maternal child health - grande international hospital
TRANSCRIPT

Maternal – Child Health

Learning objectives
1. Describe the role of infection prevention and control in maternal child health.
2. Identify potential infection risks in this setting.
3. Explain practices for prevention and control of infection for these patients.
De
ce
mb
er
1, 2
01
3
2

Time involved
• 60 minutes
De
ce
mb
er
1, 2
01
3
3

Key points• Infection prevention and control strategies based on the
principle of combined care
• For neonates requiring intensive care, the newborn’senvironment must be clearly delineated, with spatial separation between incubators
• Sharing of equipment and supplies must be preceded by thorough cleaning and appropriate disinfection/sterilisation
• Standard Precautions should be applied for all patient care
• Prevention strategies include hand hygiene, patient hygiene, environmental cleaning and immunisation
De
ce
mb
er
1, 2
01
3
4

Background• The World Health Organization (WHO)
estimates that approximately 210 million women become pregnant each year and that 529,000 die from complications
• In the immediate post-partum period, sepsis and haemorrhage are the commonest causes of maternal death
• Severe infections cause more than one-third of neonatal deaths
De
ce
mb
er
1, 2
01
3
5

Neonatal risk factors - 1
• Maternal infections
• Foetal gestational age at the time of the infection
• Complications of delivery
De
ce
mb
er
1, 2
01
3
6

Neonatal risk factors - 2 • Premature infants are at risk for infection due to:
• Absence of normal microbial flora• Increases the risk of colonisation with pathogens
• Colonisation by gastrointestinal flora • Risk differs between breast fed babies versus formula-fed
babies
• Abnormal colonisation that occurs most often in newborns in neonatal intensive care units
• Fragile, underdeveloped organs that normally provide a barrier to infectious pathogens• Such as the skin and lining of the lung
• A poor immune (antibody) response
De
ce
mb
er
1 2
01
3
7

Neonatal infections
• Occur in the first 28 days of life
• May be spread:
• In utero• By the transplacental route
• Intrapartum• When in contact with the maternal genital tract, blood
or stool
• Postpartum• When in contact with the mother, family and visitors,
other neonates in the nursery, health care workers, or contaminated equipment
De
ce
mb
er
1, 2
01
3
8

Infant infections• For full term newborns - superficial infections of the
skin, eye and mucous membranes.
• Additional infections occur in intensive care
• Bacteraemia associated with central lines, pneumonia and gastrointestinal infections
• Microorganisms associated with neonatal infections
• Staphylococcus aureus, coagulase negative staphylococci, Group B streptococci, Escherichia coli and Candida
• Other pathogens often associated with outbreaks in the nursery • Klebsiella, Serratia, Enterobacter, Citrobacter and
Pseudomonas species
De
ce
mb
er
1, 2
01
3
9
Maternal Risk Factors
• Prolonged rupture of membranes (>24 hours)
• Obesity
• Interferes with wound healing
• Diabetes mellitus
• Invasive tests and procedures
De
ce
mb
er
1, 2
01
3
10

Maternal Infections• Common infections include:
• Endometritis• Infection of the lining and wall of the uterus (endometrium
and myometrium)
• Mastitis• Inflammation and infection of the breast
• Caesarean surgical site infections
• Episiotomy site infections• Infection at the site of incision of the perineum
• Sepsis• Bloodstream infection which causes a systemic inflammatory
response
De
ce
mb
er
1, 2
01
3
11
Prevention Strategies
• Standard Precautions
• Hand Hygiene
• Protective barriers
• Cohorting
• Additional precautions
• Single rooms
• Cleaning
De
ce
mb
er
1, 2
01
3
12

Standard Precautions
• Basic hygienic precautions are recommended for all patient encounters
De
ce
mb
er
1, 2
01
3
13

Hand Hygiene
• Use soap and running water or alcohol-based hand rubs:
• before and after contact • with the mother
• with the neonate
• with their immediate environment
• before an aseptic procedure
• after handling blood and body fluids
• after removal of gloves
De
ce
mb
er
1, 2
01
3
14
Protective barriers
• Gloves worn for all contact with mucous membranes, non-intact skin and moist body substances
• Masks and/or protective eyewear or face shields worn when body substances are likely to splash skin or mucous membrane
• Gowns and/or plastic aprons worn when body substances are likely to soil clothing or skin
• Gowns worn for holding infant to the uniform
De
ce
mb
er
1, 2
01
3
15

Cohorting
Cohorting infants with the same infection helps prevent spread of infections in the nursery
De
ce
mb
er
1, 2
01
3
16

Additional Precautions
• May be indicated for infants colonised or infected with epidemiologically significant microorganisms
• Suspected or confirmed infections should be handled according to guidelines developed by the Infection Control Team
De
ce
mb
er
1, 2
01
3
17
Single Rooms
• Priority given to mothers who soil articles in the environment with body substances and those colonised or infected with epidemiologically significant microorganisms
• Infants and/or mothers with diagnosed or suspected infections transmitted by the airborne route must be placed in a single room with negative pressure and the door closed
De
ce
mb
er
1, 2
01
3
18

Cleaning
• For labour and delivery suites, post delivery, remove soiled linens using gloved hands
• The delivery table/bed and the immediate patient environment should be cleaned after each use
• Use non-toxic disinfectants for cleaning neonatal equipment and incubators
• Avoid phenolic disinfectants
De
ce
mb
er
1, 2
01
3
19

General Infection prevention and control - 1• Parent/infant contact encouraged
• Except for the occasional case when there is a risk of transmitting infection
• Labouring mothers may shower or bath
• Post partum, instruct patient on daily perineal care after toileting
• Reviewing good hygienic policies with parents is vital to protect both mother and infant from acquiring or spreading infections
De
ce
mb
er
1, 2
01
3
20
General Infection prevention and control - 2• Prenatal assessment – to identify risk factors for
maternal/ newborn infection and allow prevention strategies
• Screen women for Group B streptococcus at 35-37 weeks gestation
• Screen for human immunodeficiency virus and Hepatitis B • HIV positive mothers should refrain from breastfeeding unless
alternatives are not available.
• Antepartum• Screen mothers upon admission for symptoms of infection
such as new onset of fever and other respiratory symptoms• New onset of cough, rash, or diarrhoea
• If the patient responds “yes” to the any of these conditions, initiate the appropriate additional precautions and spatial separation from other patients (> 2 metres)
De
ce
mb
er
1, 2
01
3
21

General Infection prevention and control - 3• Breast milk is protective as it provides specific
IgA antibody and helps establish normal flora in the neonate
• Provide post-partum hygiene for the mother and infant immunisations as required
• For facilities with little room and overcrowding, consider kangaroo mother care
• This includes skin to skin positioning of the baby on the mother’s chest
De
ce
mb
er
1, 2
01
3
22

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
AIDS Standard
Precautions
Standard
Precautions
Permitted No
Amnionitis Standard
Precautions
Standard
Precautions
Permitted Permitted
Antibiotic Resistant Organisms -Mother
VRE/MRSA:
Contact
Precautions
Standard
Precautions
Permitted Permitted
Antibiotic Resistant
Organisms - Infant
Mother uses
Standard
Precautions
VRE/MRSA:
Contact
Precautions
Permitted Permitted
Candida -
Mother
Standard
Precautions
Standard
Precautions
Permitted Permitted
Candida - Infant Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
23

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Chickenpox
Mother ill – healthy
term infant
Airborne
precautions
Infant room in
with mother
Permitted Permitted
Chickenpox
Mother ill – Infant
in NICU
Airborne
precautions
Mother may not
visit the NICU
Standard
Precautions until
day 10. As of day
10 to and including
day 28 start
Airborne
Precautions
Not Permitted Permitted (as
expressed breast
milk)
Infant in NICU –
chickenpox or
contact
Only parents &
visitors who are
immune may
visit.
Airborne
precautions
Permitted if
woman is immune.
Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
24
Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
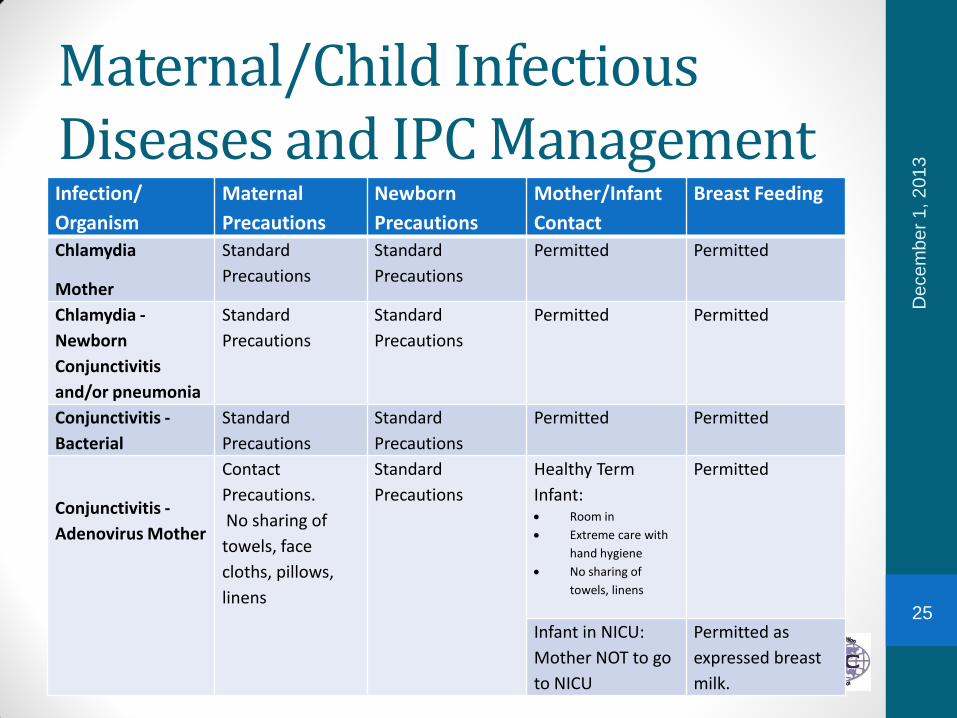
Chlamydia
Mother
Standard
Precautions
Standard
Precautions
Permitted Permitted
Chlamydia -
Newborn
Conjunctivitis
and/or pneumonia
Standard
Precautions
Standard
Precautions
Permitted Permitted
Conjunctivitis -
Bacterial
Standard
Precautions
Standard
Precautions
Permitted Permitted
Conjunctivitis -
Adenovirus Mother
Contact
Precautions.
No sharing of
towels, face
cloths, pillows,
linens
Standard
Precautions
Healthy Term
Infant: Room in
Extreme care with
hand hygiene
No sharing of
towels, linens
Permitted
Infant in NICU:
Mother NOT to go
to NICU
Permitted as
expressed breast
milk.
De
ce
mb
er
1, 2
01
3
25

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Conjunctivitis
Adenovirus Infant
Standard
Precautions
Contact
Precautions.
No sharing of
patient care items.
As above As above
Cytomegalovirus
Mother
Standard
Precautions
Standard
Precautions
Permitted Permitted
Cytomegalovirus -
Infant
Standard
Precautions
Standard
Precautions
Permitted Permitted
Diarrhoea
Mother
Bacterial
(suspected or
confirmed)
Standard
Precautions
Single room with
toilet
Standard
Precautions
Healthy Term
Infant: Permitted
with Standard
Precautions.
Infant in NICU: Not
permitted until
asymptomatic for
48 hours.
Healthy Term
Infant: Permitted
Infant in NICU:
Permitted as
expressed breast
milk.
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
26

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Diarrhoea
Mother
Antibiotic
associated/C.
difficile
Contact
precautions
Single room with
toilet
Standard
Precautions
Permitted Permitted
Diarrhoea
Mother
Viral (e.g.,
norovirus)
Contact
precautions
Single room with
toilet
Contact
precautions
Single room with
toilet
Healthy Term
Infant: Permitted
with Standard
Precautions
Infant in NICU:
Woman is not
permitted in the
NICU until
asymptomatic for
48 hours
Healthy Term
Infant: Permitted
Infant in NICU:
Permitted as
expressed breast
milk.
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
27

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Diarrhoea
Infant
Bacterial
(suspected or
confirmed
Standard
Precautions
Contact
precautions
Permitted Permitted
Diarrhoea
Infant
Viral (e.g.
norovirus)
Standard
Precautions
Contact
precautions
Permitted Permitted
Endometritis Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
28
Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
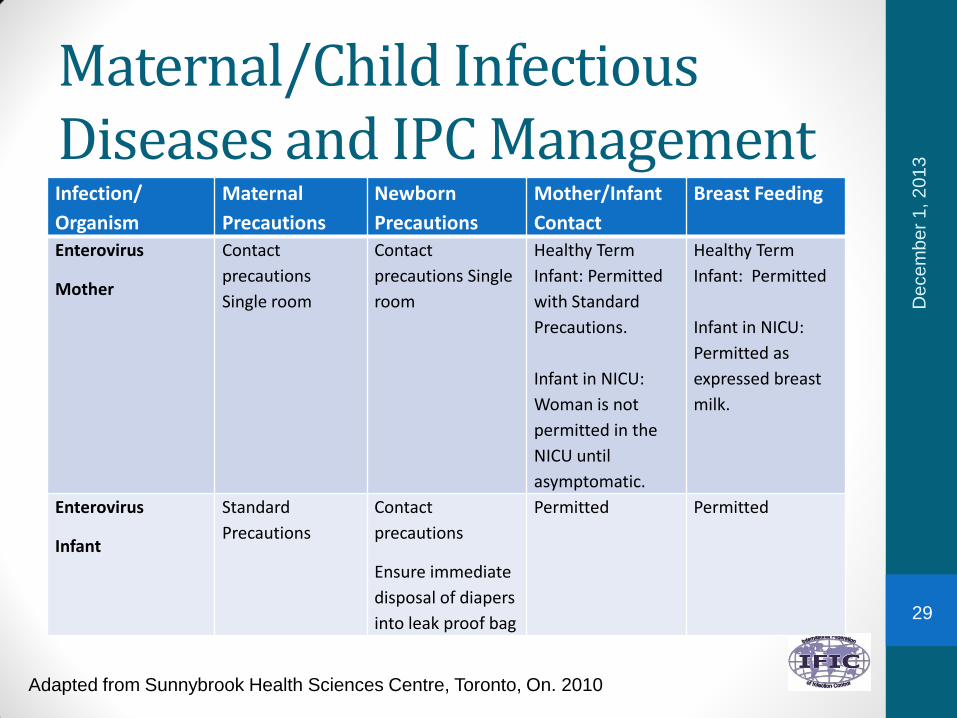
Enterovirus
Mother
Contact
precautions
Single room
Contact
precautions Single
room
Healthy Term
Infant: Permitted
with Standard
Precautions.
Infant in NICU:
Woman is not
permitted in the
NICU until
asymptomatic.
Healthy Term
Infant: Permitted
Infant in NICU:
Permitted as
expressed breast
milk.
Enterovirus
Infant
Standard
Precautions
Contact
precautions
Ensure immediate
disposal of diapers
into leak proof bag
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
29

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Gonococcal
Infections
Mother-Untreated
or <24 hours of
treatment
Standard
Precautions
Standard
Precautions
Permitted Permitted
Gonococcal
Infections - Infant
Conjunctivitis,
scalp abscess,
sepsis
Standard
Precautions
Standard
Precautions
Permitted Permitted
Hepatitis – Mother,
Type A
Standard
Precautions
Standard
Precautions
After prophylaxis
of infant
After prophylaxis
of infant
Hepatitis – Mother,
Type B (HbsAg+)
Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
30
Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
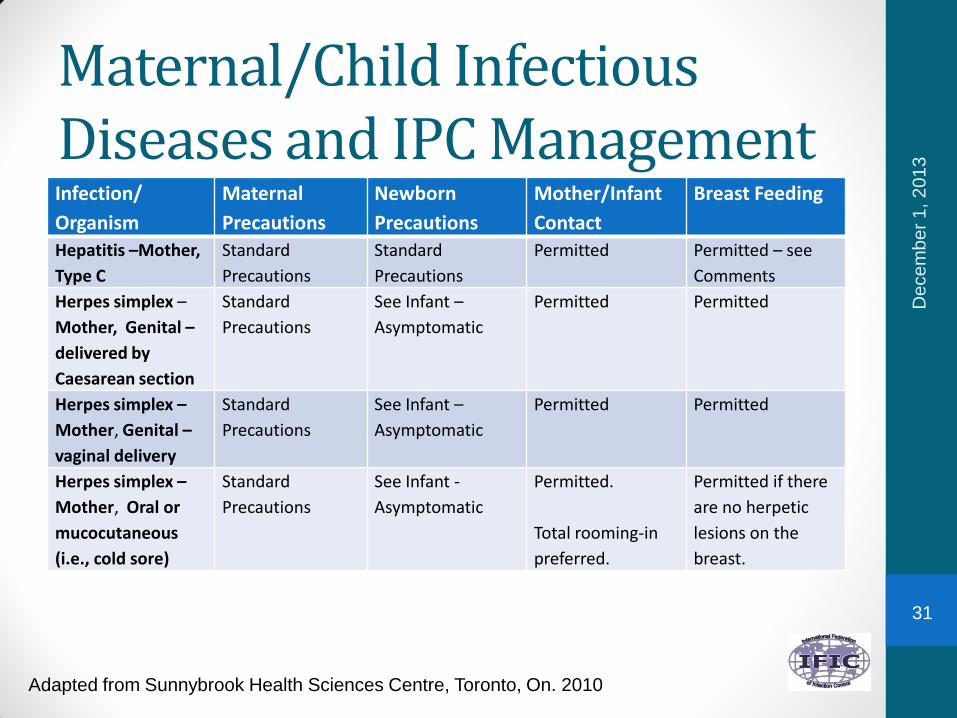
Hepatitis –Mother,
Type C
Standard
Precautions
Standard
Precautions
Permitted Permitted – see
Comments
Herpes simplex –
Mother, Genital –
delivered by
Caesarean section
Standard
Precautions
See Infant –
Asymptomatic
Permitted Permitted
Herpes simplex –
Mother, Genital –
vaginal delivery
Standard
Precautions
See Infant –
Asymptomatic
Permitted Permitted
Herpes simplex –
Mother, Oral or
mucocutaneous
(i.e., cold sore)
Standard
Precautions
See Infant -
Asymptomatic
Permitted.
Total rooming-in
preferred.
Permitted if there
are no herpetic
lesions on the
breast.
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
31
Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
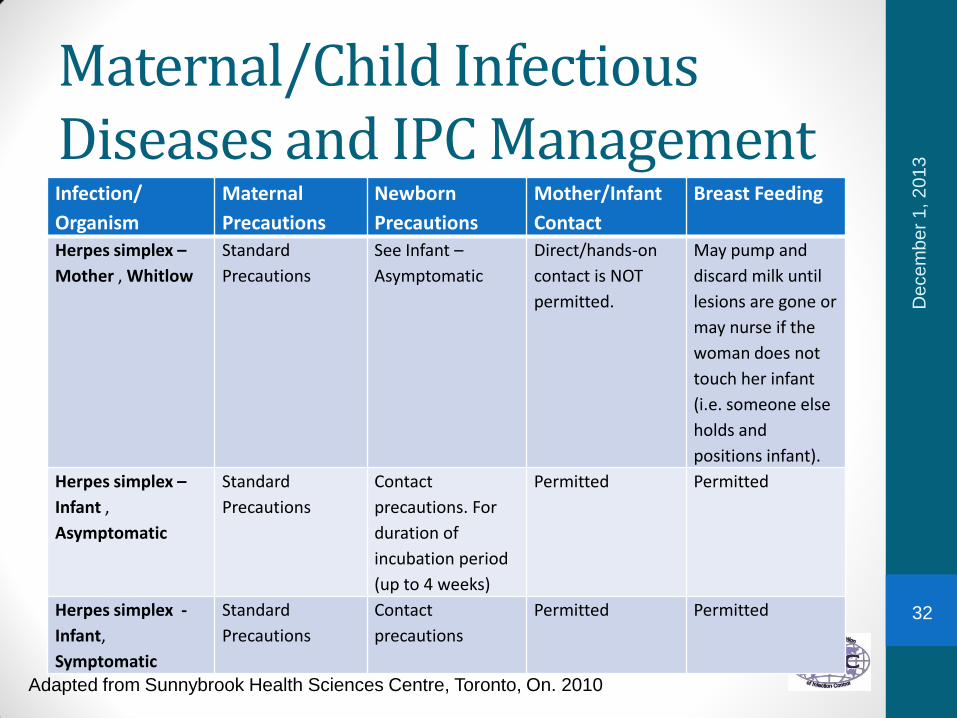
Herpes simplex –
Mother , Whitlow
Standard
Precautions
See Infant –
Asymptomatic
Direct/hands-on
contact is NOT
permitted.
May pump and
discard milk until
lesions are gone or
may nurse if the
woman does not
touch her infant
(i.e. someone else
holds and
positions infant).
Herpes simplex –
Infant ,
Asymptomatic
Standard
Precautions
Contact
precautions. For
duration of
incubation period
(up to 4 weeks)
Permitted Permitted
Herpes simplex -
Infant,
Symptomatic
Standard
Precautions
Contact
precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
32

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast
Feeding
Herpes
zoster(shingles) -
Mother – localized
Standard
Precautions in
single room.
Only immune
staff may care for
patient.
Standard Precautions Permitted. Total
rooming-in
preferred. Mother
may not go to
nursery until
lesions are
crusted.
Permitted if
lesions are not
on breast.
Herpes
zoster(shingles)
Mother –
disseminated
Airborne
precautions
Immune staff only
Term Infant Rooming-
in: Standard
Precautions
Infant in NICU:Airborne precautions from day 10 from 1st
exposure to day 21 of last exposure (or day 28 if infant has been given VarIG).
Permitted. Total
rooming-in
preferred. Mother
may not go to
nursery until
lesions are
crusted.
Infant in NICU:
Woman may NOT
go to the NICU
until lesions are
crusted.
Permitted if
lesions are not
on breast.
Infant in NICU:Provide expressed milk.
De
ce
mb
er
1, 2
01
3
33

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Influenza
Mother
Droplet &Contact
Precautions
Single room
preferred
Standard
Precautions
Healthy Term
Infant: Permitted.
Woman must wear
a surgical mask
when within 2
metres of infant.
Infant in NICU:
Woman is not
permitted to go to
NICU.
Healthy Term
Infant: Permitted
Infant in NICU:
Permitted as
expressed breast
milk.
Influenza - Infant Standard
Precautions
Droplet &Contact
Precautions
Permitted Permitted
Listeria
Mother
Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
34

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/In
fant
Contact
Breast Feeding
Listeria
Infant
Standard Precautions Standard Precautions Permitted Permitted
Measles (Rubeola)
Mother ill – Term
healthy infant
Airborne Precautions Immune staff only
Only immune family
and visitors
permitted
Standard Precautions Room in
with woman
Permitted if
rooming in with
woman. May
provide expressed
breast milk if not
rooming in.
Measles (Rubeola)
Mother ill – infant
in NICU
Airborne Precautions
Immune staff only
Only immune
family and visitors
permitted
From 8 days from 1st
exposure to 12 days
from last exposure
Airborne Precautions
Immune staff only
Only immune family
and visitors
permitted
Woman not
permitted in
NICU until 4
days after
the
appearance
of the rash.
Permitted as
expressed breast
milk only until
woman no longer
infectious
De
ce
mb
er
1, 2
01
3
35

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Measles (Rubeola)
Infant ill or
exposed
(i.e. exposed in
NICU)
Standard
Precautions
Airborne
Precautions
Immune staff
only
Only immune
family and
visitors
permitted
Woman immune –
permitted to see
infant
Woman
susceptible –
woman not
permitted to see
infant
Permitted
Woman
susceptible –
Permitted as
expressed breast
milk only until
infant no longer
infectious
Meningitis
Neissera
meningitidis/
Haemophilus
influenzae
Droplet
precautions until
24 hrs. after
appropriate
antimicrobial
therapy
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
36

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Inf
ant Contact
Breast Feeding
Mumps
Mother
Droplet/Contact
precaution Immune Staff
only
Only immune
family and
visitors permitted
Standard Precautions Term Infant:
Permitted
Term Infant:
Permitted
Mumps
Infant in NICU
Exposed or ill
Standard
Precautions
Droplet/Contact
precautions starting
from 10 days from
first exposure to 26
days from last
exposure. Single room
Immune Staff only
Only immune family
and visitors
permitted
Woman
immune –
permitted to
see infant
Woman
susceptible –
woman not
permitted to
see infant
Woman immune –
Permitted
Woman
susceptible –
Permitted as
expressed breast
De
ce
mb
er
1, 2
01
3
37
Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
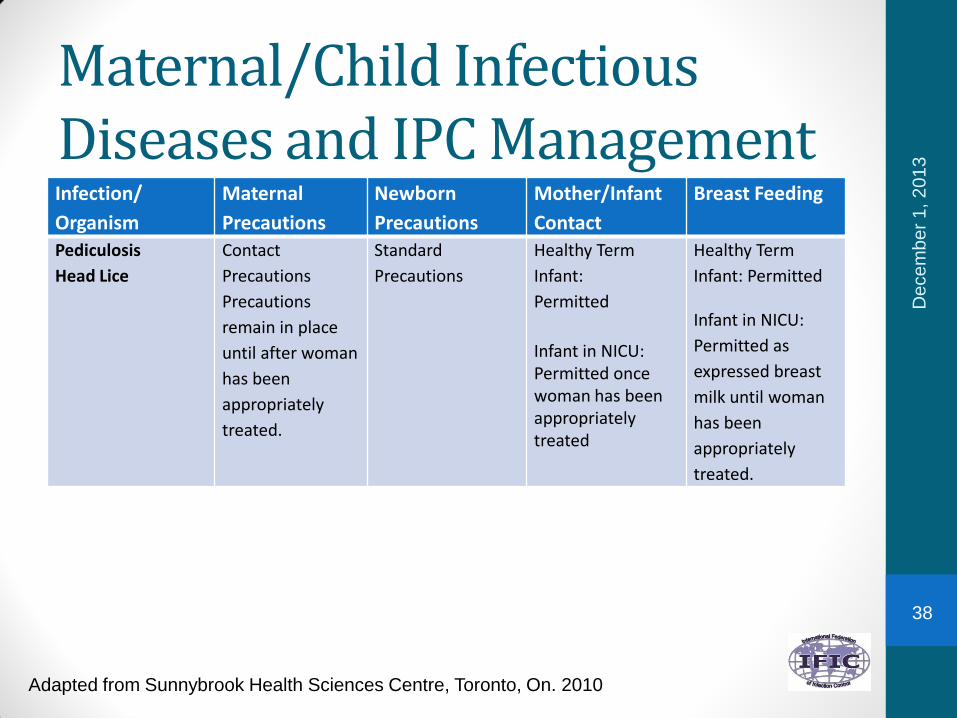
Pediculosis
Head Lice
Contact
Precautions
Precautions
remain in place
until after woman
has been
appropriately
treated.
Standard
Precautions
Healthy Term
Infant:
Permitted
Infant in NICU: Permitted once woman has been appropriately treated
Healthy Term
Infant: Permitted
Infant in NICU:
Permitted as
expressed breast
milk until woman
has been
appropriately
treated.
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
38
Maternal/Child Infectious Diseases and IPC Management
Infection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant Contact Breast
Feeding
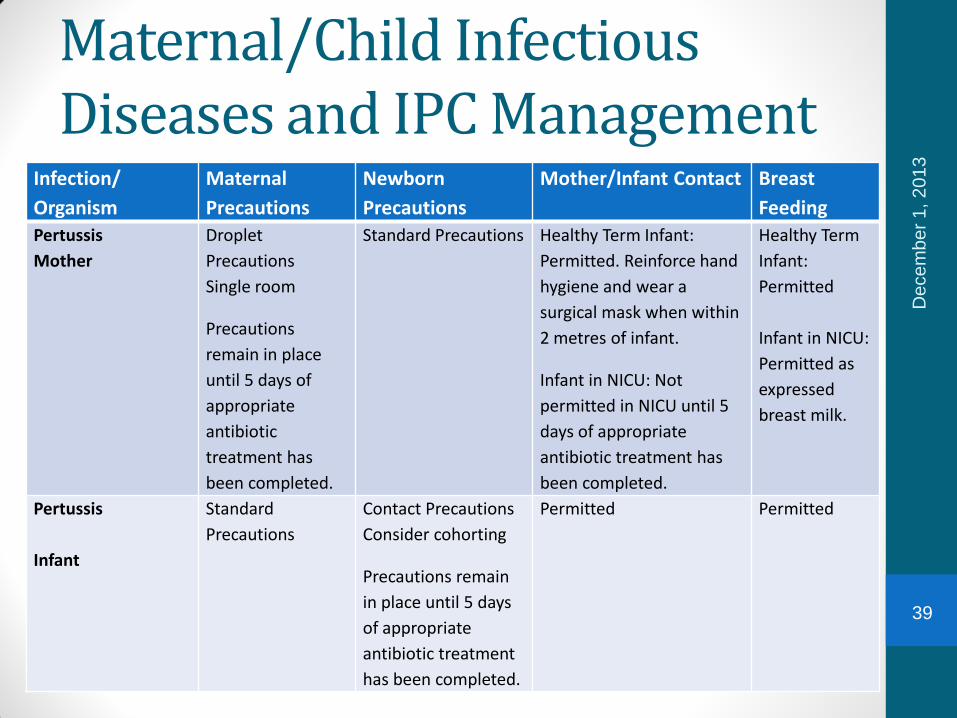
Pertussis
Mother
Droplet
Precautions
Single room
Precautions
remain in place
until 5 days of
appropriate
antibiotic
treatment has
been completed.
Standard Precautions Healthy Term Infant:
Permitted. Reinforce hand
hygiene and wear a
surgical mask when within
2 metres of infant.
Infant in NICU: Not
permitted in NICU until 5
days of appropriate
antibiotic treatment has
been completed.
Healthy Term
Infant:
Permitted
Infant in NICU:
Permitted as
expressed
breast milk.
Pertussis
Infant
Standard
Precautions
Contact Precautions
Consider cohorting
Precautions remain
in place until 5 days
of appropriate
antibiotic treatment
has been completed.
Permitted Permitted
De
ce
mb
er
1, 2
01
3
39

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Respiratory Virus
Infections
Mother ill
Droplet/Contact
Precautions
Single room
Standard
Precautions
Healthy Term
Infant: Permitted.
Reinforce hand
hygiene and wear
a surgical mask
when within 2
metres of infant
Infant in NICU: Not
permitted in NICU.
Healthy Term
Infant: Infant
rooming-in:
Permitted
Infant in NICU:
Permitted as
expressed breast
milk.
Respiratory Virus
Infections -
Infant ill
Standard
Precautions
Droplet /Contact
Precautions
Permitted Permitted
Infant in NICU –
chickenpox or
contact
Only parents &
visitors who are
immune may
visit.
Airborne
precautions
Permitted if
woman is immune.
Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
40

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Rubella
Mother
Droplet
precautions
Immune staff only
Droplet
precautions
Immune staff only
Healthy Term
Infant: Permitted
Infant in NICU:Woman cannot go into the NICU until 7 days after the onset of the rash.
Healthy Term
Infant: Permitted
Infant in NICU:Expressed breast milk as the woman cannot go into the NICU until 7 days after the onset of the rash.
Rubella
Infant (Congenital)
Standard
Precautions
Droplet
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
41

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Scabies Contact
Precautions
Precautions
remain in place
until after woman
has been
appropriately
treated.
Standard
Precautions
Healthy Term
Infant:
Permitted once
woman has been
appropriately
treated.
Infant in NICU:Permitted once woman has been appropriately treated.
Healthy Term
Infant:
Permitted once
woman has been
appropriately
treated or may
provide expressed
breast milk.
Infant in NICU:Permitted once woman has been appropriately treated or may provide expressed breast milk.
Staphylococcus
aureus - Mother
Mastitis
Standard
Precautions
Standard
Precautions
Permitted Permitted (see
Comments)
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
42

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Staphylococcus
aureus - Mother,
Breast Abscess
Standard
Precautions
Standard
Precautions
Permitted Healthy Term
Infant:
Permitted
Infant in NICU:
Permitted on the
unaffected breast
Staphylococcus
aureus – Mother,
Minor Wound
Infection
(contained) or Toxic
Shock Syndrome
Standard
Precautions
Standard
Precautions
Permitted if
draining lesion is
adequately
contained
Permitted
Staphylococcus
aureus - Mother,
Major Wound (not
contained)
Contact
Precautions
Standard
Precautions
Permitted if
draining can be
adequately
contained
Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
43
Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
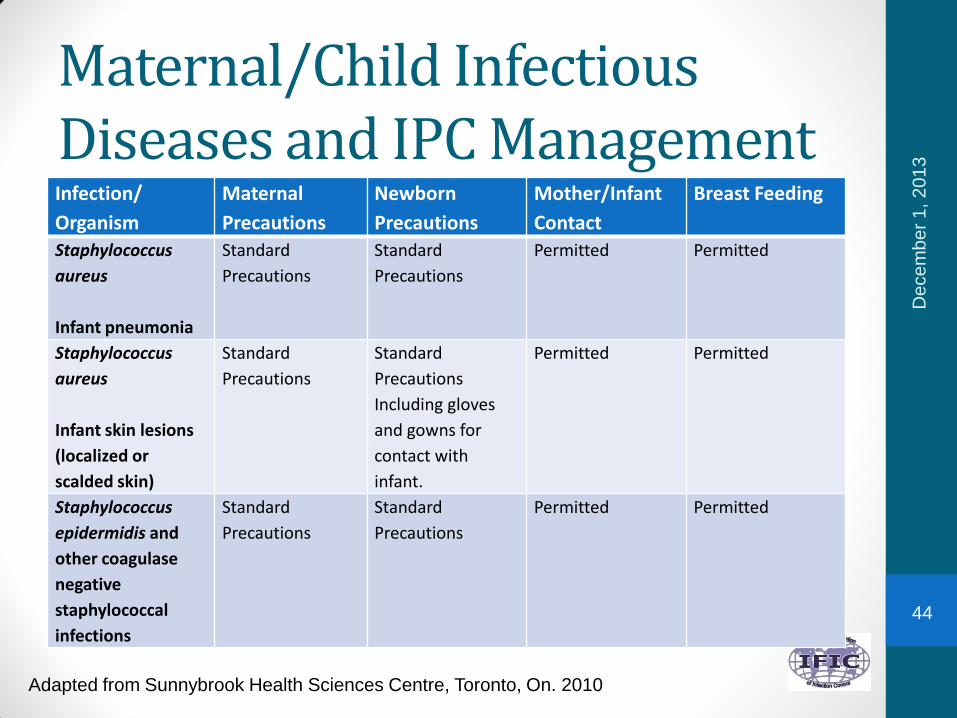
Staphylococcus
aureus
Infant pneumonia
Standard
Precautions
Standard
Precautions
Permitted Permitted
Staphylococcus
aureus
Infant skin lesions
(localized or
scalded skin)
Standard
Precautions
Standard
Precautions
Including gloves
and gowns for
contact with
infant.
Permitted Permitted
Staphylococcus
epidermidis and
other coagulase
negative
staphylococcal
infections
Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
44

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Streptococcal
Disease Group A -
Mother, Minor
Wound Infection
(contained)
Single room
until 24 hours
after effective
treatment.
Standard
Precautions
Permitted Permitted
Streptococcal
Disease Group A -
Mother, Major
wound infection or
endometritis
Single room
until 24 hours
after effective
treatment.
Standard
Precautions
Permitted Permitted
Streptococcal
Disease
Group A -
Mother, Invasive
Disease
Single room
until 24 hours
after effective
treatment.
Standard
Precautions
Permitted after
24 hours of
effective
treatment.
Permitted after 24
hours of effective
treatment.
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
45

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infa
nt Contact
Breast Feeding
Streptococcal
Disease
Group A -
Mother,
Pharyngitis (strep
throat)
Droplet Precautions.
Single room .
Precautions remain in
place until 24 hours
after effective
treatment
Standard
Precautions
Permitted after
24 hours of
effective
treatment
Permitted after 24
hours of effective
treatment.
Streptococcal
Disease
Group A (GAS) -
Infant
Standard Precautions Contact
Precautions
Precautions
remain in place
until 24 hrs. after
effective
treatment.
Streptococcal
Disease
Group A (GAS)
Infant
Standard
Precautions
Streptococcal
Disease
Group B (GBS) -
Mother,
Colonization
Standard Precautions Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
46
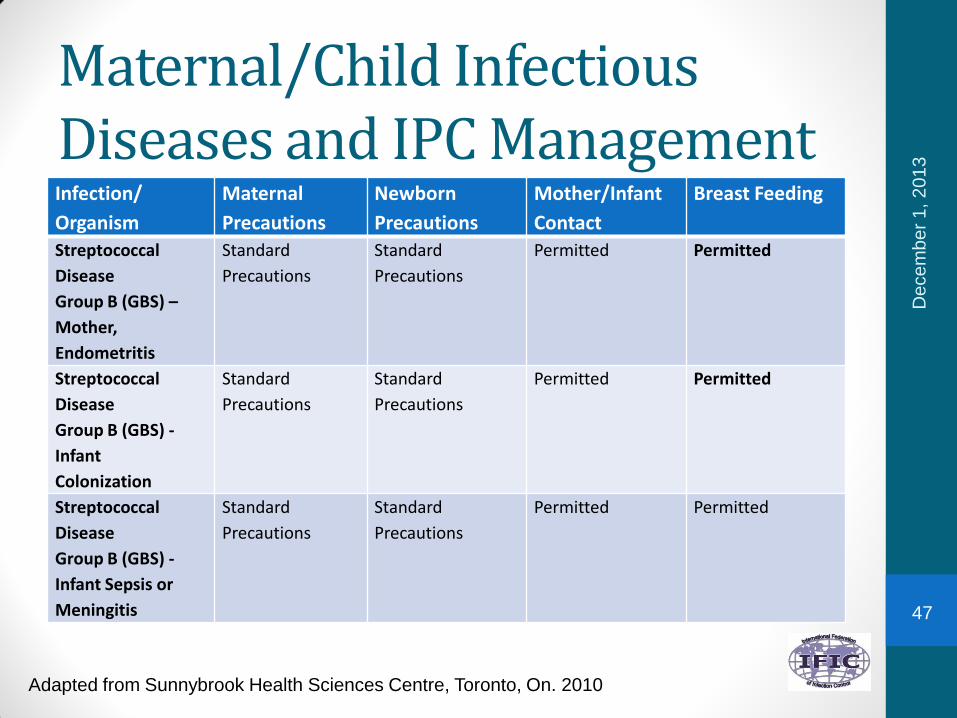
Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Streptococcal
Disease
Group B (GBS) –
Mother,
Endometritis
Standard
Precautions
Standard
Precautions
Permitted Permitted
Streptococcal
Disease
Group B (GBS) -
Infant
Colonization
Standard
Precautions
Standard
Precautions
Permitted Permitted
Streptococcal
Disease
Group B (GBS) -
Infant Sepsis or
Meningitis
Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
47
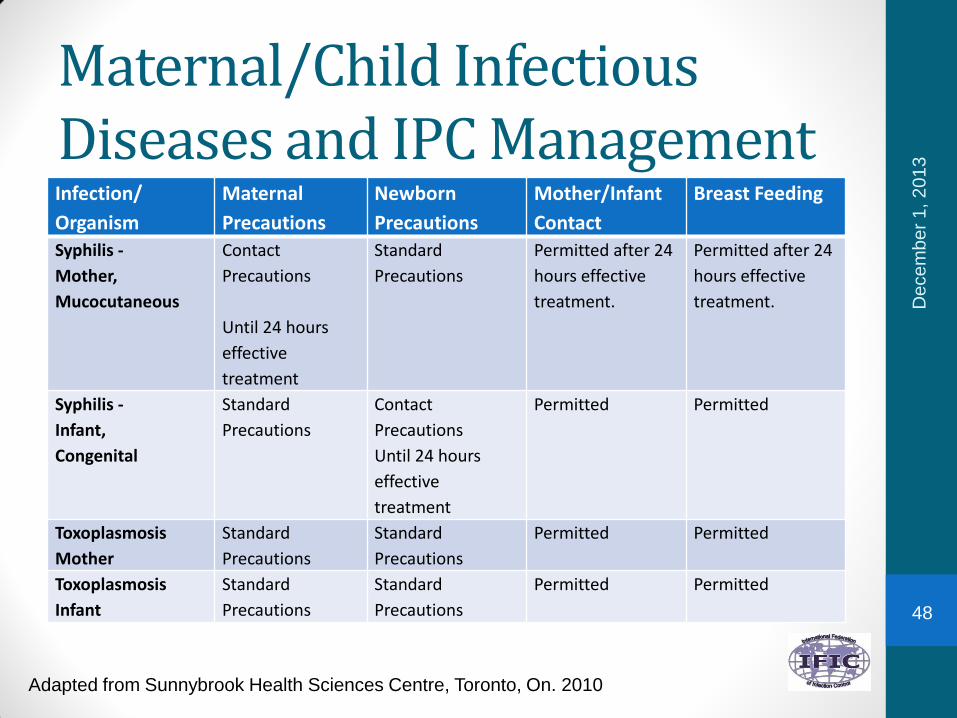
Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Syphilis -
Mother,
Mucocutaneous
Contact
Precautions
Until 24 hours
effective
treatment
Standard
Precautions
Permitted after 24
hours effective
treatment.
Permitted after 24
hours effective
treatment.
Syphilis -
Infant,
Congenital
Standard
Precautions
Contact
Precautions
Until 24 hours
effective
treatment
Permitted Permitted
Toxoplasmosis
Mother
Standard
Precautions
Standard
Precautions
Permitted Permitted
Toxoplasmosis
Infant
Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
48

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Tuberculosis -
Mother,
Positive Skin test –
asymptomatic
Standard
Precautions
Standard
Precautions
Permitted Permitted
Tuberculosis -
Mother,
Pulmonary or
laryngeal on
effective treatment
Standard
Precautions
Standard
Precautions
Permitted Permitted
Tuberculosis -
Mother,
Pulmonary or
laryngeal – newly
diagnosed, on
inadequate
treatment or
noncompliant
Airborne
Precautions
Standard
Precautions
Not permitted
until woman is no
longer infectious
Mother may
provide expressed
breast milk.
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
49

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Tuberculosis
Mother
Extrapulmonary
Standard
Precautions
Standard
Precautions
Permitted Permitted unless
the
extrapulmonary TB
is causing a breast
abscess. Not
permitted until TB
abscess is treated.
Urinary Tract
Infection
Standard
Precautions
Standard
Precautions
Permitted Permitted
West Nile Virus Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
50

Maternal/Child Infectious Diseases and IPC ManagementInfection/
Organism
Maternal
Precautions
Newborn
Precautions
Mother/Infant
Contact
Breast Feeding
Wound Infections -
Mother,
Minor or Limited
Standard
Precautions
Standard
Precautions
Permitted Permitted
Wound Infections -
Mother,
Major
Standard
Precautions
Standard
Precautions
Permitted Permitted
Wound Infections -
Infant
Standard
Precautions
Standard
Precautions
Permitted Permitted
Yeast Standard
Precautions
Standard
Precautions
Permitted Permitted
De
ce
mb
er
1, 2
01
3
Adapted from Sunnybrook Health Sciences Centre, Toronto, On. 2010
51

References - 1• Committee on Infectious Diseases. (2012). The Red Book
29th Edition. Elk Grove Village, Illinois: American Academy of Pediatrics.
• Guidelines for the Prevention of Invasive Group A Streptococcal Disease, CCDR 2006; V32S2. http://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/06pdf/32s2_e.pdf
• World Health Organization (WHO): Practical Guidelines for Infection Control in health Care settings, 2003. http://whqlibdoc.who.int/wpro/2003/a82694.pdf
De
ce
mb
er
1, 2
01
3
52
References - 2• World Health Organization, Geneva, 2010. Packages of
Interventions for Family Planning, Safe Abortion Care, Maternal, Newborn and Child Health.http://whqlibdoc.who.int/hq/2010/WHO_FCH_10.06_eng.pdf
• APIC. (2009). In APIC Text Infection Control and Epidemiology, 3rd Edition (Chapters 37, 38, 39). Washington: Association of Professionals for Infection Prevention and Control and Epidemiology
• World Health Organization (WHO): Recommendations for Routine Immunization 2010. http://www.who.int/immunization/policy/immunization_tables/en/index.html
De
ce
mb
er
1, 2
01
3
53
Quiz1. There are specific precautions required when mothers or
infants have communicable diseases. The issues centre around breast feeding and needed precautions. T/F?
2. Maternal infection risks area) Prolonged rupture of membranes (>24 hours)
b) Diabetes mellitus
c) Invasive tests and procedures
d) All of the above
3. Infection prevention strategies specific to maternal child health include all except:
a) Single rooms
b) Cohorting
c) Type of carpet in patient rooms
d) Screening for streptococcus
De
ce
mb
er
1, 2
01
3
54
International Federation of Infection Control• IFIC’s mission is to facilitate international networking in
order to improve the prevention and control of healthcare associated infections worldwide. It is an umbrella organisation of societies and associations of healthcare professionals in infection control and related fields across the globe .
• The goal of IFIC is to minimise the risk of infection within healthcare settings through development of a network of infection control organisations for communication, consensus building, education and sharing expertise.
• For more information go to http://theific.org/
De
ce
mb
er
1, 2013
55