medical management of ulcerative colitis€¦ · medical management of ulcerative colitis gerhard...
TRANSCRIPT

University HospitalZurich
U
Medical management of ulcerative colitis
Gerhard Rogler, Zürich

18.05.2009 / 2
University HospitalZurich
UStep up approach to therapy of Ulcerative colitisStep up approach to therapy of Ulcerative colitis
SurgerySurgeryCyclosporineCyclosporineTacrolimusTacrolimusInfliximabInfliximab
AZA/6AZA/6--MP MP Corticosteroids Corticosteroids
(topical/systemic)(topical/systemic)
AminosalicylatesAminosalicylates(topical/systemic)(topical/systemic)
Seve
re
Mod
erat
e
Mild

18.05.2009 / 3
University HospitalZurich
U
SASP 5-ASA top. SASP/ASAPrednisolone
Steroid Enema0
20
40
60
80
100% Success
Drug
Placebo
TA
39%TA
41%
TA
56%TA
56%TA
41%
MetaMeta--analysis of drug analysis of drug treatment treatment
of ulcerative colitisof ulcerative colitis
Kornbluth, 1993

18.05.2009 / 4
University HospitalZurich
UCase 1: Musician with proctosigmoiditis
Started 5-ASA enemas with initial successSwitched to oral 5-ASA 2.4 g for flareSteroids 40 mg/day for subsequent flares still has 8 BM/day, malaise without fever. Works but wants to feel good.
What next ???

18.05.2009 / 5
University HospitalZurich
U
Treatment Success at Weeks 3 & 6Pooled Moderate Population
58%53%
72%62%
0%10%20%30%40%50%60%70%80%
Week 3 Week 6
% o
f Pat
ient
s Im
prov
ed
2.4 g/day4.8 g/day
5-ASA: More is Better
p=0.0034p=0.058
N=223 N=223N=198 N=200
*
ASCEND I, II
Hanauer et al. Am J Gastroenterol 2005

18.05.2009 / 6
University HospitalZurich
UDose finding for 5-ASA in active ulcerative colitis
Kruis et al., Clin Gastroenterol Hepatol 2003
8 weeks 3 x 0.5 g 3 x 1.0 g 3 x 1.5 g(n = 104) (n = 104) (n = 104)
Remission (CAI < 4) 50 66 * 55
Time to response 27.5 26.5 21.6(days, mean)
Endoscopic remission (%) 28 48 * 49
Histological improvement (%) 42 56 * 63
Stop due to side effects (n) 11 7 9

18.05.2009 / 7
University HospitalZurich
U
5-ASA topical therapyis preferable
% R
emis
sion
% R
emis
sion
MonthsMonths
D’Albasio. Am J Gastroenterol 1997
4 g QOD enema4 g QOD enema
1.6 g/day oral1.6 g/day oral
00
2020
4040
6060
8080
100100
120120
22 44 66 88 1010 1212 1414 1616 1818 2020 2222 2424
18.05.2009 / 8
University HospitalZurich
U
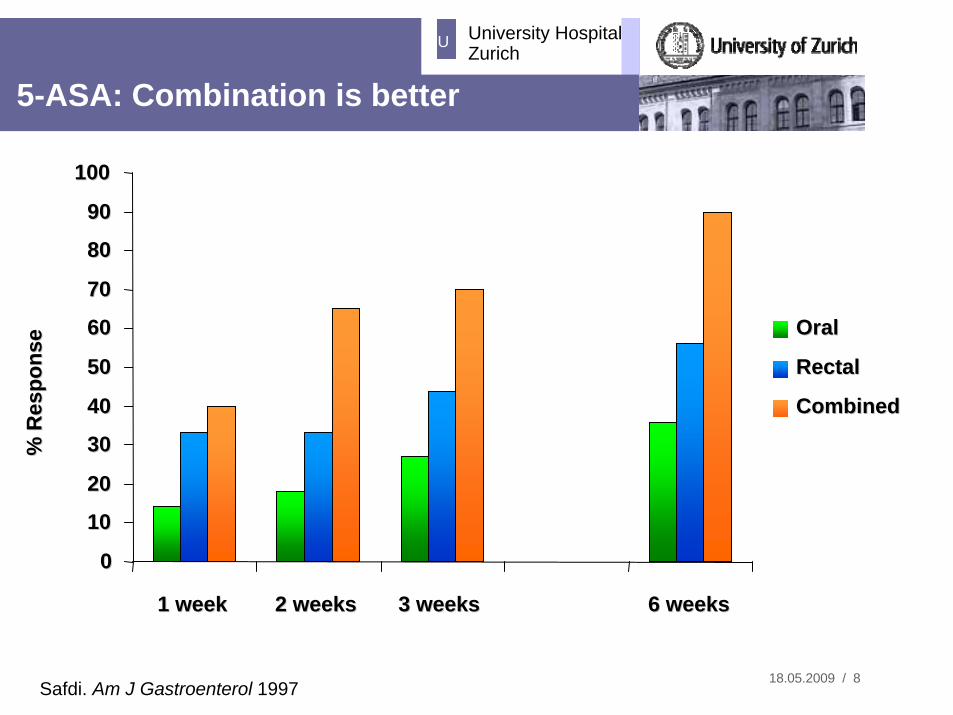
5-ASA: Combination is better
Safdi. Am J Gastroenterol 1997
% R
espo
nse
% R
espo
nse
00
1010
2020
3030
4040
5050
6060
7070
8080
9090
100100
1 week1 week 2 weeks2 weeks 3 weeks3 weeks 6 weeks6 weeks
Oral Oral
RectalRectal
CombinedCombined

18.05.2009 / 9
University HospitalZurich
UCorticosteroids: Short and Long Term Efficacy
*30 days after initiating corticosteroid therapy Faubion W, et al. Gastroenterology. 2001;121:255.
1-Month Outcomes*(n=63)
1-YearOutcomes(n=63)
Steroid Dependent
22%(n=14)
Prolonged Response
49%(n=31)
Surgery 29%
(n=18)
Complete Remission
54%(n=34)
Partial Remission
30%(n=19)
No Response
16%(n=10)

18.05.2009 / 10
University HospitalZurich
U
Days
% C
umul
ativ
e Pr
obab
ility
0
20
40
60
80
100
0 30 60 90 182 365
Risk of Resection in UC After 1st Course of Steroids:
Faubion WA Jr, et al. Gastroenterology. 2001;121:255.
*185 patients in Olmsted County, MN diagnosed with UC from 1970 to 1993

18.05.2009 / 11
University HospitalZurich
U
05
10152025303540
ACT 1 ACT 2
PlaceboInflix. 5 mg/kgInflix. 10 mg/kg
remission after 8 weeks (%)
Infliximab 5 mg/kg or 10 mg/kg in ACT 1 and 2 significantly better than placebo
Infliximab for the induction of remission in active ulcerative colitis
Rutgeerts et al. NEJM 2005;353:2462-76
14.9
38.8
32.0
5.7
33.9
27.5
p < 0.001 p < 0.001
p = 0.002 p < 0.001

18.05.2009 / 12
University HospitalZurich
U
%%
0
5
10
15
20
25
30
Week 30
21,7%
10,1%
Patients without steroids
Infliximab for the induction of remission in active ulcerative colitis
Rutgeerts et al. NEJM 2005;353:2462-76

18.05.2009 / 13
University HospitalZurich
UCase 2: Actor with refractory pan-colitis
Formerly in remission on AZA 10-20 BM/dayProgressive weight lossTransferred by air ambulanceIV steroids, PRBC, TPN

18.05.2009 / 14
University HospitalZurich
UDoes anti-viral therapy help?
64 non-refractory IBD pts ( UC 23:CD 43) 1• 42 (66%) had + serology• 1 had CMV Ag and biopsy-proven CMV colitis
• only this patient had benefit
47 inpatients with UC checked for CMV Ag in blood2
• 12/16 UC pts with +CMV treated • 8 (66.7 %) responded62 pts with severe colitis (55 UC;7 CD)3
• 7 (5UC,2 CD) out of 19 (36%) pts with refractory disease: CMV found in rectal bx
• 5/6 treated patients went into remission after antiviral treatment; 1 did not->surgery
1) de Saussure P. APT 2004;20;13232) Wada Y Dis Col Rect. 2003 ;46(10):S59-65.3) Cottone M. AJG. 2001. 96(3):773-5.

18.05.2009 / 15
University HospitalZurich
UCurrent therapeutic choices in severe UC
CyA/TacrolimusInfliximabClinical TrialColectomy
Choice will depend on center expertise with drug choices and availability of expert surgical support
Arseneau K. Clin Gastro Hep 2006. 4(9);1135-1142

18.05.2009 / 16
University HospitalZurich
U5-ASA orally for relapse prevention in
ulcerative colitis
Miner, 1995
5-ASA Placebo(n = 103) (n = 102)
Remission at 12 months (%) 64 38
Left sided (%) 63 41
Extensive colitis (%) 67 31

18.05.2009 / 17
University HospitalZurich
U
Acute flarewithin 12 months
36 % E. Coli Nissle
E.coli Nissle E.coli Nissle in UCin UC
E. coli Nissle(Mutaflor)200 mg
222 patients
33 % 5-ASA
5-ASA 1.5 g
Kruis et al, GUT, Nov 2004

18.05.2009 / 18
University HospitalZurich
U
OR
Continous 5-ASA intake 0.25 (0.13 - 0.48)*
Continously 5-ASA > 1.2 g/day 0.19 (0.05 - 0.61)*< 1.2 g/day 0.18 (0.02 - 1.92)
SASP 2g/day 0.85 (0.32 - 2.26)
Regular visit to physician (> 2/year) 0.16 (0.04 - 0.60)*
Number of colonoscopies after diagnosis no effect
Positive family history 5.0 (1.10 - 22.82)**
* p < 0.01 ** p < 0.04
Carcinoma prevention in UC: Role of 5-ASA
Eaden, 2000

18.05.2009 / 19
University HospitalZurich
U
Compliance is crucial!!
Kane et al, Am J Med, 2003

18.05.2009 / 20
University HospitalZurich
U
Final Points
There is no “one size fits all” to UC therapy• Therapy and decision making are tailored to the individual
Mild to moderate disease:• Remember topical therapy
Success of algorithms depends upon optimization of each step of therapy and considerable judgment about each outcome
• Skillful application of medical therapy makes the difference in outcomes: topical therapy, combination of oral and rectal administration, appropriate dosage

18.05.2009 / 21
University HospitalZurich
U
Thank you for your attention!!