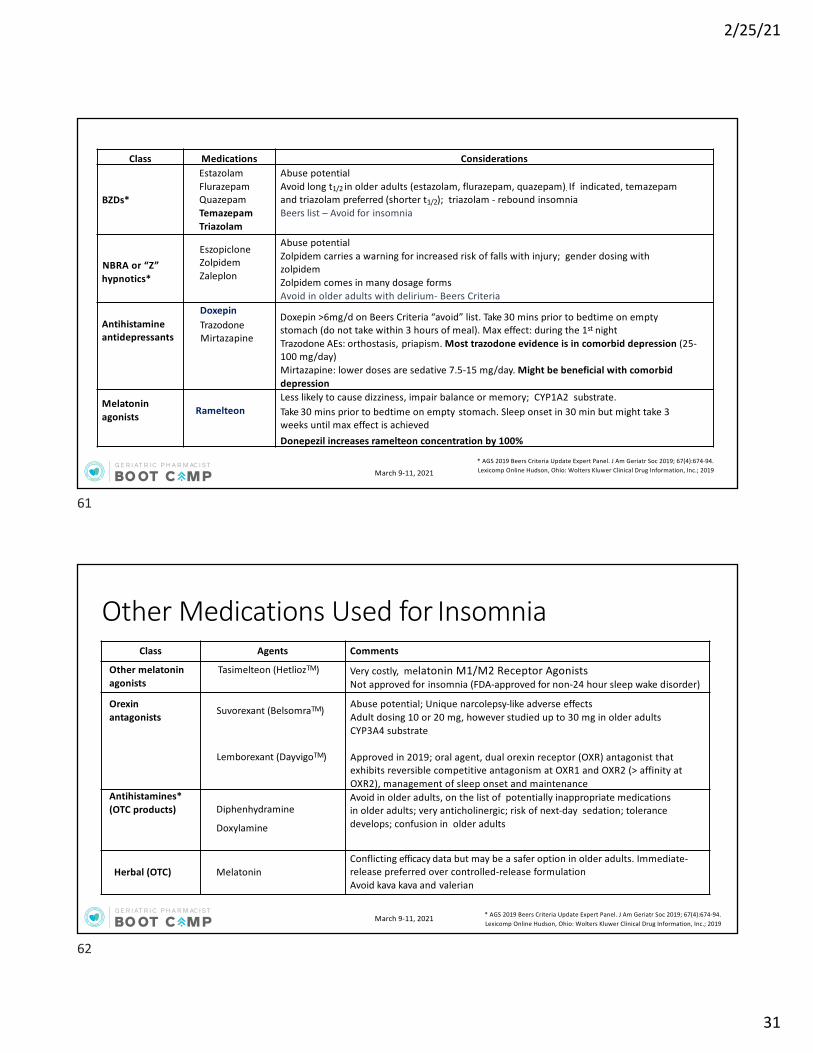
Class Medications Considerations
BZDs*
EstazolamFlurazepamQuazepamTemazepamTriazolam
Abuse potentialAvoid long t1/2 in older adults (estazolam, flurazepam, quazepam). If indicated, temazepam and triazolam preferred (shorter t1/2); triazolam - rebound insomniaBeers list – Avoid for insomnia
NBRA or “Z”hypnotics*
EszopicloneZolpidem Zaleplon
Abuse potentialZolpidem carries a warning for increased risk of falls with injury; gender dosing withzolpidemZolpidem comes in many dosage formsAvoid in older adults with delirium- Beers Criteria
Antihistamine antidepressants
Doxepin Trazodone Mirtazapine
Doxepin >6mg/d on Beers Criteria “avoid” list. Take 30 mins prior to bedtime on empty stomach (do not take within 3 hours of meal). Max effect: during the 1st nightTrazodone AEs: orthostasis, priapism. Most trazodone evidence is in comorbid depression (25-100 mg/day)Mirtazapine: lower doses are sedative 7.5-15 mg/day. Might be beneficial with comorbid depression
Melatonin agonists Ramelteon
Less likely to cause dizziness, impair balance or memory; CYP1A2 substrate. Take 30 mins prior to bedtime on empty stomach. Sleep onset in 30 min but might take 3 weeks until max effect is achievedDonepezil increases ramelteon concentration by 100%
* AGS 2019 Beers Criteria Update Expert Panel. J Am Geriatr Soc 2019; 67(4):674-94.Lexicomp Online Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2019
61
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Other Medications Used for InsomniaClass Agents Comments
Other melatonin agonists
Tasimelteon (HetliozTM) Very costly, melatonin M1/M2 Receptor AgonistsNot approved for insomnia (FDA-approved for non-24 hour sleep wake disorder)
Orexin antagonists Suvorexant (BelsomraTM)
Lemborexant (DayvigoTM)
Abuse potential; Unique narcolepsy-like adverse effectsAdult dosing 10 or 20 mg, however studied up to 30 mg in older adultsCYP3A4 substrate
Approved in 2019; oral agent, dual orexin receptor (OXR) antagonist that exhibits reversible competitive antagonism at OXR1 and OXR2 (> affinity at OXR2), management of sleep onset and maintenance
Antihistamines* (OTC products) Diphenhydramine
Doxylamine
Avoid in older adults, on the list of potentially inappropriate medications in older adults; very anticholinergic; risk of next-day sedation; tolerance develops; confusion in older adults
Herbal (OTC) MelatoninConflicting efficacy data but may be a safer option in older adults. Immediate-release preferred over controlled-release formulationAvoid kava kava and valerian
* AGS 2019 Beers Criteria Update Expert Panel. J Am Geriatr Soc 2019; 67(4):674-94.Lexicomp Online Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2019
62
2/25/21
32
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
A 72-year-old female presents to the clinic with complaints of early morning awakening several days per week. She completed several weeks of cognitive behavioral therapy for insomnia and has made recommended changes in her sleep hygiene and lifestyle modifications. What would be the most appropriate recommendation at this time?
A. Diphenhydramine 25 mg at bedtimeB. Doxepin 3 mg at bedtimeC. Temazepam 15 mg at bedtimeD. Zolpidem 5 mg at bedtime
Self-Assessment Questions #3:
63
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
When To Consider Antidepressants for Insomnia
• Patients with comorbid anxiety/depression• Patients with comorbid substance abuse/substance use disorder• Although most TCAs are on the Beers list, low-dose doxepin is not.• It was studied in older adults and did not appear to have increased
risks of confusion and anticholinergic events• Trazodone: Monitor for orthostasis; caution in African-American
men with sickle cell disease
Bossini L et al. Expert Opin Pharmacother 2012; 13:1707-17.Vande Griend JP et al. J Am Pharm Assoc 2012; 52:e210-9.Lankford A, et al. Sleep Med 2012; 13:133-8.
64

2/25/21
33
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Screening Tool: STOP-Bang for OSAS Snoring Snore loudly?
T Tired Daytime sleepiness? Fatigue?
O Observed Stopping breathing during your sleep?
P Pressure History of or being treated for HTN?
B Body Mass Index > 35 kg/m2
A Age > 50
N Neck circumference > 40 cm (16 inches)Updated is ≥16 inches if female, ≥ 17 inches if male
G Gender Male?
Scoring: Low Risk: 0-2
Intermediate: 3-4 High Risk: 5 or greater
http://stopbang.ca/translation/pdf/caeng.pdf.. Accessed on January 26, 2021. Makesh B, et al., Clev Clin J Med 2016; 83:25-7.
65
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Obstructive Sleep Apnea (OSA) Management
Qaseem A, et al., Management of obstructive sleep apnea in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med 2013; 159(7):471-83.
First-Line Weight reduction (adjunctive to other therapy)CPAP (nasal preferred over oral or oronasal route)
Second-Line Oral mandibular devices/appliances (needs to have at least 16 healthy teeth)Treatment of excessive daytime sleepiness in those adherent to CPAPo modafinil, armodafinil
Third-Line Bariatric surgery in those with BMI >40 kg/m2
Surgery (if a good candidate): septoplasty, tonsillectomy, adenoidectomy, laryngeal surgeries
Other non-pharmacologic modalities: smoking cessation, avoid alcohol and other CNS depressants, positional change (sleep on a side)
66

2/25/21
34
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Restless Leg Syndrome (RLS) Management1
1 Winkelman JW, et al. practice guideline summary: treatment of restless leg syndrome in adults. Report of the guideline, development, dissemination, implementation Subcommittee of the American Academy of Neurology. Neurology 2016; 87(24):2585-93.
First-Line Reduce dose of eliminate triggers (antidepressants, antihistamines)Dopamine agonists (preferred in very severe RLS, comorbid depression, obesity)
o Pramipexoleo Rotigotineo Ropinirole
Alpha-2-delta ligands (preferred in comorbid pain, anxiety, insomnia, history of impulse control disorder)
o Gabapentin enacarbilo Pregabalin
IV ferric carboxymaltose (despite of ferritin levels)
• If intermittent RLS (frequency <2 times/week): use dopamine agonist (pramipexole) as needed• Role of iron is unclear BUT it is reasonable to check iron levels in new or worsening RLS cases (American
Academy of Neurologyo Serum ferritin level <75 mcg/dL: initiate ferrous sulfate 325 mg TID with vitamin C
67
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
Supported in part by an educational grant from the ASCP Foundation. March 9-11, 2021
Substance Use Disorders
68

2/25/21
35
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Diagnosis of Substance Use Disorder
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
• Problematic pattern of substance use leading to clinically significant impairment or distress, as manifested by at least 2 of the following, occurring within a 12-month period
1. Substance is often taken in larger amounts or over a longer period than was intended2. Persistent desire or unsuccessful efforts to cut down or control substance use3. Great deal of time is spent in activities necessary to obtain the substance, use the
substance, or recover from its effects4. Craving or a strong desire or urge to use substance5. Recurrent substance use resulting in failure to fulfill major role obligations at work, school or
home6. Continued substance use despite having persistent or recurrent social or interpersonal
problems caused or exacerbated by the effects of substance7. Important social, occupational, or recreational activities are given up or reduced because of
substance use8. Recurrent substance use in situations in which it is physically hazardous9. Substance use is continued despite knowledge of having a persistent or recurrent physical or
psychological problem that is likely to have been caused or exacerbated by the substance10. Tolerance11. Withdrawal
69
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Clinical Presentation of Alcohol Use Disorder (AUD)Alcohol IntoxicationRecent ingestion of alcohol and clinically significant maladaptive behavior of psychological changes during or shortly thereafter. One or more signs:• Slurred speech• Incoordination• Unsteady gait• Nystagmus• Inattention, memory impairment• Stupor or unconsciousness
Alcohol Withdrawal≥ 2 signs after cessation or reduction of alcohol consumption
• Autonomic hyperactivity• Hand tremor• Insomnia• Hallucinations or illusions• Psychomotor agitation• Nervousness• Seizure activity
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
70
2/25/21
36
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
CAGE Questionnaire: Cut Down, Annoyed, Guilty, Eye-opener1. Have you ever felt you should Cut down on your drinking? 2. Have people Annoyed you by criticizing your drinking? 3. Have you ever felt bad or Guilty about your drinking?4. Have you ever had a drink first thing in the morning to steady your nerves
or to get rid of a hangover (Eye opener)?
Scoring: Item responses on the CAGE are scored 0 or 1• a higher score an indication of alcohol problems• ≥ 2 a positive screen suggesting issue with drinking and further need for
assessment
Ewing JA. JAMA1984;252:1905-07
71
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Complications of Chronic Alcohol Use
• Peripheral neuropathy: bilateral limb numbness, tingling, and paresthesias• Occurs in ~10% of chronic alcohol users
• Wernicke’s encephalopathy: vitamin B1 (thiamine) deficiency• Anemia (often macrocytic): folic acid and vitamin B12 deficiency• Cognitive changes, brain atrophy: possibly leading to dementia• Psychiatric problems: depression and anxiety• Epigastric distress and gastrointestinal bleeding• Liver failure, cirrhosis and pancreatitis• Skeletal muscle weakness caused by acute alcoholic myopathy
• Occurs in ~1/2 to 2/3 of chronic alcohol users
72
2/25/21
37
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
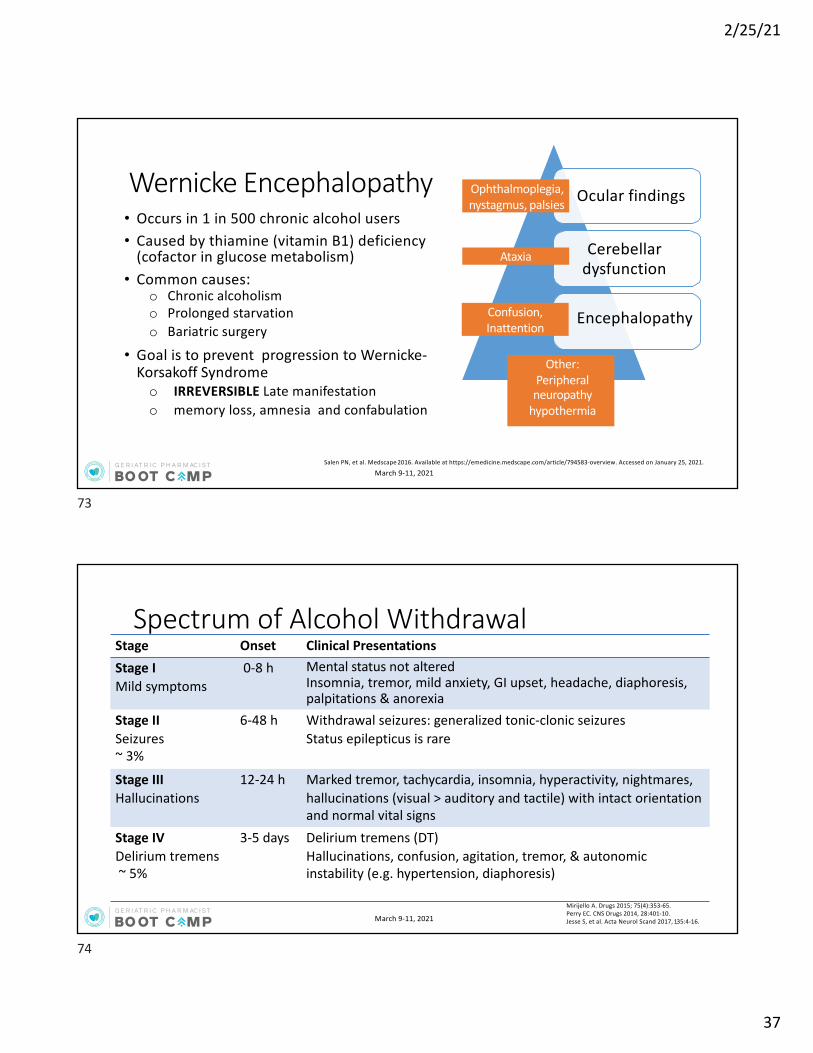
Wernicke Encephalopathy• Occurs in 1 in 500 chronic alcohol users• Caused by thiamine (vitamin B1) deficiency
(cofactor in glucose metabolism)• Common causes:
o Chronic alcoholismo Prolonged starvationo Bariatric surgery
• Goal is to prevent progression to Wernicke-Korsakoff Syndrome o IRREVERSIBLE Late manifestationo memory loss, amnesia and confabulation
Ocular findings
Cerebellar dysfunction
Encephalopathy
Ophthalmoplegia,nystagmus, palsies
Ataxia
Salen PN, et al. Medscape 2016. Available at https://emedicine.medscape.com/article/794583-overview. Accessed on January 25, 2021.
Confusion, Inattention
Other:Peripheral neuropathy
hypothermia
73
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Spectrum of Alcohol WithdrawalStage Onset Clinical PresentationsStage IMild symptoms
0-8 h Mental status not alteredInsomnia, tremor, mild anxiety, GI upset, headache, diaphoresis, palpitations & anorexia
Stage IISeizures~ 3%
6-48 h Withdrawal seizures: generalized tonic-clonic seizuresStatus epilepticus is rare
Stage IIIHallucinations
12-24 h Marked tremor, tachycardia, insomnia, hyperactivity, nightmares, hallucinations (visual > auditory and tactile) with intact orientation and normal vital signs
Stage IVDelirium tremens~ 5%
3-5 days Delirium tremens (DT)Hallucinations, confusion, agitation, tremor, & autonomic instability (e.g. hypertension, diaphoresis)
Mirijello A. Drugs 2015; 75(4):353-65.Perry EC. CNS Drugs 2014, 28:401-10. Jesse S, et al. Acta Neurol Scand 2017, 135:4-16.
74

2/25/21
38
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Sullivan JT et al. Br J Addict 1989; 84:1353-7.https://www.drugabuse.gov/sites/default/files/files/ClinicalOpiateWithdrawalScale.pdf.Accessed on January 25, 2021.
Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
Scoring:
8-14 = Moderate withdrawal≥ 15 = Severe withdrawal
CIWA-Ar > 8 BZD medication indicated
75
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Management of AUDLevel of Intervention APA (2018)1 WFSBP (2017)2
First-Line Alcohol withdrawal: BZD
AUD: naltrexone or acamprosate
Alcohol withdrawal: BZD
AUD: naltrexone or acamprosate
Second-LineAlcohol withdrawal: b-blockers, clonidine, carbamazepine, divalproex sodium
AUD: disulfiram, topiramate, gabapentin
Supportive care: thiamine and fluid
Alcohol withdrawal: gabapentin,carbamazepine, sodium valproate, clonidine
AUD: disulfiram, baclofen
1 American Psychiatric Association : Reus VI et al. Am J Psychiatry 2018; 175(1):86-90.World Federation of Societies of Biological Psychiatry: Soyka M, et al. World J Biol Psychiatry 2017; 18(2):86-119.
Withdrawal: monitor VS, maintain ABO, glucose if indicated (administer after thiamine!!!), manage nausea/vomitingFDA-approved BZD for alcohol withdrawal: chlordiazepoxide, clorazepate, diazepam, and oxazepamOff-label BZD for alcohol withdrawal: lorazepam
76

2/25/21
39
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Alcohol Withdrawal Management1. Fixed-schedule BZD therapy
• Patient with history of seizures, delirium tremens or major alcohol withdrawal should be managed on fixed dosing of diazepam or chlordiazepoxide or other BDZs
2. Symptom-triggered therapy: CIWA-Ar >8 • Patient at risk for withdrawal should be closely monitored & treated with
BZD if CIWA scores >8
3. Delirium tremens (DT) should be treated with IV diazepam until stable
4. Refractory DT treated with phenobarbital or propofol
77
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Acamprosate
NMDA receptor antagonist enhancing GABAergic activation and GABA/Glutamate balanceHelps achieve abstinence; may decrease cravingMonitor: renal function; CI: CrCl ≤ 30 mL/min; Requires renal dose adjustmentOral formulation dosed three time daily (onset 3-8 hours)
Naltrexone
Opioid mu-receptor antagonist (CI: use of opioid within 7-10 days, acute opioid withdrawal, acute hepatitis, severe liver impairment (LFT > 3 UNL)Oral (onset 1-60 min) and intramuscular formulation (onset 2-3 days)Beneficial for cravings and achieving abstinence Monitor: LFT (baseline, 1 month, 6 months, then annually)Useful for co-morbid AUD and opioid use disorder
DisulfiramDisulfiram reaction (blocks irreversibly aldehyde dehydrogenase, effect lasts 1-2 weeks); not much data in older adults; caution in DM and hepatic insufficient; Interaction with metronidazole (psychosis) and alcohol; monitor LFT
Gabapentin Off-label, renal dosage adjustment. Associated with decreased I heavy drinking days and increase abstinence rates
Topiramate Off-label, renal dosage adjustment. Associated with decreased I heavy drinking days
Pharmacologic Treatments of AUD
Reus VI, et al. Am J Psych 2018; 175:86-90.Lexicomp Online Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2019
78

2/25/21
40
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
A 68-year-old male is safely treated for alcohol withdrawal. He was found to have a broken wrist and ankle and has been receiving oxycodone for his severe pain. At discharge he asks if there is a medication to help him remain abstinent from alcohol. His liver function tests are elevated and renal function is within normal limits.Which medication would be the most appropriate at this time?
A. NaloxoneB. DisulfiramC. NaltrexoneD. Acamprosate
Self-Assessment Question #4:
79
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Clinical Presentation of Opioid Use Disorder (OUD)
Opioid IntoxicationRecent ingestion of opioid and clinically significant maladaptive behavior of psychological changes during or shortly thereafter. Constriction of pupils plus one of the following:• Drowsiness or coma• Slurred speech• Impaired attention or memory
Opioid Withdrawal≥ 3 signs after termination (or administration of opioid antagonist):
• Dysphoria• Nausea/vomiting• Myalgias• Lacrimation, Rhinorrhea, Diarrhea• Mydriasis• Piloerection• Sweating• Yawning• Fever• Insomnia
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013
80

2/25/21
41
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Clinical Opiate Withdrawal Scale (COWS)• Used in opiate detoxification
o follow the course of withdrawal symptoms and medication effectiveness
• 11 symptoms (max. 48 points)
• Higher score = higher withdrawal severity
Clonidine Helps reduce overall symptoms (e.g. sweats, piloerection, tearing)Loperamide Treats diarrheaOndansetron Treats nauseaIbuprofen Treats muscle cramping/pain (caution in older adults)Dicyclomine Treats GI cramping
1 American Psychiatric Association: Practice guideline for the treatment of patients with substance use disorders. 2nd ed; 2006.2 American Society of Addiction Medicine. Kampman K, et al. J Addict Med 2015; 9(5):358-67.3 Canadian Research Initiative in Substance Misuse. Bruneau J, et al. CMAJ 2018; 190(9):E247-E257.I
81
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Management of OUDLevel of Intervention APA (2006)1 ASAM (2015)2
First-Line Opioid Intoxication: naloxone
Opioid Withdrawal: buprenorphine, methadone
Opioid Dependence (maintenance treatment): buprenorphine, methadone
Opioid Intoxication: naloxone
Opioid Withdrawal: buprenorphine, methadone
Opioid Dependence (maintenance treatment): buprenorphine, methadone, naltrexone
Second-LineOpioid Withdrawal: clonidine
Opioid Dependence: naltrexone
Opioid Withdrawal: clonidine
1 American Psychiatric Association: Practice guideline for the treatment of patients with substance use disorders. 2nd ed; 2006.2 American Society of Addiction Medicine. Kampman K, et al. J Addict Med 2015; 9(5):358-67.3 Canadian Research Initiative in Substance Misuse. Bruneau J, et al. CMAJ 2018; 190(9):E247-E257.
Note: 2018 Canadian Research Initiative in Substance Misuse3 strongly recommends against offering withdrawalmanagement in isolation and instead recommends slow (>1 month) opioid agonist taper. Also recommends for opioid dependence: buprenorphine/naloxone as the 1st line therapy and methadone as the 2nd line.
82

2/25/21
42
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Naloxone: Rescue Therapy• Opioid overdose antidote
• Opioid receptor ANTAGONIST• higher affinity
• No pharmacologic effect in opioid naïve individuals (no harm)
• Onset 1-3 min
• Duration: 30-90 min
• No potential for abuse
• Naloxone IV, IM or intra-nasal
Restored breathing, consciousness, HR & BP
Shaw LV et al. Syst Rev 2019; 8:138.
83
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
THERAPY/REGIMEN• Advanced age• Drug-drug interactions• Use of methadone at any dose• ER/LA formulations• Higher opioid dose ≥50 MME/day• Changes in tolerance• Opioid polypharmacy• Concurrent use of CNS depressants
• Benzodiazepines• Antidepressant• Muscle relaxants• Alcohol• Gabapentin/Pregabalin
CONDITION• CYP450 polymorphisms
• Advanced age
• History of overdose
• History of SUD
• Renal dysfunction and/or hepatic disease
• Smoking status
• Pulmonary condition
Who is at Risk of Opioid Overdose?
Opioid CYP450 IsoformOxycodone CYP2D6; CYP3A4Methadone CYP2D6; CYP3A4Fentanyl CYP3A4Buprenorphine CYP3A4
Dahan A et al. Pain Physician 2013; 16:E85-E9412
84

2/25/21
43
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
March 9-11, 2021
Medication Assisted Treatment of OUD
Buprenorphine Available as SL, implants, Sub-Q, and injection
Buprenorphine/Naloxone
Combo preferred, theoretically less abuse potential. Available SL tabs or filmsNeed to be in moderate withdrawal to initiateCan receive Rx for multiple daysAbuse deterrent
MethadoneCan only be dispensed from a Methadone Maintenance Program; typically liquidformulation, once daily;Baseline: vital signs, LFT, ECG More likely to have drug interactions as it is metabolite for CYP3A4, CYP2D6 with narrow therapeutic index
NaltrexoneNot opioid replacement therapy and not a controlled substanceOpioid antagonist. Available in oral and IM formulationsUseful for treatment of AUD but also co-occurring AUD and OUD
1American Psychiatric Association: Practice guideline for the treatment of patients with substance use disorders. 2nd ed; 2006.2American Society of Addiction Medicine. Kampman K, et al. J Addict Med 2015; 9(5):358-67.3Canadian Research Initiative in Substance Misuse. Bruneau J, et al. CMAJ 2018; 190(9):E247-E257.I
85
G E R I AT R I C P H A R M AC I ST
BO OT C MPA
Supported in part by an educational grant from the ASCP Foundation. March 9-11, 2021
Psychiatric Disorders in the Older Adult
Marketa Marvanova, PharmD, PhD, BCGP, BCPP, FASCPDean and Professor
University of Montana, College of Health/Skaggs School of Pharmacy
86