mechanism based adverse cardiovascular events and specific inhibitors of cox-2 garret a. fitzgerald...
TRANSCRIPT

MECHANISM BASED ADVERSE CARDIOVASCULAR EVENTS AND SPECIFIC
INHIBITORS OF COX-2
Garret A. FitzGerald M.D.Robinette Professor of Cardiovascular Medicine
Elmer Bobst Professor of PharmacologyUniversity of Pennsylvania


McAdam et al. Proc Natl Acad Sci USA. 1999;96:272.
*20 M arachdonic acid as agonist.
Inh
ibit
ion
of
pla
tele
t ag
gre
gat
ion
(% c
on
tro
l)
0
100
Placebo
20
IbuprofenCelecoxib (mg)
100 400 800
40
60
80
10
30
50
70
90
P<0.01 vs placebo
Coxibs are not platelet inhibitors

COX in Human Platelets: Western Blot Analysis
AnitbodiesCOX-1: monoclonalantibody raised againstpurified ram COXCOX-2: monoclonalantibody raised against theCOOH peptide of humanCOX-2
COX-1
Protein (µg) 10 50 100 30 3010 50 100 10 50 100
45 –
66 –
97 –
117 –
COX-1
EC + PMA
COX-2 COX-2(max exposure)
CO
X-2
CO
X-1
Platelets
COX-2
COX-1
Habib A 2000

Inhibition of prostacyclin synthesis by celecoxib and rofecoxib
* PGI-M = 2,3-dinor-6-keto-PGF1; † P<0.01 vs Placebo; ‡ P<0.05 vs Placebo.
0
40
80
120
160
200
Placebo(n=7)
Celecoxib 400 mg(n=7)
Ibuprofen 800 mg(n=7)
Mea
n u
rin
ary
PG
I-M
* ±
SE
(p
g/m
g c
reat
inin
e)
†
‡
Placebo(n=12)
Rofecoxib50 mg qd
(n=12)
Indomethacin50 mg tid
(n=10)
†
†
0
40
80
120
160
200
McAdam et al. Proc Natl Acad Sci USA. 1999;96:272; Catella-Lawson et al. J Pharmacol Exp Ther. 1999;289:735.
Celecoxib 800 mg(n=7)
†

REGULATED EXPRESSION OF COX-2 IN ENDOTHELIUM BY LAMINAR SHEAR
COX-2
COX-1
Topper et al. Proc Natl Acad Sci USA. 1996
Co
ntr
ol
LS
S 1
hr
LS
S 6
hr
Co
ntr
ol
TS
S 1
hr
TS
S 6
hr
Co
ntr
ol
IL-1
1 h
r
IL-1
6 h
r

PGI2 modulates the cardiovascular response to TxA2 in vivo
Cheng et al Science. 296: 539 – 541, 2002.
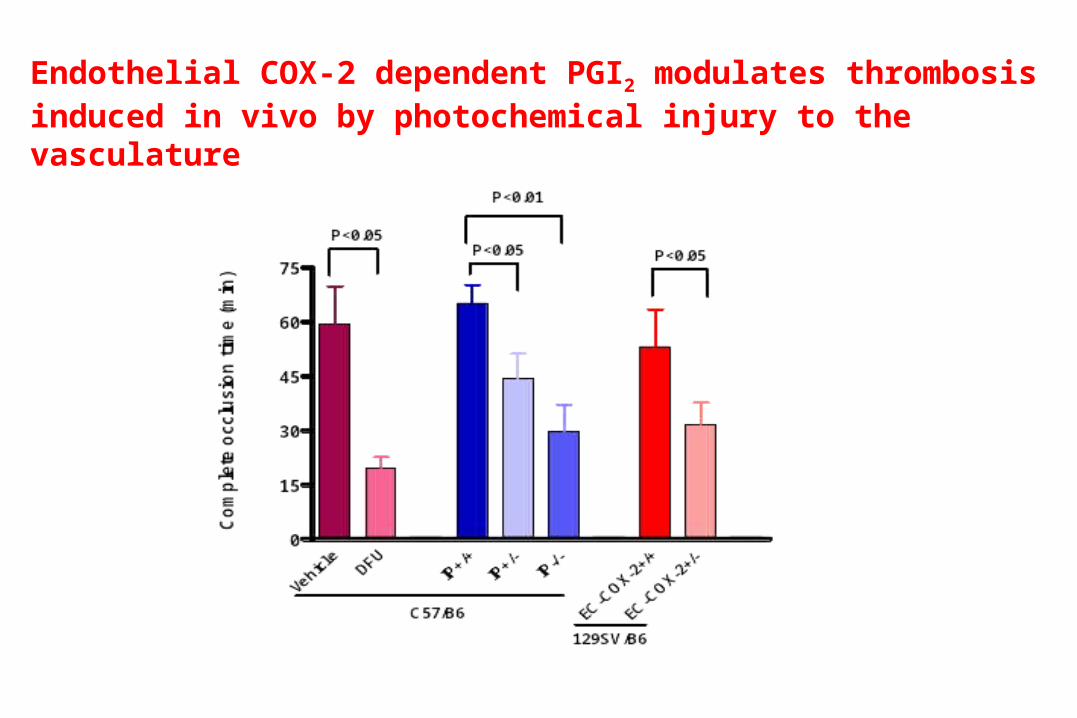
Endothelial COX-2 dependent PGI2 modulates thrombosis induced in vivo by photochemical injury to the vasculature


0
25
50
75
100 PGHS1 KOPGHS1Neo/Neo
WT(10)
(12)
(10)
Co
mp
lete
oc
clu
sio
n t
ime
(m
in)
#
50 mg/kg 100 mg/kg0
25
50
75
100PGHS1 KOPGHS1Neo/Neo
WT
(8) (7)
(12)
(4) (3)
(5)
Re
sis
tan
ce
to
AA
-In
du
ce
dT
hro
mb
os
is (
% S
urv
iva
l)
**
Yu et al JCI (in press) 2005
DELETION OR 98% KNOCK DOWN OF COX-1 PROTECTS AGAINST THROMBOSIS

Parecoxib/valdecoxib and combined coronary
and cerebrovascular events
• Study Valde Plcb Valde Plcb RR 95%CI• =========================================• Ott 311 151 14 2 3.40 0.82-13.98• 2nd CABG 1088 548 17 3 2.85 0.81-10.02 • Meta-analytic RR 3.08 1.20-7.87
• p-value 0.019• p-value heterogeneity 0.86
Furberg, Psaty and FitzGerald Circ 111;249,2005

A. B.
Fig. 1: Ventilation-Perfusion Scan (VQ Scan). A. After inhalation of 20.1mCi of Xenon-133 gas, scintigraphic images were obtained in the posterior projection showing uniform ventilation to lungs. B. After IV injection of 4.1mCi of Tc-99m-labeled MAA, scintigraphic images were obtained in the posterior projection showing decreased activity in the following regions: apical segment of right upper lobe, anterior segment of right upper lobe, superior segment of right lower lobe, posterior basal segment of right lower lobe, anteromedial basal segment of left lower lobe, and lateral basal segment of left lower lobe.
VALDECOXIB AND ENVIRONMENTAL PREDISPOSTION TO THROMBOSIS

MECHANISM BASED CARDIOVASCULAR HAZARD - 1
• HEMODYNAMIC INDUCTION OF ENDOTHELIAL COX-2 DERIVED PROSTACYCLIN
• PROSTACYCLIN CONSTRAINS PLATELET ACTIVATION AND THROMBOGENESIS IN VIVO
• SUPPRESSION OF PROSTACYCLIN DOES NOT CAUSE SPONTANEOUS THROMBOSIS , BUT AUGMENTS THE RESPONSE TO THROMBOGENIC STIMULI IN VIVO
• HAZARD FROM COXIBS PARTICULARLY IN THOSE OTHERWISE PREDSIPOSED TO THROMBOSIS
• HAZARD ATTENUATED BY >98% INHIBITION OF COX-1

Breyer and colleagues 2002

100
110
120
130
140
150
160
170
Normal salt Low salt High Salt
SB
P (
mm
Hg
)
**
† ‡
§
*
SALT SENSITIVE HYPERTENSION IN IPKOs
Francois et al 2004

MECHANISM BASED CARDIOVASCULAR HAZARD -2
• SUPPRESSION OF COX-2 DERIVED PGI2 AND PGE2 INCREASES BP AND AUGMENTS THE RESPONSE TO HYPERTENSIVE STIMULI
• DELETION OR INHIBITION OF COX-1 DEPRESSES THE RESPONSE TO VASOSCONSTRICTORS IN VIVO
• HYPERTENSION ON NSAIDS RELATES TO INHIBITION OF COX-2 AND THE SELECTIVITY WITH WHICH IT IS ATTAINED
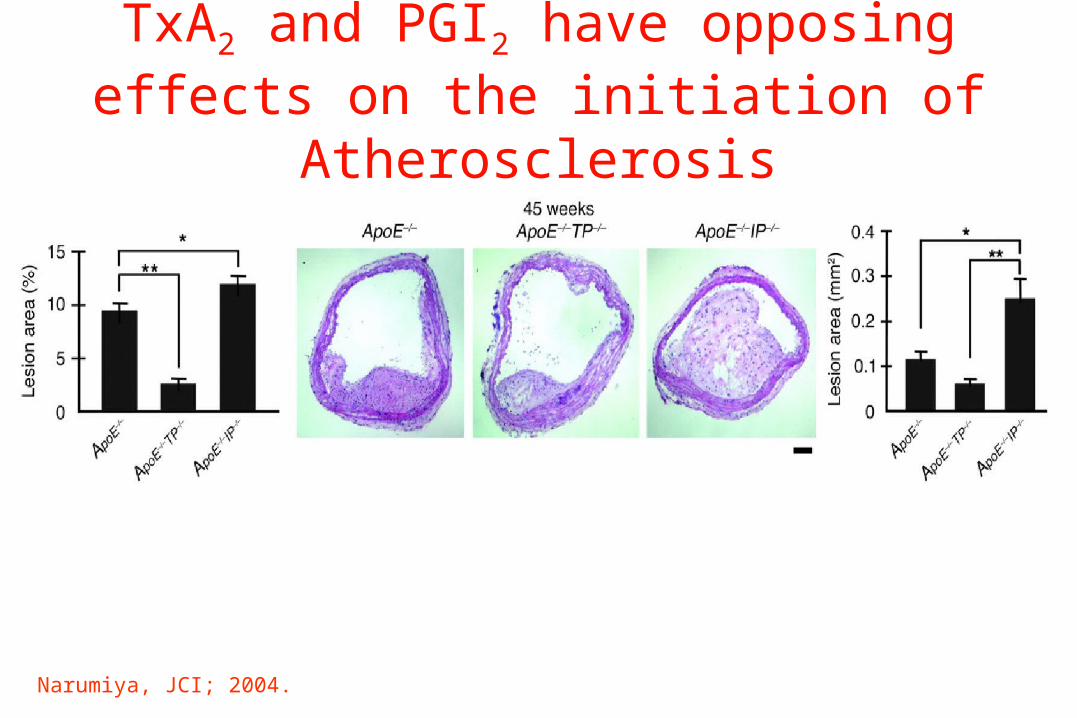
Narumiya, JCI; 2004.
TxA2 and PGI2 have opposing effects on the initiation of Atherosclerosis

DELETION OF THE IP REDUCES MARKEDLY THE ANTIATHEROSCLEROTIC EFFECT OF ESTROGEN IN VIVO
Egan et al Science 306; 1954- 1957, 2004

MECHANISM BASED CARDIOVASCULAR HAZARD -3
• INITIATION AND ACCELERATION OF EARLY ATHEROGENESIS BY DELETION OF THE IP
• FOSTERS PLATELET AND NEUTROOPHIL ACTIVATION AND VASCULAR INTERATIONS
• REMOVES CONSTRAINT ON ATTENDANT OXIDANT STRESS.
• HYPERTENSION ALSO ACCELERATES ATHEROGENESIS
• PREDISPOSITION TO ATHEROSCLEROSIS AND HYPERTENSION ATTENUATED BY COINCIDENT INHIBITION OF COX-1

Confirmed Thrombotic EndpointKaplan-Meier Estimates (95% CI)
RR(95% CI): 1.96 (1.20, 3.19)*
* p<0.05
Patients at RiskPlacebo
Rofecoxib 25 mg1299 1192 1148 1079 1039 1002 4701287 1123 1050 986 935 898 411
0 6 12 18 24 30 36
Month
0
2
4
6
8C
umul
ativ
e In
cide
nce(
%)
with
95%
CI
PlaceboRofecoxib 25mg

COX-2COX-2
PGIPGI22
COX-1 COX-1
BPBP
TXATXA22
COX-1COX-1
COX-2 COX-2
Cardiac Cardiac FibrosisFibrosis

HIGHHIGH
Detection of a Cardiovascular Signal
NNT &/or Trial DurationNNT &/or Trial Duration
INTERINTER
LOWLOW
CABGCABG
? RA? RA
OA /OA /?? PolypsPolyps
LOWLOW
INTERINTER
HIGHHIGH
Intrinsic Intrinsic CV RiskCV Risk
Drug Exposure Drug Exposure and Selectivity and Selectivity in vivoin vivo

VARIATION WITHIN A CLASS EFFECT
• Underlying substrate of cardiovascular risk
• Dose, duration of dosing
• Duration of drug action
• Volume of distribution?
• Concomitant therapy – eg ASA





WHAT ABOUT
TRADITIONAL NSAIDs?

Effects of Aspirin or Ibuprofen Alone on COX-1
Ibuprofen 400mg tid x6 days
Aspirin 81mg qd x6 daysHOURS
2 6 240
25
50
75
100
0
25
50
75
100
HOURS2 6 24
PLATELET AGGREGATION
% inhibition
SERUM THROMBOXANE
Catella et al NEJM 345:1809 -1817,2001

RR=1.04 [1.00-1.08
RR=0.88 [0.8-0.95]
RR = 1.03 [.96-1.1]
NSAIDs
NAPROXEN
IBUPROFEN
NAPROXEN : HALF AS GOOD AS ASPIRIN?
RR OF MYOCARDIAL INFARCTION
Garcia Rodriguez 2004

The VIGOR Study
Event Rofecoxib Naproxen
Stroke 9 (0.2%) 8 (0.2%)
Myocardial Infarction 20 (0.5%) 4 (0.1%)
*

Differential Recovery From Steady-State Inhibition Of Platelet COX-1 By Low-Dose ASA and
Naproxen
ASA = aspirin; COX = cyclooxygenase.
Capone et al 2003
6065707580859095
100
PlateletCOX-1
%Inhibition
P <.01
Naproxen (N = 9)ASA (N = 8)
P <.01
Time (hours after last administration)
P =.074
1 3 12 24

Human Whole Blood COX 1/COX 2 Assays
Updated from FitzGerald & Patrono, N Engl J Med 2001; 345:433-442
Indomethacin
Naproxen
Ibuprofen
6-MNA
Acetaminophen
Diclofenac
CelecoxibNimesulideMeloxicam
Rofecoxib
Valdecoxib
Etoricoxib
Lumiracoxib
0,01COX-1 IC50
M
COX-2 IC50 M
0,01
0,1
1
10
100
0,1 1 10 100

Diclo COX-2
Diclo COX-1
0
20
40
60
80
100 Cele COX-1Cele COX-2
% Inhibition
Diclofenac = Celebrex in whole human blood in vitro
Patrignani et al 2005

Aspirin / Ibuprofen vs Aspirin / Diclofenac
*
0
25
50
75
100
HOURS
2 6 12 24
Aspirin 81mg qd /Diclofenac-DR 75mg bid
Aspirin 81mg qd / Ibuprofen 400mg tid
HOURS
2 6 12 24
* *
0
25
50
75
100
PLATELET AGGREGATION
% inhibition
SERUM THROMBOXANE

Diclofenac = Celecoxib
• Same selectivity in whole blood in vitro
• No pharmacodynamic interaction with asa
• No clinical asa interaction in MI protection
• Superimposition of GI and CV events in CLASS
• EDGE and MEDAL – comparisons within the class



tNSAIDs and CV risk
• Evidence that naproxen achieves sustained platelet inhibition in some individuals. A “dilute” aspirin?
• Evidence that diclofenac is a COX-2 inhibitor like celebrex ( with hepatic AEs )
• Evidence that ibuprofen might undermine benefit from asa
• No rationale for lumping diclofenac and ibuprofen as “non-naproxen NSAIDs”

DEAD DRAGONS
• It’s all naproxen
• Hypertension is a different mechanism
• Off target fantasies
• It’s just a matter of reducing the dose
• Time for a study of coxibs in ACS

Lumen
Laminin Smooth muscle cell actin
TP antagonism with COX-2 inhibition results in plaque destabilizationTP antagonism with COX-2 inhibition results in plaque destabilization
Vehicle
COX 2
TP
COX 2 / TP
Egan et al Circulation 111;334-342,2005

THE WAY FORWARD?
• Exclude patients at high intrinsic risk of thrombosis from exposure to selective inhibitors of COX-2
• Dose reduction alone does not protect from individual hazard due to variability in dose – response
• Subject drugs already approved to the same requirements for extended dosing as drugs yet to be approved
• Restrict duration of dosing until the parameters of safety for extended dosing are established

Interindividual variability in the responses to coxibs
ex vivo COX-2 assay ex vivo COX-1 assay
urinary 2,3 dinor-6-keto PGF1a urinary 11-dehydro TxB2
Inhi
bitio
n se
rum
PG
E2
(pos
t dos
e / p
re d
ose
ratio
)
0.1
1
5
placebo rofecoxib celecoxib
Inhi
bitio
n se
rum
TxB
2
(pos
t dos
e / p
re d
ose
ratio
)
placebo rofecoxib celecoxib
urin
ary
PG
I-M
(pg/
mg
crea
tinin
e)
10
50
100
200
300
placebo rofecoxib celecoxib
50
100
500
1000
2000
placebo rofecoxib celecoxib
urin
ary
TxM
(pg/
mg
crea
tinin
e)
Fig. 3
A B
DC
0.1
1
5


PERSONALIZED MEDICINE AND THE FUTURE OF THE COXIBS
• Restrict to individuals intolerant of tNSAIDs plus PPIs
• Determine whether risk transformation occurs during chronic dosing
• Combine physiologic, biochemical and genomic variables in discriminant analysis of evolving risk in existing trials – APPROVe, APC etc
• Validate prospectively in studies of extended dosing

CONCLUSIONS• Selective inhibitors of COX-2 depress PGI2 without
concomitant inhibition of TxA2
• This can result in an augmented response to thrombotic and hypertensive stimuli and acceleration of atherogenesis in mice
• An increase in MI and/or stroke has been seen in 5 placebo controlled trials with 3 structurally distinct COX-2 inhibitors
• Hazard would be expected to relate to drug selectivity, dose and duration of exposure and to interindividual differences in drug response