metal endoprostheses for limb salvage surgery in …
TRANSCRIPT

METAL ENDOPROSTHESES FOR LIMB SALVAGE SURGERY IN DOGS WITH
DISTAL RADIAL OSTEOSARCOMA: EVALUATION OF FIRST AND SECOND
GENERATION METAL ENDOPROSTHESES AND INVESTIGATION OF A NOVEL
ENDOPROSTHESIS
Katherine Elizabeth Mitchell
orcid.org/0000-0003-1370-2856
613348
Submitted in partial fulfilment of the requirements of the degree of
Master of Veterinary Science (Clinical)
June 2017
Faculty of Veterinary Science
The University of Melbourne

i
This is to certify that:
The thesis comprises only my original work towards the masters except where indicated in
the Preface,
Due acknowledgement has been made in the text to all other material used,
The thesis is less than 30,000 words in length, exclusive of tables, maps, bibliographies and
appendices.
____________________________
Katherine Elizabeth Mitchell
Preface: work carried out in collaboration – nature and proportion of contribution
Chapter 3 includes work from published manuscript provided in Appendix 1. Katherine Mitchell
was the primary author and contributed over 90% of authorship. The nature of collaboration
was data collection from the following contributors: Sarah Boston, Nicole Ehrhart, Marvin Kung,
Sarah Dry, Rod Straw, Julius Liptak, Martin Havlicek, Radboud Kemme, James Simcock and
James Farese. Stewart Ryan, a supervisor on this thesis, contributed review and editing of the
manuscript.
Chapter 4 includes continuation of research into a novel endoprosthesis that was designed by
Snehal Shetye, Christian Puttlitz, Stewart Ryan & Nicole Ehrhart. All endoprosthesis designers
collaborated in design of experiments performed in this thesis, however all work and authorship
is by Katherine Mitchell.
Peter Lee, Mike Xie & Nirmal Menon collaborated in the manufacture of endoprosthesis via rapid
prototyping.

ii
Abstract
Osteosarcoma (OSA) is the most commonly diagnosed primary bone tumour in dogs, usually affecting
middle-aged, large breed dogs. The standard of care surgical treatment for local tumour control in
dogs with osteosarcoma is limb amputation; however limb-sparing surgery is gaining wider
acceptance as an alternative surgical treatment. All limb sparing techniques show high complication
rates, including infection, construct failure or fracture and local recurrence. Metal endoprosthesis (EN)
limb-sparing surgery was developed to overcome limitations of other techniques, including access to
specialised equipment and facilities such as radiation therapy or bone bank facilities. The first
generation of metal EN (GEN1) was shown to be biomechanically superior, but not clinically different
to the cortical allograft. A second generation metal EN (GEN2) was developed but biomechanical
studies and clinical outcomes have not been reported other than in single case reports.
The first component of this thesis is a multi-institutional retrospective case series that evaluated
surgical and oncologic outcomes for dogs treated with GEN1 or GEN2 for OSA of the distal radius.
Records from 45 dogs with distal radial OSA were examined; 28 dogs received GEN1 and 17 dogs
received GEN2. One or multiple complications occurred in 43 dogs (96%, 14 minor, 29 major) including
35 with infection (78%), 16 with implant-related complication (36%) and 11 with local recurrence
(24%). This study showed no significant difference in case (surgical or oncologic) outcomes between
dogs receiving GEN1 and GEN2 endoprosthesis for limb-sparing surgery of the distal radius. The
frequency of complications, including infection and those implant-related, remains unacceptably high
for both generations of endoprosthesis. Further refinement of the endoprosthesis or re-evaluation of
the surgical technique for implantation of the endoprosthesis is indicated.
A finite element (FE) model of the canine forelimb has been designed by a multi-disciplinary team
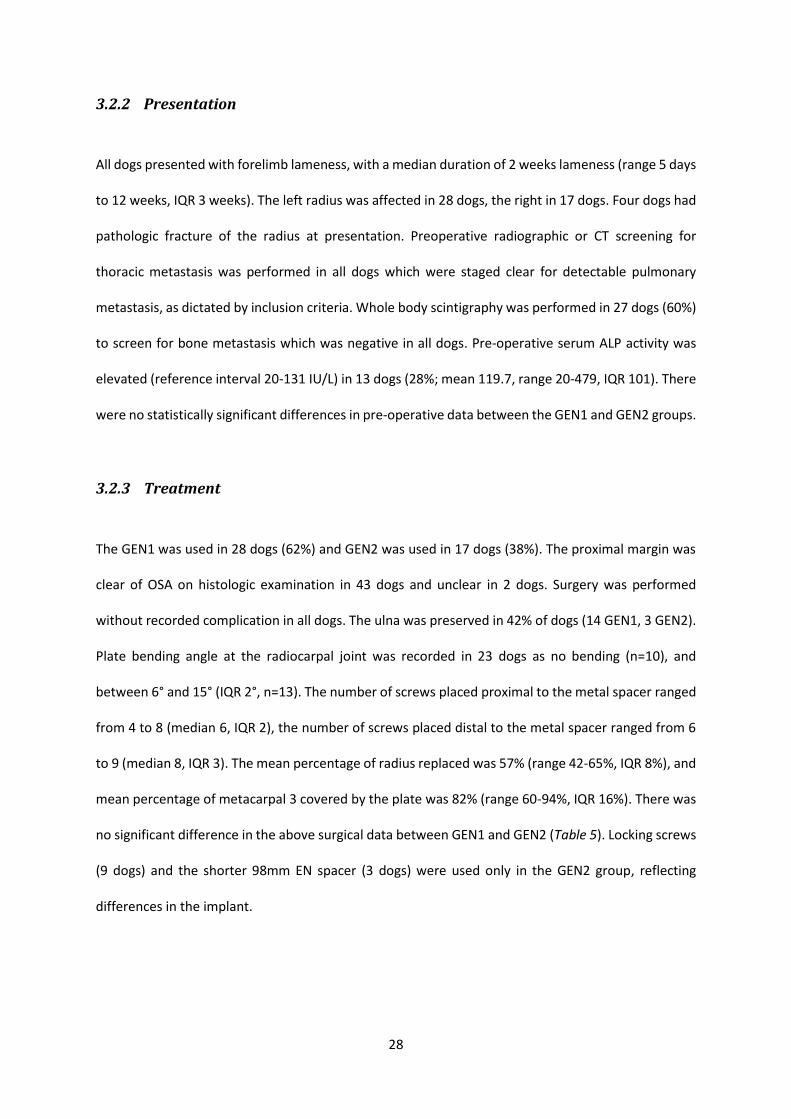
from Colorado State University. Evaluation of GEN2 in the FE model predicted stresses in the proximal
radius that exceeded the fatigue limit and yield stress of 316L stainless steel; the predicted stresses of
GEN2 are too high for sustained performance. An engineering specific approach was taken to design

iii
a novel EN and evaluation in the FE model resulted in 50% reduction in peak stresses in the radial
screws compared to GEN2 in the FE model.
The second component of this thesis is evaluation of the suitability of the novel EN for clinical use. The
novel EN prototypes were manufactured using three-dimensional printing (3DP) in plastic and
stainless steel. Three size variations of the novel EN were designed using a computer-aided design
(CAD) program and implanted into large breed cadaver radii. There was a large variation in radius
morphology between and within large breeds; making the novel EN unlikely to be suitable as an off
the shelf implant. The most appropriate application of the novel EN would be via rapid prototyping
based on an individual’s computed tomography scan.
This thesis highlights the difficulties associated with limb sparing surgery in veterinary surgery. The
currently available procedures provide an alternative for pet-owners that are averse to amputation.
However, pet-owners must be aware of the high complication frequencies associated with the
techniques. Once refined; the novel EN has potential to decrease implant-related complication rates,
however the infection rates are likely to remain high.

iv
Acknowledgements
Stewart Ryan
Ted Whittem
Chris Whitton
Brenton Chambers
Adrian Wallace
The Veterinary Society of Surgical Oncologists
Retrospective Study: Sarah Boston, Nicole Ehrhart, Marvin Kung, Sarah Dry, Julius Liptak, Martin
Havlicek, Radboud Kemme, Rod Straw, Mary Lafferty, James Simcock, James Farese
Statistical analysis: Louise Mitchell, Garry Anderson
Novel Endoprosthesis: Snehal Shetye, Christian Puttlitz, Nicole Ehrhart, Peter Lee, Mike Xie, Ben
Baxter, Chris Henry, Nirmal Menon

v
Table of Contents
Abstract ................................................................................................................................................... ii
Acknowledgements ................................................................................................................................ iv
Table of Contents .................................................................................................................................... v
List of tables ......................................................................................................................................... viii
List of figures .......................................................................................................................................... ix
List of abbreviations ............................................................................................................................... xi
1. Introduction ................................................................................................................................... 1
1.1 Background on Osteosarcoma ................................................................................................ 1
1.1.1 Risk factors for the development of osteosarcoma ........................................................ 1
1.1.2 Presentation .................................................................................................................... 2
1.1.3 Diagnosing osteosarcoma ............................................................................................... 2
1.1.4 Evaluation for metastasis ................................................................................................ 4
1.1.5 Evaluation of tumour margins ........................................................................................ 6
1.1.6 Prognostic indicators....................................................................................................... 6
1.2 Curative Intent Treatment for Osteosarcoma ...................................................................... 10
1.2.1 Limb amputation ........................................................................................................... 10
1.2.2 Limb-sparing surgery ..................................................................................................... 11
1.2.3 Metal endoprosthesis for limb-sparing surgery............................................................ 18
1.2.4 Adjuvant therapies ........................................................................................................ 22
2. Aims and Objectives ..................................................................................................................... 24

vi
2.1 Multi-institutional Retrospective Study on Metal Endoprosthesis....................................... 24
2.2 Evaluation of a Novel Endoprosthesis .................................................................................. 24
3. Multi-institutional Retrospective Study on Metal Endoprosthesis .............................................. 25
3.1 Methods ................................................................................................................................ 25
3.1.1 Statistical analysis ......................................................................................................... 26
3.2 Results ................................................................................................................................... 27
3.2.1 Signalment .................................................................................................................... 27
3.2.2 Presentation .................................................................................................................. 28
3.2.3 Treatment ..................................................................................................................... 28
3.2.4 Surgical outcomes ......................................................................................................... 29
3.2.5 Oncologic outcomes ...................................................................................................... 31
3.3 Discussion .............................................................................................................................. 32
3.4 Conclusion ............................................................................................................................. 35
4. Evaluation of a Novel Endoprosthesis .......................................................................................... 37
4.1 Background ........................................................................................................................... 37
4.1.1 Evaluation of second generation endoprosthesis......................................................... 37
4.1.2 Novel endoprosthesis design ........................................................................................ 39
4.2 Three Dimensional Printing of Novel Implant ....................................................................... 42
4.3 Cadaver Implantation Trials .................................................................................................. 43
4.3.1 Cadaver Limb Collection ............................................................................................... 43
4.3.2 Cadaver Limb Measurements ....................................................................................... 43
4.3.3 Cadaver Implantation with Novel Endoprothesis ......................................................... 45

vii
4.4 Future Work .......................................................................................................................... 54
4.4.1 Photoelastic Strain Testing ............................................................................................ 55
4.4.2 Testing in Axial Compression ........................................................................................ 57
4.5 Discussion .............................................................................................................................. 58
5. Conclusions .................................................................................................................................. 62
6. List of References ......................................................................................................................... 63
Appendix 1: Manuscript for multi-institutional retrospective study on metal endoprosthesis………… I
Appendix 2: Veterinary Society of Surgical Oncology study proposal………………………………………………. II
Appendix 3: Veterinary Society of Surgical Oncology data accrual form………………………………………….. III
Appendix 4: Surgical procedure for novel implant…………………………………………………………………………… IV

viii
List of tables
1. Classification for tumour grade determination from Kirpensteijn et al. (2002) 7
2. Classification for tumour grade determination from Loukopoulos et al. (2007) 8
3. Staging system for canine and human osteosarcoma 8
4. Summary of major studies investigating cortical allograft for limb sparing surgery 13
5. Frequencies and comparisons of surgical outcomes between endoprosthesis generations 29
6. Variables tested for association with implant-related complication and local recurrence 30
7. Reported lameness in post-operative period 31
8. Comparison of oncologic outcomes between endoprosthesis generations 32
9. Computed Tomography measurements of five similar sized greyhound cadaver radii 44

ix
List of figures
1. Radiograph of distal radius osteosarcoma 3
2. Osteosarcoma staining positive for alkaline phosphatase 3
3. Cortical allograft limb sparing surgery 12
4. Pasteurised autograft limb sparing surgery 12
5. Vascularised ulnar transposition limb sparing surgery 12
6. Bone transport osteogenesis limb sparing surgery 17
7. First generation metal endoprosthesis implants 18
8. Photograph and radiograph of metal endoprosthesis limb sparing surgery 20
9. Proximal screw breakage in metal endoprosthesis limb sparing case 20
10. Second generation metal endoprosthesis with hydroxyapatite coated ends 21
11. Second generation metal endoprosthesis implants 22
12. Tantalum distal radial endoprosthesis 22
13. Final FE model incorporating second generation endoprosthesis construct 38
14. Graph showing von Mises stress predictions of GEN2 in FE model 39
15. Novel endoprosthesis: proximal endoprosthesis component 40
16. Novel endoprosthesis: mid-diaphyseal endoprosthesis component 41
17. Novel endoprosthesis: distal endoprosthesis component 41
18. Measurements of greyhound cadaver radii 44

x
19. Technique for cadaver implantation 46
20. Prototype 1 CAD with scaling measurements 47
21. Prototype 1 in plastic and stainless steel 48
22. Post-implantation radiograph of prototype 1 48
23. Prototype 2 in plastic 49
24. Prototype 2 distal component on radiocarpal bone 50
25. Final protoype in 316L stainless steel 51
26. Final prototype implanted in Boxer and German Shepherd cadaver specimens 52
27. Radiographs of final prototype implanted in Boxer and German Shepherd specimens 53
28. Radiographs of final prototype implanted in Greyhound specimen 54
29. Final prototype implanted in Rottweiler 54
30. Photoelastic strain testing 55
31. Materials testing machine and strain gauge measurement 58
32. Photograph of Greyhound and Rottweiler radius morphology 60
33. Angle-stable interlocking nail bolt system 61

xi
List of abbreviations
3DP three-dimensional printing
ALP alkaline phosphatase
BALP bone alkaline phosphatase
BTO bone transport osteogenesis
CA core aspirate cytology
CAD computer-aided design
CI confidence interval
CT computed tomography
DCP dynamic compression plate
DEC distal endoprosthesis component
DFI disease free intervals
EN endoprosthesis
FE finite element
FNA fine needle aspirate
GEN1 first generation metal endoprosthesis
GEN2 second generation metal endoprosthesis
IORT intraoperative extracorporeal irradiation
IQR interquartile range
KM Kaplan-Meier
MEC mid-diaphyseal endoprosthesis component
MFI metastasis free interval
MRI magnetic resonance imaging
MST median survival time
OPLA-Pt open cell polylactic acid polymer sponges implanted with cisplatin
OSA osteosarcoma
PEC proximal endoprosthesis component
PMMA polymethyl-methacrylate
SALP serum alkaline phosphatase
ST survival time

1
1. Introduction
1.1 Background on Osteosarcoma
Osteosarcoma (OSA) is the most common primary bone tumour in dogs,13 accounting for up to 85%
of malignancies of the skeleton.14 Osteosarcoma is more common in the appendicular skeleton (up to
70%), less common in the axial skeleton and extra-skeletal tissues (27.1% and 2.8% respectively).15
1.1.1 Risk factors for the development of osteosarcoma
The risk of developing OSA is highest for large and giant breed dogs,13,15-17 with 92% of dogs diagnosed
with OSA weighing over 20kg.18 The risk of bone sarcoma in dogs weighing over 36kg is 61 times higher
than the risk in dogs weighing less than 9kg.19 Greyhounds, Rottweilers and Great Danes have
increased risk of developing OSA compared to mixed breed dogs,20,21 however weight and height are
considered a more important risk factor than breed.16
A trend of increasing OSA risk is observed with increasing age, with a plateau after 10 years of age.16
The vast majority of cases present between 7 and 9 years.14,15,17,18,22-26 However, the age at
presentation is bimodal, with up to 10% of cases presenting under two years of age.14 The youngest
reported case is in a 10 month old Great Dane puppy.27 Rottweilers have been shown to be
significantly younger at presentation than other breeds.24
Neutered dogs have been shown to have a twofold greater risk of developing appendicular OSA
compared to sexually intact dogs.16 A study of Rottweilers showed that the risk of bone sarcoma was
significantly increased by desexing early in life.28
2
Ionizing radiation can cause OSA in dogs as a late complication of radiation therapy.29 Most reported
cases developed OSA following coarse fractions, therefore, megavoltage irradiation used in a finer
fraction scheme may minimise this risk.
Sites of previous fracture and/or internal fixation with an implant are reported as possible risk factors
for the development of OSA.26,30-35. OSA at the proximal tibial site following tibial plateau levelling
osteotomy is also reported.36-41
1.1.2 Presentation
Lameness and localised limb swelling are the most common reason for presentation. Lameness is
caused by periosteal inflammation, micro-fractures and occasionally pathologic fractures. Swelling
usually results from extra-compartmental extension of bone tumour into adjacent soft tissues.13
The most frequent sites of OSA are the distal radius and proximal humerus,14,20,22,42 with up to 40% of
cases diagnosed with distal radial OSA.43 Other common appendicular skeletal sites include the
proximal and distal femur and tibia.14 The three types of OSA are endosteal, periosteal and parosteal.
Periosteal and paraosteal originate from the periosteum and are rare compared to endosteal OSA.13
Rarely, OSA can originate in diaphyseal or metaphyseal bone on both sides of a joint.16
1.1.3 Diagnosing osteosarcoma
Radiographs are recommended for tentative diagnosis and staging of OSA, although radiography
cannot definitively distinguish different tumour types or between tumour and inflammation.44
Radiographic features of endosteal OSA include destruction of cortical or medullary bone, sclerosis or
periosteal new bone formation, palisading cortical bone (sunburst effect), periosteal lifting caused by
subperiosteal haemorrhage (Codman’s triangle), loss of fine trabecular pattern in metaphyseal bone
and pathologic fracture with metaphyseal collapse (Figure 1).45

3
Fine needle aspirate (FNA) has the potential to provide a rapid diagnosis to allow pet-owners to make
informed treatment decisions. Other benefits include low mortality, minimal bone disruption and
short procedure time. Diagnostic accuracy of FNA ranges from 69% to 92%.46 Limitations of FNA
cytology of bone tumours includes hypocellular samples, differentiating neoplastic from reactive
bone, and difficultly differentiating between different bone tumours.4
An alkaline phosphatase (ALP) stain can differentiate OSA from other tumours that express vimentin
by immunohistochemistry (Figure 2).4,47 Reactive bone will also stain ALP positive, therefore, careful
cytologic analysis for evidence of malignancy and lack of inflammation is required for appropriate
interpretation. The high sensitivity and specificity (100% and 89% respectively) make the ALP stain a
useful adjunct test for diagnosing OSA.47
A novel method of core aspirate cytology (CA) diagnosis was described in a prospective study by
Neihaus et al.4 in which CA was compared to FNA and histopathology for 20 dogs with lytic or
proliferative bone lesions. The authors were able to diagnose OSA in 85% of cases via FNA, and 95%
of cases via CA, however there was no significant difference in diagnostic accuracy between the two
tests, and the final recommendation was to use FNA with ALP staining as an initial diagnostic test.
Figure 1: Radiograph of distal radius osteosarcoma. Image from North 2009 8
Figure 2: Osteosarcoma staining positive for alkaline phosphatase. Positive staining is indicated by black-brown granules within the cytoplasm of
neoplastic cells (arrow). From Neihaus et al. 2011.4

4
Histopathology remains the gold standard for diagnosing OSA, and bone biopsy can be performed
using open or closed techniques. Open bone biopsy risks wound breakdown, haematoma formation,
infection, pathological fracture, seeding of tumour along biopsy tract.48 Closed biopsies are often
obtained with a Michelle trephine, or a Jamshidi needle. Multiple specimens increased the probability
of accurate diagnosis, and the radiographic center of the lesion was the most accurate location.49 The
larger core diameter of a Michelle trephine yields a diagnostic accuracy rate of 93.8% but has an
increased risk of pathologic fractures compared to the Jamshidi biopsy technique.49 Jamshidi biopsy
technique is technically simple, and safe to perform, with an accuracy rate for determining tumour
versus non-tumour of 91.9% and sub-classification of OSA in 62.5% of cases.48 Bone biopsy is not
always recommended, and histopathological diagnosis is often performed following curative intent
surgery.
1.1.4 Evaluation for metastasis
Appendicular OSA is highly malignant; approximately 10% of dogs have gross pulmonary or bone
metastatic disease and up to 90% of dogs are suspected to have micro-metastatic disease at time of
first presentation.13,23 Metastatic spread occurs primarily through haematogenous routes; with
between 60% and 70% of metastatic spread occurring in the lungs, and between 5% and 20% to other
bones.22,23,50 Regional lymph node metastasis is rare in dogs with appendicular OSA (4.4% - 25%).22,51
Cutaneous and splenic metastasis has been reported rarely.52 Rottweilers were shown to have a higher
rate of brain and mammary tissue metastasis than other breeds.24 Patients should be evaluated for
clinical metastasis prior to curative intent surgery using thorough physical examination and diagnostic
imaging. The detection of metastasis for staging purposes is important because the presence of
metastases negatively impacts prognosis and restricts potential treatment options.

5
Pulmonary metastasis
Pulmonary metastasis is most commonly detected with three-view thoracic radiography or computed
tomography (CT). Three-view thoracic radiography consists of right and left lateral and ventrodorsal
or dorsoventral views. Lesions of 6mm or more in diameter can be detected on radiographs.13
Computed tomography is considered the gold standard for detecting pulmonary metastasis in humans
because CT is able to detect smaller nodules with greater frequency than survey radiography.53 The
two main advantages of CT are elimination of superimposition by thoracic structures and superior
contrast resolution.54 Studies comparing the two methods in dogs found that CT was more sensitive
than radiography, particularly evident in large and giant breed dogs, and that significantly smaller
nodules (2mm diameter) were detected with CT (P = 0.0007). 54,55
Skeletal metastasis
Bone scintigraphy can be used to detect occult osseous metastasis. The technique uses intravenous
radiopharmaceutical agents (typically Technetium-99m), which localise in bone principally by binding
to hydroxyapatite crystals. Bone with increased metabolic activity will appear as a foci of increased
radioisotope uptake.56 Bone scintigraphy is more sensitive than radiography,56 however, can also
reveal non-neoplastic lesions, such as degenerative joint disease or osteomyelitis, that must be
differentiated from neoplasia by focused diagnostic imaging or histopathology. Prior to the
accessibility of scintigraphy to veterinary patients, whole body radiographic bone surveys were
completed to screen for metastatic spread. One study reported the use of radiographic bone surveys
found non-clinically detectable neoplastic bone lesions in 7.1% of cases (3/42 dogs).57

6
1.1.5 Evaluation of tumour margins
Accurate determination of tumour margins prior to surgical treatment is critical if the patient is to
undergo limb-sparing surgery. Many studies have attempted to evaluate which diagnostic imaging
technique yields the most accurate measure of tumour length.
Magnetic resonance imaging (MRI) with T1 weighted non-contrast images are reportedly the most
accurate method to detect the extent of intrameduallary OSA.58 MRI tends to overestimate tumour
length, compared to radiographs, nuclear scintigraphy and CT.58-61 Human studies report 96-99%
accuracy rate in defining intramedullary tumour extent with MRI when compared to 75-86% for CT
and 56-63% for nuclear scintigraphy.62 Underestimation of tumour size has the potential to lead to
incomplete tumour resection for limb-sparing surgery, and risk of local tumour recurrence, however,
overestimation of tumour size has the potential to exclude suitable patients as candidates for limb-
sparing surgery. The conclusion is that two or more imaging modalities should be evaluated in
conjunction for the most accurate measurement of tumour length.
1.1.6 Prognostic indicators
Host factors
Increasing age is correlated with shorter disease free intervals (DFI).16,20,63, and mortality.64 Survival
time is longest in dogs between 7 and 10 years of age, and shortest in those both younger and older.50
Increasing weight is also associated with an increase in risk of metastasis and mortality.64

7
Tumour factors
OSA location in the proximal humerus is correlated with shorter survival times than with other
locations in the appendicular skeleton; in a meta-analysis study humeral OSA had a median survival
time (MST) that was 132 days shorter than other locations.63,65,66 An individual patient data meta-
analysis study found that distal radial OSA location is associated with a decreased hazard of
metastasis.64
Histologic grade can provide an assessment of the biologic aggressiveness of the tumour, and is shown
to be of prognostic significance in human OSA.67,68 Kirpensteijn et al. (2002)22 proposed a histologic
grading system for canine OSA (Table 1). Grades I, II and III were represented in 4.2%, 20.5% and 75.3%
of OSA tumours respectively (appendicular, axial and extra-skeletal included).22 Grade I and II OSA had
a significantly better prognosis than grade III, with Grade III tumours having significantly decreased
MST and DFI.22
Tumour Grade Pleomorphism Mitosis Tumour Matrix Tumour Cells Necrosis
I 0-1 (<25%) <10 1 (>50%) 1 (<25%) 0-1 (<25%) II 2 (25-50%) 10-20 2 (25-50%) 2 (25-50% 2 (25-50%) III 3-4 ( >50%) >21 3 (< 25%) 3-4 (>50%) 3-4 (>50%)
Table 1: Classification for tumour grade determination from Kirpensteijn et al. (2002)22
The original grading system was then further modified by Straw et al. (1996) (Table 2) and
subsequently used by Loukopoulos et al. (2007) to investigate prognosis associated with grade. In
contrast to the previous study the distribution across grades was more uniform; 35% grade I, 37%
grade II and 28% grade III.15 Primary tumours that had metastasized were significantly higher grade
than non-metastatic tumours.15 Dogs younger than 4 years of age had OSA of higher grade, score and
mitotic index than older animals.15

8
Parameter Description Value
Nuclear pleomorphism None Mild
Moderate Marked
0 1 2 3
Mitotic index (# of mitoses per 10 fields at x400) 1-10 11-20 21-30 >30
1 2 3 4
Degree of necrosis (%) None <15
15-50 >50
0 1 2 3
Table 2: Classification for tumour grade determination modified from Straw69 and used by Loukopoulos15. Histological grade is determined by combined scores (1-5 = grade I; 6-7 = grade II; 8-10 = grade III.
Metastasis
Clinical stage is prognostic, with stage III patients having shorter survival times than stage I or II (Table
3). Most dogs present with stage IIb disease.8 A study by Boston et al. (2006) showed that dogs with
metastasis to the bone had significantly longer survival times compared to those with metastasis to
the lung (P = 0.003) and lymph node (P = 0.001).23 Lymph node metastasis is significantly associated
with shorter median survival time and disease free interval compared to those without metastasis.51
Stage Characteristics
I Low grade without evidence of metastasis II High grade without evidence of metastasis III Any grade with metastasis a Intracompartmental b Extracompartmental
Table 3: Staging system for canine and human osteosarcoma.8
Pre-treatment blood analysis
Serum alkaline phosphatase (SALP) in normal dogs mostly consists of isoenzymes derived from liver
and bone.70 The enzyme has been recognised as a prognostic indicator in human OSA for many years,
however is thought to be limited by its lack of specificity for tumour tissue.71 Ehrhart et al. (1998)72
first investigated the association between SALP and bone specific (BALP) isoenzyme fractions of

9
alkaline phosphatase. The retrospective study involved 75 dogs with appendicular OSA and found that
survival time and disease free intervals were significantly associated with pre-operative SALP and
BALP. Total SALP greater than 110 U/L was significantly associated with a shorter survival interval,
with a MST of 177 days compared to 495 days in those with SALP ≤ 100 U/L.72 Other studies
corroborate these findings,22,64,65,70 although it should be noted that ALP measurements after
treatment were not significantly correlated with survival.70 Recent work found that absolute tumour
burden is a determinant of serum BALP, and as such the association between pre-treatment BALP and
negative clinical prognosis may simply be attributed to greater initial tumour burden.73
Higher numbers of circulating monocytes (>0.4 x 103 cells/μL) and lymphocytes (>1.0 x 103 cells/μL)
before treatment were found to be significantly associated with a shorter disease free interval.74 Many
of the animals in this retrospective study had monocytes within the normal reference range, indicating
that subtle variations within the range of leukocyte values might have prognostic significance.74
Infection and limb-sparing surgery
A significant relationship between post-operative infection and MST/DFI for dogs with OSA treated
with limb-sparing surgery and adjuvant chemotherapy has been found.75 Thrall et al. (1990), Lascelles
et al. (2005) and Liptak et al. (2006) report increased MST,1,75,76 and increased disease free intervals.1
Dogs with post-operative infection survived 252 days longer, were half as likely to have metastasis
diagnosed, and half as likely to die, as those without infection.76
The mechanism responsible for the relationship between infection and MST and DFI is not yet
understood but is presumed to be secondary to a non-specific immunologic stimulation. Other
possibilities include that the combined effect of chemotherapy and infection may be more
pronounced, that up-regulation of macrophages or other cytotoxic cells can release anti-angiogenic

10
factors, that certain antibiotics (such as fluroquinolones) can have anti-cancer effects or that the
rejection of the allograft might result in rejection of the OSA.76
1.2 Curative Intent Treatment for Osteosarcoma
The standard of care for curative-intent treatment for dogs with OSA involves limb amputation for
local tumour control followed with adjuvant chemotherapy for treatment or prevention of systemic
metastatic disease.77 Limb amputation is contraindicated in some patients; obese patients and those
with neurological or orthopaedic disease in other limbs.78,79 In addition, some pet-owners are adverse
to the idea of amputation.80-82 For these reasons, limb-sparing techniques are becoming more
common.77 Chemotherapy is required to reduce the risk of developing metastatic disease and prolong
a good quality of life.
1.2.1 Limb amputation
The goal of limb amputation is complete resection of the primary tumour via radical surgical resection
to prevent local tumour recurrence and improve overall survival times. While amputation without
adjuvant therapy is only palliative, the prognosis remains better than with no treatment.50 Forequarter
amputation is recommended for the forelimb for both tumour control and cosmetic reasons.13
Amputation of the hindlimb can be performed with disarticulation of the hip joint or proximal femoral
shaft amputation, based on tumour location and surgeon preference. Amputation of the whole
hindlimb with en bloc resection of the acetabulum is recommended for tumours of the proximal
femur.83 Complications of limb amputation are rare and include haemorrhage, air embolism,
inadvertent thoracotomy, infection and local recurrence.84 Post-operatively, most dogs can ambulate
unassisted within 12 to 24 hours.84

11
Limb amputation may be contraindicated in cases with concurrent orthopaedic or neurological
disease or in cases of severe obesity.77 Kirpensteijn et al. (2000) performed a force plate analysis study
that compared normal dogs and dogs with a limb amputation. They found that amputation of a limb
causes significant changes to normal gait, with greater changes seen in cases with forelimb
amputations compared to hindlimb amputations. For dogs undergoing forelimb amputation, each
hindlimb carries 27% of body weight while the remaining forelimb carries 46%.79 After a hindlimb
amputation, the remaining hindlimb carries 26% of the load, while the forelimbs carry 37% each.79
These changes warrant thorough investigation of the remaining contralateral limb prior to surgery,
especially in dogs undergoing forelimb amputations.
Some pet-owners are averse to the idea of limb amputation. Kirpensteijn et al. (1999) interviewed 44
pet-owners about their experiences with their dog following limb amputation. Forty-two of the 44
dogs adapted satisfactorily to locomotion on three legs, and most adapted within a month of surgery,
faster than most pet-owner expectations.80 Weight or age had no significant association with
adaptation.80 Almost half the respondents had initial objections to the surgery because of the
expected appearance after amputation, although 37 of 43 pet-owners indicated they would make the
same decision if a similar problem arose.80 A questionnaire study by Withrow and Hirsch (1979)
similarly reported that many pet-owners initially were hesitant to amputate the limb, however post-
amputation satisfaction was high.82 Another study reported that the majority of pet-owners remarked
that although the initial decision to amputate was very difficult, they were satisfied with the decision.81
1.2.2 Limb-sparing surgery
Limb-sparing techniques involve marginal tumour resection and reconstruction of the bony
column.78,85,86 The ideal limb-sparing technique should have biological affinity for the host tissue,
resistance to infection, sufficient biomechanical strength and resilience.87 The ideal candidate for limb-
sparing surgery has OSA with minimal invasion into adjacent soft tissues, tumour length less than 50%

12
the bone length, absence of pathological fracture and no evidence of metastatic spread.13,84 For
properly selected cases, many cases are weight bearing by 2 weeks following limb-sparing surgery and
up to 90% of dogs attain good to excellent limb function.77 Limb-sparing techniques in the distal radius
have produced the most favorable results, largely because pancarpal arthrodesis is well tolerated by
dogs.13 Arthrodesis of the shoulder or stifle joint results in poor functionality of the limb.12,77,88
Cortical allograft
Cortical allograft limb-sparing surgery allows replacement of the resected bone with a cortical allograft
which is stabilized with plate and screws (Figure 3). The allograft allows osteoinduction in the recipient
and provides osteoconduction.89 Aseptically harvested, frozen cortical allografts are kept in a bone
bank facility. Availability of allografts or maintenance of a bone bank is a significant disadvantage of
the technique.1,89 Use of the allograft is reported for distal radius, proximal humerus, distal femur,
ulnar, metacarpus, proximal and distal tibia and the metatarsus.75,85,89
Figure 4: Pasteurised autograft following plate removal 708 days post-operative. From Buracco et
al (2002)12
Figure 3: Intraoperative and postoperative cortical allograft.
From Liptak et al (2006)1
Figure 5: Vascularised ulnar transposition immediately post-
operative and 142 days post-operative. From Séguin et al. (2003)9

13
Table 4 summarizes the major studies investigating outcomes following cortical allograft and
chemotherapy. Complication rates occur in more than 50% of patients.84 Infection rates range from
20-60%.1,75,77,85,89,90 Potential causes of the high infection rate include inadequate soft tissue coverage,
poor blood supply to distal radius and impaired healing secondary to chemotherapy.76 Implant-related
complications rates range from 11-53%.1,75,85,89 Local recurrence rates range from 10-28%.1,75,77,85,89,90
Local recurrence is reduced with histologically clean margins and the use of adjuvant chemotherapy
or radiation therapy.1,77,84
Reference Case numbers
Local recurrence
Infection rate
Implant failure
rate
MST (days)
Comments
LaRue et al.(1989) 85 17 21% 31% 24% 240 Included sites other than distal radius.
Thrall et al.(1990) 75 17 24% 41% 53% 180 Included sites other than distal radius.
Berg et al.(1992) 90 5 20% 20% N/A N/A Small sample size. Straw & Withrow (1996) 77 220 25% after
1 year 44% N/A N/A Review article, not
in peer-reviewed clinical trial.
Morello et al. (2001) 89 18 28% 39% 11% 266 Included sites other than distal radius (majority distal
radius). Liptak et al. (2006) 1 10 10% 60% 40% 412
Table 4: Summary of major studies investigating cortical allograft for limb sparing surgery.
The studies by Berg et.al (1992) and Liptak et.al (2006) investigate distal radius OSA only, and the study
by Morello et al. (2001) was mostly distal radius OSA. Berg et al. (1992) reported lower complication
rates than previous; with 1 case each developing local tumour recurrence and infection.90 Morello et
al. (2001) reported good to excellent limb function in 72% of cases, that most dogs were able to use
the leg within one month of surgery and that best outcomes were seen in those that underwent carpal
arthrodesis.89 In the prospective clinical trial by Liptak et al. (2006) 6 dogs developed infection, with a
median time to infection of 80 days.1 One of the dogs required debridement surgery and another
required limb amputation to assist management of the severe infection. Four dogs developed
construct failure with a median time to failure of 309 days.1 Screw loosening or breakage was the

14
mechanism of failure in all cases, and occurred either in the metacarpal bone (3 of the 4 dogs) or in
the radio-carpal bone (1 of the 4 dogs). In 70% of the dogs, limb function was graded as good to
excellent. Screw loosening or breakage distal to the allograft were the most common complications.1
Kirpensteijn et al. (1998) compared the use of cemented and non-cemented allografts in dogs with
distal radial osteosarcoma. Complications associated with implant loosening or fixation failure may
decrease after inserting polymethyl-methacrylate (PMMA) into the bone marrow space of allografts.
The authors found that the use of cemented allografts significantly decreased complications of
implant loosening and allograft failure, but delayed allograft healing.91 The mean radiographic scores
for combined proximal and distal union were significantly greater in the non-cemented group at
2,3,6,9,15 and 24 months.91
Autografts
Autogenous limb-sparing techniques involve sterilization of the affected bone with pasteurization,
autoclaving or irradiation. The major advantages are good anatomic fit into recipient site and no bone
bank requirements.12,92
Pasteurization of an autograft (Figure 4) was developed because of the difficulties associated with
creating and maintaining a cortical allograft bone bank. Pasteurization of host bone is performed in
sterile saline at 65°C for 40 minutes. The segment is then replaced in the defect and secured using a
plate in similar fashion to the cortical allograft. Complications and outcomes are similar to that seen
with cortical allograft; local recurrence (15%), infection (31%) and implant failure (23%).92 Limb
function following autograft placement also reflected those of cortical allograft with 92% of patients
having good limb function post-surgery. The MST and DFI were 324 days and 255 days respectively.92
This technique is not recommended in cases with severe bone lysis.12,92

15
Intraoperative extracorporeal irradiation (IORT) involves local resection of the tumour, irradiation of
the bone segment with a single fraction of 50-300Gy, removal of the extraneous-irradiated soft tissues
and re-implantation and internal fixation of the irradiated bone. Doses greater than 50Gy are
tumouricidal and result in complete necrosis of OSA bone tumour.93 The primary advantage of IORT is
that the treatment can be focused on the tumour whilst sparing normal adjacent tissues, creating a
sterile autograft that histologically shows evidence of healing at the osteotomy site.94 A major
disadvantage is the inability to check for complete bone margins with post-operative histopathology.94
Overall, limb function and complication rates are similar to other limb-sparing techniques.13,94,95
Pathological fracture is the most common complication, likely caused by a combination of radiation
induced necrosis and osteolysis from the tumour.94,95 Other complications include implant failure
(38%), infection (23%) local reoccurrence (23%) and radiation-induced side effects.95 A major
complication unique to this technique was collapse of the articular cartilage and subchondral bone in
the radio-carpal joint.94 In one study 75% of dogs required amputation secondary to post-operative
complications, therefore strict case selection should be employed.94 The ideal case should have
minimal soft tissue involvement, minimal osteolysis, no involvement of the ulna and allow for at least
3 bi-cortical screws proximal to the osteotomy site.
Ulnar transposition
Vascularised ulnar transposition (Figure 5) uses the ipsilateral distal ulna to replace the distal radial
defect following tumour excision. The rollover transposition allows pivoting of a bone graft on its intact
vascular pedicle, accelerating the process of union and allowing hypertrophy of the graft. The method
is proposed to decrease the high incidence of infection seen with cortical allografts, as well as remove
the need for a cortical allograft bone bank.
The technique was first described by Séguin et al. (2003) who performed an anatomical study and
then described three clinical cases. Two of the three dogs suffered post-operative complications; one

16
dog fractured the proximal radius and the other developed screw loosening and/or osteomyelitis.9 A
further two cases were reported by Irvine-Smith et al. (2006) who reported clinical union in both cases
and visible hypertrophy of the graft post-operatively. A larger retrospective case series of 8 dogs was
published by Hodge et al. (2011), who reported recurrence of tumour in 25%, metastasis in 50%,
implant loosening in 37.5%, implant failure in 12.5% and infection in 62.5% of dogs. The study yielded
similar long term complications and limb function as cortical allograft and metal endoprosthesis.96
Biomechanical evaluation of the ulnar transposition graft and cortical radial allograft using a cadaveric
model indicated that the ulnar transposition is biomechanically weaker than the cortical allograft.97
Paired cadaver forelimbs were tested in axial loading until failure and the cortical allograft constructs
had significantly greater stiffness, yield load, maximum load, maximum energy, and post-yield energy
compared to the ulnar transposition constructs. This weakness is a result of the size of the ulnar graft
and cranial position of the graft against the plate. However, over time the ulnar autograft is expected
to hypertrophy in response to forces experienced by the bone. Further research is required to
establish healing times for ulnar vascularized grafts, time until implant removal, and the extent of
radial bone that could ultimately be replaced by the ulna.
Bone transport osteogenesis
Distraction osteogenesis is a surgical process which relies on the normal healing process that occurs
between two osteotomised bone segments. Bone transport osteogenesis (BTO) for OSA involves
transportation of a small portion of normal bone adjacent to the bony defect, while new bone forms
in the trailing distraction pathway (Figure 6). The success of BTO relies on prolonged, progressive and
gradual distraction to not disrupt blood supply and allow local tissues to accommodate.5 The reported
advantages include a highly vascularized autogenous graft that is highly resistant to infection.
Disadvantages include the length of time that the fixator must remain in place and intensive post-

17
operative care requirements. BTO is not recommended in patients that have already undergone
radiation therapy.5
Degna et al. (2000) and Ehrhart (2005) have reported six and nine cases respectively. One series
reported complications of local recurrence (2 of 6 cases) and necrosis of regenerate bone (1 of 6
cases).98 The other series reported wire breakage or pull-out (56%), non-union at docking site (11%),
local recurrence (22%), flexor contracture (11%).5 Two of the cases in the study by Ehrhart (2005) were
performed as salvage procedures following allograft limb-sparing surgery. Limb function was good to
excellent in all but 2 dogs at follow-up (minimum 9 months post-operatively).5
Double BTO applies simultaneous longitudinal transport of two adjacent bone segments at different
rates allowing the defect to be filled in less time (1.5mm/day vs 1mm/day).99 Another novel technique
utilizes transverse ulnar BTO to resolve large radial defects in substantially less time by shortening the
transport distance.100
Figure 6: (A) Immediate post-operative radiograph of a bone transport osteogenesis. (B) 4 weeks. (C) 8 weeks. (D) 16 weeks. (E) 9 months: the fixator has been off for 9 weeks. From Ehrhart (2005).5

18
1.2.3 Metal endoprosthesis for limb-sparing surgery
The metal endoprosthesis (EN) (Veterinary Orthopedic Implants; Burlington VT) was developed to
allow reconstruction of radial bone defects with a readily available, biologically inert material implant
that required minimal preparation prior to implantation. The first generation implant consists of a 24
hole limb-sparing plate and a solid 122mm segment of 316L surgical steel with a flared distal end
(Figure 7 & 8). The limb-sparing plate has a greater cross-sectional area than a 3.5mm broad or 4.5mm
narrow dynamic compression plate, round rather than oval screw holes, proximal screw hole
diameters which accommodate 3.5 and 4.5mm cortical bone screws and 4.0 cancellous bone screws,
and a tapered distal end for the metacarpus with screw hole diameters to accommodate 2.7 or 3.5mm
cortical bone screws.
Liptak et al. (2006) performed a cadaveric study in which the biomechanical properties of EN and
cortical allograft limb-sparing surgeries were compared. Cadaver forelimbs were prepared and a
110mm segment of the distal radius was resected using the standard limb-salvage technique. The
osseous defect was filled with either a cortical bone graft or first generation EN. The bone plate was
applied without any bending at the level of the proximal radio-carpal bone. The reconstructed limbs
were placed in a materials testing system and after preconditioning with cyclic compressive loads the
constructs were ramped to failure in axial compression at a rate of 300 N/s. This biomechanical study
did not evaluate the effects of cyclic loading, which may increase the risk of implant loosening and
Figure 7: First generation metal endoprosthesis produced by Veterinary Orthopedic Implant; Disassembled view. From Liptak et al (2006).3

19
failure over time. Construct failure was observed in 5 EN limbs (41.7%), compared to 92% of limbs
reconstructed with cortical allograft. The construct failure level was at the metacarpus (n=4) or
proximal radius (1). Plastic deformation of the bone plate was seen in 2 EN limbs (16.7%) compared
to 58.3% of limbs reconstructed with cortical allograft. In both cases plate bending was associated
with metacarpal fracture or screw pullout from the metacarpus. The mean yield load for the cortical
bone graft (1580-2225N) and EN (2922-3260N) constructs exceeded the peak vertical ground reaction
force at a trot by up to 5- and 8-fold, respectively. Catastrophic failure of EN constructs occurred at
loads 229-258% greater than the jumping load in limbs. The EN constructs were significantly stronger
in axial loading (failure and yield points) and absorbed significantly greater amounts of energy before
yield and failure. However, there were no significant differences in stiffness between the EN and
cortical allograft constructs, despite the EN constructs being 26-33% stiffer than the cortical allograft
constructs.3 There was no significant difference in stiffness, yield load and energy, and ultimate load
and energy at failure with preservation or resection of the ulna in either constructs.3
A clinical trial followed the biomechanical testing, in which the first generation EN (GEN1) and cortical
allograft were compared in a prospective cohort study of 20 dogs with OSA of the distal radius.1 Limb
function was graded as good to excellent in 70% of the cortical allograft cohort and 80% of the EN
cohort. Complications seen in the EN group included infection (60%), construct failure (40%) and local
recurrence (20%). Infection was graded as mild in 1 dog, moderate in 1 dog and severe in 3 dogs. One
dog with severe infection required amputation. Median time to infection was 61 days. Construct
failures involved screw loosening or fracture in the proximal aspect of the radius (Figure 9). The
increased risk of proximal failure in the EN was hypothesized to be due to the difference in the
modulus of elasticity between stainless steel of the implant and host cortical bone, resulting in
concentration of forces at the proximal bone interface. In 2 dogs, construct failure was considered to
be secondary to severe infection. Construct failure was graded as mild in 2 dogs, moderate in 1 dog
and severe in 1 dog. Surgical revision was performed in 2 dogs in which screws were removed and
replaced. Median time to construct failure was 180 days. Local tumour recurrence occurred in two

20
dogs, both of which had the ulna preserved intraoperatively. Metastatic rate was 60% with a
metastasis free interval of 188 days. Overall median disease free interval was significantly longer in
dogs with surgical infection. Median survival time was 705 days. There were no significantly different
outcomes between the two techniques.1
Figure 9: Construct failure following limb sparing surgery with first
generation metal endoprosthesis. From Liptak et al. (2006).1
Figure 8: Intraoperative photograph and post-operative radiograph of first generation metal endoprosthesis. From
Liptak et al. (2006).1

21
A second generation EN (GEN2) has been developed to combat the high failure rate associated with
GEN1 and has employed significant weight reduction strategies in the radial defect spacer (Figure 10).
The spacer is available in two sizes, to accommodate variations in tumor size and in radius length
(Figure 11). Angle stable bone plates, in which the screws lock into the bone and the plate, have been
added with the hope to reduce the risk of construct failure. Hydroxyapatite (HA), previously used to
promote osseous integration in total-hip arthroplasties, has been added as a coating in the hope to
achieve greater percent bone apposition than uncoated prosthesis surfaces (Figure 10).101 Currently,
GEN2 has not been biomechanically tested nor had clinical outcomes reported in a large scale study.
A single case report describes the use of the GEN2 with locking plate and screws, which developed an
implant-related complication 4 months post-operatively.6 Another single case report describes the
successful use of a custom made tantalum EN in the distal radius (Biomedtrix; Boonton NJ) (Figure
12).2
Figure 10: Photograph of second generation metal endoprosthesis spacer with hydroxyapatite coated ends. Image courtesy of James Farese.

22
1.2.4 Adjuvant therapies
Chemotherapy has been undoubtedly proven to increase survival times of dogs with OSA.18,23,63,66,102-
106 Amputation or limb-sparing surgery alone in dogs with no evidence of metastatic disease, is
associated with a median survival time of 19 weeks and 1 year survival rate of 11.5%.50 Surgery should
be followed by 3 to 6 cycles of either single agent platinum or doxorubicin based chemotherapy
protocol, or an alternating combination of the two.107
A biodegradable implant containing chemotherapy drug cisplatin can be implanted at the site of limb-
sparing surgery to increase the local concentration of chemotherapy, while reducing side effects and
toxicity associated with systemic chemotherapy.108 A prospective study by Withrow et al. (2004)
found that dogs treated with the cisplatin implant were 53.5% less likely to develop local recurrence
Figure 12: Intra-operative photograph of tantalum distal radial endoprosthesis. From
MacDonald et al (2010).2
Figure 11: Second generation metal endoprosthesis with locking limb salvage plate,
a 98-mm and 122-mm spacer and one of the two machine threaded screws for attaching the spacer to the plate. From Venzin et al. (2012).6

23
than dogs that did not receive the implant, although the finding was not statistically significant (P =
0.071).109 Once metastatic disease has been detected, chemotherapy is usually ineffective.110
Pamidronate is an aminobisphosphonate that produces analgesic and anti-resorptive effects by
impeding osteoclast activity and inducing apoptosis. Pamidronate used in conjunction with
carboplatin was shown to have comparable DFI and MST to carboplatin alone, with no additional
unwanted side effects.111
Pulmonary metastatectomy has been shown to increase survival times.112 Case criteria includes
complete remission of the primary tumour, less than 2 radiographically detectable nodules and no
other sites of distant metastasis.

24
2. Aims and Objectives
2.1 Multi-institutional Retrospective Study on Metal Endoprosthesis
The aims of this study are to report the surgical and oncologic outcomes in dogs with distal radial
OSA treated with metal endoprosthesis limb-sparing surgery and adjuvant chemotherapy and to
compare the outcomes between GEN1 and GEN2.
2.2 Evaluation of a Novel Endoprosthesis
The aims of this study are to manufacture a novel EN using three dimensional printing (3DP) and to
assess different size variations of the implant in a cadaver setting.

25
3. Multi-institutional Retrospective Study on Metal Endoprosthesis
This chapter includes the methods, results, discussion and conclusion from a published manuscript
for which the primary author contributed over 90% of authorship. This manuscript can be seen in full
in Appendix 1 or by DOI: http://onlinelibrary.wiley.com/doi/10.1111/vsu.12423/abstract.
3.1 Methods
The study was a multi-institutional retrospective case series approved by the Veterinary Society of
Surgical Oncology (see Appendix 2 for proposal). Medical records of participating institutions were
reviewed for dogs with distal radial OSA that were treated with limb-sparing surgery with a metal
endoprosthesis and adjuvant chemotherapy between 2001 and 2013. Dogs were included if there
was a histologic diagnosis of OSA, no radiographic or computed tomography (CT) evidence of
pulmonary metastasis at the time of surgery and if the dog received a minimum of one scheduled
chemotherapy treatment after limb-sparing surgery.
Data retrieved from the patient record included: signalment, body weight, presenting complaint,
pre-operative lameness evaluation, results of staging tests performed, serum alkaline phosphatase
(SALP) activity on admission, therapy prior to surgery, description of surgery and type of
endoprosthesis used, chemotherapy administered, lameness evaluation after repair, post-operative
surgical complications, metastasis, cause of death, date last reported alive or date lost to follow up.
Case information was collected using a case accrual form filled out by the contributors (Appendix 3).
Lameness was graded using a subjective semi-quantitative grading system based on patient records
as 0 (no lameness), 1 (mild lameness), 2 (moderate weight bearing lameness) or 3 (severe non
weight bearing lameness). A surgical infection was defined as presence one or more draining sinus
tracts at the surgical site and was graded as mild (draining sinus tracts that resolve after oral
antibiotic therapy), moderate (draining sinus tracts that respond to oral antibiotics but did not

26
resolve) or severe (draining sinus tracts that are refractory to oral antibiotic therapy and require
surgical intervention). Surgical implant-related complications were defined as loosening or breakage
of bone screws, plate or endoprosthesis and/or fracture of the radius or metacarpal bones and were
graded as mild (did not require surgical revision), moderate (required minor surgical revision, such as
removing, tightening, or replacing loosened bone screws) or severe (requiring major surgical
revision, such as bone plate replacement or limb amputation). Minor complications were defined as
mild implant-related complications or mild/moderate infections that were treated conservatively
and major complications were defined as local recurrence or complications that required
amputation or revision surgery.
Days to complication was defined as the number of days from limb-sparing surgery to evidence in
the patient record of infection, implant complication or local recurrence. Metastasis free interval
(MFI) was defined as the number of days from limb-sparing surgery to documentation of metastatic
disease in the patient record. Survival time (ST) was defined as the number of days from limb-
sparing surgery to death or euthanasia as noted in patient record. Cases were right censored (when
the value of measurement is only partially known) on the date of case accrual if they were still alive,
on the date of death if from other causes, or on the last date of followup if lost to followup before
case accrual.
3.1.1 Statistical analysis
Data were examined for normality using Shapiro-Wilk tests and by inspecting histograms of the data.
All variables were described and summarized by frequencies and 95% confidence interval (CI) for
categorical variables and interquartile range (IQR) for numeric values. The data were categorized by
explanatory variables in 3 different ways for exploration: categorized by generation implant (GEN1,
GEN2), implant-related complication (presence, absence), and local recurrence (presence, absence).
Univariate analysis was performed to explore associations between explanatory categories and

27
categorical outcomes using Fisher’s exact test (for cell counts < 5) or Pearson Chi-Square tests (χ2;
for cell counts > 5). Continuous outcomes were compared across explanatory categories using
Student’s t-tests where normally distributed (age, weight, pre-operative ALP) or Mann-Whitney U-
test where not normally distributed (severity of lameness or complication). Kaplan-Meier (KM)
product limit estimates and 95% CI were calculated for days to complication, days to local
recurrence, MFI and ST. A log rank test was used to compare KM functions stratified on GEN1 and
GEN2, with/without elevated preoperative ALP (> 131 IU/L), with/without infection, with/without
implant-related complication, and with/without local recurrence. KM estimates and log rank test
were performed for days to implant-related complication, stratified on locking/non-locking screws. A
P<.05 was considered significant and post-hoc power analysis was performed for all non-significant
results. Data were analyzed using IBM SPSS Statistics v22.
3.2 Results
3.2.1 Signalment
Forty-five dogs from 7 institutions met the inclusion criteria. Surgery was performed by 15 board
certified veterinary surgeons. Breeds were mixed breed (11), Doberman (5), Great Dane (4), Labrador
Retriever (4), Great Pyrenees (3), Greyhound (2), Irish Wolfhound (2), Rottweiler (3), Golden Retriever
(2), Bull Mastiff (2) and 1 each of Old English Sheepdog, Bernese Mountain Dog, Malamute, Akita,
Leonberger, Irish Setter and Australian Shepherd. There were 27 castrated males, 14 spayed females,
3 entire males and 1 entire female. Median age at surgery was 7.5 years (range 2-13.3, IQR 3). Median
body weight was 45.5 kg (range 24.1-71, IQR 15.7).
28
3.2.2 Presentation
All dogs presented with forelimb lameness, with a median duration of 2 weeks lameness (range 5 days
to 12 weeks, IQR 3 weeks). The left radius was affected in 28 dogs, the right in 17 dogs. Four dogs had
pathologic fracture of the radius at presentation. Preoperative radiographic or CT screening for
thoracic metastasis was performed in all dogs which were staged clear for detectable pulmonary
metastasis, as dictated by inclusion criteria. Whole body scintigraphy was performed in 27 dogs (60%)
to screen for bone metastasis which was negative in all dogs. Pre-operative serum ALP activity was
elevated (reference interval 20-131 IU/L) in 13 dogs (28%; mean 119.7, range 20-479, IQR 101). There
were no statistically significant differences in pre-operative data between the GEN1 and GEN2 groups.
3.2.3 Treatment
The GEN1 was used in 28 dogs (62%) and GEN2 was used in 17 dogs (38%). The proximal margin was
clear of OSA on histologic examination in 43 dogs and unclear in 2 dogs. Surgery was performed
without recorded complication in all dogs. The ulna was preserved in 42% of dogs (14 GEN1, 3 GEN2).
Plate bending angle at the radiocarpal joint was recorded in 23 dogs as no bending (n=10), and
between 6° and 15° (IQR 2°, n=13). The number of screws placed proximal to the metal spacer ranged
from 4 to 8 (median 6, IQR 2), the number of screws placed distal to the metal spacer ranged from 6
to 9 (median 8, IQR 3). The mean percentage of radius replaced was 57% (range 42-65%, IQR 8%), and
mean percentage of metacarpal 3 covered by the plate was 82% (range 60-94%, IQR 16%). There was
no significant difference in the above surgical data between GEN1 and GEN2 (Table 5). Locking screws
(9 dogs) and the shorter 98mm EN spacer (3 dogs) were used only in the GEN2 group, reflecting
differences in the implant.

29
Outcome Overall (n=45) GEN1 (n=28) GEN2 (n=17) P-value Post-hoc
power
Infection 35 (78%) 20 (71%) 15 (88%) .19 (χ2) 0.23
Implant-related complication 16 (36%) 9 (32%) 7 (41%) .54 (χ2) 0.09
Amputation 9 (20%) 4 (14%) 5 (29%) .22 (χ2) 0.24
Days to infection 129 (59-199) 131([11-251) 123 (4-242) .71 (log-rank) 0.03
Days to implant-related complication 169 (119-219) 169 (89-249) 118 (101-135) .09 (log-rank) 0.71
Days to amputation 125 (18-232) 457 (0-1099) 125 (31-219) .18 (log-rank) 0.99
Table 5: Frequency of, and Estimated Median (95% Confidence Intervals) Days to, Surgical Outcomes of Dogs Receiving First-(GEN1) and Second-Generation (GEN2) Endoprostheses
All dogs had post-operative chemotherapy, as dictated by inclusion criteria. The most frequent post-
operative protocols included a platinum agent (carboplatin or cisplatin) and doxorubicin as a single
agent or in combination. Open cell polylactic acid polymer sponges impregnated with cisplatin (OPLA-
Pt) were used in 11 dogs (10 GEN1, 1 GEN2). The OPLA-Pt was used in 2/4 cases that presented with
pathologic fracture.
3.2.4 Surgical outcomes
Surgical complications occurred in 43 dogs (96%) with minor complications in 14 dogs (31%) and major
in 29 dogs (64%; Table 5). There were no significant differences in the severity or frequency of surgical
complication or days to complication between GEN1 or GEN2. Infections were mild (n=16), moderate
(n=10) or severe (n=9). The most frequent isolates were Staphylococcus spp. (n=11), Pseudomonas
spp. (n=5), Escherichia coli (n=4) and Enterobacter spp. (n=4). Three of the cultures were multi-drug
resistant. Implant-related complications were mild (n=4), moderate (n=4) or severe (n=8). Implant-
related complications included screw loosening (n=8) or screw breakage (n=8), plate fracture (n=3)
and fracture to the radius (n=1) or metacarpal bone 3 (n=1). Treatment for implant-related
complication was conservative (n=5), revision surgery (n=9) or amputation (n=2). The KM-estimated
survival functions for days to implant-related complication, stratified on locking or non-locking screws,
were not significantly different (P = .08).

30
Local recurrence occurred in the radius (n=5), distal ulna (n=4), radial carpal bone (n=1), and
surrounding soft tissues (n=1). Two of the 11 dogs treated with OPLA-Pt developed local recurrence.
This included 1 dog presenting with pathologic fracture. Only infection was associated with local
recurrence (P=.01, Table 6).
Outcome (n) Categorisation n P-value
Implant-related complication (16)
Ulna preserved Ulna not preserved
25 16
0.75 (χ2)
Non locking screws Locking screws
18 9
0.33 (FET)
No plate bending at radiocarpal joint Plate bending at radiocarpal joint
12 11
0.45 (FET)
41-55% radius replaced 56-70% radius replaced
12 16
0.09 (FET)
60-79% metacarpal covered 80-99% metacarpal covered
6 16
0.27 (FET)
Infection No infection
10 35
0.24 (χ2)
Local recurrence (11)
Pathological fracture No pathological fracture
4 41
0.69 (FET)
Ulna preserved Ulna not preserved
25 16
0.94 (χ2)
41-55% radius replaced 56-70% radius replaced
12 16
0.52 (FET)
OPLA-Pt use No OPLA-Pt
10 32
0.61 (χ2)
Histologically incomplete margins Histologically complete margins
2 36
0.39 (χ2)
Infection No infection
10 35
0.01 (FET)
† Pearson χ2 test; FET Fisher’s exact test; n = number of dogs
Table 6: Categorical Explanatory Variables Tested Univariate Association with Implant-Related Complication and Local Recurrence.
There were no significant differences in post-operative lameness scores between dogs receiving GEN1
or GEN2 at any time points (Table 7). Amputation was performed in 9 dogs because of local recurrence
in 4 dogs, severe infection in 3 and implant-related complication in 2.

31
None (n) Mild (n) Moderate (n) Severe (n) Total (n)
Post-op GEN1 GEN2 GEN1 GEN2 GEN1 GEN2 GEN1 GEN2 GEN1 GEN2
0-4 weeks 0 2 17 9 5 4 2 0 24 15
1-6 months 1 2 6 5 8 5 5 4 20 16
> 6 months 0 0 2 2 1 1 2 2 5 5
Table 7: Post-operative Lameness for Dogs Receiving First-Generation (GEN1) and Second-Generation (GEN2) Endoprostheses
3.2.5 Oncologic outcomes
Survival analysis included 34 dogs with complete endpoints of euthanasia for tumour- or procedure
related disease (Table 8). This included 4 dogs with infection, 2 with local recurrence, 28 with
metastatic disease, and 4 dogs that died from tumour-related disease (pleural effusion presumed
secondary to pulmonary metastasis). Seven cases were right censored with 2 alive at study accrual
and 5 dead from other causes as noted in the medical record (lymphoma, gastric dilation and
volvulus, neurologic disease, cardiac disease and renal disease). No cases were lost to follow up.
Metastatic disease was confirmed in 27 dogs and suspected in 3. Location of metastasis included
pulmonary (n=14), bone (n=5), pulmonary and bone (n=4), pulmonary and other (n=2), lymph node
(n=2). Suspected hepatic (n=2) and brain (n=1) metastases were not confirmed with histology.
Survival time ranged from 34 days to 6.1 years with an estimated median of 289 days (95% CI 207-
371). The 1-, 2-, and 3-year survival was 33%, 16%, and 4% respectively. The KM-estimated functions
for survival were not different when stratified on with/without elevated pre-operative ALP (P=.12),
with/without infection (P=.81) or with/without local recurrence (P=.46). The estimated KM functions
for survival time, stratified on with/without implant-related complication, were significantly
different (P=.004). Further stratification on GEN1/GEN2 (4 functions) was also significant (P=.04).

32
Outcome Overall (n=45)
GEN1 (n=28)
GEN2 (n=17)
P-value Post-hoc
power
Local recurrence 11 (24%) 7 (25%) 4 (24%) .91 (χ2) 0.03
Metastasis 30 (67%) 19 (68%) 11 (65%) .83 (χ2) 0.04
Days to local recurrence 125 (40-210) 99 (0-226) 125 (41-209) .35 (log-rank) 0.15
Metastasis free interval (days)
188 (126-250) 212 (168-256) 102 (49-155) .06 (log-rank) 0.68
Survival time (days) 289 (207-371) 294 (183-405) 255 (222-
288) .71 (log-rank) 0.05
Table 8: Frequency of, and Estimated Median (95% Confidence Intervals) Days to, Oncologic Outcomes for Dogs Receiving First-Generation (GEN1) and Second-Generation (GEN2) Endoprostheses
3.3 Discussion
The use of GEN2 did not result in any significant differences in the frequency of surgical complications
or days to complications, contrary to our hypothesis. Metastasis frequency, MFI, or survival time were
not significantly different between dogs receiving either endoprostheses.
The frequency of implant-related complications (32% GEN1, 41% GEN2) is similar to that reported
previously. Liptak and others reported a 40% frequency of implant-related complication for GEN1.1 In
that case series, construct failure was due to screw loosening or breakage in the proximal aspect of
the radius, theorised to be due to a mismatch in modulus of elasticity or poor load sharing between
host cortical bone and metal endoprosthesis.1 In the present study, implant failure varied for the 2
endoprostheses, with failure at both proximal and the distal aspects of the construct. Angle stable
bone plates and lighter weight spacer are features of the GEN2 designed to reduce construct failure.
The present study did not show a difference in the frequency of implant-related complications
between GEN1 and GEN2, or between locking or non-locking screws. These findings, combined with a
report of construct failure with a GEN2 locking system,6 suggest that implant failure is not averted by
the use of locking screws. In the present study, the presence of infection was not associated with
implant-related complication, a finding consistent with reports on the GEN1.1 The percentage of radius

33
replaced or percentage of metacarpus covered by plate was not significantly associated with implant-
related complications. However, the most dogs had the larger spacer implanted despite the GEN2
spacer being available in 2 lengths (98mm and 122mm) and the percentage of radius replaced was
similar for GEN1 and GEN2 (median 57% for both). Hydroxyapatite coating for osseous integration has
been proposed to improve load transfer and decrease stress concentration over time but its impact
on implant-related complications could not be evaluated in this study.
The 78% frequency of infection in the present study was higher than previously reported. A case series
reported infection in 5/10 dogs with GEN1.1 In that study 4/5 infections were moderate or severe,
whereas almost half of the infections in the present study were graded as mild. Regardless, the
frequency of surgical infection with limb-sparing remains unacceptably high. Implicated factors
include poor soft tissue coverage in this area, extensive soft tissue resection, a large inert implant, and
immunosuppression from neoplasia and chemotherapy which are all related to limb-sparing surgery
regardless of the type of implant used.
Post-operative lameness within 4 weeks of surgery was subjectively graded as none/mild in 33 dogs
(73%). This is comparable to previous reports for both allograft and endoprosthesis (69-75% graded
good/excellent).1,85,89 Lameness scores did not differ significantly between GEN1 and GEN2 at any
post-operative time point, although assessment is clearly limited by data quality. Objective
measurements would be required for more definitive comparison. Overall survival for limb-sparing
was 76%, comparable to 85% reported for GEN1.1
Local recurrence (24%) fell within the 11-28% range previously reported for limb-sparing in the distal
radius.1,5,76,85,92 Pathologic fracture is considered a contraindication for limb-sparing because of
tumour seeding into adjacent soft tissue. Only 1/4 dogs that presented with pathologic fracture
developed local recurrence despite perceived risks of local recurrence. Local recurrence occurred in
the proximal radius in 5/11 cases, despite all having clean margins on post-operative histology. Two
dogs had histologic evidence of incomplete proximal margins but only 1 dog developed local

34
recurrence (ulna). Accurate determination of local tumour extent is critical to determine the level for
radial osteotomy. Magnetic resonance imaging (MRI) with T1-weighted non-contrast images is the
most accurate method to detect the extent of intramedullary OSA but MRI does overestimate tumour
length compared to radiographs, nuclear scintigraphy and CT.58,59,61 Local recurrence in the ulna
occurred in 4/11 cases but distal ulna preservation was not significantly associated with increased
local recurrence in univariate analysis. Regardless, the authors recommend en-bloc resection of the
radius and ulna to be consistent with oncologic principles, to remove the distal ulna as a potential
local recurrence site, and to decrease surgical time. In addition, there is no biomechanical advantage
to ulna preservation when using GEN1.3 Use of OPLA-Pt in cortical allograft limb-sparing surgery
showed dogs treated with OPLA-Pt were 54% less likely to develop local recurrence than dogs without
OPLA-Pt.109 In the present study, there was no association between treatment with OLPA-Pt and local
recurrence (22% with OPLA-Pt, 39% without).
There were no significant differences in metastasis frequency, median MFI and survival times for dogs
receiving GEN1 and GEN2 and chemotherapy, the overall findings were similar to that reported for
amputation and chemotherapy.18,90,103,104,113,114 Different adjuvant chemotherapy protocols across
multi-institutions were used in the present study but no chemotherapy protocol appears superior for
OSA.1
Dogs with implant-related complication had significantly increased ST (482 days) compared to dogs
without implant-related complication (201 days). This relationship is difficult to understand but it is
unlikely that increased ST allowed capture of more implant-related complications given that the
median days to implant-related complication (169 days) were shorter than the median ST (289 days).
This finding is reported previously for GEN1, where dogs without construct failure were 17 times more
likely to die than dogs with construct failure.1
Post-operative infection is reported previously as positively associated with decreased local
recurrence frequency,109 and increased MFI and ST.65,76,95,115 In the present study, infection was not

35
significantly associated with either implant-related complication or survival time. However, univariate
analysis showed that infection significantly associated with a lower frequency of local recurrence. The
relationship between infection and improved outcome is not fully understood but is thought to be
related to inflammation and immunologic reactions.1,76
Elevated pre-operative SALP activity is negatively associated with ST for dogs with OSA. 64,65,70,72
However, the present study showed no separation of the survival functions for dogs with and without
elevated SALP. Recent work suggests that the negative association between pre-treatment SALP
activity and outcome may simply reflect greater initial tumour burden.73
Limitations of the present study include the retrospective data collection and the reliance on
documentation to make subjective assessment of lameness and infection. Infection was not always
confirmed by bacterial culture and categorization of infection did not use the standardised
classification for surgical site infection.116 Days to implant-related complication, amputation and MFI
were the only analyses with appropriate statistical power. For the other analyses, depending on the
examined variable, between 252 and 39,295 dogs would be required to achieve a power of 85%, and
thus, type II error is high. Multiple institutions were retrospectively involved, which creates biases in
surgical management (variations in technique, pre and post-operative management). Frequencies of
complications, local recurrence and metastasis may be underestimated as complete examination and
follow up was not consistent.
3.4 Conclusion
This study showed no significant difference in case (surgical or oncologic) outcomes between dogs
receiving GEN1 and GEN2 endoprosthesis for limb-sparing surgery of the distal radius. The frequency
of complications, including infection and those implant-related, remains unacceptably high for both
generations of endoprosthesis. Oncologic outcomes of dogs receiving either generation

36
endoprosthesis remain similar to amputation and other limb-sparing techniques that are combined
with adjuvant curative intent chemotherapy.18,90,103,104,113,114 Further refinement of the endoprosthesis
or re-evaluation of the surgical technique for implantation of the endoprosthesis is indicated.

37
4. Evaluation of a Novel Endoprosthesis
4.1 Background
The finite element (FE) method has been applied to biological tissues for numerous studies in human
orthopaedics. It involves the use of mesh generation techniques to divide a complex problem into
multiple small elements. FE has been used previously to investigate the canine antebrachium.117
Investigators at Colorado State University developed and validated a FE model of the canine forelimb
to aid in the evaluation of metal EN for limb-sparing surgery.7,118 The aims of the project were to
evaluate GEN2 and design a novel EN using the FE model.7
4.1.1 Evaluation of second generation endoprosthesis
Efficiency of the GEN2 implant was evaluated by applying physiological loads equivalent to the forces
experienced during canine trot to the GEN2 implant in the FE model of the canine forelimb (Figure
13). The geometry of GEN2 was obtained from engineering drawings and direct measurement of the
implants. The dynamic compression plate (DCP) was implanted with a 10 degree angulation at the
radio-carpal junction. The radius was resected by 50% from distal end by deleting corresponding
elements from the FE model. The construct was tested with cortical screws and DCP (coefficient of
friction value of 0.25 at plate and screw heads) and with locking screws and plate (tie-construct
between screw heads and plate to simulate locking mechanism). All models were loaded to 110% body
weight in axial compression (equating to 400N for a 38kg dog).
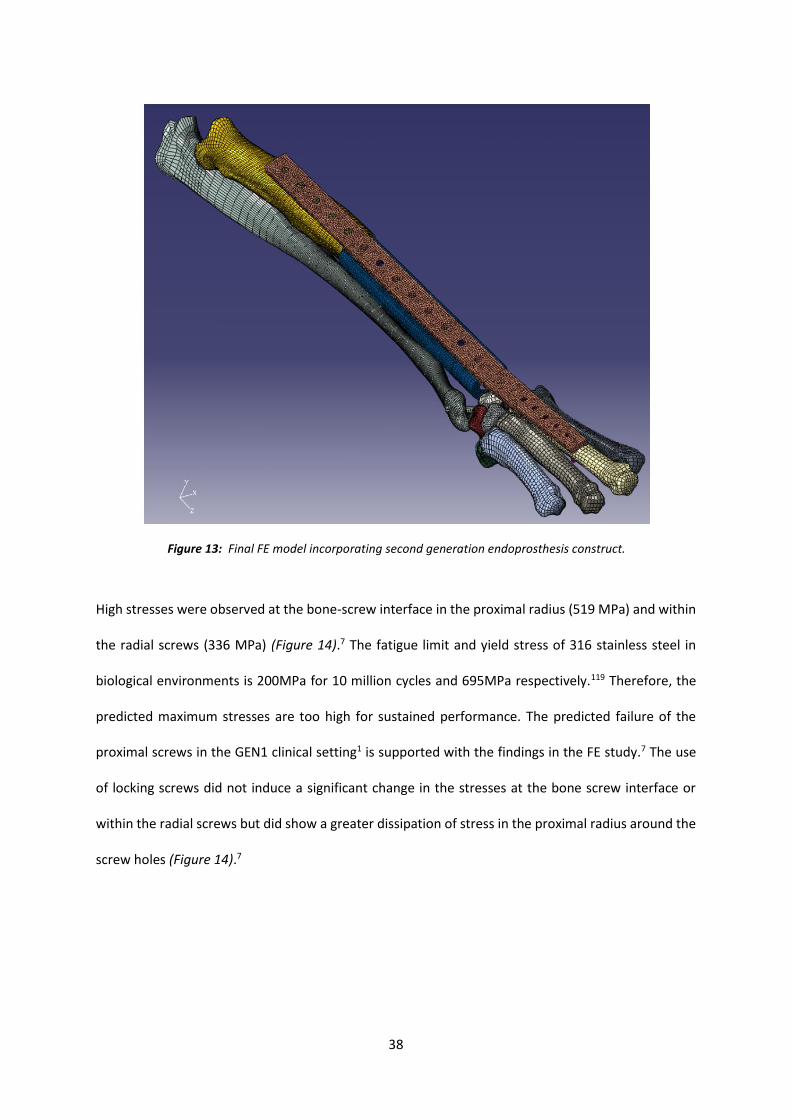
38
High stresses were observed at the bone-screw interface in the proximal radius (519 MPa) and within
the radial screws (336 MPa) (Figure 14).7 The fatigue limit and yield stress of 316 stainless steel in
biological environments is 200MPa for 10 million cycles and 695MPa respectively.119 Therefore, the
predicted maximum stresses are too high for sustained performance. The predicted failure of the
proximal screws in the GEN1 clinical setting1 is supported with the findings in the FE study.7 The use
of locking screws did not induce a significant change in the stresses at the bone screw interface or
within the radial screws but did show a greater dissipation of stress in the proximal radius around the
screw holes (Figure 14).7
Figure 13: Final FE model incorporating second generation endoprosthesis construct.

39
4.1.2 Novel endoprosthesis design
The unfavorable results of FE modelling-based evaluation of GEN2 (Section 4.1.1), and the high
number of implant-related complications seen in the GEN1 clinical trials,1 emphasized the need for an
engineering specific approach to design a novel limb-sparing EN. High stresses in the radial screws
were due to off-axis loading of the construct coupled with high shear stresses of the non-locking plate
design.7 The implant was designed to be placed in-line with the loading axis of the radius to ensure
equal load distribution. A modular design was chosen to accommodate breed size variations. The
implant consisted of three independent parts; proximal endoprosthesis component (PEC), mid-
diaphyseal endoprosthesis component (MEC) and distal endoprosthesis component (DEC). All
components were designed with an elliptical profile to mimic the natural shape of the radius. An intra-
Figure 14: Comparison of von Mises stress predictions between the non-locking (blue) and locking (red) constructs. Graph from Shetye (2010).7
40
operative apparatus (jig) was designed to allow correct alignment between the proximal radius and
the carpus following tumour resection. The novel implant was designed with locking screws to reduce
shear stresses within the radial screws.
The PEC consisted of an intramedullary stem and a 180 degree wrap around plate with locking screws
at 45 degrees to the sagittal plane of the radius. The distal surface of the radius is fully supported by
the PEC, to potentially reduce the bending effects on radial screws (Figure 15). The MEC was designed
to be simple and to provide the surgeon with the ability to match the EN to the patient limb length
(Figure 16). The DEC component was designed with 6 2.7mm locking screw holes for fixation to the
third metacarpal, and a proximal 3.5mm cortical screw hole for the radial carpal bone. The radio-carpal
junction was created with zero degree bend (Figure 17).
Figure 15: Proximal endoprosthesis component (PEC). Image from Shetye (2010).7

41
The novel implant was evaluated in the FE model loaded to 500N. Contact was established between
surfaces of the implant with a coefficient of friction of 0.25, and between the distal radius and the PEC
with a coefficient of friction of 0.1. The changes in the novel implant resulted in a 50% reduction of
the peak von Mises stress within the radial screws compared to the GEN2 implant.7 Removal of the
Figure 16: Mid-diaphyseal endoprosthesis component (MEC). Image from Shetye (2010).7
Figure 17: Distal endoprosthesis component (DEC). Image from Shetye (2010).7

42
intramedullary stem in the FE model resulted in relatively high bending stresses within the radial
screws where they entered the radius, hence the stem plays an integral part in reducing the bending
stresses within the screws. The FE model also showed no mechanical benefit to the addition of ulnar
support. The highest stresses of the novel implant were seen in the 2.7mm locking screws of the distal
metacarpus.7 However, the peak von Mises stress (153MPa) were below the endurance limit of 316L
stainless steel. Based on these results, the novel EN design was approved for further biomechanical
testing, fatigue analysis and clinical trials.
4.2 Three Dimensional Printing of Novel Implant
Three-dimensional printing (3DP) or rapid prototyping involves the fabrication of physical parts based
on a 3D computer-aided design (CAD). The CAD model is sliced into layers to allow stereolithography
where the physical part is fabricated layer by layer using laser fusion of a powder material. Rapid
prototyping has previously been used for surgical planning in the veterinary surgery field.120-124
However, custom made orthopaedic implants using rapid prototyping have not been reported in the
veterinary field. Rapid prototyping was chosen for the evaluation of a novel implant to allow cost
effective and fast model creation during the assessment phase, however, the expectation is that if
found to be suitable, rapid protoyping could be used to manufacture final implants in titanium or
stainless steel.
The Advanced Manufacturing Precinct of the Royal Melbourne Institute of Technology (RMIT) was
approached to manufacture prototypes of the novel implant. Stereolithic models of the implant as
created in the CAD drawings were produced in acrylonitrile butadiene styrene plastic using a 3D
printer. Metal prototypes were 3D printed using 420 Stainless Steel infused with bronze (60% steel
and 40% bronze). Each implant was subsequently testing in a cadaver setting (Section 4.3).

43
The final prototype was manufactured by a human orthopaedic trauma device manufacturer in 316
surgical stainless steel (Austofix; North Plympton, South Australia). An EOS M280 3D printing machine
was used to create the final metal implant from the CAD drawings using 10-70 micron powder. Hand
grinding was used to create the smooth finish. Implants were then placed in a tumbling machine for
24 hours for final polishing. Shot peening was used to avoid the propagation of microcracks from the
surface. Thread milling was used to create holes and threads suitable for locking screws (Austofix;
North Plympton, South Australia).
4.3 Cadaver Implantation Trials
4.3.1 Cadaver Limb Collection
Paired thoracic forelimbs were harvested from 9 skeletally mature dogs euthanized for reasons
unrelated to this study. This included a 9y male neutered Boxer, a 6y female desexed German
Shepherd Dog, a 2y male Rottweiler and 6 skeletally mature female Greyhounds. Each forelimb was
examined and cranial-caudal and medial-lateral radiographs or CT scan were obtained to confirm
skeletal maturity and the absence of gross pathology. Paired limbs were harvested with skin and
musculature intact and sealed in a single plastic bag and frozen at -80°C within 24 hours of euthanasia.
For implantation with novel implant, limbs were thawed in 4°C refrigerator for 24-36 hours.
4.3.2 Cadaver Limb Measurements
A number of Greyhound cadavers were available for testing, however there was some concern that
the original FE model, which was modelled on a 38kg Chesapeake Bay Retriever, would not fit the
Greyhound radii. The fit of the wrap around plate and intramedullary stem of the PEC was the main
concern. The locking nature of the plate and screws allows some elevation from the bone; however

44
the plate should ideally be no further than 2mm from the bone surface.125 As such, five Greyhound
cadaver limbs were chosen for measurement to determine suitability of implantation of the novel EN.
Limbs were measured with a ruler from humero-radial joint to radio-carpal joint and five cadavers
with radial length between 21 and 22cm were chosen for testing. This length of limb was chosen to fit
the novel endoprosthesis. The limbs were placed through CT scanner and standardised measurements
performed (Figure 18 and Table 9).
Cadaver # 1 2 3 4 5
Radial length (mm) 211 216 215 219 217 Metacarpal 3 length (mm) 90.5 92.5 92.3 92.1 94.8 Radial diameter(mm)* 18.7x12.3 19x12.6 16.7x10.2 19x12.3 19.3x12.1 Intramedullary diameter(mm)* 6x4.6 7.2x5.2 6.4x3.8 6.5x4.8 8.2x4.5
*measurement taken 100mm proximal to radiocarpal joint
Table 9: Computed Tomography measurements of five similar sized greyhound cadaver radii
Figure 18: Computed Tomography measurement of greyhound cadaver radii. A: Radial length; B: Metacarpal 3 length; C: Cross section of outer cortex at level of proposed osteotomy (100mm proximal to
radiocarpal joint); D: Cross section of medullary canal at level of proposed osteotomy.

45
4.3.3 Cadaver Implantation with Novel Endoprothesis
Section 4.3.2 highlighted the variation in radius size and shape within and between large breed dogs
and as such, three modifications of the novel EN were produced for cadaver trial implantation.
Prototype 1 and 2 were modified to fit Greyhound radii available for testing; one scaled universally
and one custom scaled. Prototype 3 was the original FE model based on the Chesapeake Bay
Retriever. The same technique was used for each of the cadaver trials.
Technique
A craniolateral skin incision from proximal radius to distal metacarpals was created using a size 15
scalpel blade (Figure 19A). Muscles overlying the cranial radius were transected at insertion and
elevated proximally to expose the cranial aspect of the entire radius and ulna. An oscillating bone saw
was used to perform an osteotomy 100mm proximal to the radiocarpal joint. Ligaments and tendons
attaching the radius and ulna to the carpus were transected using a scalpel blade and the distal radius
and ulna were removed en-bloc (Figure 19B). The proximal radius medullary canal was reamed using
4.5mm drill bits and burrs until the PEC intramedullary stem was able to be introduced (Figure 19C).
The PEC was placed on the cranial aspect of the proximal radius until the abutting segment of PEC was
hard against the radial bone (Figure 19D). The PEC was held in place with K-wire (plastic prototype) or
2.5mm locking screws (Austofix; North Plympton, South Australia) (stainless steele prototype). The
proximal aspect of the radiocarpal bone was flattened with oscillating bone saw or spinal burr to allow
placement of the abutting segment of DEC. The tuberosity of the proximal aspect of metcarpal 3 was
removed using oscillating bone saw or burr to allow the DEC to sit flush against the bone (Figure 19E).
The DEC was placed on the cranial aspect of metacarpal 3 with the abutting segment of DEC hard
against the radiocarpal bone (Figure 19F). The DEC was stabilised with K-wires (plastic prototype) or
3.5mm cortical screw in radiocarpal bone and 2.5mm locking screws in metacarpal 3 (stainless steel
prototype). A locking screw guide (Austofix; North Plympton, South Australia) was used to place all

46
locking screws. Mediolateral and ventrodorsal radiographic projections of the construct were taken
following implantation. Implants were reused on multiple cadaver specimens if required.
Figure 19: Technique for cadaver implantation. A: Craniolateral skin incision; B: Removal of distal radius and ulna en-bloc; C: Ream intramedullary canal; D: Proximal endoprosthesis component; E: Remove
tuberosity of metacarpal 3 with oscillating bone saw; F: Distal endoprosthesis.component

47
Prototype 1
The original FE model was universally scaled to accommodate the radial length of one Greyhound
cadaver. The radial bone diameter at the proposed osteotomy site (100mm from radiocarpal joint)
was measured as 15.6x10mm. Universal scaling of novel EN was performed such that the curved plate
of PEC would closely match the chosen cadaver (Figure 20). The final CAD measurements of the PEC
proximal plate were 16.9x13.3mm. The MEC was elongated to 80.1mm in length to accommodate the
desired 100mm resection of radius. Plastic and stainless steel models were manufactured via rapid
prototyping (Figure 21).
Prototype 1 was implanted into the Greyhound cadaver. Surgical technique was defined (Appendix 4).
The proposed osteotomy site was 100mm proximal to the radio-carpal joint. The ulna was removed
en-bloc with the radius. A burr was required to widen the medually canal of the radius and allow
placement of the intramedullary stem of PEC; a custom made reamer or broach may need to be
manufactured for clinical trials. The distal component resulted in metacarpal coverage of
approximately 50% (Figure 22). Limitations of prototype 1 included less than optimal metacarpal 3
coverage. The universal scaling of the prototype to fit the proportionally smaller radial diameter of
the greyhound resulted in a short endoprosthesis. This led to the production of a second prototype
model.
Figure 20: Prototype 1 CAD with scaling measurements.
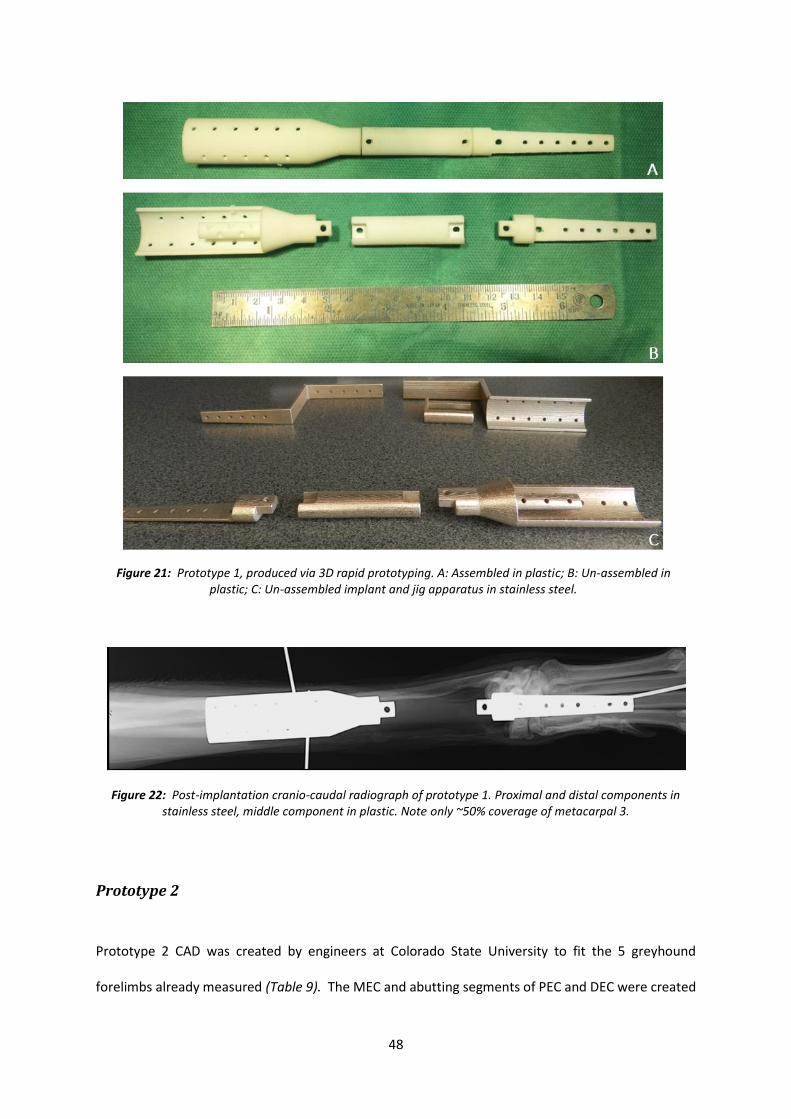
48
Prototype 2
Prototype 2 CAD was created by engineers at Colorado State University to fit the 5 greyhound
forelimbs already measured (Table 9). The MEC and abutting segments of PEC and DEC were created
Figure 21: Prototype 1, produced via 3D rapid prototyping. A: Assembled in plastic; B: Un-assembled in plastic; C: Un-assembled implant and jig apparatus in stainless steel.
Figure 22: Post-implantation cranio-caudal radiograph of prototype 1. Proximal and distal components in stainless steel, middle component in plastic. Note only ~50% coverage of metacarpal 3.

49
to span the desired 100mm defect. The diameter of PEC plate was created to allow placement on the
largest radial diameter (19.3 x 12.6mm) and the stem created to allow placement in the smallest
medullary canal (6.0 x 3.9mm). The median metacarpal 3 length was 92mm. The DEC was created with
a length to cover approximately 80% of metacarpal 3 (74mm overlying metacarpal 3). The prototype
was manufactured in plastic by rapid prototyping (Figure 23). The model was implanted onto 1 of the
5 greyhound cadaver limbs. The distal component resulted in approximately 90% metacarpal
coverage. However, the portion of distal component to abut onto the cut radio-carpal bone was
deemed to be too narrow to adequately share load (Figure 24). This led to production of a third
prototype model.
Figure 23: Prototype 2, produced via 3D rapid prototyping. A: Assembled in plastic, cranial view; B: Assembled in plastic, caudal view; C: Unassembled in plastic.

50
Final prototype
Prototype 3 is a model of the original FE design. Prototype 1 and 2 highlighted the large variability in
bony anatomy between breeds and the difficulties associated with scaling the FE model. The long and
narrow bones of the Greyhound were subjectively different to that seen in Retriever breeds. Any
further refinement of the implant to allow fit the greyhound cadaver limbs would result in a
significantly different EN to that tested in the FE model. The decision was made to source cadaver
forelimbs from medium breed dogs that closely mimicked that seen in the FE model. Three large breed
(Boxer, German Shepherd, Rottweiler) cadavers that were euthanized for reasons not related to this
study were collected and stored as per Section 4.3.1.
The final prototype was manufactured by in 316L stainless steel (Austofix; North Plympton, South
Australia) (Figure 25). 2.5mm locking screw profiles were used in all holes expecting the radiocarpal
bone screw hole and joining holes between components. 3.5mm smooth holes were used at the
radiocarpal bone screw hole (to accommodate 3.5mm cortical screw) and 4.0mm smooth holes at the
junctions between endoprosthesis components (to accommodate 4.0mm bolt). Locking screws and
locking guide were provided by the manufacturer of the stainless steel prototype (Austofix; North
Plympton, South Australia).
Figure 24: Prototype 2 distal component to abut on cut surface of radiocarpal bone.

51
Prototype 3 was implanted into 4 cadaver radii; one of the original Greyhound cadavers, and the three
large breed cadavers collected specifically for prototype 3. Subjectively, prototype 3 fit well in the
Boxer and German Shepherd (Figure 26). Minimal reaming was required for placement of PEC and the
curved plate surface was less than 2mm from the bone surface. Over 60% of metacarpal 3 was covered
by the DEC plate (Figure 27). The Greyhound cadaver again highlighted breed differences; less than
50% of metacarpal 3 was covered by the DEC plate and the marked procurvatum of the proximal radius
made placement of the PEC difficult and a gap of greater than 2mm at the proximal aspect of the
Figure 25: Final novel endoprosthesis in 316L stainless steel. A: Cranial view; B: Lateral view; C: Caudal view with locking guide and 2.5mm locking screw.

52
curved plate (Figure 28). The Rottweiler cadaver had a short radius compared to the other 3 breeds,
and placement of PEC was impossible due to the natural flare seen in the proximal radius (Figure 29).
Figure 26: Final novel endoprosthesis. A: Boxer construct; B: Boxer - Proximal curved plate against the radial bone; C: Boxer - Locking guide in distal endoprosthesis component; D: German Shepherd construct.

53
Figure 27: Cranio-caudal and medio-lateral radiographs of final prototype construct. A: Boxer; B: German Shepherd. The final prototype is appropriately sized and shaped for these forelimbs.

54
4.4 Future Work
The next step for novel EN investigation is testing of biomechanical properties. The proposed testing
schedule would include photoelastic strain testing to determine areas of high strain and allow
appropriate placement of strain gauges for strain gauge testing in axial compression. Biomechanical
properties such as construct stiffness, yield load and ultimate load to failure can be calculated from
axial compression testing. These findings can be used to predict failure mechanisms and compare in
vitro findings with the FE model predictions.
Figure 28: Cranio-caudal and medio-lateral radiographs of final prototype in Greyhound. The
prototype is too short for this forelimb.
Figure 29: Cranial view photograph of proximal radius and final prototype PEC in Rottweiler. The
prototype is too long for this forelimb.

55
4.4.1 Photoelastic Strain Testing
Photoelasticity is an experimental technique used to determine stress distribution in a material. The
method is based on birefringence, a property of certain transparent materials where a ray of light
passing through the material experiences 2 refractive indices. This change in index of refraction is a
function of the resulting strain.126 When photoelastic materials are observed under crossed polarized
light a series of continuous coloured bands (‘fringes’) are seen (Figure 30). Fringes appear because
the material has become optically anisotropic under loading. When there is uniform surface strain
there are no fringes. By bonding a photoelastic plastic to implants and bones, the material
undergoes strains similar to that of the underlying material being tested.127
Strains from photoelastic coating have been found to correlate well with strain gauge
measurement.128,129 Photoelastic coating has been used for human orthopaedic research to assess
the general distribution of strains in a loaded specimen.130-132 It has also been used to determine
best site for placement of strain gauges.133
Figure 30: Photoelastic strain testing. Photograph credit: University of Rhode Island.

56
Materials and Methods
Paired thoracic forelimbs are harvested from skeletally mature dogs euthanized for reasons unrelated
to this study. Radiographs are performed to ensure the distal forelimb is free from orthopaedic
disease. Paired limbs are harvested with skin and musculature intact and sealed in a single plastic bag
and frozen at -80°C within 24 hours of euthanasia. Limbs are thawed in 4°C refrigerator for 24-36 hours
prior to testing. All soft tissues excluding intrinsic tendons and ligaments for radiocarpal, carpal and
carpometacarpal stability are stripped from the limb. Novel EN prototype is implanted into each
cadaver limb following standardised surgical procedure immediately prior to testing. The
humerus/elbow and metacarpal bones are secured into custom made test fittings with dental plaster,
ensuring that the plaster is distal enough to grip the proximal radius, while still allowing at least 3cm
of normal radius above the proximal extent of the endoprosthesis and ensuring the distal quarter of
the metacarpal bones are included in the potting mixture.
Cleaned bones are stripped of periosteum, towel dried then superficially defatted with gauze soaked
in acetone. The bones and implant are coated in a thin layer of reflective adhesive (PC-1 Bipax
Cement: Micro-measurements; Raleigh, North Carolina, USA) and left to harden overnight.
Photoelastic plastic coating (PL-8 Photoelastic plastic: Micro-measurements; Raleigh, North Carolina,
USA) is first cast as a 2mm-thin sheet using polytetrafluoroethylene-coated thermostatically
controlled casting plate (Model 012-1H; Micro-measurements; Raleigh, North Carolina, USA). The
amount of plastic required can be calculated according to size and thickness of sheet to be cast using
the following equation:
W = P x A x t
W = amount of resin in grams
P = plastic density [1.13 (10-3)g/mm3]
A = area of sheet to be cast
T = desired thickness [2mm]

57
Resin and hardener are warmed to 32-35°C and then mixed slowly using circular motion to avoid
introduction of air bubbles. The photoelastic plastic is mixed for 30 minutes until it reaches pouring
temperature 52-55°C before pouring onto previously heated casting plate. The plastic coating is left
for 1.5-2 hours until it reaches required moulding consistency. The coating is cut to size then
moulded to fit the dorsal and lateral aspect of each cadaver construct. Fine wire is tied around each
end of the construct to hold coating in place while it is left to harden overnight. Photoelastic moulds
are adhered to constructs using aluminium impregnanted reflective cement adhesive (PC-1 Bipax
Cement: Micro-measurements; Wendell, North Carolina, USA). Cement is left to set for 12 hours
prior to testing. Constructs with photoelastic coating were viewed through a polarising filter to
identify fringes that may have been introduced during preparation.
Constructs with photoelastic moulds are then loaded in a Materials Testing System and axially
loaded. The fringes are recorded by digital camera at each load interval (0, 100N, 200N, 300N, 500N,
1000N, 1500N and 2000N) with only the light from the polariscope illuminating the surface.
4.4.2 Testing in Axial Compression
Photoelastic strain testing (Section 4.1.1) will highlight areas of high strain within the construct.
Multiple 350-Ω strain gauge rosettes (Micro-measurements; Raleigh, North Carolina, USA) are
implanted on each area of high strain. Briefly, the strain gauges are prepared in the following way:
periosteum removed from bone and bone swabbed with alcohol, exposed bone and back of gauge
covered with thin layer of adhesive and held in place for 2 minutes, lead wires are connected to
gauge solder tabs. The wires are connected to a signal conditioning amplifier (2120A Micro-
measurements; Raleigh, North Carolina, USA). Constructs are loaded in a Materials Testing System
for axial loading (Figure 31). Strain gauge measurement should be calibrated to zero before the
construct is axially loaded. Materials Testing System is ramped to failure in axial compression at a
rate of 300 N/s until failure of limb or implant. Force (N) and displacement (mm) data are acquired

58
at 100 Hz to produce force-displacement curve. The following variables can be derived from the
force-displacement curve: construct stiffness (N/mm), yield load (N), ultimate load (N), yield energy
absorbed (Nmm), ultimate energy absorbed (Nmm). Strain gauge measurements at each load
interval can be compared to FE model predictions.
4.5 Discussion
This chapter has investigated the clinical suitability of the novel EN as proposed by a collaborative
team at Colorado State University. Rapid prototyping was successfully employed to create plastic
models and stainless steel EN implant. The novel EN was successfully implanted into cadaver
forelimbs of similar size to the Retriever that the EN was modelled on. However, the novel EN was
not suitable for implantation into all dogs which highlights the concerns of creating a modular
implant that fits the majority of patients.
The novel EN has been designed to improve biomechanical performance compared to the GEN1 and
GEN2 metal EN currently available. The major contributing factor for failure in GEN2 is increased
Figure 31: Example of Materials Testing Machine and strain gauge testing.10

59
stress within the proximal radius screws.7 The main design change in the novel EN is the addition of
an intramedullary stem and 180 degree wrap around of the PEC which aligns the loading axis of the
implant with the radius. The stem and wrap around plate have been successfully manufactured in
surgical stainless steel using rapid prototyping and the use of a locking guide allowed accurate
placement of the locking screws through the intramedullary stem. There was some difficulty
associated with placement of the PEC and intramedullary stem during cadaver implantation. The
large variation in medullary canal size, and the natural procurvatum of the radius did not allow
placement of the stem without a moderate amount of medullary canal reaming. This was obtained
with drill and burr attachments during cadaver testing, however, a size matched reamer will need to
be produced for the product if it progresses to clinical trials. The large variation in medullary size and
shape between breeds is a concern for the PEC of the novel EN (Figure 32). If the intramedullary
stem of PEC was removed or shortened, the implant would be more likely to fit a variety of radii and
would remove the need for special equipment and additional surgical time associated with reaming.
However, removal of the stem in the FE model resulted in relatively high bending stresses (167.6
MPa) within the radial screws as they entered the radius, hence, then stem is an integral part of the
novel EN design.7
The novel EN has been proposed as a modular implant, with small, medium and large components
available as an off the shelf implant. Cadaver implantation trials highlighted the large variation seen
with and between breeds. Goals of locking plate and pancarpal arthrodesis surgery suggest that we
should not exceed more than 2mm of space between bone surface and locking plate and that at
least 50% of metacarpal 3 should be covered by the plate, with smaller risks of metacarpal fracture
associated with longer metacarpal coverage.125,134 Modular implants, while convenient, are unlikely
to meet these criteria in every patient and patient selection will be rigorous. The implant could be
designed in multiple size and shape variations, for example small/medium/large,
narrow/normal/wide, to accommodate the different radii morphology. However, this creates the
requirement for a large implant inventory and additional costs associated with this.

60
An alternative proposal is to provide the novel EN as a custom designed and manufactured implant
for individual patients. CAD drawings of the novel EN can be matched to a patient CT scan and the
implant manufactured in surgical stainless steel or titanium by rapid prototyping. The stainless steel
implant used in cadaver trials took approximately 4 weeks for production and post-processing for
screws. This is a delayed time frame, to allow other models to be produced at the same time for less
costs. We estimate an individual implant could be manufactured in less than a week, although costs
are likely to be significantly higher as a result. The ethical considerations of allowing a patient with
distal radial OSA awaiting production of the implant certainly need to be considered. However,
appropriate palliation may be provided with supportive external coaptation and analgesia. Further
work will need to be performed to assess the clinical and financial suitability of a novel EN for
custom manufacture.
Figure 32: Difference in radial medullary canal morphology (marked with yellow cross) between Greyhound (left) and Rottweiler (right). Both radii have been resected 10cm proximal to the radiocarpal joint.
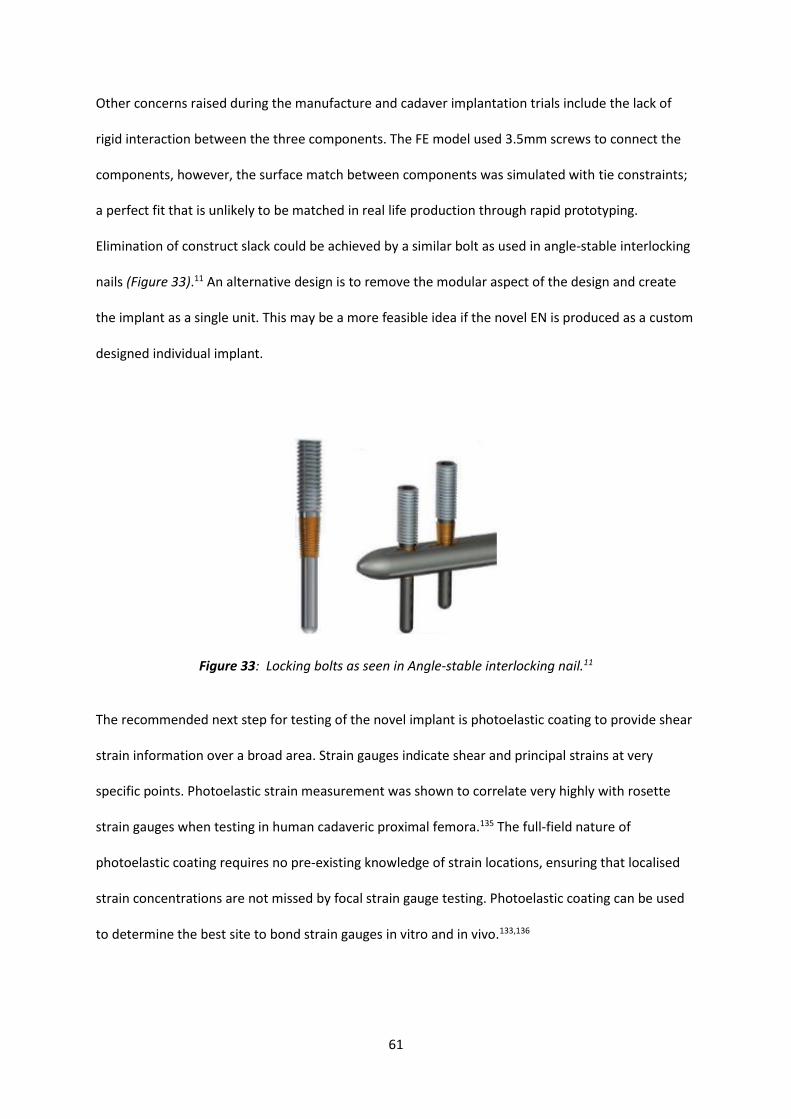
61
Other concerns raised during the manufacture and cadaver implantation trials include the lack of
rigid interaction between the three components. The FE model used 3.5mm screws to connect the
components, however, the surface match between components was simulated with tie constraints;
a perfect fit that is unlikely to be matched in real life production through rapid prototyping.
Elimination of construct slack could be achieved by a similar bolt as used in angle-stable interlocking
nails (Figure 33).11 An alternative design is to remove the modular aspect of the design and create
the implant as a single unit. This may be a more feasible idea if the novel EN is produced as a custom
designed individual implant.
The recommended next step for testing of the novel implant is photoelastic coating to provide shear
strain information over a broad area. Strain gauges indicate shear and principal strains at very
specific points. Photoelastic strain measurement was shown to correlate very highly with rosette
strain gauges when testing in human cadaveric proximal femora.135 The full-field nature of
photoelastic coating requires no pre-existing knowledge of strain locations, ensuring that localised
strain concentrations are not missed by focal strain gauge testing. Photoelastic coating can be used
to determine the best site to bond strain gauges in vitro and in vivo.133,136
Figure 33: Locking bolts as seen in Angle-stable interlocking nail.11

62
5. Conclusions
The aim of this thesis was to provide further information on metal endoprosthesis for limb sparing
surgery in the distal canine radius. Chapter 3 was devoted to a retrospective study of the currently
available metal endoprosthesis. This study has shown no significant difference in outcomes between
the two generations of metal endoprosthesis, and unacceptably high complication rates of infection
and implant failure. Infection is secondary to the nature of limb sparing surgery; lack of soft tissue
coverage, poor blood supply to the distal radius and implantation of a large foreign body. Implant
failure of GEN 2 was investigated and was thought to be due to the offset loading of the construct and
mismatch of modulus of elasticity between the host cortical bone and implant. Chapter 4 discusses
the design of a novel EN through FE modelling and the clinical suitability. The novel EN was
manufactured by rapid prototyping in plastic and 316L stainless steel and locking screw profile was
obtained by post-processing. Three variations of the novel EN were developed and tested in cadaver
implantation trials. There was a large variation in radius morphology between and within large breeds;
making the novel EN unlikely to be suitable as an off the shelf implant. The most appropriate
application of the novel EN may be via rapid prototyping based on an individual’s computed
tomography scan.
This thesis highlights the difficulties associated with limb sparing surgery in veterinary surgery. The
currently available procedures provide an alternative for pet-owners that are averse to amputation.
However, pet-owners must be aware of the high complication frequencies that are associated with
these techniques. Once refined; the novel EN has potential to decrease implant-related complication
rates through improved biomechanical load distribution especially at the implant-radius interface,
however the infection rates are likely to remain high due to large implant size and limited soft tissue
coverage. Future work in the investigation of the novel EN includes photoelastic strain testing and
axial compression biomechanical testing.

63
6. List of References
1. Liptak JM, Dernell WS, Ehrhart N, et al: Cortical allograft and endoprosthesis for limb-sparing surgery in dogs with distal radial osteosarcoma: a prospective clinical comparison of two different limb-sparing techniques. Vet Surg 35:518-533, 2006.
2. MacDonald TL, Schiller TD: Limb-sparing surgery using tantalum metal endoprosthesis in a dog with osteosarcoma of the distal radius. Can Vet J 51:497-500, 2010.
3. Liptak JM, Ehrhart N, Santoni BG, et al: Cortical bone graft and endoprosthesis in the distal radius of dogs: a biomechanical comparison of two different limb-sparing techniques. Vet Surg 35:150-160, 2006.
4. Neihaus SA, Locke JE, Barger AM, et al: A novel method of core aspirate cytology compared to fine-needle aspiration for diagnosing canine osteosarcoma. J Am Anim Hosp Assoc 47:317-323, 2011.
5. Ehrhart N: Longitudinal bone transport for treatment of primary bone tumors in dogs: technique description and outcome in 9 dogs. Vet Surg 34:24-34, 2005.
6. Venzin C, Grundmann S, Montavon PM: Loss of implant-bone interface following distal radial locking-plate endoprosthesis limb-sparing surgery in a dog. J Small Anim Pract 53:57-62, 2012.
7. Shetye S: Development of a novel endoprosthesis for canine limb-sparing using a finite element approach. Doctor of Philosophy: Colorado State University, 2010.
8. North S, Banks T: Tumours of the skeletal system, in North S, Banks T (eds): Small Animal Oncology : An Introduction, Vol. Oxford, Saunders Elsevier, 2009.
9. Séguin B, Walsh P, Mason D, et al: Use of an ipsilateral vascularized ulnar transposition autograft for limb-sparing surgery of the distal radius in dogs: an anatomic and clinical study. Veterinary Surgery 32:69-79, 2003.
10. Guillou RP, Demianiuk RM, Sinnott MT, et al: In vitro mechanical evaluation of a limited contact dynamic compression plate and hybrid carpal arthrodesis plate for canine pancarpal arthrodesis. Vet Comp Orthop Traumatol 25:83-88, 2012.
11. Dejardin LM, Cabassu JB, Guillou RP, et al: In vivo biomechanical evaluation of a novel angle-stable interlocking nail design in a canine tibial fracture model. Vet Surg 43:271-281, 2014.
12. Buracco P, Morello E, Martano M, et al: Pasteurized tumoral autograft as a novel procedure for limb sparing in the dog: A clinical report. Vet Surg 31:525-532, 2002.
13. Dernell W, Straw R, Withrow S: Tumors of the skeletal system, in Withrow S, MacEwan E (eds): Small Animal Clinical Oncology, Vol. Philadelphia, WB Saunders, 2001, pp 378-417.
14. Brodey R, Riser W: Canine osteosarcoma. A clinicopathologic study of 194 cases. Clinical Orthopaedics and Related Research 62:54-64, 1969.
15. Loukopoulos P, Robinson WF: Clinicopathological relevance of tumour grading in canine osteosarcoma. J Comp Pathol 136:65-73, 2007.
16. Ru G, Terracini B, Glickman L: Host Related Risk Factors for Canine Osteosarcoma. The Veterinary Journal 156:31-39, 1998.
17. Brodey RS, Abt DA: Results of surgical treatment in 65 dogs with osteosarcoma. J Am Vet Med Assoc 168:1032-1035, 1976.
18. Mauldin G, Matus R, Withrow S, et al: Canine Osteosarcoma Treatment by Amputation Versus Amputation and Adjuvant Chemotherapy Using Doxorubicin and Cisplatin. Journal of Veterinary Internal Medicine 2:177-180, 1988.
19. Tjalma RA: Canine bone sarcoma: estimation of relative risk as a function of body size. J Natl Cancer Inst 36:1137-1150, 1966.
20. Rosenberger J, Pablo N, Crawford C: Prevalence of and intrinsic risk factors for appendicular osteosarcoma in dogs: 179 cases (1996-2005). Journal of the American Veterinary Medical Association 231:1076-1080, 2007.
21. Misdorp W, Hart A: Some Prognostic and Epidemiologic Factors in Canine Osteosarcoma. Journal of the National Cancer Institute 63:537-545, 1979.

64
22. Kirpensteijn J, Kik M, Rutteman GR, et al: Prognostic Significance of a New Histologic Grading System for Canine Osteosarcoma. Veterinary Pathology 39:240-246, 2002.
23. Boston S, Ehrhart N, Dernell W, et al: Evaluation of survival time in dogs with stage III osteosarcoma that undergo treatment: 90 cases (1985-2004). Journal of the American Veterinary Medical Association 228:1905-1908, 2006.
24. McNeill C, Overley B, Shofer F, et al: Characterization of biological behaviour of appendicular osteosaroma in Rottweilers and a comparison with other breeds: a review of 258 dogs. Veterinary and Comparative Oncology 5:90-98, 2007.
25. Liu S, Dorfman H, Hurvitz A, et al: Primary and secondary bone tumours in the dog. Journal of Small Animal Practice 18:313-326, 1977.
26. Brodey RS, Sauer RM, Medway W: Canine Bone Neoplasms. J Am Vet Med Assoc 143:471-495, 1963.
27. Evans LB: Osteosarcoma in a young Great Dane dog. J S Afr Vet Assoc 54:271-273, 1983. 28. Cooley D, Beranek C, Schlittler D, et al: Endogenous Gonadal Hormone Exposure and Bone
Sarcoma Risk. Cancer Epidemiology, Biology & Prevention 11:1434-1440, 2002. 29. Chun R, de Lorimier LP: Update on the biology and management of canine osteosarcoma. Vet Clin
North Am Small Anim Pract 33:491-516, vi, 2003. 30. Banks WC, Morris E, Herron MR, et al: Osteogenic sarcoma associated with internal fracture
fixation in two dogs. J Am Vet Med Assoc 167:166-167, 1975. 31. Harrison JW, McLain DL, Hohn RB, et al: Osteosarcoma associated with metallic implants. Report
of two cases in dogs. Clin Orthop Relat Res:253-257, 1976. 32. Keel SB, Jaffe KA, Petur Nielsen G, et al: Orthopaedic implant-related sarcoma: a study of twelve
cases. Mod Pathol 14:969-977, 2001. 33. Madewell BR, Pool RR, Leighton RL: Osteogenic sarcoma at the site of a chronic nonunion fracture
and internal fixation device in a dog. J Am Vet Med Assoc 171:187-189, 1977. 34. Stevenson S, Hohn RB, Pohler OE, et al: Fracture-associated sarcoma in the dog. J Am Vet Med
Assoc 180:1189-1196, 1982. 35. Bennett D, Campbell JR, Brown P: Osteosarcoma associated with healed fractures. J Small Anim
Pract 20:13-18, 1979. 36. Sartor AJ, Ryan SD, Sellmeyer T, et al: Bi-institutional retrospective cohort study evaluating the
incidence of osteosarcoma following tibial plateau levelling osteotomy (2000-2009). Vet Comp Orthop Traumatol 27, 2014.
37. Selmic LE, Ryan SD, Boston SE, et al: Osteosarcoma following tibial plateau leveling osteotomy in dogs: 29 cases (1997-2011). J Am Vet Med Assoc 244:1053-1059, 2014.
38. Atherton MJ, Arthurs G: Osteosarcoma of the tibia 6 years after tibial plateau leveling osteotomy. J Am Anim Hosp Assoc 48:188-193, 2012.
39. Boudrieau RJ, McCarthy RJ, Sisson RD, Jr.: Sarcoma of the proximal portion of the tibia in a dog 5.5 years after tibial plateau leveling osteotomy. J Am Vet Med Assoc 227:1613-1617, 1591, 2005.
40. Harasen GL, Simko E: Histiocytic sarcoma of the stifle in a dog with cranial cruciate ligament failure and TPLO treatment. Vet Comp Orthop Traumatol 21:375-377, 2008.
41. Straw M: What is your diagnosis? Fracture/implant-associated osteosarcoma following TPLO procedures. J Small Anim Pract 46:457-459, 2005.
42. Wolke RE, Nielsen SW: Site incidence of canine osteosarcoma. J Small Anim Pract 7:489-492, 1966. 43. Knect: Musculoskeletal Tumors in Dogs. Journal of the American Veterinary Medical Association
172, 1978. 44. Jongeward SJ: Primary bone tumors. Vet Clin North Am Small Anim Pract 15:609-641, 1985. 45. Thrall D: Bone tumor versus bone infections, in Thrall D (ed): Textbook of Veterinary Diagnostic
Radiology, Vol. Philadelphia, WB Saunders, 1998, pp 161-168.

65
46. Berzina I, Sharkey L, I M: Correlation between cytologic and histopathologic diagnosis of bone lesions in dogs: a study of the diagnostic accuracy of bone cytology. Veterinary Clinical Pathology 37:332-338, 2008.
47. Barger A, Graca R, Bailey K, et al: Use of alkaline phosphatase staining to differentiate canine osteosarcoma from other vimentin-positive tumors. Vet Pathol 42:161-165, 2005.
48. Powers BE, LaRue SM, Withrow SJ, et al: Jamshidi needle biopsy for diagnosis of bone lesions in small animals. J Am Vet Med Assoc 193:205-210, 1988.
49. Wykes P, Withrow S, Powers B: Closed biopsy for diagnosis of long bone tumors: accuracy and results. Journal of the American Animal Hospital Association 21:489-494, 1985.
50. Spodnick GJ, Berg J, Rand WM, et al: Prognosis for dogs with appendicular osteosarcoma treated by amputation alone: 162 cases (1978-1988). J Am Vet Med Assoc 200:995-999, 1992.
51. Hillers KR, Dernell WS, Lafferty MH, et al: Incidence and prognostic importance of lymph node metastases in dogs with appendicular osteosarcoma: 228 cases (1986-2003). J Am Vet Med Assoc 226:1364-1367, 2005.
52. Gorman E, Barger AM, Wypij JM, et al: Cutaneous metastasis of primary appendicular osteosarcoma in a dog. Vet Clin Pathol 35:358-361, 2006.
53. Davis SD: CT evaluation for pulmonary metastases in patients with extrathoracic malignancy. Radiology 180:1-12, 1991.
54. Armbrust L, Biller D, Bamford A, et al: Comparison of three-view thoracic radiography and computed tomography for detection of pulmonary nodules in dogs with neoplasia. Journal of the American Veterinary Medical Association 240:1088-1094, 2012.
55. Alexander K, Joly H, Blond L, et al: A comparison of computed tomography, computed radiography, and film-screen radiography for the detection of canine pulmonary nodules. Vet Radiol Ultrasound 53:258-265, 2012.
56. Berg J, Lamb CR, O'Callaghan MW: Bone scintigraphy in the initial evaluation of dogs with primary bone tumors. J Am Vet Med Assoc 196:917-920, 1990.
57. LaRue SM, Withrow SJ, Wrigley RH: Radiographic bone surveys in the evaluation of primary bone tumors in dogs. J Am Vet Med Assoc 188:514-516, 1986.
58. Wallack S, Wisner E, Werner J, et al: Accuracy of magnetic resonance imaging for estimating intrameduallary osteosarcoma extent in pre-operative planning of canine limb-salvage procedures. Veterinary Radiology & Ultrasound 43:432-441, 2002.
59. Davis G, Kapatkin A, Craig L, et al: Comparison of radiography, computed tomography, and magnetic resonance imaging for evaluation of appendicular osteosarcoma in dogs. Journal of the American Veterinary Medical Association 220:1171-1176, 2002.
60. Karnik KS, Samii VF, Weisbrode SE, et al: Accuracy of computed tomography in determining lesion size in canine appendicular osteosarcoma. Vet Radiol Ultrasound 53:273-279, 2012.
61. Lamb CR, Berg J, Bengtson A: Preoperative measurement of canine primary bone tumors, using radiography and bone scintigraphy. Journal of the American Veterinary Medical Association 196:1474-1478, 1990.
62. O'Flanagan SJ, Stack JP, McGee HM, et al: Imaging of intramedullary tumour spread in osteosarcoma. A comparison of techniques. J Bone Joint Surg Br 73:998-1001, 1991.
63. Phillips B, Powers B, Dernell W, et al: Use of Single-Agent Carboplatin as Adjuvant or Neoadjuvant Therapy in Conjunction With Amputation for Appendicular Osteosarcoma in Dogs. Journal of the American Animal Hospital Association 45:33-38, 2009.
64. Schmidt AF, Nielen M, Klungel OH, et al: Prognostic factors of early metastasis and mortality in dogs with appendicular osteosarcoma after receiving surgery: An individual patient data meta-analysis. Prev Vet Med 112:414-422, 2013.
65. Boerman I, Selvarajah GT, Nielen M, et al: Prognostic factors in canine appendicular osteosarcoma - a meta-analysis. BMC Vet Res 8:56, 2012.
66. Bergman PJ, MacEwen EG, Kurzman ID, et al: Amputation and carboplatin for treatment of dogs with osteosarcoma: 48 cases (1991 to 1993). J Vet Intern Med 10:76-81, 1996.

66
67. Grundmann E, Roessner A, Ueda Y, et al: Current aspects of the pathology of osteosarcoma. Anticancer Res 15:1023-1032, 1995.
68. Mukaratirwa S: Prognostic and predictive markers in canine tumours: rationale and relevance. A review. Vet Q 27:52-64, 2005.
69. Straw RC, Powers BE, Klausner J, et al: Canine mandibular osteosarcoma: 51 cases (1980-1992). J Am Anim Hosp Assoc 32:257-262, 1996.
70. Garzotto CK, Berg J, Hoffmann WE, et al: Prognostic significance of serum alkaline phosphatase activity in canine appendicular osteosarcoma. J Vet Intern Med 14:587-592, 2000.
71. McKenna R, Schwinn C, Soong K, et al: Sarcomata of the Osteogenic Series (Osteosarcoma, Fibrosarcoma, Chondrosarcoma, Parosteal Osteogenic Sarcoma, and Sarcomata Arising in Abnormal Bone) An Analysis of 552 Cases. The Journal of Bone and Joint Surgery 48:1-26, 1966.
72. Ehrhart N, Dernell WS, Hoffmann WE, et al: Prognostic importance of alkaline phosphatase activity in serum from dogs with appendicular osteosarcoma: 75 cases (1990-1996). J Am Vet Med Assoc 213:1002-1006, 1998.
73. Sternberg RA, Pondenis HC, Yang X, et al: Association between absolute tumor burden and serum bone-specific alkaline phosphatase in canine appendicular osteosarcoma. J Vet Intern Med 27:955-963, 2013.
74. Sottnik JL, Rao S, Lafferty MH, et al: Association of blood monocyte and lymphocyte count and disease-free interval in dogs with osteosarcoma. J Vet Intern Med 24:1439-1444, 2010.
75. Thrall DE, Withrow SJ, Powers BE, et al: Radiotherapy prior to cortical allograft limb sparing in dogs with osteosarcoma: a dose response assay. Int J Radiat Oncol Biol Phys 18:1351-1357, 1990.
76. Lascelles BD, Dernell WS, Correa MT, et al: Improved survival associated with postoperative wound infection in dogs treated with limb-salvage surgery for osteosarcoma. Ann Surg Oncol 12:1073-1083, 2005.
77. Straw R, Withrow S: Limb-sparing surgery versus amputation for dogs with bone tumors. Veterinary Clinics of North America Small Animal Practice 26:135-143, 1996.
78. Straw R, Withrow S, Powers B: Management of canine appendicular osteosarcoma. Veterinary Clinics of North America Small Animal Practice 20:1141-1161, 1990.
79. Kirpensteijn J, Ven den Bos R, Van den Brom W, et al: Ground reaction force analysis of large breed dogs when walking after amputation of a limb. Veterinary Record 146:155-159, 2000.
80. Kirpensteijn J, van den Bos R, Endenburg N: Adaptation of dogs to the amputation of a limb and their owners' satisfaction with the procedure. Vet Rec 144:115-118, 1999.
81. Carberry C, Harvey H: Owner Satisfaction with Limb Amputation in Dogs and Cats. Journal of the American Animal Hospital Association 23:227-232, 1989.
82. Withrow SJ, Hirsch VM: Owner response to amputation of a pet's leg. Vet Med Small Anim Clin 74:332, 334, 1979.
83. Boston S: Musculoskeletal Neoplasia and Limb-Sparing Surgery, in Tobias K, Johnston S (eds): Veterinary Surgery : Small Animal, Vol 1. Missouri, Elsevier Saunders, 2012, pp 1159 - 1177.
84. Liptak J, Dernell W, Ehrhart N, et al: Canine appendicular osteosarcoma: curative-intent treatment. Compendium Continuing Education for Veterinarians 26:186-196, 2004.
85. LaRue SM, Withrow SJ, Powers BE, et al: Limb-sparing treatment for osteosarcoma in dogs. J Am Vet Med Assoc 195:1734-1744, 1989.
86. Endicott M: Principles of treatment for osteosarcoma. Clin Tech Small Anim Pract 18:110-114, 2003.
87. Tsuchiya H, Tomita K, Minematsu K, et al: Limb salvage using distraction osteogenesis. A classification of the technique. J Bone Joint Surg Br 79:403-411, 1997.
88. Kuntz CA, Asselin TL, Dernell WS, et al: Limb salvage surgery for osteosarcoma of the proximal humerus: outcome in 17 dogs. Vet Surg 27:417-422, 1998.
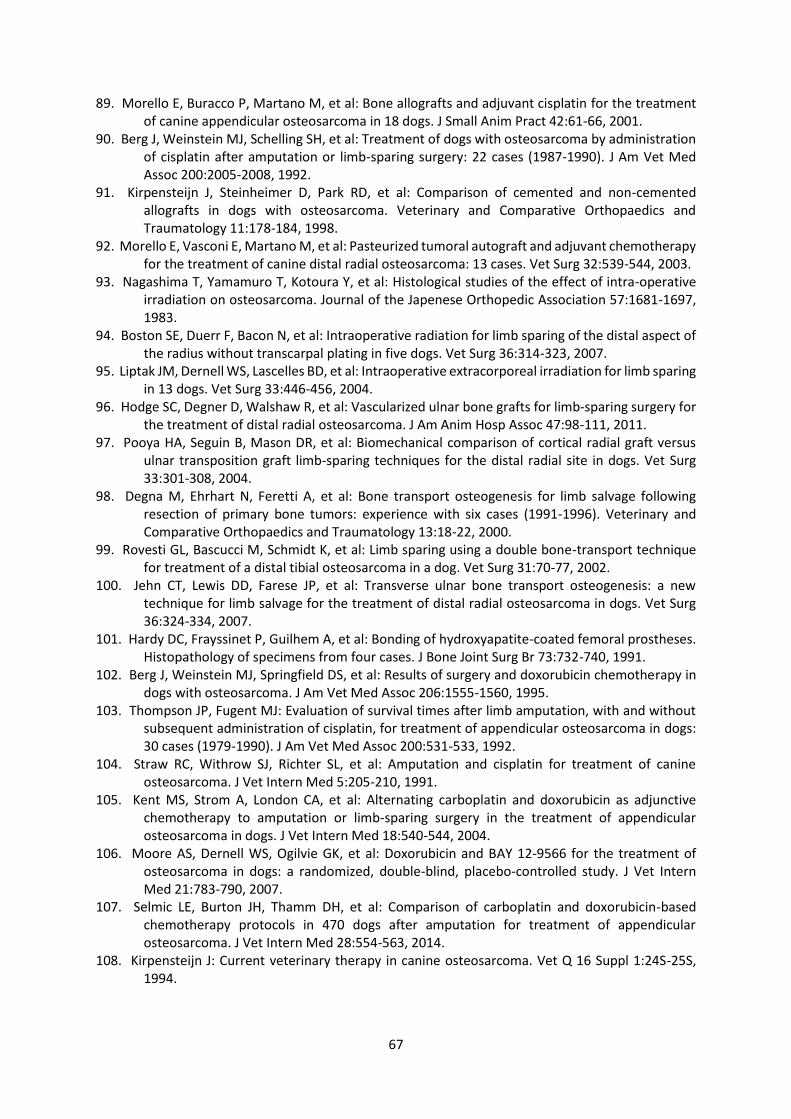
67
89. Morello E, Buracco P, Martano M, et al: Bone allografts and adjuvant cisplatin for the treatment of canine appendicular osteosarcoma in 18 dogs. J Small Anim Pract 42:61-66, 2001.
90. Berg J, Weinstein MJ, Schelling SH, et al: Treatment of dogs with osteosarcoma by administration of cisplatin after amputation or limb-sparing surgery: 22 cases (1987-1990). J Am Vet Med Assoc 200:2005-2008, 1992.
91. Kirpensteijn J, Steinheimer D, Park RD, et al: Comparison of cemented and non-cemented allografts in dogs with osteosarcoma. Veterinary and Comparative Orthopaedics and Traumatology 11:178-184, 1998.
92. Morello E, Vasconi E, Martano M, et al: Pasteurized tumoral autograft and adjuvant chemotherapy for the treatment of canine distal radial osteosarcoma: 13 cases. Vet Surg 32:539-544, 2003.
93. Nagashima T, Yamamuro T, Kotoura Y, et al: Histological studies of the effect of intra-operative irradiation on osteosarcoma. Journal of the Japenese Orthopedic Association 57:1681-1697, 1983.
94. Boston SE, Duerr F, Bacon N, et al: Intraoperative radiation for limb sparing of the distal aspect of the radius without transcarpal plating in five dogs. Vet Surg 36:314-323, 2007.
95. Liptak JM, Dernell WS, Lascelles BD, et al: Intraoperative extracorporeal irradiation for limb sparing in 13 dogs. Vet Surg 33:446-456, 2004.
96. Hodge SC, Degner D, Walshaw R, et al: Vascularized ulnar bone grafts for limb-sparing surgery for the treatment of distal radial osteosarcoma. J Am Anim Hosp Assoc 47:98-111, 2011.
97. Pooya HA, Seguin B, Mason DR, et al: Biomechanical comparison of cortical radial graft versus ulnar transposition graft limb-sparing techniques for the distal radial site in dogs. Vet Surg 33:301-308, 2004.
98. Degna M, Ehrhart N, Feretti A, et al: Bone transport osteogenesis for limb salvage following resection of primary bone tumors: experience with six cases (1991-1996). Veterinary and Comparative Orthopaedics and Traumatology 13:18-22, 2000.
99. Rovesti GL, Bascucci M, Schmidt K, et al: Limb sparing using a double bone-transport technique for treatment of a distal tibial osteosarcoma in a dog. Vet Surg 31:70-77, 2002.
100. Jehn CT, Lewis DD, Farese JP, et al: Transverse ulnar bone transport osteogenesis: a new technique for limb salvage for the treatment of distal radial osteosarcoma in dogs. Vet Surg 36:324-334, 2007.
101. Hardy DC, Frayssinet P, Guilhem A, et al: Bonding of hydroxyapatite-coated femoral prostheses. Histopathology of specimens from four cases. J Bone Joint Surg Br 73:732-740, 1991.
102. Berg J, Weinstein MJ, Springfield DS, et al: Results of surgery and doxorubicin chemotherapy in dogs with osteosarcoma. J Am Vet Med Assoc 206:1555-1560, 1995.
103. Thompson JP, Fugent MJ: Evaluation of survival times after limb amputation, with and without subsequent administration of cisplatin, for treatment of appendicular osteosarcoma in dogs: 30 cases (1979-1990). J Am Vet Med Assoc 200:531-533, 1992.
104. Straw RC, Withrow SJ, Richter SL, et al: Amputation and cisplatin for treatment of canine osteosarcoma. J Vet Intern Med 5:205-210, 1991.
105. Kent MS, Strom A, London CA, et al: Alternating carboplatin and doxorubicin as adjunctive chemotherapy to amputation or limb-sparing surgery in the treatment of appendicular osteosarcoma in dogs. J Vet Intern Med 18:540-544, 2004.
106. Moore AS, Dernell WS, Ogilvie GK, et al: Doxorubicin and BAY 12-9566 for the treatment of osteosarcoma in dogs: a randomized, double-blind, placebo-controlled study. J Vet Intern Med 21:783-790, 2007.
107. Selmic LE, Burton JH, Thamm DH, et al: Comparison of carboplatin and doxorubicin-based chemotherapy protocols in 470 dogs after amputation for treatment of appendicular osteosarcoma. J Vet Intern Med 28:554-563, 2014.
108. Kirpensteijn J: Current veterinary therapy in canine osteosarcoma. Vet Q 16 Suppl 1:24S-25S, 1994.
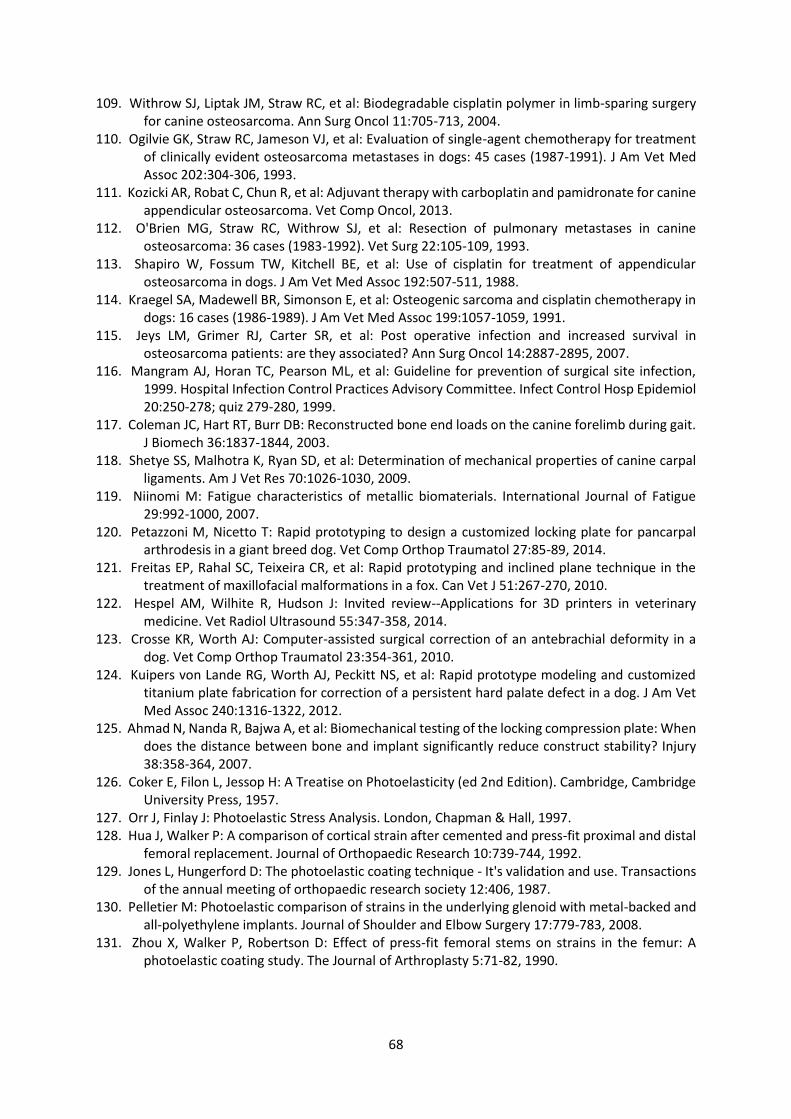
68
109. Withrow SJ, Liptak JM, Straw RC, et al: Biodegradable cisplatin polymer in limb-sparing surgery for canine osteosarcoma. Ann Surg Oncol 11:705-713, 2004.
110. Ogilvie GK, Straw RC, Jameson VJ, et al: Evaluation of single-agent chemotherapy for treatment of clinically evident osteosarcoma metastases in dogs: 45 cases (1987-1991). J Am Vet Med Assoc 202:304-306, 1993.
111. Kozicki AR, Robat C, Chun R, et al: Adjuvant therapy with carboplatin and pamidronate for canine appendicular osteosarcoma. Vet Comp Oncol, 2013.
112. O'Brien MG, Straw RC, Withrow SJ, et al: Resection of pulmonary metastases in canine osteosarcoma: 36 cases (1983-1992). Vet Surg 22:105-109, 1993.
113. Shapiro W, Fossum TW, Kitchell BE, et al: Use of cisplatin for treatment of appendicular osteosarcoma in dogs. J Am Vet Med Assoc 192:507-511, 1988.
114. Kraegel SA, Madewell BR, Simonson E, et al: Osteogenic sarcoma and cisplatin chemotherapy in dogs: 16 cases (1986-1989). J Am Vet Med Assoc 199:1057-1059, 1991.
115. Jeys LM, Grimer RJ, Carter SR, et al: Post operative infection and increased survival in osteosarcoma patients: are they associated? Ann Surg Oncol 14:2887-2895, 2007.
116. Mangram AJ, Horan TC, Pearson ML, et al: Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol 20:250-278; quiz 279-280, 1999.
117. Coleman JC, Hart RT, Burr DB: Reconstructed bone end loads on the canine forelimb during gait. J Biomech 36:1837-1844, 2003.
118. Shetye SS, Malhotra K, Ryan SD, et al: Determination of mechanical properties of canine carpal ligaments. Am J Vet Res 70:1026-1030, 2009.
119. Niinomi M: Fatigue characteristics of metallic biomaterials. International Journal of Fatigue 29:992-1000, 2007.
120. Petazzoni M, Nicetto T: Rapid prototyping to design a customized locking plate for pancarpal arthrodesis in a giant breed dog. Vet Comp Orthop Traumatol 27:85-89, 2014.
121. Freitas EP, Rahal SC, Teixeira CR, et al: Rapid prototyping and inclined plane technique in the treatment of maxillofacial malformations in a fox. Can Vet J 51:267-270, 2010.
122. Hespel AM, Wilhite R, Hudson J: Invited review--Applications for 3D printers in veterinary medicine. Vet Radiol Ultrasound 55:347-358, 2014.
123. Crosse KR, Worth AJ: Computer-assisted surgical correction of an antebrachial deformity in a dog. Vet Comp Orthop Traumatol 23:354-361, 2010.
124. Kuipers von Lande RG, Worth AJ, Peckitt NS, et al: Rapid prototype modeling and customized titanium plate fabrication for correction of a persistent hard palate defect in a dog. J Am Vet Med Assoc 240:1316-1322, 2012.
125. Ahmad N, Nanda R, Bajwa A, et al: Biomechanical testing of the locking compression plate: When does the distance between bone and implant significantly reduce construct stability? Injury 38:358-364, 2007.
126. Coker E, Filon L, Jessop H: A Treatise on Photoelasticity (ed 2nd Edition). Cambridge, Cambridge University Press, 1957.
127. Orr J, Finlay J: Photoelastic Stress Analysis. London, Chapman & Hall, 1997. 128. Hua J, Walker P: A comparison of cortical strain after cemented and press-fit proximal and distal
femoral replacement. Journal of Orthopaedic Research 10:739-744, 1992. 129. Jones L, Hungerford D: The photoelastic coating technique - It's validation and use. Transactions
of the annual meeting of orthopaedic research society 12:406, 1987. 130. Pelletier M: Photoelastic comparison of strains in the underlying glenoid with metal-backed and
all-polyethylene implants. Journal of Shoulder and Elbow Surgery 17:779-783, 2008. 131. Zhou X, Walker P, Robertson D: Effect of press-fit femoral stems on strains in the femur: A
photoelastic coating study. The Journal of Arthroplasty 5:71-82, 1990.

69
132. Grecula M, Morris R, Laughlin J, et al: Femoral surface strain in intact composite femurs: a custom computer analysis of the photoelastic coating technique. Transactions on Biomedical Engineering 47:926-933, 2000.
133. Davies H: Ex vivo calibration and validation of in vivo equine bone strain measures. Equine Veterinary Journal 41:225-228, 2009.
134. Whitelock R, Dyce J, Houlton J: Metacarpal fractures associated with pancarpal arthrodesis in dogs. Veterinary Surgery 28:25-30, 1999.
135. Glisson R, Musgrave D, Graham R, et al: Validity of Photoelastic Strain Measurement on Cadaveric Proximal Femora. Journal of Biomechanical Engineering 122:423-429, 2000.
136. Judge R, Palamara J, Taylor R, et al: Description of a photoelastic coating technique to describe surface strain of a dog skull loaded in vitro. Journal of Prosthestic Dentistry 90:92-96, 200

I
Appendix 1: Manuscript for multi-institutional retrospective study on
metal endoprosthesis
Mitchell KE, Boston SE, Kung M, Dry S, Straw E, Ehrhart NP, Ryan SD: Outcomes of Limb-Sparing
Surgery Using Two Generations of Metal Endoprosthesis in 45 Dogs With Distal Radial
Osteosarcoma. A Veterinary Society of Surgical Oncology Retrospective Study. Veterinary
Surgery 2016; 45:36-43.
DOI: http://onlinelibrary.wiley.com/doi/10.1111/vsu.12423/abstract

Outcomes of Limb-Sparing Surgery Using Two Generationsof Metal Endoprosthesis in 45 Dogs With Distal RadialOsteosarcoma. A Veterinary Society of Surgical OncologyRetrospective StudyKatherine E. Mitchell1, Sarah E. Boston2, Marvin Kung3, Sarah Dry4, Rod C. Straw3, Nicole P. Ehrhart5,and Stewart D. Ryan1
1Translational Research and Animal Clinical Trial Study (TRACTS) Group, University of Melbourne Veterinary Teaching Hospital, Werribee,Australia, 2College of Veterinary Medicine, University of Florida, Gainesville, Florida, 3Australian Animal Cancer Foundation, Brisbane VeterinarySpecialist Centre, Albany Creek, Australia, 4Southpaws Specialty Surgery for Animals, Moorabbin, Australia and 5College of Veterinary Medicineand Biomedical Sciences, Colorado State University, Fort Collins, Colorado
Corresponding AuthorKatherine MitchellTranslational Research and Animal ClinicalTrial Study (TRACTS) GroupUniversity of Melbourne Veterinary TeachingHospital250 Princes HighwayWerribee [email protected]
Submitted March 2015Accepted September 2015
DOI:10.1111/vsu.12423
Objective: To report outcomes in dogs with distal radial osteosarcoma (OSA) treatedwith metal endoprosthesis limb-sparing surgery and compare outcomes between 2generations of endoprosthesis.Study Design: Multi-institutional retrospective case series.Animals: Forty-five dogs with distal radial OSA treated with endoprosthesis andchemotherapy.Methods: Data of dogs treated with either first-generation endoprosthesis (GEN1) orsecond-generation endoprosthesis (GEN2) were sourced from medical records andradiographs. Surgical outcomes included postoperative lameness assessment and thepresence, severity, and time to onset of complications. Oncologic outcomes includedpresence of local recurrence ormetastasis, time to onset of local recurrence, metastasis-free interval (MFI), and survival time. Results for surgical and oncologic outcomeswere compared between GEN1 and GEN2.Results: Twenty-eight dogs received GEN1 and 17 dogs received GEN2. There were39 complications (96%, 14 minor, 29 major) including infection (78%), implant-related complication (36%), and local recurrence (24%). Metastatic frequency was67% and median MFI was 188 days (95% confidence interval [CI]: 126–250 days).Survival time ranged from 34 days to 6.1 years with a median of 289 days (95% CI:207–371 days). There was no significant difference in complication severity,frequency, time to complication, MFI, or survival time between dogs receivingGEN1 and GEN2.Conclusion: There was no significant difference in outcomes between dogs receivingGEN1 and GEN2 for limb-sparing surgery of the radius. Metastatic frequency andsurvival time for metal endoprosthesis were similar to that of amputation with curativeintent chemotherapy.
Osteosarcoma (OSA) is the most common primary bone tumorin dogs, usually affecting middle-aged, large breed dogs.1 Upto 40% of cases are reported in the distal radial OSA.2–5 Limbamputation with adjuvant chemotherapy is the standard ofcurative-intent treatment.6–12
Limb-sparing techniques can be used for dogs whereamputation is prohibitive such as orthopedic or neurologicdisease in other limbs, or owner request.13–17 Traditional limb-sparing surgery involves tumor resection and reconstruction ofthe bonycolumnwith a plate.Alternate limb-sparing techniquesused in the distal radius include pasteurized autografts,18,19
irradiated autografts,20,21 ulnar transposition,22–24 and bonetransport osteogenesis.25–28 Median survival times with limb-
sparing have been reported to be comparable to amputationwhen combined with adjuvant chemotherapy.7,8,29–33 Limb-sparing of the distal radius has produced favorable results andthe resultant pancarpal arthrodesis iswell tolerated by dogs.29,32
The ideal candidates for limb-sparing surgery are those with atumor that occupies less than 50% the length of the bone, hasminimal soft tissue involvement, and there is no pathologicfracture or evidence of metastasis.7
The first limb-sparing technique described for use in dogsreplaced the radial defect with a large cortical allograft.29,33
This technique is associated with high complication ratesincluding infection, fracture, instability, and local tumorrecurrence, and requires maintenance or access to a bone
36 Veterinary Surgery 45 (2016) 36–43 © Copyright 2015 by The American College of Veterinary Surgeons

banking facility. A 316L surgical stainless steel endoprosthesis(Veterinary Orthopedic Implants, Burlington, VT) wasdeveloped as an alternate to the cortical allograft. The first-generation endoprosthesis (GEN1) consists of a solid 122mmsegment of surgical steel with a flared distal end to abut theradial carpal bone, which is stabilized with a dedicated plate(Fig 1).
A biomechanical study comparing GEN1 and corticalallografts found endoprosthesis constructs were significantlystronger than cortical bone allografts at yield and failure pointsunder axial compression.34 However, there were no significantdifferences in stiffness or energy to failure between theendoprosthesis and cortical allograft constructs.34 A prospec-tive study comparing case outcomes after endoprosthesis andcortical allograft implantation showed no significant differ-ences between the techniques.35 Dogs receiving the endopros-thesis had an infection rate of 60%, construct failure in 40%,and local recurrence in 20%, whereas dogs receiving theallograft had comparable complication rates of 50%, 40%, and10%, respectively.35 Endoprosthesis construct failed becauseof screw loosening or fracture in the proximal aspect of theradius, thought secondary to a mismatch in modulus ofelasticity between stainless steel and host cortical bone.35
Limb function was graded as good to excellent in 80% of dogswith an endoprosthesis and 70% of dogs with the corticalallograft.35
A second-generation endoprosthesis (GEN2) was devel-oped to address the high failure rate associated with GEN1implant (Fig 2). The radial defect spacer is available in 2lengths (98 and 122mm) and has weight reduction throughvoid regions. It is available with a hydroxyapatite coating topromote osseous integration and is used with a dedicatedangle-stable locking plate and screws. The GEN2 has not beenbiomechanically tested and case outcomes have not beenreported in a large scale study. A single case report describesthe use of GEN2 with locking plate and screws, whichdeveloped an implant-related complication 4 months postop-erative.36 Another single case report describes the successfuluse of a custom-made tantalum endoprosthesis in the distalradius.37
This study reports the case outcomes (surgical andoncologic) in dogs with distal radial OSA treated with GEN1and GEN2 metal endoprosthesis limb-sparing surgery andadjuvant chemotherapy. We hypothesized that dogs receivingGEN2 would have less surgical complications than thosereceiving GEN1.
MATERIALS AND METHODS
The study was a multi-institutional retrospective case seriesauthorized by the Veterinary Society of Surgical Oncology.Medical records of participating institutions were reviewedfor dogs with distal radial OSA that underwent limb-sparingsurgery with a metal endoprosthesis and adjuvant chemo-therapy between 2001 and 2013. Dogs were included if therewas a histologic diagnosis of OSA, no radiographic orcomputed tomography (CT) evidence of pulmonary metas-tasis at the time of surgery, and if the dog received aminimum of one scheduled chemotherapy treatment afterlimb-sparing surgery.
Data retrieved included signalment, body weight,presenting complaint, preoperative lameness evaluation,results of staging tests performed, serum alkaline phosphatase(ALP) activity on admission, therapy before surgery, descrip-tion of surgery and type of endoprosthesis used, chemotherapyadministered, lameness evaluation after repair, postoperativesurgical complications, metastasis, cause of death, date lastreported alive, or date lost to follow-up. Case information wascollected using a standardized case accrual form filled out bythe contributors.
Figure 1 First-generation 122mm endoprosthesis (GEN1) and dedi-cated limb-sparing bone plate for distal radius limb-sparing surgery indogs (courtesy of Dr. Julius Liptak).
Figure 2 Second-generation 122mm endoprosthesis (GEN2) anddedicated limb-sparing bone plate for distal radius limb-sparing surgeryin dogs. (A) Disassembled view (courtesy of Dr. Julius Liptak),(B) postoperative caudal-cranial radiographic projection, (C) postopera-tive medial-lateral radiographic projection.
Veterinary Surgery 45 (2016) 36–43 © Copyright 2015 by The American College of Veterinary Surgeons 37
Mitchell et al. Limb Sparing Endoprosthesis for Canine Radial Osteosarcoma

Lameness was graded using a subjective, semi-quantita-tive grading system based on descriptions in the medicalrecords; 0 (no lameness), 1 (mild lameness), 2 (moderateweight bearing lameness), or 3 (severe non-weight bearinglameness). A surgical infection was defined as presence of 1 ormore draining sinus tracts at the surgical site and wascategorized as mild (draining sinus tracts that resolve after oralantibiotic therapy), moderate (draining sinus tracts thatrespond to oral antibiotics but did not resolve), or severe(draining sinus tracts that are refractory to oral antibiotictherapy and that requires implantation of antibiotic containingbeads or surgical intervention). Surgical implant-relatedcomplications included loosening or breakage of bone screws,plate or endoprosthesis, and/or fracture of the radius ormetacarpal bones. Implant-related complications were cate-gorized as mild (did not require surgical revision), moderate(required minor surgical revision, such as removing, tighten-ing, or replacing loosened bone screws), or severe (requiringmajor surgical revision, such as bone plate replacement or limbamputation). Overall, minor complications comprised mildimplant-related complications or mild/moderate surgicalinfections that were treated conservatively and majorcomplications comprised local recurrence or complicationsthat required amputation or revision surgery.
Days to complication were the number of days from limb-sparing surgery to documentation of infection, implantcomplication, or local recurrence. Metastasis-free interval(MFI) was the number of days from limb-sparing surgery todocumentation of metastatic disease. Survival time was thenumber of days from limb-sparing surgery to death oreuthanasia. Cases were right censored on the date of caseaccrual if they were still alive, on the date of death if fromother causes, or on the last date of followup if lost to followupbefore case accrual.
Statistical Analysis
Data were examined for normality using Shapiro–Wilk testsand by visually inspecting histograms of the data. All variableswere described and summarized by frequencies and 95%confidence interval (CI) for categorical variables andinterquartile range (IQR) for numeric values. The data werecategorized by explanatory variables in 3 different ways forexploration: categorized by generation implant (GEN1,GEN2), implant-related complication (presence, absence),and local recurrence (presence, absence). Univariate analysiswas performed to explore associations between explanatorycategories and categorical outcomes using Fisher’s exact test(for cell counts<5) or Pearson’s Chi squared tests (x2; for cellcounts >5). Continuous outcomes were compared acrossexplanatory categories using Student’s t-tests where normallydistributed (age, body weight, preoperative ALP) or Mann–Whitney U-test where not normally distributed (severity oflameness or complication). Kaplan–Meier (KM) productlimit estimates and 95% CI were calculated for days tocomplication, days to local recurrence,MFI, and survival time.A log-rank test was used to compare KM functions stratifiedon GEN1 and GEN2, with/without elevated preoperative
ALP (> 131 IU/L), with/without infection, with/without im-plant-related complication, and with/without local recurrence.KM estimates and a log-rank test were performed for daysto implant-related complication, stratified on locking/non-locking screws. A P<.05 was considered significant and posthoc power analysis was performed for all nonsignificantresults. Data were analyzed using IBM SPSS Statistics v22.
RESULTS
Forty-five dogs from 7 institutions met the inclusion criteria.Surgery was performed by 15 board certified veterinarysurgeons. Breeds were mixed breed (11), doberman (5), GreatDane (4), Labrador retriever (4), Great Pyrenees (3),greyhound (2), Irish wolfhound (2), rottweiler (3), Goldenretriever (2), bull mastiff (2), and 1 each of Old Englishsheepdog, Bernese Mountain dog, malamute, akita, Leon-berger, Irish setter, and Australian shepherd. There were 27castrated males, 14 spayed females, 3 entire males, and 1 entirefemale. Median age at surgery was 7.5 years (range 2–13.3,IQR 3). Median body weight was 45.5 kg (range 24.1–71, IQR15.7).
All dogs presented with forelimb lameness of a medianduration of 2 weeks (range 5 days to 12 weeks, IQR 3 weeks).The left radius was affected in 28 dogs, the right in 17 dogs.Four dogs had pathologic fracture of the radius at presentation.Preoperative radiographic or CT screening for thoracicmetastasis was performed in all dogs which were staged clearfor detectable pulmonary metastasis, as dictated by inclusioncriteria. Whole-body scintigraphy was performed in 27 dogs(60%) to screen for bone metastasis which was negative inall dogs. Preoperative serum ALP activity was elevated(reference interval 20–131 IU/L) in 13 dogs (28%; mean119.7 IU/L, range 20–479, IQR 101I). There were nosignificant differences in signalment and preoperative databetween dogs receiving GEN1 or GEN2.
The GEN1 was used in 28 dogs (62%) and GEN2 in 17dogs (38%). The proximal margin was clear of OSA onhistologic examination in 43 dogs and unclear in 2 dogs.Surgery was performed without recorded complication in alldogs. The ulna was preserved in 42% of dogs (14 GEN1, 3GEN2). Plate bending angle at the radiocarpal joint wasrecorded for 23 dogs as no bending (n¼ 10) and between 6°and 15° (IQR 2°, n¼ 13). The number of screws placedproximal to themetal spacer ranged from 4 to 8 (median 6, IQR2) and the number of screws placed distal to the metal spacerranged from 6 to 9 (median 8, IQR 3). The mean percentagelength of radius replaced was 57% (range 42–65%, IQR 8%),and mean percentage length of metacarpal 3 covered by theplate was 82% (range 60–94%, IQR 16%). There was nosignificant difference in the above surgical data betweenGEN1 and GEN2 (Table 1). Locking screws (9 dogs) and theshorter 98mm radial defect spacer (3 dogs) were only used indogs with the GEN2, reflecting the differences in the implant.
All dogs had postoperative chemotherapy, as dictated byinclusion criteria. The most frequent postoperative protocols
38 Veterinary Surgery 45 (2016) 36–43 © Copyright 2015 by The American College of Veterinary Surgeons
Limb Sparing Endoprosthesis for Canine Radial Osteosarcoma Mitchell et al.

included a platinum agent (carboplatin or cisplatin) anddoxorubicin as a single agent or in combination. Open cellpolylactic acid polymer sponges impregnated with cisplatin(OPLA-Pt) were used in 11 dogs (10 GEN1, 1 GEN2). TheOPLA-Pt was used in 2/4 dogs that presented with pathologicfracture.
Surgical complications occurred in 43 dogs (96%) withminor complications in 14 dogs (31%) and major in 29 dogs(64%; Table 1). There were no significant differences in theseverity or frequency of surgical complication or days tocomplication between GEN1 or GEN2. Infections were mild(n¼ 16), moderate (n¼ 10), or severe (n¼ 9). The mostfrequent isolates were Staphylococcus spp. (n¼ 11), Pseudo-monas spp. (n¼ 5), Escherichia coli (n¼ 4), and Enterobacterspp. (n¼ 4). Three of the cultures were multi-drug resistant.Implant-related complications were mild (n¼ 4), moderate(n¼ 4), or severe (n¼ 8). Implant-related complicationsincluded screw loosening (n¼ 8) or screw breakage (n¼ 3),plate fracture (n¼ 3), and fracture to the radius (n¼ 1) or
metacarpal bone 3 (n¼ 1). Treatment for implant-relatedcomplications was conservative (n¼ 5), revision surgery(n¼ 9), or amputation (n¼ 2). The KM-estimated survivalfunctions for days to implant-related complication, stratifiedon locking or non-locking screws, were not significantlydifferent (P¼.08).
Local recurrence occurred in the radius (n¼ 5), distal ulna(n¼ 4), radial carpal bone (n¼ 1), and surrounding soft tissues(n¼ 1). Two of 11 dogs treated with OPLA-Pt developed localrecurrence. This included 1 dog presenting with pathologicfracture. Only infection was associated with local recurrence(P¼.01, Table 2).
There were no significant differences in postoperativelameness scores between dogs receiving GEN1 or GEN2 atany time points (Table 3). Amputation was performed in 9dogs because of local recurrence in 4 dogs, severe infection in3, and implant-related complications in 2.
Survival analysis included 34 dogs with completeendpoints of euthanasia for tumor- or procedure-related
Table 1 Frequency of, and EstimatedMedian (95% Confidence Intervals) Days to, Surgical Outcomes of Dogs Receiving First- (GEN1) and Second-Generation (GEN2) Endoprostheses
OutcomeOverall(n¼ 45)
GEN1(n¼ 28)
GEN2(n¼ 17) P-Value
Post HocPower
Infection 35 (78%) 20 (71%) 15 (88%) .19 (x2) 0.23Implant-related complication 16 (36%) 9 (32%) 7 (41%) .54 (x2) 0.09Amputation 9 (20%) 4 (14%) 5 (29%) .22 (x2) 0.24Days to infection 129 (59–199) 131 (11–251) 123 (4–242) .71 (log-rank) 0.03Days to implant-related complication 169 (119–219) 169 (89–249) 118 (101–135) .09 (log-rank) 0.71Days to amputation 125 (18–232) 457 (0–1099) 125 (31–219) .18 (log-rank) 0.99
Table 2 Categorized Explanatory Variables Tested for Univariate Association With Implant-Related Complication and Local Recurrence
Outcome (n) Categorization n P-Value
Implant-related complication (16) Ulna preserved 25 0.75 (x2)Ulna not preserved 16
Non locking screws 18 0.33 (FET)Locking screws 9
No plate bending at radiocarpal joint 12 0.45 (FET)Plate bending at radiocarpal joint 11
41–55% radius replaced 12 0.09 (FET)56–70% radius replaced 16
60–79% metacarpal covered 6 0.27 (FET)80–99% metacarpal covered 16
Infection 10 0.24 (x2)No infection 35
Local recurrence (11) Pathologic fracture 4 0.69 (FET)No pathologic fracture 41
Ulna preserved 25 0.94 (x2)Ulna not preserved 16
41–55% radius replaced 12 0.52 (FET)56–70% radius replaced 16
OPLA-Pt use 10 0.61 (x2)No OPLA-Pt 32
Histologic incomplete margins 2 0.39 (x2)Histologic complete margins 36
Infection 10 0.01 (FET)No infection 35
FET, Fisher's exact test; OPLA-Pt, open cell polylactic acid polymer sponges impregnated with cisplatin.
Veterinary Surgery 45 (2016) 36–43 © Copyright 2015 by The American College of Veterinary Surgeons 39
Mitchell et al. Limb Sparing Endoprosthesis for Canine Radial Osteosarcoma

disease (Table 4). This included 4 dogs with infection, 2 withlocal recurrence, 28 with metastatic disease, and 4 dogs thatdied from tumor-related disease (pleural effusion presumedsecondary to pulmonary metastasis). Seven dogs were rightcensored with 2 dogs alive at study accrual and 5 dead fromother causes as noted in the medical record (lymphoma, gastricdilation and volvulus, neurologic disease, cardiac disease, andrenal disease). No dogs were lost to follow-up. Metastaticdisease was confirmed in 27 dogs and suspected in 3. Locationof metastasis included pulmonary only (n¼ 14), bone only(n¼ 5), pulmonary and bone (n¼ 4), pulmonary and other(n¼ 2), and lymph node (n¼ 2). Suspected hepatic (n¼ 2) andbrain (n¼ 1) metastases were not confirmed with histology.Survival time ranged from 34 days to 6.1 years with anestimated median of 289 days (95% CI 207–371). The 1-, 2-,and 3-year survival was 33%, 16%, and 4%, respectively. TheKM-estimated functions for survival time, stratified on GEN1and GEN2, were not significantly different (P¼.71, Fig 3).The KM-estimated functions for survival were not differentwhen stratified on with/without elevated preoperative ALP(P¼.12), with/without infection (P¼.81), or with/withoutlocal recurrence (P¼.46). The estimated KM functions forsurvival time, stratified on with/without implant-relatedcomplication, were significantly different (P¼.004). Furtherstratification on GEN1/GEN2 (4 functions) was also signifi-cant (P¼.04).
DISCUSSION
The use of GEN2 did not result in any significant differences inthe frequency of surgical complications or days to complica-tion, contrary to our hypothesis. Metastasis frequency, MFI, orsurvival time were not significantly different between dogsreceiving either endoprostheses.
The frequency of implant-related complications (32%GEN1, 41% GEN2) is similar to that reported previously.Liptak and others reported a 40% frequency of implant-relatedcomplications for GEN1.35 In that case series, construct failurewas because of screw loosening or breakage in the proximalaspect of the radius, thought because of amismatch inmodulusof elasticity or poor load sharing between host cortical boneand metal endoprosthesis.35 In the present study, implantfailure varied for the 2 endoprostheses with failure at bothproximal and the distal aspects of the construct. Angle-stablebone plates and a lighter weight spacer are features of theGEN2 designed to reduce construct failure. The present studydid not show a difference in the frequency of implant-relatedcomplications between GEN1 and GEN2, or between lockingor nonlocking screws. These findings, combined with a reportof construct failure with a GEN2 locking system,36 suggestthat implant failure is not averted by the use of locking screws.In the present study, the presence of infection was notassociated with implant-related complication, a findingconsistent with reports on the GEN1.35 The percentage ofradius replaced or percentage of metacarpus covered by platewas not significantly associated with implant-related compli-cations. However, most dogs had the larger spacer implanteddespite the GEN2 spacer being available in 2 lengths (98 and122mm) and the percentage of radius replaced was similar forGEN1 and GEN2 (median 57% for both). Hydroxyapatitecoating for osseous integration has been proposed to improveload transfer and decrease stress concentration over time but itsimpact on implant-related complications could not beevaluated in this study.
The 78% frequency of infection in the present study washigher than previously reported. A case series reportedinfection in 5/10 dogs with GEN1.35 In that study, 4/5infections were moderate or severe, whereas almost halfof infections in the present study were mild. Regardless, thefrequency of surgical infection with limb-sparing remains
Table 3 Postoperative Lameness for Dogs Receiving First-Generation (GEN1) and Second-Generation (GEN2) Endoprostheses
None (n) Mild (n) Moderate (n) Severe (n) Total (n)
Postop GEN1 GEN2 GEN1 GEN2 GEN1 GEN2 GEN1 GEN2 GEN1 GEN2
0–4 weeks 0 2 17 9 5 4 2 0 24 151–6 months 1 2 6 5 8 5 5 4 20 16>6 months 0 0 2 2 1 1 2 2 5 5
Table 4 Frequency of, and EstimatedMedian (95%Confidence Intervals) Days to, OncologicOutcomes for Dogs Receiving First-Generation Implant(GEN1) and Second-Generation Endoprostheses (GEN2)
OutcomeOverall(n¼ 45)
GEN1(n¼ 28)
GEN2(n¼ 17) P-Value
Post HocPower
Local recurrence 11 (24%) 7 (25%) 4 (24%) .91 (x2) 0.03Metastasis 30 (67%) 19 (68%) 11 (65%) .83 (x2) 0.04Days to local recurrence 125 (40–210) 99 (0–226) 125 (41–209) .35 (log-rank) 0.15Metastasis-free interval (days) 188 (126–250) 212 (168–256) 102 (49–155) .06 (log-rank) 0.68Survival time (days) 289 (207–371) 294 (183–405) 255 (222–288) .71 (log-rank) 0.05
40 Veterinary Surgery 45 (2016) 36–43 © Copyright 2015 by The American College of Veterinary Surgeons
Limb Sparing Endoprosthesis for Canine Radial Osteosarcoma Mitchell et al.

unacceptably high. Implicated factors include poor soft tissuecoverage, extensive soft tissue resection, a large inert implant,and immunosuppression from neoplasia and chemotherapywhich are all related to limb-sparing surgery rather than thetype of implant used.
Postoperative lameness within 4 weeks of surgery wassubjectively graded as none/mild in 33 dogs (73%). This iscomparable to previous reports for both allograft andendoprosthesis (69–75% graded good/excellent).29,32,35
Lameness scores did not differ significantly between GEN1and GEN2 at any postoperative time point, althoughassessment is clearly limited by data quality. Objectivemeasurements would be required for more definitive compari-son. Overall survival for limb sparing was 76%, comparable to85% reported for GEN1.35
Local recurrence (24%) fell within the 11–28% rangepreviously reported for limb-sparing in the distalradius.19,27,29,35,38 Pathologic fracture is considered a contra-indication for limb-sparing because of tumor seeding intoadjacent soft tissue. Only 1/4 dogs that presented withpathologic fracture developed local recurrence contrary toperceived risks of local recurrence. Local recurrence occurredin the proximal radius in 5/11 dogs, despite all having cleanmargins on postoperative histology. Two dogs had histologicevidence of incomplete proximal margins but only 1 dogdeveloped local recurrence (ulna). Accurate determination oflocal tumor extent is critical to determine the level for radialosteotomy. Magnetic resonance imaging (MRI) with T1-weighted noncontrast images is the most accurate method todetect the extent of intramedullary OSA but MRI doesoverestimate tumor length compared to radiographs, nuclearscintigraphy, and CT.39–41 Local recurrence in the ulnaoccurred in 4/11 dogs but distal ulna preservation was not
significantly associated with local recurrence in univariateanalysis. Regardless, the authors recommend en bloc resectionof the radius and ulna to be consistent with oncologicprinciples, to remove the distal ulna as a potential localrecurrence site, and to decrease surgical time. In addition, thereis no biomechanical advantage to ulna preservation whenusing GEN1.34 Use of OPLA-Pt in cortical allograft limb-sparing surgery showed dogs treated with OPLA-Pt were 54%less likely to develop local recurrence than dogs withoutOPLA-Pt.42 In our study, there was no association betweentreatment with OLPA-Pt and local recurrence (22% withOPLA-Rt, 39% without).
There were no significant differences in metastasisfrequency, median MFI, and survival times for dogs receivingGEN1 and GEN2 and chemotherapy, and the overall findingswere similar to that reported for amputation and adjuvantchemotherapy.8,9,31,43–45 Different adjuvant chemotherapyprotocols across multi-institutions were used in the presentstudy but no chemotherapy protocol appears superior forOSA.46
Dogs with implant-related complication had significantlyincreased survival time (482 days) compared to dogs withoutimplant-related complication (201 days). This relationship isdifficult to understand but it is unlikely that increased survivaltime allowed capture of more implant-related complicationsgiven that the median days to implant-related complication(169 days) were shorter than the median survival time (289days). This finding is reported previously for GEN1, wheredogs without construct failure were 17 times more likely to diethan dogs with construct failure.35
Postoperative infection is reported previously as posi-tively associated with decreased local recurrence frequency,42
and increased MFI and survival time.20,38,46,47 In the present
Figure 3 Estimated Kaplan–Meier survival functions for 28 dogs treatedwith first-generationmetal endoprosthesis (GEN1) and 17 dogs treatedwithsecond-generation metal endoprosthesis (GEN2).
Veterinary Surgery 45 (2016) 36–43 © Copyright 2015 by The American College of Veterinary Surgeons 41
Mitchell et al. Limb Sparing Endoprosthesis for Canine Radial Osteosarcoma

study, infection was not significantly associated with implant-related complications or survival time. However, univariateanalysis showed that infection was significantly associatedwith a lower frequency of local recurrence. The relationshipbetween infection and improved outcome is not fullyunderstood but is thought to be related to inflammation andimmunologic reactions.35,38
Elevated preoperative serum ALP activity is negativelyassociated with survival time for dogs with OSA.46,48–50
However, the present study showed no separation of thesurvival functions for dogs with and without elevated ALP.Recent work suggests that the negative association betweenpretreatment ALP activity and outcome may simply reflectgreater initial tumor burden.51
Limitations of our study include retrospective datacollection and the reliance on documentation to makesubjective assessment of lameness and infection. Infectionwas not confirmed by bacterial culture and categorization ofinfection did not use the standardized classification for surgicalsite infection.52 Days to implant-related complication,amputation, and MFI were the only analyses with appropriatestatistical power. For the other analyses, depending on theexamined variable, between 252 and 39,295 dogs would berequired to achieve a power of 85%, and thus type II error ishigh. Multiple institutions were retrospectively involved,which creates biases in surgical management (variations intechnique, pre- and postoperative management). Frequenciesof complications, local recurrence, and metastasis may beunderestimated as complete examination and follow-up wasnot consistent.
This study showed no significant difference in case(surgical or oncologic) outcomes between dogs receivingGEN1 and GEN2 endoprostheses for limb-sparing surgery ofthe distal radius. The frequency of complications, includinginfection and those implant-related, remains unacceptablyhigh for both generations of endoprosthesis. Oncologicoutcomes of dogs receiving either generation endoprosthesisremain similar to amputation and other limb-sparing techni-ques that are combined with adjuvant curative-intentchemotherapy.8,9,31,43–45 Further refinement of the endopros-thesis or re-evaluation of the surgical technique for implanta-tion of the endoprosthesis is indicated.
ACKNOWLEDGMENTS
The authors acknowledge the assistance of Dr. Julius Liptak,Dr. Martin Havlicek, Dr. Radboud Kemme, Mary Lafferty,Dr. James Simcock, Dr. James Farese, and the Veterinary Societyof Surgical Oncology with case accrual and Dr. Louise Mitchellwith statistical analysis.
DISCLOSURE
The authors declare no conflicts of interest related to thisreport.
REFERENCES
1. Ru G, Terracini B, Glickman L: Host related risk factors forcanine osteosarcoma. Vet J 1998;156:31–39
2. Knect CD: Musculoskeletal tumors in dogs. J Am Vet Med Assoc1978;172:72–74
3. Rosenberger J, Pablo N, Crawford C: Prevalence of and intrinsicrisk factors for appendicular osteosarcoma in dogs: 179 cases(1996–2005). J Am Vet Med Assoc 2007;231:1076–1080
4. Brodey R, Riser W: Canine osteosarcoma. A clinicopathologicstudy of 194 cases. Clin Orthop Relat Res 1969;62:54–64
5. Wolke RE, Nielsen SW: Site incidence of canine osteosarcoma.J Small Anim Pract 1966;7:489–492
6. KentMS, StromA, London CA, et al: Alternating carboplatin anddoxorubicin as adjunctive chemotherapy to amputation or limb-sparing surgery in the treatment of appendicular osteosarcoma indogs. J Vet Int Med 2004;18:540–544
7. Straw R,Withrow S: Limb-sparing surgery versus amputation fordogs with bone tumors. Vet Clin N Am Sm Anim Pract1996;26:135–143
8. Mauldin G, Matus R, Withrow S, et al: Canine osteosarcomatreatment by amputation versus amputation and adjuvantchemotherapy using doxorubicin and cisplatin. J Vet Int Med1988;2:177–180
9. Thompson JP, Fugent MJ: Evaluation of survival times after limbamputation, with and without subsequent administration ofcisplatin, for treatment of appendicular osteosarcoma in dogs: 30cases (1979–1990). J Am Vet Med Assoc 1992;200:531–533
10. Bergman PJ, MacEwen EG, Kurzman ID, et al: Amputation andcarboplatin for treatment of dogs with osteosarcoma: 48 cases(1991 to 1993). J Vet Intern Med 1996;10:76–81
11. Kozicki AR, Robat C, Chun R, et al: Adjuvant therapy withcarboplatin and pamidronate for canine appendicularosteosarcoma. Vet Comp Oncol 2015;13:229–236
12. Selmic LE, Burton JH, Thamm DH, et al: Comparison ofcarboplatin and doxorubicin-based chemotherapy protocols in470 dogs after amputation for treatment of appendicularosteosarcoma. J Vet Intern Med 2014;28:554–563
13. Straw R, Withrow S, Powers B: Management of canineappendicular osteosarcoma. Vet Clin N Am Sm Anim Pract1990;20:1141–1161
14. Kirpensteijn J, Ven den Bos R, van den Brom W, et al: Groundreaction force analysis of large breed dogs when walking afteramputation of a limb. Vet Rec 2000;146:155–159
15. Kirpensteijn J, van den Bos R, Endenburg N: Adaptation of dogsto the amputation of a limb and their owners’ satisfaction with theprocedure. Vet Rec 1999;144:115–118
16. Carberry C, Harvey H: Owner satisfaction with limb amputationin dogs and cats. J Am Anim Hosp Assoc 1989;23:227–232
17. Withrow SJ, Hirsch VM: Owner response to amputation of a pet’sleg. Vet Med Small Anim Clin 1979;74:332
18. Buracco P, Morello E, Martano M, et al: Pasteurized tumoralautograft as a novel procedure for limb sparing in the dog: aclinical report. Vet Surg 2002;31:525–532
19. Morello E, Vasconi E, Martano M, et al: Pasteurized tumoralautograft and adjuvant chemotherapy for the treatment of caninedistal radial osteosarcoma: 13 cases. Vet Surg 2003;32:539–544
42 Veterinary Surgery 45 (2016) 36–43 © Copyright 2015 by The American College of Veterinary Surgeons
Limb Sparing Endoprosthesis for Canine Radial Osteosarcoma Mitchell et al.

20. Liptak JM, Dernell WS, Lascelles BD, et al: Intraoperativeextracorporeal irradiation for limb sparing in 13 dogs. Vet Surg2004;33:446–456
21. Boston SE, Duerr F, Bacon N, et al: Intraoperative radiation forlimb sparing of the distal aspect of the radius without transcarpalplating in five dogs. Vet Surg 2007;36:314–323
22. Seguin B, Walsh P, Mason D, et al: Use of an ipsilateralvascularized ulnar transposition autograft for limb-sparingsurgery of the distal radius in dogs: an anatomic and clinical study.Vet Surg 2003;32:69–79
23. Irvine-Smith GS, Lobetti RG: Ipsilateral vascularised ulnartransposition autograft for limb-sparing surgery of the distalradius in 2 dogs with osteosarcoma. J S Afr Vet Assoc2006;77:150–154
24. Pooya HA, Seguin B, Mason DR, et al: Biomechanicalcomparison of cortical radial graft versus ulnar transposition graftlimb-sparing techniques for the distal radial site in dogs. Vet Surg2004;33:301–308
25. Degna M, Ehrhart N, Feretti A, et al: Bone transport osteogenesisfor limb salvage following resection of primary bone tumors:experience with six cases (1991–1996). Vet Comp OrthopTraumatol 2000;13:18–22
26. Rovesti GL, Bascucci M, Schmidt K, et al: Limb sparing using adouble bone-transport technique for treatment of a distal tibialosteosarcoma in a dog. Vet Surg 2002;31:70–77
27. Ehrhart N: Longitudinal bone transport for treatment of primarybone tumors in dogs: technique description and outcome in 9dogs. Vet Surg 2005;34:24–34
28. Jehn CT, Lewis DD, Farese JP, et al: Transverse ulnar bonetransport osteogenesis: a new technique for limb salvage for thetreatment of distal radial osteosarcoma in dogs. Vet Surg2007;36:324–334
29. LaRue SM, Withrow SJ, Powers BE, et al: Limb-sparingtreatment for osteosarcoma in dogs. J Am Vet Med Assoc1989;195:1734–1744
30. Thrall DE, Withrow SJ, Powers BE, et al: Radiotherapy priorto cortical allograft limb sparing in dogs with osteosarcoma: adose response assay. Int J Radiat Oncol Biol Phys1990;18:1351–1357
31. Berg J, Weinstein MJ, Schelling SH, et al: Treatment of dogs withosteosarcoma by administration of cisplatin after amputation orlimb-sparing surgery: 22 cases (1987–1990). J Am Vet Med Assoc1992;200:2005–2008
32. Morello E, Buracco P, Martano M, et al: Bone allografts andadjuvant cisplatin for the treatment of canine appendicularosteosarcoma in 18 dogs. J Small Anim Pract 2001;42:61–66
33. Kirpensteijn J, Steinheimer D, Park RD, et al: Comparison ofcemented and non-cemented allografts in dogs withosteosarcoma. Vet Comp Ortho Traumatol 1998;11:178–184
34. Liptak JM, Ehrhart N, Santoni BG, et al: Cortical bone graft andendoprosthesis in the distal radius of dogs: a biomechanicalcomparison of two different limb-sparing techniques. Vet Surg2006;35:150–160
35. Liptak JM, Dernell WS, Ehrhart N, et al: Cortical allograftand endoprosthesis for limb-sparing surgery in dogs withdistal radial osteosarcoma: a prospective clinical comparisonof two different limb-sparing techniques. Vet Surg2006;35:518–533
36. Venzin C, Grundmann S, Montavon PM: Loss of implant-boneinterface following distal radial locking-plate endoprosthesislimb-sparing surgery in a dog. J Small Anim Pract 2012;53:57–62
37. MacDonald TL, Schiller TD: Limb-sparing surgery usingtantalum metal endoprosthesis in a dog with osteosarcoma of thedistal radius. Can Vet J 2010;51:497–500
38. Lascelles BD, Dernell WS, Correa MT, et al: Improved survivalassociated with postoperative wound infection in dogs treatedwith limb-salvage surgery for osteosarcoma. Ann Surg Oncol2005;12:1073–1083
39. Wallack S, Wisner E, Werner J, et al: Accuracy of magneticresonance imaging for estimating intrameduallary osteosarcomaextent in pre-operative planning of canine limb-salvageprocedures. Vet Radiol Ultrasound 2002;43:432–441
40. Davis G, Kapatkin A, Craig L, et al: Comparison of radiography,computed tomography, and magnetic resonance imaging forevaluation of appendicular osteosarcoma in dogs. J Am Vet MedAssoc 2002;220:1171–1176
41. Lamb CR, Berg J, Bengtson A: Preoperative measurement ofcanine primary bone tumors, using radiography and bonescintigraphy. J Am Vet Med Assoc 1990;196:1474–1478
42. Withrow SJ, Liptak JM, Straw RC, et al: Biodegradable cisplatinpolymer in limb-sparing surgery for canine osteosarcoma. AnnSurg Oncol 2004;11:705–713
43. Straw RC, Withrow SJ, Richter SL, et al: Amputation andcisplatin for treatment of canine osteosarcoma. J Vet Intern Med1991;5:205–210
44. Shapiro W, Fossum TW, Kitchell BE, et al: Use of cisplatin fortreatment of appendicular osteosarcoma in dogs. J Am Vet MedAssoc 1988;192:507–511
45. Kraegel SA, Madewell BR, Simonson E, et al: Osteogenicsarcoma and cisplatin chemotherapy in dogs: 16 cases (1986–1989). J Am Vet Med Assoc 1991;199:1057–1059
46. Boerman I, Selvarajah GT, Nielen M, et al: Prognostic factors incanine appendicular osteosarcoma—a meta-analysis. BMC VetRes 2012;8:56
47. Jeys LM, Grimer RJ, Carter SR, et al: Post operative infection andincreased survival in osteosarcoma patients: are they associated?Ann Surg Oncol 2007;14:2887–2895
48. Schmidt AF, Nielen M, Klungel OH, et al: Prognostic factors ofearly metastasis and mortality in dogs with appendicularosteosarcoma after receiving surgery: an individual patient datameta-analysis. Prev Vet Med 2013;112:414–422
49. Garzotto CK, Berg J, Hoffmann WE, et al: Prognosticsignificance of serum alkaline phosphatase activity in canineappendicular osteosarcoma. J Vet Intern Med 2000;14:587–592
50. Ehrhart N, Dernell WS, Hoffmann WE, et al: Prognosticimportance of alkaline phosphatase activity in serum from dogswith appendicular osteosarcoma: 75 cases (1990–1996). J Am VetMed Assoc 1998;213:1002–1006
51. Sternberg RA, Pondenis HC, Yang X, et al: Association betweenabsolute tumor burden and serum bone-specific alkalinephosphatase in canine appendicular osteosarcoma. J Vet InternMed 2013;27:955–963
52. Mangram AJ, Horan TC, Pearson ML, et al: Guideline forprevention of surgical site infection, 1999. Hospital infectioncontrol practices advisory committee. Infect Control HospEpidemol 1999;20:250–278
Veterinary Surgery 45 (2016) 36–43 © Copyright 2015 by The American College of Veterinary Surgeons 43
Mitchell et al. Limb Sparing Endoprosthesis for Canine Radial Osteosarcoma

II
Appendix 2: Veterinary Society of Surgical Oncology study proposal

I. Title
First and second generation metal endoprostheses for limb sparing surgery in dogs with distal radial
osteosarcoma: a retrospective evaluation of surgical and oncological outcomes.
II. Study Investigators
Katherine Mitchell University of Melbourne, Australia
Stewart Ryan University of Melbourne, Australia
III. Aims and objectives of the study
1. Report surgical and oncological outcomes in dogs with distal radial osteosarcoma treated by
a combination of endoprosthesis (first or second generation) limb-sparing surgery and
adjuvant chemotherapy.
2. Report and compare outcomes (e.g. limb use, surgical infection, implant related
complications, local tumor recurrence, distant metastasis, survival time) for the first and
second generation endoprosthesis.
3. Evaluate factors that may be associated with outcomes and complications.
IV. Background and significance
The standard for curative-intent treatment for dogs with osteosarcoma (OSA) involves limb
amputation with adjuvant chemotherapy. Limb amputation is may have relative contrainidcations in
some patients; obese patients and those with neurological or orthopaedic disease in other limbs.1 In
addition, some owners are adverse to the idea of amputation.2 For these reasons, limb-sparing
techniques are becoming more common.
Several limb-sparing techniques have been described to treat distal radial OSA. Reported techniques
include distraction osteogenesis, vascularized, irradiated and pasteurized autografts, cortical
allografts and stereotactic radiosurgery. A first generation stainless steel endoprosthesis was

developed as an alternative to massive cortical allografts. The advantages of an endoprosthesis
include a readily available implant, minimal preparation prior to implantation and no requirement
for a bone banking facility or access to external radiation beam therapy. One of the expected
advantages was a reduction in post-operative infections compared to a massive cortical allograft.
Biomechanical comparisons in canine cadaver limbs between cortical allografts and the first
generation endoprosthesis in acute axial loading showed that limbs reconstructed with the
endoprosthesis were significantly stronger and up to 33% stiffer.3 However, there were no
significant differences in surgical and oncologic outcomes between the first generation
endoprosthesis and the cortical allograft in a clinical trial by Liptak et al.4 Infection rates between the
endoprosthesis and allograft constructs were similar (60% of cortical allografts and 50% of
endoprosthesis constructs).4 The major failures of the first generation endoprosthesis were loss of
screw purchase and screw breakage in the proximal radius whereas the cortical allograft
predominantly failed in the distal limb. The increased risk of proximal failure in the endoprosthesis
was hypothesized to be due to the difference in the modulus of elasticity between the stainless steel
implant and the host cortical bone, resulting in concentration of forces at the proximal bone
endoprosthesis interface.
A second generation endoprosthesis was developed to address the high complication rate
associated with the first generation model. This second generation endoprosthesis has significant
weight reduction by hollowing out of the prosthesis and is available now with hydroxyapatite
coating in an effort to improve osseous integration. The second generation implant is available in
two lengths (98mm and 122mm) to allow a smaller percent of radius to be resected in smaller dogs.
A further evolution is the use of locking screws with a second generation endoprosthesis.5 Currently,
the second generation endoprosthesis has not been evaluated by biomechanical testing or had
clinical surgical/oncologic outcomes reported.

We hypothesize that limb-sparing surgery of the distal radius with a second generation
endoprosthesis would result in a superior surgical outcome (decreased implant related complication
rate) compared with the first generation endoprosthesis, but there would be no difference in
oncologic outcome between the two endoprosthesis.
1. Kirpensteijn J, van den Bos R, van den Brom WE, et al: Ground reaction force analysis of large breed
dogs when walking after the amputation of a limb. Vet Rec 146:155-159, 2000.
2. Kirpensteijn J, van den Bos R, Endenburg N: Adaptation of dogs to the amputation of a limb and their
owners' satisfaction with the procedure. Veterinary Record 144:115-118, 1999.
3. Liptak JM, Ehrhart N, Santoni BG, et al: Cortical bone graft and endoprosthesis in the distal radius of
dogs: a biomechanical comparison of two different limb-sparing techniques. Vet Surg 35:150-160,
2006.
4. Liptak JM, Dernell WS, Ehrhart N, et al: Cortical allograft and endoprosthesis for limb-sparing surgery
in dogs with distal radial steosarcoma: a prospective clinical comparison of two different limb-sparing
techniques. Vet Surg 35:518-533, 2006.
5. Venzin C, Grundmann S, Montavon P: Loss of implant-bone interface following distal radial locking-
plate endoprosthesis limb-sparing surgery in a dog. J Small Anim Pract 53:57-62, 2012.
VI. Experimental Design
a) Brief Description: Multi-institutional retrospective study
b) Patient Eligibility
Dogs with spontaneously occurring, non-metastatic OSA of the distal aspect of the
radius that underwent limb-sparing surgery between 1st January 2001 and 1st January
2013 with a metal endoprosthesis will be included.
Definitive diagnosis of OSA must be confirmed by histopathology of a pre-surgical biopsy
or the resected bone segment. Full histopathology reports should be provided. There
will be no need to provide original histopathology slides.

Dogs must have received a minimum of one scheduled chemotherapy treatment after
limb salvage surgery, demonstrating curative intent therapy.
Imaging requirements for study inclusion will include pre- and post-operative regional
limb radiographs and 3-view thoracic radiographs or chest computed tomography to
screen for pulmonary metastases. Ideally copies of any imaging performed will be
provided. If copies cannot be accessed then accurate radiological interpretations will
suffice.
c) Patient ineligibility criteria
Patients that did not undergo any chemotherapy following limb salvage surgery
Patients with evidence of metastatic disease at time of limb salvage surgery
d) Patient resources
Case accrual rate estimate: Colorado State University is expected to yield up to 35 cases.
We expect a further 20-30 cases across North America, approximately 10 across Europe,
and approximately 5 across Australia and New Zealand. We aim to have up to 65 cases
seen over a 12 year period (Jan 2001 – Jan 2013).
Incentives: Veterinarians that provide ≥ 10% of the case accrual numbers will be invited
to join as co-contributor and co-author on manuscript(s) produced from the study.
e) Study endpoints - Data retrieval
Patient Details
Institution specific patient number
Signalment (date of birth, sex, neuter status, breed)
Weight at time of surgery
Pre-operative evaluation
Presenting complaint (eg: lameness or swelling)

Any concurrent disease (eg: pathological fracture, arthritis)
Affected limb
Degree of lameness pre-operatively (see below for grading system)
Duration of lameness (weeks)
Results of incisional biopsies if performed (attach reports)
Metastatic screening tests and results (attach copies of images, or reports)
Total serum alkaline phosphatase levels. Concentration and time point
Details of any pre-operative radiation therapy (dose and protocol)
Details of any other therapy prior to surgery (eg: NSAID use)
Surgical evaluation
Date of surgery
Name of primary surgeon
Note if ulna was preserved
Angle of plate bending performed at the radiocarpal junction
Number of screws proximal and distal to endoprosthesis
Percentage of radius replaced by implant
Percentage of the metacarpus coverage
Note if a cisplatin implant was used
Endoprosthesis details
Generation (First vs Second)
Locking or non-locking screws
Length of endoprosthesis
Note if hydroxyapatite coating used
Post-operative evaluation
Histopathology results from removed segment of radius (attach reports)
Chemotherapy agent, protocol and patient response
Surgical Outcomes
Limb Use at 3 time points if available. See below for grading system.
0-4 weeks post-operative
1-6 months post-operative
> 6 months post-operative
Surgical Infection (defined as ≥1 draining sinus tracts at surgical site). See below for
grading system.
Date of infection
Microbial culture and sensitivity results (attach results)
Antimicrobial type and duration
Implant related complication (defined as loosening or breakage of either bone
screws or bone plate and/or fracture of the radius, endoprosthesis, or metacarpus).
See below for grading system.
Date of complication
Type of complication (screw loosening, screw breakage, plate breakage,
endoprosthesis fracture, fracture proximal to endoprosthesis and fracture
distal to endoprosthesis)
Treatment of complication (conservative, revision surgery, amputation,
euthanasia)
Oncologic Outcomes
Local tumor recurrence
Location of local recurrence (eg: proximal radius)
Date of recurrence
Treatment of local recurrence (conservative, limb amputation, radiation
therapy, euthanasia)
Metastasis free interval
Date of metastasis
Location of metastasis
Method of diagnosis
Survival time
Note if the animal is currently alive or deceased
If deceased – note date of death
If deceased – note cause of death (tumor related vs. not-tumor related)
If alive – last follow up date and any further information
The following grading systems to be adhered to whenever possible:
Limb use
0 = no lameness
1 = mild lameness
2 = moderate weight bearing lameness
3 = severe non-weight bearing lameness
Surgical infection
Mild = draining sinus tracts that resolve after oral antibiotic therapy
Moderate = draining sinus tracts that respond to oral antibiotics but do not
resolve
Severe = draining sinus tracts that are refractory to oral antibiotic therapy
and that requires implantation of antibiotic containing beads or surgical
intervention.
Implant related complication
Mild = does not require surgical revision

Moderate = requiring minor surgical revision, such as removing, tightening,
or replacing loosened bone screws
Severe = requiring major surgical revision, such as bone plate replacement
or limb amputation
j) Duration of study
Case accrual between September and November 2013
Data analysis will occur between December 2013 and March 2014
Draft manuscript will be prepared by June 2014

III
Appendix 3: Veterinary Society of Surgical Oncology accrual form

SIGNALMENT PRE-
OPERATIVE ASSESSMENT
Patient/case number
Date of Birth (dd/mm/yyyy)
Gender Breed Weight
(kg) Presenting complaint
Concurrent disease
Affected limb
Degree of lameness
Duration of
lameness (weeks)
Incisional biopsy
performed?
Incisional biopsy results
Thoracic radiographs performed?
Thoracic radiograph
results
EXAMPLE 25/01/2005 FS Rottweiler 35.2 Lameness Bilateral hip
osteoarthritis L
1 = Mild lameness
8 Y Osteosarcoma
(OSA) Y
No evidence
of metastasis
SURGICAL DETAILS
CT scan performed?
CT scan results
Bone scan performed?
Bone scan results
Serum total alkaline
phosphatase measurements
Pre-operative radiation therapy
performed?
Radiation dose and protocol
Other therapy prior to surgery
Date of Surgery
(dd/mm/yyyy)
Name of primary surgeon
Ulna preserved?
Plate bending at radiocarpal
junction
Number of
proximal screws
Number of distal screws
Y
No evidence
of metastasis
Y
No evidence
of metastasis
Pre-operative = 240 U/L
N -
4 weeks of NSAID
carprofen @ 4
mg/kg/day
25/02/2011 - N Y - 40% 5 8

IMPLANT DETAILS
POST-OPERATIVE
ASSESSMENT
Percentage of radius
replaced by implant
Percentage of metacarpus
coverage
Cisplatin implant used?
Generation of implant
used
Locking screws used?
Length of endoprost
hesis
Hydroxyapatite coating used?
Post-operative histopathology results - PLEASE
ATTACH
Histopathology margin evaluation
Chemotherapy post-surgery?
Chemotherapy agent
Chemotherapy protocol
Chemotherapy adverse
reactions?
60% 78% Y 2nd Locking 122mm N Clean Y Doxorubicin every 21
days for 5 doses
N
SURGICAL OUTCOMES
Limb use 0-4 weeks
post-operatively
Limb use 1-6
months post-
operatively
Limb use > 6 months
post-operatively
Surgical infection present?
Surgical infection severity
Date of surgical
infection (dd/mm/yyyy)
Culture and Sensitivity results - PLEASE ATTACH
Treatment : Antimicrobial and duration
Implant related
complication
Implant related
complication severity
Implant related
complication type
Date of implant related
complication
Implant related
complication treatment
1 = Mild lameness
1 = Mild lameness
Not Assessed
Y Mild 25/03/2011 Staphylococcus
intermedius
Cephalexin 30mg/kg PO q8h 30 days
Y Mild Screw
loosening 25/04/2011
Conservative treatment
ONCOLOGICAL OUTCOMES
Local tumour recurrence
Location of local tumour
recurrence
Date of Recurrence
(dd/mm/yyyy)
Treatment of local
recurrence
Metastasis detected
post-surgery?
Date of metastasis detection
(dd/mm/yyyy)
Location of
metastasis
Method of diagnosis of metastasis
Animal currently
deceased or alive?
Date of death (dd/mm/yyyy)
Cause of death
If alive - last follow up date
and further information
Y Proximal
radius 25/05/2011
Conservative treatment
Y 25/06/2011 Pulmonary CT Scan and
thoracic radiographs
Deceased 25/07/2011 Tumour related
euthanasia -

IV
Appendix 4: Surgical procedure for novel implant

Materials required:
Endoprosthesis & jig
General & Orthopaedic surgical pack
2.5 and 3.5 locking screw set
Drill & Oscillating saw
Procedure
Surgical Exposure 1. Make a cranio-lateral approach to antebrachium from distal metacarpal to proximal radius.
2. Expose radius, carpal and metacarpal bones and retract soft tissues with self-retaining retractors.
3. Place hypodermic needles in the radiocarpal joint space to identify the radiocarpal joint and proximal extent of the radiocarpal bone.
Jig placement: 4. Place assembled jig on anterior surface of radius, carpal and metacarpal bones.
5. Distal jig placement
a. Position the distal jig on the radiocarpal bone with proximal end of distal jig at the level of planned radiocarpal osteotomy.
b. If plate does not sit flat then transect attachment of extensor carpi radialis from proximal metacarpal 3 and use burr or oscillating bone saw to remove the tuberosity of proximal aspect of metacarpal 3 until flat. The tendon can be sutured to the attachment on proximal metacarpal 2.
c. Verify appropriate jig placement and proposed radiocarpal osteotomy position with mediolateral and anterioposterior view fluoroscopy.
d. Affix the distal jig section to the radiocarpal bone and proximal and distal metacarpal bones by drilling, tapping and placing locking screws through the radiocarpal holes and one proximal and distal metacarpal hole in the jig plate section. Use locking screw drill guide.
6. Proximal jig placement
a. Position the proximal jig on the radius with the distal end of the proximal jig at the level of the planned radial osteotomy (should be ≥ 3cm beyond proximal extent of tumour based on pre-operative and intra-operative imaging).
b. Verify the proposed osteotomy position with fluoroscopy.
c. Place 2 locking screws in proximal end of jig. Use locking screw drill guide.
7. Determine size and length of modular endoprosthesis segment that will be required.

Radius tumour resection: 8. Uncouple jig hinge to provide free access to distal radius for tumour removal.
9. Place osteotomy guide on proximal jig end and make proximal radial osteotomy with oscillating saw.
10. Collect bone marrow sample from remaining proximal radius segment and submit as proximal marrow margin.
11. Use Kern retractors to hold proximal end of radius section to be removed
12. Disarticulate the antebrachiocarpal joint to remove radial segment.
13. If there is evidence of distal ulna involvement, remove the ulnar styloid process en bloc with the tumour specimen by disarticulation and distal ulna osteotomy.
14. Ink and submit tumour specimen for radiography and histopathology.
15. Place osteotomy guide on distal jig end and make radiocarpal osteotomy with oscillating saw.
Placement of distal endoprosthesis segment: 16. Remove distal jig segment by removing pre-placed locking screws.
17. Transect extensor carpi radialis tendon at insertion on proximal metacarpal 3, suture to branch inserting onto metacarpal 2
18. Use burr or oscillating bone saw to flatten the tuberosity of proximal metacarpal 3. Ensure that distal endoprosthesis is sitting flush along carpus and metacarpal bone.
19. Fix the distal endoprosthesis to the radiocarpal and metacarpal bones using 2.5 and 3.5mm locking screws placed in the pre-drilled holes.
Placement of proximal endoprosthesis segment: 20. Remove proximal jig segment by removing pre-placed screws.
21. Ream intramedullary canal of proximal radius with broach (or burr) until able to fit test intramedullary stem implant.
22. Lavage and dry intramedullary canal
23. Insert proximal endoprosthesis component by introducing intramedullary stem and sliding proximal endoprosthesis component in proximal direction until the collar engages the cortical bone at the radial osteotomy site.
24. Replace pre-drilled screws, and fill remaining empty holes with 2.5mm self-tapping locking screws. Use locking screw drill guide and ensure screws are passing through intramedullary stem component.
Placement of modular endoprosthesis segment: 25. Place modular spacer between proximal and distal components and secure with bolts/locking
screw.
Closure and post-operative care: Lavage surgical site and close soft tissues in multiple layers. Radiograph immediately post-operatively. Place light padded bandage and recover from anaesthesia.

Minerva Access is the Institutional Repository of The University of Melbourne
Author/s:
Mitchell, Katherine Elizabeth
Title:
Metal endoprostheses for limb salvage surgery in dogs with distal radial osteosarcoma:
evaluation of first and second generation metal endoprostheses and investigation of a novel
endoprosthesis
Date:
2017
Persistent Link:
http://hdl.handle.net/11343/194248
File Description:
Metal endoprostheses for limb salvage surgery in dogs with distal radial osteosarcoma
Terms and Conditions:
Terms and Conditions: Copyright in works deposited in Minerva Access is retained by the
copyright owner. The work may not be altered without permission from the copyright owner.
Readers may only download, print and save electronic copies of whole works for their own
personal non-commercial use. Any use that exceeds these limits requires permission from
the copyright owner. Attribution is essential when quoting or paraphrasing from these works.