medication-assisted treatment for opiate addictionoct 20, 2008 · medication-assisted treatment...
TRANSCRIPT
Medication-Assisted Treatmentfor Opiate Addiction
First in a Four-Part Series on Innovations in Health PolicyFriday, October 17, 2008, 3:00 pm EDT
Supported by the Robert Wood Johnson Foundation as part of the NCSL Critical Health Areas Project (CHAP)
Supported through an unrestricted grant from Reckitt Benckiser Pharmaceuticals as part of the
NCSL Medication-Assisted Treatment for Opiate Addiction Project (MAT)
SpeakersSpeakersRepresentative Jerry MaddenRepresentative Jerry Madden, Texas, Texas
Frank Vocci, Ph.D.Frank Vocci, Ph.D., Director, Division of , Director, Division of Pharmacotherapies and Medical Pharmacotherapies and Medical Consequences of Drug Abuse, National Consequences of Drug Abuse, National Institute on Drug Abuse (NIDA), National Institute on Drug Abuse (NIDA), National Institutes of Health (NIH), U.S. Department Institutes of Health (NIH), U.S. Department of Health and Human Services (HHS) of Health and Human Services (HHS)
Doug AllenDoug Allen, Director, Division of Alcohol , Director, Division of Alcohol and Substance Abuse (DASA), Washington and Substance Abuse (DASA), Washington Department of Social and Health Services Department of Social and Health Services (DSHS) (DSHS)

Medication Assisted Treatment for Opiate Addiction
Frank Vocci, Ph.D.Director, Division of
Pharmacotherapies and Medical Consequences of Drug Abuse

Copyright restrictions may apply.
Heroin Addiction History
Hser, Y.-I. et al. Arch Gen Psychiatry 2001;58:503-508.

Efficacy of Methadone Concurrent Control Studies
• 100 male narcotic addicts randomized to methadone or placebo in a treatment setting
• Both groups initially stabilized on 60 mg methadone per day
• Both groups had dosing adjustments:– Methadone could go up or down– Placebo – 1 mg per day tapered withdrawalOutcome measures: treatment retention and imprisonment
Weeks in Treatment
% Retention Methadone
GroupPlacebo Group
32 76 10156 56 2
Imprisonment rate: twice as great for placebo group

Efficacy of Methadone Concurrent Control Studies
• 34 patients assigned to methadone or no methadone at one clinic
• Outcomes: percent drug freeFollow-up
TimePercent Drug Free
"Methadone Group"
Percent Drug Free “No Methadone
Group"2 years12/17 1/17
Five year follow-up: No methadone group offered methadone
Those choosing methadone: 8/9Those not choosing methadone: 1/95 Died of ODs, 2 Imprisoned

Evidence for the Efficacy of Methadone Dose Response Studies
• Dose Response Trials• Retention and illicit opiate use
N Methadone Doses
Results212
0,20,50 mg50 mg > 20 mg > 0
Strain, E., et al. Ann. Int. Med. 119:23-27, 1993
N Methadone Doses
Results162
20, 60 mg60 mg > 20 mg
Johnson RE, Jaffe J, Fudala PJ, JAMA, 267(20), 1992
Evidence for the Efficacy of Methadone Dose Response Studies
• Dose Response Analysis in Treatment: Effect on Retention
Capelhorn JRM, Bell J, J Med J Australia, 154, 1991
N Methadone Doses
Results286 < 60, 60-79, > 80 mg
80 mg > 60-79 mg > 60
• Dose Response Analysis in Treatment: Effect on IV Drug Use
N Methadone Doses
Results633 10-80mg
Dose related decrease in IV drug use
Ball JC, et al., Health Soc Behavior, 29, 1988
Evidence for the Efficacy of Methadone Dose Response Studies
• Outcomes: Retention and illicit opiate use
Ling et al, Arch Gen Psych, 53(5), 1996
N Methadone Doses
Results225 30 and 80 mg 80 > 30 mg
N Methadone Doses
Results140 20 and 65 mg 65 > 20 mg
Schottenfeld R, et al., 1993

0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12
In Treatment
Rate
28.9%
Months Since Drop Out
1-3Months
Later
4-6Months
Later
45.5%
57.6%
72.7%82.1%
7-9Months
Later
10-12Months
Later
Ball, JC, Ross A. The Effectiveness of Methadone Maintenance Treatment, Springer-Verlag, New York, 1991
Perc
ent I
V U
sers
Relapse to IV Drug Use After Termination of Methadone Maintenance Treatment

Efficacy of Methadone Epidemiological Studies and
Clinical StudiesStudy Size Treatment
% WeeklyDropout
NYC Avg 20,653 Methadone 0.76
DARP 12,297 Methadone 1.4Therapeutic Community 3.2
Drug Free Model 4.7TOPS 9,989 Methadone 2
Methadone Residential 3.7Outpatient 4.8
Newman 100 Methadone 0.85Placebo 7.1
Strain 212 Methadone 50 mg 2.3Methadone 20 mg 3.6
Placebo 7.1Capelhorn 238 Over 80 mg 0.3
60-80 mg 0.8Under 60 mg 2.1

Evidence for the Efficacy of Methadone
N Treatment Annual Death RateAge Adjusted
Control4,776 Untreated 7.0 0.6100 Treated 3.4 0.3109 Detox 8.33,000 MM 0.8368 MM 1.4 0.17
1
2
33
4
1 Prescore MJ, US Public Health Report, Suppl 170, 19432 Valliant GE, Addictive States, 1992¾ Gearing MF, Neurotoxicology, 19774 Grondblah L, ACTA Psych Scand, 82, 1990

0
2
4
6
8
MatchedCohort
Methadone VoluntaryDischarge
InvoluntaryDischarge
Untreated
0.150.85
1.65
6.91 7.20
Death Rates in Treated and Untreated Heroin Addicts
Annu
al R
a te

MM and Addicts’ Risk of Fatal Heroin Overdose
Authors Country # of Ss Comparison Groups
RR
Gearing, 1974
USA 14,474 1,170
Maint/ Discharged
0.27
Cushman, 1977
USA 1,623291
Maint/ Discharged
0.32
Gunne, 1981
Sweden 34/32 MM/No MM 0
Gronbladh, 1990
Sweden 1,143 1,406 MM/ Discharged
0.25
Poser, 1995
Germany 149/167 MM/Heroin 0.22
Caplehorn J. et al., Substance Abuse & Misuse, 1996

47%
23%
17%12.5%
6%
0%
10%
20%
30%
40%
50%Not in Tx
Currently in Tx
In Tx 5 years
C&D
No needle use since admission to Tx
A B C D
All subjects were male, heterosexual IV drug users in NYC. Treatment
provided was methadone maintenance.
The Effect of Methadone Treatments on HIV Seropositivity Rates
Novick et al., Presented at CPDD, 1985
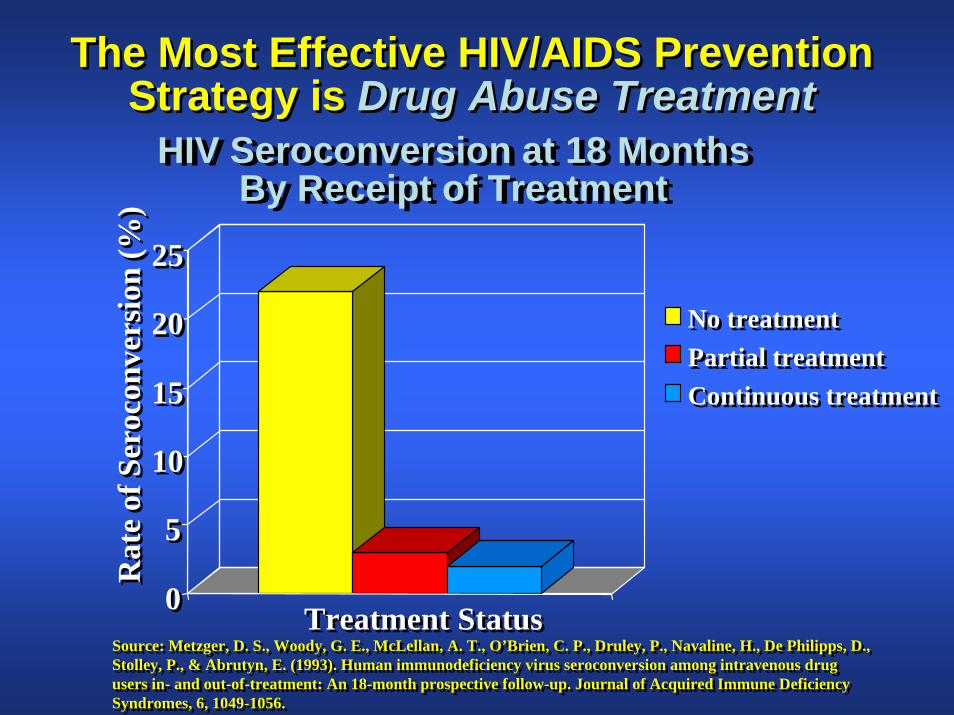
HIV Seroconversion at 18 MonthsBy Receipt of Treatment
HIV Seroconversion at 18 MonthsBy Receipt of Treatment
00
55
1010
1515
2020
2525
Rat
e of
Ser
ocon
vers
ion
(%)
Rat
e of
Ser
ocon
vers
ion
(%)
Treatment StatusTreatment Status
No treatmentNo treatmentPartial treatmentPartial treatmentContinuous treatmentContinuous treatment
Source: Metzger, D. S., Woody, G. E., McLellan, A. T., O’Brien, C. P., Druley, P., Navaline, H., De Philipps, D., Stolley, P., & Abrutyn, E. (1993). Human immunodeficiency virus seroconversion among intravenous drug users in- and out-of-treatment: An 18-month prospective follow-up. Journal of Acquired Immune Deficiency Syndromes, 6, 1049-1056.
Source: Metzger, D. S., Woody, G. E., McLellan, A. T., O’Brien, C. P., Druley, P., Navaline, H., De Philipps, D., Stolley, P., & Abrutyn, E. (1993). Human immunodeficiency virus seroconversion among intravenous drug users in- and out-of-treatment: An 18-month prospective follow-up. Journal of Acquired Immune Deficiency Syndromes, 6, 1049-1056.
The Most Effective HIV/AIDS PreventionStrategy is Drug Abuse Treatment
The Most Effective HIV/AIDS PreventionStrategy is Drug Abuse Treatment

Criminality in Addicted and No Longer Addicted Opiate Addicts_
Nurco et al., 1985


Buprenorphine(Heroin, Morphine, Methadone)
(Buprenorphine)
“Ceiling Effect”

Mu Opiate Partial Agonist
• Ceiling effect imparts safety• Less respiratory depression• Less risk of overdose• Less physical dependence capacity• Naloxone added to reduce abuse
liability

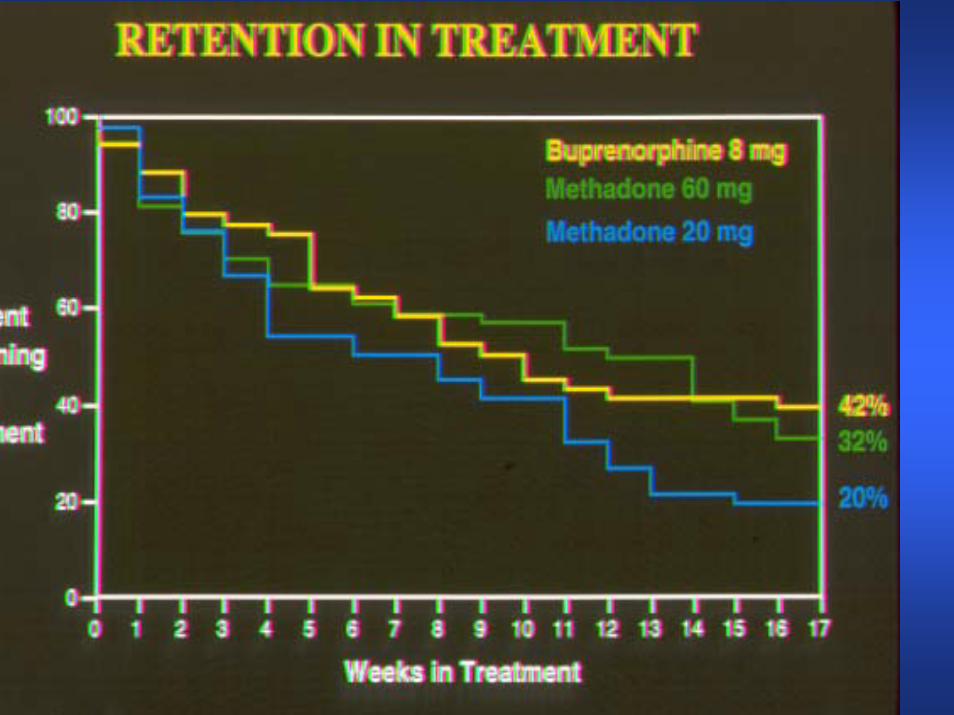
Initial Efficacy study
• Performed in Baltimore at the ARC/ IRP• Investigators- Johnson, Jaffe, Fudala• Compared 8 mg sublingual buprenorphine
to 20 and 60 mg of oral methadone in a randomized, double dummy design for 17 weeks
• Evaluated opiate use and retention in treatment
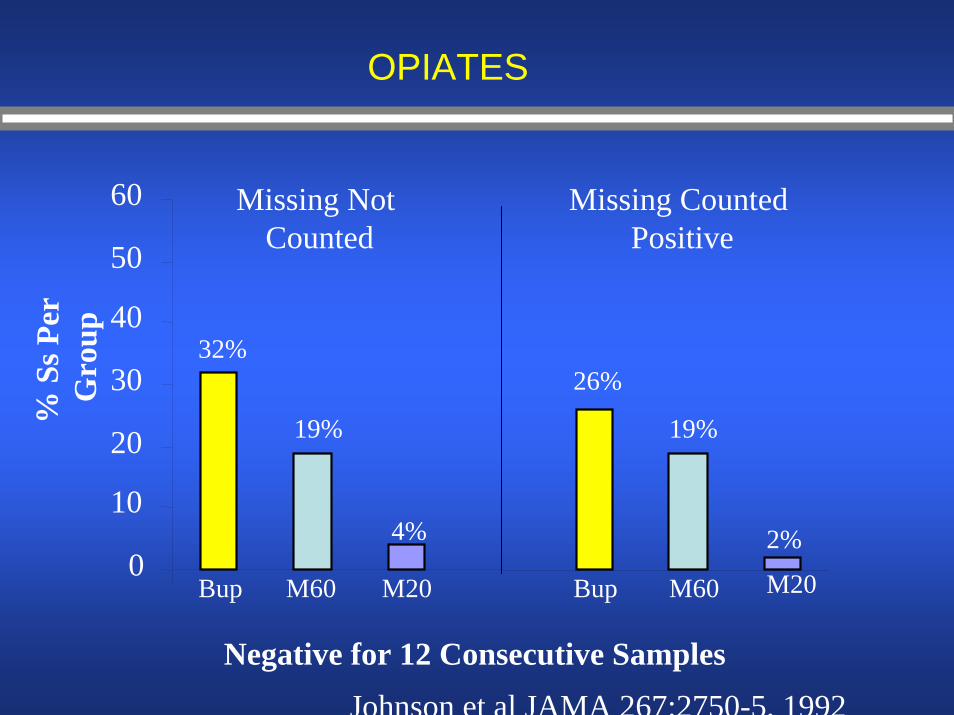
OPIATES
0
10
20
30
40
50
60
% S
s Per
G
rou p
Negative for 12 Consecutive Samples
Missing Not Counted
Missing Counted Positive
32%
19%
4%
26%
19%
2%
Bup BupM60 M60M20 M20
Johnson et al JAMA 267:2750-5, 1992
First Multicenter Study of Buprenorphine
• Performed in VA methadone clinics• 1, 4, 8 and 16 mg doses of buprenorphine
administered to 735 opiate dependent subjects
• A priori comparison was 1 versus 8 mg• Evaluated reduction in opiate use and
retention

Study #999A: Buprenorphine’s Effect on Opiate Use
0
5
10
15
20
25
30
1 4 8 16
Buprenorphine Dose (mg)
% S
s with
13
Con
secu
tive
Opi
ate
Free
Uri
nes
Ling et al Addiction 93:475-86, 1998

Buprenorphine Tablet Efficacy Trial



Buprenorphine Status
• Buprenorphine Products Mono (SUBUTEX) and combo (SUBOXONE)– Approved by FDA in October 2002
• DATA of 2000 allows qualified physicians to prescribe FDA approved opiates for opiate addiction … Waiver program run by SAMHSA
• Over 20,000 physicians have become qualified to prescribe buprenorphine products
• New mode of therapy… office-based
Buprenorphine Status
• Over 500,000 patients have been treated with the buprenorphine products
• About 170,000 patients are receiving one of the buprenorphine products at any time

Drug Misuse/Abuse-Related EmergencyDepartment (ED) Visits in the United States
(Source: U.S. SAMHSA; DAWN 2005 Report)
http://dawninfo.samhsa.gov
*Includes single drug and drug combination products
HeroinNarcotic analgesicsHydrocodone *Oxycodone *Fentanyl *Buprenorphine *
020,00040,00060,00080,000
100,000120,000
140,000
160,000
180,000
164,572160,363
51,22542,810
9,1600

• Prescription opiate users were younger, had fewer years of opiate use, less drug txhistory, more likely to be white, earn more income, and less likely to be Hep C +
• More likely to complete tx• More likely to stay in tx longer• Had a higher % of opiate-free urines
J GIM 2007

A Comparison of Levomethadyl Acetate, Buprenorphine, andMethadone for Opioid Dependence
Rolley E. Johnson, Pharm.D., Mary Ann Chutuape, Ph.D., Eric C. Strain, M.D., Sharon L. Walsh, Ph.D., Maxine L. Stitzer, Ph.D., and George E. Bigelow, Ph.D. NEJM 343:1290-1297,2002
ABSTRACT
Background Opioid dependence is a chronic, relapsing disorder with important public health implications.
Methods In a 17-week randomized study of 220 patients, we comparedlevomethadyl acetate (75 to 115 mg), buprenorphine (16 to 32 mg), and high-dose 60 to 100 mg) and low-dose (20 mg) methadone as treatments for opioid dependence. Levomethadyl acetate and buprenorphine were administered three times a week. Methadone was administered daily. Doses were individualized except in the group assigned to low-dose methadone. Patients with poor responses to treatment were switched to methadone.

Comparative efficacy of LAAM, methadone and buprenorphine

BUP-START & POATS
• 1000 opiate dependent patients will be randomized to either Bup/Nx or methadone in opiate treatment programs associated with the CTN
• Patients will have viral hepatitis exposure and HIV status assessed at beginning of trial
• Liver transaminases will be assessed• POATS – evaluation of Bup/Nx in
prescription opiate dependent patients -CTN study

Naltrexone • Is a narcotic antagonist• Is indicated for the prevention of relapse in
formerly dependent opiate users• Is used primarily by health professionals & other
highly motivated persons• Is available in oral and depot injection dosage
forms• The depot form has not been approved for use
in treatment of opiate dependence • NIDA just funded a multi-center trial in treatment
of opiate dependent subjects in the Criminal Justice System




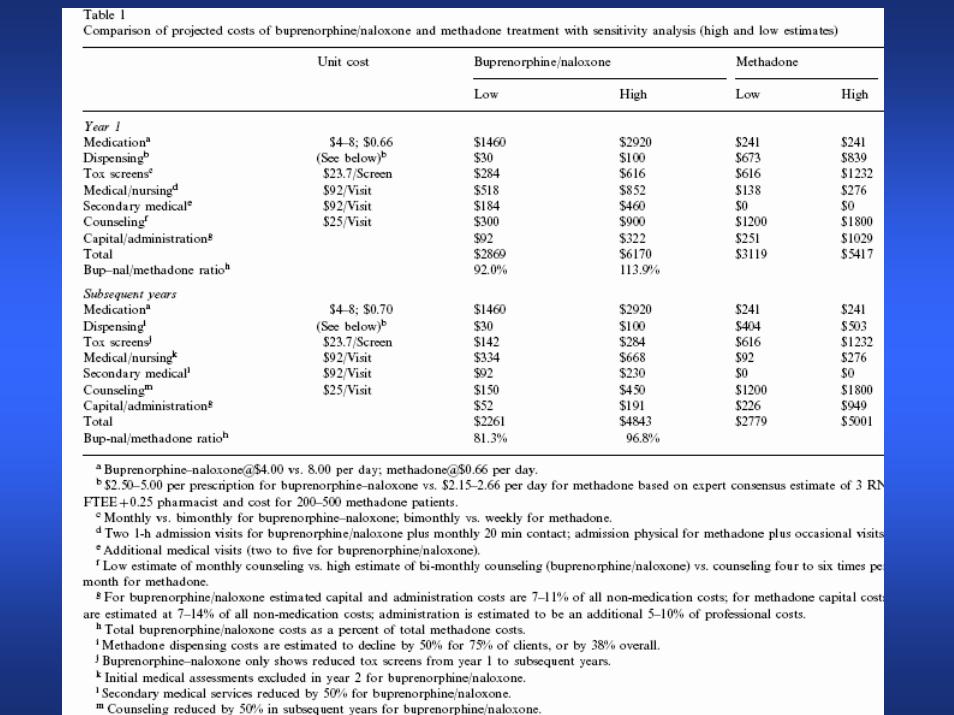
Cost of Opiate Treatment Delivery
• Methadone is dispensed in specialty clinics- Opiate Treatment Programs
• The cost of methadone itself is nominal ( < $1 /day) but the cost of treatment far exceeds that
• Naltrexone and Buprenorphine can be prescribed– Office visit fee– Fee for the medicine
0
5,000
10,000
15,000
20,000
25,000
Untreated Incarceration Adolescent Adult Methadone Drug Free
Residential Outpatient
$1,575$1,750
$8,250$9,825
$20,000$21,500
No Treatment
In Treatment Program
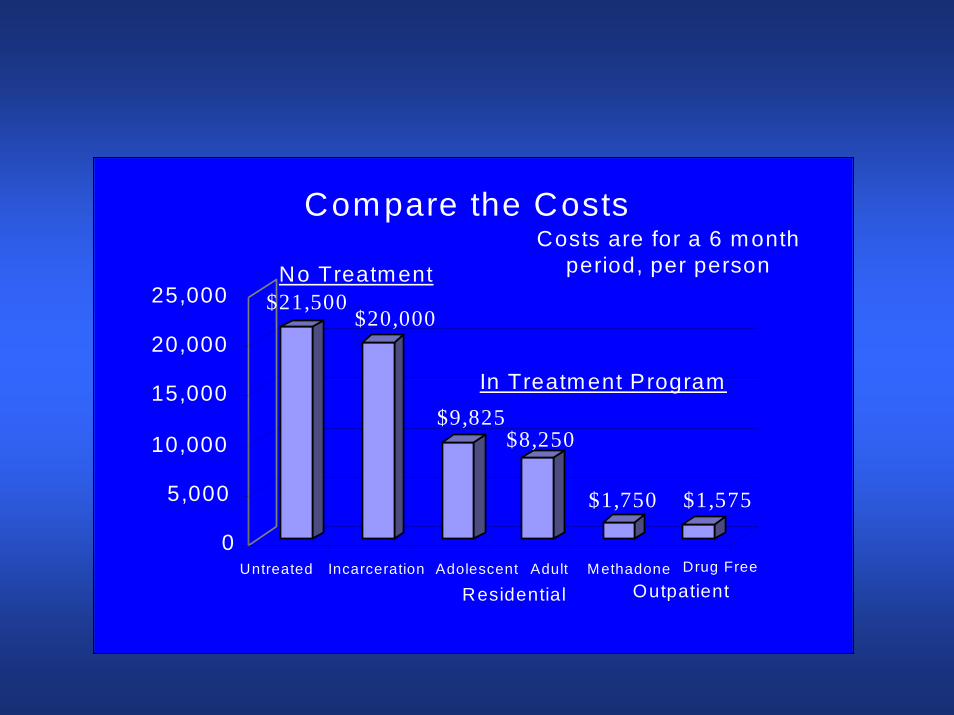
Compare the CostsCosts are for a 6 month
period, per person

Cost-comparison Between Treatment and Incarceration
• Incarceration costs @ $ 55,000 per year• Treatment with methadone costs @ $
5000 per year• Treatment with buprenorphine/naloxone
costs @ $ 6000 per year• Both are significantly cheaper that
incarceration

Summary
• Treatment of opiate dependence with methadone reduces opiate use and the risk of death by overdose, reduces injection drug use and the risk of contracting and spreading HIV, improves the health of the patients, and reduces criminal activity
• Methadone and buprenorphine therapy for opiate dependence cost @ 1/10 the cost of incarceration

Thanks for your Attention

Treatment Outcome- DATOS

Outcomes of Treatment-Australian Treatment Outcome Study

Outcome of Treatment -NTORS

Medication-Assisted Treatment for Opioid Addiction
State Actionsand
Policies
Doug AllenDirector, Division of Alcohol & Substance AbuseState of WashingtonOctober 17, 2008

Medication-Assisted Treatment (MAT)
• Why consider MAT?
– Increase in misuse/abuse of prescription drugs and heroin.
– Clinical - greater relapse in abstinence-based programs for opioid addiction.
– Treatment is effective - decreased medical costs, rearrest rates, improved employment, social well-being.

Methadone(Antagonist)
• Clinic-Based (Stationary or Mobile)
– Regulated 42 CFR Part B accreditation (JACHO, CARF, State)• Medical services, exam, medication• Psycho-Social
– Access - Community issues, large numbers– Funding (Medicaid, state, private pay)– Diversion Issues

Suboxone(Partial Antagonist)
• Office-Based Opioid Treatment – Physicians
– Physician training– Psycho-social needs to be coordinated– Access - physician’s office vs. treatment
center– Funding (Medicaid, private, state)– Cost– 30 patients/waiver for more

Suboxone (cont’d)
• Opioid Treatment Programs (OTP)
– Physician training– 42 CFR applies– Psycho-social included– Access– Funding (Medicaid, state)– Stigma

Suboxone (cont’d)
• Substance Abuse Treatment Centers
– Physician training required– Psycho-social included– Access– Funding (Medicaid, state, private)
Naltrexone(Receptor Blocker)
• Patient
– Stable lifestyle– Highly motivated

References• 42 CFR, Part B
• “Medication-Assisted Treatment for Opioid Addition in Opioid Treatment Programs,” TIP 43
• NASADAD - “State Issue Brief on the Use of Buprenorphine and Implications for State AOD Systems
• “Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction,” TIP 40
• Buprenorphine - Physician and Treatment Program Locator,http://www.buprenorphine.samhsa.gov/bwns_locator/index.html
• National Council of State Legislators - MAT - Medication-Assisted Treatment for Opiate Addiction, http://www.ncsl.org/programs/health/forum/mat.htm

Any QuestionsAny Questions
Among the Panelists?Among the Panelists?
From the audience?From the audience?–– Use Q and A option in your webUse Q and A option in your web--assisted assisted
audioconference.audioconference.
After the callAfter the call–– [email protected]@ncsl.org

To follow upTo follow upFeel free to contact us for more Feel free to contact us for more information atinformation [email protected]@ncsl.org
For more program information and related For more program information and related links, and to see past links, and to see past programs:programs: http://www.ncsl.org/programs/http://www.ncsl.org/programs/health/webcast2.htmhealth/webcast2.htm
This program was recorded and will be This program was recorded and will be made available on line.made available on line.

Additional resourcesAdditional resources
National Institute on Drug Abuse National Institute on Drug Abuse http://www.nida.nih.govhttp://www.nida.nih.gov
Washington Division of Alcohol and Washington Division of Alcohol and Substance AbuseSubstance Abusehttp://www1.dshs.wa.gov/dasahttp://www1.dshs.wa.gov/dasa

Resources from NCSLResources from NCSL
MedicationMedication--Assisted Treatment for Opiate Assisted Treatment for Opiate AddictionAddictionhttp://www.ncsl.org/programs/health/forum/mat.htmhttp://www.ncsl.org/programs/health/forum/mat.htm
Forum for Health Policy LeadershipForum for Health Policy LeadershipCritical Health Areas ProjectCritical Health Areas Project
http://www.ncsl.org/programs/health/forum/chap/inhttp://www.ncsl.org/programs/health/forum/chap/index.htmdex.htm