mi in ems: system response - emcongress.org · mi in ems: system response montreal rescu team ......
TRANSCRIPT

1
MI in EMS: system response
Montreal RESCU TeamAlain Vadeboncoeur MD et al.SITGES 2003
Disclosure : Dr Vadeboncoeur’s team have received grant from Roche
Objectives
Patient delay factor: what can be doneECG factor– On site ECG: should we implement it?– Transmitted ECG: is it effective?
Thrombolysis delay factor– Break the clot faster: how?– Lyse on site: why?
Reperfusion choice factor– PTCA vs Thrombolysis: which is the best?– Triage of patients: how for EMS?
EMS : a fast system responseThrombolysis
EM
PTCAHospital
ECG

2
Why fast?
Rapid revascularisation: key element– Thrombolysis: 60 000 randomized
patients against placebo, impact + on the mortality
– Delay of 60 to 90 minutes for peak effectBenefit: greater < 1 to 2 hours 30 minutes = 1 year of life saved…
» Rawles JM. Quantification of the benefit of earlierthrombolytic therapy: five-year results of the Grampian Region Early Anistreplase Trial (GREAT). Am J Coll Cardiol. 1997;30:1181.
Why fast?
Canadian RegistryFastrac II, 2000 (3523 patients): – D to D = 62 minutes (median)– Pain to D = 2,8 hours (median)– NHAAP program: small improvement
How fast are we?

3
Patient delay factor
Patient recognition phase still constitutes around 2/3 of total delayPatients with known ischemic disease have same delay times (median of 2.0 hours)
» 159. Goff DC Jr, Feldman HA, McGovern PG, et al: EMS delay in patients hospitalized with heart attack symptoms in the United States: The REACT trial. Am Heart J 138:1046-1057, 1999.
REACT study– targeted mass media, – community organizations, – professional, public, and patient education
20 American cities « matched »20 364 patients consulted at theemergency with final diagnosis of MI
Patient delay factor
+ 20% use of EMSPopulation consulted at the emergency: idem
» JAMA 2000 Jul 5;284(1):60-7
Intervention community
Reference community
p value
Decrease in delay time -4.7% -6.8% .54
Increase/decrease in EMS use per year
+16% - 3% < .005
Patient delay factor

4
ECG factor and AHA 2000
We recommend implementation of out-of-hospital 12-lead ECG diagnosis program in urban and suburban paramedic systems (Class I)
» Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, Part 7: The Era of Reperfusion. Section 1: Acute Coronary Syndrome. Circulation. 2000; 102(suppl I): I-175 - I-176.ECG
SCA vs. dynamic changes of ST2,665 patients (pre-thrombolysis phase)
Sensibility and specificity of ECG URG vs. PH+URG
0,34
0,96
0,46
0,93
0
0,2
0,4
0,6
0,8
1
SENS SPEC
%
URGPH+URG
ECG prehosp: reliabilityKudenchuk
ECG
ECG Prehosp: Security+ Delays or - Delays?
Gain on the timing of the diagnosticGain on the global delay of thrombolysis at the emergency ( ≈ 30 minutes)
vs.On site delay + ???– 0,3 minutes
» 23. Karagounis et al. Impact of Field-Transmitted Electrocardiography on time to in-hospital thrombolytictherapy in acute myocardial infarction.
» AM J Cardiol. 1990;66 :786-791.
ECG

5
Milwaukee EMS Chest Pain Project– acquisition + transmission of ECG– 439 patients – an increase in mean “on-scene time” of 4
minutes over a historical control group.MITI trial– 522 patients had transmitted ECG – estimated that the added time for acquisition
was 7 minutes compared to a historical control group
ECG Prehosp: Security+ Delays or - Delays?
ECG
Transmitted ECG : feasible?Grim: transmission of PH ECG comparing to the ED acquired ECG as a gold standard.Heart rate, QRS duration and axes, QT andQTc intervals, + complex morphologic patterns. No significant differences between both groups. No comparison of ST segmentSmall sample size (23)Non cardiac patients– Grim et al. Cellular Telephone Transmission of 12-
lead Electrocardiograms from Ambulance to Hospital. Am J Cardiol. 1987;60 :715-720.
ECG
– On 680 patients• Aufderheide TP et al.
Milwaukee EMS Chest Pain Project: phase I: feasibility and accuracy of EMS thrombolyticcandidate selection. Am J Cardiol. 1992;69:991-996.
Efficiency of the ECG Transmisson
0%
20%
40%
60%
80%
100%
Global 1 mois Plus tard
RéussiNon-réussi
Efficiency of the Transmission
0%
20%
40%
60%
80%
100%
Initiale Plus tard
RéussiNon-réussi
– Weaver WD et al. Myocardial Infarction Triage and Interventional Project-Phase I: patients characteristics and feasibility of EMS initiation ofthrombolytic therapy. J Am Coll Cardiol. 1990;15:925-931.
Transmitted ECG : feasible?
ECG

6
Failure Rate: 6% total> 60% land-line< 40% cellular phone (and problems)Portable ECG Machine + CellularsTechnology improvement?
» Welsch J. Communication personnelle. Présentation des données de Assent III-+ à l’Institut de cardiologie de Montréal.
Cellular phones: problematic (≈ 60% success)– Montreal data (to be published)
Transmitted ECG : how?
ECG
Thrombolysis delay factorHow to fast it all?–Acceleration of thrombolysis
at the emergency (prehospECG) ≈ - 30 minutes
–EMS Thrombolysis?
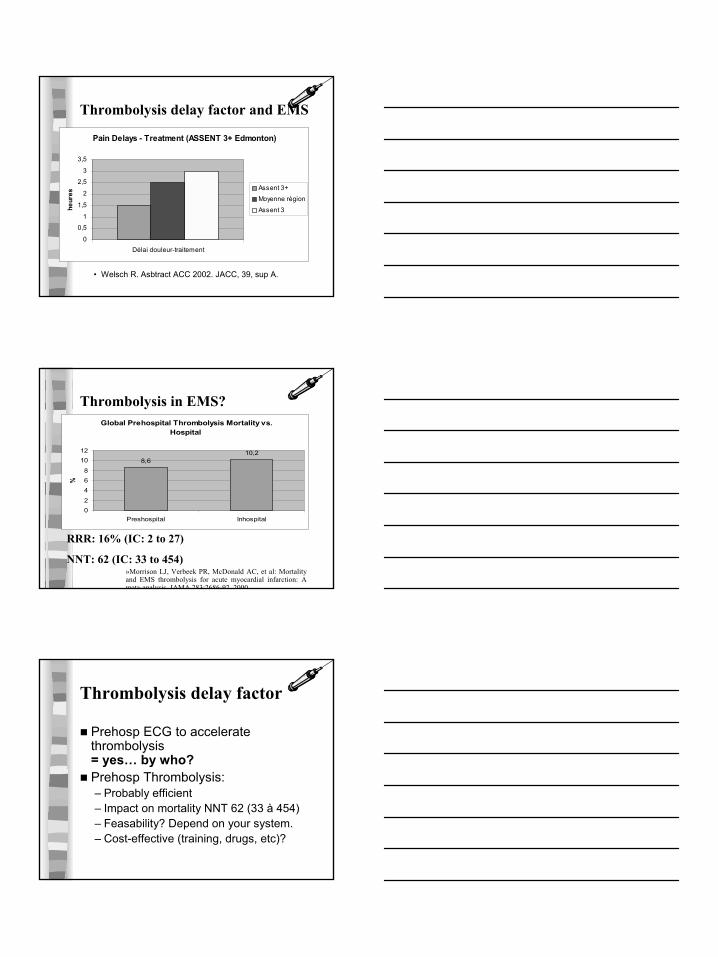
Thrombolysis delay factor and EMS
7
• Welsch R. Asbtract ACC 2002. JACC, 39, sup A.
Pain Delays - Treatment (ASSENT 3+ Edmonton)
0
0,5
1
1,5
2
2,5
3
3,5
Délai douleur-traitement
heur
es
Assent 3+Moyenne région
Assent 3
Thrombolysis delay factor and EMS
Global Prehospital Thrombolysis Mortality vs. Hospital
8,610,2
02
468
1012
Preshospital Inhospital
%
RRR: 16% (IC: 2 to 27)
NNT: 62 (IC: 33 to 454)»Morrison LJ, Verbeek PR, McDonald AC, et al: Mortality and EMS thrombolysis for acute myocardial infarction: A meta-analysis JAMA 283:2686-92 2000
Thrombolysis in EMS?
Prehosp ECG to accelerate thrombolysis = yes… by who?Prehosp Thrombolysis:– Probably efficient– Impact on mortality NNT 62 (33 à 454)– Feasability? Depend on your system.– Cost-effective (training, drugs, etc)?
Thrombolysis delay factor
8
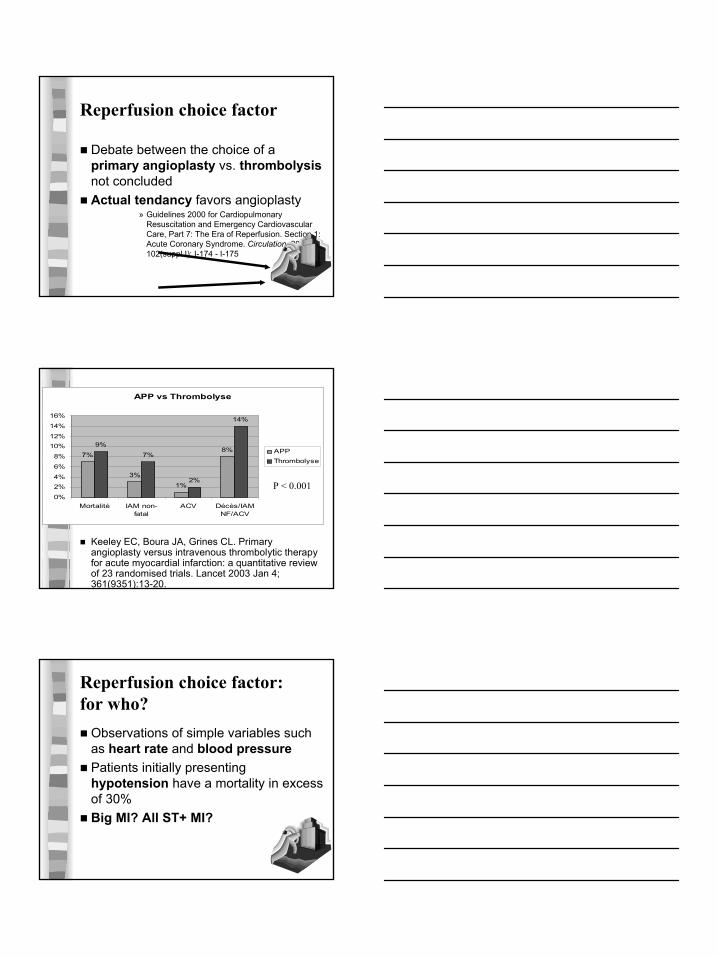
Reperfusion choice factor
Debate between the choice of a primary angioplasty vs. thrombolysisnot concludedActual tendancy favors angioplasty
» Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, Part 7: The Era of Reperfusion. Section 1: Acute Coronary Syndrome. Circulation. 2000; 102(suppl I): I-174 - I-175
APP vs Thrombolyse
7%
3%
1%
8%9%
7%
2%
14%
0%
2%4%
6%
8%
10%12%
14%
16%
Mortalité IAM non-fatal
ACV Décès/IAMNF/ACV
APPThrombolyse
Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapyfor acute myocardial infarction: a quantitative reviewof 23 randomised trials. Lancet 2003 Jan 4; 361(9351):13-20.
P < 0.001
Observations of simple variables such as heart rate and blood pressure Patients initially presentinghypotension have a mortality in excess of 30%Big MI? All ST+ MI?
Reperfusion choice factor: for who?
9
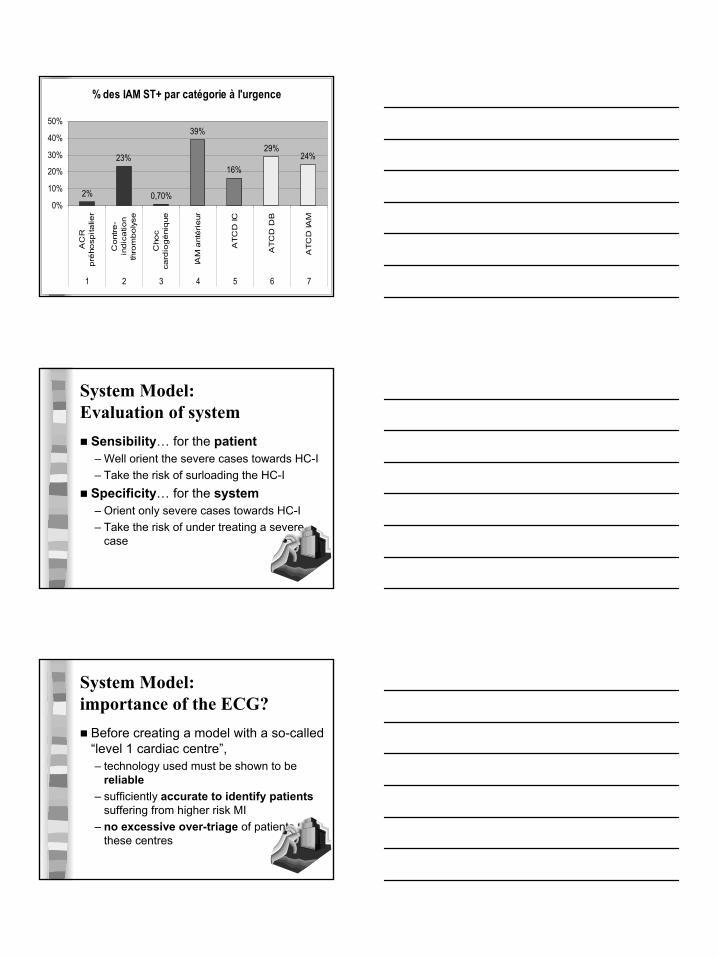
% des IAM ST+ par catégorie à l'urgence
2%
23%
0,70%
39%
16%
29%24%
0%
10%
20%
30%
40%
50%
AC
Rp
rého
spita
lier
Cont
re-
ind
ica
tion
thro
mbo
lyse
Cho
cca
rdio
gé
niq
ue
IAM
ant
éri
eur
AT
CD
IC
AT
CD
DB
AT
CD
IAM
1 2 3 4 5 6 7
System Model: Evaluation of system
Sensibility… for the patient– Well orient the severe cases towards HC-I– Take the risk of surloading the HC-I
Specificity… for the system– Orient only severe cases towards HC-I– Take the risk of under treating a severe
case
System Model: importance of the ECG?
Before creating a model with a so-called“level 1 cardiac centre”, – technology used must be shown to be
reliable– sufficiently accurate to identify patients
suffering from higher risk MI – no excessive over-triage of patients to
these centres

10
CAPTIM STUDY
Outcome EMSfibrinolysis
Primary angioplast
y
Risk difference (95% CI)
p
Composite end point
8.2% 6.2% 1.96 (-1.53-5.46)
0.29
Mortality 3.8% 4.8% -0.93 (-3.67-1.81)
0.61
Reinfarction
3.7% 1.7% 1.99 (-0.27-4.24)
0.13
Disabling stroke
1.0% 0 1.00(0.02-1.97
0.12
System model: where is the proof?
System Model of Prague
NNT: 12 14 NNT global: 7
– Widimsky P, et Al. : The PRAGUE Study. Eur Heart J, 21:823-831, 2000
Death, ACV or Re-infarctus: The Prague Study
0
5
10
15
20
25
Thrombolysecommunauté
Thrombolyse + centretertiaire
PTCA centre tertiaire
%
System Model: DANAMI-2
Fresh from press! NEJM August 2003Danemark24 general hospital an 5 University hospital centres of reference56 km on average between thesebuildings1572 patients, ST ↑Score ST ≥ 4 mm, less than 12 hours

11
System model: DANAMI
NNT: 18 18 17
DANAMI: Deaths, Re-infarctus and ACV
02468
10121416
Total Tertiaires Transferts
%
ThrombolysePTCA
System Model: DANAMI
NNT mortality: 100 NNT ACV: 111NNT: re-MI: 26
7,6
2
4,1
6,6
1,10,3
0
5
10
15
%
Thrombolyse PTCA
Actual Composition of the end-point of DANAMI
MIACVMortalité
System Model: DANAMI2.5% of patients had an episode of acute AF during transfer2.3% had 2-3 degree AV blockRescue PTCA rate of 2.5% (low)PCI group, 87% had balloon angioplasty, 89% achieved TIMI 3 flow, and of these 93% received a stent (« respect of the randomization »)

12
System Model: PTCA… in which hospital?
C-PORT: primairy PTCA in smallhospitals withous surgical backup = good?DANAMI: hospitals without experienceof PTCA in 3 cases out of 5Raises questions: Do we need on place surgery?
Thrombolysis EM
PTCAHospital
ECG
?
+ WHO?
+
$? + HOW?
Conclusions
Patient delay factor: desperate!ECG factor– On site ECG: YES?– Transmitted ECG: YES by landline?
Thrombolysis delay factor– ECG is good for this– Lyse on site: cost-effective?
Reperfusion choice factor– Go for PTCA?– Bring the right patient at the right place?

13
Questions… at the end of presentation