medrech issn no. 2394-3971 type 2 diabetes with... · face, and hirsutism (3). ... tsh 0.61...
TRANSCRIPT

Downloaded from www.medrech.com
“Type 2 diabetes with recurrent osteoporotic fractures, or Cushing’s syndrome?”
Dyrmishi B. et al., Med. Res. Chron., 2016, 3 (1), 110-114
Med
ico R
esearc
h C
hro
nic
les, 2016
110
Submitted on: February 2016 Accepted on: February 2016 For Correspondence Email ID:
TYPE 2 DIABETES WITH RECURRENT OSTEOPOROTIC FRACTUR ES, OR CUSHING’S SYNDROME?
Blertina Dyrmishi¹*; Taulant Olldashi²; Prof Asc Th anas Fureraj3; Prof Asc Majlinda Ikonomi 4; Dorina Ylli 5; Prof Agron Ylli 6
1.Endocrinologist, department of Internal Medicine, Hygeia Hospital, Tirana, Albania, 2.Surgeon, Hygeia Hospital, Tirana, Albania, 3. Endocrinologist, UHC Mother Theresa, Tirana,
Albania, 4. Pathologist, Hygeia Hospital, Tirana, Albania, 5. Endocrinologist, UHC Mother Theresa, Tirana, Albania, 6. Endocrinologist, Head of Endocrine Department, UHC “Mother
Theresa” , Tirana, Albania
Original Research Article
Medrech ISSN No. 2394-3971
ABSTRACT: Aim: Presentation of a case with secondary osteoporosis and compressive fracture in Cushing’s syndrome. Clinical Case: A 41 years old male was admitted to our hospital with inability to move the legs, severe back pain, which started 6 months ago. The patient was bedridden for a month due to severe pain. He was under treatment for hepatitis B and had been for more than three years under treatment for diabetes. One year ago he was treated for deep venous thrombosis. Laboratory data: Loss of circadian rhythm of cortisol, increased free urinary cortisol level, lack of suppression of cortisol after 1 mg dexamethasone test. DXA: Osteoporosis. Spine x-Ray: recurrent osteoporotic compressive thoracic fracture. Abdominal MRI showed left adrenal nodular mass with dimensions 2.5 x 3.3 cm. The patient underwent surgery: Left adrenalectomy. 12 months after surgery the patient continuing the treatment with hydrocortisone, alendronate, calcium and vitamin D, normal values of blood glucose and blood pressure without treatment and in DXA an improvement of the bone density was noticed. Keywords: Cushing’s syndrome; secondary osteoporosis; osteoporotic compressive fracture Introduction: Cushing’s disease was first described in 1932 from the American neurosurgeon Harvey Cushing (1). The incidence of Cushing’s syndrome is not exact, because of the undiagnosed cases with slight hypercortisolemia and the lack of data about iatrogenic Cushing (1). Cushing’s syndrome is a serious condition associated with high rates of morbidity and mortality that result
from excessive levels of systemic glucocorticoids (2). Cushing’s syndrome is associated with increased risks of cardiovascular, metabolic, and respiratory disorders, psychiatric complication, osteoporosis and infection, which all lead to increased rates of morbidity and mortality (2). The classic features of Cushing’s syndrome include central obesity, moon face, and hirsutism (3). Cushing’s syndrome
Downloaded from www.medrech.com
“Type 2 diabetes with recurrent osteoporotic fractures, or Cushing’s syndrome?”
Dyrmishi B. et al., Med. Res. Chron., 2016, 3 (1), 110-114
Med
ico R
esearc
h C
hro
nic
les, 2016
111
is an important cause of secondary diabetes, hypertension, venous thromboembolism and osteoporosis (4). Patient with Cushing syndrome have a high incidence of osteoporotic fractures. 30-50% of patients experience fractures, particularity in the vertebral body. The prevalence of osteoporosis in patients with Cushing’s syndrome is 50% (5). CLINICAL CASE: A 41 years old male was admitted to our hospital with inability to move the legs,
severe back pain, which started 6 months ago, bedridden for a month due to severe pain. The upper and lower limbs were thin; he presented a “moon face”, high blood pressure and high glucose values. He had normal motor and sensor function of leg. He was under treatment for hepatitis B and had been for more than three years under treatment for diabetes. One year ago he was treated for deep venous thrombosis. The diagnosis of Cushing’s syndrome was suspected.
Laboratory data:
Table no 1: Laboratory data.
Variable On
Admission Normal range Sodium 142 136-145 mEq/L Potassium 4.4 3.5-5.1 mEq/L Phosphate 2.8 2.5-4.9 mg/dl Total calcium 8.6 8.5-10.1 mg/dl Chloride 105 98-107 mEq/L Magnesium 2.1 1.8-2.4 mg/dl ALT 68 14-59 U/L AST 29 15-37 U/L GGT 67 5-85 U/L ALP 165 50 -136 U/L BUN 32 15-39 mg/dl Creatinine 0.6 0.6-1. 1 mg/dl Glucose 190 70-106 mg/dl WBC 14.1 x 10 ³ 4.0-10 x 10³/l RBC 5.4 x 10⁶ 4.2-5.4 x 10⁶/l HBG 15.8 12-16 g/dl Eos 0% 0-5 % PLT 443 x 10³ 150 - 350 x 10³ TSH 0.61 0.35-4.78 mUi/ml Cortisol 8 :00 23.9 3.2-22 g/dl ACTH 12.4 10-60 pg/ml CLU 730 20.9 - 290 µg/24 h Chromogranin A 231 < 200 ng/ml Vitamin D 23 > 30 pg/ml PTH 25.4 10-65 pg/mL HbA1c 7% 4 -6 % HBsAg > 1000 <1
Downloaded from www.medrech.com
“Type 2 diabetes with recurrent osteoporotic fractures, or Cushing’s syndrome?”
Dyrmishi B. et al., Med. Res. Chron., 2016, 3 (1), 110-114
Med
ico R
esearc
h C
hro
nic
les, 2016
112
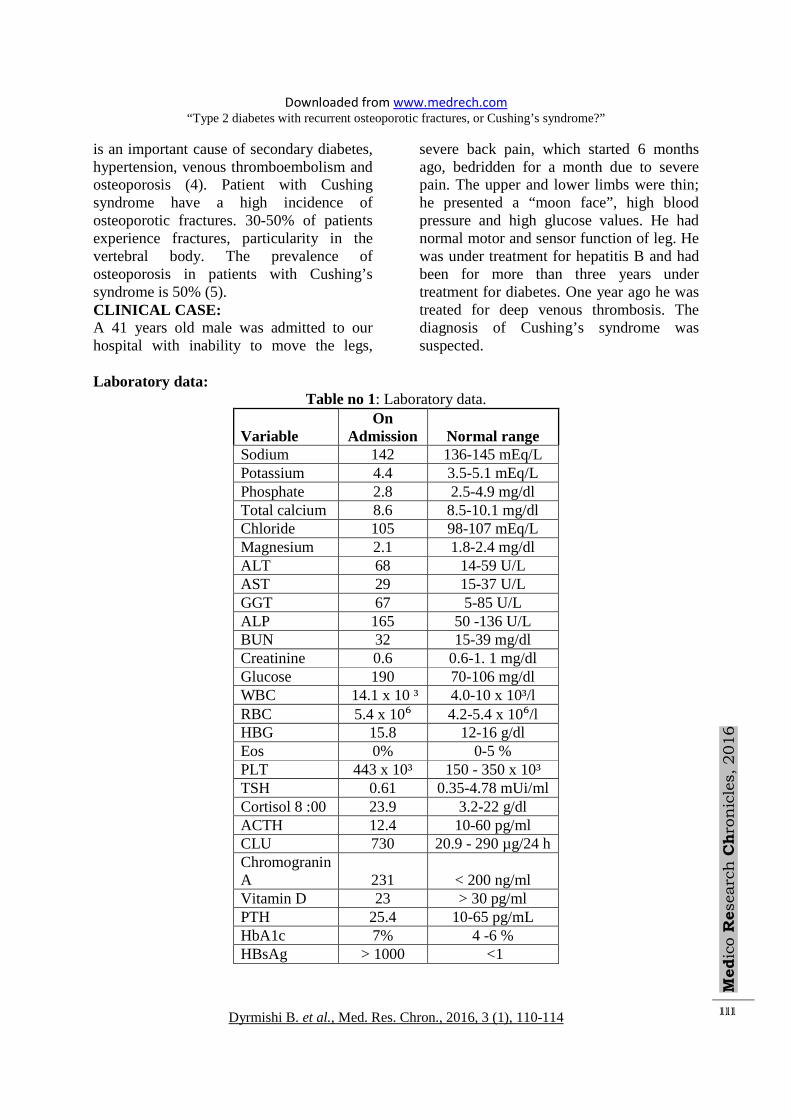
The laboratory examinations showed a loss of the circadian rhythm of cortisol, increased level of free urinary cortisol. A one mg over night dexamethasone suppression test was performed; the plasma cortisol was not suppressed and abdominal magnetic resonance imaging (MRI) was requested, it showed left adrenal nodular mass with dimensions 2.5 x 3.3 cm.
0
5
10
15
20
25
30
8:00 12:00 16:00 20:00 0:00 4:00
plasma cortisol values ng/dl
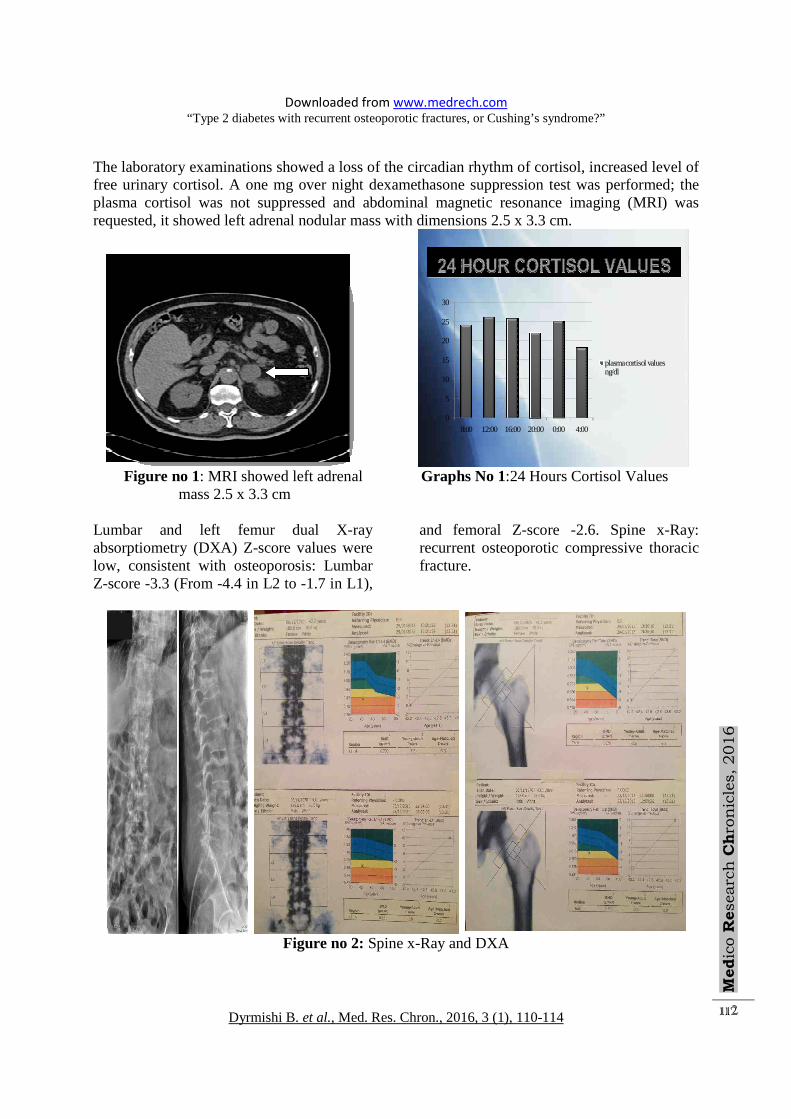
Figure no 1: MRI showed left adrenal Graphs No 1:24 Hours Cortisol Values mass 2.5 x 3.3 cm Lumbar and left femur dual X-ray absorptiometry (DXA) Z-score values were low, consistent with osteoporosis: Lumbar Z-score -3.3 (From -4.4 in L2 to -1.7 in L1),
and femoral Z-score -2.6. Spine x-Ray: recurrent osteoporotic compressive thoracic fracture.
Figure no 2: Spine x-Ray and DXA

Downloaded from www.medrech.com
“Type 2 diabetes with recurrent osteoporotic fractures, or Cushing’s syndrome?”
Dyrmishi B. et al., Med. Res. Chron., 2016, 3 (1), 110-114
Med
ico R
esearc
h C
hro
nic
les, 2016
113
Since the clinical, laboratory and image dates confirmed the diagnosis of Cushing’s syndrome, the patient underwent surgery, left adrenalectomy. Immune histopathological examination of adrenocortical adenoma confirmed the diagnosis of Cushing’s syndrome. The patient was treated with intravenous
hydrocortisone the first days after the surgery and after that with hydrocortisone 30 mg/day, calcium, vitamin D supplementation and alendronate for osteoporosis, since first line treatment of osteoporosis with teriparatide was not disponible at that moment.
Figure no 3: Microscopic image of adrenal adenoma Six month after surgery, the physical symptoms and signs of Cushing’s syndrome disappeared. Blood pressure and glucose values without treatment returned within the normal range. Rapid ACTH stimulation test was performed six months and twelve months after surgery. The test did not show changes of cortisol values 60 minutes after the 250 µg cosyntropin injection (cortisol 1.2 ng/dl before test, 1.0 ng/dl 30 minutes after test and 1.1 ng/dl 60 minutes after test). The patient continued the treatment with hydrocortisone, alendronate, calcium and vitamin D. 12 months after the treatment with bisphosphonates an improvement of the bone density was noticed. Discussions: Our case had the classical clinic appearance of Cushing’s syndrome with the occurrence of secondary diabetes, high blood pressure,
deep vein thrombosis and lately compressive fracture of the thoracic spine. The occurrence not at the same time of all the typical clinical signs makes the early diagnosing of Cushing’s syndrome often difficult (6). The physicians should take carefully the personal history of the patient and the signs occurred in different times must be connected with each other in order to make the right diagnosing. Our case had been under treatment for three years for diabetes mellitus, he had a history of deep vein thrombosis an year ago, but a Cushing’s syndrome was never suspected until he was admitted to our hospital with inability to move the legs, severe back pain. The prevalence of osteoporosis in patients with Cushing’s syndrome is 50% in some studies (5). Patient with Cushing’s syndrome have a high incidence of osteoporotic

Downloaded from www.medrech.com
“Type 2 diabetes with recurrent osteoporotic fractures, or Cushing’s syndrome?”
Dyrmishi B. et al., Med. Res. Chron., 2016, 3 (1), 110-114
Med
ico R
esearc
h C
hro
nic
les, 2016
114
fractures, where mainly the trabecular bones are affected. 30-50% of patients experience fracture, particularly in the vertebral body. Although the bone mineral density is improved after the treatment of Cushing’s syndrome, it preferred to start alongside the osteoporosis treatment. In our case the patient had also compressive fractures and in this case the chosen treatment would be teriparatide (8,9), but since its application was impossible, the treatment with bisphosphonate drug was started. Conclusions: The diagnosis of Cushing’s syndrome sometimes is difficult to suspect. Since osteoporosis and fractures occur frequently in Cushing’s syndrome, the diagnosis should be suspected in young patients and the treatment of Cushing’s syndrome is necessary. References: 1- Larsen, Kronenberg, Melmed, Polonsky.
Williams test book of endocrinology, 2003.pp 508-509.
2- Newell-Price J, Bertagna X, Grossman AB, Nieman LK. Cushing’s syndrome. Lancet 2006; 13(5); 367:1605-1617.
3- Nieman LK, Biller Mb, Findling JW et al. The diagnosis of Cushing’s syndrome: an Endocrine Society Clinical Practice Guidelines. J Clin Endocrinol Metab 2008: 93(5): 1526-1540.
4- Colao A, Petersenn S, Newell –Price J, et al. Pasireotide B2305 Study Group. A 12 – month phase 3 study of pasireotide in Cushing’s disease. N Engl J Med 2012; 366 (10): 914-924
5- Ju Young Han, Jungjin Lee et al. A case of Cushing Syndrome Diagnosed by Recurent Pathologic Fractures in a Young Woman. J Bone metab. 2012. 19 (2): 153-158.
6- Arnaldi G, Angeli A, Atkinson AB, et al. Diagnosis and complications of Cushing’s syndrome: a consensus statement. J Clin Endocrinol Metab 2003; 88 (12): 5593-5602.
7- Pereira RM, Carvalho JF, Paula AP, and al. Guidelies for the prevention and treatment of glucocortikoid-induced osteoporosis. Rev Bras Reumatol 2012; 52 (4): 580-593.
8- Rehman Q, Lang TF, Arnaud CD, et al. Daily treatment with parathyroid hormone is associate with an increase in vertebral cross-sectional area in postmenopausal women with glucocorticoid-induced osteoporosis. Int 2003; 14(1): 77-81.
9- Saag KG, Shane E, Boonen S, et al. Teriparatide or alendronate in glucocorticoid-induced osteoporosis. N Engl J Med 2007; 357: 2028-2039