medicinal use of cannabis - conference.co.nz 02 ben jansen... · medicinal use of cannabis dr ben...
TRANSCRIPT

Medicinal Use Of Cannabis
Dr Ben JansenDirector @ Burleigh Heads Cannabis
FRNZCGP FRACGP FRCUCP

Medicinal Use Of Cannabis

BurleighHeadsCannabis.com
Take Home Messages
● No direct mortality from cannabis use, ever.
● Medicinal Cannabis does not need to get the patient “high”
● CBD, among other cannabinoids, modulate THC effects
● Start low and titrate dose to effect: THC 1mg, CBD 5mg BD PO
● Monitor co-administered drug levels or end organ function if required
● The non-psychoactive oral natural raw acid forms of the cannabinoids are being used for CB2 reception modulation and preventing oxidative stress (among other effects)
Historical Medicinal Use Of Cannabis
https://www.youtube.com/watch?v=CJlqsdezhhk

Historical Medicinal Use Of Cannabis
Public Opinion On Regulation?
● Prohibition
● Medication Restricted
● Medication Open
● Recreational Use* (still requires a level of quality
and control for sale)
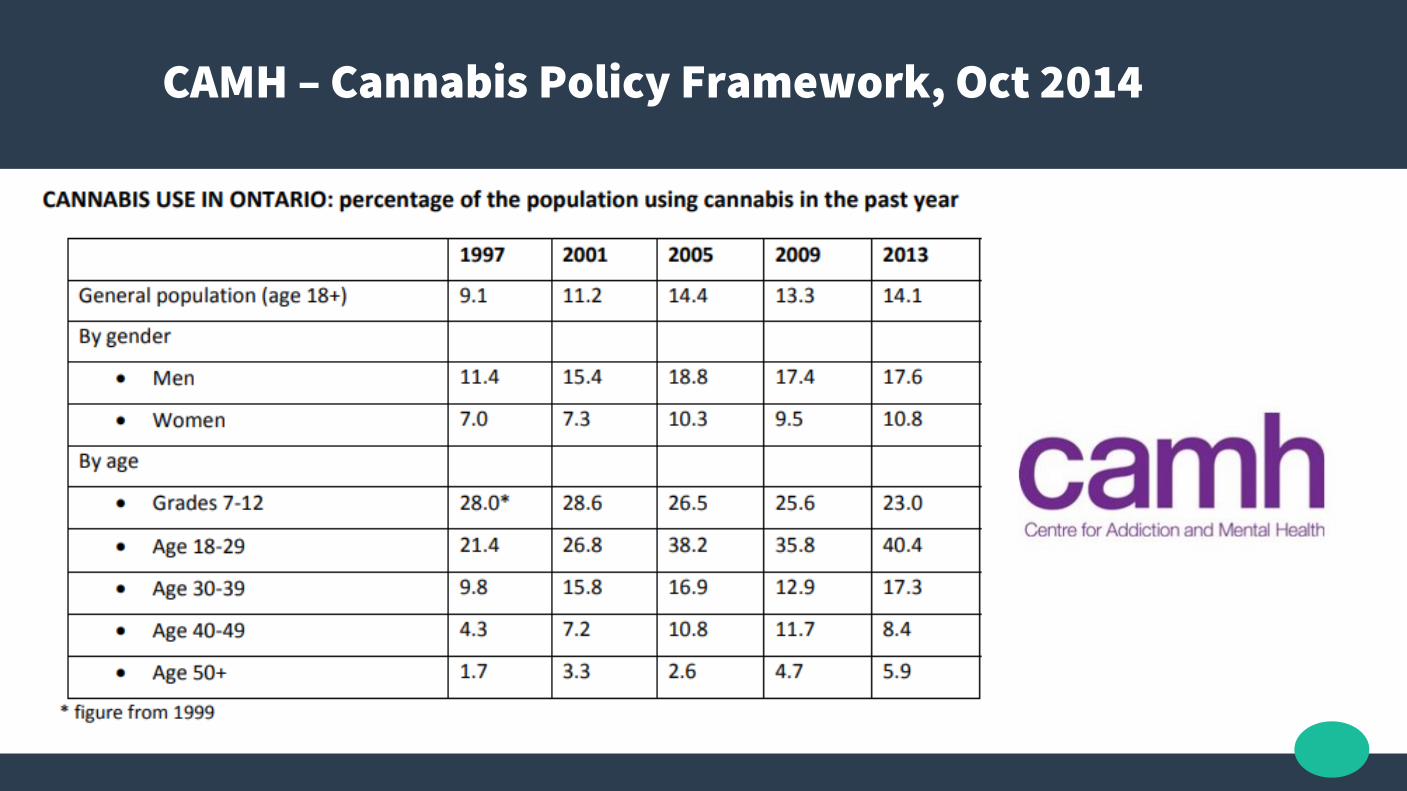
CAMH – Cannabis Policy Framework, Oct 2014
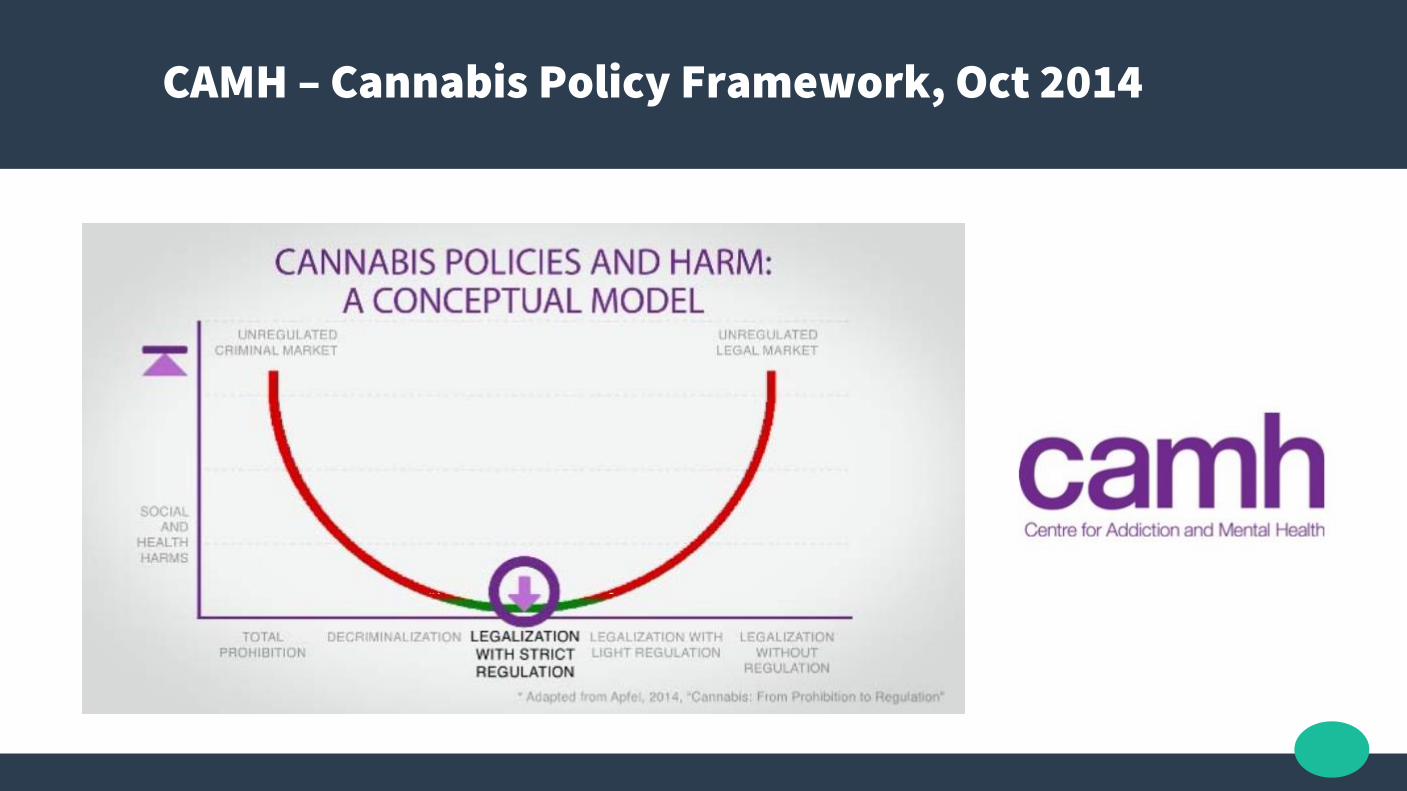
CAMH – Cannabis Policy Framework, Oct 2014
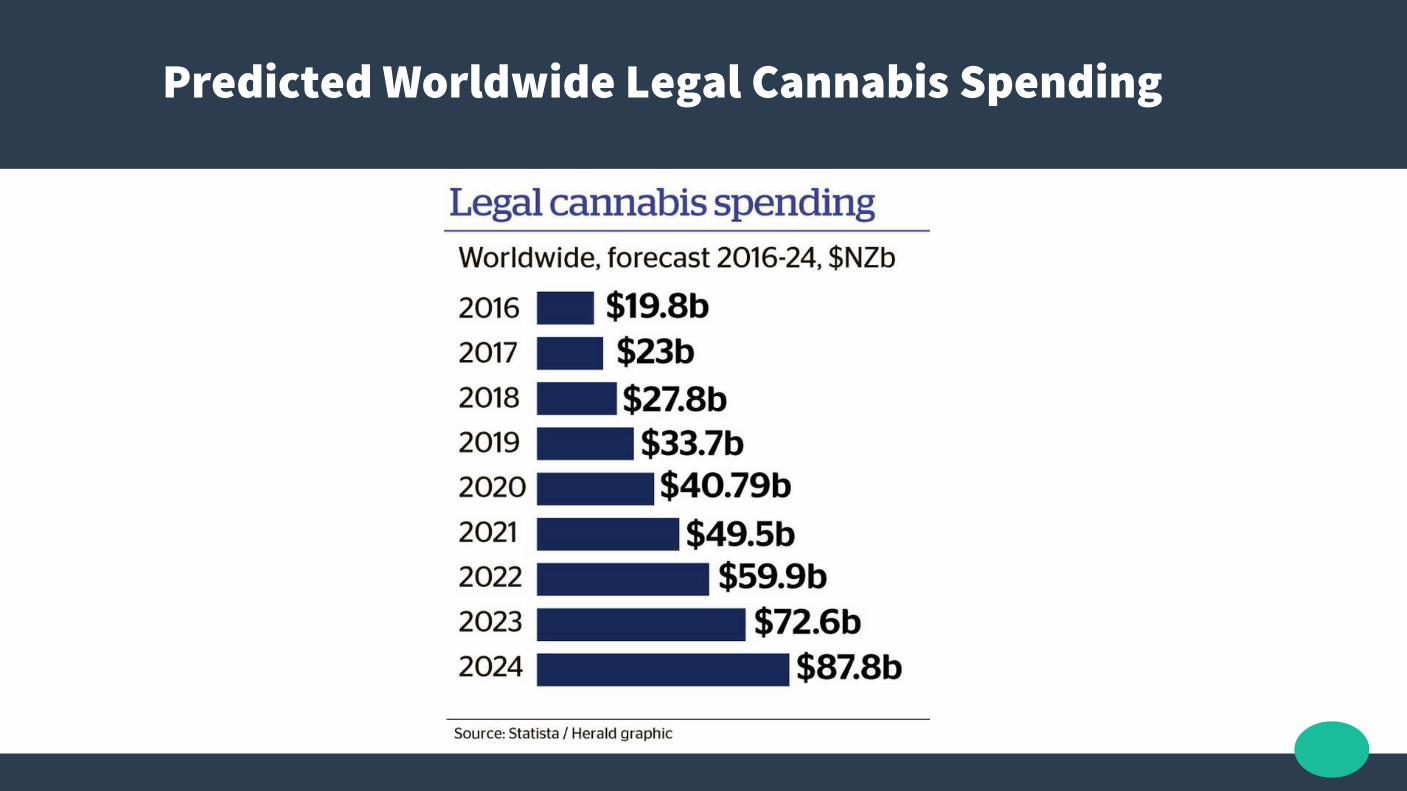
Predicted Worldwide Legal Cannabis Spending
PubMed search 2017/4/1
● 31945 results for Cannabis, or Marijuana, or THC, or CBD
● Compared to 23924 for Paracetamol, or Acetaminophen
● Compared to 7511 for Metoprolol● Compared to 2598 for Ramipril
PubMed search 2018/4/1
● 37252 results for Cannabis, or Marijuana, or THC, or CBD
● Compared to 25303 for Paracetamol, or Acetaminophen
● Compared to 7724 for Metoprolol● Compared to 2652 for Ramipril

Mortality

Mortality
● 69000+ Opioid deaths estimated Worldwide in 2014 by the WHO.
● 22598 deaths from Opioid Pain Relievers in the USA 2015. National Center on Health Statistics, CDC WONDER
● 56,000 emergency room visits and 26,000 hospitalizations yearly from Paracetamol, and 458 deaths in the USA. Nourjah P et
al. Pharmacoepidemiol Drug Saf. 2006 Jun;15(6):398-405.
● 3,200 deaths annually as a result of NSAID-induced GI bleeding in the USA. Tarone RE et al. Am J Ther. 2004;11(1):17-25.
● Zero deaths from Cannabis, ever! Dr Lester Grinspoon MD, Professor
Emeritus, Harvard Medical School.

Mortality
● Bachhuber et al, 2014 – Medical Cannabis Laws And Opioid Overdose Mortality In The USA, 1999 – 2010.
● States with medicinal cannabis had a 24.8% lower mean annual opioid overdose mortality rate (95% CI, -37.5% to -9.5%)
Endocannabinoid System
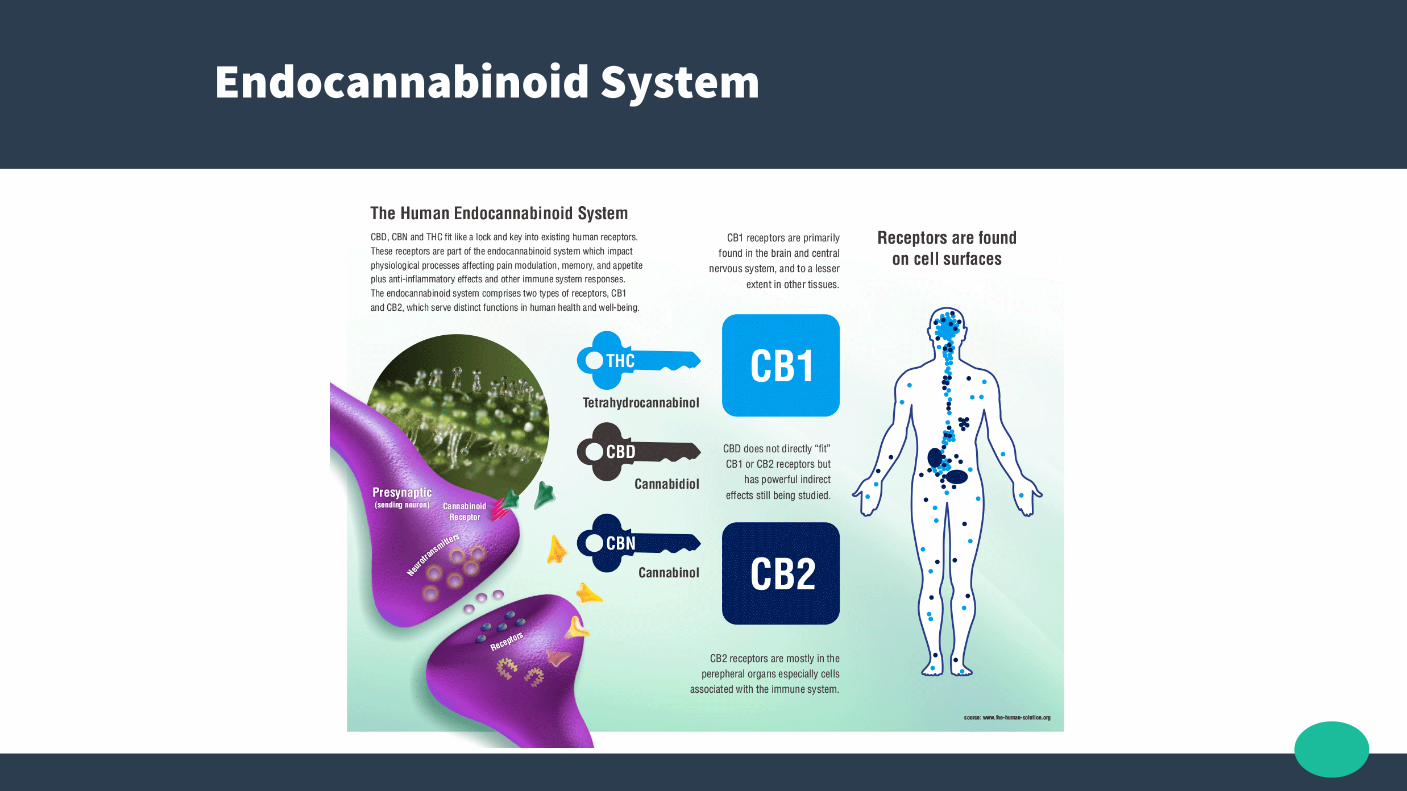
Endocannabinoid System
● “The Bodies Own Cannabinoid System”
● Named because it was unknown until the effects of THC were being investigated
● Mostly cell membrane G protein-coupled receptors
● Related to homeostasis, memory, immune function, ….

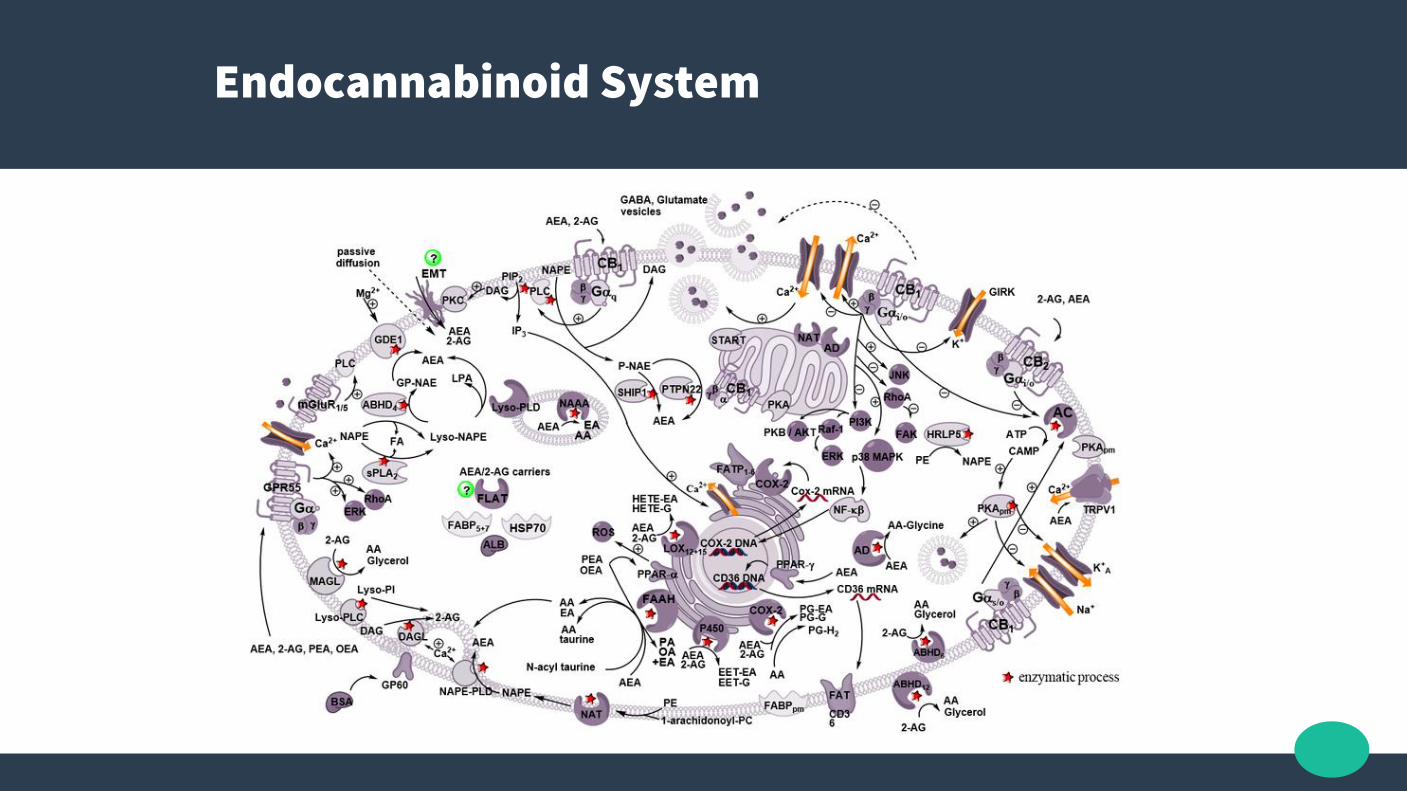
Endocannabinoid System
● ECS homeostatic roles have been summarized as “relax, eat, sleep, forget, and protect.”
Endocannabinoid System
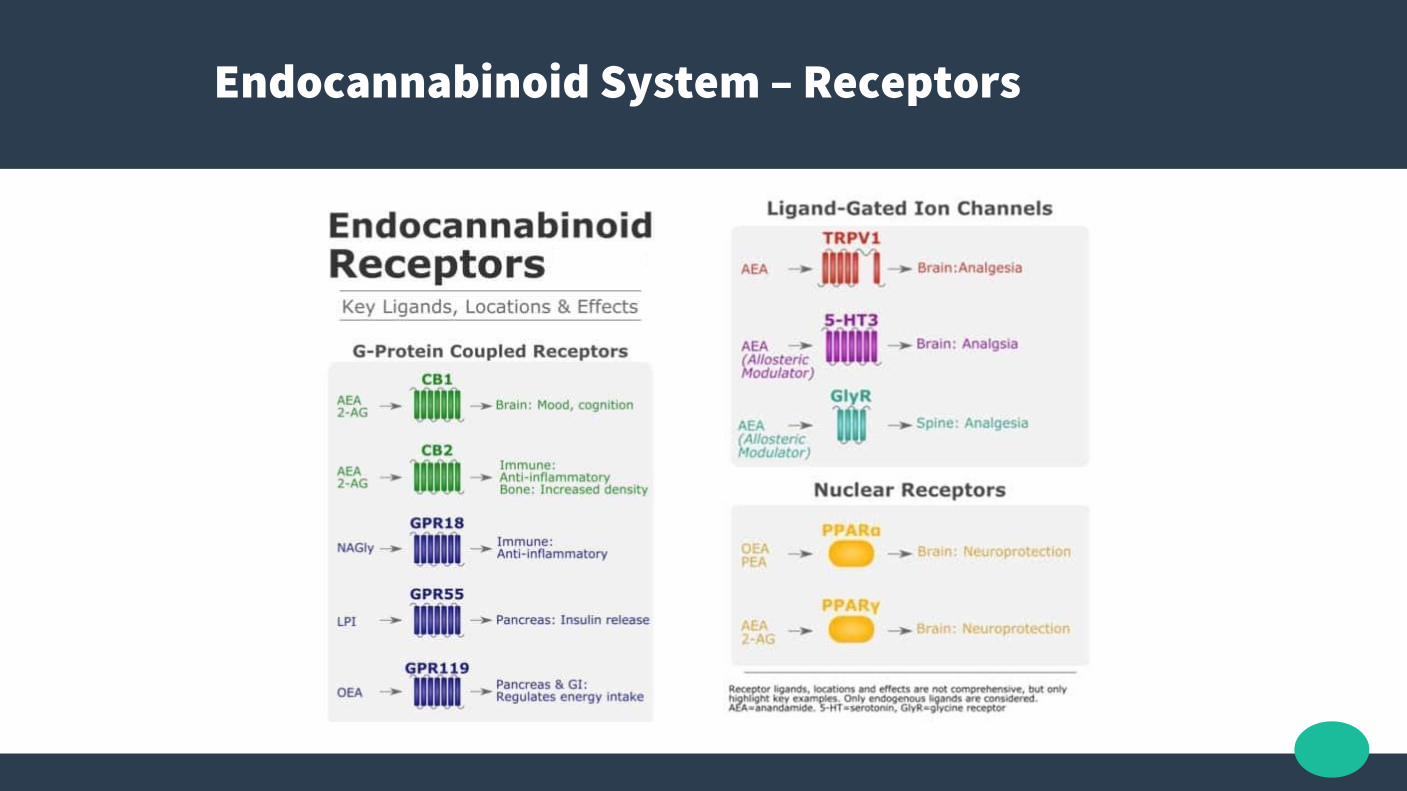
Endocannabinoid System – Receptors
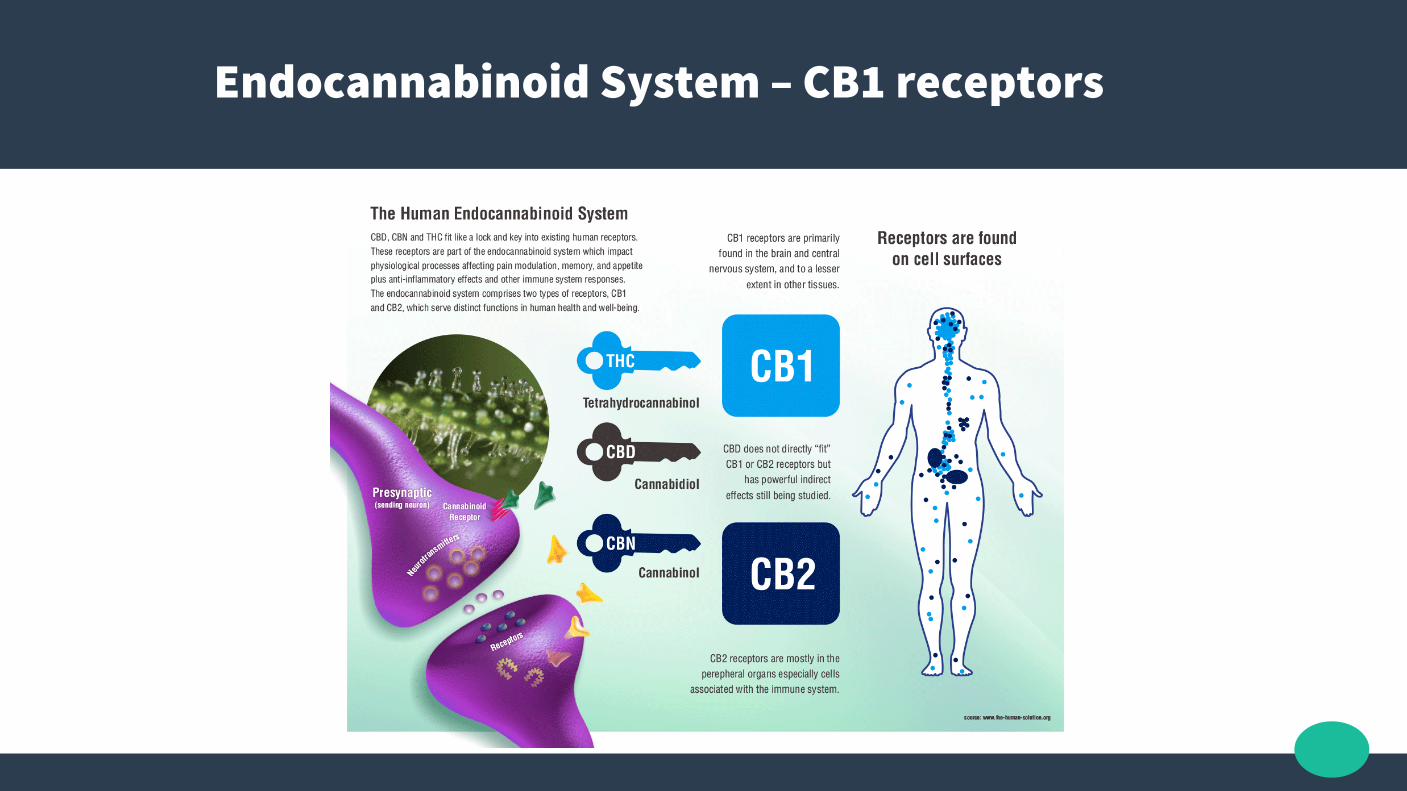
Endocannabinoid System – CB1 receptors

Endocannabinoid System – CB2 receptors
● The other main endocannabinoid is 2-Arachidonoylglycerol (2-AG) which is active at both cannabinoid receptors, along with its own mimetic phytocannabinoid, CBD
● 2-AG and CBD are involved in the regulation of appetite, immune system functions, pain management, and homeostasis

Endocannabinoid System – Endogenous ECs
Reggio PH. Endocannabinoid Binding to the
Cannabinoid Receptors: What Is Known and
What Remains Unknown. Current medicinal
chemistry. 2010;17(14):1468-1486.
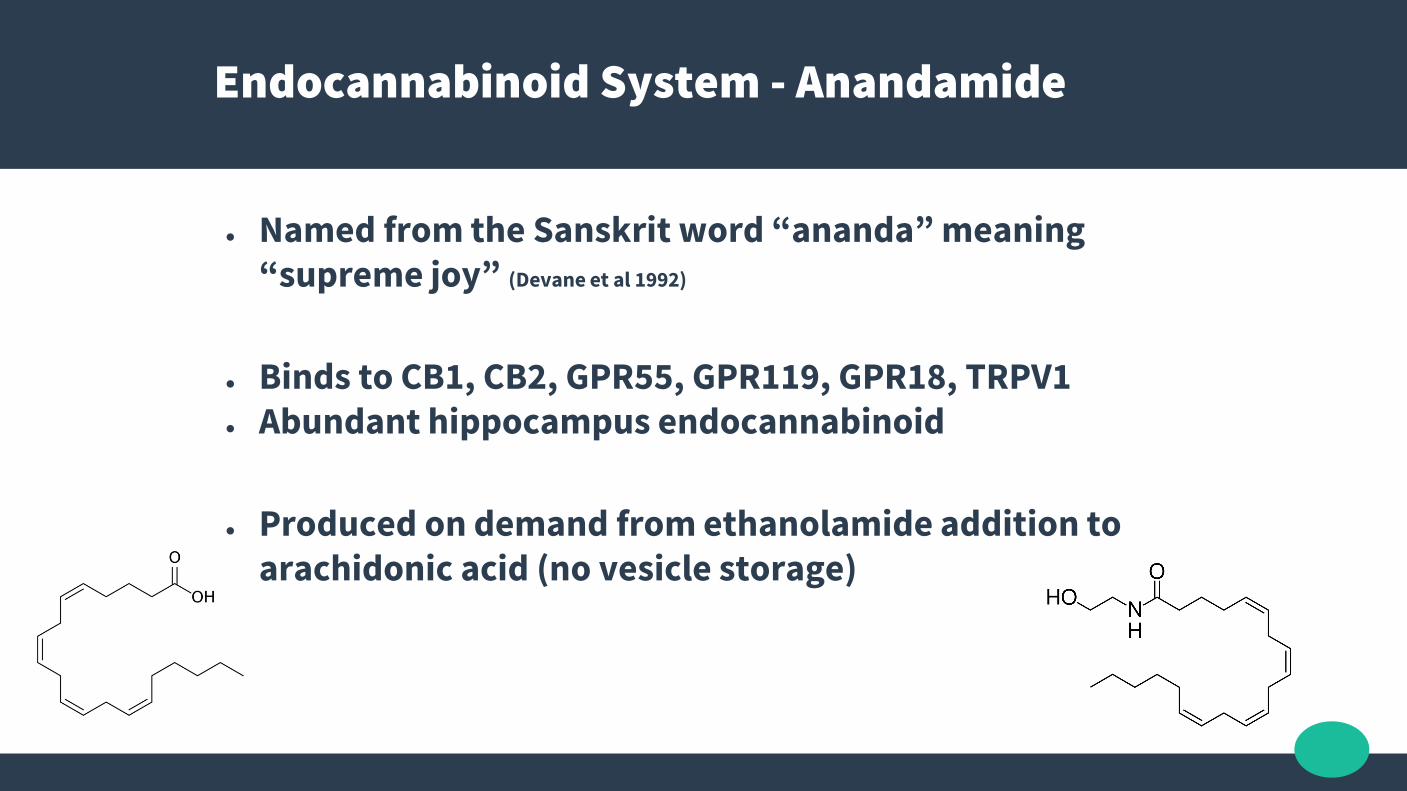
Endocannabinoid System - Anandamide
● Named from the Sanskrit word “ananda” meaning “supreme joy” (Devane et al 1992)
● Binds to CB1, CB2, GPR55, GPR119, GPR18, TRPV1● Abundant hippocampus endocannabinoid
● Produced on demand from ethanolamide addition to arachidonic acid (no vesicle storage)
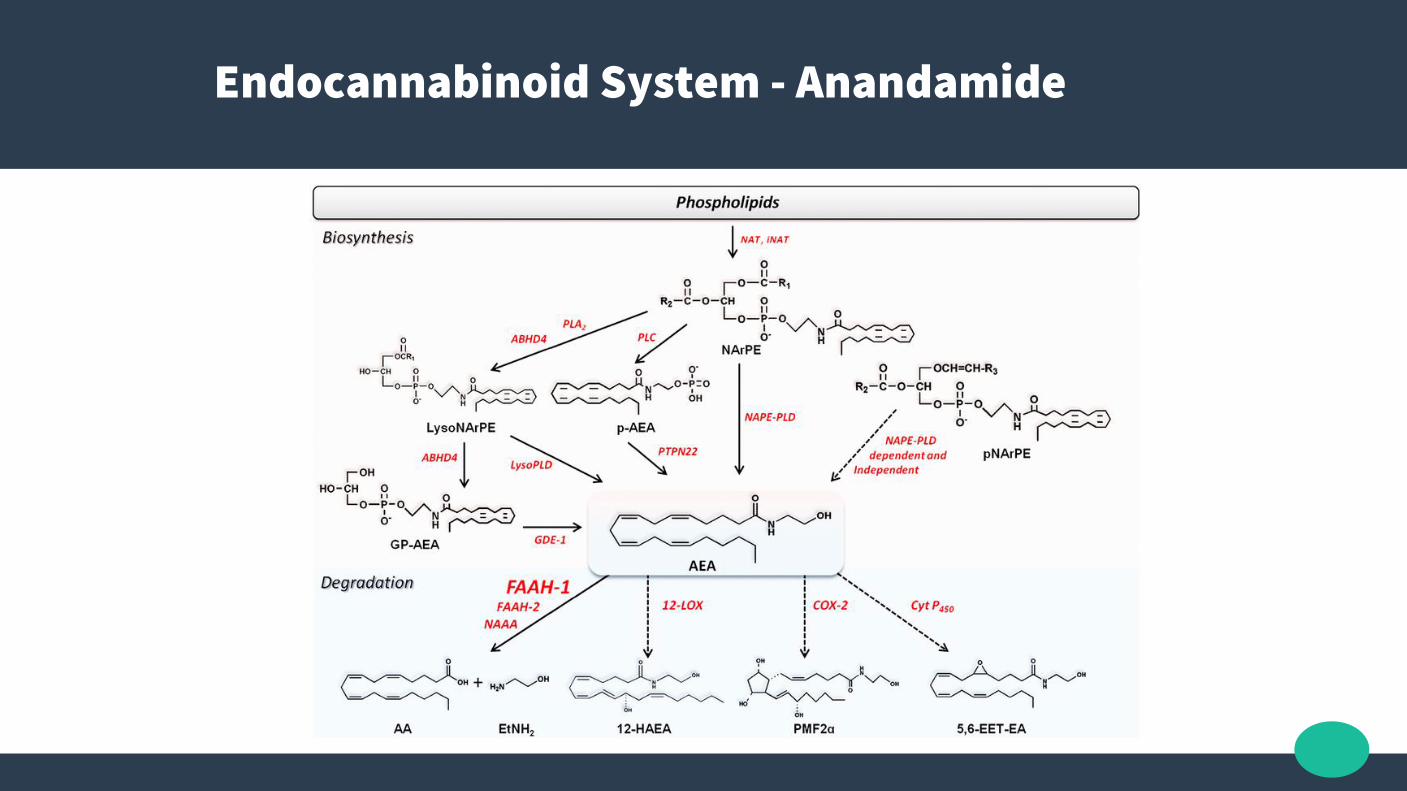
Endocannabinoid System - Anandamide
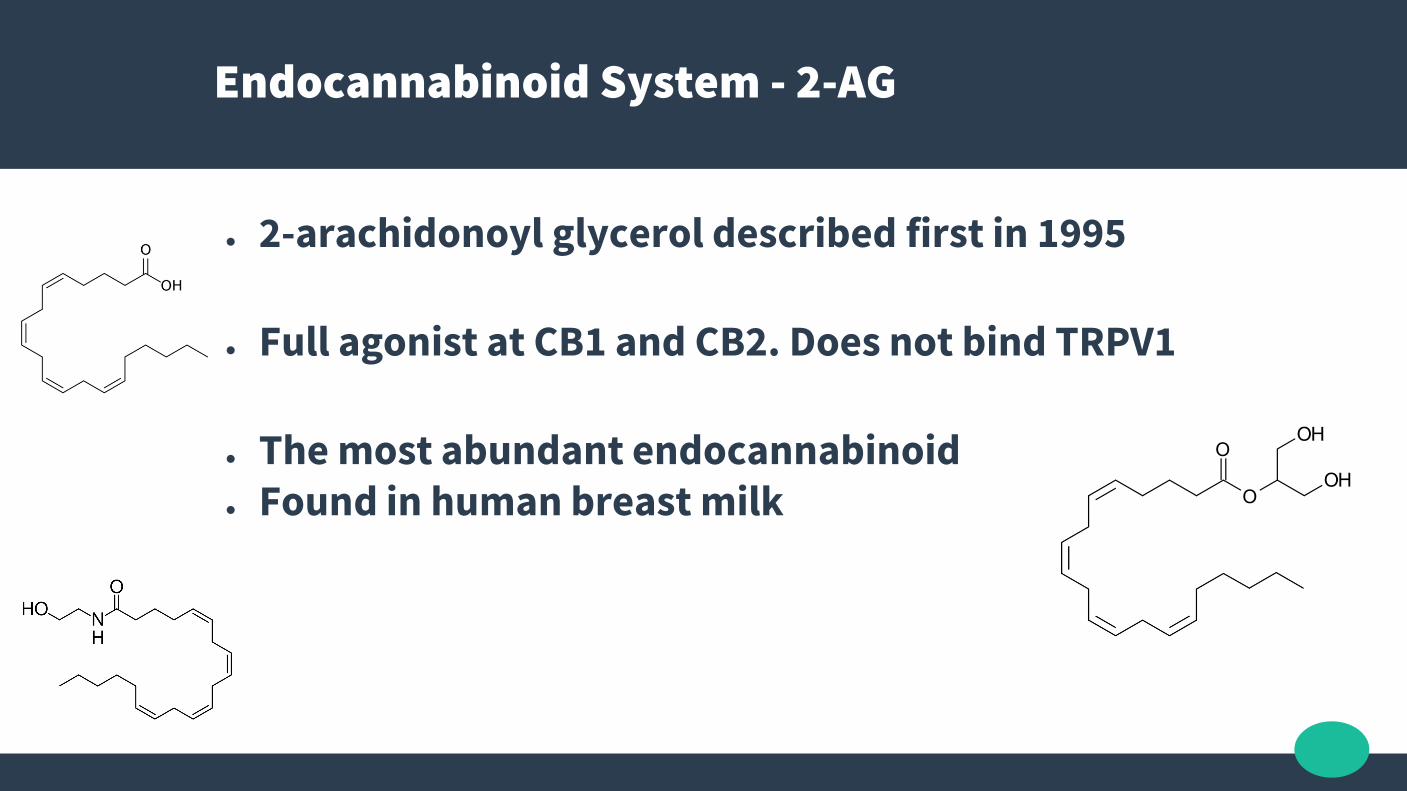
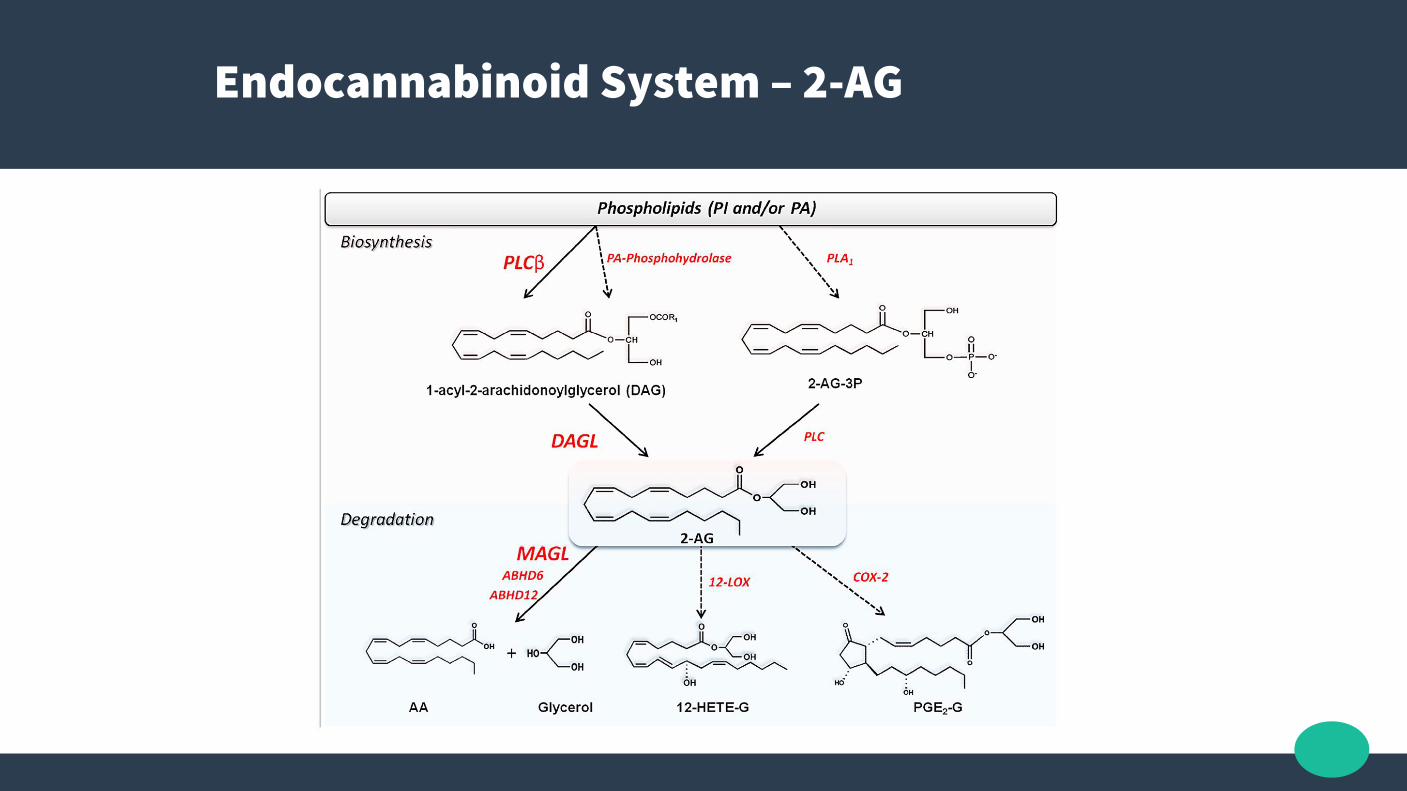
Endocannabinoid System - 2-AG
● 2-arachidonoyl glycerol described first in 1995
● Full agonist at CB1 and CB2. Does not bind TRPV1
● The most abundant endocannabinoid● Found in human breast milk
Endocannabinoid System – 2-AG
TRPV1 receptor
Aka Capsaicin receptor & the Vanilloid receptor 1 (Transient receptor potential cation channel subfamily V member 1)
● Involved in heat sensation and pain detection, and also regulation of body temperature
● Agonists possibly cause down regulation egCapsaicin cream
● Cannabidiol is an agonist
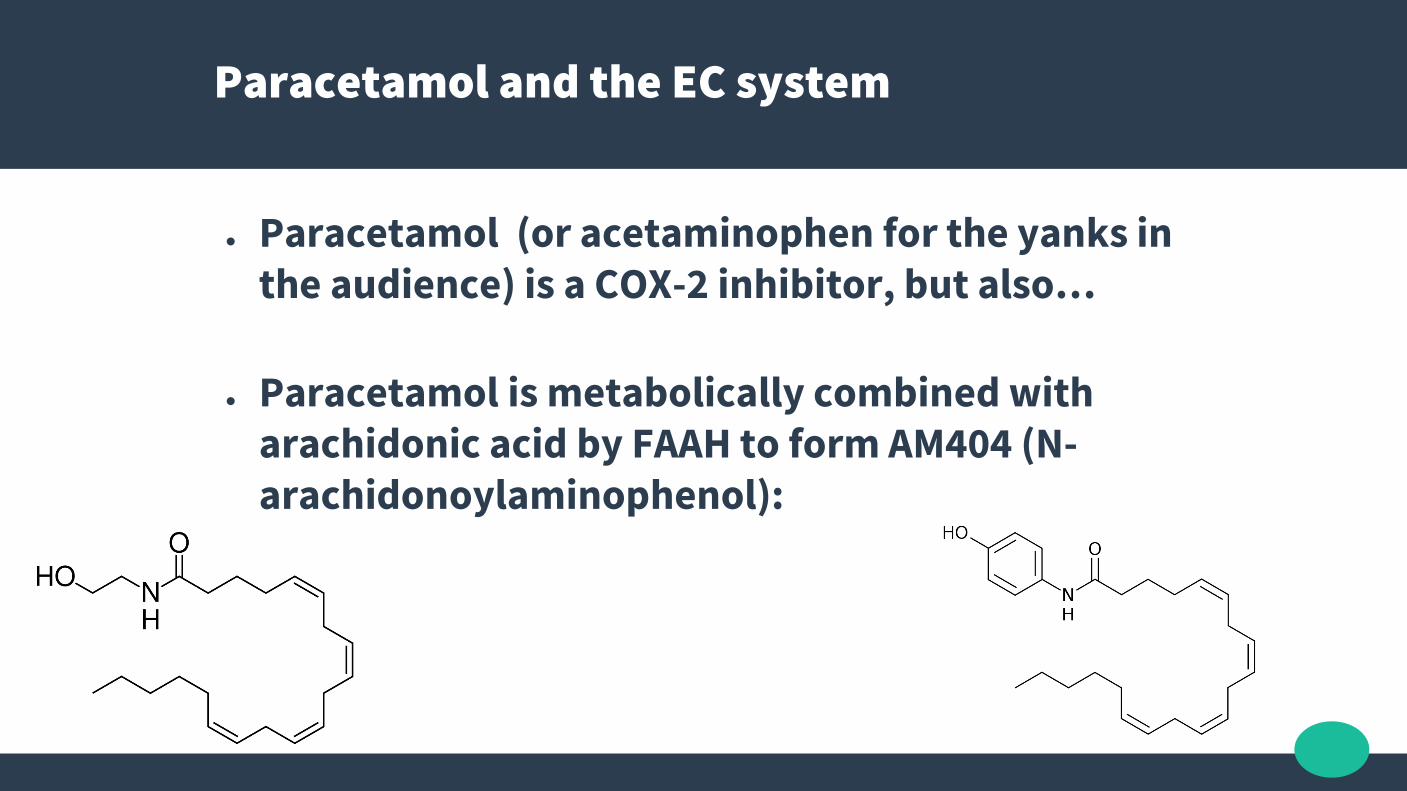
Paracetamol and the EC system
● Paracetamol (or acetaminophen for the yanks in the audience) is a COX-2 inhibitor, but also…
● Paracetamol is metabolically combined with arachidonic acid by FAAH to form AM404 (N-arachidonoylaminophenol):

Paracetamol and the EC system
● AM404 a potent agonist at the TRPV1 vanilloidreceptor, a weak agonist at both CB1 and CB2 receptors, and an inhibitor of anandamide reuptake
● As a result, anandamide levels in the body and brain are elevated
● In this fashion, paracetamol acts as a pro-drug for an endocannabinoid metabolite

Endocannabinoid System
● ECS homeostatic roles have been summarized as “relax, eat, sleep, forget, and protect.”
● Suboptimal ECS functioning considerations: migraine, fibromyalgia, irritable bowel syndrome, “failure to thrive” syndrome, depressive illnesses, uncompensated schizophrenia, multiple sclerosis, Huntington's, uncompensated Parkinson's, uncompensated anorexia, and chronic motion sickness.
● Correcting CEDS may be accomplished via at least three molecular mechanisms:− 1. Augmenting Endocannabinoid ligand biosynthesis; − 2. Decreasing Endocannabinoid ligand degradation; − 3. Augmenting or increasing receptor density or function.
● McPartland JM, Guy GW, Di Marzo V. Care and Feeding of the Endocannabinoid System: A Systematic Review of Potential Clinical Interventions that Upregulate the Endocannabinoid System. Romanovsky AA, ed. PLoS ONE. 2014;9(3):e89566. doi:10.1371/journal.pone.0089566.
CEDS – Clinical Endocannabinoid Def Syn
Cannabis Components
● 400+ molecules in raw Cannabis● 100+ Terpenes (volatile unsaturated
hydrocarbons found in the essential oils)● 112+ different Cannabinoids● Cannabinoids in acid forms● Fibre● PUFA’s, phytosterols, vit E, G+C Linoleic Acid,
omega 3’s + 6’s, folate, Mg, Fe, Zn, Protein
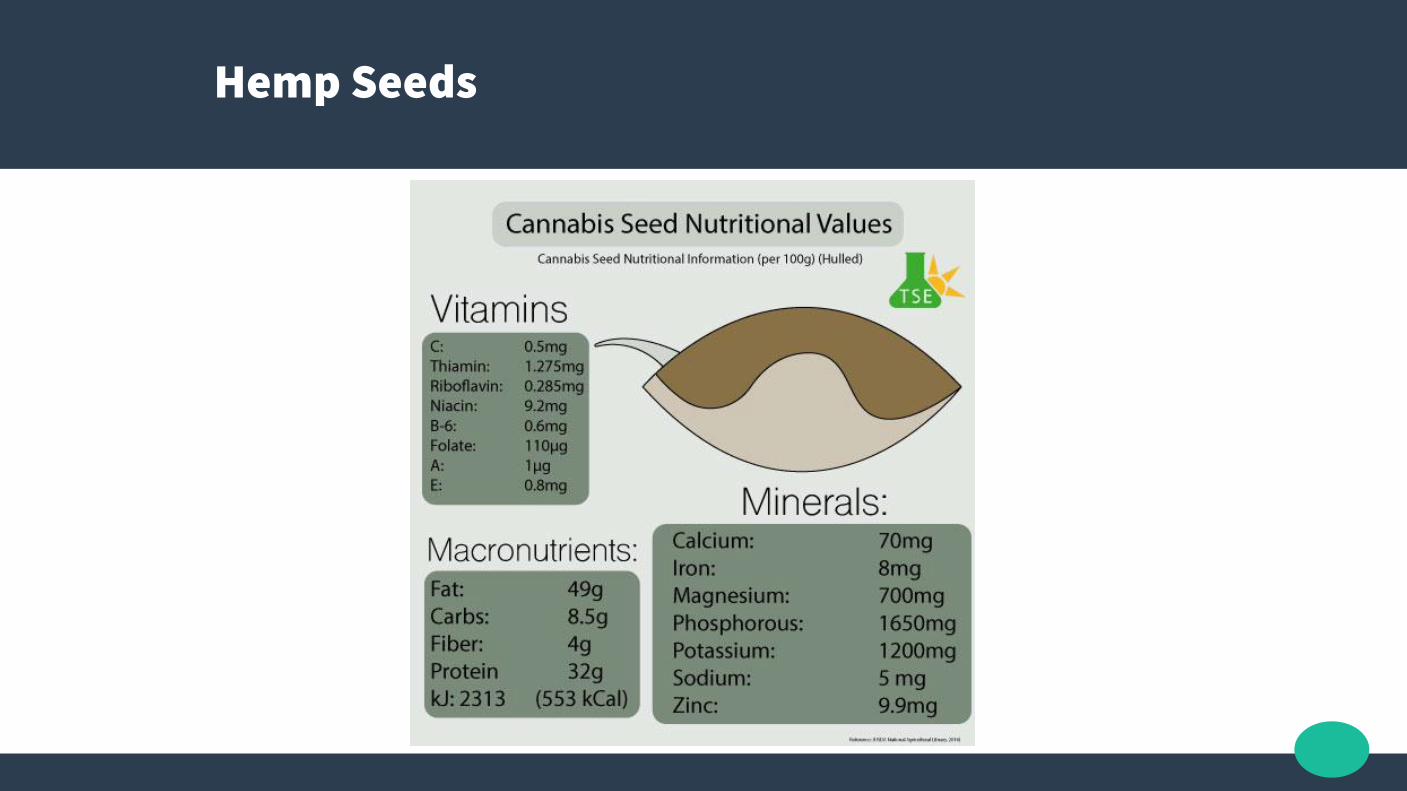
Hemp Seeds
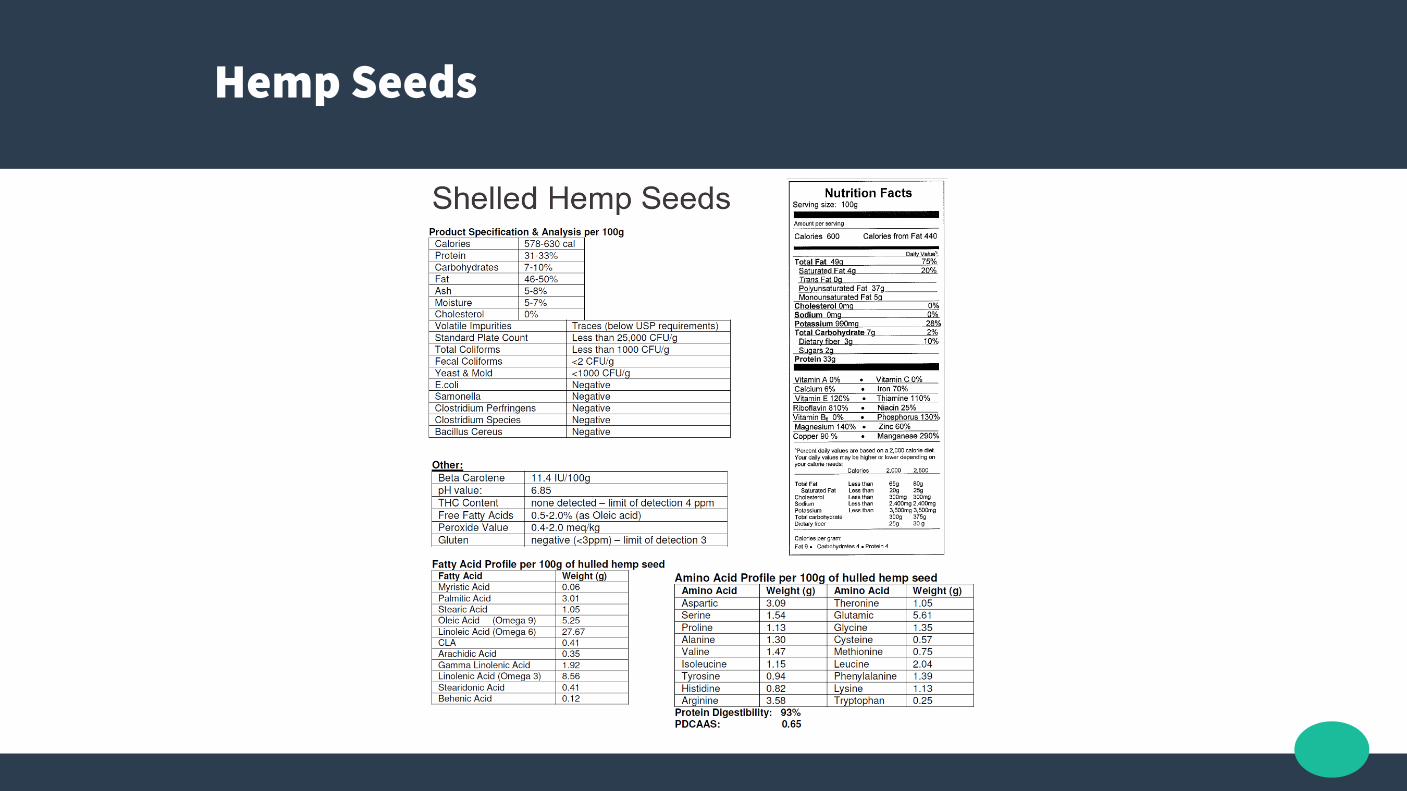
Hemp Seeds
Phytocannabinoids
● CBG (Cannabigerol)● CBC (Cannabichromene)● CBL (Cannabicyclol)● CBV (Cannabivarin)● THCV (Tetrahydrocannabivarin)● CBDV (Cannabidivarin)● CBCV (Cannabichromevarin)● CBGV (Cannabigerovarin)● CBGM (Cannabigerol Monomethyl Ether)● THC (Tetrahydrocannabinol)● THCA (Tetrahydrocannbinolic acid)● CBD (Cannabidiol)● CBDA (Cannabidiolic Acid)
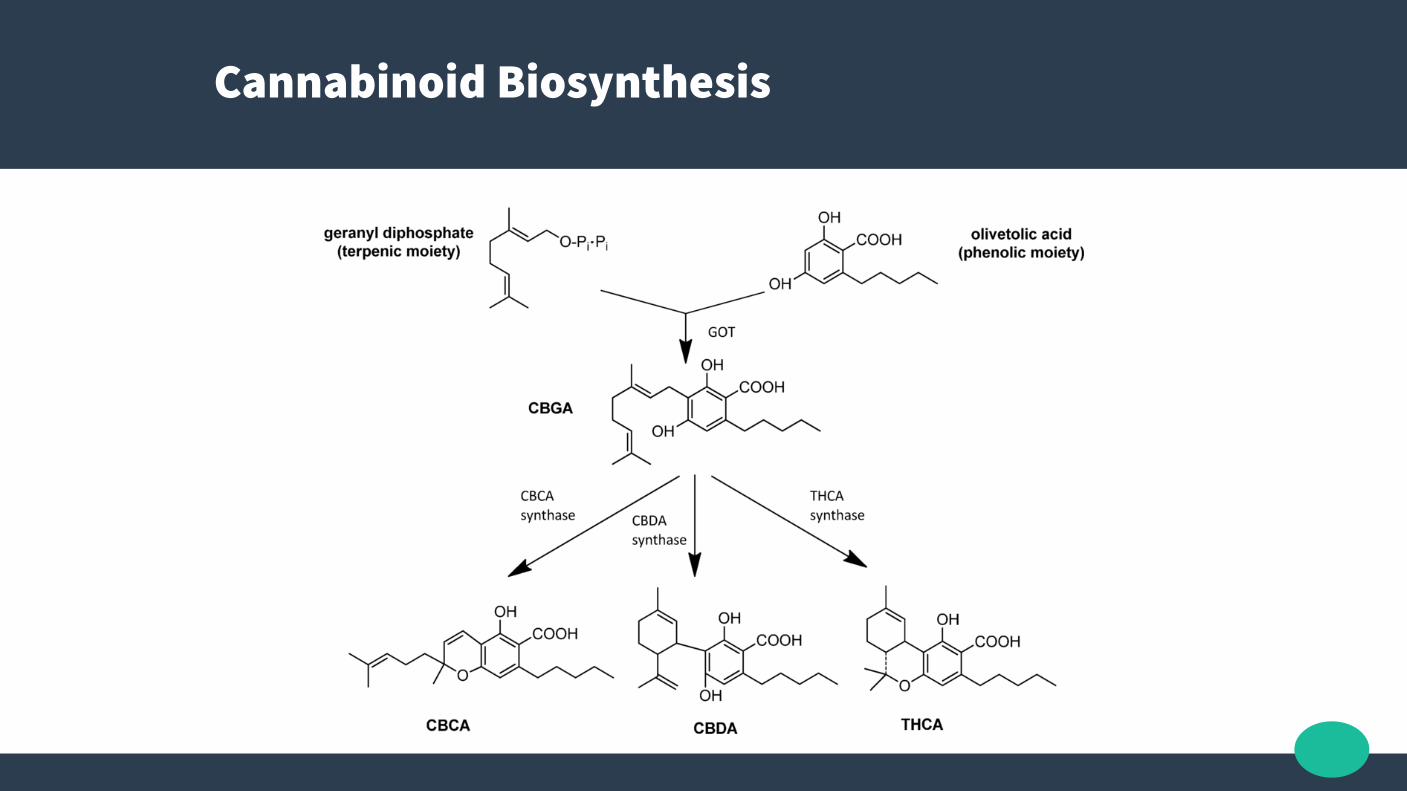
Cannabinoid Biosynthesis
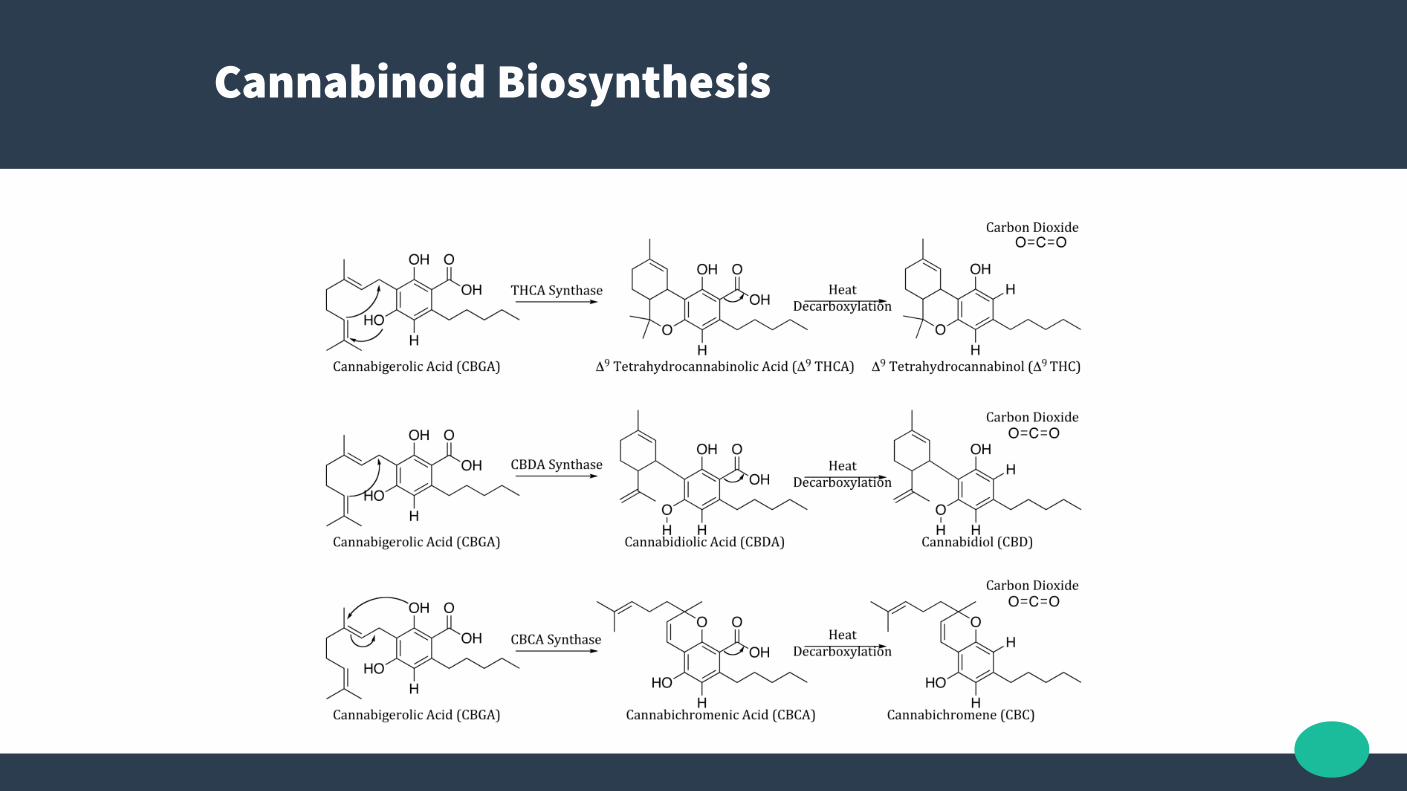
Cannabinoid Biosynthesis
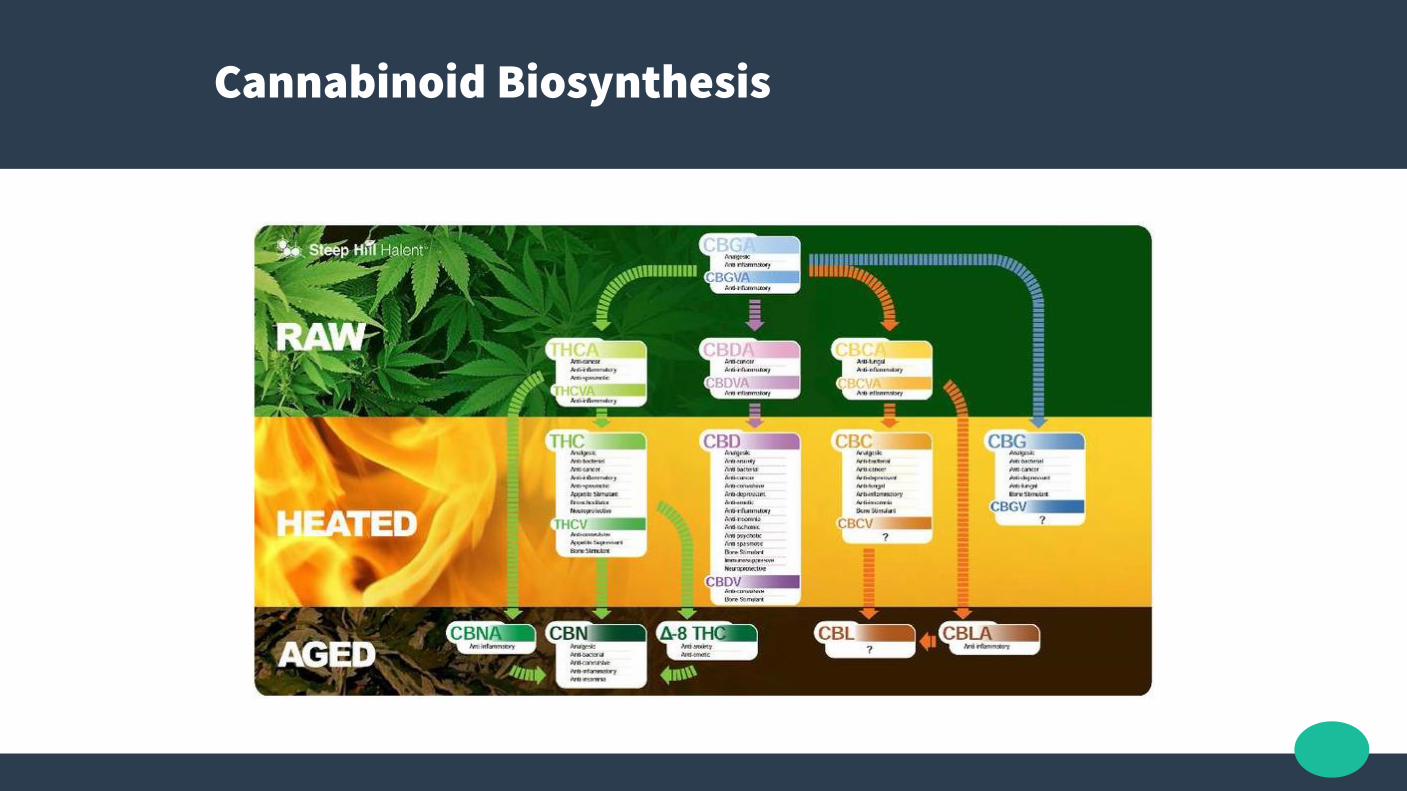
Cannabinoid Biosynthesis
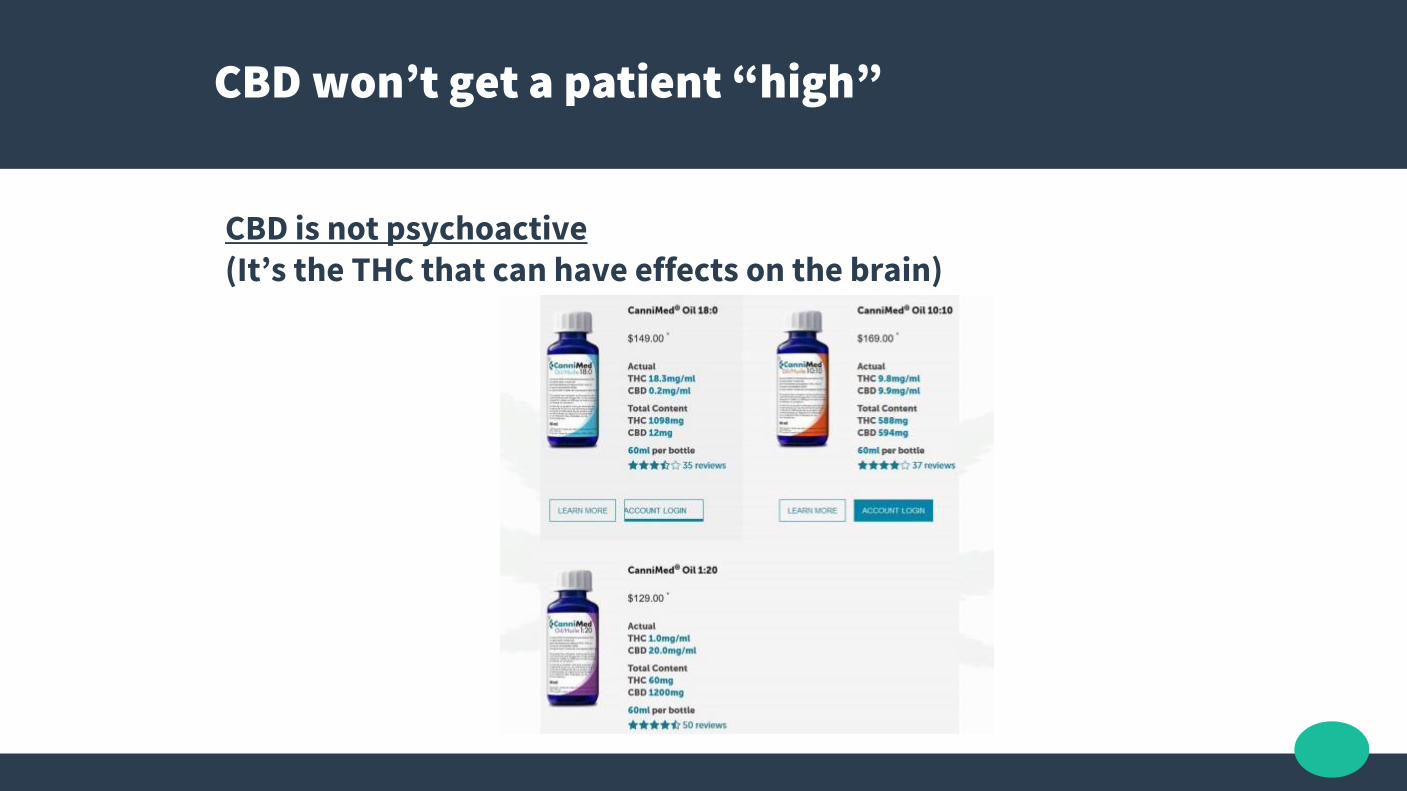
CBD won’t get a patient “high”
CBD is not psychoactive(It’s the THC that can have effects on the brain)
Cannabidiol – CBD (key slide to remember)
● No “high”; Not Psychoactive
● Side effects in high dose > cotton mouth, P450 inhibition, inhibit anti-epileptic medication metabolism, ?drug interactions
● Low binding affinity for CB1 and CB2 receptors, but activates several non-cannabinoid receptors and ion channels, and...
● Delays the reuptake and breakdown of endogenous endocannabinoids (such as anandamide or 2AG) – this is the entourage effect with other cannabinoids.

Cytochrome P450 Enzyme Interactions
● CYP450 enzymes are primarily located in the liver ● CYP450 enzymes production and breakdown organic
molecules, especially some drugs● In vitro interactions are minimal

CBD effects
● 5-HT1A serotonin receptor agonist with antidepressant activity (CBDa more of an agonist)
● TRPV1 agonist, with analgesic effects● GPR55 antagonist, with anti-osteoporosis and anticancer cell
proliferation effects● CBD's anti-inflammatory and anti-anxiety effects are in part
attributable to its inhibition of adenosine reuptake. A1A and A2A adenosine receptors play significant roles in cardiovascular function, regulating myocardial oxygen consumption and coronary blood flow. These receptors have broad anti-inflammatory effects throughout the body

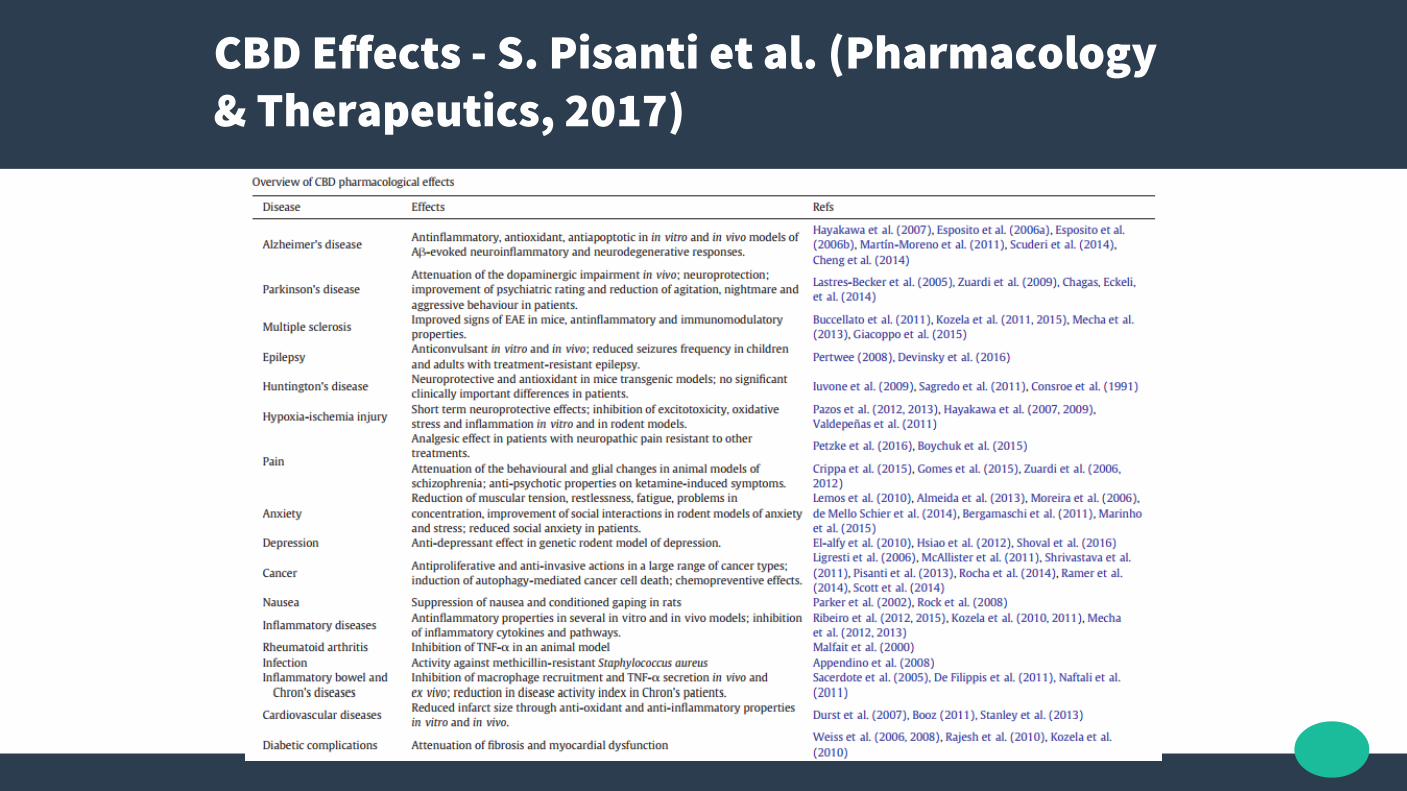
CBD Effects - S. Pisanti et al. (Pharmacology & Therapeutics, 2017)
CBD Myocardial Protection
● “Cannabidiol, a nonpsychoactive Cannabis constituent, protects against myocardial ischemic reperfusion injury”. Durst et al. Am J of Physiology - Heart and Circ Physiology, 1 Dec 2007; 293 (6), H3602-H3607. DOI: 10.1152/ajpheart.00098.2007
● The LAD coronary artery was transiently ligated for 30 min, and the rats were treated for 7 days with CBD (5 mg/kg ip) or placebo vehicle.
● Infarct size was reduced by 66% in CBD-treated animals.
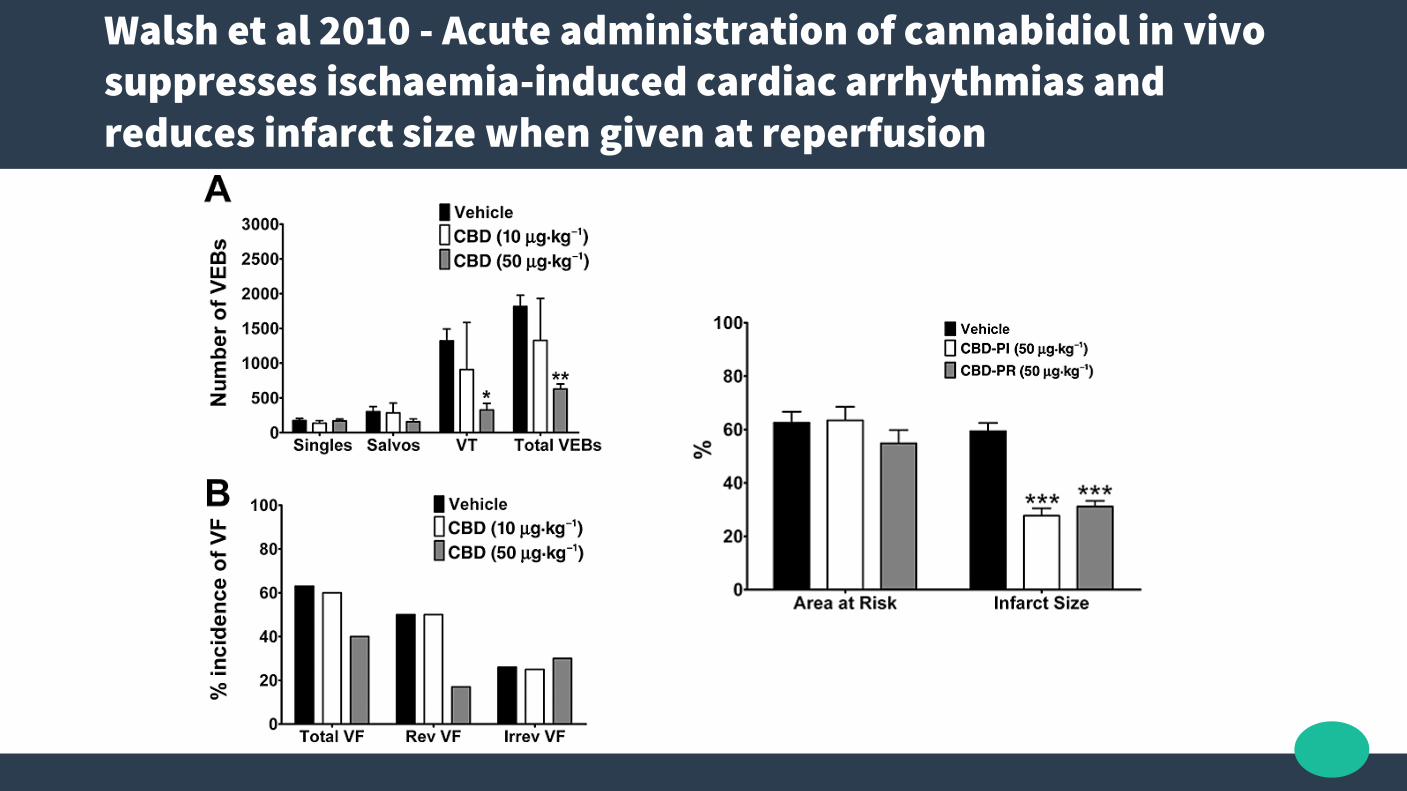
Walsh et al 2010 - Acute administration of cannabidiol in vivo suppresses ischaemia-induced cardiac arrhythmias and reduces infarct size when given at reperfusion
CBD Neuroprotection - US Patent US6630507
● US Patent US6630507 - CANNABINOIDS AS ANTIOXIDANTS AND NEUROPROTECTANTS (2003) Assignee: The United States of America as represented by the
Department of Health and Human Services, Washington, DC (US)
● “This new found property makes Cannabinoids useful in the treatment and prophylaxis of a wide variety of oxidation associated diseases, such as ischemic, age-related, inflammatory and autoimmune diseases.”
● “The Cannabinoids are found to have particular application as neuroprotectants, for example in limiting neurological damage following ischemic insults, such as stroke and trauma, or in the treatment of neurodegenerative diseases, such as Alzheimer’s disease, Parkinson’s disease and HIV dementia.”

CBD Neuroprotection - US Patent US6630507
● US Patent US6630507 - CANNABINOIDS AS ANTIOXIDANTS AND NEUROPROTECTANTS (2003) Assignee: The United States of America as represented by the Department of Health
and Human Services, Washington, DC (US)
● Example 7 “The middle cerebral artery of chloral hydrate anaesthetised rats was occluded by insertion of suture thread into it. The animals were allowed to recover from the anesthetic and move freely for a period of two hours. After this time the suture was removed under mild anesthetic and the animals allowed to recover for 48 hours.”
● “Infarct size was approximately halved in the animals treated with cannabidiol, which was also accompanied by a substantial improvement in the neurological status of the animal.”
CBD Neuroprotection - US Patent US6630507
● US Patent US6630507 - CANNABINOIDS AS ANTIOXIDANTS AND NEUROPROTECTANTS (2003) Assignee: The United States of America as represented by the
Department of Health and Human Services, Washington, DC (US)
● “Non-psychoactive Cannabinoids, such as cannabidiol, are particularly advantageous to use because they avoid toxicity that is encountered with psychoactive Cannabinoids at high doses.”

2015 England et al - Cannabinoids and stroke: a systematic review
Sharf 2017 - Translating Endocannabinoid Biology into Clinical Practice - Cannabidiol for Stroke Prevention
● Double-blind RCT of placebo, Cannabidiol(CBD) 75 mg/day or CBD 300 mg/day.
● Groups treated with placebo and CBD 300 mg/day had significantly different mean total scores in the PDQ-39 (well-being and quality of life) (p = 0.05).
Chagas et al (2014) - Effects of cannabidiol in the treatment of patients with Parkinson's disease: an exploratory double-blind trial (RCT, n=21)
● Double-blind RCT of Cannabidiol vs Amisulpride (a potent antipsychotic).
● Either treatment was safe and led to significant clinical improvement, but Cannabidiol displayed a markedly superior side-effect profile.
● Acutely psychotic patients age 18 to 50 years with a total Brief Psychiatric Rating Scale (BPRS) score ⩾36 and a BPRS THOT factor (thought disorders) score ⩾12.
● Patients were randomized (1:1) to receive either Cannabidiol or Amisulpride starting with 200 mg per day each and increased stepwise by 200 mg per day to a daily dose of 200 mg four times daily (total 800 mg per day) each within the first week. A dose reduction to 600mg per was allowed after week 2 if side effects.
Leweke et al (2012) - Cannabidiol enhances anandamide signaling and alleviates psychotic symptoms of schizophrenia (RCT, n=42)
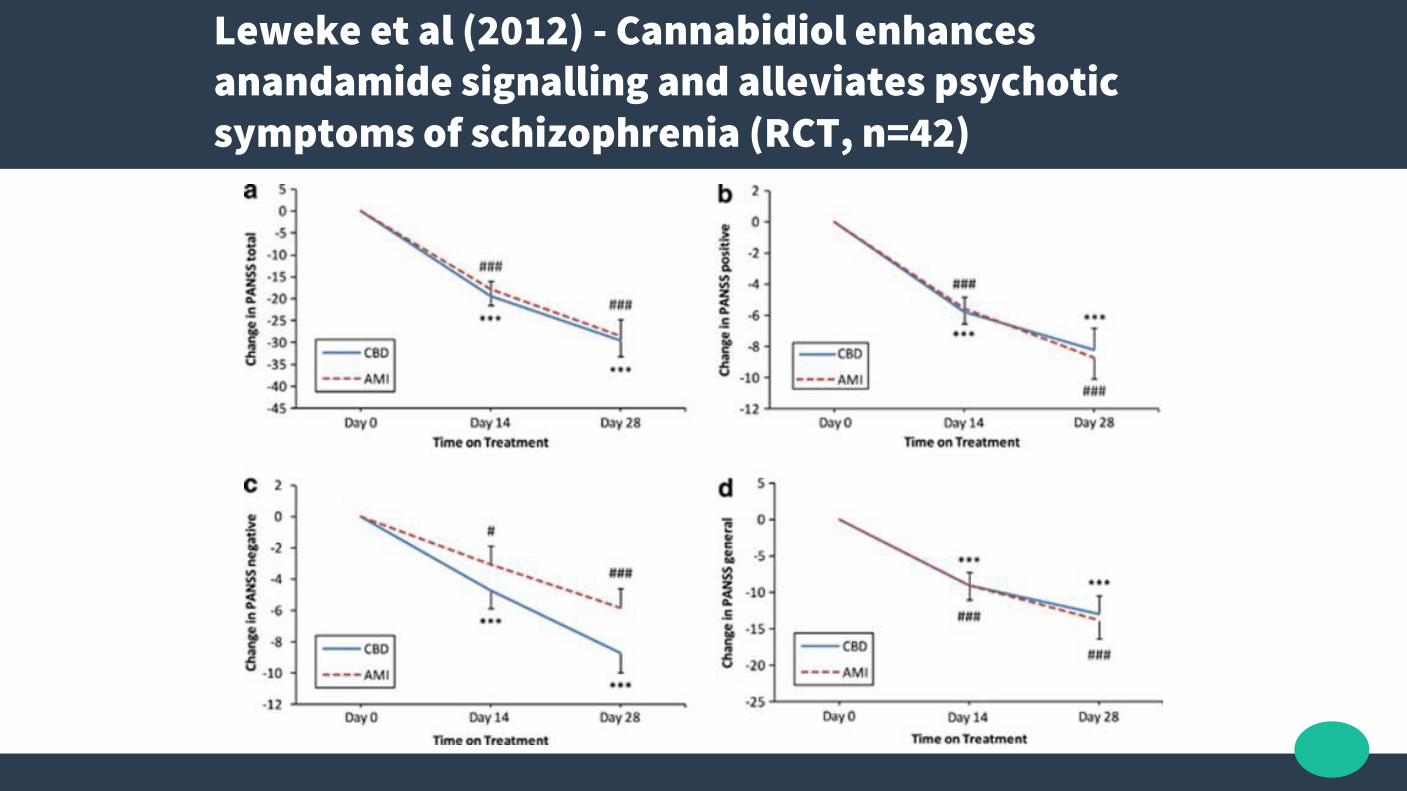
Leweke et al (2012) - Cannabidiol enhances anandamide signalling and alleviates psychotic symptoms of schizophrenia (RCT, n=42)
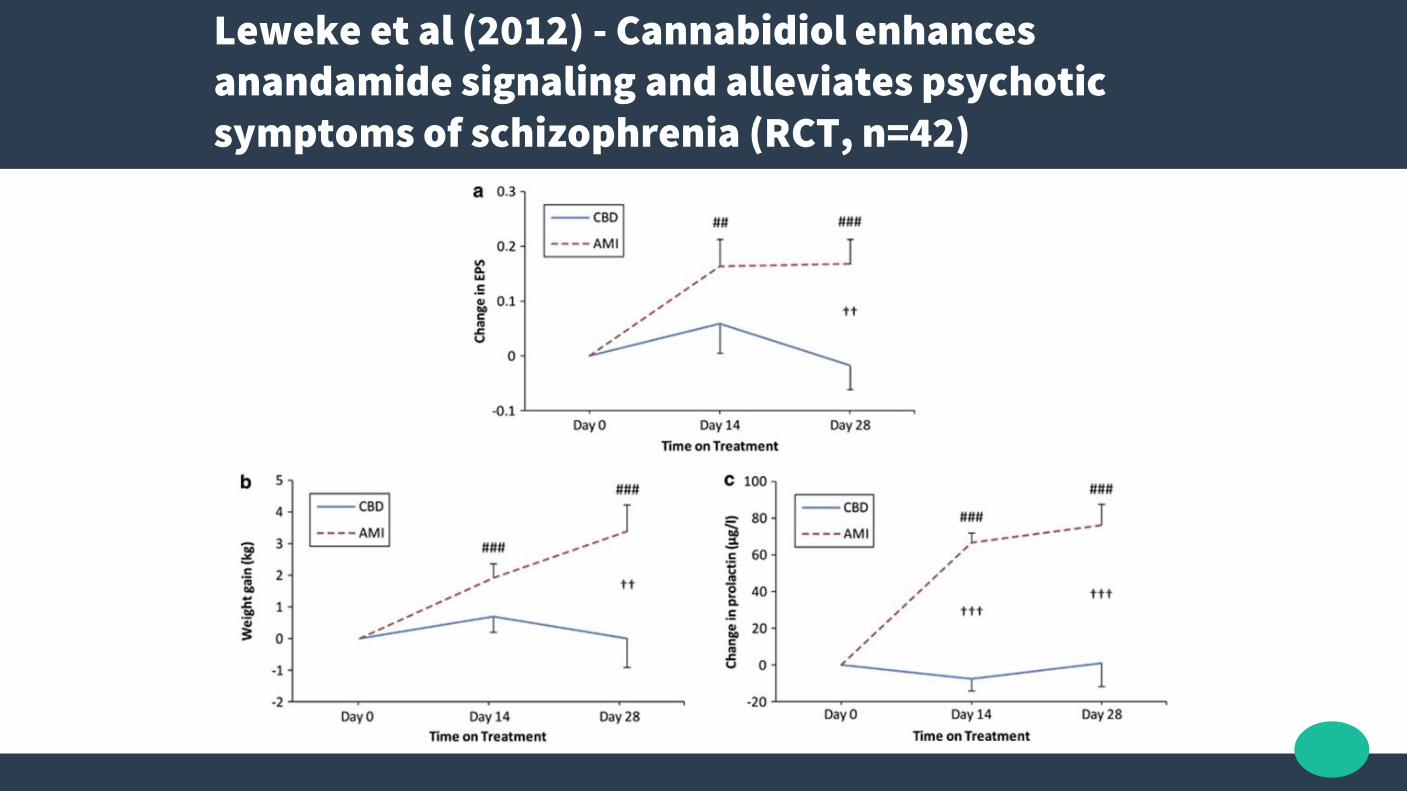
Leweke et al (2012) - Cannabidiol enhances anandamide signaling and alleviates psychotic symptoms of schizophrenia (RCT, n=42)

McGuire et al (2017) - Cannabidiol (CBD) as an Adjunctive Therapy in Schizophrenia: A Multicenter Randomized Controlled Trial (n = 88)
● 1000mg/day vs placebo for 6weeks, RCT, n=88● On 4+weeks stable antipsychotic dose, and partial response to
antipsychotic medication

McGuire et al (2017) - Cannabidiol (CBD) as an Adjunctive Therapy in Schizophrenia: A Multicenter Randomized Controlled Trial (n = 88)
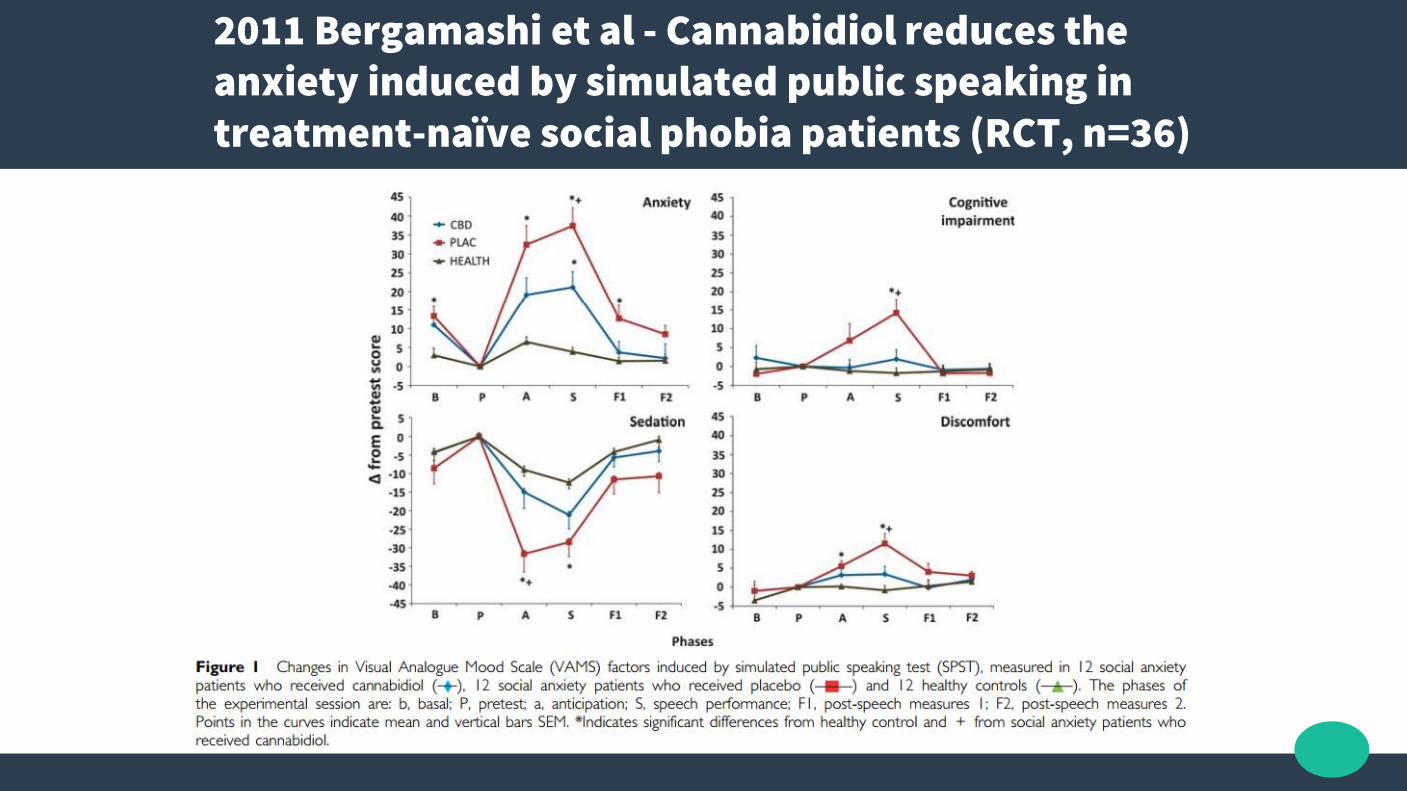
2011 Bergamashi et al - Cannabidiol reduces the anxiety induced by simulated public speaking in treatment-naïve social phobia patients (RCT, n=36)

2015 Blessing et al - Cannabidiol as a Potential Treatment for Anxiety Disorders

2018 Crombie et al - Psychobiological Responses to Aerobic Exercise in Individuals With Posttraumatic Stress Disorder (Blunted ECS in PTSD patients)
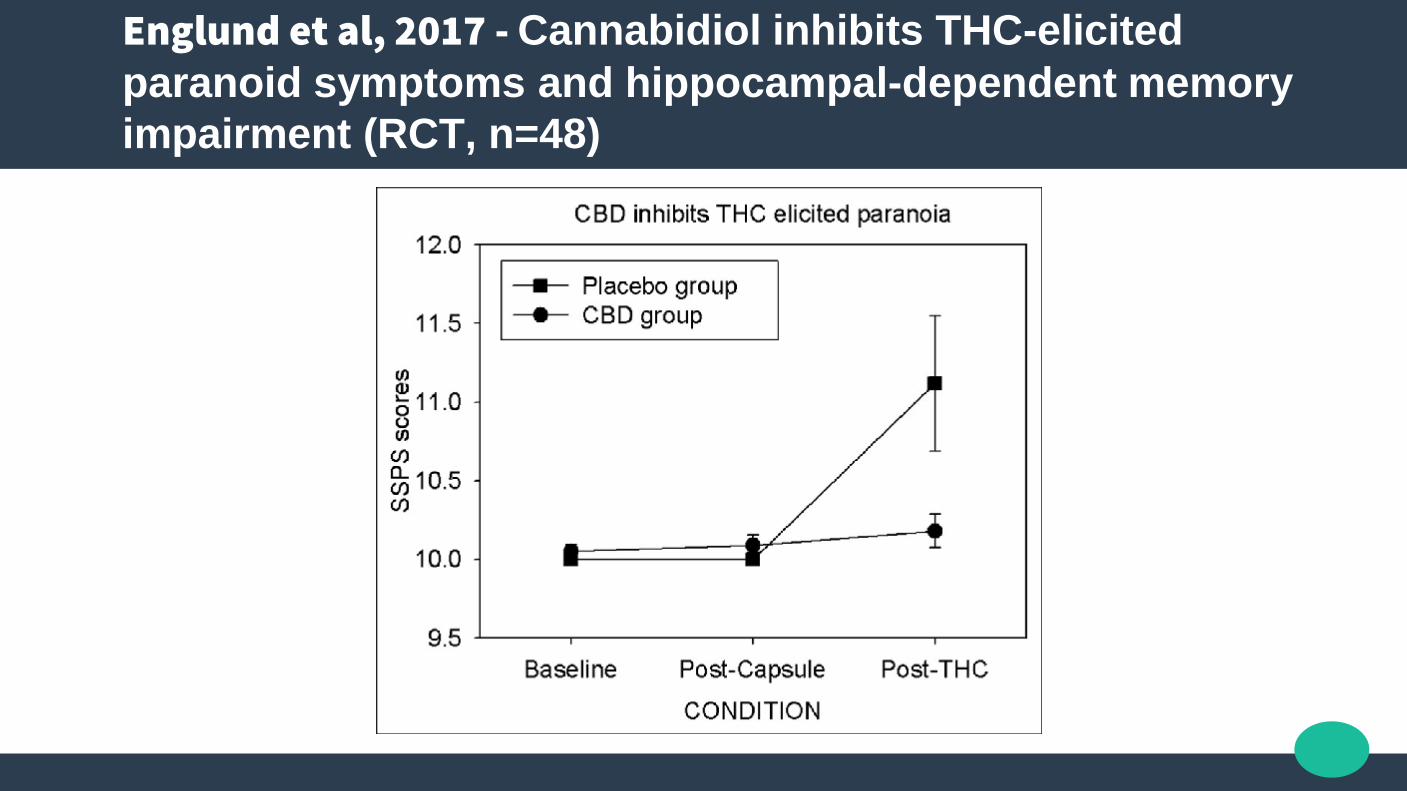
Englund et al, 2017 - Cannabidiol inhibits THC-elicited
paranoid symptoms and hippocampal-dependent memory
impairment (RCT, n=48)

Trial of CBD for Drug-Resistant Seizures in Dravet Syndrome, 2017 NEJM
● N=120, RCT

Ayurveda text (5000yrs BCE) and Sir. William Brooke O'Shaughnessy (1800’s) already knew Cannabis worked for seizure disorders
On the preparations of the Indian hemp, or gunjah (Cannabis Indica), their
effects on the animal system in health, and their utility in the treatment of
tetanus and other convulsive disorders (O’Shaghnessy 1843)
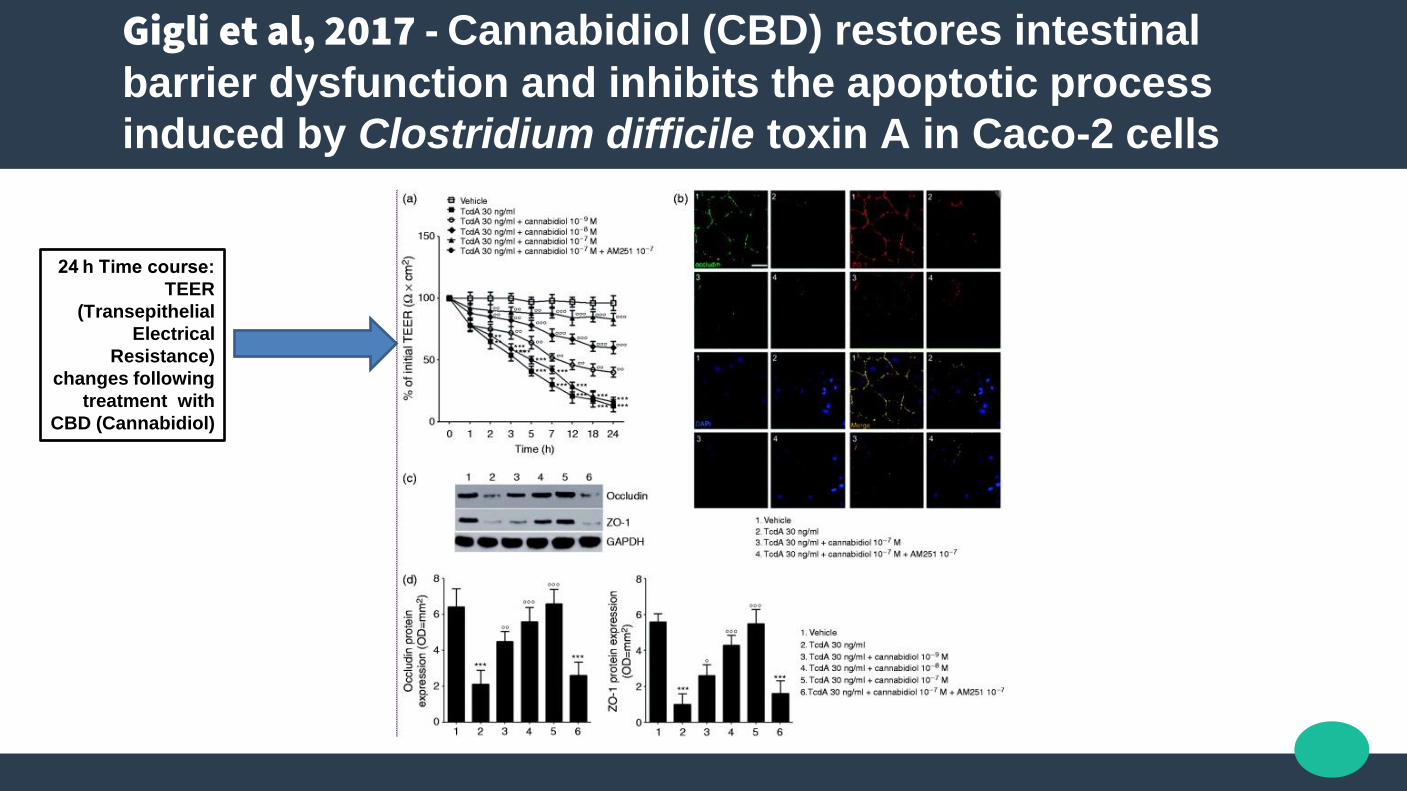
Gigli et al, 2017 - Cannabidiol (CBD) restores intestinal
barrier dysfunction and inhibits the apoptotic process
induced by Clostridium difficile toxin A in Caco-2 cells
24 h Time course:
TEER
(Transepithelial
Electrical
Resistance)
changes following
treatment with
CBD (Cannabidiol)
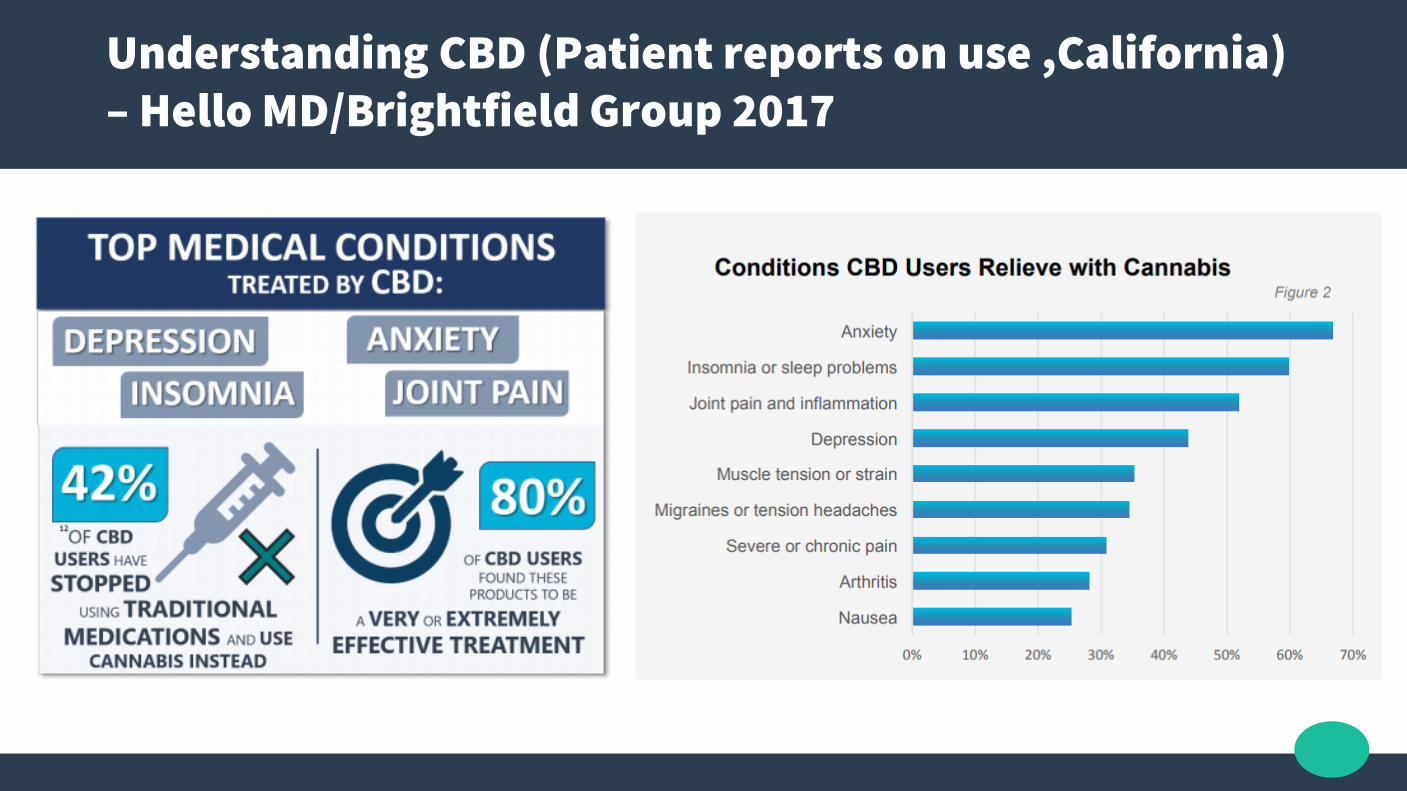
Understanding CBD (Patient reports on use ,California) – Hello MD/Brightfield Group 2017

CBD Dose
● To decrease THC neurological effects: 1:1+ THC<CBD ratio
● Start 5mg BD
● Chronic pain: 2.5-20 mg CBD by mouth for an average of 25 days● Anxiety: 5-100 mg CBD by mouth for four weeks● Epilepsy: 200-600 mg of CBD by mouth daily for up to 4.5 months● Movement problems associated with Huntington’s disease: 10 mg per kilogram
of CBD by mouth daily for six weeks● Sleep disorders: 40-160 mg CBD by mouth● Multiple Sclerosis symptoms: Cannabis plant extracts containing 2.5-120 mg of
a THC-CBD combination by mouth daily for 2-15 weeks● Schizophrenia: 40-1,280 mg CBD by mouth daily for up to four weeks
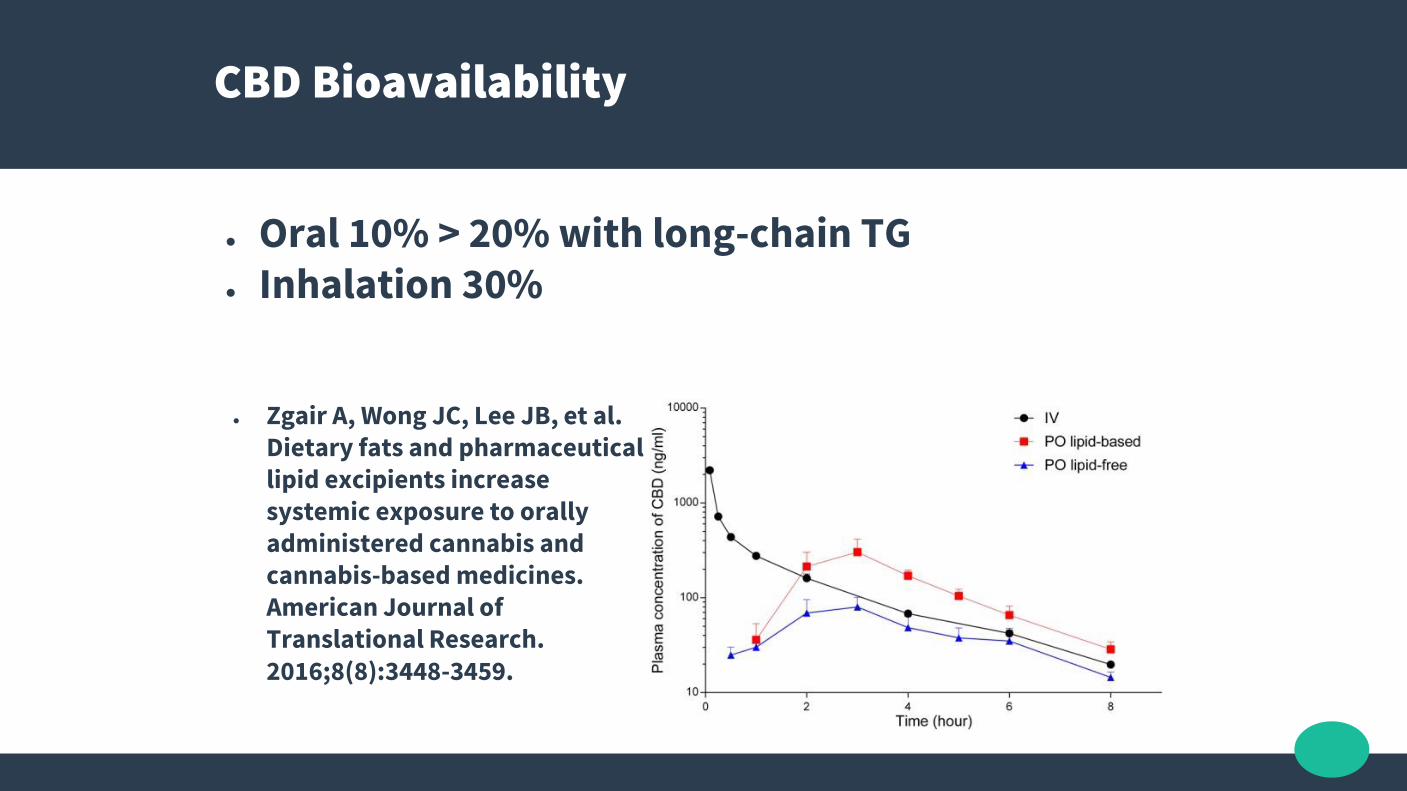
CBD Bioavailability
● Oral 10% > 20% with long-chain TG● Inhalation 30%
● Zgair A, Wong JC, Lee JB, et al. Dietary fats and pharmaceutical lipid excipients increase systemic exposure to orally administered cannabis and cannabis-based medicines. American Journal of Translational Research. 2016;8(8):3448-3459.
WHO Expert Committee on Drug Dependence, Nov 2017
● “In humans, CBD exhibits no effects indicative of any abuse or dependence potential”.
● “CBD has been demonstrated as an effective treatment of epilepsy in several clinical trials, with one pure CBD product (Epidiolex®) currently in Phase III trials. There is also preliminary evidence that CBD may be a useful treatment for a number of other medical conditions”.
● “Across a number of controlled and open label trials CBD of the potential therapeutic effects of CBD it is generally well tolerated, with a good safety profile”.
● http://www.who.int/medicines/access/controlled-substances/5.2_CBD.pdf
Tetrahydrocannabinolic acid - THCA
● No “high”; Not Psychoactive● Weak CB1 and CB2 binding. ● Inhibitor of PC-PLC, COX-1, COX-2, TRPM8, TRPV1, FAAH, NAAA, MGL, and DGLα, and an
inhibitor of anandamide transport, as well as an agonist of TRPA1 and TRPV2.
● Analgesic – Relieves pain, Cox-2 Inhibition.● Anti-Emetic – Reduces vomiting and nausea.● Anti-Inflammatory – Especially GI inflammation.● Anti-Proliferative – Inhibits cancer cell growth, TNF inhibition● Modulates Immune System – THCa has been shown to both improve and
potentially suppress the immune system functions.● Neuroprotective – in cellular and animal models.

Cannabis “Juicers” - Raw Acid Cannabinoids
● Dr. Courtney has researched the benefits of raw cannabis and has come to the following conclusions:− Smoking cannabis may not treat the disease, only the symptoms− Therapeutic levels of cannabinoids are better achieved through ingestion− When cannabis is heated or burned, the chemical structure of the plant
compounds are changed, specifically the acidity of THC, which alters its ability to be therapeutic
− Raw cannabis activates the brain’s cannabinoid system, which triggers an antioxidant release
− These antioxidants act as a “cleaner” and remove damaged cells from the body− Raw cannabis improves the efficiency of the cells in our body− Creating oils, butters or eating the raw plant is the best way to get the necessary
beneficial compounds
− Dr Courtney’s wife successfully treats her lupus with raw cannabis
Cannabis “Juicers”
● Juicing specifically takes a lot of material; Dr.Courtney suggests 20-30 big shade leaves or 2-3 raw buds (2-3 inches in length) per day for therapeutic benefits
● Added to salads or sprinkled on foods
● Keep below 100*c to remain non-psychoactive
● GI anti-inflammatory, higher antioxidants
THC
Δ9-Tetrahydrocannabinol – THC
● THCa is not psychoactive (no high) > but heated to 120*c will turn into THC which is psychoactive
● LD50 could not be determined in either rhesus monkeys or dogs, as single oral doses of up to 9000 mg/kg of either delta-8- or delta-9-THC in dogs or monkeys were
non-lethal (Compare to Nicotine: for rats – 50 mg/kg, for humans – 0.5-1 mg/kg)
Thompson, G. R. et. al., 1973. Toxicol. Appl. Pharmacol. 25: 373-390
● The LD50 values for Fischer rats treated orally with single doses of delta-9-THC and delta-8THC, and observed for 7 days, are 1910 mg/kg and 1980mg/kg (for males) respectively and 860 mg/kg (for females)

Δ9-Tetrahydrocannabinol - THC
● THC is a partial agonist at CB1 > CB2 receptors
● THC binding to CB1 pathways acts as a downregulator of those neurons
● THC may act on some areas to increase endogenous endocannabinoid activity Pertwee RG. Brit J of
Phar, 2008. 153 (2): 199–215.
● THC is positive allosteric modulator of the μ- and δ-opioid receptors Kathmann M et al. Naunyn Schmiedebergs Arch. Pharmacol,
2006 372 (5): 354–61.

THC Effects
● Analgesic – Relieves pain● Anti-Emetic – Reduces vomiting and nausea● Anti-Proliferative – Inhibits cancer cell growth● Antioxidant – Prevents the damage of oxidatio to other molecules in the
body● Antispasmodic – Suppresses muscle spasms● Anxiolytic – While not fully recognized as an anxiolitic compound THC does
seem to assist in the anxiety associated with PTSD● Appetite Stimulant – Δ9-THC is the only cannabinoid identified that is an
appetite stimulant, giving people the stereotypical “munchies” many users describe
● Euphoriant – Produces feelings of euphoria, promotes happiness and relaxation
● Neuroprotective
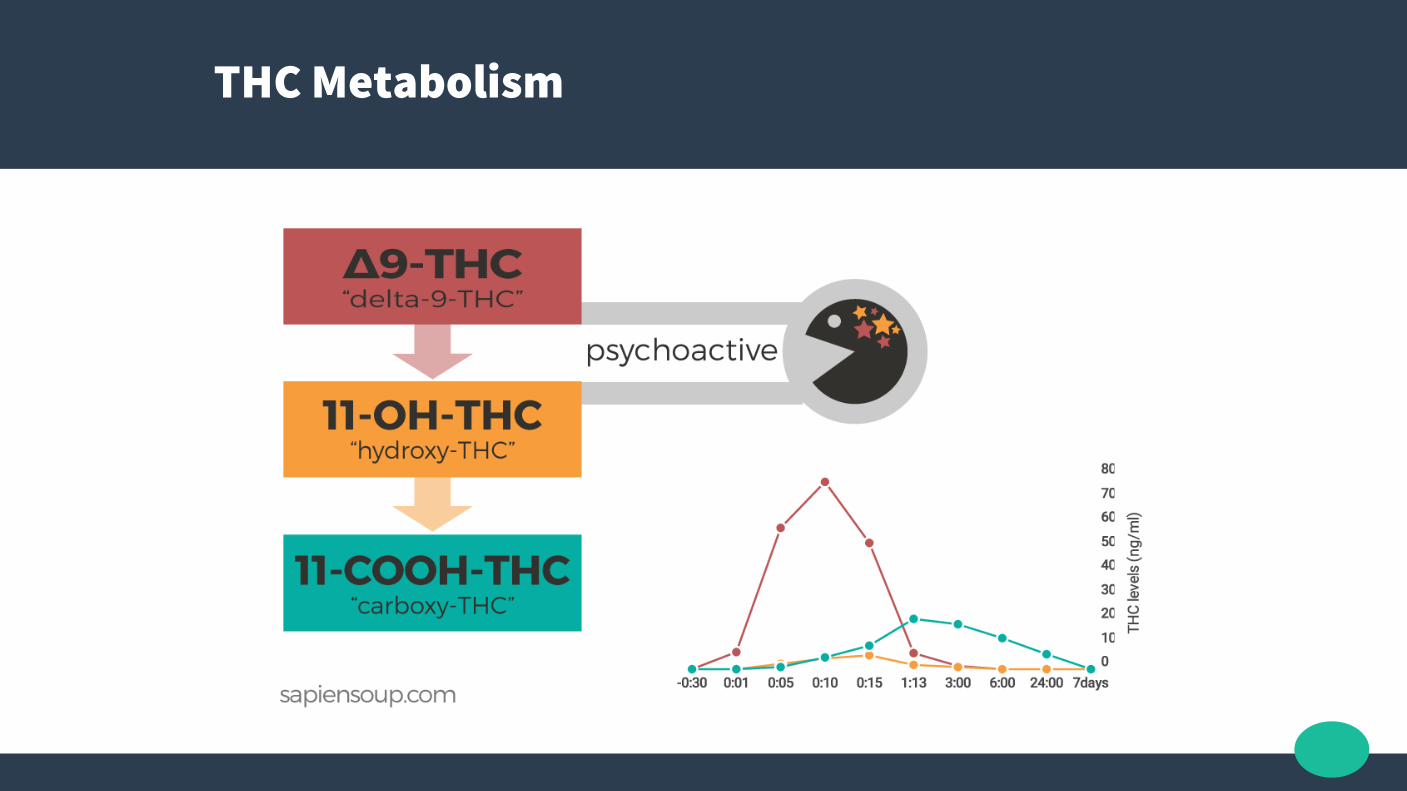
THC Metabolism

THC Metabolism
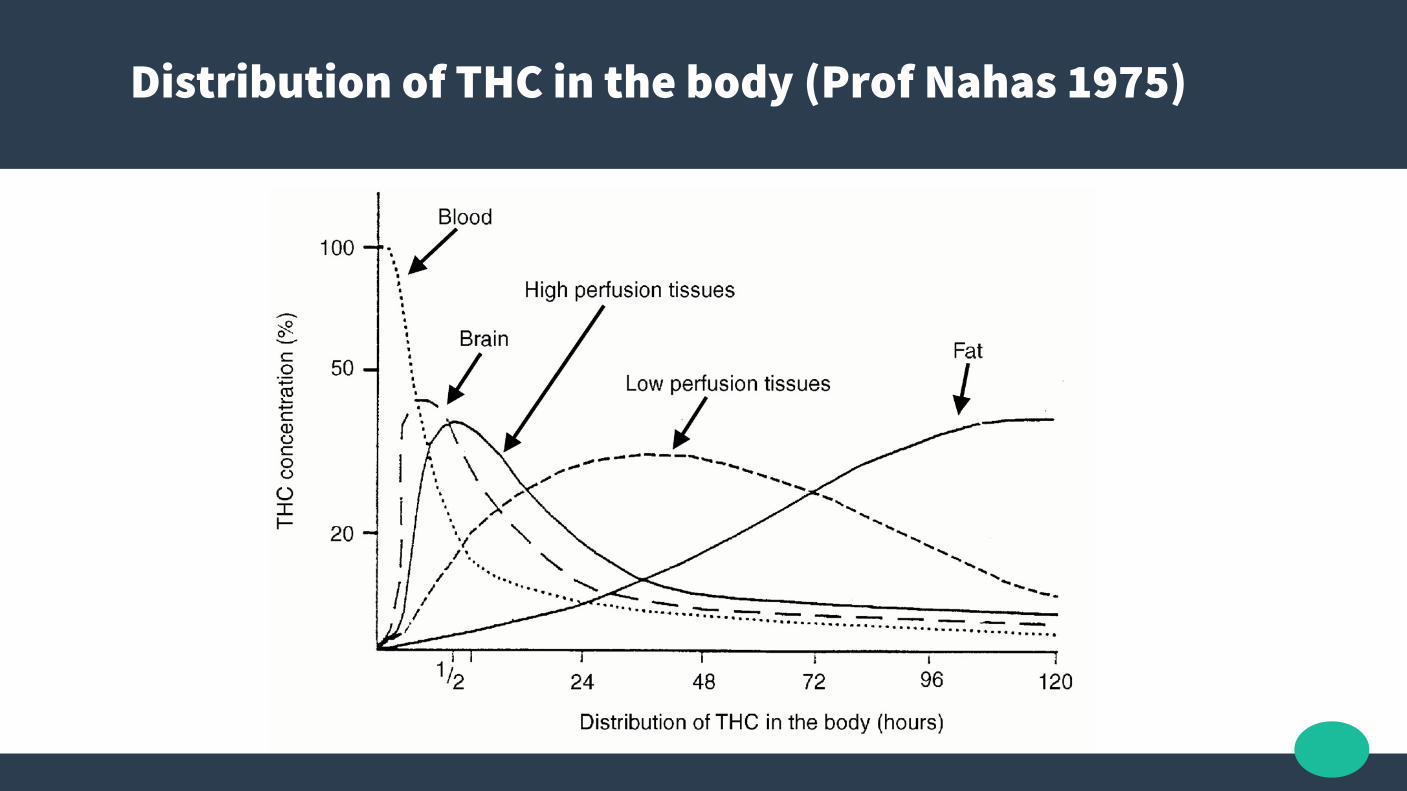
Distribution of THC in the body (Prof Nahas 1975)
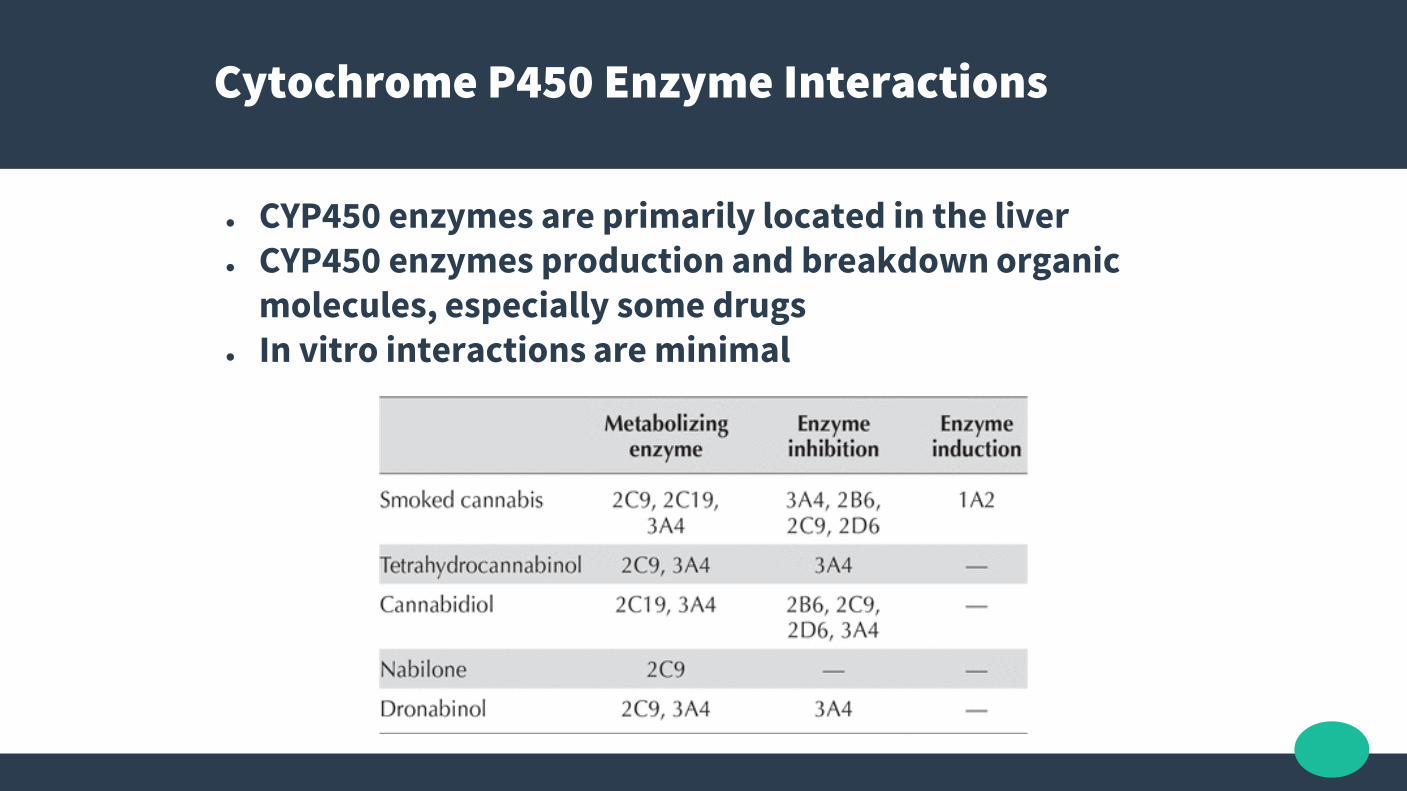
Cytochrome P450 Enzyme Interactions
● CYP450 enzymes are primarily located in the liver ● CYP450 enzymes production and breakdown organic
molecules, especially some drugs● In vitro interactions are minimal

Cytochrome P450 Enzyme Interactions
● “In clinical trials where Sativex has been taken concomitantly with other drugs metabolised by the CYP450 enzyme system, no clinically apparent drug-drug interactions have been seen at clinical doses.”
● “The inhibitory effects of Sativex on the CYP450 system seen in vitro and in animal models were only seen at exposures significantly higher doses than the maximal observed in clinical trials.”
Cytochrome P450 Enzyme Interactions*
● There is genetic variation in P450 metabolism, and thus metabolism of cannabinoids
● THC and CBD inhibit some P450 enzymes, while smoking cannabis can induce P450 1A2
● Thus, if taking a medication that needs to have levels monitored, and there is addition/removal/change of dose of cannabinoids, then testing should occur
Drug Interactions - THC
● Besides possible P450 interactions, pharmacodynamic interactions should be expected between THC and:
- drugs with sympathomimetic activity (tachycardia, hypertension)- central nervous system depressants(drowsiness, ataxia)- drugs with anticholinergic effects (tachycardia, drowsiness)
THC dosing – titration to effect
● Inhaled (vapourised) THC has immediate effects that the patient can titrate, with maximal effects at 4 minutes, and terminal effects ended by 4 hours
● 1-2mg THC inhaled is a good starting dose, with pharmacist consideration on the strength of the cannabis or THC resin
● 0.1g cannabis or a less than a quarter of a SMALL would be a relatively equivalent visible amount

THC dosing – titration to effect
THC dosing – titration to effect
● Oral use is slower to titrate; start with 2.5mg THC, a dose factor of 2.5 increase over inhalation
● Oral effects are variable from 30mins to 60mins, and lasting 4 to 8 hours generally, in a dose dependant manner
● First dosing should be in a safe familiar location in case of adverse emotional feelings, consider stat benzodiazepine PRN
THC Contraindications
● Unstable or severe cardiovascular disease● Hypotension as Cannabis will lower blood
pressure● Psychotic illness or a risk of psychotic illness –
remember to screen with PQ-16 Screening Test (Prodromal Questionaire)
● Addiction risk factors● History of Cannabis abuse
THC adverse effects
● Dose dependant*● Red conjunctiva● Increased hunger● Euphoria● Impaired short term memory● Sedation and impaired cognitive function● Anxiety, paranoia, thought disorder

THC adverse effects - Cannabinoids in the management of difficult to treat pain, Russo 2008

THC adverse effects
● High dose can lead to intoxication and thus:− Extreme sleepiness/sedation− Cognitive deficits− Depersonalisation− Hallucinations/illusion− Toxic psychosis generally lasting hours but
occasionally as long as a week
(Radhakrishnan et al. Gone to pot – A review of the association between cannabis and psychosis. Frontiers in Psychiatry, 2014. 5 (54). doi: 10.3389/fpsyt.2014.00054)
THC adverse effects – Meier et al 2016 (Dunedin longitudinal study)
● Cannabis joint-years from ages 26 to 38 years
was associated with poorer periodontal health
at age 38 years.
● However, cannabis use was unrelated to
other physical health problems. Unlike
cannabis use, tobacco use was associated
with worse lung function, systemic
inflammation, and metabolic health at age 38
years, as well as within-individual decline in health from ages 26 to 38 years.

Degenhardt et al (2003) - Testing hypotheses about the relationship between cannabis use and psychosis
“There was a steep rise in the prevalence of cannabis use in Australia over the past 30 years
and a corresponding decrease in the age of initiation of cannabis use.
There was no evidence of a significant increase in the incidence of schizophrenia over the past 30
years.”
Degenhardt et al (2003) - Testing hypotheses about the relationship between cannabis use and psychosis
“Conclusions: Cannabis use does not appear to be causally related to the incidence of schizophrenia,
but its use may precipitate disorders in persons who are vulnerable to developing psychosis and worsen the course of the disorder among those
who have already developed it.”
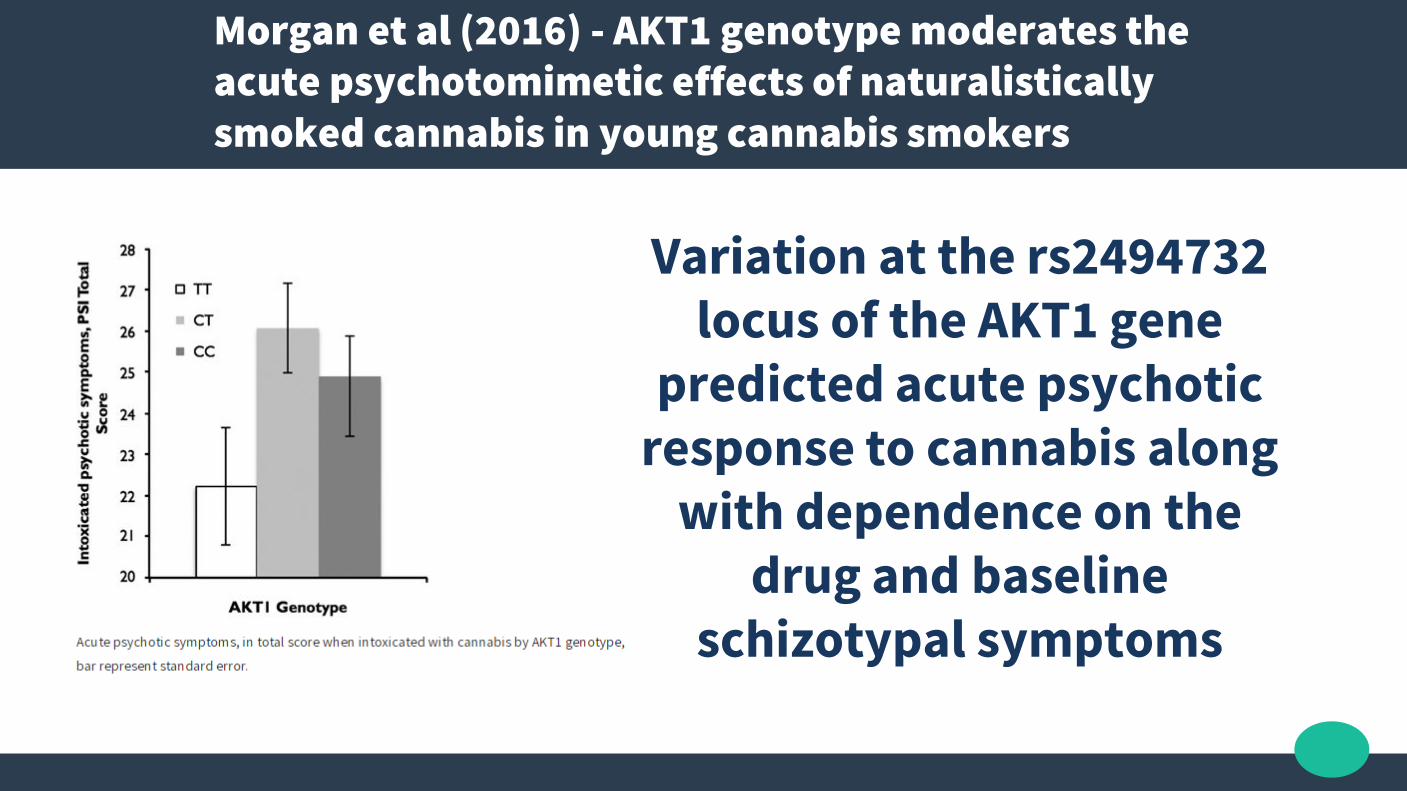
Morgan et al (2016) - AKT1 genotype moderates the acute psychotomimetic effects of naturalistically smoked cannabis in young cannabis smokers
Variation at the rs2494732 locus of the AKT1 gene
predicted acute psychotic response to cannabis along
with dependence on the drug and baseline
schizotypal symptoms

Wang et al, 2017 - Adverse effects of medical cannabinoids: a systematic review (THC)
● 23 randomized controlled trials and 8 observational studies of medicinal cannabis− 96.6% of side effects were not serious− Of the 164 serious adverse events, the most common was relapse
of multiple sclerosis (12.8%), vomiting (9.8%) and urinary tract infection (9.1%).
− The rate of non-serious adverse events was higher among participants assigned to medical cannabinoids than among controls (RR 1.86, 1.57-2.21 95% CI)
− The rates of serious adverse events did not differ significantly between these 2 groups (RR 1.04, 0.78-1.39 95% CI).
− Dizziness was the most commonly reported non-serious adverse event (15.5%) among people exposed to cannabinoids.
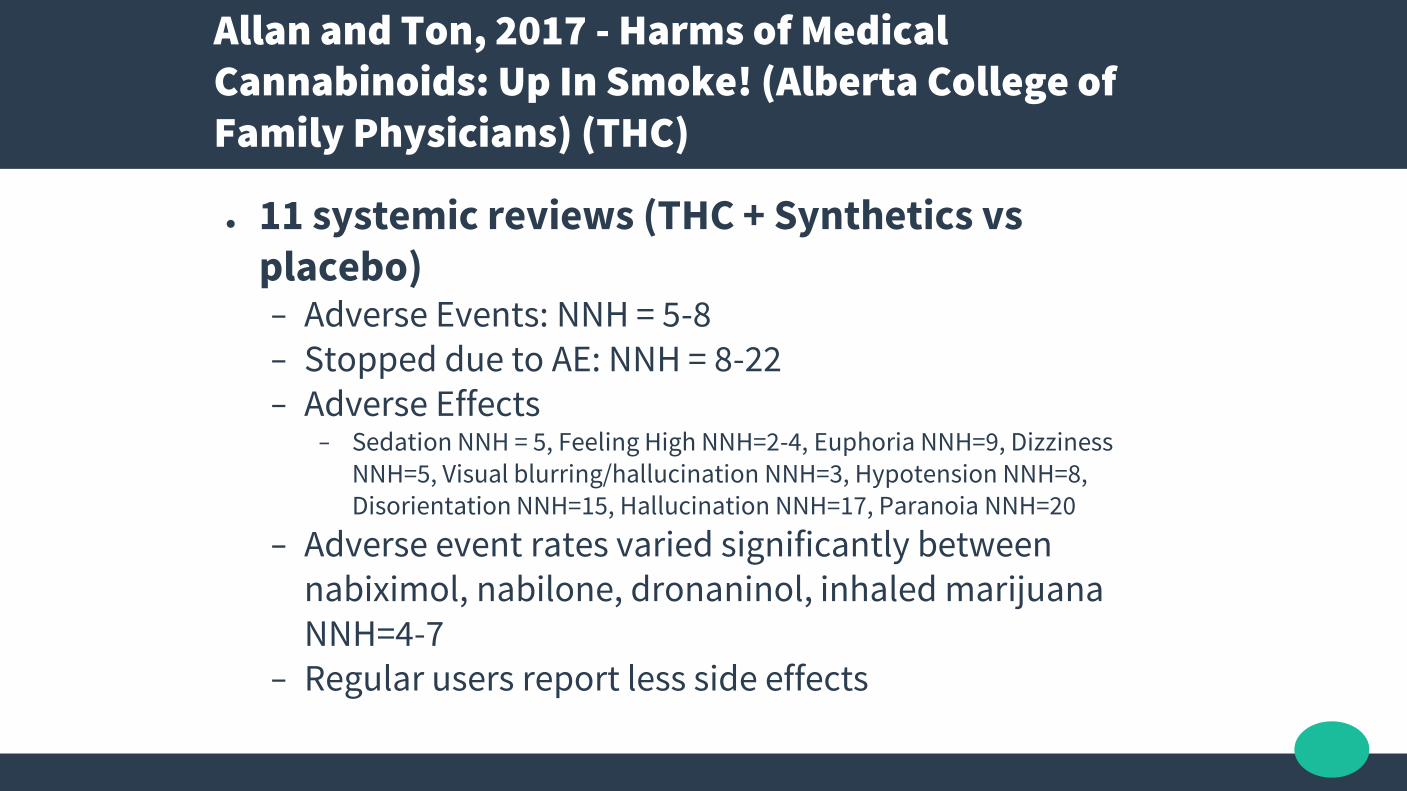
Allan and Ton, 2017 - Harms of Medical Cannabinoids: Up In Smoke! (Alberta College of Family Physicians) (THC)
● 11 systemic reviews (THC + Synthetics vs placebo)− Adverse Events: NNH = 5-8− Stopped due to AE: NNH = 8-22− Adverse Effects
− Sedation NNH = 5, Feeling High NNH=2-4, Euphoria NNH=9, Dizziness NNH=5, Visual blurring/hallucination NNH=3, Hypotension NNH=8, Disorientation NNH=15, Hallucination NNH=17, Paranoia NNH=20
− Adverse event rates varied significantly between nabiximol, nabilone, dronaninol, inhaled marijuana NNH=4-7
− Regular users report less side effects
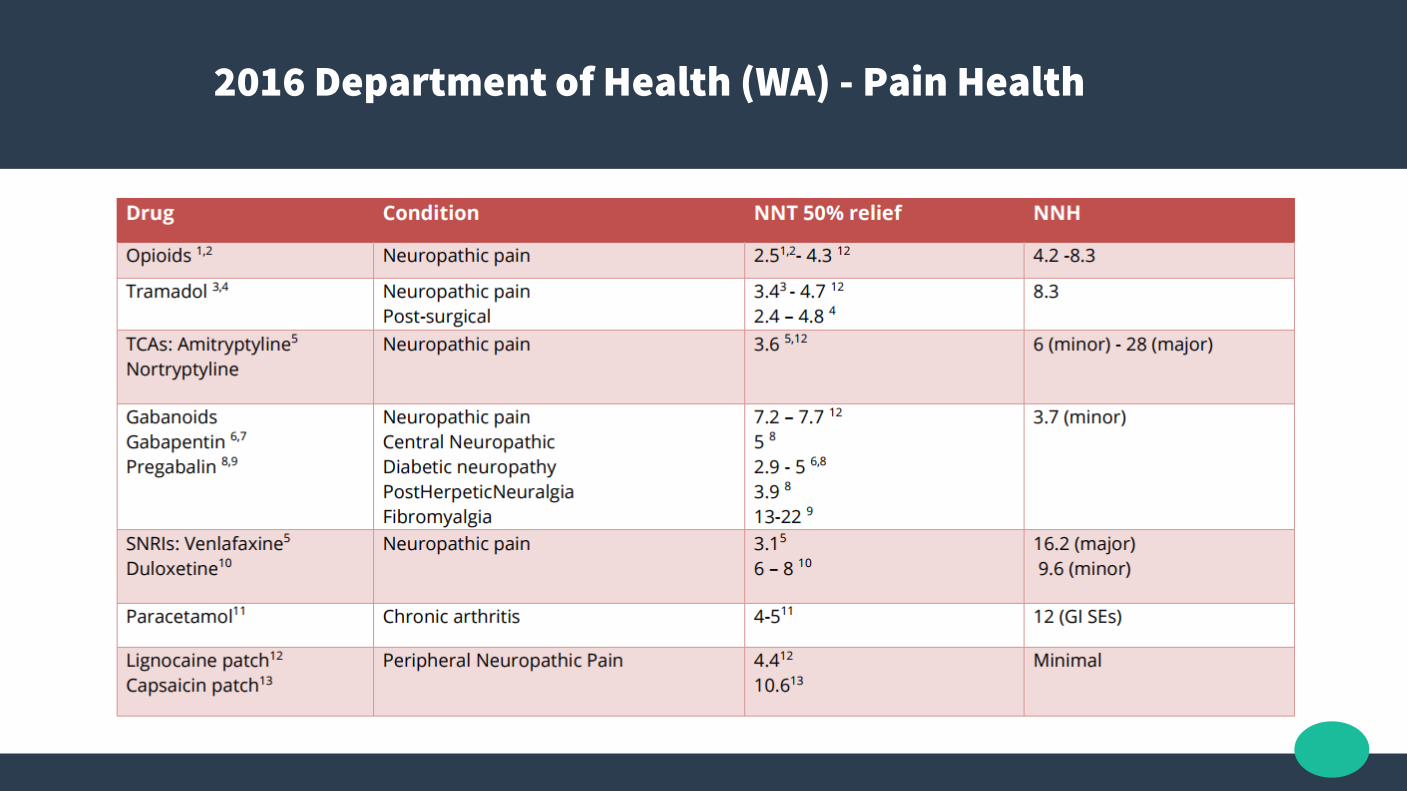
2016 Department of Health (WA) - Pain Health

Improved control and decreased access of cannabis to youth after legalisation measures – Colorado and Washington States
2014
legalisation

Braga et al, 2012 - Cognitive and clinical outcomes associated with cannabis use in patients with bipolar I disorder
● N=200● Those with Cannabis Use Disorder (CUD ) and Bipolar 1
had better neurocognitive performance
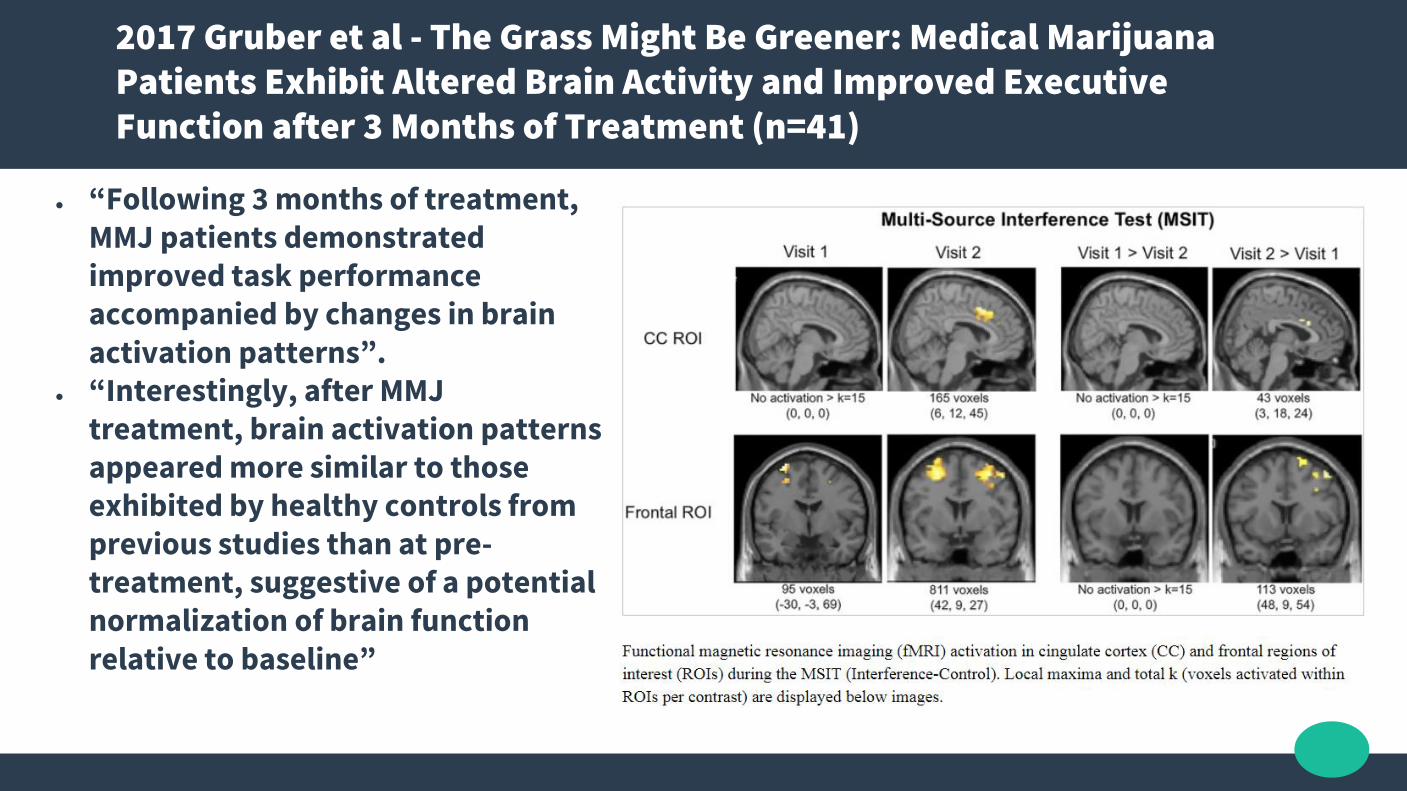
2017 Gruber et al - The Grass Might Be Greener: Medical Marijuana Patients Exhibit Altered Brain Activity and Improved Executive Function after 3 Months of Treatment (n=41)
● “Following 3 months of treatment, MMJ patients demonstrated improved task performance accompanied by changes in brain activation patterns”.
● “Interestingly, after MMJ treatment, brain activation patterns appeared more similar to those exhibited by healthy controls from previous studies than at pre-treatment, suggestive of a potential normalization of brain function relative to baseline”

Cannabis effects on driving lateral control with and without alcohol – Hartman et al, 2015

THC Therapeutic Evidence

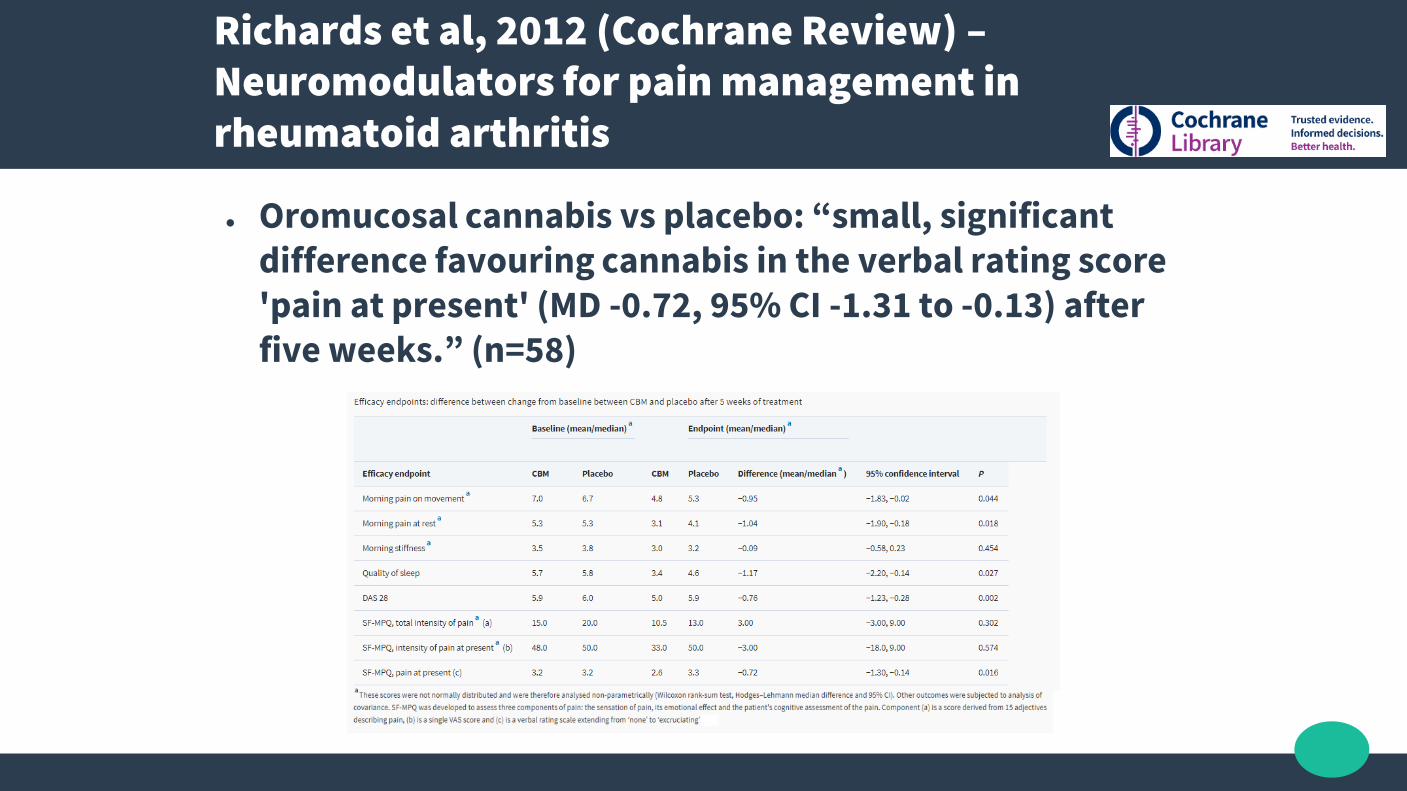
Richards et al, 2012 (Cochrane Review) –Neuromodulators for pain management in rheumatoid arthritis
● Oromucosal cannabis vs placebo: “small, significant difference favouring cannabis in the verbal rating score 'pain at present' (MD -0.72, 95% CI -1.31 to -0.13) after five weeks.” (n=58)

Prospective analysis of safety and efficacy of medical cannabis in large unselected population of patients with cancer –Schleider et al, 2018 (n=2970) > Pain intensity:

Prospective analysis of safety and efficacy of medical cannabis in large unselected population of patients with cancer –Schleider et al, 2018 (n=2970) > QOL assessment:
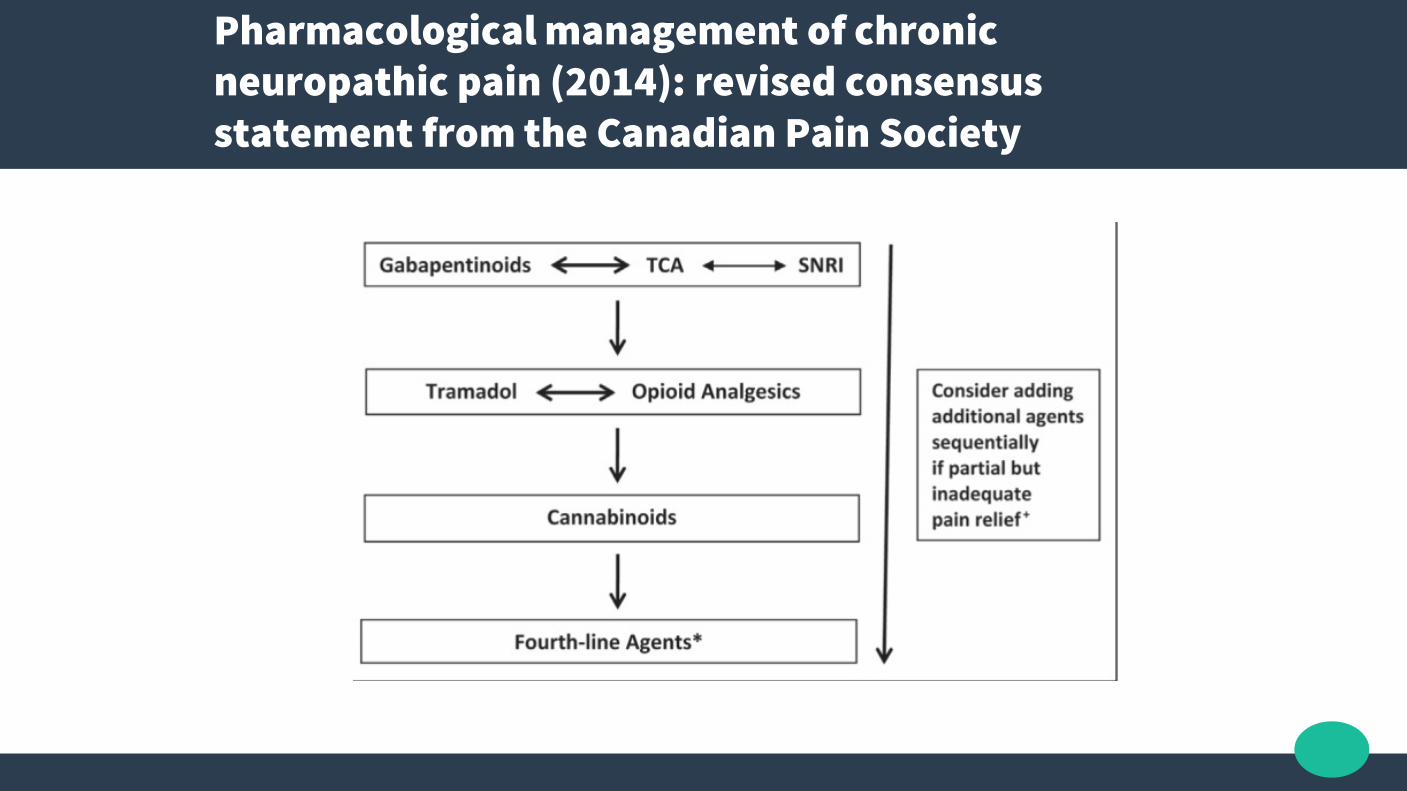
Pharmacological management of chronic neuropathic pain (2014): revised consensus statement from the Canadian Pain Society
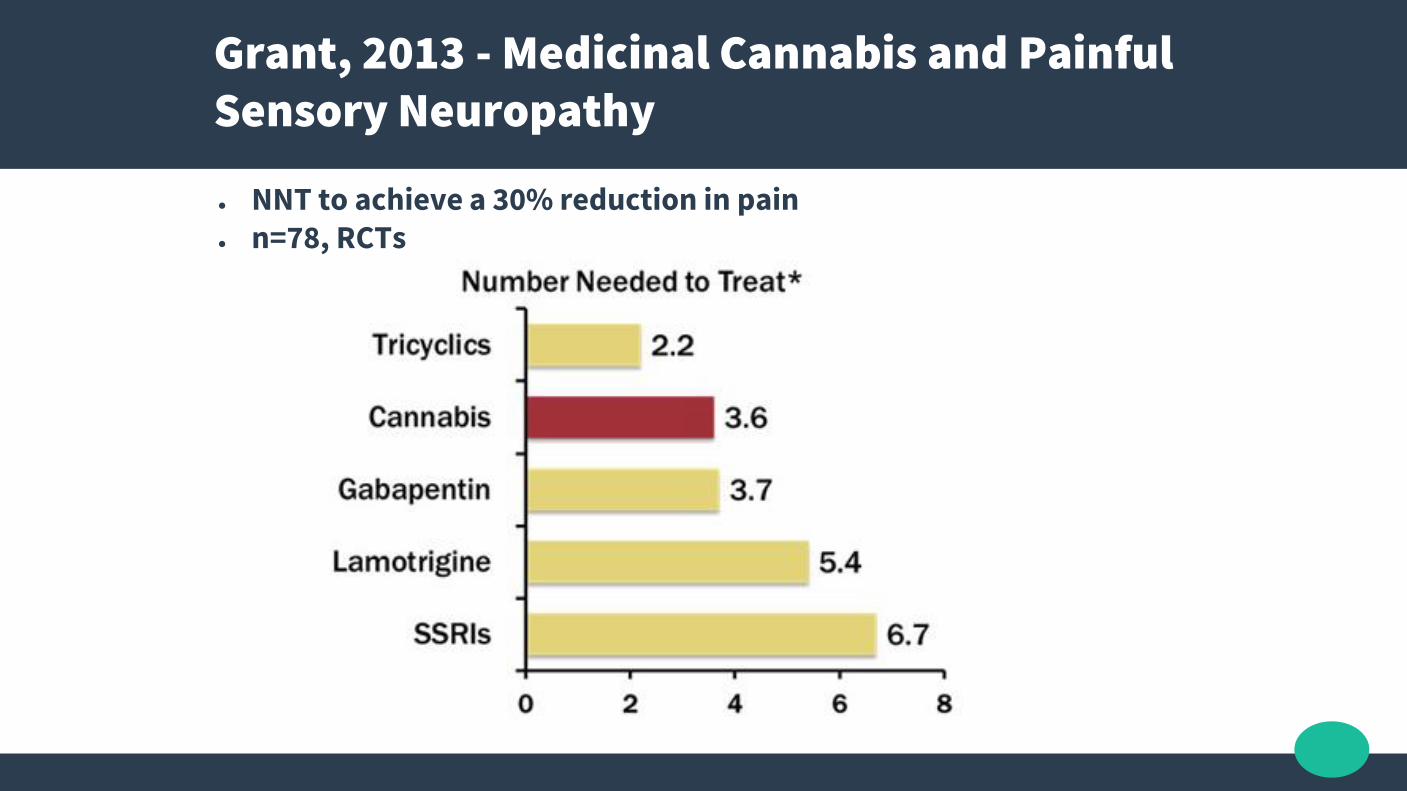
Grant, 2013 - Medicinal Cannabis and Painful Sensory Neuropathy
● NNT to achieve a 30% reduction in pain● n=78, RCTs

Bradford, 2015 – Medical Marijuana Laws Reduce Rx Medication Use In Medicare (Per Physician Per Year!)
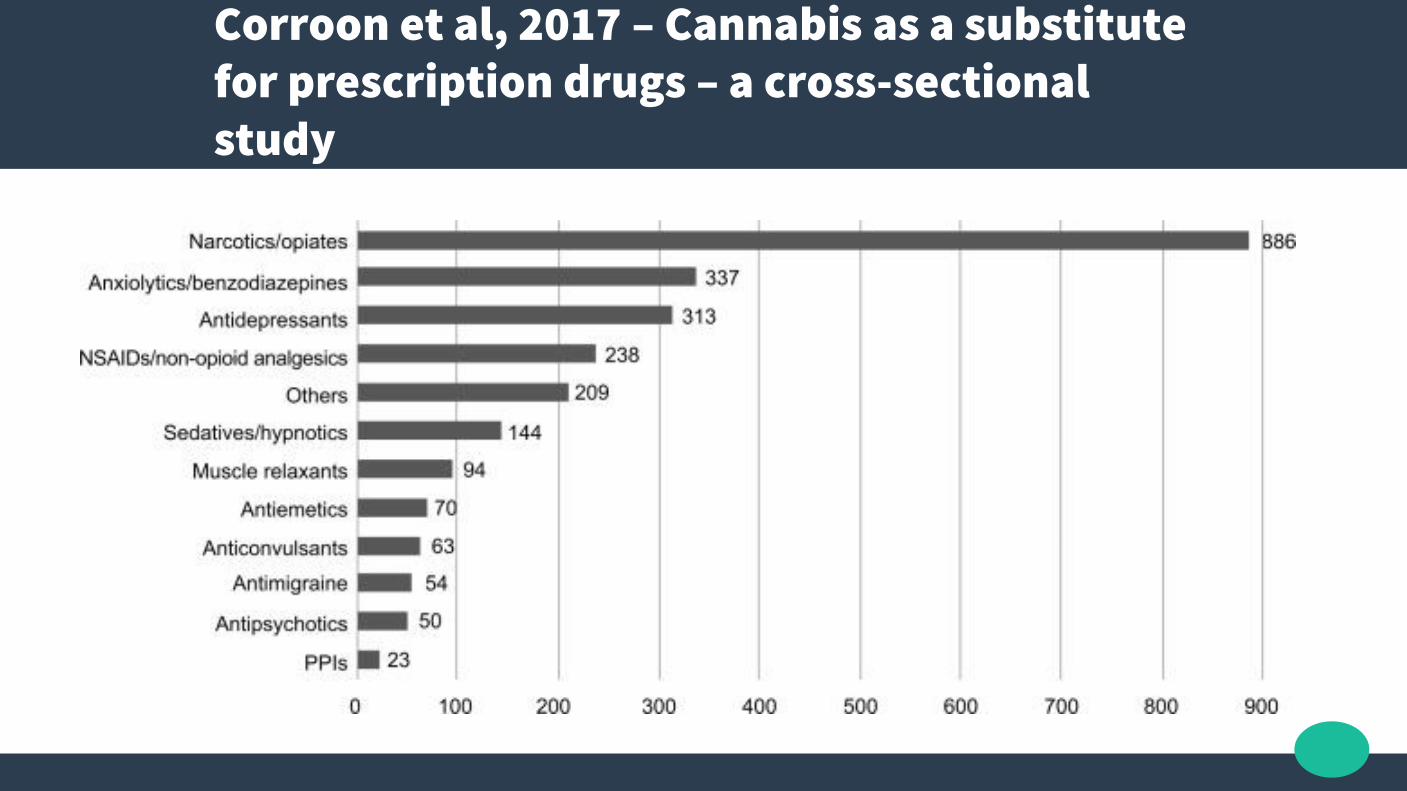
Corroon et al, 2017 – Cannabis as a substitute for prescription drugs – a cross-sectional study

2017 – GW Pharma Phase 2 THC + CBD for Recurrent Gliobastoma Multiforme
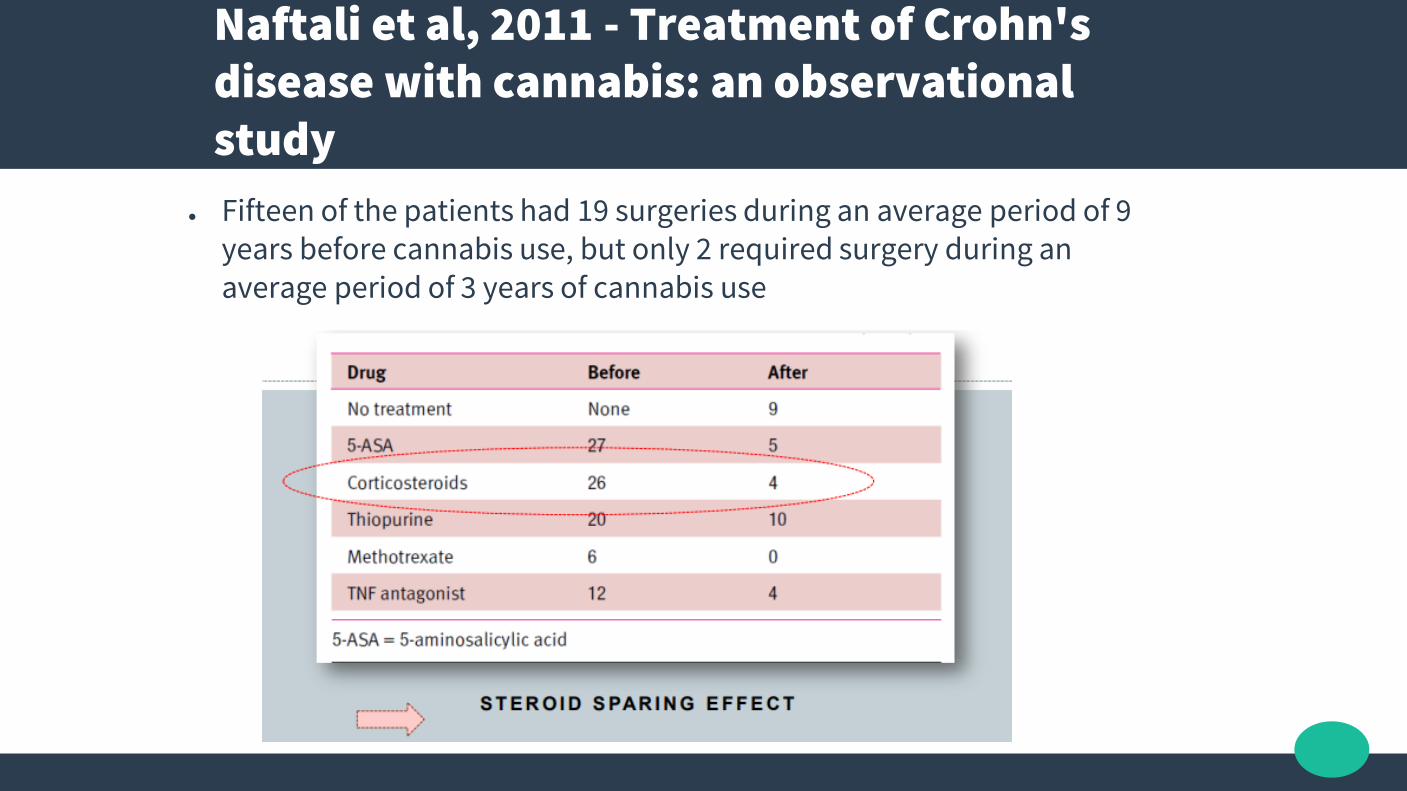
Naftali et al, 2011 - Treatment of Crohn's disease with cannabis: an observational study
● Fifteen of the patients had 19 surgeries during an average period of 9 years before cannabis use, but only 2 required surgery during an average period of 3 years of cannabis use
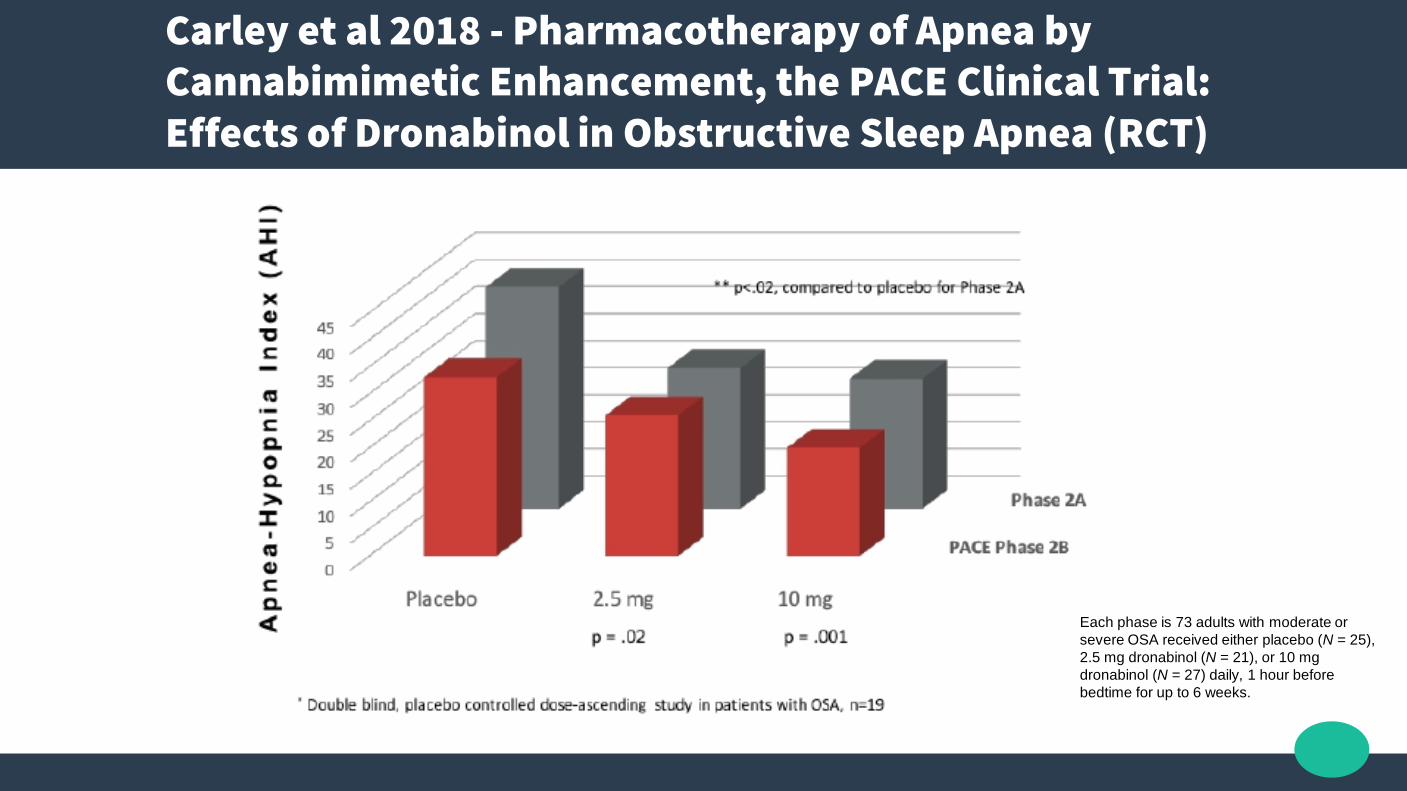
Carley et al 2018 - Pharmacotherapy of Apnea by Cannabimimetic Enhancement, the PACE Clinical Trial: Effects of Dronabinol in Obstructive Sleep Apnea (RCT)
Each phase is 73 adults with moderate or
severe OSA received either placebo (N = 25),
2.5 mg dronabinol (N = 21), or 10 mg
dronabinol (N = 27) daily, 1 hour before
bedtime for up to 6 weeks.
Rhyne et al, 2016 - Effects of Medical Marijuana on Migraine Headache Frequency in an Adult Population
● N=121, retrospective study● Migraine headache frequency on average decreased
from 10.4 to 4.6 headaches per month with cannabis medication use
● Vapourised or smoked cannabis use by some patients to abort migraines.
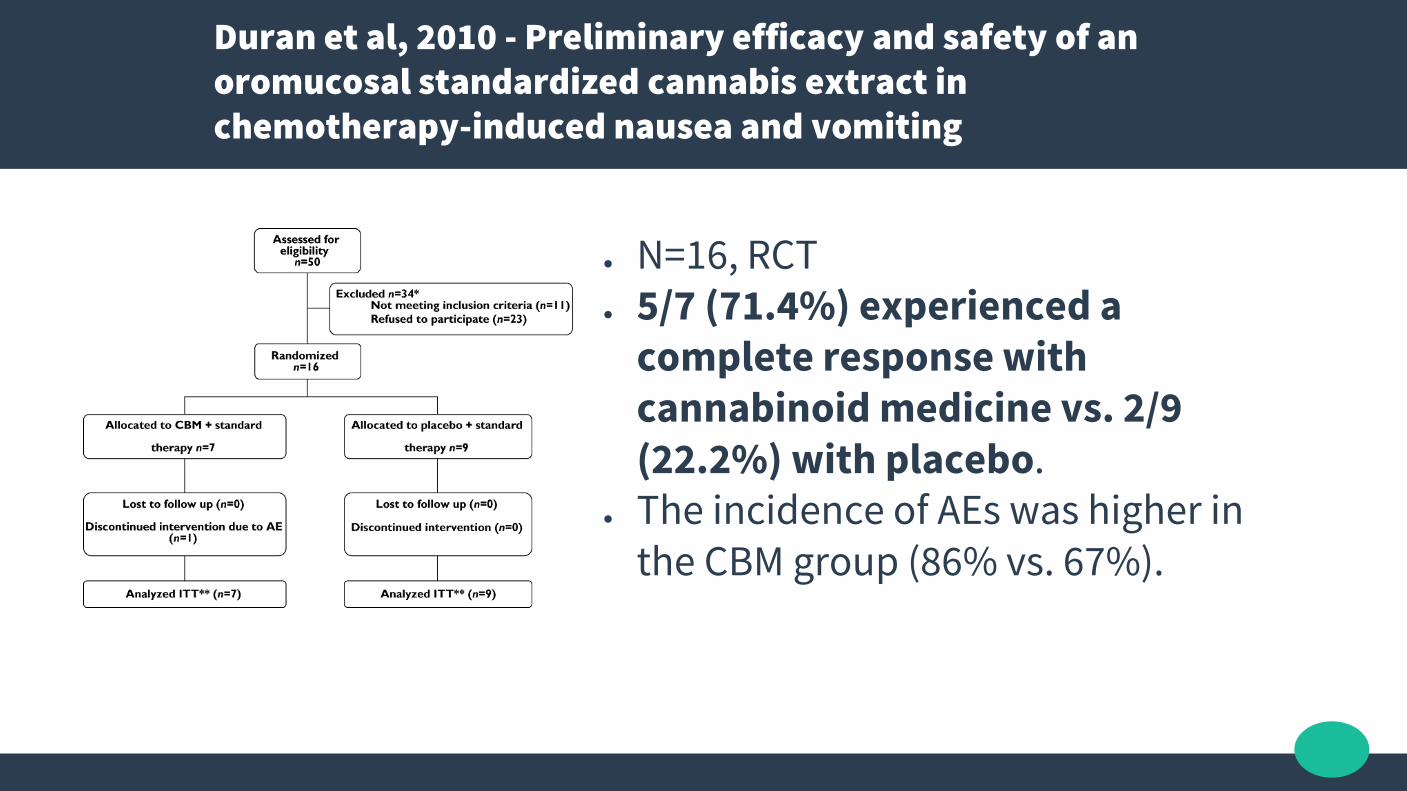
Duran et al, 2010 - Preliminary efficacy and safety of an oromucosal standardized cannabis extract in chemotherapy-induced nausea and vomiting
● N=16, RCT● 5/7 (71.4%) experienced a
complete response with cannabinoid medicine vs. 2/9 (22.2%) with placebo.
● The incidence of AEs was higher in the CBM group (86% vs. 67%).

Smith et al, 2015 (Cochrane Database) - Cannabinoids for nausea and vomiting in adults with cancer receiving chemotherapy
● 23 RCTs, cannabis-based medication with either placebo or with a conventional anti-emetic in adults
● Vs Placebo complete absence of vomiting RR 5.7; 95% CI 2.6 to 12.6
● Vs Prochlorperazine – equivalence or better● no nausea (5 trials; 258 participants; RR 1.5; 95% CI 0.67 to 3.2)● no vomiting (4 trials; 209 participants; RR 1.11; 95% CI 0.86 to 1.44)● complete absence of nausea and vomiting (4 trials; 414 participants; RR 2.0;
95% CI 0.74 to 5.4)● preference for cannabinoids (7 trials; 695 participants; RR 3.3; 95% CI 2.2 to 4.8)
● “Comparisons with metoclopramide, domperidone and chlorpromazine, there was weaker evidence, based on fewer trials and participants”
Adejumo et al, 2015 - Cannabis use is associated with reduced prevalence of progressive stages of alcoholic liver disease
● N=319,514. Analysis of 2014 Healthcare Cost and Utilization Project - Nationwide Inpatient Sample (NIS) discharge records of patients 18years and older, who had a past or current history of abusive alcohol use.
● Three cannabis exposure groups: non-cannabis-users (90.39%), non-dependent-cannabis-users (8.26%) and dependent cannabis users (1.36%).
● Cannabis users (dependent and non-dependent cannabis use) showed significantly lower odds of developing: alcoholic steatosis = AOR: 0.55 (0.48-0.64), steatohepatitis = 0.57 (0.53-0.61), fibrosis/cirrhosis = 0.45 (0.43-0.48) and hepatocellular carcinoma 0.62 (0.51-0.76).
● Further, dependent users had significantly lower odds than non-dependent users for developing liver disease
Lotan et al, 2014 - Cannabis (medical marijuana) treatment for motor and non-motor symptoms of Parkinson disease: an open-label observational study
● Unified Parkinson Disease Rating Scale score improved significantly from 33.1 (13.8) at baseline to 23.2 (10.5) after cannabis consumption (t = 5.9; P < 0.001).
● Analysis of specific motor symptoms revealed significant improvement after treatment in
- tremor (P < 0.001)- rigidity (P = 0.004)- bradykinesia (P < 0.001)

Cannabis Products

Cannabis Devices
Cannabis Devices
Cannabis Devices

Further Information
www.cannabis-med.org/studies/study
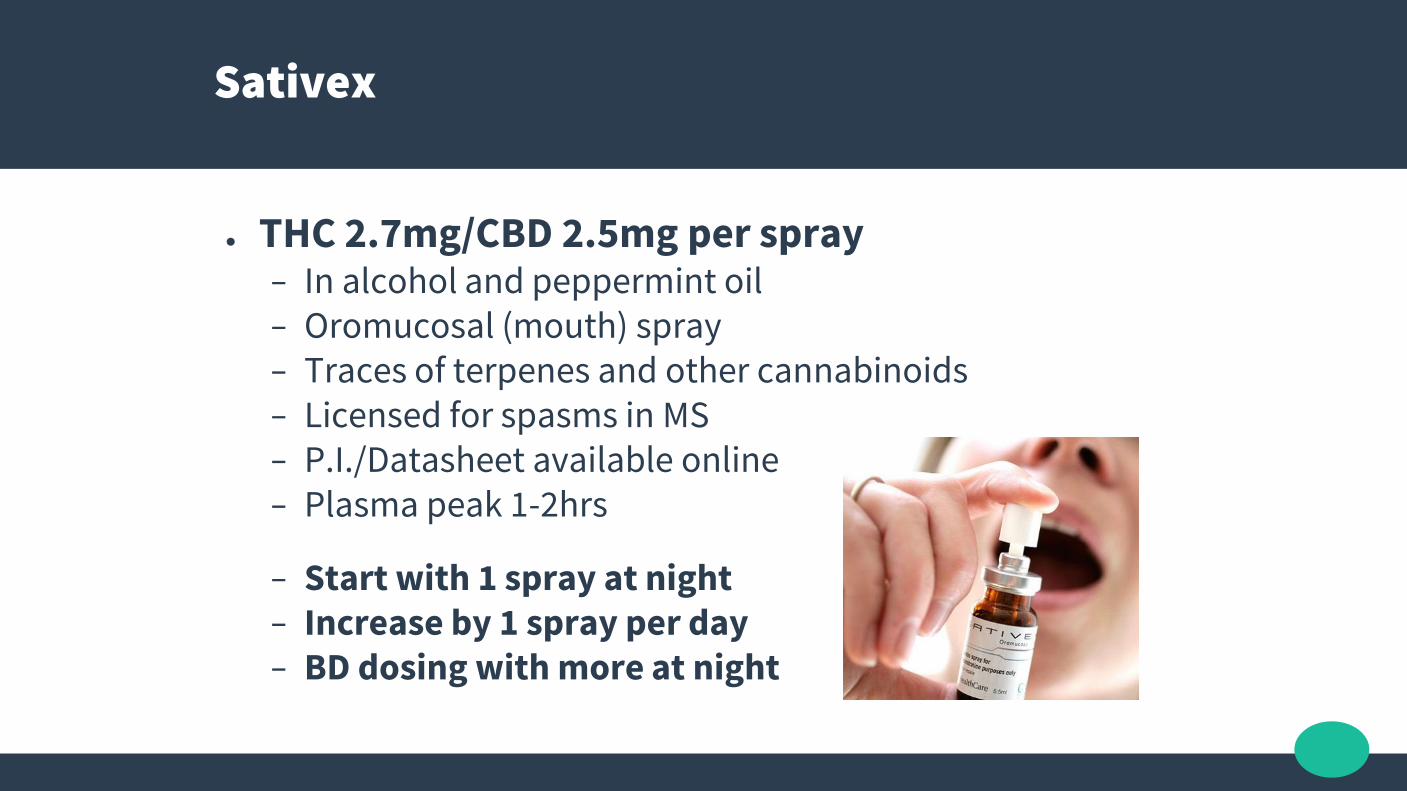
Sativex
● THC 2.7mg/CBD 2.5mg per spray− In alcohol and peppermint oil− Oromucosal (mouth) spray− Traces of terpenes and other cannabinoids− Licensed for spasms in MS− P.I./Datasheet available online− Plasma peak 1-2hrs
− Start with 1 spray at night− Increase by 1 spray per day− BD dosing with more at night
Cannabis Prescription
● Patient screening, education and consent● THC:CBD ratio product selection● Government application
● Rx: CBD > THC/CBD- CBD 5mg BD PO- THC 1mg dose vape/2.5mg oral- Titrate both gradually to effect
● Monitor, Review, Report

Take Home Messages
● No direct mortality from cannabis use, ever.
● Medicinal Cannabis does not need to get the patient “high”
● CBD, among other cannabinoids, modulate THC effects
● Start low and titrate dose to effect: THC 1mg, CBD 5mg BD PO
● Monitor co-administered drug levels or end organ function if required
● The non-psychoactive oral natural raw acid forms of the cannabinoids are being used for CB2 reception modulation and preventing oxidative stress (among other effects)