medical final report
TRANSCRIPT
Prepared By David T. Farr and Kenneth W. McDonald, PhD
Department of Systems Engineering United States Military Academy
Robert D. Prins, PhD
Nuclear Science and Engineering Center Defense Threat ReducFon Agency
Mary O. Keith
McGill University
CENTER FOR NATION RECONSTRUCTION AND CAPACITY DEVELOPMENT
United States Military Academy West Point, New York 10996
White Paper 2015-‐2 July 2015
Medical Resources Needed to Respond to
Weapons of Mass DestrucKon in a MegaciKes Environment
Abstract A major threat to naFonal security in the twenty-‐first century is the ever-‐improving access to Weapons of Mass DestrucFon (WMD). WMDs have the ability to produce mass casualFes and long-‐term health implicaFons, denial of key and essenFal services, public panic, and property destrucFon. WMDs are generally classified by the acronym CBRNE which stands for Chemical, Biological, RadioacFve, Nuclear and High Yield Explosives. Not only have WMDs become a greater threat due to increased technology that allows them greater damage capability, but also they are much more dangerous because they are becoming accessible to a wider range of demographics. MegaciFes are an operaFonal environment that is quickly gaining importance because of populaFon migraFon, density, and their role as the centers for cultural, economic, and governmental operaFons. Such importance makes megaciFes prime targets for WMD aYacks. Adequate health service support is a leading concern for any response to a WMD event. Health Service Support following a WMD strike becomes very complicated and complex in a megacity environment and depends upon the integrated efforts of public and private enFFes. The vulnerabiliFes of the integrated and interconnected systems have not been well defined or characterized. This research was conducted to invesFgate causality and dependency of health and human services for a megacity WMD event. Research has shown this to be a major driver with regards to casualFes during a WMD event. We chose to focus on the nuclear element of a CBRNE aYach simply because it is of the most concern. The most important aspect of the medical field in a megacity environment for public officials and response agencies to focus on in response to a megacity event is public health. Urban environments are already extremely suscepFble to the spread of diseases due to the close confines that the inhabitants live in. Close confines combined with the infrastructure breakdown exponenFally increases the chances for disease spread.

The views and opinions expressed or implied in this report are solely those of the authors and should not be
construed as policy or carrying the official sancFon of the United States Army, the Department of Defense, United States Military Academy, or other agencies or departments of the US government.
Photo taken from hYps://search.usa.gov/search/images?affiliate=www.army.mil&m=false&page=2&query=medical&uc8=✓ 19 May 2015
About Us The Superintendent of the United States Military Academy (USMA) at West Point officially approved the creation of the Center for Nation Reconstruction and Capacity Development (C/NRCD) on 18 November 2010. Leadership from West Point and the Army realized that the US Army, as an agent of the nation, would continue to grapple with the burden of building partner capacity and nation reconstruction for the foreseeable future. The Department of Defense (DoD), mainly in support of the civilian agencies charged with leading these complex endeavors, will play a vital role in nation reconstruction and capacity development in both pre and post conflict environments. West Point affords the C/NRCD an interdisciplinary and systems perspective making it uniquely postured to develop training, education, and research to support this mission. The mission of the C/NRCD is to take an interdisciplinary and systems approach in facilitating and focusing research, professional practice, training, and information dissemination in the planning, execution, and assessment of efforts to construct infrastructure, networks, policies, and competencies in support of building partner capacity for communities and nations situated primarily but not solely in developing countries. The C/NRCD will have a strong focus on professional practice in support of developing current and future Army leaders through its creation of cultural immersion and research opportunities for both cadets and faculty. The research program within the C/NRCD directly addresses specific USMA needs:
• Research enriches cadet education, reinforcing the West Point Leader Development Systems through meaningful high impact practices. Cadets learn best when they are challenged and when they are interested. The introduction of current issues facing the military into their curriculum achieves both.
• Research enhances professional development opportunities for our faculty. It is important to develop and grow as a professional officer in each assignment along with our permanent faculty.
• Research maintains strong ties between the USMA and Army/DoD agencies. The USMA is a tremendous source of highly qualified analysts for the Army and DoD.
• Research provides for the integration of new technologies. As the pace of technological advances increases, the Academy's education program must not only keep pace but must also lead to ensure our graduates and junior officers are prepared for their continued service to the Army.
• Research enhances the capabilities of the Army and DoD. The client-based component of the C/NRCD research program focuses on challenging problems that these client organizations are struggling to solve with their own resources. In some cases, USMA personnel have key skills and talent that enable solutions to these problems.
For more information please contact:
Center for Nation Reconstruction and Capacity Development Attn: Dr. John Farr, Director Department of Systems Engineering Mahan Hall, Bldg. 752 West Point, NY 10996 [email protected] 845-938-5206
This Page Intentionally Left Blank

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 1
Chapter 1 Introduction
1.1 Introduction A major threat to national security in the twenty-first century is the ever-improving access to Weapons of Mass Destruction (WMD). WMDs have the ability to produce mass casualties and long-term health implications, denial of key and essential services, public panic, and property destruction. Not only have WMDs become a greater threat due to increased technology allowing them greater damage capability, but also they are much more dangerous because of their accessibility to a wider range of countries and populations. WMDs are generally classified by the acronym CBRNE (Chemical, Biological, Radioactive, Nuclear and High Yield Explosives). As shown by Figure 1, the Department of Defense has adopted a four-prong strategy to dealing with CBRNE events. The focus for this research is on the “deny” or minimize effects of this strategy. Many of the support agencies such as the Department of Health and Human Service (DHHS) has generally adopted a strategy of developing and acquiring medical countermeasures for post-event response to CBRNE threats.1
Figure 1. Department of Defense strategic approach countering WMD2 Of all the CBRNE events, nuclear weapons are often the most visible because of their destructive capabilities. Nuclear weapons—like virtually all other weapons—have changed dramatically over the past four decades.3 Understanding the weapons’ destructive abilities and their first and second order effects is essential in building secure and resilient systems. The systems need to be able to rebound in the event of an attack in order to provide the appropriate services, so that the affected area can be rebuilt and reconstructed accordingly. 1 U.S. Department of Health and Human Services, HHS Public Health Emergency Medical Countermeasure Enterprise Implementation Plan for Chemical, Biological, Radiological and Nuclear Threats, Doc., at 20 (2007). 2 United States. Department of Defense, Department of Defense Strategy for Countering Weapons of Mass Destruction, Doc., at 32
(2014). 3 The New Era of Nuclear Weapons, Deterrence, and Conflict. (2013). Strategic Studies Quarterly, 3-14.
Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 2
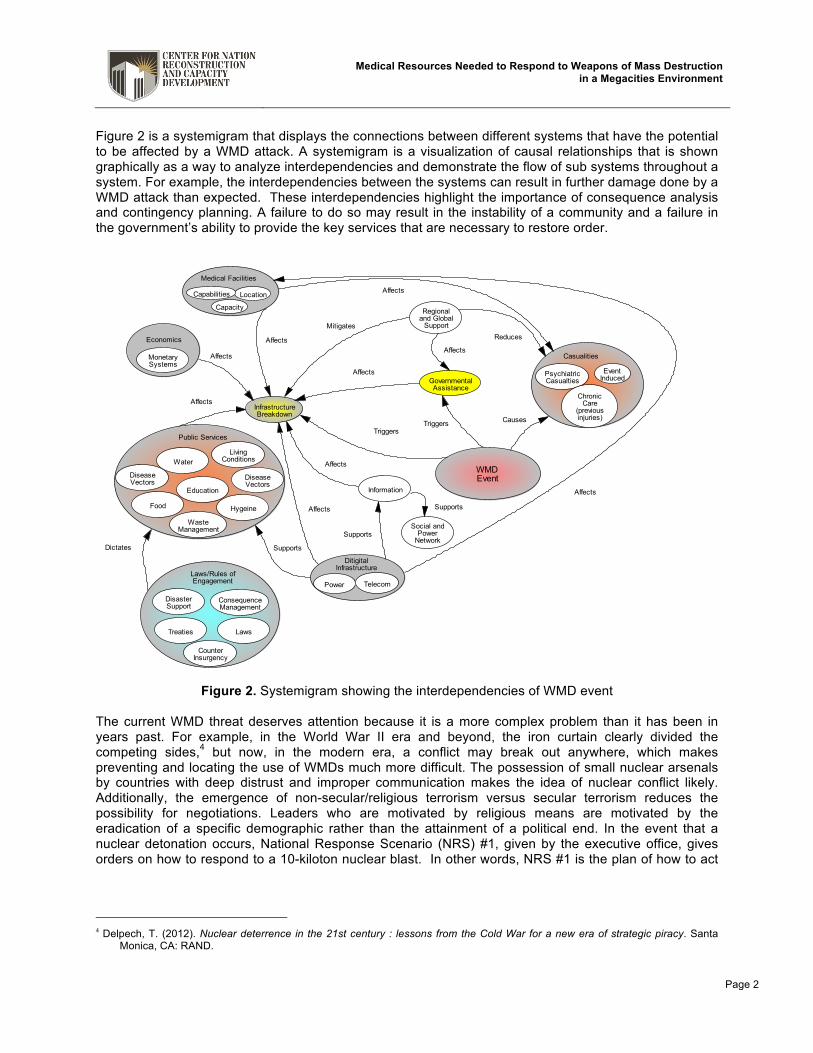
Figure 2 is a systemigram that displays the connections between different systems that have the potential to be affected by a WMD attack. A systemigram is a visualization of causal relationships that is shown graphically as a way to analyze interdependencies and demonstrate the flow of sub systems throughout a system. For example, the interdependencies between the systems can result in further damage done by a WMD attack than expected. These interdependencies highlight the importance of consequence analysis and contingency planning. A failure to do so may result in the instability of a community and a failure in the government’s ability to provide the key services that are necessary to restore order.
Figure 2. Systemigram showing the interdependencies of WMD event The current WMD threat deserves attention because it is a more complex problem than it has been in years past. For example, in the World War II era and beyond, the iron curtain clearly divided the competing sides,4 but now, in the modern era, a conflict may break out anywhere, which makes preventing and locating the use of WMDs much more difficult. The possession of small nuclear arsenals by countries with deep distrust and improper communication makes the idea of nuclear conflict likely. Additionally, the emergence of non-secular/religious terrorism versus secular terrorism reduces the possibility for negotiations. Leaders who are motivated by religious means are motivated by the eradication of a specific demographic rather than the attainment of a political end. In the event that a nuclear detonation occurs, National Response Scenario (NRS) #1, given by the executive office, gives orders on how to respond to a 10-kiloton nuclear blast. In other words, NRS #1 is the plan of how to act
4 Delpech, T. (2012). Nuclear deterrence in the 21st century : lessons from the Cold War for a new era of strategic piracy. Santa
Monica, CA: RAND.
DiseaseVectors
PsychiatricCasualties
InfrastructureBreakdown
ChronicCare
(previousinjuries)
DisasterSupport
ConsequenceManagement
CounterInsurgency
GovernmentalAssistance
Location
Capacity
Capabilities
Power Telecom
MonetarySystems
EventInduced
Regionaland Global
Support
Hygeine
LivingConditions
Food
Water
Education
WasteManagement
DiseaseVectors
Information
Social andPower
Network
Treaties Laws
WMDEvent
Medical Facilities
DitigitalInfrastructure
Economics
Casualities
Public ServicesTriggers
Triggers
Affects
Affects
Affects
ReducesMitigates
Affects
Dictates
Causes
Supports
Supports
Supports
Affects
Affects
Affects
Affects
Affects
Laws/Rules ofEngagement

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 3
in the event of an “improvised nuclear device attack.”5 This scenario gives a foundation for preparedness and strategic solutions, as well as initial response action. If a nuclear attack occurs, the effects will be tremendous, so there needs to be a source for treatment and survival, which is given by Health Service Support (HSS). HSS is defined as all services performed, provided, or arranged by the supporting personnel to promote, improve, conserve, or restore the mental and physical well being of personnel.6 HSS is an extremely important part of any area, particularly urban settings, because of their dense multitude of peoples. Urban environments are well known for their high population density, which greatly increases the odds for diseases to spread rapidly due to certain vectors, including rodents, insects, humans, air, water, food, and displaced populations. Should HSS services be disabled in an urban environment, the after effects of a nuclear attack on a population would be significantly increased. Due to the complexity and interdependencies of urban environments, particularly megacities (cities over a population of 10 million people), their problems can best be solved using systems thinking. Systems thinking is a way to problem solve and explore the interdependencies of a system in order to result in a better, more structured system. 1.2 Problem Statement Megacities are an operational environment that is quickly gaining importance because of population migration, density, and their role as the centers for cultural, economic, and governmental operations. Such importance makes megacities prime targets for CBRNE attacks. Adequate HSS is a leading concern for any response to a CBRNE event. HSS following a WMD strike becomes very complicated and complex in a megacity environment and depends upon the integrated efforts of public and private entities. The vulnerabilities of the integrated and interconnected systems have not been well defined or characterized.
5 United States. National Security Staff Interagency Policy Coordination Subcommittee for Preparedness & Response to
Radiological and Nuclear Threats, Planning Guidance for Response to a Nuclear Detonation: Second Edition, Doc., at 135 (2010).
6 Health service support. (n.d.). In The Free Dictionary. Retrieved from http://www.thefreedictionary.com/health+service+support

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 4
Chapter 2 Background
2.1 Introduction Preparing for the future operational environment today is vital to the success of the Army. Megacities are a growing trend and are presently of major importance7. All around the world, megacities are showing signs of growing economically, politically, and culturally. In fact, megacities make up about 2% of the Earth’s surface, but use up 75% of its resources.8 In this case, it can be concluded that megacities and their surrounding areas hold dense numbers of people, which are resulting in major centres for governance, high transportation rates, increased poverty, and thus, increased crime rates. The importance of megacities, the urbanization of the world’s population, and the increasing wealth gap makes understanding the future environments of megacities an essential mission for both the leaders of today and tomorrow. 2.2 Joint Operational Environment Urbanization as an operational environment will continue to be a growing trend in the future. For example, over 60%, an estimated 4.9 billion people, of the world population will be living in cities by 2030.9 One problem associated with rapid urban growth is the increase of crime resulting in population instability. This probelm has been exhibited by many cities that are growing at a fast pace economically, but still struggle with large portions of their population living in poverty. For example, in Hong Kong nearly 20% of the population lives below the poverty line, even though they have the world’s seventh largest economy.10 This enormous disparity has already fuelled protests in the Hong Kong region.11 The problem of having such a large wealth gap presents an important factor in social unrest, which can result in an increase in crime. This makes large urban environments a likely operating environment for armed forces in the future. 2.3 Megacities Every megacity has its own unique issues and challenges requiring specific and local solutions. Furthermore, they all face a common set of economic, governance, and social challenges. There are three basic “archetypes”: Emerging Cities, Transitional Cities and Mature Cities, depending on their stage of economic and social development.12 The following definitions have been developed:
• Emerging Cities: Emerging megacities tend to be characterized by high growth rates driven by migration and natural growth, much of which occurs in informal settlements not served by the installed base of infrastructure and services. Annual growth rates are on the order of between 3% and 6%. A 3.5% growth rate implies a doubling of population in 20 years. Emerging cities are typically in countries with urban populations of less than 50%. Populations tend to be younger and more male, with a high proportion of poorly educated rural migrants. Social polarity, and the gaps in wealth, health, education, and political power between groups is generally highest in Emerging Cities. Using Army terminology this would be classed as 3rd Tier/ Loosely integrated- decentralized and informal systems, poor quality infrastructure, and unregulated flow capacity (i.e., Dhaka and Lagos13).
7 Megacity Challenges: A stakeholder perspective. (2007). Munich: Siemens AG. 8 Mega Cities. (2013). European Association of National Metrology Institiutes, 1-5. 9 Command, U. J. F. (2007). Joint Operating Environment—Trends and Challenges for the Future Joint Force Through 2030. 10 Hu, F., & Yun, M. (2013, September 29). Hong Kong Poverty Line Shows Wealth Gap With One in Five Poor. Retrieved June 26,
2015, from http://www.bloomberg.com/news/articles/2013-09-29/hong-kong-poverty-line-shows-wealth-gap-with-one-in-five-poor
11 Ibid. 12 Megacity Challenges: A stakeholder perspective. (2007). Munich: Siemens AG. 13 Ibid.
Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 5
• Transitional Cities: Transitional megacities have often developed mechanisms to more effectively manage dynamic growth, and may be seeing a slowing of annual growth rates. Continued population growth stems largely from migration, with lower natural population increases; several of these cities are seeing the first signs of an ageing population. Growth rates are typically of the order of 2%-3% per annum and Transitional Cities are often in countries that are more than 50% urbanized. Transitional Cities have similar infrastructure challenges as compared with Emerging Cities but are better able to respond financially and organizationally. Increasing affluence in these cities places additional demands on infrastructure as growth in demand for items such as transportation, water, energy, and services greatly outpace the population growth. Using Army terminology this would be classed as 2nd Tier/ Moderately integrated - mix of formal and informal systems, mixed quality of infrastructure, self-regulated flow capacity (i.e., Sao Paulo, Mexico City, Rio de Janeiro14)
• Mature Cities: Mature megacities have much slower growth rates than both Emerging and Transitional megacities, at around 1% on average. In some of these cities, the population has stagnated or is shrinking. Mature megacities also have older population profiles. They exist in countries that are typically around 75% urban. Mature megacities have built out their basic infrastructure to serve their populations one or two generations ago. With high-quality infrastructure in place, the challenge has shifted in different directions: to coping with the need for renewal of ageing systems or to dealing with obsolescence where the installed infrastructure no longer meets the regulatory requirements or changing service expectations. The other growing focus of Mature Cities is responding to the increased and changing demands for services of all types posed by their ageing populations. Using Army terminology this would be classed as 1st Tier/ Highly integrated - centralized and formal system, high quality infrastructure, regulated flow capacity. (i.e., New York City, Tokyo, Paris15)
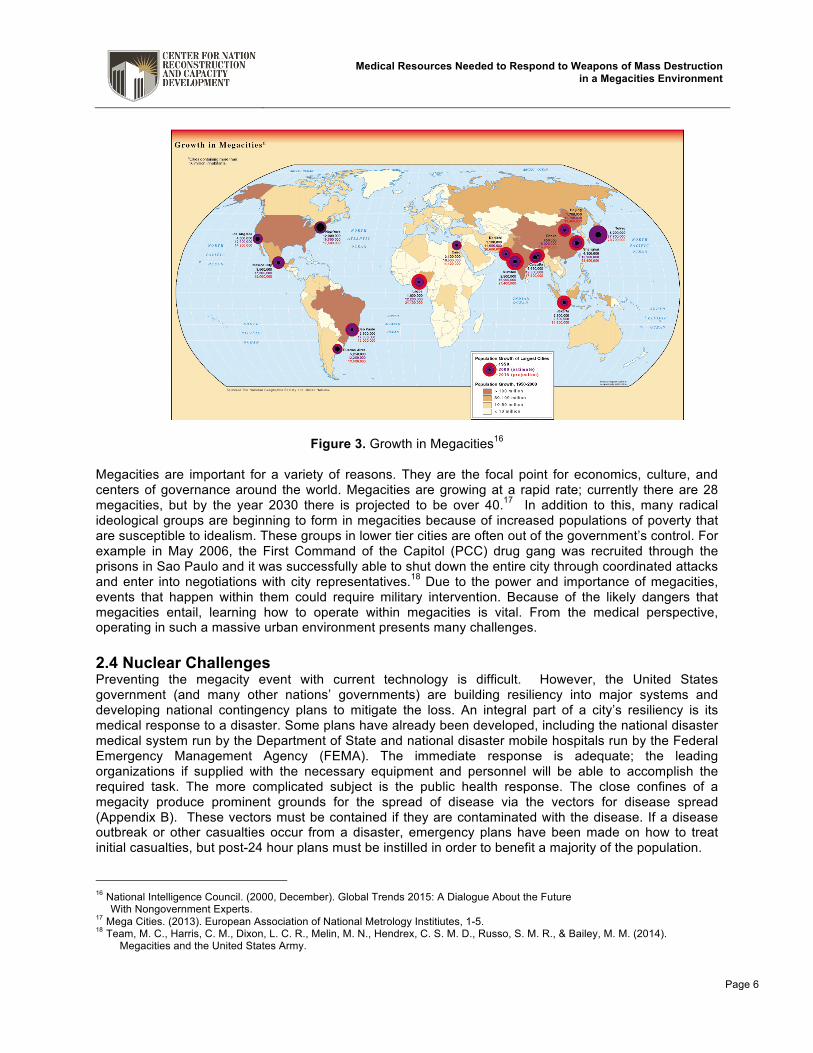
Figure 3 shows the growth of megacities from 1950 to 2015. Each circle represents a megacity. The middle black color of each circle is the population growth in 1950, the purple is the estimate of population growth in 2000, and the outside red color is the projected population growth for 2015. The magnitude of each color represents the type of growth. For example, Lagos has a small black dot and gets continuously larger with purple and then red, representing an emerging city. Sau Paulo also starts with a slow population growth in 1950, but it grows tremendously by 2000 and only slightly until 2015, representing a transitional city. Finally, New York City grows mostly in 1950 and only slightly continues to grow in 2000 and 2015, representing a mature city.
14 Ibid. 15 Ibid.
Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 6
Figure 3. Growth in Megacities16 Megacities are important for a variety of reasons. They are the focal point for economics, culture, and centers of governance around the world. Megacities are growing at a rapid rate; currently there are 28 megacities, but by the year 2030 there is projected to be over 40.17 In addition to this, many radical ideological groups are beginning to form in megacities because of increased populations of poverty that are susceptible to idealism. These groups in lower tier cities are often out of the government’s control. For example in May 2006, the First Command of the Capitol (PCC) drug gang was recruited through the prisons in Sao Paulo and it was successfully able to shut down the entire city through coordinated attacks and enter into negotiations with city representatives.18 Due to the power and importance of megacities, events that happen within them could require military intervention. Because of the likely dangers that megacities entail, learning how to operate within megacities is vital. From the medical perspective, operating in such a massive urban environment presents many challenges. 2.4 Nuclear Challenges Preventing the megacity event with current technology is difficult. However, the United States government (and many other nations’ governments) are building resiliency into major systems and developing national contingency plans to mitigate the loss. An integral part of a city’s resiliency is its medical response to a disaster. Some plans have already been developed, including the national disaster medical system run by the Department of State and national disaster mobile hospitals run by the Federal Emergency Management Agency (FEMA). The immediate response is adequate; the leading organizations if supplied with the necessary equipment and personnel will be able to accomplish the required task. The more complicated subject is the public health response. The close confines of a megacity produce prominent grounds for the spread of disease via the vectors for disease spread (Appendix B). These vectors must be contained if they are contaminated with the disease. If a disease outbreak or other casualties occur from a disaster, emergency plans have been made on how to treat initial casualties, but post-24 hour plans must be instilled in order to benefit a majority of the population.
16 National Intelligence Council. (2000, December). Global Trends 2015: A Dialogue About the Future With Nongovernment Experts. 17 Mega Cities. (2013). European Association of National Metrology Institiutes, 1-5. 18 Team, M. C., Harris, C. M., Dixon, L. C. R., Melin, M. N., Hendrex, C. S. M. D., Russo, S. M. R., & Bailey, M. M. (2014).
Megacities and the United States Army.

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 7
Figure 4 is an example of the effects of a 10-kiloton bomb on New York City. The initial blast of the bomb would create significant damage within a 10-mile radius of its detonation and the other surrounding areas would receive damaging fallout of up to 20 miles downwind.19 The first order effects of the blast would include radiation, electromagnetic pulses (EMP), nuclear heat, shockwave, and an overabundance of smoke. These effects would be carried into the fallout and depending on the type of nuclear detonation, the fallout could be potentially damaging (i.e. radiation poisoning, burning, or irritants).
Figure 4. New York City hit by a 10-kiloton nuclear bomb with a wind of 15 MPH North20 Nuclear blasts can create severe second and third order effects, which can lead to long-term effects on public health. A radiological nuclear blast will initially create a cloud of radiation. Exposure to radiation can create non-stochastic and stochastic effects. Non-stochastic pertains to effects that are expected, whereas stochastic effects are random. Radiation concluding in non-stochastic effects can result in erythema, skin blisters, and/or a reduction in the number of blood cells. Death can occur if the exposure to radiation is high enough. On the other hand stochastic effects are delayed effects that are not visible to the human eye, such as DNA impairment. These types of effects can result in cancer or hereditary changes. Exposure to nuclear heat or shockwave can result in skin penetrations and/or burn wounds. Also, people looking towards the blast could likely be blinded by the brightness. Nuclear electromagnetic pulses (NEMP) are not known to have any physical damage on a person, but psychological damage can be caused through confusion and chaos. Nuclear electromagnetic pulses damage power infrastructure and thus can have a negative effect on medical equipment. In this case, people using medical equipment for their health will experience the effects of NEMP. Focusing on these long-term effects of nuclear blasts will help communities prepare for these effects in the event of a blast.
19 Buddemeier, B.R., Valentine, J.E., Millage, K.K., & Brandt, L.D. (2011). National Capital Region Key Response Planning Factors
for the Aftermath of Nuclear Terrorism. 20 Wellerstein, A. (n.d.). Nukemap. Retrieved June 26, 2015, from http://nuclearsecrecy.com/nukemap/. (This website produced an estimated death toll of 103,000 with an estimated number of injuries of 213,400)
Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 8
Chapter 3 Systems Approach to Megacities and
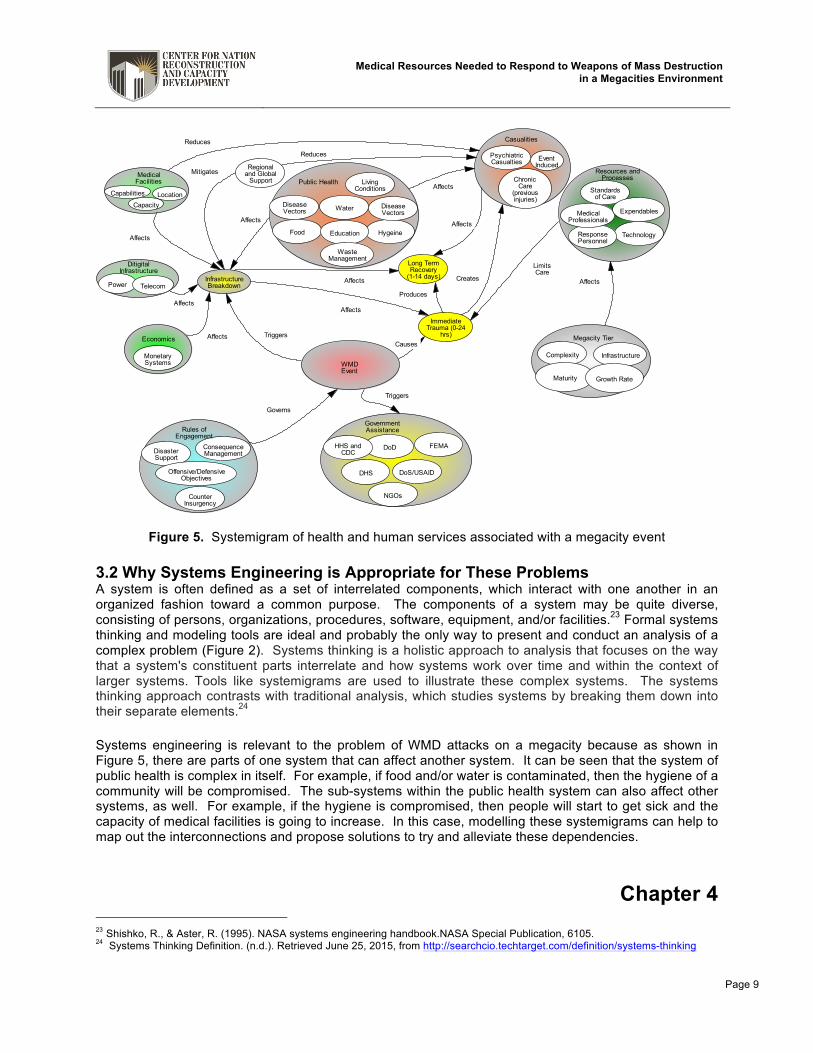
Public Health and Services 3.1 Introduction Systemigrams are a visualization of causal relationships, used to analyze interdependencies and relationships in order to create conclusions and make solutions about issues. These issues can include counterinsurgency in Afghanistan, narcotics trafficking in Mexico, complex commuter rail systems, nuclear weapons proliferation, etc. In this case, systemigrams work as powerful tools for detecting interdependencies between leading actors and their functions and consequences. Furthermore, systemigrams provide us with “a basis for systems architecting,”21 which allows us to make and understand connections throughout a single system. Therefore, systemigrams are a graphically thorough way of demonstrating the flow of sub-systems throughout a system. Figure 5 is a systemigram of health and human services surrounding a megacity event. The figure exemplifies the relationship between a megacity event and the primary effects it has on the environment, with an emphasis on health services. The primary areas of focus for our current problem are on public health (complete health of a population) and medical facilities because they have the highest influence on human health in the megacity environment.22 The systemigram portrays several relationships that public health and medical facilities have through interdependencies, both directly and indirectly. For example, the megacity event triggers some infrastructure breakdowns and consequentially, medical facilities are one area affected by infrastructure breakdown. Infrastructure breakdown can be alleviated by regional and global powers providing aid to the megacity affected. This means that the support would have a direct effect on mitigating the infrastructure breakdown, therefore directly affecting the medical facilities, and thus reducing casualties. The systemigram displays several relationships similar to the medical facilities. There is plenty of room for future research on the interdependencies of different systems in order to mitigate the after effects of a WMD attack on a megacity.
21 Boardman, J., & Sauser, B. A. (2008). Systems Thinking: Coping with 21st Century Problems. Boca Raton, FL: CRC Press. 22 Prins, R., Farr, J., McDonald, K., Fitzgerald, S., & Sanchez, D. (2015). Using Systemigrams and Fuzzy Cognitive Maps to Understand and Quantify Causality. Proceedings of the 2015 Industrial and Systems Engineering Research Conference.
Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 9
Figure 5. Systemigram of health and human services associated with a megacity event 3.2 Why Systems Engineering is Appropriate for These Problems A system is often defined as a set of interrelated components, which interact with one another in an organized fashion toward a common purpose. The components of a system may be quite diverse, consisting of persons, organizations, procedures, software, equipment, and/or facilities.23 Formal systems thinking and modeling tools are ideal and probably the only way to present and conduct an analysis of a complex problem (Figure 2). Systems thinking is a holistic approach to analysis that focuses on the way that a system's constituent parts interrelate and how systems work over time and within the context of larger systems. Tools like systemigrams are used to illustrate these complex systems. The systems thinking approach contrasts with traditional analysis, which studies systems by breaking them down into their separate elements.24 Systems engineering is relevant to the problem of WMD attacks on a megacity because as shown in Figure 5, there are parts of one system that can affect another system. It can be seen that the system of public health is complex in itself. For example, if food and/or water is contaminated, then the hygiene of a community will be compromised. The sub-systems within the public health system can also affect other systems, as well. For example, if the hygiene is compromised, then people will start to get sick and the capacity of medical facilities is going to increase. In this case, modelling these systemigrams can help to map out the interconnections and propose solutions to try and alleviate these dependencies.
Chapter 4 23 Shishko, R., & Aster, R. (1995). NASA systems engineering handbook.NASA Special Publication, 6105. 24 Systems Thinking Definition. (n.d.). Retrieved June 25, 2015, from http://searchcio.techtarget.com/definition/systems-thinking
DiseaseVectors
Node
PsychiatricCasualties
InfrastructureBreakdown
ChronicCare
(previousinjuries)
ImmediateTrauma (0-24
hrs)
DisasterSupport
Offensive/DefensiveObjectives
ConsequenceManagement
CounterInsurgency
DoS/USAID
DoD
DHS
Standardsof Care
TechnologyResponsePersonnel
MedicalProfessionals
Long TermRecovery
(1-14 days)
LocationCapacity
Capabilities
Expendables
HHS andCDC
Power Telecom
MonetarySystems
EventInducedRegional
and GlobalSupport
Complexity Infrastructure
Maturity
Hygeine
LivingConditions
Food
Water
Education
WasteManagement
DiseaseVectors
Growth Rate
FEMA
NGOs
WMDEvent
MedicalFacilities
DitigitalInfrastructure
Economics
Resources andProcesses
Casualities
Megacity Tier
Public Health
GovernmentAssistance
TriggersCauses
Produces
Affects
Affects
Affects
Affects
LimitsCare
Affects
Creates
Affects
Reduces
Mitigates
Governs
Affects
Triggers
Reduces
Affects
Affects
Rules ofEngagement

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 10
Public Health Concerns 4.1 Introduction Public health can be defined as an “ongoing system that protects people from diseases and encourages them to change harmful behaviors.”25 Should a 10-kiloton nuclear bomb detonate in a megacity, public health would be the most important area of focus for the medical field. Public health is a primary concern in several cases of disaster worldwide for a variety of reasons. The initial response to wide scale emergencies has been well practiced. The portion of the population that is going to survive because of the blast will not change significantly dependent on the chosen initial response techniques. However, the actions taken after the initial 24 hours could have a major impact on the majority of the population. The following case studies exhibit public health disasters around the world, as well as how the leading organizations handled the situation. 4.2 Case Studies Case studies are often used as analogies to the problem of interest. The following case studies are used to illustrate public health issues affect a natural or man-made disaster. Pandemic Influenza Mitigation Strategies for Pandemic Influenza in the United States Authors: Germann, Timothy C., Kadau, Kai, Longini Jr., Ira M., Macken, Catherine A. Pandemic influenza is a global outbreak of an influenza strain. The influenza spreads through communities and interactions with people. If caught early, the strain can be contained and prevented from spreading. There are two ways to contain the strain: instigate a mass vaccination and/or quarantine those affected. When vaccinating, prophylaxis are offered specific to the strain to the patients having and being exposed to the virus. If everyone exposed to the virus is offered prophylaxis, the possibility of false positives and false negatives is eliminated, and thus assuming everybody has the virus. Furthermore, if the virus can be contained, it would restrict the possibility of a case of pandemic influenza. Ways to contain the virus to stop the spreading would include closing schools, restricting community interactions, and restricting travel.26 By taking the preventative measures, the spread of disease could be contained and would not as greatly affect other systems outside of public health. Outbreak of 2009 Pandemic Influenza A (H1N1) at a New York City School Authors: Lessler, Justin, Reich, Nicholas G., Cummings, Derek A.T., New York City Department of Health and Mental Hygiene Swine Influenza Investigation Team In 2009, a pandemic influenza had an outbreak at a New York City High School. Students were having symptoms similar to those of a normal flu virus. Once students began catching the virus, the school closed for nine days in order to ensure the health of the students and to contain the virus from spreading. Those students who were quarantined in their homes for recovery exposed the virus to their families and family members went on to spread the virus further. By this outbreak and spread of influenza, public health can be compromised and be problematic for a large majority of people. It is unlikely that a strain of influenza could be detected within the first 24-hours and after that period, the strain could have potentially spread quite a bit, therefore, for total public health, measures such as containment and vaccination must be used to restrict the spreading of the disease further.27
25 What is Public Health? (2015, April 20). Retrieved June 25, 2015, from http://health.usf.edu/publichealth/definition.html 26 Germann, T. C., Kadau, K., Longini, I. M., & Macken, C. A. (2006). Mitigation Strategies for Pandemic Influenza in the United
States. Proceedings of the National Academy of Sciences of the United States of America, 103(15), 5935-5940. 27 Lessler, J., Reich, N. G., & Cummings, D. A.T. (2009). Outbreak of 2009 Pandemic Influenza A (H1N1) at a New York City
School. New England Journal of Medicine, 361(27), 2628-2636.

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 11
Fukushima Daiichi The Disaster at Japan’s Fukushima-Daiichi Nuclear Power Plant after the March 11, 2011 Earthquake and Tsunami, and the Resulting Spread of Radioisotope Contamination Author: Ohnishi, Takeo In Japan in 2011, an earthquake of intensity 9.0 (out of 10.0) followed by a 13-meter high tsunami hit the Fukushima-Daiichi Nuclear Power Plant. The nuclear power plant suffered three hydrogen explosions, each releasing radioactivity into the air. Radioisotopes were dispersed throughout areas among the power plant and evacuation areas were mapped out based on distances from the power plant and the direction of where the contamination was spreading. The Japanese government took precautions in limiting the intake of tap water and the sale of potentially contaminated foods. Some workers were exposed both lightly and severely to the radioisotopes, but no health problems were detected. To protect the heath of the public, measures were taken to reduce the possibility of another hydrogen explosion.28 These measures can further secure the public health system in the event of a disaster, such as a WMD attack. Health risk assessment from the nuclear accident after the 2011 Great East Japan Earthquake and Tsunami based on a preliminary dose estimation Author: World Health Organization The exposure to the radioisotope contamination could have had serious long-term effects on those affected. These health risks include different types of cancers, specifically leukemia, thyroid cancer, and breast cancer. In order to prevent these risks, Japan took the necessary steps to evacuate, shelter, and limit the intake of food and water from the affected area. Furthermore, to promote public health, it was suggested that those who were contaminated be screened for the possibility of a disease and if detected early, effective treatment be made available. Considering the extreme significance that this contamination had on people’s lives and social behaviors, there must have been psychological and mental health effects. Those in the population may have reactions from the trauma such as fear, anxiety, or depression. People may also acquire a feeling of helplessness and vulnerability leading to post-traumatic stress disorder (PTSD), alcoholism, or other mental health conditions. In order to focus on the complete long-term well-being of a population after a trauma, all aspects of public health must be considered. After the initial 24-hours, people must be taken care of, whether that is being treated in a hospital, getting counseling, or just being protected from contaminated areas and foods. In this case, focusing on long-term public health is essential in maintaining and protecting a community29, so that systems related to public health are not affected. The Bhopal Disaster The Bhopal Disaster Author: Tachakra, S. S. In Bhopal, the capital of Madhya Pradesh in India, there was a pesticide leak in the Union Carbide Limited factory including the chemical methyl-iso-cyanate (MIC). When the sirens warning the nearby inhabitants of the leak sounded, many people were in a state of panic and did not know how to proceed. They ran towards the chemical instead of away from it. Exposure to the chemical MIC has symptoms including burning and/or watering eyes, light intolerance, burning nasal mucosa and throat, dry cough, and nausea and vomiting.30 The longer the exposure to the chemical, the more severe the symptoms. Right away,
28 Ohnishi, T. (2012). The Disaster at Japan's Fukushima-Daichii Nuclear Power Plant after the March 11, 2011 Earthquake and
Tsunami, and the Resulting Spread of Radioisotope Contamination. Radiation Research, 177(1), 1-14. 29 World Health Organization. (2013). Health risk assessment from the nuclear accident after the 2011 Great East Japan earthquake
and tsunami, based on a preliminary dose estimation. World Health Organization. 30 Tachakra, S.S. (1987). The Bhopal Disaster. Journal of the Royal Society of Health, 107(1), 1-2.

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 12
hospitals were set up and sections were organized to accommodate for extreme casualties, common casualties, and psychological effects. With this organization, people with the same or similar symptoms could be treated collectively. The hospitals were fully staffed and volunteers came to assist. Also drugs and equipment were sent to the hospitals from other hospitals around the world, allowing them to have enough supplies for the patient treatments. In order to relieve the fear and anxiety from the people, the dead were quickly removed and people were able to stay together for communal support. After this trauma, the community was instructed on what to do in the event of an alarmed siren, signaling evacuation. The Bhopal leaders were able to focus on the complete public health of those affected by the tragedy by not only focusing on the casualties, but also on the psychological effects. The Bhopal community was able to do an admirable job in not only the initial treatment, but also in the long-term treatment by focusing on the needs of the patients and the community in order to ensure their well-being and health.31 This treatment results in aiding the public health system after a disaster and thus further stabilizes the other codependent systems. Hurricane Katrina The Federal Response to Hurricane Katrina: Lessons Learned Author: U.S. Government Hurricane Katrina was a devastating event to those who were affected by it. There were no set plans to prepare for the disaster, but improvements will be made because of the lack of preparedness. The outcome of Hurricane Katrina consisted in demolished or damaged homes, piles of debris, a higher unemployment rate and rising gas prices, damaged power infrastructure, and multiple oil spills. The community’s public health was at risk due to the piling of water, oil, sewage, chemicals, and corpses. Furthermore, the medical support needed for the survivors was lacking and unorganized. For future preparation, public health for the people could be improved by having specific plans to give immediate medical attention to the survivors in order to assess their well-being and to judge if they need further care. One way to perform this is to set up Joint Force Offices (JFO) supplied with the necessary resources and equipment (i.e. food, water, shelter, power, medicine, etc.), so that in the event of a disaster, people will have access to necessities. As demonstrated during Hurricane Katrina, one voice (see DoD, 2014) is needed to ensure command and control, to interact with the press, etc. In addition to the medical attention, total public health includes psychological attention. Survivors are going to need programs for counseling and support. A system should be developed in order to deliver these services immediately to those affected by the disaster in order to reduce the reactions of grievances and depression. Incident management teams (IMT) can be stationed at JFOs and be on command and ready to deploy into the community with care packages and assist the people to ensure complete public health. While the United States government did not have a long-term plan, the procedures that it made in the event of another disaster are good protective and considerate strategies to guarantee the long-term health of the population affected.32 By focusing on these strategies in managing public health, the systems that are codependent with public health will be stabilized. 4.3 Conclusion As seen through the previous case studies, public health problems can be caused by nuclear, chemical, and natural disasters. In order to prepare for these disasters, there must be an understanding of the possible long-term effects on public health. Then, a plan can be created and implemented so that in the event of a disaster, the affected people can be treated effectively. This will ensure that the public health of a population will be a primary concern after a disaster and that the treatment and attention given to the patients will be satisfactory. In this case, in the previously discussed case studies, only the disaster at Fukushima Daiichi had a productive plan implemented. The others, including Pandemic Influenza A
31 Ibid. 32 United States, Executive Office of the President, The Federal Response to Hurricane Katrina: Lessons Learned, Doc., at 228
(2006).

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 13
(H1N1), the Bhopal Disaster, and Hurricane Katrina had to learn from their mistakes and prepare accordingly. Now, in the event of a new pandemic influenza, the people affected will be quarantined to contain the virus and a maximum number of people will be vaccinated to prevent the spread of the disease. With the Bhopal Disaster, people have an evacuation plan in place that will be followed if another chemical leak occurs. Finally, the United States Government recognized their mistakes with Hurricane Katrina and has created strategies and procedures when the next disaster strikes, including places of shelter and officials aiding the communities affected. These strategies focus on the long-term well being and complete public health of societies that have encountered and will encounter disasters.

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 14
Chapter 5
Conclusions This research was conducted to investigate causality and dependency of health and human services for a megacity WMD event. Other research has shown that this subject of casualties during a WMD event is an important aspect of recovery when considering CBRNE attacks.33 Our research focuses on the nuclear element of a CBRNE attack because it is of the most concern and probably the most likely at the moment. In order to map out the pathways that lead from a WMD attack to a total infrastructure breakdown, systemigrams are used as visual aids. Throughout this research, the pathway being focused on was public health and how it could be maintained in a megacity if t a nuclear attack occurs. To recap, when examining the medical field in a megacity environment, it is important to focus on public health in the event of a megacity disaster. The populations of megacities are so dense that a nuclear detonation could cause tremendous damage to these communities, both physically and psychologically. Likewise, urban environments are already extremely susceptible to the spread of diseases due to the close confines of the inhabitants, but these close boundaries combined with an infrastructure breakdown could exponentially increase the chances for diseases to spread. This rapid spread of disease then has the potential to create a web of problems, indicated by the systemigrams, that if not treated effectively, could lead to a total infrastructure breakdown. The research presented here defines a solid problem statement and an initial effort to understand the complexities and dependencies of health and human services on casualties for a megacity environment. The problem of public health maintenance in the event of a WMD attack is tremendously complex and requires further research at the individual service levels and their interactions. Our research simply examined this problem from a qualitative perspective, but future research is needed to quantify the effects of resources, planning, etc., for health and human services. Additionally, detailed research is needed to understand how elements of health and human services interact. For example, as seen in Figure 5, water is able to affect all of the elements of public health, which can create long-term causalities. In other words, public health needs to be defined as a primary concern and afterwards, solutions need to be determined to focus on public health and ensure complete public health after a disaster in a megacity.
33 Prins, R., Farr, J., McDonald, K., Fitzgerald, S., & Sanchez, D. (2015). Using Systemigrams and Fuzzy Cognitive Maps to
Understand and Quantify Causality. Proceedings of the 2015 Industrial and Systems Engineering Research Conference.
Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 15
Chapter 6 References
References Boardman, J., & Sauser, B. A. (2008). Systems Thinking: Coping with 21st Century Problems. Boca Raton, FL: CRC Press. Buddemeier, B.R., Valentine, J.E., Millage, K.K., & Brandt, L.D. (2011). National Capital Region Key Response Planning Factors for the Aftermath of Nuclear Terrorism. Clements, B. (2009). Disasters and Public Health: Planning and Response. Butterworth-Heinemann. Command, U. J. F. (2007). Joint Operating Environment—Trends and Challenges for the Future Joint
Force Through 2030. Delpech, T. (2012). Nuclear deterrence in the 21st century : lessons from the Cold War for a new era of strategic piracy. Santa Monica, CA: RAND. Germann, T. C., Kadau, K., Longini, I. M., & Macken, C. A. (2006). Mitigation Strategies for Pandemic
Influenza in the United States. Proceedings of the National Academy of Sciences of the United States of America, 103(15), 5935-5940.
Headquarters, Department of the Army, Planning for Health Service Support, Doc., at 415 (1994). Health service support. (n.d.). In The Free Dictionary. Retrieved from
http://www.thefreedictionary.com/health+service+support Hu, F., & Yun, M. (2013, September 29). Hong Kong Poverty Line Shows Wealth Gap With One in Five Poor. Retrieved June 26, 2015, from http://www.bloomberg.com/news/articles/2013-09-29/hong-kong-
poverty-line-shows-wealth-gap-with-one-in-five-poor Joint Chiefs of Staff, Countering Weapons of Mass Destruction, Doc., at 117 (2014). Kimsey, L. G. (2009). How Efficient are Military Hospitals? A Comparison of Technical Efficiency Using
Stochastic Frontier Analysis. University of Kentucky Doctoral Dissertations, 1-153. Lessler, J., Reich, N. G., & Cummings, D. A.T. (2009). Outbreak of 2009 Pandemic Influenza A (H1N1) at
a New York City School. New England Journal of Medicine, 361(27), 2628-2636. Lindell, B. (1987). Radiation and Health. Bulletin of the World Health Organization, 65(2), 139-148. Mega Cities. (2013). European Association of National Metrology Institiutes, 1-5. Megacity Challenges: A stakeholder perspective. (2007). Munich: Siemens AG. National Intelligence Council. (2000, December). Global Trends 2015: A Dialogue About the Future With Nongovernment Experts. Ohnishi, T. (2012). The Disaster at Japan's Fukushima-Daichii Nuclear Power Plant after the March 11,
2011 Earthquake and Tsunami, and the Resulting Spread of Radioisotope Contamination. Radiation Research, 177(1), 1-14.
Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 16
Prins, R., Farr, J., McDonald, K., Fitzgerald, S., & Sanchez, D. (2015). Using Systemigrams and Fuzzy Cognitive Maps to Understand and Quantify Causality. Proceedings of the 2015 Industrial and Systems Engineering Research Conference. Shishko, R., & Aster, R. (1995). NASA systems engineering handbook.NASA Special Publication, 6105. Systems Thinking Definition. (n.d.). Retrieved June 25, 2015, from
http://searchcio.techtarget.com/definition/systems-thinking Tachakra, S.S. (1987). The Bhopal Disaster. Journal of the Royal Society of Health, 107(1), 1-2. Team, M. C., Harris, C. M., Dixon, L. C. R., Melin, M. N., Hendrex, C. S. M. D., Russo, S. M. R., & Bailey,
M. M. (2014). Megacities and the United States Army. The New Era of Nuclear Weapons, Deterrence, and Conflict. (2013). Strategic Studies Quarterly, 3-14. U.S. Department of Health and Human Services, HHS Public Health Emergency Medical
Countermeasure Enterprise Implementation Plan for Chemical, Biological, Radiological and Nuclear Threats, Doc., at 20 (2007).
United States. Department of Defense, Department of Defense Strategy for Countering Weapons of Mass
Destruction, Doc., at 32 (2014). United States, Executive Office of the President, The Federal Response to Hurricane Katrina: Lessons
Learned, Doc., at 228 (2006). United States. National Security Staff Interagency Policy Coordination Subcommittee for Preparedness &
Response to Radiological and Nuclear Threats, Planning Guidance for Response to a Nuclear Detonation: Second Edition, Doc., at 135 (2010).
Wellerstein, A. (n.d.). Nukemap. Retrieved June 26, 2015, from http://nuclearsecrecy.com/nukemap/ What is Public Health? (2015, April 20). Retrieved June 25, 2015, from
http://health.usf.edu/publichealth/definition.html World Health Organization. (2013). Health risk assessment from the nuclear accident after the 2011
Great East Japan earthquake and tsunami, based on a preliminary dose estimation. World Health Organization.

Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 17
Appendix A Acronyms and Annotated Bibliography
A.1 Acronyms
Acronym Definition ARS Acute Radiation Syndrome CA Consequence Analysis CDC Center for Disease Control CM Consequence Management CBRNE Chemical, Biological, Radioactive, Nuclear and High Yield Explosives CEO/CFO/CIO Chief Executive Office/Chief Financial Officer/Chief Information Officer CONUS Continental United States DHHS Department of Health and Human Services DHS Department of Homeland Security DoD Department of Defense DoS Department of State EPA United States Environmental Protection Agency EURAMET European Association of National Metrology Institutes FCM Fuzzy Cognitive Mapping FEMA Federal Emergency Management Agency HSS Health Service Support IMT Incident Management Teams JFO Joint Force Offices MIC methyl-iso-cyanate MPH Miles Per Hour NEMP Nuclear electromagnetic pulses NGO Non Governmental Organization PTSD post-traumatic stress disorder RERT Radiological Emergency Response Team USAID US Agency for International Development WMD Weapons of Mass Destruction
Medical Resources Needed to Respond to Weapons of Mass Destruction
in a Megacities Environment
Page 18
Appendix B Health Service Support
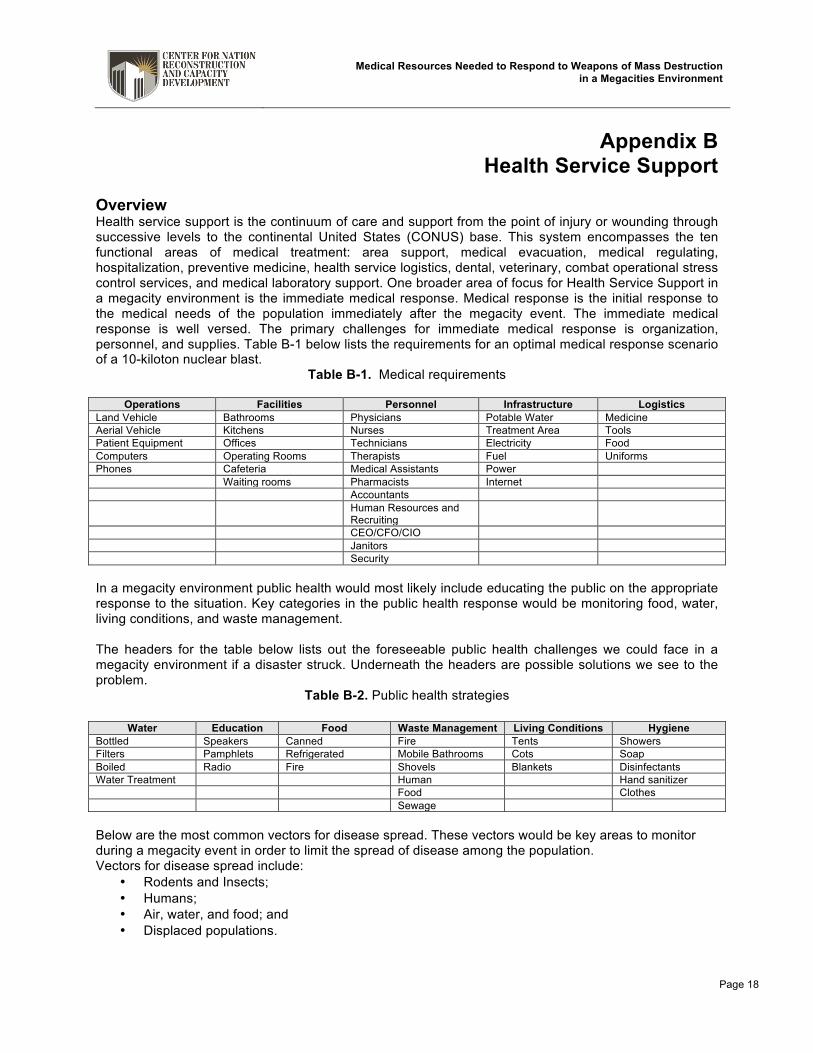
Overview Health service support is the continuum of care and support from the point of injury or wounding through successive levels to the continental United States (CONUS) base. This system encompasses the ten functional areas of medical treatment: area support, medical evacuation, medical regulating, hospitalization, preventive medicine, health service logistics, dental, veterinary, combat operational stress control services, and medical laboratory support. One broader area of focus for Health Service Support in a megacity environment is the immediate medical response. Medical response is the initial response to the medical needs of the population immediately after the megacity event. The immediate medical response is well versed. The primary challenges for immediate medical response is organization, personnel, and supplies. Table B-1 below lists the requirements for an optimal medical response scenario of a 10-kiloton nuclear blast.
Table B-1. Medical requirements
Operations Facilities Personnel Infrastructure Logistics Land Vehicle Bathrooms Physicians Potable Water Medicine Aerial Vehicle Kitchens Nurses Treatment Area Tools Patient Equipment Offices Technicians Electricity Food Computers Operating Rooms Therapists Fuel Uniforms Phones Cafeteria Medical Assistants Power Waiting rooms Pharmacists Internet Accountants Human Resources and
Recruiting
CEO/CFO/CIO Janitors Security In a megacity environment public health would most likely include educating the public on the appropriate response to the situation. Key categories in the public health response would be monitoring food, water, living conditions, and waste management. The headers for the table below lists out the foreseeable public health challenges we could face in a megacity environment if a disaster struck. Underneath the headers are possible solutions we see to the problem.
Table B-2. Public health strategies
Water Education Food Waste Management Living Conditions Hygiene Bottled Speakers Canned Fire Tents Showers Filters Pamphlets Refrigerated Mobile Bathrooms Cots Soap Boiled Radio Fire Shovels Blankets Disinfectants Water Treatment Human Hand sanitizer Food Clothes Sewage Below are the most common vectors for disease spread. These vectors would be key areas to monitor during a megacity event in order to limit the spread of disease among the population. Vectors for disease spread include:
• Rodents and Insects; • Humans; • Air, water, and food; and • Displaced populations.


Department of Systems Engineering United States Military Academy West Point, New York 10096 www.nrcd.usma.edu