memorial medical center - digisonics.com · and a patent ductus arteriosus is seen. the main and...
TRANSCRIPT
Memorial Medical Center100 Memorial Medical Drive
Houston, TX 77001Ph: (713) 555-1000
Pediatric Echocardiography Report
Patient Name: Trend Plot, PediStudy Date: 11/16/2018Height: 37 inWeight: 40 lbBSA: 0.66 m²Patient Category:Out PatientICD: R01.1
Gender: MPatient ID: 123876Priority: ROUTINEOrdering MD: Jennifer Barry, MDInterpreting MD: Jessica Brown, MDTechnologist: Karen Allen, RDCSDOB, Age: 4/5/2012, 6 yrTechnical CPT: 93306
Indications: Cardiac murmur, unspecifiedHistory/Clinical: Congenital heart diseaseProcedure: TTE - D+C, CompleteQuality: ExcellentPrevious Study: Date: 02/01/2018
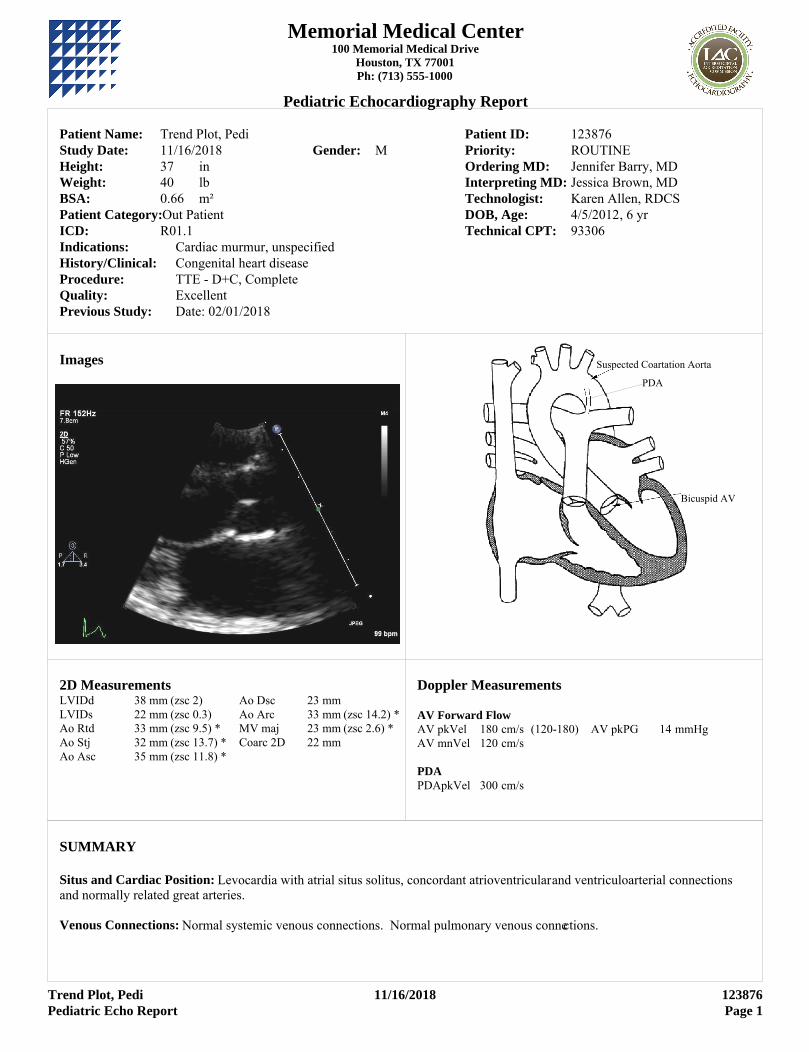
Images
Bicuspid AV
PDA
Suspected Coartation Aorta
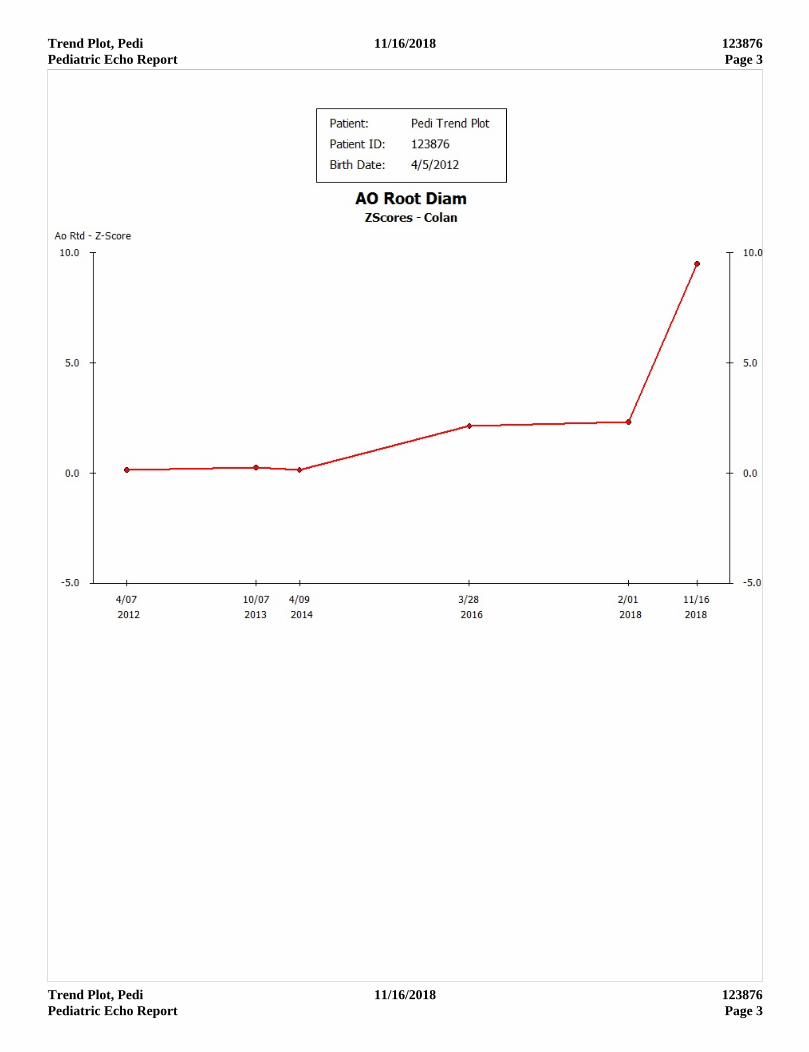
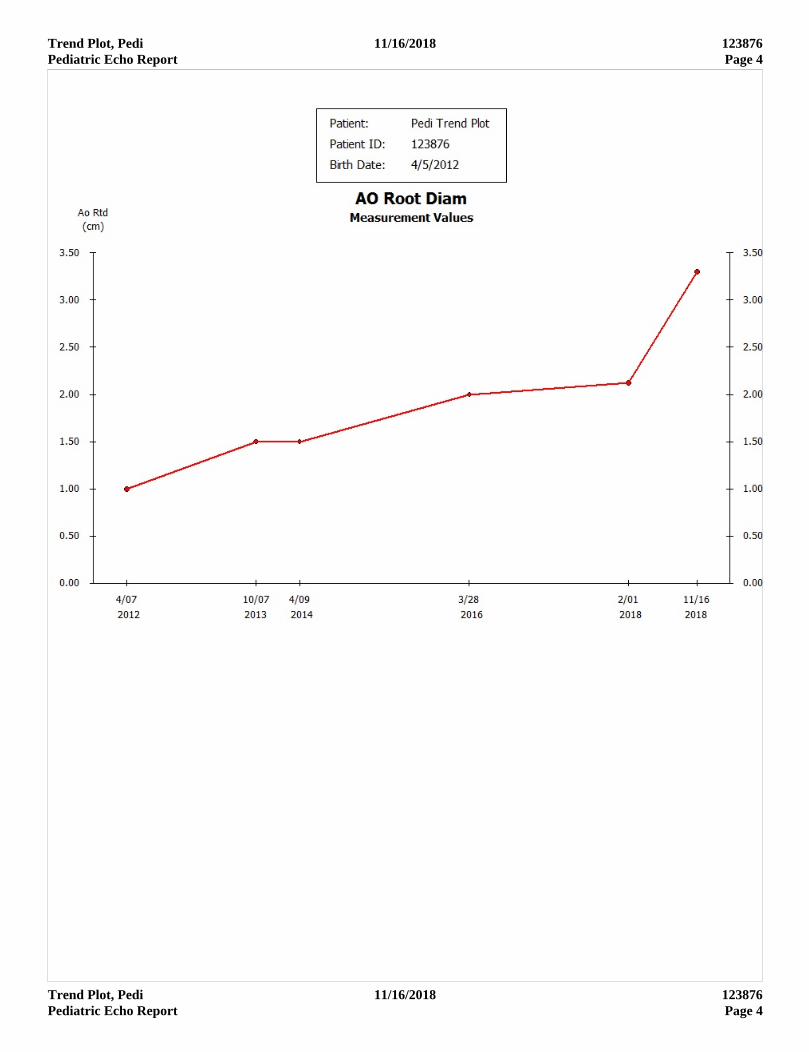
2D MeasurementsLVIDd 38 mm (zsc 2) Ao Dsc 23 mmLVIDs 22 mm (zsc 0.3) Ao Arc 33 mm (zsc 14.2) *Ao Rtd 33 mm (zsc 9.5) * MV maj 23 mm (zsc 2.6) *Ao Stj 32 mm (zsc 13.7) * Coarc 2D 22 mmAo Asc 35 mm (zsc 11.8) *
Doppler Measurements
AV Forward FlowAV pkVel 180 cm/s (120-180) AV pkPG 14 mmHg AV mnVel 120 cm/s
PDA PDApkVel 300 cm/s
SUMMARY
Situs and Cardiac Position: Levocardia with atrial situs solitus, concordant atrioventricular and ventriculoarterial connections and normally related great arteries.
Venous Connections: Normal systemic venous connections. Normal pulmonary venous connections.
Trend Plot, Pedi 11/16/2018 123876Pediatric Echo Report Page 1

Trend Plot, Pedi 11/16/2018 123876Pediatric Echo Report Page 2
Atria: The left atrium (LA) is normal in size. The right atrium (RA) is normal in size.
Atrial Septum: Intact atrial septum with no evidence of interatrial shunting.
Atrioventricular Junction: Structurally and functionally normal mitral valve with normal spectral and color flow Doppler. Structurally and functionally normal tricuspid valve with no regurgitation.
Ventricles: The left ventricle (LV) is normal in size with normal wall thickness and normal systolic function. The right ventricle (RV) is normal in size with normal wall thickness and normal systolic function.
Ventricular Septum: Intact ventricular septum. No evidence of ventricular level shunting.
Outflow tracts: The left ventricular outflow tract is normal in size with unobstructed flow. The right ventricular outflow tract is normal in size with unobstructed flow.
Semilunar Valves: The aortic valve is bicuspid and the leaflets are moderately thickened. Normal antegrade flow with moderate regurgitation. The pulmonary valve (PV) is structurally and functionally normal. Normal antegrade flow; physiologic regurgitation.
Aortic & Pulmonary Root: The aortic root, sinuses of Valsalva, sinotubular junction and proximal ascending aorta are all dilated. The pulmonary root is normal, without dilation or stenosis.
Thoracic Arteries: The ascending aorta is moderately dilated. Left aortic arch with normal brachiocephalic artery branching. There is normal antegrade flow in the aortic arch. There is evidence of coarctation of the aorta with elevated color flow velocities and a patent ductus arteriosus is seen. The main and branch pulmonary arteries are of normal size with normal flow velocities.
Coronary Arteries: The origin and proximal course of the right and left coronary arteries are normal.
Pericardium/Pleural: No pericardial effusion. No pleural effusion seen.
Follow up study recommended in 6 months.
_____________________________________Jessica Brown, MD
Trend Plot, Pedi 11/16/2018 123876Pediatric Echo Report Page 2
Trend Plot, Pedi 11/16/2018 123876Pediatric Echo Report Page 3
Trend Plot, Pedi 11/16/2018 123876Pediatric Echo Report Page 3
Trend Plot, Pedi 11/16/2018 123876Pediatric Echo Report Page 4
Trend Plot, Pedi 11/16/2018 123876Pediatric Echo Report Page 4
MMC Childrens
Pediatric Catheterization
Patient Name: Diaz, JohnnyStudy Date: 5/18/2018Height: 73.7 cmWeight: 16.4 kgBSA: 0.53 m²
Gender: MBP: 138/67HR: 85
Patient ID: 56222Priority: ROUTINEReferring MD: Benjamin Shah, MDInterpreting MD: Hector Garcia, MDDOB, Age: 11/8/2015, 2 yrCPT: 93453, 93567
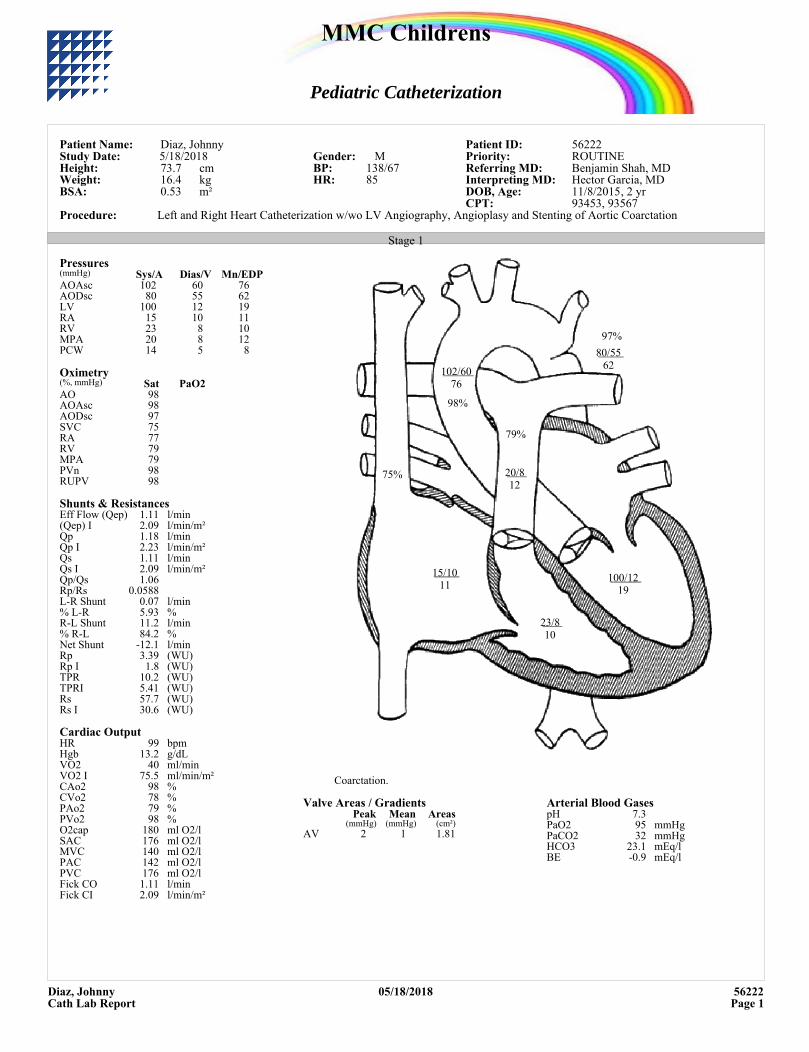
Procedure: Left and Right Heart Catheterization w/wo LV Angiography, Angioplasy and Stenting of Aortic Coarctation
Stage 1
102/6076
80/5562
100/1219
15/1011
23/810
75%
79%
98%
97%
20/812
Coarctation.
Pressures(mmHg) Sys/A Dias/V Mn/EDPAOAsc 102 60 76AODsc 80 55 62LV 100 12 19RA 15 10 11RV 23 8 10MPA 20 8 12PCW 14 5 8
Oximetry(%, mmHg) Sat PaO2AO 98AOAsc 98AODsc 97SVC 75RA 77RV 79MPA 79PVn 98RUPV 98
Shunts & ResistancesEff Flow (Qep) l/min1.11(Qep) I l/min/m²2.09Qp l/min1.18Qp I l/min/m²2.23Qs l/min1.11Qs I l/min/m²2.09Qp/Qs 1.06Rp/Rs 0.0588L-R Shunt l/min0.07% L-R %5.93R-L Shunt l/min11.2% R-L %84.2Net Shunt l/min-12.1Rp (WU)3.39Rp I (WU)1.8TPR (WU)10.2TPRI (WU)5.41Rs (WU)57.7Rs I (WU)30.6
Cardiac OutputHR bpm99Hgb g/dL13.2VO2 ml/min40VO2 I ml/min/m²75.5CAo2 %98CVo2 %78PAo2 %79PVo2 %98O2cap ml O2/l180SAC ml O2/l176MVC ml O2/l140PAC ml O2/l142PVC ml O2/l176Fick CO l/min1.11Fick CI l/min/m²2.09
Valve Areas / GradientsPeak Mean Areas
(mmHg) (mmHg) (cm²)AV 2 1 1.81
Arterial Blood GasespH 7.3PaO2 mmHg95PaCO2 mmHg32HCO3 mEq/l23.1BE mEq/l-0.9
Diaz, Johnny 05/18/2018 56222Cath Lab Report Page 1
Diaz, Johnny 05/18/2018 56222Cath Lab Report Page 2
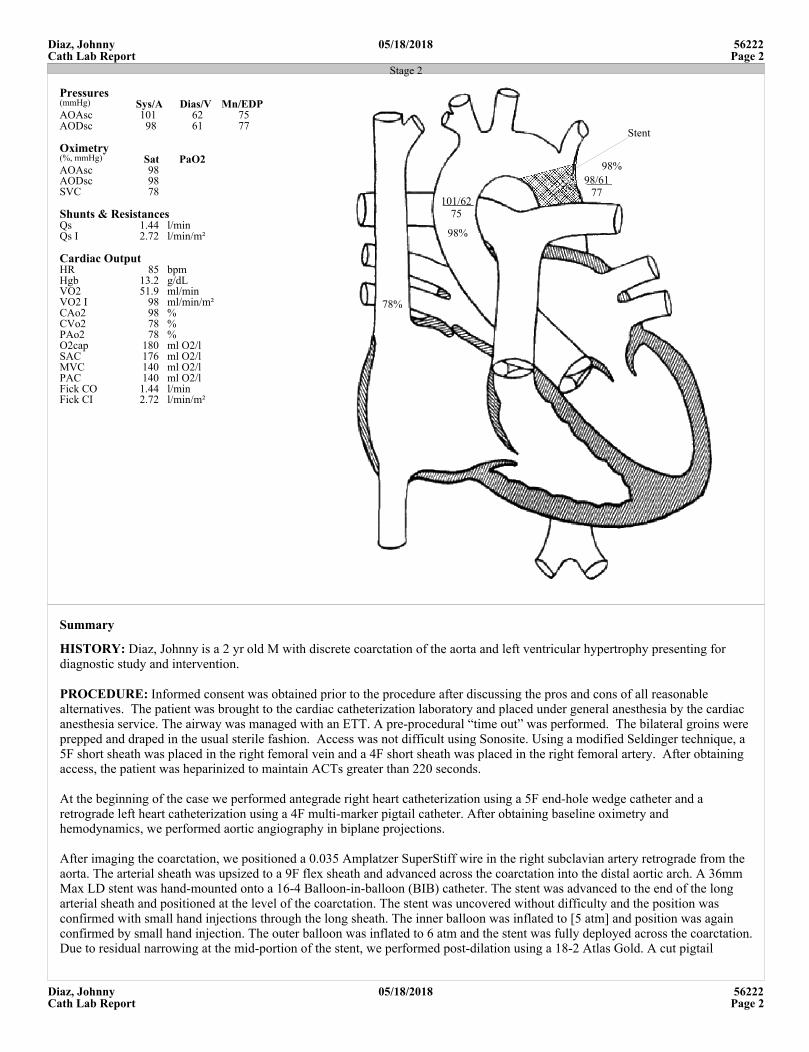
Stage 2
101/6275
98/6177
78%
98%
98%
Stent
Pressures(mmHg) Sys/A Dias/V Mn/EDPAOAsc 101 62 75AODsc 98 61 77
Oximetry(%, mmHg) Sat PaO2AOAsc 98AODsc 98SVC 78
Shunts & ResistancesQs l/min1.44Qs I l/min/m²2.72
Cardiac OutputHR bpm85Hgb g/dL13.2VO2 ml/min51.9VO2 I ml/min/m²98CAo2 %98CVo2 %78PAo2 %78O2cap ml O2/l180SAC ml O2/l176MVC ml O2/l140PAC ml O2/l140Fick CO l/min1.44Fick CI l/min/m²2.72
Summary
HISTORY: Diaz, Johnny is a 2 yr old M with discrete coarctation of the aorta and left ventricular hypertrophy presenting for diagnostic study and intervention.
PROCEDURE: Informed consent was obtained prior to the procedure after discussing the pros and cons of all reasonable alternatives. The patient was brought to the cardiac catheterization laboratory and placed under general anesthesia by the cardiac anesthesia service. The airway was managed with an ETT. A pre-procedural “time out” was performed. The bilateral groins were prepped and draped in the usual sterile fashion. Access was not difficult using Sonosite. Using a modified Seldinger technique, a 5F short sheath was placed in the right femoral vein and a 4F short sheath was placed in the right femoral artery. After obtaining access, the patient was heparinized to maintain ACTs greater than 220 seconds.
At the beginning of the case we performed antegrade right heart catheterization using a 5F end-hole wedge catheter and a retrograde left heart catheterization using a 4F multi-marker pigtail catheter. After obtaining baseline oximetry and hemodynamics, we performed aortic angiography in biplane projections.
After imaging the coarctation, we positioned a 0.035 Amplatzer SuperStiff wire in the right subclavian artery retrograde from the aorta. The arterial sheath was upsized to a 9F flex sheath and advanced across the coarctation into the distal aortic arch. A 36mm Max LD stent was hand-mounted onto a 16-4 Balloon-in-balloon (BIB) catheter. The stent was advanced to the end of the long arterial sheath and positioned at the level of the coarctation. The stent was uncovered without difficulty and the position was confirmed with small hand injections through the long sheath. The inner balloon was inflated to [5 atm] and position was again confirmed by small hand injection. The outer balloon was inflated to 6 atm and the stent was fully deployed across the coarctation. Due to residual narrowing at the mid-portion of the stent, we performed post-dilation using a 18-2 Atlas Gold. A cut pigtail
Diaz, Johnny 05/18/2018 56222Cath Lab Report Page 2

Diaz, Johnny 05/18/2018 56222Cath Lab Report Page 3
catheter was then advanced across the coarctation and pressures were measured above and below the stent simultaneously. The wire was removed and a final angiogram was performed through the cut pigtail.
At the end of the case, ropivacaine was infused for additional analgesia. Sheaths were pulled and hemostasis was obtained by manual pressure. There was no hematoma and no pulse loss. The patient was extubated in the cath lab and transferred to the cath recovery unit in stable condition.
Complications: none.Total fluoroscopy time: 10 minTotal contrast used: 20 mLEstimated Blood Loss: 20 mL
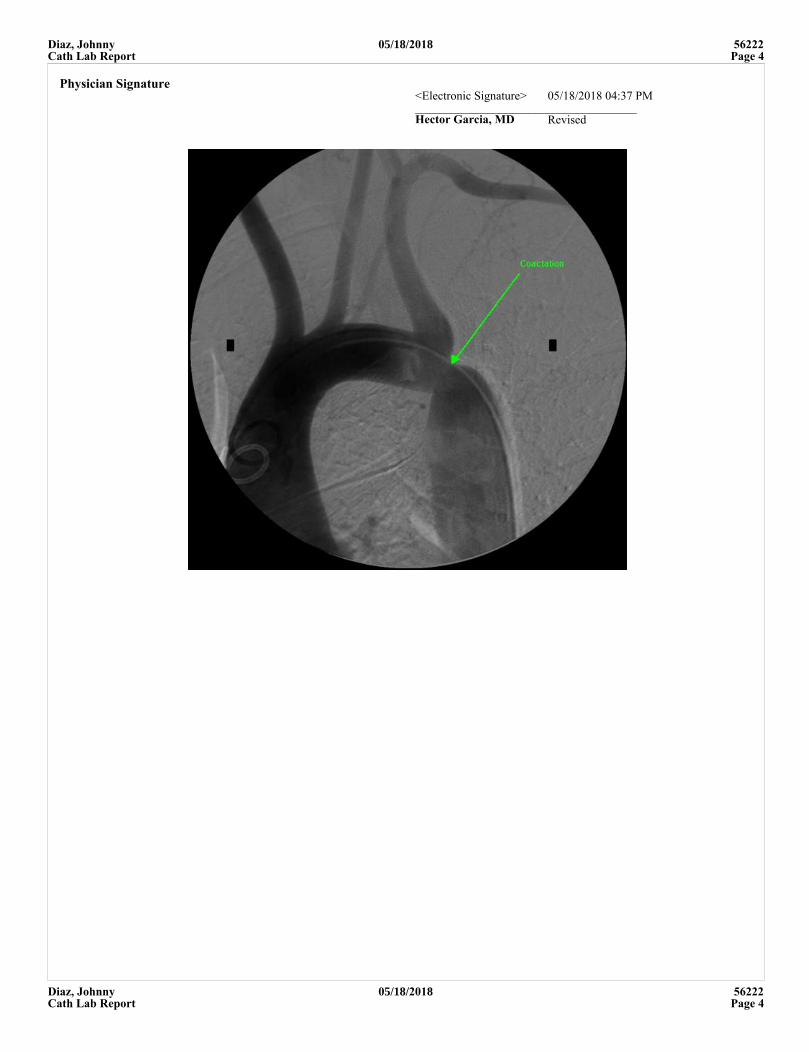
Angiographya. A 3D rotational angiography was performed with a power injection in the ascending aorta with RV pacing. Angiography showed a mildly dilated ascending aorta with a normal transverse aorta. There is a Left aortic arch with normal branching pattern of the head and neck vessels. There is severe discrete coarctation of the distal arch with normal caliber descending aorta. There are multiple collaterals seen on this injection
b. In straight AP and lateral projections, a multi-marker pigtail catheter has been advanced retrograde across the coarctation into the distal aortic arch. Power injection into the distal aortic arch demonstrate mildly dilated ascending aorta with a normal transverse aorta. There is a Left aortic arch with normal branching pattern of the head and neck vessels. There is severe discrete coarctation of the distal arch with normal caliber descending aorta. There are multiple collaterals seen on this injection.
IMPRESSION: Diaz, Johnny is a 2 yr old M with discrete coarctation of the aorta and left ventricular hypertrophy presenting for diagnostic study and intervention.
1) Normal baseline cardiac index.2) Severe juxtaductal coarctation with peak-to-peak gradient of 30 mmHg gradient.3) Coarctation stented primarily with 36 mm Max LD and post-dilated using 18 mm Atlas Gold with significant angiographic improvement and reduction in peak-to-peak gradient to < 10mmHg.4) No complications.
Hector Garcia, MD was present throughout the entire case.
cc: primary cardiologist and primary care
Cath Procedure
Description: Complications: none.Total fluoroscopy time: 10 minTotal contrast used: 20 mLEstimated Blood Loss: 20 mL
Medications Administered:Heparin, 500 units, IV, Bolus. AnticoagulationPercutaneous entry: Right Femoral arteryComplications: NONE
Post Procedure
PulsesBilateral DP: BoundingBilateral PT: Bounding
Staff:Cardiac Cath Physician Hector Garcia, MD Circulating Nurse Dave Minor, RNInterventionalist Hector Garcia, MD Radiologic Tech Julia Chris, RTScrub Staff Bill Taylor, RCIS Monitoring Staff Gregg Abbott, RCIS
Diaz, Johnny 05/18/2018 56222Cath Lab Report Page 3
Diaz, Johnny 05/18/2018 56222Cath Lab Report Page 4
Physician Signature<Electronic Signature> 05/18/2018 04:37 PM_____________________________________Hector Garcia, MD Revised
Diaz, Johnny 05/18/2018 56222Cath Lab Report Page 4
Memorial Medical Center100 Memorial Medical Drive, Houston, TX 77001
Cardiac MR Report
Patient Name: Soros, MarlowStudy Date: 11/13/2017Height: 136 cmWeight: 28.9 kgBSA: 1.06 m²
Gender: MPatient ID: D154113Interpreting MD: Joseph Franklin, MDDOB, Age: 7/31/2010, 7 yr
Indications: BAV, aortic coarctation and LSVC to coronary sinus S/P balloon aortoplasty January 2011History/Clinical: Coartation balloon arterioplastyLab Tests: Creatine, <0.3, 11/7/17
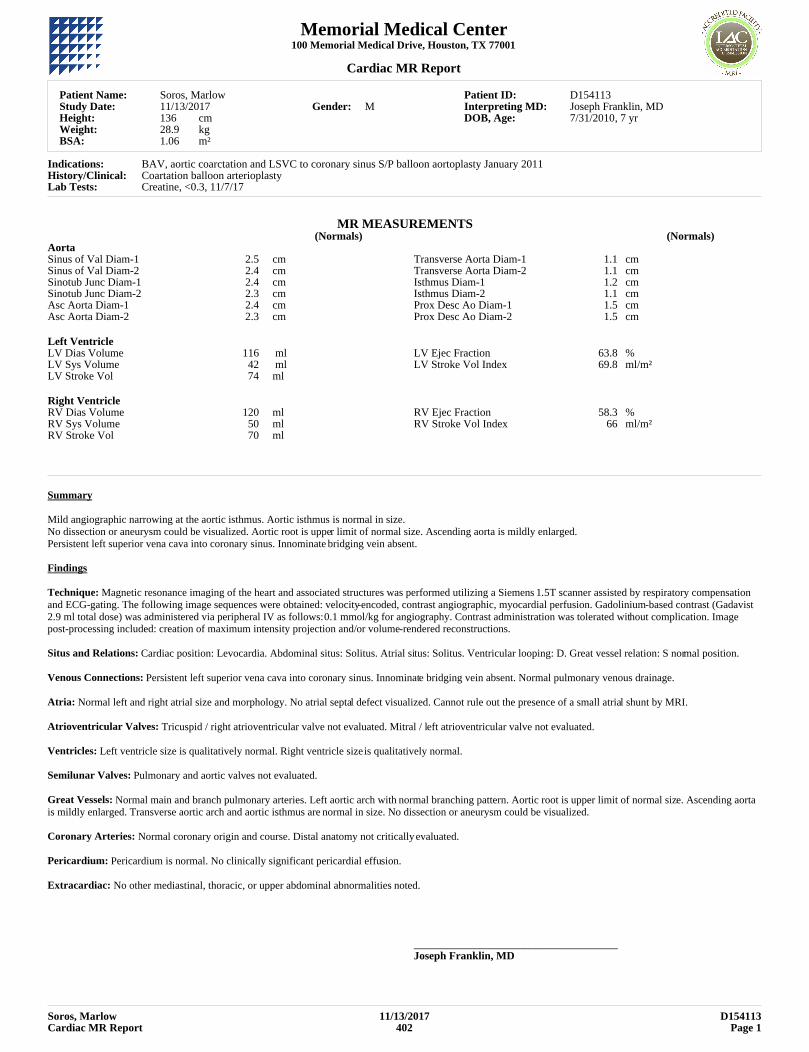
MR MEASUREMENTS(Normals) (Normals)
Aorta Sinus of Val Diam-1 2.5 cm Transverse Aorta Diam-1 1.1 cmSinus of Val Diam-2 2.4 cm Transverse Aorta Diam-2 1.1 cmSinotub Junc Diam-1 2.4 cm Isthmus Diam-1 1.2 cmSinotub Junc Diam-2 2.3 cm Isthmus Diam-2 1.1 cmAsc Aorta Diam-1 2.4 cm Prox Desc Ao Diam-1 1.5 cmAsc Aorta Diam-2 2.3 cm Prox Desc Ao Diam-2 1.5 cm
Left Ventricle LV Dias Volume 116 ml LV Ejec Fraction 63.8 %LV Sys Volume 42 ml LV Stroke Vol Index 69.8 ml/m²LV Stroke Vol 74 ml
Right Ventricle RV Dias Volume 120 ml RV Ejec Fraction 58.3 %RV Sys Volume 50 ml RV Stroke Vol Index 66 ml/m²RV Stroke Vol 70 ml
Summary
Mild angiographic narrowing at the aortic isthmus. Aortic isthmus is normal in size. No dissection or aneurysm could be visualized. Aortic root is upper limit of normal size. Ascending aorta is mildly enlarged. Persistent left superior vena cava into coronary sinus. Innominate bridging vein absent.
Findings
Technique: Magnetic resonance imaging of the heart and associated structures was performed utilizing a Siemens 1.5T scanner assisted by respiratory compensation and ECG-gating. The following image sequences were obtained: velocity-encoded, contrast angiographic, myocardial perfusion. Gadolinium-based contrast (Gadavist 2.9 ml total dose) was administered via peripheral IV as follows: 0.1 mmol/kg for angiography. Contrast administration was tolerated without complication. Image post-processing included: creation of maximum intensity projection and/or volume-rendered reconstructions.
Situs and Relations: Cardiac position: Levocardia. Abdominal situs: Solitus. Atrial situs: Solitus. Ventricular looping: D. Great vessel relation: S normal position.
Venous Connections: Persistent left superior vena cava into coronary sinus. Innominate bridging vein absent. Normal pulmonary venous drainage.
Atria: Normal left and right atrial size and morphology. No atrial septal defect visualized. Cannot rule out the presence of a small atrial shunt by MRI.
Atrioventricular Valves: Tricuspid / right atrioventricular valve not evaluated. Mitral / left atrioventricular valve not evaluated.
Ventricles: Left ventricle size is qualitatively normal. Right ventricle size is qualitatively normal.
Semilunar Valves: Pulmonary and aortic valves not evaluated.
Great Vessels: Normal main and branch pulmonary arteries. Left aortic arch with normal branching pattern. Aortic root is upper limit of normal size. Ascending aorta is mildly enlarged. Transverse aortic arch and aortic isthmus are normal in size. No dissection or aneurysm could be visualized.
Coronary Arteries: Normal coronary origin and course. Distal anatomy not critically evaluated.
Pericardium: Pericardium is normal. No clinically significant pericardial effusion.
Extracardiac: No other mediastinal, thoracic, or upper abdominal abnormalities noted.
_____________________________________Joseph Franklin, MD
Soros, Marlow 11/13/2017 D154113Cardiac MR Report 402 Page 1
Memorial Medical Center100 Memorial Medical Drive
Houston, TX 77001Ph: (713) 555-1000
Fetal Echocardiography Report
Patient Name: Zabrek, JennyStudy Date: 8/26/2014Height: 64 inWeight: 166 lbBSA: 1.81 m²Patient Category: Out Patient
BP: 120/56
Patient ID: 26550Priority: ROUTINEReferring MD: Amy Jones, MDOrdering MD: Kimberly Connors, MDInterpreting MD: Frank Smith, MDTechnologist: Fred Thomas, RDCSDOB, Age: 8/26/1977, 37 yrCPT: 93303
GA & EDD: 36w2d, 9/27/2014History/Clinical: AsthmaProcedure: 2D, M-mode, DopplerQuality: AdequatePrevious Study: Date: 07/26/2014
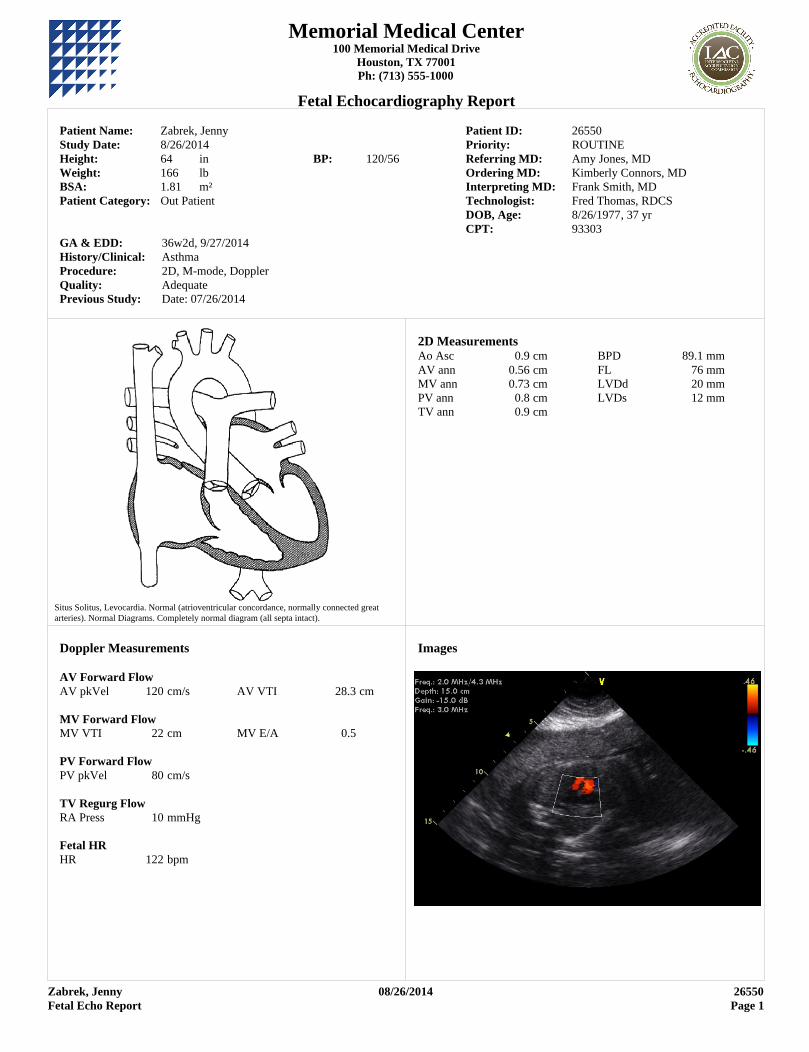
Situs Solitus, Levocardia. Normal (atrioventricular concordance, normally connected great arteries). Normal Diagrams. Completely normal diagram (all septa intact).
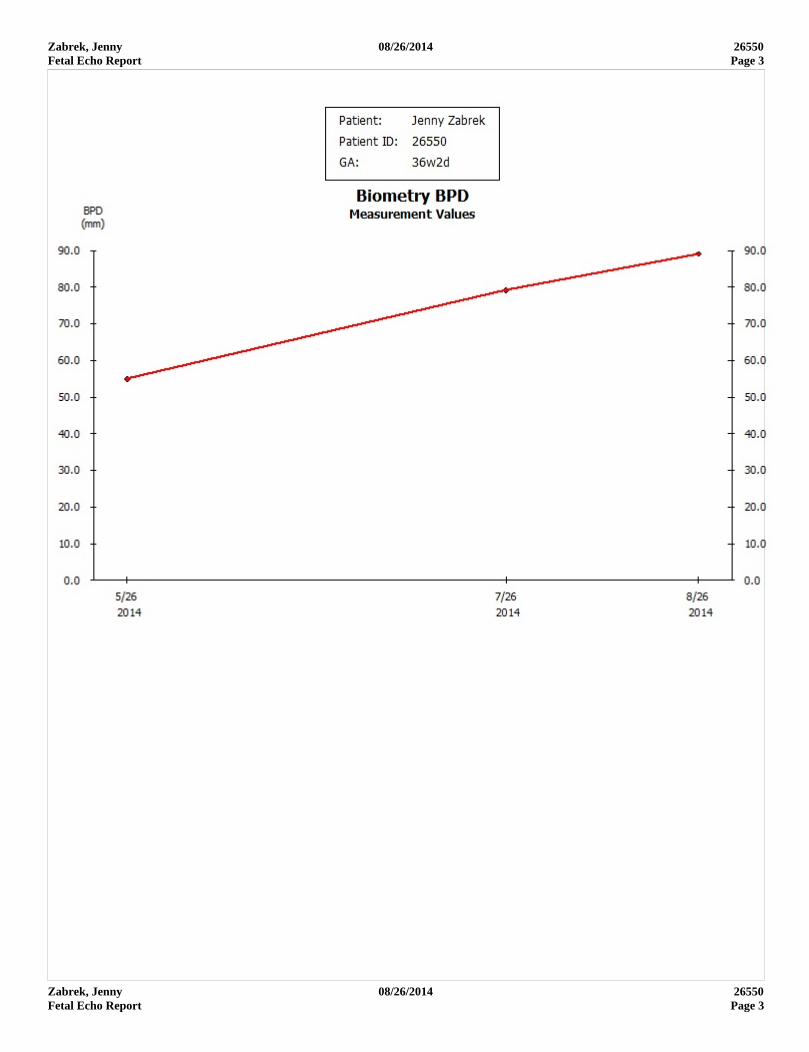
2D MeasurementsAo Asc 0.9 cm BPD 89.1 mmAV ann 0.56 cm FL 76 mmMV ann 0.73 cm LVDd 20 mmPV ann 0.8 cm LVDs 12 mmTV ann 0.9 cm
Doppler Measurements
AV Forward FlowAV pkVel 120 cm/s AV VTI 28.3 cm
MV Forward FlowMV VTI 22 cm MV E/A 0.5
PV Forward FlowPV pkVel 80 cm/s
TV Regurg FlowRA Press 10 mmHg
Fetal HR HR 122 bpm
Images
Zabrek, Jenny 08/26/2014 26550Fetal Echo Report Page 1
Zabrek, Jenny 08/26/2014 26550Fetal Echo Report Page 2
Situs and Cardiac Position: Levocardia with atrial situs solitus, concordant atrioventricular and ventriculoarterial connections and normally related great arteries.
Venous Connections: The right-sided superior vena cava drains normally to the right atrium. Normal IVC and hepatic venous flow is seen by Doppler. The IVC and hepatic veins drain normally to the right atrium. Normal laminar flow is seen in the superior vena cava by Doppler interrogation. At least two pulmonary veins are demonstrated draining to the left atrium with laminar flow by color Doppler.
Atria: The left atrium (LA) is normal in size. The right atrium (RA) is normal in size.
Atrial Septum: Small patent foramen ovale (PFO) with unobstructed predominantly right to left flow. The foramenal flap is seen in the left atrium.
Atrioventricular Junction: Structurally and functionally normal mitral valve. The mitral valve annulus measures 5mm. Spectral Doppler and color flow mapping of the mitral valve is normal. Structurally and functionally normal tricuspid valve with normal spectral and color flow Doppler. The tricuspid valve annulus measures 0.90 cm in the apical four chamber view.
Ventricles: The morphologic left ventricle is located posteriorly adjacent to the spine. The left ventricular (LV) chamber size is normal. There is normal global left ventricular systolic function. The morphologic right ventricle is located anteriorly. The right ventricle (RV) is normal in size with normal wall thickness and normal systolic function.
Ventricular Septum: Intact ventricular septum. No evidence of ventricular level shunting. Interventricular septal motion is normal. There is normal interventricular septal thickness.
Outflow tracts: The left ventricular outflow tract is normal in size with unobstructed flow. The right ventricular outflow tract is normal in size with obstructed flow.
Semilunar Valves: The aortic valve is structurally and functionally normal. The aortic valve annulus measures 5.6 mm. There is laminar antegrade flow with no regurgitation. The PV annulus is normal in size and measures 8mm. Normal antegrade flow across pulmonary valve.
Aortic & Pulmonary Root: The aortic root, sinuses of Valsalva, sinotubular junction and proximal ascending aorta are normal. The pulmonary root is normal, without dilation or stenosis.
Thoracic Arteries: The aortic arch is normal in appearance with normal brachiocephalic arteries and normal antegrade flow. The descending aorta is of normal size with laminar flow. The ductal arch is normal. The flow is normal with right to left shunting The main and branch pulmonary arteries are of normal size with normal flow velocities.
Pericardium/Pleural: No pericardial effusion. No pleural effusion seen.
Maternal-Fetal Connections: Three vessel cord seen.
Fetal: Estimated date of delivery is 09/27/2014 First day of last menstrual cycle is 12/20/2013. Single intrauterine pregnancy. Vertex presentation. Normal active fetus. The gestational age by dates is 36 weeks. Biparietal diameter (leading edge to leading edge) is 8.9 cm. The cardiac area is 22 cm2. The heart area to chest area ratio is 1.1. Range of fetal heart rate is 122-125 bpm. No fetal arrhythmias noted. This study cannot exclude the presence of coarctation of the aorta, secundum ASD, small VSD's, partial anomalous pulmonary venous return, subtle valvular dysplasias, coronary artery anomalies, peripheral pulmonary stenosis, persistent ductus arteriosus beyond the neonatal period, development of arch gradient after ductal closure or predict the onset of late trimester cardiomyopathy.
_____________________________________Frank Smith, MD
Zabrek, Jenny 08/26/2014 26550Fetal Echo Report Page 2
Zabrek, Jenny 08/26/2014 26550Fetal Echo Report Page 3
Zabrek, Jenny 08/26/2014 26550Fetal Echo Report Page 3