marketing to professionals
DESCRIPTION
A collection of marketing materials created byTRANSCRIPT
VSL#3 JuniorSigmaTau Pharmaceuticals

LIFE’S APICNIC WHENYOU PICK NEW
It’s the high-potency probiotic medical food for the dietary management of IBS.

PICK FOR THE DIETARY MANAGEMENT OF IBS THAT DELIVERS CLINICALLY-PROVEN BENEFITS.
HOW DIETARY MANAGEMENT WITH VSL#3 JUNIOR WORKS Results of pre-clinical studies suggest that VSL#3:
• Strengthenstheintestinalepithelialbarriervia changes to bacterial luminal microbiota1
• Enhancestheintegrityofthetightjunctions2,3
• Increasesmucinsecretions4
• Competeswithnon-commensalbacteria for nutrients5
Well-established safety profile
• Studiedinhundredsofchildren
• GRAS(GenerallyRecognizedAsSafe)
• VSL#3JUNIORismanufacturedinaccordance withFDAguidelinesonCurrentGood Manufacturing Practice6
• VSL#3istheonlyprobioticmedicalfoodto beutilizedinapediatric,randomized,placebo- controlledtrialforchildrenwithIBS7
• All8bacterialstrainshavedecadesof established use6 Great new children’s formulation
• Watermelonflavorkidswilllove
• Allnatural,noartificialsweeteners,kosherand gluten free
FORMULATED WITH A PRECISE MIX OF 8 PROPRIETARY STRAINS OF LIVE BACTERIA
•Effectsofprobioticsarehighlystrain-specific9
•Simultaneousadministrationofmultiplebacterial strainsinspecifiedratiosmayprovidearange ofbenefitsthatcannotbeachievedwithsingle- strain probiotics2
VSL#3 JUNIOR THE MOST POTENT PROBIOTIC AVAILABLE11
•Provides225 billion bacteria perpacket
•Well-toleratedsafetyprofile
REFRIGERATION PRESERVES LIVE BACTERIA AND HELPS MAINTAIN POWERFUL POTENCY •Asamedicalfood,VSL#3JUNIORisintendedforthe dietarymanagementofchildrenwithIBS,andmustbe usedundermedicalsupervision
•50timesmorepotentthantheaverageprobiotic8
•Potencyisclinicallyimportant
o Ahighbacteriacountensuresthatbacteria survivestomachacidandbilesaltstocolonize the intestine1
Lactobacillus acidophilus Bifidobacteria infantis
Lactobacillus plantarum Bifidobacteria longum
Lactobacillus paracasei Bifidobacteria breve
Lactobacillus delbrueckii subsp. bulgaricus Streptococcus thermophilus

VSL#3 JUNIOR IS A WELCOME ADJUNCT TO THE THERAPEUTIC STRATEGIES FOR CHILDREN AND TEENAGERS WITH IBS.10
PICK FOR DIETARY MANAGEMENT OF IBS PATIENTS.
IBS IN CHILDREN AFFECTS THE ENTIRE FAMILYIn a double-blind placebo controlled study in 59 pediatric patients10
Duringthestudyperiod,caregiverswerequestioned aboutperceivedchangesinoverallfunctioningoffamily lifedisruptions.Studyshowedscorereductionsat:
•2weeksP<0.05vs.studystart
•4weeksP<0.01vs.studystart
•6weeksP<0.001vs.studystart VSL#3 was significantly superior to placebo (P<0.05)10
EffectofVSL#3andofplaceboonthecaregivers’assessmentoffamilylifedisruption.
Resultsarereportedona0-4scale(seetext).Barsindicate1SD.*P<0.05comparedwith
studystart.**P<0.01comparedwithstudystart.***P<0.001comparedwithstudystart.
#P<0.01betweenpatientswhiletakingprobioticvs.patientswhiletakingplacebo.
2.5
2
1.5
1
0.5
0
Fam
ily
lif
e d
isru
pti
on s
core
*
***
#**
*
baseline study start 2 weeks 4 weeks 6 weeks
PlaceboVSL#3
DIETARY MANAGEMENT WITH VSL#3 IMPROVES DISCOMFORT, BLOATING/GASSINESS IN PEDIATRIC IBS PATIENTS10
•PatientsreceivingVSL#3alsohadsignificantlygreater improvementsvs.bothbaselineandplaceboinabdominal discomfortandbloating/gassiness(P<0.05)
Abdominal discomfort was better when taking VSL#3 JUNIOR than when taking placebo10
ResultsofVSL#3andofplaceboonabdominaldiscomfortwerereportedona0-4scale.Bars
indicate1SD.*P<0.05comparedwithstudystart.**P<0.01comparedwithstudystart.**P<0.001
comparedwithstudystart.#P<0.05betweenpatientswhiletakingprobioticvs.patientswhile
takingplacebo
3
2.5
2
1.5
1
0.5
0
Ab
dom
inal
dis
com
fort
sco
re
PlaceboVSL#3
*
***
*#
#
**
baseline study start 2 weeks 4 weeks 6 weeks

THE POTENT PROBIOTIC THAT PRACTITIONERS LIKE YOU PICK FOR KIDS WITH IBS.
ASK THE PHARMACIST TO STOCK VSL#3 JUNIOR, THE NEWEST ADDITION TO THE VSL#3 FAMILY.
STORAGE AND RECOMMENDED DAILY INTAKE Storage instructions:
• Refrigerationmaintainsthehighpotency ofVSL#3
• Ifneeded,VSL#3canbekeptatroom temperatureforupto2weekswithout any loss of potency6 Recommended daily intake to start for IBS:
• VSL#3JUNIOR:1packet/day
• Refrigeratedtopreservehighpotency
• Contains225billionlivebacteriaand
8proprietarystrainsperpacket
• Greatnewwatermelonflavorthatkidslove
• Clinicallyproventoprovidesignificant
benefits in the dietary management
of IBS10
• Well-establishedGRASsafetyprofile
• Improvecompliance,onlytaken1x/day
References
1. FedorakRN.Gastroenterology & Hepatology2010;6:11;688-690.
2. Madsen K et al. Gastroenterology2001;121:580-591.
3. FedorakRN.J Clin Gastroenterol2008;42:S3;S111-115.
4. Caballero-FrancoCetal.Am J Physiol Gastrointest Liver Physiol
2007;292:G315-22.
5. OtteJM,PodolskyDK.Am J Physiol Gastrointest Liver Physiol
2004;286:G613–G626.
6. Dataonfile.Sigma-TauPharmaceuticals,Inc.2012.
7. MieleEetal.A. Am J Gastroenterology2009;104:437-443.
8. BasedonIRIretaildataendingweekof12.25.11.
9. HelwigUetal.World J Gastroenterol2006;12:5978-86.
10.GuandaliniSetal.J Pediatr Gastroenterol Nutr.2010;51:24-34.
11.BasedonCFUcount(dataonfile).
Made in the USA
Distributed by Sigma-Tau Pharmaceuticals, Inc., Gaithersburg MD
© 2012 Sigma-Tau Pharmaceuticals, Inc. All rights reserved. V11250712
For further information call 1-866-GET-VSL3 (438-8753)
or visit www.vsl3.com
PRODUCTS STRAINS CFU IN BILLIONS
COST PER PACKET/
CAPSULE8
VSL#3 JUNIOR 8 225 $1.80
VSL#3 CAPSULES 8 112.5 $0.87
Florastor® Kids 1 5 $0.90
Culturelle® Kids 1 1 $0.67
PROBIOTIC COMPARISON

VSL#3 SigmaTau Pharmaceuticals

VSL#3a probiotic so potent ithas to be supervised andrefrigerated. Very cool.

Formulated with a precise mix of8 proprietary strains of live bacteria
Lactobacillus acidophilus Bifidobacterium infantis*
Lactobacillus plantarum Bifidobacterium longum*
Lactobacillus paracasei Bifidobacterium breve
Lactobacillus delbrueckii subsp., bulgaricus
Streptococcus thermophilus
*Recently reclassified as B. lactis
• VSL#3 is a high potency probiotic medical food for the dietary
management of IBS, UC and an ileal pouch.
• VSL#3 must be used under medical supervision.
Lowest cost per CFU1
• Comparison of probiotic capsules available at pharmacies
Product # strains Probiotic CFU(in billions)
Cost per capsule (SRP)
Align®
capsules 1 1.0 $0.88
CulturelleTM
capsules 1 10.0 $0.59
Florastor®
capsules 1 5.0 $0.60
LactinexTM
tablets 2 0.001 $0.42
VSL#3®
capsules 8 112.5 $0.87
VSL#3 the MOST potent probiotic
Probiotic medical food available in 3 formulations
• VSL#3 Capsules 112.5 billion
bacteria per capsule
• VSL#3 450 billion bacteria
per packet
• VSL#3 DS (Rx only) 900 billion
bacteria per packet
Refrigeration preserves more live bacteria and helps maintain powerful potency
• VSL#3 is up to 100 times more
potent than the average
probiotic2
• Potency is clinically important
o A high CFU count ensures
that bacteria survive
stomach acid and bile salts
to colonize the intestinal
tract3

VSL#3 provides superior dietary management for patients with UC vs. placeboIn a double-blind, placebo-controlled,
12-week study in Ulcerative Colitis (UC)
patients (N=147), those receiving
dietary management with VSL#3
experienced:7
• Significantly higher remission rates
vs. placebo (42.9% vs 15.7%,
respectively, P=0.001)
• Significantly greater improvements
in UCDAI scores vs. placebo (32.5%
achieved ≥50% decrease by week
6 vs. 10% of the placebo group,
P=0.001)
Dietary management with VSL#3 improves IBS in adult and pediatric patients
Dietary management with VSL#3 demonstrated
benefit in 2 double-blind, placebo-controlled studies
in adult IBS patients:
• In a study of 25 patients receiving 8 weeks of
treatment, patients receiving VSL#3 experienced
significant reduction from baseline in bloating
(P=0.046)4
• In a study of 48 patients receiving 4 (n=31) or
8 (n=17) weeks of treatment, 46% of patients
receiving VSL#3 reported satisfactory relief of
bloating during at least half of their treatment
period vs. 33% in the placebo group5
In a placebo-controlled, double-blind study in 59
pediatric IBS patients, those receiving VSL#3
experienced:6
• Significantly greater improvements in SGARC
scores vs. both baseline and placebo (P<0.05)
• Significantly greater improvements in discomfort,
bloating/gassiness, and family assessment of life
disruption vs. both baseline and placebo (P<0.05)
VSL#3 Clinically proven in the dietary management of IBS and UC

• Refrigerated to preserve high potency
• Contains a high CFU count of 8 proprietary strains of live bacteria
• Lowest cost per CFU of all leading probiotic products1
• Clinically proven to provide significant benefit in the dietary
management of IBS and UC5,6
• Well-established safety profile
o Mild abdominal bloating may occur for the first few days
as intestines adjust to VSL#3.
Ordering information
VSL#3 Medical Food SKU UPC WAC SRP
VSL#3 Box of 10 packets 7-45749-01777-2 $ 23.00 $ 34.00
VSL#3 Box of 30 packets 7-45749-01778-9 $ 63.00 $ 86.00
VSL#3 Box of 30 unflavored packets 7-45749-01780-2 $ 63.00 $ 86.00
VSL#3 Bottle of 60 capsules 7-45749-01781-9 $ 37.00 $ 52.00
Rx only Medical Food SKU UPC WAC SRP
VSL#3-DS Box of 20 packets 7-45749-01782-6 $ 90.00 N/A
Made in the USADistributed by Sigma-Tau Pharmaceuticals Inc., Gaithersburg MD© 2011 Sigma-Tau Pharmaceuticals, Inc. All rights reserved.
VSL#3 a probiotic that providesclinically proven benefits. Way cool.
Storageinstructions:
• Refrigeration maintains
the high potency of
VSL#3
o Store at 39-46°F
o If required for travel,
VSL#3 can be kept
at room temperature
for up to 2 weeks
without any loss of
potency
Recommended intakes to start with:
• VSL#3 Capsules:
2 capsules/day
• VSL#3:
2 packets/day
• VSL#3 DS:
1 packet/day
V1110511
References: 1. www.drugstore.com. Accessed April 2011. 2. AC Nielsen, 12.2009. 3. Fedorak RN. Gastroenterology & Hepatol-ogy 6: 11; 688-609 (2010). 4. Kim HJ et al. Aliment Pharmacol Ther 17:895-904 (2003). 5. Kim HJ et al. Neurogastroenterol Motil 17:1–10 (2005). 6. Guandalini S et al. J Pediatr Gastroen-terol Nutr 51:24-34 (2010). 7. Sood A et al. Clin Gastroenterol Hepatol 11:1202-9 (2009).
All formulations of VSL#3 are medical foods and must be used under medical supervision. Therefore,
please make sure that patients who are considering VSL#3 talk to their healthcare provider about VSL#3.
For more information, please visit www.vsl3.com
FlorastorBiocodex USA
877-356-7787LTCDA607
Florastor Saccharomyces boulardii lyo
® Florastor Saccharomyces boulardii lyo
®
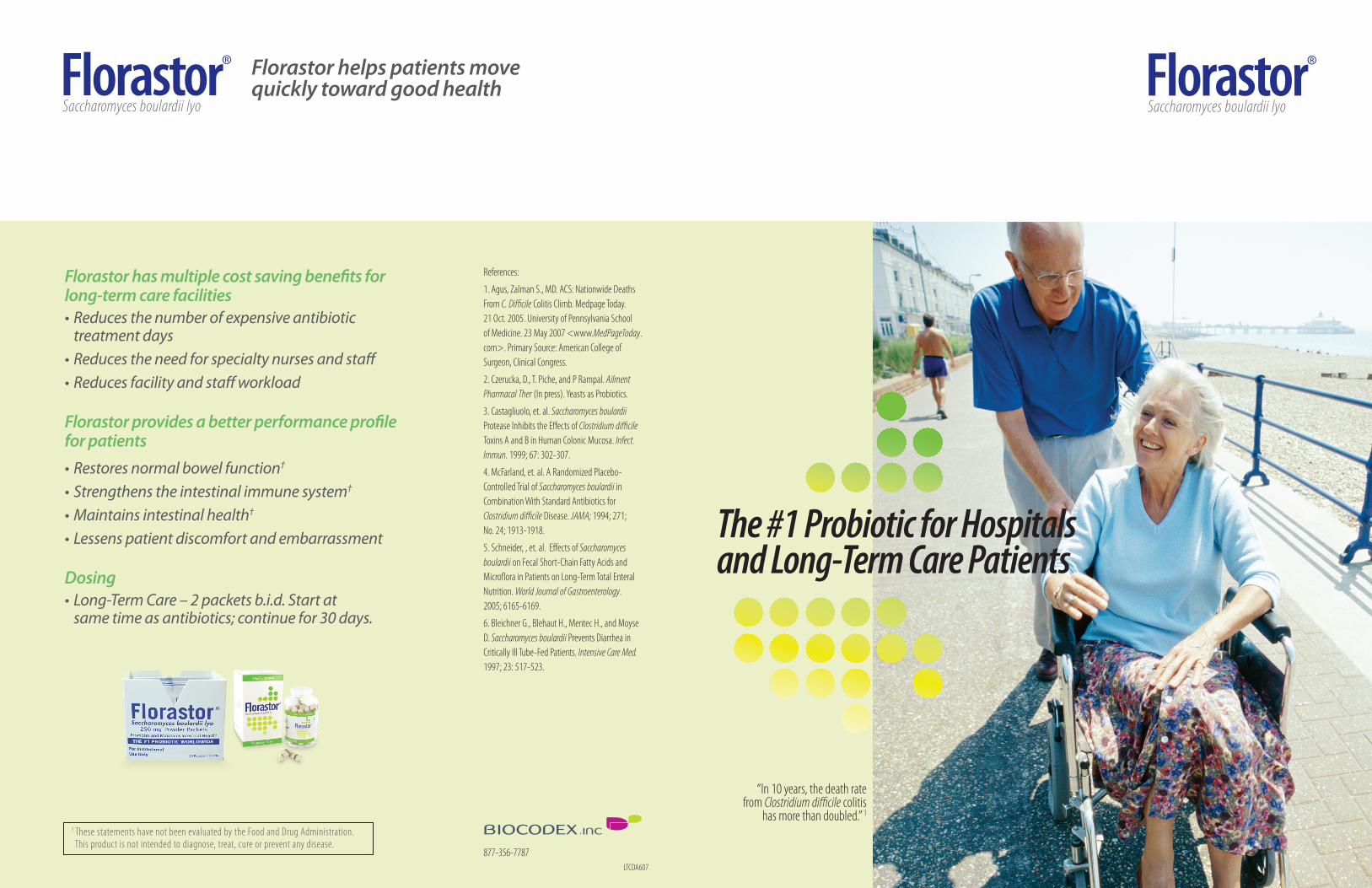
Florastor has multiple cost saving benefits for long-term care facilities•Reducesthenumberofexpensiveantibiotictreatmentdays
•Reducestheneedforspecialtynursesandstaff•Reducesfacilityandstaffworkload
Florastor provides a better performance profile for patients•Restoresnormalbowelfunction†•Strengthenstheintestinalimmunesystem†
•Maintainsintestinalhealth†
•Lessenspatientdiscomfortandembarrassment
Dosing•Long-TermCare–2packetsb.i.d.Startatsametimeasantibiotics;continuefor30days.
Florastor helps patients move quickly toward good health
References:
1. Agus, Zalman S., MD. ACS: Nationwide Deaths From C. Difficile Colitis Climb. Medpage Today. 21 Oct. 2005. University of Pennsylvania School of Medicine. 23 May 2007 <www.MedPageToday.com>. Primary Source: American College of Surgeon, Clinical Congress.
2. Czerucka, D., T. Piche, and P Rampal. Ailment Pharmacal Ther (In press). Yeasts as Probiotics.
3. Castagliuolo, et. al. Saccharomyces boulardii Protease Inhibits the Effects of Clostridium difficile Toxins A and B in Human Colonic Mucosa. Infect. Immun. 1999; 67: 302-307.
4. McFarland, et. al. A Randomized Placebo-Controlled Trial of Saccharomyces boulardii in Combination With Standard Antibiotics for Clostridium difficile Disease. JAMA; 1994; 271; No. 24; 1913-1918.
5. Schneider, , et. al. Effects of Saccharomyces boulardii on Fecal Short-Chain Fatty Acids and Microflora in Patients on Long-Term Total Enteral Nutrition. World Journal of Gastroenterology. 2005; 6165-6169.
6. Bleichner G., Blehaut H., Mentec H., and Moyse D. Saccharomyces boulardii Prevents Diarrhea in Critically Ill Tube-Fed Patients. Intensive Care Med. 1997; 23: 517-523.
† These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure or prevent any disease.
“In 10 years, the death rate from Clostridium difficile colitis has more than doubled.”
The #1 Probiotic for Hospitals and Long-Term Care Patients
“In 10 years, the death rate from Clostridium difficile colitis
has more than doubled.” 1

The #1 Probiotic Worldwide
Prevents diarrhea in critically ill and tube-fed patientsFlorastor
Saccharomyces boulardii lyo
® Florastor Saccharomyces boulardii lyo
®
Florastor is a gentle, effective and time-tested treatment for many forms of diarrhea†
•Florastorisnotabsorbedintothebloodstreamsoitwillnotinteractwithanyothermedication
•Florastorisresistanttoallantibiotics,gastricjuicesandbilesalts
Florastor has a positive effect on enteric pathogens†
•Neutralizesbacterialtoxins•Reducespro-inflammatoryresponseduringbacterialinfections2
Florastor destroys bacterial toxins associated with Clostridium difficile pathogen3
• InC. diff cases,asadjunctivetherapyFlorastorpromotesrecoveryandreducesrecurrenceby50%comparedtoplacebo4
Florastor helps treat many forms of institutional diarrhea†
•63%ofpatientswithenteralfeedingdevelopdiarrhea5
•Florastorreducesdiarrheadaysby25%6
• In“atrisk”patients,Florastorreducesdiarrheabyasmuchas52%6
Adding Florastor to ethical drug therapy will:• Increasewaterandelectrolyteabsorptionmechanisms†
•Promotecellgrowthandmaturation†
•Ensurebetterenterocytehealth†
•Reducepatientneedforfurtherantibiotictherapy†
StresamBiocodex, Inc.
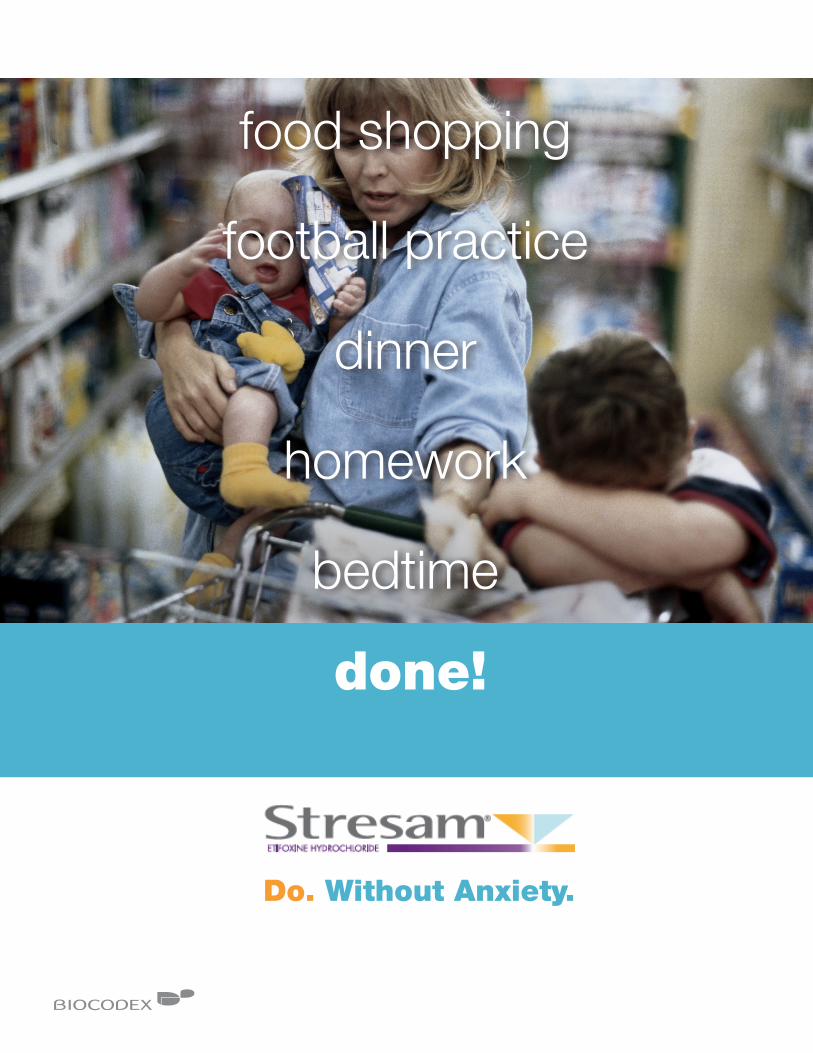
Do. Without Anxiety.
food shopping
football practice
dinner
homework
bedtime
done!

For anxiety that goes beyond what is natural for your patient...
pressure at work
moving house
children
financial stress
unemployed
tense home life
too many obligations
divorce
sick parent
too many worries
With symptoms that limit social and professional life… • 79% of anxious patients are employed 1
That can occur frequently. • 2 out of 5 people have experienced symptoms of acute anxiety at least
once in their lives 2
Severe anxiety
No anxiety
Disabling anxiety level
Stressful life events can trigger anxiety symptoms.
Dealing with anxiety is tough enough without adding the impairment of other anxiety treatments.
Autonomic
symptoms
Gastrointestinal
symptoms
Respiratory
symptoms
Cardiovascular
symptoms
Somatic
complaints
Fears
Tension
Anxious
mood

Try Stresam® first. Stresam helps people manage anxiety symptoms Proven anxiolytic efficacy among patients receiving Stresam 3
Thanks to a novel mechanism of action modulating GABAergic transmission...
Stresam offers a unique, dual mechanism of action • Stresam binds selectively to the beta subunit of the GABAAreceptor 4
• Stresam stimulates the production of neurosteroids 5
25.6
lorazepam (n=94)
Stresam® (n=91)
lorazepam (n=94)
Stresam® (n=91)
Day 0 Day 28
30%
25%
20%
15%
10%
5%
0
Anxiolytic efficacy [3]
185 patients received first-line treatment
*p = 0.0002 - Non-inferiority test
*
Pro
gres
s of
tot
al a
vera
ge
HA
M-A
sco
re in
ITT
grou
p
78.9%
lorazepam (n=96)
Stresam® (n=93)
80%
70%
60%
50%
40%
30%
20%
10%
0
Efficacy/Safety [3]
185 patients received first-line treatment
*%
of p
atie
nts
whe
re a
nxie
ty d
imin
ishe
d
with
out
und
esira
ble
effe
cts
*p = 0.0383
12.2
±6.4 ±5.9
62.6%
Stresam relieves moderate to severe symptoms in patients suffering from anxiety.
Stresam demonstrates a better therapeutic index than the comparator and avoids the side effects often seen in anti-anxiety therapy.
Do. Without Anxiety.
Stresam is the only treatment focused on managing anxiety.
11.4
±3.5±4.225.2

5. Schlichter R. et al. Modulation of GABAergic synaptic transmission by the non-benzodiazepine anxiolytic etifoxine. Neuropharmacology. 2000;39:1523-1535.
6. Micallef J. et al. A double blind parallel group placebo controlled comparison of sedative and mnesic effects of etifoxine and larazepam in healthy subjects. Fundam. Clin. Pharmacol. 2001;15:209-216.
7. SmPC January 2008 .
8. Stresam® technical file
This document, property of BIOCODEX, is reserved for the exclusive use of its partners, and under no circumstances, is to be given to the medical profession.
Dosing: 3 to 4 capsules per day
• Depending on the intensity of the patient’s anxiety, for several days to several weeks
• Maximum duration of prescription = 12 weeks
1. Semaan W. et al. Cross-sectional study of the prevalence of adjustment disorder with anxiety in general practice. L’Encephale 2001;27(3):238-44.
2. Ropper AH, Brown RH. Fatigue, Asthenia, Anxiety and Depressive Reactions. Adams and Victor’s Principles of Neurology. 8th Ed.New York,NY:McGraw-Hill Medi-cal;2005:433-441
3. Nguyen N. Fakra E. Pradel V. et al. Efficacy of etifoxine compared to lorazepam monotherapy in the treatment of patients with adjustment disorders with anxi-ety: a double-blind controlled study in general practice. Hum Psychopharmacol. 2006;2(3):139-149.
4. Verleye M. et al. Interactions of etifoxine with the chloride coupled to the GABA (A) receptor complex. Neuroreport. 1999;10:3207-3210.
See for yourself how anxiety modulation is…done.• First-line anxiolytic treatment
• With unique, dual, selectively GABAergic activity 4,5
• That modulates symptoms for effective relief 3
• With no impact on attention, alertness or memory 6
• No rebound effect 7 and no dependence 8
Do. Without Anxiety.

MyozymeGenzyme Corporation

PomPe Disease Differential Diagnosis training Manual
2011
Genzyme Corporation – Confidential – Internal Use Only2
© 2011 Genzyme Corporation
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the copyright owner.
No responsibility is assumed by the Publisher for any injury and/or damage to persons or property as a matter of products liability, through negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein. Because of rapid advances in the medical sciences, the Publisher recommends that independent verification of diagnoses and drug dosages should be made.

Genzyme Corporation – Confidential – Internal Use Only 3
CoNTeNTs
introduction ...................................................................................................................................................... 5
myozyme® vision ......................................................................................................................................... 11
Chapter 1. Neurologists and neuromuscular specialists.......................................................... 12
Chapter 2. Neuromuscular diseases .......................................................................................................
Chapter 3. a clinical approach to the differential diagnosis
of myopathic diseases ............................................................................................................
Chapter 4. Diagnostic tests used to diagnose myopathic diseases ........................................
Chapter 5. Facilitating the early diagnosis of Pompe disease ...................................................
summary ................................................................................................................................................................
Progress check answers .................................................................................................................................
abbreviations ......................................................................................................................................................
Glossary ..................................................................................................................................................................
References .............................................................................................................................................................

CerezymeGenzyme Corporation

I have...
A dream about collegeBut worry about being tired all the time
A passion for gymnasticsYet muscles too weak for the big moves
A best friend I totally understand And bone pain I don’t understand
What does it all mean?
Abbreviated Summary of Product Characteristics
Cerezyme® 200 U / Cerezyme® 400 U: powder for concentrate for solution for infusion (imiglucerase).Prescription only medicine. Product composition: Each vial of Cerezyme contains 200 U or 400 U of imiglucerase, the recombinant form of the natural form of human ß-glucocerebrosidase, and the following excipients: mannitol, sodium citrate, citric acid mono-hydrate and polysorbate 80. Cerezyme should be reconstituted with water for Injections and further diluted in 0.9% sodium chloride intravenous solution. Indication: Cerezyme is indicated for use as long-term enzyme replacement therapy in patients with a confirmed diagnosis of non-neuronopathic (Type 1) or chronic neuronopathic (Type 3) Gaucher disease and who exhibit clinically significant non-neuronological manifestations of the disease. Contraindications: hypersensitivity to the active substance or to any of the excipients. Dosage and administration: Therapy should be directed by physicians knowledgeable in the management of Gau-cher disease. Initial doses of 60 U/kg of body weight once every 2 weeks have shown improvement in haematological and visceral parameters within 6 months of therapy and continued use has either stopped progression of or improved bone disease. Administration of doses as low as 2.5 U/kg of body weight three times a week or 15 U/kg of body weight once every 2 weeks has been shown to improve haematological parameters and organomegaly, but not bone parameters. The reconstituted and diluted preparation is administered by intravenous infusion over 1 to 2 hours.
Precautions:Hypersensitivity: IgG antibodies to imiglucerase are formed in approximately 15% of the treated patients. It appears that patients will rarely develop antibodies to Cerezyme after 12 months of therapy. Patients with antibody to Cer-ezyme have a higher risk of hypersensitivity reactions.Pulmonary hypertension: Pulmonary hypertension is a known complication of Gaucher disease. It has been ob-served both in patients receiving and not receiving enzyme replacement therapy. No causal relationship with enzyme replacement therapy has been established. Patients with respiratory symptoms should be evaluated for the presence of pulmonary hypertension. Interaction: Interactions between Cerezyme and other medicinal products have not been studied. Other forms of interactions such as with food are unlikely. Pregnancy and lactation: It is not known whether Cerezyme can affect reproductive capacity, or cause foetal harm when administered to a pregnant woman, or is excreted in human milk. Therefore, caution should be exercised when Cerezyme is administered to pregnant or nursing women. Undesirable effects: In a small number of patients undesirable effects have been reported which are related to the route of administration: discomfort, pruritus, burning, swelling or sterile abscess at the site of venipuncture. In approximately 3% of the patients symptoms suggestive of hypersensitivity have been noted, like pruritus, flushing, urticaria/angioedema, chest discomfort, tachycardia, cyanosis, respiratory symptoms and paraesthesia. Hypotension associated with hypersensitivity has also been reported rarely. Additional undesirable adverse effects have been reported in a limited number of patients: headache, dizziness, nausea, vomiting, abdominal cramping, diarrhoea, rash, arthralgia, fever, rigors and fatigue. Overdose: No case of overdose has been reportedMedical or healthcare professionals are encouraged to register non-neuronopathic (Type 1) and chronic neuronopathic (Type 3) Gaucher patients in the ‘ICGG’ Gaucher Registry to enhance the understanding of the disease and evaluate the effectiveness of the treatment.
Read the full prescribing information before using the product. Status SmPC 09/2007.
Marketing authorisation holder: Genzyme Europe B.V., Gooimeer 10, 1411 DD Naarden, The Netherlands.EU/1/97/053/001-005
Cerezyme is a registered trademark of Genzyme Corporation© Genzyme Corporation Cz/29/P060/0-05/08
12 Data on file, Genzyme.22 De Fost M, Hollak CEM, Groener JMFG, et al. Increased incidence of cancer in adult Gaucher disease in Western
Europe. Blood. 2006;36:53-58.32 Data on file, Genzyme.4 2Thomson Physicians World GmbH52 Grabowsky GA, Kacena K, Hollak CEM, et al. Analysis of enzyme replacement therapy dose-response relationships
in patients with type 1 Gaucher disease. Presented at the American Association for the Study of Liver Diseases Annual Meeting, Boston, MA, November 2-6, 2007.
62 Charrow J, Dulisse B, Grabowski GA, et al. The effect of enzyme replacement therapy on bone crisis and bone pain in patients with type 1 Gaucher disease. Clin Genet 2007; 71: 205-211.
72 Wenstrup RJ, Kacena JA, Kaplan P, et al. Effect of enzyme replacement therapy with Imiglucerase on BMD in type 1 Gaucher disease. J Bone Miner Res 2007; 21:119-126.
82 Diagnose und therapie bei Morbus Gaucher. Ed. Claus Niedeau. Uni-med Science 2005. ISBN 3-89599-770-6.92 Andersson HC, Charrow J, Kaplan P, et al. Individualization of long-term enzyme replacement therapy for Gaucher
disease. Genet Med. 2005:Feb;105-110.10 Pastores G, Weinreb N, Aerts H, et al. Therapeutic goals in the treatment of Gaucher disease. Semin Hematol
2004, 41(4 Suppl 5): 4-14.11 Weinreb N, Aggio M, Andersson H, et al. Gaucher disease type 1: Revised recommendations on evaluations and
monitoring for adult patients. Semin Hematol 2004, 41(4 Suppl 5): 15-22.12 Weinreb NJ, Charrow J, Andersson HC, et al. Effectiveness of enzyme replacement therapy in 1028 patients
with type 1 Gaucher disease after 2 to 5 years of treatment: a report from the Gaucher Registry. Am J Med 2002;113:112-119.
13 Mistry P. Therapeutic Goals in Gaucher disease. Rev Med Interne. 2007 Oct;28 Suppl 2:S171-5.14 Sims KB, Pastores GM, Weinreb NJ, et al. Improvement of bone disease by imiglucerase (Cerezyme) therapy in
patients with skeletal manifestations of type 1 Gaucher disease: results of a 48-month longitudinal cohort study. Clin Genet. 2008 May; 73(5):430-40.
15 Mistry P, Sadan S, Yang R, et al. Consequences of diagnostic delays in type 1 Gaucher disease:The need for greater awareness among Hematologists–Oncologists and an opportunity for early diagnosis and intervention Am J Hema-tol. 2007 Aug;82(8):697-701.
16 Weinreb N, Barranger J, Packman S, et al. Imiglucerase (Cerezyme®) improves quality of life in patients with skel-etal manifestations of Gaucher disease. Clin Genet 2007 Jun;71(6):576-88.
17 Gaucher Registry Annual Report 2008.

Sometimes familiar symptoms don’t add up to a familiar diagnosis
Diagnosing non-familiar serious conditions requires a real problem-solver. In cases like Sophia’s, haematologists have considered the following diagnoses1:
Leukemia Multiple myeloma Myelodysplasia Immune thrombocytopenic purpuraLymphoma Viral infection Liver disease
Gaucher disease Myeloproliferative disorder
Bleeding disorder
Does this patient remind you of anyone in your practice?
And here is my story:
“When I was young, I was often ill with infections, and sometimes had abdominal pain.“
“Later, as a teenager, I had heavy menstrual bleeding. Also, I had severe pain in my knees, so I could hardly stand. I slept all the time and couldn’t keep up with my school work.” “At 19, I visited a hospital because of excruciating pain in my groin. They discovered my platelets were too low and referred me to a haematologist, who found I also had mild anaemia, thrombocytopenia, splenomegaly, and slight hepatomegaly.”
Children 2-3Adults > 65
How various conditions overlap in presentation
Manifestations
Gaucher cellson biopsy
Bone pain
Bruising/bleeding
Leukemia
Hepatomegaly
Splenomegaly
Fatigue
Typical age(years) of onset
Non-Hodgkin’slymphoma
Gaucherdisease
Multiplemyeloma
10 0-80 70
Sometimespseudo-Gauchercells
Sometimespseudo-Gauchercells
Sometimespseudo-Gauchercells
Sometimespseudo-Gauchercells
Often occursin clusters
Lesscommon
Lesscommon
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes

Before you really know the patient, you must understand the disease
A chronic progressive disease
• May cause disability, negatively impact quality of life and shorten life span
• Available treatment may reverse manifestations and prevent complications
A complex multi-systemic pathology
Inherited enzyme insufficiency •
Dysfunction of tissue macrophages • developing into Gaucher cells
Infiltration of multiple organs, such as • bone marrow, liver, and spleen
Causing cytopenia, visceromegaly and • creating a disruption in bone metabolism
Gaucher disease increases the risk of • haematological malignancies, in particular multiple myeloma (up to 50x)2
Proximal femur removed from patient with Gaucher disease showing gross pathology.
Bone marrow biopsy (HE, 40x) of patient with Gaucher disease who developed ALL.
I am Sophia and I have Gaucher disease.
The varying clinical presentations of Gaucher disease are unlikely tofitthetextbookdescriptions
Fatigue • Anaemia 37%
Bleeding tendency • Thrombocytopenia 60%
Abdominal enlargement and pain• Splenomegaly 86%• Hepatomegaly 65%
Bone problems (83%)• Marrow infiltration (81%) • Pain (34%)• Osteonecrosis sometimes accompanied by excruciating bone crises• Osteopenia (49%), osteoporosis• Pathological fractures, joint collapse and destruction
Lymphoblasts
Gaucher cells
Photo courtesy of Prof. J Barranger Photo courtesy of Prof. MD Cappellini

This is where haematologists can make all the difference
Haematologists can ensure timely intervention and prevention of irreversible complications
• Sibling and family screening may aid early detection
• Diagnostic testing in the presence of cytopenia, bleeding tendency, hepatosplenomegaly and bone pain, particularly in people from Jewish background should be considered
I am Dr. Kureti
Engaged in a demanding and busy practiceBut motivated most by a new clinical challenge
Trained in medical school to look for horsesEager as a specialist to recognize a zebra
Offering a proven treatment for a life-threatening disorderAnd providing a new perspective to a previously frustrated, undiagnosed patient
9 out of 10 patients with Gaucher disease will eventually see a haematologist
Haematology is the specialty best suited to diagnose and treat patients with Gaucher disease.
Haematologists are most likely to makeadefinitiveandearlydiagnosis
A bone marrow smear or biopsy is • not always definitive
A simple glucocerebrosidase enzyme • activity assay confirms diagnosis
DNA analysis may be done to • determine the mutations involved
Patients can present at any age, but are mostly diagnosed after childhood
0%
Order in whichphysicians areconsulted alongthe path to diagnosis3
First
Second
Third
Fourth
Fifth +
Perc
enta
ge o
f pat
ient
s se
ekin
g di
agno
sis
100%
80%
20%
40%
60%
Pedi
atri
cian
Fam
ily /
GP
Endo
crin
olog
ist
Gas
troe
nter
olog
ist
Gen
etic
ist
Hae
mat
olog
ist
/ O
ncol
ogis
t
Neu
rolo
gist
Ort
hopa
edic
Sur
geon
Rhe
umat
olog
ist
Oth
er
30%
20%
10%
0%11-20 71-8051-6041-5031-4021-30< 10
Age of diagnosis of Gaucher disease4

Cerezyme lets patients live the lives they have chosen for themselves
This is Cerezyme (imiglucerase), the gold standard for treating Gaucher disease
• Prevents, halts and/or reverses disease pathology
• Reduces morbidity and prevents complications
• Improves or normalizes quality of life
0
-1
-20 42 6 8
Dose-dependent improvement in bone mineral density with Cerezyme®7
Normal healthy populationGaucher patients not treated with CerezymeCerezyme 60 U/kg BW/2 wksCerezyme 30 U/kg BW/2 wksCerezyme 15 U/kg BW/2 wks
Years on Cerezyme
Lum
bar
sp
ine
DE
XA
Z-s
core
% p
atie
nts
60
119
38
74*
10*
71*
1*
73*
6*
50
40
30
20
10
01 2 3
Reduction in bone pain and criseswith Cerezyme therapy
Year before therapy
Years on Cerezyme
% patients reporting bone pain (n=244)% patients reporting bone crisis (n=219)
Cerezyme® dose-response
relationship in patients withtype 1 Gaucher disease5
Platelet count
Cerezyme 60 U/kg BW/2 wksCerezyme 30 U/kg BW/2 wksCerezyme 15 U/kg BW/2 wks
Pla
tele
t co
un
t (x
103 /m
m3 )
Months following initiation of imiglucerase
180
165
150
135
120
105
90
75
60
0 12 24 36 48 60 72 84 96
Treatment is simple
Patients are infused with Cerezyme usually • once every 2 weeks
The recommended initial dose is 60 U/kg • BW/2 wks in children and adults at increased risk of continued, progressive, or new-onset complications9
Maintenance dosing and dose adjustments • should be based on results of regular comprehensive monitoring, aiming to maintain all therapeutic goals10,11
Experts can help develop an individualised • monitoring and management plan for your patients
Outcomes are proven More than 15 years and ± 40,000 patient years of documented efficacy and safety
Improvements are dose dependent
Initial doses of 60 U/kg BW/2 wks have • shown improvement in haematological and visceral parameters
Changes in blood parameters and • liver/spleen volumes may be seen within 6 months of starting therapy
Treatment at 60U/ kg BW/2 wks • resulted in improvement in bone pain as early as 3 months, a decrease in bone crises within 12 months, normalisation of aspects of quality of life and improve-ment in osteopenia of the lumbar spine or femoral neck at 24 months6
Near normalisation of bone density of • the lumbar spine in adults however may take 8 years2 Asterisks indicate significant change (p<0.05).
Before and after MRI of bone marrowinfiltrationwithCerezyme®
at 60 U/kg body weight for 3 years8
Images courtesy of Dr LW Poll
Within 6 months of initiation, continued use has either stopped progression of or improved bone disease
Before After

Cerezyme at a glance
Clinical success
Cerezyme can reverse the symptoms of Gaucher disease12
Cerezyme prevents long-term irreversible complications such as bone disease, life-threatening bleeding and need for splenectomy2,13,14
Early diagnosis and treatment with Cerezyme significantly reduces morbidity and improves quality of life15,16
Cerezyme is the gold standard of care in Gaucher disease management13
Commitment Cerezyme’s efficacy and safety are well documented for more than 15 years, representing around ± 40,000 patient years of use.17
Our support for the Gaucher community spans diagnosis, information and infusion resources, education, ongoing pioneering research, and the International Collaborative Gaucher Group (ICGG) patient registry
The ICGG tracks outcomes of routine clinical practice. •
Data on over 5,000 patients in nearly 60 countries has • been collected to help establish treatment guidelines
Genzyme is committed to supporting health care providers caring for people affected by Gaucher disease
Committed to sustainable access to therapy for • people with Gaucher disease
Committed to researching and developing • treatments for people living with Gaucher disease
I am Sophia
21 years oldRecent graduate
Living with GaucherStarting a new career
Need more time to relaxAlways time for Cerezyme

SepraSprayGenzyme Corporation

HELP PROTECT YOUR PATIENT’S FUTURE WITH SEPRASPRAYTM
SEPRASPRAY IS INTENDED AS AN ADJUNCT IN ABDOMINAL, PELVIC AND THORACIC SURGERY TO REDUCE THE INCIDENCE, EXTENT AND SEVERITY OF POSTOPERATIVE ADHESIONS, AND TO REDUCE ADHESIVE SMALL BOWEL OBSTRUCTION WHEN PLACED IN THE ABDOMEN.
Well-studied compound with proven efficacy—same active compound as •Seprafilm® (sodium hyaluronate/carboxymethylcellulose [HA/CMC])
Established safety profile—no contraindications •
Innovative spray formulation—easy to use in both laparoscopy and laparotomy •
Cost-effective—helps lower costs by reducing hospital readmissions, reducing •operating room time, and preventing complications such as adhesive small bowel obstruction 1-4[Bristow 2007, Kusunoki 2005, Ellis 1999, Fazio 2005]
CONTACT US FOR MORE INFORMATION TODAY
Call XXX-XXX-XXXX or visit www.sepraspray.xx to receive a product demonstration and/or and assistance with internal purchasing presentations
REORDER # NAME HOW SUPPLIED COVERAGE AREA
ALL PRODUCTS ABOVE ARE CLASS III MEDICAL DEVICES
6510–20 Sepraspray Kit 200 1 gram spray, Sprayer, Cannula 200 cm2
6510–40 Sepraspray Kit 400 2 grams spray, Sprayer, Cannula 400 cm2
6610–20 Sepraspray Re-Load 200 1 gram spray re-load 200 cm2
6610–40 Sepraspray Re-Load 400 2 gram spray re-load 400 cm2
4301–03 Seprafilm Adhesion Barrier 1 sheet per pouch10 pouches per box 200 cm2
©2009 Genzyme Corporation. Sepraspray, Seprafilm and Genzyme are registered trademarks of Genzyme Corporation, Cambridge, Massachusetts, USA.
TM
Bristow RE, Santillan A, Diaz-Montes TP, et al. Prevention of adhesion formation after radical hysterectomy using a sodium hyaluronate-carboxymethylcellulose (HA-CMC) barrier: a cost-effectiveness analysis. Gynecol Oncol. 1. 2007;104(3):739-46.Kusunoki M, Ikeuchi H, Yanagi H, et al. Bioresorbable hyaluronate-carboxymethylcellulose membrane (Seprafilm) in surgery for rectal carcinoma: a prospective randomized clinical trial. Surg Today. 2005;35(11):940-5.2. Ellis H, Moran B, Thompson J, et al. Adhesion-related hospital readmissions after abdominal and pelvic surgery: a retrospective cohort study. Lancet. 1999; 353:1476-1480.3. Fazio V, Cohen Z, Fleshman J, et al. reduction in adhesive small-bowel pbstrauction by Seprafilm® adhesion barrier after intestinal resection. Dis Colon Rectum. 2005;49:1-11.4.

TM
ADHESIONS: A FREQUENT COMPLICATION WITH UNDER-RECOGNIZED DANGERS
ADHESIONS ARE NOT PREVENTABLE BY SURGICAL TECHNIQUE ALONE 1-2[DeWilde 2007, Menzies, Ellis 1990]
Adhesions develop routinely following open and laparoscopic abdominal surgery, and are reported at second-look surgery to occur in 93% of patients following initial laparotomy. 2[Menzies 1990, Ellis 1990]
ADHESIONS MAY HAVE SERIOUS CONSEQUENCES
Complicated surgeries
Inadvertant enterotomy
Secondary infertility
Adhesions prolong operative time and limit access to surgical sites 8-10[Beck 2000, VanGoor 2007, Coleman 2000]
Adhesions are the primary reason for conversion from laparoscopy to laparotomy 9[Veldkamp 2004]
Adhesions increase risk of iatrogenic bowel injury by 10% to 25% 11-12[van der Krabben 1999, Swank 2003]
Adhesions are the leading cause of secondary female infertility (reported to cause 20% to 40% of cases) 13[DeWilde 2007]
INTRODUCING SEPRASPRAYTM
Efficacy and safety profile of HA/CMC is well established by extensive Seprafilm trials and clinical history
A sprayable powder formulation of Sodium Hyaluronate/Carboxymethylcellulose (HA/CMC)—two bioresorbable, inert, non-animal-derived polysaccharides
Spray formulation is easy to use in both open and laparoscopic surgery
Offers targeted, site-specific coverage
Sepraspray efficacy has been demonstrated in a prospective, randomized, controlled, double-blinded preclinical study to significantly reduce adhesions com-pared to untreated controls (N=60) [Colt, ASRM 2005 abstract]
CLINICAL BENFITS
NOW HA/CMC IS AVAILABLE IN AN INNOVATIVE SPRAY FORMULATION
THE TRUSTED ACTIVE COMPOUND IN SEPRAFILM®
Adhesive Small Bowel Obstruction
Lysis of dense pelvic adhesions
Small bowel obstruction (SBO)
Adhesions are responsible for up to 80% of reported cases 3[Farinella 2009]
Adhesive SBO has a high risk of recurrence with mortality rates ranging from 3% to10% 3-7[Farinella XXX, Menzies 2001, Roseano 2007, Wysocki 2003, Fevang 2004]
DeWilde RL, Trew G. Postoperative abdominal adhesions and their prevention in gynaecological surgery. Expert consensus position. Part 2─steps to reduce adhesions. Gynecol Surg. 2007;4:243-1. 253. Menzies D, Ellis H. Intestinal obstruction from adhesionshow big is the problem? Ann Royal Coll Surg Eng. 1990;72:60-63. 2. Farinella E, Cirocchi R, La Mura F, et al. feasibility of laparoscopy for small bowel obstruction. World J Emerg Surg. 4:3. 3. [NOTE: this article is a study report, but fact cited in MS comes from another study referenced in the intro of this one]Menzies D, Parker M, Hoare R, et al. Small bowel obstruction due to postoperative adhesions: treatment patterns and associated costs in 110 hospital admissions. Ann R Coll Surg Engl. 4. 2001;83:40-46.Roseano M, Dobrinja C, Turoldo A, et al. [Adhesive small bowel occlusion: a clinical and therapeutic study of 163 consecutive patients. Article in Italian. Chir Ital. 2007;59(5):651-9.5. Wysocki A, Poźniczek M, Kulawik J, et al. [Peritoneal adhesions as cause of small bowel obstruction. Article in Polish]. Przegl Lek. 2003;60 Suppl 7:32-5.6. Fevang BT, Fevang J, Lie SA. Long-term prognosis after operation for adhesive small bowel obstruction. Ann Surg. 2004;240(2):193-201.t7. Beck DE, Ferguson MA, Opelka FG, et al. Effect of previous surgery on abdominal opening time. Dis Colon Rectum. 2000;43(12):1749-53.8. van Goor H. Consequences and complications of peritoneal adhesions. Colorectal Dis. 2007;9(Suppl 2):25-34.9. Coleman MG, McLain AD, Moran BJ. Impact of previous surgery on time taken for incision and division of adhesions during laparotomy. Dis Colon Rectum. 2000;43(9):1297-9.10. Van Der Krabben AA, Dijkstra FR, Nieuwenhuijzen M, et al. Morbidity and mortality of inadvertent enterotomy during adhesiotomy. Br J Surg. 2000;87(4):467-71.11. Swank D, Swank-Bordewijk S, Hop W, et al. Laparoscopic adhesiolysis in patients with chronic abdominal pain: a blinded randomised controlled multi-centre trial. Lancet. 361:1247-1251.12. [NOTE: this article is a study report, but fact cited in MS comes from another study referenced in the intro of this one]De Wilde R, Trew G. Postoperative abdominal adhesions and their prevention in gynaecological surgery. Expert consensus position. Gynecol Surg. 2007;4:161-168.13.
Colt J, Corazzini R, Skinner K, et al. Abstract presented at American Society of Reproductive Medicine 1. meeting, 2005.[NOTE: the ref provided by the client did not include the full citation for this, so not sure how to site…]
check reference

TM
As demonstrated in prospective, randomised Seprafilm® clinical trials,
HA/CMC REDUCES ADHESIONS AND SIMPLIFIES REOPERATIONS
As demonstrated in prospective, randomised Seprafilm® clinical trials,
HA/CMC SIGNIFICANTLY REDUCES ADHESION-RELATED MORBIDITY
Randomised, prospective,
multicenter, international,
single-blind trial evaluat-
ing the use of HA/CMC
(as Seprafilm) to prevent
ASBO in patients under-
going intestinal resection
(N=1701; mean follow-up
3.5 yr). 1[Fazio 2005]
Randomised, prospective
double-blind, multicenter
study (N=183) evaluating
the use of HA/CMC
(Seprafilm) to prevent
adhesions in patients
undergoing 2-stage
intestinal resection. 1[Becker 1996]
Randomised, prospective
trial (N=59) evaluating the
use of HA/CMC (Seprafilm)
in cancer patients to
prevent adhesions after
radical rectal resection.2[Kusunoki]
DECREASED REOPERATIVE ADHESIVE SMALL BOWEL OBSTRUCTION (ASBO)
DECREASED EARLY POST-OPERATIVE INTESTINAL OBSTRUCTION (EPSBO)
SIGNIFICANTLY REDUCED THE INCIDENCE OF ADHESIONS
100
90
80
70
60
50
40
30
20
10
0
94%
49%
P<.001
% P
atie
nts
wit
h A
dhes
ions
HA/CMC-treated patientswere 8.5 times
more likely to be adhesion-free
Untreatedcontrols (n=90)
HA/CMC-treatedpatients (n=89)
Randomised, prospective
trial evaluating the use of
HA/CMC (Seprafilm) to re-
duce early post-operative
SBO (within 30 days) after
colorectal cancer surgery
(N=427). 2[Park 2009]
P<.043
P<.045
7%
47% risk reduction
66% risk reduction
Becker JM, Dayton MT, Fazio VW, et al. Prevention of postoperative abdominal adhesions by a sodium hyaluronate-based bioresorbable membrane: a prospective, randomized, double-blind 1. multicenter study. J Am Coll Surg. 1996;183(4):297-306. Kusunoki M, Ikeuchi H, Yanagi H, et al. Bioresorbable hyaluronate-carboxymethylcellulose membrane (Seprafilm) in surgery for rectal carcinoma: a prospective randomized clinical trial. Surg Today. 2. 2005;35(11):940-5.
Fazio V, Cohen Z, Fleshman J, et al. reduction in adhesive small-bowel pbstrauction by Seprafilm® 1. adhesion barrier after intestinal resection. Dis Colon Rectum. 2005;49:1-11.Park CM, Lee WY, Cho YB, et al. Sodium hyaluronate-based bioresorbable membrane (Seprafilm) 2. reduced early postoperative intestinal obstruction after lower abdominal surgery for colorectal cancer: the preliminary report. Int J Colorectal Dis. 2009;(3):305-10.
SIMPLIFIED OSTOMY REVERSAL
P<.05
TM
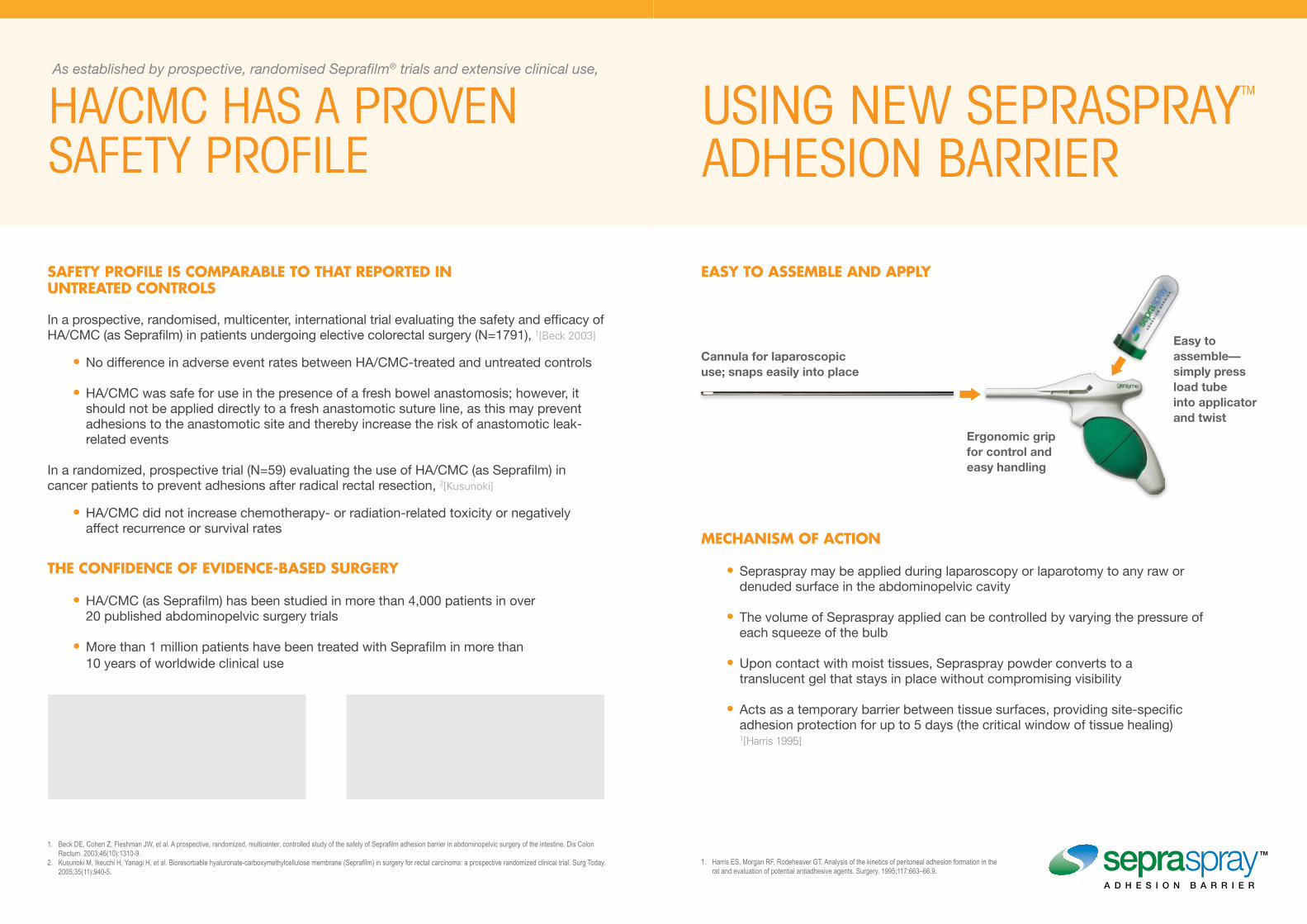
As established by prospective, randomised Seprafilm® trials and extensive clinical use,
HA/CMC HAS A PROVEN SAFETY PROFILE
SAFETY PROFILE IS COMPARABLE TO THAT REPORTED IN UNTREATED CONTROLS
In a prospective, randomised, multicenter, international trial evaluating the safety and efficacy of HA/CMC (as Seprafilm) in patients undergoing elective colorectal surgery (N=1791), 1[Beck 2003]
No difference in adverse event rates between HA/CMC-treated and untreated controls •
HA/CMC was safe for use in the presence of a fresh bowel anastomosis; however, it •should not be applied directly to a fresh anastomotic suture line, as this may prevent adhesions to the anastomotic site and thereby increase the risk of anastomotic leak-related events
In a randomized, prospective trial (N=59) evaluating the use of HA/CMC (as Seprafilm) in cancer patients to prevent adhesions after radical rectal resection, 2[Kusunoki]
HA/CMC did not increase chemotherapy- or radiation-related toxicity or negatively •affect recurrence or survival rates
THE CONFIDENCE OF EVIDENCE-BASED SURGERY
HA/CMC (as Seprafilm) has been studied in more than 4,000 patients in over •20 published abdominopelvic surgery trials
More than 1 million patients have been treated with Seprafilm in more than •10 years of worldwide clinical use
MECHANISM OF ACTION
Sepraspray may be applied during laparoscopy or laparotomy to any raw or •denuded surface in the abdominopelvic cavity
The volume of Sepraspray applied can be controlled by varying the pressure of •each squeeze of the bulb
Upon contact with moist tissues, Sepraspray powder converts to a •translucent gel that stays in place without compromising visibility
Acts as a temporary barrier between tissue surfaces, providing site-specific •adhesion protection for up to 5 days (the critical window of tissue healing) 1[Harris 1995]
EASY TO ASSEMBLE AND APPLY
USING NEW SEPRASPRAYTM ADHESION BARRIER
Cannula for laparoscopic use; snaps easily into place
Easy to assemble— simply press load tube into applicator and twist
Ergonomic grip for control and easy handling
Beck DE, Cohen Z, Fleshman JW, et al. A prospective, randomized, multicenter, controlled study of the safety of Seprafilm adhesion barrier in abdominopelvic surgery of the intestine. Dis Colon 1. Rectum. 2003;46(10):1310-9. Kusunoki M, Ikeuchi H, Yanagi H, et al. Bioresorbable hyaluronate-carboxymethylcellulose membrane (Seprafilm) in surgery for rectal carcinoma: a prospective randomized clinical trial. Surg Today. 2. 2005;35(11):940-5.
Harris ES, Morgan RF, Rodeheaver GT. Analysis of the kinetics of peritoneal adhesion formation in the 1. rat and evaluation of potential antiadhesive agents. Surgery. 1995;117:663–66.9.