medical device regulatory, reimbursement and compliance congress randel e. richner, bsn, mph...
Post on 19-Dec-2015
218 views
TRANSCRIPT

Medical Device Regulatory, Reimbursement and Medical Device Regulatory, Reimbursement and Compliance CongressCompliance Congress
Randel E. Richner, BSN, MPH
President, Founder
March 27, 2008
Value-Based Pricing: The Good, The Bad, and The Ugly
Reform
“There is no problem, however difficult, which if we roll up our sleeves, we cannot completely ignore”. |
--George Carlin

Policy OverviewPolicy OverviewTechnology Is Good.
Technology per se, does not “cause” increased health care costs…
1. It is only randomly possible to accurately detect the true value of technology due to a fragmented care delivery, migration of services, and system issues (complex overlay of private/public insurers to track and monitor care and value).
Misaligned payment systems may cause perverse care incentives and artificial determinants of “value”.
2. The calculation of risk in determining the threshold of “value” is largely ignored.
3

New, Innovative and Complex TechnologiesNew, Innovative and Complex Technologies
• Devices are getting smarter and are providing more information– Intelligent devices
– Biotechnology Revolution
– Personalized Medicine
– Combination Products
– Information-Rich Therapeutics
4

Ear
l y a
do
pt e
r E
arl y
Ma j
or i
ty
Lat
e m
aj o
rity
Prove Principle Drive Adoption Change Standard
IntroduceDisruptiveProduct
ValidateLaunch post-FDA
Typical Market Development
Promote clinical utility
Establish a network of advocates
Position for Market Penetratio
n
Drive your message into the market
Secure satisfactory reimburse-ment.
Promote improved care

Innovation: PTCA
Time (in years)
% P
enet
ratio
n
Intensity of adoption: • Highly respected pioneer• Decreased procedural costs• Improves patient satisfaction• Shortens LOS
Intensity of adoption: • Highly respected pioneer• Decreased procedural costs• Improves patient satisfaction• Shortens LOS
Uptake: • Replaces CABG• Moves procedure from OR to CCL• Creates new medical specialty
Uptake: • Replaces CABG• Moves procedure from OR to CCL• Creates new medical specialty
Length of Reign: • Continuous improvement• Unsatisfactory alternatives
explored• Upgrade to stents
Length of Reign: • Continuous improvement• Unsatisfactory alternatives
explored• Upgrade to stents

Technology Assessment and Value

Local
Regional
Geographic Level
National
Technology AccessTechnology Access Decision-Making Occurs at Multiple Levels
• CMS, (Global--International) • Major national third party payers and
benefit managers
• Medicare Intermediaries and Carriers, DMERCs
• Regional health plans
• Medicaid administrators• IDNs• Physician groups• Hospitals
Organizations Involved
8

FDA/CMS DivergenciesFDA/CMS Divergencies
Treatable Population
FDA Label Indicated
PopulationCMS
Covered Population
Uncertainties:
How will CMS define and pay for incremental benefit?
How long will full coverage of labeled indications take?
•FDA regulator: public health/safety• Safe products
• Assumes Market sorts out clinical value and comparative effectiveness
• Standards vary by risk
CMS regulator: purchaser
– Improved health for good value
– Increased focus on clinical benefits blur into public health effort
– Decisions are broad, policy-based
9
Evidence Development and Value Evidence Development and Value Technology Assessment:
• Evidence Based Medicine: • Coverage with Evidence Requirements• Practice Based Management • Pay for Performance• Quality Outcomes• Outcomes Assessment:• Cost-Effectiveness Analsyis
• Outcomes Demonstration Projects
• Overuse, Underuse, Misuse
• Superior Medical outcomes
• Least Costly Alternative
• Substantial Equivalence
• Comparative Effectiveness

Type of data you collect depends on the Type of data you collect depends on the category of productcategory of product
Similar to Another Product
Expansion of Existing Technology
Truly New and Innovative
Evidence Required Usually FDA approval with same indications suffice for inclusion in
existing coverage
Publication of Controlled Studies (usually 1-2)
Coverage under Protocol
Publication of 2 – 4 RCTs with ongoing study
through Registry Data, Cost-Effectiveness Data
Evidence Should Prove
Similar clinical efect and outcomes, cost-efficacy a
plus for differentiation
Incremental clinical and / or economic value of the
device relative to its predicate
Higher degree of certainty. RCTs show
improved outcomes over other treatments, with
lower costs
Clinical Trial Data Types
Necessary/
Optional
Regulatory approval, Practical clinical trial,
limited cost study
RCTs, Cost-effectiveness, Long-term
outcomes, Ongoing Practical Clinical Trials
RCTs, Cost-effectiveness, Long-term
outcomes, Practical Clinical Trial, Post-market
registry

Payment Misalignments and determining Value

Medicare’s Complex Reimbursement Medicare’s Complex Reimbursement ProcessesProcesses
• Each payment system has its own rules, based in statute, and uses data from the providers it pays• Different payments in different sites for the same
items or services• Can create inappropriate incentives• Providers learn to balance underpaid/overpaid
services to achieve bottom-line• Benefits of less invasive services, migration to less
costly settings, not recognized in value calculations
13

Major CMS Payment SystemsMajor CMS Payment Systems
• PROSPECTIVE PAYMENT SYSTEMS:– Inpatient PPS
– Outpatient PPS
– Inpatient Rehab
– Long-term Care Hospital
– Inpatient Psych
– Skilled Nursing Facility
– Home Health
• FEE SCHEDULES:– Physicians
– Ambulatory Surgical Centers
– Clinical Labs
– Durable Medical Equipment, Prosthetics & Orthotics
– Ambulance
– ESRD
14
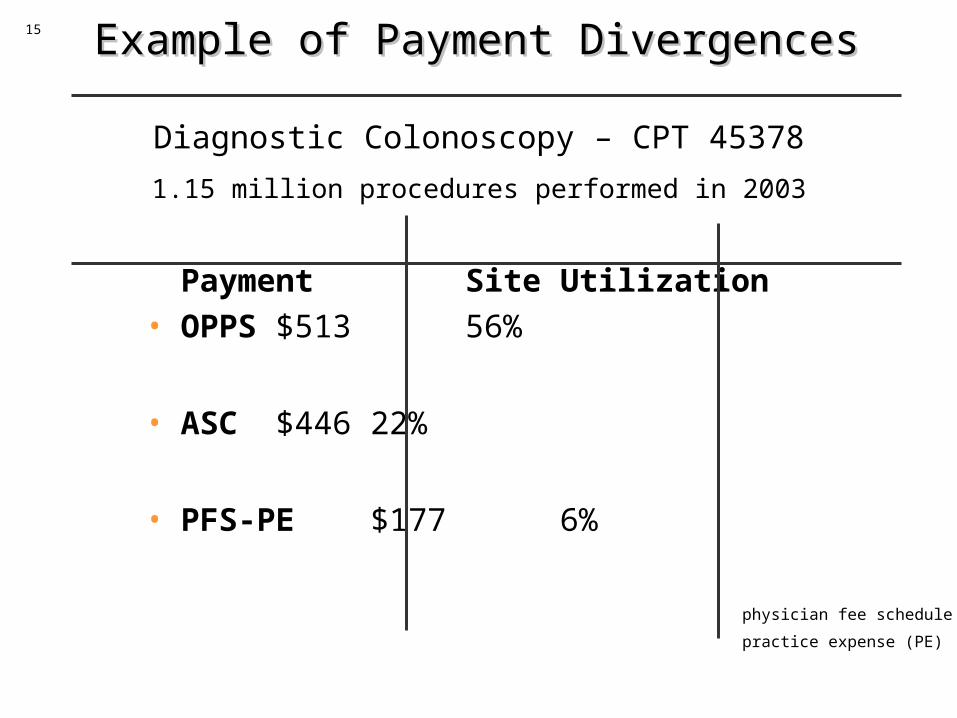
Example of Payment DivergencesExample of Payment Divergences
Payment Site Utilization• OPPS $513 56%
• ASC $446 22%
• PFS-PE $177 6%
Diagnostic Colonoscopy – CPT 45378
1.15 million procedures performed in 2003
physician fee schedule (PFS)
practice expense (PE)
15

Home Hemodialysis provides great value; providers limit adoption
• Major clinical benefits– LVH, heart failure improvement– Anemia– Rehabilitation/QOL
• 15-25% annual savings potential ($10-17K of 70K costs)
– Kaiser promoting home dialysis
VS.

Daily home dialysis challenges
Largest savings in hospital costs, which are part of a different
budget (Part A vs. Part B) and are not
realized by the dialysis provider
Risks

Consider Unique technology-specific issues
• Risk: should the level of “evidence” be the same for a new MRI test as for a new brain aneurysm stent?
• Operator Skill: How does one design the impact of physician end-user skills on patient outcomes and study design?
• Life Cycles: How do we expect to use traditional study approaches with minimum of 3 years from start to pubs when technology changes within a 2 years?
• Combinatorial science: How does the study account for the manufacturing changes (polymers, voltages, wires and metals, drugs) on the effect of patient outcomes?
• Physician end-user involvement: How are physicians mobilizing to determine the outcomes critical to study to determine value?

0.07
2.8
10.4
3565 76
0.01
0.1
1
10
100
1000
Small
pox v
accin
e
Antihi
stamine
s
Daily a
spirin
Clozap
ine
Tysab
ri fo
r MS
VioxxD
ea
ths
pe
r 1
00
,00
0 p
ers
on
-ye
ars
Drug Risks:Near-Term Fatalities Per Person-Year
Log Scale
3 OrdersOf
Magnitude

Transportation
0.07
2.8
10.4
3565 76
0.01
0.1
1
10
100
1000
Smal
lpox v
accin
e
Antih
istam
ines
Daily a
spirin
Clozap
ine
Tysab
ri fo
r MS
Vioxx
De
ath
s p
er
10
0,0
00
pe
rso
n-y
ea
rs
Commercial airplane: 0.15
Passenger car: 11
Truck drivers: 45
Motorcycle: 450
Cell phones + driving: 1.3

Solution 1: Value• New Study Paradigm. Encourage access, innovation• Risk-based stratification of evidence• Physician end-user involvement• Focus on treatment comparisons rather than individual
product comparisons • Electronic records, and HIT advances; invest in this
infrastructure. • Gold standard, database, epidemiological studies• Bayesian analysis: “preexisting” data are constantly
adjusted using new data as acured: potential reduction of sample sizes, and ability to continually update probability of success or failure.
• Collaborate with NIH, AHRQ, Private, public entities. • Global interactions and use of data

Solution 2: Reward the Future• Reward preventative services and interventions that can clearly
demonstrate a significant value over existing products.
• Integrate nanotechnology, IT, molecular diagnostics and combination therapies (drugs/devices) into existing payment schemas.
• Evaluate new medical technologies at CMS through the Council of Medical Technology and Innovation; adapt payment mechanisms.
• Use an episode of care as a reward technology that moves from acute to home setttings (works in Kaiser-like systems where physician payment is not linked to utilization; providers and payers are aligned)
• Include physician payments and incentives in the episode of care.
• PREEMPTIVE, PREDICTIVE, PERSONALIZED, and PARTICIPATIVE

Solution 3: Value includes Risk
• Avoid the temptation to regulate when events occur before the technology is tested thoroughly.
• Partner with industry and medicine on improved methods to accurately measure risk.
• Use FDA-critical path initiatives as model.

• Progress in the leading technology of our time has been so dramatic that it has brought about, time and again, swift qualitative changes in the material world around us, change that surely cannot be expressed simply as variations in prices or quanities”.
• Trajtenberg, Economist, 1990.
