medicaid pcmh lonnie robinson, md, faafp arkansas academy of family physicians regional family...
TRANSCRIPT

Medicaid PCMHLonnie Robinson, MD, FAAFPArkansas Academy of Family Physicians
Regional Family Medicine
Beth Milligan, MD, FAAFPArkansas Foundation for Medical Care
Saline Med-Peds
Sheena Olson, JDAssistant Director of Medical Services
Arkansas Medicaid

Overview• PCMH Background/Context• My PCMH Experience• Medicaid PCMH Requirements• Questions and Answers

Alternative Titles• Practical PCMH• DIY PCMH• “PCMH for the workin’ doc” • PCMH: Yeah, right!• PCMH: All theory, no (green) substance?• PCMH: Why are we still talking about this?• PCMH: Why it (still) matters

Why before How
“He who has a why to live for can bear almost any how.” -Nietzche
Why PCMH?• Increasing healthcare costs, percentage of GDP• Poorer health outcomes• Patient lifestyle/low engagement in care• Increasing understanding of the value and ROI
from primary care• Failure of FFS model (incentivize disease and
intervention over prevention and wellness)• Burden of chronic disease• Momentum from big business…

Personal Health CostsMedical CarePharmaceutical costsWorkers’ Compensation Costs
Productivity Costs
Presenteeism OvertimeTurnover
Temporary StaffingAdministrative Costs
Replacement TrainingOff-Site Travel for Care
Customer DissatisfactionVariable Product Quality
Absenteeism Short-term Disability Long-term Disability
Frustration with poor health -- both employers and employees
Iceberg of Additional Costs to Employers from
Poor Health
Sources: Loeppke, R., et al., "Health and Productivity as a Business Strategy: A Multi-Employer Study", JOEM.2009; 51(4):411-428. and Edington DW, Burton WN. Health and Productivity. In McCunney RJ, Editor. A Practical Approach to Occupational and Environmental Medicine. 3rd edition. Philadelphia, PA. Lippincott, Williams and Wilkens; 2003: 40-152
70
%3
0 %

Why PCMH is important for Family Physicians…
• Primary care is receiving a LOT of attention in the health care debate
• The era of value-based purchasing means there is a new normal arriving
• Fee For Service with no accountability is becoming a thing of the past
• Change is coming…change or die!• You don’t want to be the slowest antelope• Most Important: it’s the right thing for our
patients!

Paralyzed by Confusion
Embracing the Opportunities
Happily Existing in
Denial
Resigned to Acceptance
UnderstandingLower Greater
Greater
Lower
Resiliency
Leadership is needed: The Four Camps of Health Organizations

Arkansas is leading!• Medicaid PCMH• Comprehensive Primary Care Initiative• Private Payer Projects (forthcoming)

Leadership: “Pissing people off at a rate
they can absorb…”
Marci Nielsen, PhD, MPHCEO, Patient Centered Primary Care Collaborative

“If you always do what you always did, you will always get
what you always got.”
- Albert Einstein

Cowboys vs. Pit Crews
Atul Gawande, MD, MPH• Harvard Professor, Surgeon, Writer• Public Health Researcher• Speech at Harvard, 2011
– “We train, hire and pay physicians to be cowboys…”• The Lone Ranger
– “…Instead, we should be training them to be like Pit Crews.”
• Focused on teamwork, disciplined, data-driven, standardized
• Also credited with “Triple Aim…Plus One”

Quadruple Aim / Triple Aim + One
Reduced Costs
Improved Outcome
Patient Sat-isfaction
Physician Satisfac-
tion

PCMH “Need to Knows”
Dr. Jonathan Sugarman, Qualis HealthAAFP Annual Leadership Focus
May 2, 2014

PCMH “Need to Knows…”
• Despite the short half-life of many health policy innovations (buzz words), medical homes continue to capture the attention of key stakeholders
• PCMH’s are living up to expectations*• The payment landscape is changing in a
positive way
*Depending on whom you ask!

16
The Hype Cycle: Waves of Irrational Exuberance
Time
Expectations
Real Progress
Trigger Peak of Inflated
Expectations
Trough of Disillusionment
Slope of Enlightenment
Plateau of Productivity
Adapted from Gartner Research
Medical Homes?

17
Are PCMH’s living up to expectations?It depends on whom you ask…

18
Feb. 25, 2014
"There are folks who believe the medical home is a
proven intervention that doesn't even need to be
tested or refined. Our findings will hopefully change
those views," said Mark W. Friedberg, a researcher
at RAND Corp. and lead author of the study,
published Tuesday in the Journal of the American
Medical Association.
(Friedberg et al. JAMA. 2014;311(8):815-825).

Response to JAMA article• “A practice could be a PCMH without achieving
certification and achieving certification does not necessarily mean that a practice is functioning as a PCMH”
• The study group received financial incentives for NCQA certification but not for controlling costs
• No after hours or extended hours• No targeting of high risk populations• Missing key features: patient-centeredness, team-
based care, and behavioral health integration• Authors response ignored results from bulk of previous
data

States with Medicaid/CHIP Medical Home Activity Since 2006

States with an Active Role in a Multi-Payer Medical Home Initiative

Medicaid PCMH
• Minimum 300 ConnectCare Medicaid Patients• Beginners welcome…No certification required • Practice Support: Qualis, AFMC• Must meet milestones, achieve metrics• Reimbursement via Alternative Payment Model:
– PMPM payments (average: $4)– Continued FFS for encounters as previously– *Opportunity to participate in “shared savings”
*Must meet eligibility requirements

Regional Family Medicine
• Formerly Kerr Medical Clinic• 8 physicians, 3 APNs, 50+ employees, • 2 locations• Inpatient / Outpatient / Obstetrics• Lab / Radiology• 27,000+ active patient charts• EHR: e-MD’s (April 2012)• MU/PQRS attested

RFM PCMH Journey• Launched e-MD’s April 2012• Applied CPCi June 30, 2012• Attested Stage I MU mid-July 2012• Formed PCMH Transformation Team • Enrolled Medicaid PCMH• January: first PMPM payment!• Pooled for shared savings with pediatric
practice in Jonesboro

RFM: Existing PCMH Characteristics
• Physician-based teams with “care coordinator”
• 24/7 live voice access• Extended office hours: Saturday• ER, hospitalization avoidance • Dr. Robert Kerr: “The Answer is ‘Yes’…”

RFM Changes• Initial:
– Identification of High Risk Patients– “Care Coordinator”– Patient notification (text)– Care Plan (“Well-written SOAP Note”)– Documentation of same day appt requests
• Upcoming/Ongoing: – Formal Quality Improvement Process– Patient Portal– SHARE– Formal Policy & Procedures– Optimizing EMR to perform key PCMH functions

PCMH Challenges• Organizational structure, inertia, momentum• Culture change (team-based care mind set)• Documentation• Overcoming Lingo/Jargon Gap• Leveraging technology• Doing all of the above in a traditionally high-
volume practice (“Just one more thing, Doc…”)• Payer Issues (comprehensive participation,
data mistrust)

Bottom Line• PCMH ain’t going away
– FFS as sole means of compensation is (rapidly?) becoming a thing of the past
– Value-Based Purchasing is becoming the new normal• Medicaid PCMH: great way to start process
– PMPM’s to assist in beginning processes– Continued FFS for episodic/acute care– Opportunity for shared savings– Practice support from AFMC, Qualis– Prepares your practice for other opportunities,
aligns with other incentives (MU, PQRS, etc.)


Medicaid PCMH Requirements
Dr. Beth Milligan, MD, FAAFPArkansas Foundation for Medical Care
Saline Med-Peds

Patient Centered Medical HomeBuilding a healthier future for all Arkansans
Health Care Payment Improvement Initiative
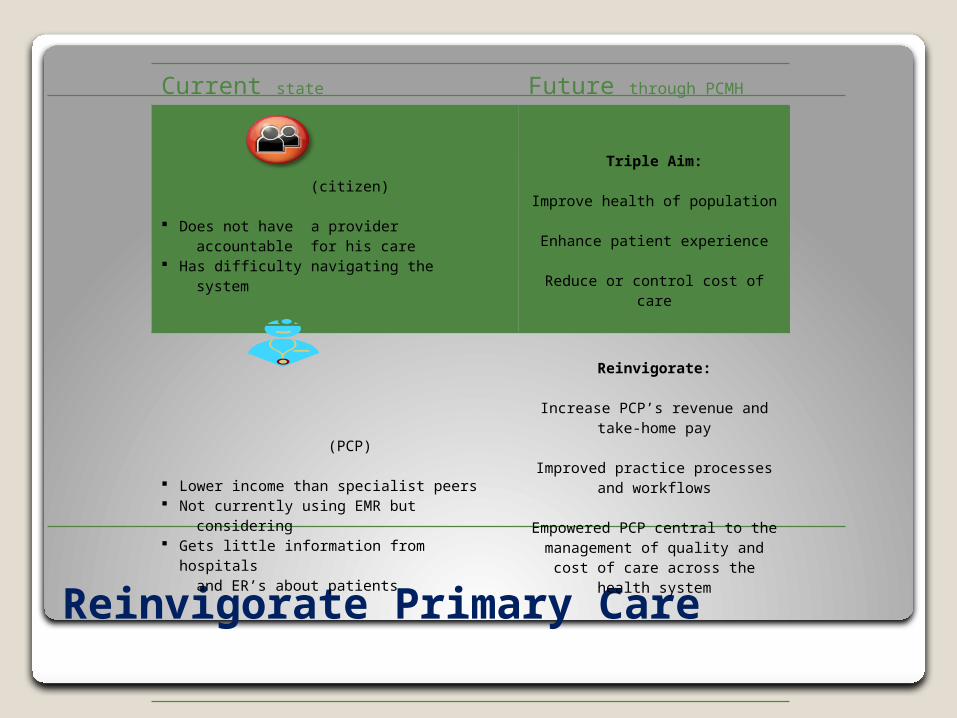
Reinvigorate Primary Care
Current state Future through PCMH
(citizen)
Does not have a provider accountable for his care Has difficulty navigating the system
Triple Aim:
Improve health of population
Enhance patient experience
Reduce or control cost of care
(PCP)
Lower income than specialist peers Not currently using EMR but considering Gets little information from hospitals and ER’s about patients
Reinvigorate:
Increase PCP’s revenue and take-home pay
Improved practice processes and workflows
Empowered PCP central to the management of quality and cost of care across the health system
Purpose
Our aim is to create a
Sustainable patient-centered health systemthrough an evidence-based approach to care delivery
Population-based care delivery systemEpisode-based care delivery
Triple Aim AccountabilityImprove the health of the populationEnhance patient experience of care
Reduce or control cost of care

Process
Commitment to transform the systemState launches PCMH
Providers enroll
Support for providersFramework for change
Financial support for care coordinationTechnical expertise and vendor support
Transparency into performance
Incentives for quality and costQuality metrics ensure provision of appropriate care
Shared savings incentives encourage management of cost of care

Enrollment/Eligibility
PCMH Participation & EligibilityPCPs enrolled in ConnectCare
Must have at least 300 beneficiariesMeet participating practice definition (Section 200.000 proposed PCMH manual)
May not participate in the PCCM Shared Savings Pilot
To Enroll:
Provider Portalwww.paymentinitiative.org
Open Enrollment through December 15January 1 through May 15, 2014
VoluntaryPractice Participation Agreement
Annual re-enrollment

Enrollment/Eligibility
Shared Savings:Incentive payments made to a shared savings entity for delivery of economic, efficient and quality
care that meets the requirements of Section 232.000
Minimum of 5,000 Medicaid beneficiaries who have been attributed for at least 6 months
Single practice or by pooling attributed benes across more than one practice (up to 2 practices per entity 2014)
Practice Support:Section 241.000 – 242.000
Shared Savings Criteria
First Performance PeriodJanuary 1, 2014
Single practice or by pooling attributed benes across more than one practice (up to 2 practices per entity 2014)
If two practices, they must agree to measure performance togetherNo default pool
Second Performance PeriodTwo practice limit for pools is removed
Default poolMust be part of a shared savings entity to participate in PCMH

Benefits
Providers will receive practice supportCare Coordination
Monthly paymentsTechnical expertise
Practice TransformationOption to utilize DMS vendor support
Quarterly performance reports
Shared SavingsReward high quality care and cost efficiency
Enrollment
Enrollment