massmutual prescription drug addendum effective january 1...
TRANSCRIPT

MassMutual Prescription Drug Addendum October 2014 Page 1 of 22
MassMutual Prescription Drug Addendum
Effective January 1, 2014
This Addendum to the Medical Summary Plan Descriptions (SPDs), published in October 2014, takes the place of any SPDs and Summaries of Material Modifications (SMMs) previously issued to you describing your benefits.
MassMutual Prescription Drug Addendum October 2014 Page 2 of 22
Table of Contents
Introduction ................................................................................................................................................................ 3
Contact Information.................................................................................................................................................... 4
How Prescription Drug Coverage Works ................................................................................................................... 5
Schedule of Benefits ................................................................................................................................................. 12
Exclusions and Limitations ...................................................................................................................................... 13
Claiming Benefits ..................................................................................................................................................... 15
Appeals Procedure .................................................................................................................................................... 17
Coordination of Benefits .......................................................................................................................................... 20
Dictionary Terms ...................................................................................................................................................... 21
MassMutual Prescription Drug Addendum October 2014 Page 3 of 22
Introduction
MassMutual’s prescription drug coverage is available when you are covered under one of the following MassMutual medical options: • Cigna High Deductible Health Plan (HDHP) Option (Option 1 or Option 2); • Cigna Open Access Plus In-Network (OAPIN) Option (for OppenheimerFunds participants only); • Cigna Hawaii Preferred Provider Organization (Hawaii PPO) Option; • Cigna Med 500 Preferred Provider Organization (Med 500 PPO) Option; or • Cigna Med 500 Indemnity, Med 1300 Indemnity or Med 2500 Indemnity Options.
This Prescription Drug Addendum applies to all participants covered under these medical options, which includes eligible employees and retired employees of MassMutual and OppenheimerFunds, as well as eligible active and retired career agents, general agents and general managers of MassMutual. Therefore, not all information in this Addendum will apply to you.
Note: If your medical option is not listed above, see the summary plan description for your medical option, which includes details about your prescription drug coverage.
Prescription drug coverage described in this addendum is administered by Express Scripts.
You will need to satisfy the requirements described in your medical option Summary Plan Description (SPD) to receive coverage. Be sure to read through this addendum to learn more about how this coverage works and what is and is not covered.
MassMutual Prescription Drug Addendum October 2014 Page 4 of 22
Contact Information
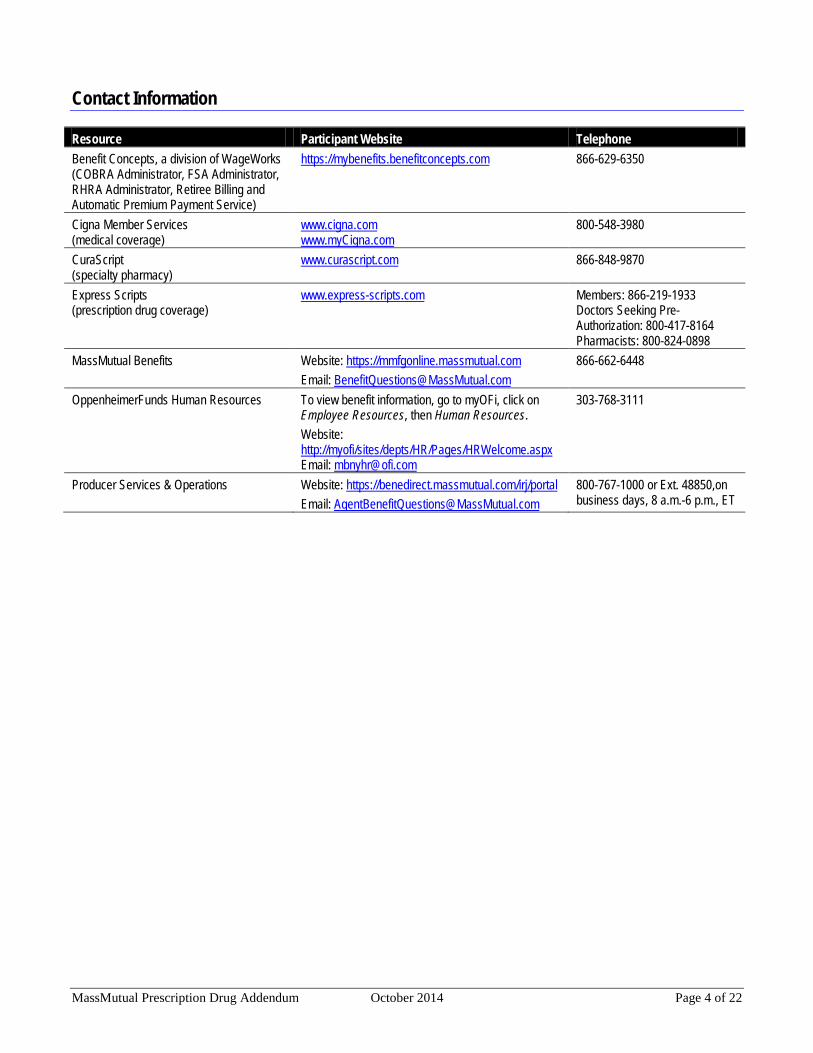
Resource Participant Website Telephone Benefit Concepts, a division of WageWorks (COBRA Administrator, FSA Administrator, RHRA Administrator, Retiree Billing and Automatic Premium Payment Service)
https://mybenefits.benefitconcepts.com 866-629-6350
Cigna Member Services (medical coverage)
www.cigna.com www.myCigna.com
800-548-3980
CuraScript (specialty pharmacy)
www.curascript.com 866-848-9870
Express Scripts (prescription drug coverage)
www.express-scripts.com Members: 866-219-1933 Doctors Seeking Pre-Authorization: 800-417-8164 Pharmacists: 800-824-0898
MassMutual Benefits
Website: https://mmfgonline.massmutual.com Email: [email protected]
866-662-6448
OppenheimerFunds Human Resources To view benefit information, go to myOFi, click on Employee Resources, then Human Resources. Website: http://myofi/sites/depts/HR/Pages/HRWelcome.aspx Email: [email protected]
303-768-3111
Producer Services & Operations Website: https://benedirect.massmutual.com/irj/portal Email: [email protected]
800-767-1000 or Ext. 48850,on business days, 8 a.m.-6 p.m., ET

MassMutual Prescription Drug Addendum October 2014 Page 5 of 22
How Prescription Drug Coverage Works
This coverage provides prescription drugs and related supplies provided by retail and home delivery pharmacies as shown in this addendum. To receive prescription drug benefits, you and your dependents may be required to pay a portion of the covered expenses, as described in this section.
If you are a retiree or a dependent of a retiree and are eligible for Medicare, you will not have this prescription drug coverage if you elect Medicare prescription drug coverage (Part D).
Deductible
The deductible is the amount you and/or your dependent are required to pay before prescription drug coverage is payable by the Plan. For more information about how your deductible works, please see your medical SPD.
High Deductible Health Plan (Options 1 and 2) and Med 500 PPO
Medical and prescription drug deductibles are combined. This means that covered medical and prescription drug expenses all apply toward the same deductible and that deductible must be met before the Plan begins to pay most medical and prescription drug covered expenses. Once the deductible maximum has been reached, you and/or your dependents do not need to satisfy any further deductible for the rest of the year. For more information about how your deductible works, please see your medical SPD.
OAPIN, Hawaii PPO and Med 500, 1300 and 2500 Indemnity Options
Prescription drug coverage includes a separate deductible, which applies only toward prescription drug coverage. Medical expenses may be subject to a separate deductible; if so, expenses do not apply to both deductibles. Once the prescription drug deductible has been reached, you and/or your dependents do not need to satisfy any further prescription drug deductible for the rest of the year.
Coinsurance
Coinsurance is the percentage of prescription charges that you are required to pay for certain covered expenses after you meet your deductible, up to the per-prescription coinsurance maximum. The percentage you pay differs based on the drug tier and whether you order a 30- or 90-day supply. In addition, the percentage you pay is based on the “net” cost of the medication; the net cost is the cost after applicable discounts, which may vary by pharmacy.
Drug Tier
The amount you pay depends on the type of medication, which may be a: • Generic medication (tier 1); • Preferred brand-name medication (tier 2); or • Non-preferred brand-name medication (tier 3).
To find out which tier your drug is in, contact Express Scripts at the number on your ID card or visit www.express-scripts.com.
Note: Several states, including Massachusetts, have mandatory generic substitution laws. This means that in states with laws supporting mandatory substitution, generic substitutions can be made without notifying you or your provider. Talk to your provider for more information about generic drug substitutions.

MassMutual Prescription Drug Addendum October 2014 Page 6 of 22
Per-Prescription Maximum
After your deductible is satisfied, the coinsurance amount you pay per 30- or 90-day supply for a prescription is a percentage of the prescription cost, but is limited to a specific, flat-dollar maximum.
Annual Out-of-Pocket Maximum
This is the maximum you and/or your dependents pay in a calendar year before the Plan begins to pay 100% of covered expenses. The maximum includes amounts you pay toward your deductible and coinsurance. For more information about how your out-of-pocket maximum works, please see your medical SPD.
High Deductible Health Plan (Options 1 and 2) and Med 500 PPO
The annual out-of-pocket maximum is a combined maximum for medical and prescription drug costs. This means that covered medical and prescription drug expenses both apply toward the same maximum and once that maximum is met, the Plan pays 100% of most covered medical and prescription drug expenses for the rest of the year. For more information, see your medical SPD.
OAPIN, Hawaii PPO and Med 500, 1300 and 2500 Indemnity Options
The prescription drug coverage maximum is separate from your medical out-of-pocket maximum. Medical expenses are subject to a separate maximum; expenses do not apply to both maximums. Once the prescription drug maximum is met, the Plan pays 100% of covered prescription drug expenses for the rest of the year.
Medications Covered at 100% (No Deductible or Coinsurance)
Certain medications are covered at 100%, with no deductible or coinsurance required. You are required to have a prescription from your doctor for these medications to be processed at 100% through the Express Scripts system. If you have a prescription from your doctor, you do not need to meet the deductible or pay any coinsurance for the following medications: • Eligible smoking cessation medications. • Generic, over-the-counter aspirin (to prevent cardiovascular disease) for men ages 45-79 and women ages 55-
79. • Generic fluoride for children ages six months through five years. • Generic, over-the-counter or prescription folic acid for women of childbearing age. • Generic, over-the-counter or prescription iron supplements for children ages 6 to 12 months who are at
increased risk for iron-deficiency anemia. • Immunizations, as recommended by the CDC vaccination schedule (available at
www.cdc.gov/vaccines/schedules/easy-to-read/index.html). • Certain colonoscopy-related preparation prescriptions, limited to two per year for participants ages 60 through 75. • Vitamin D supplements for participants age 65 and older provided the supplement contains up to 1,000 I.U. of
Vitamin D2 or D3 per dose. Covered supplements can include tablets that contain calcium. You can have your prescription for a Vitamin D supplement (containing up to 1,000 I.U. of Vitamin D2 or D3 per dose) filled at a participating retail pharmacy or through the mail-order service.

MassMutual Prescription Drug Addendum October 2014 Page 7 of 22
• The plan also covers two prescriptions in 365 days for colonoscopy prescriptions (“bowel preps”) for participants age 50 to age 75.
• Certain contraceptive drugs and devices. Note: The contraceptive must be a generic or a brand-name with no generic equivalent. If you choose a brand-name instead of a generic, you pay the same you would pay for other medications (see the Schedule of Benefits). However, if your prescriber writes a prescription for a brand-name for which a generic equivalent is available and indicates that it should be dispensed as written (DAW), then the prescription will be covered at 100%. For specific information about contraceptive drugs and devices, contact Express Scripts at the number on your ID card or visit www.express-scripts.com.
Preventive Medications
For certain prescription medications classified as preventive by the federal government, the deductible does not apply and you pay only your coinsurance, subject to the per-prescription coinsurance maximum. What you pay in coinsurance will apply toward your out-of-pocket maximum.
For more information on what medications are considered preventive, and therefore not subject to the deductible, contact Express Scripts at the number on your ID card or review Express Scripts’ Preventive Drug flyer at www.express-scripts.com.
Using a Retail Pharmacy
Express Scripts has a national network of over 64,000 participating pharmacies. You can have your prescription filled at a retail pharmacy for up to a 30-day supply.
When filling a prescription you must: • Get a prescription from your physician for up to a 30-day supply; • Bring your prescription to a participating pharmacy; • Show your Express Scripts ID card to the pharmacist; • Verify that the pharmacist has the correct information about you; and • Pay your coinsurance (if you have not yet met your deductible, you may need to pay the entire cost of the
medication).
Contact Express Scripts at the number on your ID card or visit www.express-scripts.com for a list of pharmacies that participate in the network.
Using the Home Delivery Pharmacy
The Express Scripts Home Delivery Pharmacy is a mail-order service that provides a convenient way for you to order up to a 90-day supply of medications to be delivered directly to your home.
To use the Express Scripts Home Delivery Pharmacy program, follow this easy step-by-step ordering process: • For new medications, ask your physician to write two prescriptions:
o One for up to a 90-day supply, plus up to three refills, to be ordered through the Home Delivery Pharmacy program; and
o One for up to a 30-day supply, to be filled immediately at a local Express Scripts-participating retail pharmacy for use until you receive your prescription order from the Home Delivery Pharmacy.
• Obtain and complete a Home Delivery Patient Profile Form. These forms are mailed to you when you receive your first prescription drug ID card. You can also print one from www.express-scripts.com.
• Send your completed form with your prescription(s) to the Express Scripts Pharmacy at the address listed on the form.
MassMutual Prescription Drug Addendum October 2014 Page 8 of 22
Note: Any prescription for more than a 30-day supply must be filled through the Express Scripts Home Delivery Pharmacy.
Prescription Drug Formulary
The Express Scripts preferred drug list (formulary) is a list of brand-name and generic medications that are preferred by the Plan. This list offers access to safe and effective medications in all therapy classes based on guidance from an independent group of expert health professionals. Medications are selected because they can safely and effectively treat most medical conditions while helping to contain costs for you and the Plan. The Express Scripts formulary of preferred drugs contains thousands of commonly prescribed medications. For more information, contact Express Scripts at the number on your ID card or view the formulary online at www.express-scripts.com.
Not all medications are covered on the Express Scripts formulary. If you are prescribed a medication that is not on the formulary, talk to your doctor. He or she can identify and prescribe an appropriate alternative that will effectively treat your condition. For more information, contact Express Scripts at the number on your ID card or view the formulary online at www.express-scripts.com.
If you fill a prescription for a medication that is not covered, your claim will be rejected. If you still want the medication, you may pay the full, non-discounted retail price. Note: Out-of-pocket costs for excluded medications do not apply to your deductible or out-of-pocket maximum.
Specialty Pharmacy Program
Under the Prescription Drug Program, you must order specialty medications through CuraScript, Express Scripts’ specialty pharmacy.
Note: If you need to fill a specialty drug immediately, you may get one 30-day supply at a retail pharmacy. Thereafter, you will be required to fill with CuraScript. If you do not fill with CuraScript, you will be required to pay 100% of the cost.
Specialty medications are usually injectable, or oral and infused medications for specific conditions. These medications often require special storage and shipping and may not be readily available at your local pharmacy. If you are taking or are prescribed a specialty medication, you will receive information about this program directly from CuraScript. Please visit www.curascript.com or call 888-773-7376 for additional information regarding CuraScript, the specialty pharmacy.
With CuraScript, you will receive additional benefits: • Program enrollment is completed with just one phone call to CuraScript; CuraScript then calls your physician
for the prescription and calls you to schedule delivery. • Convenient overnight delivery to your home, work or physician’s office within 48 hours of ordering. • Consultation with a pharmacist or nurse experienced in injectable medications available 24 hours a day. • Contact from CuraScript initiating delivery arrangements and refill reminders each month. • A team of patient care coordinators who serve as your healthcare advocates. These highly trained experts
work with your physician and the Plan to obtain prior authorization and coordinate claims and billing.

MassMutual Prescription Drug Addendum October 2014 Page 9 of 22
Quantity Limits
With CuraScript, you can only order up to a 30-day supply of your specialty medications. There is an exception to the 30-day supply maximum. You may be allowed to fill a 90-day supply of your specialty drug prescription through CuraScript if: • You have been taking the medication, in its current dosage, for at least six months; and • The medication is:
o A growth hormone; o Used to treat Multiple Sclerosis; or o Used to treat certain inflammatory conditions.
Your doctor must contact Express Scripts for pre-authorization (see the Pre-Authorization section) and verify that you have been on the same medication and dosage for at least six months. If pre-authorized, your copayment is the same copayment amount that you would pay for a 90-day supply.
Drug Quantity Management Program
The Drug Quantity Management Program is designed to ensure that you receive the medication you need in a quantity considered safe by the Food and Drug Administration (FDA), the drug’s manufacturer and medical studies.
With this program, you are always able to leave the pharmacy with the allowed amount of medicine. If you require a quantity greater than the amount initially allowed, your doctor can request an exception by contacting Express Scripts and providing information about you and your prior use of the medication.
The Drug Quantity Management Program includes a list of medications, which is available at www.express-scripts.com. This list is subject to change as new drugs are approved by the FDA and brought to market.
Step Therapy
Step therapy is a method of treating a medical condition with the most cost-effective and safest drug therapy first, and then progressing to other more costly or risky therapies only if necessary, with the goal of minimizing risks and controlling costs.
If your prescription is subject to step therapy, your pharmacist will contact your prescribing provider to approve a lower-cost alternative before your prescription is filled. If approved, the lower-cost alternative will be dispensed. If your provider does not agree with the substitute, he/she must request and receive prior authorization from Express Scripts for the pharmacist to dispense as written. For more information, contact Express Scripts.
Step therapy applies to certain prescription drug categories when a prescription is filled for the first time. Note: If you wait 130 days or more after the last prescription refill, you will have to go through the step therapy process again.

MassMutual Prescription Drug Addendum October 2014 Page 10 of 22
For a listing of prescription drug categories that are subject to step therapy (and pre-authorization), contact Express Scripts at the number on your ID card or visit www.express-scripts.com. Following are some of the categories that are currently included: • ADHD stimulants; • Alpha-1 proteinase inhibitors (subject to pre-
authorization); • Alzheimer’s disease; • Asthma/allergy; • Atopic dermatitis; • Benign prostatic hypertrophy; • Blood pressure, angiotensin receptor blockers; • Cancer; • Cholesterol; • Cryopyrin-associated periodic syndrome
(subject to pre-authorization); • Depression; • Erythroid stimulants (subject to pre-
authorization); • Gout; • Growth hormones (subject to pre-authorization); • Hepatitis; • Hypercholesterolemia;
• Hypertension; • Infections/acne; • Infertility (subject to pre-authorization); • Inflammatory conditions (subject to pre-
authorization); • Insomnia; • Migraine treatments; • Multiple sclerosis (subject to pre-authorization); • Narcotic oral pain relievers; • Osteoporosis; • Pain and inflammation/arthritis; • Prostate cancer GnRH analogs (subject to pre-
authorization); • Pulmonary arterial hypertension (subject to pre-
authorization). • Seizures/nerve-related pain; • Skin inflammation/itching; • Stomach acid; and • Urinary frequency and incontinence.
In addition, preauthorization is required for compound medications used to treat a variety of conditions.
The list of medications included in the step therapy program is updated on a regular basis and is subject to change. Contact Express Scripts at the number on your ID card or visit www.express-scripts.com for the most current listing of medications subject to step therapy.
If your prescription falls into one of these categories, it is subject to step therapy; however if you have already completed a step therapy program, you do not need to go through the step therapy process again, unless your prescription changes or you let your current prescription lapse for 130 days or more before refilling.
Pre-Authorization
Pre-authorization is required for some medications before they will be covered under the Plan. The pre-authorization process is designed to encourage safe, cost-effective use of prescription medications by confirming the medical necessity of a specific medication before it is approved for coverage. Pre-authorization focuses on medications that may have risks, serious side effects, dangerous drug interactions, or restrictions for use with a specific condition.

MassMutual Prescription Drug Addendum October 2014 Page 11 of 22
For a listing of conditions with medications that require pre-authorization contact Express Scripts. Some conditions with medications currently requiring pre-authorization include, but are not limited to: • Acne and other skin conditions; • Anemia; • Asthma/COPD; • Blood cell deficiency; • Blood thinners; • Bone health; • Cancer; • Chemical dependence; • Diabetes; • Dry eyes; • Emphysema; • Endocrine disorders; • Erectile dysfunction; • Fungal infections; • Genetic based therapy; • Glaucoma; • Growth conditions; • Hepatitis;
• Immune serums; • Infantile spasms; • Infections; • Inflammatory conditions; • Mental health; • Multiple sclerosis; • Muscle spasms; • Narcolepsy; • Narcotic pain medications; • Osteoporosis; • Psoriasis; • Pulmonary hypertension; • RSV prevention; • Seizures; • Skin conditions; • Testosterone products; • Topical wound care; and • Weight conditions.
The list of medications that require pre-authorization is updated on a regular basis and is subject to change. The above conditions do not represent all conditions with medications where pre-authorization is required. Contact Express Scripts for the most current listing of medications requiring pre-authorization.
If you know at your medical appointment that your prescription requires pre-authorization, ask your health care professional to call Express Scripts at 800-417-8164. Otherwise, ask your pharmacist to contact either your health care professional or Express Scripts at 800-824-0898. Only your health care professional (or sometimes a pharmacist) can give Express Scripts the information needed to see if your medication can be covered. Express Scripts’ pre-authorization phone lines are open 24 hours a day, seven days a week, so a determination can be made right away.
If your physician requests coverage for a prescription medication for which pre-authorization is required, your physician may contact Express Scripts to request the pre-authorization. If the request is approved, your physician and the pharmacy system will receive confirmation to allow you to have your prescription filled.
If the request is denied, you and your physician will be notified. If you disagree with the denial, you may appeal that decision in accordance with the provisions of the Plan.
Covered Expenses
Covered expenses include charges made by a pharmacy for medically necessary prescription medications and related supplies ordered by a licensed physician, registered nurse practitioner or physician’s assistant for you and/or your eligible, covered dependent(s) while eligible for prescription drug coverage. Coverage also includes medically necessary prescription medications and related supplies dispensed for a prescription issued to you or your covered dependents by a licensed dentist for the prevention of infection or pain in conjunction with a dental procedure.
MassMutual Prescription Drug Addendum October 2014 Page 12 of 22
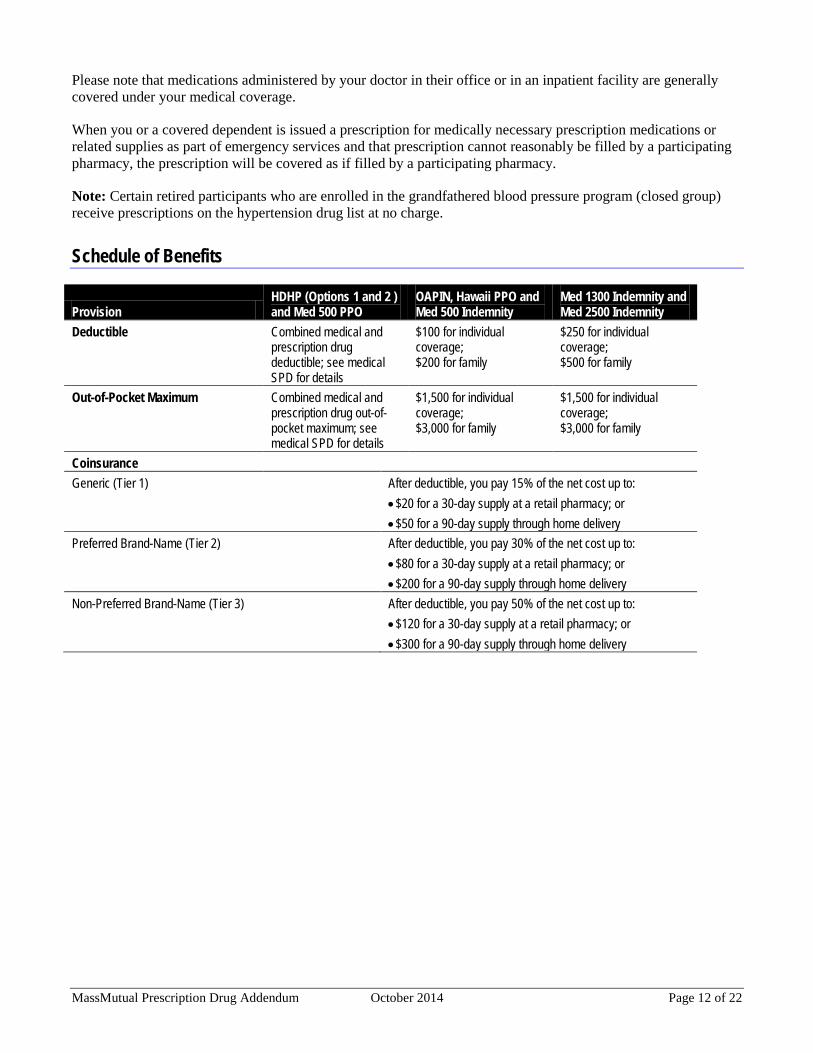
Please note that medications administered by your doctor in their office or in an inpatient facility are generally covered under your medical coverage.
When you or a covered dependent is issued a prescription for medically necessary prescription medications or related supplies as part of emergency services and that prescription cannot reasonably be filled by a participating pharmacy, the prescription will be covered as if filled by a participating pharmacy.
Note: Certain retired participants who are enrolled in the grandfathered blood pressure program (closed group) receive prescriptions on the hypertension drug list at no charge.
Schedule of Benefits
Provision HDHP (Options 1 and 2 ) and Med 500 PPO
OAPIN, Hawaii PPO and Med 500 Indemnity
Med 1300 Indemnity and Med 2500 Indemnity
Deductible Combined medical and prescription drug deductible; see medical SPD for details
$100 for individual coverage; $200 for family
$250 for individual coverage; $500 for family
Out-of-Pocket Maximum Combined medical and prescription drug out-of-pocket maximum; see medical SPD for details
$1,500 for individual coverage; $3,000 for family
$1,500 for individual coverage; $3,000 for family
Coinsurance Generic (Tier 1)
After deductible, you pay 15% of the net cost up to: • $20 for a 30-day supply at a retail pharmacy; or • $50 for a 90-day supply through home delivery
Preferred Brand-Name (Tier 2) After deductible, you pay 30% of the net cost up to: • $80 for a 30-day supply at a retail pharmacy; or • $200 for a 90-day supply through home delivery
Non-Preferred Brand-Name (Tier 3) After deductible, you pay 50% of the net cost up to: • $120 for a 30-day supply at a retail pharmacy; or • $300 for a 90-day supply through home delivery

MassMutual Prescription Drug Addendum October 2014 Page 13 of 22
Exclusions and Limitations
No payment will be made for any of the following. • Drugs available over-the-counter that do not require a prescription by federal or state law, except as otherwise
specified as covered (for example, over-the-counter medications used for preventive care may be covered if they are prescribed).
• Drugs, other than insulin, that do not require a federal legend (a federal designation for drugs requiring supervision of a physician).
• Any drug, other than insulin, that is a pharmaceutical alternative to an over-the-counter drug. • Alternative medications or vitamins that are not FDA approved. • A drug class in which at least one of the drugs is available over the counter and the drugs in the class are
deemed to be therapeutically equivalent. • Injectable drugs that require physician supervision and are not typically considered self-administered drugs.
Note: Medications administered in a physician’s office or healthcare facility may be covered under your medical benefits.
• Food and Drug Administration (FDA) approved drugs used for purposes other than those approved by the FDA.
• Prescription and non-prescription supplies, such as ostomy supplies, devices and appliances other than related supplies.
• Experimental or investigational drugs. • Drugs used for cosmetic purposes, such as drugs used to reduce wrinkles, promote hair growth, control
perspiration or fade cream products. • Diet pills or appetite suppressants (anorectics), except some drugs used to treat morbid obesity. • Immunization agents, biological products for allergy immunization, biological sera, blood, blood plasma and
other blood products or fractions and medications used for travel prophylaxis. • Replacement of prescription drugs and/or related supplies due to loss or theft. • Drugs used to enhance athletic performance. • Drugs that are to be taken by or administered to you while you are a patient in a licensed hospital, skilled
nursing facility, rest home or similar institution that operates on its premises or allows to be operated on its premises a facility for dispensing pharmaceuticals. Note: Medications administered in a physician’s office or healthcare facility may be covered under your medical benefits.
• Prescriptions in excess of dosage and/or dispensing limits. • Prescriptions more than one year from the original date of issue. • Expenses that you or any one of your dependents is in any way paid or entitled to payment for, by or through
a public program, other than Medicaid. • Expenses for or in connection with an injury or sickness that is due to war, declared or undeclared. • Charges that you are not obligated to pay, for which you are not billed or for which you would not have been
billed except that they were covered under this Plan.

MassMutual Prescription Drug Addendum October 2014 Page 14 of 22
• Expenses for or in connection with experimental, investigational or unproven services. Other than expenses for any items or services consistent with the coverage provided in this addendum that is typically covered for a qualified individual who is not enrolled in a clinical trial. Experimental, investigational and unproven services are medical, surgical, diagnostic, psychiatric, substance abuse or other health care technologies, supplies, treatments, procedures, drug therapies or devices that are determined by utilization review to be: o Not demonstrated, through existing peer-reviewed, evidence-based, scientific literature, to be safe and
effective for treating or diagnosing the condition or sickness for which its use is proposed; o Not approved by the Food and Drug Administration (FDA) or other appropriate regulatory agency to be
lawfully marketed for the proposed use; o The subject of review or approval by an institutional review board for the proposed use; or o The subject of an ongoing phase I, II or III clinical trial.
• Prescription drugs for a person age 65 or older covered under a MassMutual medical option as a retiree or their dependent who is enrolled in Medicare prescription drug coverage (Part D).
• Prescription drugs for a person on Medicare due to a disabling condition covered under a MassMutual medical option as a retiree or their dependent who is enrolled in Medicare prescription drug coverage (Part D).
• Prescription drugs denied by a primary plan because they were received from a non-participating provider (for example, a prescription drug will not be covered under this Plan if it would have been covered under your primary plan if you had followed that plan’s provisions).
• Expenses for or in connection with an injury or sickness arising out of, or in the course of, any employment for wage or profit.
• Charges that would not have been made if the person had no insurance. • Expenses incurred outside the United States or Canada, unless you or your dependent is a U.S. or Canadian
resident and the charges are incurred while traveling on business or for pleasure. • Charges made by any covered provider who is a member of your family or your dependent’s family. • Prescription drug costs for an infant child of a dependent, unless the infant child is otherwise eligible under
the Plan. • Prescription drug costs for non-medically necessary prescription drugs or related supplies.
MassMutual Prescription Drug Addendum October 2014 Page 15 of 22
Claiming Benefits
Filing a Claim
When you or your dependents purchase your prescription at a participating retail pharmacy or through the home delivery program, you pay any applicable coinsurance or deductible at the time of purchase. You do not need to file a claim form.
If you need to purchase a covered medication without your ID card, or if you purchase a covered medication from a non-participating pharmacy, your pharmacist will charge you the full price and you must submit a claim for eligible reimbursement. If you lose your ID card or need help submitting a claim for reimbursement, contact Express Scripts.
Claim forms are available from Express Scripts Member Services. Read the Express Scripts Prescription Drug Claim Form carefully, fill it out completely and sign it. Incomplete forms will be returned, causing a delay in payment. Send the completed claim form with the original prescription receipts from the pharmacy to the address listed on the form.
Note: If you pay cash at a pharmacy and you do not show your Express Scripts ID card at the time of purchase, you will not receive negotiated, discounted pricing and your deductible and coinsurance will be applied to the full purchase price if you complete a paper claim reimbursement form later.
Foreign Care Claims
If you are an expatriate or are traveling outside the country when you need to have a prescription filled, you will need to pay for your prescription when you have it filled and then submit a claim for reimbursement. Contact MassMutual Benefits, OppenheimerFunds Human Resources or Producer Services & Operations for more information. However, note that prescriptions for medications that are not approved by the FDA are not covered by the Plan; see the Exclusions and Limitations section.
Claim Determinations on Prescriptions That Do Not Require Pre-Authorization
If you or your authorized representative submits a paper claim relating to medications or supplies that do not require prior authorization, a determination will be made within 30 days after the claim is received. You or your authorized representative will be notified of a decision within this 30-day period.
Claim Determinations on Prescriptions that Require Pre-Authorization
Prior authorization requests submitted to Express Scripts will be treated as a pre-service claim. A decision regarding a pre-authorization request will be made within 15 days after Express Scripts receives your request. Your physician will be notified within this 15-day period if the pre-authorization is approved. If pre-authorization is denied, you or your authorized representative will be notified in writing within this 15-day period.
If a Claim Is Denied or Reduced
If your claim for benefits is denied or reduced, or if your coverage is rescinded (or cancelled) on a retroactive basis, you will be notified in writing of the reason for the denial. The notice will include: • The specific reason or reasons for the adverse determination; • Information sufficient to identify the claim;

MassMutual Prescription Drug Addendum October 2014 Page 16 of 22
• Reference to the specific Plan provisions on which the determination is based; • A description of any additional material or information necessary to correct the claim and an explanation of
why such material or information is necessary; • A description of the Plan’s internal appeals and external review procedures and the time limits applicable,
including a statement of your rights to bring a civil action under Section 502(a) of ERISA following an adverse benefit determination on appeal;
• Upon request and free of charge, a copy of any internal rule, guideline, protocol or other similar criterion that was relied upon in making the adverse determination regarding your claim, and an explanation of the scientific or clinical judgment for a determination that is based on a Medical Necessity, experimental treatment or other similar exclusion or limit;
• In the case of a claim involving urgent care, a description of the expedited review process applicable to that claim; and
• Contact information for any applicable office of health insurance consumer assistance or ombudsman that will assist you with internal claims and appeals and the external review process.

MassMutual Prescription Drug Addendum October 2014 Page 17 of 22
Appeals Procedure
For this section, any reference to “you” or “your” also refers to a representative or provider designated by you to act on your behalf, unless otherwise noted.
If you are dissatisfied with a denial of a paper claim or pre-authorization request, you may contact Express Scripts Member Services and/or appeal the decision.
Start with Member Services
As an alternative, or in addition, to an appeal, you may contact Express Scripts to clarify any questions you have regarding why your claim was denied. You are not required to contact Member Services before appealing.
Appeals Process
There is a two-step appeals procedure for coverage decisions. To initiate an appeal, you must submit a request for an appeal in writing to Express Scripts within 180 days of receipt of a denial notice. You should state the reason why you feel your appeal should be approved and include any information supporting your appeal. If you are unable or choose not to write, you may ask Express Scripts to register your appeal by telephone. Call or write to Express Scripts at the toll-free number or address on your benefit identification card, explanation of benefits or claim form. Express Scripts is the ERISA claims fiduciary and has full authority to determine claims and appeals under this coverage.
Exception: Send appeals related to Plan eligibility matters (including loss or denial of coverage) within 180 days of loss or denial of coverage to the Claims Review Committee. If your appeal to the Claims Review Committee is denied, you may initiate a second-level appeal with the Plan Administrative Committee. Decisions made by the Plan Administrative Committee are final. The Claims Review and Plan Administrative Committees may be contacted at:
MassMutual Benefits 1295 State Street, F105 Springfield, MA 01111-0001
Your appeal must be filed within 180 days of the date you receive the notice of denial.
Level One Appeal
As part of your appeal, you can submit written comments, documents, records or other information relating to your claim. In addition, you will be provided, upon written request and free of charge, reasonable access to (and copies of) all documents, records and other information relevant to your claim. The review will take into account all comments, documents, records and other information submitted relating to the claim regardless of whether the information was submitted or considered in the initial benefit determination. However, no consideration will be given to the initial denial of your claim during the review of the claim or appeal. Your appeal will be reviewed and the decision made by someone not involved in the initial decision. Appeals involving medical necessity or clinical appropriateness will be considered by a health care professional.

MassMutual Prescription Drug Addendum October 2014 Page 18 of 22
If any new or additional information (evidence) is considered, relied upon or generated by Express Scripts in connection with your appeal, Express Scripts will provide this information to you as soon as possible and sufficiently in advance of its decision, so that you will have an opportunity to respond. Also, if any new or additional rationale is considered by Express Scripts, Express Scripts will provide the rationale to you as soon as possible and sufficiently in advance of its decision so that you will have an opportunity to respond. Express Scripts will also provide you with the identity of any medical experts involved in the initial decision. • 15 calendar days after receipt of the appeal for an appeal involving a pre-authorization claim; or • 30 calendar days after receipt of an appeal that does not relate to a pre-authorization determination.
You may request that the appeal process be expedited if the time frames under this process would seriously jeopardize your life, health or ability to regain maximum functionality or in the opinion of your physician would cause you severe pain that cannot be managed without the requested services.
Express Scripts’ physician reviewer, in consultation with the treating physician, will decide if an expedited appeal is necessary. When an appeal is expedited, Express Scripts will respond by telephone with a decision within 72 hours, followed up in writing.
Level Two Appeal
If you are dissatisfied with the level one appeal decision, you may request a second review from Express Scripts. To initiate a level two appeal, follow the same process required for a level one appeal.
For an appeal involving pre-authorization, a determination will be made within 15 calendar days; for all other appeals, a determination will be made within 30 calendar days.
You will be notified in writing of the decision within five business days after a determination is made.
As with a level one appeal, you may be eligible to request an expedited appeal review. When an appeal is expedited, Express Scripts will respond by telephone with a decision within 72 hours, followed up in writing.
If an Appeal Is Denied
If your appeal is denied, you will be notified in writing of the reason for the denial. The notice will include: • The specific reason or reasons for the adverse determination; • Information sufficient to identify the claim; • Reference to the specific Plan provisions on which the determination is based; • A statement that you are entitled to receive, upon request and free of charge, reasonable access to and copies
of all documents, records and other relevant information as defined; • A description of any additional voluntary appeal procedures offered by the Plan, including the opportunity for
you to request an external review by an independent review organization, and a statement of your rights to bring a civil action under Section 502(a) of ERISA following an adverse benefit determination on your level two appeal;
• Upon request and free of charge, a copy of any internal rule, guideline, protocol or other similar criterion that was relied upon in making the adverse determination regarding your claim, and an explanation of the scientific or clinical judgment for a determination that is based on a medical necessity, experimental treatment or other similar exclusion or limit; and
• Contact information for any applicable office of health insurance consumer assistance or ombudsman that will assist you with internal claims and appeals and the external review process.

MassMutual Prescription Drug Addendum October 2014 Page 19 of 22
Independent Review Procedure
If you are not fully satisfied with the level two appeal review decision regarding a medical necessity, clinical appropriateness or rescission of coverage issue, you may request that your appeal be referred to an Independent Review Organization. The Independent Review Organization is composed of persons who are not employed by Express Scripts or any of its affiliates. A decision to use the voluntary level of appeal will not affect your rights to any other benefits under the Plan.
There is no charge for you to initiate this Independent Review Process. Express Scripts will abide by the decision of the Independent Review Organization.
To request a referral to an Independent Review Organization, the reason for the denial must be based on a medical necessity or clinical appropriateness determination or a rescission of coverage. Administrative, eligibility or benefit coverage limits or exclusions are not eligible for appeal under this process.
To request a review, you must notify the Appeals Coordinator within four months of your receipt of a level two appeal review denial. Within five business days after receipt of the request, Express Scripts will complete a preliminary review to determine if your claim is eligible for external review, and provide you with notice of its decision within one business day.
If your request is complete but not eligible for review, the notice will explain the reason(s) for ineligibility and provide contact information for the Employee Benefits Security Administration.
If your request is incomplete, the notice will describe the information needed to complete the request. You will have until the later of the end of the one-year period you had to file a request for external review or the 48-hour period following receipt of the notice to provide all of the needed information.
If your claim is eligible for external review, the file will then be forwarded to the Independent Review Organization. If there is any information (or evidence) you want to submit in support of the request for an external review that was not previously provided, you may include the information with your request for an external review.
The Independent Review Organization will render an opinion within 30 days. When requested and when a delay would be detrimental to your medical condition, the review will be completed within three days. All Independent Review Organization decisions are final.
The Independent Review Program is a voluntary program arranged by Express Scripts.
Relevant Information
Relevant information is any document, record or other information that: • Was relied upon in making the benefit determination; • Was submitted, considered or generated in the course of making the benefit determination, without regard to
whether such document, record or other information was relied upon in making the benefit determination; • Demonstrates compliance with the administrative processes and safeguards required by federal law in making
the benefit determination; or • Constitutes a statement of policy or guidance with respect to the Plan concerning the denied treatment option
or benefit for the claimant’s diagnosis, without regard to whether such advice or statement was relied upon in making the benefit determination.
MassMutual Prescription Drug Addendum October 2014 Page 20 of 22
Legal Action
This Plan is governed by ERISA. You have the right to bring a civil action under ERISA Section 502(a) if you are not satisfied with the outcome of the appeals procedure. In most instances, you may not initiate a legal action against the Plan until you have completed the appeal processes. If your appeal is expedited, there is no need to complete the process before bringing legal action. No legal action may begin more than one year after the date you have exhausted the Plan’s claim and appeal process. No legal action may begin more than one year after the date you have exhausted the Plan’s claim and appeal process.
Coordination of Benefits
If you are enrolled in Medicare Part B, there is a separate process for any Medicare Part B-eligible medications and supplies. The process is: • Medicare Part B pays its portion for these items first. • Your retirement benefit plan picks up its portion next. • Finally, any remaining balance is your responsibility.
If you are a Medicare beneficiary, you have the right to use any Medicare Part B supplier of your choice. However, for your convenience, Express Scripts has teamed up with NationsHealth, a participating Medicare Part B supplier, to provide Medicare Part B medications and supplies.
Medicare Part B-Eligible Medications and Supplies
This process only applies to: • Diabetes testing supplies (glucose monitors, strips, lancets, etc.); • Respiratory medications and supplies that are used with a nebulizer (this does not include metered dose
inhalers); • Immunosuppressant medications; and • Oral anti-cancer and anti-nausea medications.

MassMutual Prescription Drug Addendum October 2014 Page 21 of 22
Dictionary Terms
Generic Drug
A drug that is chemically identical to a brand-name drug and meets the same standards of the Food and Drug Administration (FDA) for safety, purity and effectiveness. Generic drugs can be legally produced if a patent has expired or for drugs that have never been patented.
Injury
An accidental bodily injury.
Medicaid
A state program of medical aid for needy persons established under Title XIX of the Social Security Act of 1965, as amended.
Medicare
The program of medical care benefits provided under Title XVIII of the Social Security Act of 1965, as amended. Medicare is health insurance for people age 65 or older, under age 65 with certain disabilities and of any age with End-Stage Renal Disease (ESRD), which is permanent kidney failure requiring dialysis or a kidney transplant.
Different parts of Medicare help cover specific services: • Medicare Part A: This is hospital insurance that covers inpatient hospital care as well as skilled nursing
facility, hospice and home health care. • Medicare Part B: This is medical insurance that covers doctors’ services, hospital outpatient care and home
health care as well as covering some preventive services to help maintain your health and to keep certain illnesses from getting worse.
• Medicare Part C: This is Medicare’s Advantage Plans (like an HMO or PPO), which are health plans run by Medicare-approved private insurance companies. Medicare Advantage Plans include Part A, Part B and usually Part D, sometimes for an extra cost.
• Medicare Part D: This is Medicare’s prescription drug coverage, which is an option run by Medicare-approved private insurance companies to help cover the cost of prescription drugs.
Non-Preferred Brand-Name Medication
A brand-name medication that has been reviewed by the same panel of physicians and pharmacists who determined that an alternative drug that is clinically equivalent and more cost effective is available. These designations may change as new clinical information becomes available.
Participating Pharmacy • A retail pharmacy with which Express Scripts has contracted to provide prescription services; • A designated home delivery pharmacy with which Express Scripts has contracted to provide mail-order
prescription services; or • A designated specialty pharmacy with which Express Scripts has contracted to provide mail-order
prescription services for specialty drug prescriptions.

MassMutual Prescription Drug Addendum October 2014 Page 22 of 22
Pharmacy
A retail, mail-order or specialty pharmacy.
Preferred Brand-Name Medication
A brand-name medication that Express Scripts and its panel of physicians and pharmacists “prefer” for their proven quality and cost-effectiveness. You pay less out-of-pocket when you use an approved brand-name drug on the Express Scripts preferred drug list.
Prescription Drug • A drug that has been approved by the Food and Drug Administration for safety and efficacy; • Certain drugs approved under the Drug Efficacy Study Implementation review; or • Drugs marketed before 1938 that are not subject to review but that can, under federal or state law, be
dispensed according to a prescription order.
Prescription Order
The lawful authorization for a prescription drug or related supply by a provider who is duly licensed to make the authorization within the course of his or her professional practice or each authorized refill thereof.
Related Supplies
Diabetic supplies (insulin needles and syringes, lancets and glucose test strips), needles and syringes for injectables covered under the Plan, and spacers for use with oral inhalers.