melanoma frontline approach
TRANSCRIPT
melanocyte
melanoma
epidermis
dermis
Frontline Approach to Metastatic BRAF-Mutant
Melanoma Diagnosis, Molecular Evaluation, and
Treatment ChoiceByEreny S. Poles
Ass.lecutrer of clinical oncology , Assuit university

45 yo man with ‘mole’ on his back for years presented with headaches and was found to have widespread (brain, liver, lung, bowel spread) liver biopsy showed metastatic melanoma

Patients with metastatic melanoma had few treatment options

2011
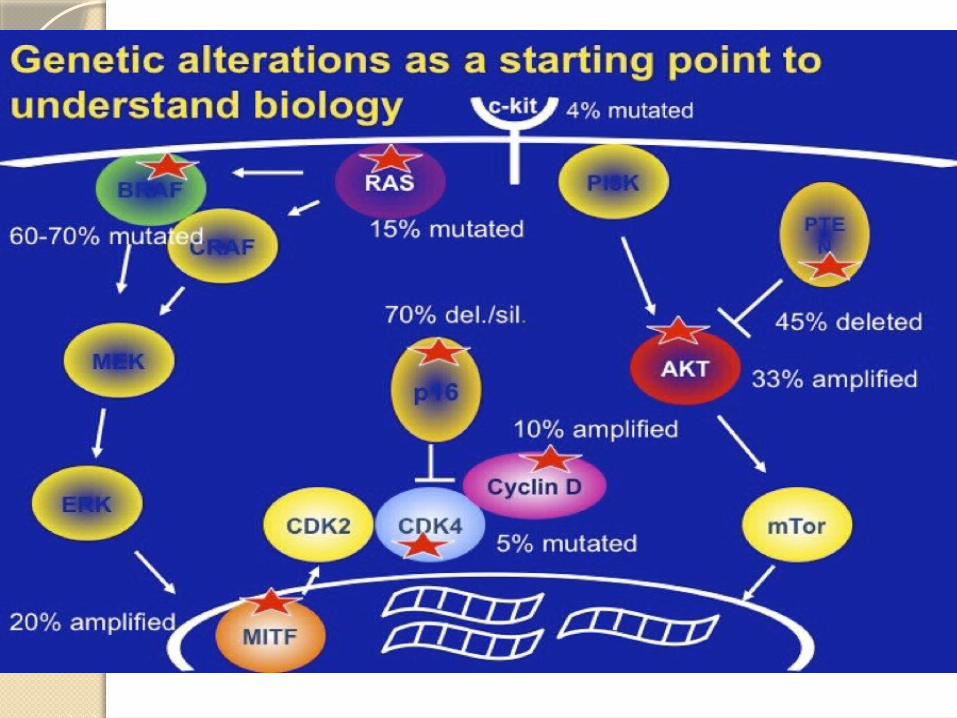
When we begin to understand the biology , it is the real beginning

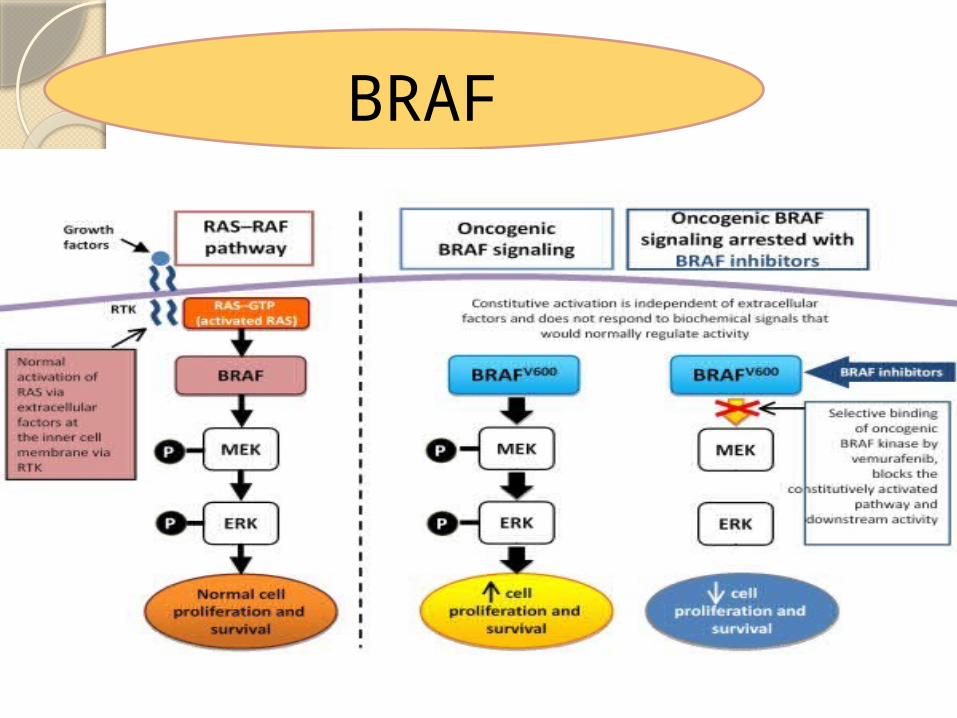
BRAF mutation
Melanoma is
immunogeneic
tumour
BRAF mutation

• BR AF is a serine/threonine protein kinase, encoded on chromosome 7q34, that activates the M AP kinase/ERKsignaling pathway. BR AF is the family member most easily activated by Ras (1)
• In fact , approximately 50 % of melanomas harbor activating
• BR AF mutations. Among the BRAF mutations observed in melanoma, over 90 % are at codon 600, and among these, over 90 % are a single nucleotide mutation resulting in substitution of glutamic acid for valine (BR AF V600E: nucleotide 1799 T > A; codon GTG > GAG).
• The second most common mutation is BRAF V600K substituting lysine for valine, that represent s 5-6 % (GTG > AAG), followed by BR AF V600R (GTG > AGG), an infrequent two-nucleotide variation of the predominant mutation, BR AF V600 ′ E2′(GTG > GAA), and BR AF V600D (GTG > GAT ) [2]. 1.Niault TS, Baccarini M: Targets of Raf in tumorigenesis. Carcinogenesis 2010,31:1165–1174
2.Long GV, Menzies AM, Nagrial AM, Haydu LE, Hamilton AL, Mann GJ, Hughes TM, Thompson JF, Scolyer RA, Kefford RF: Prognostic and
clinicopathologic associations of oncogenic BRAF in metastaticmelanoma. J Clin Oncol 2011, 29:1239–1246.

BR AF V600E has been implicated in different mechanisms of melanoma progression, and principally the activation of the downstream MEK/ERK pathway, evasion of senescence and apoptosis, unchecked replicative potential, angiogenesis (through MEK-dependent activation of HIF-1α and VEGF)*
*Maurer G, Tarkowski B, Baccarini M: Raf kinases in cancer-roles andtherapeutic opportunities. Oncogene 2011, 30:3477–3488.
The second step is MEK- ERK

Now there are two targets
BRAF mutation V600E
MEK – ERK Pathway

First how to assess BRAF mutation ?
Immunohistochemistry
or genetic assay
1-Real-time Polymerase Chain Reaction
2-Next-generation sequencing
3-Immunohistochemistry 4-Circulating tumor-derived DNA
Done only for proven metaststic disease
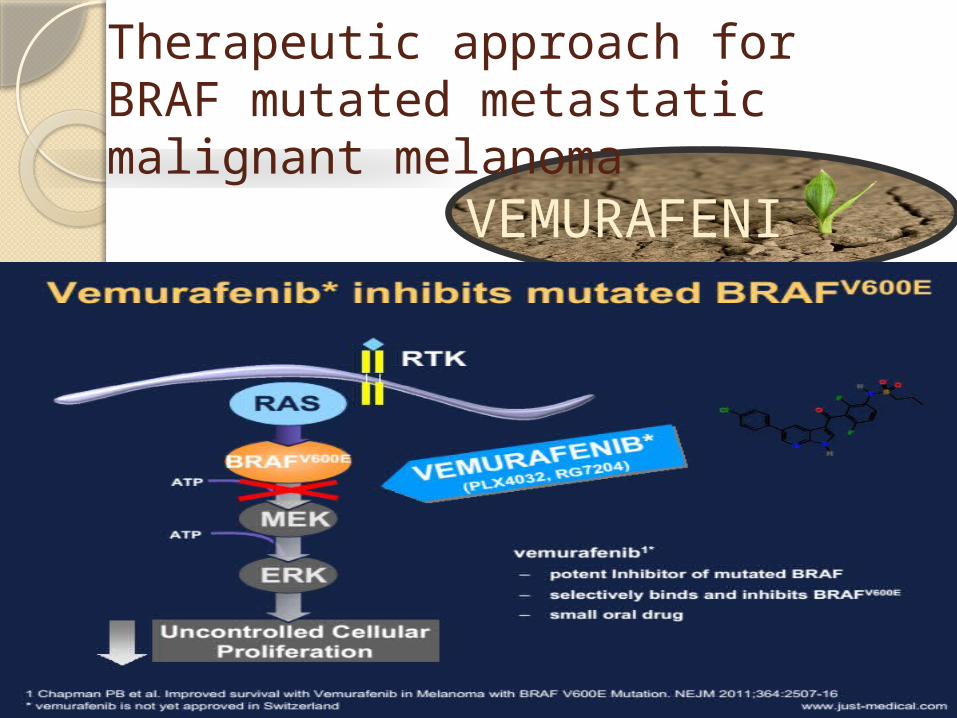
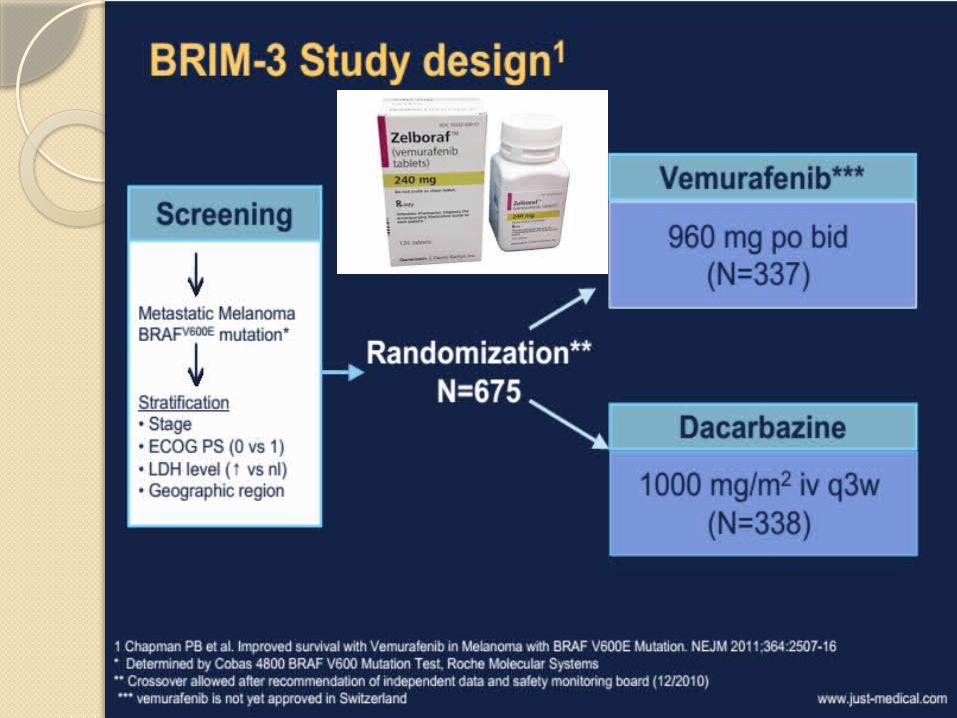
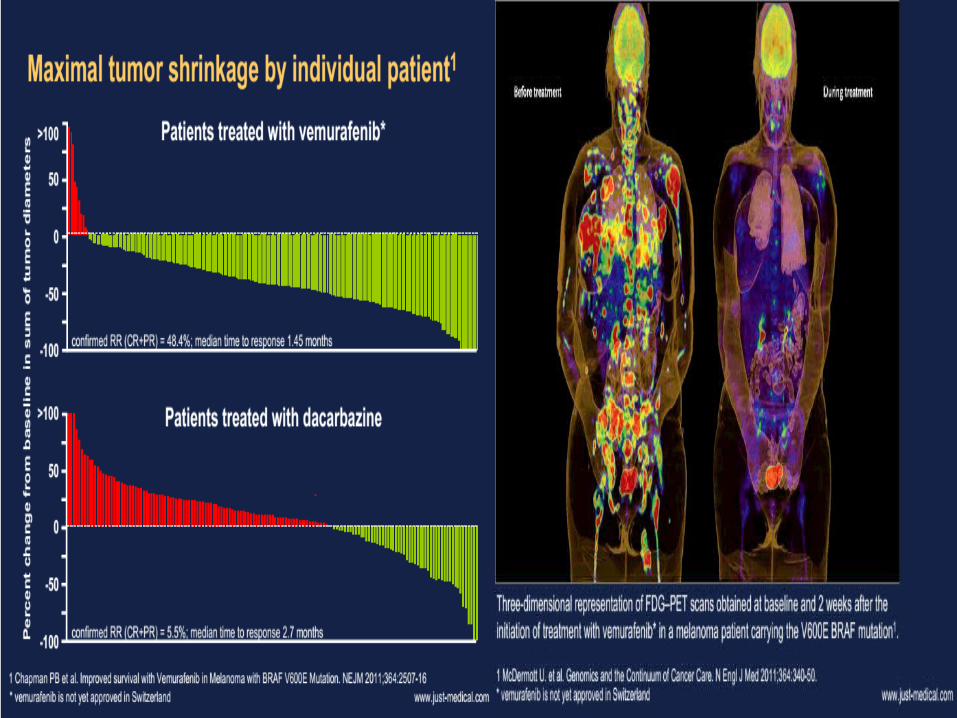
Therapeutic approach for BRAF mutated metastatic malignant melanoma
VEMURAFENIB

Dabrafenib : Second FDA approved BRAF inhibitor


Do we solve the problem? NO
Now there are two targets
BRAF mutation V600E
MEK – ERK Pathway
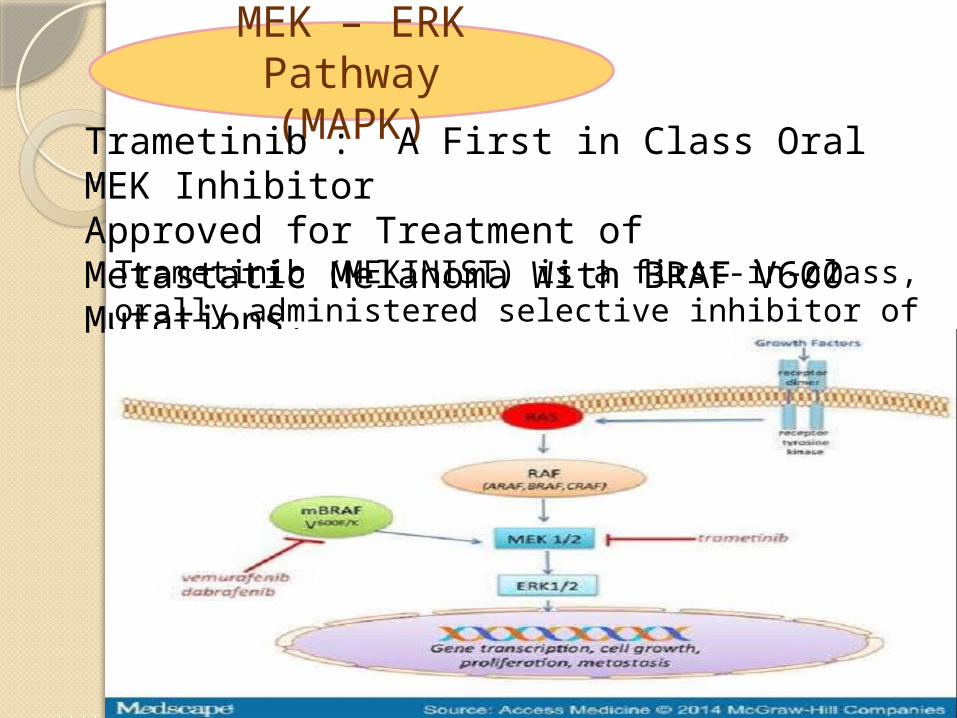
MEK – ERK Pathway (MAPK)
Trametinib : A First in Class Oral MEK InhibitorApproved for Treatment of Metastatic Melanoma With BRAF V600 Mutations.Trametinib (MEKINIST) is a first-in-class, orally
administered selective inhibitor of MEK1/2 serine threonine kinase.
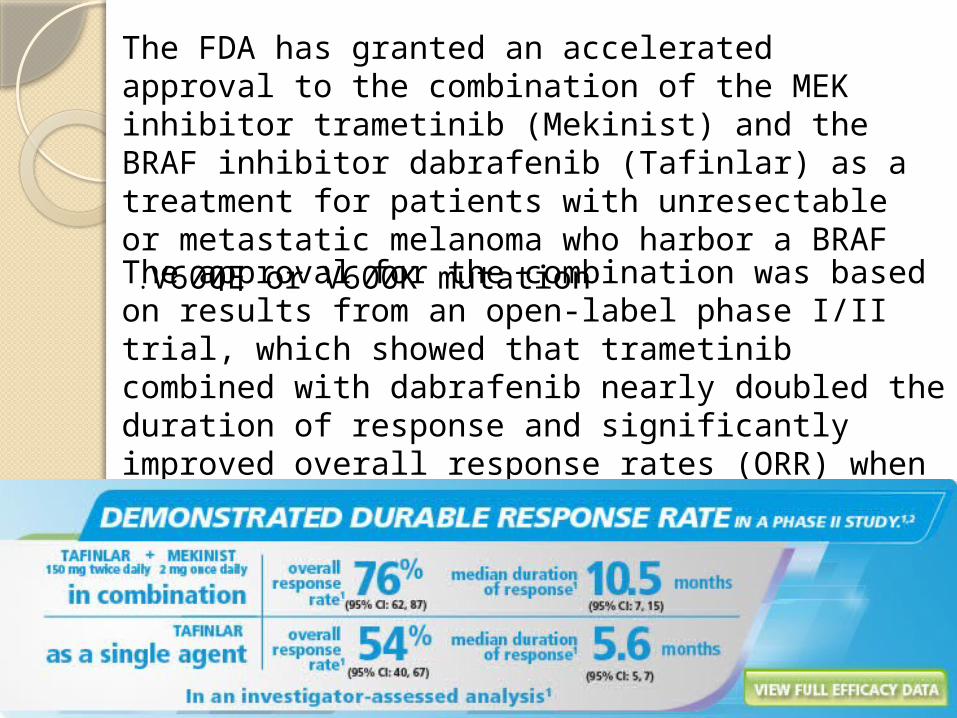
The FDA has granted an accelerated approval to the combination of the MEK inhibitor trametinib (Mekinist) and the BRAF inhibitor dabrafenib (Tafinlar) as a treatment for patients with unresectable or metastatic melanoma who harbor a BRAF V600E or V600K mutation .
The approval for the combination was based on results from an open-label phase I/II trial, which showed that trametinib combined with dabrafenib nearly doubled the duration of response and significantly improved overall response rates (ORR) when compared with dabrafenib alone .

Cobimetinib (another MEK inhibitor)

BRAF mutation
Melanoma is
immunogeneic
tumour
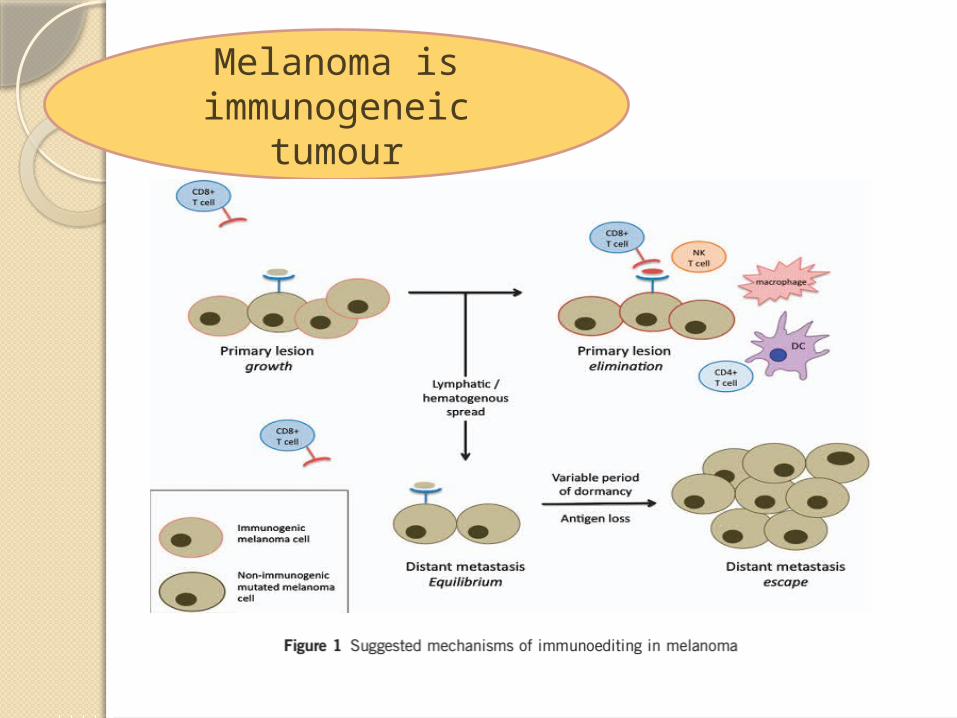
Melanoma is immunogeneic
tumour

Why Melanoma is an immunogeneic
tumour1-The reason underlying the immunogenicity of
melanoma isunclear. One hypothesis relates to the high mutation rate seen within melanomas compared with other tumor types.2- The majority of these mutations are passenger mutations that are non-essential for the survival of the tumor but offer an opportunity for immune recognition.3- where the mutation rate is higher,the chance of generating a mutation with the capacity to bind major histocompatibility complex could also be higher. Others have argued that the extensive research in melanoma immunology is largely opportunistic and stems from the failure of standard chemotherapeutic agents, leaving a therapeutic void for patients with metastatic disease.

As melanoma is immunogenic so it can be
eliminated naturally by host immune system Immune escape
Tumors utilize a number of pathways to avoid immune detection .
1-Antigen expression and presentation mechanisms may be suppressedthrough decreased major histocompatibility complex class I expression .
2-Tumors are also able to limit an immune response by releasingimmunosuppressive paracrine mediators including adenosine, transforming growth factor- b, vascular endothelial growth factor-A andindoleamine 2,3-dioxygenase (IDO) to suppress T-cell activation.
3- Tumors further create an immunosuppressive microenvironment by recruiting other cell populations, such as T regs and myeloid-derived suppressor cells to the tumor microenvironment.
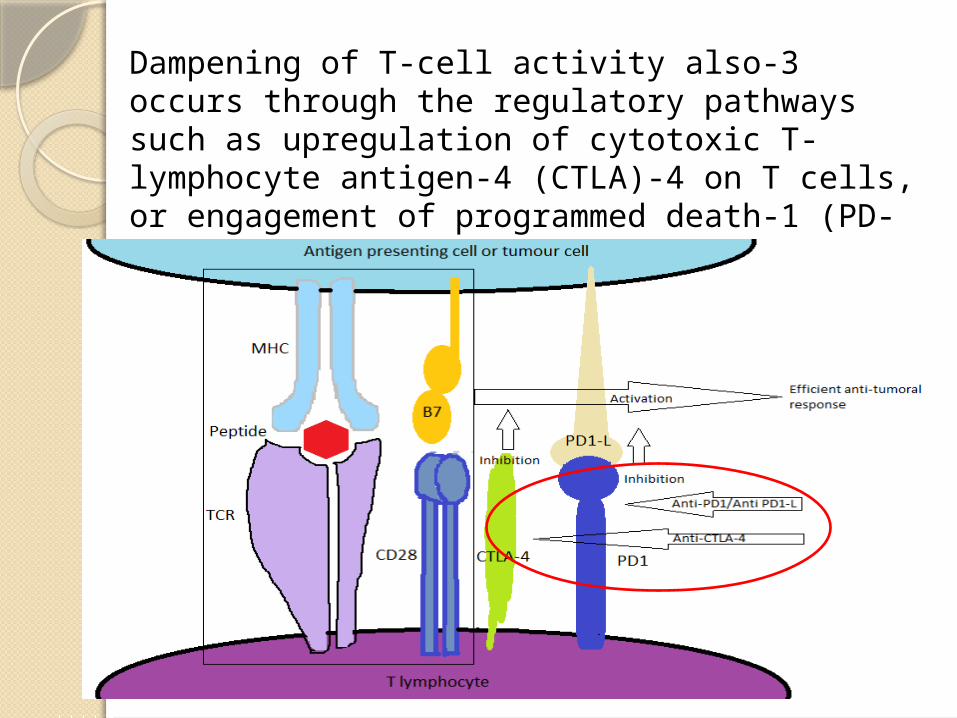
3-Dampening of T-cell activity also occurs through the regulatory pathways such as upregulation of cytotoxic T-lymphocyte antigen-4 (CTLA)-4 on T cells, or engagement of programmed death-1 (PD-1), an inhibitory T-cell co-receptor, with its ligand, B7-H1 (PD-L1) on tumor cells
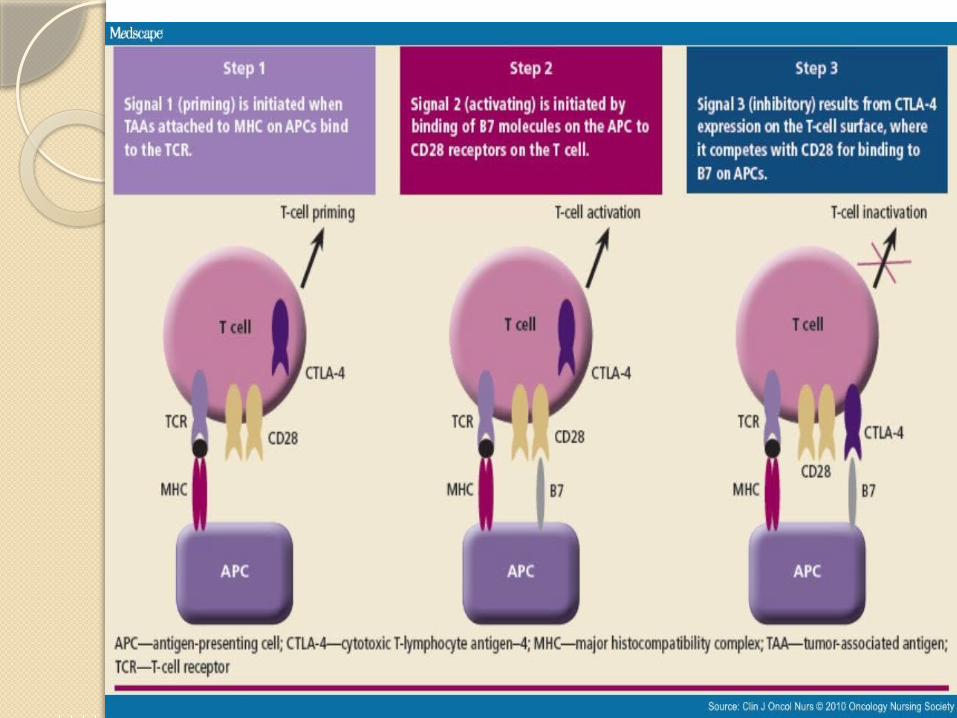

T- lymphocyte antigen 4 antibody(CTLA 4)

Ipilimumab ( CTLA4 antibody)

Anti programmed death1 antibodies (PD-1) antibodies
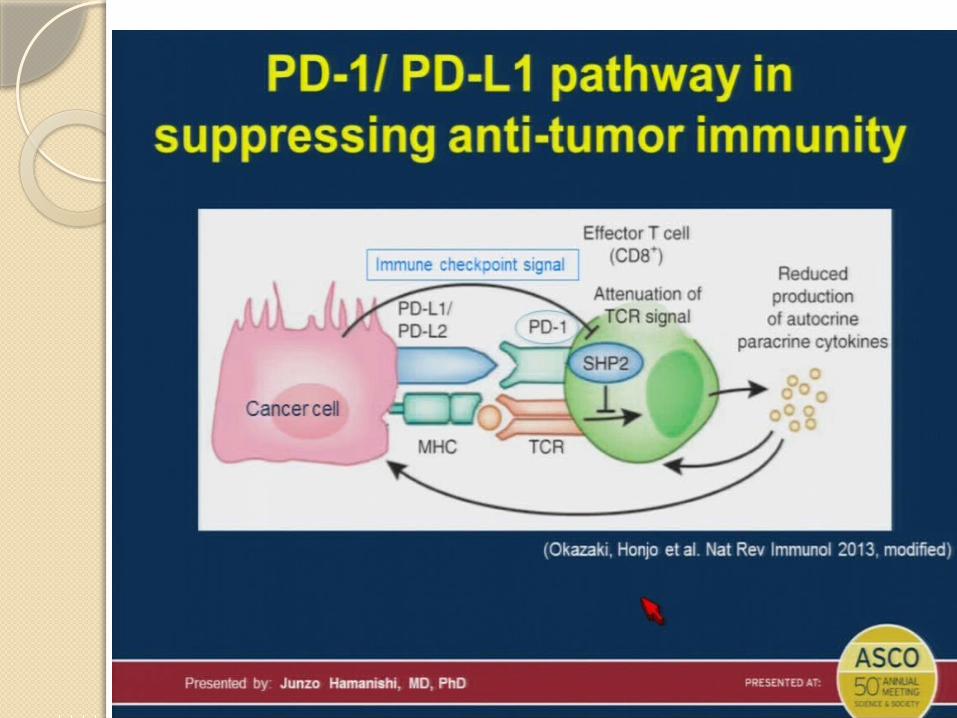

Mechanism of action of anti –PD1
NOWIS 2015 EMERGING
APROACHAsort of permution and
combinations

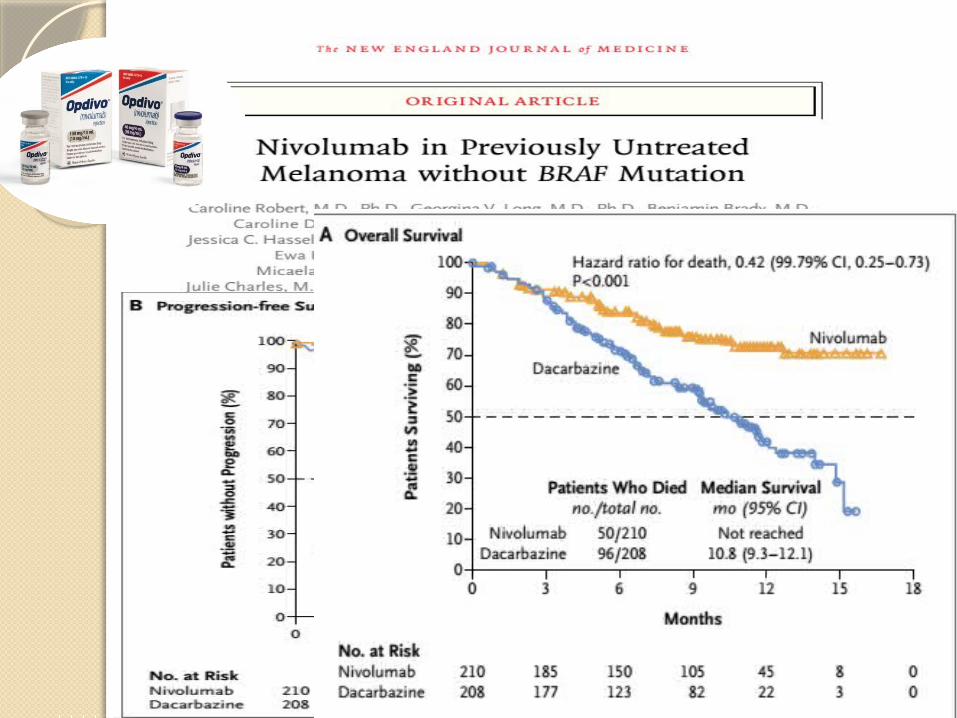
Participating investigators randomly assigned patients 2:1 to receive an intravenous infusion of nivolumab 3 mg/kg every 2 weeks or ICC(dacarbazine 1000 mg/m every 3 weeks or paclitaxel 175 mg/m combined with carboplatin area under the curve 6 every 3 weeks) until progression or unacceptable toxic effects


Thank you