medical informatics and population-based medicine: an introduction to the clinical data repository...
Post on 21-Dec-2015
213 views
TRANSCRIPT

Medical Informatics andPopulation-Based Medicine:
An Introduction to the Clinical Data Repository
Jason Lyman, MD, MS
Department of Health Evaluation Sciences
University of Virginia School of MedicineJanuary 14, 2003

“The U.S. health care system is in need of fundamental change. Americans ought to be able to count on receiving care that is safe and uses the best scientific knowledge. But there is strong evidence that this is not the case. Health care today harms too frequently, and fails to deliver its potential benefits routinely. As medical science and technology have advanced at a rapid pace, the health care delivery system has foundered. Between the care we have and the care we could have lies not just a gap, but a wide chasm.”
Crossing the Quality Chasm: A New Health System for the 21st Century Institute Of Medicine, National Academy of Sciences, 2001

Six Aims for Improvement
Health care needs to be:• Safe
• Effective
• Patient-centered
• Timely
• Efficient
• Equitable
Applying evidence to healthcare delivery
Using information technology
Aligning financial incentiveswith quality improvement
Preparing the workforce

Are we really that far off?
Aren’t our patients safe?
Don’t we deliver effective care?
Don’t we do so equitably?

Health Care Should Be Safe, …
44,000 – 98,000 people die each year from preventable medical errors (defined as the failure of a planned action to be completed as intended, or the use of the wrong plan to achieve an aim)
Costs of errors approximated at $17 billion to $29 billion per year in hospitals nationwide
To Err Is Human: Building a Safer Health SystemInstitute Of Medicine, National Academy of Sciences, 2000
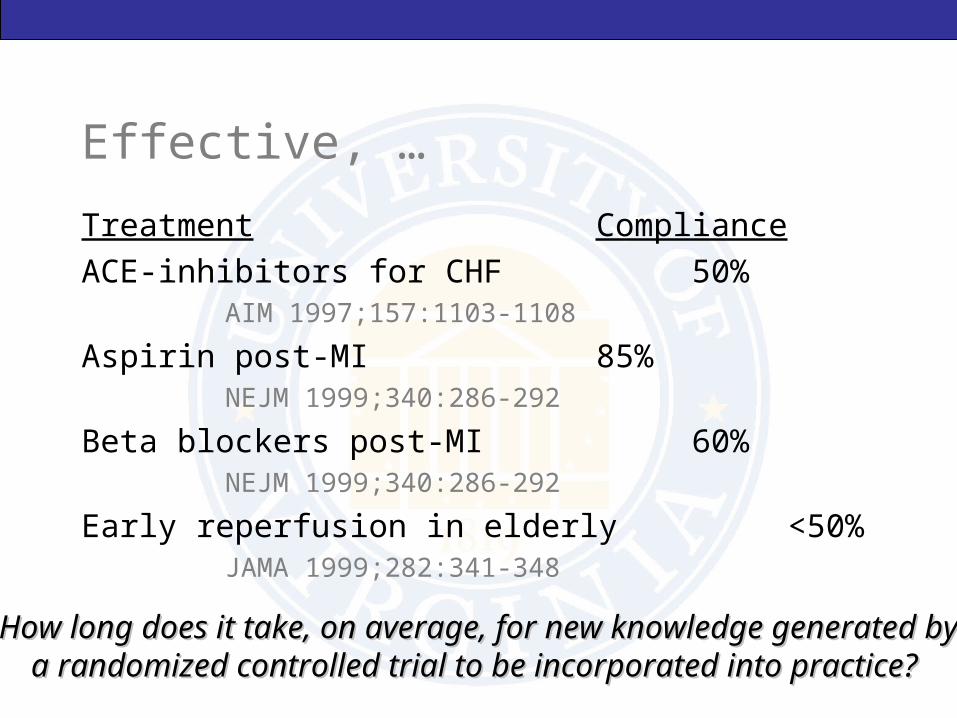
Effective, …
Treatment Compliance
ACE-inhibitors for CHF 50%AIM 1997;157:1103-1108
Aspirin post-MI 85%NEJM 1999;340:286-292
Beta blockers post-MI 60%NEJM 1999;340:286-292
Early reperfusion in elderly <50%JAMA 1999;282:341-348
How long does it take, on average, for new knowledge generated byHow long does it take, on average, for new knowledge generated bya randomized controlled trial to be incorporated into practice? a randomized controlled trial to be incorporated into practice?

And EquitableMortality
• The rate of suicide in American Indian males is twice as high as young white males
Morbidity
• Incidence rates for specific types of cancer (e.g. prostrate) are as much as 60% in African-American males as white males
Health behaviors
• Smoking in adolescents vary widely by geography – 19% in rural counties vs. 11% in non-rural counties
Preventive medicine
• Women below the poverty line are 27% less likely to undergo screening mammography than their counterparts above the poverty line
Access to care
• 28% of children from families at 1-1.5x the poverty level are uninsured vs. 5% in families at 2x or above.
Roadmaps for Clinical Practice: Primer on Population-Based MedicinePeters & Elster, AMA, January 2002

So…
What factors affect health disparity?
Why is compliance with proven therapies suboptimal?
Why do have so many errors?
What can be done about it?

One Approach: A Population-Based Perspective
Can be helpful for addressing health disparities
Can be useful for evaluating the quality of health care, including the:• processes of care (e.g. efficiency, evidence-based care)
• and outcomes (e.g. morbidity, mortality, complications)
Complements traditional individual-oriented care
Can be incorporated into clinical practice

Today’s Agenda
What is Population-Based Medicine (PBM)?
The role of PBM
Medical Informatics and PBM
The Clinical Data Repository (CDR)• Introduction
• Demo
The CDR as a PBM resource for the POM course

The Continuum of Clinical Care
“It is the duty of the physician to promote and safeguard the
health of the people.”
World Medical Association Declaration of Helsinki, 1964
“ The health of my patient will be my first consideration.”
Declaration of Geneva of the World Medical Association, 1948

What is Population-Based Medicine (PBM)?
“…medicine that addresses the health care of whole populations rather than that of individual patients. It represents a community-based strategy for disease management and health promotion and places each individual patient within the context of the larger community made up of both sick and healthy people.”
Robert Wood Johnson Foundation

PBM In Practice
Identifying health disparity in your own practice / population of patients
Improving chronic disease management for specific conditions (e.g. asthma, diabetes, heart failure)
Identifying at-risk populations in your own practice
Using Healthy People 2010
Implementing practice guidelines (e.g. treatment of acute myocardial infarction)
Integrating preventive service recommendations (e.g. screening, counseling, immunization)

Sample PBM Resources
Healthy People 2010 (http://www.healthypeople.gov/)Healthy Virginians 2010 (http://www.vdh.state.va.us/hv2010/index.html)CDC National Center for Health Statistics (http://www.cdc.gov/nchs/)Agency for Healthcare Research and Quality (http://www.ahrq.gov/)National Guidelines Clearinghouse (http://www.guidelines.gov)Guide to Clinical Preventive Services (USPSTF) (http://www.ahrq.gov/clinic/prevnew.htm)

A Population-Based Approach
Identify and characterize a population of patients• E.g. all the patients of a specific provider, clinic, or healthcare
institution
Identify the health care problems of highest priority• By prevalence, outcome, utilization, etc.
Adapt office procedures to maximize delivery of appropriate services• What is the problem, and how best can it be addressed?
Assess impact and provide feedback

PBM-Related Information Needs
What kind of information do you need to implement these efforts?
Where does the data come from?
Is the data valid?
How is the data recorded and stored?
How is the information provided in a timely fashion?

Medical Informatics
“..the scientific field that deals with the storage, retrieval, sharing, and optimal use of biomedical information, data, and knowledge for problem solving and decision making.”
Shortliffe, 2001

Medicine is Data-Intensive…
Clinical medicine• History, physical exam
• Laboratory tests
• Imaging modalities
• Monitoring data (OR, ICU)
Population health
Health services research• Clinical trials
• Outcomes research
Size of the biomedical literature databases• MEDLINE contains approx. 11 million citations, with 400,000 new
references added each year
…But the Practice of Medicine Can Be Information-Poor
When did this patient last have a colonoscopy?
What is the prognosis for my patient with end stage renal failure?
Did the female I sent for a rheumatology referral manage to get an appointment? Did she go? What happened?
What did this man’s prostate biopsy show?
Where is the *$#@! chart?!

What is Medical Informatics?
Electronic Medical Records (EMR)
Physician Order Entry (POE)
Information Retrieval (IR)
Computerized Decision Support Systems (DSS)
Medical Terminology
Medicine and the Internet
Handheld Computers in Clinical Practice
Multimedia Medical Education
Privacy and Security

A National Perspective on Informatics
“Information technology, including the Internet, holds enormous potential for transforming the health care delivery system, which today remains relatively untouched by the revolution that has swept nearly every other aspect of society.…. the committee calls for a nationwide commitment of all stakeholders to building an information infrastructure to support health care delivery, consumer health, quality measurement and improvement, public accountability, clinical and health services research, and clinical education. This commitment should lead to the elimination of most handwritten clinical data by the end of the decade.” (emphasis added)
Crossing the Quality Chasm: A New Health System for the 21st Century Institute Of Medicine, National Academy of Sciences, 2001

Informatics and PBM
Where do we find all the data we need to incorporate a population-based medicine approach?The holy grail of medical informatics is the development and widespread adoption of comprehensive electronic medical records that collect detailed, longitudinal data about patient encounters• CC, HPI, PMH, FH, SH, Allergies, Meds, Immunizations• Diagnoses (admitting, working, discharge)• Procedures (therapeutic and diagnostic)• Labs, Radiology• Images / text / waveform / numeric• Providers

Electronic Medical Record: The Holy Grail
Discharge Summary
Admission Note
Computer-ReadableCoded Data
Automatic, co
mprehensiv
e
accurate an
d reliab
le
Assist ordering
Error prevention
Facilitate access to knowledge
Research
PBM
The potential!
Reality
Chief complaintHistory and
Physical Daily ProgressNotes
VitalsOrders
Nursing NotesOperative Notes
Dietary Notes DischargeSummariesLaboratory
Results

So, In the Meantime…
Clinicians must find ways to use existing electronic data (demographics, financial, limited coded diagnoses and procedures, labs) • E.g. Dr. Joel Shectman, Internal Medicine – compiling laboratory
and visit data to evaluate the care of diabetic patients at Uva and provide feedback to residents
OR
Implement processes to capture additional data• E.g. Dr. Scott Strayer, Family Medicine – capture of tobacco use
data on handheld computers
• Creation of specialized office information systems*
*A Primer on Population-Based Medicine, AMA, 2002

Information Retrieval: Accessing Population Data
State / regional / national data available for some conditions (CDC, AHRQ)
In most academic and community health care institutions, aggregate patient data is unavailable to health care providers and researchers

Pasteur describes work on germ theory
Hippocrates born
First textbook of anatomypublished by Vesalius
A Brief History of Medicine
460 BC
1543 AD
?
1864
1995




The UVa Clinical Data Repository is Born

What is the CDR?
The UVa Clinical Data Repository (CDR) is a unique local resource for integrating clinical data from Uva patients into a single WWW-based database.• Laboratory data
• Billing data
• Registration data
• Virginia Department of Health (VDH)

Purpose of the CDR
Originally developed as a tool for clinical researchers
Enable flexible and rapid retrospective queries of patient data• “Show me all patients admitted with pneumonia in 1999”
Supply data sets for research and medical management applications
Provide insights into opportunities for improving outcomes and containing costs• What therapies tend be associated with better patient outcomes?

Data Contents
Coded diagnoses and procedures for each inpatient or outpatient visitLaboratory resultsMedications (inpatient visits only)DemographicsUtilization and financial dataMortality data
What’s missing?• Symptoms• Exam findings• Outpatient pharmacy• Microbiology (culture results)• ….

Security and Confidentiality
Disguised Patient and MD Identifiers
Authorization Required for Access
All Uses are Tracked and Audited
2nd Level Authorization Required to obtain real identifiers

The Query Process
1. Define a population
2. Submit your query to the database
3. Display standard reports or download data

Define a Population
By diagnosis• Patient visits for which ACUTE MI was diagnosed
By procedure• Patient visits in which SCREENING MAMMOGRAPHY was
performed
• Patients who received a BLOOD TRANSFUSION
By age, race, gender
By date
By unit

Define a Population
By medication• Patients who received ASPIRIN
By lab test• Patients who had a HCT < 25%
By physician, clinic, age, sex, date range, insurance type, ...

Standard Reports – Summary
How many patients / visits were there that met your criteria?
Demographics
Comorbidities (the presence of other diseases in this patient population)
Diagnoses / procedures that were coded during these visits
Lab results
Mortality
…
Diagnoses and Procedures in the CDR
For every hospitalization, clinic visit, ER visit, etc., the diagnoses assigned and procedures performed must be recorded for the clinic/provider/hospital to be reimbursed!In clinic – done by providers (you’ll get to know this all too well…)In the hospital, trained coders carefully review the chart and make a list of diagnoses assigned.Every visit has one PRINCIPAL diagnosis, but potentially many more SECONDARY diagnoses.
• A patient might be admitted for an asthma exacerbation, but then develop pneumonia, develop a drug allergy, etc.
• Her principal diagnosis would be asthma, and secondary diagnoses would include pneumonia, allergic reaction, etc.
Diagnoses are represented using a system of codes called ICD9.Procedures are represented using CPT (outpatient) and ICD9 (inpatient).

Diagnoses and Procedures
To specify the diagnosis and/or procedures you want to use as conditions, you must identify the ICD-9/CPT codes that match the concepts you’re interested in.
The CDR allows you to search for specific codes or browse through a hierarchical classification (CCHPR).
See CDR FAQ (in the Documentation link of the menu)
More on this later…..

CDR Demonstration
Goals/objectives of Healthy Virginians 2002 include:• Eliminating health disparities• Reducing the hospitalization rate for pediatric asthma (among
other conditions)• Reducing emergency department visits for asthma
Before we can make progress, we need to know where we stand!Let’s take a closer look at pediatric asthma at UVa….• What disparities exist?• How often are kids hospitalized with asthma?• How often do they go to the ED for this condition?

Asthma Prevalence by Race, GenderCount of Ptid RaceHx_of_RAD A B H I O W (blank) Grand TotalN 96.92% 86.76% 94.44% 100.00% 96.37% 93.37% 100.00% 92.03%Y 3.08% 13.24% 5.56% 0.00% 3.63% 6.63% 0.00% 7.97%Grand Total 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Count of Ptid SexHx_of_RAD F M Grand TotalN 93.75% 90.48% 92.03%Y 6.25% 9.52% 7.97%Grand Total 100.00% 100.00% 100.00%

Insurance, Utilization, and Asthma
Percentage with a history of
asthma
Average Number of ER Visits (over
a five-year period)
Self-Pay 9.19 1.51
Medicaid 9.35 1.23
Other 6.55 .57

ED Visits for Asthma In those patients with a history of RAD, what percentage have had the
following number of ER visits for RAD:
None 1-3 4-6 7 or more
Self-Pay 69.75 28.71 0.96 0.58
Medicaid 75.40 22.24 1.60 0.75
Other 83.11 14.57 1.77 0.54

Our Goals for PBM / CDR in POM
Introduce you to the principles and promise of population-based medicine
Provide you with access to aggregate data to explore these principles first hand
Teach you how to use the CDR

CDR and POM
Three PBM exercises throughout the course of the semester• Two students per group will complete a given exercise in a special
session held in the library classroom (Carter). Each student will attend one of these sessions.
The exercises will focus on specific PBM objectives as described in this lecture, for example• What heath disparities exist in UVa patients?• How can our data be used to measure quality of care?• How are our patients with chronic illness being managed and how
might we improve?• How well are preventive services being administered?
How else might you use the CDR?
A helpful tool for comparing information in textbooks with real patient data (disease prevalence and practice patterns can vary widely) – e.g. how do physicians here treat meningitisComing into a new rotation:• what kinds of patients will I see? • What kinds of conditions?
Learning about patients with complex chronic illnesses• What diseases / complications is my patient with chronic renal
failure at risk for?
Potential source of data for a research project

Need Help?
On-line code tables and documentation
Available CDR project team-members• Jason Lyman, MD, MS, CDR Director
([email protected], 924-8240)
• Ken Scully, MS, Developer and Database Administrator
([email protected], 982-4035)

Next Steps
We will let you know the dates that the PBM sessions are scheduled
Stay tuned…
Please fill out the CDR Access Request Form (top half only) and return to me or Robin Stevens