massive acute aortic regurgitation after infected pacemaker lead removal: a word of caution
TRANSCRIPT

ofrclitor
AwbctatHcudmswt
irBtevg(f
cn
ohbthotistol
aivnps(habTstpvabWww
ufoitu
Hlp
Massive Acute Aortic RegurgitationAfter Infected Pacemaker LeadRemoval: A Word of CautionMichele Rossi, MD, Francesco Pirone, MD,Sunil Nair, MD, and Uday Trivedi, MD, FRCS-ChT
Departments of Cardiac Surgery and Cardiology, Royal SussexCounty Hospital, Brighton, United Kingdom
We report a case of massive acute aortic valve regurgita-tion in a 54-year-old man secondary to a percutaneousextraction of infected permanent pacemaker leads. Thiscase emphasizes how carefully patients should be mon-itored during and after the procedure, regardless of theirhemodynamic status. The patient successfully under-went urgent surgical intervention.
(Ann Thorac Surg 2011;92:e29–31)© 2011 by The Society of Thoracic Surgeons
Management of infected permanent pacemaker(PPM) devices is challenging and requires collab-
rative efforts between cardiologists, surgeons, and in-ective disease specialists. Standard treatment includesemoval of infected PPM devices combined with antimi-robial therapy. Percutaneous removal of infected PPMeads is not free from deleterious complications, includ-ng traumatic rupture of intracardiac structures and sys-emic embolization of infected material. We report a casef massive acute aortic valve regurgitation secondary toemoval of infected PPM leads.
54-year-old man presented to the emergency roomith a low-grade temperature, malaise, and shortness ofreath. His past medical and surgical history includedongenital left kidney atrophy with preserved renal func-ion and dual chamber PPM implant for Mobitz type IItrioventricular block 2 years earlier. On examination,he patient was tachycardiac and hypotensive (70/40 mm
g). Renal function was significantly deranged with areatinine of 5.67 mg/dL, urea 51 mg/dL, and a glomer-lar filtration rate of 11 mL/min. An arterial blood gasemonstrated metabolic acidosis. A plain computed to-ographic scan of the chest showed bilateral lung con-
olidation. Fluid resuscitation and intravenous antibioticsere started on the likely diagnosis of lower respiratory
ract infection complicated by sepsis.The following day, the patient was transferred to the
ntensive care unit for further respiratory support andenal replacement therapy due to acute renal failure.lood cultures were positive for Staphylococcus aureus and
argeted antibiotic therapy was started. Transesophagealchocardiogram showed vegetations on the atrial andentricular pacing leads with mild tricuspid valve regur-itation and multiple vegetations on the tricuspid valveFig 1). The aortic valve had a trileaflet configuration andunctioned normally with no vegetations seen (Fig 2).
For the next 2 days, the patient remained afebrile and hisondition improved with a complete recovery in hemody-amic and renal function. He was reviewed by our cardiol-
Accepted for publication March 17, 2011.
Address correspondence to Dr Rossi, Department of Cardiac Surgery,
eRoyal Sussex County Hospital, Eastern Rd, Brighton, BN2 5BE UK; e-mail:[email protected].
© 2011 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
gy team and scheduled for a percutaneous extraction ofis infected PPM system. The pacing leads were removedy simple traction under local anesthesia and mild seda-
ion. After removal, the patient was stable but in completeeart block at 60 bpm with an unsupported blood pressuref 150/45 mm Hg. A decision was made not to place aransvenous temporary pacing wire to minimize the risk ofnfection. Unfortunately, 3 hours later, an acute onset ofhortness of breath, hypotension, and oliguria developed inhe patient. An urgent transthoracic echocardiogram dem-nstrated, new, severe aortic regurgitation through a pro-
apsing noncoronary cusp (Fig 3).The patient was referred to the cardiothoracic team
nd was urgently transferred to the operating room. Anntraoperative inspection revealed that the tricuspidalve appeared to be completely destroyed. The noncoro-ary cusp of the aortic valve had torn away and wasrolapsing toward the left ventricle. A small ventriculareptal defect was also noticed below the aortic annulusFig 4). These lesions, secondary to PPM extraction, mayave resulted from an extension of the infective processnd formation of adhesions between the leads, the fi-rous trigone of the heart, and the aortic valve structures.ricuspid and aortic valve replacement with bioprosthe-es were performed. Of surgical note, the implantation ofhe aortic prosthesis was performed prior to the tricuspidrosthesis. This allowed for enhanced visualization of theentricular septal defect and prevented distortion of theortic annulus. The ventricular septal defect was closedy direct closure with interrupted mattress stitches.eaning from cardiopulmonary bypass was achievedith the use of an intra-aortic balloon pump and pacingith temporary epicardial wires.The patient was discharged from the intensive care
nit on postoperative day 8. He remained in the hospitalor 6 weeks to complete a course of intravenous antibi-tics. The patient subsequently underwent a new PPM
mplantation with the ventricular lead inserted throughhe coronary sinus. At his 6-month follow-up he contin-es to be asymptomatic and well.
Comment
Mortality rates for infected PPM devices range from 31%to 66% when the device is not explanted. Better out-comes, with mortality rates of 18% or less, have beenreported when a combined management with deviceremoval and antimicrobial therapy is adopted [1, 2]. AsPPM insertion rates have been constantly rising for thepast decade, it is becoming more likely to encounter anincreasing number of infective complications related tothese devices in our clinical practice [3 ,4]. Device-relatedendocarditis has been reported in 23% of infected PPMs,the remainder being pocket infections [5]. Pacemaker-related sepsis or endocarditis is a class I indication forlead extraction, according to the North American Societyof Pacing and Electrophysiology guidelines [6, 7]. Inaccordance with the current literature, the best outcomeis achieved with percutaneous removal of infected de-vices by applying external traction on the leads [5, 8].
owever, this relatively short and simple procedure canead to catastrophic complications, ranging from embolichenomena to tricuspid valve injury, subclavian vein lac-
ration, hemothorax, pocket hematoma, massive hemor-0003-4975/$36.00doi:10.1016/j.athoracsur.2011.03.116
r
e30 CASE REPORT ROSSI ET AL Ann Thorac SurgAORTIC REGURGITATION AFTER PACEMAKER EXTRACTION 2011;92:e29–31
rhage, and lead fracture requiring surgical intervention[6–8].
We believe that our case showed an unprecedentedcomplication of infected pacing lead extraction with ven-tricular septal defect formation and massive acute aorticregurgitation, requiring urgent surgical treatment. Intra-operative cultures of the aortic valve and ventricularseptal defect edges did not show any significant growth,supporting the hypothesis that the prolapse of the non-coronary cusp was due to lack of support on the valvestructure. This also highlights how carefully these pa-tients should be monitored during and after extractionregardless of their hemodynamic status. Because acutehemodynamic decompensation may result from trau-matic rupture of intracardiac structures adhered to theinfected lead, we believe that performing the lead extrac-
Fig 1. Pre-lead extraction transesophageal echocardiography four-chamber view shows multiple vegetations on the tricuspid valve(long arrow) and pacing leads (short arrow). (LA � left atrium;LV � left ventricle; RA � right atrium; RV � right ventricle.)
Fig 2. Pre-lead extraction transesophageal echocardiography mid-esophageal short-axis view shows a competent tri-leaflet aortic
valve. (LA � left atrium; RA � right atrium; RV � right ventricle.) vtion under general anesthesia and within the vicinity ofan operating room would be prudent. A cardiothoracicsurgical team should be available to assist, if required.Echocardiography should be performed in all patientsprior to leaving the catheter laboratory. In cases that areperformed under general anesthesia, intraoperativetransesophageal echocardiogram would be the recom-mended choice, which has been safe, cost effective, andideally suited for prompt detection of life-threateningcomplications that warrant urgent surgical intervention.
Fig 3. Post-lead extraction. Transthoracic echocardiography para-sternal long axis view of the aortic valve. Prolapse of the noncoro-nary cusp (white arrow). (Ao � aorta; LV � left ventricle; RV �ight ventricle.)
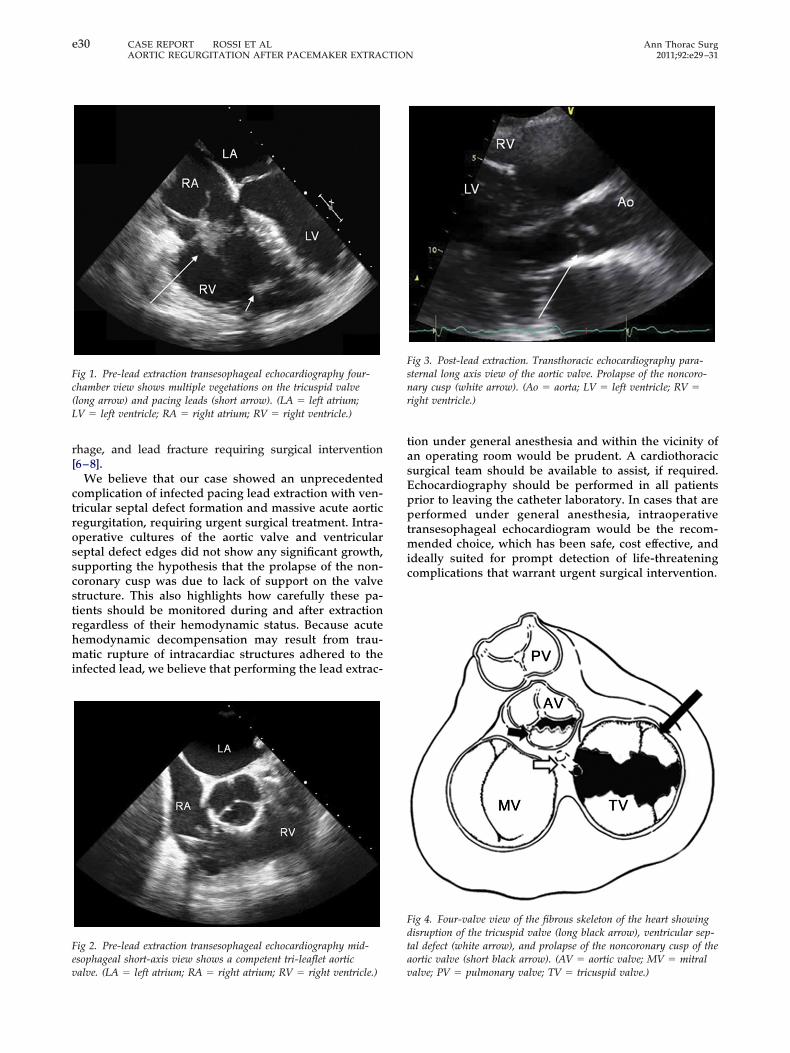
Fig 4. Four-valve view of the fibrous skeleton of the heart showingdisruption of the tricuspid valve (long black arrow), ventricular sep-tal defect (white arrow), and prolapse of the noncoronary cusp of theaortic valve (short black arrow). (AV � aortic valve; MV � mitral
alve; PV � pulmonary valve; TV � tricuspid valve.)
e31Ann Thorac Surg CASE REPORT ROSSI ET AL2011;92:e29–31 AORTIC REGURGITATION AFTER PACEMAKER EXTRACTION
References
1. Cacoub P, Leprince P, Nataf P, et al. Pacemaker infectiveendocarditis. Am J Cardiol 1998;82:480–4.
2. Klug D, Lacroix D, Savoye C, et al. Systemic infection relatedto endocarditis on pacemaker leads: clinical presentation andmanagement. Circulation 1997;95:2098–107.
3. Zhan C, Baine WB, Sedrakyan A, Steiner C. Cardiac device im-plantation in the United States from 1997 through 2004: a popula-tion-based analysis. J Gen Intern Med 2008;23(Suppl 1):13–9.
4. Voigt A, Shalaby A, Saba S. Rising rates of cardiac rhythmmanagement device infections in the United States: 1996through 2003. J Am Coll Cardiol 2006;48:590–1.
5. Sohail MR, Uslan DZ, Khan AH, et al. Management and outcome
of permanent pacemaker and implantable cardioverter-defibrillator infections. J Am Coll Cardiol 2007;49:1851–9.6. Love CJ, Wilkoff BL, Byrd CL, et al. Recommendations forextraction of chronically implanted transvenous pacing anddefibrillator leads: indications, facilities, training. NorthAmerican Society of Pacing and Electrophysiology Lead Ex-traction Conference Faculty. Pacing Clin Electrophysiol 2000;23(4 Part 1):544–51.
7. Wilkoff BL, Love CJ, Byrd CL, et al; Heart Rhythm Society;American Heart Association. Transvenous lead extraction:Heart Rhythm Society expert consensus on facilities, training,indications, and patient management: this document wasendorsed by the American Heart Association (AHA). HeartRhythm 2009;6:1085–104.
8. Ruttmann E, Hangler HB, Kilo J, et al. Transvenous pace-maker lead removal is safe and effective even in large vege-
tations: an analysis of 53 cases of pacemaker lead endocardi-tis. Pacing Clin Electrophysiol 2006;29:231–6.