medullary thyroid carcinoma metastatic to breast ... · pdf filemedullary thyroid carcinoma...
TRANSCRIPT

ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 24, No. 5Copyright © 1994, Institute for Clinical Science, Inc.
Medullary Thyroid Carcinoma Metastatic to Breast Masquerading as Infiltrating Lobular Carcinoma*SYED Z. ALI, SAUL TEICHBERG, Ph.D.,tJOSEPH N. ATTIE, M.D.§ and MYRON SUSIN, M.D.t
Division o f Surgical Pathology, Department o f Laboratories,tDepartment o f Pediatrics,t
and Department o f Surgery,§ North Shore University H ospital-
Com eli University Medical College, Manhasset, NY 11030
ABSTRACTMetastatic tumors to the breast from an extramammary site are rare enti
ties and may present diagnostic difficulties for the surgical pathologist because of frequent histological similarities to primary neoplasms in this location. A case is reported of medullary thyroid carcinoma metastatic to the breast in a 28-year-old woman with a family history of MEN IIA (Sip- ple’s) syndrome. Histological features resembled infiltrating lobular carcinoma and included the so-called “targetoid” and “Indian file” patterns. Immunostaining revealed the true nature of the lesion and was diffusely positive for calcitonin, chromogranin, and carcinoembryonic antigen. Electron microscopy disclosed typical neurosecretory granules confirming the diagnosis. A brief review of the literature and differential diagnosis is also presented.
IntroductionMetastatic tumors to the breast account
for 0 .8% to 6 .6% of all breast malignancies.1,2 In almost one-third of the cases, the metastatic focus represents the initial clinical presentation of an occult primary, usually a carcinoma,3 although more frequently it is a sign of widespread dissemination of the tumor.1 Metastatic carcinoma from the opposite breast is the
* Address reprint requests to: Myron Susin, M.D., North Shore University Hospital—Cornell University Medical College, 300 Community Drive, Manhasset, NY 11030.
commonest secondary tumor to the breast in females as opposed to hematopoietic tumors (lymphomas and leukemias) and prostate carcinoma which are the commonest metastatic tumors to the male breast.1,2,4 In addition to these, metastatic disease has been associated with malignant melanoma,1,5,6,7,8 lung carcinoma (oat cell type in particular),1,6,8,9 renal cell carcinoma, gastrointestinal carcinoma,5,6 thyroid (papillary and follicular carcinomas),6,10 carcinoids,11,12,13,14 ovarian carcinoma ,3,5,8,15 endom etrial carcinoma, pancreatic carcinom a ,5 as well as hepatoma and neuroblastoma.8 In children rhabdomyosarcoma,16 medullo-
4410091-7370/94/0900-0441 $01.20 © Institute for Clinical Science, Inc.

4 4 2 ALI, TEICHBERG, ATTIE, AND SUSIN
blastoma and glioblastoma17,18 have been reported. A case of metastatic medullary thyroid carcinoma to the breast diagnosed in fine needle aspirate has been reported ;19 to our knowledge, the current study is the first report of medullary thyroid carcinom a m etastatic to the breast with a description of histological, immunohistochemical, and ultrastruc- tural features.
Case ReportA 28-year-old female was admitted to North Shore
University Hospital for the evaluation and treatm ent of a right breast lump which was noted by her a few weeks prior to admission. Past medical history was significant for a diagnosis of MEN IIA (Sip- p le’s) syndrome and for m ultiple surgical procedures. In January, 1988, she presented with a thyroid lump and underw ent a total thyroidectomy for a multifocal and bilateral medullary thyroid carcinoma with positive right paratracheal lymph nodes. H er postoperative calcitonin dropped but never reached normal limits, and a month later she was readmitted for a palpable node in the right neck. She underw ent a right modified neck dissection w ith m etasta tic m edu llary carcinom a in n ine regional lymph nodes. Again her postoperative calcitonin levels remained elevated, and she was readm itted six months later. Although no nodes were felt at this time, she underw ent an elective left modified neck dissection again with positive lymph nodes. Her calcitonin level returned to normal post- operatively. Fam ily history was significant for MEN IIA syndrome in the patient’s father, sister, and daughter.
During the current admission in June, 1993, a sonogram of the breast showed a w ell circumscribed solid mass thought to be a fibroadenoma vs breast carcinoma. She underw ent a lumpectomy with removal of a 1 cm nodular mass. Frozen section showed a carcinoma with an infiltrating pattern. P ertinen t laboratory findings at that time included a mildly elevated calcitonin level. She had an uneventful postoperative recovery.
Materials and Methods L i g h t M ic r o s c o p y
Specimen was fixed in 10% neutral buffered formalin, embedded in paraffin, sectioned at 4 microns, and stained with hematoxylin and eosin.
IMMUNOHISTOCHEMISTRY
Sections were cut at 3 microns, depar- affinized in xylene, rehydra ted and quenched in methanol with 4% hydrogen peroxide for twenty minutes. Slides were incubated with primary antibody overnight at 4°C. L abelled avidin biotin method was used, and immunostaining was demonstrated with diaminobenzi- dine-hydrogen peroxide reaction and counterstained with Gill’s III hematoxylin. All antibodies were used with appropriate controls.
E l e c t r o n M i c r o s c o p y
Form alin-fixed paraffin em bedded tumor, in the breast, was rehydrated, post fixed in buffered 1% osmium tetroxide, buffered with 0.1 M cacodylate (pH 7.3), stained en bloc with uranyl acetate, dehydrated in a graded series of ethanols, and embedded in effapoxy resin. One micron plastic sections were stained with tolu- idine blue. Thin sections were stained with uranyl acetate and lead citrate and examined on a JOEL JEM 100 CXII electron microscope.
Results
M o r p h o l o g i c a n d I m m u n o h i s t o c h e m i c a l F i n d in g s
Grossly, the specimen was a tan-grey n odu le , w ell c ircu m scrib ed w ith a smooth pale white cut surface, and a maximum diameter of 1 cm. Light microscopic studies showed a well circumscribed tumor with a histologic pattern resem bling infiltrating lobular carcinoma. The predominant feature was the typical “ ta rg e to id ” or “ b u ll’s ey e” arrangement of small to interm ediate

MEDULLARY THYROID CARCINOMA METASTATIC TO BREAST 4 4 3
sized uniform cells with hyperchromatic nuclei and scanty amount of amphophilic cytoplasm. This pattern was characterized by the formation of the concentric rings around residual mammary ducts (figure 1).
In addition, the classical pattern of individual malignant cells arranged in single files or so called “Indian file” with intervening strands of thick collagenous stroma was also seen in areas (figure 2). Also noted were areas in which tumor cells formed distinct lobular structures as well as more solid nodules. No organoid architecture was noted, and none of the re s id u a l m am m ary ducts or lo b u les showed an in situ component. Spindle cells and extracellular amorphous material resembling amyloid were also absent from the lesion, and congo red stain was negative. Immunohistochemical studies were done (figure 3) and are summarized in table I.
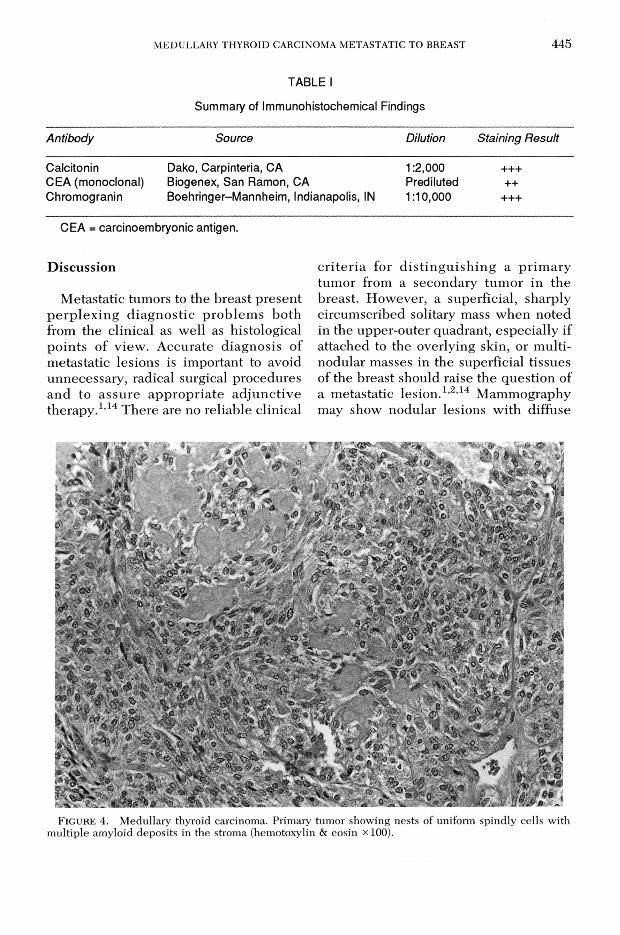
Sections from the thyroidectomy specimen with the primary medullary carcinom a w ere rev iew ed and show ed a variegated histological pattern consisting predominantly of nests of uniform angu- lated or spindly cells (figure 4) admixed with round or oval cells within a delicate fibrovascular stroma which, in places, c o n ta in e d m asses o f h o m o g en eo u s eosinophilic material which was strongly congophilic, consisten t w ith am yloid deposits. Multifocal capsular and vascular invasion were present.U l t r a s t r u c t u r a l F i n d i n g s
By electron microscopy, the cytoplasm of the tumor cells contained variable numbers of relatively small, round, dense core granules (figure 5). There was also a w ell deve lop ed , rough endo p lasm ic reticulum, clusters of intermediate filaments, and lysosomes.
FIGURE 1. M e d u lla ry th y ro id c a rc in o m a m e ta s ta t ic to b re a s t . A c e n tra l m a m m a ry d u c t is s u r r o u n d e d c irc u m fe r e n t ia l ly b y in te r m e d ia te s iz e d tu m o r c e l ls g iv in g a ‘t a rg e to id ’ a p p e a ra n c e (h e m o to x y lin & e o s in xlOO).

444 ALI, TEICHBERG, ATTIE, AND SUSIN
FIGURE 2. Medullary thyroid carcinoma metastatic to breast. Collagenous mammary stroma with columns of tumor cells forming ‘Indian files’ (hemotoxylin & eosin x200).
F i g u r e 3. Medullary thyroid carcinoma metastatic to breast. Tumor cells with strong immunostaining for calcitonin. A mammary duct with negative staining is seen at the top of the picture (calcitonin X200).
MEDULLARY THYROID CARCINOMA METASTATIC TO BREAST 4 4 5
TABLE I
Summary of Immunohistochemical Findings
Antibody Source Dilution Staining Result
Calcitonin Dako, Carpinteria, CA 1:2,000 +++CEA (monoclonal) Biogenex, San Ramon, CA Prediluted ++Chromogranin Boehringer-Mannheim, Indianapolis, IN 1:10,000 +++
CEA = carcinoembryonic antigen.
DiscussionM etastatic tumors to the breast present
p erp le x in g d ia g n o stic p rob lem s both from the clin ical as w ell as h istological p oin ts o f v iew . A ccurate d iagn osis o f m etastatic lesions is important to avoid unnecessary, radical surgical procedures and to assu re appropriate ad ju n ctive therapy.1,14 There are no reliable clinical
criteria for d is t in g u ish in g a prim ary tumor from a secondary tum or in the breast. H ow ever, a superficial, sharply circum scribed solitary mass w h en noted in the upper-outer quadrant, esp ecia lly if attached to the overlying skin, or multi- nodular m asses in the superficial tissues o f the breast should raise the question of a m etastatic le s io n .1,2,14 M ammography may show nodular lesions w ith diffuse
F i g u r e 4 . M e d u lla ry th y ro id c a rc in o m a . P r im a ry tu m o r s h o w in g n e s ts o f u n ifo rm sp in d ly c e l ls w ith m u l t ip le a m y lo id d e p o s i ts in th e s tro m a (h e m o to x y lin & e o s in x 100).

4 4 6 ALI. TEICHBERG. ATTIE, AND SUSIN
F i g u r e 5. Electron micrograph of a portion of a metastatic tumor cell showing several round dense core granules (arrow). Nucleus is at N. Bar equals 1 micron x 28,500.
thickening o f the skin15 and absence of spiculations or m icrocalcification.3 H istological features w hich may b e suggestive o f metastatic d isease include a periductal or perilobular distribution in the absence o f any in s itu ductal or lobular com ponent. There is m inim al elastosis and des- m oplasia associated with these lesion s.4 F in a l co n firm a tio n u su a lly req u ires im m u n o h isto ch em ica l and ultrastruc- tural studies to establish the d iagnosis o f metastasis.
F ine n eed le aspiration b iopsy can also play an important role in identify ing a su sp ected m etastatic n eop lasm in the breast. E specia lly w hen com bined with im m u n ocytoch em istry , th e sen s it iv ity
and diagnostic capability o f this process is further enhanced and is extrem ely u seful in d ifferentiating secondary m alignancies o f the organ.8,19
The current case report exem p lifies som e of these difficulties because o f the h isto lo g ic sim ilarity o f the m etastatic medullary thyroid carcinoma to a primary infiltrating lobular carcinoma o f the breast, ow in g to a p rom inen t p erid u cta l and perilobular distribution o f the neoplastic cells. W hen faced with such a situation at the tim e o f intraoperative consultation, it is prudent to defer the final diagnosis, aw aitin g the resu lts o f im m u n oh isto chem ical or ultrastructural studies. The n eed for good com m unication b etw een the surgeon and the surgical pathologist in these cases cannot be over-emphasized.
Most o f the metastatic tumors in breast have been described in younger or mid- dle-aged w om en, perhaps b ecau se the better b lood supply in this age group encourages blood-borne m etastasis, the most frequent m ode o f cancer spread to this organ.9 Overall prognosis o f these ca ses is u su a lly grave w ith ap p rox imately 90% of the patients dying within
AcknowledgmentOur gratitude is expressed to Gladys Seiden for
her excellent secretarial assistance.
References1. Hajdu SI, Urban JA. Cancers metastatic to the
breast. Cancer 1972;29:1691-6.2. Toombs BD, Kalisher L. Metastatic disease to
the breast. C linical, pathologic and radio- graphic features. Am J Radiol 1977;129:673-6.
3. McCrea ES, Johnson C, Haney DJ. Metastases to the breast. Am J Radiol 1983;141:685-90.
4. Azzopardi JG. Problems in breast pathology. In: Bennington JL. Major problems in pathology, vol II. Philadelphia, WB Saunders Co 1979; 311-4.
5. DiBonito L, Luchi M, Giarelli L, Falconieri G, Viehl P. Metastatic tumors to the female breast. An autopsy study of twelve cases. Pathol Res Pract 1991;187:432-6.
6. Nielsen M, Andersen JA, Henriksen FW, et al. Metastases to the breast from extramammary
MEDULLARY THYROID CARCINOMA METASTATIC TO BREAST 4 4 7carcinomas. Acta Pathol Microbiol Scand 1981; 89:251-6.
7. Pressm an PI. M alignant melanoma and the breast. Cancer 1973;23:784-8.
8 . Silverman JF, Feldm an PS, Covell JL, Frable WJ. Fine needle aspiration cytology of neoplasms m etastatic to the breast. Acta Cytol 1987;31:291-300.
9. Deeley TJ. Secondary deposits in the breast. Br J Cancer 1965;19:738-43.
10. Chisholm RC, Chung EB, Tuckson W, Khan T, White JE. Follicular carcinoma of the thyroid with metastasis to the breast. J Natl Med Ass 1980;72:1101-4.
11. Chodoff H. Solitary breast metastasis from a carcinoid of the ileum. Am J Surg 1965;109:814-5.
12. Harrist TJ, Kalisher L. Breast metastasis: an unusual manifestation of a malignant carcinoid tumor. Cancer 1977;40:3102-6.
13. Hawley RR. A case of secondary carcinoid tumor in both breasts following excision of pri
mary carcinoid tumor of the duodenum. Br J Surg 1966;53:818-20.
14. W arner TFCS, Seo IS. Bronchial carcinoid appearing as a breast mass. Arch Pathol Lab Med 1980;104:531-4.
15. Paulus DD, L ibshitz HI. M etastasis to the breast. Radio Clin North Am 1982;20:561-8.
16. H ow arth CB, Caces JN, P ratt CB. B reast m etastases in children w ith rhabdom yosarcoma. Cancer 1980;46:2520-4.
17. Brutschin P, Culver GJ. Extracranial metastasis from medulloblastoma. Radiology 1973;107: 359-62.
18. Byepes MT, D’Angio GJ. Extracranial metastasis from central nervous tumors in children and adolescents. Radiology 1966;87:55-63.
19. Ordonez NG, Katz RL, Luna MA, Samaan NA. M edullary thyroid carcinoma m etastatic to breast diagnosed by fine need le aspiration biopsy. Diagn Cyto Pathol 1988;4:254-7.