medication therapy management of chronic … therapy management of chronic obstructive pulmonary ......
TRANSCRIPT

1
Medication Therapy Management of Chronic Obstructive Pulmonary
Disease

2
Overview and Epidemiology of Chronic Obstructive Pulmonary
Disease (COPD)

3
COPD
• COPD is a chronic disease characterized by airflow limitation that is not fully reversible
• This airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases
Chronic obstructive pulmonary disease is characterized by airflow limitation that’s not fully reversible. The airflow limitation in COPD is typically progressive and it’s associated with an abnormal inflammatory response of the lungs to noxious particles or gases.

4
COPD: The Forgotten Disease
• For more than a decade, COPD has been largely ignored because clinicians felt that there was nothing that could be done.
• With new knowledge and new therapies, there is renewed interest about the prevention and management of COPD.

5
Jemal, A. et al. JAMA 2005;294:1255-1259.
Trends in Age-Standardized Death Rates for the 6Leading Causes of Death in the United States, 1970-2002

6
COPD Facts
• In United States, 10.7 million people have physician diagnosis of COPD
• 24 million have impaired lung function• COPD is 4th leading cause of death• In 2002, reported deaths from
COPD=120,555• Between 1965 and 1998, COPD death
rate increased 163%
American Lung Association. Trends. May 2005.
Switching to some COPD statistics, in the United States nearly 11 million people have a physician diagnosis of COPD, but the impact of the disease is felt to be much higher in that in various surveys nearly 24 million people report having impaired lung function as measured by spirometry. COPD is a leading cause of death in the United States, currently representing the fourth leading cause of death. In 2002, over 120,000 deaths in the United States were attributed to COPD. And since the turn of the century, female death rate from COPD has exceeded that of males.

7
COPD Mortality Rates
NHLBI. Morbid Mortal Chartbook. 2004.
This slide summarizes the growth in death rate from COPD that’s been observed over the last 20 years and the more rapid death rate growth seen in females compared to males.

8
Epidemiology
• COPD is a leading cause of morbidity and mortality worldwide, and results in an economic and social burden that is both substantial and increasing.
• Prevalence and morbidity data greatly underestimate the total burden of COPD because the disease is usually not diagnosed until it is clinically apparent and moderately advanced.

9
Indirect costs44%
Direct Expenditures
56%
Indirect Morbidity
45%
Early Mortality
55%
Economic Cost of COPD
American Lung Association. Trends in Chronic Bronchitis and Emphysema. May 2005.
Total costs: $37.2 billion (estimated)
Direct costs: $20.9 billion (56%)
Indirect costs: $16.3 billion
The economic cost of COPD is very significant as well. In this case, you can see the direct cost and the indirect cost are fairly equal.

10
Medication Management and Related Services for the COPD Patient
• Tobacco cessation counseling and risk factor avoidance
• Immunizations• Recommendation and selection of
medication and device products• Education about proper use of medication• Monitoring for safety and efficacy of
therapy• Considering therapeutic alternatives and
cost

11
Medication Management and Related Services for the COPD Patient
(continued)
• Monitoring co-morbidities and potential interactions
• Provision and monitoring of oxygen therapy
• Provision of home care equipment and supplies
• Referral to other community services and resources

12
COPD Etiology
• 80% to 90% of COPD is attributed to a current or past history of cigarette smoking
• Other causes/factors include:– Air pollution– Exposure to secondary cigarette smoke– History of serious respiratory infections during
childhood– Genetics (including Alpha-1 antitrypsin (AAT)
deficiency)– Occupational exposures
The primary causative factor of COPD is a current or past history of cigarette smoking. Other causes include exposure to environmental pollutants as might occur during air pollution or due to occupational exposures, exposure to secondhand tobacco smoke, a history of serious respiratory infections during childhood. There’s also a rare inherited disorder, called 1-antitrypsin deficiency, which can result in emphysema.

13
COPD Phenotypes
• Chronic bronchitis– Chronic inflammation present in bronchial
tubes, increased mucus production, and productive cough
– Common features: chronic cough with mucus production, shortness of breath, and recurrent infections
• Emphysema– Destruction of alveoli units resulting in
decreased gas exchange– Common features: cough, shortness of breath,
and decreased exercise tolerance
COPD is commonly broken down into two major phenotypes or two presentations of the disease. Patients with chronic bronchitis typically have chronic inflammation in the airway, increased mucus production, and a chronic cough. These patients have a cough during several months of the year, and their main complaints are shortness of breath and they suffer from recurrent infections of the airway.
The other major type is emphysema. In emphysema there’s destruction of the alveolar units of the airway resulting in decreased gas exchange. Patients with emphysema chronically complain of a cough, although it’s typically nonproductive. They also complain of shortness of breath and reduced exercise tolerance.

14
COPD Pathogenesis
Lung inflammation
COPD pathology
Oxidative stress Proteinases
Antioxidants Antiproteinases
Noxious particles and gases
Repair mechanisms
www.goldcopd.com
Chronic exposure to noxious particles and gases that are present in tobacco smoke or in the environment result in inflammation in COPD. This chronic inflammation results in an increase in oxidative stress and in the activity of various proteinases that are present in the airway. These two processes result in the damage that characterizes COPD.

15
releaserelease
Inflammatory Process in COPD
Adapted from: NHLBI/WHO. Global Initiative for Chronic Obstructive Lung Disease. April 2001 (Updated 2003). Barnes PJ. N Engl J Med. 2000;343:269-80.
activatesactivates
NeutrophilsNeutrophils
Macrophages inrespiratory
tract
Macrophages inrespiratory
tract
ProteasesProteases result inresult in
releaserelease
ParenchymalDestruction
Although inflammation also plays a role in COPD, the nature of the inflammation differs from that seen in asthma. The most common cause of COPD is an exposure to tobacco smoke. As I’ve summarized on this slide: components of tobacco smoke stimulate an inflammatory reaction involving various cells in the airway of patients with COPD, and ultimately resulting in parenchymal destruction or loss of lung tissue.
16
Dyspnea
Activity
Exercise Tolerance
Consequences of Airflow Limitation
Exacerbations
Lung HyperinflationGas Trapping
Airflow Limitation
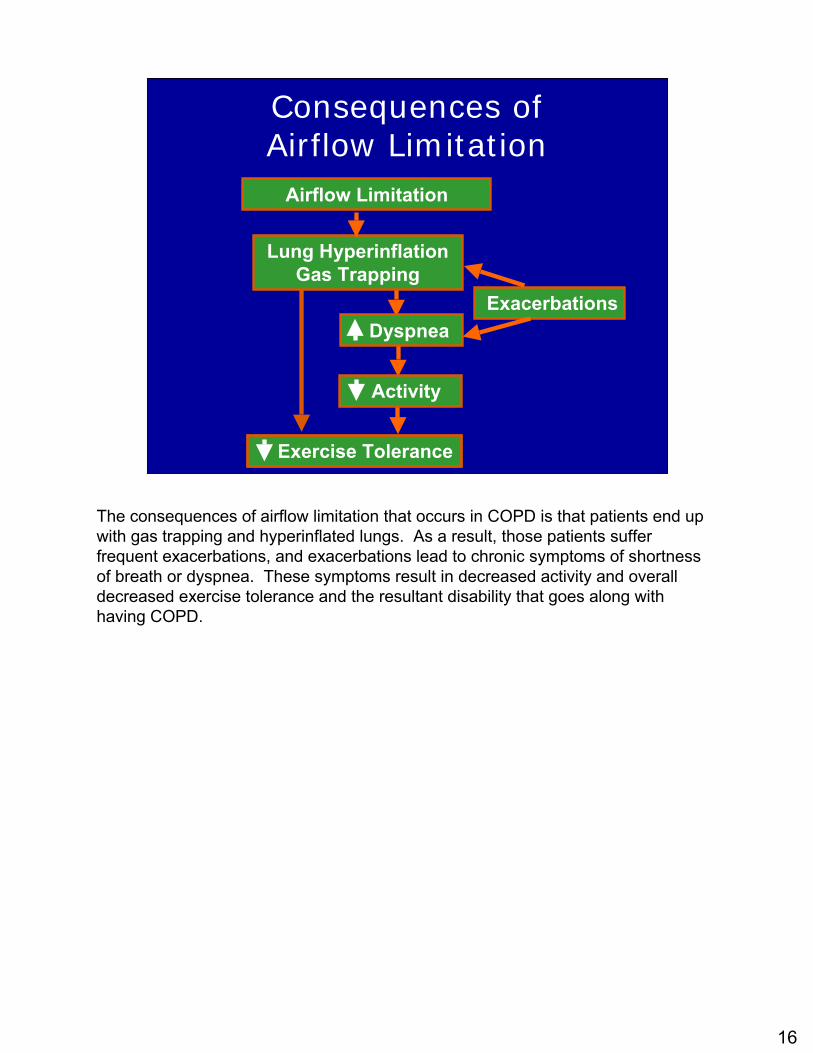
The consequences of airflow limitation that occurs in COPD is that patients end up with gas trapping and hyperinflated lungs. As a result, those patients suffer frequent exacerbations, and exacerbations lead to chronic symptoms of shortness of breath or dyspnea. These symptoms result in decreased activity and overall decreased exercise tolerance and the resultant disability that goes along with having COPD.

17
Diagnosis of COPD
• Diagnosis of COPD should be considered in any patient who has the following:– Symptoms of cough– Sputum production– Dyspnea– History of exposure to risk factors for the disease
• Spirometry should be obtained in all persons with the following history:– Exposure to cigarettes and/or environmental or
occupational pollutants– Family history of chronic respiratory illness– Presence of cough, sputum production or dyspnea

18
Spirometry Patterns
0
1
2
3
4
5
6
0 1 2 3 4 6 7
Normal
COPD
Asthma (Pre-albuterol)Asthma (Post-albuterol)
Lite
rs
Seconds
This graph demonstrates spirometry results for normal patients as well as patients with asthma and COPD. The top line represents spirometry from a normal patient.
After taking a maximal inhalation, a patient is instructed to blow out as hard and fast as possible. In the normal situation, the majority of air that leaves the lung comes out within the first second and then the remainder of the air leaves the lung over the next several seconds.
In a patient with COPD, as demonstrated on the bottom line, both the rate of airflow out of the lung and the total amount of air that leaves the lung is actually reduced.
In a patient with asthma, as is depicted in the middle two lines, before treatment of asthma the rate of airflow out the lung is decreased and actually looks similar to a patient with COPD. Because the airflow obstruction in asthma is largely reversible after treatment with a bronchodilator, the rate of airflow out of the lung approaches that of a normal person.

19
Biologic Features
Squamous metaplasia of epitheliumParenchymal destructionMucous metaplasiaGlandular enlargement
Fragile epitheliumThickened basement membraneMucous metaplasiaGlandular enlargement
Structural consequences
LTB4
IL-8TNF-alpha
LTD4
IL-4, IL-5Mediators
NeutrophilsMacrophagesCD8+ lymphocytes
EosinophilsCD4+ TH2 lymphocytesActivation of mast cells
Cellular infiltration
COPDAsthma

20
Clinical Features
Airflow limitation -largely irreversibleAirway hyperresponsiveness -variable
Airflow limitation -largely reversibleAirway hyperresponsiveness -significant
Physiologic
Midlife onsetSlowly progressive symptomsProminent smoking history
Early onset (<40 years)Varying or intermittent symptomsNight-time symptomsPresence of allergy, rhinitis, eczema or combination of theseFamily history
History & presentation
COPDAsthma
Mucous

21
Severity Classification for COPD
<30%<0.7Very Severe COPD
>30% up to 50%
<0.7Severe COPD
>50% up to 80%
<0.7Moderate COPD
> 80%<0.7Mild COPD
>80%>0.7At Risk*
Predicted FEV1
Post-BD FEV1/FVC
Severity
*Patients with positive smoking history or exposure to pollutants; symptoms of cough, sputum production or dyspnea; or family history of respiratory disease.
Post-BD = post bronchodilator, FEV1 = forced expiratory volume at 1 second
FVC = Forced Expiratory Vital Capacity American Thoracic Society. 2005.
The American Thoracic Society and the GOLD Guidelines also provide a severity classification for patients with COPD. COPD is categorized based on spirometry results; the primary result being the predicted FEV1. This ranges from patients with mild COPD, or patients who are at risk for COPD who have fairly normal FEV1’s at greater than or equal to 80%. Patients who have FEV1’s of less than 80% are categorized as having COPD ranging in severity from moderate to very severe disease.

22
Patient Characteristics
• At Risk: experiences morning cough • Stage 1: no limitation, but symptoms with
exercise• Stage 2: activities are limited, symptoms
more chronic• Stage 3: patient is restricted in what they
can do; dyspnea is chronic; frequent exacerbations
• Stage 4: ‘bed to chair’ existence; end of life planning appropriate

23
Limitation of Activities Due to COPD
ATS = American Thoracic SocietyCoultas DB et al. Am J Respir Crit Care Med. 2001;164:372-7.
(severe)(moderate)
(mild)(mild)
Perc
ent
0
5
10
15
20
25
30
35
40
45
50
Normal ATS Ia ATS Ib ATS II ATS III
Difficulty walking 1/4 mile
Poor general health
Difficulty lifting/carrying 10 lb
Needing help with personal care
From a patient’s perspective, you can see the impact that COPD has on their activities in daily living and some normal activities that patients might participate in, again, ranging from mild to severe disease.

24
Factors Determining Severity Of Chronic COPD
• Severity of symptoms, including dyspnea• Severity of airflow limitation• Frequency and severity of exacerbations• Presence of complications of COPD• Presence of respiratory insufficiency• Co-morbidity• General health status (including nutrition)
– Low BMI (<21) associated with poor outcomes
• Number of medications taken

25
COPD Exacerbations Impact onCOPD Exacerbations Impact onLung FunctionLung Function
Donaldson GC, et al. Thorax 2002;57:847Donaldson GC, et al. Thorax 2002;57:847
0.750.75
0.800.80
0.850.85
0.900.90
0.950.95
FEVFEV11 (L)(L)
1100 22
Years in studyYears in study33 44
Infrequent Infrequent exacerbatorsexacerbators (n = 16)(n = 16)FEVFEV11 change = 32 ml/yearchange = 32 ml/year
Frequent Frequent exacerbatorsexacerbators (n = 16)(n = 16)FEVFEV11 change = 40 ml/yearchange = 40 ml/year
(>2.92/yr)
(<2.92/yr)

26
Gunen H et al. Eur Respir J. 2005;26:234-41
COPD Exacerbations: Survival
0.5
0.6
0.7
0.8
0.9
1.0
0 200 400 600 800 1000Follow-up daysn = 205 patients
Cum
ulat
ive
surv
ival
24%
33%39%
49%
1200
8.3% mortality 1st admission

27
Impact of Exacerbations on COPD Mortality
• Following hospitalization for a COPD exacerbation, mortality rates are –22 to 43% after 1 year–36 to 49% after two years
• Factors associated with higher mortality– Increasing age–Higher partial carbon dioxide(pCO2)–Chronic prednisone therapy–Reduced health status and co-
morbidities

28
Management Strategies for COPD

29
CTSCTSGOLDGOLD
ATS/ERS
NICENICE
Available Guidelines for COPD
BalterBalter et al. et al. Can Respir J.Can Respir J. 2003;10:3B2003;10:3B--32B (A); 32B (A); Global Initiative for Chronic Obstructive Lung Global Initiative for Chronic Obstructive Lung Disease. Workshop Report Updated 2005. Available at: Disease. Workshop Report Updated 2005. Available at: http://www.http://www.goldcopdgoldcopd.com/.com/GuidelineitemGuidelineitem.asp?l1=2&l2=1&.asp?l1=2&l2=1&intIdintId=989. Accessed October 20, =989. Accessed October 20, 2005 (A).2005 (A).; Celli et al and the ATS/ERS Task Force. ; Celli et al and the ATS/ERS Task Force. Eur Respir JEur Respir J. 2004;23:932. 2004;23:932--946 (A); 946 (A); National Institute for Clinical Excellence. Clinical Guideline 1National Institute for Clinical Excellence. Clinical Guideline 12; February 2004 (A).2; February 2004 (A).

30
Objectives of COPD Management
• Prevent disease progression • Relieve symptoms• Improve exercise tolerance• Improve health status• Prevent and treat exacerbations• Prevent and treat complications• Reduce mortality• Minimize side effects from treatment

31
Components of COPD Management
• Patient education• Assess and monitor disease• Reduce risk factors• Manage stable COPD• Manage exacerbations

32
Treatment Strategies Based on Severity

33
Patient Education
• Causes and natural course of COPD• Recognizing signs and symptoms• Avoiding exposure to risk factors• Role and proper use of medications• Inhalation techniques• Pulmonary rehabilitation• Supplemental oxygen therapy• Recognizing exacerbations• End of life decisions

34
Chronic Management Of COPD(GOLD Guidelines Am J Respir Crit Care Med 2001;163:1256-1276)
DiagnoseDiagnose
Reduce Reduce RiskRisk
Smoking cessationImmunizeReduce other exposures
Reduce Reduce SymptomsSymptoms
Reduce Reduce ComplicationsComplications
BronchodilatorsConsider inhaled steroidsPulmonary rehabilitation
Consider oxygenTreat exacerbations
Spirometry
Education
Education
Education
Education
35
Reduce Risk Factors:Key Points
• Reducing exposure to tobacco smoke, occupational dusts, and chemicals, and indoor and outdoor air pollutants
• Smoking cessation is the single most effective -- and cost-effective -- intervention to reduce the risk of developing COPD and stop its progression
36
Reduce Risk Factors:Key Points
• Brief tobacco dependence treatment is effective and every tobacco user should be offered at least this treatment at every visit
• Three types of counseling are especially effective: practical counseling, social support as part of treatment, and social support arranged outside of treatment

37
100
75
50
25
025 50 75
Smokedregularly andsusceptible toits effects
Never smokedor notsusceptibleto smoke
Stoppedat 45
Stopped at 65
Disability
Death
AGE (YEARS)
FEV
(% o
f val
ue a
t age
25)
1
† †
Fletcher & Peto, BMJ, 1977
COPD Risk and Cigarette Smoking
In women severe obstruction associated with accelerated decline.
38
The 5 As for Tobacco Cessation
ASK about tobacco USE
ADVISE tobacco users to QUIT
ASSESS READINESS to make a quit attempt
ASSIST with the QUIT ATTEMPT
ARRANGE FOLLOW-UP care
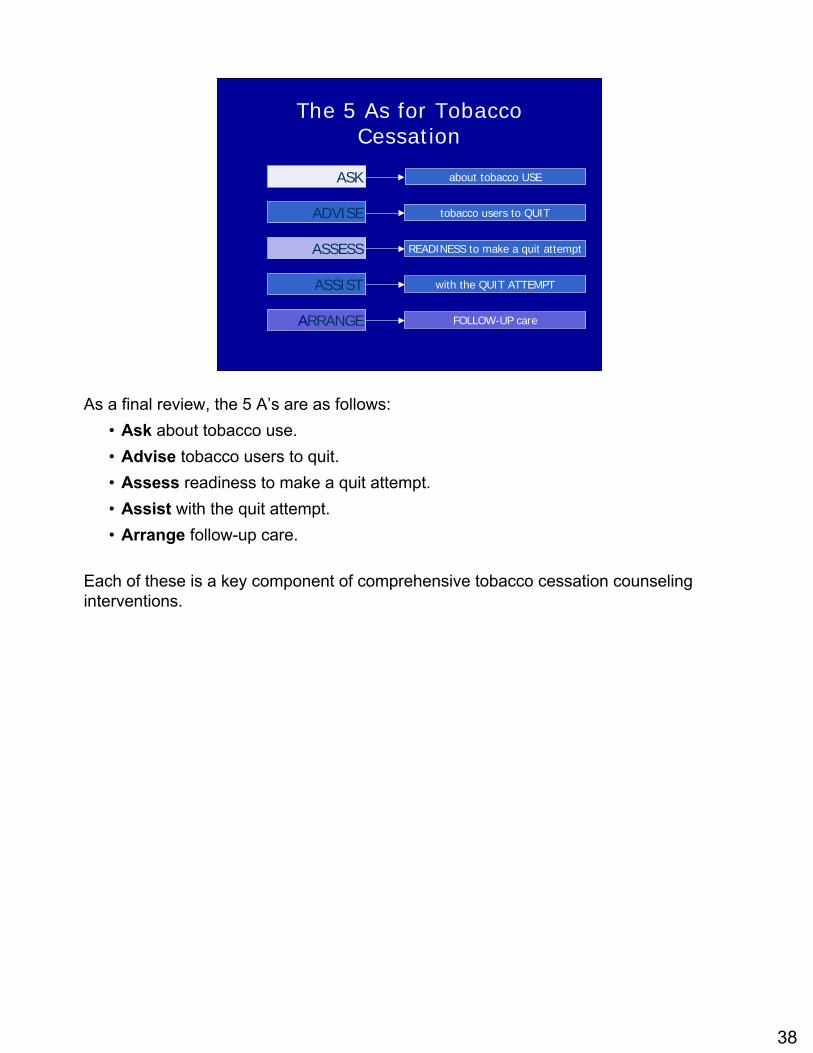
As a final review, the 5 A’s are as follows:• Ask about tobacco use.• Advise tobacco users to quit.• Assess readiness to make a quit attempt.• Assist with the quit attempt.• Arrange follow-up care.
Each of these is a key component of comprehensive tobacco cessation counseling interventions.

39
The 5 Rs—Methods for increasing motivation:–Relevance
–Risks
–Rewards
–Roadblocks
–Repetition
Fiore et al. (2000). Treating Tobacco Use and Dependence. Clinical Practice Guideline.Rockville, MD: USDHHS, PHS.
NOT READY to QUITCounseling Strategies
For patients who are not ready to quit, clinicians can deliver tailored, motivational messages by applying the 5 R’s:
Relevance: Encourage the patient to indicate why quitting is personally relevant. Be as specific as possible. Motivational information has the most impact if it is relevant to the patient’s disease status or risk, family or social situation (e.g., having children in the home), health concerns, age, sex, and other important patient characteristics (e.g., prior quitting experience, personal barriers to cessation).Risks: Ask the patient to identify consequences of tobacco use. Suggest and highlight those that seem most relevant to the patient and emphasize that other forms of tobacco (such as smokeless, or lower-tar-level cigarettes) will not eliminate the risks. Risks of tobacco use are discussed in the Epidemiology of Tobacco Use and Pathophysiology of Tobacco-Related Disease modules.Rewards: Ask the patient to identify benefits of quitting. Highlight those that seem relevant to the patient. Examples of benefits of cessation are discussed in the Epidemiology of Tobacco Use module. Roadblocks: Ask the patient to identify barriers to quitting and potential methods for circumventing each barrier. Suggest and highlight those that seem most relevant to the patient. Common barriers include withdrawal symptoms, fear of failure, weight gain, lack of support, depression, and enjoyment of tobacco.Repetition: Repeat the motivational intervention whenever possible. Tobacco users who have failed in previous quit attempts should be reminded that most people make repeated quit attempts before they are successful.
Fiore MC, Bailey WC, Cohen SJ, et al. (2000). Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service.

40
Effects of Clinician Interventions
Fiore et al. (2000). Treating Tobacco Use and Dependence. Clinical Practice Guideline.Rockville, MD: USDHHS, PHS.
0
10
20
30
No clinician Self-helpmaterial
Nonphysicianclinician
Physicianclinician
Type of Clinician
Esti
mat
ed a
bsti
nenc
e at
5+
m
onth
s1.0 1.1
(0.9,1.3)
1.7(1.3,2.1)
2.2(1.5,3.2)
n = 29 studies
Decades of research tell us that clinicians can have an important impact on their patients’ likelihood of achieving cessation. A meta-analysis of 29 studies determined that patients who received a tobacco cessation intervention from a nonphysicianclinician or a physician clinician were 1.7 and 2.2 times as likely to quit (at 5 or more months postcessation), respectively, compared with patients who did not receive suchan intervention (Fiore et al., 2000). Self-help materials were only slightly better than no clinician.
Fiore MC, Bailey WC, Cohen SJ, et al. (2000). Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service.

41
• Discuss coping strategies–Cognitive coping strategies
• Focus on retraining the way a patient thinks
–Behavioral coping strategies
• Involve specific actions to reduce risk for relapse
STAGE 2: READY to QUITFacilitate Quitting Process
The clinician and patient should discuss and develop effective cognitive and behavioral coping strategies for handling specific situations in which a person will be tempted to use tobacco.
Research shows that using both cognitive and behavioral strategies increases a patient’s likelihood of quitting (Prochaska & DiClemente, 1992). These strategies are described in the next few slides.
♪ Note to instructor(s): Have students refer to the Coping with Quitting: Cognitive and Behavioral Strategies handout. This handout provides specific examples of coping strategies for various situations.
Prochaska JO, DiClemente CC. (1992). Stages of change in the modification of problem behaviors. In: Progress in Behavior Modification, edited by Hersen M, Eisler RM, Miller PM. Sycamore, IL: Sycamore, pp. 184–218.

42
Reduce Risk Factors:Key Points
• There are effective pharmacotherapies for tobacco dependence
• Add medications to counseling if necessary
• Progression of many occupationally induced respiratory disorders can be reduced or controlled by reducing inhaled particles and gases

43
FDA Approvals: Smoking Cessation
1984
Rx nicotine
gum 1991
Rx transdermal nicotine patch
1996
OTC nicotine gum & patch;Rx nicotine nasal spray
1997
Rx nicotine inhaler;
Rx bupropion SR
2002
OTC nicotine lozenge
2006
Rx varenicline
♪ Note to instructor(s): Throughout this module, Rx and OTC are used to indicate prescription and over-the-counter (nonprescription) products, respectively.
This slide shows the years when the different pharmacologic agents for smoking cessation received FDA approval:
• In 1984, the nicotine gum (Nicorette) was the first nicotine replacement product to be approved by the FDA.
• In 1991, prescription transdermal nicotine patches became available.• In 1996, Nicorette gum, Nicoderm CQ patches, and Nicotrol patches (no longer
available) became available without a prescription; the prescription nicotine nasal spray (Nicotrol NS) was approved the same year.
• Bupropion SR (Zyban) was approved in 1997 as the only nonnicotine product to be used as an aid for smoking cessation. The nicotine inhalation system (Nicotrol inhaler) also received FDA approval for prescription use in 1997.
• The most recent nicotine replacement product to be approved by the FDA is the nicotine lozenge (Commit). This product was approved for nonprescription use in 2002.
• In 2006, a new class of medications is introduced with the FDA approval of varenicline (Chantix).

44
Long-Term (≥6 Month) Quit Rates for Available Cessation Medications
0
5
10
15
20
25
30
Nicotine gum Nicotinepatch
Nicotinelozenge
Nicotinenasal spray
Nicotineinhaler
Bupropion Varenicline
Active drugPlacebo
Data adapted from Silagy et al. (2004). Cochrane Database Syst Rev; Hughes et al., (2004). Cochrane Database Syst Rev.; Gonzales et al., (2006). JAMA and Jorenby et al., (2006). JAMA
Perc
ent q
uit
Few head-to-head trials have compared the various tobacco cessation therapies. In a randomized controlled trial comparing the four NRT formulations available at the time, the products performed similarly, but patient compliance was higher with the patch, followed by the gum, which was higher than the inhaler and nasal spray (Hajek et al., 1999).
This bar chart summarizes the long-term (≥6-month) quit rates observed with the different NRT products, bupropion SR and varenicline (Gonzales et al., 2006; Hughes et al., 2004; Jorenby et al., 2006; Silagy et al., 2004). These data derive from 124 different placebo-controlled trials; therefore, it is inappropriate to compare the active medications with respect to clinical efficacy. What this chart does illustrate, however, is that the quit rates from each of the methods is approximately twice that of its corresponding placebo control treatment arm.
Each of the pharmacotherapy options depicted in the chart is considered effective. When patients ask for assistance with their quit attempt, any product can be recommended, if not contraindicated. However, when assisting patients in choosing a product, clinicians should consider additional factors. The number of cigarettes smoked per day (or time to first cigarette, for the nicotine lozenge), level of dependence, advantages and disadvantages of each product, methods used for prior quit attempts and reasons for relapse, and the patient’s own product preference need to be considered. Behavioral counseling should be used in conjunction with all pharmacologic therapies.
Gonzales D, Rennard SI, Nides M, et al. (2006). Varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial. JAMA 296:47-55. Hajek P, West R, Foulds J, Nilsson F, Burrows S, Meadow A. (1999). Randomized comparative trial of nicotine polacrilex, a transdermal patch, nasal spray, and an inhaler. Arch Intern Med 159:2033–2038.Hughes JR, Stead LF, Lancaster. (2004). Antidepressants for smoking cessation. Cochrane Database Syst Rev4:CD000031.Jorenby DE, Hays JT, Rigotti NA, et al. (2006). Efficacy of varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial.JAMA 296:56-63.
45
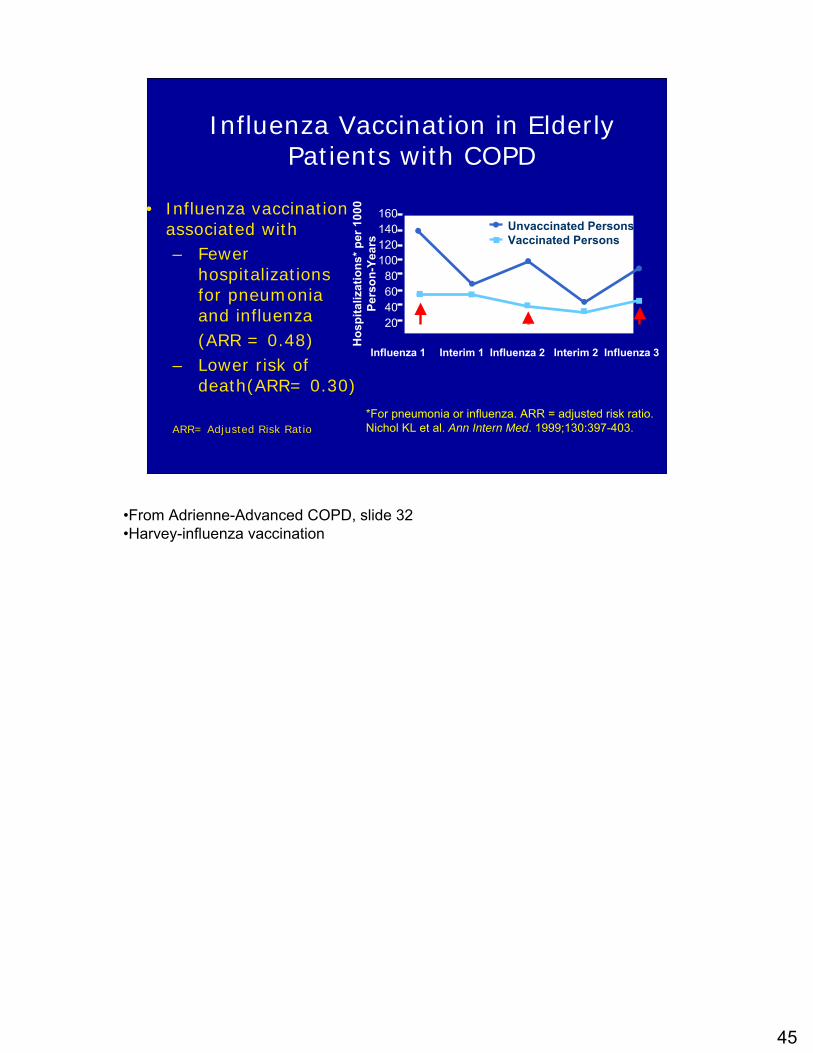
Influenza Vaccination in Elderly Patients with COPD
• Influenza vaccination associated with– Fewer
hospitalizations for pneumonia and influenza (ARR = 0.48)
– Lower risk of death(ARR= 0.30)
ARR= Adjusted Risk Ratio*For pneumonia or influenza. ARR = adjusted risk ratio.Nichol KL et al. Ann Intern Med. 1999;130:397-403.
160140120100
80604020
Hos
pita
lizat
ions
* per
100
0 Pe
rson
-Yea
rsInfluenza 1 Interim 1 Influenza 2 Interim 2 Influenza 3
Period
Unvaccinated PersonsVaccinated Persons
•From Adrienne-Advanced COPD, slide 32•Harvey-influenza vaccination

47
Medications for COPD
• Short-acting, inhaled beta2 agonists –Albuterol, pirbuterol, levalbuterol
• Inhaled anticholinergics (short and long-acting)– Ipratropium, tiotropium
• Long-acting, inhaled beta2 agonists – Formoterol, salmeterol, arformoterol
• Theophylline• Inhaled or systemic corticosteroids• Combination LABA/ICS

48
Manage Stable COPD
• Stepwise increase in treatment based on disease severity
• Health education can play a role in improving skills, ability to cope with illness, and health status. It is effective in accomplishing certain goals, including smoking cessation
• None of the existing medications for COPD affects long-term decline in lung function that is the hallmark of this disease
• Pharmacotherapy for COPD is used to decrease symptoms and/or complications

49
Monitoring Outcomes from COPD Therapy
• Improve lung function• Reduce symptoms, including
dyspnea• Reduce complications
–exacerbation frequency and severity–Reduce hospitalizations
• Improve quality of life• Avoid side effects from medications

50
Route of Delivery for Inhalation Therapies
• Method of delivery of inhalation therapy varies among settings
• Clinical studies suggest equal efficacy between nebulization and Metered dose inhaler (MDI) (with holding chamber)
• Dry powder inhaler (DPI) administration difficult in acute setting

51
Managing Stable COPDGOLD Stage
IInhaled Therapy
As-needed short-acting bronchodilator (ipratropium, albuterol, or combination)
Tiotropium + short-acting agent
Formoterol or salmeterol + short-acting agent
Tiotropium + LABA LABA +ICS
Combinations of tiotropium + LABA + ICS
+/- theophylline
II
0
III
IV
Adapted from: Tashkin DP et al. Chest. 2004;125:249-59.
Tiotropium+ ICS
Tobacco cessation and immunization strategies
LABA = Long acting beta agonist
ICS = Inhaled corticosteroid
This algorithm, defined according to the GOLD Guidelines, talks about a rational approach to patients with COPD, starting at the top with very mild disease and progressing through the most extensive disease. For patients at risk for COPD, one of the first interventions is tobacco cessation and making sure the patient receives appropriate immunization. At Stage I, patients still experience very intermittent symptoms and could be controlled with short-acting bronchodilator therapy. But as we progress to more extensive COPD, combinations of bronchodilators or bronchodilators combined with inhaled corticosteroids are often required.
52
Bronchodilators in Stable COPD
• Bronchodilator medications are central to symptom management in COPD.
• Inhaled therapy is preferred.
• The choice between bronchodilators or combination therapy depends on availability and individual response in terms of symptom relief and side effects.

53
Bronchodilators in Stable COPD
• Bronchodilators are prescribed on an as needed or on a regular basis to prevent or reduce symptoms.
• Regular treatment with long-acting inhaled bronchodilators is more effective and convenient than treatment with short-acting bronchodilators, but more expensive.
• Combining bronchodilators may improve efficacy and decrease the risk of side effects compared to increasing the dose of a single bronchodilator.

54
Rapid-acting Bronchodilators
• No evidence for substantial advantage of one class over another– Short-acting beta agonists (SABAs) onset is 5
min; peak within 15 to 30– Anticholinergic agents onset is 15 min; peak in
30 to 60• Primary considerations
– Efficacy of individual agents– Efficacy of combinations– Route of administration
• Many rapid-acting bronchodilators are also short-acting

55
β2-Agonists
• Primary action: bronchodilation due to relaxation of bronchial smooth muscle by stimulating action at adrenergic receptor
• Classified as short-acting (albuterol, levalbuterol, pirbuterol) or long-acting (formoterol, salmeterol)
• Short-acting β2-agonists are the primary rescue therapy used by patients with asthma or COPD
• Common side effects: tachycardia, muscle tremor
First class are the 2-agonists. 2-Agonists work to cause bronchodilation by relaxing bronchial smooth muscle at the adrenergic receptor. 2-Agonists are classified as either short-acting, and I’ve given some examples here, or long-acting. Short-acting 2-agonists are the primary rescue therapy used by patients with either asthma or COPD; whereas long-acting 2-agonists are used on a more chronic basis in those diseases.
The common side effects that this class of agents can cause include tachycardia, or an increase in heart rate, and a fine skeletal muscle tremor.

56
Changes in Albuterol Availability
• After December 2008, Chloroflurocarbon(CFC) containing albuterol products are banned in the U.S.
• Spot shortages of albuterol MDI (CFC and non-CFC) are expected during the transition period.
• Hydrofluoroalkane (HFA)-containing albuterol MDIs are equally safe and effective as the CFC-containing products.

57
Anticholinergics
• Primary action (inhaled): bronchodilation due to relaxation of bronchial smooth muscle by inhibiting action at cholinergic receptor
• Classified as short-acting (ipratropium) or long-acting (tiotropium)
• Primary role is for COPD treatment although ipratropium may be used for acute asthma
• Common side effect: dry mouth
The next class of agents are the anticholinergics. Anticholinergic agents are delivered by inhalation therapy for patients with lung disease as well, and they result in bronchodilation by relaxing bronchial smooth muscle by inhibiting action at the cholinergic receptor.
Currently, we have two agents that are anticholinergics: the short-acting ipratropium bromide, or the long-acting tiotropium. These agents are used primarily in the treatment for COPD; although ipratroprium is used for acute asthma, especially for patients in the emergency department or the hospital. Inhaled anticholinergics are very well tolerated with the most common side effect being a complaint of dry mouth.
58
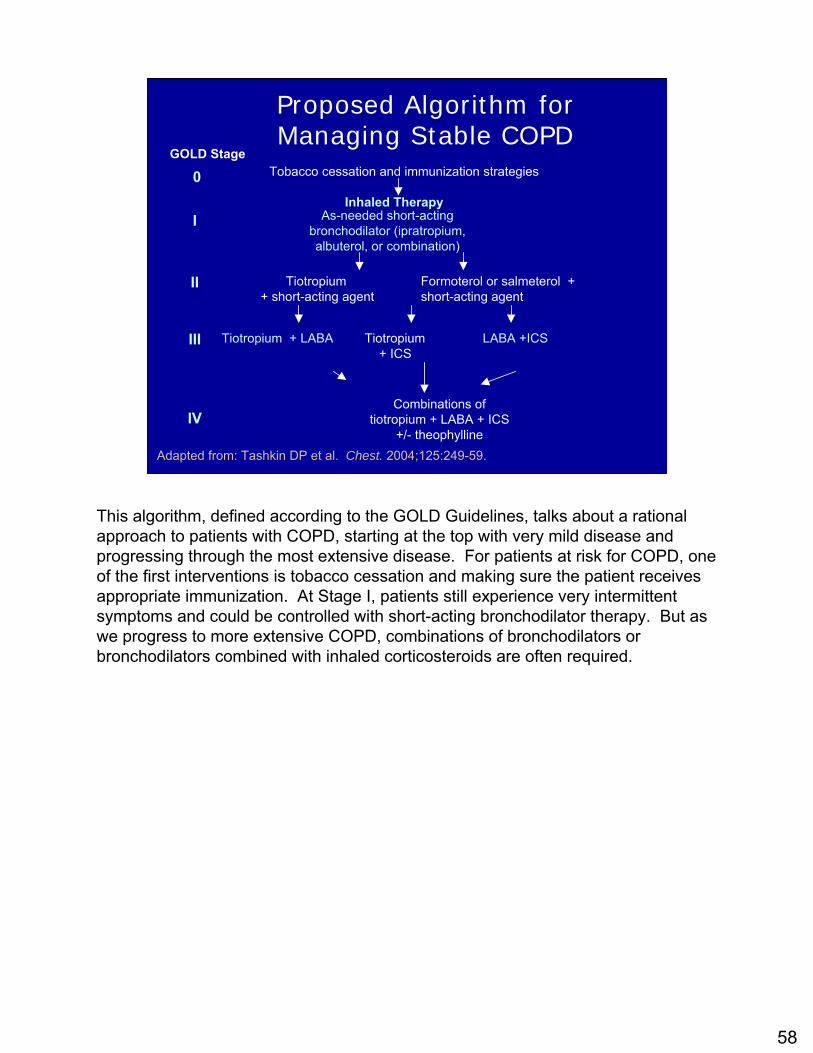
Proposed Algorithm for Managing Stable COPD
GOLD Stage
IInhaled Therapy
As-needed short-acting bronchodilator (ipratropium, albuterol, or combination)
Tiotropium + short-acting agent
Formoterol or salmeterol + short-acting agent
Tiotropium + LABA LABA +ICS
Combinations of tiotropium + LABA + ICS
+/- theophylline
II
0
III
IV
Adapted from: Tashkin DP et al. Chest. 2004;125:249-59.
Tiotropium+ ICS
Tobacco cessation and immunization strategies
This algorithm, defined according to the GOLD Guidelines, talks about a rational approach to patients with COPD, starting at the top with very mild disease and progressing through the most extensive disease. For patients at risk for COPD, one of the first interventions is tobacco cessation and making sure the patient receives appropriate immunization. At Stage I, patients still experience very intermittent symptoms and could be controlled with short-acting bronchodilator therapy. But as we progress to more extensive COPD, combinations of bronchodilators or bronchodilators combined with inhaled corticosteroids are often required.
59
Long-acting Bronchodilators
• Long-acting Beta2 agonists– Includes: arformeterol, formoterol,
salmeterol–Side effects: tachycardia, black box
warning (relevant for asthma)
• Long-acting Anticholinergic–Tiotropium–Side effects: dry mouth

60
Significant Issues in COPD Pharmacotherapy
• Which long-acting bronchodilator should be used first?
• Are combinations of long-acting bronchodilators beneficial and cost-effective?
• When should inhaled corticosteroids be introduced into the regimen?
61
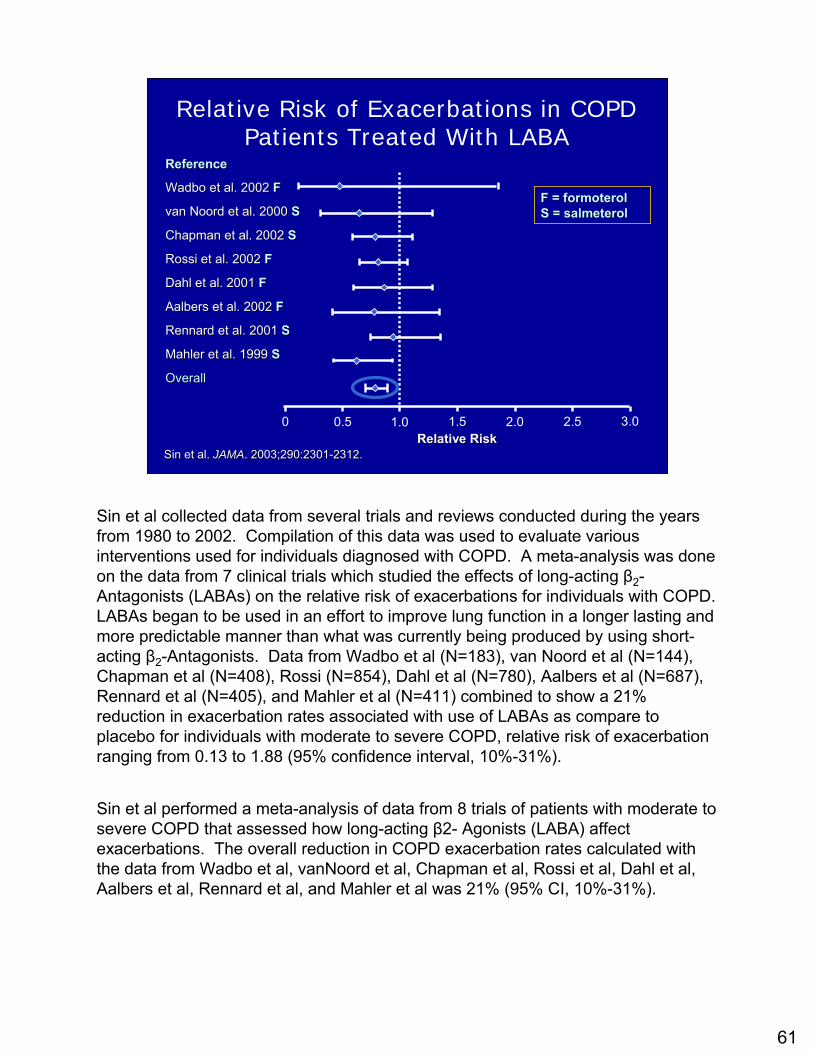
Relative Risk of Exacerbations in COPD Patients Treated With LABA
Sin et al. Sin et al. JAMAJAMA. 2003;290:2301. 2003;290:2301--2312.2312.
ReferenceReference
WadboWadbo et al. 2002 et al. 2002 FF
van van NoordNoord et al. 2000 et al. 2000 SS
Chapman et al. 2002 Chapman et al. 2002 SS
Rossi et al. 2002 Rossi et al. 2002 FF
Dahl et al. 2001 Dahl et al. 2001 FF
AalbersAalbers et al. 2002 et al. 2002 FF
RennardRennard et al. 2001 et al. 2001 SS
Mahler et al. 1999 Mahler et al. 1999 SS
OverallOverall
0 0.5 1.0 1.5 2.0 2.5 3.0Relative RiskRelative Risk
F = formoterol F = formoterol S = salmeterolS = salmeterol
Sin et al collected data from several trials and reviews conducted during the years from 1980 to 2002. Compilation of this data was used to evaluate various interventions used for individuals diagnosed with COPD. A meta-analysis was done on the data from 7 clinical trials which studied the effects of long-acting β2-Antagonists (LABAs) on the relative risk of exacerbations for individuals with COPD. LABAs began to be used in an effort to improve lung function in a longer lasting and more predictable manner than what was currently being produced by using short-acting β2-Antagonists. Data from Wadbo et al (N=183), van Noord et al (N=144), Chapman et al (N=408), Rossi (N=854), Dahl et al (N=780), Aalbers et al (N=687), Rennard et al (N=405), and Mahler et al (N=411) combined to show a 21% reduction in exacerbation rates associated with use of LABAs as compare to placebo for individuals with moderate to severe COPD, relative risk of exacerbation ranging from 0.13 to 1.88 (95% confidence interval, 10%-31%).
Sin et al performed a meta-analysis of data from 8 trials of patients with moderate to severe COPD that assessed how long-acting β2- Agonists (LABA) affect exacerbations. The overall reduction in COPD exacerbation rates calculated with the data from Wadbo et al, vanNoord et al, Chapman et al, Rossi et al, Dahl et al, Aalbers et al, Rennard et al, and Mahler et al was 21% (95% CI, 10%-31%).

62
Exacerbations in COPD Patients Decreased by Tiotropium
Adapted from Barr et al. Adapted from Barr et al. Cochrane Database of Systematic Reviews.Cochrane Database of Systematic Reviews. 2005, Issue 22005, Issue 2
ReferenceReference
BeehBeeh et al. 2004et al. 2004
BrusascoBrusasco et al. 2003et al. 2003
CalverleyCalverley et al. 2003et al. 2003
CasaburiCasaburi et al. 2002et al. 2002
Celli et al. 2003Celli et al. 2003
LittnerLittner et al. 2000et al. 2000
NiewoeherNiewoeher et al. 2005et al. 2005
OO’’Donnell et al. 2004Donnell et al. 2004
VinckenVincken et al 2002et al 2002
OverallOverall
0.5 1.0 5.0 10.0Odds RatioOdds Ratio
Sin et al collected data from several trials and reviews conducted during the years from 1980 to 2002. Compilation of this data was used to evaluate various interventions used for individuals diagnosed with COPD. A meta-analysis was done on the data from 7 clinical trials which studied the effects of long-acting β2-Antagonists (LABAs) on the relative risk of exacerbations for individuals with COPD. LABAs began to be used in an effort to improve lung function in a longer lasting and more predictable manner than what was currently being produced by using short-acting β2-Antagonists. Data from Wadbo et al (N=183), van Noord et al (N=144), Chapman et al (N=408), Rossi (N=854), Dahl et al (N=780), Aalbers et al (N=687), Rennard et al (N=405), and Mahler et al (N=411) combined to show a 21% reduction in exacerbation rates associated with use of LABAs as compare to placebo for individuals with moderate to severe COPD, relative risk of exacerbation ranging from 0.13 to 1.88 (95% confidence interval, 10%-31%).
Sin et al performed a meta-analysis of data from 8 trials of patients with moderate to severe COPD that assessed how long-acting β2- Agonists (LABA) affect exacerbations. The overall reduction in COPD exacerbation rates calculated with the data from Wadbo et al, vanNoord et al, Chapman et al, Rossi et al, Dahl et al, Aalbers et al, Rennard et al, and Mahler et al was 21% (95% CI, 10%-31%).

63
Theophylline
• Primary action is bronchodilation due to various mechanisms including inhibiting adenosine
• Exerts modest anti-inflammatory actions• Significant intrapatient and interpatient
variability in dosage requirements and frequent risk for drug interactions
• Common side effects: gastrointestinal, cardiac, central nervous system
The next class of medication used for asthma and COPD are the methylxanthines or theophylline. Theophylline works as a bronchodilator by a variety of mechanisms including the inhibition of adenosine, another endogenous bronchoconstrictor. Theophylline’s also been shown to exert some modest anti-inflammatory effect in the airway.
Theophylline is a difficult drug to use because there’s significant intrapatient and interpatient variability in both dosage requirements and ultimate clearance from the body. Theophylline also has the potential risk for frequent drug interactions.
Common side effects associated with theophylline therapy that limits its use include side effects in the gastrointestinal tract, the cardiac system, and the central nervous system.

64
Theophylline in COPDCurrent Role
• Often 3rd line• Bronchodilator and anti-inflammatory
actions• Added to other therapies• Deterioration occurs when withdrawn• May benefit small airways (systemic
administration)• No role in acute exacerbation
Barnes PJ. Proc Am Thorac Soc 2005;2:334-339.

65
Approach to COPD Therapy
NHLBI/WHO. Global Initiative for Chronic Obstructive Lung Disease. April 2001 (Updated 2005).
Add long-term O2 if chronic respiratory failure Consider surgical treatments
Add inhaled corticosteroids if repeated exacerbations
Add regular treatment with one or more long-acting bronchodilatorsAdd rehabilitation
Add short-acting bronchodilatoras needed for intermittent symptoms
Smoking cessation andSmoking cessation andavoid risk factors; avoid risk factors; influenza vaccinationinfluenza vaccination
Stage IV:Very Severe
Stage II:Moderate
Stage III:Severe
Stage I:Mild
Stage 0:At Risk
And in summary, patients with COPD are treated with pharmacotherapy according to the stage of their disease. The initial treatment of COPD, from a pharmacologic perspective, typically focuses on bronchodilator therapy; although patients who suffer frequent exacerbations may benefit from the use of inhaled corticosteroids. Patients with the most severe form of COPD may require supplemental oxygen therapy, or in some cases, surgical options along with pharmacologic therapy.
66
Manage Stable COPD Inhaled Corticosteroids
• Regular treatment with inhaled glucocorticosteroids is appropriate for symptomatic COPD patients with an FEV1 < 50% predicted (Stage III: Severe COPD and Stage IV: Very Severe COPD) and repeated exacerbations e.g. 3 in the last three years.
• This treatment has been shown to reduce the frequency of exacerbations and improve health status.

67
Inhaled Corticosteroids (ICS)
• Primary action: reduce and control airway inflammation through intracellular inhibition of inflammatory reaction at steroid receptor
• Several products available that differ in milligram potency
• Frequently used with spacer devices and mouth rinsing to reduce systemic effects
• Common side effects: sore throat, hoarseness
The next major class of agents are the inhaled corticosteroids. Corticosteroids work against inflammation at the cellular level at the steroid receptor. There are several corticosteroid products available on the market in the United States, and these differ primarily by milligram potency.
Inhaled corticosteroids are the primary therapy for patients with asthma and they are also beneficial for some patients with COPD when used in combination with bronchodilators. To reduce the systemic effects of corticosteroids, these products are frequently used with spacer devices or a mouth rinsing procedure to reduce systemic side effects. The common local side effects associated with inhaled corticosteroids are complaints of a sore throat or hoarseness.

68
Inhaled Steroids (ICS) in Stable COPD
• Regular treatment with ICS does not modify the long-term decline in FEV1.
• Appropriate for symptomatic COPD patients with an FEV1 < 50% and repeated exacerbations (Stage III and IV).
• ICS reduce frequency of exacerbations and improve health status.
• ICS combined with long-acting β2-agonist more effective than individual components.
ISOLDE trial pts with fev1 50% predicted had 25% less exacerbations

69
ICS and Acute Exacerbations of COPD:
Meta-AnalysisRelative Risk of Exacerbations in Patients With
COPD Treated With Inhaled Corticosteroids vs Placebo
Alsaeedi A, Sin D. Am J Med. 2002;113:59-65.
Vestbo et al
Bourbeau et al
Burge et al
Lung Health Study
Weir et al
Paggiaro et al
Overall
0.0 0.5 1.0 1.5 2.0 2.5 3.0Relative Risk

70
ICS and Mortality in COPD
Sin DD, et al. Thorax 2005;60:992-997.

71
Macie, C. et al. Chest 2006;130:640-646
COPD Mortality Based on Time to Introduction of ICS Therapy following Hospitalization

72
Significant Issues in COPD Pharmacotherapy
• Which long-acting bronchodilator should be used first?
• Are combinations of long-acting bronchodilators beneficial and cost-effective?
• When should inhaled corticosteroids be introduced into the regimen?

73
Potential COPD Combination Therapies
• Short-acting anticholinergic + SABA scheduled
• LABA + short-acting anticholinergic• LABA• Tiotropium• LABA + tiotropium• LABD + ICS • LABD combination + ICS• Any of the above + oral theophylline
LABD: Long-acting bronchodilator.
(each with SABA as needed)
There are a variety of combination therapies that can be used for patients with varying degrees of COPD. A short-acting anticholinergic agent can be used with a short-acting 2-agonist. A long-acting 2-agonist can be used alone or in combination with a short-acting anticholinergic therapy. Another option would be the use of a long-acting anticholinergic therapy such as tiotroprium.
In some cases, a long-acting 2-agonist can be combined with the long-acting anticholinergic tiotroprium. Or, long-acting bronchodilator therapies can be combined with inhaled corticosteroid therapy directed against the inflammatory components of COPD. Or, long-acting bronchodilator therapies could be used in combination along with anti-inflammatory therapies.
In patients who can’t be controlled with other means, any of the combinations of above could be used in combination with oral theophylline therapy.

74
Major Trials in COPD
• TORCH (Towards a Revolution in Towards a Revolution in COPD Health) (recently completed)COPD Health) (recently completed)–– Salmeterol and Salmeterol and FluticasoneFluticasone
•• UPLIFT (Tiotropium and its Effect UPLIFT (Tiotropium and its Effect on Rate of Decline of FEVon Rate of Decline of FEV1)(ongoing)–Tiotropium

75
TORCH COPD Study
• 6,100 subjects received salmeterol, fluticasone, combo, or placebo.
• Salmeterol/Fluticasone (50/500) showed a 17% relative reduction in mortality over 3 years in COPD compared with placebo.

77
Hospitalization due to COPD: Tiotropium vs. Placebo
0.80
0.85
0.90
0.95
1.00
0 50 100 150 200 250 300 350
Tiotropium (n = 550)
Placebo (n = 371)
Days on Treatment
Time to first hospitalization: Time to first hospitalization: p = p = 0.007*0.007*
* Log Rank Test
Prob
abili
ty o
f Hos
pita
lizat
ion
Casaburi ERJ 2002;19:217

78
COPD: Tiotropium + Formoterol
0
50
100
150
200
250
Trough FEV1 FEV1 (0-12) FEV1 (12-24)
Mea
n ch
ange
from
bas
elin
e (m
l)TioForm bidTio + Form
Van Van NoordNoord et al ERJ 2003: 167:A320et al ERJ 2003: 167:A320

79
Other Management Considerations

80
Oxygen Therapy in Stable COPD
• The long-term administration of oxygen (>15 hours per day) to patients with chronic respiratory failure has been shown to increase survival.
• Improvement in quality of life in patients with severe COPD and chronic hypoxemia (partial pressure of arterial oxygen, <55 mm Hg).

81
Pulmonary Rehabilitation
• Pulmonary rehabilitation consisting of a structured program of education, exercise, and physiotherapy has been shown in controlled trials to improve exercise capacity and quality of life among patients with severe COPD and to reduce the amount of health care needed.

82
Lung Volume Reduction Surgery
• National Emphysema Treatment Trial Research Group
• 1,218 patients with severe emphysema underwent pulmonary rehabilitation and were randomly assigned to undergo lung-volume reduction surgery or to receive continued medical treatment
• Increases chance of improved exercise capacity but does not confer a survival advantage
• Survival advantage for patients with predominantly upper-lobe emphysema and low base-line exercise capacity

83
Manage ExacerbationsKey Points
• Exacerbations of respiratory symptoms requiring medical intervention are important clinical events in COPD.
• The most common causes of an exacerbation are infection of the tracheobronchial tree and air pollution, but the cause of about one-third of severe exacerbations cannot be identified.

84
COPD Exacerbation
• A sustained worsening of the patient's condition, from the stable state and beyond normal day-to-day variations, that is acute in onset and necessitates a change in regular medication in a patient with underlying COPD. It frequently requires the patient to seek medical attention or alter treatment.
Rodriguez-Roisin R. Toward a consensus definition for COPD exacerbations. Chest. 2000; 117(5 suppl 2):398S-401S.

85
Components of Treatment: Acute Exacerbations
• Intensify treatment with bronchodilators• Consider using nebulizer if MDI cannot be
used effectively• Short course systemic corticosteroids • Consider antibiotics if change in sputum
volume, purulence, or increased dyspnea• Supplemental oxygen therapy• Treat co-morbidities or other contributory
exacerbators of COPD
http://www.oqp.med.va.gov/cpg/copd/archive/module_b/b2.htm

86
Co-Morbid Conditions that can Impact COPD Exacerbation Management
• Congestive heart failure • Pneumonia • Pulmonary embolism • Spontaneous pneumothorax • Inappropriate oxygen therapy • Psychotropic drugs (hypnotics, tranquilizers,
narcotics, etc.) • Drug allergy (penicillin, cephalosporin, etc.) • Metabolic disease (diabetes mellitus, electrolyte
disorders) • Poor nutritional status • Myopathy (e.g., steroid myopathy) • Other acute illness (acute abdomen, GI hemorrhage,
CVA, etc.) http://www.oqp.med.va.gov/cpg/copd/archive/module_b/b2.htm

87
Manage ExacerbationsKey Points
• Non-invasive intermittent positive pressure ventilation (NIPPV) in exacerbations improves blood gases and pH, reduces in-hospital mortality, decreases the need for invasive mechanical ventilation and intubation, and decreases the length of hospital stay.

88
Components of COPD Management
• Patient education• Assess and monitor disease• Reduce risk factors• Manage stable COPD• Manage exacerbations

89
New Anti-inflammatory Drugs In Development
• Phosphodiesterase 4 inhibitors, which have an inhibitory effect on key inflammatory cells involved in COPD, including: macrophages, neutrophils, and cytotoxic T lymphocytes. (Cilomilast, Roflumilast)– A limitation of drugs in this class is the
common side effect of nausea.• Other novel anti-inflammatory approaches
under development include: inhibitors of NF-(kappa)B, inhibitors of p38 mitogen-activated protein kinase, and interleukin-10

90
Medication Therapy Management Activities
• Educating the patient– Understanding of
therapy– Arranging for drug
therapy monitoring– Reinforcing proper
use of all medications and related equipment
– Achieving patient understanding
• Ensuring medications, equipment, supplies received by patient in timely fashion
• Documenting steps to implement plan– Baseline monitoring– Barriers
• Reducing risks and exposures
• Communicating plan to patient and other clinicians

91
Medication Management and Related Services for the COPD Patient
• Tobacco cessation counseling and risk factor avoidance
• Immunizations• Recommendation and selection of
medication and device products• Education about proper use of medication• Monitoring for safety and efficacy of
therapy• Considering therapeutic alternatives and
cost

92
Medication Management and Related Services for the COPD Patient
(continued)
• Monitoring co-morbidities and potential interactions
• Provision and monitoring of oxygen therapy
• Provision of home care equipment and supplies
• Referral to other community services and resources

93
Key educational messages for COPD
• Stage 0– Information/advice about risk reduction
• Stage 1-3– Information about disease– Inhaler skills/adherence– Recognize exacerbations– Minimize dyspnea
• Stage 4– Complications– Oxygen therapy– Advance directives/end of life decisions

94
COPD: The Current View
• Emerging evidence about the value of various pharmacotherapies
• Renewed optimism for the patient• Numerous opportunities for the
pharmacist to assist the patient in achieving optimal outcomes