medical policy genetic testing - paramount … related to a heritable or acquired disorder. this can...
TRANSCRIPT

POLICY: PG0041
ORIGINAL EFFECTIVE: 01/01/12
LAST REVIEW: 01/25/18
MEDICAL POLICY
Genetic Testing
GUIDELINES This policy does not certify benefits or authorization of benefits, which is designated by each individual policyholder contract. Paramount applies coding edits to all medical claims through coding logic software to evaluate the accuracy and adherence to accepted national standards. This guideline is solely for explaining correct procedure reporting and does not imply coverage and reimbursement.
DESCRIPTION A genetic test is the analysis of human DNA, RNA, chromosomes, proteins, or certain metabolites in order to detect alterations related to a heritable or acquired disorder. This can be accomplished by directly examining the DNA or RNA that makes up a gene (direct testing), looking at markers co-inherited with a disease-causing gene (linkage testing), assaying certain metabolites (biochemical testing), or examining the chromosomes (cytogenetic testing). Clinical genetic tests are those in which specimens are examined and results reported to the provider or patient for the purpose of diagnosis, prevention or treatment in the care of individual patients.
Genetic testing is performed for a variety of intended uses:
Diagnostic testing (to diagnose disease)
Predictive testing (generally performed to gather genetic data that can assist in clinical management, including therapeutic decision for an individual.
Pre-symptomatic genetic testing (to predict future disease)
Carrier testing (to identify carriers of genetic mutations)
Prenatal testing (offered during pregnancy to identify fetuses that have certain diseases)
Pre-implantation genetic testing (done in conjunction with invitro fertilization to determine whether embryos for implantation carry genes that could cause disease)
Newborn screening (to test newborns shortly after birth to determine whether they have certain diseases known to cause problems with health and development)
Pharmacogenetic testing (to determine the likelihood of an individual being responsive to a particular drug and/or to predict serious toxicity from a drug in order to optimize drug selection or drug dosage)
Research genetic testing (used to help with research and development of gene-based therapy) Several hundred genetic tests are currently in use, and more are being developed. Although genetic testing can provide helpful information for diagnosing, treating, and preventing illness, there are limitations. For example, in a healthy patient, a positive result from a non-malignant genetic test does not always mean the patient will develop a disease. On the other hand, in some situation, a negative result does not guarantee the patient will not have a certain disorder.
POLICY Prior authorization is required for genetic testing unless otherwise noted in one of our policies. Some genetic testing requires prior authorization or may be non-covered. A provider must refer to the Paramount prior authorization list and specific medical policy in reference to specific tests for coverage determinations (this list may not be all-inclusive):
PG0065 Colorectal Cancer Screening (81327, 81401, 81528)
PG0067 Genetic Testing for Breast and Ovarian Cancers (81162, 81211, 81212, 81213, 81214, 81215, 81216, 81217, 81432, 81433, 81445, 81455)
PG0125 DNA-Based Testing for Adolescent Idiopathic Scoliosis (AIS) (0004M)
PG0280 Genetic Testing for Cardiac Conditions (81413, 81414, 81439, S3861-S3866)
PG0287 Cell-Free DNA Tests For Fetal Aneuploidy (81420, 81422, 81507, 0009M)
PG0296 Comparative Genomic Hybridization (CGH) (81228, 81229, S3870)
PG0298 Afirma® Thyroid FNA Analysis (81545)
PG0301 Genetic Expression Assays for Breast Cancer Prognosis (81479, 81519, 81520, 81521, 0008M, S3854)
PG0302 Genetic Testing for Colorectal Cancer (81201-81203, 81292-81301, 81317-81319, 81403)
PG0334 ThyroSeq® (81479, 81599)

- 2 -
PG0336 PTEN Gene Testing (81321-81323)
PG0340 AlloMap™ Molecular-Expression Blood Test (81595)
PG0355 Genetic Testing for Hereditary Thrombophilia (81240, 81241, 81291)
PG0357 Gene Expression Profiling for Colorectal Cancer (81525)
PG0360 Genetic Testing for FMR1 Mutations Including Fragile X Syndrome (81243, 81244)
PG0362 Vectra® DA (81490)
PG0363 CORUS® CAD (81493)
PG0364 Cancer Type ID (81540)
PG0367 Gene Expression Analysis for Prostate Cancer (81313, 81479, 81539, 81541, 81551, 0005U)
PG0368 GeneSight® Assay for Refractory Depression (81479)
PG0375 Molecular Cytogenetic Testing (88271)
PG0390 Genetic Testing for Warfarin Dose (G9143, 81227, 81355)
PG0411 Genetic Testing for Duchenne and Becker Muscular Dystrophy (81161, 81408)
PG0417 Proprietary Laboratory Analyses (PLA) Codes (0001U-0034U) HMO, PPO, Individual Marketplace Genetic testing codes that require prior authorization for HMO, PPO, Individual Marketplace: 81105, 81106, 81107, 81108, 81109, 81110, 81111, 81112, 81120, 81121, 81161, 81162, 81175, 81176, 81201, 81202, 81203, 81211-81217, 81225, 81226, 81227, 81228, 81229, 81235, 81238, 81242, 81243, 81244, 81247, 81248, 81249, 81251, 81258, 81259, 81269, 81283, 81287, 81288, 81292-81304, 81313, 81317-81319, 81321-81323, 81328, 81332, 81334, 81335, 81346, 81361, 81362, 81363, 81364, 81400-81408, 81413, 81414, 81420, 81432, 81435, 81436, 81439, 81445, 81448, 81450, 81455, 81479, 81504, 81509, 81519, 81599, G0452, S3865, S3866, S3870 Genetic testing codes that do not require prior authorization for HMO, PPO, Individual Marketplace: 81170, 81206-81208, 81210, 81218-81224, 81245, 81246, 81250, 81255-81256, 81261-81268, 81270, 81272, 81273, 81275, 81276, 81310, 81311, 81314-81316, 81340-81342, 81350, 81355, 81370-81383, 81437, 81528, 81545, 81595 Genetic testing codes that are non-covered for HMO, PPO, Individual Marketplace: 81200, 81205, 81209, 81230, 81231, 81232, 81240, 81241, 81252, 81253, 81254, 81257, 81260, 81290, 81291, 81324-81326, 81327, 81330, 81331, 81410, 81411, 81412, 81415-81417, 81422, 81425-81427, 81430, 81431, 81433, 81434, 81438, 81440, 81442, 81460, 81465, 81470, 81471, 81490, 81493, 81500, 81503, 81506-81512, 81525, 81535-81538, 81539, 81540, 0001M-0004M, 0006M, 0007M, 0008M, 0009M, S3800-S3853, S3854, S3861 Elite Genetic testing codes that require prior authorization for Elite: 81105, 81106, 81107, 81108, 81109, 81110, 81111, 81112, 81120, 81121, 81161, 81162, 81175, 81176, 81201, 81202, 81203, 81211-81217, 81225, 81226, 81227, 81228, 81229, 81235, 81238, 81247, 81248, 81249, 81283, 81287, 81288, 81292-81301, 81313, 81317-81319, 81321-81323, 81332, 81334, 81335, 81346, 81400-81408, 81413, 81414, 81420, 81432, 81435, 81436, 81439, 81445, 81448, 81450, 81455, 81479, 81493, 81504, 81509, 81519, 81599, 0008M, G0452, S3865, S3866, S3870 Genetic testing codes that do not require prior authorization for Elite: 81170, 81206-81208, 81210, 81218-81224, 81245, 81246, 81250, 81255-81256, 81261-81268, 81270, 81272, 81273, 81275, 81276, 81310, 81311, 81314-81316, 81340-81342, 81350, 81355, 81370-81383, 81437, 81490, 81525, 81528, 81540, 81545, 81595 Genetic testing codes that are non-covered for Elite: 81200, 81205, 81209, 81230, 81231, 81232, 81240, 81241, 81242, 81243, 81244, 81251, 81252, 81253, 81254, 81257, 81258, 81259, 81260, 81269, 81290, 81291, 81302-81304, 81324-81326, 81327, 81328, 81330, 81331, 81361, 81362, 81363, 81364, 81410, 81411, 81412, 81415-81417, 81422, 81425-81427, 81430, 81431, 81433, 81434, 81438, 81440, 81442, 81460, 81465, 81470, 81471, 81500, 81503, 81506-81512, 81535-81538, 81539, 0001M-0004M, 0006M, 0007M, 0009M, S3800-S3853, S3854, S3861 Advantage Genetic testing codes that require prior authorization for Advantage: 81105, 81106, 81107, 81108, 81109, 81110, 81111, 81112, 81120, 81121, 81161, 81162, 81175, 81176, 81200, 81201, 81202, 81203, 81205, 81209, 81211-81217, 81225, 81226, 81227, 81228, 81229, 81230, 81231, 81232, 81235, 81238, 81240, 81241, 81242, 81243, 81244, 81247, 81248, 81249, 81251, 81252, 81253, 81254, 81257,

- 3 -
81258, 81259, 81260, 81269, 81283, 81287, 81288, 81290, 81291, 81292-81304, 81313, 81317-81319, 81321-81326, 81328, 81330-81332, 81334, 81335, 81346, 81361, 81362, 81363, 81364, 81400-81408, 81410, 81411, 81412, 81413, 81414, 81415-81417, 81420, 81422, 81425-81427, 81430-81436, 81438, 81439, 81440, 81442, 81445, 81448, 81450, 81455, 81460, 81465, 81470, 81471, 81479, 81509, 81519, 81539, 81599, G0452, S3854, S3865, S3866 Genetic testing codes that do not require prior authorization for Advantage: 81170, 81206-81208, 81210, 81218-81224, 81245, 81246, 81250, 81255-81256, 81261-81268, 81270, 81272, 81273, 81275, 81276, 81310, 81311, 81314-81316, 81327, 81340-81342, 81350, 81355, 81370-81383, 81437, 81528, 81545 Genetic testing codes that are non-covered for Advantage: 81490, 81493, 81500-81512, 81525, 81535-81538, 81540, 81595, 0001M-0004M, 0006M, 0007M, 0008M, 0009M, S3800-S3853, S3861, S3870 All Product Lines Cytogenetic studies (88230-88299) do not require prior authorization for all product lines. Code 88271 has a limit of 25 units per 365 days.
HMO, PPO, Individual Marketplace, Elite, Advantage Coverage and authorization for genetic testing is determined by review. The testing must have direct effect on the management and clinical care of the individual being tested, and must contain all of the following criteria:
The genetic disorder is associated with a significant disability or has a lethal natural history
The risk of the significant disability or lethality from the genetic disorder cannot be determined through other diagnostic testing
A specific mutation, or set of mutations, has been proven valid in the scientific literature to be reliable, associated with the disease
The results of the genetic test could impact the medical management of the individual being tested
The genetic test will likely result in an anticipated improvement in net health outcomes for the individual being tested (i.e. the disease is treatable or preventable)
When requesting prior authorization review, the patient’s medical history/record and details of the lab facility providing the requested service must be provided. An approved request will only be given to a specific lab for a specific provider for a specific service. Genetic testing may be denied as experimental or not medically necessary based on the information submitted. The physician, lab or facility ordering the service will be financially responsible if prior authorization is not obtained. Members who choose to precede with unauthorized genetic testing bear the responsibility for the cost. The provider should always secure a Waiver of Responsibility prior to providing the testing to assure member understanding of their financial responsibility.
Paramount covers cytogenetic studies (88230-88299) when they are reasonable and necessary for the diagnosis or treatment of the following conditions:
Genetic disorders (e.g., mongolism) in a fetus
Failure of sexual development
Chronic myelogenous leukemia
Acute leukemias lymphoid (FAB L1-L3), myeloid (FAB M0-M7), and unclassified
Mylodysplasia NOTE: Molecular cytogenetics; DNA probe each (88271) will have a limit of 25 units per 365 days. Modifier 91 will not allow for additional units.
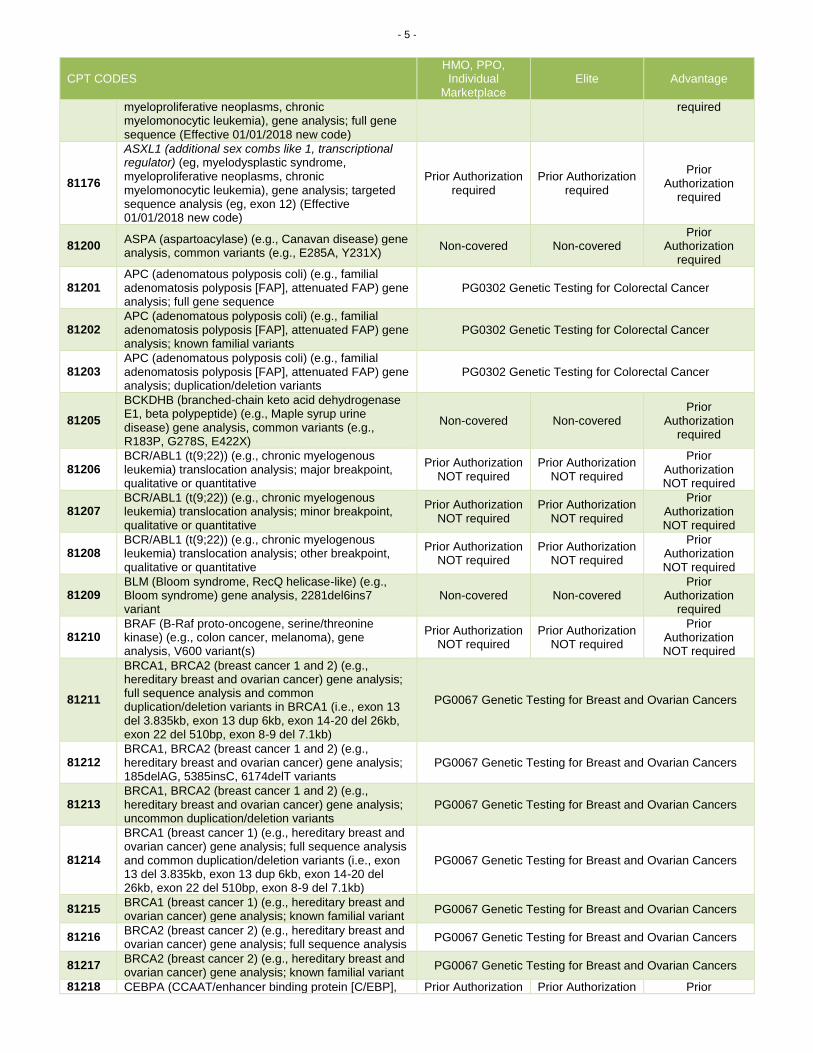
CODING/BILLING INFORMATION The appearance of a code in this section does not necessarily indicate coverage. Codes that are covered may have selection criteria that must be met. Payment for supplies may be included in payment for other services rendered.
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
Tier 1 Molecular Pathology Procedures
81105 Human Platelet Antigen 1 genotyping (HPA-1), ITGB3 (integrin, beta 3 [platelet glycoprotein IIIa], antigen
Prior Authorization required
Prior Authorization required
Prior Authorization

- 4 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
CD61 [GPIIIa]) (eg, neonatal alloimmune thrombocytopenia [NAIT], post-transfusion purpura), gene analysis, common variant, HPA-1a/b (L33P) (Effective 01/01/2018 new code)
required
81106
Human Platelet Antigen 2 genotyping (HPA-2), GP1BA (glycoprotein Ib [platelet], alpha polypeptide [GPIba]) (eg, neonatal alloimmune thrombocytopenia [NAIT], posttransfusion purpura), gene analysis, common variant, HPA-2a/b (T145M) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81107
Human Platelet Antigen 3 genotyping (HPA-3), ITGA2B (integrin, alpha 2b [platelet glycoprotein IIb of IIb/IIIa complex], antigen CD41 [GPIIb]) (eg, neonatal alloimmune thrombocytopenia [NAIT], post-transfusion purpura), gene analysis, common variant, HPA-3a/b (I843S) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81108
Human Platelet Antigen 4 genotyping (HPA-4), ITGB3 (integrin, beta 3 [platelet glycoprotein IIIa], antigen CD61 [GPIIIa]) (eg, neonatal alloimmune thrombocytopenia [NAIT], post-transfusion purpura), gene analysis, common variant, HPA-4a/b (R143Q) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81109
Human Platelet Antigen 5 genotyping (HPA-5), ITGA2 (integrin, alpha 2 [CD49B, alpha 2 subunit of VLA-2 receptor] [GPIa]) (eg, neonatal alloimmune thrombocytopenia [NAIT], post-transfusion purpura), gene analysis, common variant (eg, HPA-5a/b (K505E)) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81110
Human Platelet Antigen 6 genotyping (HPA-6w), ITGB3 (integrin, beta 3 [platelet glycoprotein IIIa, antigen CD61] [GPIIIa]) (eg, neonatal alloimmune thrombocytopenia [NAIT], post-transfusion purpura), gene analysis, common variant, HPA-6a/b (R489Q) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81111
Human Platelet Antigen 9 genotyping (HPA-9w), ITGA2B (integrin, alpha 2b [platelet glycoprotein IIb of IIb/IIIa complex, antigen CD41] [GPIIb]) (eg, neonatal alloimmune thrombocytopenia [NAIT], post-transfusion purpura), gene analysis, common variant, HPA-9a/b (V837M) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81112
Human Platelet Antigen 15 genotyping (HPA-15), CD109 (CD109 molecule) (eg, neonatal alloimmune thrombocytopenia [NAIT], post-transfusion purpura), gene analysis, common variant, HPA-15a/b (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81120 IDH1 (isocitrate dehydrogenase 1 [NADP+], soluble) (eg, glioma), common variants (eg, R132H, R132C) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81121 IDH2 (isocitrate dehydrogenase 2 [NADP+], mitochondrial) (eg, glioma), common variants (eg, R140W, R172M) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81161 DMD (dystrophin) (e.g., Duchenne/Becker muscular dystrophy) deletion analysis, and duplication analysis, if performed
PG0411 Genetic Testing for Duchenne and Becker Muscular Dystrophy
81162
BRCA1, BRCA2 (breast cancer 1 and 2) (eg, hereditary breast and ovarian cancer) gene analysis; full sequence analysis and full duplication/deletion analysis
PG0067 Genetic Testing for Breast and Ovarian Cancers
81170
ABL1 (ABL proto-oncogene 1, non-receptor tyrosine kinase) (eg, acquired imatinib tyrosine kinase inhibitor resistance), gene analysis, variants in the kinase domain
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81175 ASXL1 (additional sex combs like 1, transcriptional regulator) (eg, myelodysplastic syndrome,
Prior Authorization required
Prior Authorization required
Prior Authorization
- 5 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
myeloproliferative neoplasms, chronic myelomonocytic leukemia), gene analysis; full gene sequence (Effective 01/01/2018 new code)
required
81176
ASXL1 (additional sex combs like 1, transcriptional regulator) (eg, myelodysplastic syndrome, myeloproliferative neoplasms, chronic myelomonocytic leukemia), gene analysis; targeted sequence analysis (eg, exon 12) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81200 ASPA (aspartoacylase) (e.g., Canavan disease) gene analysis, common variants (e.g., E285A, Y231X)
Non-covered Non-covered Prior
Authorization required
81201 APC (adenomatous polyposis coli) (e.g., familial adenomatosis polyposis [FAP], attenuated FAP) gene analysis; full gene sequence
PG0302 Genetic Testing for Colorectal Cancer
81202 APC (adenomatous polyposis coli) (e.g., familial adenomatosis polyposis [FAP], attenuated FAP) gene analysis; known familial variants
PG0302 Genetic Testing for Colorectal Cancer
81203 APC (adenomatous polyposis coli) (e.g., familial adenomatosis polyposis [FAP], attenuated FAP) gene analysis; duplication/deletion variants
PG0302 Genetic Testing for Colorectal Cancer
81205
BCKDHB (branched-chain keto acid dehydrogenase E1, beta polypeptide) (e.g., Maple syrup urine disease) gene analysis, common variants (e.g., R183P, G278S, E422X)
Non-covered Non-covered Prior
Authorization required
81206 BCR/ABL1 (t(9;22)) (e.g., chronic myelogenous leukemia) translocation analysis; major breakpoint, qualitative or quantitative
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81207 BCR/ABL1 (t(9;22)) (e.g., chronic myelogenous leukemia) translocation analysis; minor breakpoint, qualitative or quantitative
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81208 BCR/ABL1 (t(9;22)) (e.g., chronic myelogenous leukemia) translocation analysis; other breakpoint, qualitative or quantitative
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81209 BLM (Bloom syndrome, RecQ helicase-like) (e.g., Bloom syndrome) gene analysis, 2281del6ins7 variant
Non-covered Non-covered Prior
Authorization required
81210 BRAF (B-Raf proto-oncogene, serine/threonine kinase) (e.g., colon cancer, melanoma), gene analysis, V600 variant(s)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81211
BRCA1, BRCA2 (breast cancer 1 and 2) (e.g., hereditary breast and ovarian cancer) gene analysis; full sequence analysis and common duplication/deletion variants in BRCA1 (i.e., exon 13 del 3.835kb, exon 13 dup 6kb, exon 14-20 del 26kb, exon 22 del 510bp, exon 8-9 del 7.1kb)
PG0067 Genetic Testing for Breast and Ovarian Cancers
81212 BRCA1, BRCA2 (breast cancer 1 and 2) (e.g., hereditary breast and ovarian cancer) gene analysis; 185delAG, 5385insC, 6174delT variants
PG0067 Genetic Testing for Breast and Ovarian Cancers
81213 BRCA1, BRCA2 (breast cancer 1 and 2) (e.g., hereditary breast and ovarian cancer) gene analysis; uncommon duplication/deletion variants
PG0067 Genetic Testing for Breast and Ovarian Cancers
81214
BRCA1 (breast cancer 1) (e.g., hereditary breast and ovarian cancer) gene analysis; full sequence analysis and common duplication/deletion variants (i.e., exon 13 del 3.835kb, exon 13 dup 6kb, exon 14-20 del 26kb, exon 22 del 510bp, exon 8-9 del 7.1kb)
PG0067 Genetic Testing for Breast and Ovarian Cancers
81215 BRCA1 (breast cancer 1) (e.g., hereditary breast and ovarian cancer) gene analysis; known familial variant
PG0067 Genetic Testing for Breast and Ovarian Cancers
81216 BRCA2 (breast cancer 2) (e.g., hereditary breast and ovarian cancer) gene analysis; full sequence analysis
PG0067 Genetic Testing for Breast and Ovarian Cancers
81217 BRCA2 (breast cancer 2) (e.g., hereditary breast and ovarian cancer) gene analysis; known familial variant
PG0067 Genetic Testing for Breast and Ovarian Cancers
81218 CEBPA (CCAAT/enhancer binding protein [C/EBP], Prior Authorization Prior Authorization Prior

- 6 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
alpha) (eg, acute myeloid leukemia), gene analysis, full gene sequence
NOT required NOT required Authorization NOT required
81219 CALR (calreticulin) (eg, myeloproliferative disorders), gene analysis, common variants in exon 9
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81220 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g., cystic fibrosis) gene analysis; common variants (e.g., ACMG/ACOG guidelines)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81221 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g., cystic fibrosis) gene analysis; known familial variants
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81222 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g., cystic fibrosis) gene analysis; duplication/deletion variants
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81223 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g., cystic fibrosis) gene analysis; full gene sequence
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81224 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g., cystic fibrosis) gene analysis; intron 8 poly-T analysis (e.g., male infertility)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81225 CYP2C19 (cytochrome P450, family 2, subfamily C, polypeptide 19) (e.g., drug metabolism), gene analysis, common variants (e.g., *2, *3, *4, *8, *17)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81226
CYP2D6 (cytochrome P450, family 2, subfamily D, polypeptide 6) (e.g., drug metabolism), gene analysis, common variants (e.g., *2, *3, *4, *5, *6, *9, *10, *17, *19, *29, *35, *41, *1XN, *2XN, *4XN)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81227 CYP2C9 (cytochrome P450, family 2, subfamily C, polypeptide 9) (e.g., drug metabolism), gene analysis, common variants (e.g., *2, *3, *5, *6)
PG0390 Genetic Testing for Warfarin Dose
81228
Cytogenomic constitutional (genome-wide) microarray analysis; interrogation of genomic regions for copy number variants (e.g., Bacterial Artificial Chromosome [BAC] or oligo-based comparative genomic hybridization [CGH] microarray analysis)
PG0296 Comparative Genomic Hybridization (CGH)
81229
Cytogenomic constitutional (genome-wide) microarray analysis; interrogation of genomic regions for copy number and single nucleotide polymorphism (SNP) variants for chromosomal abnormalities
PG0296 Comparative Genomic Hybridization (CGH)
81230
CYP3A4 (cytochrome P450 family 3 subfamily A member 4) (eg, drug metabolism), gene analysis, common variant(s) (eg, *2, *22) (Effective 01/01/2018 new code)
Non-covered Non-covered Prior
Authorization required
81231
CYP3A5 (cytochrome P450 family 3 subfamily A member 5) (eg, drug metabolism), gene analysis, common variants (eg, *2, *3, *4, *5 *6, *7) (Effective 01/01/2018 new code)
Non-covered Non-covered Prior
Authorization required
81232
DPYD (dihydropyrimidine dehydrogenase) (eg, 5-fluorouracil/5-FU and capecitabine drug metabolism), gene analysis, common variant(s) (eg, *2A, *4, *5, *6) (Effective 01/01/2018 new code)
Non-covered Non-covered Prior
Authorization required
81235
EGFR (epidermal growth factor receptor) (e.g., non-small cell lung cancer) gene analysis, common variants (e.g., exon 19 LREA deletion, L858R, T790M, G719A, G719S, L861Q) (LCD L32288)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81238 F9 (coagulation factor IX) (eg, hemophilia B), full gene sequence (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81240 F2 (prothrombin, coagulation factor II) (e.g., hereditary hypercoagulability) gene analysis, 20210G>A variant
PG0355 Genetic Testing for Hereditary Thrombophilia
81241 F5 (coagulation Factor V) (e.g., hereditary hypercoagulability) gene analysis, Leiden variant
PG0355 Genetic Testing for Hereditary Thrombophilia
81242 FANCC (Fanconi anemia, complementation group C) Prior Authorization Non-covered Prior

- 7 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
(e.g., Fanconi anemia, type C) gene analysis, common variant (e.g., IVS4+4A>T)
required Authorization required
81243 FMR1 (Fragile X mental retardation 1) (e.g., fragile X mental retardation) gene analysis; evaluation to detect abnormal (e.g., expanded) alleles
PG0360 Genetic Testing for FMR1 Mutations Including Fragile X Syndrome
81244 FMR1 (Fragile X mental retardation 1) (e.g., fragile X mental retardation) gene analysis; characterization of alleles (e.g., expanded size and methylation status)
PG0360 Genetic Testing for FMR1 Mutations Including Fragile X Syndrome
81245 FLT3 (fms-related tyrosine kinase 3) (eg, acute myeloid leukemia), gene analysis; internal tandem duplication (ITD) variants (i.e., exons 14, 15)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81246 FLT3 (fms-related tyrosine kinase 3) (eg, acute myeloid leukemia), gene analysis; tyrosine kinase domain (TKD) variants (eg, D835, I836)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81247
G6PD (glucose-6-phosphate dehydrogenase)
(eg,hemolytic anemia, jaundice), gene analysis; common variant(s) (eg, A, A-) (Effective 01/01/18 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81248
G6PD (glucose-6-phosphate dehydrogenase)
(eg,hemolytic anemia, jaundice), gene analysis; known familial variant(s) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81249 G6PD (glucose-6-phosphate dehydrogenase) (eg,hemolytic anemia, jaundice), gene analysis; full gene sequence (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81250
G6PC (glucose-6-phosphatase, catalytic subunit) (e.g., Glycogen storage disease, Type 1a, von Gierke disease) gene analysis, common variants (e.g., R83C, Q347X)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81251 GBA (glucosidase, beta, acid) (e.g., Gaucher disease) gene analysis, common variants (e.g., N370S, 84GG, L444P, IVS2+1G>A)
Prior Authorization required
Non-covered Prior
Authorization required
81252 GJB2 (gap junction protein, beta 2, 26kDa, connexin 26) (e.g., nonsyndromic hearing loss) gene analysis; full gene sequence (LCD L32288)
Non-covered Non-covered Prior
Authorization required
81253 GJB2 (gap junction protein, beta 2, 26kDa; connexin 26) (e.g., nonsyndromic hearing loss) gene analysis; known familial variants (LCD L32288)
Non-covered Non-covered Prior
Authorization required
81254
GJB6 (gap junction protein, beta 6, 30kDa, connexin 30) (e.g., nonsyndromic hearing loss) gene analysis, common variants (e.g., 309kb [del(GJB6-D13S1830)] and 232kb [del(GJB6-D13S1854)]) (LCD L32288)
Non-covered Non-covered Prior
Authorization required
81255 HEXA (hexosaminidase A [alpha polypeptide]) (e.g., Tay-Sachs disease) gene analysis, common variants (e.g., 1278insTATC, 1421+1G>C, G269S)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81256 HFE (hemochromatosis) (e.g., hereditary hemochromatosis) gene analysis, common variants (e.g., C282Y, H63D)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81257
HBA1/HBA2 (alpha globin 1 and alpha globin 2) (e.g., alpha thalassemia, Hb Bart hydrops fetalis syndrome, HbH disease), gene analysis; common deletions or variant (e.g., Southeast Asian, Thai, Filipino, Mediterranean, alpha3.7, alpha4.2, alpha20.5, and Constant Spring)
Non-covered Non-covered Prior
Authorization required
81258
HBA1/HBA2 (alpha globin 1 and alpha globin 2) (e.g., alpha thalassemia, Hb Bart hydrops fetalis syndrome, HbH disease), gene analysis; known familial variant (Effective 01/01/2018 new code)
Prior Authorization required
Non-covered Prior
Authorization required
81259
HBA1/HBA2 (alpha globin 1 and alpha globin 2) (e.g., alpha thalassemia, Hb Bart hydrops fetalis syndrome, HbH disease), gene analysis; full gene sequence (Effective 01/01/2018 new code)
Prior Authorization required
Non-covered Prior
Authorization required
81260 IKBKAP (inhibitor of kappa light polypeptide gene enhancer in B-cells, kinase complex-associated
Non-covered Non-covered Prior
Authorization

- 8 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
protein) (e.g., familial dysautonomia) gene analysis, common variants (e.g., 2507+6T>C, R696P)
required
81261
IGH@ (Immunoglobulin heavy chain locus) (e.g., leukemias and lymphomas, B-cell), gene rearrangement analysis to detect abnormal clonal population(s); amplified methodology (e.g., polymerase chain reaction)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81262
IGH@ (Immunoglobulin heavy chain locus) (e.g., leukemias and lymphomas, B-cell), gene rearrangement analysis to detect abnormal clonal population(s); direct probe methodology (e.g., Southern blot)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81263 IGH@ (Immunoglobulin heavy chain locus) (e.g., leukemia and lymphoma, B-cell), variable region somatic mutation analysis
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81264
IGK@ (Immunoglobulin kappa light chain locus) (e.g., leukemia and lymphoma, B-cell), gene rearrangement analysis, evaluation to detect abnormal clonal population(s)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81265
Comparative analysis using Short Tandem Repeat (STR) markers; patient and comparative specimen (e.g., pre-transplant recipient and donor germline testing, post-transplant non-hematopoietic recipient germline [e.g., buccal swab or other germline tissue sample] and donor testing, twin zygosity testing, or maternal cell contamination of fetal cells)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81266
Comparative analysis using Short Tandem Repeat (STR) markers; each additional specimen (e.g., additional cord blood donor, additional fetal samples from different cultures, or additional zygosity in multiple birth pregnancies) (List separately in addition to code for primary procedure)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81267
Chimerism (engraftment) analysis, post transplantation specimen (e.g., hematopoietic stem cell), includes comparison to previously performed baseline analyses; without cell selection
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81268
Chimerism (engraftment) analysis, post transplantation specimen (e.g., hematopoietic stem cell), includes comparison to previously performed baseline analyses; with cell selection (e.g., CD3, CD33), each cell type
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81269
HBA1/HBA2 (alpha globin 1 and alpha globin 2) (eg, alpha thalassemia, Hb Bart hydrops fetalis syndrome, HbH disease), gene analysis; duplication/deletion variants (Effective 01/01/2018 new code)
Prior Authorization required
Non-covered Prior
Authorization required
81270 JAK2 (Janus kinase 2) (e.g., myeloproliferative disorder) gene analysis, p.Val617Phe (V617F) variant
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81272
KIT (v-kit Hardy-Zuckerman 4 feline sarcoma viral oncogene homolog) (eg, gastrointestinal stromal tumor [GIST], acute myeloid leukemia, melanoma), gene analysis, targeted sequence analysis (eg, exons 8, 11, 13, 17, 18)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81273 KIT (v-kit Hardy-Zuckerman 4 feline sarcoma viral oncogene homolog) (eg, mastocytosis), gene analysis, D816 variant(s)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81275 KRAS (Kirsten rat sarcoma viral oncogene homolog) (e.g., carcinoma) gene analysis, variants in exon 2 (eg, codons 12 and 13)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81276 (KRAS (Kirsten rat sarcoma viral oncogene homolog) (eg, carcinoma) gene analysis; additional variant(s) (eg, codon 61, codon 146)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
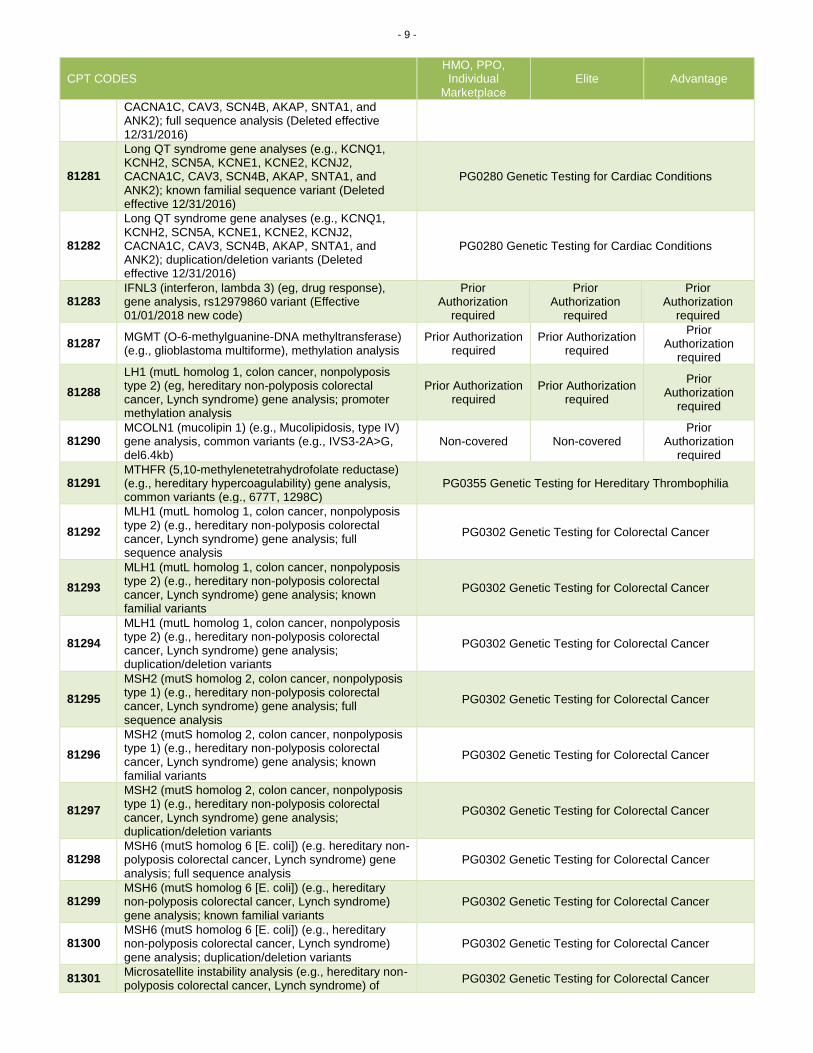
81280 Long QT syndrome gene analyses (e.g., KCNQ1, KCNH2, SCN5A, KCNE1, KCNE2, KCNJ2,
PG0280 Genetic Testing for Cardiac Conditions
- 9 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
CACNA1C, CAV3, SCN4B, AKAP, SNTA1, and ANK2); full sequence analysis (Deleted effective 12/31/2016)
81281
Long QT syndrome gene analyses (e.g., KCNQ1, KCNH2, SCN5A, KCNE1, KCNE2, KCNJ2, CACNA1C, CAV3, SCN4B, AKAP, SNTA1, and ANK2); known familial sequence variant (Deleted effective 12/31/2016)
PG0280 Genetic Testing for Cardiac Conditions
81282
Long QT syndrome gene analyses (e.g., KCNQ1, KCNH2, SCN5A, KCNE1, KCNE2, KCNJ2, CACNA1C, CAV3, SCN4B, AKAP, SNTA1, and ANK2); duplication/deletion variants (Deleted effective 12/31/2016)
PG0280 Genetic Testing for Cardiac Conditions
81283 IFNL3 (interferon, lambda 3) (eg, drug response), gene analysis, rs12979860 variant (Effective 01/01/2018 new code)
Prior Authorization
required
Prior Authorization
required
Prior Authorization
required
81287 MGMT (O-6-methylguanine-DNA methyltransferase) (e.g., glioblastoma multiforme), methylation analysis
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81288
LH1 (mutL homolog 1, colon cancer, nonpolyposis type 2) (eg, hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; promoter methylation analysis
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81290 MCOLN1 (mucolipin 1) (e.g., Mucolipidosis, type IV) gene analysis, common variants (e.g., IVS3-2A>G, del6.4kb)
Non-covered Non-covered Prior
Authorization required
81291 MTHFR (5,10-methylenetetrahydrofolate reductase) (e.g., hereditary hypercoagulability) gene analysis, common variants (e.g., 677T, 1298C)
PG0355 Genetic Testing for Hereditary Thrombophilia
81292
MLH1 (mutL homolog 1, colon cancer, nonpolyposis type 2) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; full sequence analysis
PG0302 Genetic Testing for Colorectal Cancer
81293
MLH1 (mutL homolog 1, colon cancer, nonpolyposis type 2) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; known familial variants
PG0302 Genetic Testing for Colorectal Cancer
81294
MLH1 (mutL homolog 1, colon cancer, nonpolyposis type 2) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; duplication/deletion variants
PG0302 Genetic Testing for Colorectal Cancer
81295
MSH2 (mutS homolog 2, colon cancer, nonpolyposis type 1) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; full sequence analysis
PG0302 Genetic Testing for Colorectal Cancer
81296
MSH2 (mutS homolog 2, colon cancer, nonpolyposis type 1) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; known familial variants
PG0302 Genetic Testing for Colorectal Cancer
81297
MSH2 (mutS homolog 2, colon cancer, nonpolyposis type 1) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; duplication/deletion variants
PG0302 Genetic Testing for Colorectal Cancer
81298 MSH6 (mutS homolog 6 [E. coli]) (e.g. hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; full sequence analysis
PG0302 Genetic Testing for Colorectal Cancer
81299 MSH6 (mutS homolog 6 [E. coli]) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; known familial variants
PG0302 Genetic Testing for Colorectal Cancer
81300 MSH6 (mutS homolog 6 [E. coli]) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; duplication/deletion variants
PG0302 Genetic Testing for Colorectal Cancer
81301 Microsatellite instability analysis (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) of
PG0302 Genetic Testing for Colorectal Cancer
- 10 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
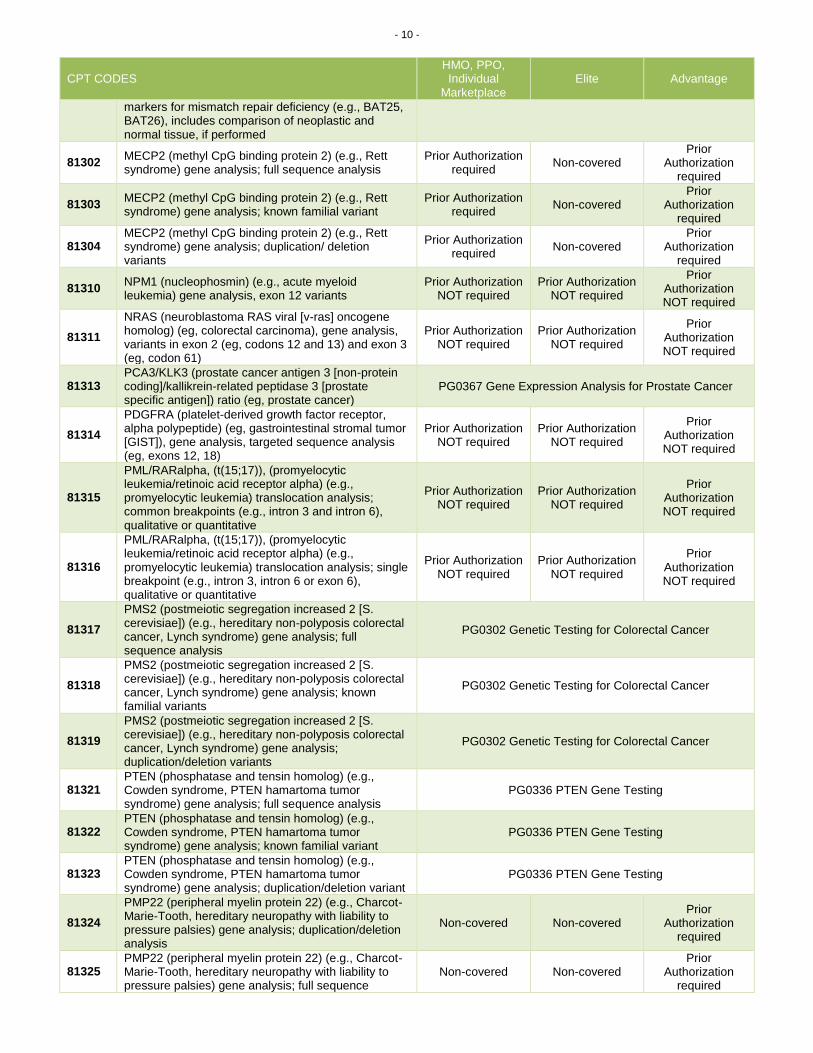
markers for mismatch repair deficiency (e.g., BAT25, BAT26), includes comparison of neoplastic and normal tissue, if performed
81302 MECP2 (methyl CpG binding protein 2) (e.g., Rett syndrome) gene analysis; full sequence analysis
Prior Authorization required
Non-covered Prior
Authorization required
81303 MECP2 (methyl CpG binding protein 2) (e.g., Rett syndrome) gene analysis; known familial variant
Prior Authorization required
Non-covered Prior
Authorization required
81304 MECP2 (methyl CpG binding protein 2) (e.g., Rett syndrome) gene analysis; duplication/ deletion variants
Prior Authorization required
Non-covered Prior
Authorization required
81310 NPM1 (nucleophosmin) (e.g., acute myeloid leukemia) gene analysis, exon 12 variants
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81311
NRAS (neuroblastoma RAS viral [v-ras] oncogene homolog) (eg, colorectal carcinoma), gene analysis, variants in exon 2 (eg, codons 12 and 13) and exon 3 (eg, codon 61)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81313 PCA3/KLK3 (prostate cancer antigen 3 [non-protein coding]/kallikrein-related peptidase 3 [prostate specific antigen]) ratio (eg, prostate cancer)
PG0367 Gene Expression Analysis for Prostate Cancer
81314
PDGFRA (platelet-derived growth factor receptor, alpha polypeptide) (eg, gastrointestinal stromal tumor [GIST]), gene analysis, targeted sequence analysis (eg, exons 12, 18)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81315
PML/RARalpha, (t(15;17)), (promyelocytic leukemia/retinoic acid receptor alpha) (e.g., promyelocytic leukemia) translocation analysis; common breakpoints (e.g., intron 3 and intron 6), qualitative or quantitative
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81316
PML/RARalpha, (t(15;17)), (promyelocytic leukemia/retinoic acid receptor alpha) (e.g., promyelocytic leukemia) translocation analysis; single breakpoint (e.g., intron 3, intron 6 or exon 6), qualitative or quantitative
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81317
PMS2 (postmeiotic segregation increased 2 [S. cerevisiae]) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; full sequence analysis
PG0302 Genetic Testing for Colorectal Cancer
81318
PMS2 (postmeiotic segregation increased 2 [S. cerevisiae]) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; known familial variants
PG0302 Genetic Testing for Colorectal Cancer
81319
PMS2 (postmeiotic segregation increased 2 [S. cerevisiae]) (e.g., hereditary non-polyposis colorectal cancer, Lynch syndrome) gene analysis; duplication/deletion variants
PG0302 Genetic Testing for Colorectal Cancer
81321 PTEN (phosphatase and tensin homolog) (e.g., Cowden syndrome, PTEN hamartoma tumor syndrome) gene analysis; full sequence analysis
PG0336 PTEN Gene Testing
81322 PTEN (phosphatase and tensin homolog) (e.g., Cowden syndrome, PTEN hamartoma tumor syndrome) gene analysis; known familial variant
PG0336 PTEN Gene Testing
81323 PTEN (phosphatase and tensin homolog) (e.g., Cowden syndrome, PTEN hamartoma tumor syndrome) gene analysis; duplication/deletion variant
PG0336 PTEN Gene Testing
81324
PMP22 (peripheral myelin protein 22) (e.g., Charcot-Marie-Tooth, hereditary neuropathy with liability to pressure palsies) gene analysis; duplication/deletion analysis
Non-covered Non-covered Prior
Authorization required
81325 PMP22 (peripheral myelin protein 22) (e.g., Charcot-Marie-Tooth, hereditary neuropathy with liability to pressure palsies) gene analysis; full sequence
Non-covered Non-covered Prior
Authorization required

- 11 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
analysis
81326
PMP22 (peripheral myelin protein 22) (e.g., Charcot-Marie-Tooth, hereditary neuropathy with liability to pressure palsies) gene analysis; known familial variant
Non-covered Non-covered Prior
Authorization required
81327 SEPT9 (Septin9) (eg, colorectal cancer) methylation analysis
PG0065 Colorectal Cancer Screening
81328
SLCO1B1 (solute carrier organic anion transporter family, member 1B1) (eg, adverse drug reaction), gene analysis, common variant(s) (eg, *5) (Effective 01/01/2018 new code)
Prior Authorization
required Non-covered
Prior Authorization
required
81330
SMPD1(sphingomyelin phosphodiesterase 1, acid lysosomal) (e.g., Niemann-Pick disease, Type A) gene analysis, common variants (e.g., R496L, L302P, fsP330)
Non-covered Non-covered Prior
Authorization required
81331
SNRPN/UBE3A (small nuclear ribonucleoprotein polypeptide N and ubiquitin protein ligase E3A) (e.g., Prader-Willi syndrome and/or Angelman syndrome), methylation analysis
Non-covered Non-covered Prior
Authorization required
81332
SERPINA1 (serpin peptidase inhibitor, clade A, alpha-1 antiproteinase, antitrypsin, member 1) (e.g., alpha-1-antitrypsin deficiency), gene analysis, common variants (e.g., *S and *Z)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81334
RUNX1 (runt related transcription factor 1) (eg, acute myeloid leukemia, familial platelet disorder with associated myeloid malignancy), gene analysis, targeted sequence analysis (eg, exons 3-8) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81335 TPMT (thiopurine S-methyltransferase) (eg, drug metabolism), gene analysis, common variants (eg, *2, *3) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81340
TRB@ (T cell antigen receptor, beta) (e.g., leukemia and lymphoma), gene rearrangement analysis to detect abnormal clonal population(s); using amplification methodology (e.g., polymerase chain reaction)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81341
TRB@ (T cell antigen receptor, beta) (e.g., leukemia and lymphoma), gene rearrangement analysis to detect abnormal clonal population(s); using direct probe methodology (e.g., Southern blot)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81342
TRG@ (T cell antigen receptor, gamma) (e.g., leukemia and lymphoma), gene rearrangement analysis, evaluation to detect abnormal clonal population(s)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81346
TYMS (thymidylate synthetase) (eg, 5-fluorouracil/5-FU drug metabolism), gene analysis, common variant(s) (eg,tandem repeat variant) (Effective 01/01/2018 new code)
Prior Authorization required
Prior Authorization required
Prior Authorization
required
81350 UGT1A1 (UDP glucuronosyltransferase 1 family, polypeptide A1) (e.g., irinotecan metabolism), gene analysis, common variants (e.g., *28, *36, *37)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81355 VKORC1 (vitamin K epoxide reductase complex, subunit 1) (e.g., warfarin metabolism), gene analysis, common variant(s) (e.g., -1639G>A, c.173+1000C>T)
PG0390 Genetic Testing for Warfarin Dose
81361
HBB (hemoglobin, subunit beta) (eg, sickle cell anemia, beta thalassemia hemoglobinopathy); common variant(s) (eg, HbS, HbC, HbE) (Effective 01/01/2018 new code)
Prior Authorization required
Non-covered Prior
Authorization required
81362 HBB (hemoglobin, subunit beta) (eg, sickle cell anemia, beta thalassemia hemoglobinopathy); known familial variant(s) (Effective 01/01/2018 new code)
Prior Authorization required
Non-covered Prior
Authorization required
81363 HBB (hemoglobin, subunit beta) (eg, sickle cell anemia, beta thalassemia hemoglobinopathy); duplication/deletion variant(s) (Effective 01/01/2018
Prior Authorization required
Non-covered Prior
Authorization required
- 12 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
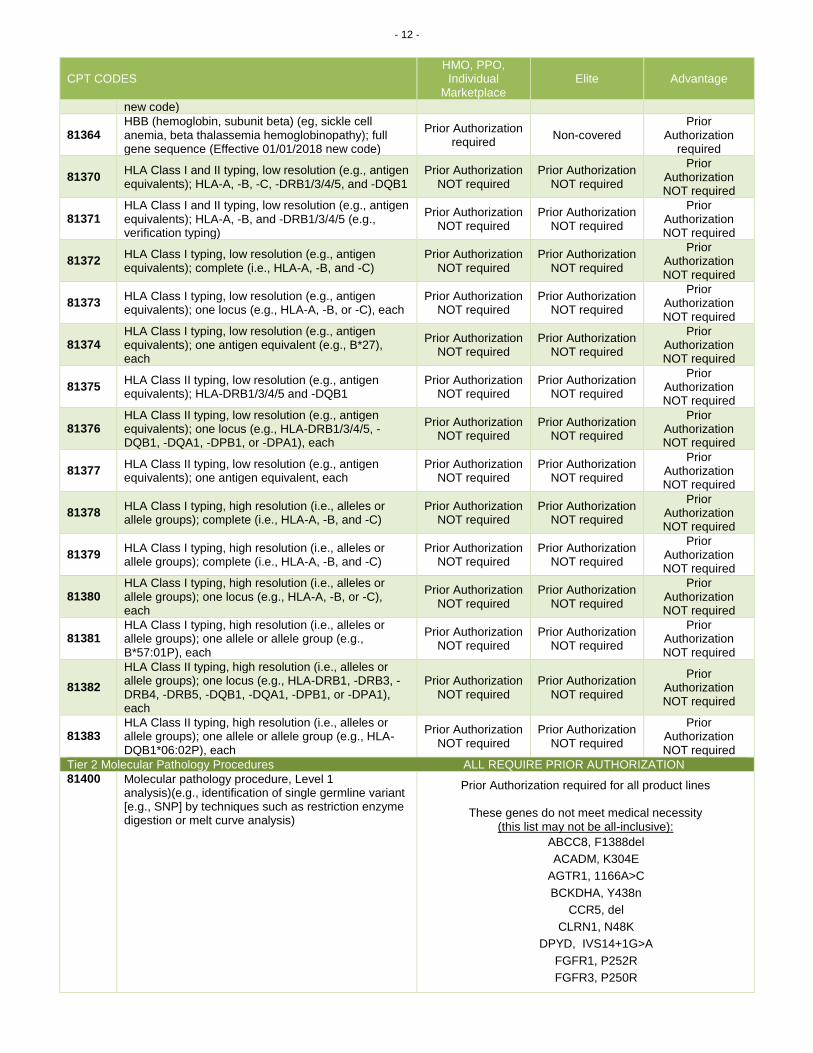
new code)
81364 HBB (hemoglobin, subunit beta) (eg, sickle cell anemia, beta thalassemia hemoglobinopathy); full gene sequence (Effective 01/01/2018 new code)
Prior Authorization required
Non-covered Prior
Authorization required
81370 HLA Class I and II typing, low resolution (e.g., antigen equivalents); HLA-A, -B, -C, -DRB1/3/4/5, and -DQB1
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81371 HLA Class I and II typing, low resolution (e.g., antigen equivalents); HLA-A, -B, and -DRB1/3/4/5 (e.g., verification typing)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81372 HLA Class I typing, low resolution (e.g., antigen equivalents); complete (i.e., HLA-A, -B, and -C)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81373 HLA Class I typing, low resolution (e.g., antigen equivalents); one locus (e.g., HLA-A, -B, or -C), each
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81374 HLA Class I typing, low resolution (e.g., antigen equivalents); one antigen equivalent (e.g., B*27), each
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81375 HLA Class II typing, low resolution (e.g., antigen equivalents); HLA-DRB1/3/4/5 and -DQB1
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81376 HLA Class II typing, low resolution (e.g., antigen equivalents); one locus (e.g., HLA-DRB1/3/4/5, -DQB1, -DQA1, -DPB1, or -DPA1), each
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81377 HLA Class II typing, low resolution (e.g., antigen equivalents); one antigen equivalent, each
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81378 HLA Class I typing, high resolution (i.e., alleles or allele groups); complete (i.e., HLA-A, -B, and -C)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81379 HLA Class I typing, high resolution (i.e., alleles or allele groups); complete (i.e., HLA-A, -B, and -C)
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81380 HLA Class I typing, high resolution (i.e., alleles or allele groups); one locus (e.g., HLA-A, -B, or -C), each
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81381 HLA Class I typing, high resolution (i.e., alleles or allele groups); one allele or allele group (e.g., B*57:01P), each
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81382
HLA Class II typing, high resolution (i.e., alleles or allele groups); one locus (e.g., HLA-DRB1, -DRB3, -DRB4, -DRB5, -DQB1, -DQA1, -DPB1, or -DPA1), each
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81383 HLA Class II typing, high resolution (i.e., alleles or allele groups); one allele or allele group (e.g., HLA-DQB1*06:02P), each
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
Tier 2 Molecular Pathology Procedures ALL REQUIRE PRIOR AUTHORIZATION
81400
Molecular pathology procedure, Level 1 analysis)(e.g., identification of single germline variant [e.g., SNP] by techniques such as restriction enzyme digestion or melt curve analysis)
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
ABCC8, F1388del
ACADM, K304E
AGTR1, 1166A>C
BCKDHA, Y438n
CCR5, del
CLRN1, N48K
DPYD, IVS14+1G>A
FGFR1, P252R
FGFR3, P250R

- 13 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
FKTN, retro ins v
GNE, M712T
HPA-6
HPA-9
IVD, A282V
LCT, 13910 C>T
NEB, exon 55
PCDH15, R245X
SHOC2, S2G
SLCO1B1, V174A
SMN1, exon 7 del
SRY, fgs
TOR1A, var
81401 81401
Molecular pathology procedure, Level 2 (e.g., 2-10 SNPs, 1 methylated variant, or 1 somatic variant [typically using nonsequencing target variant analysis], or detection of a dynamic mutation disorder/triplet repeat) Molecular pathology procedure, Level 2 (e.g., 2-10 SNPs, 1 methylated variant, or 1 somatic variant [typically using nonsequencing target variant analysis], or detection of a dynamic mutation disorder/triplet repeat)
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
ABCC8, cv
ACADM, cv
ADRB2, cv
AFF2, detect abn
APOB, cv
APOE, cv
AR, alleles
ATN1
ATXN1
ATXN10
ATXN2
ATXN3
ATXN7
ATXN8OS
CACNA1A
CBS, cv
CFH_ARMS2, cv
CNBP
CSTB
CYP3A4, cv
CYP3A5, cv
DEK/NUP214, ta
DMPK, detect eval
EML4_ALK, ta or ia
ETV6/NTRK3
EWSR1_ATF1
FGFR3, cv
FLG, cv
FUS/DDIT3
FXN, alleles
GALC, cv
GALT, cv
H19, ma
HBB, cv
HTT, alleles
KCNQ1OT1, ma

- 14 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
LRRK2, cv
MED12, cv
MEG3_DLK1, ma
MLL_AFF1, ta qual quan
MLL_MLLT3, ta, qual quan
MT-ATP6, cv
MT-ND4, MT-ND6, cv
MT-ND5, cv
MT-RNR1, cv
MT-TK, cv
MT-TL1, cv
MT-TS1_MT-RNR1, cv
NOD2
NPM1_ALK, ta
PABPN1
PPP2R2B
PRSS1, cv
PYGM, cv
SEPT9, ma
SMN1_SMN2, dosage
SMN1_SMN2, dup_del
SS18_SSX1, ta
SS18_SSX2, ta
TBP, aa
81402
Molecular pathology procedure, Level 3 (eg, >10 SNPs, 2-10 methylated variants, or 2-10 somatic variants [typically using non-sequencing target variant analysis], immunoglobulin and T-cell receptor gene rearrangements, duplication/deletion variants of 1 exon, loss of heterozygosity [LOH], uniparental disomy [UPD])
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
C18q
C1p-/19q, del
COL1A1/PDGFB, mbp qual quan
CYP21A2, cv
ESR1_PGR, ratio
MEFV, cv
MPL, cv
TRD, delta
UPD, str
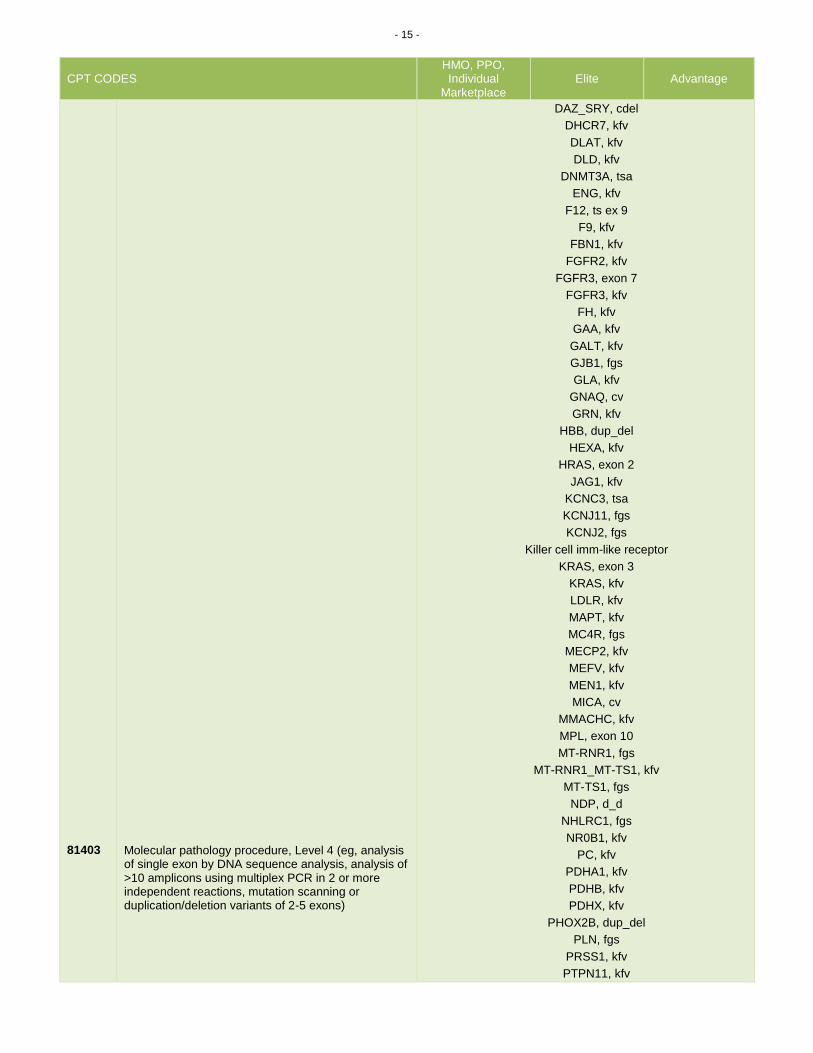
81403
Molecular pathology procedure, Level 4 (eg, analysis of single exon by DNA sequence analysis, analysis of >10 amplicons using multiplex PCR in 2 or more independent reactions, mutation scanning or duplication/deletion variants of 2-5 exons)
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
ACADS, kfv
ACADVL, kfv
ACTA2, kfv
ANG, fgs
ARX, d_d
BTD, kfv
CASR, kfv
CDH1, kfv
CEL, exon 11
COL1A2, kfv
CTNNB1, tsa
CTNNB1, tsa
CYP21A2, kfv
- 15 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81403
Molecular pathology procedure, Level 4 (eg, analysis of single exon by DNA sequence analysis, analysis of >10 amplicons using multiplex PCR in 2 or more independent reactions, mutation scanning or duplication/deletion variants of 2-5 exons)
DAZ_SRY, cdel
DHCR7, kfv
DLAT, kfv
DLD, kfv
DNMT3A, tsa
ENG, kfv
F12, ts ex 9
F9, kfv
FBN1, kfv
FGFR2, kfv
FGFR3, exon 7
FGFR3, kfv
FH, kfv
GAA, kfv
GALT, kfv
GJB1, fgs
GLA, kfv
GNAQ, cv
GRN, kfv
HBB, dup_del
HEXA, kfv
HRAS, exon 2
JAG1, kfv
KCNC3, tsa
KCNJ11, fgs
KCNJ2, fgs
Killer cell imm-like receptor
KRAS, exon 3
KRAS, kfv
LDLR, kfv
MAPT, kfv
MC4R, fgs
MECP2, kfv
MEFV, kfv
MEN1, kfv
MICA, cv
MMACHC, kfv
MPL, exon 10
MT-RNR1, fgs
MT-RNR1_MT-TS1, kfv
MT-TS1, fgs
NDP, d_d
NHLRC1, fgs
NR0B1, kfv
PC, kfv
PDHA1, kfv
PDHB, kfv
PDHX, kfv
PHOX2B, dup_del
PLN, fgs
PRSS1, kfv
PTPN11, kfv

- 16 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
RHD, del a
RHD, maternal
SDH, kfv
SH2D1A, dup_del
SMN1, kfv
TGFBR1, kfv
TGFBR2, kfv
TTR, kfv
TWIST, kfv
TWIST1, dup_del
UBA1, tsa
VKORC1, kfv
81404 81404
Molecular pathology procedure, Level 5 (eg, analysis of 2-5 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 6-10 exons, or characterization of a dynamic mutation disorder/triplet repeat by Southern blot analysis) Molecular pathology procedure, Level 5 (eg, analysis of 2-5 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 6-10 exons, or characterization of a dynamic mutation disorder/triplet repeat by Southern blot analysis)
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
ACADS, tsa
AFF2, characterize
AQP2, fgs
ARX, fgs
AVPR2, fgs
BBS10, fgs
BTD, fgs
C10orf2, fgs
CAV3, fgs
CD40LG, fgs
CLRN1, fgs
COX6B1, fgs
CPT2, fgs
CRX, fgs
CSTB, fgs
CYP1B1, fgs
DMPK, characterize alleles
EGR2, fgs
EMD, Dup_del
EPM2A, fgs
FGF23, fgs
FGFR2, tsa
FGFR3, tsa
FHL1, fgs
FKRP, fgs
FOXG1, fgs
FSHMD1A, ab a
FSHMD1A, hap
FXN, fgs
GH1, fgs
GP1BB, fgs
HBA1_HBA2, dup_del
HBB, fgs
HNF1B, dup_del
HRAS, fgs
HSD11B2, fgs
HSD3B2, fgs

- 17 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
HSPB1, fgs
INS, fgs
KCNJ1, fgs
KCNJ10, fgs
LITAF, fgs
MEFV, fgs
MEN1, dup_del
MMACHC, fgs
MPV17, dup_del
NDP, fgs
NDUFA1, fgs
NDUFAF2, fgs
NDUFS4, fgs
NIPA1, fgs
NLGN4X, dup_del
NPC2, fgs
NR0B1, fgs
PDX1, fgs
PHOX2B, fgs
PIK3CA, tsa
PLP1, Dup_del
PQBP1, Dup_del
PRNP, fgs
PROP1, fgs
PRPH2, fgs
RAF1, tsa
RHO, fgs
RP1, fgs
SCN1B, fgs
SCO2, fgs
SDHC, dup_del
SDHD, fgs
SGCG, dup_del
SH2D1A, fgs
SLC16A2, dup_del
SLC25A20, dup_del
SLC25A4, fgs
SOD1, fgs
SPINK1, fgs
STK11, dup_del
TACO1, fgs
THAP1, fgs
TOR1A, fgs
TP53, 2-5 exons
TTPA, fgs
TTR, fgs
TWIST1, fgs
TYR, fgs
USH1G, fgs
VWF, tsa
ZEB2, dup_del
ZNF41, fgs

- 18 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81405 81405
Molecular pathology procedure, Level 6 (eg, analysis of 6-10 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 11-25 exons, regionally targeted cytogenomic array analysis) Molecular pathology procedure, Level 6 (eg, analysis of 6-10 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 11-25 exons, regionally targeted cytogenomic array analysis)
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
ABCD1, fgs
ACADS, fgs
ACTA2, fgs
ACTC1, fgs
ANKRD1, fgs
APTX, fgs
AR, fgs
ARSA, fgs
BCKDHA, fgs
BCS1L, fgs
BMPR2, dup_del
CASQ2, fgs
CASR, fgs
CDKL5, dup_del
CHRNA4, fgs
CHRNB2, fgs
COX10, fgs
COX15, fgs
CYP11B1, fgs
CYP17A1, fgs
CYP21A2, fgs
DBT, dup_del
DCX, fgs
DES, fgs
DFNB59, fgs
DGUOK, fgs
DHCR7, fgs
EIF2B2, fgs
EMD, fgs
ENG, dup_del
EYA1, dup_del
F9, fgs
FGFR1, fgs
FH, fgs
FKTN, fgs
FTSJ1, dup_del
GABRG2, fgs
GCH1, fgs
GDAP1, fgs
GFAP, fgs
GHR, fgs
GHRHR, fgs
GLA, fgs
HBA1_HBA2, fgs
HNF1A, fgs
HNF1B, fgs
HTRA1, fgs
IDS, fgs
IL2RG, fgs

- 19 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81405
Molecular pathology procedure, Level 6 (eg, analysis of 6-10 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 11-25 exons, regionally targeted cytogenomic array analysis)
ISPD, fgs
KRAS, fgs
LAMP2, fgs
LDLR, dup_del
MMAA, fgs
MMAB, fgs
MPI, fgs
MPV17, fgs
MPZ, fgs
MTM1, dup_del
MYL2, fgs
MYL3, fgs
MYOT, fgs
NDUFS7, fgs
NDUFS8, fgs
NDUFV1, fgs
NEFL, fgs
NF2, dup_del
NLGN3, fgs
NLGN4X, fgs
NPHP1, dup_del
NPHS2, fgs
NSD1, dup_del
OTC, fgs
PAFAH1B1, dup_del
PARK2, dup_del
PCCA, dup_del
PCDH19, fgs
PDHA1, dup_del
PDHB, fgs
PINK1, fgs
PLP1, fgs
POU1F1, fgs
PQBP1, fgs
PRX, fgs
PSEN1, fgs
RAB7A, fgs
RAI1, fgs
REEP1, fgs
RPS19, fgs
RRM2B, fgs
SCO1, fgs
SDHB, fgs
SDHC, fgs
SGCA, fgs
SGCB, fgs
SGCD, fgs
SGCE, dup_del
SGCG, fgs
SHOC2, fgs
SHOX, fgs
SIL1, fgs

- 20 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
SLC16A2, fgs
SLC22A5, fgs
SLC25A20, fgs
SLC2A1, fgs
SMAD4, dup_del
SMN1, fgs
SPAST, dup_del
SPG7, dup_del
SPRED1, fgs
STAT3, tsa
STK11, fgs
SURF1, fgs
TARDBP, fgs
TBX5, fgs
TCF4, dup_del
TGFBR1, fgs
TGFBR2, fgs
THRB, fgs_tsa >5 exons
TK2, fgs
TNNC1, fgs
TNNI3, fgs
TP53, fgs or tsa >5 exons
TPM1, fgs
TSC1, dup_del
TYMP, fgs
WT1, fgs
ZEB2, fgs
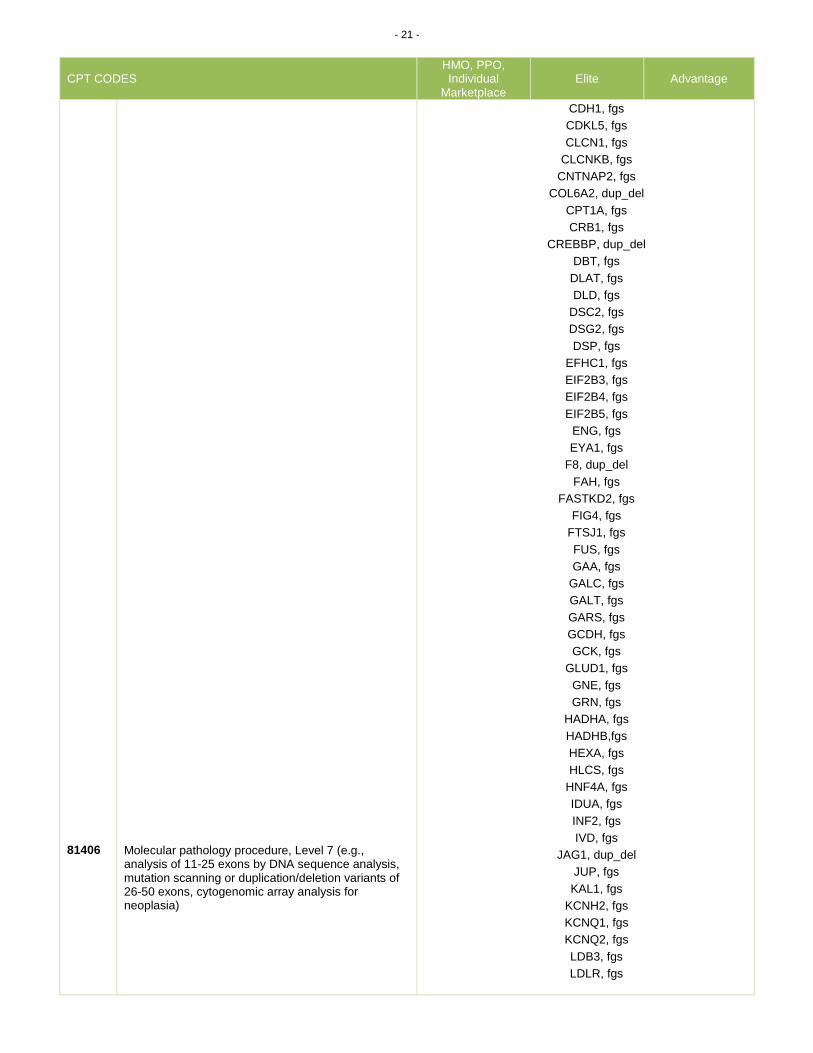
81406 81406
Molecular pathology procedure, Level 7 (e.g., analysis of 11-25 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 26-50 exons, cytogenomic array analysis for neoplasia) Molecular pathology procedure, Level 7 (e.g., analysis of 11-25 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 26-50 exons, cytogenomic array analysis for neoplasia)
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
ACADVL, fgs
ACTN4, fgs
AFG3L2, fgs
AIRE, fgs
ALDH7A1, fgs
ANO5, fgs
APP, fgs
ASS1, fgs
ATL1, fgs
ATP1A2, fgs
ATP7B, fgs
BBS1, fgs
BBS2, fgs
BCKDHB, fgs
BEST1, fgs
BMPR2, fgs
BRAF, fgs
BSCL2, fgs
BTK, fgs
CACNB2, fgs
CAPN3, fgs
CBS, fgs
- 21 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81406
Molecular pathology procedure, Level 7 (e.g., analysis of 11-25 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 26-50 exons, cytogenomic array analysis for neoplasia)
CDH1, fgs
CDKL5, fgs
CLCN1, fgs
CLCNKB, fgs
CNTNAP2, fgs
COL6A2, dup_del
CPT1A, fgs
CRB1, fgs
CREBBP, dup_del
DBT, fgs
DLAT, fgs
DLD, fgs
DSC2, fgs
DSG2, fgs
DSP, fgs
EFHC1, fgs
EIF2B3, fgs
EIF2B4, fgs
EIF2B5, fgs
ENG, fgs
EYA1, fgs
F8, dup_del
FAH, fgs
FASTKD2, fgs
FIG4, fgs
FTSJ1, fgs
FUS, fgs
GAA, fgs
GALC, fgs
GALT, fgs
GARS, fgs
GCDH, fgs
GCK, fgs
GLUD1, fgs
GNE, fgs
GRN, fgs
HADHA, fgs
HADHB,fgs
HEXA, fgs
HLCS, fgs
HNF4A, fgs
IDUA, fgs
INF2, fgs
IVD, fgs
JAG1, dup_del
JUP, fgs
KAL1, fgs
KCNH2, fgs
KCNQ1, fgs
KCNQ2, fgs
LDB3, fgs
LDLR, fgs
- 22 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
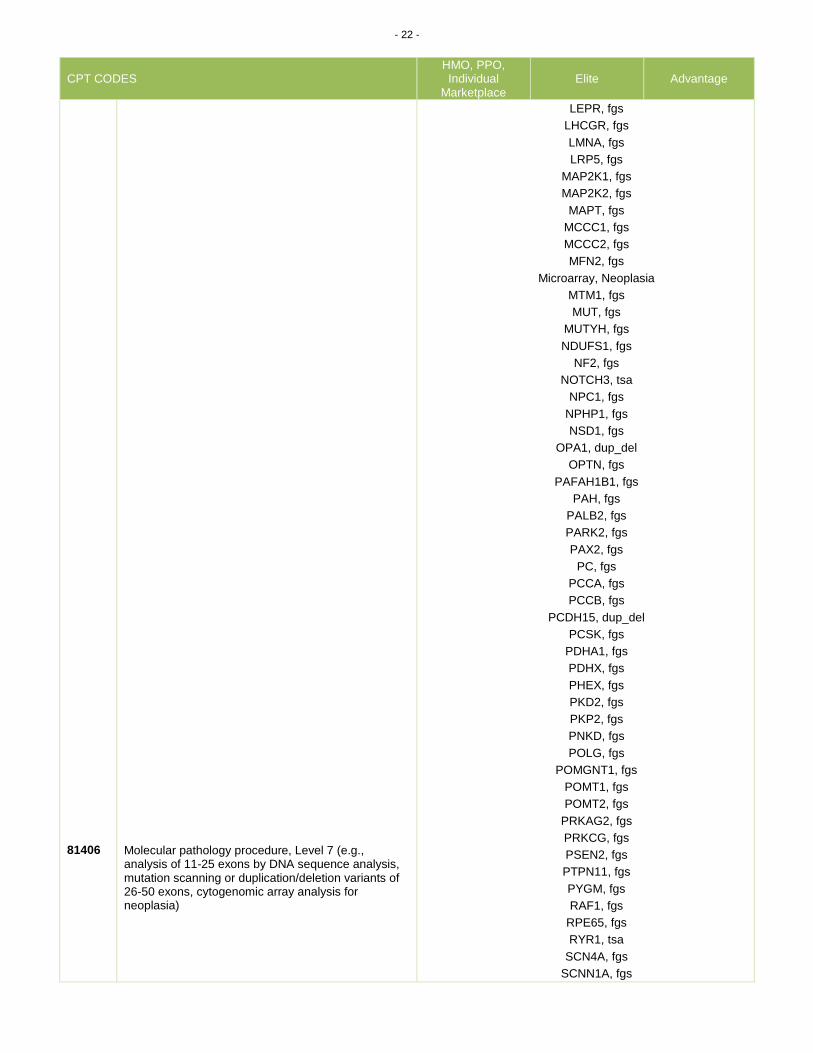
81406
Molecular pathology procedure, Level 7 (e.g., analysis of 11-25 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of 26-50 exons, cytogenomic array analysis for neoplasia)
LEPR, fgs
LHCGR, fgs
LMNA, fgs
LRP5, fgs
MAP2K1, fgs
MAP2K2, fgs
MAPT, fgs
MCCC1, fgs
MCCC2, fgs
MFN2, fgs
Microarray, Neoplasia
MTM1, fgs
MUT, fgs
MUTYH, fgs
NDUFS1, fgs
NF2, fgs
NOTCH3, tsa
NPC1, fgs
NPHP1, fgs
NSD1, fgs
OPA1, dup_del
OPTN, fgs
PAFAH1B1, fgs
PAH, fgs
PALB2, fgs
PARK2, fgs
PAX2, fgs
PC, fgs
PCCA, fgs
PCCB, fgs
PCDH15, dup_del
PCSK, fgs
PDHA1, fgs
PDHX, fgs
PHEX, fgs
PKD2, fgs
PKP2, fgs
PNKD, fgs
POLG, fgs
POMGNT1, fgs
POMT1, fgs
POMT2, fgs
PRKAG2, fgs
PRKCG, fgs
PSEN2, fgs
PTPN11, fgs
PYGM, fgs
RAF1, fgs
RPE65, fgs
RYR1, tsa
SCN4A, fgs
SCNN1A, fgs
- 23 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
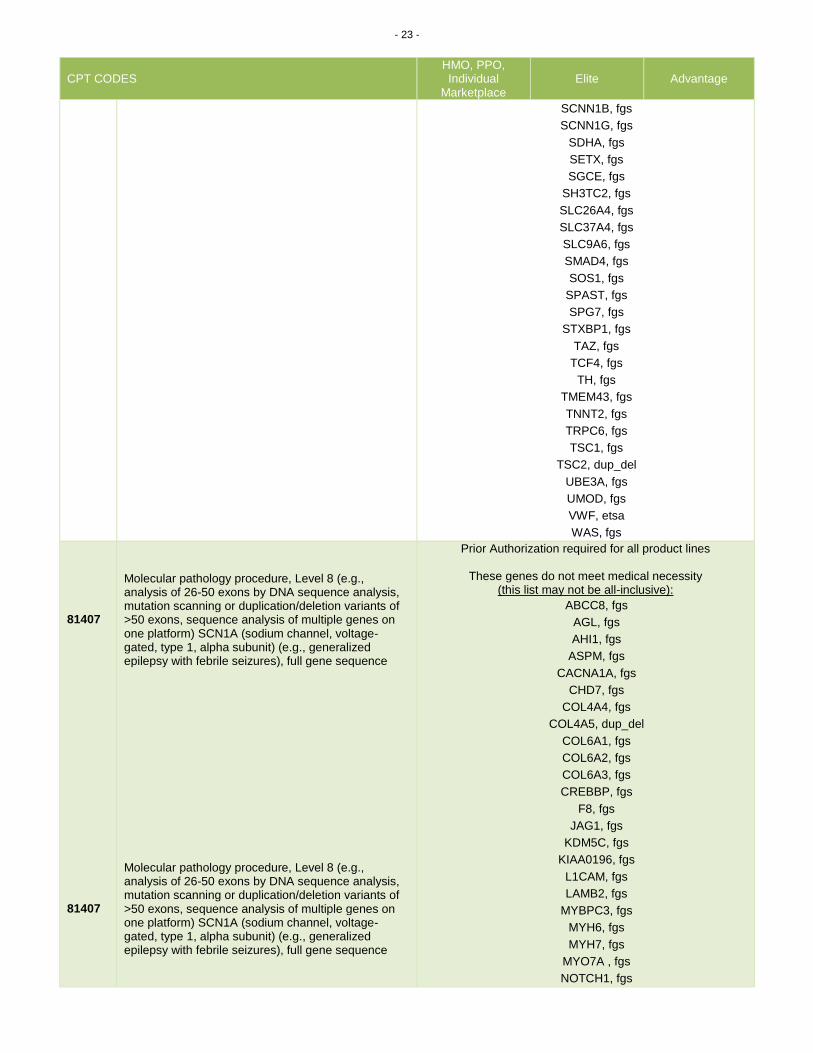
SCNN1B, fgs
SCNN1G, fgs
SDHA, fgs
SETX, fgs
SGCE, fgs
SH3TC2, fgs
SLC26A4, fgs
SLC37A4, fgs
SLC9A6, fgs
SMAD4, fgs
SOS1, fgs
SPAST, fgs
SPG7, fgs
STXBP1, fgs
TAZ, fgs
TCF4, fgs
TH, fgs
TMEM43, fgs
TNNT2, fgs
TRPC6, fgs
TSC1, fgs
TSC2, dup_del
UBE3A, fgs
UMOD, fgs
VWF, etsa
WAS, fgs
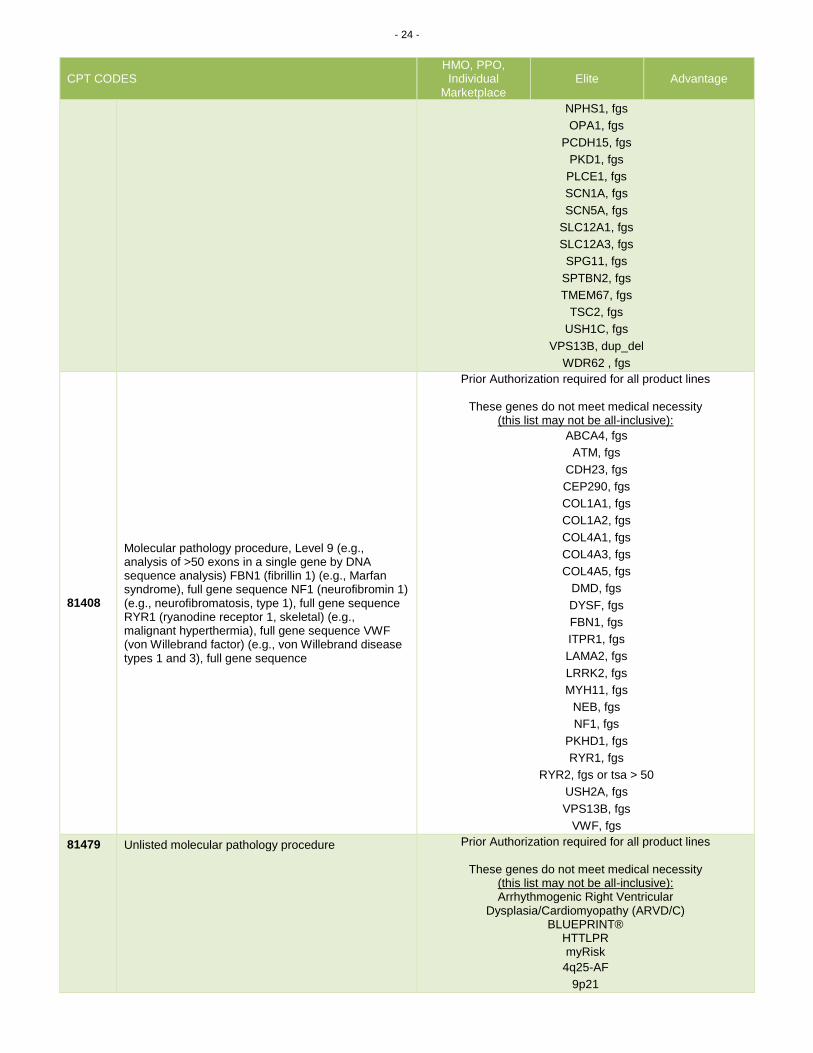
81407 81407
Molecular pathology procedure, Level 8 (e.g., analysis of 26-50 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of >50 exons, sequence analysis of multiple genes on one platform) SCN1A (sodium channel, voltage-gated, type 1, alpha subunit) (e.g., generalized epilepsy with febrile seizures), full gene sequence Molecular pathology procedure, Level 8 (e.g., analysis of 26-50 exons by DNA sequence analysis, mutation scanning or duplication/deletion variants of >50 exons, sequence analysis of multiple genes on one platform) SCN1A (sodium channel, voltage-gated, type 1, alpha subunit) (e.g., generalized epilepsy with febrile seizures), full gene sequence
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
ABCC8, fgs
AGL, fgs
AHI1, fgs
ASPM, fgs
CACNA1A, fgs
CHD7, fgs
COL4A4, fgs
COL4A5, dup_del
COL6A1, fgs
COL6A2, fgs
COL6A3, fgs
CREBBP, fgs
F8, fgs
JAG1, fgs
KDM5C, fgs
KIAA0196, fgs
L1CAM, fgs
LAMB2, fgs
MYBPC3, fgs
MYH6, fgs
MYH7, fgs
MYO7A , fgs
NOTCH1, fgs
- 24 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
NPHS1, fgs
OPA1, fgs
PCDH15, fgs
PKD1, fgs
PLCE1, fgs
SCN1A, fgs
SCN5A, fgs
SLC12A1, fgs
SLC12A3, fgs
SPG11, fgs
SPTBN2, fgs
TMEM67, fgs
TSC2, fgs
USH1C, fgs
VPS13B, dup_del
WDR62 , fgs
81408
Molecular pathology procedure, Level 9 (e.g., analysis of >50 exons in a single gene by DNA sequence analysis) FBN1 (fibrillin 1) (e.g., Marfan syndrome), full gene sequence NF1 (neurofibromin 1) (e.g., neurofibromatosis, type 1), full gene sequence RYR1 (ryanodine receptor 1, skeletal) (e.g., malignant hyperthermia), full gene sequence VWF (von Willebrand factor) (e.g., von Willebrand disease types 1 and 3), full gene sequence
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive):
ABCA4, fgs
ATM, fgs
CDH23, fgs
CEP290, fgs
COL1A1, fgs
COL1A2, fgs
COL4A1, fgs
COL4A3, fgs
COL4A5, fgs
DMD, fgs
DYSF, fgs
FBN1, fgs
ITPR1, fgs
LAMA2, fgs
LRRK2, fgs
MYH11, fgs
NEB, fgs
NF1, fgs
PKHD1, fgs
RYR1, fgs
RYR2, fgs or tsa > 50
USH2A, fgs
VPS13B, fgs
VWF, fgs
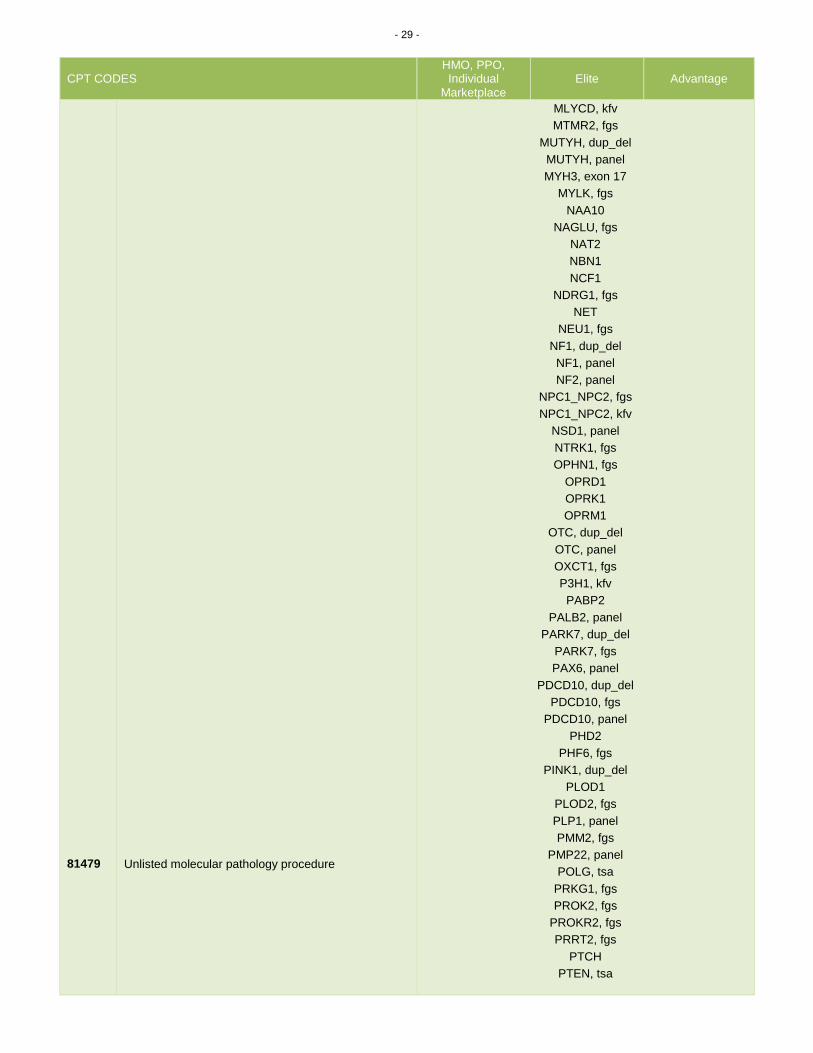
81479
Unlisted molecular pathology procedure
Prior Authorization required for all product lines
These genes do not meet medical necessity (this list may not be all-inclusive): Arrhythmogenic Right Ventricular
Dysplasia/Cardiomyopathy (ARVD/C) BLUEPRINT®
HTTLPR myRisk
4q25-AF
9p21

- 25 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81479
Unlisted molecular pathology procedure
ABCB1, cv
ACADM, fgs
ACADM, panel
ACADVL, d_d
ACADVL, panel
ACSL4, fgs
ACVRL1, d_d
ACVRL1, ENG
ACVRL1, ENG, kfv
ACVRL1, ENG, SMAD4
ADAMTS13
ADRA2A
AFP
AGA
AGXT
ALDOB
ALG6, fgs
ALPL, fgs
ALPL, kfv
ANK3
ANKK1
APC, panel
APP, panel
ARSB, fgs
AR-V7
ARX, panel
ASHKENAZI JEWISH PNL, < 9
ASXL, dup_del
ASXL1, fgs
ASXL1, tsa
ATP7A, fgs
ATRX
AZF
BAALC
BAG3
BARD1
BCOR, tsa
BDNF
BLM, fgs
BMPR1A
BMPR2, panel
BRAF, panel
BSND, fgs
C9ORF72
CACNA1C
CALR
CAPN3, dup_del
CARD11
CASK, fgs
CBL, tsa
CC2D2A, fgs
CCM, panel
- 26 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
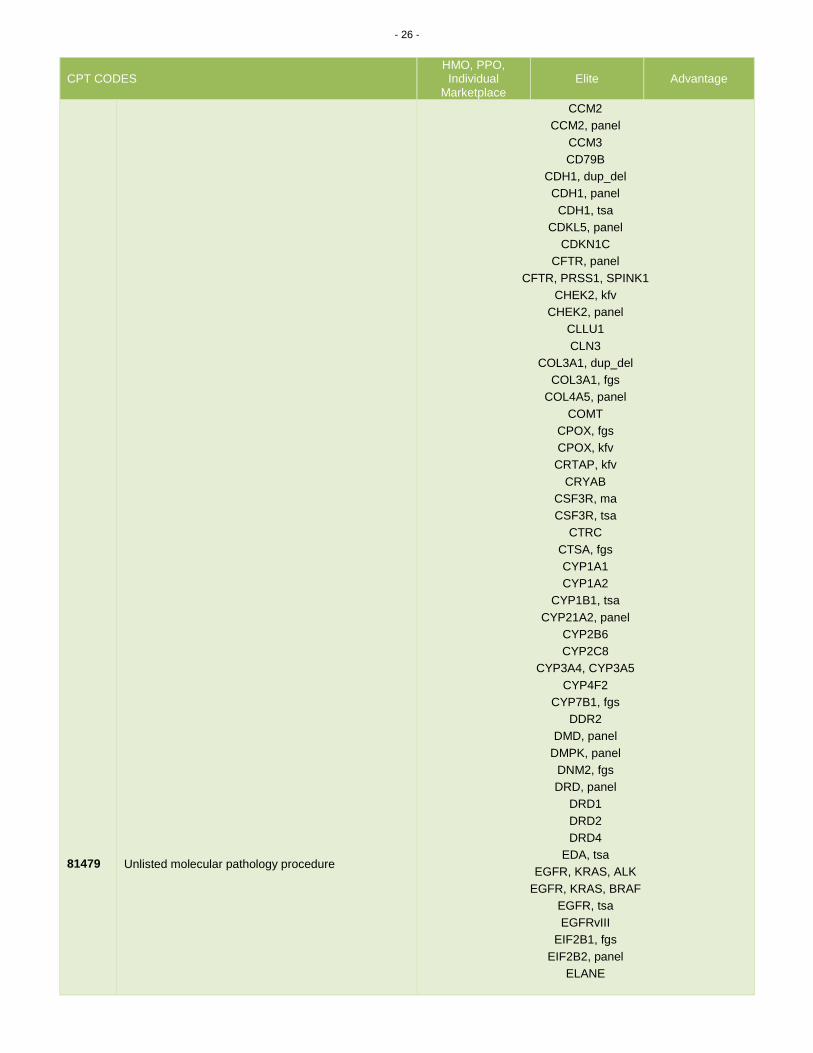
81479
Unlisted molecular pathology procedure
CCM2
CCM2, panel
CCM3
CD79B
CDH1, dup_del
CDH1, panel
CDH1, tsa
CDKL5, panel
CDKN1C
CFTR, panel
CFTR, PRSS1, SPINK1
CHEK2, kfv
CHEK2, panel
CLLU1
CLN3
COL3A1, dup_del
COL3A1, fgs
COL4A5, panel
COMT
CPOX, fgs
CPOX, kfv
CRTAP, kfv
CRYAB
CSF3R, ma
CSF3R, tsa
CTRC
CTSA, fgs
CYP1A1
CYP1A2
CYP1B1, tsa
CYP21A2, panel
CYP2B6
CYP2C8
CYP3A4, CYP3A5
CYP4F2
CYP7B1, fgs
DDR2
DMD, panel
DMPK, panel
DNM2, fgs
DRD, panel
DRD1
DRD2
DRD4
EDA, tsa
EGFR, KRAS, ALK
EGFR, KRAS, BRAF
EGFR, tsa
EGFRvIII
EIF2B1, fgs
EIF2B2, panel
ELANE
- 27 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
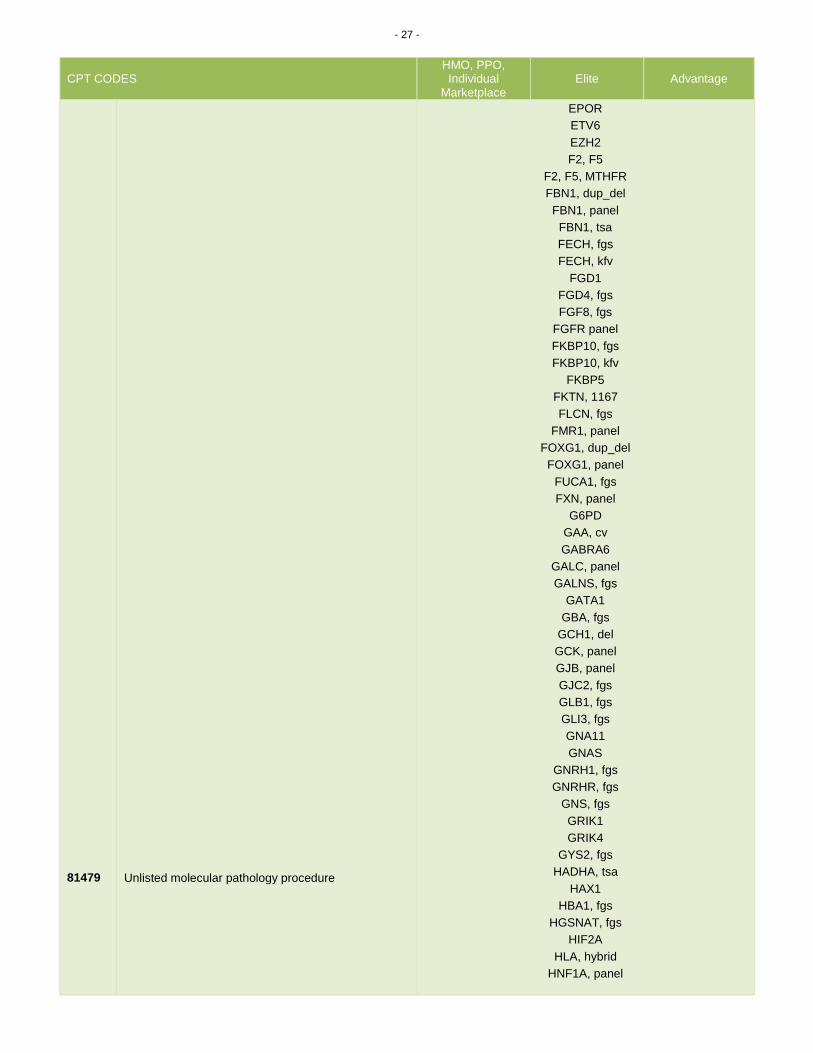
81479
Unlisted molecular pathology procedure
EPOR
ETV6
EZH2
F2, F5
F2, F5, MTHFR
FBN1, dup_del
FBN1, panel
FBN1, tsa
FECH, fgs
FECH, kfv
FGD1
FGD4, fgs
FGF8, fgs
FGFR panel
FKBP10, fgs
FKBP10, kfv
FKBP5
FKTN, 1167
FLCN, fgs
FMR1, panel
FOXG1, dup_del
FOXG1, panel
FUCA1, fgs
FXN, panel
G6PD
GAA, cv
GABRA6
GALC, panel
GALNS, fgs
GATA1
GBA, fgs
GCH1, del
GCK, panel
GJB, panel
GJC2, fgs
GLB1, fgs
GLI3, fgs
GNA11
GNAS
GNRH1, fgs
GNRHR, fgs
GNS, fgs
GRIK1
GRIK4
GYS2, fgs
HADHA, tsa
HAX1
HBA1, fgs
HGSNAT, fgs
HIF2A
HLA, hybrid
HNF1A, panel
- 28 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
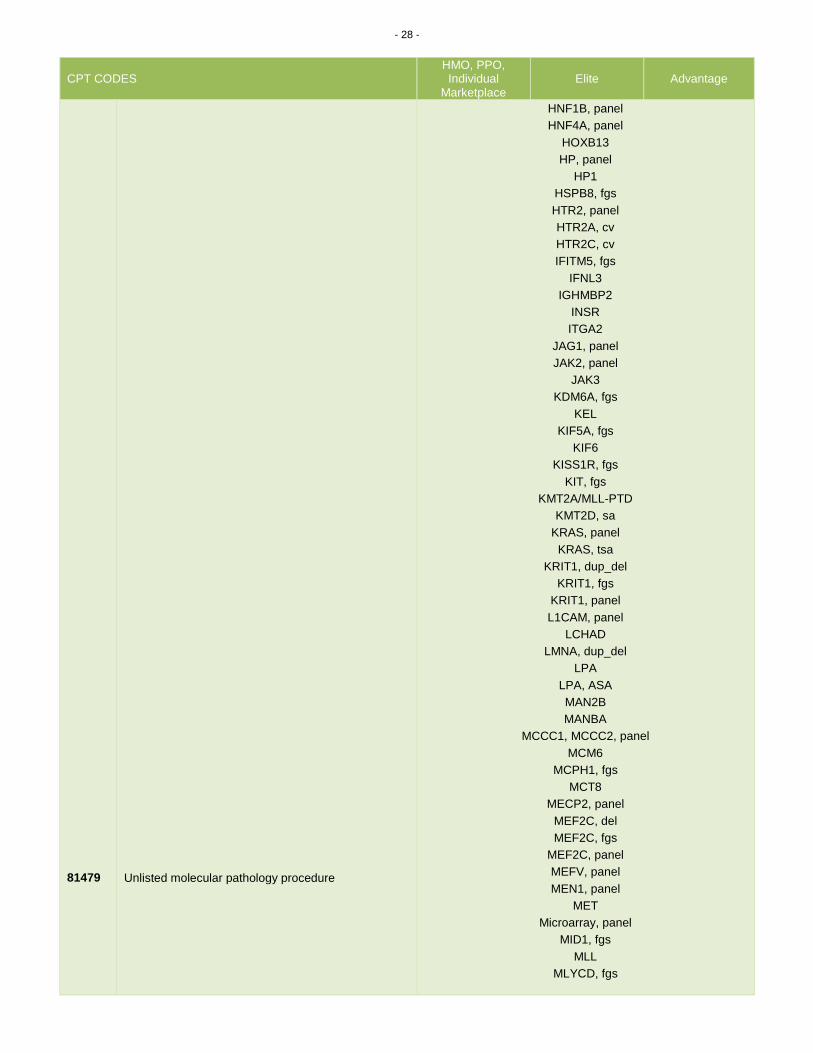
81479
Unlisted molecular pathology procedure
HNF1B, panel
HNF4A, panel
HOXB13
HP, panel
HP1
HSPB8, fgs
HTR2, panel
HTR2A, cv
HTR2C, cv
IFITM5, fgs
IFNL3
IGHMBP2
INSR
ITGA2
JAG1, panel
JAK2, panel
JAK3
KDM6A, fgs
KEL
KIF5A, fgs
KIF6
KISS1R, fgs
KIT, fgs
KMT2A/MLL-PTD
KMT2D, sa
KRAS, panel
KRAS, tsa
KRIT1, dup_del
KRIT1, fgs
KRIT1, panel
L1CAM, panel
LCHAD
LMNA, dup_del
LPA
LPA, ASA
MAN2B
MANBA
MCCC1, MCCC2, panel
MCM6
MCPH1, fgs
MCT8
MECP2, panel
MEF2C, del
MEF2C, fgs
MEF2C, panel
MEFV, panel
MEN1, panel
MET
Microarray, panel
MID1, fgs
MLL
MLYCD, fgs
- 29 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81479
Unlisted molecular pathology procedure
MLYCD, kfv
MTMR2, fgs
MUTYH, dup_del
MUTYH, panel
MYH3, exon 17
MYLK, fgs
NAA10
NAGLU, fgs
NAT2
NBN1
NCF1
NDRG1, fgs
NET
NEU1, fgs
NF1, dup_del
NF1, panel
NF2, panel
NPC1_NPC2, fgs
NPC1_NPC2, kfv
NSD1, panel
NTRK1, fgs
OPHN1, fgs
OPRD1
OPRK1
OPRM1
OTC, dup_del
OTC, panel
OXCT1, fgs
P3H1, kfv
PABP2
PALB2, panel
PARK7, dup_del
PARK7, fgs
PAX6, panel
PDCD10, dup_del
PDCD10, fgs
PDCD10, panel
PHD2
PHF6, fgs
PINK1, dup_del
PLOD1
PLOD2, fgs
PLP1, panel
PMM2, fgs
PMP22, panel
POLG, tsa
PRKG1, fgs
PROK2, fgs
PROKR2, fgs
PRRT2, fgs
PTCH
PTEN, tsa

- 30 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81479
Unlisted molecular pathology procedure
PTPN11, tsa
PTPN22
RAD21, tsa
RAS, panel
RASA1
RB1
REEP1, dup_del
RhCE
RPL19
RPL26
RPS6KA3, fgs
RRM1
RUNX1, tsa
SBDS
SBF2, fgs
SCA1
SCA10
SCA12
SCA13, tsa
SCA14
SCA17
SCA2
SCA5
SCA6
SCA7
SCA8
SCN1A, dup_del
SCN1A, panel
SDH, kfv
SDH, panel
SDHAF2, fgs
SDHB, panel
SDHC, panel
SDHD, panel
SEPT9, fgs
SEPT9, panel
SERPINA1, fgs
SERPINA1, panel
SERPINA10, rs2232698
SERPING1, kfv
SETBP1, tsa
SF3B1, tsa
SFTPB
SFTPC
SGCA, dup_del
SGSH, fgs
SHANK2, fgs
SHANK3
shox, panel
SLC22A5, dup_del
SLC22A5, panel
SLC25A13, fgs

- 31 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81479
Unlisted molecular pathology procedure
SLC47A1
SLC6A4
SLC6A8, fgs
SLCO1B1, tsa
SLCO2A1, kfv
SMAD3, fgs
SMAD3, kfv
SMAD4, kfv
SMAD4, panel
SMC1A, fgs
SMC3, tsa
SMN1_SMN2, fgs
SMN1_SMN2, panel
SMPD1, fgs
SNCA, dup_del
SNCA, fgs
SPAST, panel
SPG21, kfv
SPRED1, dup_del
SPTLC1, fgs
SPTLC2, fgs
SRSF2, tsa
STAG2, tsa
STAR
STK11, panel
STR, panel
SULT4A1
SYNGAP1, fgs
SYT, panel
SYT-SSX, ta
TACI, fgs
TACR3, fgs
TBX5, panel
TERT/TERC
TET2, fgs
TET2, tsa
TGFB2, kfv
TGFBR1/TGFBR2
TMEM216, cv
TMEM216, fgs
TP53, panel
TRB, panel
TRPV4, fgs
TSC1, TSC2
U2AF1, tsa
UBQL1
UBQLN2
UGT2B15, tsa
UGT2B7, tsa
VCP
VEGF, fgs
VEGF, tsa

- 32 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
VEGFR2
VWF, D1472H
VWF, panel
WNK1, fgs
WRAP53
WT1, tsa
YARS, fgs
ZAP70, ma
ZFYVE26, fgs
ZRSR2, tsa
Molecular Multianalyte Assays (MAA)
81410
Aortic dysfunction or dilation (eg, Marfan syndrome, Loeys Dietz syndrome, Ehler Danlos syndrome type IV, arterial tortuosity syndrome); genomic sequence analysis panel, must include sequencing of at least 9 genes, including FBN1, TGFBR1, TGFBR2, COL3A1, MYH11, ACTA2, SLC2A10, SMAD3, and MYLK
Non-covered Non-covered Prior
Authorization required
81411
Aortic dysfunction or dilation (eg, Marfan syndrome, Loeys Dietz syndrome, Ehler Danlos syndrome type IV, arterial tortuosity syndrome); duplication/deletion analysis panel, must include analyses for TGFBR1, TGFBR2, MYH11, and COL3A1
Non-covered Non-covered Prior
Authorization required
81412
Ashkenazi Jewish associated disorders (eg, Bloom syndrome, Canavan disease, cystic fibrosis, familial dysautonomia, Fanconi anemia group C, Gaucher disease, Tay-Sachs disease), genomic sequence analysis panel, must include sequencing of at least 9 genes, including ASPA, BLM, CFTR, FANCC, GBA, HEXA, IKBKAP, MCOLN1, and SMPD1
Non-covered Non-covered Prior
Authorization required
81413
Cardiac ion channelopathies (eg, Brugada syndrome, long QT syndrome, short QT syndrome, catecholaminergic polymorphic ventricular tachycardia); genomic sequence analysis panel, must include sequencing of at least 10 genes, including ANK2, CASQ2, CAV3, KCNE1, KCNE2, KCNH2, KCNJ2, KCNQ1, RYR2, and SCN5A (Effective 01/01/17 new code)
PG0280 Genetic Testing for Cardiac Conditions
81414
Cardiac ion channelopathies (eg, Brugada syndrome, long QT syndrome, short QT syndrome, catecholaminergic polymorphic ventricular tachycardia); duplication/deletion gene analysis panel, must include analysis of at least 2 genes,
PG0280 Genetic Testing for Cardiac Conditions

- 33 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
including KCNH2 and KCNQ1 (Effective 01/01/17 new code)
81415 Exome (eg, unexplained constitutional or heritable disorder or syndrome); sequence analysis
Non-covered Non-covered Prior
Authorization required
81416
Exome (eg, unexplained constitutional or heritable disorder or syndrome); sequence analysis, each comparator exome (eg, parents, siblings) (List separately in addition to code for primary procedure)
Non-covered Non-covered Prior
Authorization required
81417
Exome (eg, unexplained constitutional or heritable disorder or syndrome); re-evaluation of previously obtained exome sequence (eg, updated knowledge or unrelated condition/syndrome)
Non-covered Non-covered Prior
Authorization required
81420
Fetal chromosomal aneuploidy (eg, trisomy 21, monosomy X) genomic sequence analysis panel, circulating cell-free fetal DNA in maternal blood, must include analysis of chromosomes 13, 18, and 21
PG0287 Cell-Free DNA Tests For Fetal Aneuploidy
81422
Fetal chromosomal microdeletion(s) genomic sequence analysis (eg. DiGeorge syndrome, Cri-du-chat syndrome), circulating cell-free fetal DNA in maternal blood (Effective 01/01/17 new code)
PG0287 Cell-Free DNA Tests For Fetal Aneuploidy
81425 Genome (eg, unexplained constitutional or heritable disorder or syndrome); sequence analysis
Non-covered Non-covered Prior
Authorization required
81426
Genome (eg, unexplained constitutional or heritable disorder or syndrome); sequence analysis, each comparator genome (eg, parents, siblings) (List separately in addition to code for primary procedure)
Non-covered Non-covered Prior
Authorization required
81427
Genome (eg, unexplained constitutional or heritable disorder or syndrome); re-evaluation of previously obtained genome sequence (eg, updated knowledge or unrelated condition/syndrome)
Non-covered Non-covered Prior
Authorization required
81430
Hearing loss (eg, nonsyndromic hearing loss, Usher syndrome, Pendred syndrome); genomic sequence analysis panel, must include sequencing of at least 60 genes, including CDH23, CLRN1, GJB2, GPR98, MTRNR1, MYO7A, MYO15A, PCDH15, OTOF, SLC26A4, TMC1, TMPRSS3, USH1C, USH1G, USH2A, and WFS1
Non-covered Non-covered Prior
Authorization required
81431
Hearing loss (eg, nonsyndromic hearing loss, Usher syndrome, Pendred syndrome); duplication/deletion analysis panel, must include copy number analyses for STRC and DFNB1 deletions in GJB2 and GJB6 genes
Non-covered Non-covered Prior
Authorization required
81432
Hereditary breast cancer-related disorders (eg, hereditary breast cancer, hereditary ovarian cancer, hereditary endometrial cancer); genomic sequence analysis panel, must include sequencing of at least 10 genes, always including BRCA1, BRCA2, CDH1, MLH1, MSH2, MSH6, PALB2, PTEN, STK11, and TP53
PG0067 Genetic Testing for Breast and Ovarian Cancers
81433
Hereditary breast cancer-related disorders (eg, hereditary breast cancer, hereditary ovarian cancer, hereditary endometrial cancer); duplication/deletion analysis panel, must include analyses for BRCA1, BRCA2, MLH1, MSH2, and STK11
PG0067 Genetic Testing for Breast and Ovarian Cancers
81434
Hereditary retinal disorders (eg, retinitis pigmentosa, Leber congenital amaurosis, cone-rod dystrophy), genomic sequence analysis panel, must include sequencing of at least 15 genes, including ABCA4, CNGA1, CRB1, EYS, PDE6A, PDE6B, PRPF31, PRPH2, RDH12, RHO, RP1, RP2, RPE65, RPGR, and USH2A
Non-covered Non-covered Prior
Authorization required

- 34 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
81435
Hereditary colon cancer disorders (eg, Lynch syndrome, PTEN hamartoma syndrome, Cowden syndrome, familial adenomatosis polyposis); genomic sequence analysis panel, must include analysis of at least 10 genes, including APC, BMPR1A, CDH1, MLH1, MSH2, MSH6, MUTYH, PTEN, SMAD4 and STK11
Prior Authorization
required
Prior Authorization
required
Prior Authorization
required
81436
Hereditary colon cancer disorders (eg, Lynch syndrome, PTEN hamartoma syndrome, Cowden syndrome, familial adenomatosis polyposis); duplication/deletion gene analysis panel, must include analysis of at least 5 genes, including MLH1, MSH2, EPCAM, SMAD4, and STK11
Prior Authorization
required
Prior Authorization
required
Prior Authorization
required
81437
Hereditary neuroendocrine tumor disorders (eg, medullary thyroid carcinoma, parathyroid carcinoma, malignant pheochromocytoma or paraganglioma; genomic sequence analysis panel, must include sequencing of at least 6 genes, including MAX, SDHB, SDHC, SDHD, TMEM127, and VHL
Prior Authorization NOT required
Prior Authorization NOT required
Prior Authorization NOT required
81438
Hereditary neuroendocrine tumor disorders (eg, medullary thyroid carcinoma, parathyroid carcinoma, malignant pheochromocytoma or paraganglioma; duplication/deletion analysis panel, must include analyses for SDHB, SDHC, SDHD, and VHL
Non-covered Non-covered Prior
Authorization required
81439
Hereditary cardiomyopathy (eg, hypertrophic cardiomyopathy, dilated cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy), genomic sequence analysis panel, must include sequencing of at least 5 cardiomyopathy-related genes (eg, DSG2, MYBPC3, MYH7, PKP2, TTN)
PG0280 Genetic Testing for Cardiac Conditions
81440
Nuclear encoded mitochondrial genes (eg, neurologic or myopathic phenotypes), genomic sequence panel, must include analysis of at least 100 genes, including BCS1L, C10orf2, COQ2, COX10, DGUOK, MPV17, OPA1, PDSS2, POLG, POLG2, RRM2B, SCO1, SCO2, SLC25A4, SUCLA2, SUCLG1, TAZ, TK2, and TYMP
Non-covered Non-covered Prior
Authorization required
81442
Noonan spectrum disorders (eg, Noonan syndrome, cardio-facio-cutaneous syndrome, Costello syndrome, LEOPARD syndrome, Noonan-like syndrome), genomic sequence analysis panel, must include sequencing of at least 12 genes, including BRAF, CBL, HRAS, KRAS, MAP2K1, MAP2K2, NRAS, PTPN11, RAF1, RIT1, SHOC2, and SOS1
Non-covered Non-covered Prior
Authorization required
81445
Targeted genomic sequence analysis panel, solid organ neoplasm, DNA analysis, and RNA analysis when performed, 5-50 genes (eg, ALK, BRAF, CDKN2A, EGFR, ERBB2, KIT, KRAS, NRAS, MET, PDGFRA, PDGFRB, PGR, PIK3CA, PTEN, RET), interrogation for sequence variants and copy number variants or rearrangements, if performed
PG0067 Genetic Testing for Breast and Ovarian Cancers
81448
Hereditary peripheral neuropathies (eg, Charcot-Marie-Tooth, spastic paraplegia), genomic sequence analysis panel, must include sequencing of at least 5 peripheral neuropathy-related genes (eg, BSCL2, GJB1, MFN2, MPZ, REEP1, SPAST, SPG11, SPTLC1) (Effective 01/01/2018 new code)
Prior Authorization
required
Prior Authorization
required
Prior Authorization
required
81450
Targeted genomic sequence analysis panel, hematolymphoid neoplasm or disorder, DNA analysis, and RNA analysis when performed, 5-50 genes (eg, BRAF, CEBPA, DNMT3A, EZH2, FLT3, IDH1, IDH2, JAK2, KRAS, KIT, MLL, NRAS, NPM1, NOTCH1), interrogation for sequence variants, and copy number variants or rearrangements, or isoform expression or
Prior Authorization required
Prior Authorization required
Prior Authorization
required

- 35 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
mRNA expression levels, if performed
81455
Targeted genomic sequence analysis panel, solid organ or hematolymphoid neoplasm, DNA analysis, and RNA analysis when performed, 51 or greater genes (eg, ALK, BRAF, CDKN2A, CEBPA, DNMT3A, EGFR, ERBB2, EZH2, FLT3, IDH1, IDH2, JAK2, KIT, KRAS, MLL, NPM1, NRAS, MET, NOTCH1, PDGFRA, PDGFRB, PGR, PIK3CA, PTEN, RET), interrogation for sequence variants and copy number variants or rearrangements, if performed
PG0067 Genetic Testing for Breast and Ovarian Cancers
81460
Whole mitochondrial genome (eg, Leigh syndrome, mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes [MELAS], myoclonic epilepsy with ragged-red fibers [MERFF], neuropathy, ataxia, and retinitis pigmentosa [NARP], Leber hereditary optic neuropathy [LHON]), genomic sequence, must include sequence analysis of entire mitochondrial genome with heteroplasmy detection
Non-covered Non-covered Prior
Authorization required
81465
Whole mitochondrial genome large deletion analysis panel (eg, Kearns-Sayre syndrome, chronic progressive external ophthalmoplegia), including heteroplasmy detection, if performed
Non-covered Non-covered Prior
Authorization required
81470
X-linked intellectual disability (XLID) (eg, syndromic and non-syndromic XLID); genomic sequence analysis panel, must include sequencing of at least 60 genes, including ARX, ATRX, CDKL5, FGD1, FMR1, HUWE1, IL1RAPL, KDM5C, L1CAM, MECP2, MED12, MID1, OCRL, RPS6KA3, and SLC16A2
Non-covered Non-covered Prior
Authorization required
81471
X-linked intellectual disability (XLID) (eg, syndromic and non-syndromic XLID); duplication/deletion gene analysis, must include analysis of at least 60 genes, including ARX, ATRX, CDKL5, FGD1, FMR1, HUWE1, IL1RAPL, KDM5C, L1CAM, MECP2, MED12, MID1, OCRL, RPS6KA3, and SLC16A2
Non-covered Non-covered Prior
Authorization required
Multianalyte Assays with Algorithmic Analyses (MAAA)
81490
Autoimmune (rheumatoid arthritis), analysis of 12 biomarkers using immunoassays, utilizing serum, prognostic algorithm reported as a disease activity score
PG0362 Vectra® DA
81493
Coronary artery disease, mRNA, gene expression profiling by real-time RT-PCR of 23 genes, utilizing whole peripheral blood, algorithm reported as a risk score
PG0363 CORUS® CAD
81500 Oncology (ovarian), biochemical assays of two proteins (CA-125 and HE-4), utilizing serum, with menopausal status, algorithm reported as a risk score
Non-covered Non-covered Non-covered
81503
Oncology (ovarian), biochemical assays of five proteins (CA-125, apolipoprotein A1, beta-2 microglobulin, transferring, and pre-albumin), utilizing serum, algorithm reported as a risk score
Non-covered Non-covered Non-covered
81504
Oncology (tissue of origin), microarray gene expression profiling of > 2000 genes, utilizing formalin-fixed paraffin-embedded tissue, algorithm reported as tissue similarity scores
Prior Authorization required
Prior Authorization required
Non-covered
81506
Endocrinology (type 2 diabetes), biochemical assays of seven analytes (glucose, HbA1c, insulin, hs-CRP, adiponectin, ferritin, interleukin 2-receptor alpha), utilizing serum or plasma, algorithm reporting a risk score
Non-covered Non-covered Non-covered
81507
Fetal aneuploidy (trisomy 21, 18, and 13) DNA sequence analysis of selected regions using maternal plasma, algorithm reported as a risk score for each trisomy
PG0287 Cell-Free DNA Tests For Fetal Aneuploidy
81508 Fetal congenital abnormalities, biochemical assays of Non-covered Non-covered Non-covered

- 36 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
two proteins (PAPP-A, hCG [any form]), utilizing maternal serum, algorithm reported as a risk score
81509
Fetal congenital abnormalities, biochemical assays of three proteins (PAPP-A, hCG [any form], DIA), utilizing maternal serum, algorithm reported as a risk score
Non-covered Non-covered Non-covered
81510 Fetal congenital abnormalities, biochemical assays of three analytes (AFP, uE3, hCG [any form]), utilizing maternal serum, algorithm reported as a risk score
Non-covered Non-covered Non-covered
81511
Fetal congenital abnormalities, biochemical assays of four analytes (AFP, uE3, hCG [any form], DIA) utilizing maternal serum, algorithm reported as a risk score (may include additional results from previous biochemical testing)
Non-covered Non-covered Non-covered
81512
Fetal congenital abnormalities, biochemical assays of five analytes (AFP, uE3, total hCG, hyperglycosylated hCG, DIA) utilizing maternal serum, algorithm reported as a risk score
Non-covered Non-covered Non-covered
81519
Oncology (breast), mRNA, gene expression profiling by real-time RT-PCR of 21 genes, utilizing formalin-fixed paraffin embedded tissue, algorithm reported as recurrence score
PG0301 Genetic Expression Assays for Breast Cancer Prognosis
81520
Oncology (breast), mRNA gene expression profiling by hybrid capture of 58 genes (50 content and 8 housekeeping), utilizing formalin-fixed paraffin embedded tissue, algorithm reported as a recurrence risk score (Effective 01/01/2018 new code)
PG0301 Genetic Expression Assays for Breast Cancer Prognosis
81521
Oncology (breast), mRNA, microarray gene expression profiling of 70 content genes and 465 housekeeping genes, utilizing fresh frozen or formalin-fixed paraffin embedded tissue, algorithm reported as index related to risk of distant metastasis (Effective 01/01/2018 new code)
PG0301 Genetic Expression Assays for Breast Cancer Prognosis
81525
Oncology (colon), mRNA, gene expression profiling by real-time RT-PCR of 12 genes (7 content and 5 housekeeping), utilizing formalin-fixed paraffin-embedded tissue, algorithm reported as a recurrence score
PG0357 Gene Expression Profiling for Colorectal Cancer
81528
Oncology (colorectal) screening, quantitative real-time target and signal amplification of 10 DNA markers (KRAS mutations, promoter methylation of NDRG4 and BMP3) and fecal hemoglobin, utilizing stool, algorithm reported as a positive or negative result
PG0065 Colorectal Cancer Screening
81535
Oncology (gynecologic), live tumor cell culture and chemotherapeutic response by DAPI stain and morphology, predictive algorithm reported as a drug response score; first single drug or drug combination
PG0122 In Vitro Chemoresistance and Chemosensitivity Assays
81536
Oncology (gynecologic), live tumor cell culture and chemotherapeutic response by DAPI stain and morphology, predictive algorithm reported as a drug response score; each additional single drug or drug combination (List separately in addition to code for primary procedure)
PG0122 In Vitro Chemoresistance and Chemosensitivity Assays
81538
Oncology (lung), mass spectrometric 8-protein signature, including amyloid A, utilizing serum, prognostic and predictive algorithm reported as good versus poor overall survival
PG0111 VeriStrat®
81539
Oncology (high-grade prostate cancer), biochemical assay of four proteins (Total PSA, Free PSA, Intact PSA and human kallikrein-2 [hK2]), utilizing plasma or serum, prognostic algorithm reported as a probability score
PG0367 Gene Expression Analysis for Prostate Cancer
81540 Oncology (tumor of unknown origin), mRNA, gene PG0364 Cancer Type ID
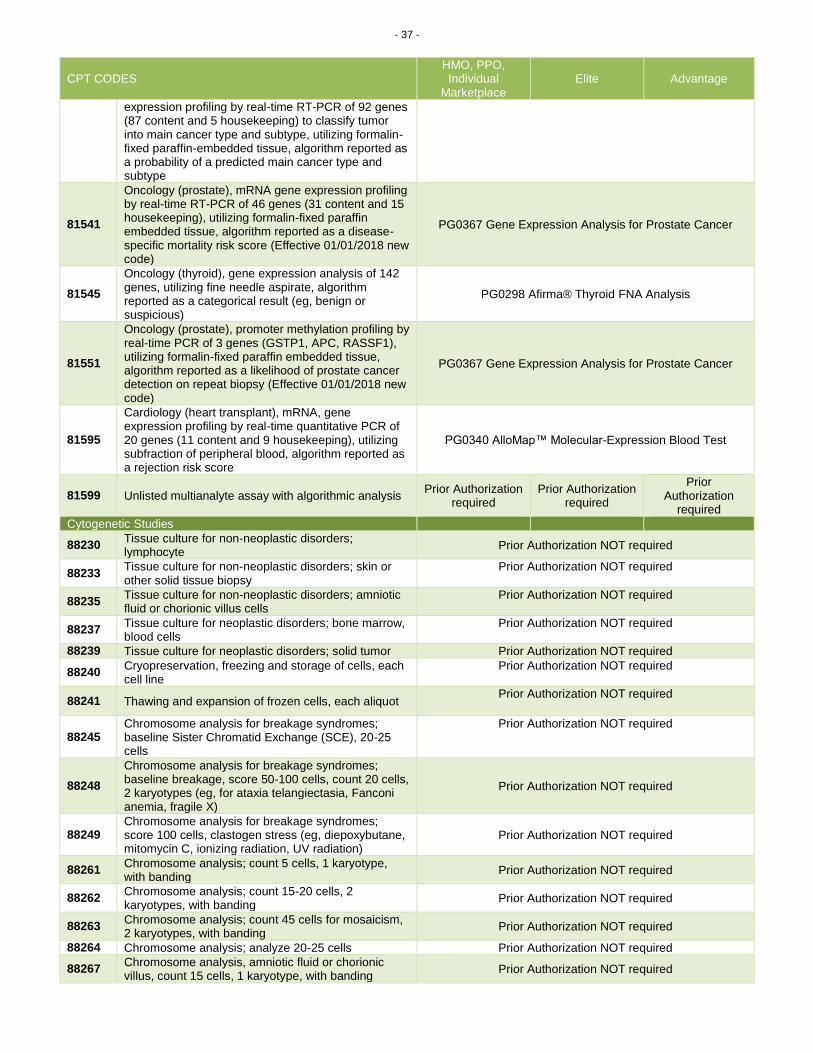
- 37 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
expression profiling by real-time RT-PCR of 92 genes (87 content and 5 housekeeping) to classify tumor into main cancer type and subtype, utilizing formalin-fixed paraffin-embedded tissue, algorithm reported as a probability of a predicted main cancer type and subtype
81541
Oncology (prostate), mRNA gene expression profiling by real-time RT-PCR of 46 genes (31 content and 15 housekeeping), utilizing formalin-fixed paraffin embedded tissue, algorithm reported as a disease-specific mortality risk score (Effective 01/01/2018 new code)
PG0367 Gene Expression Analysis for Prostate Cancer
81545
Oncology (thyroid), gene expression analysis of 142 genes, utilizing fine needle aspirate, algorithm reported as a categorical result (eg, benign or suspicious)
PG0298 Afirma® Thyroid FNA Analysis
81551
Oncology (prostate), promoter methylation profiling by real-time PCR of 3 genes (GSTP1, APC, RASSF1), utilizing formalin-fixed paraffin embedded tissue, algorithm reported as a likelihood of prostate cancer detection on repeat biopsy (Effective 01/01/2018 new code)
PG0367 Gene Expression Analysis for Prostate Cancer
81595
Cardiology (heart transplant), mRNA, gene expression profiling by real-time quantitative PCR of 20 genes (11 content and 9 housekeeping), utilizing subfraction of peripheral blood, algorithm reported as a rejection risk score
PG0340 AlloMap™ Molecular-Expression Blood Test
81599 Unlisted multianalyte assay with algorithmic analysis Prior Authorization
required Prior Authorization
required
Prior Authorization
required
Cytogenetic Studies
88230 Tissue culture for non-neoplastic disorders; lymphocyte
Prior Authorization NOT required
88233 Tissue culture for non-neoplastic disorders; skin or other solid tissue biopsy
Prior Authorization NOT required
88235 Tissue culture for non-neoplastic disorders; amniotic fluid or chorionic villus cells
Prior Authorization NOT required
88237 Tissue culture for neoplastic disorders; bone marrow, blood cells
Prior Authorization NOT required
88239 Tissue culture for neoplastic disorders; solid tumor Prior Authorization NOT required
88240 Cryopreservation, freezing and storage of cells, each cell line
Prior Authorization NOT required
88241 Thawing and expansion of frozen cells, each aliquot Prior Authorization NOT required
88245 Chromosome analysis for breakage syndromes; baseline Sister Chromatid Exchange (SCE), 20-25 cells
Prior Authorization NOT required
88248
Chromosome analysis for breakage syndromes; baseline breakage, score 50-100 cells, count 20 cells, 2 karyotypes (eg, for ataxia telangiectasia, Fanconi anemia, fragile X)
Prior Authorization NOT required
88249 Chromosome analysis for breakage syndromes; score 100 cells, clastogen stress (eg, diepoxybutane, mitomycin C, ionizing radiation, UV radiation)
Prior Authorization NOT required
88261 Chromosome analysis; count 5 cells, 1 karyotype, with banding
Prior Authorization NOT required
88262 Chromosome analysis; count 15-20 cells, 2 karyotypes, with banding
Prior Authorization NOT required
88263 Chromosome analysis; count 45 cells for mosaicism, 2 karyotypes, with banding
Prior Authorization NOT required
88264 Chromosome analysis; analyze 20-25 cells Prior Authorization NOT required
88267 Chromosome analysis, amniotic fluid or chorionic villus, count 15 cells, 1 karyotype, with banding
Prior Authorization NOT required

- 38 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
88269 Chromosome analysis, in situ for amniotic fluid cells, count cells from 6-12 colonies, 1 karyotype, with banding
Prior Authorization NOT required
88271 Molecular cytogenetics; DNA probe, each (eg, FISH) PG0375 Molecular Cytogenetic Testing
Limit of 25 units/365 days
Prior Authorization NOT required
88272 Molecular cytogenetics; chromosomal in situ hybridization, analyze 3-5 cells (eg, for derivatives and markers)
Prior Authorization NOT required
88273 Molecular cytogenetics; chromosomal in situ hybridization, analyze 10-30 cells (eg, for microdeletions)
Prior Authorization NOT required
88274 Molecular cytogenetics; interphase in situ hybridization, analyze 25-99 cells
Prior Authorization NOT required
88275 Molecular cytogenetics; interphase in situ hybridization, analyze 100-300 cells
Prior Authorization NOT required
88280 Chromosome analysis; additional karyotypes, each study
Prior Authorization NOT required
88283 Chromosome analysis; additional specialized banding technique (eg, NOR, C-banding)
Prior Authorization NOT required
88285 Chromosome analysis; additional cells counted, each study
Prior Authorization NOT required
88289 Chromosome analysis; additional high resolution study
Prior Authorization NOT required
88291 Cytogenetics and molecular cytogenetics, interpretation and report
Prior Authorization NOT required
88299 Unlisted cytogenetic study Prior Authorization NOT required Proprietary Laboratory Analyses (PLA) Codes
0001U
Red blood cell antigen typing, DNA, human erythrocyte antigen gene analysis of 35 antigens from 11 blood groups, utilizing whole blood, common RBC alleles reported
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0002U
Oncology (colorectal), quantitative assessment of three urine metabolites (ascorbic acid, succinic acid and carnitine) by liquid chromatography with tandem mass spectrometry (LC-MS/MS) using multiple reaction monitoring acquisition, algorithm reported as likelihood of adenomatous polyps
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0003U
Oncology (ovarian) biochemical assays of five proteins (apolipoprotein A-1, CA 125 II, follicle stimulating hormone, human epididymis protein 4, transferrin), utilizing serum, algorithm reported as a likelihood score
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0004U
Infectious disease (bacterial), DNA, 27 resistance genes, PCR amplification and probe hybridization in microarray format (molecular detection and identification of AmpC, carbapenemase and ESBL coding genes), bacterial culture colonies, report of genes detected or not detected, per isolate
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0005U Oncology (prostate) gene expression profile by real-time RT-PCR of 3 genes (ERG, PCA3, and SPDEF), urine, algorithm reported as risk score
PG0417 Proprietary Laboratory Analyses (PLA) Codes PG0367 Gene Expression Analysis for Prostate Cancer
0006U
Prescription drug monitoring, 120 or more drugs and substances, definitive tandem mass spectrometry with chromatography, urine, qualitative report of presence (including quantitative levels, when detected) or absence of each drug or substance with description and severity of potential interactions, with identified substances, per date of service
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0007U
Drug test(s), presumptive, with definitive confirmation of positive results, any number of drug classes, urine, includes specimen verification including DNA authentication in comparison to buccal DNA, per date of service
PG0417 Proprietary Laboratory Analyses (PLA) Codes
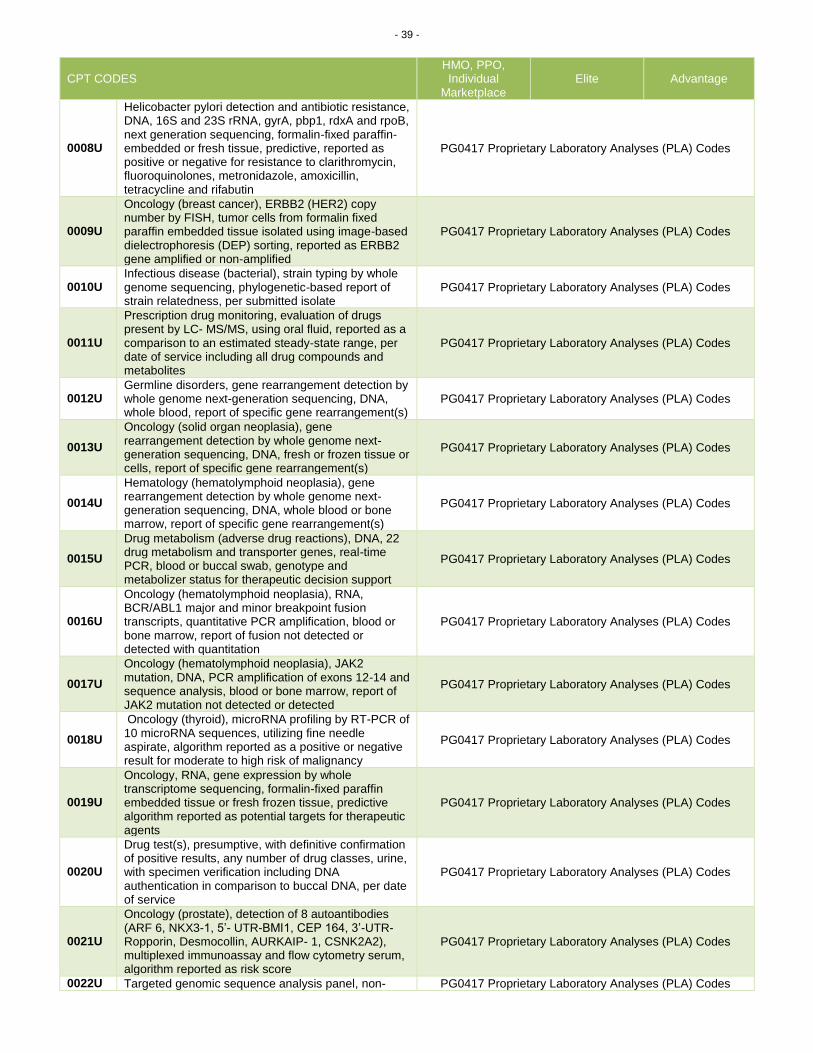
- 39 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
0008U
Helicobacter pylori detection and antibiotic resistance, DNA, 16S and 23S rRNA, gyrA, pbp1, rdxA and rpoB, next generation sequencing, formalin-fixed paraffin-embedded or fresh tissue, predictive, reported as positive or negative for resistance to clarithromycin, fluoroquinolones, metronidazole, amoxicillin, tetracycline and rifabutin
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0009U
Oncology (breast cancer), ERBB2 (HER2) copy number by FISH, tumor cells from formalin fixed paraffin embedded tissue isolated using image-based dielectrophoresis (DEP) sorting, reported as ERBB2 gene amplified or non-amplified
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0010U Infectious disease (bacterial), strain typing by whole genome sequencing, phylogenetic-based report of strain relatedness, per submitted isolate
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0011U
Prescription drug monitoring, evaluation of drugs present by LC- MS/MS, using oral fluid, reported as a comparison to an estimated steady-state range, per date of service including all drug compounds and metabolites
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0012U Germline disorders, gene rearrangement detection by whole genome next-generation sequencing, DNA, whole blood, report of specific gene rearrangement(s)
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0013U
Oncology (solid organ neoplasia), gene rearrangement detection by whole genome next-generation sequencing, DNA, fresh or frozen tissue or cells, report of specific gene rearrangement(s)
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0014U
Hematology (hematolymphoid neoplasia), gene rearrangement detection by whole genome next- generation sequencing, DNA, whole blood or bone marrow, report of specific gene rearrangement(s)
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0015U
Drug metabolism (adverse drug reactions), DNA, 22 drug metabolism and transporter genes, real-time PCR, blood or buccal swab, genotype and metabolizer status for therapeutic decision support
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0016U
Oncology (hematolymphoid neoplasia), RNA, BCR/ABL1 major and minor breakpoint fusion transcripts, quantitative PCR amplification, blood or bone marrow, report of fusion not detected or detected with quantitation
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0017U
Oncology (hematolymphoid neoplasia), JAK2 mutation, DNA, PCR amplification of exons 12-14 and sequence analysis, blood or bone marrow, report of JAK2 mutation not detected or detected
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0018U
Oncology (thyroid), microRNA profiling by RT-PCR of 10 microRNA sequences, utilizing fine needle aspirate, algorithm reported as a positive or negative result for moderate to high risk of malignancy
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0019U
Oncology, RNA, gene expression by whole transcriptome sequencing, formalin-fixed paraffin embedded tissue or fresh frozen tissue, predictive algorithm reported as potential targets for therapeutic agents
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0020U
Drug test(s), presumptive, with definitive confirmation of positive results, any number of drug classes, urine, with specimen verification including DNA authentication in comparison to buccal DNA, per date of service
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0021U
Oncology (prostate), detection of 8 autoantibodies (ARF 6, NKX3-1, 5’- UTR-BMI1, CEP 164, 3’-UTR- Ropporin, Desmocollin, AURKAIP- 1, CSNK2A2), multiplexed immunoassay and flow cytometry serum, algorithm reported as risk score
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0022U Targeted genomic sequence analysis panel, non- PG0417 Proprietary Laboratory Analyses (PLA) Codes
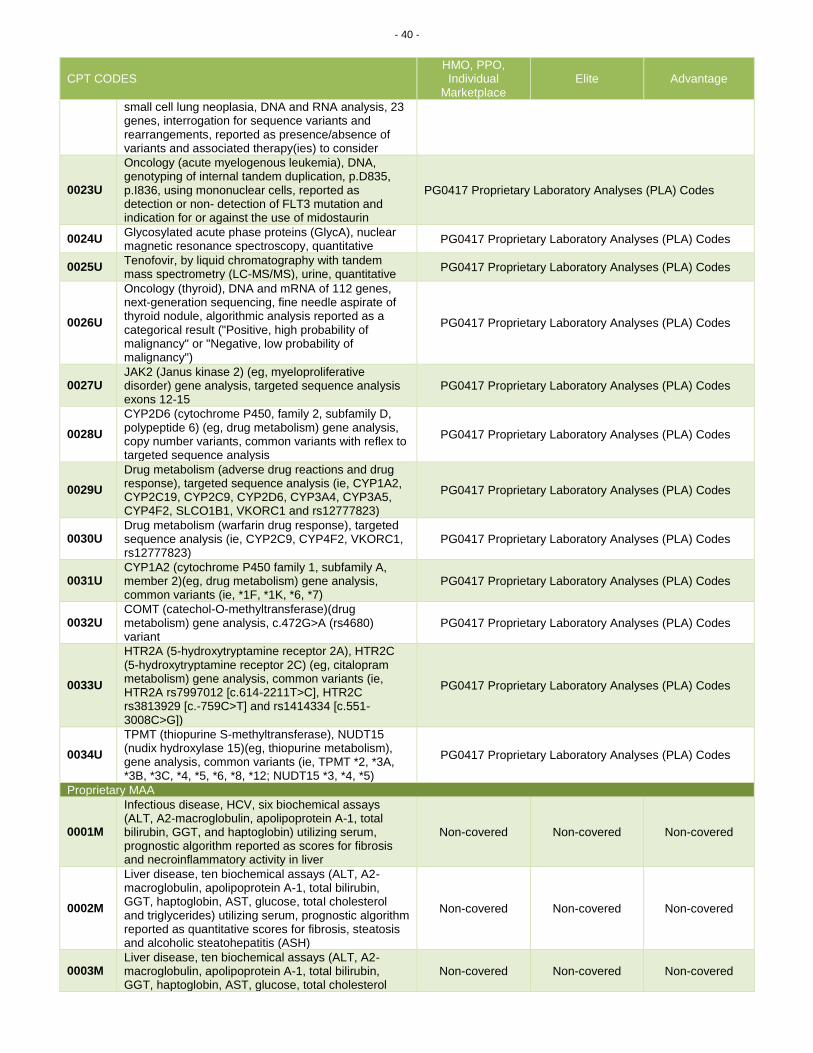
- 40 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
small cell lung neoplasia, DNA and RNA analysis, 23 genes, interrogation for sequence variants and rearrangements, reported as presence/absence of variants and associated therapy(ies) to consider
0023U
Oncology (acute myelogenous leukemia), DNA, genotyping of internal tandem duplication, p.D835, p.I836, using mononuclear cells, reported as detection or non- detection of FLT3 mutation and indication for or against the use of midostaurin
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0024U Glycosylated acute phase proteins (GlycA), nuclear magnetic resonance spectroscopy, quantitative
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0025U Tenofovir, by liquid chromatography with tandem mass spectrometry (LC-MS/MS), urine, quantitative
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0026U
Oncology (thyroid), DNA and mRNA of 112 genes, next-generation sequencing, fine needle aspirate of thyroid nodule, algorithmic analysis reported as a categorical result ("Positive, high probability of malignancy" or "Negative, low probability of malignancy")
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0027U JAK2 (Janus kinase 2) (eg, myeloproliferative disorder) gene analysis, targeted sequence analysis exons 12-15
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0028U
CYP2D6 (cytochrome P450, family 2, subfamily D, polypeptide 6) (eg, drug metabolism) gene analysis, copy number variants, common variants with reflex to targeted sequence analysis
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0029U
Drug metabolism (adverse drug reactions and drug response), targeted sequence analysis (ie, CYP1A2, CYP2C19, CYP2C9, CYP2D6, CYP3A4, CYP3A5, CYP4F2, SLCO1B1, VKORC1 and rs12777823)
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0030U Drug metabolism (warfarin drug response), targeted sequence analysis (ie, CYP2C9, CYP4F2, VKORC1, rs12777823)
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0031U CYP1A2 (cytochrome P450 family 1, subfamily A, member 2)(eg, drug metabolism) gene analysis, common variants (ie, *1F, *1K, *6, *7)
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0032U COMT (catechol-O-methyltransferase)(drug metabolism) gene analysis, c.472G>A (rs4680) variant
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0033U
HTR2A (5-hydroxytryptamine receptor 2A), HTR2C (5-hydroxytryptamine receptor 2C) (eg, citalopram metabolism) gene analysis, common variants (ie, HTR2A rs7997012 [c.614-2211T>C], HTR2C rs3813929 [c.-759C>T] and rs1414334 [c.551-3008C>G])
PG0417 Proprietary Laboratory Analyses (PLA) Codes
0034U
TPMT (thiopurine S-methyltransferase), NUDT15 (nudix hydroxylase 15)(eg, thiopurine metabolism), gene analysis, common variants (ie, TPMT *2, *3A, *3B, *3C, *4, *5, *6, *8, *12; NUDT15 *3, *4, *5)
PG0417 Proprietary Laboratory Analyses (PLA) Codes
Proprietary MAA
0001M
Infectious disease, HCV, six biochemical assays (ALT, A2-macroglobulin, apolipoprotein A-1, total bilirubin, GGT, and haptoglobin) utilizing serum, prognostic algorithm reported as scores for fibrosis and necroinflammatory activity in liver
Non-covered Non-covered Non-covered
0002M
Liver disease, ten biochemical assays (ALT, A2-macroglobulin, apolipoprotein A-1, total bilirubin, GGT, haptoglobin, AST, glucose, total cholesterol and triglycerides) utilizing serum, prognostic algorithm reported as quantitative scores for fibrosis, steatosis and alcoholic steatohepatitis (ASH)
Non-covered Non-covered Non-covered
0003M Liver disease, ten biochemical assays (ALT, A2-macroglobulin, apolipoprotein A-1, total bilirubin, GGT, haptoglobin, AST, glucose, total cholesterol
Non-covered Non-covered Non-covered
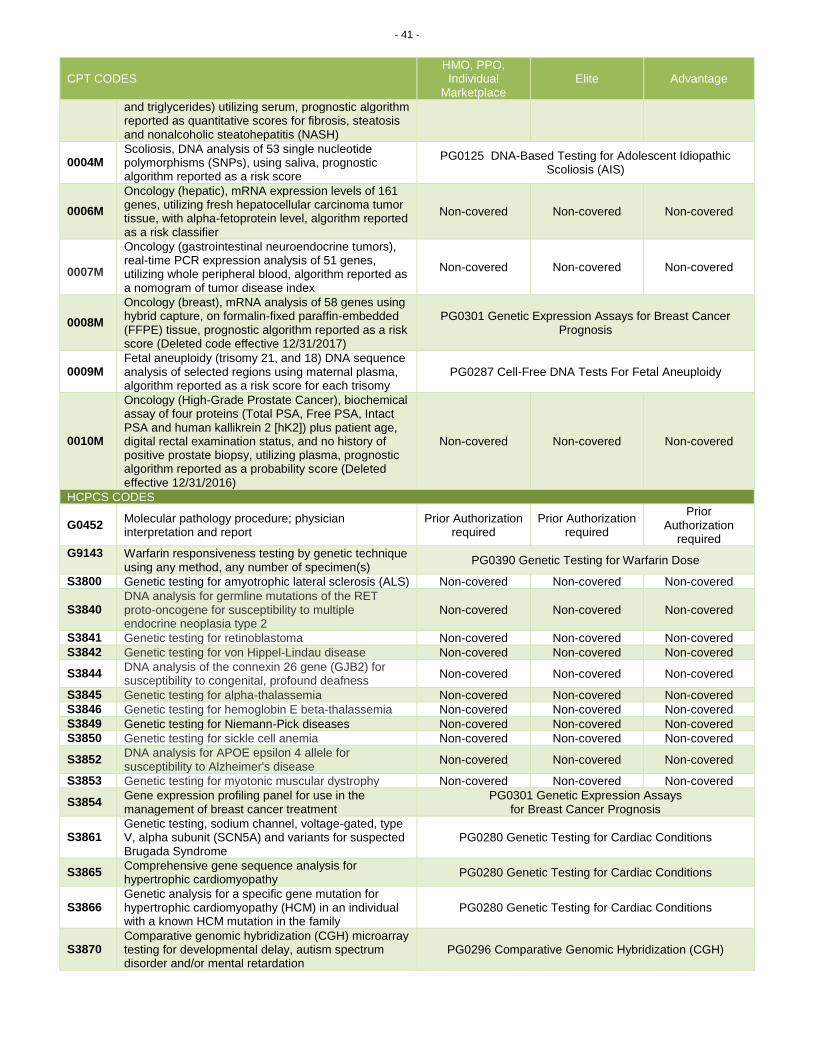
- 41 -
CPT CODES HMO, PPO, Individual
Marketplace Elite Advantage
and triglycerides) utilizing serum, prognostic algorithm reported as quantitative scores for fibrosis, steatosis and nonalcoholic steatohepatitis (NASH)
0004M Scoliosis, DNA analysis of 53 single nucleotide polymorphisms (SNPs), using saliva, prognostic algorithm reported as a risk score
PG0125 DNA-Based Testing for Adolescent Idiopathic Scoliosis (AIS)
0006M
Oncology (hepatic), mRNA expression levels of 161 genes, utilizing fresh hepatocellular carcinoma tumor tissue, with alpha-fetoprotein level, algorithm reported as a risk classifier
Non-covered Non-covered Non-covered
0007M
Oncology (gastrointestinal neuroendocrine tumors), real-time PCR expression analysis of 51 genes, utilizing whole peripheral blood, algorithm reported as a nomogram of tumor disease index
Non-covered Non-covered Non-covered
0008M
Oncology (breast), mRNA analysis of 58 genes using hybrid capture, on formalin-fixed paraffin-embedded (FFPE) tissue, prognostic algorithm reported as a risk score (Deleted code effective 12/31/2017)
PG0301 Genetic Expression Assays for Breast Cancer Prognosis
0009M Fetal aneuploidy (trisomy 21, and 18) DNA sequence analysis of selected regions using maternal plasma, algorithm reported as a risk score for each trisomy
PG0287 Cell-Free DNA Tests For Fetal Aneuploidy
0010M
Oncology (High-Grade Prostate Cancer), biochemical assay of four proteins (Total PSA, Free PSA, Intact PSA and human kallikrein 2 [hK2]) plus patient age, digital rectal examination status, and no history of positive prostate biopsy, utilizing plasma, prognostic algorithm reported as a probability score (Deleted effective 12/31/2016)
Non-covered Non-covered Non-covered
HCPCS CODES
G0452 Molecular pathology procedure; physician interpretation and report
Prior Authorization required
Prior Authorization required
Prior Authorization
required
G9143 Warfarin responsiveness testing by genetic technique using any method, any number of specimen(s)
PG0390 Genetic Testing for Warfarin Dose
S3800 Genetic testing for amyotrophic lateral sclerosis (ALS) Non-covered Non-covered Non-covered
S3840 DNA analysis for germline mutations of the RET proto-oncogene for susceptibility to multiple endocrine neoplasia type 2
Non-covered Non-covered Non-covered
S3841 Genetic testing for retinoblastoma Non-covered Non-covered Non-covered
S3842 Genetic testing for von Hippel-Lindau disease Non-covered Non-covered Non-covered
S3844 DNA analysis of the connexin 26 gene (GJB2) for susceptibility to congenital, profound deafness
Non-covered Non-covered Non-covered
S3845 Genetic testing for alpha-thalassemia Non-covered Non-covered Non-covered
S3846 Genetic testing for hemoglobin E beta-thalassemia Non-covered Non-covered Non-covered
S3849 Genetic testing for Niemann-Pick diseases Non-covered Non-covered Non-covered
S3850 Genetic testing for sickle cell anemia Non-covered Non-covered Non-covered
S3852 DNA analysis for APOE epsilon 4 allele for susceptibility to Alzheimer's disease
Non-covered Non-covered Non-covered
S3853 Genetic testing for myotonic muscular dystrophy Non-covered Non-covered Non-covered
S3854 Gene expression profiling panel for use in the management of breast cancer treatment
PG0301 Genetic Expression Assays for Breast Cancer Prognosis
S3861 Genetic testing, sodium channel, voltage-gated, type V, alpha subunit (SCN5A) and variants for suspected Brugada Syndrome
PG0280 Genetic Testing for Cardiac Conditions
S3865 Comprehensive gene sequence analysis for hypertrophic cardiomyopathy
PG0280 Genetic Testing for Cardiac Conditions
S3866 Genetic analysis for a specific gene mutation for hypertrophic cardiomyopathy (HCM) in an individual with a known HCM mutation in the family
PG0280 Genetic Testing for Cardiac Conditions
S3870 Comparative genomic hybridization (CGH) microarray testing for developmental delay, autism spectrum disorder and/or mental retardation
PG0296 Comparative Genomic Hybridization (CGH)

- 42 -
TAWG REVIEW DATES: 02/26/2016, 03/25/2016, 04/22/2016, 09/23/2016, 03/24/2017 REVISION HISTORY EXPLANATION 01/01/13: Updated 07/08/13: Per Medical Director Review, genetic subcommittee, the following genetic codes will not require a prior authorization; 81206-81208, 81210, 81220-81223, 81240-81245, 81250-81251, 81255-81256, 81261-81268, 81270, 81275, 81291, 81310, 81315-81316, 81340-81342, 81350, 81355, 81378-81383. 12/31/13: Per 2014 new code review, updated the configuration code sets to include procedures G0452 and 81287 to require prior authorization, and procedures 81504 and 81507 to be denied as non-covered. 05/13/14: Added codes 81161, 84999, 85999, 86849, 87999, 88199, 88299, 88380, 88381, 88399, 89398. Removed code S3870. Changed title of medical policy from Genetic and Experimental Laboratory Services to Genetic Testing. Policy reviewed and updated to reflect most current clinical evidence per Medical Policy Steering Committee. 01/13/15: Added reference to PG0296 Comparative Genomic Hybridization (CGH) for codes 81228 & 81229 per Medical Policy Steering Committee. 06/09/15: Added code effective 1/1/15: 81246, 81288, 81313, 81410, 81411, 81415-81417, 81420, 81425-81427, 81430, 81431, 81435, 81436, 81440, 81445, 81450, 81455, 81460, 81465, 81470, 81471, 81519. Updated descriptions for revised codes effective 1/1/15: 81402-81405. Policy reviewed and updated to reflect most current clinical evidence per Medical Policy Steering Committee. 10/26/15: For multianalyte assay with algorithmic analyses code 81519 refer to PG0301 Genetic Expression Assays for Breast Cancer Prognosis for coverage determination. 02/26/16: Added effective 1/1/16 new codes 81162, 81432, 81433, 81434 that require prior authorization; 81170, 81218, 81219, 81272, 81273, 81276, 81311, 81314, 81412, 81437, 81438, 81442, 81528, 81545, 81595 that do not require prior authorization; and 81490, 81493, 81525, 81535, 81536, 81538, 81540 that are non-covered. Updated effective 1/1/16 revised codes 81210, 81275, 81355, 81435, 81436, 81445, 81450, & 81455. Added codes 88230-88299, and 0001M-0010M. Code 88271 has a limit of 25 units per 365 days. Removed codes 88380 & 88381. Policy reviewed and updated to reflect most current clinical evidence per The Technology Assessment Working Group (TAWG). 03/25/16: Coverage changes made per CMS guidelines: Non-covered for all product lines - 81161, 81507, 0009M; Non-covered for HMO, PPO, Individual Marketplace, Elite and covered with prior authorization for Advantage - 81200. 81205, 81209, 81224, 81252, 81253, 81254, 81257, 81260, 81290, 81324, 81325, 81326, 81330, 81331, 81410, 81411, 81412, 81415, 81416, 81417, 81425, 81426, 81427, 81430, 81431, 81433, 81434, 81438, 81440, 81442, 81460, 81465, 81470, 81471; Covered with prior authorization for HMO, PPO, Individual Marketplace, Elite and Non-covered for Advantage - 81490, 81504, 81525, 81540; Covered with prior authorization for Elite and Non-covered for HMO, PPO, Individual Marketplace, Advantage – 81493. Policy reviewed and updated to reflect most current clinical evidence per TAWG. 04/22/16: Codes 81242, 81251, 81302, 81303, 81304 are covered with prior authorization for HMO, PPO, Individual Marketplace, & Advantage and are non-covered for Elite per CMS guidelines. Added specific non-covered genes/gene components determination for 81400-81408, & 81479 per CMS guidelines as non-covered for all product lines. Added myRisk test (81479) as non-covered for all product lines per CMS guidelines. Added reference to new policies: PG0355 Genetic Testing for Hereditary Thrombophilia (81240, 81241, 81291), PG0357 Gene Expression Profiling for Colorectal Cancer (81525), PG0360 Genetic Testing for FMR1 Mutations Including Fragile X Syndrome (81243, 81244), PG0363 CORUS® CAD (81493), PG0364 Cancer Type ID (81540), & PG0368 GeneSight® Assay for Refractory Depression (81479). Policy reviewed and updated to reflect most current clinical evidence per TAWG. 6/24/16: Policy updated per TAWG determination for PG0298 Afirma® Thyroid FNA Analysis, PG0334 ThyroSeq® v.2 Next Generation Sequencing, and PG0367 Gene Expression Analysis for Prostate Cancer. 10/28/16: CPT code 81224 is now covered without prior authorization for HMO, PPO, Individual Marketplace, & Elite, in addition, to Advantage. Policy reviewed and updated to reflect most current clinical evidence per TAWG. 03/24/17: Added effective 01/01/17 new CPT code 81327 per PG0065 Colorectal Cancer Screening. Added effective 01/01/17 new CPT codes 81413, 81414, 81439 per PG0280 Genetic Testing for Cardiac Conditions. Added effective 01/01/17 new CPT code 81422 per PG0287 Cell-Free DNA Tests For Fetal Aneuploidy. Added CPT code S3854 per PG0301 Genetic Expression Assays for Breast Cancer Prognosis. Added CPT codes S3861-S3866 per PG0280 Genetic Testing for Cardiac Conditions. Added CPT code S3870 per PG0296 Comparative Genomic Hybridization (CGH). Added effective 01/01/17 new CPT codes 81539 as requires prior authorization for Advantage & non-covered for HMO, PPO, Individual Marketplace, & Elite. Added CPT codes S3800-S3853 as non-covered for all product lines. Deleted effective 12/31/16 CPT code 0010M (replaced by 81539). Deleted effective 12/31/16 CPT codes 81280-81282 per PG0280 Genetic Testing for Cardiac Conditions. Effective 01/01/17 code 81595 is now non-covered for Advantage per ODM guidelines (continues to be covered without prior authorization for HMO, PPO, Individual Marketplace, & Elite) for PG0340 AlloMap™ Molecular-Expression Blood Test. Policy
- 43 -
reviewed and updated to reflect most current clinical evidence per The Technology Assessment Working Group (TAWG). 01/25/18: Added effective 01/01/18 new CPT codes 81520 & 81521 per PG0301 Genetic Expression Assays for Breast Cancer Prognosis. Added effective 01/01/18 new CPT codes 81541 & 81551 per PG0367 Gene Expression Analysis for Prostate Cancer. Effective 12/31/17 deleted code 0008M (replaced by 81520) per PG0301 Genetic Expression Assays for Breast Cancer Prognosis. Added Proprietary Laboratory Analyses (PLA) Codes 0001U-0034U per PG0417 Proprietary Laboratory Analyses (PLA) Codes & PG0367 Gene Expression Analysis for Prostate Cancer. Revised effective 01/01/18 codes 81257, 81432, & 81439. Added effective 01/01/18 new codes 81105, 81106, 81107, 81108, 81109, 81110, 81111, 81112, 81120, 81121, 81175, 81176, 81238, 81247, 81248, 81249, 81283, 81334, 81335, 81346, 81448 as covered with prior authorization for all product lines per CMS & ODM guidelines. Added effective 01/01/18 new codes 81230, 81231, 81232 as covered with prior authorization for Advantage per ODM guidelines and non-covered for HMO, PPO, Individual Marketplace, & Elite per CMS guidelines. Added effective 01/01/18 new codes 81258, 81259, 81269, 81328, 81361, 81362, 81363, 81364 as covered with prior authorization for HMO, PPO, Individual Marketplace, & Advantage and non-covered for Elite per CMS guidelines. Added code G9143 per PG0390 Genetic Testing for Warfarin Dose. Refer to PG0390 Genetic Testing for Warfarin Dose for coverage determination of codes G9143, 81227 & 81355. Refer to PG0367 Gene Expression Analysis for Prostate Cancer for coverage determination of codes 81313 & 81539. Refer to PG0375 Molecular Cytogenetic Testing for coverage determination of code 88271. Refer to PG0411 Genetic Testing for Duchenne and Becker Muscular Dystrophy for coverage determination of codes 81161 & 81408. Codes 81432, 81435, 81436, 81445, 81455 removed from PG0336 PTEN Hamartoma Tumor Syndrome. Policy reviewed and updated to reflect most current clinical evidence per The Technology Assessment Working Group (TAWG).
REFERENCES/RESOURCES Centers for Medicare and Medicaid Services, CMS Manual System and other CMS publications and services Ohio Department of Medicaid http://jfs.ohio.gov/ American Medical Association, Current Procedural Terminology (CPT®) and associated publications and services Centers for Medicare and Medicaid Services, Healthcare Common Procedure Coding System, HCPCS Release and Code Sets Industry Standard Review Hayes, Inc.