meeting of the trust board of staffordshire … board papers... · stuart poynor sp chief executive...
TRANSCRIPT

Page 1 of 2
MEETING OF THE TRUST BOARD OF
STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST Wednesday 22 February 2017 at 09.30hrs to 13.00hrs
Brampton Room, Morston House, Newcastle under Lyme, Staffordshire
AGENDA Item Enc
V – verbal R - report
Description Time
1. V Welcome and Apologies David Pearson 09.30 2. V Questions from Members of the Public David Pearson 09.35 3. V Declarations of Interest David Pearson 09.40
4. R Minutes of the last Staffordshire and Stoke on Trent Partnership NHS Trust Board meeting held on 25 January 2017 and matters arising David Pearson
09.45
Living our values of Quality, People and Responsibility (QPR) 5. R Chief Executive Officer Report Stuart Poynor 10.00 6. V Patient Story 10.20
We put quality first (Q)
7. R Assurance Report – Chair of the Quality and Safety Committee Elizabeth Jarrett
10.50
8. R Safe Staffing report Rose Goodwin 10.55 9. R CQC Improvement Plan Rose Goodwin 11.05
Break We focus on people (P)
10. R Education, Learning and Development Strategy Julie Tanner/Claire Spencer 11.15 We take responsibility (R)
11. V Assurance Report – Chair of the Finance, Investment & Performance Committee Jane Gaddum
11.25
12. R Finance Report Jayne Deaville 11.30 13. R Integrated Performance Report Jayne Deaville 11.50 14. R Corporate Risk Register Rose Goodwin 12.10 15. R Well Led Framework Jenna Davies 12.30
16. V Any Other Business • Review of meeting and outcomes • Review of risks David Pearson
12.50
Date of Next Meeting: Wednesday 29 March 2017, Edric House, Rugeley, WS15 1UW

Page 2 of 2

Page 1 of 24
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS
TRUST BOARD
TO BE HELD ON: WEDNESDAY 22 FEBRUARY 2017
Subject: Minutes of the Staffordshire and Stoke on Trent Partnership NHS Public Trust Board Meeting on Wednesday 25 January 2017
Strategic Goal: (tick as applicable)
x We will provide high quality and safe services which provide an excellent experience and best possible outcomes
x We will work with users and carers to deliver integrated systems, simply and effectively
x Our organisation will develop and deliver sustainable, innovative services that support independence
x Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
x We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Mr David Pearson, Chairman
Recommendation: For Approval & Assurance
x For Discussion For Information
PURPOSE OF THE REPORT:
The unapproved draft minutes of the Staffordshire and Stoke on Trent Partnership NHS Trust Board meeting held on Wednesday 25 January 2017 are enclosed for review and approval.
INTER DEPENDENCIES: Legal and/or Risk The Trust Board reviews the outcomes of each meeting and
considers whether any risks should be referred to the Executive Risk Management Committee for review and reporting onto the Corporate Risk Register.
Clinical See content of Sub-Committee meeting minutes
Financial See content of Sub-Committee meeting minutes
HR See content of Sub-Committee meeting minutes
Staff and Trade Union involvement actions undertaken/planned
See content of Sub-Committee meeting minutes
Social Care See content of Sub-Committee meeting minutes
Patient & Public Involvement
The Patient/Staff story informs the Trust Board of any developments or improvements to the Services that we provide
Equality Impact See content of Sub-Committee meeting minutes

Page 2 of 24
Information exempt from Disclosure
This is a public document
Requirement for further review
Action arising from the Minutes are tracked and reviewed each month
RECOMMENDATIONS: The Trust Board is requested to appraise and approve the minutes of the Trust Board Meeting held on Wednesday 25 January 2017 and to review and discuss progress or further action for the outstanding actions.
Page 3 of 24
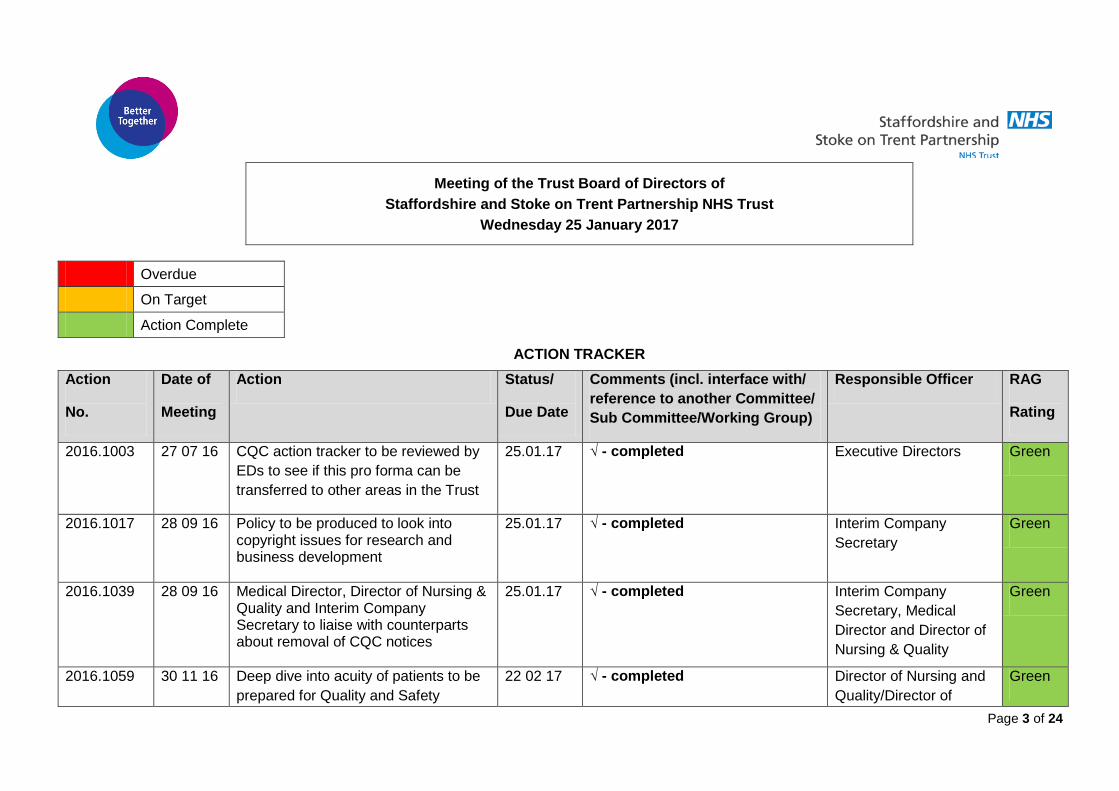
Meeting of the Trust Board of Directors of Staffordshire and Stoke on Trent Partnership NHS Trust
Wednesday 25 January 2017
Overdue
On Target
Action Complete
ACTION TRACKER
Action
No.
Date of
Meeting
Action Status/
Due Date
Comments (incl. interface with/ reference to another Committee/ Sub Committee/Working Group)
Responsible Officer RAG
Rating
2016.1003 27 07 16 CQC action tracker to be reviewed by EDs to see if this pro forma can be transferred to other areas in the Trust
25.01.17 √ - completed Executive Directors Green
2016.1017 28 09 16 Policy to be produced to look into copyright issues for research and business development
25.01.17 √ - completed Interim Company Secretary
Green
2016.1039 28 09 16 Medical Director, Director of Nursing & Quality and Interim Company Secretary to liaise with counterparts about removal of CQC notices
25.01.17 √ - completed Interim Company Secretary, Medical Director and Director of Nursing & Quality
Green
2016.1059 30 11 16 Deep dive into acuity of patients to be prepared for Quality and Safety
22 02 17 √ - completed
Director of Nursing and Quality/Director of
Green

Page 4 of 24
Action
No.
Date of
Meeting
Action Status/
Due Date
Comments (incl. interface with/ reference to another Committee/ Sub Committee/Working Group)
Responsible Officer RAG
Rating
Committee Operations
2016.1058 30 11 16 Medical Director to liaise with UHNM regarding the governance issues regarding the discharge process
25 01 17 √ - completed Medical Director Green
2016.1058 30 11 16 Patient story to be written up to enable learning within the Trust
22 02 17 √ - completed Associate Director of Communications
Green
2017.1084 25 01 17 Councillor Loades and the Acting Ambassador for Cultural Change and Freedom to Speak up Guardian to meet to discuss the role and her report.
22 02 17 √ - completed
Acting Ambassador for Cultural Change and Freedom to Speak up Guardian
Green

Page 5 of 24
Present: David Pearson DP Chairman Claire Bailey CB Acting Director – Strategy, Business & Redesign Gary Crowe GC Non-Executive Director Jenna Davies JD Interim Company Secretary (part) Jayne Deaville JDea Acting Director of Finance & Resources (part) Rosie Goodwin RG Director of Nursing & Quality Jane Gaddum JG Non-Executive Director Kieron Murphy KM Director of Operations Stuart Poynor SP Chief Executive Officer Simon Robson SR Director of Social Care (Interim) Dr John Scarpello JS Non-Executive Director Dr James Shipman JSh Medical Director Julie Tanner JkT Director of Workforce & Development Paul Weston PW Associate Non-Executive Director Apologies: Geraint Griffiths GG Deputy Chief Executive Elizabeth Jarrett EJ Non-Executive Director Andy Talbot AT Associate Non-Executive Director In attendance Nic Glover NG Executive Assistant to Chairman and CEO Jenny Harvey JH Staffside Representative David Loades DL Staffordshire County Council observer Clare Neill CN Associate Director of Communications 2017.1076 Welcome and Apologies
The Chairman welcomed Board Members, Staff Members and Members of the Public. Apologies were received from Geraint Griffiths, Elizabeth Jarrett and Andy Talbot. The Chairman informed Board Members that there had been an accident on the A50, so there may be a few members of the Trust Board who would be late. The Chairman welcomed Members of the Public to the Trust Board. The Chairman welcomed members of staff to the Trust Board.
MEETING OF THE TRUST BOARD OF STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST
Wednesday 25 January 2017 Brampton Room, Morston House, Newcastle under Lyme

Page 6 of 24
2017.1077 Questions from Members of the Public The Chairman invited questions from the members of the public, confirming that there would be a further opportunity at the end of the meeting to ask questions of the Board.
2017.1078 Declarations of Interest The Chairman asked if Trust Board Members had any declarations of interest to declare. Associate Non-Executive Director, Mr Weston declared he was the Chief Financial Officer for Housing and Care 21. The Medical Director declared he was a salaried GP within the local health economy. The Interim Director of Finance and Resources declared she was Director of Finance at South Staffordshire and Shropshire Foundation NHS Trust.
2017.1079 Minutes of the meeting and matters arising The Chairman referred Trust Board Members to the minutes of the Trust Board meeting held on 30 November 2016 and Board Members agreed the minutes as a correct records apart from the following changes: • Page 5 – “Acting Director of Finance” to be changed to “Interim Director of
Finance” • Page 9 – 2016.1059 – Ambassador for Cultural Change section, at the end of
that sentence should read “…wider health economy both regionally and nationally”.
• Page 19 – 2016.1065, first paragraph, addition to be added after “coding” “…down to “coding” (including IT and Estates).
• Page 19 – Mrs Gaddum would liaise with NG regarding the addition of specific points in the Assurance report for FIP
Board Members went through the action tracker and all were either on track or completed.
2017.1080 Chief Executive Officer Report The Chief Executive Officer presented his report to Board Members which highlighted a number of national and local items as follows: We put quality first • Urgent care pressures • Service User and Carer Experience • Launch of Celebrating Excellence People • Our stroke team is recognised • Award for Musculoskeletal Interface Service at the Haywood Hospital • Box of Trix • Improving patient care and reducing unplanned hospital admissions • Comments welcome on new strategy

Page 7 of 24
• First Deafblind awards Responsibility • Financial challenges • Quality improvement plan update • Four improvement projects launched • STP published • Becoming an antibiotic guardian • Box of Trix National • Chief Nurse calls for more care in the community • NHS England announces support for Type 2 diabetes • New quality framework published • Consultation on well-led assessment • NHS England announces £101 million of new funding for new care model
vanguards • New toolkit supports healthcare professionals to recruit more patients to
dementia research • Nursing apprenticeships announced The Chief Executive Officer informed Board Members that the local health economy was still in a challenging position and there were unacceptable waits for patients and poor performance for four hour waits in the local acute trust and much work had been undertaken in the local health economy between all trusts and agencies to ensure that this situation was remedied. The Chief Executive Officer informed Board Members that the Trust was taking forward a new discharge to assess programme which should improve flow and improve outcomes for patients. Non-Executive Director, Dr Scarpello asked for clarity around the assessment and length of stay process and the Chief Executive Officer and Director of Social Care responded to this point. Non-Executive Director, Mr Crowe congratulated the Trust on its work in this discharge to assess process. Medical Director, Dr Shipman also congratulated teams in the Trust on the discharge to assess process and thanked the whole health economy as all stakeholders needed to work together to ensure this process worked. Staffside Representative, Ms Harvey was concerned about the urgent care issues as services were being ceased such as alcohol dependency services and this would have further impact on the system. Staffside Representative, Ms Harvey was also concerned about the reduction in resources for the Lifestyle service and Councillor Loades responded by saying there was no resource reduction, however there would be efficiency of service savings. The Chief Executive Officer informed Board Members that the Trust had signed off its contracts with Commissioners and thanked the Interim Director of Finance, Mrs Deaville and her contracting team. The Chief Executive Officer informed Board Members that much work had been

Page 8 of 24
undertaken regarding the Trust’s financial position and the Trust had met with NHSI and financial plans would be signed off imminently. Non-Executive Director, Mrs Gaddum asked for an update on the financial position regarding Bradwell to do with the winter plan and the Chief Executive Officer and Interim Director of Finance both confirmed that any additional services regarding Bradwell would be financed by University Hospital of North Midlands. The Chief Executive Officer thanked the Director of Nursing and Governance and her team for all of their work on the Trust’s CQC action plan. The Chief Executive Officer informed Board Members that Staffordshire’s STP had now been published. The Chief Executive Officer asked Board Members to read the Word from last week regarding a member of staff’s testimonial on her working at the Trust, which was an exemplar on how induction for newly quality staff should be. The Chairman informed Board Members that he had attended the inaugural Deafblind Awards which had been a privilege. The Chairman noted the Nursing Apprentice Scheme and Councillor Loades noted that the Council would like to link into this work. Staffside Representative, Ms Harvey noted there needed to be further work on communications regarding the STP for staff and the Chief Executive Officer responded that a special workshop was being set up regarding this. The Trust Board noted the contents of the Chief Executive Officer report. The Chairman thanked the Chief Executive Officer for his report.
2017.1081 Patient Story The Chairman informed Board Members that there would be no patient story this month.
2017.1082 Assurance Report - Quality and Safety Committee Non-Executive Director, Dr Scarpello presented the Quality and Safety Committee Assurance report to Board Members informing them of the matters and business of the meeting of the Committee of the 11 January 2017. Non-Executive Director, Dr Scarpello informed Board Members that key points in the report are: • Quality Improvement Plan: the Committee received assurance on the Quality
Improvement Plan which now shows success measures. They were informed of a planned workshop with key leaders to reinforce the progress made to date and agree the method of on-going measurement of outcomes. The Committee recommended that Commissioners are appraised of the further developments and assurance mechanisms of the plan at the Clinical Quality Review Meeting.
• MCA/DOLS: The Committee was impressed by the completeness of the training programme developed and the high compliance rates.
• Pressure Ulcer Review: The Committee received an in-depth review concerning initiatives designed to reduce frequency of pressure ulcers. The number of avoidable ulcers occurring in patients under the care of the Trust remains a concern and further work is needed. It was recognised that many

Page 9 of 24
aetiological factors are outside Trust control, for example: smoking and prescription drugs. The Committee received assurance that further work would be undertaken which would involve an in depth review of grade 2 pressure ulcers and review of the risk assessment criteria.
• Procedural Register The Committee noted the procedural register and recommended that all the out of date policies are reviewed and updated by the end of March 2017.
The Trust Board received the assurance report of the Chair of the Quality & Safety Committee into the matters and business arising from the meeting of the Committee on the 11 January 2017. The Chairman thanked Dr Scarpello for his report.
2017.1083 Safe Staffing report The Director of Nursing and Quality presented the safe staffing report to Board Members which provided an overview of nurse staffing levels in the Community Hospitals operated by the Trust during both November and December 2016. The Director of Nursing and Quality informed Board Members that key points in the nurse staffing levels summary for November 2016 are. • Safe staffing has been maintained throughout November 2016. • Day time fill rate for RN’s – 95.8% and for HCSW – 105.1%. • Night time fill rate for RN’s – 99.5% and for HCSW – 104.8%. • CHPPD for November 2016 was 7.1 hours (RN – 3.2h and 3.9 h for care
workers). • With the exception of Broadfield Ward (1:9) all remaining wards are compliant
with RN to patient ratio parameters. • 8 shifts where professional concern raised (1.27%). • There were 3 shifts where there was only one registered nurse on duty. • Registered nurse vacancies remain high at 17.18WTE and for care workers
the figure has fallen slightly to 2.55WTE. The Director of Nursing and Quality informed Board Members that key points in the nurse staffing levels summary for December 2016 are: • Safe staffing has been maintained throughout December 2016. • Day time fill rate for RN’s – 93.0% and for HCSW – 100.5%. • Night time fill rate for RN’s – 99.4% and for HCSW – 104.8%. • CHPPD for December 2016 was 7.0 hours (RN – 3.1h and 3.9 h for care
workers). • Both Broadfield and Cottage wards report a RN to patient ratio of 1:9, whereas
the other wards lie within excepted parameters • 18 shifts where professional concern raised (2.76%). • There were 8 shifts where there was only one registered nurse on duty. • Registered nurse vacancies remain high at 18.3WTE and for care workers the
figure has increased slightly to 3.65WTE. The Chairman noted that there were some challenges and asked the Director of Nursing and Governance to give assurance to the Trust Board that staffing was at a safe standard within the Trust and the Director of Nursing and Governance confirmed that even though there were challenges, it was safe. The Chairman asked that then there was sub-optimal situations with staffing, if members of staff were thanked and supported and the Director of Nursing and Governance confirmed that they were.

Page 10 of 24
The Chief Executive Officer noted that the benchmarking for staff against other Trusts was in a very enviable position and the Trust met the Royal College of Nursing’s benchmark. Non-Executive Director, Dr Scarpello asked for clarity around the care hours v patient and the Director of Nursing and Governance informed Dr Scarpello that this was around national guidance. The Trust Board received the report for both November and December 2016 and were assured that the organisation is monitoring and mitigating issues relating to safe staffing establishments. The Chairman thanked the Director of Nursing and Quality for her report.
2017.1083 Assurance Report – Chair of the Workforce Matters Committee In the absence of Associate Non-Executive Director and Chair of the Workforce Matters Committee, Mr Talbot, Non-Executive Director, Mrs Gaddum gave a verbal report to Board Members and informed Board Members that the Workforce Matters Committee had discussed the following issues: • Agency and temporary staffing • Internal recruitment - Internal recruitment is on-going on a month by month
basis and regular attendance at Corporate Welcome Days also continues with the aim to recruit new Trust staff to the Bank
• Additional training for bank staff - Additional training being provided to ensure that all bank staff have a minimum set of Statutory & Mandatory Training in place before undertaking a shift.
• Reduction of agency spend - Work continues on the reduction of agency spend. Total spend to 31 December is £5.271m which is £1.837m below the NHSI agency ceiling.
• Talent pool - Feedback received from the Implementing Change Programme on a rapid improvement event that they completed relating to the “offer” that the Trust makes to staff in the talent pool as well as how the Trust uses these skills on projects and secondments. A proposal had been made that all recruiting managers need to liaise with the OD Team on who may be available in the pool ready for their next opportunity and that WMC reviews/evaluates how the recommendations from the IPC have been implemented in July 2017.
• The Trust is continuing with the procurement process to identify the best option for temporary staffing going forward since the current provider Talent (Neutral Vendor) has given notice to terminate the contract at the end of March 2017 as they are discontinuing their business in this area
• New Monthly Report developed for both WMC and FIP - overall spend is reducing with the monthly spend having reduced by circa £200k per month since the start of the financial year. Regular scrutiny taking place on every agency person in post – efforts being made to do without or to convert to fixed term contracts where possible.
• The Committee received a revised version of the proposed Education and Training Strategy for comment and approval. Agreed that this now needs to be translated into a “Strategy on a Page” outlining what this means for staff. Also WMC need to consider a dashboard to monitor progress against this strategy. It is proposed that the strategy is ratified by Trust Board in February.
• The Committee approved the Operational Guide for Using Bank and Agency Staff. This procedure had been a recommendation following the Agency Staffing Audit conducted in Autumn 2016.
• The Committee undertook a deep dive in to risk SO04- Failure to have

Page 11 of 24
appropriate leadership skills and capacity at all levels to deliver new ways of working and appropriate ways of leading.
• The Committee were assured that appropriate actions and initiatives were in place or underway (via the OD Strategy – coming to Trust Board today). However, close monitoring would take place to ensure that “green” areas did not decline over the coming months.
• The Committee will undertake a deep dive into the 2 further BAF risks in March 2017.
Non-Executive Director, Mr Crowe congratulated the Committee on the work that was being undertaken by them. The Trust Board received and noted the Report of the Workforce Matters Committee. The Chairman thanked Non-Executive Director, Mrs Gaddum for her report.
2017.1084 Raising Concerns Update The Acting Ambassador for Cultural Change and Freedom to Speak up Guardian, Mrs Powell presented the Raising Concerns Update to Board Members which provided an overview of Raising Concerns in the last quarter and to report on Trends and Themes. The Acting Ambassador for Cultural Change and Freedom to Speak up Guardian, Mrs Powell informed Board Members that key points in the report related to: • Activities undertaken to promote raising Concerns • Meeting with Cultural Change Champions • New Raising Concerns Policy on Intranet for Staff use • Raising Concerns training for Staff and Managers • Job Description revision • Trends and Themes identified across the Trust. The Director of Workforce and Development noted to Board Members that she had watched the raising concerns videos and they were excellent. Councillor Loades noted that the Freedom to Speak Up Guardian role was excellent and asked for further information on it and some of the points highlighted in the Acting Ambassador for Cultural Change and Freedom to Speak up Guardian’s report and Mrs Powell would meet with Councillor Loades outside of the meeting. The Chairman asked the Acting Ambassador for Cultural Change and Freedom to Speak up Guardian how the Trust benchmarked against other organisations and the Acting Ambassador for Cultural Change and Freedom to Speak up Guardian responded that this was one of the only trusts that had a whole dedicated person in this role and also had administrative support. The Trust Board noted the report and approved the raising concerns protocol. The Chairman thanked the Acting Ambassador for Cultural Change and Freedom to Speak up Guardian, Mrs Powell for her report and for her work to link into national and regional networks.
EP
2017.1085 Assurance Report – Finance, Investment & Performance Committee

Page 12 of 24
Non-Executive Director and Chair of the Finance, Investment& Performance Committee, Mrs Gaddum gave a verbal report to Board Members and informed Board Members that the Finance, Investment & Performance Committee had discussed the following issues: • Agency spend - a consistent report to FIP is required that will demonstrate grip
and give full visibility to the FIP committee. This is being developed for the next meeting and will reviewed monthly.
• Financial position - the financial position was noted, which indicated a continuation of the position reflected in the approved plan submitted to NHSI on 23 December 2017. Whilst the deficit position is not where FIP would like to be, FIP were assured that numbers remain unchanged from the forecast shared with NHSI, and the drivers for overspend are also unchanged, and clearly understood. FIP have yet to be assured on the financial sustainability towards 2017/18 and 2018/19 targets, but expect to review this assurance as detailed forward plans are shared at the February and March FIP Committee meetings. The following finance papers will be considered at future FIP meetings this financial year: • Further detail on the recovery plan to deliver 2016/17 financial position • Further detail around the delivery of future years savings required from
social care remodelling. • A paper providing the approach to budget setting for next year indicating
the cost improvements required of each division within the organisation. • Divisional CIP performance - the performance report was received and the 4
targets missed were discussed together with the results from the deep dives undertaken. • Social Care - Delayed Transfers of Care • Social Care - Proportion of clients receiving Direct Payments • 2 – 2.5 year review in Health Visiting • Breastfeeding at 6-8 week check
• Estates - the regular update report was received by the committee. It was agreed that the strategy for the management of estates together with a high level plan be brought to FIP as soon as possible
• Business development – The format of the report to be reviewed to better identify business opportunities, criteria to be applied for bids together with associated risks, success rate of winning tenders and performance of new tenders against the criteria to be delivered
• IM&T - the regular update report was received by the committee. It was agreed that the strategy for the management of IM&T together with a high level plan be brought to FIP as soon as possible
• Section 75 - This item was deferred to the next meeting as the director of social care was unable to attend
• Board Assurance Framework - Change required as Trust financial Performance is recommended to be merged with CIP achievement
Non-Executive Director, Dr Scarpello asked how medical agency spend was progressing and both Non-Executive Director, Mrs Gaddum and the Medical Director, Dr Shipman responded that there continued to be issues due to national shortage in the areas of rheumatology and geriatrics. The Trust Board received and noted the Report of the Chairman of the Committee. The Chairman thanked the Chair of the Finance, Investment & Performance Committee for her report.

Page 13 of 24
2017.1086 Assurance Report – Audit Committee Non-Executive Director and Chair of the Audit Committee, Mr Crowe gave a verbal report to Board Members and informed Board Members that the Audit Committee had discussed the following issues: • External audit • Internal audit reports • Well led framework • Board assurance framework The Trust Board received and noted the verbal report of the Chairman of the Committee. The Chairman thanked the Chair of the Audit Committee for his report.
2017.1087 Finance Report The Interim Director of Finance and Resources presented the Month 9 Finance Report to Board Members up to 31 December 2016. The Interim Director of Finance and Resources informed Board Members that the Trust is reporting an actual deficit of £21.868m at the end of Month 9 and the position is £16.270m in excess of the planned deficit of £5.598m. The Interim Director of Finance and Resources informed Board Members that the key variances against YTD plan is driven in the main by those key themes articulated to the Trust Board over the course of the financial year: • a deficit in Adult Social Care of £8.5m; • the YTD impact of £2.1m associated with the outcome of the national dispute
resolution process related to the North CCGs contract; • pump priming investment in relation to the MARS savings scheme (£1.3m)
impacting non-recurrently in June and December; • planned expectations (£2.0m in year) in relation to reducing the operating
deficit in relation to financially stressed services (primarily community hospitals) have not materialised to date.
The Interim Director of Finance and Resources informed Board Members the Trust has remained in close contact with the NHSI in relation to the spread of financial risk facing the Trust which was assessed at Quarter 1 of between £18.5m to £23.5m after financial recovery intervention. The Interim Director of Finance and Resources reminded Board Members that the report to the Trust Board at Quarter 2 raised serious concerns regarding the sustained “bottom line” trajectory, and the traction and achievability of financial recovery measures over the remainder of the year and a critical review and strengthening of financial recovery measures has taken place in light of performance at Quarter 2, together with an assessment of emerging pressures and financial recovery is now well established and remains a key priority and focus of the Executive Leadership Team and operational governance groups across the Trust. The Interim Director of Finance and Resources went on to say that the actions undertaken continue to support a forecast financial deficit of £21.8m for planning purposes and the final outcome will be heavily influenced by decisions in relation to “capital to revenue” funding transfer which is planned at £5m.
Page 14 of 24
The Chairman asked how embedded the plan was within the organisation and the Interim Director of Finance and Resources responded that she was very confident that in the current financial year that the Trust would meet its target, with the proviso of the capital to revenue transfer. The Interim Director of Finance and Resources did say that detailed plans were being worked up in the next few months to ensure that the Trust hit the ground running from April for the next financial year. Councillor Loades asked for clarity around the income to expenditure figures and the Interim Director of Finance and Resources responded that a plan was now in place to recover the position. The Trust Board received and noted the financial performance of the Trust at 31 December 2016 (Month 9) and reinforced the requirement for sustained action and scrutiny by the Executive Team. The Chairman thanked the Interim Director of Finance and Resources for her report.
2017.1089 Integrated Performance Report The Interim Director of Finance and Resources presented the Integrated Performance Report to Board Members to provide a concise integrated view of performance across the organisation for December 2016, which provided a summary of performance including Quality, Operational, Finance and Workforce indicators, incorporating trends and benchmarks where appropriate in line with the performance framework that has been adopted by the Trust. The Interim Director of Finance and Resources went on to say that the presentation of quality indicators is based on the Trust’s Quality Priority areas given that the full suite of quality indicators are presented to the Quality and Safety Committee for discussion and assurance each month and the list of Operational indicators reported to FIP in 2016/17 has been rationalised in response to feedback from FIP and Internal Audit, with the full list of contractual indicators being monitored and managed at Divisional Business Meetings. The Interim Director of Finance and Resources went on to say that social care performance indicators and targets have not yet been agreed for 2016/17, so the Trust continues to report based on the 2015/16 framework. The Interim Director of Finance and Resources informed Board Members that FIP and QSC follow different reporting periods based on the need for performance data to be available quickly to respond to contractual processes whereas quality reporting focusses on answering the ‘so what’ question by reporting the full governance cycle once causal investigation is complete and therefore Performance data relates to December 2016 and Quality data relates to November 2016. The Interim Director of Finance and Resources informed Board Members that there are two Red indicators for November 2016 data and two indicators rated Amber these are: 1) Patient feedback on the Quality of Care: The number of respondents who are
extremely satisfied with the quality of their clinical treatment or care is 82% against a Trust target of 90% (a decrease from 86% for the previous reporting month). This relates to service users identifying delays in waiting times, appointments and being unable to gain telephone contact to the booking centre.
2) Community avoidable and attributable Grade 3 & 4 pressure ulcers: The Trust has exceeded the tolerance of 21 cases maximum in community services set for our 2016/17 Quality Priorities. There was one case deemed avoidable and

Page 15 of 24
attributable at Pressure Ulcer Review Group in November therefore this brings the total since the beginning of April to 23 for the Trust - the case deemed avoidable and attributable to community teams in November was for Leek ILCT. This has been reported as a Serious Incident (STEIS) and a full analysis report into the prevalence of grade 3 & 4 pressure ulcers within community services was presented to the Quality and Safety Committee on 11 January 2016 and a number of on-going actions have been agreed and will be reported back to QSC. This will include a further analysis of the Grade 2 pressure damage.
The Interim Director of Finance and Resources informed Board Members that: • Staffing level incidents are the second highest cause group for incidents across
the Trust during this reporting period, at 81 (this was previously 63 and 81 for October and September respectively. The majority of these (66) relate to ILCT teams in Stafford (27), Tamworth and Lichfield (1), Stoke (17), Leek (1), Cannock (5) and Newcastle (15).
• Community Grade 3 & 4 pressure ulcers reported: There were 27 Grade 3 & Grade 4 reported pressure ulcers during November (one of which was classified as grade 4); the RCAs for these incidents will all have been reviewed by PURG by the end of January and an update will be available at the next Committee.
• Ten Quality Assurance Visits were delivered in November 2016; seven teams were rated overall as Good and three teams were rated Requires Improvement against the CQC Key Lines of Enquiry. Immediate actions have been delivered where required with the Quality Team scheduling targeted follow up to those teams requiring improvement to evidence the outcome of remedial actions. • The number of formal complaints received has decreased from 32 in
October to 24 in November. • The number of PALs contacts in relation to the new continence product
supplier has reduced to two in November. • Friends and Family Test: From the 3235 service users and carers who
answered the Friends and Family Test in November, 97% of respondents (3125 respondents) would recommend the Trust to friends and family if they needed similar care or treatment, with 1% (24 respondents) who would not recommend the Trust.
The Interim Director of Finance and Resources informed Board Members that overall, of the 38 Trust’s Board performance indicators with targets attached, 20 are green, 5 are amber, and 13 are red, with 1 indicator improving its RAG rating from “Amber” to “Green” in December: • The percentage of older people still at home and needing no on-going Social
Care services 91days following receipt of reablement services increased from 53.8% to 56.4% against a target of 55%.
The Interim Director of Finance and Resources informed Board Members that performance concerns were around the following areas: • Social Care:
• Social care delayed transfers of care (bed days in the month) was 2,015 in December against a target of 1,015. This high volume of delays per month was reached following 6 consecutive months of rapid increases from 1,535 in May. If must be noted that only 30.3% of delays were attributable to assessment and care management (the Trust). The rest of the delays are due to factors not controllable by the Trust (lack of capacity and response times in the care market).
• The proportion of clients receiving Direct Payments was 22.2% against a target of 28%, still showing no signs of improvement. Commissioners are starting to acknowledge the additional challenges to roll out direct payments: • New laws now state that when in receipt of a direct payment the client is

Page 16 of 24
responsible for employee liability, CRB checks, sickpay, arranging sick cover and redundancy etc this deters clients away from opting for direct payments.
• Care Act 2014 Impact - Negative impact of new legislation in requiring options to be presented to service users beyond Direct Payment. Cannot insist on Direct Payments in interacting with service users, which used to be default practice in some circumstances.
• Children’s Services: • Percentage of New Births that receive a face-to-face new birth visit within
10-14 days by a Health Visitor improved from 75.6% to 79.5% against a target of 95-98%. Year to date Performance is 88.0%.
• The percentage of children who received a 2-2.5 year review improved from 86.2 to 86.8 against the 95-98% target. Year to date performance is 87.9% - Health Visiting issues are concentrated in the South Division. It was agreed at the October DBM that a watching brief would be kept on this indicator, taking into account the challenges the service was experiencing: both services going out to tender, and approx. 140 Health Visitors at risk as a result of service reductions introduced by the commissioner. A performance improvement plan will now be initiated to accelerate recovery.
• We continue to RAG rate Breastfeeding as red while we await Q3 figures. A Performance Improvement Plan is still in place.
• Finance: • The gap between Financial Performance and Planned Performance
increased again in December, reaching £21.9 m. CIPs delivery remains at 76% against the YTD Plan .
• Better Payment Practice Code by volume and value were at 82% and 88%, against a target of 95%.
• Non-NHS payables > 90 days were at 32% against a target of 5%. • Non-NHS receivables > 90 days improved from 42% to 36% against a
target of 5%. • Workforce:
• Information Governance training compliance has been static for four months in the 84-85% range, currently at 84.47% against the 95% target.
• Staff turnover (cumulative) remains “Red” at 10.91% against the 7.50% target profile for December.
The Trust Board noted the content of the executive summary and performance scorecard. The Chairman thanked the Interim Director of Finance and Resources for her report.
2017.1090 CIP The Interim Director of Finance and Resources Director of Finance and Resources presented the CIP report to Board Members to share the latest position regarding delivery of the 2016/17 Cost Improvement Programme. The Interim Director of Finance and Resources informed Board Members that the current (month 9) in-year forecast of approx. £7.8m (not risk-weighted, approx. £6k lower than in month 8), projects an in-year positive variance of approx. £700k vs the revised in-year plan of £7.1m. The Interim Director of Finance and Resources went on to say that the month 9 year-to-date (YTD) position exceeds the revised YTD target of £4.6m by £817k, with a net decrease of approx. £25k vs the month 8 variance and despite the fact

Page 17 of 24
that the delivery plan is relatively highly skewed towards the second half of the year, with the so-called “hockey stick” effect kicking in from around month 7, so far the YTD delivery proved resilient and kept consistently above target. The Interim Director of Finance and Resources informed Board Members that in due course of the month, the in-year forecast registered a positive variance of approx. £138k, including the following: • North Division: £21k from an additional reduction in agency staff costs and a
further £12k relating to anticipated income for Pluerex Drains. • Community Hospitals: £30k from an additional reduction in nursing agency staff
costs. • South Division: £22k from an additional reduction in agency staff costs, a further
£18k to reflect the accrued income relating to Divisional SLAs and another £9k relating to a reduction in spend on continence products.
• Dental: £23k from a decision to hold vacant posts for quarter. • There were a number of other schemes that contributed to the positive variance
in the in-year forecast. Details can be found in the individual Directorate/Division Exception reports.
The Interim Director of Finance and Resources went on to say that conversely, in month 9 the in-year forecast also registered a negative variance of approx. £144k, including the following: • Community Hospitals: £51k relating to an increase in Medical Agency cover
required. • South Division: £27k relating to the Cannock Estates scheme which now will not
deliver in full until next year, savings have been identified relating to the estates charges for West Chadsmoor which has now closed and forms part of the wider moves anticipated in the Cannock Area. Also there has been a decrease of £38k relating the Management savings scheme which has been adjusted to reflect the current plans.
• Finance Directorate - £15k as the scheme relating to the Lillie UHL move to Inform which was due to start delivering savings from January 2017 but has now been delayed until June 2017 to ensure the safe transition of the service onto the new system. Commissioners have been informed of the change in timescale
• There were a number of other schemes that contributed to a negative variance in the course of the month. Details can be found in the individual Directorate/Division Exception reports.
The Interim Director of Finance and Resources said that in order to further substantiate the in-year forecast, we are tracking each CIP scheme through a range, with the bottom-end as the minimum that the scheme will deliver in-year and the top-end as the maximum potentially achievable and the cumulative bottom-end of the range is currently £6.8m and the top-end £8.3m, with a middle point of approx. £7.6m (both ends and middle point marginally higher than the previous month) and the middle point of the range is currently approx. £200k lower than the in-year forecast of £7.8m, which is not risk weighted, with the full-year, recurring effect of the current CIP schemes has remained the same as month 8 at £10.8m. The Interim Director of Finance and Resources went on to say that while approx. £5.4m of the £7.8m in-year forecast projects are considered ‘low risk’ or have already been implemented, the remaining initiatives are rated either ‘medium’ risk (£2.3m, approx. £100k lower than month 8) or ‘high’ risk (less than £100k, which is lower that the £200k than month 8). The Interim Director of Finance and Resources informed Board Members that the

Page 18 of 24
key ‘medium’ and ‘high’ risk elements include: • Estates, in particular in the South Division • Some procurement projects • Other specific projects e.g. Hybrid mail and prioritised action plans remain in place in order to mitigate these potential downside risks, wherever possible and in parallel, we keep focusing on identifying potential upside benefits, with potential opportunity areas including: • Agency spend • Provider-to-provider (P2P) contracts (demand and scope reduction/cost
challenge) The Interim Director of Finance and Resources reported that as well as providing potential upside, those incremental opportunities could also support further mitigation of potential downside risks and however, as we approach the last quarter of the financial year, the options to identify material incremental in-year benefits are inevitably reducing. Non-Executive Director, Mr Crowe noted the level of the challenge in the next two years for the Trust. The Trust Board scrutinised the current position regarding the 16/17 CIP programme and risks and opportunities identified. The Chairman thanked the Interim Director of Finance and Resources for her report.
2017.1091 Corporate Risk Register The Director of Nursing and Quality presented the Corporate Risk Register to Board Members for review and to note the changes that have taken place through the Executive Risk Management Committee at its meetings on 20 December 2016 and 10 January 2017. The Director of Nursing and Quality informed Board Members that the Risk Register has been reviewed and the following changes have been made at the Executive Risk Management Committee. • Risk Ref 01 ~ Insufficient standard Domiciliary Care capacity. The risk has
been updated to include the following - where the Living Independent Staffordshire (LIS) as ‘provider of last resort’ is required by Commissioners to provide maintenance packages of care (PoC) due to Independent Sector capacity shortfalls, the relevant clauses within the new Section 75 Adult Social Care Agreement ensure that these requests are not to the financial detriment to the Trust.
• Risk Ref 04B ~ District Nursing Capacity (South Division). It was discussed and agreed that this risk would be separated out into two elements, underfunding of commissioned services and impact of lack of capacity on front line services. This risk will be redefined and presented to ERMC in February 2017 for approval.
• Risk Ref 677 ~ Inability to recruit and sustain staffing levels in Community Hospitals. This risk has been updated to include the uncertainty of Commissioner Intentions to the risk cause and therefore the risk has been saved as a new version.
The Director of Nursing and Quality said that three risks were considered and agreed for migration from the Corporate Risk Register to the Board Assurance

Page 19 of 24
Framework (BAF) and the risks agreed for migration to the BAF (and therefore removed from the Corporate Risk Register) from January 2017 are: • Risk Ref 760 ~ Risk of non-delivery of the Cost Improvement Programme
(CIP) target for 2016/17 • Risk Ref 766 ~ Risk that the Sustainability and Transformation Plan (STP)
model creates an Organisational form that does not empower the delivery of a County wide infrastructure to support the establishment and development of an Multi-speciality Community Provider (MCP) framework
• Risk Ref 773 ~ Risk of poor clinical outcomes for patients across the Local Health Economy due to continued poor performance of local A&E’s against a four hour target. This may result in a reputational risk to the Trust due to association with a failing urgent care system.
The Director of Nursing and Quality said that one risk was discussed and agreed for removal from the Corporate Risk Register: • Risk Ref 699 ~ Overarching cyber security risk. It was agreed that the risk was
no longer required on the Corporate Risk Register due to actions that have been completed. It was agreed that this risk could be closed and the individual elements managed via the local Risk Register where they are already captured.
The Director of Nursing and Quality informed Board Members that no new risks were discussed for addition to the Corporate Risk Register in December 2016 or January 2017 and that the Nursing and Quality Directorate and Transformation Directorate Risk Registers were presented at Executive Risk Management Committee in December 2016 and January 2017 as part of the deep dive schedule and no risks were identified from either deep dive for escalation to the Corporate Risk Register. The Director of Nursing and Quality also informed Board Members that the Executive Risk Management Committee reviewed the terms of reference and it has been agreed that the BAF will be received at ERMC, alongside the Corporate Risk Register and therefore the terms of reference have been amended to reflect the BAF inclusion. The Trust Board: • Noted the updated version of the Corporate Risk Register appended to
this Report; • Noted the actions that are being taken to manage the reported risks; • Noted the other activities undertaken by the Executive Risk Management
Committee during December 2016 and January 2017. The Chairman thanked the Director of Nursing and Quality for her report.
2017.1092 Well Led Framework The Interim Company Secretary presented the Well Led Framework report to Board Members. The Interim Company Secretary reminded Board Members that the CQC inspected the Trust in November 2015 and rated the Trust as ‘requires improvement’, and inadequate for the ‘Well Led Domain’ and following on from this NHSI commissioned a capacity and capability review into the leadership and governance of the organisation. The Interim Company Secretary said that the plan has been developed to ensure

Page 20 of 24
that the recommendations from the following have been captured and responded to: 1. Well-Led Review 2. NHSI capacity and capability review 3. CQC inspection (only Well-led actions) 4. NHSI observations 5. Red 10 Board Development sessions The Interim Company Secretary informed Board Members that this is the first cycle of reporting against the actions outlined within the Governance improvement plan and reports have been presented at the Audit Committee as well as Workforce matters and as part of the process which was outlined to the Board in November the Interim Company Secretary has meet with the majority of director leads to discuss the actions for which they are responsible. The Interim Company Secretary informed Board Members of progress to date:
Key theme Number of Actions Completed On
Track Some Issues
Off Track
Strategy and Development 24 5 15 4 0
Risk Management 20 8 10 2 0
Board skills and Capacity 13 3 10 0 0
Culture and Organisational Development
16 10 5 1 0
Leadership 29 12 17 0 0
Governance 40 13 27 0 0
The Interim Company Secretary informed Board Members that the following recommendations are currently rated as ‘off track’: • SD02- Some services lacked a specific strategy that articulated the detailed
objectives and plans for the service; this meant some staff did not understand their role in contributing to the strategy - All actions within this recommendation (4) are currently rated off track. These actions relate to the CQC recommendation. Whilst strategies have been developed for a number of areas, there is limited evidence that staff understand these fully and their role in contributing to its delivery. These actions are being monitored by the Quality Improvement Steering Group as well as Quality Committee
• RM01/ RM07- The Board Assurance Framework is currently being reviewed to ensure that each risk is owned by an executive lead and a Board Sub Committee - these actions relate to the BAF and having a board approved plan. The completed BAF is on the agenda for the January Board.
• OD05- Staff morale in community adult nursing services was low - the Trust has responded to the annual staff survey (2015) with a number of focussed action plans and refocused organisational health activities to support improved morale and given the level of tendering, contractual renegotiation and decommissioning associated with services delivered by the Trust this has had an impact on staff and their morale and leaders have pre-empted change where possible to engage staff in planned service tender and change processes (i.e. children’s service review). However given the continued
Page 21 of 24
difficulties in maintaining a stable workforce and managing demand within community nursing further targeted work is required to support morale and encourage staff retention.
The Interim Company Secretary informed Board Members that these actions are being monitored by the CQC steering group as well as Workforce Matters. The Medical Director noted that there was an issue with the table on this report and the Interim Company Secretary would rectify this. The Board of Directors:
• Noted the updates against the well led improvement plan • Approved that a summary report will be presented to future Board
Meetings and the full plan reported by exception The Chairman thanked the Interim Company Secretary for her report.
2017.1093 Board Assurance Framework The Interim Company Secretary presented the Board Assurance Framework report to Board Members. The Interim Company Secretary informed Board Members that key points in the report are: • The Board Assurance Framework is an important document for providing
assurance that the Board is aware of the risks to its key objectives and has a robust system of internal control
• The 2016/17 Assurance Framework is included at Appendix 1 • Since the last review of the Board Assurance framework the risks have been
reviewed with Director leads and also reviewed at executive risk management committee
• The First Committee deep dives have also taken place at FIP and Workforce Matters.
The Board discussed the risks identified in the Board Assurance Framework and approved the current BAF. The Chairman thanked the Interim Company Secretary for her report.
2017.1094 Section 75 public consultation The Interim Company Secretary presented a report to Board Members on the Section 75 public consultation which updated them on the outcome of the statutory consultation into the proposals which underpin the proposed new Section 75 Agreement, the proposed Services – Assessment and Care Management, Reablement and Occupational Therapy, and service model. The Interim Company Secretary informed Board Members that as the Board agreed to enter into a new Agreement with the County Council at its confidential meeting on the 26th September 2016 and as the County Council and the Trust have agreed that a new Section 75 Agreement will be entered into then the statutory duty of consultation is engaged and the Director of Operations has led the discussions and has acted as the lead Director for the Trust. The Interim Company Secretary went on to say that the Associate Director of Communications worked with her counterpart at the County Council in formulating the questions and “case stories” which were incorporated into the consultation documents and that the consultation

Page 22 of 24
was launched on 4th November 2016 and ran for just over 5 weeks, until the 13 December 2016 and a total of 51 responses have been received overall. The Board noted the outcome of the Public Consultation. The Chairman thanked the Interim Company Secretary for her report.
2017.1095 Board cycle of business The Interim Company Secretary presented a report to Board Members on the Board’s cycle of business which sets out those matters proposed to be considered by the Board of Directors and is intended to capture those items which the Board of Directors can expect to receive over the course of the next 12 months to enable to the Board to fulfil its purpose. The Interim Company Secretary informed Board Members that additional specific items may be added to the agenda for a particular meeting as directed by the Board of Directors, or if considered appropriate by the Chairman and in year amendments to the cycle may be necessary as the Trust develops and reviews its priorities. The Medical Director asked if the Mortality Report and Caldicott Guardian reports should be added to this cycle and the Interim Company Secretary confirmed this would be added to the cycle. The Board agreed the Cycle of Business. The Chairman thanked the Interim Company Secretary for her report.
2017.1096 Any Other Business The Chairman asked Board Members if there was any other business to be raised and the Director of Workforce and Development confirmed that she would like to raise the organisational development strategy as this had been placed on the Trust Board Development agenda in error. Organisational Development Strategy The Director of Workforce and Development presented the full updated organisational development and Leadership Strategy for 2017-2019 to the Trust Board. The Director of Workforce and Development informed Board Members that this report has been developed following a presentation of the outline aims and framework to Workforce Matters Committee on 23 September 2016 followed by a presentation to Trust Board on 30 November 2016 and feedback received from the Workforce Matters Committee members and Trust Board members and the report reflects the suggestions made. The Director of Workforce and Development informed Board Members that key points within the report were: • This revised organisational development strategy is designed to provide a
detailed framework and activity plan over the next 2 years • An organisational development aim has been designed to support the delivery
of each Trust organisational goal • The activity has been carefully aligned to the proposed actions within the Quality
Improvement Plan for Well-led and the Trust Operational Plan that was approved in December 2016
• The recommendations within the STP will require significant organisational

Page 23 of 24
development intervention to ensure that the workforce is fully engaged, involved and supported to help recommend and take responsibility for redesign of services. This has also been considered within the organisational development aims and choice of activities
• The SSOTP Leadership Programme has therefore been refreshed with the addition of the element of ‘Trust’. This has been added to the existing elements of Appreciation and Compassion so the programme is now described as ‘Leadership to Act’
• The range of activities to deliver the organisational development aims has been grouped into five key work areas of • Leadership • Learning • Team and Personal Development • Staff Engagement and Communications • External Focus for business and relationships
• Priority will be given to the team leaders involved with the four improvement projects that have been agreed within the Operational Plans well as the Section 75 transformation programme with Social Care staff
• Funding from HEWM has recently been approved to enable additional organisational development resource to deliver a specific transformation project. This provides an opportunity for SSOTP to lead across the MCPs on a framework for integrated working
• The capacity and capability to deliver the organisational development activity has been carefully considered and planned to ensure that the resource available is sufficient to meet the objectives. Mitigation is in place to ensure that activities can be completed on schedule
• The success of the organisational development aims will be monitored through results of staff surveys and feedback and reports on progress provided at quarterly divisional business meetings, Workforce Matters Committee and an annual Trust Board report
The Associate Director of Communications confirmed that this document would be added to the website with the public trust board documents. The Trust Board approved the five organisational development aims in November 2016 are noted and approved the content of this organisational development and Leadership Strategy. The Chairman thanked the Director of Workforce and Development for her report. Review of meeting and outcomes The Chairman asked all Board Members if they felt they had adequate time to raise points at today’s meeting and all Board Members agreed that they had. Review of risks The Chairman asked all Board Members if they felt all risks had been mitigated and Board Members agreed that they had. The Chairman asked if any members of the public had any questions they wanted to raise, no questions were raised.
2017.1097 Date of next meeting The next Public Trust Board Meeting will be held on Wednesday 22 February 2017, Morston House, Newcastle under Lyme, ST5 1QG

Page 24 of 24
1
REPORT TO: Staffordshire and Stoke on Trent Partnership NHS Trust Board
TO BE HELD ON: 22nd February 2017
Subject: Chief Executive Report
Strategic Goal: (tick as applicable)
We will provide high quality and safe services which provide an excellent experience and best possible outcomes
We will work with users and carers to deliver integrated services, simply and effectively
Our organisation will develop and deliver sustainable, innovative services that support independence
Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Stuart Poynor, Chief Executive
Recommendation: For Approval & Assurance
For Discussion For Information x
PURPOSE OF THE REPORT
To update the Board on the key issues within the Partnership Trust and progress on embedding our values. This report provides updates on key issues with a general summary of actions that demonstrate how we are embedding our values. It is for information and not assurance. There are more detailed reports on the agenda the purpose of which is to provide assurance.
KEY POINTS
Local Quality
• Launch of care strategy engagement • Quality Priorities Consultation 2017/18 • Care Quality Commission rate LIS Newcastle as Good

2
People • Shortlisted for Health Service Journal award • Staff visits update • Continuing our integration offer
Responsibility • Financial position • Discharge to Assess: finding solutions to urgent care • Development programme progressing well • Business continuity month • Mental Capacity Act compliance
National • Productivity review in community trusts • ‘Allied Health Professions into Action’ - using AHPs to transform health, care and
wellbeing • Blog looks at how STPs can dissolve organisational boundaries • Sir Peter Carr Award – applications now open
INTER DEPENDENCIES:
Legal and/or risk None
Clinical None
Financial None
HR None
Social care None
Patient & public involvement
None
Staff and Trade Union involvement actions undertaken/ planned Equality impact
None
Information exempt from disclosure
None
Requirement for further review
None
RECOMMENDATIONS / ACTION REQUIRED
This report is for information only.

3
We put quality first: we deliver quality and do the very best we can Launch of care strategy engagement Rose Goodwin, Director of Nursing and Quality, and Dr James Shipman, Medical Director, have launched an engagement exercise with staff to help them develop a care strategy for the Trust. They are proposing that the strategy is organised around five pledges:
• We promise to work in partnership with individuals, families and communities to equip them to make informed choices and support them to manage their own health through strong, visible leadership, a highly skilled workforce and working with those that use our services and other providers.
• We promise that we will have the right staff in the right place at the right time and that our staff will receive the right education, training and development to deliver well led, high quality care.
• We promise to respond to what matters most to our staff and colleagues.
• We promise to learn from what we do, using research, audit and evidence to support caring high quality services.
• We promise to use technology and informatics to support and improve practice, address unwarranted variation in care and improve outcomes for those that use our services.
Each week staff are being asked to focus on one of the pledges. Any directors visiting staff will take the opportunity to discuss these pledges with them. Non-Executive Directors are invited to the do the same. For each pledge, we are asking:
• Where are we now?
• What do we plan to achieve?
• How will we do this?
• How will we measure success? Quality Priorities Consultation 2017/18 Each year we develop a set of quality priorities to support our vision, values and strategy. These priorities aim to improve the safety, experience and effectiveness of our services. Each year we report progress against the priorities in our Quality Account. For 2017/18 our aim is to develop a set of focussed quality indicators that are meaningful to service users and staff, which ensure We Put Quality First. We are consulting on our quality improvement priorities until 24 February 2017.

4
Care Quality Commission rate LIS Newcastle as Good Following their inspection in October of last year, the Care Quality Commission (CQC) rated Living Independently Staffordshire (LIS) Newcastle as Good. The service received ‘Good’ ratings in four of the five areas inspected (safe, effective, caring and well-led) and ‘Outstanding’ in being responsive to people’s needs. The report complemented the service for providing people with ‘outstanding personalised care and support’. It recognised that the service was focused on continuously improving quality and that all staff that work within the service ‘demonstrate strong values and a desire to learn about and implement best practice.’ The CQC rated the responsiveness of the service as ‘Outstanding’ and reflected that people’s levels of needs were assessed and reviewed to ensure they got person-centred care which was flexible and responsive to their individual needs. One relative said: “The care staff are very good at supporting my mum to become more independent, they support her to have her medication on time and log this on their medication administration record. The notes they keep are excellent.” They join our other Living Independently Staffordshire services based in Cannock, East Staffordshire, Tamworth and Lichfield, Moorlands, South Staffordshire and Stafford who have also received ‘Good’ ratings. I am also pleased to be able to announce that we have received investment in LIS in Stafford, which will help us build a discharge to assess (D2A) service around County Hospital.
5
We focus on people: we treat people as individuals and take time to respect and understand their point of view Team who presented at Board shortlisted for Health Service Journal award Gail Lowe and Nichola Humphries have previously presented at Board and now their project has been shortlisted for a Health Service Journal (HSJ) Value in Healthcare award. The project involves working with frequent users of services in North Staffordshire to coordinate their care and treatment across different services and to improve their experience whilst receiving care. The project has been shortlisted in the category of ‘Community health service redesign’ which recognises projects designed to provide efficient, high quality community-based care in the most appropriate setting for patients. The winners will be announced at an award ceremony on 24 May. Gail and Nichola presented at the first 1Vision of the year. They were joined by colleagues from Co-ordinating Isolated Support Services (CISS) and Children’s Speech and Language Therapy, City and North. The presenters shared their experience and learning with over 120 members of staff from across the Trust. Staff visits update I continue to visit our services, despite the work for Together We’re Better taking up more of my time. I am often humbled when I meet the people to whom we provide a service. This was certainly the case earlier this month. I spent almost a whole day with our asylum seeker and refugee service. We all watch, listen or read the news and learn about war-torn countries. I was reminded that there are people living in our communities, maybe neighbours, who have experienced life-changing situations and survived. I have the utmost respect for the people who come here seeking peace and to the people who listen to their stories, and go on to provide care and support. At our weekly directors’ meeting we review the visits that have taken place in the previous week. I am pleased to say that my directors are out and about as well, and thank our Non-Executive Directors for joining them when they can. I would like to take this opportunity to acknowledge all our staff who are experiencing uncertainty about their jobs and roles as a result of changes in the services that are commissioned from us. Since the last Board meeting, we have been advised that our lifestyle service will end in April. As a result 39 members of staff have been served notice of their employment. Our focus is to ensure that those staff are fully supported to find alternative employment and that service users continue to receive high quality support to complete their programmes. Continuing our integration offer A considerable amount of work has been undertaken in recent weeks between officers of the Trust and Staffordshire County Council on the contract to provide adult social care and we anticipate being able to sign the section 75 within a week of the Board meeting. The contract is in three parts; enablement, occupational therapy and assessment & case management Significant transformation is required to deliver the new models and a project plan and team are in place. Staff are being briefed about the changes and how they are likely to impact on their role.

6
We take responsibility: we take personal ownership of things and see them through; we focus on finding solutions Financial position Our financial position remains a challenge and I regret that we are not able to show improvement more quickly. We are in dialogue with our regulators, NHS Improvement, with whom we have shared a two year recovery programme. Members of the Finance, Investment and Performance committee will receive more information about our approach to this at their meeting prior to the Board. Discharge to Assess: finding solutions to urgent care In recognition of our success in supporting the flow of people through urgent care in the county, we have been asked by commissioners to lead the implementation of a discharge to assess (D2A) service accross the county. In line with our health and care economy’s home first policy, it has been agreed that from April of this year, assessments for on going care will not be done in hospital, but in a person’s usual place of residence. This will involve identifying them in A&E and working quickly to return them home. If they are not able to go home immediately, a track and triage team will follow them through the acute hospital. This has the potential to make a real difference to how people experience the urgent care system and is very exciting. We will continue to work with partners where working together will bring benefit for people locally. Development programme progressing well As part of our leadership development programme, we established a senior leadership team last year. This is made up, mostly, of line reports to directors and reports into Executive Leadership Team on a weekly basis. The group has continued to grow and we held our first joint business meeting this month. There was a lot of big issues on the agenda and it was a very productive meeting. We worked through the corporate objectives and the outcome of that discussion is being presented to Board members in the development session on the day of the public Board meeting. Business continuity month Further to the papers received by Board towards the end of last year, we have started the countdown to business continuity planning month which begins on 1 March. All teams in all divisions will receive a business continuity plan template, which needs to be completed during March. Teams will be selected at random for testing, to ensure their plans are fit for purpose. Mental Capacity Act Compliance Mandatory Mental Capacity Act training compliance rates have significantly improved and are now exceeding the 90% target. The current compliance is 94%.
7
National Productivity review in community trusts NHS Improvement has started a review into community and mental health trusts, building on the approach of the Carter report on operational productivity and performance in NHS acute hospitals. He will follow a similar structure and methodology to that of his original acute review, with some significant tailoring to community and mental health. The review will look to understand:
• how organisations in mental health and community trusts operate • what good looks like • what approaches to improving productivity and efficiency are already in
place and what opportunities there are to drive these further • what metrics and indicators are required to support the development of the
model for these sectors. 23 Trusts have been chosen to support the review and share their learning. ‘Allied Health Professions into Action’ - using AHPs to transform health, care and wellbeing Since the last Board meeting, ‘AHPs into Action’ has been launched. It is intended to inform and inspire AHPs, leaders and decision makers across the health and care system, offering:
• a clear view of the transformative potential of AHPs • 53 examples of innovative AHP practice • a framework to help develop local delivery plans
It also defines how AHPs can support local Sustainability and Transformation Plans (STPs) and implement actions to respond to the three priorities set out in the Five Year Forward View: driving improvements in health and wellbeing, restoring and maintaining financial balance, and delivering core quality standards. Blog looks at how STPs can dissolve organisational boundaries A blog by Dr Arvind Madan, NHS England Director of Primary Care on the NHS England website looks at how the STPs can help dissolve boundaries within the NHS and between healthcare and social care. Sir Peter Carr Award – applications now open The Sir Peter Carr Award is a £30,000 award which will be made to a clinician and manager partnership (£15,000 each) to invest in their professional development over a year to support the delivery of a shared improvement objective. Both the winners and partnerships shortlisted for the award (up to five in total) will also receive access to support including mentoring, networks and opportunities to attend events during the year, such as the upcoming International Forum on Quality and Safety in Healthcare. Applications opened on the 31 January 2017 and close 14 March 2017.

8

Page 1 of 2
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS
TRUST BOARD MEETING
TO BE HELD ON: WEDNESDAY 22 FEBRUARY 2017 Subject: Assurance Report of the Chair of the Quality & Safety Committee
Strategic Goal (tick as appropriate):
x We will provide high quality and safe services which provide an excellent experience and best possible outcomes
We will work with users and carers to deliver integrated services, simply and effectively
x Our organisation will develop and deliver sustainable, innovative services that support independence
Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Rose Goodwin, Director of Nursing & Quality
Recommendation: For Approval & Assurance
x For Discussion For Information
PURPOSE OF THE REPORT: To receive an assurance report from the Chair of the Quality & Safety Committee as to the matters and business of the meeting of the Committee of the 8 February 2017, summarised in the key points below, and referred to the Board for its consideration and action (as required). KEY POINTS: Items of Business for Review by the Trust Board:
• Q3 Health and Safety Report – the Committee noted the work required to accelerate fire training and compliance. The Committee requested that the Health and Safety Committee review the level of analysis within the report and provide an exception report to the Quality and Safety Committee. The Fire Lead and Health and Safety Manager provided assurance that the buildings the Trust has responsibility for are serviced and fit for purpose and that the Trust is compliant with all of the certificated processes which fall within its responsibility.
• Care Strategy – The draft Care Strategy was presented for approval of the initial position and engagement process. The strategy is based on the Chief Nursing Officer’s Strategy commitments and is aligned to the Trust values and priorities. The strategy was well received and the Committee looks forward to receiving a final version in April in readiness for submitting to the April Board meeting for final sign off.
• Q3 Infection Control report - The committee was pleased to note the progress reported in Infection Control activities during quarter 3 and that the Trust is compliant with hygiene standards.
• Quality Improvement Plan - The Quality Improvement Plan continues to develop well and the Committee was assured by the ongoing attention paid to outcomes through audit and Quality visits.
• Q3 Children’s Safeguarding Report - The quarter 3 Children’s Safeguarding Report was

Page 2 of 2
received and considerable progress in respect of training was welcomed. There was some discussion concerning level 3 training and the committee offered its support in ensuring that targets are met. The Safeguarding Policy was presented for approval. Some minor adjustments are to be made to the Equality Impact Analysis and it was noted that a review of the Named Doctor requirement is being undertaken and will be reported to the March committee. Interim arrangements are in place to provide assurance.
• CIP QIA Panel - The Committee signed off the Terms of Reference for the Quality Impact Assessment Panel along with the process used by the panel.
• Transfer of Patients into Community Hospital Beds - A comprehensive report was submitted setting out the measures in place to ensure that the needs of patients admitted to Community hospital beds are appropriate for the service available and matched to staffing levels and skills. The Committee was assured that the process is thorough and suitable escalation procedures are in place.
• Board Assurance Framework (BAF) - A presentation was received which set out the elements of the BAF relating to the functions of the Quality Safety Committee, covering risk control, planned actions and progress. The Committee noted its considerable responsibilities but was reassured that the work is well in hand.
INTER DEPENDENCIES: Legal and/or Risk Regulatory and reputational risk as a consequence of
the overall “requires improvement” rating published by the Care Quality Commission. The Committee has an oversight function in relation to the actions taken to address the required improvements.
Clinical Clinical risks are highlighted in the Quality scorecard and associated reports.
Financial None at this time.
HR None at this time.
Social Care Social Care is an integral part of the reporting system to Quality Safety Committee.
Staff and Trade Union involvement actions undertaken/planned
Staff have been kept appraised of the changes to services.
Patient & Public Involvement The experience of Patients and Services Users and their families is considered in the experience and effectiveness reports to the Committee.
Equality Impact None at this time.
Information exempt from Disclosure None at this time. Requirement for further review None at this time. RECOMMENDATIONS: The Trust Board is recommended to:
• receive the assurance report of the Chair of the Quality & Safety Committee into the matters and business arising from the meeting of the Committee on the 8 February 2017.
• and to consider whether any further action is required to address the matters highlighted in the key points above.

Page 1 of 5
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD MEETING
TO BE HELD ON: WEDNESDAY 22ND FEBRUARY 2017
Subject: Safe Nurse Staffing in Community Hospitals
Strategic Goal: (tick as applicable)
X We will provide high quality and safe services which provide an excellent experience and best possible outcomes
We will work with users and carers to deliver integrated services, simply and effectively
Our organisation will develop and deliver sustainable, innovative services that support independence
X Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Rose Goodwin - Director of Nursing & Quality
Recommendation: For Approval & Assurance
X For Discussion For Information
PURPOSE OF THE REPORT: This paper provides an overview of nurse staffing levels in the Community Hospitals operated by Staffordshire and Stoke on Trent Partnership NHS Trust during January 2017.
KEY POINTS: The nurse staffing levels summary is attached for January 2017 (Appendix 1).
• Safe staffing has been maintained throughout January 2017. • Day time fill rate for RN’s – 94.9% and for HCSW – 100.1%. • Night time fill rate for RN’s – 98.5% and for HCSW – 101.1%. • CHPPD for January 2017 was 6.8 hours (RN – 3.2h and 3.6 h for care workers). • Broadfield Ward continues to report a daytime RN to patient ratio of 1:9 and Cottage Ward
reports a night-time RN to patient ratio of 1:11; all other wards lie within excepted parameters
• 4 shifts where professional concern raised (0.61%). • There were 8 shifts where there was only one registered nurse on duty, 6 of these instances
occurred on Cottage Ward. • Registered nurse vacancies remain high having increased from 18.3WTE to 20.1WTE since
the last report and for care workers the figure has remained static at 3.65WTE. INTER DEPENDENCIES: Legal and/or Risk It is a requirement of NHS England to provide monthly updates on safe

Page 2 of 5
staffing levels. Failure to comply will risk reputational damage with the public.
Clinical The link between safe nurse staffing levels is clear. Ensuring that the right staff are on duty to deliver care in a timely manner is a priority for the Partnership Trust
Financial There are no direct financial implications associated with this paper however there are additional costs associated with temporary staff usage.
HR On-going recruitment and management of staff sickness is reliant upon HR support. The Staffing Establishment has been approved by and supported by the Board
Staff and Trade Union involvement actions undertaken/planned
Support from staff side colleagues is essential in managing staff absence and supporting safe recruitment practices.
Social Care This paper relates to safe nurse staffing levels in Community Hospitals only.
Patient & Public Involvement
There has been no direct involvement of public groups in the development of this paper. Safe staffing information is available to the wider public through NHS Choices and the organisations website.
Equality Impact Safe nurse staffing levels has an impact on all users of service regardless of culture or ethnicity. This paper describes how a safe staffing profile is monitored and this is available to the public via the organisations website.
Information exempt from Disclosure
None. This paper will be published on the Partnership Trust website to allow public scrutiny.
Requirement for further review
Safe nurse staffing levels will continue to be monitored on a monthly basis
RECOMMENDATIONS / ACTION REQUIRED: The Trust Board is requested to:
1. To receive the report for January 2017 and be assured that the organisation is monitoring and mitigating issues relating to safe staffing establishments.

Page 3 of 5
Report on Safe Nurse Staffing in Community
Hospitals – January 2017 This report provides information regarding the safe staffing position across the seven wards operated by Staffordshire and Stoke on Trent Partnership NHS Trust at Leek Moorlands and Haywood hospitals. The report relates to nursing staff (direct patient care) and does not include supporting roles such as house-keeping, diversional therapy or AHP staff. The information which is included within this report is verified by the Ward Sisters and Hospital Matrons and is subject to further scrutiny and challenge through a weekly conference call, facilitated by the Professional Head of Nursing. Safe Nurse Staffing Safe staffing has been maintained during January 2017 across the community hospital in-patient wards. There have been no patient safety incidents associated with staffing levels. Fill Rate NHS England requires all NHS organisations to provide information relating to ‘Fill Rate’ for both day and night time shifts. The term ‘Fill Rate’ relates to the total planned hours (staff scheduled to work on roster) versus actual hours worked and not to the number or skill mix required in agreed shift establishment. The fill rate during day time shifts for registered nurses (RN) in January 2017 is reported at 94.9% compared to 93% in December 2016 and 95.8% in November 2016. For care workers the day time fill rate has continued to fall to 100.1% (103.9% in December 2016 and 105.1% in November 2016), reflecting the reduction in additional staffing above establishment. Night time fill rate for registered nurses is reported at 98.5%, little change from the previous two months (approx. 99.5%). A number of the wards are continuing to report low fill rates (day time) for registered nursing staff; Cottage Ward – 90.8%, Broadfield Ward – 86.6% and Sneyd Ward – 93.2% and for Scotia Ward the daytime fill rate for care workers remains low at 87.4%. Cottage Ward has reported a further falling night time fill rate for January 2017 (90.3%) which coincides with six night shifts, where due to short term sickness absence, only one registered nurse was on duty. The inability to meet planned staffing relates to high vacancy factors within these specific wards, combined with proportionally high sickness within the teams. Care Hours per Patient Day (CHPPD) The Care Hours per Patient Day (CHPPD) for registered nurses in January 2017 is reported at 3.2 hours and 3.6 hours for care workers; with an overall care per patient per day of 6.8 hours. These figures have continued to reduce month on month since this information was added to the dashboard in July 2016; a reflection of the increasing vacancies across the service and a reduction in additional staff above establishment. There are no defined acceptable parameters for CHPPD with the data being collated nationally to provide benchmarking at a future point in time. RN to Patient Ratio Nationally there is a recognition that during day time shifts a ratio of one registered nurse to eight patients is considered the minimum level at which care should be safe; this is not an exact science and additional factors relating to patient acuity and dependency, ward layout and additional external factors may influence safety. At night, this figure may vary and safety is dependent on a number of diverse factors but typically a ratio of 1:10/1:12 is considered appropriate.

Page 4 of 5
The Partnership Trust has demonstrated an overall registered nurse (RN) to patient ratio within acceptable parameters, 1:7 (day time) and 1:9 (night time), during January 2017. Broadfield Ward at Haywood Hospital continue to report a daytime registered nurse to patient ratio of 1:9, slightly above the 1:8 ratio deemed as a safe upper limit nationally, as a result of staff vacancy and an inability to source registered nursing staff to fill these gaps. The ward operates a more integrated approach to care and rehabilitation and support from Allied Health Professionals to aide care delivery has resulted in no patient safety issues associated with staffing and skill mix. Cottage Ward at Leek Moorlands Hospital has reported a night-time registered nurse to patient ratio of 1:11, which is above the 1:10 ratio set for the ward. This is related to the high proportion of shifts, six out of the eight reported, where there was only one registered nurse on duty. This has resulted in a reduced night time fill rate (90.3%) compared to December 2016 where the night time fill rate was noted to be 96.7%. Unplanned sickness on top of a relatively high vacancy factor and an inability to source additional registered nurse cover being the reasons for this situation arising; measures were put in place to mitigate risk and again there were no patient safety issues as a result. There were eight shifts, seven of which were night shifts and one late shift, where there was only one registered nurse on duty during January 2017. Seasonal illness, amongst permanent staff, and an inability to source alternative registered nurse cover was the cause in all cases. Additional care workers were utilised to fill registered nurse gaps wherever possible, so as to mitigate risk, and work activities were reprioritised as well as staff from the preceding shift working additional hours to support peak activity e.g. meal times, medication round, supporting patients to prepare for sleep. During these shifts mutual aid from colleagues on site was provided so as to maintain safety. Only one of these shifts (night shift) was also of professional concern as a result of escalating patient acuity/deterioration in health status coinciding with reduced staffing numbers and skill mix. There were no patient safety incidents as a result of staffing during the month. Number of Shifts Deviating from Agreed Staffing Levels Each ward has a staffing establishment and skill mix developed from safe staffing reviews, based on patient acuity. The number of instances where the shift by shift establishment has deviated from the agreed staffing profile is reported as part of the summary dashboard. The number of shifts falling below agreed staffing for registered nurses is reported as 147 (22.6%), a reduction compared to that reported in December 2016 (27.7%). The proportion of shifts where care worker staff fell below the agreed level continues to rise, with an increase from thirty nine shifts (5.9%) in December to sixty four shifts (9.8%) in January 2017. The number of shifts above the agreed establishment for registered nurses is relatively unchanged with twenty five (3.8%) shifts being reported in January 2017 compared to twenty one (3.2%) in December 2016. Chatterley Ward at Haywood Hospital continues to be the prime user of additional registered nurses, twenty two shifts were noted to have additional registered nursing staff on duty. Additional registered staffing usage is related to supporting those at the end of their life and the additional registered nursing activities required at this point. All additional staff usage, particularly where this is sourced from a nursing agency, is authorised through the hospital management structure to support safe care delivery. The proportion of shifts where additional care worker staff were utilised has fallen from three hundred and thirty seven shifts (51.8%) in December 2016 to three hundred and two shifts (46.4%) in January 2017. These staff are required to provide support for individuals with additional care and monitoring needs, particularly those at risk of falls as well as to fill gaps in the rota, where registered nurse cover could not be sourced. Professional Concerns There were four shifts (0.6%) reported as being of professional concern (red) during January 2017, a significant reduction compared to that reported in December 2016 (2.7%). These concerns related to increased patient care needs, with Grange Ward reporting three of the four instances. The proportion of shifts reported as ‘amber’ has continued to rise since November 2016 (20.9%) to 36.4% (237 shifts) during January 2017 and reflects the demand and overall pressures experienced across the service.

Page 5 of 5
Agency Staff Usage The proportion of registered nurses utilised from a temporary staffing agency has increased slightly from two to three percent during January 2017 and for care workers it has fallen from seven to four percent. Agency use as a percentage of the staff on duty is noted to be highest on Chatterley Ward for registered nurses (12%) and Grange Ward for care workers (7%). Agency staff are only used where alternatives cannot be sourced and patient safety is of concern. There is a rigorous process in place to ensure this resource is not used inappropriately, which is overseen by the hospital management team. Vacancies and Recruitment The number of vacancies for registered nursing across the service has increased further from reported at 18.3WTE in December 2016 to 20.1WTE in January 2017 and for care workers the vacancy figure has remained static at 3.65WTE. Recruitment in to the service continues on a rolling programme, with a further event having taken place on 03 February 2017; of the seven candidates shortlisted for interview (and having accepted) only one candidate attended. This individual was appointed and awaits a start date with the Trust. Interest remains low in relation to Leek Moorlands Hospital as the future of the service is thought by candidates to be uncertain. Sickness The average percentage sickness absence for January 2017 is reported at 4.99WTE (6.23%) for registered nurses and 4.72WTE (5.61%) for care workers. Although these figures have fallen slightly since December 2016, the impact on ability to meet planned staffing levels persists. The majority of sickness absence relates to short term sickness e.g. seasonal colds and flu like symptoms. Operational managers continue to work with HR colleagues to reduce sickness and support early return to work for these staff. Safety It has been necessary to close a bay on Grange Ward, to admissions, following identification of a further patient with influenza symptoms. The ward team recognised the symptoms at an early stage and implemented appropriate infection prevention and control measures in a timely manner. There has been no avoidable pressure damage reported within the community hospital services during January 2017. The NHS Safety Thermometer data for the service demonstrates a prevalence of No New Harms of 96.35%, which exceeds the 95% national target. There have been no patient safety issues reported during the month as a result of staffing issues. Recommendations The Trust Board is requested to:
1. To receive the report for January 2017 and be assured that the organisation is monitoring and mitigating issues relating to safe staffing establishments.

Hospital Ward Bed Numbers Green Amber Red RN - Day HCSW - Day RN - Night HSCW - Night RN HCSW Overall Day Night RN HCSW RN HCSWOnly 1 RN on
ShiftRN HCSW RN HCSW Vacancies - RN
Vacancies - HCSW
Posts appointed to but not yet
started
Maternity Leave
Sickness Professional Assurance Statement
Cottage 19 50 42 1 90.8% 100.9% 90.3% 112.9% 2.7 3.1 5.8 1:8 1:11 15.14 11.82 45 0 6 0 55 1% 4% 3.73 0.00 0.00 0.00
0.78 - HSCW(5.70%)
1.10 - RN (9.71%)
Safe staffing has been maintained during January 2017. There was one shift (Night) which was of professional concern (red) which also had only one
registered nurse on duty. There were five further shifts where there was only registered nurse on duty, all of which were night shifts but were not classed
as being of professional concern. All incidents arose as a result of permanent staff sickness and an inability to cover the shifts with another
registered nurse. Professional concern related to increased patient acuity and a reduction in staffing numbers. No patient safety incidents relating to
staffing were reported as a result of altered skill mix and number. Safety was maintained by staff from preceding shift working additional hours, use of additional care workers and repriotising work activities, whilst recieving
mutual aid from colleagues on site as necessary. Additional care workers have been utilised to support gaps in the rota where registered nurses could
not be sourced and to provide additional observation and monitoring for those at risk of falls.
Saddler 17 46 47 0 100.0% 99.8% 98.3% 102.8% 3.0 3.5 6.4 1:8 1:9 15.14 10.82 48 1 1 0 55 2% 1% 2.43 0.00 1.00 0.00
0.63 - HSCW(5.69%)
0.71 - RN (6.58%)
Safe staffing has been maintained during January 2017. There were no shifts which were of professional concern and one shift (Night) where there was only one registered nurse on duty, as a result of permanent staff sickness. On this occasion it was not possible to source alternative registered nurse
cover and an additional care worker was utilised. Safety was further maintained by repriotising work activities and support from colleagues on previous shift and those on site on another ward. There were no patient
safety incidents reported during the month. Additional care workers have been utilised to support gaps in the rota where registered nurses could not be sourced and to provide additional observation and monitoring for those at risk
of falls.
Total Leek 36 96 89 1 95.0% 100.3% 94.3% 107.5% 2.8 3.3 6.1 1:8 1:10 30.28 22.64 93 1 7 0 110 1% 3% 6.16 0.00 1.00 0.00
1.41 - HSCW(5.69%)
1.81 - RN (8.15%)
Broadfield 23 57 36 0 86.6% 104.5% 100.0% 98.4% 3.0 4.5 7.5 1:9 1:11 16.01 22.65 28 11 0 3 28 3% 5% 2.00 2.65 0.00 0.29
0.95- HSCW(5.27%)1.38- RN (8.99%)
Safe staffing has been maintained during January 2017. There were no shifts which were of professional concern or where there was only one registered
nurse on duty. Additional care workers have been utilised to support gaps in the rota where registered nurses could not be sourced and to provide
additional observation and monitoring for those at risk of falls.
Chatterley 21 83 10 0 96.7% 102.3% 100.0% 100.0% 2.8 4.3 7.1 1:8 1:12 16.85 15.80 4 3 0 22 37 12% 5% 4.79 1.00 0.00 0.00
0.42- HSCW(2.76%)
1.00 - RN (6.75%)
Safe staffing has been maintained during January 2017. There were no shifts which were of professional concern or where there was only one registered nurse on duty. Additional registered nurses and care workers have been
utilised to provide additional support at the end of life as well as further observation and monitoring for those at risk of falls.
Grange 32 10 80 3 98.6% 96.9% 100.0% 101.1% 3.1 3.6 6.7 1:7 1:10 22.54 19.22 8 1 0 0 89 0% 7% 4.35 0.00 1.00 0.00
0.00 - HSCW(0.00%)
0.00 - RN (0.00%)
Safe staffing has been maintained during January 2017. There were three shifts (1 x Early and 2 x Late) where professional concern was raised and no shifts where there was only one registered nurse on duty. Concerns related
to increased patient flow (admissions and discharges) and high levels of acuity amongst patient group. The ward has been closed due to an outbreak
of Influenza A during the month; the team identified potential infection and acted accordingly. There have been no patient safety incidents reported
relating to staffing levels during January 2017. Additional care workers have been utilised to support the increased patient care needs and support those
at risk of falls.
Scotia 10 83 10 0 99.2% 87.4% 100.0% NA 6.4 2.4 8.8 1:4 1:4 11.89 6.12 1 16 1 0 3 0% 2% 1.00 0.00 0.00 0.00
0.80- HSCW(12.62%)
0 - RN (0.00%)
Safe staffing has been maintained during January 2017. There were no shifts which were of professional concern and one shift (Late) where there was only one registered nurse on duty as the member of staff became unwell whilst on duty and was unable tpo continue with the shift. Support was recieved from
colleagues on site and there were no patient safety issues reported as a result of reduced staffing.
Sneyd 20 81 12 0 93.2% 100.2% 99.5% 96.8% 3.4 3.2 6.6 1:6 1:10 17.01 14.23 13 32 0 0 35 2% 3% 3.80 0.00 0.00 0.00
1.14 - HSCW(7.01%)
0.80 - RN (5.82%)
Safe staffing has been maintained during January 2017. There were no shifts which were of professional concern or where there was only one registered
nurse on duty. The ward has temporarily altered staffing figures on each late (+1) and night (-1) shift to improve efficiency and effectiveness. There have
been no patient safety incidents as a result of staffing levels or skill mix.
Total Haywood 126 314 148 3 94.9% 100.0% 99.9% 99.5% 3.3 3.8 7.1 1:7 1:9 84.30 78.02 54 63 1 25 192 4% 4% 13.94 3.65 1.00 0.29
3.31- HSCW(5.53%)
3.18 - RN (4.31%)
Overall
Total
274 410 237 4 94.9% 100.1% 98.5% 101.1% 3.2 3.6 6.8 1:7 1:9 114.58 100.66 147 64 8 25 302 3% 4% 20.10 3.65 2.00 0.29
4.72 - HSCW(5.61%)
4.99 - RN (6.23%)
Haywood
Jan-17
Number of shifts ABOVE agreed establishment
Safe Staffing (Community Hospitals)
Professional Judgement Monthly Fill Rate (NHS Choices) Staffing Ratios Low StaffingProfessional Assurance
Vacancies and Leave
No of shifts RAG rated by nurse in charge Actual V Rostered Staffing (Hours) Average RN to Patient RatioNumber of shifts BELOW agreed
establishment
High Staffing
WTEs vacant or not filled due to sickness/maternity leave
Leek
Agency StaffAverage % of Actual Staffing
Agency Staff
EstablishmentWard Establishment
(WTE)
Care Hours per Patient Day (CHPPD)
Number of patients v Number of Staffing Hours

Page 1 of 4
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST – TRUST BOARD
TO BE HELD ON: WEDNESDAY 22 FEBRUARY 2017
Subject: Quality Improvement Plan – Update Report
Strategic Goal (tick as appropriate):
We will provide high quality and safe services which provide an excellent experience and best possible outcomes
We will work with users and carers to deliver integrated services, simply and effectively
Our organisation will develop and deliver sustainable, innovative services that support independence
Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Rose Goodwin; Director of Nursing and Quality
Recommendation: For Approval & Assurance
For Discussion For Information PURPOSE OF THE REPORT: The report provides the Trust Board with an update on the progress of delivery against the Quality Improvement Plan including the testing of the evidence of outcomes of actions delivered. The report reviews the progress of actions due by the end of January 2017. There are no actions due by the end of February 2017, the Steering Group will focus on preparedness of a CQC revisit in Q1 of 2017-18. This report has previously been discussed at the Quality and Safety Committee on the 7 February. KEY POINTS: Further CQC Inspection The Trust is expecting an inspection visit in quarter 1 of 2017-18. CQC visits will now be smaller and more targeted than the previous comprehensive inspection the Trust received in 2015. CQC give four weeks’ notice of these inspections and will target inspections on areas that were previously rated inadequate. A twelve week readiness plan has been developed to focus on those areas that require an escalation or acceleration of actions to ensure that the improvement outcome required is delivered. The priority areas within this plan have been developed from the work of the CQC Steering Group both from assurance reviews against the Quality Improvement Plan and escalations identified by the group. Additionally work to brief staff and test their understanding of the changes in practice delivered within the Quality Improvement Plan forms part of this readiness plan. Assurance Review The Adult Community assurance review completed in December has now been shared with Divisions going to the South DBM on January. The areas requiring further assurance are:
• Staffing Levels in Community Adult Nursing – the Trust has an on-going programme of recruitment and targeting university graduates to fill staff nurse posts, due to a shortage of

Page 2 of 4
specialist trained community nurses development posts have been created to train these staff internally. Teams are using an updated e-community desktop system including the reporting of re-scheduled visits, an additional mobile application is awaiting development in February and is expected to be rolled out in March.
• Monitoring of rescheduled appointments – the upgraded version of e-community allows the recording and monitoring of rescheduled appointments with a monthly safer staffing dashboard produced for both internal review and external reporting to CQRM (commissioners).
• Review of caseloads and workloads of community nurses – a caseload review tool has been developed and is currently being piloted to support an objective and systematic review of caseloads through a supported caseload supervision process. Initial roll out has been met with enthusiasm by piloted staff.
• Sharing the learning of incidents and complaints – the Senior Leadership Team is currently reviewing the organisations processes for the dissemination of wider learning to standardise the approach for each level of the organisation.
• Medicines storage audits – the medicines management team are currently completing the audit of all community bases to identify compliance with storage of medicines requirements. This is expected to be completed by the end of March 2017.
Update There were 144 actions due for completion by the end of January 2017 of these:
• 88 are rated BLUE action complete with evidence of assurance • 51 are rated GREEN lead notification that action complete, assurance evidence required • 5 are rated AMBER due to partial completion or limited evidence of completion • There are no actions rated RED. (see Appendix: 2 (Quality Improvement Plan)).
The Amber rated Actions are identified below: Review and re-launch the training for Line Managers on how to manage staff concerns. WL09 – the Trust has training in place for all staff however currently training is not in place specifically for line managers to respond to staff concerns. The interim Ambassador for Cultural Change is currently exploring the use of an existing HEE training package for managers, and will meet with Director of Workforce in early February to agree the Trust approach. Sexual Health Services, Develop and implement a consistent and robust service-wide approach to triage: SH01 - Audit of compliance against triage SOP guidance – sexual health services are auditing compliance against this SOP with a plan for completion by the end of January 2017. End of Life Last Days of Life Care Plan EoL02 – action 2) Roll out of the last days of life care plan and 3) Deliver training programme – the end of life steering group has previously agreed to launch the care plan once 75% of community nursing staff are trained in its use. Additional training dates have been identified and a condensed one hour session has been developed to deliver in team bases to boost awareness in preparation. Currently Litchfield, Seisden and the Macmillan team are trained beyond the 75% threshold. Response times for EoL patients: EOL09 - Discuss and agree robust commissioning intentions with commissioners in relation to end of life care, including an agreed definition for fast tracked patients. – This action relates to the South division end of life services as the PCCC in the North has clear timescales for fast track within its service specification. The paused EOL Staffordshire commissioning programme was reinstated in December 2016 following a review by NHSE. The Trust is currently seeking clarity on the status of its original partnership bid approach. This forms part of the plan’s risk log.

Page 3 of 4
Changes to the Plan There has been one change to the plan since the last report (January) this is listed in appendix 1 below. INTER DEPENDENCIES: Legal and/or Risk Non-compliance with CQC could lead to legal action and reputational
damage
Clinical Non-compliance may pose risks for staff and service users
Financial Non-compliance may result in financial implications linked to litigation, reputational damage and loss of business. The issue of a warning notice precludes the Trust from applying for tenders.
HR Recommendations include workforce implications and associated actions
Staff and Trade Union involvement actions undertaken/planned
None Identified
Social Care The quality improvement plan is Trust wide and covers social care services within ILCT’s
Patient & Public Involvement
The CQC improvement plan takes account of service user and carer feedback and areas for improvement
Equality Impact None identified at this time
Information exempt from Disclosure
No
Requirement for further review
On-going and weekly updates will be provided to the Executive Leadership Team on an exception basis, with monthly board updates.
RECOMMENDATIONS: • The Trust Board is to note the update against the Quality Improvement Plan actions. • The Trust Board approves the proposed changes against the plan as identified in the decision
log.
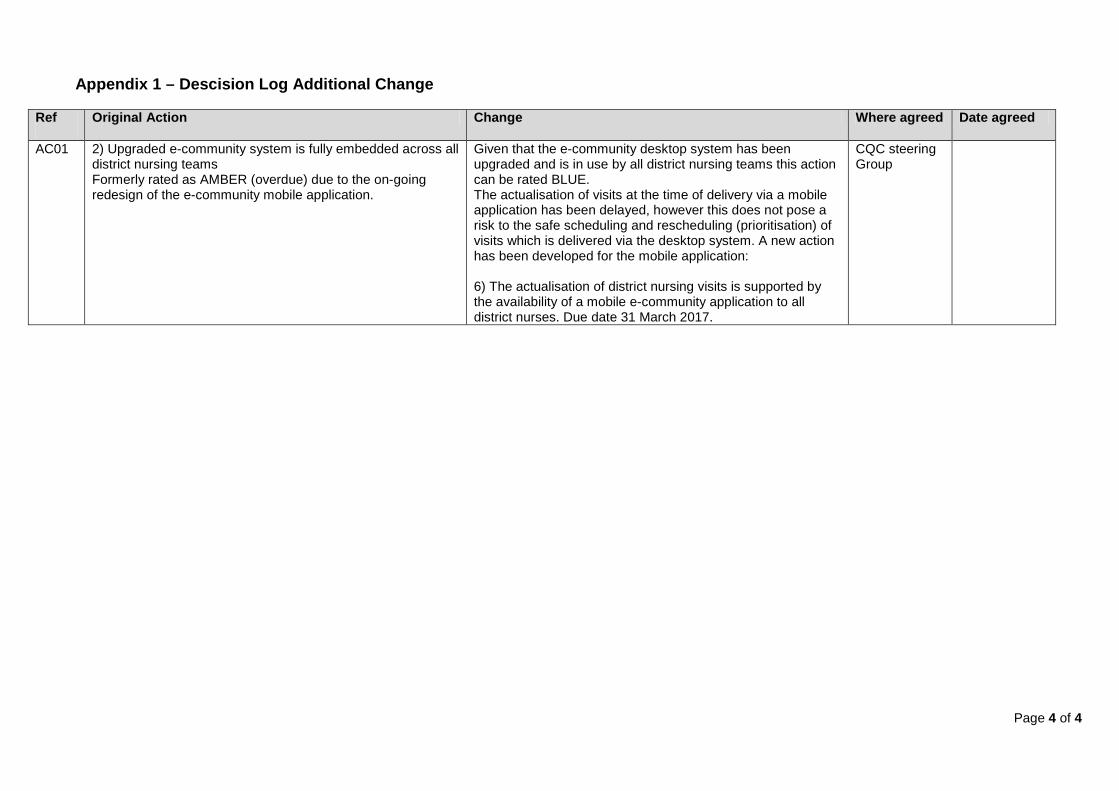
Page 4 of 4
Appendix 1 – Descision Log Additional Change
Ref
Original Action Change Where agreed Date agreed
AC01 2) Upgraded e-community system is fully embedded across all district nursing teams Formerly rated as AMBER (overdue) due to the on-going redesign of the e-community mobile application.
Given that the e-community desktop system has been upgraded and is in use by all district nursing teams this action can be rated BLUE. The actualisation of visits at the time of delivery via a mobile application has been delayed, however this does not pose a risk to the safe scheduling and rescheduling (prioritisation) of visits which is delivered via the desktop system. A new action has been developed for the mobile application: 6) The actualisation of district nursing visits is supported by the availability of a mobile e-community application to all district nurses. Due date 31 March 2017.
CQC steering Group
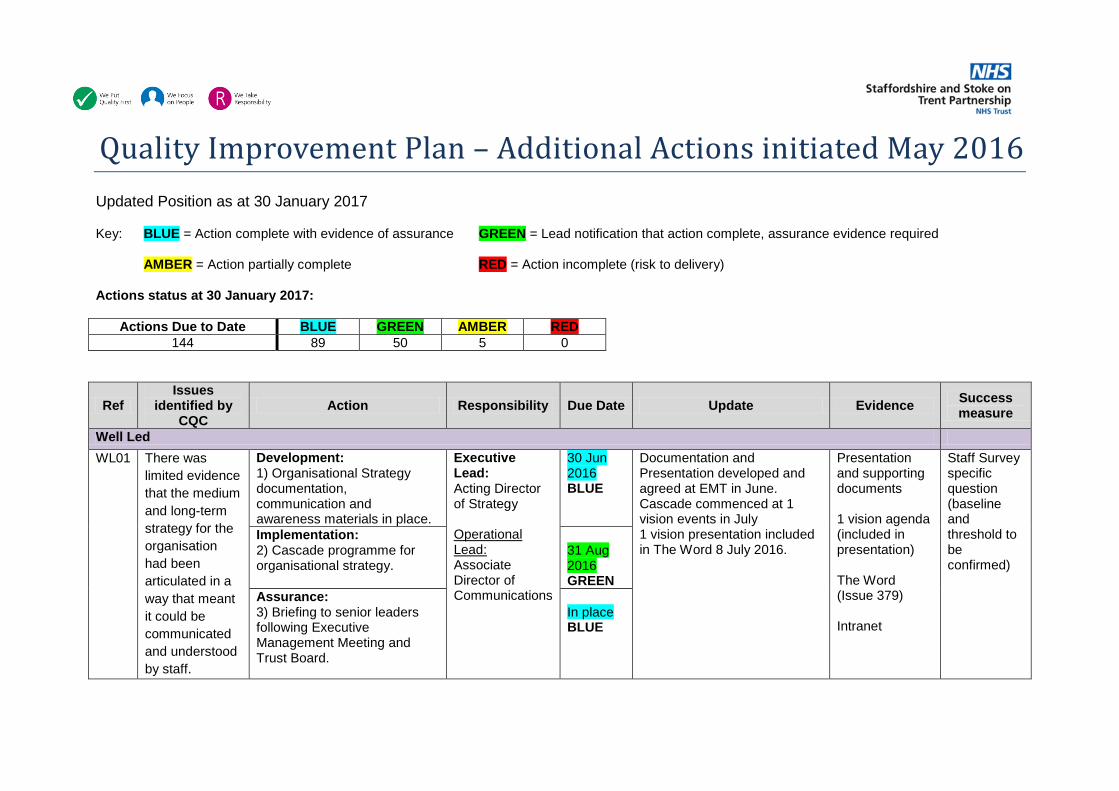
Quality Improvement Plan – Additional Actions initiated May 2016 Updated Position as at 30 January 2017
Key: BLUE = Action complete with evidence of assurance GREEN = Lead notification that action complete, assurance evidence required
AMBER = Action partially complete RED = Action incomplete (risk to delivery)
Actions status at 30 January 2017:
Actions Due to Date BLUE GREEN AMBER RED 144 89 50 5 0
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
Well Led WL01 There was
limited evidence that the medium and long-term strategy for the organisation had been articulated in a way that meant it could be communicated and understood by staff.
Development: 1) Organisational Strategy documentation, communication and awareness materials in place.
Executive Lead: Acting Director of Strategy Operational Lead: Associate Director of Communications
30 Jun 2016 BLUE
Documentation and Presentation developed and agreed at EMT in June. Cascade commenced at 1 vision events in July 1 vision presentation included in The Word 8 July 2016.
Presentation and supporting documents
1 vision agenda (included in presentation) The Word (Issue 379) Intranet
Staff Survey specific question (baseline and threshold to be confirmed)
Implementation: 2) Cascade programme for organisational strategy.
31 Aug 2016 GREEN
Assurance: 3) Briefing to senior leaders following Executive Management Meeting and Trust Board.
In place BLUE

2 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
WL02 Few staff we spoke with during the inspection understood the Trust values.
Implementation: 1) Agenda for Trust Board and Executive Management Team aligned to the Trust Values 2) Trust templates (e.g. powerpoint template) feature the Trust values. 3) Screen savers incorporate the Trust values 4) Team Brief (monthly news cascade to staff) is structured using the Trust values 5) Quarterly ‘1 Vision’ events revised to offer front line staff presentation of best practice, executive update organised around the Trust values. 6) Staff appraisal aligned to Trust values
Executive Lead: Director of Workforce Operational Lead: Associate Director of Communications
In place BLUE In place BLUE In place BLUE In place BLUE In place BLUE In place BLUE
Minutes of Board and EMT aligned to values. Templates of Trust documents on intranet pages. Team brief editions. 1 Vision events. Appraisal documentation and completion rate. Staff survey response.
Agenda Trust templates Screen savers Team Brief 1 vision presentation Appraisal paperwork
Staff Survey specific question (baseline and threshold to be confirmed) Quality Assurance Visit specific question
Assurance: 7) Test staff understanding through Quality Assurance Visit Programme
31 Mar 2017
WL03 Some services lacked a specific strategy that articulated the detailed objectives and plans for the
1) Service specific strategy development actions (see CYP02, DS01 and EOL01) 2) Align service strategies to commissioning strategies for Adult Community Services (MCP) and Children’s Services 3) Align service specific strategies to overarching Trust
Executive Lead: Acting Director of Strategy Operational Lead: Chief Operating Officers
Refer to CYP02, DS01, EOL01
Realigned structure Service specific strategy in place for each service element Strategies align to Trust overarching strategy
Staff can see a standardised approach to Trust strategies with the values identified throughout. Staff are engaged with
See CYP02, DS01, EOL01
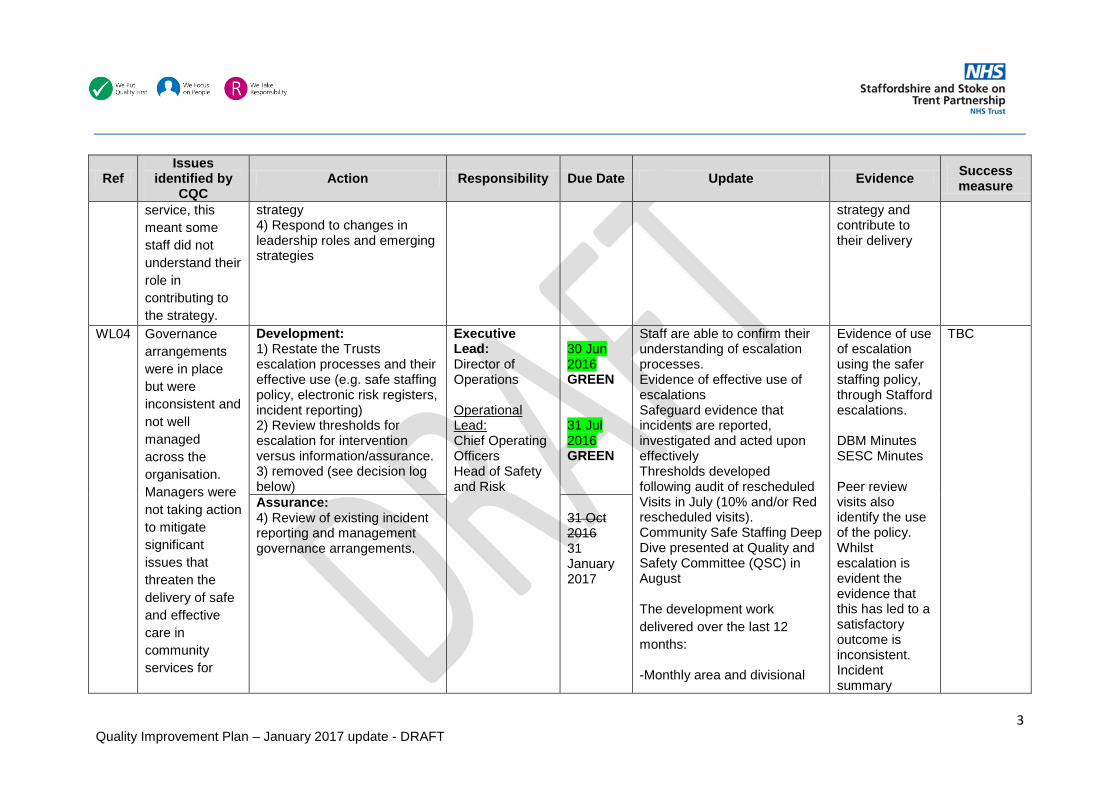
3 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
service, this meant some staff did not understand their role in contributing to the strategy.
strategy 4) Respond to changes in leadership roles and emerging strategies
strategy and contribute to their delivery
WL04 Governance arrangements were in place but were inconsistent and not well managed across the organisation. Managers were not taking action to mitigate significant issues that threaten the delivery of safe and effective care in community services for
Development: 1) Restate the Trusts escalation processes and their effective use (e.g. safe staffing policy, electronic risk registers, incident reporting) 2) Review thresholds for escalation for intervention versus information/assurance. 3) removed (see decision log below)
Executive Lead: Director of Operations Operational Lead: Chief Operating Officers Head of Safety and Risk
30 Jun 2016 GREEN 31 Jul 2016 GREEN
Staff are able to confirm their understanding of escalation processes. Evidence of effective use of escalations Safeguard evidence that incidents are reported, investigated and acted upon effectively Thresholds developed following audit of rescheduled Visits in July (10% and/or Red rescheduled visits). Community Safe Staffing Deep Dive presented at Quality and Safety Committee (QSC) in August The development work delivered over the last 12 months:
-Monthly area and divisional
Evidence of use of escalation using the safer staffing policy, through Stafford escalations. DBM Minutes SESC Minutes Peer review visits also identify the use of the policy. Whilst escalation is evident the evidence that this has led to a satisfactory outcome is inconsistent. Incident summary
TBC
Assurance: 4) Review of existing incident reporting and management governance arrangements.
31 Oct 2016 31 January 2017

4 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
adults. reports, with weekly summary to Executive Leadership Team. -Incidents reported through the Quality Scorecard at divisional and Trust level, and through the community nursing safer staffing dashboard. -Strengthened Duty of Candour reporting and monitoring. -Quality Assurance Visits assess the incident reporting and governance arrangements at a team level.
A sample of incidents of all harm levels is currently under review. This includes patient death through the MRG process, moderate harm and above through DoC and PURG processes, and low/no harm incidents through local sign off processes. Review in line for completion at the end of January, results to be reported through the CQC steering group.
commenced 28 June to EMT, reported to SLT from 12 July 16 Deep Dive Report QGC Agenda/Minutes Quality Visit Reports

5 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
WL05 There were not robust systems or processes to assess, monitor and improve the quality and safety of services.
Implementation: 1) Revised Audit programme for 2016-17 focussing on assurance 2) Systems for monitoring, investigation and learning from incidents through: Pressure Ulcer Review Group, Falls Review Group, Infection Prevention Committee. 3) Integrated quality and performance reporting to Board 4) Quality Assurance Visit programme
Executive Lead: Director of Nursing and Quality Operational Lead: Associate Director of Quality
In place BLUE In place BLUE 30 Jun 2016 BLUE In place BLUE
Audit programme monitored monthly through PAG. Actions from incident review groups including lessons. Trust Board Minutes reporting integrated quality and performance report. Integrated Reporting to Board (June Board) Outcome reports and actions from Quality visits.
Audit Programme Continuous improvement cycle for quality through; monitoring, review, and learning. Lessons are communicated to key staff and services to reduce risk of impact on quality. Board Report and Minutes (June 16) Quality Assurance Visit schedule
Outcomes and learning from incidents, complaints, audit and quality visits
Assurance: 5) Update reports on the outcomes of learning from incidents, complaints, audit and quality visits to be presented to Divisional Business Meetings and Quality and Safety Committee.
TBC
WL06 Few of the issues identified during this inspection were
Development: 1) The Trust has a multi-layered approach to its electronic risk register from service to Board
Executive Lead: Director of Nursing and Quality
In place BLUE
Electronic risk registers. Service level, DBM, and executive risk management committee minutes considering registered risks
Systems for registering, escalating, mitigating and monitoring risk
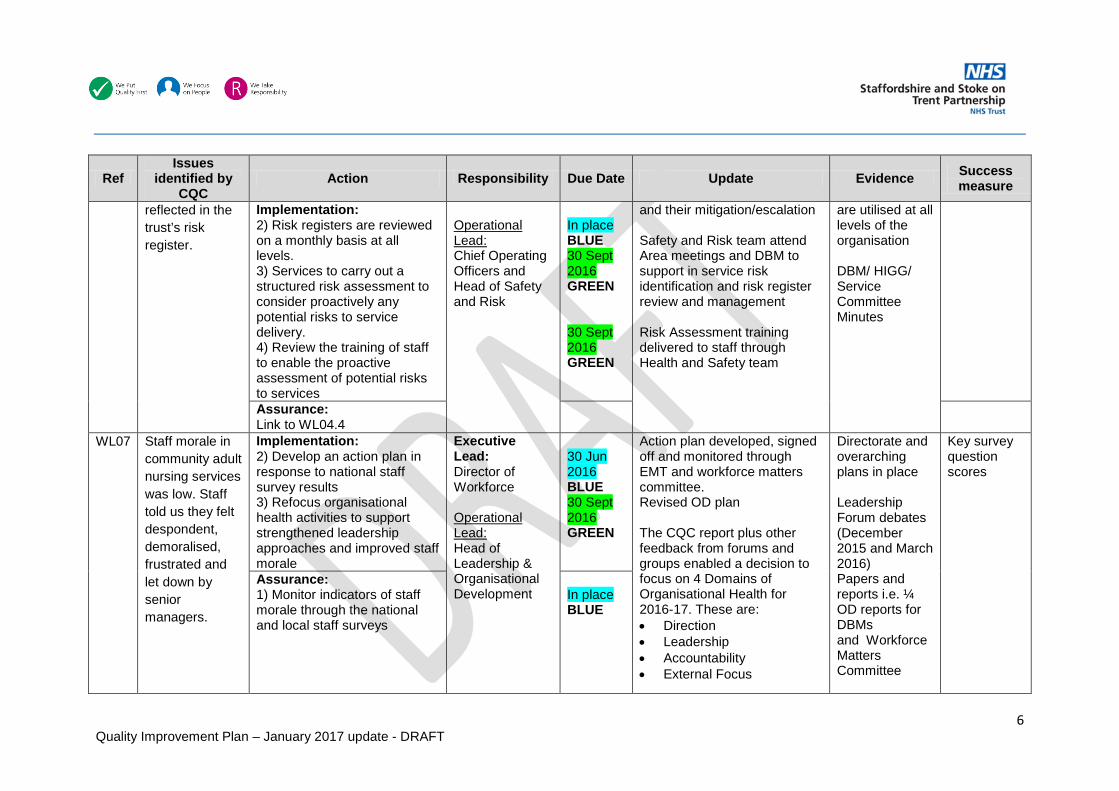
6 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
reflected in the trust’s risk register.
Implementation: 2) Risk registers are reviewed on a monthly basis at all levels. 3) Services to carry out a structured risk assessment to consider proactively any potential risks to service delivery. 4) Review the training of staff to enable the proactive assessment of potential risks to services
Operational Lead: Chief Operating Officers and Head of Safety and Risk
In place BLUE 30 Sept 2016 GREEN 30 Sept 2016 GREEN
and their mitigation/escalation Safety and Risk team attend Area meetings and DBM to support in service risk identification and risk register review and management Risk Assessment training delivered to staff through Health and Safety team
are utilised at all levels of the organisation DBM/ HIGG/ Service Committee Minutes
Assurance: Link to WL04.4
WL07 Staff morale in community adult nursing services was low. Staff told us they felt despondent, demoralised, frustrated and let down by senior managers.
Implementation: 2) Develop an action plan in response to national staff survey results 3) Refocus organisational health activities to support strengthened leadership approaches and improved staff morale
Executive Lead: Director of Workforce Operational Lead: Head of Leadership & Organisational Development
30 Jun 2016 BLUE 30 Sept 2016 GREEN
Action plan developed, signed off and monitored through EMT and workforce matters committee. Revised OD plan The CQC report plus other feedback from forums and groups enabled a decision to focus on 4 Domains of Organisational Health for 2016-17. These are: • Direction • Leadership • Accountability • External Focus
Directorate and overarching plans in place Leadership Forum debates (December 2015 and March 2016) Papers and reports i.e. ¼ OD reports for DBMs and Workforce Matters Committee
Key survey question scores
Assurance: 1) Monitor indicators of staff morale through the national and local staff surveys
In place BLUE

7 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
Each domain has actions agreed by the Organisational Health Group. Staff Morale being monitored through the 9 questions used in the Staff Survey and repeated in Staff FFT Q1. Where scores have been low, this has been investigated and actions identified as part of local action plans.
Staff engagement scores ( Staff Survey 2015, FFT Q1 July 2016) Staff Survey Action Plans
WL08 The visibility of Trust executives (other than the Chief Executive) and senior management was inconsistent.
Development: 1) Revise executive and senior leadership visits, including non-executive involvement to offer a co-ordinated approach against the directory of services. 2) Update the Trusts Directory of Services
Executive Lead: Chief Executive Officer Operational Lead: Associate Director of Communications
30 Jun 2016 BLUE 30 Jun 2016 BLUE
Executive visits in place on Fridays managed by EA team Updated Manual Directory of services in place. Non-Executive Directors are invited to join quality assurance visits.
Visits schedule Manual Directory of Services updated
Executive team coverage via executive visits, one vision events
Enabler Action: 3) Maintain the Trusts Directory of Services utilising an automated process linked to ESR.
Operational Lead: To be confirmed
31 Mar 2017
WL09 Ensure a strong leadership focus on the
Development: 1) Revised internal processes for raising concerns.
Executive Lead: Chief Executive Officer
In place (15 Mar 2016)
The policy has been approved by: • Policy Group 19 August
Policy document Trust Board
TBC

8 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
challenges faced in delivering care with a consistent response to staff concerns.
2) Review of internal policy for raising concerns
Operational Lead: Company Secretary
GREEN 31 Jul 2016 BLUE
2016 • Joint Staff Partnership 7
September 2016 • Quality & Safety
Committee 12 October 2016
• Trust Board 30 November 2016
Intranet page has been updated. Staff informed in July’s Team Brief Ambassador for Cultural Change role has been aligned to the national Freedom to Speak Up Guardian. New ‘Freedom to Speak up’ campaign launch and poster circulated to DBMs in September. Featured in The Word through August and September. There is a training package on ESR for Freedom to Speak Up which is aimed at all NHS staff. The Trust is exploring the use of an existing HEE training package for managers, meeting in diary on 1 Feb to
minutes Team Brief Intranet The Word New campaign launch and poster
Implementation: 3) Re-launch the Ambassador for Cultural Change role in line with the national Freedom to Speak up Guardian guidance. 4) Review and re-launch the training for Line Managers on how to manage staff concerns. 5) All routes for raising concerns to be reinforced including incident reporting, professional leads, HR, line managers and union representatives.
31 Oct 2016 BLUE 31 Oct 2016 AMBER 31 Oct 2016 GREEN
Assurance: 6) Regular Report into Trust
Board
In place BLUE

9 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
discuss this with Director of Workforce. Escalation and raising concerns is picked up as part of the quality assurance visits. Response from staff indicates awareness and use of these processes.
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
Children’s Services CYP01 Must - Ensure
that staff have regular access to appraisals in order for them to develop their skills and competency.
Development/Implementation: 1) New appraisal process in place in 16-17 annual cycle of completion between April and July for all appraisals
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
31 Jul 2016 BLUE
At 30 November the reported compliance rate for CYP was 94.35%.
Training compliance report DBM Minutes WM Minutes
Appraisal compliance rate above 90%
Assurance: 2) Compliance is monitored on a monthly basis at Executive Management Team, Children's Leadership Meeting and DBM, and Workforce Matters (two monthly)
31 Jul 2016 BLUE

10 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
CYP02 Must - Ensure that there is a clear vision and strategy for CYP services linked to the trust strategy and it is shared and understood by all staff in the service
Development: 1) Complete Children’s service redesign programme 2) Completion of Strategy and vision forms a work stream of the redesign programme
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
30 Sept 2016 28 February 2017 30 Sept 2016 28 February 2017 30 Sept 2016 31 March 2017
Given the complexities of the associated commissioning changes to the Trusts CYP services the development of a strategy has been difficult, Engagement with staff is now complete. Engagement with external stakeholders will take place throughout December and January. Expectation of completion of final draft strategy is end of January.
Staff are clear of and can contribute to the strategic direction of the service
TBC
Implementation: 3) Communication of strategy to Staff Assurance:
CYP03 Must - Ensure that there is a medicines policy developed specifically for children to ensure medicines are prescribed, managed and administered in a safe way.
Development: 1) Amend the Trusts Medicines management policy to offer Children specific guidance. 2) Ratify policy - Medicines Management Committee and SESC
Executive Lead: Medical Director Operational Lead: Chief Pharmacist
31 May 2016 BLUE 30 Jun 2016 BLUE
Policy has been revised to include children’s specific guidance. Signed off at SESC 9 June 2016. Uploaded to Document Library. Included in updated policies in August’s Team Brief
SESC Minutes (June) Policy has been uploaded to Document Library Team Brief August
TBC
Implementation: 3) Circulate policy amendments to Children services
31 Jul 2016 BLUE
Assurance:

11 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
CYP04 Must - Undertaken a full analysis of staff requiring safeguarding training for children above level 1 reflecting
Development: 1) Revise Training Needs Analysis and cross reference this with line managers 2) Ratify Level 2 training in an e-learning package 3) Review Training data pathway for ESR compatibility
Executive Lead: Director of Nursing and Quality Operational Lead: Children’s
All 30 Jun 16 1) BLUE 2) BLUE 3) GREEN
Level 2 training is available via ESR. Pathways have been reviewed by the Training Team and Children’s Safeguarding Team. All ESR system changes have been put into place with the
ESR training (OLM) eLearning package screenshot DBM and Workforce
Training compliance against each identified safeguarding children level – target 90%

12 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
the requirements of the Royal College of Paediatrics and Child Health “Safeguarding Children and Young people: roles and competences for health care staff”, Intercollegiate Document.
Assurance: 4) Monthly training compliance report for levels 2 and above, to DBM and QGC
Safeguarding Lead
30 Jun 16 4) GREEN
delay currently sitting with the Children Safeguarding team who are required to update ESR with those staff who have received training in levels 2 and above. All records have been updated on ESR and reports can now be run. Further work is needed to ensure reports pull out all eligible courses and to embed this in to statutory and mandatory reports. Expected in November. Work has been completed and compliance reports pull out all eligible courses. As of November, training compliance is: Safeguarding Children Level 2: 55% compliant Safeguarding Children Level 3: 62% compliant Training compliance reports still group levels 1-3; awaiting confirmation as to when these will be reported separately. Reports will then be sent to managers to check for accuracy and to identify and support those staff outstanding.
Matters minutes

13 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
CYP05 Must- Ensure care pathways or arrangements for transition to adult services for children with complex needs are developed.
Implementation: 1) Children have an Education Health and Care Plan on a needs led basis, transition from old statement approach (LA led) 2) Individual Needs are supported to transition on a case by case basis, through multi-agency approaches
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
In place GREEN In Place GREEN
All children who require one have an Education Health and Care Plan Evidence of person centred transition of health and social care need Escalation process agreed and in place
Children continue to receive services appropriate to their needs as they transition into adulthood
TBC
Development: 3) Develop a mechanism for escalating issues through a multi-provider clinical escalation approach
31 Mar 2017
Assurance:
CYP06 Must -Ensure that staff are up to date with their mandatory training requirements
Central action for all services – Development/Implement: 1) Compliance report is sent monthly from ESR and checked by managers for accuracy. 2) Removed (duplicate)
Executive Lead: Director of Workforce Operational
31 Jul 2016 GREEN
Training compliance is reported monthly, average compliance rate for CYP 92.81% at 30 November.
Monthly compliance reports and DBM, WM minutes.
Mandatory training compliance – Target 90%

14 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
and that compliance is monitored on a regular basis to ensure compliance is maintained.
Assurance: 3) Compliance is monitored monthly at; Divisional Business Meeting, and Workforce Matters
Lead: Chief Operating Officer
31 Jul 2016 BLUE
ESR Compliance
CYP07 Should - Clarify the funding arrangements for consumables for families of patients who require complex care packages.
Implementation: 1) The Trust will transfer the continuing healthcare service to SSSFT in July 2016 2) Confirmation sought from Commissioners re. funding arrangements for consumables, (Commissioners confirmed that cost is their responsibility in March 2016) 3) Arrangements in place through CCG for the provision of consumables
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer, Neighbourhood Manager Children’s Services
31 Jul 2016 BLUE 31 Mar 2016 BLUE In place BLUE
Transfer of service. TUPE date 01.07.16 Funding agreement in place Service no longer delivered within the Trust
TUPE Transfer of the service has superseded previous actions
CYP08 Should - Ensure that there is a documented
Implementation: 1) Documentation in place for monitoring anaphylaxis kits.
Executive Lead: Director of
30 Apr 2016
Immunisation teams have a procedure and associated documentation to monitor
To be tested TBC
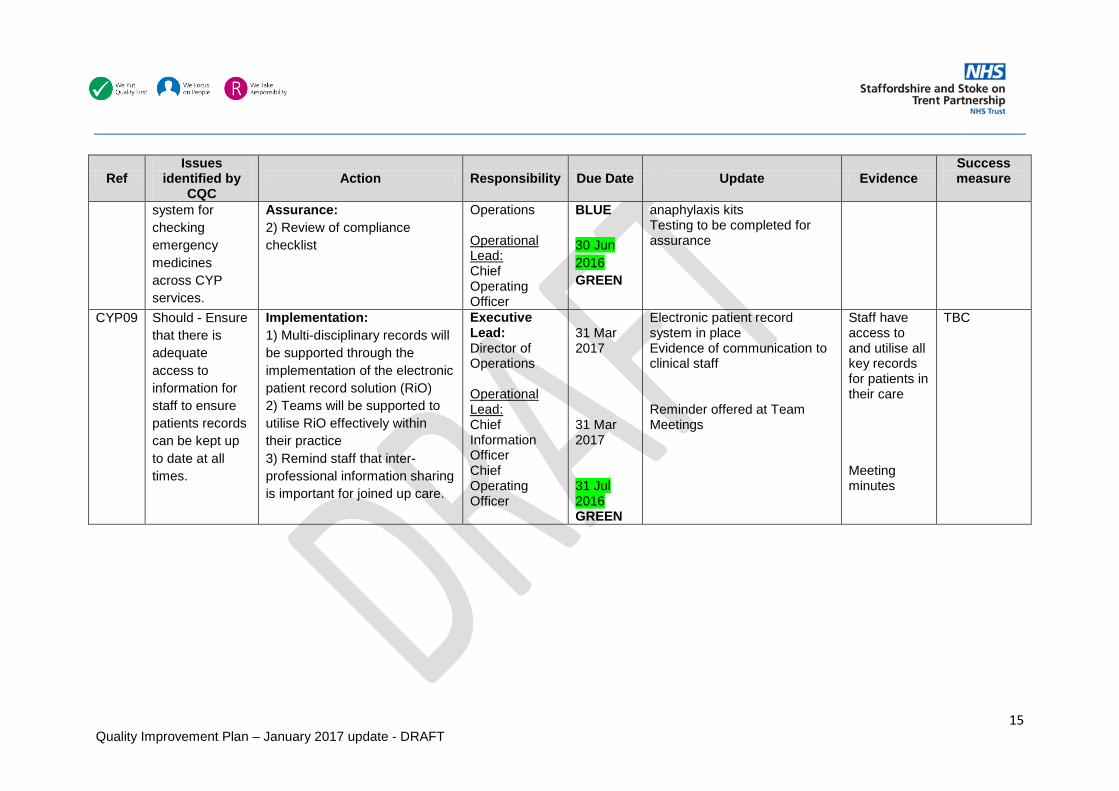
15 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success measure
system for checking emergency medicines across CYP services.
Assurance: 2) Review of compliance checklist
Operations Operational Lead: Chief Operating Officer
BLUE 30 Jun 2016 GREEN
anaphylaxis kits Testing to be completed for assurance
CYP09 Should - Ensure that there is adequate access to information for staff to ensure patients records can be kept up to date at all times.
Implementation: 1) Multi-disciplinary records will be supported through the implementation of the electronic patient record solution (RiO) 2) Teams will be supported to utilise RiO effectively within their practice 3) Remind staff that inter-professional information sharing is important for joined up care.
Executive Lead: Director of Operations Operational Lead: Chief Information Officer Chief Operating Officer
31 Mar 2017 31 Mar 2017 31 Jul 2016 GREEN
Electronic patient record system in place Evidence of communication to clinical staff Reminder offered at Team Meetings
Staff have access to and utilise all key records for patients in their care Meeting minutes
TBC

16 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
Sexual Health Services SH01 Must - Develop
and implement a consistent and robust service-wide approach to triage, which meets national guidelines and ensures patients can access services in a safe and timely manner.
Development: 1) Develop Triage SOP and sign off at Business committees and DBM
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
31 May 2016 BLUE
A process has been created to test and monitor the implementation and the use of SOPs within the service. The testing will be carried out by a team of peer reviewers from another SHS on an annual rotational basis. The process and the template were agreed in principle at the Lifestyle’s Managers Meeting on 16 November 2016. Reviews will start in December and all services will have been reviewed by January 2017. Triage, Partner Notification, and Medicines Management will all be audited in the first cycle.
Team meeting minutes (Evidence of cascade) For testing
Compliance against SOP – Target TBC
Implementation: 2) Implement SOPs in practice
30 Jun 2016 GREEN
Assurance: 3) Audit of compliance against SOP guidance
30 Nov 2016 AMBER
SH02 Must - The trust must ensure that patients and the public were not put at risk by ensuring that all post-test contact systems were properly
Implementation: 1) Formalise a manual system in Leicester to monitor all samples sent against results returned to ensure that no specimens are lost 2) Implementation of INFORM (electronic) system across all Sexual health services (agreed by the Trust, awaiting
Executive Lead: Director of Operations Operational Lead: Chief Information Officer Chief
In place BLUE 31 Mar 2017
Manual system evidences the return of all samples. Quality Assurance Visit took place 24 November 2016, manual system observed. Funding from NHSI secured for INFORM system; implementation currently scheduled for end of March
Specimens are monitored and services users receive treatment where needed.
Performance KPI – target TBC
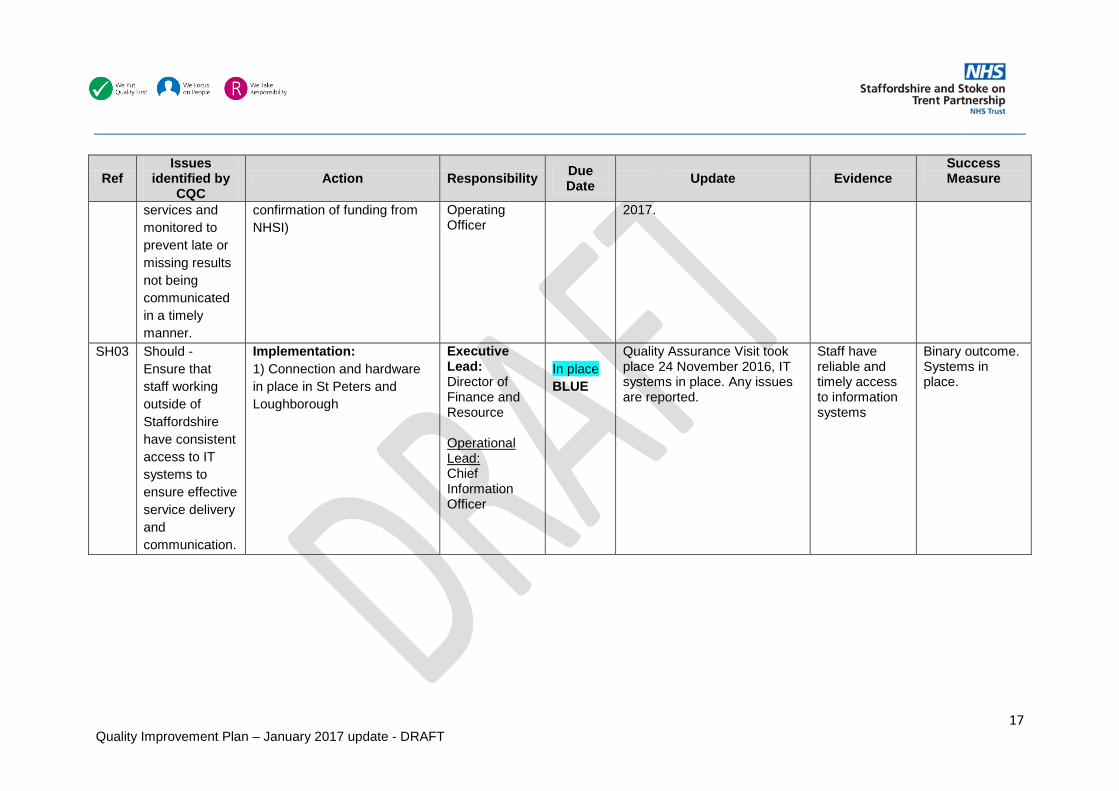
17 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
services and monitored to prevent late or missing results not being communicated in a timely manner.
confirmation of funding from NHSI)
Operating Officer
2017.
SH03 Should - Ensure that staff working outside of Staffordshire have consistent access to IT systems to ensure effective service delivery and communication.
Implementation: 1) Connection and hardware in place in St Peters and Loughborough
Executive Lead: Director of Finance and Resource Operational Lead: Chief Information Officer
In place BLUE
Quality Assurance Visit took place 24 November 2016, IT systems in place. Any issues are reported.
Staff have reliable and timely access to information systems
Binary outcome. Systems in place.
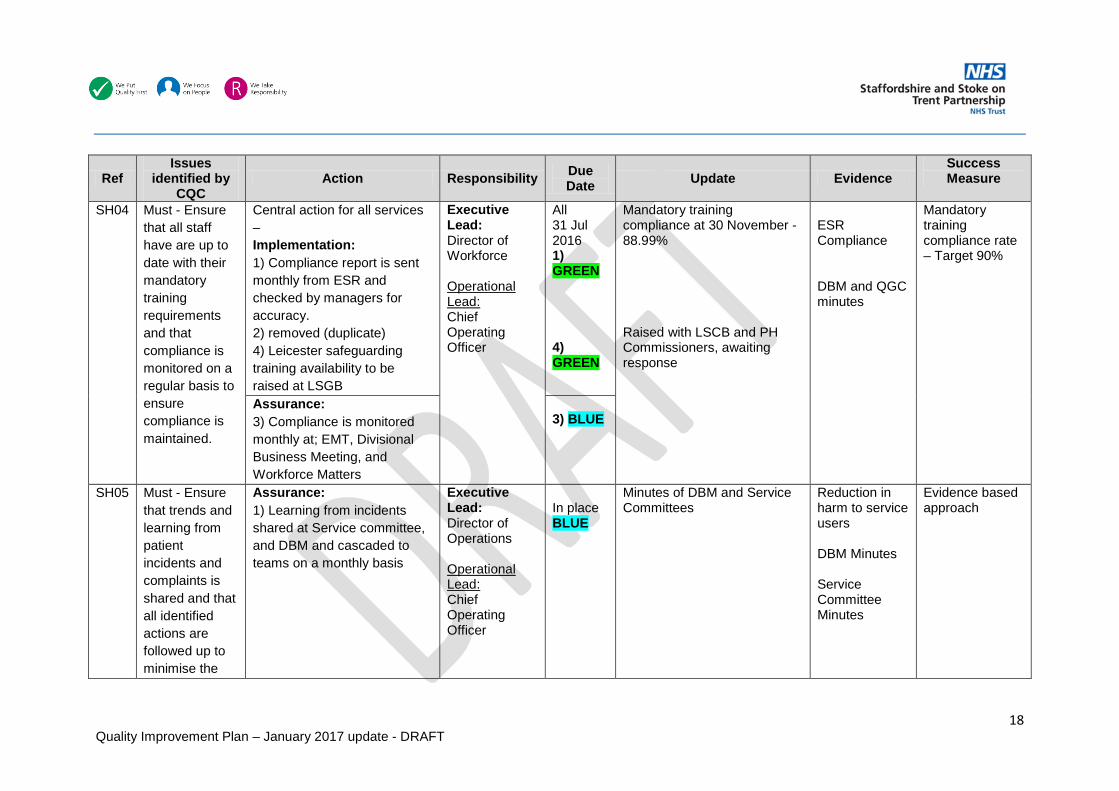
18 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
SH04 Must - Ensure that all staff have are up to date with their mandatory training requirements and that compliance is monitored on a regular basis to ensure compliance is maintained.
Central action for all services – Implementation: 1) Compliance report is sent monthly from ESR and checked by managers for accuracy. 2) removed (duplicate) 4) Leicester safeguarding training availability to be raised at LSGB
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
All 31 Jul 2016 1) GREEN 4) GREEN
Mandatory training compliance at 30 November - 88.99% Raised with LSCB and PH Commissioners, awaiting response
ESR Compliance DBM and QGC minutes
Mandatory training compliance rate – Target 90%
Assurance: 3) Compliance is monitored monthly at; EMT, Divisional Business Meeting, and Workforce Matters
3) BLUE
SH05 Must - Ensure that trends and learning from patient incidents and complaints is shared and that all identified actions are followed up to minimise the
Assurance: 1) Learning from incidents shared at Service committee, and DBM and cascaded to teams on a monthly basis
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
In place BLUE
Minutes of DBM and Service Committees
Reduction in harm to service users DBM Minutes Service Committee Minutes
Evidence based approach

19 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
likelihood of reoccurrence and improve care.
SH06 Must - Establish systems to monitor the number of patients who are not seen on first visit, including the types of service they tried to engage with so that they can improve services in those areas.
Implementation: 1) Local system of monitoring patients who choose to leave before being seen, including the offering of further appointments.
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
All 30 Jun 2016 1) GREEN 2) GREEN
Monitoring in place. Draft report developed by performance. Reported to DBM via each area exception report.
DBM exception reports DBM Minutes
Local Performance KPI – Target TBC
Assurance: 2) Monitored at Service committee, and DBM on a monthly basis
SH07 Must - Review staffing levels to ensure that the numbers and skill mix of staff are able to meet the demands of the
Implementation: 1) Leicester demand and capacity analysis complete to understand demands on the service 2) Presentation of outcome of analysis to Commissioners 3) Roll out demand and
Executive Lead: Director of Operations Operational Lead: Chief Operating
31 Jul 2016 BLUE 31 Jul 2016 BLUE
LLR Demand and Capacity Analysis complete and presented outcome of analysis to Commissioners. Demand and capacity analysis has been completed for the North Staffordshire and South Staffordshire services.
LLR Demand and Capacity Analysis Presentation to Commissioners DBM Minutes
Reporting of the rate of service users leaving without being seen is a proxy measure for demand/capacity balance.

20 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
service and patients are able to access care in a safe and timely manner
capacity analysis to North and South Staffordshire services
Officer 30 Sept 2016 BLUE On-going GREEN
Service Committee Minutes Assurance:
4) Continue to monitor waiting times KPIs through service committees and DBM with reporting to commissioners on a monthly basis
SH08 Must - The trust must ensure that governance systems are in place which enable managers to monitor and compare performance both within the trust and nationally.
Assurance: 1) Monthly Monitoring of performance through service committees and DBM, with performance reporting and escalation to local commissioners 2) Complete analysis of the available national standards/benchmark data to identify what can be reported.
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
In place BLUE
30 Sept 2016 BLUE
Minutes of service committees and DBM Each of our sexual health services contribute to national data sets through activity uploads. This in turn generates local authority area sexual health profile reports which allow us to nationally and locally benchmark.
Performance and Quality can be measured and is maintained DBM Minutes Service Committee Minutes Sexual health profiles
Results shown within benchmarking reports – target TBC

21 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
SH09 Must - Undertaken a full analysis of staff requiring safeguarding training for children above level 1 reflecting the requirements of the Royal College of Paediatrics and Child Health “Safeguarding Children and Young people: roles and competences for health care staff”, Intercollegiate Document.
Implementation: 1) Revise Training Needs Analysis and cross reference this with line managers 2) Ratify Level 2 training in an e-learning package 3) Review Training data pathway for ESR compatibility
Executive Lead: Director of Nursing and Quality Operational Lead: Children’s Safeguarding Lead
All 30 Jun 2016 1) BLUE 2) BLUE 3) GREEN
Level 2 training is available via ESR Pathways have been reviewed by the Training Team and Children’s Safeguarding Team. All ESR system changes have been put into place with the delay currently sitting with the Children’s Safeguarding team who are required to update ESR with those staff who have received training in levels 2 and above. All records have been updated on ESR and reports can now be run. Further work is needed to ensure reports pull out all eligible courses and to embed this in to statutory and mandatory reports. Expected in November. Work has been completed and compliance reports pull out all eligible courses. As of November, training compliance is:
ESR training (OLM) eLearning package screenshot TNA – safeguarding leads DBM and QGC minutes
Training compliance against each identified safeguarding children level – target 90%
Assurance: 4) Monthly training compliance report for levels 2 and above, to DBM and QGC
4) GREEN

22 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
Safeguarding Children Level 2: 55% compliant Safeguarding Children Level 3: 62% compliant Training compliance reports still group levels 1-3; awaiting confirmation as to when these will be reported separately. Reports will then be sent to managers to check for accuracy and to identify and support those staff outstanding.
SH10 Should - Ensure that all staff have regular access to appraisals in order for them to develop their skills and competency.
Implementation: 1) New appraisal process in place in 16-17 annual cycle of completion between April and July for all appraisals
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
31 Jul 2016 GREEN
At 30 November the reported compliance rate for SH was 93.28%,
Monthly compliance reports and meeting minutes ESR Compliance DBM Minutes
Appraisal compliance rate above 90%
Assurance: 2) Compliance is monitored on a monthly basis at EMT, Service Committee and DBM, and Workforce Matters (two monthly)
31 Jul 2016 BLUE

23 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
Dental Services DS01 Should - The
service should ensure that the vision and strategy for the service is fully developed and articulated to staff, with clear objectives for the service.
Development: 1) Develop Vision and Strategy 2) Sign off through Dental STM and DBM
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer Clinical Director
31 July 2016 BLUE 31 Aug 2016 BLUE
Dental Strategy presented to Professional Reference Group on 21 July 2016 Presented at North and specialist DBM and agreed in September 2016. The dental teams have been engaged in the development of the working draft. Formal awareness was raised through a launch in December at staff meetings – 13th December for South teams and 15th December for North teams. Email disseminated to all staff issuing the strategy and accompanying presentation.
Minutes of PRG Minutes of North and Specialist DBM September 2016 Minutes of staff December meetings Dissemination email
TBC
Implementation: 3) Raise awareness through staff group
31 Dec 2016 BLUE

24 Quality Improvement Plan – January 2017 update - DRAFT
DS02 Should - The service should ensure that staff have are up to date with their mandatory training requirements and that compliance is monitored on a regular basis to ensure compliance is maintained.
Central action for all services – Implementation: 1) Compliance report is sent monthly from ESR and checked by managers for accuracy. 2) Reporting includes all levels of adult and children’s safeguarding.
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
All 31 Jul 2016 1) GREEN 2) GREEN 3) BLUE
Mandatory training compliance at 30 November – 95.30% All ESR system changes have been put into place with the delay currently sitting with the Children Safeguarding team who are required to update ESR with those staff who have received training in levels 2 and above. All records have been updated on ESR and reports can now be run. Further work is needed to ensure reports pull out all eligible courses and to embed this in to statutory and mandatory reports. Expected in November. Work has been completed and compliance reports pull out all eligible courses. As of November, training compliance is:
Training compliance reports, meeting minutes ESR Compliance DBM Minutes
Mandatory training compliance rate – Target 90%

25 Quality Improvement Plan – January 2017 update - DRAFT
Assurance: 3) Compliance is monitored monthly at; EMT, Divisional Business Meeting, and Workforce Matters
Safeguarding Children Level 2: 55% compliant Safeguarding Children Level 3: 62% compliant Training compliance reports still group levels 1-3; awaiting confirmation as to when these will be reported separately. Reports will then be sent to managers to check for accuracy and to identify and support those staff outstanding.
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
Adult Community Services AC01 Must - Ensure
staffing levels in community adult nursing are sufficient to ensure that patients receive safe and
Development: 1) Upgrade of e-community system to deliver capacity and demand information. This is key to monitoring and managing capacity and demand in district nursing services.
Executive Lead: Director of Operations Operational Lead: Chief Information
30 Sept 2016 GREEN
The App has been withdrawn from use as of beginning of November 2016. This is currently in the process of being rewritten and is not likely to be available until February 2017. The Desktop version of e-community is still in use across community
Quality Assurance Peer Review Visit reports Rescheduled visit SOP Service
Outcome of bi-annual safe staffing review (contractual requirement)

26 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
effective care in a timely way and that this is continually reviewed using a systematic approach to determining the number of staff and range of skills required.
Implementation: 2) Upgraded e-community system is fully embedded across all district nursing teams 3) Rescheduled appointments are monitored manually by community nursing teams 4) Monthly exception report to Divisional Business Meeting identifying rescheduled visits including the impact on patients 5) Continued recruitment processes utilising the Trust’s nursing recruitment strategy 6) The actualisation of district nursing visits is supported by the availability of a mobile e-community application to all district nurses.
Officer Chief Operating Officer
30 Sept 2016 BLUE 31 May 2016 BLUE 31 Jul 2016 GREEN On-going GREEN 31 March 2017
nursing services. Spreadsheet in place and standardised process implemented. Community Safer Staffing Dashboard is submitted monthly from November to include the percentage of rescheduled visits and any associated harms. Rescheduled visit SOP guidance developed and shared with teams. Divisions report that the monitoring of rescheduled visits is in place. Escalation reports are offered to DBMs. Audit in August identified variance in the documents in use escalated to operational leads for resolution.
Committee and DBM Minutes Community Safer Staffing Dashboard
AC02 Must - Ensure that policies and procedures in relation to Duty of Candour
Assurance: 1) Monitor the on-going delivery of duty of candour training 2) Culture of delivery and levels of defensiveness tested during quality visits. 3) Monitor of individual cases
Executive Lead: Director of Nursing and Quality Operational Lead:
All On-going 1) BLUE 2) BLUE 3) GREEN
Outcomes of reviews by internal audit and KPMG to test the effectiveness of the Duty of Candour process have been received. A Duty of Candour deep dive exercise was presented to Quality and Safety Committee in October
Monitoring reports Direct feedback from staff
Contractual reporting of breaches Evidence from Quality assurance visits

27 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
support a culture of openness and transparency and all staff have received appropriate training and there arrangements in place to support staff involved in a Duty of Candour incident.
through the risk team process Chief Operating Officer Head of Quality Governance Head of Risk
2016. Duty of Candour policy is currently under review.
AC03 Must - Monitor response times to urgent and routine appointments within community adult services and monitor the number and frequency of
Aligned to AC01 above Implementation: 1) Review response time criteria in service specifications 2) Develop systems to monitor response times aligned to the roll out of the electronic patient record system (RiO)
Executive Lead: Director of Operations Operational Lead: Chief Operating Officers
30 Sept 2016 BLUE 31 Mar 2017
Development of response times standards across community services Stafford & Cannock service specification is party to a contract variation to adopt for all remaining CCGs in the South.
DN Service Specification SES & Seisdon
Performance KPI in place

28 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
cancelled appointments to ensure patients receive care in a timely manner.
AC04 Must - Review arrangements for compliance with the MCA and improve staff competence to discharge their responsibilities under the Act.
Assurance: 1) On-going monitoring of monthly training compliance 2) Review of the effectiveness of training in supporting staff in practice (focus group) 3) Audit of Consent practice quarterly
Executive Lead: Director of Nursing and Quality Operational Lead: Chief Operating Officer Head of Quality Governance
All 31 Jul 2016 1) BLUE 2) BLUE 3) BLUE
Adult Community training compliance rates at 30 November – 92.22% (GREEN). Pilot review of training completed feeding into an iterative Quarterly audit process. Q1 consent audit identified that 92% of records audited had written evidence that consent was sought.
Training compliance report MCA Pilot report Consent Audit (June 2016)
Training compliance – Target 90%
AC05 Must - Review arrangements for handover between teams to ensure this is effective and staff are able to manage the risks to people using services.
Development: 1) Handover SOP to be signed off at DBMs in May 2016
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
31 May 2016 BLUE
SOP signed off at DBMs in June, cascaded to teams Handover SOP utilised in practice. Feedback from teams given to developers
DBM minutes To be assessed by peer review visits. DBM minutes
Evidence from Quality assurance visits Consider compliance audit
Implementation: 2) Implementation of the SOP across all community teams
31 Jul 2016 GREEN

29 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
AC06 Must - Review caseloads and workloads of staff in the community adult teams to ensure that the significant issues that threatened the delivery of safe and effective care and addressed and mitigated.
Aligned to AC01 Implementation: 1) Develop caseload supervision and management process for community staff 2) Support staff through master class programme 3) Embed caseload supervision and management
Executive Lead: Director of Operations Operational Lead: Chief Operating Officers Professional Leads
31 Oct 2016 GREEN 31 Oct 2016 GREEN 31 March 2017
Evidence through the peer reviews and quality assurance visits show that teams are utilising handover to deliver peer caseload supervision. Through the North Division and Stafford escalation processes, caseload cleansing has taken place. Masterclasses and associated guidance were held in November, one in the North and one in the South; staff members were able to review the caseload review tool in its’ testing phase (launch will be in early January 2017).
Staff feel effectively supported to manage their caseloads
Assurance Audit outcome
AC07 Should - Review and improve storage of medicines to ensure they are appropriately and safely stored.
Assurance: 1) Medicines storage audit undertaken in all teams annually.
Executive Lead: Medical Director Operational Lead: Clinical Director Pharmacy Services
31 Mar 2017
Outcome of Audit and remedial actions
Medicines storage meets regulatory requirements
Outcome of medicines storage audit in community settings

30 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
AC08 Should - Review the quality of record keeping in adult community services to ensure patients records are maintained to ensure risks are managed.
Development: 1) Record keeping audit revised to monitor the quality of records through assessment planning delivery and evaluation
Executive Lead: Director of Nursing and Quality Operational Lead: Chair of Records Management Group Audit Manager
31 Jul 2016 BLUE
Audit of documentation quality developed with focussed pilot to test effectiveness. Pilot carried out and report available. Amended tool developed following pilot which has been disseminated to teams. Launch held 7 October 2016 for audit. Discussed at DBMs on 25 October 2016. All information from the launch, including presentation and tool available on the intranet. Data collection has been carried out for Quarter 3. Report will be available in January.
Audit documentation Pilot results
Outcome of quality of record audit
Implementation/Assurance: 2) Roll out of revised audit
31 Oct 2016 GREEN
AC09 Must - Ensure a strong leadership focus on the challenges faced in delivering care with a consistent response to staff concerns.
See WL09 Executive Lead: Chief Executive Officer Operational Lead: Company Secretary

31 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
AC10 Must - Ensure that all staff have are up to date with their mandatory training requirements and that compliance is monitored on a regular basis to ensure compliance is maintained.
Central action for all services – Implementation: 1) Compliance report is sent monthly from ESR and checked by managers for accuracy. 2) Reporting includes all levels of adult and children’s safeguarding.
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
31 Jul 2016 GREEN 31 Jul 2016 GREEN
Mandatory training compliance for the service - 89.08% at 30 November. All ESR system changes have been put into place with the delay currently sitting with the Children Safeguarding team who are required to update ESR with those staff who have received training in levels 2 and above. All records have been updated on ESR and reports can now be run. Further work is needed to ensure reports pull out all eligible courses and to embed this in to statutory and mandatory reports. Expected in November. Work has been completed and compliance reports pull out all eligible courses. As of November, training compliance is: Safeguarding Children Level 2: 55% compliant Safeguarding Children Level 3: 62% compliant
Training compliance reports, meeting minutes DBM Minutes
Mandatory training compliance rate – Target 90%
Assurance: 3) Compliance is monitored monthly at; EMT, Divisional Business Meeting, and Workforce Matters
31 Jul 2016 BLUE

32 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
Training compliance reports still group levels 1-3; awaiting confirmation as to when these will be reported separately. Reports will then be sent to managers to check for accuracy and to identify and support those staff outstanding.
AC11 Must - Ensure that all staff have regular access to appraisals in order for them to develop their skills and competency.
Implementation: 1) New appraisal process in place in 16-17 annual cycle of completion between April and July for all appraisals
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
31 Jul 2016 BLUE
At 30 November the reported compliance rate for Adult Community was 90.58%.
Monthly compliance reports and meeting minutes ESR Compliance DBM Minutes
Appraisal Compliance – Target 90%
Assurance: 2) Compliance is monitored on a monthly basis at EMT, DBM, and Workforce Matters (two monthly)
31 Jul 2016 BLUE
AC12 Must - Ensure that learning from patient incidents and complaints is shared and that all identified actions are followed up to
Implementation: 1) Learning from Incidents and complaints features fed through DBM and service meetings 2) Learning from lessons available through the publication of lessons to staff
Executive Lead: Director of Operations Operational Lead: Chief Operating Officers
On-going BLUE 30 Sept 2016 GREEN
Minutes of DBM Team leader forum inaugural meeting in October, learning will be built into this quarterly programme. The Word will include shared learning case studies. Shared learning alerts will be cascaded through Safeguard
DBM Reports and Minutes Area Reports
Evidence based approach
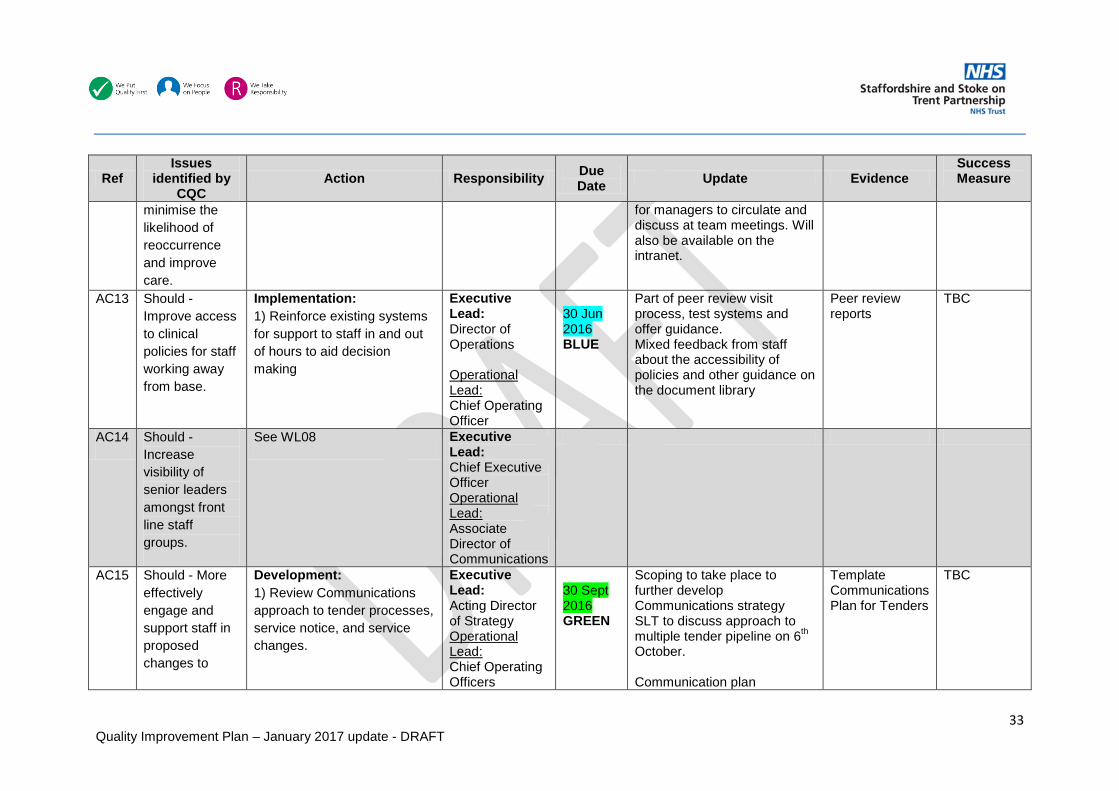
33 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
minimise the likelihood of reoccurrence and improve care.
for managers to circulate and discuss at team meetings. Will also be available on the intranet.
AC13 Should - Improve access to clinical policies for staff working away from base.
Implementation: 1) Reinforce existing systems for support to staff in and out of hours to aid decision making
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
30 Jun 2016 BLUE
Part of peer review visit process, test systems and offer guidance. Mixed feedback from staff about the accessibility of policies and other guidance on the document library
Peer review reports
TBC
AC14 Should - Increase visibility of senior leaders amongst front line staff groups.
See WL08 Executive Lead: Chief Executive Officer Operational Lead: Associate Director of Communications
AC15 Should - More effectively engage and support staff in proposed changes to
Development: 1) Review Communications approach to tender processes, service notice, and service changes.
Executive Lead: Acting Director of Strategy Operational Lead: Chief Operating Officers
30 Sept 2016 GREEN
Scoping to take place to further develop Communications strategy SLT to discuss approach to multiple tender pipeline on 6th October. Communication plan
Template Communications Plan for Tenders
TBC

34 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence
Success Measure
service configuration and their role within the service.
AD Communications
documentation has been developed to support the engagement of staff and stakeholders in service change/tenders North and South Divisions have completed a service mapping exercise to inform an updated Directory of Services – 02 Dec 16.
Implementation: 2) Directory of Services using common language and service structure across the Trust Linked to WL08.3
To be confirmed
31 Mar 2017
AC16 Should - Review the process for completing Root Cause Analysis investigations to ensure they consistent and an action plan is developed.
Implementation: 1) RCA investigation officer training, with co-investigator process until competent 2) Incident reporting template revised 3) Action planning
Executive Lead: Director of Nursing and Quality Operational Lead: Head of Nursing Head of Safety and Risk
30 Sept 2016 BLUE 30 Sept 2016 BLUE 30 Sept 2016 BLUE
Trained LI register Investigation template revised and completed and delivered with Investigating Officer training RCA Investigating Officer training developed and now provided monthly – bookable via e-learning Action plan template complete – embedded into investigation template
Investigation template Action plan template Training available on ESR
Outcome of RCA reviews at PURG and Falls review Group
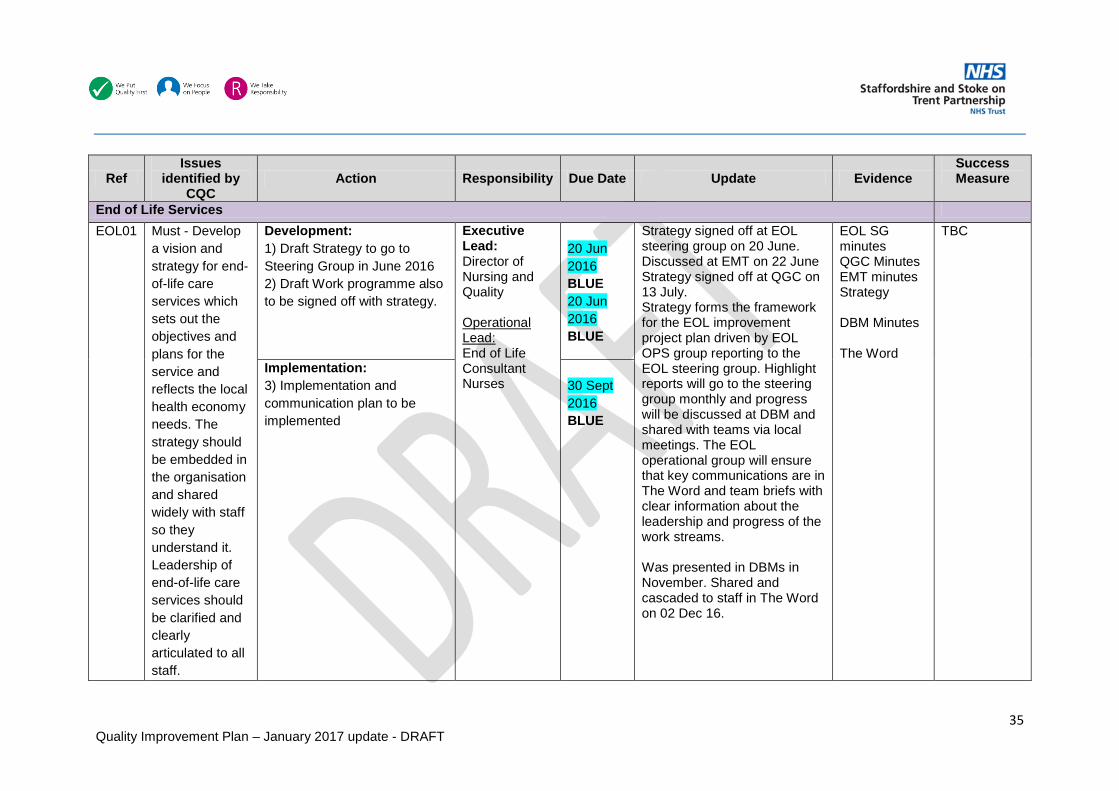
35 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
End of Life Services EOL01 Must - Develop
a vision and strategy for end-of-life care services which sets out the objectives and plans for the service and reflects the local health economy needs. The strategy should be embedded in the organisation and shared widely with staff so they understand it. Leadership of end-of-life care services should be clarified and clearly articulated to all staff.
Development: 1) Draft Strategy to go to Steering Group in June 2016 2) Draft Work programme also to be signed off with strategy.
Executive Lead: Director of Nursing and Quality Operational Lead: End of Life Consultant Nurses
20 Jun 2016 BLUE 20 Jun 2016 BLUE
Strategy signed off at EOL steering group on 20 June. Discussed at EMT on 22 June Strategy signed off at QGC on 13 July. Strategy forms the framework for the EOL improvement project plan driven by EOL OPS group reporting to the EOL steering group. Highlight reports will go to the steering group monthly and progress will be discussed at DBM and shared with teams via local meetings. The EOL operational group will ensure that key communications are in The Word and team briefs with clear information about the leadership and progress of the work streams. Was presented in DBMs in November. Shared and cascaded to staff in The Word on 02 Dec 16.
EOL SG minutes QGC Minutes EMT minutes Strategy DBM Minutes The Word
TBC
Implementation: 3) Implementation and communication plan to be implemented
30 Sept 2016 BLUE

36 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
EOL02 Must - Ensure care planning documentation is properly completed.
Development: 1) Last Days of Life Care Plan documentation signed off and printed
Executive Lead: Director of Nursing and Quality Operational Lead: End of Life Consultant Nurses
31 Jul 2016 BLUE
Documentation developed As agreed at EOL Steering Group, 75% of staff are to be training before roll out of the plan. Due to staffing escalations in the North, attendance on training has been affected. Additional sessions have been planned and training has been condensed and delivered in practice to improve uptake. The target is for 75% of frontline staff (excluding long term sick and maternity leave) to be trained by the third week in January and by the fourth week for staff at the Haywood Hospital. Within the South, staff outstanding the training are currently being identified along with additional training dates (throughout January and February). Partially complete: Early engagement with the
Patients in their last days of life are appropriately supported Copy of Last Days of Life Care Plan documentation
Outcome of compliance audit
Implementation: 2) Roll out of the use of the Care Plan document 3) Deliver training programme for key staff in its use 4) Engagement with Primary Care – documentation to LMC, CCG, and Educational Leads (GP), NHSE
31 Oct 2016 AMBER 31 Oct 2016 AMBER 31 Oct 2016 GREEN
Assurance: 5) Audit cycle to assure the quality of implementation supported by local CQUIN scheme
31 Mar 2017

37 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
health economy via CCG DoN to commence wider engagement. Proposed link through MCP groups. Communication with wider stakeholders in particular GP’s has received positive feedback to date, further communication with GP locality boards and CCG lead is planned over the next few months.
EOL03 Must - Ensure that DNACPR practice across the trust is consistent, the effectiveness of the DNACPR policy and procedures and regularly reviewed and audited.
Assurance: 1) Quarterly DNACPR and MCA compliance audit.
Executive Lead: Medical Director Operational Lead: Chief Operating Officers
31 Jul 2016 BLUE
Outcome of Audit and improvement actions Average audit compliance rate is 97.5% in community teams, 92.5% in community hospitals.
Patients receive the appropriate care Audit of DNACPR (June 2016)
Outcome of assurance audits
EOL04 Must - Review arrangements for compliance with the MCA and improve
Assurance: 1) On-going monitoring of monthly training compliance 2) Review of the effectiveness of training in supporting staff in
Executive Lead: Director of Nursing and Quality
31 Jul 2016 BLUE 31 July 2016
Overall Trust compliance for MCA training at 30 November – 93.02% (GREEN). Pilot review of training completed feeding into an iterative Quarterly audit
Training reports
Outcome of assurance audit
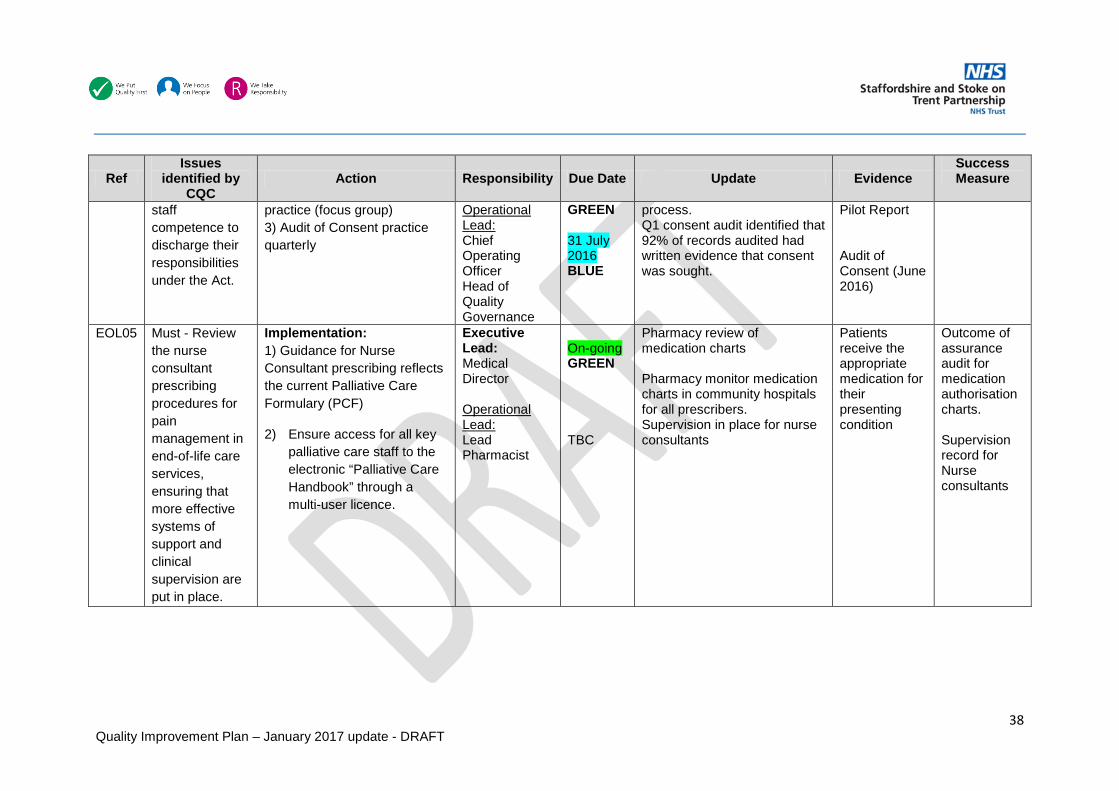
38 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
staff competence to discharge their responsibilities under the Act.
practice (focus group) 3) Audit of Consent practice quarterly
Operational Lead: Chief Operating Officer Head of Quality Governance
GREEN 31 July 2016 BLUE
process. Q1 consent audit identified that 92% of records audited had written evidence that consent was sought.
Pilot Report Audit of Consent (June 2016)
EOL05 Must - Review the nurse consultant prescribing procedures for pain management in end-of-life care services, ensuring that more effective systems of support and clinical supervision are put in place.
Implementation: 1) Guidance for Nurse Consultant prescribing reflects the current Palliative Care Formulary (PCF)
2) Ensure access for all key palliative care staff to the electronic “Palliative Care Handbook” through a multi-user licence.
Executive Lead: Medical Director Operational Lead: Lead Pharmacist
On-going GREEN TBC
Pharmacy review of medication charts Pharmacy monitor medication charts in community hospitals for all prescribers. Supervision in place for nurse consultants
Patients receive the appropriate medication for their presenting condition
Outcome of assurance audit for medication authorisation charts. Supervision record for Nurse consultants
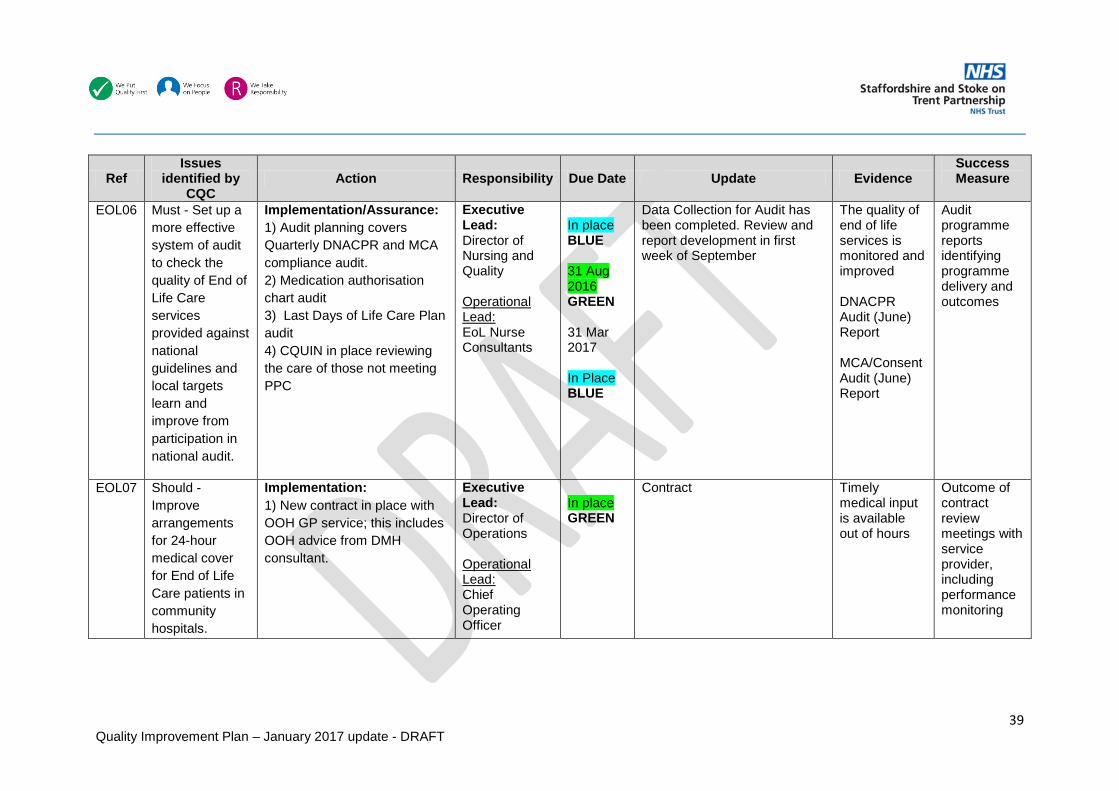
39 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
EOL06 Must - Set up a more effective system of audit to check the quality of End of Life Care services provided against national guidelines and local targets learn and improve from participation in national audit.
Implementation/Assurance: 1) Audit planning covers Quarterly DNACPR and MCA compliance audit. 2) Medication authorisation chart audit 3) Last Days of Life Care Plan audit 4) CQUIN in place reviewing the care of those not meeting PPC
Executive Lead: Director of Nursing and Quality Operational Lead: EoL Nurse Consultants
In place BLUE 31 Aug 2016 GREEN 31 Mar 2017 In Place BLUE
Data Collection for Audit has been completed. Review and report development in first week of September
The quality of end of life services is monitored and improved DNACPR Audit (June) Report MCA/Consent Audit (June) Report
Audit programme reports identifying programme delivery and outcomes
EOL07 Should - Improve arrangements for 24-hour medical cover for End of Life Care patients in community hospitals.
Implementation: 1) New contract in place with OOH GP service; this includes OOH advice from DMH consultant.
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
In place GREEN
Contract Timely medical input is available out of hours
Outcome of contract review meetings with service provider, including performance monitoring
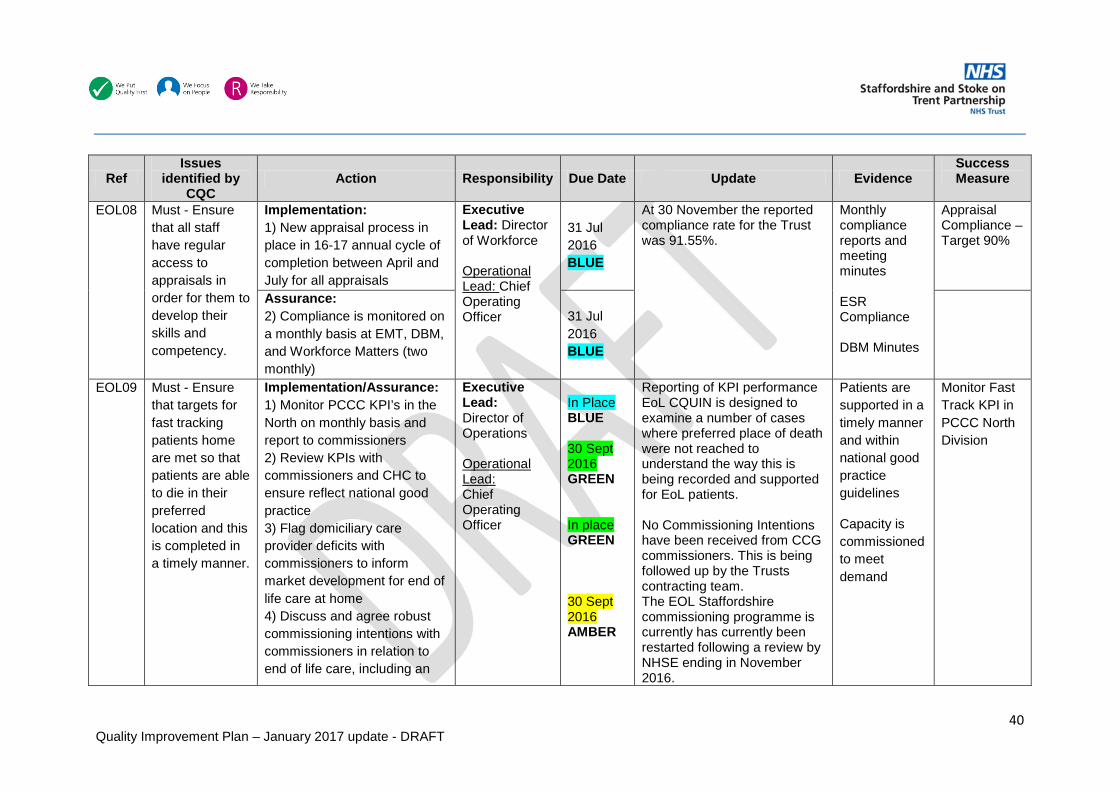
40 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
EOL08 Must - Ensure that all staff have regular access to appraisals in order for them to develop their skills and competency.
Implementation: 1) New appraisal process in place in 16-17 annual cycle of completion between April and July for all appraisals
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
31 Jul 2016 BLUE
At 30 November the reported compliance rate for the Trust was 91.55%.
Monthly compliance reports and meeting minutes ESR Compliance DBM Minutes
Appraisal Compliance – Target 90%
Assurance: 2) Compliance is monitored on a monthly basis at EMT, DBM, and Workforce Matters (two monthly)
31 Jul 2016 BLUE
EOL09 Must - Ensure that targets for fast tracking patients home are met so that patients are able to die in their preferred location and this is completed in a timely manner.
Implementation/Assurance: 1) Monitor PCCC KPI’s in the North on monthly basis and report to commissioners 2) Review KPIs with commissioners and CHC to ensure reflect national good practice 3) Flag domiciliary care provider deficits with commissioners to inform market development for end of life care at home 4) Discuss and agree robust commissioning intentions with commissioners in relation to end of life care, including an
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
In Place BLUE 30 Sept 2016 GREEN In place GREEN 30 Sept 2016 AMBER
Reporting of KPI performance EoL CQUIN is designed to examine a number of cases where preferred place of death were not reached to understand the way this is being recorded and supported for EoL patients. No Commissioning Intentions have been received from CCG commissioners. This is being followed up by the Trusts contracting team. The EOL Staffordshire commissioning programme is currently has currently been restarted following a review by NHSE ending in November 2016.
Patients are supported in a timely manner and within national good practice guidelines
Capacity is commissioned to meet demand
Monitor Fast Track KPI in PCCC North Division
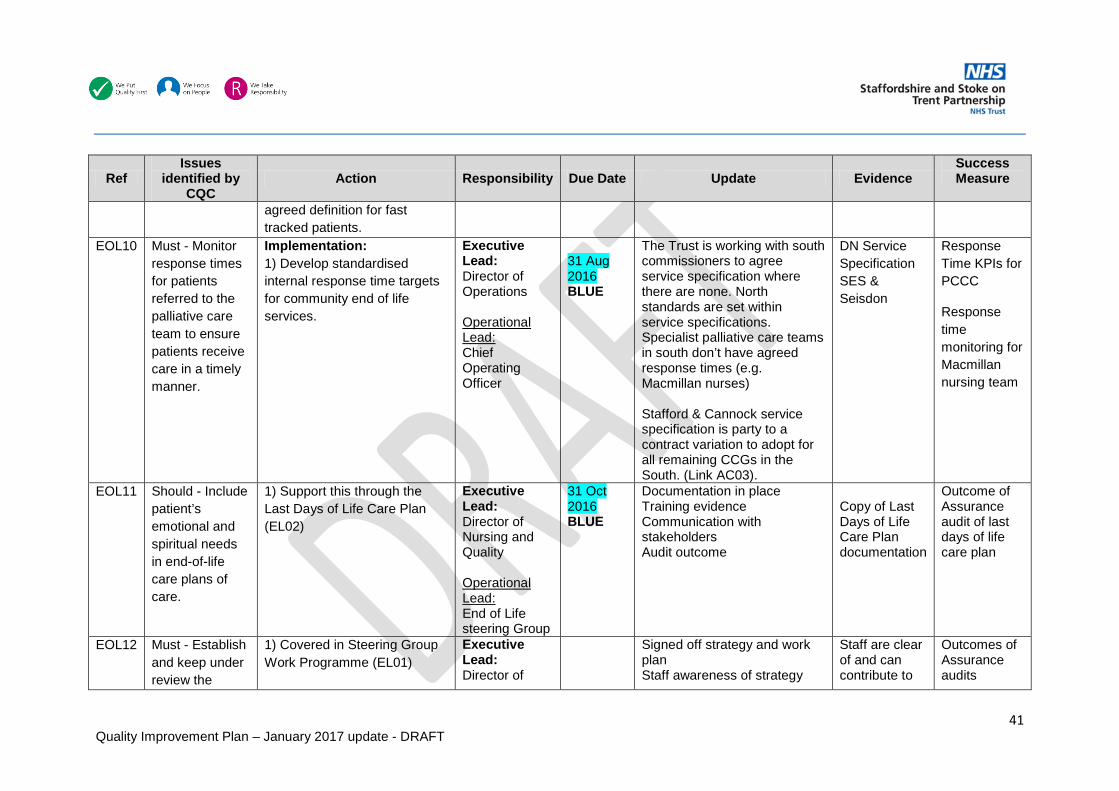
41 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
agreed definition for fast tracked patients.
EOL10 Must - Monitor response times for patients referred to the palliative care team to ensure patients receive care in a timely manner.
Implementation: 1) Develop standardised internal response time targets for community end of life services.
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
31 Aug 2016 BLUE
The Trust is working with south commissioners to agree service specification where there are none. North standards are set within service specifications. Specialist palliative care teams in south don’t have agreed response times (e.g. Macmillan nurses) Stafford & Cannock service specification is party to a contract variation to adopt for all remaining CCGs in the South. (Link AC03).
DN Service Specification SES & Seisdon
Response Time KPIs for PCCC
Response time monitoring for Macmillan nursing team
EOL11 Should - Include patient’s emotional and spiritual needs in end-of-life care plans of care.
1) Support this through the Last Days of Life Care Plan (EL02)
Executive Lead: Director of Nursing and Quality Operational Lead: End of Life steering Group
31 Oct 2016 BLUE
Documentation in place Training evidence Communication with stakeholders Audit outcome
Copy of Last Days of Life Care Plan documentation
Outcome of Assurance audit of last days of life care plan
EOL12 Must - Establish and keep under review the
1) Covered in Steering Group Work Programme (EL01)
Executive Lead: Director of
Signed off strategy and work plan Staff awareness of strategy
Staff are clear of and can contribute to
Outcomes of Assurance audits

42 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
operation of systems and processes to more effectively monitor and improve the quality and safety of End of Life Care services.
Nursing and Quality Operational Lead: End of Life Consultant Nurses
and work plan the strategic direction of end of life care
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
Community Inpatient Services CH01 Must - The trust
must ensure that learning for incidents is shared across all community hospitals and that all identified actions are followed up to minimise the likelihood of
Implementation: 1) Incidents and their learning are shared via HIGG meeting, cascaded to ward leadership level for team meetings.
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
In Place BLUE
Learning from complaints and incidents are presented to HIGG
HIGG minutes
Evidence based approach

43 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
reoccurrence and improve care.
CH02 Must - The trust must ensure that staff have are up to date with their mandatory training requirements and that compliance is monitored on a regular basis to ensure compliance is maintained.
Central action for all services – Implementation: 1) Compliance report is sent monthly from ESR and checked by managers for accuracy. 2) Reporting includes all levels of adult and children’s safeguarding.
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
31 Jul 2016 GREEN 31 Jul 2016 GREEN
Mandatory training compliance 81.42% as of 30 November. All ESR system changes have been put into place with the delay currently sitting with the Children Safeguarding team who are required to update ESR with those staff who have received training in levels 2 and above. All records have been updated on ESR and reports can now be run. Further work is needed to ensure reports pull out all eligible courses and to embed this in to statutory and mandatory reports. Expected in November. Work has been completed and compliance reports pull out all eligible courses. As of November, training compliance is: Safeguarding Children Level 2: 55% compliant
Training compliance reports, meeting minutes ESR Compliance DBM/HIGG Minutes
Mandatory training compliance rate – Target 90%
Assurance: 3) Compliance is monitored monthly at EMT, Divisional Business Meeting, and Workforce Matters
31 Jul 2016 BLUE

44 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
Safeguarding Children Level 3: 62% compliant Training compliance reports still group levels 1-3; awaiting confirmation as to when these will be reported separately. Reports will then be sent to managers to check for accuracy and to identify and support those staff outstanding.
CH03 Must - The trust must ensure that staff have regular access to appraisals in order for them to develop their skills and competency.
Implementation: 1) New appraisal process in place in 16-17 annual cycle of completion between April and July for all appraisals
Executive Lead: Director of Workforce Operational Lead: Chief Operating Officer
31 Jul 2016 BLUE
At 30 November the reported compliance rate for community hospitals was 90.99%
Monthly compliance reports and meeting minutes ESR Compliance DBM/HIGG Minutes
Appraisal Compliance rate – Target 90%
Assurance: 2) Compliance is monitored on a monthly basis at EMT, DBM, and Workforce Matters (two monthly)
31 Jul 2016 BLUE
CH04 Must- The trust must review the systems and processes for managing and recording the
Development/Implementation: 1) Medicines safety thermometer audit data collection tool to be reviewed to collect further information on omitted doses. Report monthly to HIGG.
Executive Lead: Medical Director Operational Lead:
31 May 2016 BLUE 31 Jul
Medicines safety thermometer submission in place forming part of NHS contract reporting requirements Quarterly audit for omitted doses was reported to HIGG in
Monthly MST upload Confirm HIGG minutes that this goes monthly for
Outcome of missed medication audit – target TBC

45 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
quality of missed medicine doses and clear action plans should be developed implemented and audited to improve reporting, documentation and auditing.
2) Quarterly audit of omitted doses. Reported at HIGG. 3) Action plan has been produced from previous audit. Report monthly to HIGG. 4) Learning feedback fed into prescriber education sessions where appropriate.
Lead Hospital Pharmacist
2016 BLUE 31 Aug 2016 BLUE 31 Aug 2016 GREEN
August review HIGG minutes following meeting
CH05 Should - The trust should ensure that out of hour’s services are able to support the medical and nursing staff by responding in a timely way to medical emergencies.
Implementation: 1) New contract in place with OOH GP service; this includes OOH advice from DMH team. 2) Strengthened KPIs See EoL07
Executive Lead: Director of Operations Operational Lead: Chief Operating Officer
In Place GREEN
Contract Timely medical input is available out of hours
Outcome of contract review meetings with service provider, including performance monitoring
CH06 Should - The trust should ensure that staff in the walk in
Implementation: 1) Reception cover in place at all times during working hours at Leek MIU.
Executive Lead: Director of Operations
In Place GREEN
Staff cover throughout operating hours
Patients will be monitored while waiting for intervention
TBC

46 Quality Improvement Plan – January 2017 update - DRAFT
Ref Issues
identified by CQC
Action Responsibility Due Date Update Evidence Success Measure
centre have the support of administration staff to assist them with ‘meet and greet’ and patient observation during and after the triage process has begun.
NB These arrangements already in place for the Walk in Centre
Operational Lead: Chief Operating Officer

47 Quality Improvement Plan – January 2017 update - DRAFT
Internal Trust Risks Associated with the Plan
Ref Action Risk to Delivery Date identified/initial score
Mitigating Actions Risk Score
AC01 Manual Monitor of rescheduled visits in community nursing services
Teams are monitoring this manually, however audit evidence has identified that not all teams are utilising the standardised template
August 2016 3x4=12
Escalated through operational leadership. Development of guiding SOP alongside monitoring template
3x2= 6 Moderate Risk Manual monitor in place and reported through community safer staffing dashboard. Risk reduced 27/10/2016
EOL End of Life (all actions) Given the significant nature of the feedback of the CQC in the area of EoL services and the breadth of the actions associated with this area (LHE wide changes) it is recognised that this will require dedicated and focussed efforts to secure the changes required to fully deliver the system changes needed.
September 2016 3x4=12
Identify a dedicated project management resource to drive the changes required in End of Life care.
3x4 = 12 High Risk
Risks Associated with the Plan – External to the Trust
Ref Action Risk to Delivery Date identified/ initial score
Mitigating Actions Risk Score
AC03 Review response time criteria in service specification adult community nursing
Not all south services have a service specification
August 2016 3x4=12
Negotiation underway with commissioners in the south to agree service specifications where none in place
2x2= 4 Low Risk Risk reduced as specification is agreed and awaiting contract variation 28/10/2016
EOL02
Engagement of Primary Care in rolling out last days of life care plan
GP engagement in triggering ‘last days of life’ is key to the effective use of the care plan
August 2016 3x4=12
Engagement process multi-factorial (i.e. LMC, CCG, STP, NHSE)
2x3= 6 Moderate Risk Risk reduced due to service level

48 Quality Improvement Plan – January 2017 update - DRAFT
engagement with GPs 27/10/2016 CYP02 Complete Children’s Service
strategy Complex and difficult commissioning landscape for children’s services, multiple tenders and financial contraction
October 2016 3x3=9
Trust engagement in Tenders and negotiation of service models in response to reduced financial envelope
3x3 = 9 High risk
EOL09 Discuss and agree robust commissioning intentions with commissioners in relation to end of life care, including an agreed definition for fast tracked patients
Commissioners end of life tender is currently on hold pending the outcome of a review by NHSE
October 2016 4x4=16
Communication with commissioners to ensure that the outcome of the review is shared. It has been confirmed that the tender has been recommenced.
3x4 = 12 High risk Risk reduced due to the End of Life tender being taken off of hold.
The consequence and likelihood of the risk has been identified using the matrix below:

49 Quality Improvement Plan – January 2017 update - DRAFT
Decision Log: Changes to Actions
Ref
Original Action Change Where agreed Date agreed
WL04 3) Implement a weekly incident review report identifying themes and risk areas including analysis of teams (those most and least likely to escalate).
Remove this action. Rationale: The governance process for the reporting of incidents and their escalation is clear and offers automatic notification followed up with Risk Team notification to managers at appropriate level based on the incident. Replace this with: 4) Review of existing incident reporting and management governance arrangements. Proposed due date 31 October 2016
SLT CQC Steering Group
26.07.16 01.08.16
WL08 2) Update and maintain the Trusts directory of services and publish this on the Trust intranet.
Split this action. 2) Update the Trusts Directory of Services 3) Maintain the Trusts Directory of Services utilising an automated process linked to ESR. Due date for 2) remains the same, action 3) due date proposed for 31 March 2017
SLT CQC Steering Group
26.07.16 01.08.16
AC08 1) Record keeping audit revised to monitor the quality of records through assessment planning delivery and evaluation
Additional action: 2) Roll out of revised audit Due date for roll out 31 October 2016
CQC Steering Group
08.08.16
AC06 Aligned to AC01 1) Develop and embed caseload supervision and management processes for community staff 2) Support staff through master class programme
Include professional leads in responsibility column CQC Steering Group
08.08.16
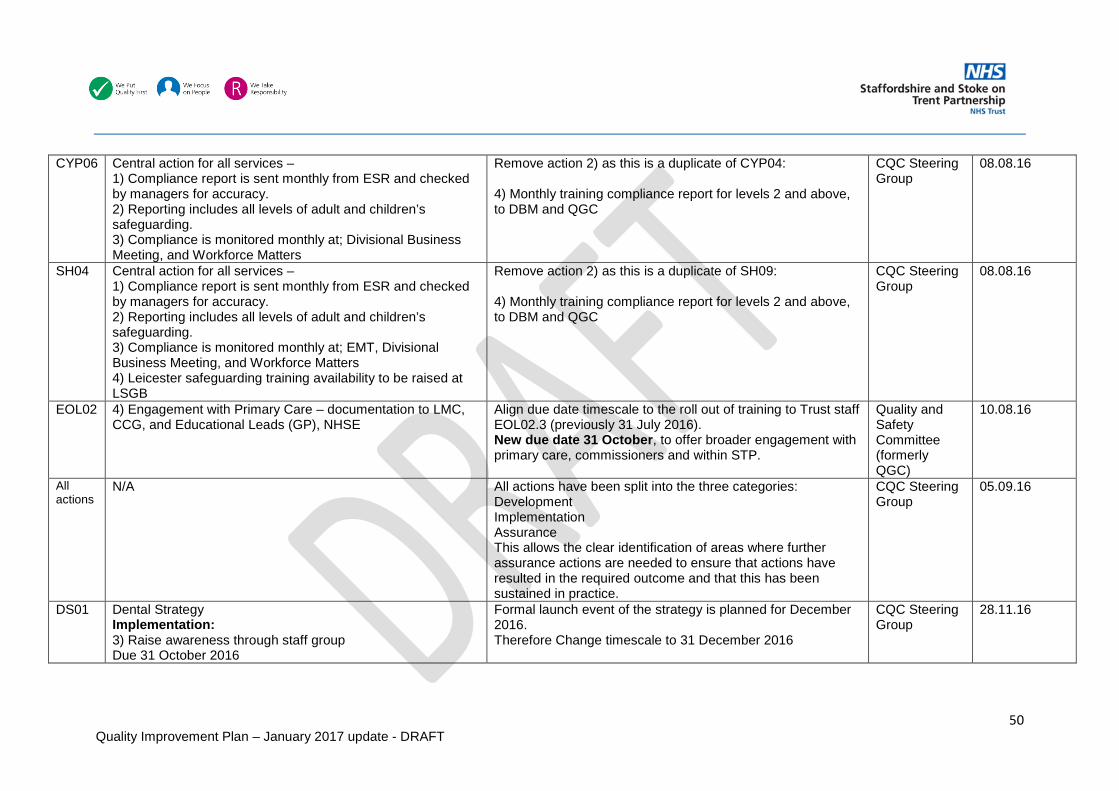
50 Quality Improvement Plan – January 2017 update - DRAFT
CYP06 Central action for all services – 1) Compliance report is sent monthly from ESR and checked by managers for accuracy. 2) Reporting includes all levels of adult and children’s safeguarding. 3) Compliance is monitored monthly at; Divisional Business Meeting, and Workforce Matters
Remove action 2) as this is a duplicate of CYP04: 4) Monthly training compliance report for levels 2 and above, to DBM and QGC
CQC Steering Group
08.08.16
SH04 Central action for all services – 1) Compliance report is sent monthly from ESR and checked by managers for accuracy. 2) Reporting includes all levels of adult and children’s safeguarding. 3) Compliance is monitored monthly at; EMT, Divisional Business Meeting, and Workforce Matters 4) Leicester safeguarding training availability to be raised at LSGB
Remove action 2) as this is a duplicate of SH09: 4) Monthly training compliance report for levels 2 and above, to DBM and QGC
CQC Steering Group
08.08.16
EOL02 4) Engagement with Primary Care – documentation to LMC, CCG, and Educational Leads (GP), NHSE
Align due date timescale to the roll out of training to Trust staff EOL02.3 (previously 31 July 2016). New due date 31 October, to offer broader engagement with primary care, commissioners and within STP.
Quality and Safety Committee (formerly QGC)
10.08.16
All actions
N/A All actions have been split into the three categories: Development Implementation Assurance This allows the clear identification of areas where further assurance actions are needed to ensure that actions have resulted in the required outcome and that this has been sustained in practice.
CQC Steering Group
05.09.16
DS01 Dental Strategy Implementation: 3) Raise awareness through staff group Due 31 October 2016
Formal launch event of the strategy is planned for December 2016. Therefore Change timescale to 31 December 2016
CQC Steering Group
28.11.16

51 Quality Improvement Plan – January 2017 update - DRAFT
WL04 4) Review of existing incident reporting and management governance arrangements. Due date 31 October 2016.
Due to the agreement to carry out an independent review of a range of incident types from simple low harm incidents where local management and closure has taken place up to full duty of candour investigation processes the date has been extended to the 31 January 2017.
CQC Steering Group Quality and Safety Committee
28.11.16 11.01.17
EOL05 N/A – New action New action following the assurance review of end of life section of the plan: Ensure access for all key palliative care staff to the electronic “Palliative Care Handbook” through a multi-user licence.
CQC Steering Group Quality and Safety Committee
28.11.16 11.01.17
ALL N/A Inclusion of a “success measures” column to identify the existing process of testing each outcome.
CQC Steering Group Quality and Safety Committee
28.11.16 11.01.17
WL05 New Assurance action Assurance: 5) Update reports on the outcomes of learning from incidents, complaints, audit and quality visits to be presented to Divisional Business Meetings and Quality and Safety Committee.
CQC Steering Group Quality and Safety Committee
28.11.16 11.01.17
WL09 New assurance action Assurance: Regular Report into Trust Board
CQC Steering Group Quality and Safety Committee
28.11.16 11.01.17
AC06 1) Develop and embed caseload supervision and management processes for community staff
Action split to acknowledge different processes for development and implementation: 1) Develop caseload supervision and management process for community staff 3) Embed caseload supervision and management Timescale for action 3) to cover roll-out programme 31 March 2017
CQC Steering Group Quality and Safety Committee
28.11.16 11.01.17

52 Quality Improvement Plan – January 2017 update - DRAFT
WL01, WL03, AC15
Executive Lead previously identified as Deputy Chief Executive Officer
New Executive Lead: Acting Director of Strategy
AC01 2) Upgraded e-community system is fully embedded across all district nursing teams Formerly rated as AMBER (overdue) due to the on-going redesign of the e-community mobile application.
Given that the e-community desktop system has been upgraded and is in use by all district nursing teams this action can be rated BLUE. The actualisation of visits at the time of delivery via a mobile application has been delayed, however this does not pose a risk to the safe scheduling and rescheduling (prioritisation) of visits which is delivered via the desktop system. A new action has been developed for the mobile application: 6) The actualisation of district nursing visits is supported by the availability of a mobile e-community application to all district nurses.
CQC steering Group

1
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD
TO BE HELD ON: 22 February 2017
Subject: Education, Training and Development Strategy
Strategic Goal: (tick as applicable)
√ We will provide high quality and safe services which provide an excellent experience and best possible outcomes
√ We will work with users and carers to deliver integrated services, simply and effectively
√ Our organisation will develop and deliver sustainable, innovative services that support independence
√ Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
√ We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Julie Tanner Director of Workforce & Development
Subject Lead: Clare Spencer Head of Training and Development
Recommendation: For Approval & Assurance
For Discussion √ For Information
PURPOSE OF THE REPORT:
• To provide the Trust Board with a proposed Education, Training and Development Strategy.Which has been reviewed and agreed at Workforce Matters.
KEY POINTS:
This strategy will ensure that the Trust is focused on supporting a workforce that can meet the challenges of the next three years and beyond, able to adapt to change and transfer skills into new and different roles as required. This will ensure that the Trust meets its five strategic aims of :
• We will provide high quality and safe services which provide an excellent experience and best possible outcomes
• We will work with users and careers to deliver integrated services in partnership, simply and effectively
• Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
• Our organisation will develop and deliver sustainable, innovative services that support independence
• We will make excellent use of our resources and improve levels of efficiency across our services

2
The aims and objectives of the Strategy are influenced by national and local health & social care drivers, which are constantly evolving and will require flexibility in the delivery of this strategy. The Trust has a Training and Development Team that is multi-professional, to ensure optimum utilisation of the resources available to meet both local and national education and training priorities. All professional staff within the team have worked in clinical practice and have a wide range of clinical expertise, which places them well to understand the challenges staff face on a daily basis and can be responsive to the changing needs of the organisation and its patients/service users.
INTER DEPENDENCIES: Legal and/or Risk Lack of appropriate training & competency can expose the Trust to patient claims
as well as damage to reputation.
Clinical Developing working practices/skills & competencies in order to successful Implementation of transformation programmes & up skilling of the workforce.
Financial Unitising training budgets according to Trust processes & in accordance to HEEWM
HR All training is aligned to trust values and workforce objectives
Social Care Training development is on-going for social care staff
Equality Impact Training is inclusive of all staff
Requirement for further review
None
RECOMMENDATIONS / ACTION REQUIRED: The Trust Board is requested to discuss and note the contents of the stratergy and to agree its implimentation.

3
Education, Training and Development Strategy
2016-2019
Providing excellent education, training and development to support the current and future
workforce in delivering the best care for our patients/service users
Introduction

4
The scale, pace and complexity of change in the health and social care profession and a vision to ensure that patients/service users receive the best care provides many challenges for the Trust, making it necessary to constantly, learn, develop and change. The Education, Training and Development Strategy 2016 – 2019 sets out how the Trust will ensure that the workforce has the right skills and knowledge to meet these challenges whilst delivering high quality care. Our mission is to:
“Have the right people at the right time, who are well trained and motivated and able
to deliver the right level of individual care” This strategy will ensure that the Trust is focused on supporting a workforce that can meet the challenges of the next three years and beyond, able to adapt to change and transfer skills into new and different roles as required. This will ensure that the Trust meets its five strategic Goals:
• We will provide high quality and safe services which provide an excellent experience
and best possible outcomes • We will work with users and careers to deliver integrated services in partnership,
simply and effectively • Our workforce will be empowered and supported to deliver care in a way that is
consistent with our values • Our organisation will develop and deliver sustainable, innovative services that
support independence • We will make excellent use of our resources and improve levels of efficiency across
our services The aims and objectives of the Strategy are influenced by national and local Health and Social Care drivers, which are constantly evolving and will require flexibility in the delivery of this strategy. These include, but are not limited to:
• Health Education England (HEE) Mandate/Workforce Strategy • Willis Report – Shape of Caring/Training • Apprenticeship Frameworks • Five Year Forward View • Talent for Care • Care Quality Commission Expectations • Care Act
Current Position
The Trust has a Training and Development Team that is multi-professional, to ensure optimum utilisation of the resources available to meet both local and national education and training priorities. All professional staff within the team have worked in clinical practice and have a wide range of clinical expertise, which places them well to understand the challenges staff face on a daily basis and can be responsive to the changing needs of the organisation and its patients/service users. The Training & Development delivery is aligned with the organisational goals and has five key priorities areas as set out below:

5
Organisational Goals
Quality and Patient/Service User
Safety Learning and education is informed by the need to continuously improve our quality and safety standards
Learning Together Interdisciplinary learning and development promotes effective teamwork, better understanding and excellent patient/service user outcomes
Enhancing Education Careers are developed and sustained so that our workforce is able to meet current and future patient/service user needs
Innovative Education Innovative and technology enhanced learning and education is adopted and optimised
Inspiring Learning Environments
Our estate and infrastructure supports and encourages high quality learning and education
Training and Development Vision
Providing excellent education, training and development to support the current and future workforce in
delivering the best care for our patients/service users
Training and Development Goal
Have the right people at the right time who are trained and motivated and able to deliver the right level of
individual care
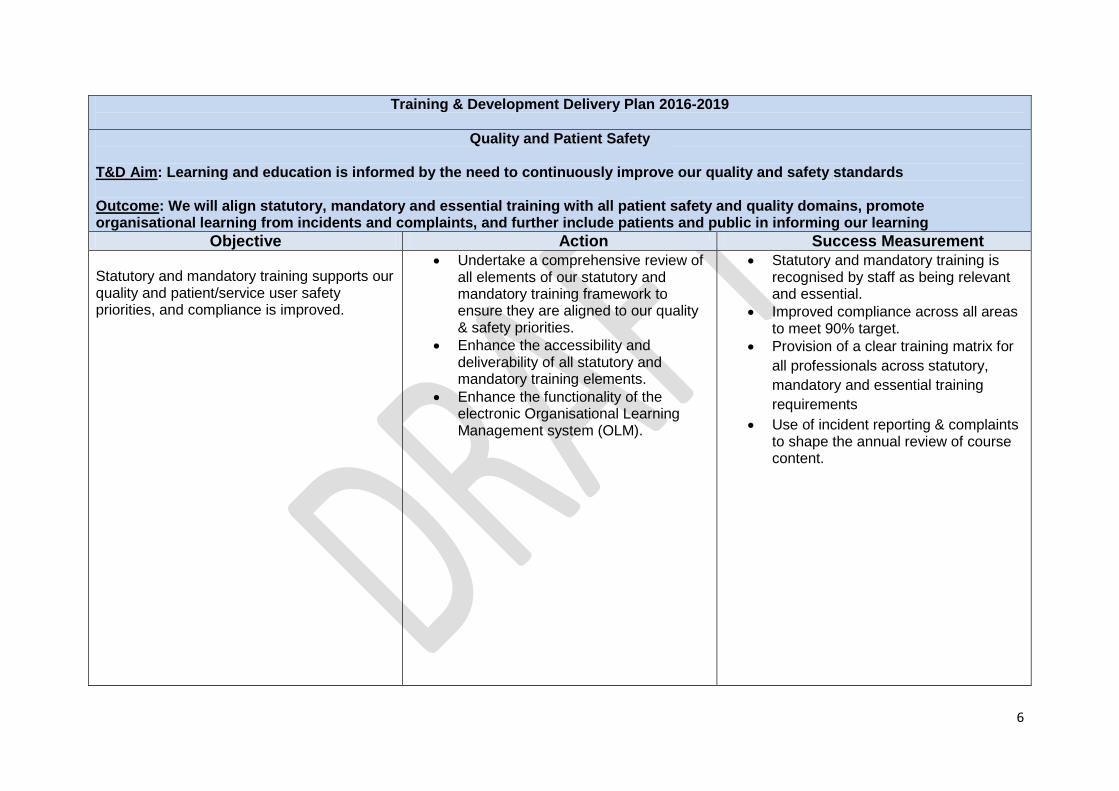
6
Training & Development Delivery Plan 2016-2019
Quality and Patient Safety
T&D Aim: Learning and education is informed by the need to continuously improve our quality and safety standards Outcome: We will align statutory, mandatory and essential training with all patient safety and quality domains, promote organisational learning from incidents and complaints, and further include patients and public in informing our learning
Objective Action Success Measurement Statutory and mandatory training supports our quality and patient/service user safety priorities, and compliance is improved.
• Undertake a comprehensive review of all elements of our statutory and mandatory training framework to ensure they are aligned to our quality & safety priorities.
• Enhance the accessibility and deliverability of all statutory and mandatory training elements.
• Enhance the functionality of the electronic Organisational Learning Management system (OLM).
• Statutory and mandatory training is recognised by staff as being relevant and essential.
• Improved compliance across all areas to meet 90% target.
• Provision of a clear training matrix for all professionals across statutory, mandatory and essential training requirements
• Use of incident reporting & complaints to shape the annual review of course content.

7
Learning Together
T&D Aim: Interdisciplinary learning and development promotes effective teamwork, better understanding and excellent patient/service user outcomes Outcome: We will build upon our current successes by identifying further opportunities to design and implement multidisciplinary learning and education interventions, and promote their benefits
Objective Action Success Measurement Use all opportunities to increase the application of multidisciplinary learning.
• Building on current practice, establish systems to identify further areas in which practice based multidisciplinary learning and education can be applied – internally and externally to the Trust.
• Develop and implement a portfolio of generic and specialty-specific multidisciplinary education and training interventions.
• Maximise the use of simulation training and research in the design and delivery of multidisciplinary learning.
• Determine ways in which patients/service users, families and carers can contribute to multidisciplinary learning.
• Develop a framework within which care delivery developments/service improvements inform multidisciplinary learning opportunities eg Team Leader Forums, Action Learning
• Incorporate research and evidence based practice within future multidisciplinary education programmes and interventions.
• Participation in interdisciplinary learning is demonstrably increased and positively evaluated.
• Improved team working. • All staff to have opportunities for
access to flexible learning opportunities
• Improved staff experience, engagement and retention

8
Enhancing Education
T&D Aim: Careers are developed and sustained such that our workforce is able to meet current and future patient needs Outcome: We will ensure future learning and education provision supports career development and is informed by emerging career frameworks
Objective Action Success Measurement All new staff receive an excellent induction experience (both corporate and local).
• Review the induction process for all staff groups to include the use of e-learning and streamlining the current organisational processes.
• Extend and strengthen the content of induction to include, , the completion of a standardised key competencies, and the provision of information and advice relating to career by developing a personal development plan opportunities.
• All new non-registered staff with face to face contact with service users to complete the care certificate
• Staff provide excellent feedback regarding the quality of their induction,
• Staff feel competent, confident and supported to undertake their new roles
• All staff feel appropriately ‘welcomed’ to our organisation.
• Reduced staff turnover and strengthened team working.
• All staff have key objectives set within 16weeks of commencement in post
• 100% new non-registered staff
complete the care certificate •
All staff have clear development plans linking with organisational and local goals
• All staff to have development discussions supported by the use of the personal development workbook
• Provide coaching conversations to support staff to reflect on their practice and evaluate how they are working.
• Evaluate the coaching network to see how well it supports development discussions
• To embed the use of supervision at all levels, e.g: managerial, professional,
• All staff to have a development plan identified via the annual appraisal process.
• All staff to own their career development & take responsibility for actions within their PDPs
• For all staff to have the opportunity to access the coaching network if required
• For all staff to have good quality supervision opportunities on a regular basis.

9
clinical. • Further develop clear funding
guidance to access CPD externally • Have a clear robust training
agreement between, staff, managers and the Trust.
• Provide a Training Prospectus so staff are aware of training provision available to them.
• Support any new skills required in line with the development of the Multi-specialty Community Provider Model of care.
• Provide a clear competency framework for all clinical/social care professionals.
• Staff are aware of how to access funding to support their CPD.
• Increased numbers of Bands1 to 4 are accessing CPD opportunities.
• All staff have a clear training agreement when accessing training externally
• All Staff have access to the training prospectus via the intranet
• Staff have the skills and knowledge to provide delivery of care as part of the MCP’s
• Staff have clear competency framework and are working towards achieving fully competency.
Training programmes are designed/commissioned and implemented, which underpin the delivery of excellent patient/service user care, and support the professional and career development of our staff.
• Ensure our education and training programmes align with existing and emerging career frameworks. E.g. associate nurse, assistant practitioner
• Evaluate training programmes to demonstrate the effectiveness of training in the workplace as well as inform changes to programmes where necessary.
• Provide Evidence based training • Provide competency based
support to staff in the workplace • Provide training to meet staff
learning styles • Review and strengthen the Trust
• More of our staff are following a recognised career pathway and are fully supported in progressing within it.
• Demonstrable progress in the implementation of the “Modernising Careers” and the implementation of career frameworks for other staff groups (e.g. allied health professionals).
• More staff benefitting from relevant and accessible CPPD opportunities.
• Improved retention and better staff experience.
• All staff have access to the Learning and Development intranet site to
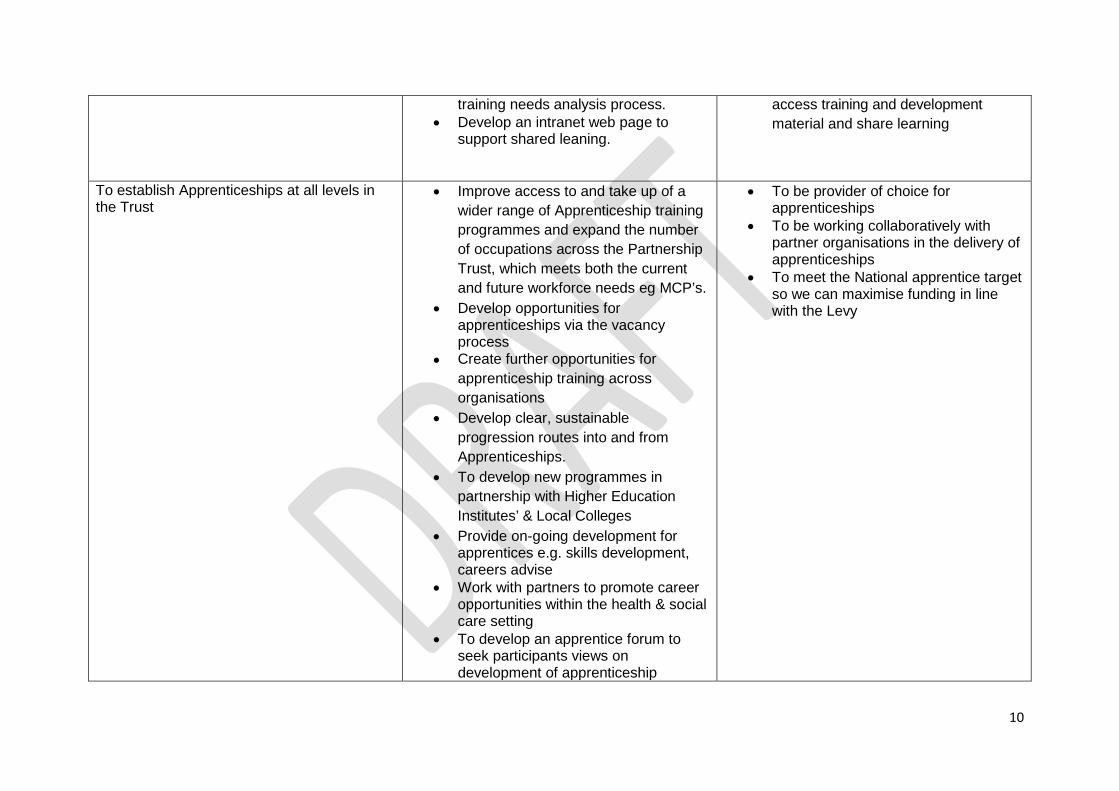
10
training needs analysis process. • Develop an intranet web page to
support shared leaning.
access training and development material and share learning
To establish Apprenticeships at all levels in the Trust
• Improve access to and take up of a wider range of Apprenticeship training programmes and expand the number of occupations across the Partnership Trust, which meets both the current and future workforce needs eg MCP’s.
• Develop opportunities for apprenticeships via the vacancy process
• Create further opportunities for apprenticeship training across organisations
• Develop clear, sustainable progression routes into and from Apprenticeships.
• To develop new programmes in partnership with Higher Education Institutes’ & Local Colleges
• Provide on-going development for apprentices e.g. skills development, careers advise
• Work with partners to promote career opportunities within the health & social care setting
• To develop an apprentice forum to seek participants views on development of apprenticeship
• To be provider of choice for apprenticeships
• To be working collaboratively with partner organisations in the delivery of apprenticeships
• To meet the National apprentice target so we can maximise funding in line with the Levy

11
programmes. • Make every effort to reach the Levy
Targets. To have work experience placements in our organisation
• Support Work experience placements working with in our organisation and across the health economy to promote local growth of talent
• Support volunteer placements
• To have an increased diverse range of people working/volunteering within the Trust.
• To have an increase in volunteer placements

12
Innovative Education
T&D Aim: Innovative and technology enhanced learning and education is adopted and optimised Outcome: As an innovative, forward-looking organisation, we will build upon our current offerings by embracing and capitalising on the opportunities presented by technology enhanced learning (TEL), simulation training and our research and development collaborations
Objective Action Success Measurement All opportunities to assess, test and apply innovative educational technologies are pursued
• Further improve and expand our e-Learning and other IT/web based applications.
• 50%of staff accessing a range of E-Learning applications, which enhance and improve the overall learning experience.
• Improved staff experience, engagement and retention.
The application of simulation training is enhanced.
• Identify ways in which the current portfolio of simulation training can be further expanded and accessed by all staff groups.
• Develop with partner organisations simulated learning environments e.g.: Staffordshire Fire & Rescue Service - Safe & Sound
• Safe & Sound (Life Skills) facility is recognised as being an leader in the provision of simulation training in Staffordshire
• Teams benefitting by participation in simulation training.

13
Inspiring Learning Environments
T&D Aim: Our estate and infrastructure supports and encourages high quality learning and education Outcome: We will establish a central ‘Training Centre’ from which high quality education and training is administered and provided within a modern, stimulating and well-resourced environment
Objective Action Success Measurement We have the necessary capability and capacity to deliver excellent education and training in inspiring environments.
• Review the capacity and capability of our delivery structure and propose changes to improve the capacity and capability of the team.
• Review our physical infrastructure and propose ways in which this should be consolidated, modernised and improved.
• Determine how our staff are afforded sufficient “time to learn”
• Work with partner organisations and education providers to investigate developing training that works across all settings and implement where there is agreement with partners
• Training & Development Team is recognised as being highly effective in the design/commissioning and delivery of high quality, relevant and accessible learning and education.
• The establishment of a “Training Centre”, as the central “home” of our learning and education provision for staff.
• ELearning is fully embedded within our delivery structure.
• Improved staff experience, engagement and retention.
Our learning and education, and leadership development provision meets or exceeds recognised “best practice” standards
• Pursue accreditation with the appropriate professional bodies
• Develop opportunities to share learning e.g. team leader forum
• Identify future challenges that will create the need for change and proactively develop education, training and development in new directions
• Accreditation is attained. • Improved staff experience,
engagement and retention • Staff demonstrate the trust values in
their day to day activities. • Evidence of embedded
learning/change in practice by doing longitudinal evaluations

14
Training and Development delivery methods
All our staff will have different “learning styles” this refers to the preferential way in which we absorb, process, comprehend and retain information. Staffs preferred learning styles have significant influence on their behavior and learning. Information that is accessed through a preferred style shows an increase in levels of comprehension, motivation. Therefore preferred learning modes should be matched with appropriate learning strategies. Allowing staff to access information in terms they are comfortable with will also increase their confidence. Therefore in order to meet the needs of our staff the Trust delivers training in the follow methods:
Simulation Classroom
E-Learning
Training & Development
Work-based learning
“on the job”
Coaching & Mentoring

15
Challenges for the Future
Workforce
• All Health and Social Care professions are experiencing difficulties in recruitment both nationally and locally. For example it is well publicised that there is a national shortage of qualified nurses. This has resulted in the Trust carrying large numbers of nursing vacancies throughout the year. The impact of this on training is that staff cannot be released in a timely manner to undertake statutory or mandatory training or development opportunities.
• All healthcare assistants and social care support workers/carers are now required to undertake the Care Certificate before working unsupervised. The Francis Inquiry identified serious challenges in some Health and Social Care settings in 2013 and as a consequence Camilla Cavendish reviewed and made recommendations on the recruitment, learning and development, management and support of healthcare assistants and social care support workers/carers, to ensure that this workforce provided compassionate care. The report recommended the development the “Care Certificate”. These standards/competencies have been developed to ensure staff are provided with a robust induction/training in order to provide high quality & safe practice/care. The trust needs to ensure that all new staff new to care complete these within the time frames given. The workforce development training team will be supporting the implementation of this across the Trust.
• There will be a need to implement a continuous cycle of workforce and skill mix review, developing and integrating new roles, where they add value, into the current and future workforce.
• There are economic and social reasons for the Trust to employ Apprentices.
Introducing younger people into the workforce enhances succession planning by “growing our own” to support an ageing workforce. However, the employment of Young People brings particular challenges in terms of pastoral support, limitations on working hours /activities and work/life balance requirements of generation Y.
It is recognised that the length of time it takes to train professionally registered staff will impact on the success of the Five Year Forward Review, therefore there is an emphasis on the need to develop existing staff to take on new or enhanced roles.
Finance
• Potential reduction in external funding to support the development of existing staff.
• The predicted NHS and Social Care funding gap will increase pressure to drive down costs whilst improving quality. This will require the development of a workforce that can take on some of the activities currently undertaken by registered

16
staff, releasing their time to concentrate on providing complex care. Reducing the number of higher banded/graded roles and supplementing them with lower bands/grades who have new roles and different ways of working needs further exploration, development and embedding into the organisation, For example Assistant Practitioner, Associate Nurse
• In July 2015, the Government announced an apprentice levy on large employers across all sectors which will come into effect by April 2017. The rate of the levy will be set at 0.5% of an employer’s pay bill and will be collected via PAYE. This will create a considerable cost pressure for the Trust if it is not able to facilitate a larger input of apprenticeship opportunities into the Trust.
Changing Health and Social Care Environment
• The Five Year Forward View describes different models for the provision of healthcare in the future; all indicate that care will move closer to the patient and be delivered in the community. As a result the workforce of the future will not only be working in different environments, but with different types of staff Identified as the care workforce.
• Increasing intensity and complexity of workload due to rising demand and acuity of patients will require advanced practice roles across all professions and necessitate a review of cross-profession working.
• Increased demands on services is making it difficult for departments to release staff for training, resulting in a high level of non-attendance. The consequences are wasted resources and staff who have not been enabled to refresh or improve their skills and knowledge.
In summary the challenges for the next three years are a shortage of registered professional staff at a time when funding is reducing and the health and social care arena is changing dramatically. The focus for the Training and Development Team therefore must be:
• Providing training and development opportunities that equip staff with the skills and knowledge required to adapt to change quickly and effectively for the needs of the patients/service user.
• Ensuring r egistered professionals are able to access education, training and development to meet statutory requirements for revalidation and continuous professional development.
• Developing education pathways to support the creation of new roles and their integration into the workforce, i.e. Assistant Practitioner apprenticeship pathways
17
• Increasing the use of simulation training to improve the safety and quality of patient/service user care
• Increase the use of technology to deliver training in the workplace, for example: using e- training and “apps” on PCs.
• Further promote and increase the usage of the library and its resources to support the delivery of high quality patient/service user care.
• Further develop quality metrics to demonstrate that the training and education delivered to staff, trainees and students is effective and impacting on the quality of care.
• Develop robust processes for the effective use of education and training funding received via Health Education, England.
• Further exploitation of income generation opportunities to support education activity across the organisation and Health Economy.

18
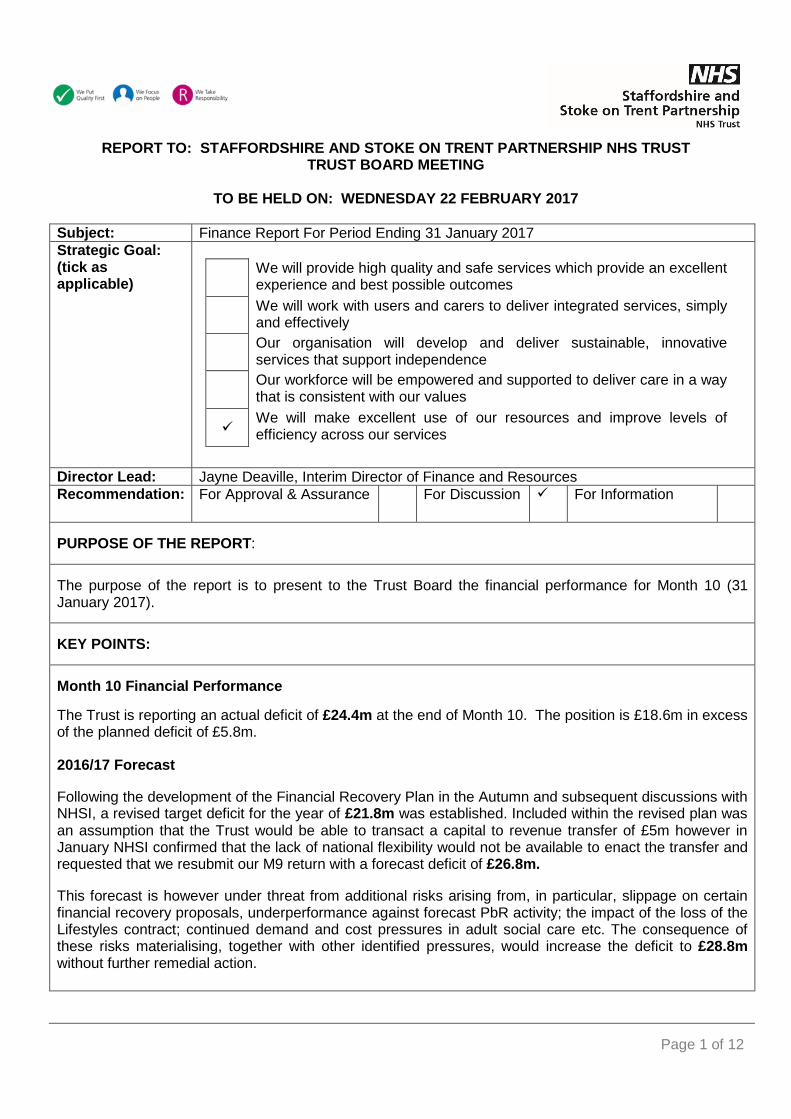
Page 1 of 12
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST TRUST BOARD MEETING
TO BE HELD ON: WEDNESDAY 22 FEBRUARY 2017
Subject: Finance Report For Period Ending 31 January 2017 Strategic Goal: (tick as applicable)
We will provide high quality and safe services which provide an excellent
experience and best possible outcomes We will work with users and carers to deliver integrated services, simply
and effectively Our organisation will develop and deliver sustainable, innovative
services that support independence Our workforce will be empowered and supported to deliver care in a way
that is consistent with our values
We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Jayne Deaville, Interim Director of Finance and Resources Recommendation: For Approval & Assurance For Discussion For Information
PURPOSE OF THE REPORT: The purpose of the report is to present to the Trust Board the financial performance for Month 10 (31 January 2017). KEY POINTS: Month 10 Financial Performance The Trust is reporting an actual deficit of £24.4m at the end of Month 10. The position is £18.6m in excess of the planned deficit of £5.8m.
2016/17 Forecast Following the development of the Financial Recovery Plan in the Autumn and subsequent discussions with NHSI, a revised target deficit for the year of £21.8m was established. Included within the revised plan was an assumption that the Trust would be able to transact a capital to revenue transfer of £5m however in January NHSI confirmed that the lack of national flexibility would not be available to enact the transfer and requested that we resubmit our M9 return with a forecast deficit of £26.8m. This forecast is however under threat from additional risks arising from, in particular, slippage on certain financial recovery proposals, underperformance against forecast PbR activity; the impact of the loss of the Lifestyles contract; continued demand and cost pressures in adult social care etc. The consequence of these risks materialising, together with other identified pressures, would increase the deficit to £28.8m without further remedial action.

Page 2 of 12
Cash The overall cash position at M10 is a cash balance of £5.6m offset by revenue support loans of £5m in the month. The unavailability of the capital to revenue transfer will require an additional £4.6m loan drawdown with the consequence that the forecast loans balance at 31 March will be £26.7m. INTERDEPENDENCIES:
Legal and/or Risk The key financial risks are identified within the report.
Clinical The Partnership Trust’s budgets need to support the delivery of Clinical Services.
Financial Failure to deliver within budget will result in deterioration in the Partnership Trust’s financial position and resilience going forwards.
HR The Partnership Trust will need to ensure that all staff with budget responsibility possess the relevant training and support to discharge their delegated duties.
Social Care This financial performance covers the whole of the Partnership Trust’s activities.
Staff and Trade Union involvement actions undertaken/planned
This report is for information.
Patient & Public Involvement
The budget supports the delivery of Services provided by the Partnership Trust, and where necessary these plans will have had Patient and Public Involvement.
Equality Impact The budget supports the delivery of Services provided by the Partnership Trust, and where necessary these plans will have had an Equality Impact Assessment.
Information exempt from Disclosure This report is for information.
Requirement for further review Financial performance will be reviewed on a monthly basis. RECOMMENDATIONS: The Trust Board is asked to consider the financial performance of the Partnership Trust at Month 10, and forecast for the remainder of this financial year.
POSITION OVERVIEW EBITDA

Page 3 of 12
• T
he Partnership Trust's Earnings before Interest, Taxation, Depreciation and Amortisation (EBITDA) for the month ending 31 January 2017 shows a deficit of £18.7m (6.6%).
• This is £18.6m behind the plan of £0.1m deficit submitted to the NHSI.
INCOME & EXPENDITURE (I&E) POSITION
• The Partnership Trust's financial position at Month 10 is an actual deficit of £24.4m, representing an adverse variance of £18.6m against the YTD plan of £5.8m deficit.
CASH
• The Partnership Trust has a cash balance of £5.6m at the end of January.
• This is a £1.0m shortfall against the year to date plan of £6.6m.
• The Partnership Trust is currently scoring a 2 for liquidity as per the Continuity of Services rating.
USE OF RESOURCE RATING
• The Partnership Trust's overall Use of Resources rating at Month 10 is 3.0, and remains in line with the target set out in the Annual Plan.
COST IMPROVEMENT PLAN (CIP) • The Partnership Trust has submitted a
planned savings programme to the NHSI for Health services of £7.1m for 2016/17. The profile of CIP delivery is demonstrated in Appendix 1, and is compared to the NHSI plan.
• The variance of £18.6m at Month 10 is primarily attributable to pressures in Adult Social Care (ASC) of £9.8m. Health pressures (£8.8m) have generally remained in line with that anticipated in the FRP however; it has been impacted by a reduction in actual and forecast reduction in PbR over performance income.
TEMPORARY STAFFING EXPENDITURE
• The Partnership Trust has spent £8.181m on temporary staff at the end of Month 10, comprising £5.467m agency staffing, and £2.714m bank staffing. Both Agency and bank costs are at their lowest levels in twelve months. Agency staffing remains below national capping limits.
USE OF RESOURCES RATING
Up to 5% adverse variance
>5% adverse variance
>5% favourable variance
Up to 5% favourable variance
On target
Cash
Use of Resources Rating
CIP Delivery
Deficit
Actual vs Plan Forecast vs Plan
EBITDA

Page 4 of 12
ACCOUNTABILITY FRAMEWORK NHS Improvement use a few financial metrics to assess financial performance (see table above) by:
• scoring providers 1 (best) to 4 against each metric.
• averaging individual providers’ scores across all the metrics to derive a use of resources score for the provider.
STATEMENT OF COMPREHENSIVE INCOME TO 31 JANUARY 2017
Area Metric Year to 31 January 2017 Weight We
ScPlan 2.0 20%
Actual 2.0 20%
Plan 4.0 20%
Actual 4.0 20%
Plan 4.0 20%
Actual 4.0 20%
Plan N/A 20%
Actual 4.0 20%
Plan 1.0 20%
Actual 1.0 20%
Plan 3.0
Actual 3.0
Agency
Financial Sustainability
Financial Efficiency
Financial Controls
I & E Margin
Distance From Plan
Capital Service Capacity (Times)
Risk Rating
Liquidity Ratio (Days)

Page 5 of 12
I&E POSITION
• The Partnership Trust's I&E financial position at Month 10 shows an actual deficit of £24.4m, representing a £18.6m adverse variance against the YTD plan of £5.8m deficit.
• The position is heavily influenced by the key pressures reported to the Trust Board over the course of the year, which are summarised below for reference.
INCOME
• Overall, income at Month 10 is marginally behind the Partnership Trust’s YTD plan.
• Arbitration rulings in respect of contract
settlements represent the main contributory factor in the Health shortfall. In addition, income generation has fallen short of original targets in respect of some services (e.g. healthy lifestyles).
• This is offset by an over recovery of Adult Social Care income of £3.4m (influenced by additional risk share funding agreed with SCC), together with other income generation of £3.2m.
YEAR TO DATE SUMMARY • The Trust is reporting an actual deficit of
£24.4m at month 10. The position is now £18.6m in excess of the planned deficit of £5.8m.
£m BudgeActivity Income
- Health
- Adult Social Care
Other Income
Operating IncomePay Expenditure (
Non-Pay Expenditure (
Operating Expenditure (2EBITDAEBITDA %Depreciation
Interest Received
Interest Payable (PFI)
Dividend
Retained Surplus / (Deficit)I&E Surplus / (Deficit) % (

Page 6 of 12
• T
he main drivers of the variance against the planned position may be attributed as follows:
• ASC (£9.8m) – demand pressures
remain intense in both volume and reported acuity levels with residential numbers and costs continuing to trend upwards, and more than counteracting the benefits of the review intervention in community service models. Containment of these pressures remains the greatest challenge for the Trust over the remaining two months as this continued level of spend is a key pressure in the ability of the Trust meeting a £26.8m deficit target;
• Health (£14.6m) – the underlying run rate in health has generally remained in line with that anticipated in the FRP however, it has been impacted by a reduction in actual and forecast reduction in PbR over performance income. A review and reconciliation of PbR activity has been undertaken to reflect the activity flowing through the new Rio information system which has resulted in actual year to date and forecast income being reduced. This is reflected in the forecast at section 3 of this report.
CASH The overall cash position at M10 is a cash balance of £5.6m offset by revenue support loans of £5m in the month. The unavailability of the capital to revenue transfer will require an additional £4.6m loan drawdown with the consequence that the forecast loans balance at 31 March will be £26.7m.
STATEMENT OF FINANCIAL POSITION AS AT 31 JANUARY 2017
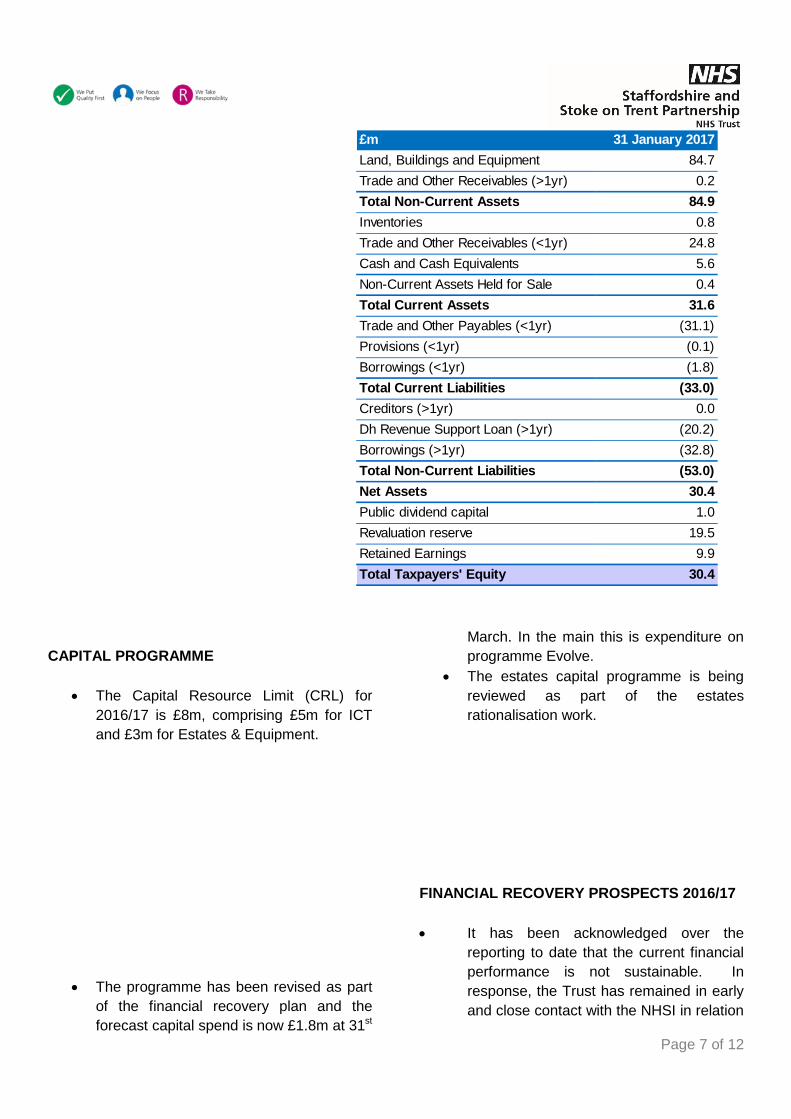
Page 7 of 12
CAPITAL PROGRAMME
• The Capital Resource Limit (CRL) for 2016/17 is £8m, comprising £5m for ICT and £3m for Estates & Equipment.
• The programme has been revised as part of the financial recovery plan and the forecast capital spend is now £1.8m at 31st
March. In the main this is expenditure on programme Evolve.
• The estates capital programme is being reviewed as part of the estates rationalisation work.
FINANCIAL RECOVERY PROSPECTS 2016/17 • It has been acknowledged over the
reporting to date that the current financial performance is not sustainable. In response, the Trust has remained in early and close contact with the NHSI in relation
31 January 2017Land, Buildings and Equipment 84.7Trade and Other Receivables (>1yr) 0.2Total Non-Current Assets 84.9Inventories 0.8Trade and Other Receivables (<1yr) 24.8Cash and Cash Equivalents 5.6Non-Current Assets Held for Sale 0.4Total Current Assets 31.6Trade and Other Payables (<1yr) (31.1)Provisions (<1yr) (0.1)Borrowings (<1yr) (1.8)Total Current Liabilities (33.0)Creditors (>1yr) 0.0Dh Revenue Support Loan (>1yr) (20.2)Borrowings (>1yr) (32.8)Total Non-Current Liabilities (53.0)Net Assets 30.4Public dividend capital 1.0Revaluation reserve 19.5Retained Earnings 9.9Total Taxpayers' Equity 30.4
£m

Page 8 of 12
to the
spread of financial risk facing the Trust.
• A thorough review of the financial “run-rate” forecast was undertaken at Quarter 2, together with a range of pressures facing the Trust over the remainder of the year. This amounted to £31.8m. In response, financial recovery themes and outline plans were established to deliver £10m of in-year savings. The revised deficit plan amounting to £21.8m was subsequently discussed in depth both internally and externally with NHSI; the Trust Board is aware of the key themes contained within the plan from previous discussions.
• During January 2017, NHSI informed the
Trust that the £5m capital to revenue transfer assumption within the £10m savings plan, being an instrument the DoH offered last financial year to improve the national revenue position, would not be available to Trust’s in 2016/17. The Trust’s forecast was refined accordingly to reflect this and a revised M9 forecast, with a £26.8m deficit, was submitted to NHSI as requested.
• The financial performance in Month 10 plus the critical review of risks at the month end has placed pressure on this revised target and the revised forecast, which is summarised in the table below, identifies a revised forecast deficit of £28.8m unless further remedial action is taken.
• The key drivers to the drift in the year end forecast, in addition to the NHSI confirmation that the £5m assumed Capital to Revenue transfer would not be receivable can be summarised as follows: • Over-Performance Review/Audit –
as referred to earlier, the forecast income for PbR over-performance has been reduced. This follows a detailed review and reconciliation of the activity information flowing through the Rio system in recent months, which has resulted in both actual and forecast activity being reduced and the income assumption being reduced accordingly.
• Healthy Lifestyles Contract – the previous forecast had assumed that while the service would be significantly reduced in 2017/18 a reduced service would continue. The confirmation from

Page 9 of 12
SCC
that this will now terminate on 31 March has resulted in having to increase its redundancy provision. Furthermore, it had been anticipated that the current year activity based contract would change to a block arrangement, as the take-up of the service had not been in line with SCC’s expectations. However as the change is not being transacted, this has reduced the income forecast by £0.3m.
• ASC Run-Rate Pressure – the pressures on the ASC services has resulted in the run rate trajectory continuing to run at a higher level than anticipated in the FRP particularly in respect of the demand and prices pressures in the residential care service.
• FRP Under-delivery – Savings in a number of areas within the FRP are projected not to deliver to the level planned. In particular, the Airs Beds transformation has not proceeded; wheelchairs savings particularly in respect of specialised savings have been less than planned, as have the procurement savings, which have slipped and/or have been scaled back following management review.
• The revised forecast deficit of £28.8m
remains subject to a number of key risks being managed as stated below:-
• Constraint in ASC demand pressures
where considerable risk of escalation over Quarter 4 is a clear concern on the direction of travel over the last 2 months, driven in the main through an upward residential trend;
• Escalation in savings from continued vacancy constraint. The panel process established is required to maintain assurance over this;
• Delivery of non-pay savings arising
from the procurement interventions, the majority of which are expected to manifest over the last quarter;
• Containment of pressures in relation to
aged debtors and performance income within the provisions made in the forecast;
• An acceptable “agreement of
balances” in relation to the transfer of long term care expenditure and income to SCC with effect from 1st April 2017. Currently parties are drawing up a set of principles for agreement as part of the new s75 contract. This is currently in an escalation process;
• A number of contract queries were
raised by health commissioners at the end of January. These are currently being assessed and discussed with commissioners and will need to be managed through without a significant adverse financial impact to deliver the forecast position.
• The outcome of the risks above will compromise the ability of the Trust to deliver the revised deficit forecast of £28.8m. Accordingly, additional rigour is required to maintain the focus on “bottom line” cost control, both across the financial recovery areas, and the underlying cost and income base of the Trust more widely. Accordingly, the Trust’s efforts must focus on both mitigating the risks above while also to continue to seek to deliver financial

Page 10 of 12
savin
gs to seek to deliver the revised target deficit of £26.8m
• It is absolutely critical to focus on a positive and full outcome in relation to the major deliverables in the assumptions above, and this will continue to be a key priority for ELT.

Page 11 of 12
APPENDIX 1: CIP PLAN v ACTUAL

Page 12 of 12

Page 1 of 5
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS
TRUST BOARD MEETING
TO BE HELD ON: 22 FEBRUARY 2017 Subject: Integrated Performance Report – Month 10
Strategic Goal (tick as appropriate):
We will provide high quality and safe services which provide an excellent experience and best possible outcomes
We will work with users and carers to deliver integrated services, simply and effectively
Our organisation will develop and deliver sustainable, innovative services that support independence
Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Jayne Deaville, Director of Finance and Resources
Rose Goodwin, Director of Nursing and Quality
Recommendation: For Approval & Assurance
X For Discussion For Information
PURPOSE OF THE REPORT: The purpose of this report is to provide a concise integrated view of performance across the organisation for December 2016 / January 2017. The report comprises of a summary of performance including Quality, Operational, Finance and Workforce indicators, incorporating trends and benchmarks where appropriate in line with the performance framework that has been adopted by the Partnership Trust. The presentation of quality indicators is based on the Trust’s Quality Priority areas given that the full suite of quality indicators are presented to the Quality and Safety Committee for discussion and assurance each month. The list of Operational indicators reported to FIP in 2016/17 has been rationalised in response to feedback from FIP and Internal Audit. The full list of contractual indicators is monitored and managed at Divisional Business Meetings. Social care performance indicators and targets have not yet been agreed for 2016/17, so we continue to report based on the 2015/16 framework. Reporting Period: FIP and QSC follow different reporting periods based on the need for performance data to be available quickly to respond to contractual processes whereas quality reporting focusses on answering the ‘so what’ question by reporting the full governance cycle once causal investigation is complete. Therefore Performance data relates to January 2017 and Quality data relates to December 2016.

Page 2 of 5
KEY POINTS: Annex 1 - Provides an overview of the Partnership Trust’s month 10 performance and detailed performance against the full suite of the Partnership Trust’s Board indicators. QSC - Quality Exceptions: There are three Red indicators for December 2016 data.
1) Patient feedback on the Quality of Care: The number of respondents who are extremely satisfied with the quality of their clinical treatment or care is 83% against a Trust target of 90%. The North Division achieved a score of 98% for their Quality of Care, the South Division achieved 79%. This relates to peoples experience with access, appointments and waiting times for the SPA, MICATS, Continence Services in Tamworth, Lichfield and Burntwood and IPOPS. Feedback has been offered to individual teams for action.
2) Community avoidable and attributable Grade 3 & 4 pressure ulcers: The Trust has exceeded the tolerance of 21 cases maximum in community services set for our 2016/17 Quality Priorities. There were no cases deemed avoidable and attributable at Pressure Ulcer Review Group in December therefore the year to date total remains 23 for the current reporting period.
3) Mortality – Review all deaths in community hospitals: 71% of deaths occurring in December have had a mortality review tool completed against a target of 100%. The Medical Director has asked colleagues to establish why 4 deaths have yet to be reviewed using the mortality review trigger tool. One death was in Leek (the first death in Leek since June 2016), the other 3 occurred over the Christmas/New Year period. Note that December was the first time in over a year that the trust has not managed to review 100% of all deaths. There is a plan to address and report this position as soon as possible.
Analysis Safety: • Staffing level incidents are the second highest cause group for incidents across the Trust during
this reporting period, at 105 (this was previously 63 and 81 for October and November respectively). The majority of these (70) relate to ILCT teams in Stafford (36), Stoke (22), and Cannock (12). There were also 12 incidents reported by Children’s Services during December 2016.
• Community Grade 3 & 4 pressure ulcers reported: There were 34 Grade 3 & Grade 4 reported
pressure ulcers during December (three of which were classified as grade 4); the RCAs for these incidents will all have been reviewed by PURG by the end of February and an update will be available at the next meeting. There were no pressure ulcers identified as avoidable and attributable at Pressure Ulcer Review Groups during December.
NHS Improvement published a Patient Safety Alert on 22nd July 2016 in relation to Nasogastric Tube Misplacement: continuing risk of death and sever harm (alert reference number: NHS/PSA/RE/2016/006). A self-assessment has been completed as required by the alert and the Trust has systems in place to ensure the delivery of safety critical requirements for initial nasogastric and orogastric tube placement checks. The self-assessment was reviewed against the Trusts current implemented Nasogastric tube standard operating procedures and which continue to be embedded and monitored within the organisation.

Page 3 of 5
Effectiveness: Four Quality Assurance Visits were delivered in December 2016; two teams were rated overall as Good and two teams were rated Requires Improvement against the CQC Key Lines of Enquiry. Immediate actions have been delivered where required with the Quality Team scheduling targeted follow up to those teams requiring improvement to evidence the outcome of remedial actions. Complaints and PALS: The number of formal complaints received has decreased from 24 in November to 19 in December. Experience: Friends and Family Test: From the 2636 service users and carers who answered the Friends and Family Test in December, 97% of respondents would recommend the Trust to friends and family if they needed similar care or treatment, with 1% who would not recommend the Trust. FIP Exceptions: RAG Rating Variations: Overall, of the 38 Partnership Trust’s Board standing performance indicators with targets attached reported through FIP, 21 are green, 3 are amber, and 14 are red. 1 indicator improved its RAG rating from “Amber” to “Green” in January:
• The percentage staff having an “in-date” appraisal increased from 92.33% to 93.30%
against a revised target of 90% (target was 95% until Dec. 2016).
1 indicator deteriorated from “Amber” to “Red” in January: The workforce sickness rate increased from 4.59% to 5.01% against a target of 4.67%. Sickness has increased steadily since September, with Winter having a noticeable effect on short-term absences.
Performance Concerns:
• Social Care: o Social care delayed transfers of care issues remain, although they improved slightly in
January from 2,015 to 1,996 (target = 1,015). In the new S.75 DeToC KPI, the Trust will only be held to account on delays caused by the assessment process (under 1/3 of the current volume of delays).
o The proportion of clients receiving Direct Payments has dropped to 22.0% against a target of 28%. The context surrounding this indicator has changed considerably since the 28% target was originally set. This will be considered during the negotiation of the 2017/18 targets.
• Children’s Services:
o Percentage of New Births that receive a face-to-face new birth visit within 10-14 days by a Health Visitor continued to improve form 79.5% to 82.5%. However, it is now too late for YTD performance currently at 87.3% to reach the 95-98% target for
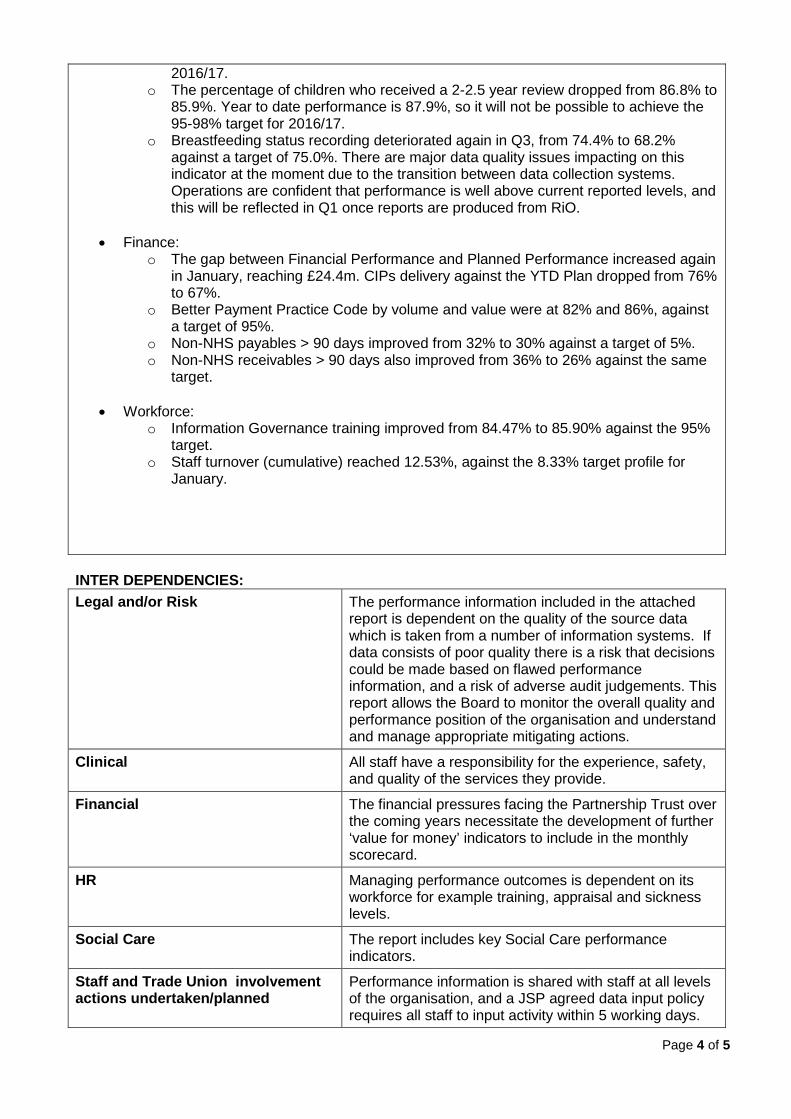
Page 4 of 5
2016/17. o The percentage of children who received a 2-2.5 year review dropped from 86.8% to
85.9%. Year to date performance is 87.9%, so it will not be possible to achieve the 95-98% target for 2016/17.
o Breastfeeding status recording deteriorated again in Q3, from 74.4% to 68.2% against a target of 75.0%. There are major data quality issues impacting on this indicator at the moment due to the transition between data collection systems. Operations are confident that performance is well above current reported levels, and this will be reflected in Q1 once reports are produced from RiO.
• Finance:
o The gap between Financial Performance and Planned Performance increased again in January, reaching £24.4m. CIPs delivery against the YTD Plan dropped from 76% to 67%.
o Better Payment Practice Code by volume and value were at 82% and 86%, against a target of 95%.
o Non-NHS payables > 90 days improved from 32% to 30% against a target of 5%. o Non-NHS receivables > 90 days also improved from 36% to 26% against the same
target. • Workforce:
o Information Governance training improved from 84.47% to 85.90% against the 95% target.
o Staff turnover (cumulative) reached 12.53%, against the 8.33% target profile for January.
INTER DEPENDENCIES: Legal and/or Risk The performance information included in the attached
report is dependent on the quality of the source data which is taken from a number of information systems. If data consists of poor quality there is a risk that decisions could be made based on flawed performance information, and a risk of adverse audit judgements. This report allows the Board to monitor the overall quality and performance position of the organisation and understand and manage appropriate mitigating actions.
Clinical All staff have a responsibility for the experience, safety, and quality of the services they provide.
Financial The financial pressures facing the Partnership Trust over the coming years necessitate the development of further ‘value for money’ indicators to include in the monthly scorecard.
HR Managing performance outcomes is dependent on its workforce for example training, appraisal and sickness levels.
Social Care The report includes key Social Care performance indicators.
Staff and Trade Union involvement actions undertaken/planned
Performance information is shared with staff at all levels of the organisation, and a JSP agreed data input policy requires all staff to input activity within 5 working days.

Page 5 of 5
Patient & Public Involvement The inclusion of service user feedback in performance reporting is essential for Trust Board assurance.
Equality Impact The use of good Data Quality to inform decision making / service delivery is key in ensuring vulnerable groups are not discriminated against. An equality impact assessment has been implemented throughout the development of the Quality Framework and associated work programmes.
Information exempt from Disclosure NA Requirement for further review Monthly RECOMMENDATIONS: The Trust Board are asked to note the content of the executive summary and performance scorecard.

INDICATORTRUST MONTH
FIGURES
2016/17 TARGET RAG DIRECTION*
2015/16 MONTHLY TRUST WIDE
AVERAGEEXPLANATION AND ACTIONS Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
No. 1) SAFETY
1.1 Total No. Incidents Reported (Safeguard system) 1199 N/A - Quality Priority 1
914 874 1026 1057 1104 1013 1072 1138 1199 9397
1.2 Percentage of reported incidents classified as serious incidents (meeting STEIS definition)
0.00% <3.47% Green Quality Priority 1 0.80% 1.19% 0.28% 1.06% 0.65% 0.72% 0.40% 0.26% 0.00% 0.60%
1.3 Serious incident Falls reported (STEIS) resulting in severe injury or death YTD
5 11 Green Quality Priority 1 1 2 3 4 4 4 4 5 5 5
1.4 Total No. Community - Avoidable and Attributable Grade 3 & 4 (YTD)
23 21 Red Quality Priority 1 3 7 7 13 18 21 22 23 23 23
1.5 Total No. Hospitals - Avoidable and Attributable Grade 3 & 4 (YTD)
0 0 Green Quality Priority 1 0 0 0 0 0 0 0 0 0 0
2) EXPERIENCE
2.1 Overall FFT Sample Score (Recommend %) 97% 90% Green 97% 98% 97% 97% 96% 98% 98% 98% 97% 97% 97%
2.2 Overall FFT Sample Score (Not Recommend %) 1% <5% Green 0.59% 1% 0.40% 1% 1% 0.44% 0.50% 0.45% 1% 1% 1%
2.3 Patient feedback on the Quality of Care(taken from service user and carer survey)
83% 90% Red 85%Due to the specific nature of feedback on
quality of care localised actions have been reported to DBMs
Quality Priority 2
84% 84% 83% 85% 86% 85% 86% 82% 83% 84%
3) EFFECTIVENESS
3.3
Feedback from service users and carers that they feel involved in decisions regarding their individualised plans of care. (taken from service user and carer survey)
95% 90% Green 96% uality Priorit 97% 97% 96% 97% 96% 96% 96% 96% 95% 96%
3.4 Mortality – Review all unexpected deaths in our community services
100% 100% Green n/a Taken from Medical Director report to CQRM
uality Priorit 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
3.5 Mortality – Review all deaths in community hospitals
71% 100% Red n/a Taken from Medical Director report to CQRM
uality Priorit 100% 100% 100% 100% 100% 100% 100% 100% 71% 100%
Quality Scorecard February 2017(December Data)
n/a
Quality Priority 2
*Sparklines provide a general direction indicator only, and should be read along with the numerical data
Quality Priorities

Page 1 of 3
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS
TRUST BOARD MEETING TO BE HELD ON: 22 FEBRUARY 2017
Subject: Corporate Risk Register
Strategic Goal (tick as appropriate):
We will provide high quality and safe services which provide an excellent experience and best possible outcomes
We will work with users and carers to deliver integrated services, simply and effectively
Our organisation will develop and deliver sustainable, innovative services that support independence
Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Rose Goodwin – Director of Nursing and Quality
Recommendation: For Approval & Assurance
X For Discussion For Information
PURPOSE OF THE REPORT: The Corporate Risk Register is appended to this Report for review and to note the changes that have taken place through the Executive Risk Management Committee on 14 February 2017. The Board is asked to take assurance that the reported risks are the subject of risk controls and actions to mitigate the residual risk reported on the Corporate Risk Register. KEY POINTS: Corporate Risk Register The Risk Register has been reviewed and the following changes have been made and approved at the Executive Risk Management Committee.
• Risk Ref 01 ~ Insufficient standard Domiciliary Care capacity. The risk has been updated to include the following: Where the Living Independent Staffordshire (LIS) as ‘provider of last resort’ is required by Commissioners to provide maintenance packages of care (PoC) due to Independent Sector capacity shortfalls, the relevant clauses within the new Section 75 Adult Social Care Agreement ensure that these requests are not to the financial detriment to the Trust.
• Risk Ref 04B ~ Community Nursing Capacity (South Division). The risk had previously been discussed and separated into two elements, underfunding of commissioned services and impact of lack of capacity on front line services. This risk has been reviewed and redefined with the addition of a new risk relating to the impact on front line services (reference 848).
• Risk Ref 677 ~ Inability to recruit and sustain staffing levels in Community Hospitals. This risk has been updated to define that the risk is specific to nurse staffing levels.

Page 2 of 3
No risks were identified for de-escalation from the Corporate Risk Register. One new risk was discussed for addition to the Corporate Risk Register. The risk added is as follows:
• Risk Ref 848 ~ Community Nursing Capacity (South Division) due to recruitment and retention difficulties.
An emerging risk relating to difficulties in the practical application and implementation of RiO was identified and discussed at the Committee. It has been agreed that this needs to be fully scoped and will be added to the Corporate Risk Register at Executive Risk Management Committee in March 2017. The Workforce Directorate and Finance Directorate Risk Registers were presented at Executive Risk Management Committee as part of the deep dive schedule. No risks were identified from either deep dive for escalation to the Corporate Risk Register. The Executive Risk Management Committee identified some potential gaps in the Finance Directorate Risk Register and has therefore requested that this is reviewed at the Committee in April 2017. A proposed deep dive schedule for 2017/18 was agreed by the Committee. The Board Assurance Framework was presented to the Committee and it was agreed not to submit to the Trust Board this month. It was agreed that both the Board Assurance Framework and the Corporate Risk Register would be reviewed, refined and refreshed at the Committee in March 2017 in preparation for the new financial year. The Corporate Risk Register and Board Assurance Framework will be presented to Trust Board in March 2017. INTER DEPENDENCIES: Legal and/or Risk An effective Risk Management Strategy linked to the Board Assurance
Framework and the Corporate Risk Register will mitigate risks the organisation’s Strategic Objectives and provides assurance that risks are being managed.
Clinical Those risks which are clinical are assigned to the relevant Directorate for mitigation with updates through the governance of the Quality & Safety Committee.
Financial Financial risks or risk with financial implications are escalated onto the corporate risk register
HR HR risks are escalated onto the Corporate Risk Register
Social Care The impact of the evolution of the integration is the subject of ongoing review by the Executive Risk Management Committee.
Staff and Trade Union involvement actions undertaken/planned
Staff and trade union involvement is through either Committee (e.g. workforce and health and safety) as risk are escalated/de-escalated or through local discussions within Divisions.
Patient & Public Involvement
We are engaging with those patients and their families who are affected by decisions to decommission services.
Equality Impact The impact on services which are decommissioned is assessed by the CCGs
Information exempt from Disclosure
None
Requirement for further review
The Corporate Risk Register is reviewed monthly.

Page 3 of 3
RECOMMENDATIONS: The Trust Board is recommended to:
• Note the updated version of the Corporate Risk Register appended to this Report; • Note the actions that are being taken to manage the reported risks; • Note the other activities undertaken by the Executive Risk Management Committee during
February 2017.

Nu
mb
er
CQ
C D
om
ain
Ad
ded
to
Reg
iste
r
Stra
tegi
c O
bje
ctiv
e Division,Direcotrate,Department
Review Cycle and Last Updated
Description of Risk
CauseEffectImpact
Init
ial R
isk
Rat
ing
Init
ial L
ikel
iho
od
Init
ial I
mp
act
Details of Risk Control Actions Planned Action Progress
Cu
rren
t Li
kelih
oo
d
Cu
rren
t Im
pac
t
Lead
Dir
ecto
r
Lead
Man
ager
Lead
Off
icer
Targ
et R
isk
Rat
ing
Targ
et L
ikel
iho
od
Targ
et Im
pac
t
Ris
k P
roxi
mty
Risk Register - Corporate Risks
Res
idu
al R
atin
g
Dir
ecto
r O
f O
per
atio
ns
Dir
ecto
r O
f O
per
atio
ns
Dir
ecto
r O
f O
per
atio
ns
3-6
Mo
nth
s
Res
po
nsi
veSa
fe
01 CorporateOperationsDirectorate
SG2 Monthy
06/02/2017Insufficient standard domiciliary care and enhanced domiciliary carepackages which presents a significant risk to the Trust as a result ofre-commissioning plans of the County Council.
Cause: There is insufficient Domiciliary Care provision in the market
Effect: Referrals of unmet need back to community services. Registeredstaff (Band 5 and above) inappropriately delivering care that could beprovided by non-registered staff (Band 2 or 3)
Impact: Additional impact on the capacity of community services ascore services are being drawn in to meet unmet market demand. Delaysto discharge from acute and community inpatient wards. Concernsabout compromise to patient safety.
4 5 44 34There is continualescalation of risk to SCCand Board to Boardescalation.
Agreement has been reachedwith Commissioners toextend the current enhancedLIS capacity (reablement)which will funded by the CCG.Stoke City Council aredeveloping in-house DomCare capacity
Plan received from CountyCouncil. Where the LIS as'provider of last resort' isrequired by Commissioners toprovide maintenance PoC dueto Independent Sector capacityshortfalls, the relevant clauseswithin the new Section 75 ASCAgreement ensure that theserequests are not to the financialdetriment of the Trust.
The North are looking intoextending the CCGcommissioned LIS service.
In the South, existing LIS serviceis currently engaged in a formalmanagement of changeprocess.
Additionally, StaffordshireCounty Council have confirmedthat they are looking to identifyIndependent Sector Dom Careproviders.
The position in Stoke iscurrently causing particularconcern across the LocalHealth Economy.
Date Entered : 10/02/2017 11:35
20 16 12
01
/08
/20
12
Risk reviewedand actionsupdated
Date Printed: 15/02/2017 Page 1 of 7

Nu
mb
er
CQ
C D
om
ain
Ad
ded
to
Reg
iste
r
Stra
tegi
c O
bje
ctiv
e Division,Direcotrate,Department
Review Cycle and Last Updated
Description of Risk
CauseEffectImpact
Init
ial R
isk
Rat
ing
Init
ial L
ikel
iho
od
Init
ial I
mp
act
Details of Risk Control Actions Planned Action Progress
Cu
rren
t Li
kelih
oo
d
Cu
rren
t Im
pac
t
Lead
Dir
ecto
r
Lead
Man
ager
Lead
Off
icer
Targ
et R
isk
Rat
ing
Targ
et L
ikel
iho
od
Targ
et Im
pac
t
Ris
k P
roxi
mty
Risk Register - Corporate Risks
Res
idu
al R
atin
g
Dir
ecto
r O
f O
per
atio
ns
Ch
ief
Op
erat
ing
Off
icer
- S
ou
th
Dir
ecto
r O
f O
per
atio
ns
0-3
Mo
nth
s
Effe
ctiv
eSa
fe
04B South DivisionOperationsDirectorate
SG2 Monthy
03/02/2017Risks to level (capacity) of service provision in Community Nursingservices - South Division
Cause: Changes in the commissioning arrangements for the communitynursing workforce. Staff turnover and sickness. Underfunding ofservices by Commissioners in the Stafford area. This is a historical riskwhich is recognised and acknowledged by Commissioners.
Effect: High pressure on services. Impact on Day and Night provision ascare carried across where visits have not been achieved.
Impact: Concerns about safety and quality of care. Low moraleamongst staff. Impact on a large number of patients.
Full impact cannot be quantified as the service is not fully staffed to allposts.
(PMO Work stream - Workforce)
4 4 44 34Safer Staffingimplementationprogramme.
Reviews at Area BusinessMeetings and DivisionalBusiness Meetings
A demand and capacityanalysis of Community NurseStaffing to be undertaken
New starters commenced inJanuary. Further recruitmenttook place 27 Janaury which willfurther support the serviceonce staff commence in posts.
Date Entered : 10/02/2017 11:47
Creation of new role forsenior District Nurses
Agreement has been reachedwith Professional NursingLeads and Director of Nursingand Quality to create a new rolefor senior District Nurses tosupport more junior staff.
The job description is currentlybeing finalised prior toadvertising as 'ILCT ClinicalLead', Band 7. The jobdescription is due to bepresented to an AFC panel 15February 2017 and should thenbe presented to CCP 28February 2017.
Date Entered : 15/02/2017 10:09
16 16 12
01
/10
/20
14
Riskamended toreflectrelation tounder-commissioning ofservice, asrequested byERMC,thereforesaved as newversion.
Dir
ecto
r O
f W
ork
forc
e A
nd
Dev
e
Ass
oci
ate
Dir
ecto
r O
f H
um
an R
eso
urc
es
Dir
ecto
r O
f W
ork
forc
e &
Dev
elo
pm
ent
0-3
Mo
nth
s
Safe06 Corporate
WorkforceDirectorateWorkforce &DevelopmentDirect
SG2 Monthy
06/02/2017Inability to sustain District Nurse staffing levels in the Trust due toturnover of staff.
Cause: There is currently a National shortage of District Nurses availableto fill current vacancies.
Effect: Increased number of vacancies and/or skills gaps withinoperational teams. Low staff morale.
Impact: Compromise to patient care and safety, less able to deliver tocontract specifications. Breach of contract delivery - penalties/fines.Staff support systems compromised, e.g. appraisals.
(PMO Work stream - Workforce)
3 5 53 43Regular monitoringthrough EMT andWorkforce MattersCommittee
Deputy to Director ofWorkforce commenced inpost.,
All vacancies notified toDirector of Workforce torapidly identify trends.
There is a 6 week Band 5Community Nursing andBand 5 CommunityHospital Nursingdevelopment programmein place to supportindividuals to undertaketheir roles effectively, tounderstand their roles
Support is being provided tonew nurse starters by theExecutive Leadership Team
Each Executive Director wasasked to contact a number ofnew starters to ensure that theyhad all the necessaryinformation, equipment etc. oncommencement of their rolesand to obtain feedback on theirexperience. This was completedand further contact will bemade with these staff 3 monthsfollowing commencement ofemployment.
Date Entered : 06/01/2017 11:54
Information obtained throughthe new exit interview processis to be collated and sorted byDivision, themes etc. Implementing Change Grouplooking at recruitment and
Implementing Change Grouppresented their report toDirector of Workforce andDevelopment and Unions inDecember 2016. A toolkit hasbeen developed. A meeting wasscheduled to take place week
15 15 12
11
/11
/20
14
Risk reviewedand actionsupdated
Date Printed: 15/02/2017 Page 2 of 7

Nu
mb
er
CQ
C D
om
ain
Ad
ded
to
Reg
iste
r
Stra
tegi
c O
bje
ctiv
e Division,Direcotrate,Department
Review Cycle and Last Updated
Description of Risk
CauseEffectImpact
Init
ial R
isk
Rat
ing
Init
ial L
ikel
iho
od
Init
ial I
mp
act
Details of Risk Control Actions Planned Action Progress
Cu
rren
t Li
kelih
oo
d
Cu
rren
t Im
pac
t
Lead
Dir
ecto
r
Lead
Man
ager
Lead
Off
icer
Targ
et R
isk
Rat
ing
Targ
et L
ikel
iho
od
Targ
et Im
pac
t
Ris
k P
roxi
mty
Risk Register - Corporate Risks
Res
idu
al R
atin
g
within the widerOrganisation and topromote and encouragestaff satisfaction
Staffing levels aremonitored weekly throughthe incident summaryreport to the ELT meeting
retention. Report to becompleted by end of July2016.
commencing 09 January 2017 toagree the roll out andimplementation of the toolkit,however, this meeting neededto be rescheduled. The meetinghas been rescheduled for 06March 2017
Date Entered : 10/02/2017 10:59
Recruitment to vacant postscontinues
Additional recruitment eventsare still being planned forDerbyshire, Shropshire andCheshire. A Keele event is beingheld week commencing 20February 2017 and a furtherevent has been arranged forBritannia Stadium.
A campaign on Facebook andTwitter ran over the weekend of04-05 February 2017.
Bradwell Hospital is due toclose 31 March 2017 and anystaff wishing to be re-deployedwill be supported to do so.
Date Entered : 15/02/2017 09:01
STP Task Force review ofnursing requirements
A task to finish group has beenestablished to look atde-ploying staff who areidentified as 'at risk'.
Discussions are underwaylooking at Internationalrecruitment opportunities foracross the Staffordshrie LocalHealth Economy.
Date Entered : 10/02/2017 11:03
Date Printed: 15/02/2017 Page 3 of 7

Nu
mb
er
CQ
C D
om
ain
Ad
ded
to
Reg
iste
r
Stra
tegi
c O
bje
ctiv
e Division,Direcotrate,Department
Review Cycle and Last Updated
Description of Risk
CauseEffectImpact
Init
ial R
isk
Rat
ing
Init
ial L
ikel
iho
od
Init
ial I
mp
act
Details of Risk Control Actions Planned Action Progress
Cu
rren
t Li
kelih
oo
d
Cu
rren
t Im
pac
t
Lead
Dir
ecto
r
Lead
Man
ager
Lead
Off
icer
Targ
et R
isk
Rat
ing
Targ
et L
ikel
iho
od
Targ
et Im
pac
t
Ris
k P
roxi
mty
Risk Register - Corporate Risks
Res
idu
al R
atin
g
Dir
ecto
r O
f W
ork
forc
e A
nd
Dev
e
Sen
ior
Hr
Bu
sin
ess
Par
tner
- C
hild
ren
'S &
Co
rpo
rat
Ass
oci
ate
Dir
ecto
r O
f H
um
an R
eso
urc
es
0-3
Mo
nth
s
Safe677 Corporate
WorkforceDirectorateWorkforce &DevelopmentDirect
SG2 Monthy
06/02/2017Inability to recruit and sustain Nurse staffing levels in CommunityHospitals due to uncertainty in Commissioner intentions
Cause: Increase turnover of staff and uncertainty of Commissionerintentions.
Effect: Increased numbers of vacancies and/or skills gaps withinoperational teams. Low staff morale.
Impact: Compromise to patient care and safety, less able to deliver tocontract specifications. Staff support systems compromised e.g.appraisals
4 5 44 43Regular monitoringthrough EMT andWorkforce MattersCommittee.
Deputy Director ofWorkforce commenced inpost.
4 UHNM employees(previously SSOTP) havereturned as substantivestaff.All vacancies notified toDirector of Workforce torapidly identify trends.
Monthly safe staffingreports are provided bythe Director of Nursingand Quality
Current uncertaintiesregarding CommunityHospitals are impacting onthe Organisations ability torecruit to current vacancies.
There are 20 WTE vacancies asat 09 January 2017.
There is a need to reducecurrent spend on bank andagency staff. If bank/agency arerequired, over current staffingestablishment, due to acuity ofpatients, beds will be closed inorder to prevent the need tobook additional bank and/oragency staff.
Formal escalation to CQRM RiskRegister by Executive Directorstook place in January 2017.
Date Entered : 10/02/2017 10:40
Information obtained throughthe new exit interview processis to be collated and sorted byDivision, themes, etc.
Implementing Change Groupare reviewing recruitment andretention and will provide areport end of July 2016
Implementing Change Grouppresented their report toDirector of Workforce andDevelopment and Unions inDecember 2016. A toolkit hasbeen developed. A meeting wasscheduled to take place weekcommencing 09 January 2017 toagree the roll out andimplementation of the toolkit,however, this meeting neededto be rescheduled. The meetinghas been rescheduled for 06March 2017
Date Entered : 10/02/2017 10:41
Ongoing recruitment tovacancies
Additional recruitment eventsare still being planned forDerbyshire, Shropshire andCheshire. A Keele event is beingheld week commencing 20February 2017 and a furtherevent has been arranged forBritannia Stadium.
Date Entered : 15/02/2017 09:03
20 16 12
21
/03
/20
16
Risk reviewedand actionsupdated
Date Printed: 15/02/2017 Page 4 of 7

Nu
mb
er
CQ
C D
om
ain
Ad
ded
to
Reg
iste
r
Stra
tegi
c O
bje
ctiv
e Division,Direcotrate,Department
Review Cycle and Last Updated
Description of Risk
CauseEffectImpact
Init
ial R
isk
Rat
ing
Init
ial L
ikel
iho
od
Init
ial I
mp
act
Details of Risk Control Actions Planned Action Progress
Cu
rren
t Li
kelih
oo
d
Cu
rren
t Im
pac
t
Lead
Dir
ecto
r
Lead
Man
ager
Lead
Off
icer
Targ
et R
isk
Rat
ing
Targ
et L
ikel
iho
od
Targ
et Im
pac
t
Ris
k P
roxi
mty
Risk Register - Corporate Risks
Res
idu
al R
atin
g
Dir
ecto
r O
f Fi
nan
ce A
nd
Res
ou
r
Dep
uty
Dir
ecto
r O
f Fi
nan
ce
Dep
uty
Dir
ecto
r O
f Fi
nan
ce
0-3
Mo
nth
s
Effe
ctiv
e719 CorporateFinanceFinancialManagement
SG5 Monthy
14/02/2017There is a risk that the Trust will not be able to meet it's financial targetdue to the current level of spending on Adult Social Care beingsignificantly higher than the contract value; this is currently assessed at£11.7 million (as at Month 9).
Cause: The level of transformation savings identified in the originalmodel have not been identified.Effect: The Trust will be unable to meet it's financial target for the year.The Trust will be required to identify additional savings to off set thedeficit.
Impact: The Trust may be put into financial special measures and besubject to a greater degree of performance management from NHSI
Links to risk ref 760 on Corporate Risk Register and risk ref 720 onFinance Directorate Risk Register
4 5 54 24KPMG have reviewed thetransformation plan andvalidated the level ofsavings deliverable in2016/17. These have beenconfirmed at £2.8 million
Weekly negotiationmeetings have beenestablished with SCC tonegotiate the section 75contract for 2016/17 andbeyond.
The Trust has given noticeon the existing section 75contract.
The Trust has recruited aDirector of Adult SocialCare
The Director of Financeand Resources has metwith the Trust's externalauditors to ensure thatthey are fully briefed onthe likely financial out turnfor the Trust
Renegotiation of s75 contractfor 2017/18, while notimpacting on the 2016/17financial performance, willsignificantly reduce thefinancial risk related to SocialCare rolling forward acrossfinancial years.
Targeting date for signing ofnew s75 agreement is the endof February 2017
Date Entered : 08/02/2017 10:11
Weekly negotiation meetingswith SCC are ongoing
Agreement has been reachedwith SCC to increase thecontract value for inflation andfor SCC's share of the projectedoverspend under the risksharing agreement
Date Entered : 04/11/2016 13:58
Financial recovery plan to bedeveloped
A paper was presented to FIPand Board in October 2016 thatpresented a financial risk rangeof £21.7 - £26.2 million if nomitigating actions areimplemented. This includes a£15.6 million projectedoverspend for Adult Social Care.
Following these meetings,financial recovery actions arebeing developed to improve onthis position and these werediscussed at ELT 08/11/2016.Additional meetings are beingarranged to review theproposals further.
Date Entered : 16/11/2016 09:56
Financial review meetings arebeing held with NHSI
The Trust is meeting with NHSIon 28 November 2016 to reviewthe financial position for theyear
Date Entered : 04/11/2016 14:01
Vacancy control processesimplemented within AdultSocial Care
There is no further update; staffare in post on fixed term tomanage the risk to servicethought the D2A developmentphase over the next few
20 20 8
02
/06
/20
16
Action 6updated
Date Printed: 15/02/2017 Page 5 of 7

Nu
mb
er
CQ
C D
om
ain
Ad
ded
to
Reg
iste
r
Stra
tegi
c O
bje
ctiv
e Division,Direcotrate,Department
Review Cycle and Last Updated
Description of Risk
CauseEffectImpact
Init
ial R
isk
Rat
ing
Init
ial L
ikel
iho
od
Init
ial I
mp
act
Details of Risk Control Actions Planned Action Progress
Cu
rren
t Li
kelih
oo
d
Cu
rren
t Im
pac
t
Lead
Dir
ecto
r
Lead
Man
ager
Lead
Off
icer
Targ
et R
isk
Rat
ing
Targ
et L
ikel
iho
od
Targ
et Im
pac
t
Ris
k P
roxi
mty
Risk Register - Corporate Risks
Res
idu
al R
atin
g
months.
Date Entered : 14/02/2017 09:23
Dir
ecto
r O
f O
per
atio
ns
Ch
ief
Op
erat
ing
Off
icer
(N
ort
h)
Dir
ecto
r O
f O
per
atio
ns
Effe
ctiv
eSa
fe
772 North Division
SG1 Monthy
10/02/2017Risk to delivery of District Nursing service across the northern divisiondue to capacity, particularly affected are City, Newcastle and Moorlandsareas
Cause: High level of absence within north division District NursingServices due to vacancies, long term and short term sickness andmaternity leave is impacting on capacity to deliver service safely to meetdemand. In addition, there is evidence that demand is increasing andgreater than the commissioned capacity; this is being monitored.
Effect: Increased pressure on staff and managers delivering the serviceto ensure that patient needs can be met safely. Daily review of servicecapacity can result in clinics cancelled and patient visits rescheduled.Some senior staff are being to work clinically resulting in them notbeing able to support new starters.
Impact: Concerns about safety and quality of care. Low moraleamongst staff. Increased risk of sickness and turnover. Patient care andsafety may be compromised, quality of documentation and recordingmay be compromised. Less support available for new starters.
4 5 44 24Redeployment on atemporary basis of stafffrom other areas ofNursing services.Specialist Teamssupporting
Daily conference calls ineach locality with ExecDirectors and OperationalLeads to manage capacity
Ongoing monitoring ofrescheduled visits toensure patient/serviceuser safety is maintained
Enhanced Team visits fromExecutive andNon-Executive Directors tosupport Teams (North andSouth)
Daily reviews of demand andcapacity continue withongoing monitoring ofrescheduled visits.
The numbers of District Nurseshas improved. There has been areduction in the number ofsafe staffing incidents beingreported. District Nursedemand and capacity work isunderway.
Date Entered : 10/02/2017 12:20
Staff are being recruited tovacant posts
The position is cautiousimprovement,Overall in DN teams we haverecruited to more vacancies andhave a cohort of newlyRegistered Staff who areworking through preceptorship.A number of teams have movedfrom Red to Amber but someteams have the correct staffnumber but some new staff asyet inexperienced incommunity nursing.Maternity Leave remainsproblematic.District Nurses are facingincreasing urgent on the dayreferrals which challengeplanned work.Sickness levels are currentlyhigh in some teams - with nospecific themes or trends. HRand Managers sicknesssurgeries are being piloted toproactively manage this.
Date Entered : 15/02/2017 09:05
20 16 8
06
/09
/20
16
Risk reviewedand actionsupdated
Date Printed: 15/02/2017 Page 6 of 7

Nu
mb
er
CQ
C D
om
ain
Ad
ded
to
Reg
iste
r
Stra
tegi
c O
bje
ctiv
e Division,Direcotrate,Department
Review Cycle and Last Updated
Description of Risk
CauseEffectImpact
Init
ial R
isk
Rat
ing
Init
ial L
ikel
iho
od
Init
ial I
mp
act
Details of Risk Control Actions Planned Action Progress
Cu
rren
t Li
kelih
oo
d
Cu
rren
t Im
pac
t
Lead
Dir
ecto
r
Lead
Man
ager
Lead
Off
icer
Targ
et R
isk
Rat
ing
Targ
et L
ikel
iho
od
Targ
et Im
pac
t
Ris
k P
roxi
mty
Risk Register - Corporate Risks
Res
idu
al R
atin
g
Dir
ecto
r O
f O
per
atio
ns
Dir
ecto
r O
f O
per
atio
ns
0-3
Mo
nth
s
Safe848 South Division
OperationsDirectorate
SG5 Monthy
10/02/2017Risk to level (capacity) of service provision in the Community NursingServices - South Division
Cause: Recruitment and retention difficulties wihtin the current DistrictNursing Services
Effect: High pressure on services. Impact on day and night provision ascare carried out across where visits have not been achieved.
Impact: Concerns about safety and quality of care. Low moraleamongst staff. Impact on large number of patients.
Links to risk ref 04B on Corporate Risk Register
4 4 44 34Safer staffingimplementationprogramme.
Reviews at Area BusinessMeetings and DivisionalBusiness Meetings.
New role for senior DistrictNurses to support morejunior staff
Agreement has been reachedwith Professional NursingLeads and Director of Nursingand Quality to create a new rolefor senior District Nurses tosupport more junior staff.
The job description is currentlybeing finalised prior toadvertising as 'ILCT ClinicalLead', Band 7. The jobdescription is due to bepresented to the vacancyscrutiny panel weekcommencing 13 February 2017
Date Entered : 10/02/2017 11:58
Demand and capacity analysisof Community Nurse staffingto be undertaken
New starters commenced inpost January 2017. Additionalrecruitment took place 27January which will support theservice once staff commence inpost.
Date Entered : 10/02/2017 12:00
Media campaigns to be heldto attract new staff
Facebook and Twitter campaignheld over weekend of 04-05February 2017.
Additional recruitment eventsare being planned forDerbyshire, Shropshire andCheshire. A Keele event hasbeen planned for weekcommencing 20 February 2017and an additional recruitmentevent at Britannia Stadium hasbeen scheduled.
Date Entered : 15/02/2017 09:06
16 16 12
10
/02
/20
17
New riskadded asrequested byERMC
Date Printed: 15/02/2017 Page 7 of 7

1
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS
TRUST BOARD MEETING
TO BE HELD ON: 22 February 2017
Subject: Well Led Improvement Plan
Strategic Goal (tick as appropriate):
We will provide high quality and safe services which provide
an excellent experience and best possible outcomes We will work with users and carers to deliver integrated
services, simply and effectively Our organisation will develop and deliver sustainable,
innovative services that support independence Our workforce will be empowered and supported to deliver
care in a way that is consistent with our values
We will make excellent use of our resources and improve levels of efficiency across our services
Director Lead: Jenna Davies- Interim Company Secretary
Recommendation: For Approval & Assurance
For Discussion X For Information
PURPOSE OF THE REPORT: The CQC inspected the Trust in November 2015 and rated the Trust as ‘requires improvement’, and inadequate for the ‘Well Led Domain’. Following on from this NHSI commissioned a capacity and capability review into the leadership and governance of the organisation. The plan has been developed to ensure that the recommendations from the following have been captured and responded to; 1. Well-Led Review 2. NHSI capacity and capability review 3. CQC inspection (only Well-led actions) 4. NHSI observations 5. Red 10 Board Development sessions KEY POINTS: Work has progressed on the delivery of the actions outlined within the Well Led Plan. No Board Committees have met since the writing of this paper and a verbal update from the Finance, Investment and Performance committee will be given at Board Progress to date;

2
Key theme Number of Actions Completed On Track Some
Issues Off Track
Strategy and Development 24 9 15 0 0
Risk Management 20 11 9 0 0
Board skills and Capacity 13 3 10 0 0
Culture and Organisational Development 16 10 5 1 0
Leadership 29 14 15 0 0
Governance 40 13 27 0 0
The following recommendations are currently rated as ‘Off Track’ OD05- Staff morale in community adult nursing services was low. Staff told us they felt despondent, demoralised, frustrated and let down by senior managers. The Trust has responded to the annual staff survey (2015) with a number of focussed action plans and refocused organisational health activities to support improved morale. Given the level of tendering, contractual renegotiation and decommissioning associated with services delivered by the Trust this has had an impact on staff and their morale. Leaders have pre-empted change where possible to engage staff in planned service tender and change processes (i.e. children’s service review). However given the continued difficulties in maintaining a stable workforce and managing demand within community nursing further targeted work is required to support morale and encourage staff retention. These actions are being monitored by the CQC steering group as well as Workforce Matters INTER DEPENDENCIES: Legal and/or Risk This paper should be considered in relation to key risks contained in
the Board Assurance Framework. The Well-Led improvement plan identifies a number of risks and these are considered and mitigated by Board Committees
Clinical The Well-Led Action plan identifies improvements to the overall Corporate governance, leadership and culture of the organisation which will support the delivery of good clinical governance and quality care
Financial There is no financial impact to deliver the Well led Improvement plan.
HR Human resource issues will be considered as the plan progresses

3
Social Care There are no social care specific issues identified
Patient & Public Involvement
There is no direct public or patient involvement in the plan however the updates against the plan will be reported monthly through the public board meetings..
Equality Impact None identified at this time
Information exempt from Disclosure
No
Requirement for further review
Bi-Weekly updates will be provided to the Executive Leadership Team. Monthly updates to Board and Board Committees
RECOMMENDATIONS: The Board of Directors is requested to;
• Note the updates against the well led improvement plan

4