medical x-ray imaging, current status and … · medical x-ray imaging, ... imaging), x-ray imaging...
TRANSCRIPT

MEDICAL X-RAY IMAGING, CURRENT STATUS AND SOME FUTURE CHALLENGES
Erik L. Ritman, M.D., Ph.D.
Department of Physiology & Biomedical Engineering
Mayo Clinic College of Medicine, 200 First Street SW, Rochester, MN 55905
ABSTRACT Biomedical x-ray imaging has proven to be an indispensable component of many medical diagnostic and treatment techniques. Major technical advances over the years, culminating in helical scanning, multi slice, x-ray computed tomography, can now provide ∼ 0.5 mm3 resolution 3D images of the spatial distribution of tissue attenuation coefficients of an entire adult human thorax or abdomen. The utility of the x-ray images is ultimately limited by two opposing factors, one is that increased image spatial and contrast resolution requires an increased number of detected x-ray photons per image resolution unit, and the other is the direct relationship between the number of x-ray photons and the increased risk of tissue damage and ultimate cancer development. This trade-off limits the utility of x-ray imaging in screening of subjects who are likely to be at risk of a disease (e.g., a family history or exposure to an environment that increases the risk of a life-threatening disease) but who have not yet developed the clinical signs or symptoms. Based on increasing experience (especially with synchrotron x-ray-based imaging), x-ray imaging of some consequences of a tissue’s x-ray refractive index, rather than x-ray attenuation, has potential for decreasing the x-ray dose and increasing contrast resolution. This approach, while presenting formidable technological problems for whole-body 3D imaging, could, if achievable in a routine clinical setting, greatly expand the applicability of x-ray imaging for screening and repeated studies of asymptomatic subjects of all ages. INTRODUCTION X-ray has been used for biomedical imaging ever since Roentgen x-rayed his wife’s hand in 1895 [1]. The speed with which the technology was implemented in medicine is phenomenal [2] by today’s standards. This is well illustrated by a note written by Edison on January 27, 1896 to a Mr. Kennelly, which said “How would you like to come over and experiment an Rotgons (sic) new radiations. I have glassblower and pumps running and all photographic apparatus. We could do a lot before others get their second wind” [3]. An important reason for this rapid acceptance is probably that it was the first time that objective evaluation of an internal organ could be made in time to act in a meaningful way, and the other reason is probably that the technology for making x-rays (i.e., high voltage electricity and the Crooke’s tube) and recording the x-ray images (i.e., photographic plate) were available because they were already in wide spread use for other purposes. Nonetheless, resistance to x-ray imaging soon followed its introduction to medical practice [4] and continues in recent times as part of effort to control spiraling medical costs by controlling the introduction of high technology into medical practice [5].
1Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
This document was presented at the Denver X-ray Conference (DXC) on Applications of X-ray Analysis. Sponsored by the International Centre for Diffraction Data (ICDD). This document is provided by ICDD in cooperation with the authors and presenters of the DXC for the express purpose of educating the scientific community. All copyrights for the document are retained by ICDD. Usage is restricted for the purposes of education and scientific research. DXC Website – www.dxcicdd.com
ICDD Website - www.icdd.com
Advances in X-ray Analysis, Volume 49
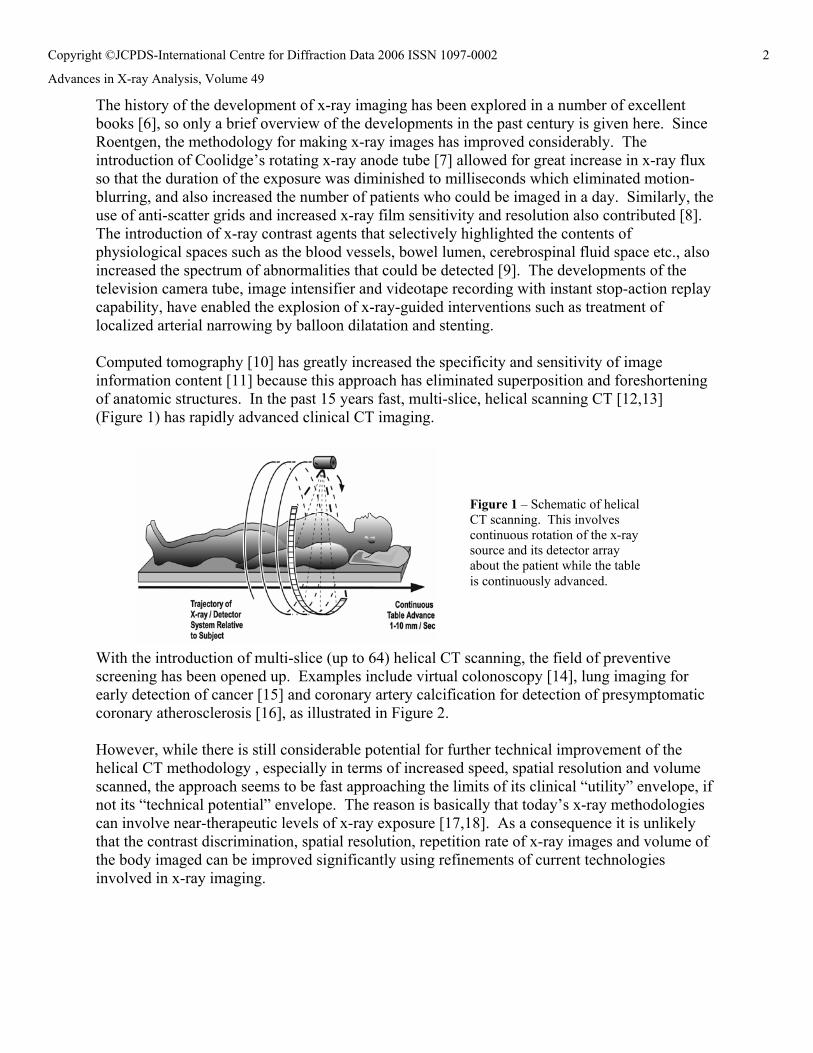
The history of the development of x-ray imaging has been explored in a number of excellent books [6], so only a brief overview of the developments in the past century is given here. Since Roentgen, the methodology for making x-ray images has improved considerably. The introduction of Coolidge’s rotating x-ray anode tube [7] allowed for great increase in x-ray flux so that the duration of the exposure was diminished to milliseconds which eliminated motion-blurring, and also increased the number of patients who could be imaged in a day. Similarly, the use of anti-scatter grids and increased x-ray film sensitivity and resolution also contributed [8]. The introduction of x-ray contrast agents that selectively highlighted the contents of physiological spaces such as the blood vessels, bowel lumen, cerebrospinal fluid space etc., also increased the spectrum of abnormalities that could be detected [9]. The developments of the television camera tube, image intensifier and videotape recording with instant stop-action replay capability, have enabled the explosion of x-ray-guided interventions such as treatment of localized arterial narrowing by balloon dilatation and stenting. Computed tomography [10] has greatly increased the specificity and sensitivity of image information content [11] because this approach has eliminated superposition and foreshortening of anatomic structures. In the past 15 years fast, multi-slice, helical scanning CT [12,13] (Figure 1) has rapidly advanced clinical CT imaging.
With the introduction of multi-slice (up to 64) helical CT scanning, the field of preventive screening has been opened up. Examples include virtual colonoscopy [14], lung imaging for early detection of cancer [15] and coronary artery calcification for detection of presymptomatic coronary atherosclerosis [16], as illustrated in Figure 2. However, while there is still considerable potential for further technical improvement of the helical CT methodology , especially in terms of increased speed, spatial resolution and volume scanned, the approach seems to be fast approaching the limits of its clinical “utility” envelope, if not its “technical potential” envelope. The reason is basically that today’s x-ray methodologies can involve near-therapeutic levels of x-ray exposure [17,18]. As a consequence it is unlikely that the contrast discrimination, spatial resolution, repetition rate of x-ray images and volume of the body imaged can be improved significantly using refinements of current technologies involved in x-ray imaging.
Figure 1 – Schematic of helical CT scanning. This involves continuous rotation of the x-ray source and its detector array about the patient while the table is continuously advanced.
2Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
To overcome this “barrier” to progress we need to look at both the ultimate biomedical needs and requirements as well as the technical possibilities, such as: 1) What radiation doses are acceptable? 2) What spatial, contrast and temporal resolution are needed? 3) What volume of the body needs to be imaged concurrently? 4) What 3D image repetition rate is needed? 5) Which, more specific and effective, contrast media need to be developed? 6) How much can prior information contribute? 7) How much can technological improvements be expected to contribute? 8) Are there x-ray/matter interactions, other than attenuation, that could be used to meet clinical
needs at orders of magnitude lower radiation dose? X-RAY DOSE CONSIDERATIONS Radiation exposure should be limited to keep deleterious biological effects to a minimum [18]. However, for a fixed signal to noise ratio in each CT image voxel (3D pixel), the x-ray exposure needs to increase by at least the cube of the resolution, i.e., by increasing from 1 to 0.5 mm3 resolution the exposure should increase at least 8 fold [19]. Just 0.1 Grey [10 Rad] absorbed dose in tissue is likely to ultimately result in cancer in up to 0.1% of people exposed [20]. In the average patient 2 Grey absorbed dose will result in erythema, (reddening of the skin) and 18 Grey will result in tissue necrosis and ulceration over several weeks. To put x-ray exposures in context, a single scan sequence of the thorax, using a multi-slice helical CT scanner, involves an exposure of 0.03-0.07 mSv/second when scanning at the level of the mid abdomen [60] which results in absorbed dose rates to the skin that are typically 2-8 mGy/second. Annual exposure at sea level from cosmic and terrestrial sources is an average, 3.6 mSieverts and a chest x-ray is 0.04 mSieverts [21].
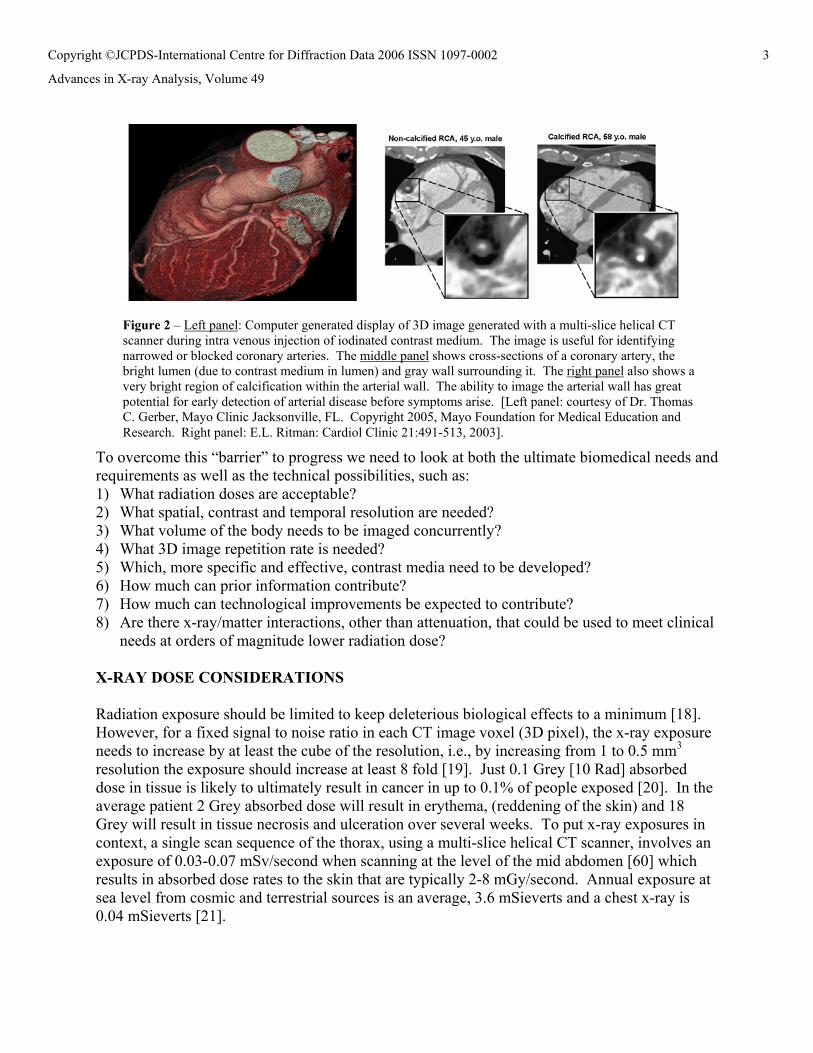
Figure 2 – Left panel: Computer generated display of 3D image generated with a multi-slice helical CT scanner during intra venous injection of iodinated contrast medium. The image is useful for identifying narrowed or blocked coronary arteries. The middle panel shows cross-sections of a coronary artery, the bright lumen (due to contrast medium in lumen) and gray wall surrounding it. The right panel also shows a very bright region of calcification within the arterial wall. The ability to image the arterial wall has great potential for early detection of arterial disease before symptoms arise. [Left panel: courtesy of Dr. Thomas C. Gerber, Mayo Clinic Jacksonville, FL. Copyright 2005, Mayo Foundation for Medical Education and Research. Right panel: E.L. Ritman: Cardiol Clinic 21:491-513, 2003].
3Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
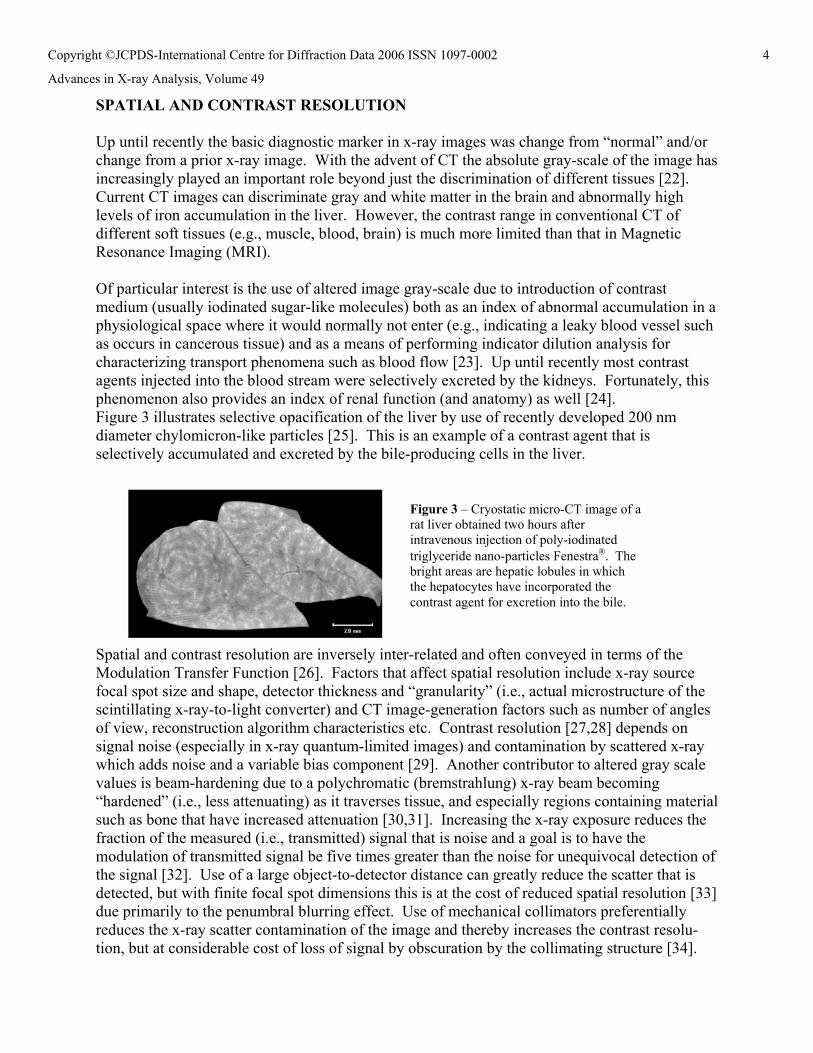
SPATIAL AND CONTRAST RESOLUTION Up until recently the basic diagnostic marker in x-ray images was change from “normal” and/or change from a prior x-ray image. With the advent of CT the absolute gray-scale of the image has increasingly played an important role beyond just the discrimination of different tissues [22]. Current CT images can discriminate gray and white matter in the brain and abnormally high levels of iron accumulation in the liver. However, the contrast range in conventional CT of different soft tissues (e.g., muscle, blood, brain) is much more limited than that in Magnetic Resonance Imaging (MRI). Of particular interest is the use of altered image gray-scale due to introduction of contrast medium (usually iodinated sugar-like molecules) both as an index of abnormal accumulation in a physiological space where it would normally not enter (e.g., indicating a leaky blood vessel such as occurs in cancerous tissue) and as a means of performing indicator dilution analysis for characterizing transport phenomena such as blood flow [23]. Up until recently most contrast agents injected into the blood stream were selectively excreted by the kidneys. Fortunately, this phenomenon also provides an index of renal function (and anatomy) as well [24]. Figure 3 illustrates selective opacification of the liver by use of recently developed 200 nm diameter chylomicron-like particles [25]. This is an example of a contrast agent that is selectively accumulated and excreted by the bile-producing cells in the liver.
Spatial and contrast resolution are inversely inter-related and often conveyed in terms of the Modulation Transfer Function [26]. Factors that affect spatial resolution include x-ray source focal spot size and shape, detector thickness and “granularity” (i.e., actual microstructure of the scintillating x-ray-to-light converter) and CT image-generation factors such as number of angles of view, reconstruction algorithm characteristics etc. Contrast resolution [27,28] depends on signal noise (especially in x-ray quantum-limited images) and contamination by scattered x-ray which adds noise and a variable bias component [29]. Another contributor to altered gray scale values is beam-hardening due to a polychromatic (bremstrahlung) x-ray beam becoming “hardened” (i.e., less attenuating) as it traverses tissue, and especially regions containing material such as bone that have increased attenuation [30,31]. Increasing the x-ray exposure reduces the fraction of the measured (i.e., transmitted) signal that is noise and a goal is to have the modulation of transmitted signal be five times greater than the noise for unequivocal detection of the signal [32]. Use of a large object-to-detector distance can greatly reduce the scatter that is detected, but with finite focal spot dimensions this is at the cost of reduced spatial resolution [33] due primarily to the penumbral blurring effect. Use of mechanical collimators preferentially reduces the x-ray scatter contamination of the image and thereby increases the contrast resolu-tion, but at considerable cost of loss of signal by obscuration by the collimating structure [34].
Figure 3 – Cryostatic micro-CT image of a rat liver obtained two hours after intravenous injection of poly-iodinated triglyceride nano-particles Fenestra®. The bright areas are hepatic lobules in which the hepatocytes have incorporated the contrast agent for excretion into the bile.
4Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
The Basic Functional Unit (BFU) of organs seems like a reasonable goal for the spatial resolution clinical whole-body imagers. BFUs are the smallest accumulations of diverse cells that function like the organ they are in, e.g., the hepatic lobule in the liver or nephron in the kidney. Generally, they occupy about 0.01 mm3, i.e., about 200 μm in diameter, which is essentially true for all organs and for all vertebrate animals. The BFU volume is essentially the upper limit of a spherical piece of tissue which can survive without its own blood supply. Hence, early ‘solid’ cancers would grow to this size before a blood supply is needed to sustain further growth [35]. Thus, an isotropic spatial resolution of 100 μm seems like a reasonable goal because it would allow us to measure their number, size and perhaps individual functional status. However, because they, and their microvascular blood supply, consist of tissue that is elementally not very different from the connective tissue in which the BFUs are embedded, this might involve very high radiation exposures to provide the signal to noise ratio needed for discriminating a BFU from its surrounding tissue matrix. Because their contrast differential is very low, either suitable contrast agents that selectively accumulate in (or avoid) them, will need to be developed (e.g., such as illustrated in Figure 3), and/or an x-ray imaging method which has inherently greater contrast (than does conventional, attenuation-based, x-ray imaging) will need to be developed. VOLUME TO BE IMAGED The volume to be scanned is determined by the need to image an entire organ. This is because the absence of a detected abnormality in an organ will only then have meaning. This would be the case for a tumor (due to cancer or some other focal pathology) or some local breakdown of the organ that could initiate a disseminating cascade of tissue failure [36,37]. The gut would require that the entire abdomen is imaged and the lung requires that the entire thorax is imaged – both being approximately 30-40 cm in cephalo-caudal height and in transverse diameter. TEMPORAL RESOLUTION In addition to 3D anatomy, the rate, amplitude, synchrony, and the spatial distribution of the movement attributes of organs are important indicators of the organs’ function(s). There are two types of involuntary motion; one can be predictively cyclic, such as the heart beat or breathing, and the other is unpredictable, and generally not reproducible, such as the movement of the bowel or the passage of a bolus of contrast agent through the blood stream. Thus, there are two issues; one is to image fast enough to stop the motion blurring i.e., the 3D imaging “aperture” time, which would need to be fast enough to stop-action the fastest moving phase of the motion; the other is the 3D image repetition (or frame) rate needed to quantitate the motion. The heart wall normally has a peak rate of thickening of approximately 50 mm/sec so that a stop-action exposure duration would need to be at most ([spatial resolution]/ [50 mm/sec]) seconds which is about 10 msec at 0.5 mm resolution, although if the imaging is to occur only during the slowest motion phase of the cardiac cycle (end diastole) that would be about 100 msec. In the case of the predictable cyclic motion, such as occurs in the heart, incremental sets of partial scan data can be acquired progressively over many sequential cycles by acquiring the scan data during a fixed phase of that cyclic motion. This “gated” scanning allows imaging of, for instance, the entire heart at one phase of multiple sequential cardiac cycles (i.e., over a scan period of one breath
5Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
hold). The other issue is the number of sequential exposures needed to adequately describe the motion. For a cardiac cycle, which in an adult is approximately half to one second in duration, for a breath this might be 5 seconds, for a blood-borne indicator dilution curve this might be 20 –30 seconds and for a bowel motion study this might be 30-60 seconds. However, the fastest motion within that cycle would determine the image “frame” rate needed – for the left ventricle of the heart this about 15 images/second [38]. However, detector lag resulting in mixing of current and previous images can also greatly degrade the image quality if the image moves during the sequential exposures. X-RAY/MATTER INTERACTION OPTIONS EXTENDING X-RAY IMAGING INFORMATION With current multi-slice helical CT scanners the x-ray volume scanned at approximately 0.5 mm3 voxel resolution can encompass the entire abdomen or thorax within a single, ∼ 20 second, breath-hold and, if ECG-gated scanning is used, 170 millisecond temporal resolution can be achieved. Thus, the main limitations of that approach are that the spatial and temporal resolutions are still not optimal and that the x-ray exposure is approaching unacceptable levels for repeated screening purposes in asymptomatic subjects. Past experience, using a one-of-a-kind CT scanner, has shown that 20 cm diameter cylindrical volumes can be scanned in 11 milliseconds and repeated at up to 60/second [39] and experience with high flux synchrotron radiation has shown that micrometer resolution dynamic x-ray projections can be generated [40]. These approaches have been useful for research applications but have not evolved into clinically useful scanners. So the question is, can the desired resolution characteristics be achieved by further technical developments of the attenuation-based imaging approach? 1) OPTIMIZATION OF ATTENUATION-BASED IMAGING BY USE OF: a) Monochromatic x-rays instead of polychromatic (bremstrahlung) x-rays [41,42] would limit the radiation exposure to just the useful x-ray photons and also make the image contrast information more quantitative. In favorable circumstances this may reduce x-ray exposure to half. If in addition photon energy discrimination could be used, most scattered photons could be identified by their lower photon energy and thus rejected without the need for mechanical collimation (thereby eliminating that source of reduced x-ray detection efficiency). b) K-edge absorption discontinuities subtraction imaging to selectively enhance contrast has been shown to be very effective [43] in terms of enhancing signal to noise. However this approach has been limited by the difficulty of generating the desired monochromatic x-rays at the intensity and photon energy needed for routine clinical use. The effectiveness of contrast agents can be greatly enhanced if the absorption K-edge of the element in the contrast agent is tightly “straddled” by the dual energy x-ray exposures. While very effective, as has been demonstrated with iodine-based contrast agent, the presence of contrast in large physiological spaces (e.g., cardiac chambers – 5 cm diameter) overlying the structure of interest (e.g., coronary artery lumen – 4 mm diameter) can greatly reduce signal to noise [44]. Contrast agents-based on elements such as Europium, would involve ∼47 keV photon energies that better penetrate through the body than does the ∼ 31 keV needed for iodine-based contrast agent. c) Counting individual photons [45]. This would eliminate the “noise” involved in the current method of integrating the signal detected in the x-ray-to-light/current converter (with an analog
6Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
circuit). If, in addition, photon energy discrimination could be used, then many scattered photons could be detected and rejected without the need for mechanical collimation. d) Scattered x-ray to provide added image information because the mode of scatter contains information not conveyed by the attenuation. However, this wouldn’t reduce radiation so much as provide more information per unit of x-ray exposure [46]. As a large proportion of x-ray photons in clinical x-ray imaging is scattered, it might be possible, in selected applications, to obtain the desired information by use of scatter detection involving lower x-ray exposures than would be needed for attenuation-based images of the same structure or its dynamics [47]. e) Inversion of the single x-ray focal spot/imaging array approach to an array of x-ray sources illuminating a single detector approach has the advantage that the entry x-ray exposure, in terms of photons/mm2 of skin is reduced, even though the total radiation dose to the body remains unchanged [48]. f) Hardware and software ‘tricks’ that can be used to reduce patient exposure. One method is to use “bow tie” shaped attenuator which spatially modulates the x-ray exposure so that the transmitted x-ray signal is more uniform in its spatial distribution, thereby increasing the effective dynamic range in the image. Another involves varying the radiation exposure at different angles of view so as to keep the transmitted x-ray signal constant at the level needed for the desired signal to noise ratio [49]. For a chest image this means that the Lateral exposure would be less than the Antero-Posterior exposure. Another approach is to restrict the x-ray exposure to just the organ of interest (e.g., the heart). This would reduce the amount of tissue exposed but needs special “limited data set” tomographic reconstruction algorithms to provide useable images [50,51]. g) A priori information to help deduce quantitative information about the sub-resolution structure of tissues by use of a suitable “inverse” model. Such a model would have a priori information about the tissue microstructure, such as has been attempted for myocardial microvasculature [52]. This approach would reduce the need for high resolution imaging in selected application and thereby reduce the x-ray exposure needed. 2) USE OF PAIR-PRODUCTION FOR IMAGING If x-rays with photon energy greater than 1.022 MeV are used to irradiate a body, pair production can result and these can be detected via the positron annihilation which results in two 511 keV gamma-ray photons being produced in essentially opposite directions. If the body is exposed in a plane, then the detection of ‘coincident’ gamma-rays on opposite sides of that irradiated plane directly provides the tomographic image information [53]. This method would have contrast discrimination by virtue of the pair production being sensitive to atomic number and density of material. Hence, it should be particularly suitable for bone imaging and with suitable contrast agents. When the exact ‘slice’ to be imaged is known – then this approach exposes only that slice with the illuminating beam. Because the attenuation of the 511 keV photons by the body on either side of the imaged slice is relatively low (∼0.1/cm), the tomographic image is only minimally degraded by attenuation of the 511 keV photons. 3) IMAGING OF X-RAY REFRACTIVE INDEX The refractive index for clinically relevant x-rays through tissue is very close to 1, but its variation amongst tissues theoretically provides greater contrast than does attenuation, especially
7Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
of low atomic weight elements [54]. Moreover, the amount of x-ray exposure needed to obtain a useable image should also be greatly reduced relative to attenuation-based imaging used to detect the same contrast differences [55,56]. a) Refraction of the x-rays, especially at sites of very rapid change in refractive index (such as occurs at the edges of tissue fibers or small ducts and blood vessel walls) results in refraction of the x-ray so that at some distance beyond the refraction site an edge enhancement can occur [57]. This approach is probably limited to several centimeters of tissue depths and tissues in which such fibrous/vascular micro-structure is an important clinical cue (e.g., mammography in which the breast is compressed down to a 4 cm thickness). A variant of this method involves use of grating interferometers placed adjacent to the detector side of the person (i.e., the phase grating) and the other just in front of the detector (i.e., the absorption grating) [58]. b) Differences in phase shifts that occur due to passage through materials of different refractive index can be used to cause Moiré patterns when ‘mixed’ with a reference beam. The Moiré pattern can be unraveled to provide a map of the phase shift distribution [59]. This works well for a small thickness of tissue in which a small number (e.g., 5) of phase shift occurs (and hence can be accounted for) but after passage through 30 cm of tissue the amount of phase shift, combined with the shorter photon wavelength needed to provide adequate penetration of the body, would make “unraveling” of the phase shift very more difficult. c) The ultimate goal would be to directly measure the spatial distribution of the transit time of individual photons. As x-ray photons travel at the speed of light each photon traverses 1 mm in approximately 3.3 x10-12 seconds, i.e., 3.3 picoseconds. However, as the velocity of x-ray through water differs little from that through air, then imaging of just the presence or absence of tissue at 1 mm resolution would require time discriminations in the low femto-second ranges and that is probably not practical at the clinical level at present. Differences between tissue types would affect the velocity of x-ray predominantly via density differences, and because proportionately fewer of the high energy photons are attenuated, the x-ray dose received by the subject is reduced. However, the overwhelming advantage of velocity measurement would be that only one photon would provide this measurement (although uncertainty in the velocity measurement would require several photons to be measured to provide an acceptable degree of certainty) whereas attenuation estimation needs more than 104 photons to be transmitted to provide a useful measurement per picture element (pixel) in the detector. CONCLUSION Current, attenuation-based x-ray imaging methods cannot be expected to increase much more in resolution due to the undesirable x-ray exposure consequences. If time-of-flight x-ray imaging can be developed for clinical applications, the power of x-ray imaging could be greatly enhanced without the added radiation consequences. AKNOWLEDGEMENTS Dr. Ritman’s research is supported in part by NIH grants HL72255 and EB000305. Dr. Ritman thanks Ms. Mara Lukenda for help with editing and formatting the manuscript.
8Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
REFERENCES [1] Roentgen, W.C., Uber eine neue art von strahlen, Wurtzburg Stahal, 1895. [2] Holtzmann-Kevles, B., Naked to the bone: medical imaging in the twentieth century,
Rutgers University Press: New Brunswick, NJ, 1997. [3] Shephard, D.A., Edison's attempts at radiography of the brain (1896), Mayo Clin. Proc.,
1974, 49, 59-61. [4] Thomas, J.L., What influence has the use of x-rays had upon treatment of fractures and dislocations, Brit. Med. J., 1906; 1, 1034. [5] Senate Bill N. 127, Introduced by Senator Keene, Jan 25, 1979 – proposed amendment to
sections 437.10 and 438.6 of the Health and Safety Code and to add section 14105.9 to the Welfare and Institution Code. California State Archives.
[6] Dolby, T.; Alker G., Origins and development of medical imaging, Carbondale and Edwardsville: Southern Illinois University Press, 1997, pp 170.
[7] Coolidge, W.D., Vacuum Tube, application to the US Patent office, May 13, 1913. [8] Bucky, G., Über die Ausschaltung der Sekunderstrahlen, Verhandlun. der Deutsch.
Rtg. Gesellsch., 1913, 9, 30-32. [9] Lebrams, H.L., Angiography, Little Drawn and Co: Boston, 1971, Vol 2. [10] Ambrose, J.; Hounsfield, G.N., Computerized transverse axial tomography, Brit. J. Radiol.,
1972, 46, 148-149. [11] Baker, Jr. H.L., The impact of computed tomography on neurological practice, Radiol.,
1975, 116, 637-640. [12] Nishimura, H.; Miyazaki, O., CT system for spirally imaging subject on a moveable bed
synchronized to x-ray tube revolution, US Patent 4789929, 1988. [13] Kalender, W.A.; Seissler, W.; Klotz, E.; Vock, P., Spiral volumetric CT with single breath-
hold technique, continuous transport and continuous scanner rotation, Radiol., 1990, 176, 181-183.
[14] Pickhardt, P.J.; Choi, J.R.; Hwang, I.; Butler, J.A.; Puckett, M.L.; Hildebrandt, H.; Wong, R. K.; Nugent, P.A.; Mysliwiec, P.A.; Schindler, W.R., Computer tomographic virtual colonscopy to screen for colorectal neoplasia in asymptomatic adults, N. Engl. J. Med., 2003, 349, 2191-2200.
[15] Yankelevitz, D.R.; Gupta, R.; Zhao, B.; Henschke, C.I., Small pulmonary nodules: evaluation with repeat CT – preliminary experience, Radiol., 1999, 212, 561-566.
[16] Ohnesorge, B.; Flohr, T.; Fischbach, R.; , Kopp, A.F.; Knez, A.; Schroder, S.; Schopf, U.J.; Crispin, A.; Klotz, E.; Reiser, M.F.; Becker, C.R., Reproducibility of coronary calcium quantification in repeat examination with retrospective ECG-gated multisection spiral CT, Eur. Radiol., 2002, 12, 1532-1540.
[17] Morin, R.L.; Gerber, T.C., McCollough, C.H., Physics and dosimetry of computed tomography, Cardiol. Clin., 2003, 21, 515-520.
[18] Wagner, L.K.; Eifel, P.J.; Geise, R.A., Potential biological effects following high x-ray dose interventional procedures (Review), J. Vasc. & Intervent. Radiol., 1994, 5, 71-84.
[19] Grodzins, L., Optimal energies for x-ray transverse tomography of small samples, Nucl. Instrum. Methods, 1983, 206, 541-545.
[20] URL: http://srab.cancer.gov/devcan/ [21] URL: http://www.epa.gov/radiation/students/calculate.html [22] Duck F.A., Physical properties of tissue, Academic Press London, 1990, pp 346.
9Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
[23] von Schulthess, G.K.; Henning, J., (eds), Functional Imaging, Lippincot-Raven Philadelphia: New York, 1998, pp 471.
[24] Rule, A.D.; Bajzer, Z.; Ritman, E.L.; Lerman, L.O., Renal handling of X-ray contrast media imaging and exploration with electron beam CT, Ann. NY Acad. Sci., 2002, 972, 317-324.
[25] Bakan, D.A.; Lee, F.T. Jr; Weichert, J.P.; Longino, M.A., Counsell, R.E., Hepatobiliary imaging using a novel hepatocyte-selective CT contrast agent, Acad. Radiol., 2002, 9, S194-199.
[26] Dowseth, D.J.; Kenny, P.A.; Johnston, R.E., The physics of diagnostic imaging, Chapman Hall Med: London, 1988.
[27] Motz, J.W.; Danos, M., Image information content and patient exposure, Med. Phys., 1978, 5, 8-22.
[28] Chesler, D.A.; Riederer, S.J.; Pelc, N.J., Noise due to photon counting statistics in computed tomography, J. Comput. Assist. Tomogr., 1977, 1, 64-74.
[29] Johns, P.D.; Yaffe, M., Scattered radiation in fan beam imaging systems, Med. Phys., 1982, 9, 464-472.
[30] Huda, W.; Scalzetti, E.M.; Levin, G., Technique factors and image quality as functions of patient weight at abdominal CT, Radiol., 2000, 217, 430-435.
[31] Rao, P.S.; Alfidi, R.J., The environmental density artifact. A beam-hardening effect in computed tomography, Radiol., 1981, 141, 223-227.
[32] Rose, A., Sensitivity performance of the human eye on an absolute scale, J. Opt. Soc. Assoc., 1948, 38, pp196.
[33] Milne, E.N.C., The role and performance of minute focal spots in roentgenology with special references to magnification, CRC Critic. Rev. in Radiol. Sci., 1971, 2, 269-310.
[34] Wager, R.F.; Barnes, G.T.; Askins, B.S., Effect of reduced scatter content on radiographic information, contrast and patient exposure: a qualitative demonstration, Med. Phys., 1980, 7, 13-18.
[35] Friedrich, M.J., Studying cancer in 3 dimensions: 3-D models foster new insights into tumorgenesis, J. Am. Med. Assoc., 2003, 290, 1977-1979.
[36] Mueller, R.; Gerber, S.C.; Hayes, W.C., Micro-compression: a novel technique for non- destructive assessment of local bone failure, Technol. Health Care, 1998, 6, 433-444.
[37] Suki, B.; Lutchen, K.R.; Ingenito, E.P., On the progressive nature of Emphysema. Roles of proteases, inflammation and mechanical forces, Am. J. Resp. Crit. Care Med., 2003, 168, 516-552.
[38] Bove, A.A.; Ziskin, M.C.; Freeman, E.; Guilnez, J.L.; Lynch, P.R., Selection of optimum cine-radiographic frame rate, relation to accuracy of cardiac measurement, Invest. Radiol., 1970, 5, 329-335.
[39] Behrenbeck, T.; Kinsey, J.H.; Harris, L.D.; Robb, R.A.; Ritman, E.L., Three-dimensional spatial, density and temporal resolution of the dynamic spatial reconstructor, J. Comput. Assist. Tomogr., 1982, 6, 1118-1147.
[40] Mori, H.; Tanaka, E.; Hyodo, K.; Mohammed, M.U.; Sekka, T.; Ito, K.; Shinozaki, Y.; Tanaka, A.; Nakazawa, M.; Abe, S.; Handa, S.; Kutota, M.; Tamoka, K.; Umetani, K.; Ando, M., Synchrotron microangiography reveals configurational changes and to-and-fro flow in intramyocardial vessels, Am. J. Physiol.: Heart Circ. Physiol., 1999, 276, H429-H437.
[41] Dilmanian, F.A., Computed tomography with monochromatic x-rays, Am. J. Physiol. Imaging, 1992, 7, 175-93.
10Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
[42] Baldelli, P.; Taibi, A.; Tuffanelli, A.; Gambaccini, M., Dose comparison between conventional and quasi-monochromatic systems for diagnostic radiology, Phys. Med. Biol., 2004, 49, 4135-46.
[43] Rubenstein, E.; Hofstadter, R.; Zeman, H.D.; Thompson, A.C.; Otis, J.N.; Brown, G.S.; Giacomini, J.S.; Gordon, H.J.; Kerkhoff, R.S.; Harrison, D.C.; Thomlisson, W., Transvenous coronary angiography in humans using synchrotron radiation. Proc. Natl. Acad. Sci. USA, 1986, 83, 9724-9728.
[44] Zeman, M.D.; Sidons, D.P., Contrast agent choice for intravenous coronary angiography, Nucl. Instrum. Methods Phys. Res., 1990, A291, 67-73.
[45] Shikhaliev, P.M.; Xu, T.; Le, H.; Molloi, S., Scanning-slit photon counting x-ray imaging system using a microchannel plate detector, Med. Phys., 2004, 31, 1061-1071.
[46] Schlomka, J-P.; Delfs, J.; Barschdorf, H.; Thran, A.; van Stevendaal, U., Experimental feasility study of energy-resolved fan-beam coherent scatter computed tomography, IN: Developments in x-ray tomography IV, Bonse U. ed., Proc of SPIE, 2004, 5535, 410-423.
[47] Weidner, W.A.; Jacob, A.M.; Kenney, E.S.; Miller, K.L.; Tilley, D.G., Dynamic radiography an evaluation of cardiac motion by the analysis of scattered radiation during fluoroscopy, Invest. Radiol., 1975, 10, 132-139.
[48] Speidel, M.A.; Wilfley, B.P.; Heanue, J.A.; Betts, T.D.; Van Lysel, M.S., Comparison of vessel contrast measured with a scanning-beam digital x-ray system and an image intensifier/television system, Med. Phys., 2001, 28, 232-240.
[49] Kalender, W.A.; Wolf, H.; Seuss, C.; Giess, M.; Greess, H.; Bautz, W.A., Dose reduction in CT by on-line tube current control; principles and validation on phantom and cadavers, Eur. Radiol., 1999, 9, 323-328.
[50] Lewitt, R.M., Processing of incomplete measurements data in computed tomography, Med. Phys., 1979, 6, 412-417.
[51] Faridani, A.; Keinert, F.; Naterrer, F.; Ritman, E.L.; Smith, K.T., Local and global tomography, F.A. Grunbaum; J.W. Helton; P. Khargonekar (eds), Signal processing Part II (IMA Control Theory and applications) Springer-Verlag: New York, 1990, 23, 241-255.
[52] Möhlenkamp, S.; Lerman, L.O.; Bajzer, Z.; Lund P.E.; Ritman, E.L., Quantitation of myocardial microcirculatory function with x-ray CT, Ann. NY Acad. Sci., 2002, 972, 307-316.
[53] Menashe, B.; Macovski, A., Stimulated positron emission for 3-D tomographic imaging and bone studies – Part I: Method feasibility and system consideration, IEEE Trans. Med. Imaging, 1989, 8, 113-123.
[54] Momose, A.; Fukuda J., Phase-contrast radiographs of nonstained rat cerebellar specimen, Med. Phys., 1995, 22, 375-379.
[55] Davis, T.; Gao, D.; Gureyev, T.; Stevenson, A.; Wilkins, S., Phase contrast imaging of weakly absorbing materials using hard x-rays, Nature, 1996, 373, 335-338.
[56] Lewis, R., Medical phase contrast x-ray imaging: current status and future prospects, Phys. in Med. and Biol., 2004, 49, 3573-3583.
[57] Wernick, M.N.; Wirjadi, O.; Chapman D, Zhong Z, Galatsanos NP, Yang Y, Brtankov JG, Oltulu O, Anastasio MA, Muehleman C., Multiple image radiography, Phys. in Med. & Biol., 2003, 48, 3875-3895.
[58] Westkamp, T.; Diaz, A.; Nohammer, B.; Pfeiffer, E.A.; Rohbeck, T.; Cloetens, P.; Stampanoni, M.; David, C., Hard x-ray phase imaging and tomography with a grating interferometer, Proc SPIE, 2004, 5535, 137-142.
11Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49
[59] Beckman, F.; Bonse, U.; Busch, F.; Gunnewig, O., X-ray micro tomography (μCT) by phase contrast for the investigation of organic matter, J. Comput. Assist. Tomogr., 1997, 21, 539-55. [60] Keat, N.L., Real time CT and CT fluoroscopy. Report MDA/00/10, Medical Devices Agency: London, 2000.
12Copyright ©JCPDS-International Centre for Diffraction Data 2006 ISSN 1097-0002
Advances in X-ray Analysis, Volume 49