med.mahidol.ac.thmed.mahidol.ac.th/surgery/sites/default/files/public/pdf... · pathology •it is...
TRANSCRIPT









3rd degree hemorrhoids

4th degree hemorrhoids

Open hemorrhoidectomy

Closed hemorrhoidectomy

Stapled Hemorrhoidectomy

Instructions following anorectal operations
• Diets
• Sitz baths
• Dressings
• Medications:
Bulk-forming agents
Anagesics; NSAIDS, Paracetamol
Antibiotics; Metronidazole, Augmentin

Anal Fissure
Pathology
• It is a tear or crack in the lower portion of the anal canal
• It may be acute or chronic
• Causes:
1- Passage of large,
hard stool .
2- Explosive diarrhea.
3-Trauma to the anus.

Anal Fissure (cont.)
-100% men posterior midline.
-10% women anterior midline.Patients tend to have high internal
sphincter tone with resulting poor
anodermal perfusion to the posterior
portion .

Anal Fissure (cont.)
History1- Pain during and after bowel motion.
2- Streaks of blood on stools or tissue paper.
AR examination:
-High anal sphincter tone.
- Just separating the skin around anus will display the fissure.
- Associated findings
• – sentinel tag externally
• – enlarged anal papilla internally
(No attempts to do P.R. during acute stage)

Anal Fissure (cont.)
acute chronic

Treatment of Anal Fissure

Anal Fissure (cont.)
Anal Fissure
Acute Chronic
Non-surgical
ResolutionLateral
Internal
Sphincterotomy
Failure
Repeat Rx
Resolution Treat as chronic
Rule out
other causes
Resolution Failure
Repeat Sphincterotomy

Vicious cycle of anal fissure

Treatment of Anal Fissure (cont.)
• Non-surgical• Dietary: high fiber, avoid spicy foods
• Local anaesthetic : 10% Xylocaine jelly
• Local hydrocortisone: proctosedyl ointment
• Local Nitrates (e.g. Glyceryl trinitrate)
• Calcium channel blockers (e.g.nifedipine, diltiazem)
• Botulinum toxin
Cochrane database of systemic reviews. 2004, Vol2

OPEN:Internal sphincter directly visualized
CLOSED:Blade no.11 stabin between the int. and ext. anal sphincter
Surgical

Anorectal Abscess/fistula
• Pathogenesis : mostly 2° to
nonspecific anal gland infection
• infection → intersphincteric abscess
• – Abscess represents acute infection
• – Fistula -chronic sequelae of anorectal abscess
•Intersphincteric
(#3)•Extending up ordown• can becircumferentialSupralevator
Ischiorectal#2
Perianal #1

Pathogenesis

Classification of Anorectal Abscesses

Clinical Presentations of Anorectal Abscess
• Pain & swelling (~95%)
• Discharge (only 15%)
• Fever (only 18%)
• M:F ~2:1
• Peak incidence 20-40 y/o
• PE: Bimanual palpation
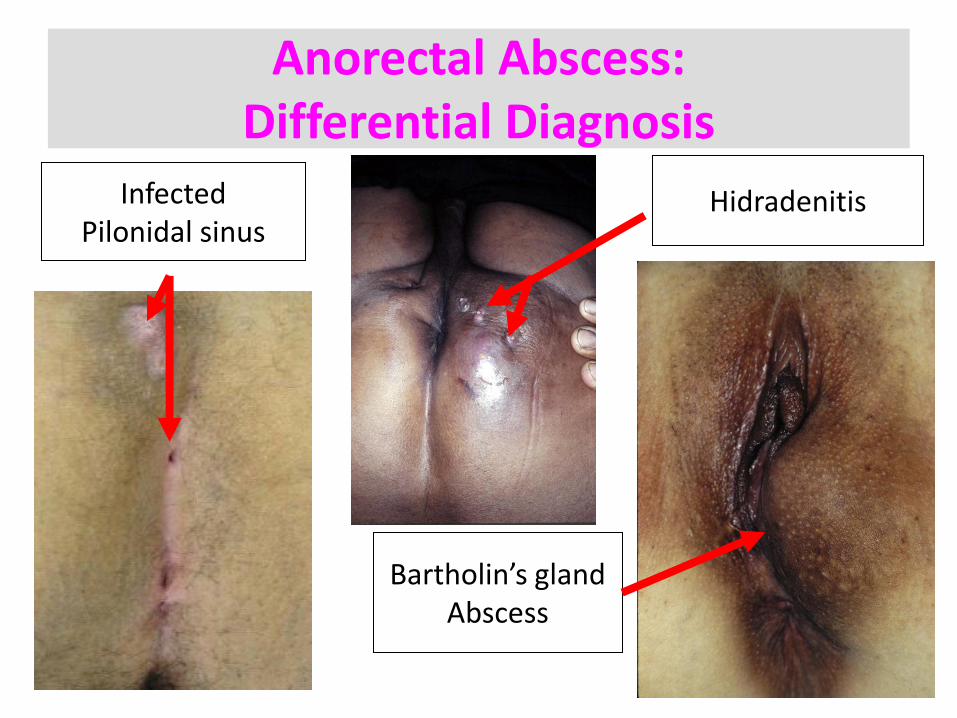
Anorectal Abscess:Differential Diagnosis
Bartholin’s glandAbscess
InfectedPilonidal sinus
Hidradenitis

Anorectal Abscess:Treatment
• Anoscopy (look for internal opening)
• Incision & Drainage: mostly under LA
• Postop: sitz baths, dressing changes, pain control, antibiotics?

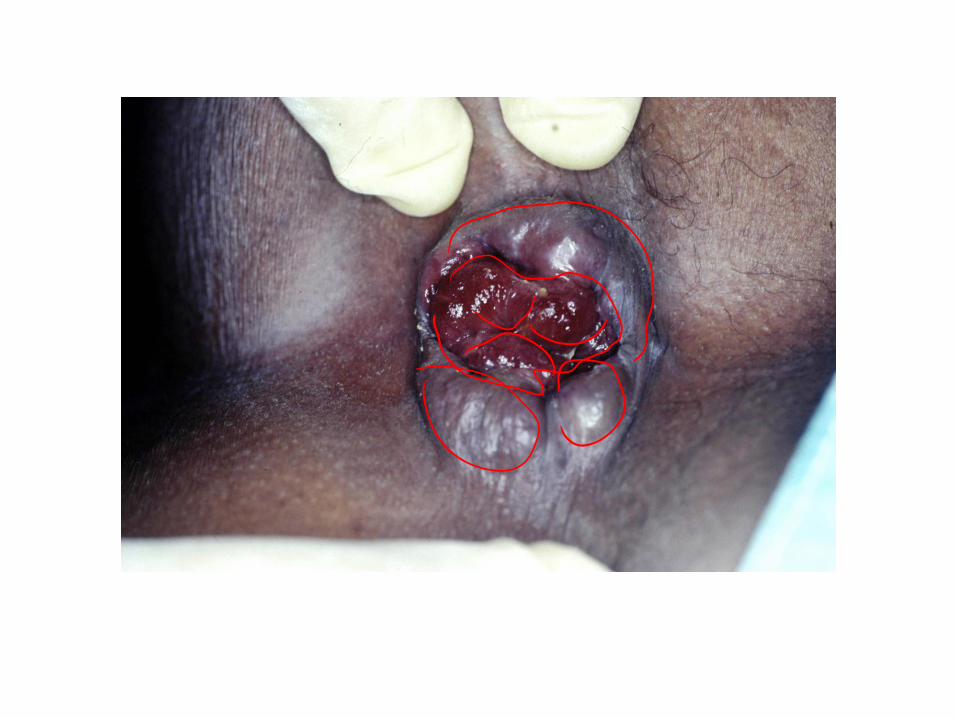
Anorectal Abscess (cont.)
• If PR finds internal bulge → internal
• sphincterotomy over abscess
• • Special situations:
• – Supralevator: drained via rectum
• – Horseshoe abscess: drained via rectum with counter drains in ischiorectal space

Horseshoe Abscess

Fistula-in-ano
• Pathogenesis• Chronic form of anorectal abscess
• Communication between the internal opening at the dentate line and the external opening at the perinealskin
• usually within 3 months following of anorectalabscess
• Incidence : 40-60% of anorectal abscess

Goodsall’s Rule
• Prediction of the tract
• between 2 openings
• • Anterior → straight
• • Posterior → curved

Classifications ofFistula-in-ano
IntersphinctericMost commonTract confined toIS plane
Transsphincteric:Goes through bothsphincters
SuprasphinctericTract loops oversphincters, goesthrough levator
ExtrasphinctericRectum to skinWith or without involvingsphincters

Fistula-in-ano
• Evaluation
• Anoscopy + gentle probe of tract
• Goodsall’s rule to anticipate fistulous tract
May use methylene blue/H2O2
• Flexible sigmoidoscopy,Fistulography,ERUS and MRI may help in complicated cases

Fistula-in-anoevaluation

Fistula-in-anoevaluation

Fistula-in-anoevaluation

Fistula-in-ano
• Treatment• Aim• healed vs. incontinence
• • Incise skin, see how much sphincter involved• – small →fistulotomy, fistulectomy• – a lot → seton (staged procedure) vs. advancement flap

Fistulectomy


WHICH DISEASE ??
MASS BLEEDING PAIN DISCHARGE
EXT.HEMORRHOIDS
++++ +/- +++ +/-
INT.HEMORRHOIDS +++ ++++ +/- +
ANAL FISSURE + + ++ ++++ +/-
ANORECTAL
ABSCESS +++ +/- ++++ +
FISTULA-IN-ANO +++ + ++ ++++

Take Home Messages
• All anal complaint is not due to hemorrhoids
• Take history of mass,bleeding,pain and discharge
• Complete anorectal examination should be part of the evaluation
• Think biopsy for ulceration or skin changes
• Fiber is the colon’s best friend

Thank YouFor
Your Attention