mdct, fdg pet, 2008
DESCRIPTION
ssTRANSCRIPT

AJR Integrative Imaging
LIFELONG LEARNING FOR RADIOLOGY
Imaging Features of Sarcoidosis on MDCT, FDG PET, and PET/CTHima B. Prabhakar1, Chad B. Rabinowitz1, Fiona K. Gibbons2, Walter J. O’Donnell2, Jo-Anne O. Shepard3, and Suzanne L. Aquino3
AJR:190, March 2008 S1
ObjectiveThe objectives of this article are to discuss the epidemiology
and natural history of sarcoidosis; to review the classic imaging features of sarcoidosis on radiography, CT, and 67Ga nuclear medicine scans; and to present clinical examples of sarcoidosis as seen on PET and PET/CT in the chest, abdomen and pelvis, and bones.
ConclusionThe imaging features of sarcoidosis are diverse and can be
seen on a variety of imaging techniques. It is important for ra-diologists and nuclear medicine physicians to recognize the com-mon imaging features and patterns of sarcoidosis in order to raise the possibility in the appropriate clinical setting.
IntroductionSarcoidosis is a multiorgan granulomatous disease with a
wide variety of imaging features. Imaging abnormalities can commonly be seen on chest radiography, MDCT, 67Ga scans, FDG PET, and PET/CT. FDG uptake from sarcoidosis is non-specific and can mimic other disease processes, including lym-phoma and diffuse metastatic disease. When combined with imaging features on other techniques, such as MDCT, FDG uptake can be useful in monitoring therapeutic response in patients with known sarcoidosis. Because imaging features of sarcoidosis can overlap considerably with those of malignant disorders, it is important for both radiologists and nuclear medicine specialists to be aware of the many varied presenta-tions of sarcoidosis in order to suggest the diagnosis in the appropriate clinical setting.
Sarcoidosis is a systemic and chronic disease of unknown cause [1]. The characteristic histologic lesion, a noncaseating granuloma, has been described as affecting all organ systems, although they are most frequently seen affecting the lungs [2].
The imaging features of sarcoidosis are protean and can be shown with a variety of imaging techniques. Diagnostic imaging can not only help suggest a diagnosis in asymptom-atic patients, but can also help in monitoring therapeutic response in symptomatic patients. FDG uptake on PET in patients with sarcoidosis is nonspecific and can mimic that in malignancies such as lymphoma and diffuse metastatic disease [2].
EpidemiologySarcoidosis has a worldwide distribution and typically af-
fects young to middle-aged adults. The highest prevalence of the disease is found in African-Americans, Swedes, and Danes. In the United States, the incidence rate of sarcoidosis is 35.5 cases per 100,000 in blacks and 10.9 cases per 100,000 in whites. Additionally, the disease incidence is slightly higher in women than in men [3].
Clinical Presentation and Natural HistoryBecause sarcoidosis affects multiple organ systems, presen-
tation varies from nonspecific constitutional symptoms to those related to specific organ involvement. Symptoms related to lung involvement (dyspnea and cough) can lead to chest radiographs that eventually yield the diagnosis of sarcoid. One third of patients have peripheral lymphadenopathy, most commonly involving the cervical, axillary, and inguinal lymph nodes. One quarter of patients show characteristic skin le-sions, including erythema nodosum and lupus pernio [3].
The natural history of sarcoidosis varies significantly from patient to patient. The disease spontaneously remits in up to one third of patients, but is chronic and progressive in up to 30%. There is a 1–5% fatality rate from the disease, most commonly resulting from severe respiratory or cardiac involvement [3].
Keywords: CT, FDG PET, MDCT, PET/CT, sarcoidosis
DOI:10.2214/AJR.07.7001
Received March 8, 2007; accepted after revision June 11, 2007.1Abdominal Imaging and Interventional Radiology, Department of Radiology, Massachusetts General Hospital, 55 Fruit St., FND 270, Boston, MA 02114. Address correspondence to H. B. Prabhakar ([email protected]).2Department of Pulmonary/Critical Care Medicine, Massachusetts General Hospital, Boston, MA.3Thoracic Radiology, Department of Radiology, Massachusetts General Hospital, Boston, MA.
AJR 2008;190:S1–S6 0361–803X/08/1903–S1 © American Roentgen Ray Society
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.72
on 1
0/31
/15
from
IP
addr
ess
114.
79.2
8.72
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

S2 AJR:190, March 2008
Prabhakar et al.
Classic Imaging Features of SarcoidosisRadiography
Chest radiographic features include mediastinal and bi-lateral hilar lymphadenopathy, parenchymal opacities, and, in more advanced cases, parenchymal fibrosis. A clinical staging system based on the chest radiograph has been de-vised to monitor disease in patients with sarcoidosis as well as to predict patient prognosis. The five-part staging sys-tem ranges from stage 0 (no radiographic abnormality) to stage 4 (pulmonary fibrosis), with varying degrees of lymphadenopathy and pulmonary parenchymal abnormal-ities in between. Spontaneous remission is more commonly seen in patients with stage 1 disease (Fig. 1) than in patients with more advanced stages [3].
MDCTLymphadenopathy and parenchymal involvement in the
neck and chest are more readily shown on MDCT. In the neck, palpable cervical lymphadenopathy is identified in one third of patients, usually in the posterior triangle. In the chest, paratracheal, mediastinal, and bilateral hilar lymphadenopathy are most commonly identified. Charac-teristic parenchymal lesions include pulmonary nodules, typically in a peribronchovascular distribution or along fis-sures [2] (Fig. 2). Less commonly, alveolar consolidation can be seen with air bronchograms, cavitation, and fibrosis [4].
In the abdomen, lesions are less characteristic, mimick-ing systemic diseases such as lymphoma, diffuse metastatic disease, or granulomatous or mycobacterial infection. In
Fig. 1—Stage 1 sarcoidosis in 54-year-old man with biopsy-proven sarcoidosis. Frontal chest radiograph shows right paratracheal and bilateral hilar lymphade-nopathy (arrows) and clear lungs.
Fig. 2—Pulmonary nodules in peribronchovascular distribution in 44-year-old woman with sarcoidosis. High-resolution chest CT image shows multiple tiny pul-monary nodules centered in peribronchovascular distribution (upper arrow). Small pulmonary nodules can also be seen lining right major fissure (lower arrow).
Fig. 3—Abdominal lymphadenopathy in 38-year-old man with biopsy-proven sarcoidosis. Contrast-enhanced axial CT image of upper abdomen shows mul-tiple periaortic lymph nodes (arrows).
Fig. 4—Lambda (λ) sign on 67Ga scan in 26-year-old man with biopsy-proven sar-coidosis. Anterior image of chest shows increased tracer uptake in right paratra-cheal and bilateral hilar lymph nodes, in configuration known as “lambda sign.”
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.72
on 1
0/31
/15
from
IP
addr
ess
114.
79.2
8.72
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:190, March 2008 S3
addition to diffuse lymphadenopathy (Fig. 3), nonspecific parenchymal lesions have been described, usually in the spleen and liver [4]. Diffuse hepatic involvement can prog-ress in some cases to confluent hepatic fibrosis [2].
Gallium-67 ScanningGallium-67 imaging has been widely used in the diagnosis
of sarcoidosis. Gallium-67 is taken up in lesions with in-creased blood flow, typically in lesions having an inflamma-tory or infectious cause. In sarcoidosis, a characteristic pat-tern of uptake in the chest has been described as the “lambda sign:” paratracheal and bilateral hilar uptake [5] (Fig. 4). An-other pattern of uptake is called the “panda sign,” caused by uptake in the lacrimal and parotid glands. Although this pat-tern can be seen in other entities, such as lymphoma and HIV, the bilateral symmetric involvement of the glands is more typical of sarcoidosis [6]. Additionally, when the panda sign is seen in conjunction with the lambda sign, it is highly specific for sarcoidosis [5].
FDG PET and PET/CTFDG PET is an important clinical tool in the evaluation of
known or suspected malignancy. Uptake of the tracer is non-specific, however, and is related to tissue metabolism. Thus, the agent is also readily taken up in some infectious and in-flammatory conditions. Prior studies show increased FDG uptake in active sarcoidosis [7, 8]. FDG uptake in sarcoidosis
is nonspecific in both intensity and pattern, and is not gener-ally useful in making an initial diagnosis. Additionally, marked FDG uptake in lymph nodes and parenchymal organs can be an important mimic of malignancy, specifically lymphoma and diffuse metastatic disease. Despite this, FDG uptake can decrease when sarcoidosis is treated, and PET can be useful in monitoring the effectiveness of therapy [8, 9].
Although FDG uptake is nonspecific in sarcoidosis, com-bining the imaging features of sarcoidosis on CT with up-take on PET can make combined FDG PET/CT a useful technique in monitoring disease progression or remission. Additionally, if characteristic patterns of chest CT lesions are identified (as described previously), along with typical patterns of lymphadenopathy, the disease can be suggested on the basis of FDG PET/CT findings. Histologic proof, however, often is still required because of the importance of excluding malignancies, particularly lymphoma [10].
Clinical Examples on FDG PET and PET/CTHead and Neck
Head and neck involvement by sarcoidosis is usually iden-tified as cervical lymphadenopathy, seen in approximately one third of patients [2]. On FDG PET, increased uptake has been described in these lymph nodes (Fig. 5), as well as in the parotid glands, in a similar distribution to that seen with 67Ga scanning [7].
ChestAlthough the radiographic and CT features of sarcoidosis
have been well described in the chest, few articles have spe-cifically addressed patterns of FDG uptake in the lungs. Me-diastinal and hilar lymphadenopathy from sarcoidosis shows increased FDG uptake, as in other parts of the body (Fig. 6). Lung parenchymal involvement and FDG uptake is less well described; however, it has been shown that FDG PET can detect lung involvement by sarcoidosis in patients after trans-plantation [9].
AbdomenAgain, as elsewhere in the body, abdominal lymph nodes
secondary to sarcoidosis can show increased FDG activity [7]. Parenchymal lesions in the abdomen have also been de-scribed as showing increased FDG uptake. For example, sarcoidosis is known to cause splenomegaly and low-density focal lesions in the spleen that have been reported to have increased FDG uptake on PET [11] (Fig. 7).
MusculoskeletalBone involvement in sarcoidosis can be seen in up to one
third of patients, usually in the hands and feet. Less com-monly, axial skeletal involvement can be seen. In both cases, lesions of sarcoid can be either osteolytic or osteosclerotic, and their nonspecific appearance can make diagnosis diffi-cult. Increased activity can be seen on bone scintigraphy.
Imaging Features of Sarcoidosis
Fig. 5—Palpable submental lymph node with FDG uptake in 56-year-old woman with palpable submental lymph node. Axial fused contrast-enhanced PET/CT im-age shows enlarged left submental lymph node (arrow) with increased FDG up-take. Lesion was biopsied and was consistent with sarcoidosis.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.72
on 1
0/31
/15
from
IP
addr
ess
114.
79.2
8.72
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

S4 AJR:190, March 2008
Prabhakar et al.
A B
C
Fig. 6—Confluent parenchymal lung nodules and mediastinal and bilateral hilar lymphadenopathy with increased FDG uptake in 56-year-old woman with biopsy- proven sarcoidosis.A–C, Axial CT image (A) shows confluent parenchymal lung nodules (yellow ar-rows) and mediastinal and bilateral hilar lymphadenopathy (blue arrows). These abnormalities show increased FDG uptake on fused PET/CT (B) and unfused PET (C) images.
A B C
Fig. 7—Splenic lesions with uptake from sarcoidosis in 43-year-old woman with history of Hodgkin’s lymphoma.A–C, Images from combined PET/CT show low-density lesions (arrows, A and C) in spleen on coronal CT image (A). Lesions show increased FDG uptake on fused PET/CT (B) and unfused PET (C) images. Because of patient’s history of lymphoma, she underwent splenectomy to assess cause of lesion, and pathology revealed nonca-seating granulomas consistent with sarcoidosis. Sarcoidosis is known to cause splenomegaly and low-density focal lesions in the spleen and has been reported to have increased FDG uptake on PET scans [11].
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.72
on 1
0/31
/15
from
IP
addr
ess
114.
79.2
8.72
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
AJR:190, March 2008 S5
Imaging Features of Sarcoidosis
A B
C
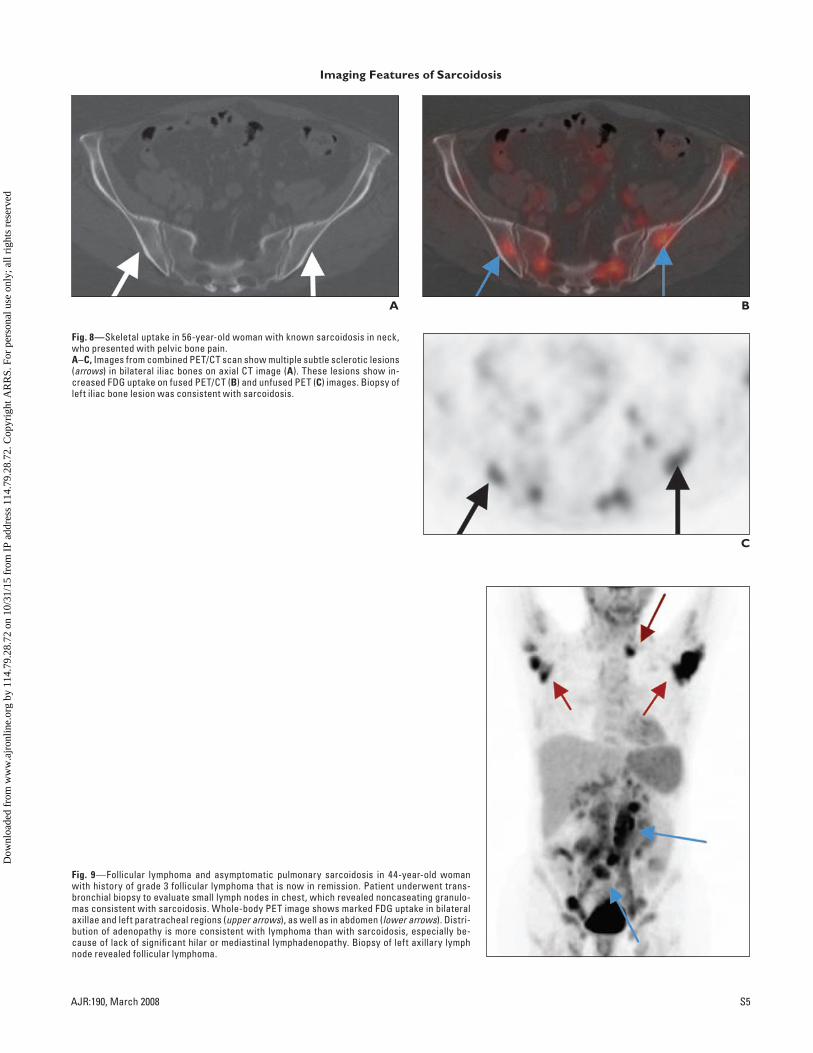
Fig. 8—Skeletal uptake in 56-year-old woman with known sarcoidosis in neck, who presented with pelvic bone pain.A–C, Images from combined PET/CT scan show multiple subtle sclerotic lesions (arrows) in bilateral iliac bones on axial CT image (A). These lesions show in-creased FDG uptake on fused PET/CT (B) and unfused PET (C) images. Biopsy of left iliac bone lesion was consistent with sarcoidosis.
Fig. 9—Follicular lymphoma and asymptomatic pulmonary sarcoidosis in 44-year-old woman with history of grade 3 follicular lymphoma that is now in remission. Patient underwent trans-bronchial biopsy to evaluate small lymph nodes in chest, which revealed noncaseating granulo-mas consistent with sarcoidosis. Whole-body PET image shows marked FDG uptake in bilateral axillae and left paratracheal regions (upper arrows), as well as in abdomen (lower arrows). Distri-bution of adenopathy is more consistent with lymphoma than with sarcoidosis, especially be-cause of lack of significant hilar or mediastinal lymphadenopathy. Biopsy of left axillary lymph node revealed follicular lymphoma.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.72
on 1
0/31
/15
from
IP
addr
ess
114.
79.2
8.72
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

S6 AJR:190, March 2008
Additionally, case reports have described increased FDG uptake in skeletal sarcoidosis (Fig. 8). In conjunction with the more characteristic findings of sarcoidosis, such as me-diastinal lymphadenopathy, bone involvement from sarcoid can be suggested in patients with increased focal bone FDG uptake rather than diffuse metastatic disease [12, 13].
Sarcoidosis as a Mimic of MalignancyThe most common radiologic finding in sarcoidosis is in-
trathoracic lymphadenopathy, seen in up to 85% of patients [2]. Abdominal lymphadenopathy is seen 30% of cases, with massive lymphadenopathy (lymph nodes > 2 cm) seen in 10% of patients [4]. Given the presence of lymphadenopathy in such a large percentage of patients with sarcoidosis, it is not surprising that one of the more common differential consider-ations in these patients is lymphoma. Additionally, as de-scribed previously, musculoskeletal involvement in sarcoidosis can manifest as increased focal uptake throughout the skele-ton, which can mimic diffuse metastatic disease [12, 13].
To further complicate matters, a known association exists between sarcoidosis and lymphoma, described in 1986 by Brinker and called “sarcoidosis–lymphoma syndrome” [14]. Several cases studies have been published describing the asso-ciation of chronic active sarcoidosis and systemic lymphoma, both Hodgkin’s and non-Hodgkin’s lymphoma [15, 16] (Fig. 9). Using data from patients with respiratory sarcoidosis who had registered with the Danish Institute of Clinical Epidemi-ology, Brinker determined that patients with sarcoidosis are at 5.5 times increased risk of developing a lymphoprolifera-tive disorder as other patients in the same age group [14].
ConclusionThe imaging features of sarcoidosis are diverse and can
be shown on a variety of imaging techniques. FDG uptake on PET in patients with sarcoidosis is variable and can mimic malignancies such as lymphoma and diffuse meta-static disease. It is important for radiologists and nuclear medicine physicians to recognize the common imaging fea-
tures and patterns of sarcoidosis in order to raise the pos-sibility in the appropriate clinical setting.
References1. Cox CE, Davis-Allen A, Judson MA. Sarcoidosis. Med Clin North Am 2005;
89:817–828
2. Koyama T, Ueda H, Togashi K, Umeoka S, Kataoka M, Nagai S. Radiologic man-ifestations of sarcoidosis in various organs. RadioGraphics 2004; 24:87–104
3. Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS), and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med 1999; 160:736–755
4. Warshauer DM, Lee JK. Imaging manifestations of abdominal sarcoidosis. AJR 2004; 182:15–28
5. Sulavik SB, Spencer RP, Weed DA, Shapiro HR, Shiue ST, Castriotta RJ. Rec-ognition of distinctive patterns of gallium-67 distribution in sarcoidosis. J Nucl Med 1990; 31:1909–1914
6. Kurdziel KA. The panda sign. Radiology 2000; 215:884–885
7. Lewis PJ, Salama A. Uptake of fluorine-18-fluorodeoxyglucose in sarcoidosis. J Nucl Med 1994; 35:1647–1649
8. Nishiyama Y, Yamamoto Y, Fukunaga K, et al. Comparative evaluation of 18F–FDG PET and 67Ga scintigraphy in patients with sarcoidosis. J Nucl Med 2006; 47:1571–1576
9. Love C, Tomas MB, Tronco GG, Palestro CJ. FDG PET of infection and in-flammation. RadioGraphics 2005; 25:1357–1368
10. Hollister D Jr, Lee MS, Eisen RN, Fey C, Portlock CS. Variable problems in lymphomas: Case 2. Sarcoidosis mimicking progressive lymphoma. J Clin On-col 2005; 23:8113–8116
11. Vento JA, Arici M, Spencer RP, Sood R. F-18 FDG PET: mottled splenomega-ly with remission of symptoms after splenectomy in sarcoidosis. Clin Nucl Med 2004; 29:103–104
12. Aberg C, Ponzo F, Raphael B, Amorosi E, Moran V, Kramer E. FDG positron emission tomography of bone involvement in sarcoidosis. AJR 2004; 182:975–977
13. Ludwig V, Fordice S, Lamar R, Martin WH, Delbeke D. Unsuspected skeletal sarcoidosis mimicking metastatic disease on FDG positron emission tomogra-phy and bone scintigraphy. Clin Nucl Med 2003; 28:176–179
14. Brinker H. The sarcoidosis-lymphoma syndrome. Br J Cancer 1986; 54:467–473
15. Schmuth M, Prior C, Illersperger B, Topar G, Fritsch P, Sepp N. Systemic sar-coidosis and cutaneous lymphoma: is the association fortuitous? Br J Dermatol 1999; 140:952–955
16. Dunphy CH, Panella MJ, Grosso LE. Low-grade B-cell lymphoma and con-comitant extensive sarcoidlike granulomas: a case report and review of the lit-erature. Arch Pathol Lab Med 2000; 124:152–156
Prabhakar et al.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.72
on 1
0/31
/15
from
IP
addr
ess
114.
79.2
8.72
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved